
Abstract
Background and Purpose:
Because of the increased use of robot-assisted laparoscopic prostatectomy (RALP) for the management of localized prostate cancer, surgeons in training face the issues of developing skills in both open surgery and the robotic console. This study compares prospectively the safety and efficacy of the first 50 open radical retropubic prostatectomy (RRP) procedures and the first 50 RALP procedures, performed by the same surgeon in the same institution.
Patients and Methods:
The patients' baseline demographic, clinical, and oncologic parameters were prospectively recorded. The study end points included oncologic outcome, functional outcomes (at 3 months), and perioperative parameters. Complications were classified according to the modified Clavien system.
Results:
No statistically significant differences were noted between the two groups in terms of preoperative patient characteristics and oncologic parameters. The operative time and mean estimated blood loss were lower in the RALP group (P<0.001), but no statistically significant difference was noted in regard to transfusion rates (P=0.362). Mean hospital stay was lower in the RALP group (P<0.001). The minor (Clavien I+II) and major (Clavien III+IV) complication rates were comparable between the two groups. The overall positive margin (PSM) rates were 20% and 18% for RRP and RALP, respectively (P=0.799), while for pT3 disease, the PSM rates were 26.1% and 22.2%% for RRP and RALP, respectively (P=0.53). The 3-month continence rates were 88% and 90% for RRP and RALP, respectively (P=0.749). For preoperatively potent patients, 3-month potency rates were comparable between the two groups (60.6% and 62.1% in the RRP and the RALP group, respectively, P=0.893).
Conclusion:
The early learning curve for RALP appears safe and results in equivalent functional and oncologic outcome, when compared with the results of open surgery.
Introduction
Robot-assisted laparoscopic prostatectomy (RALP) has a shorter learning curve compared with standard laparoscopy. This improvement may be attributed to a number of technical factors, including three-dimensional visual field, seven degrees of freedom for instrument movement, filtering of tremor, and ergonomic surgical console that limits the surgeon's fatigue. 2 Despite the fact that radical retropubic prostatectomy (RRP) is still considered a standard option for organ-confined prostate cancer, 3 many surgeons experienced in open surgery are currently converting to robot-assisted surgery. Surgeons in training, however, still face the issues of developing skills in both open surgery and the robotic console. The caseload necessary to develop these skills may be different for open and robotic surgery.
This study compares prospectively the safety and efficacy of the first 50 open RRP vs the first 50 RALP procedures performed by the same surgeon in the same institution. All data were collected prospectively, and functional and oncologic outcomes were compared between the two methods.
Patients and Methods
Between October 2007 and December 2008, a newly appointed consultant performed 50 consecutive RRP procedures (group A). Between November 2008 and January 2010, 50 consecutive RALP procedures using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) were performed by the same surgeon (group B). Mentored cases performed before this were excluded from this study. None of the patients included in the study had neoadjuvant androgen deprivation therapy or preoperative radiotherapy. The preoperative diagnostic and staging workup was identical for all the patients who underwent radical prostatectomy during the study period.
Having completed 3 years of core urology training, the surgeon (ER) underwent 2 years of subspeciality training in uro-oncology. During this period, he participated in more than 200 RRP as first assistant and performed parts of the procedure under the direct supervision of a consultant. He also participated in more than 100 RALP procedures as a patient-side assistant, but had no experience in pure laparoscopic radical prostatectomy. The surgeon performed his first unsupervised RRP in October 2007 and performed a total of 50 RRP procedures over a period of 14 months. In November 2008, the department launched a robotic program, and all patients who presented as candidates for radical prostatectomy were offered a robot-assisted procedure. An open procedure was offered thereafter only in the presence of specific contraindications for RALP.
RRP was performed in all 50 cases via an infraumbilical midline incision, according to the principles described by Walsh. 4 All RALP procedures were performed by using the four-arm da Vinci robotic system. A transperitoneal six-port antegrade approach was used, and the same points of technique were used in all 50 cases. 5,6
Preoperative hematocrit (Hct) level was measured in a blood sample 48 to 96 hours before admission, during a consultation in a dedicated preoperative clinic. Postoperative Hct level was routinely measured 12 hours after the procedure. The volume of intraoperative blood loss was estimated by the anesthesiologist. The indications for transfusion were those recommended by internal protocols, with a general transfusion trigger of Hct <28% in hemodynamically stable patients. In the presence of symptoms indicative of inadequate oxygen-carrying capacity, transfusion therapy was started at higher Hct values. Autologous donation or cell-saver autotransfusion were not offered to the patients included in the present study.
