
Abstract
Purpose:
To perform a prospective randomized study to evaluate aspiration and sclerotherapy vs. laparoscopic deroofing in the management of symptomatic simple renal cysts.
Patients and Methods:
Forty patients with symptomatic simple renal cysts were randomized to treatment either by ultrasonography-guided aspiration and sclerotherapy (group A–20 patients) or by laparoscopic deroofing (group B–20 patients). Two patients in group A and one patient in group B had a parapelvic cyst. Patients were evaluated by urine analysis, serum creatinine level, coagulation profile, ultrasonography, and CT urography. In group A patients, after aspiration, 1% polidocanol in a volume equivalent to 10% of cyst volume was instilled. In group B patients, laparoscopic deroofing was performed. All patients were followed up by ultrasonography up to 1 year after treatment.
Results:
In group A, aspiration and sclerotherapy was performed on an outpatient basis, and none of the patients needed postoperative analgesia. Eighteen of 20 patients had complete regression; two of these had parapelvic cyst. Partial regression with relief of pain was noted in one patient, whereas treatment failed in one patient. None of the patients had any significant complication and none required analgesia. All the patients were discharged two hours after the procedure. In group B, laparoscopic deroofing was successfully performed in 19 of 20 patients. Laparoscopic deroofing could not be performed in one patient with parapelvic cyst because of failure of access. The mean analgesic requirement was 285±57.98 (200–400) mg tramadol, and average hospital stay was 2.1±0.32 (2–3) days.
Conclusion:
Percutaneous aspiration and sclerotherapy with polidocanol is an effective, safe, and minimally invasive therapeutic option for symptomatic simple renal cysts, with equal efficacy and lower morbidity and hospital stay in comparison with laparoscopic deroofing.
Introduction
The classic treatment of patients with symptomatic renal cysts is deroofing, which can be performed by open surgery or laparoscopy. Surgical treatment is associated with some morbidity and even mortality, especially in elderly patients. 5 Laparoscopic deroofing is an effective minimally invasive approach and has gained popularity in recent years. 6,7
Simple aspiration and sclerotherapy is a minimally invasive procedure, and various sclerosing agents have been used for the management of symptomatic renal cysts. 8 Polidocanol has been used extensively as an effective sclerosing agent in the treatment of varicose veins, 9 hydroceles, epididymal cysts, 10 and esophageal varices 11 apart from renal cysts. 12
This randomized study was undertaken to compare the effectiveness of aspiration and sclerotherapy using polidocanol with laparoscopic deroofing in the treatment of patients with symptomatic simple renal cysts.
Patients and Methods
From June 2007 to May 2010, 40 patients with symptomatic simple renal cysts were randomized to treatment either by aspiration and sclerotherapy (group A–20 patients) or by laparoscopic deroofing (group B–20 patients). The study was conducted after obtaining Institutional Review Board approval, and randomization was performed using systematic sampling technique. The methodology followed was as per the CONSORT statement. Patients' demographic details and characteristics are summarized in Table 1.
Indication for intervention was simple renal cortical cyst corresponding to Bosniak category I (thin walled, clear lumen with no echoes within cyst) 13 that was symptomatic (pain, hypertension, hematuria, or obstruction of the pelvicaliceal system). Patients with polycystic disease of the kidney, complex cysts, any history of treatment for cysts, and cyst size <2 cm were excluded from the study. Two patients in group A and one patient in group B had parapelvic cysts.
Patients were evaluated by urine analysis, serum creatinine level, coagulation profile, renal ultrasonography, and CT urography. Diagnosis of simple renal cyst was based on CT scan and ultrasonography that showed a smooth, well-defined wall, echo-free cavity with good transmission leading to posterior enhancement, and a well demarcated posterior wall. Volume of the cyst was measured by ultrasonography. In all patients, written informed consent was obtained.
In group A, the patient was placed prone, and under local anesthesia with 2% lidocaine, an 18-gauge puncture needle was inserted into the cyst under ultrasonographic guidance, followed by aspiration of 10 to 20 mL of fluid. If the fluid was clear, an equivalent volume of water-soluble contrast medium was injected to delineate the cyst outline. If the wall was smooth and there was no communication with the pelvicaliceal system and no extravasation outside the cyst wall, the cyst was aspirated completely. After aspiration, 1% polidocanol in a volume equivalent to 10% of cyst volume (to a maximum of 20 mL) was instilled into the cyst. This was performed as an outpatient procedure, and patient was sent home after 2 hours. No attempt was made to aspirate or drain the sclerosant after instillation.
