
Abstract
Purpose:
To investigate a modified laparoscopic retroperitoneal lymph node dissection technique using an extraperitoneal approach and to evaluate its feasibility.
Patients and Methods:
A group of consecutive patients from a single institution underwent extraperitoneal laparoscopic retroperitoneal lymph node dissection (EL-RLND) at weeks after orchiectomy for primary testicular nonseminomatous germ cell tumors (NSGCT). All patients were placed in the supine position and tilted up 15 degrees on the affected side. Four trocars were introduced. The templates of lymph node dissection conformed to those of Weissbach and Boedefeld.
Results:
EL-RLND was successfully performed in 15 patients (left, 6 patients; right, 9 patients). The mean total operative time for the entire series was 164±49 minutes. The mean blood loss was 118±74 mL. One intraoperative complication was injury of the vena cava, which occurred in one patient. Ureteral obstruction occurred in another patient. The mean postoperative intestinal function recovery time was 2 days. The mean postoperative hospitalization was 5.5±1.1 days. Normal antegrade ejaculation was preserved in all patients. Pathologic studies revealed positive lymph nodes in three (20%) patients. No recurrence or distant metastasis occurred during 2 to 32 months of follow-up.
Conclusions:
EL-RLND is a safe and feasible procedure using an improved extraperitoneal approach that provides minimal invasion and rapid recovery of patients.
Introduction
Patients and Methods
Clinical information
Between July 2008 and March 2011, 15 consecutive patients with primary testicular NSGCT underwent EL-RLND at 27±5 days after orchiectomy (6 on the left side and 9 on the right side). Pathologic studies of testicular tumors after orchiectomy revealed eight embryonal carcinomas, five spermatocytomas combined with embryonal carcinoma, one yolk sac tumor, and one embryonal tumor combined with an immature teratoma. All patients underwent preoperative examinations including ultrasonography of the abdomen and retroperitoneum, CT of the chest and abdomen, and serum tests for tumor markers of fetoprotein and human chorionic gonadotropin; results were negative in all cases. Clinical staging showed stage I in 11 patients and IIa in 4 patients.