The patients' baseline demographic, clinical, and oncologic parameters were prospectively recorded in an electronic database, and prostate volume was measured by transrectal ultrasonography. The D'Amico criteria were used to stratify the patients in risk categories preoperatively. 7
Positive surgical margins (PSM) were defined as tumor cells reaching the inked surface of the specimen. The study end points included oncologic outcome (PSM rates, 12-month biochemical recurrence-free rates), functional outcomes (urinary continence and potency at 3 months), and perioperative parameters. Perioperative and early postoperative (28-day) complications were classified according to the modified Clavien system. 8 Urinary continence was defined as absence of any urinary leakage or use of only one “safety” pad. Potency was defined as presence of erection sufficient for intercourse with or without the use of phosphodiesterase-5 (PDE-5) inhibitors. Biochemical recurrence was defined as two consecutive prostate-specific antigen (PSA) measurements ≥0.2 ng/mL. 9
Data were summarized as means for continuous variables and in frequency tables for categorical variables. Statistical analysis was performed with the SPSS software package (SPSS 13.0 Inc, Chicago, IL). Chi-square testing and Fisher exact test were used for comparison of nominal data. To evaluate the learning curve in terms of procedure duration, the operative time was plotted in a scatter chart for each group, and a plateau phase was estimated. Numeric data were compared by using the Wilcoxon rank sum test. Statistical significance was defined as P≤0.05.
Results
Preoperative demographic and clinical parameters (age, body mass index, American Society of Anesthesiologists score, prostate volume) were comparable between the two groups (Table 1). In terms of preoperative oncologic parameters (PSA level, biopsy Gleason score, clinical stage, D'Amico risk stratification), no statistically significant difference was noted between the two study groups.
Wilcoxon rank sum test.
Chi-square test.
Fisher exact test.
SD=standard deviation; BMI=body mass index; ASA=American Society of Anesthesiologists; PSA=prostate-specific antigen.
