
Abstract
Conventional laparoscopic dismembered pyeloplasty (LP) is an established alternative to open pyeloplasty given equivalent intermediate-term outcomes and decreased morbidity. Laparoendoscopic single-site (LESS) pyeloplasty has the potential to further decrease the morbidity of LP, while yielding superior cosmesis. It is, however, technically very challenging even with the use of an accessory port, largely because of the difficulty of intracorporeal suturing through a single umbilical incision. Application of the da Vinci robotic surgical platform to LESS pyeloplasty (R-LESS) has the potential to overcome these limitations. We describe our technique for R-LESS pyeloplasty using the da Vinci Si robot. We have found that use of the robotic system in conjunction with certain technique modifications helps to reduce the technical difficulty of LESS pyeloplasty and to shorten the physical learning curve associated with the procedure.
Introduction
Accordingly, efforts at further minimizing the morbidity of laparoscopic surgery led to the development and clinical application of laparoendoscopic single-site (LESS) surgery, which entails the use of a single abdominal incision via which a specialized multichannel port that accommodates articulating or bent instruments is inserted. 2 LESS surgery in urology has been shown to be feasible for a wide variety of procedures, yielding comparable perioperative outcomes to those of conventional laparoscopy, while resulting in superior cosmesis. 3 –8 Patient selection for LESS procedures remains highly selective, however, restricted to the few patients with minimal comorbidities.
For complex reconstructive procedures such as pyeloplasty, however, conventional LESS surgery is technically difficult. The loss of instrument triangulation, the difficulty of crosshanded surgery, and the reduced visibility and maneuverability associated with the coaxial orientation of instruments relative to the laparoscope all add to the technical challenge of the already complex task of intracorporeal suturing, despite the frequent use of an accessory port to enhance triangulation. 5,6 Complication rates early in the surgical experience approached 50% in one series, underscoring the steep learning curve associated with the procedure. 9
Use of a robotic surgical platform can potentially minimize some of these limitations. During robot-assisted laparoendoscopic single-site (R-LESS) surgery, instruments remain crisscrossed at the umbilicus to maximize triangulation, but the robotic console is reprogrammed for intuitive instrument control such that the left instrument is controlled by the right hand effector and vice versa. 10 Early clinical reports have demonstrated the feasibility of R-LESS for a variety of urologic procedures. 11,12 We have recently reported our perioperative outcomes for our initial series of 10 patients, and here describe our technique for R-LESS pyeloplasty using the da Vinci® Si robotic surgical system (Intuitive Surgical, Sunnyvale, CA). 13
Technique
Patient preparation
All patients undergo a bowel cleansing preparation with magnesium citrate on the day before surgery. First the patient undergoes cystoscopy with insertion of a Double-J ureteral stent. The patient is then placed in a partial flank position with the anterior superior iliac spine over the table break. The table is gently flexed to maximize the distance between the costal margin and the pelvic girdle, and adjusted such that the torso is in a relatively horizontal plane. The ipsilateral arm is secured in a neutral, straight position to the patient's side, to accommodate docking of the robotic arms (Fig. 1).

Patient positioning.
Port placement
We use a transperitoneal approach in all cases. A 3-cm curvilinear intraumbilical incision is made along the natural skin fold, and dissection is carried down to the anterior abdominal fascia using a combination of electrocautery and blunt dissection. The 2-0 polyglactin holding stitches are placed alongside a planned vertical fascial incision after which the anterior fascia and underlying transversalis fascia and peritoneum are incised, entering the peritoneal cavity.
A GelPoint® access platform (Applied Medical, Rancho Santa Margarita, CA) is inserted into the umbilical incision; this is preloaded with two pediatric 5-mm robotic ports, a 12-mm standard laparoscopic camera port, and a 12-mm assistant trocar, spaced by 3 cm in a diamond-shaped configuration (Fig. 2). The abdomen is insufflated through the insufflation port on the GelPoint. 14 The camera port is placed at the apex of the triangle, the robotic ports at the base, and the assistant port is subtended below the two robotic ports. For right-sided procedures, a 3-mm subxiphoid liver retractor is used if necessary (Fig. 2). A conventional 30-degree laparoscope is used to inspect the abdomen after obtaining access to rule out visceral injuries or potential obstacles to completing the R-LESS procedure.