Patient preparation
Mechanical bowel preparation using an osmotic laxative was performed in all patients. Clysters were administered before surgery. Intravenous antibiotics were administered at induction of general anesthesia.
Follow-up
Postoperatively, patients were reviewed at 2 weeks, 1 month, 3 months, and every 6 months thereafter by a urologist from the research team responsible for the evaluation of laparoscopic technology. The contralateral testicle was palpated at each follow-up examination. Assessment of serum tumor markers, chest radiography, and CT of the abdomen was performed at each visit.
Technique of EL-RLND
Patient positioning
The patients were placed in the supine position and tilted up 15 degrees on the affected side. The surgeon stood ipsilateral to the tumor, next to an assistant who held the camera. Another assistant stood on the opposite side. A video monitor was also placed on the opposite side near the patient's head to provide a comfortable view for each operator (Fig. 1-A).
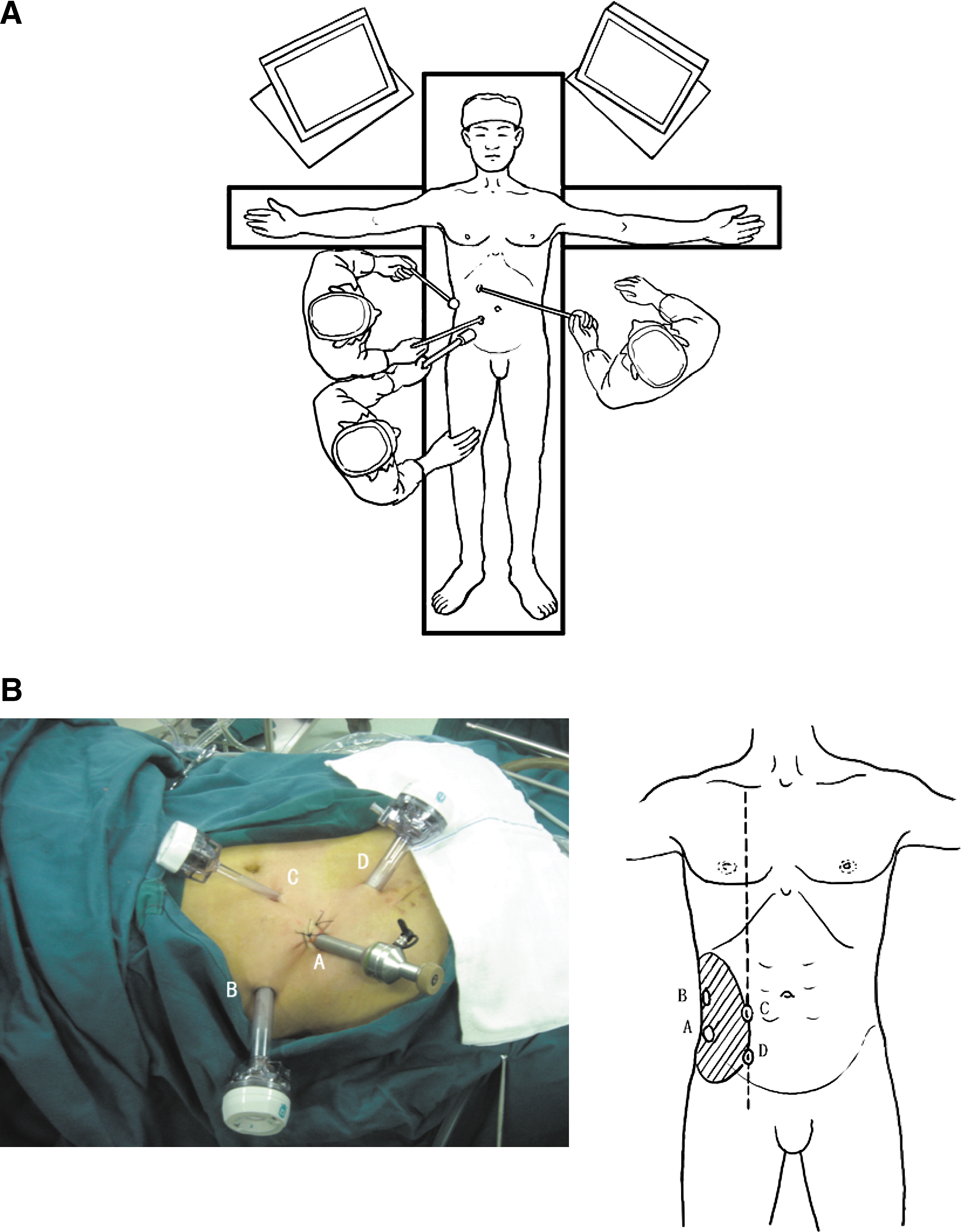
Trocar placement
A 1.5-cm abdominal incision was made ipsilateral to the tumor and 2 cm medial to the anterosuperior iliac spine. The various muscular layers were bluntly divided along their fibers until the extraperitoneal space was accessed. The peritoneum was pushed inward with the forefinger through the incision. A self-made balloon was then inserted into the space and inflated with 900 mL of gas to create an extraperitoneal space. The balloon was dislodged, and a 10-mm trocar (trocar A) for the lens was placed in the incision. Pneumoperitoneum was created with a pressure of 15 mm Hg.
Under monitoring, a 12-mm operative trocar (trocar B) was introduced into the extraperitoneal space of the flank on the midaxillary line midway between the 11th rib and iliac crest. The lateral peritoneum was then separated from the parietal muscles using an elastic separating plier cephalic enough to introduce another two trocars into the extraperitoneal space. Two 12-mm operative trocars (trocars C and D) were placed at the lateral rectus abdominis (Fig. 1-B).