The intraoperative and perioperative data are summarized in Table 2. The mean (standard deviation [SD]) operative time was 125 (30) minutes for RRP and 212 (71) minutes for RALP (P<0.001). The procedure duration is demonstrated as a scatter chart (Fig. 1) for both groups, and a best fit line is plotted. In the RRP group, the procedure duration decreased slightly after the first 10 procedures and reached its plateau after the 20th open procedure. In the RALP group, the operative time decreased abruptly up to the 15th robot-assisted procedure and reached a plateau after the 30th robot-assisted procedure. In Figure 2, the docking time for RALP is displayed as a scatter plot.

Transition in procedure duration (and the corresponding best fit line plot) for the two groups. RRP=radical retropubic prostatectomy; RALP=robot-assisted laparoscopic prostatectomy.
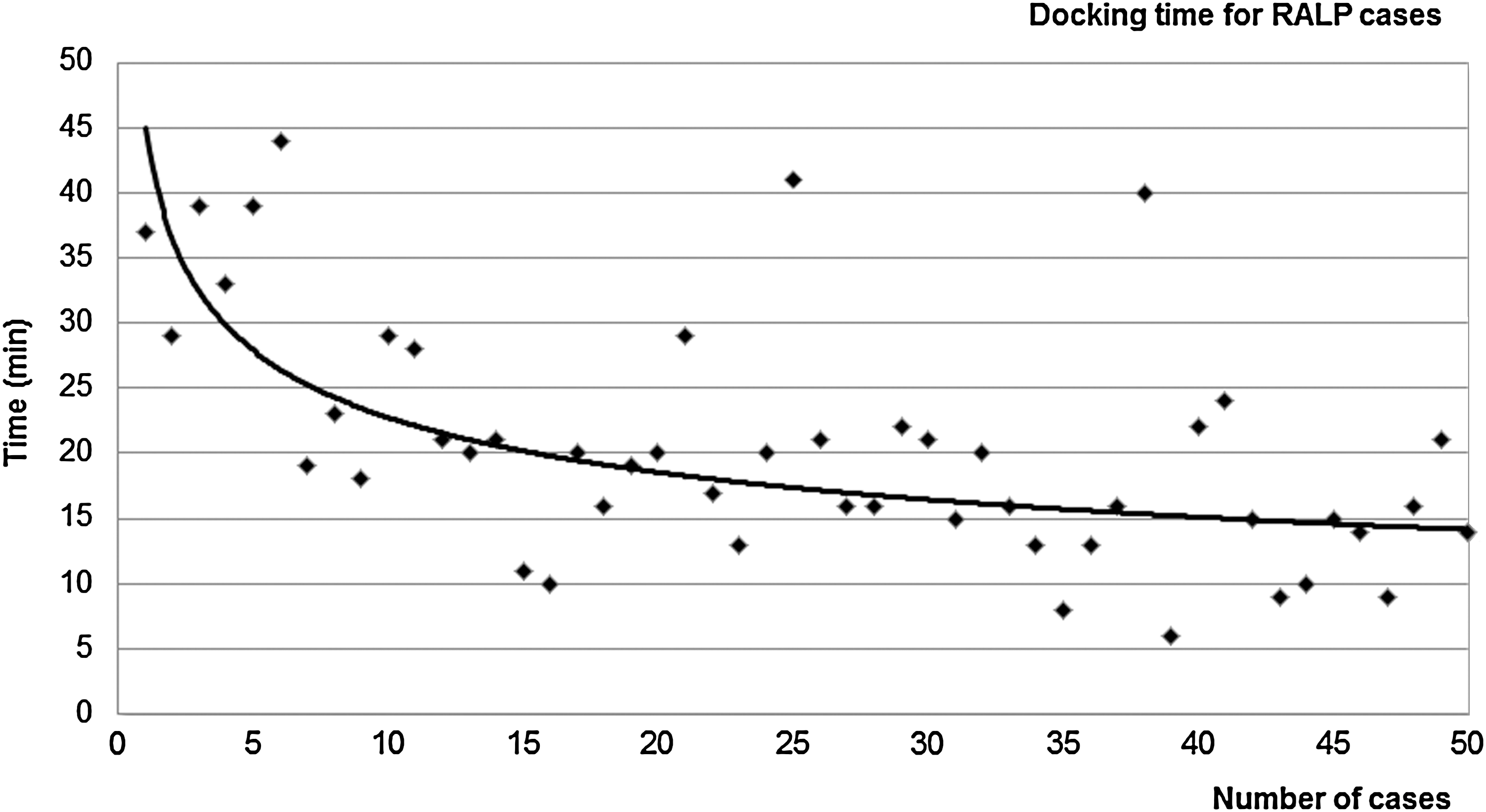
Transition in docking time for the robot-assisted laparoscopic prostatectomy (RALP) group (in cases no. 26 and no. 40, extensive laparoscopic adhesiolysis before docking was necessary).
Chi-square test.
Fisher exact test.
Wilcoxon rank sum test.
SD=standard deviation; Hct=hematocrit.
There were no conversions from RALP to open surgery. A statistically significant difference was noted in terms of estimated intraoperative blood loss and postoperative decrease in Hct (Table 2). Mean (SD) estimated blood loss was 513 (343) mL for RRP and 132 (151) mL for RALP (P<0.001). In terms of transfusion rates, no statistically significant difference was noted between the two groups (transfusion rates in RRP and RALP were 8% and 2%, respectively, P=0.362). In all cases, blood was transfused in the recovery bay or in the postoperative ward. No intraoperative transfusions were administered in either of the two groups. Mean (range) hospital stay was 3.82 (2–7) days for RRP and 1.30 (1–3) days for RALP, and this difference was statistically significant (P<0.001).
Perioperative and early postoperative (28-day) complication rates are summarized in Table 3. In total, 78% and 88% of patients had an uneventful recovery in the RRP and the RALP group, respectively (P=0.183, chi-square test). According to the modified Clavien system, major complication rates (Clavien III+IV) for RRP and RALP were 4% and 2%, respectively (P=0.879, Fisher exact test). No Clavien Grade IIIb or IV were noted in either of the two groups. Minor complication rates (Clavien I+II) were 18% and 10% for RRP and RALP, respectively (P=0.250, chi-square test). In terms of late postoperative complications (>28 days), the rate of anastomotic strictures observed during follow-up was 8% for the RRP group and 4% for the RALP group (P=0.678, Fisher exact test).
