
Abstract
Background and Purpose:
Current guidelines recommend routine second transurethral resection (TUR) for accurate diagnosis and to prevent understaging of muscle-invasive bladder cancer. We evaluated the diagnostic accuracy of immediate second resection of the tumor bed during initial TUR and its prognostic significance.
Patients and Methods:
Patients (n=126) undergoing TUR were prospectively randomized to undergo (n=63) or not undergo (n=63) immediate second resection of the tumor bed after complete TUR. Second resection was repeated until muscularis propria (MP) was identified in the specimen and the depth of tumor invasion was inspected. The results of second resection were compared with final pathology results for diagnostic accuracy. Recurrence and progression rates were compared in the two groups, and factors affecting recurrence were evaluated.
Results:
Patient age, sex distribution, number of tumors, pathologic T stage and grade were similar in the groups. MP was included in all TUR specimens in the immediate second resection group, compared with 41 of 63 (65.1%) in the nonsecond resection group. The concordance rate of second resection with final pathology was r=0.810 (P<0.01). The sensitivity and specificity of second resection for T2 disease were 90.9% and 98.0%, respectively, and the positive and negative predictive values of second resection for T2 disease were 90.0% and 96.2%, respectively. Among the 94 patients followed up, those in the second resection group had significantly higher 2-year recurrence-free survival rate (77.0% vs 45.8%, P=0.025), but there was no difference in progression-free survival rate.
Conclusions:
Immediate second resection of the tumor bed after complete TUR improves the effectiveness of resection by immediately confirming the presence of MP in the specimen and accurately differentiating muscle-invasive disease. The advantages of immediate second resection were precise prediction of final pathology results and reduced early recurrence.
Introduction
Although a second TUR may identify patients with poorer prognosis and may improve patient outcomes, 6 this second TUR may imply failure of initial technique and another surgery after TUR potentially poses inevitable surgical morbidity as well as economic burden to the patient. Thus, several new techniques have been proposed to improve the quality of TUR, including transurethral en bloc resection, 7 en bloc holmium laser resection, 8 and transurethral Tru-Cut® biopsy. 9 As yet little has been clarified regarding the quality of the obtained specimens, and they may necessitate special additional instruments.
To overcome these drawbacks, we investigated whether immediate second resection during TUR could confirm the presence of MP in the specimen, provide a more accurate pathologic diagnosis, and improve the recurrence-free survival (RFS) rate of patients with NMIBC.
Patients and Methods
Patients
Between January 2008 and December 2009, a total of 126 consecutive patients undergoing TUR by a single surgeon (HA) were randomized into two groups, with 63 patients undergoing immediate second resection and 63 not undergoing second resection. Patients were included if (1) the major axis of tumor was >2 cm, (2) there were two or more tumors, (3) the patient had previous intermediate or high-risk tumors, (4) the tumors were nonpapillary, and (5) the tumors had a broad-based shape.
Randomization protocol
In the immediate second resection group, after complete TUR grossly, TUR of the tumor bed was performed, and the result was confirmed by the frozen biopsy results during TUR, TUR was repeated until MP was included in the specimen; the depth of tumor invasion was also determined. Eleven (17.5%) patients needed a further resection because of the absence of MP in the first frozen specimen. In five patients, multiple cold cup biopsies were performed instead of TUR to avoid bladder perforation. In the nonsecond resection group, no additional procedures were performed after complete TUR.
Patient follow-up
Twenty five (19.8%) patients underwent cystectomy within 3 months after TUR, 12 in the second resection group, comprising 4 with T1G3 and 8 with T2 disease, and 13 in the nonsecond resection group, comprising 2 with T1G3 and 11 with T2 disease. Among the remaining 97 patients with NMIBC who were followed up, 21 in the second resection group and 26 in the nonsecond resection group received intravesical bacilli Calmette-Guérin (BCG) instillation therapy weekly for 6 weeks. The mean follow-up period was not different between the groups (second resection group 16.0±7.69 mos, nonsecond resection group 17.2±9.32 mos). Our follow-up protocol after TUR of the bladder includes cystoscopy, urinalysis, and voided urine cytology every 3 months for 1 year, biannually for the next 2 years, and then annually. In the case of high-risk disease, first year protocol was extended to the first 2 years.
Data analysis
The diagnostic accuracy of immediate second resection was evaluated by comparison of frozen biopsy results and final TUR pathology, with the concordance rate determined by Pearson correlation analysis. The sensitivity, specificity, positive predictive value, and negative predictive value of pathology results for T2 disease were determined by chi-square tests. RFS and progression-free survival (PFS) were determined by the Kaplan-Meier method and compared using the log-rank test. Multivariate analysis using a Cox proportional hazards model was used to determine independent variables predictive of tumor recurrence. P<0.05 was considered statistically significant.