Laparoscopic procedures
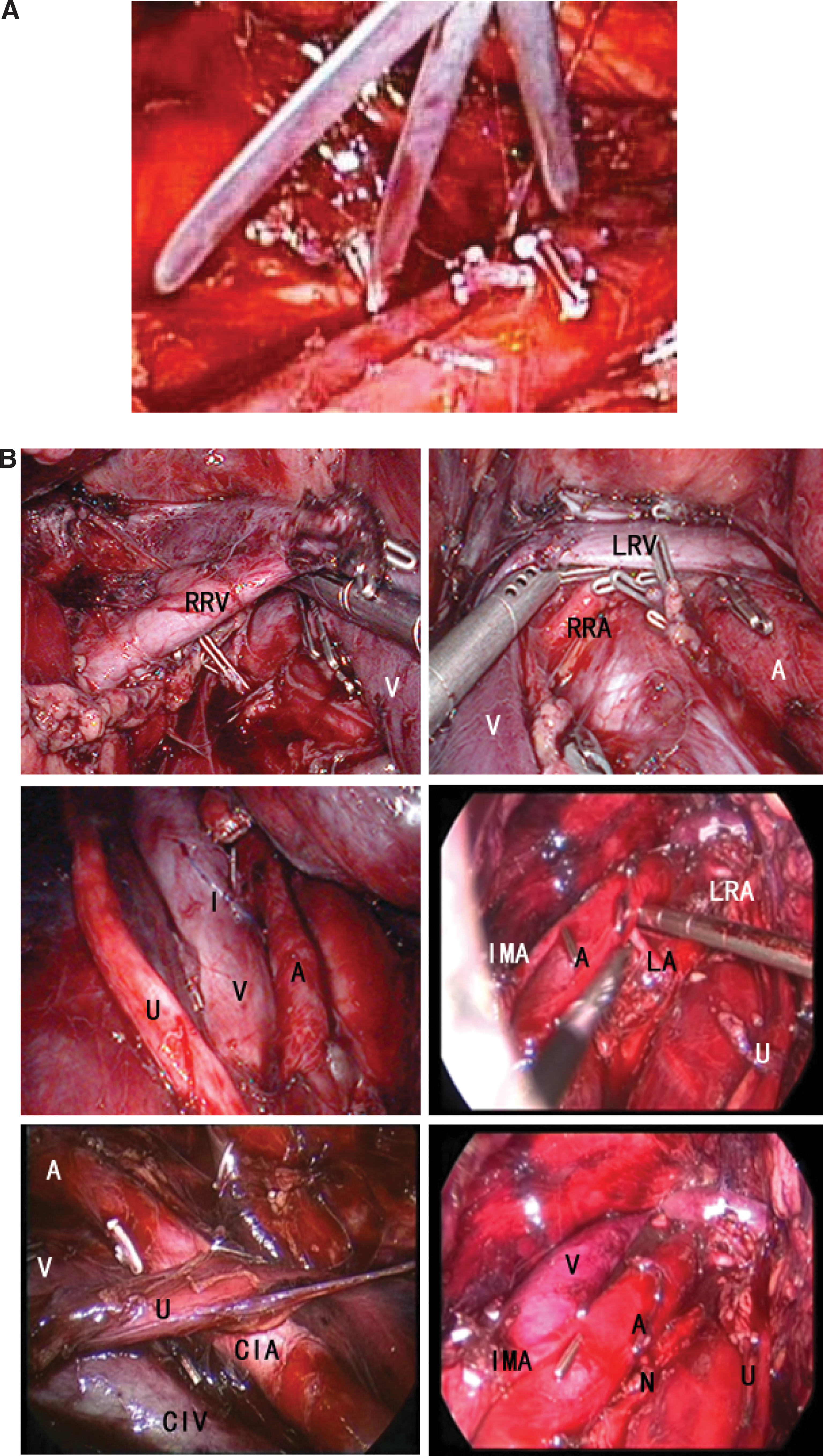
On entering the extraperitoneal space, extraperitoneal fat was removed with a harmonic scalpel. The extraperitoneal space was created by pushing the peritoneum medially until the ureter was visible and the ipsilateral great vessel was reached (Fig. 2-A). The remnant seminal duct was dissected. The templates of lymph node dissection conformed to those of Weissbach and Boedefeld.
Right EL-RLND
Blunt and sharp dissection started from the surface of the psoas muscle to free the lateral and anterior aspects of the vena cava. Tissues posterior to the vena cava were then removed to access the interaortocaval nodes and facilitate dissection along the prevertebral plane. Interaortocaval dissection continued proximally to the left renal veins and right renal artery. Particular care was taken to avoid injuring the lumbar vessels on the posterior side and renal vessels on the cranial side. The main postganglionic nerves from the second or third right sympathetic ganglia were preserved. Finally, the right common iliac nodes were excised distal to its bifurcation.
Left EL-RLND
The lymphatic tissues were gently separated off the aorta by blunt and sharp dissection. To minimize the risk of sexual problems, the anterior aortal aspect below the origin of the inferior mesenteric artery was identified instead of isolated to protect the superior hypogastric plexus. At the same time, lymph nodes around the left sympathetic chain and main postganglionic fibers were carefully dissected using suction and removed (Fig. 2-B). Division of the lumbar vessels was not obligatory and retrovascular lymphadenectomy might process between lumbar pedicles. Proximal dissection was carefully performed around the left renal vein, and the large interaortocaval lymphatic trunks were ligated with clips and divided.
Resection of gonadal vessels and final steps
The gonadal vein was freed from the distal ligated part and transacted proximal to the renal vein on the left side and vena cava on the right side. At the end of the procedure, the gonadal vessels and resected lymph nodes were placed in an endoscopy bag and extracted from the extraperitoneal cavity through the trocar.