RRP=radical retropubic prostatectomy; RALP=robot-assisted laparoscopic prostatectomy; GI=gastrointestinal.
The histopathologic data of the surgical specimen are summarized in Table 4. Overall, there were no statistically significant differences between the two patient groups. The overall (T2 and T3) PSM rates were 20% for RRP and 18% for RALP (P=0.799, chi-square test). For pT3 disease, the PSM rates were 26.1% for RRP and 22.2%% for RALP (P=0.53, chi-square test).
Fisher exact test.
Chi-square test.
RRP=radical retropubic prostatectomy; RALP=robot-assisted laparoscopic prostatectomy; PSM=positive surgical margin.
Mean (SD) duration of follow-up was 32.5 (4.2) months and 19.5 (4.3) months for the RRP and RALP groups, respectively (P<0.001, Wilcoxon rank sum test). To overcome the difference in duration of follow-up and achieve meaningful comparisons in terms of short-term oncologic outcome, 12-month biochemical recurrence-free survival (BRFS) rates were compared between the two groups. The 12-month BRFS rates were 88% for RRP and 92% for RALP (P=0.505, chi-square test). To date, no case of port site metastasis was reported in the RALP group.
Early (3-month) continence rates were 88% for RRP and 90% for RALP (P=0.749, chi-square test). Among patients who were potent preoperatively without the use of oral phosphodiesterase type 5 (PDE-5) inhibitors and underwent unilateral or bilateral nerve sparing, early (3-month) recovery of erectile function with or without PDE-5 inhibitors was achieved in 60.6% in the RRP group and in 62.1% in the RALP group (P=0.893, chi-square test).
Discussion
In 2001, Binder and Kramer 10 performed the first RALP, and since then, the technique has been widely adopted at a rapid rate. Perhaps one of the major advantages of RALP is the reduction of the learning curve, compared with standard laparoscopic surgery. 11,12 Many surgeons experienced in open surgery are currently adopting RALP. Nevertheless, the existence of a learning curve still appears to influence results and is considered an issue of utmost importance in the context of proper patient counseling. 13 –17
A number of studies have focused on the comparative analysis of oncologic and functional outcomes for RRP and RALP. 15 –22 Some studies have also attempted a comparison of outcomes between RALP during the learning curve and RRP performed by surgeons experienced in open surgery. 21 –23 The findings of these studies, however, may be limited by a bias in favor of RRP, because outcomes of less experienced robotic surgeons are compared with outcomes from surgeons experienced in open surgery. To overcome this limitation, we attempted to compare the results of the learning curves for both RRP and RALP performed by the same surgeon.
While robotic technology facilitates the acquisition of some of the necessary skills, the initial learning curve of RALP remains daunting. RALP is a complex and technically demanding operation, the results of which depend on the experience of the surgeon. 13 According to the findings by Zorn and associates, 14 lack of laparoscopic experience does not have a negative impact on the learning curve for RALP. Many of the skills acquired with RRP are transferrable to RALP, but some aspects of RALP, such as the different approach (retrograde in RRP vs antegrade in RALP) and the functions of the robotic console, pose a challenge, even for a surgeon experienced in open surgery.
Robot console time gradually decreases as surgical experience with RALP expands. 24 As expected, during the learning curve, operative times were longer for RALP vs RRP, and the so-called 3-hour proficiency was not achieved during the first 50 cases. The number of cases needed to achieve the “3-hour rule” has not been clarified, and it may be as low as 25 to 50 cases 12 or it may exceed 100 cases. 23 When assessing operative times during the learning curve for RALP, the cases needed for the operating theater personnel to familiarize with the new technique should also be taken into account and the observed transition in docking times for RALP (Fig. 2) may reflect this fact. The learning curve does not only impact the console surgeon, but also the patient side assistant, anesthetist, and theater staff. A well trained, motivated team is vital for success.