In group B patients, before laparoscopic deroofing, any caliceal communication was excluded by retrograde ureteropyelography. A retroperitoneal laparoscopic approach with three ports was used. With the patient in the flank position under general anesthesia, a space was created using the Gaur balloon technique, followed by port placement using the Hassan cannula. The renal capsule was exposed; the cyst wall was excised and perinephric fat interposed to prevent recurrence.
The patients were followed up with ultrasonography at 1 month, 3 months, 6 months, and 1 year. The effect of treatment was assessed by comparing the volume of the recurrent cyst with the pretreatment cyst volume and the disappearance of symptoms.
Complete disappearance of symptoms and reduction in volume to <5% of the initial renal cysts was deemed to be “complete regression.” Relief of symptoms with reduction in cyst volume by more than half was considered as a “partial regression.” The treatment was considered a failure when the cyst could not be accessed initially, or recurred to more than half of the pretreatment volume in follow-up, or symptoms persisted after treatment.
Statistical analysis was performed using SPSS software. The statistical tests used were the chi-square test and Student t test.
Results
As shown in Table 2 and Fig. 1, in group A (aspiration and sclerotherapy), the cyst was accessed successfully in all patients. Complete aspiration was achieved under ultrasonography guidance in all cases. None of the patients had infection after aspiration. In all patients, findings of biochemical and cytologic examination of the fluid, as expected for simple cysts, were unremarkable, and the fluid was negative for malignant cells.
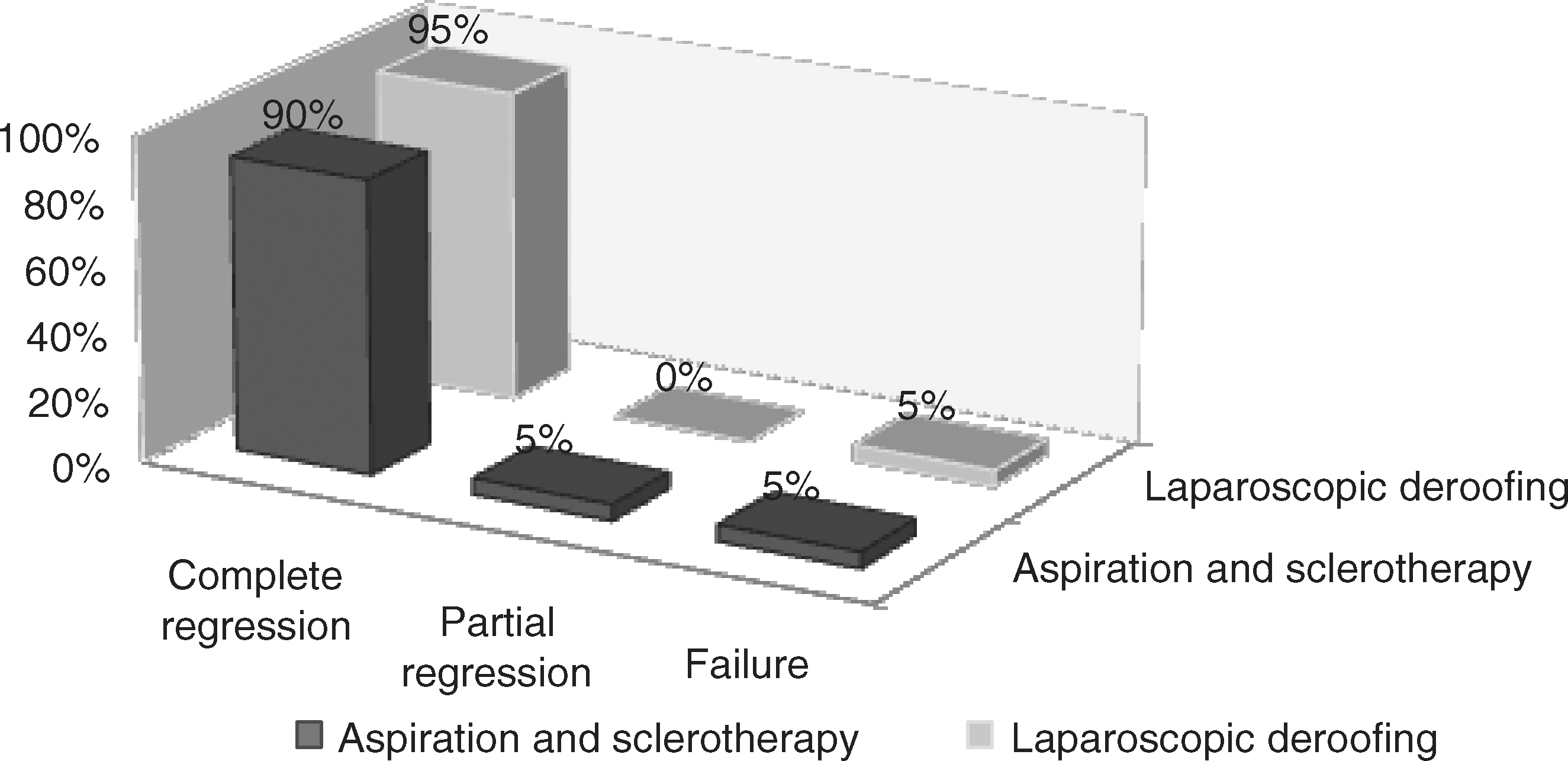
Success rate: Aspiration and sclerotherapy vs. laparoscopic deroofing.
