
Abstract
Purpose:
To present our early experience with retroperitoneal laparoendoscopic single-site (LESS) simple nephrectomy.
Patients and Methods:
A total of 16 patients with benign nonfunctioning kidney underwent retroperitoneal LESS nephrectomy by one experienced laparoscopic surgeon. A single-port access was inserted through an approximately 3-cm lumbar incision made below the 12th rib along the midaxillary line. Standard steps of multisite retroperitoneoscopic nephrectomy technique with a combination of conventional and bent laparoscopic instruments were performed.
Results:
Retroperitoneal LESS nephrectomy was performed in 15 cases successfully. The procedure of one patient (genitourinary tuberculosis) needed conversion to open surgery because of the severe adhesions surrounding the kidney, which resulted in failure to progress. Overall, the mean operative time was 85 (75–140) minutes, and estimated blood loss was 56 (20–110) mL. The mean time to resume oral diet was 1.5 days. The mean postoperative hospital stay was 4 (3–5) days. Perioperative complications were limited to one case of transient postoperative fever. No major intraoperative and postoperative complication occurred.
Conclusions:
Retroperitoneal LESS nephrectomy performed by an experienced laparoscopic surgeon is feasible and safe, offering improved cosmesis, although it remains technically challenging. Retroperitoneal LESS nephrectomy should be selectively used in terms of patients' specific conditions.
Introduction
Current attempts to reduce the morbidity of laparoscopic surgery and improve cosmetic outcomes focus on reducing the total number of necessary skin incisions for trocar positioning. Early clinical experiences have demonstrated the feasibility as well as the safety and successful completion of laparoendoscopic single-site (LESS) surgery for some urologic procedures, where multiple laparoscopic instruments are placed through a single abdominal incision. 2 –12
To the best of our knowledge, because of a small working space and difficulty in anatomic orientation by the retroperitoneal approach, there has been very limited experience with retroperitoneal LESS for nephrectomy. 3,4 In this study, we report our initial experience with retroperitoneal LESS nephrectomy with a combination of conventional and bent laparoscopic instruments.
Patients and Methods
From March 2011 to August 2011, a total of 16 consecutive patients with benign nonfunctioning kidney underwent retroperitoneal LESS simple nephrectomy by one experienced laparoscopic surgeon. The 16 cases comprised 9 men and 7 women with an average age of 41.5 years (range 36–58 y); their average body mass index (BMI) was 25.7 kg/m2 (range 20.6–29.1 kg/m2). The indications for nephrectomy were nonfunctioning kidney associated with ureteral stone (n=4), pelvic stone (n=7), ureteropelvic junction obstruction (n=4), and genitourinary tuberculosis (n=1).
This study obtained informed consent from the patients and ethics approval from the ethics committee at Xiangya Hospital, Central South University. The parameters were retrospectively collected, including the operative time, estimated blood loss, complications, conversion to standard laparoscopy or open surgery, time to resume oral diet, and length of hospital stay.
Operative technique
Under general endotracheal anesthesia, the patient was placed on a maximally flexed table to extend the ipsilateral flank in the full lateral decubitus position. An approximately 3-cm transverse skin incision was made below the 12th rib along the midaxillary line (Fig. 1). The muscular layer and lumbodorsal fascia were bluntly divided using vascular forceps, and then an index finger was inserted to bluntly separate the retroperitoneal space as far as possible. A homemade balloon dissector was placed into the initial retroperitoneal space, and 300 to 400 mL physiologic saline was slowly infused to maintain the balloon dilation for 3 to 5 minutes. The saline was then evacuated, and the balloon dissector was removed.

An approximately 3-cm transverse skin incision was made below the 12th rib along the midaxillary line (right side).