Results
Perioperative parameters
EL-RLND was completed successfully in all patients with no conversions to open surgery. The nerve-sparing technique was used in all patients. Preoperative details are summarized in Table 1. The mean age±standard deviation (SD) was 30.3±5.1 years. The intraoperative and postoperative details of patients are presented in Table 2. The mean total operative time±SD for the entire series was 164±49 minutes. This was the time from the first skin incision to closure of the final incision. The mean blood loss±SD was 118±74 mL; no patient needed a blood transfusion. All patients were able to get out of bed on the second postoperative day. The mean postoperative intestinal function recovery time was 2 days. There was no chyliform drainage, and drainage tubes were removed on the third postoperative day. The mean postoperative hospitalization time±SD was 5.5±1.1 days.
S/E: spermatocytoma/embryonal carcinoma; E/I: embryonal/immature teratoma.
CS=American Joint Committee on Cancer clinical stage.
Histopathologic results
A mean±SD of 19±2.1 lymph nodes were retrieved during EL-RLND. Lymph node metastases were detected in three (20.0%) patients, and 10 positive lymph nodes were confirmed through pathologic studies. Four and two positive lymph nodes were located in the paracaval region in two patients, respectively, and four positive lymph nodes were preaortic in the other patient. Pathologic stage conformed to the clinical stage (Tables 1 and 2).
Complications
The complication rate was 13.3% as summarized in Table 3. Injury of the vena cava occurred in case 1. The injury was controlled with suturing (Fig. 2-B). Ureteral obstruction occurred in case 4, and open ureteroplasty was performed 2 weeks after the operation. There were no trocar-site metastases in the series. Lymphocele and intestinal injuries were absent in all series (Table 2).
Oncologic and functional follow-up
At a mean follow-up of 17.4 (range, 2–32) months, normal antegrade ejaculation and erection were seen in all patients. All patients were alive and did not receive adjuvant therapy. Periodic ultrasonography and CT revealed no recurrence or distant metastasis. Ultrasonography and urography for patients with ureteral obstruction 6 months after open ureteroplasty revealed no restricture.
Discussion
Most LRLNDs have been performed via a transperitoneal approach, including robot-assisted LRLND. 7,8 By comparing LRLND with open surgery, some scholars 9 have suggested significant advantages associated with LRLND, such as fewer injuries and complications of paralysis and bowel adhesion, quicker postoperative recovery, shorter hospitalization, and higher quality-of-life score.
LeBlanc and associates 6 reported their exploration of LRLND via an extraperitoneal approach, which avoided interference with abdominal organs and obtained better exposure. The extraperitoneal approach preserves the integrity of the peritoneum, avoids spillage of blood into the abdominal cavity. Compared with the transperitoneal approach, it further decreases complications of injury to surrounding visceral organs, bowel paralysis, adhesion, and ejaculatory disorders. In addition, we made some modifications to improve the extraperitoneal approach, which could preserve the peritoneum and provide better exposure of the retroperitoneal space for manipulation around the great vessels to guarantee adequate boundaries for lymph node dissection.
One of the modifications involves trocar placement, which is essential for the whole process. Appropriate placement of trocars facilitates exposure and manipulation. Trocars B, C, and D should be placed under screen monitoring to avoid penetrating the peritoneal cavity. In our study, blunt finger dissection, balloon dilation, and instrumental separation were obligatory steps for a well-preserved peritoneum. Perforation or laceration of the peritoneum during placement of trocars and intraoperative manipulation may lead to leakage of carbon dioxide into the abdominal cavity, and a lap-retractor is needed for a sustained space.
Through Trocar C, a fan-shaped retractor operated by an assistant was applied. The laparoscopic fan-shaped retractor is an ideal instrument for intraoperative exposure (Fig. 2-A). It serves as a brace to effectively hold the peritoneum and abdominal organs and provides an adequate working space. We performed the operations using this lap-retractor in case of peritoneum perforation. Consequently, bilateral renal vessels and the bifurcations of the iliac and inferior mesenteric arteries were clearly exposed during the surgical procedure (Fig. 2-B).
Some controversies exist in terms of the extent of RLND. Most scholars adopt the extent of open-RLND raised by Weissbach and Boedefeld. 10,11 Janetschek and colleagues 12 performed LRLND according to these boundaries and suggested different extents in different stages of NSGCT. It is difficult to expose the contralateral renal veins and abdominal aorta from the right side and the vena cava from the left side by a traditional extraperitoneal approach. In our study, the aorta from the right side and the vena cava from the left side were clearly exposed, and the preaortic/cava nodes and nodes between the two major vessels were successfully removed using our modified approach with the fan-shaped lap-retractor. Therefore, our approach is well adapted for clinical stage I and II NSGCTs.