Mean time taken for the procedure in group A was significantly lower than group B (P<0.01) (33.5 vs. 112 minutes). Analgesia requirement was determined according to assessment of pain using the visual analog scale score. In group A, none of the patients needed analgesia, whereas in group B, the mean requirement of tramadol was 285±57.96 mg in the first 24 hours. All patients were discharged 2 hours after the procedure in group A, whereas the mean duration of hospital stay in group B was 50.4±7.68 hours.
At 1 year follow-up, in group A, complete and partial regression was achieved in 18 (90%) and 1 (5%) cases, respectively, and there was no recurrence of symptoms in any of these patients. Two patients with complete regression had parapelvic cyst. In only one patient, treatment was a failure. In group B, complete regression was achieved in 19 (95%) patients. In one patient, the parapelvic cyst could not be accessed laparoscopically. There was no significant difference between groups in terms of complete regression (P>0.05).
None of the patients in either group had any significant complication except port site infection in one patient in group B. There was no recurrence in any of patients in follow-up.
Discussion
Renal cysts are common, with an incidence increasing with age from average 0.22% (0.1%–0.45%) up to age 18 years, to >20% by the fourth decade and approximately 36% after the sixth decade of life. 2 The vast majority of simple cysts develop in otherwise normal kidneys, and their origin remains obscure. 2 Ischemia, local obstruction of nephrons with subsequent proximal nephron dilation, and small diverticula on renal tubules increasing with age have been implicated. 13
Renal cysts have been classified using morphologic characteristics. 14 Clinically, renal cysts are commonly referred to as either simple or complex. The majority of cysts are simple, thin and smooth walled, with no calcification, septation, or enhancement after contrast studies. They have an insignificant risk of malignancy.
Most renal cysts remain asymptomatic, but some patients have symptoms that are likely to be related to the cyst size. When cysts are very large, they may produce the mechanical effects of space-occupying lesions. There is an increase in the size and number of cysts over time in the cyst-bearing person.
Only symptomatic or complicated cysts need treatment. Several treatments have been proposed, such as surgical or laparoscopic excision or marsupialization, simple percutaneous aspiration or drainage followed by instillation of a sclerosing agent. Other treatment options include endoscopic marsupialization and percutaneous endoscopic resection.
Aspiration without sclerotherapy of simple renal cysts has a recurrence rate of >90% because the cysts are lined by secretory epithelium. 15 Aspiration followed by sclerotherapy has been reported to have a much lower recurrence rate. 8,15 –18 Various sclerosants have been used after cyst aspiration to provoke inflammation of the cyst wall, leading to adhesion of the walls and reduction or resolution of the cyst.
The ideal sclerosing agent should be safe, painless, have no significant side effects, and minimize recurrence. Sterile ethanol (95%–99%) had been widely used for symptomatic renal cyst. Bean 8 first reported the use of ethanol as the sclerosing substance for the management of a symptomatic renal cyst in 1981. Hanna and Dahniya 16 reported the recurrence rate to be 80% in cysts that were managed with aspiration only and 32% in cysts after a single ethanol injection. Ethanol use, however, is associated with various complications, including pain, fever, and occasionally systemic reactions, such as drunken state or shock. Okeke and associates 7 described failure of single-session ethanol sclerotherapy for the management of renal cysts in all of their six selected patients in whom symptoms recurred.
To overcome the drawbacks that are associated with the use of alcohol as a sclerosing agent, various other sclerosing agents have been used, including glucose, phenol, iophendylate, urea chlorohydrolactate, pantopaque, 8 polidocanol, 12 acetic acid, 19 bismuth phosphate, 20 povidone iodine, 21 ethanolamine oleate, 22 and minocycline hydrochloride, 23 with varying degrees of success.
