
Abstract
Purpose:
We present our single-center experience with three patients who were undergoing laparoendoscopic single-site (LESS) diverticulectomy through a single-port device introduced directly into the bladder.
Patients and Methods:
During March and April 2011, we operated on three men aged 62 to 76 years (mean 67 y) for symptomatic bladder diverticula using a standard lithotomy position and general anesthesia. The procedure was performed transvesically (percutaneous intraluminal approach) with a single-port device (four-channel) via a 1.5-cm incision made 2 cm above the pubic symphysis. Standard 10-mm optic and rigid laparoscopic instruments were used. The defect of the bladder wall was closed with an absorbable 3/0 running V-Loc suture. An 18F Foley catheter was left for 4 to 7 days.
Results:
The average operative time was 128 minutes (range 80–175 min). The blood loss was minimal. Patients were discharged on the third postoperative day with no intra-, nor postoperative complications. The 3-month follow-up confirmed good operative results in all cases.
Conclusion:
We consider laparoendoscopic single-port transvesical excision of bladder diverticulum as a feasible and safe procedure and a valuable treatment option for bladder diverticulectomy.
Introduction
Surgical management of bladder diverticula includes open, endoscopic, laparoscopic, and robot-assisted techniques. The feasibility, safety, and efficacy of these approaches have been reported and confirmed in the literature. 2 –5 The use of standard laparoscopy for transvesical access, for either diverticulectomies or other bladder disorders, has been described by numerous investigators. 4 –6
Further attempts to reduce the morbidity related to laparoscopic surgery have led to the emergence of techniques that consolidate multiple laparoscopic trocars through a single incision.
Recently, a series of four cases of laparoendoscopic single-site (LESS) transperitoneal bladder diverticulectomies have been reported. 7 Moreover, a percutaneous transvesical single-port access was developed by Desai and associates 8,9 and seems to be an attractive, minimally invasive alternative to either open or laparoscopic surgery for various lower urinary tract disorders. 9 –11
We present our initial experience with diverticulectomies using the LESS approach made directly to the bladder. The advantages of this method are minimal tissue manipulation, the availability of urethral access, the use of standard laparoscopic equipment, good clinical exposure, and the relatively short operative time. The disadvantages are the relatively limited operative space, instrument clashing, and possible gas leakage, especially when the multichannel port is torn.
This pilot study reports the feasibility and favorable outcomes of the method, similar to other recent, minimally invasive techniques.
Patients and Methods
From March to April 2011, three men with a mean age of 67 years (range 62–76 y) were operated on for bladder diverticula with the use of the LESS transvesical technique. All procedures were performed by one experienced laparoscopist. The patients presented typical histories of benign prostatic hyperplasia with a PVR of >80 mL, but not a significant obstruction, according to urodynamic results (Table 1). They previously underwent standard therapies with alpha-blockers with a favorable response; therefore, they were advised to continue this treatment. In two of them, the diverticula were associated with recurrent UTIs. They experienced treatment failure with numerous series of antibiotics. We considered carefully the potential role of bladder outlet obstruction for UTIs in patients 1 and 2, but our preoperative diagnostic findings (uroflowmetry, ultrasonography) confirmed a major role of the diverticula in the pathophysiology of the disease.
BMI=body mass index; Qmax=maximum flow rate; PVR=postvoid residual; UTI=urinary tract infection; TCC=transitional-cell carcinoma.
In the third patient, an intradiverticular nonmuscle-invasive, low-grade urothelial tumor was previously treated unsuccessfully with transurethral resection.
The diagnosis was made by ultrasonography, followed by cystoscopy or intravenous urography. We considered whether to perform voiding cystourethrography preoperatively, although this is not our routine procedure in such patients. Nevertheless, both the urographic and ultrasonographic examinations showed clearly the significant PVR volume of urine, and the urinary flow rates were relatively good. We then refrained from performing the additional radiologic examination.
