
Abstract
Purpose:
To present our experience with robot-assisted simple prostatectomy in patients with large gland adenoma (>100 g) that would not be amenable to transurethral treatments.
Patients and Methods:
From August 2009 to May 2011, 13 robot-assisted simple suprapubic prostatectomies were performed in patients with symptomatic large gland (>100 g) prostatomegaly on transrectal ultrasonography (mean 163 cc). Essential aspects of our technique include a transverse cystotomy just proximal to the prostatovesical junction and use of a robotic tenotomy grasper to aid in adenoma dissection.
Results:
Mean operative time was 179 minutes (range 90–270 min), and mean estimated blood loss was 219 mL (range 50–500 mL). Mean hospital stay was 2.7 days (range 1–8 d), and the mean urethral catheterization time was 8.8 days (range 5–14 d). None of the patients needed blood transfusion. One patient had an intraoperative urinary leak after bladder closure that was managed with prolonged urethral catheterization (14 d). Histopathologic analysis confirmed benign prostatic hyperplasia (BPH) in all patients, and mean specimen weight on pathologic examination was 127 g (range 100–165 g). Mean follow-up duration was 7.2 months with all patients having a minimum of a 4-month follow-up. Significant improvements were noted in the International Prostate Symptom Score (preoperative vs postoperative 18.1 vs 5.3, p<0.001) and the maximum urine flow rate (preoperative vs postoperative 4.3 vs 19.1 mL/min, P<0.001).
Conclusions:
Minimally invasive robot-assisted simple prostatectomy is techincally feasible in patients with large volume (>100 g) BPH and is associated with significant improvements in obstructive urinary symptoms. Surgeons with robotic expertise may consider using this approach for treatment of their patients with large volume BPH.
Introduction
The surgical approach used is dependent on the prostate gland size and the presence of concurrent bladder stones and/or diverticuli, with transurethral resection being the gold standard for treatment of small- to medium-sized adenomas. Although techniques such as holmium laser enucleation, photoselective vaporization, and bipolar resection have been described for treatment of large gland adenoma, open simple prostatectomy, first described by Millin 2 in 1947 remains the treatment of choice for symptomatic, large volume BPH with glands >80 g. Laparoscopic simple prostatectomy was first described by Mariano and associates 3 in 2002, and several series have reported equivalence to the open procedure in improving obstructive symptoms and quality of life. 3,4 In addition, studies have found less blood loss and shorter duration of hospitalization and urethral catheterization with the laparoscopic approach. 4,5
With continued expansions in the field of robotic surgery and its associated benefits over laparoscopy (three-dimensional vision, more degrees of freedom, efficient intracorporeal suturing), urologists have been able to transfer the principles of open surgery to a minimally invasive approach to treat patients with symptomatic BPH. While the feasibility of robot-assisted simple prostatectomies has been reported, these studies are limited to medium-sized prostates that may have been amenable to transurethral treatments. 6 –8 We think the true role of robot-assisted simple prostatectomy is in the treatment of large glands and report our experience and outcomes with treatment of glands >100 g using the robotic approach.
Patients and Methods
From August 2009 to May 2011, 13 robot-assisted simple suprapubic prostatectomies were performed at our two institutions. Medical treatment for symptomatic BPH had failed in all patients, and the indications for surgery were persistent obstructive symptoms (n=4), frequent urinary tract infections (n=2), and urinary retention (n=7). Preoperative evaluation consisted of a history and physical examination including digital rectal examination, International Prostate Symptom Score (IPSS) questionnaire, and routine laboratory tests including prostate-specific antigen (PSA). In addition, all patients underwent uroflowmetry and transrectal ultrasonography to determine total prostate volume. Patients were offered all treatment alternatives (including transurethral techniques), and a recommendation of simple prostatectomy was given to all patients with a gland >100 cc.
Perioperative characteristics, including operative time, blood loss, hospital stay, duration of urethral catheterization, blood transfusion requirements, and complications, were evaluated. Patients were followed up at 3 months postoperatively and then every 6 months. Follow-ups included PSA, IPSS questionnaire, and uroflowmetry. Statistical analysis was performed using SPSS (International Business Machines, Armonk, N.Y.) statistical software.