Percutaneous sclerotherapy of simple renal cysts with polidocanol offers a high rate of success 12,24 –26 without the need for repeated interventions associated with sclerotherapy performed with ethanol. 27 Ohta and collealgues 12 reported the efficacy of this treatment as 93%. Polidocanol belongs to a newer generation of sclerosing agents, more successful and safer 24,25 than the conventional agents such as ethanol and phenol. In some of the previous studies, 12,24 –26 3% polidocanol was used, but we used 1% polidocanol because the study performed by Hamel-Desnos and coworkers 9 demonstrated equivalent efficacy for 1% and 3% polidocanol in sclerotherapy for varicose veins.
The recurrence of renal cysts after sclerotherapy can be attributed to incomplete ablation of the cyst wall, 8 and it is likely that the longer time of contact between the sclerosant and the renal cyst epithelium may cause higher success rates. 27 In contrast to the majority of earlier studies in which the sclerosing agent was drained after 20 to 30 minutes of instillation, 7,8,16 –18 we retained the sclerosant within the cyst to prolong the contact time. In our opinion, this has also contributed to a lower recurrence rate and improved results in our study.
In our study, 1% polidocanol in a volume equivalent to 10% of cyst volume was instilled for adequate sclerosis of cyst walls; at the same time, we kept the maximal volume limited to 20 mL to allow adequate apposition of cyst walls to facilitate obliteration of the space.
Pain was relieved in all our patients in whom there was complete or partial resolution of the cyst. Pain relief after regression indicated that the residual cyst does not necessarily need further intervention, as long as pain or other significant symptoms or signs disappear or improve.
Percutaneous renal cyst aspiration sclerotherapy is rarely associated with significant complications. 20 We had no major complication after aspiration and sclerotherapy. Peripelvic renal cysts have been excluded for sclerosing therapy by some investigators 17,28 because of a report of extravasation of the sclerosing substance into the peripelvic tissue with resulting fibrosis of the ureteropelvic junction. 29 In our study, however, two patients with parapelvic renal cysts underwent aspiration and sclerotherapy with satisfactory therapeutic result and no procedure-related complications.
Laparoscopic treatment seems an attractive alternative. It offers a minimally invasive modality to decompress cysts under direct vision. For laparoscopic deroofing surgery, a 90% success rate has been reported. 6 Abbaszadeh and associates 30 reported laparoscopic transperitoneal decortication as an effective and safe treatment option in the management of symptomatic renal cysts. In this study, patients who experienced complete pain relief had significantly larger cyst sizes compared with patients with partial pain relief.
Like open surgery, laparoscopic deroofing of the cyst appears to be effective by removing part of the cyst wall and providing adequate drainage of the cyst. It combines the advantage of a minimally invasive procedure with the effectiveness of cyst marsupialization achieved by open surgery. Both modalities are invasive, however, necessitating general anesthesia with the accompanying operative morbidity and complications. In our study, one patient had port site infection while in one patient with parapelvic cyst, laparoscopic deroofing could not be performed because of failed access.
Although the gold standard in the management of a renal cyst is deroofing by open or laparoscopic surgery, aspiration with sclerotherapy is more minimally invasive, has fewer complications with equal efficacy and safety. Aspiration with sclerotherapy needs no analgesia and is performed as an outpatient procedure. Parapelvic cyst can also be treated more easily by aspiration and sclerotherapy. One patient in group B in whom the parapelvic cyst could not be accessed laparoscopically was successfully treated by sclerotherapy. In addition, in case of failure, laparoscopic deroofing cannot be repeated as easily as aspiration and sclerotherapy. It may be argued that when a symptomatic cyst is established, aspiration and sclerotherapy may be chosen as the first therapeutic procedure, reserving laparoscopic deroofing for cases of failure of the former.
A rigorous clinical evaluation is advised before ascribing any loin pain to a simple renal cyst found on imaging. Any communication with the pelvicaliceal system must be excluded, which could potentially lead to retroperitoneal urinoma or urinary ascites after laparoscopic deroofing and sclerosis of the pelvicaloceal sytem after sclerotherapy. This can be done by intravenous urography, CT urography, or retrograde pyelography preoperatively, or by injection of contrast under fluoroscopy during ultrasonography-guided aspiration.
The major limitation of the present study is the small number of cases, which was somewhat inevitable given the fact that only symptomatic simple renal cysts can be considered for therapeutic intervention. Another limitation of this study is a relatively short follow-up, although we had no recurrence of symptoms in the 1-year period of follow-up. A larger study with longer follow-up may be needed to validate these results.
Conclusion
Single-session aspiration and sclerotherapy using polidocanol compares favorably with laparoscopic deroofing surgery for the management of symptomatic simple renal cysts and can be considered the first procedure of choice because it is more minimally invasive, safe, easy to perform, and offers an equivalent rate of success.
Footnotes
Disclosure Statement
No competing financial interests exist.