All data were collected after local ethics committee approval and all patients signed informed consent previously accepted by the committee.
Results
MP was confirmed in all final TUR specimens in the second resection group, compared with 41 of 63 in the nonsecond resection group (65.1%), including 46.9% of patients with Ta, 72.2% with T1, and 100% with T2 disease. There were no differences between the groups in age, sex, number of tumors, largest tumor diameter, T stage, or tumor grade (Table 1). None of the patients experienced any complications related to immediate second resection.
TUR=transurethral resection; SD=standard deviation; T=tumor; CIS=carcinoma in situ; MP=muscularis propria.
Of the 11 patients who received a diagnosis of muscle-invasive cancer on immediate second resection, 10 were found to have T2 disease and 1 had T1 disease; in the latter patient, a second TUR was performed to confirm NMIBC. Of the 52 patients who had a diagnosis of NMIBC on immediate second resection, 50 were confirmed as having NMIBC, including 32 with Ta, 16 with T1, and 2 with CIS; 2 patients had T2 disease. The concordance rate between frozen pathology and TUR pathology results was r=0.810 (P<0.01). In detecting T2 disease, immediate second resection had a sensitivity of 90.9%, a specificity of 98.0%, a positive predictive value of 90.0%, and a negative predictive value of 96.2%.
Of the 97 patients followed-up, 31 (32.0%) experienced tumor recurrence, including 8 of 47 (17.0%) patients in the immediate second resection group and 23 of 50 (46.0%) patients in the nonsecond resection group (P=0.002). The 1-year and 2-year RFS rates were 87.5% and 77.0%, respectively, in the immediate second resection group, compared with 62.0% and 45.8%, respectively, in the nonsecond resection group (Fig. 1, log-rank P=0.025), In the high-risk group (any T1 or TaG3), 2-year RFS rate of the immediate resection group was higher than the nonresection group (72.5% vs 42.0%, log-rank P=0.015). In the low-risk group, no significant difference was detected between the group (49.6% vs 47.4%, log-rank P=0.085). On multivariate analysis, the immediate second resection was an independent prognostic factor for RFS (P=0.004) along with tumor grade (P=0.018) (Table 2).
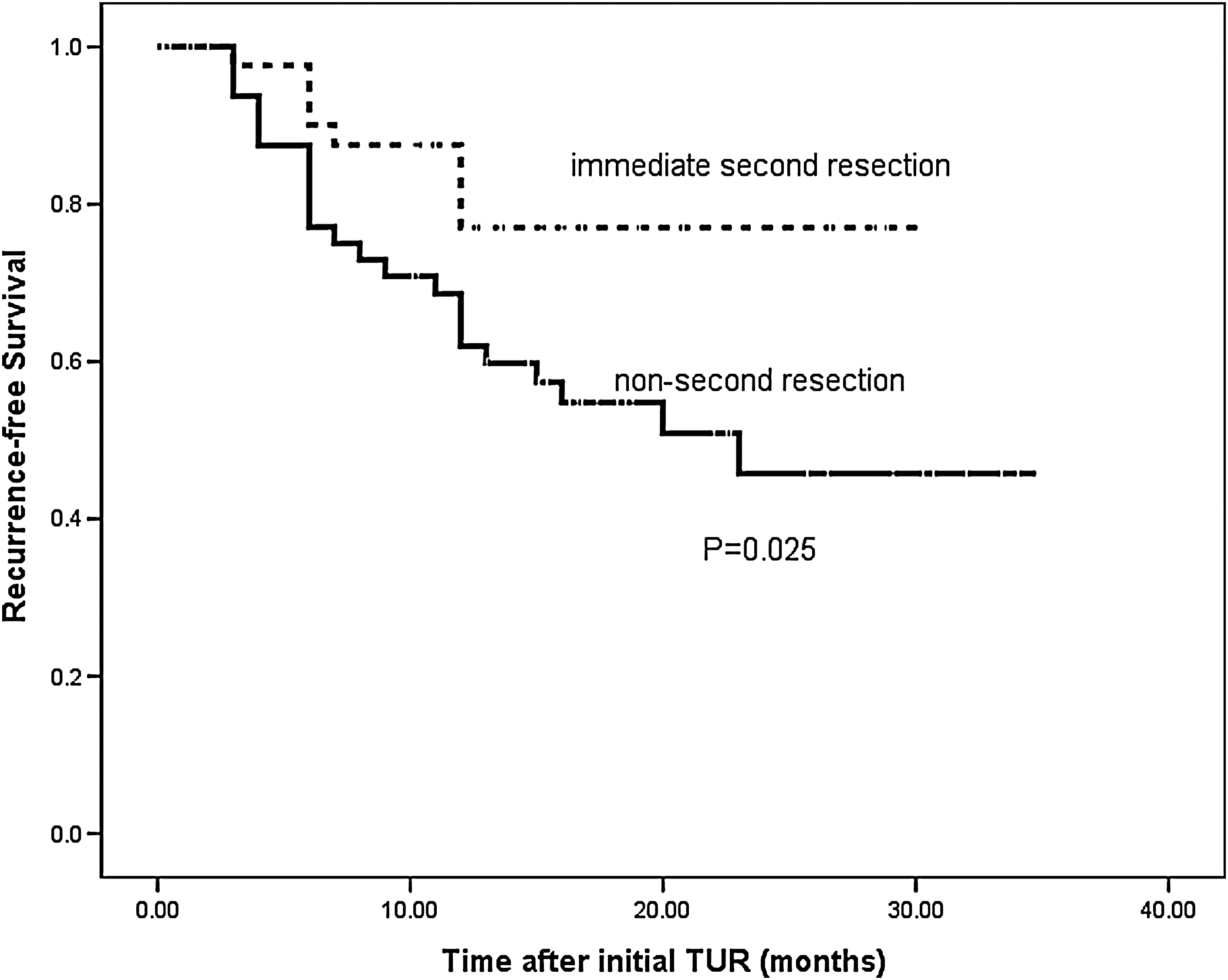
Kaplan-Meier curves of recurrence-free survival rates in the immediate second resection group and nonsecond resection group. TUR=transurethral resection.
HR=hazard ratio; CI=confidence interval; T=tumor; BCG=bacille Calmette-Guérin; TUR=transurethral resection.
Recurrence at the first follow-up cystoscopy occurred in six patients, all in the nonsecond resection group (12.0%), with three having recurrences at the previous TUR site. PFS rate did not differ between the second resection (97.4%) and nonsecond resection (80.1%) groups.