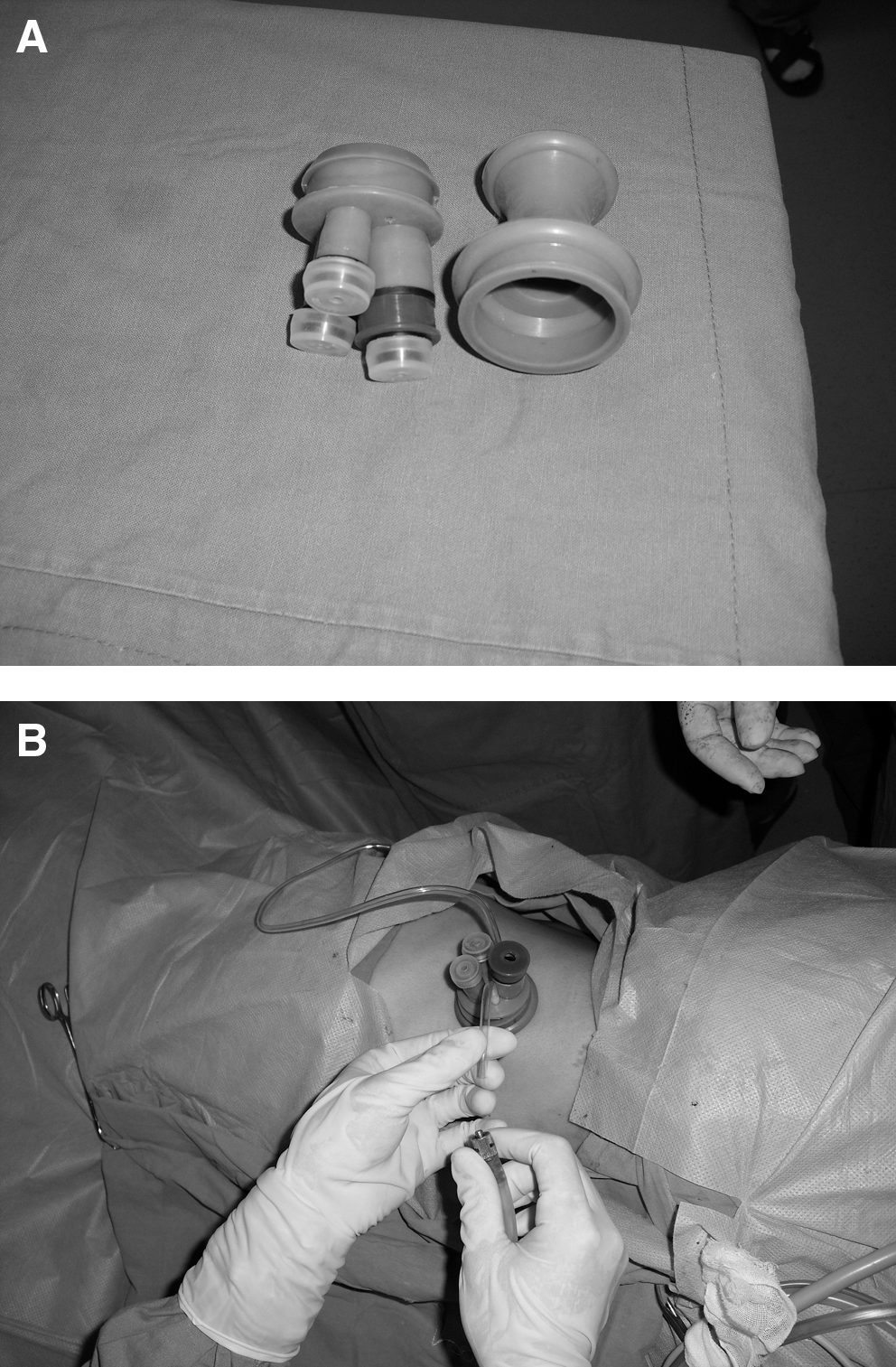
A single-port access was inserted through the lumbar incision (Figs. 2A, 2B). Pneumoretroperitoneum was established with the intraretroperitoneal pressure of 12 to 14 mm Hg. The standard retroperitoneal nephrectomy technique was performed with a combination of conventional and bent laparoscopic instruments (Fig. 3). Urine from hydronephrotic atrophic kidneys was aspirated before the specimen was put into the homemade laparoscopic bag. If needed, the incision was extended after the port was removed (the length of the incision was determined by the expected size needed for the specimen to be removed). Then the specimen was retrieved through this incision. A 22F suction drainage was placed in the renal fossa through the incision for observation of potential postoperative hemorrhage. Then the incision was closed in layers (Fig. 4).