With our modified technique, high surgical efficiency was achieved with a mean operation time of 164 minutes, which was significantly less than that in other studies, and increased intraoperative complications did not occur (Table 2). Our surgical approach can sufficiently expose the surgical field, make the operation more convenient, and shorten the operative time. This was especially evident after the first five patients in the early exploratory stage; the surgical operative time of the subsequent 10 patients did not exceed 170 minutes, and the shortest was only 90 minutes.
We think several factors may contribute to the less operative time than others in literature. One lies on our familiarity with retroperitoneal anatomy. We routinely take the retroperitoneal approach for the surgery of he kidney and ureter, and we accumulated abundant experience. The second factor is our modified trocar placement and techniques involving creating the retroperitoneal space that facilitate our retroperitoneal exposure. Finally, we could deal with complications of major vessels injury laparoscopically efficiently because of our sufficient experience on extended pelvic lymphadenectomy during radical cystectomy and retroperitoneal lymphadenectomy during radical nephrectomy.
Vascular injuries and ureteral obstructions were two major complications in our study. A meta-analysis of LRLND by Kenney and Tuerk 13 revealed that vascular injury and hemorrhage occurred in 2.2% to 20% of reported cases, respectively, which were the most common intraoperative complications. Table 3 shows that severe bleeding occurred in some studies. 14 –16 In our experience, hemostasis can be obtained with a harmonic scalpel when dissecting around large vessels. Small branches of the vena cava can be clipped with titanium clips and transacted to prevent severe bleeding. Gentle pulling of the vena cava is needed for posterior dissection, and tearing of the lumbar vein or artery necessitates immediate clipping.
Large vessel injury (eg, vena cava) may be compressed with gauze, and hemostasis is established by exposing the bleeding part with an aspirator, then closing the rupture with clips or 5-0 polypropylene suture. In our series, bleeding from cava branches was successfully controlled by suturing. This injury of the vena cava occurred in case 1, the first case that we used the extraperitoneal approach for lymph node dissection. This complication is because of our limited experience for the initial attempting. The vena cava injury, however, was repaired successfully, and none of the major vessel complications occurred in the following 14 cases. It proved that the technique is feasible and safe when we have become familiar with this approach.
Bowel injury in LRLND is an infrequent but potentially catastrophic complication. 16 In our practice, bowel injury is avoided when the peritoneum is pushed aside with a fan-shaped retractor.
Reported rates of retrograde ejaculation after LRLND are <5%, but rates of retrograde ejaculation of up to 12.5% have been reported in postchemotherapy LRPLND. 17 A nerve-sparing technique for postoperative ejaculatory function was used for the patients in our series; retrograde ejaculation did not develop in any patient. Preservation of lumbar vessels during posterior dissection, blunt dissection with an aspirator to protect sympathetic chains, and preservation of the hypogastric plexus and postganglionic sympathetic fibers contributed to normal antegrade ejaculation. 13,18 We used titanium clips or a Hem-o-lok to block major lymphatic vessels before excision to minimize complications of chylous ascites and lymphoceles. 15,19,20 These complications were not observed in our study.
Postoperative ureteral obstruction occurred in one patient who presented with progressive hydronephrosis, and a second operation was performed. Postoperative ureteral obstruction may have been caused by retroperitoneal adhesion surrounding the ureter, leading to kinking or torsion. Regional ischemia caused by excessive dissection along the ureter may have also played a role. As a result, we inserted a Double-J stent under cystoscopy before the operation in the next six patients and removed it 2 to 3 weeks postoperatively. With accumulation of experience, however, we found that preoperative Double-J tube stent placement was not necessary. It should be noted that surrounding ureter tissues should not be totally excised intraoperatively for an adequate blood supply to its midpart. If ureteral injury occurs, an endoprosthesis might be needed before suturing the wound. Double-J tube stent placement was not performed in the last four patients, and they both recovered well. No ureteral complications occurred in the last 10 patients.
For the patients with positive nodes, we had more active surveillance than for those with negative nodes, including more frequent tumor marker detection and abdominal CT scan. During the period of follow-up, we had not found any recurrence within the template or distant site.
Conclusion
Our modified EL-RLND technique simplified the complicated LRLND procedure and was proven to be safe, effective, and promising based on our initial lymph node assessment in early-stage testicular NSGCT.
Footnotes
Disclosure Statement
No competing financial interests exist.