Among the patients in the immediate second resection group who underwent cystectomy, one (25.0%) showed upstaging and four (33.3%) showed downstaging. In the nonsecond resection group, two patients (100%) were upstaged and one (9.1%) was downstaged.
Discussion
A complete and correct TUR is essential for correct assessment of bladder tumors. Despite TUR and immediate postoperative intravesical instillations, the early recurrence rate in patients with NMIBC is high, up to 45%. 10 It is commonly believed that early recurrences are, in fact, residual or overlooked tumors present at initial TUR, strongly emphasizing the importance of TUR quality. Residual tumors at second TUR have been reported to be present in 20% to 78% of patients with NMIBC. 3,11 –15 The presence of MP in the tumor specimen is crucial for accurately discriminating stage and is important for TUR quality. 4,16,17 Of TUR of bladder tumor (TURBT) specimens, however, 15% to 66% lack MP, 2,3,18 –20 and this lack may result in understaging of tumors and suboptimal treatment. Absence of muscle has been shown to be a significant predictor of clinical understaging, with understaging reported in 64% of tumors without and 30% of tumors with MP in the biopsy specimen. 4
We found that a major advantage of immediate second resection after complete TUR was our ability to confirm the presence of MP in specimens before the end of the initial procedure. Although two-thirds of Ta disease in the nonsecond resection group failed to have proper muscle in the pathology specimen, it does not seem to have an influence on the decision for further treatment or the prognosis of the disease. As for T1 disease, however, despite visual certainty of cutting the proper muscle layer in the nonsecond resection group, MP was not contained on the pathology specimen in one-third of the cases. These patients may have been understaged and at higher risk for disease recurrence and/or progression. Our recurrence data confirmed our ominous prognostication.
To improve the effectiveness of initial TUR, new TUR techniques have been introduced to overcome the limitations of conventional TURBT. Transurethral resection in one piece was found to be an accurate pathologic staging tool for bladder cancer. 7 In 82% of tumor specimens, a portion of the MP was attached beneath the tumor base, whereas in the remaining 18%, the MP was absent or its presence was uncertain. Although this technique represented a significant improvement in obtaining MP in specimens, it still failed to obtain MP in a substantial number of tumors.