The standard retroperitoneal nephrectomy technique was performed with a combination of conventional and bent laparoscopic instruments.

A 22F suction drainage was placed in the renal fossa through the approximately 3-cm incision.
Results
Retroperitoneal LESS nephrectomy was performed successfully in 15 patients. The procedure of one patient (genitourinary tuberculosis) needed conversion to open surgery because of the severe adhesions surrounding the kidney, which resulted in failure to progress. Overall, the mean operative time was 85 (75–140) minutes, and estimated blood loss was 56 (20–110) mL. The mean time to resume oral diet was 1.5 days. The mean postoperative hospital stay was 4 (3–5) days. Perioperative complications were limited to one case of transient postoperative fever. No major intraoperative and postoperative complication occurred.
Discussion
The traditional laparoscopic nephrectomy usually uses three to six ports. Although port-site morbidity is typically low and often not a problem for the patient, each additional port may result in a consequent potential risk of bleeding, infection, concordant organ damage, incisional hernia, pain, multiple scar formation, and compromised cosmetic outcome. 2,3 To further decrease the morbidity associated with laparoscopic surgery, an increasing enthusiasm has emerged for LESS surgery by consolidating all ports through a single incision. 2 –12
Because surgical instruments were placed in parallel, the major problems performing LESS nephrectomy were lack of triangulation, lack of additional assistant trocars for retraction, and the crowding of instruments outside the port and in the operative field. These made this surgical procedure a technical challenge, especially if there was no appropriate “bendable” type laparoscopic instrument. 2,13
In our experience, intensive experience with performing traditional urologic laparoscopy is essential before embarking on single-site surgery. Furthermore, surgeons should be familiar with the benefits and limitations of newly available surgical instrumentation. Because using at least one bent instrument was able to offset the shafts adequately to accomplish a satisfactory degree of triangulation, we advocated using one bent instrument and one straight instrument to minimize the impact of the instruments because of the lack of triangulation, thus easing the dissection. Also, clashing of instruments outside may be avoided by the combination of conventional and bent instruments because these instruments have different lengths.
Although intra-abdominal sutures fixed to the parietal peritoneum or transcutaneous sutures grasped with extracorporeal handling was suggested to provide retraction, 5 neither of those methods was used in our procedure. In our experience, it was very important to keep the integrity of the peritoneal envelope for the good exposure of the surgical field.
LESS can be completed through a single incision, either by a transperitoneal or retroperitoneal approach. The transperitoneal approach, often concealed at the umbilicus, is typically used. 6 –12,14 –16 To our knowledge, although the reported retroperitoneoscopic LESS nephrectomy remained very limited, this procedure has been proven to be technically feasible 3,4 and to provide adequate flexibility and spacing of port placements as well as acceptable operative outcomes. 3
A study by Ryu and associates 4 included 14 successful cases of retroperitoneoscopic LESS surgery, although only 3 of them underwent nephrectomy. Recently, Chueh and coworkers 3 performed their initial retroperitoneoscopic LESS nephrectomy (n=8); They used the GelPOINT apparatus as an access platform, and the median operative time was 164 (87–198) minutes and median estimated blood loss was 50 (10–200) mL. The median length of hospital stay was 2 (1–3) days.
The retroperitoneal approach has the disadvantages of the limited working space over the transperitoneal approach. 13 This retroperitoneal approach for LESS nephrectomy, however, offers various obvious advantages. First, it provides a shorter distance from the incision to the kidney, without mobilization of intraperitoneal organs or retraction of organs, such as the spleen or liver. Furthermore, the distance and angle to dissect the upper pole of the kidney are much easier. 3 In contrast, the transperitoneal transumbilical approach usually makes the laparoscopic instrument hard to reach the upper pole of the kidney, especially in the kidney with a larger hydronephrosis.