The median diameter of the diverticula was 5.3 cm (range 5–6 cm). The average PVR volume was 110 mL (range 80–150 mL), and the average maximum flow rate was 17.7 mL/s (range 15–21 mL/s). We assessed that significant and even greater amounts of residual urine were observed in diverticula than in the right bladder. Therefore, we assumed that diverticulectomy should decrease significantly the PVR volume and might even improve the bladder contractility, as described by Adot Zurbano and colleagues. 12 Thus, it might result in more effective emptying of the bladder. 13
The patients were certain candidates for standard open or laparoscopic surgery. In this group, we applied the same indications for diverticulectomy that we had used in previous patients. In such cases during the last 2 years, we have performed transvesical laparoscopic diverticulectomy, according to the technique described by Pansadoro and coworkers. 5 Therefore, the transvesical access was well recognized by and familiar to our team.
Nevertheless, because our team had performed several LESS transvesical operations (including eroded polypropylene tape removals and ureteral reimplantation) over the previous year, we decided to use this technique to remove the diverticula using a single port introduced directly into the bladder. We applied the LESS technique, because it was a logical transfer from the laparoscopic transvesical multiport access to a potentially less invasive approach. We obtained written informed consent from the patients, as well as approval from the local ethics committee.
The LESS approach is similar in basic principles to the laparoscopic procedure. All men were operated on in the same manner. The patient was placed in the lithotomy position, the bladder was filled with 300 mL of sterile 0.9% sodium chloride solution, and a standard cystoscopy was performed. We made a 1.5-cm longitudinal skin incision 2 cm superior to the pubic symphysis. The inner ring of a TriPort+® access system (Olympus Winter & IBE GmbH, Hamburg, Germany) was preloaded onto an unbladed introducer. The introducer was then inserted directly into the bladder through the skin incision under cystoscopic control (Fig. 1). A small rectus sheath incision was made in two cases and stay sutures in one.
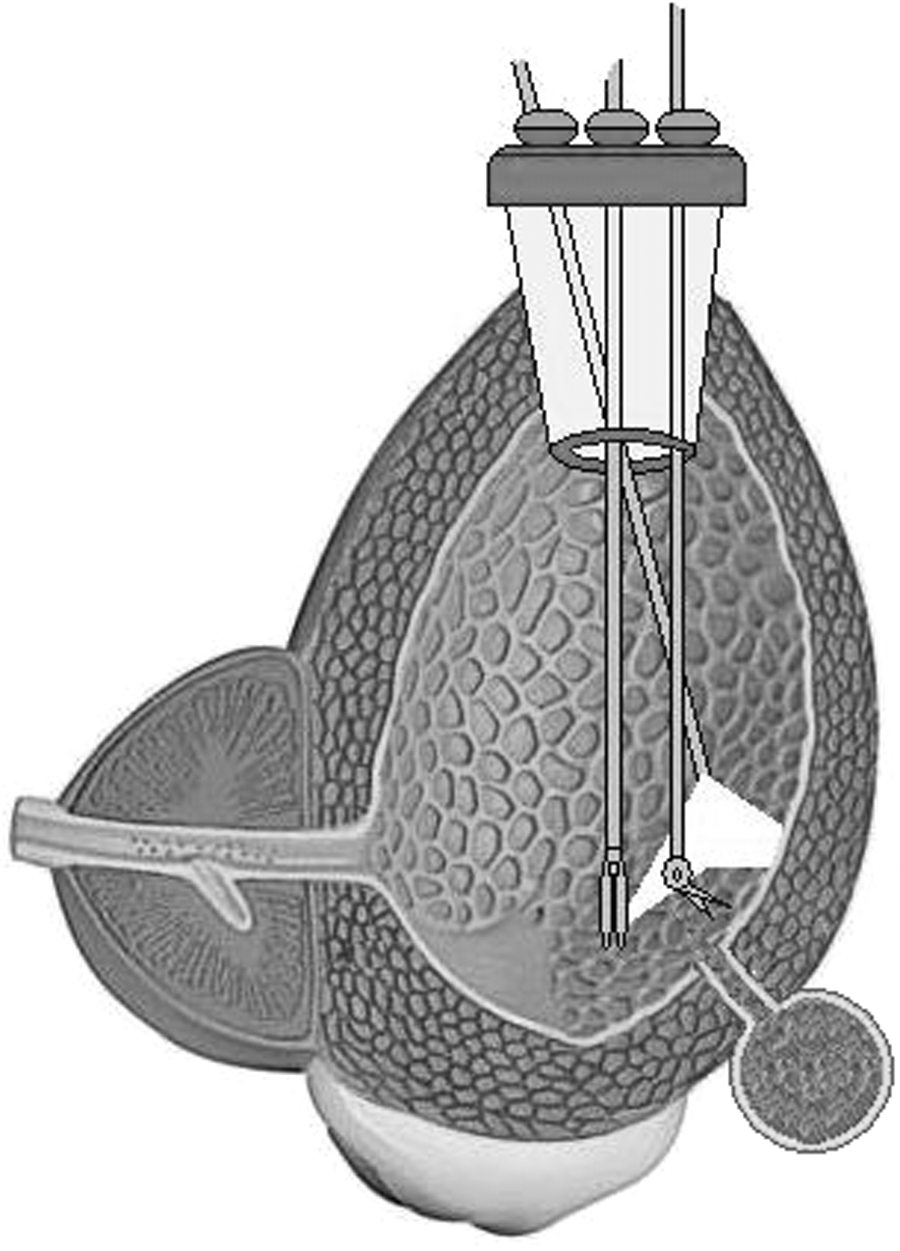
A schematic view of the transvesical approach for diverticulectomy with the TriPort+.