Tru-Cut biopsy guns have been used to obtain cross-sectional core specimens containing all histologic layers in one piece, with all samples showing muscle invasion on histopathologic examination of tissue cores. 9 This method, however, is indicated only for patients with large bladder tumors, highly suspected of muscle invasion. Its diagnostic yield may be lower in patients with less invasive tumors, and the puncture procedure carries a risk of direct tumor implantation outside the organ. In contrast, our method has several advantages, in addition to improving diagnostic accuracy: It is familiar to every urologist; it does not necessitate additional instruments or training; and it may have additional therapeutic benefits, including further resection, even in patients with NMIBC.
The underestimation of T2 disease on initial TUR was reported to be 9.1% in patients who underwent second TUR. 3,12,13,21 –23 Immediate second TUR of the tumor bed could accurately differentiate T2 from T1 disease in 89.7% of patients, comparable to results from second TUR studies (Table 3). A conventional second TUR can increase RFS and PFS. The decreased recurrence rates after second TUR in two recent randomized studies may be because of the removal of residual tumor on second TUR or a change in treatment (eg, cystectomy).
Differentiate T2 from T1 disease.
TUR=transurethral resection.
In one study, in which patients routinely received adjuvant chemotherapy, the 2-year RFS rates were 77.7% and 42.3% in patients who did and did not undergo second TUR, respectively. In a long-term follow-up study after second TUR, 5-year RFS rates were 52% and 21% in second TUR and no second TUR group, respectively. In their study, 2-year RFS rates were approximately 70% and 50% in the second TUR group and initial TUR only group, respectively. 24
Although it is difficult to directly compare these results with ours because of different distributions of tumor stage and grade, we found that the 2-year RFS rates of our immediate second resection group were similar to rates observed in patients who underwent a second TUR. These findings suggest that our immediate second resection method has diagnostic as well as therapeutic advantages, comparable to a second TUR, because our method resected another whole layer of tissue instead of randomly sampling several sites. Further evidence that the immediate second resection improved the completeness of TUR was the absence of early recurrence at first follow-up cystoscopy.
The initial resection site has been reported to be the most common (26%–81%) site of recurrence at first follow-up cystoscopy, suggesting that this recurrence is because of residual tumor from the previous resection. 14,25 Recurrence at first follow-up cystoscopy, dbecause of primarily incomplete tumor resection, is a strong predictor of subsequent recurrence and possibly even prognosis in patients with T1 and/or higher-grade disease. 10 We observed recurrence at first follow-up cystoscopy in 12% of patients in the nonfrozen biopsy group, with half these recurrences at the previous resection site. Furthermore, one-third of the cystectomized specimens in the frozen biopsy group resulted in downstaging from T2 to T1 disease, compared with 9.1% in the nonfrozen biopsy group.
Second TUR has been reported to affect recurrence after TUR, along with traditional factors such as tumor stage, grade, multiplicity and size of tumor, previous recurrence, and intravesical BCG treatment. 26 –29 Our multivariate analysis showed that immediate second resection of the tumor bed had the greatest impact on recurrence, followed by tumor grade. In contrast, we did not observe effects of tumor multiplicity, size, or stage on recurrence. It can be explained that most patients with T1 disease or multiple, large Ta tumors received BCG treatment and a substantial portion of patients with multiple, large T1G3 tumors (25% of T1G3 tumors) underwent early cystectomy. Patients who underwent cystectomy were excluded from follow-up analysis. Of 29 T1 patients (1 with grade 1, 10 with grade 2, and 24 with grade 3), six with T1G3 tumors were excluded because of cystectomy. This exclusion may be responsible for this discrepancy with other study.
In the view of grade, two years after TUR, the recurrence rate was significantly increased. Moreover, performing frozen biopsy may have proved the most impactful on recurrence, because frozen biopsy made a distinct difference at early recurrence and our follow-up was insufficient. Further analysis with longer follow-up is necessary to solidly confirm our results.
Although our patients were well randomized and our frozen biopsy method is familiar to urologists, immediate second resection of the tumor bed has some limitations. First, there were some technical difficulties because of separate complete resection of the resection floor in the thin-walled bladder. To overcome these problems and to obtain a noncauterized specimen, we sometimes used cold cup biopsy. Second, although this procedure did not increase surgical morbidity, it increased overall operative time. Third, follow-up was too short to accurately compare RFS or PFS. Additional follow up is warranted to confirm our preliminary results.
Conclusions
Immediate second resection of the tumor bed after complete TUR improves the effectiveness of resection by immediately confirming the presence of MP in the specimen and accurately differentiating muscle invasive disease. The diagnostic and therapeutic advantages of this procedure were more precise prediction of final pathology results and reduced rate of early recurrence.
Footnotes
Disclosure Statement
No competing financial interests exist.