Surgical technique
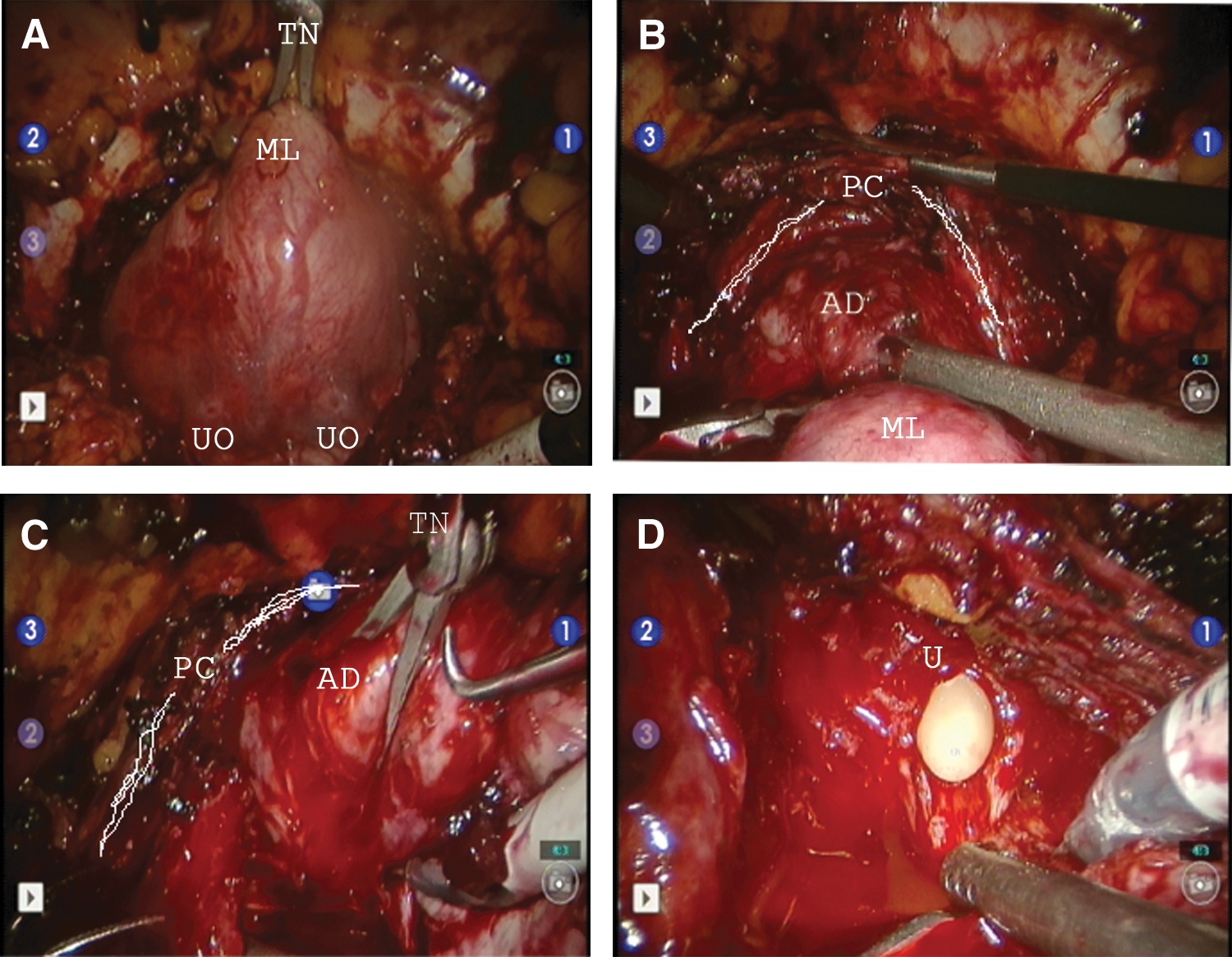
All procedures were performed with a four-arm da Vinci-S Surgical System (Intuitive Surgical, Sunnyvale, CA). A five-port transperitoneal access technique similar to the one used in robot-assisted radical prostatectomy was used. After the retropubic space was developed, the bladder was filled with 200 mL of saline. A transverse cystotomy was made at the bladder neck to expose the prostate base and the trigone. The adenoma was identified, and a traction suture was placed on the posterior adenoma/median lobe. This allowed mobilization of the adenoma posteriorly, with the dissection involving sweeping laterally and anteriorly. An essential aspect of our dissection included use of a robotic tinaculum grasper (Fig. 1) to aid in retraction of the adenoma, with enucleation achieved with electrocautery and blunt dissection. After posterior and lateral dissection, anterior dissection was performed to expose the urethra at the apex where the urethra is divided under direct vision without damaging the urethral sphincter mechanism at the prostatic apex.
Hemostatasis was achieved with figure of eight 2-0 polyglactin stitches at the 5 and 7 o'clock positions at the bladder neck. Trigonization of the prostatic urethra was performed by approximating the posterior bladder neck to the posterior urethra with interrupted 2-0 polyglactin stitches. A 22F three-way Foley catheter with 30 cc balloon was placed before the cystotomy was closed. Continuous bladder irrigation was immediately initiated, and the specimen was removed via the assistant ports after morcellation.
Results
We performed 13 robot-assisted simple prostatectomies on patients with glands >100 g without any open conversion. Average patient age was 67.1 years (Table 1), and the mean prostate volume on preoperative transrectal ultrasonography was 163 cc (range 110–220 cc). Mean operative time was 179 minutes (range 90–270 min), and mean estimated blood loss was 219 mL (range 50–500 mL). Mean hospital stay was 2.7 days (range 1–8 d), and the mean urethral catheterization time was 8.8 days (range 5–14 d). None of the patients needed blood transfusion. One patient had an intraoperative urinary leak after bladder closure that was managed with prolonged urethral catheterization (14 d).
SD=standard deviation.