The rings of the TriPort+ were matched to the abdomen wall and fixed exactly (Fig. 2). After aspirating the saline, the bladder was filled with carbon dioxide up to 14 mm Hg pressure.

The TriPort+ is matched and fixed to the abdomen wall.
We used a 10-mm rigid, 30-degree videolaparoscope (Olympus Europa GmbH, Hamburg, Germany), which was introduced through the 10-mm channel of the TriPort+. The three 5-mm working channels were used as follows: (1) For a 5-mm standard laparoscopic dissector in the left hand, and (2) for 5-mm monopolar rigid hook scissors or a 5-mm rigid needle-driver (Karl Storz, Tuttlingen, Germany) in the right hand. When needed, we introduced the suction tube through the third 5-mm channel of the TriPort+ or through the urethra. Moreover, a standard laparoscopic grasper was inserted through the urethra to take the traction of the diverticular sac when needed.
The surgical strategy followed the transvesical diverticulectomy technique, which has been described in detail. 5 The 8- to 10-mm wide diverticular ostium was identified easily and separated from the bladder mucosa by a circular cut, using a hook electrode.
The diverticular neck was then mobilized from the surrounding detrusor muscle and pulled toward the vesical cavity with a laparoscopic grasper introduced through the TriPort+. When tractioning the edges of the diverticular wall became insufficient because of limited intravesical space, we introduced transurethrally another grasper, which significantly facilitated the traction of the diverticulum. This maneuver allowed the sac wall to be dissected from the neighboring tissue with a hook electrode, as well as to be drawn relatively rapidly and easily into the bladder. The diverticular sac was then removed intact through the disconnected TriPort+. The bladder wall defect was closed with an absorbable 3/0 running suture (The V-Loc™ 90 Absorbable Wound Closure Device, Covidien, Norwalk, CT). The TriPort+ was removed from the bladder, and the skin incision was sutured with two stitches.
An 18F Foley catheter was retained for 4 to 7 days after the operation. Because of the uneventful intra- and postoperative course, we did not expect any leak, and we did not perform cystography before removing the catheter. We proceeded in a manner similar to that after previous transvesical laparoscopic diverticulectomies.