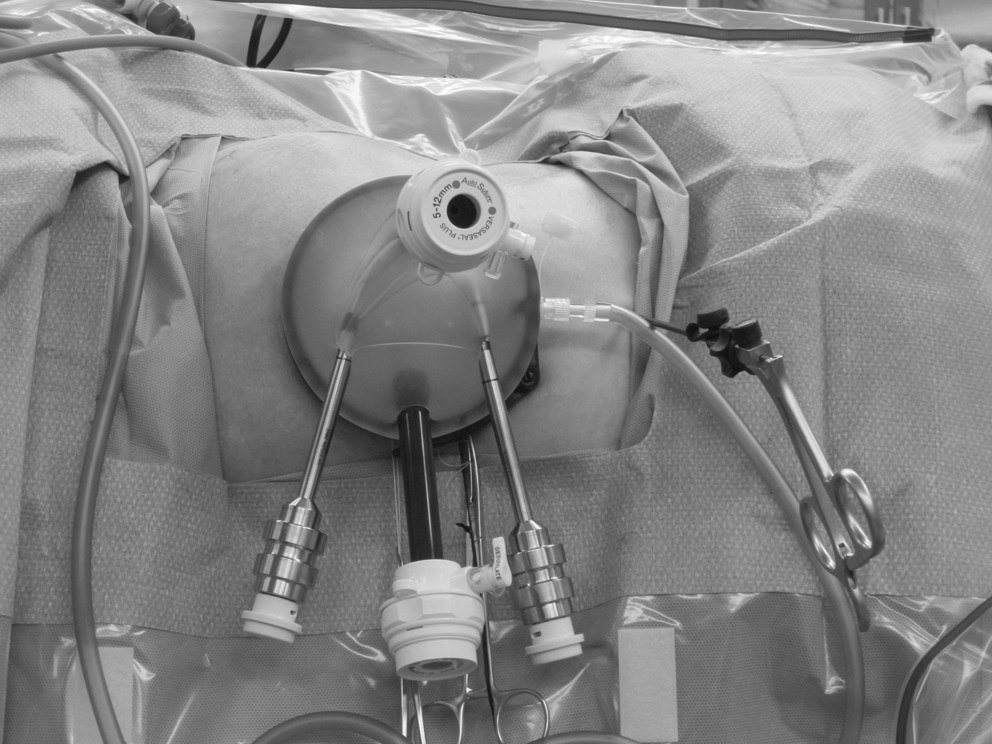
Port placement.
Docking the robot
We use a da Vinci Si robot that has smaller profile robotic arms than earlier generations, helping to reduce external clashing between the arms and/or camera. A 10-mm robotic camera lens in a 30-degree upward orientation is inserted through the camera port. After docking the robotic arms, the robotic ports are adjusted under direct vision, such that their remote centers of motion (black lines) are placed at the level of the anterior abdominal fascia. Use of the camera lens in a 30-degree upward orientation through the superior port helps to further diminish external robotic arm clashing and preserves access to the assistant trocar (Fig. 3). A left 5-mm hook cautery (or scissors) and a right 5-mm tissue grasper are inserted through the respective robotic ports, crisscrossing these at the level of the skin incision. The robotic console is programmed such that the surgeon's right hand controls the left-sided instrument and vice versa, resulting in intuitive manipulation of the instruments.

Docking the da Vinci Si robot.
Surgical technique
Given the space constraints at the patient's bedside, the surgical assistant is able to provide only limited help. The assistant, however, performs tasks such as instrument exchange, suction to clear the operative field, insertion and removal of sutures, and clipping of blood vessels when needed, among others. Throughout the procedure, the robotic camera lens and instruments must be moved synchronously, given their coaxial orientation relative to each other. Meticulous attention is paid to scaling down the degree of excursion of the instruments relative to the camera with each move.
Medial reflection of the colon and abdominal viscera is first performed. The ureter and renal pelvis are identified and mobilized. If present, crossing vessels are dissected and preserved, and the ureter and renal pelvis are circumferentially dissected posterior to the crossing vessels using a combination of cautery and blunt dissection. Meticulous hemostasis is maintained throughout, to minimize the need for assistance through the assistant trocar, given the limited working envelope.