Histopathologic analysis confirmed BPH in all patients, and mean specimen weight on pathologic examination was 127 g (range 100–165 g,). Mean follow-up duration was 7.2 months with all patients having a minimum of a 4-month follow-up. Significant improvements were noted in the IPSS (preoperative vs postoperative 18.1 vs 5.3, P<0.001), maximum urine flow rate (preoperative vs postoperative 4.3 vs 19.1 mL/min, P<0.001), and postvoid residual (preoperative vs postoperative 207.3 vs 12.7 mL, P<0.001) (Table 2).
IPSS=International Prostate Symptom Score; Qmax=maximum flow rate; PVR=postvoid residual; PSA=prostate-specific antigen; SHIM=Sexual Health Inventory for Men.
Discussion
Total gland size has traditionally been the most important factor in determining the surgical approach in patients with symptomatic BPH who need surgical therapy. Transurethral incision is the preferred method of treatment in patients with <30 cc. Transurethral resection of the prostate remains the gold standard for medium-sized glands. 9 Simple prostatectomy is the treatment of choice in patients with large prostate size (>80 cc) and in patients who are poor candidates for transurethral resection of the prostate (inablility to tolerate dorsal lithotomy, concurrent bladder diverticula, or stones). 10
Since 2002, several simple prostatectomy series have been published in which minimally invasive techniques including laparoscopic and robot-assisted surgery have been used. Baumert and colleagues 4 in 2006 published the first series that compared a minimally invasive approach with open surgery. 4 When comparing their first 30 laparoscopic simple prostatectomies with a historical cohort of 30 open cases, the laparoscopic patients had less blood loss and shorter duration of catheterization and hospital stay. In addition, only six of the experimental group needed bladder irrigation postoperatvely. Although operative time was longer in the laparoscopic group, there were no differences in the incidence or severity of complications. These results were validated in 2009 when McCollough and coworkers 5 published a series of 280 patients undergoing either open or laparoscopic simple prostatectomy. The laparoscopic group in that series also had less catheter time and hospital stay with longer operative times. 5 There also have been reports of single-site and transvesical prostatectomy 11,12 ; however, the surgical learning curve for these techniques could be high.
In 2008, Sotelo and colleagues 6 first described the use of the robotic technique to perform a simple prostatectomy. Robotic surgery provides all the advantages of standard laparoscopy with a potentially shorter learning curve. A comparison of the studies using robotics has been highlighted in Table 3. Patients who had undergone robot-assisted prostatectomy had significant improvements in urinary flow, postvoid residual measurements, and IPSS scores. The operative times and estimated blood loss were similar to those seen in laparoscopic series. Patients undergoing robot-assisted simple prostatectomy seem to have a shorter hospital stay, decreased analgesic requirement, lower incidence of blood transfusion, and better cosmetic results compared with those who have open surgery, although no head-to-head comparison has been published in the current literature. 5 –8,13,14
EBL=estimated blood loss; LOS=length of stay.
While the early robotic series were important in defining the feasibility of the approach, most patients in those studies had smaller glands that are easily amenable to transurethral treatments (Table 3). In the series by Sotelo and associates 6 series of seven cases, the mean pathologic gland size was 51 g. In 2009, John and coworkers 8 performed 13 using a preperitoneal robotic approach with assistance of a single finger to aid in enucleation of the adenoma. Mean specimen weight in that series was 82 g. Even in the largest series published—Uffort and associates 13 in 2010—the average pathologic weight was below the typical cutoff for simple prostatectomy (46 g, n=15).
The clinical significance of our series is to establish outcomes of robot-assisted simple prostatectomy in patients who are poor candidates for transurethral treatment secondary to large gland size. We report statistically significant improvements in postvoid urine residual, urine flow rates, and IPSS scores (P<0.001) in our series of patients with adenoma >100 g. The operative time, estimated blood loss, incidence of blood transfusion, Foley catheter duration, and length of hospital stay were similar to those seen with laparoscopic simple prostatectomy. The risk of blood transfusion and duration of hospital stay appears to be lower than that seen in open series.
Our technique replicates the technique of an open suprapubic simple prostatectomy and can be used in patients with bladder stones and diverticuli. Although we prefer the transperitoneal technique, it may be performed using an extraperitoneal approach as well. The essential component of our technique was the use of the robotic tenaculum in the assistant robotic arm for static and dynamic cephalad retraction of the adenoma. This is especially important in patients with large prostates because the adenoma may come in the way of performing an apical dissection.
The limitation of our study lies in the small sample size and the retrospective nature of the study. The majority of patients with prostate volumes up to 100 g, however, are treated using bipolar resection at our institution, thereby limiting our patient recruitment. We believe that while alternatives to simple prostatectomy exist for patients with small- to medium-sized adenomas, robot-assisted simple prostatectomy for large adenomas is not only feasible, but can consistently produce excellent outcomes.
Conclusions
Minimally invasive robot-assisted simple prostatectomy is technically feasible in patients with large volume (>100 g) BPH and is associated with significant improvements in obstructive urinary symptoms. Surgeons with robotic expertise may consider using this approach for treatment of their patients with large volume BPH.
Footnotes
Acknowledgments
The authors acknowledge the contributions of Drs. John Lynch and Mohan Verghese.
Disclosure Statement
No competing financial interests exist.