Results
All patients were treated adequately in the manner presented above. The length of the skin incision was 1.5 cm. No extra port was introduced. The average operative time was 128 minutes, and no significant blood loss was observed (Table 1). The postoperative period was uneventful in all cases. The patients needed one or two doses of ketoprofen (50 mg intramuscularly) on the first postoperative day. Pathology examinations of the resected specimens were normal, except that of patient 3, in whom the examination showed a completely removed diverticulum with a small (1-cm in diameter) mass of superficial, low-grade urothelial cancer. The tumor was found in the middle part of the diverticulum.
The patients continued the treatment with alpha-blockers.
In the 3-month follow-up, all men presented decreased PVR (<40 mL) and negative bacteriologic urine assessment. In patients 1 and 3, the ultrasonographic examination showed small (less than 1.5-cm in diameter) extravesical hematomas close to the bladder wall on the operated sides. Patients 1 and 2 refused the treatment with transurethral resection of the prostate, being satisfied with the course of alpha-blockers. Careful follow-up with ultrasonography and laboratory examinations and cystoscopic evaluation every 3 months was recommended for patient 3.
Discussion
Bladder diverticula are usually secondary to bladder outlet obstruction. Although most diverticula are asymptomatic, some patients may present with hematuria, UTI, neoplasm formation, urinary retention, or even acute abdomen from rupture. 13 –15 The majority of patients can be treated conservatively; others may need surgical treatment, even if no obstruction is present. 13,14 Nevertheless, correction of bladder outlet obstruction is the first line of therapy in patients with diverticula caused by prostatic disease. There are several approaches to treat bladder diverticula, including either open or endoscopic procedures. 2 –5,13,14
Ever since Parra and associates 3 described the first laparoscopic bladder diverticulectomy, several further reports have been presented, and this approach is considered safe and effective, with clinical outcomes similar to those of open surgery. 4,16 The reported operative time ranged between 80 and 230 minutes, with a hospital stay from 2 to 6 days. 16
Single access techniques, such as LESS or natural orifice translumenal endoscopic surgery, have been introduced for their potential advantages over standard laparoscopy in terms of better cosmesis and lower morbidity. 7,17 Demanding procedures, including radical prostatectomy or live donor nephrectomy, have been performed with such techniques. 18,19 LESS has also been applied to the treatment of conditions both in the upper and lower urinary tract. 7,17,20 –22
Nevertheless, for the treatment of patients with bladder diseases, the approach directly through the bladder wall has not been commonly used. There are few reports on the use of such access. Sotelo and colleagues 11 used the transvesical LESS approach for bladder cuff excision, and Desai and coworkers 9 reported a series of adenomectomies. The successful removal of intravesical foreign bodies and eroded polypropylene tapes was also described. 10,23
The percutaneous transvesical LESS approach allows the surgeon to be supported by maneuvers and instruments delivered via the urethra and renders the use of articulable or bent instruments unnecessary. Bent devices often need more space than we can obtain in the bladder, and articulable instruments do not facilitate tissue traction during dissection.
Because the diverticula in our patients were located in the posterolateral walls and were relatively small, we neither catheterized ureters nor introduced the balloon catheter to the diverticulum before the operation. Although the visualization inside the bladder was sufficient to recognize and control all anatomic structures, we were able to perform cystoscopy at any phase of the operation for inserting ureteral catheters to avoid injury of the ureter.
We did not use ultrasonography for introducing the TriPort+. Finger palpation of the bladder dome, visualized cystoscopically, was sufficient for single-port insertion. We did not enter the Retzius space. In fact, the insertion of the TriPort+ (four-channel) is a bit more difficult than using the classic TriPort (three-channel), because the tip of the TriPort+ inserter is rounded. We were familiar with introducing the classic TriPort, which has a sharper end, and we adopted the same technique to the four-channel port. Our access does not differ much from the approach of Desai and associates, 9 although we did not create an anterior cystotomy. Stay sutures on the bladder dome may be helpful in some cases, however.