A sufficient amount of ureter and renal pelvis that would enable a tension-free anastomosis after ureteropelvic junction (UPJ) dismemberment is mobilized. The ureter is sharply transected above the level of obstruction, and any abnormal segment of the UPJ is excised, care being taken to avoid cutting the preplaced stent. The proximal pigtail of the Double-J ureteral stent is then pulled out of the renal pelvis, without displacing the stent distally. Next the renal pelvis and ureter are then both spatulated for approximately 1.5 cm, cutting the ureter along its lateral aspect. The robotic grasper and scissors are exchanged for two 5-mm robotic needle drivers. 3-0 polyglactin suture is introduced through the assistant port, and a running anastomosis is performed over the stent in the standard fashion. During dissection and sewing, it is often necessary to transpose the left and right-handed instruments (switch which one is on top and bottom), to maximize retraction or optimize needle angles respectively (Fig. 4A–C).
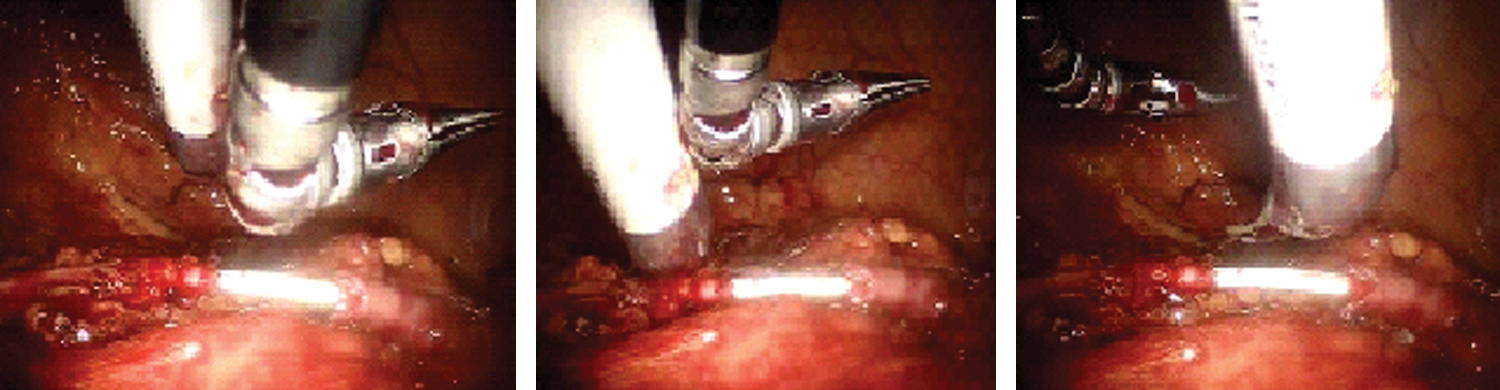
Transposition of instruments during dissection and sewing.
After the final needle is removed from the abdominal cavity, a 10F round drain is positioned lateral to the anastomosis and is retroperitonealized by reapproximating the colon to the lateral abdominal wall using Hem-o-lok clips. It is externalized through the umbilical incision or a separate small lateral stab incision. All ports and the GelPoint device are removed, and fascia and skin are closed.
Instruments/Equipment
• 21F, 30-degree cystoscope
• 0.038-inch guidewire
• Double-pigtail ureteral stent
• GelPoint device
• Standard 30-degree laparoscope
• Two 12-mm trocars
• Two 5- or 8-mm robotic trocars
• Robotic 5-mm articulating grasper
• Robotic 5-mm hook cautery device
• Robotic 5-mm scissors
• Robotic 5-mm needle drivers×2
• Laparoscopic suction/irrigator device
• Laparoscopic needle driver
• Hem-o-lok clip appliers; 5-mm/10-mm
• 3-0 polyglactin sutures on RB-1 needles
• 10F Blake drain
Role in Urologic Practice
LESS pyeloplasty, although feasible, is technically very challenging. In our initial experience, we have found that application of the da Vinci Si robotic platform with technique modifications as described above helps to significantly improve the technical ease of LESS pyeloplasty, eliminate the need for an accessory port to facilitate the anastomosis, and to shorten the physical learning curve associated with the procedure. R-LESS is not without its own challenges. The current robotic platform and instruments are not specifically designed for LESS surgery. There are robotic platforms already in clinical use in Europe and pending FDA approval in the United States that facilitate the use of LESS surgery.
Experience with conventional laparoscopic surgery, however, remains an important factor for success with R-LESS pyeloplasty. Pending further study and evaluation of longer-term outcomes, its role as an alternative approach to the minimally invasive surgical management of UPJ obstruction remains to be verified.
Footnotes
Disclosure Statement
No competing financial interests exist.