Second, the retroperitoneal approach allows early and direct access to the renal hilum and thus facilitates dissection of the renal hilum. Finally, because the retroperitoneal approach does not violate the peritoneal cavity, it reduces the risk of spillage of the contents from the hydronephrotic kidney into the peritoneal cavity. 17,18 Therefore, the retroperitoneoscopic LESS approach offers an alternative to the patients with suspected infection of hydronephrotic kidneys or the patients with previous transperitoneal surgery.
To overcome the disadvantage of the limited working space, in our experience, the retroperitoneal fat and adjacent tissues outside of he Gerota fascia should be routinely dissected and removed to widen the initial working space. Although the retroperitoneum initially affords a significantly smaller working space than the peritoneal cavity, as the dissection proceeds, the retroperitoneal space can be readily enlarged and developed as necessary. 19
Compared with the transperitoneal transumbilical approach, the retroperitoneal approach may compromise the cosmetic benefit. When compared with traditional retroperitoneoscopic surgery (one port vs at least three ports), however, retroperitoneoscopic LESS nephrectomy still has an obvious advantage with respect to cosmetic outcome, although the three-port retroperitoneoscopic surgery often results in only one extraction incision and another 5-mm port site and thus minimizes this benefit. In fact, our patients who underwent surgery with only a single lumbar access were highly satisfied with the cosmetic outcome.
It was worth noting that although the potential advantages of LESS could be the reduced port-related morbidity (eg, trocar incision hernia and bleeding from the trocar tract), decreased postoperative pain, and faster recovery, 20 those are just theoretical and have not been proven to date. Raman and colleagues 7 reported a retrospective case-control study comparing 11 LESS nephrectomies and 22 conventional laparoscopic nephrectomies. Their results showed that there was no difference between single-incision laparoscopic surgery and conventional laparoscopy cases in the median operative time, changes in the hemoglobin levels, analgesic use, length of hospital stay, and complication rate. Therefore, additional studies are very necessary to further evaluate whether patients undergoing retroperitoneal LESS surgery have improved perioperative outcomes compared with those undergoing standard retroperitoneoscopic surgery, especially with regard to the reduced port-related morbidity.
There is no doubt that LESS is more technically challenging than traditional laparoscopy, 21 especially through a retroperitoneal approach. Therefore, we believe that LESS nephrectomy should be selectively used. Because the thick abdominal wall interferes with the instruments and restricts their movement, obese patients present a more technical challenge in LESS as other investigators have reported. 4,20,21 Therefore, patients with a BMI>30 in our center were not included in our preliminary attempts at retroperitoneoscopic LESS surgery.
Our opinions were similar to that of Mir and coworkers 22 who reported that LESS influenced patient selection by creating a selected cohort that had lower BMI and were more likely to be undergoing surgery for benign indications. In our experience, the younger patients or the patients with benign renal diseases seem to focus on cosmetic outcomes and preferred to choose LESS, while the older patients or the patients with malignant renal diseases preferred to choose traditional laparoscopy in hopes of avoiding the additional technical challenges of LESS.23 In our series, the procedure of one patient (genitourinary tuberculosis) necessitated conversion to open surgery because of the severe adhesions surrounding the kidney. Therefore, we believe that LESS surgery should be avoided in the patients who were expected to have severe adhesions in the retroperitoneum.
The limitation in our study was that an extraction incision has not been measured and reported for objectively proving the advantage of cosmetic outcome in the retroperitoneal LESS surgeries. In subsequent procedures, the data of the incision length will be collected.
Conclusions
Retroperitoneal LESS nephrectomy performed by an experienced laparoscopic surgeon is feasible and safe, offering improved cosmesis, although it remains technically challenging. Retroperitoneal LESS nephrectomy should be selectively used in terms of patients' specific conditions.
Footnotes
Disclosure Statement
No competing financial interests exist.