Once or twice during the procedure, we inserted graspers blindly through the urethra. This did not increase the risk of urethral injury. The delicate passing of the grasper through the urethra, using extreme care, is crucial for the safety of the maneuver. The use of a rigid cystoscope sheath is also possible. We performed this procedure once in one patient to facilitate the introduction of the grasper, and we think that it could potentially reduce the risks of this approach. A visual control of the passing of the grasper through the bladder neck, using the laparoscope, was helpful in avoiding injury to the prostatic urethra or the bladder neck. Likewise, during our previous transvesical LESS procedures, we did not observe a significant gas leakage through the urethra, either when the grasper was introduced, or when the urethral access was not used.
In patients 1 and 2, we also considered the laparoscopic approach to perform adenomectomy and diverticulectomy in one session. Nevertheless, because the prostate glands were relatively small, we preferred the use of transurethral techniques (transurethral resection of the prostate or laser), rather than open or laparoscopic adenomectomies, for decreasing any obstruction, if still present. Moderate obstruction that was revealed in uroflowmetry allowed us to put the patients under surveillance after the initial diverticulectomies.
The authors considered potential risks of an inadequate resection and management of the tumor found in patient 3. To avoid dissemination of the tumor, we followed the same principles that are emphasized by other authors. 2,14,15 The delicate traction of the diverticular cuff by the grasper introduced through the urethra facilitated keeping the diverticular sac closed, thereby avoiding the undesired dissemination of tumor cells. Furthermore, with respect to oncologic completeness, this novel single-port approach seems to be even safer than multiport laparoscopic access, either transvesical or extravesical.
We did not close the bladder wall with a separate suture, because the detrusor muscle was opened bluntly, without cutting the muscle fibers, with the trocar being a few millimeters wider in diameter than a standard 11-mm laparoscopic port used during transvesical laparoscopic procedures. In such cases, we remove trocars from the bladder and suture only the skin incisions and, occasionally, the rectus sheath openings. Both in this and other series of transvesical LESS procedures, which we have been performing since 2009, we have not noticed any recurrent urine leakage.
Establishing a Foley catheter for 4 to 7 days was sufficient to achieve a proper closure of the bladder wall, and we observed no complications in this regard. The overall results were similar to those reported by other authors. 4,7,16 The average operative time was 265 minutes in the laparoscopic group, 4 130 minutes in the transperitoneal LESS series, 7 and 128 minutes in our patients.
Contrary to a classic TriPort, the rings of a TriPort+ can be disconnected when needed; this makes it easier to place the suture into the bladder and enables the faster removal of the resected specimen. Moreover, a 1.5-cm–long skin incision was appropriate for introducing the TriPort+. Although our patients were very satisfied with the postoperative cosmetic effects, this outcome may need further quantification by means of questionnaires.
With the use of this newer device, gas leakage is less than that in the classic TriPort procedures. After establishing pneumovesicum, the bladder volume remained approximately the same as that during cystoscopy (300 cc). We did not observe any significant gas leak through the urethra or the bladder opening after removal of the diverticulum. The critical point is the air-tightness of the TriPort+ itself or around the rings. Using the TriPort+ in one case, we observed a major gas leakage through the connection of rings. Putting a thin strip of ribbon between the rings fixed the problem. We also did not notice any significant difference in working space volume depending on bladder compliance.
We think that advances in LESS technology, as well as the increasing experience of surgeons in this area, will allow the removal of almost all diverticula with this approach. In the case of larger diverticula, the catheterization of ureters would be recommended. We presume that only diverticula located near the apex of the bladder or with a wide ostium would not fit the selection criteria.
To our knowledge, this is the first report of direct, single-port transvesical access for the excision of a bladder diverticulum. The present analysis, however, is limited by its nonrandomized nature, the short follow-up period, and the small number of patients. As both the instrumentation and experience with the method evolve, a longer follow-up in a larger group of patients and a prospective comparison with other minimally invasive techniques will determine the place of this technique in the management options for bladder diverticula.
Conclusions
Percutaneous transvesical LESS excision of bladder diverticulum is technically feasible. This approach provides patients with a minimally invasive access through a single, small incision and comparable outcomes to that of the laparoscopic technique.
Footnotes
Disclosure Statement
No competing financial interests exist.