In our cohort, blood loss with RALP was significantly lower compared with RRP. This consistent finding 2,16,22 could be attributed to the tamponade effect of pneumoperitoneum and the superior vision and high magnification of the robotic endoscope. Comparative studies 1,16,22 and database analyses 15,18 have also demonstrated that RALP is associated with lower transfusion rates compared with RRP. According to our findings, during the learning curve, transfusion rates were lower in the RALP group, but this difference was not statistically significant. This lack of statistical significance can be attributed to the small study sample. One should note, however, that modern RRP studies report transfusion rates as low as 0.5%. 25
Overall, the 28-day complication rate in the RALP group was lower, but this difference was not statistically significant. Previous single-center studies using the Clavien classification system have shown that RALP is associated with decreased rates of Clavien grade IIIb-IV complications. 16,21 One important finding in our study was the lower rate of anastomotic strictures associated with RALP (4% vs 8% for RRP). This difference is consistent with the existing literature 15,16,18,26,27 and may be attributed to the use of a running anastomotic suture and better visualization, contributing to a watertight anastomosis with the robotic approach.
The concept of “learning curve” is not confined to achieving acceptable operative times, but also refers to other important parameters for patient care such as oncologic and functional outcomes. Especially for functional outcomes (continence and potency), the learning curve is more difficult to approach objectively, because of the lack of standardized outcome reporting. The rates for postoperative continence were equivalent between the two groups and comparable to the results reported by others. 18,21,22 Tewari and colleagues, 19 however, have shown that the time interval to restoration of continence may be shorter after RALP. Potency rates (with or without PDE-5 inhibitors) were comparable between the two groups (60.6% vs 62.1% in the RRP and RALP groups, respectively). These rates are consistent with the findings of older studies. The 12-month potency rates for RALP and RRP were reported as 70% and 63%, respectively, by Krambeck and coworkers 27 and as 84% and 70% respectively by Menon and colleagues. 2
Because the long-term oncologic outcomes of RALP are not available, surrogate end points such as PSM rates have been extensively reported in the literature. According to the results from comparative studies of RALP vs RRP, PSM rates are highly variable. 19,20,28,29 Most of these studies have demonstrated lower rates of PSM for patients in the RALP group, even during the learning period for robot-assisted surgery. 28 In our series, the overall PSM rates (20% for RRP and 18% for RALP) were in accordance to current international experience. Vickers and associates 30 recently reported an overall PSM rate of 27% in a retrospective analysis of 7765 patients treated with RRP in four major American academic medical centers. They also showed that PSMs are strongly influenced by surgical experience. According to the findings of a multi-institutional study analyzing the results of 8418 RALP procedures, the overall PSM rate was 15.7%. 31 The role of margin status as a measure of cancer control, however, is an area of controversy. 30,32 PSA levels at 12 months postoperatively have limited clinical significance but may represent possible residual tumor/benign tissue or progression and they are worth considering in the context of comparative analysis.
Standardized fellowship and mentorship programs aim to shorten the learning curve for RALP, 33 but concerns in regard to the safety and efficacy of the procedure during early robotic experience still remain. These results have traditionally been compared with those of RRP performed by experienced surgeons. The current study, however, compares the outcomes of both RRP and RALP performed during the initial experience of the same surgeon. The institutional transition from open to robotic radical prostatectomy led to a change of the surgeon's practice from RRP to RALP in a consecutive fashion, thus allowing the comparison between the two learning curves. Patient selection for both procedures was based on identical institutional inclusion criteria, thus minimizing “adopter bias.” The follow-up protocol of the department was also the same during the study period. The modified Clavien system was used to assess perioperative and postoperative morbidity in a standardized manner.
The relatively short follow-up represents one of the main limitations of the present study. The sample size is small but reflects a unique situation created by an institutional change in practice. Since November 2008, RRP procedures were occasionally performed in the department, in the presence of specific contraindications for RALP (12 cases in total). This represents a barrier in extending the comparison between the two learning curves beyond the 50th case. The comparative assessment of functional outcomes (potency and continence) was based on definitions and did not include the use of validated questionnaires. A prospective study that involves the use of validated patient self-assessment tools is currently ongoing and aims to assess the trends in the surgeon's robotic learning curve.
Conclusion
The learning curve for surgery (improvement in surgical outcomes with increasing surgeon experience) remains primarily a theoretical concept. The learning curve is difficult to define and in essence it never ends, because surgical practice increases in parallel to experience. With the introduction of increasing numbers of robotic systems throughout the world, more newly qualified surgeons are performing robot-assisted surgery. In this study, we have shown that the early outcomes for a new robotic surgeon performing robot-assisted radical prostatectomy are comparable to those when the early procedures are performed through the open technique. The early learning curve for RALP appears safe and does not confer any increased risk to the patient both in terms of functional and oncologic outcome, when compared with the results of open surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.