
Abstract
Background and Purpose:
Recent literature has focused on the importance of maximal nephron preservation during partial nephrectomy to avoid complications associated with chronic renal insufficiency. Accurate differentiation of tumor from normal surrounding parenchyma is critical to ensure excessive normal renal tissue is not made ischemic or excised along with the tumor. The feasibility of a novel intraoperative imaging technique to differentiate tumor from surrounding parenchyma during laparoscopic and robot-assisted partial nephrectomy was evaluated.
Patients and Methods:
Patients who were scheduled to undergo laparoscopic or robot-assisted partial nephrectomy were recruited from April 2009 to July 2010. The Endoscopic SPY Imaging System was used as an adjunct to intraoperative imaging in all cases. Patients received intravenous injections of indocyanine green (ICG), which was visualized intraoperatively with the near infrared fluorescence (NIRF) imaging capability of the SPY scope. The degree of tumor fluorescence compared with surrounding renal parenchyma was qualitatively assessed before tumor resection, and partial nephrectomy was then performed with standard techniques while intermittently using NIRF imaging.
Results:
Nineteen patients underwent intravenous administration of ICG followed by NIRF during partial nephrectomy. Average tumor size was 3.0 cm (range 0.8–5.9 cm). Thirteen masses were malignant on final pathology results, and all of these were seen to be hypofluorescent compared with surrounding renal parenchyma during intraoperative imaging. The imaging behavior of benign tumors ranged from isofluorescent to hyperfluorescent compared with normal parenchyma. No complications were associated with ICG injection.
Conclusion:
NIRF imaging after intravenous ICG administration may be a useful intraoperative imaging tool to differentiate malignant tumors from normal renal parenchyma during laparoscopic and robot-assisted partial nephrectomy. Advanced intraoperative imaging techniques such as this one may become increasingly helpful as more complicated tumors are resected with minimally invasive approaches.
Introduction
Advances in surgical technology have now made it feasible to resect most renal tumors with a robot-assisted or pure laparoscopic approach. 7,8 Even complex partial nephrectomies are now being performed routinely with minimally invasive techniques. 9 –11 As the importance of nephron preservation becomes increasingly clear and more challenging cases are undertaken, advanced intraoperative imaging techniques may become necessary to help maximize the benefits of partial nephrectomy. Intraoperative ultrasonography has been used most commonly for this purpose and certainly has a role in this procedure. 12 It can be cumbersome to use for some tumors, however, and its utility is variable based on operator-dependent factors. An ideal intraoperative imaging adjunct would allow accurate differentiation of tumor tissue from normal parenchyma, monitoring of regional kidney ischemia after arterial clamping, and simultaneous use in real time during tumor resection.
We have previously reported the feasibility of near infrared fluorescence (NIRF) imaging of intravenously injected indocyanine green (ICG, Akorn, Lake Forest, IL) to aid in intraoperative imaging during open partial nephrectomy. 13 A recent advancement in the most commonly available robotic system has also allowed NIRF imaging integration directly into the surgical console. 14 Robotic technology, however, is not ubiquitous, and many centers with a surgical robot do not yet have NIRF capabilities. We therefore evaluated the Endoscopic SPY® Imaging System (Novadaq, Inc, Missisaugua, Ontario, Canada) and its feasibility for use during laparoscopic partial nephrectomy (LPN) and robot-assisted laparoscopic partial nephrectomies (RALPN).
ICG is a fluorescent tricarbocyanine dye that absorbs near infrared light and subsequently emits light at slightly longer wavelengths. ICG binds to albumin when intravenously injected and therefore remains primarily in the vasculature. It has been used during surgical procedures for cardiac, vascular, and ophthalmologic applications primarily as a method of angiography. 15 –17 The ICG dye is cleared by hepatic metabolism and is not nephrotoxic, making it an ideal agent for partial nephrectomy procedures.
The goals of this study were to evaluate the feasibility of the Endoscopic SPY Imaging System to assist with tumor identification during LPN and RALPN, as well as to evaluate any qualitative differences in fluorescent signal between different tumor histologies.
Patients and Methods
After Institutional Review Board approval, 19 patients who were scheduled to undergo LPN or RALPN signed informed consent to receive intraoperative injection of ICG followed by NIRF during their procedure. Demographic information, operative parameters, pathologic data, postoperative course, and follow-up data were recorded for all participants. All procedures were performed from April 2009 to July 2010 at the University of Rochester Medical Center by one of three experienced robotic surgeons. Inclusion criteria for the study were clinical tumor stage T1 or T2, no evidence of metastatic disease, and medical ability to tolerate a partial nephrectomy. Exclusion criteria included cirrhosis or other liver dysfunction; serum creatinine >2.0 mg/dL; history of allergy to ICG, iodine, or other intravenous contrast agents; active participation in another ongoing medical protocol; or other health conditions that made the subject a poor candidate for an investigational procedure (ie, significant congestive heart failure).
Of the 19 procedures performed, 2 were pure LPN procedures and the remaining 17 were RALPN procedures performed using the da Vinci Si Surgical System (Intuitive Surgical, Sunnyvale, CA). The imaging system used for all procedures was the Endoscopic SPY Imaging System (Fig. 1). This imaging system contains a near infrared light source that emits light at a wavelength of 806 nm, as well as a fluorescence capable camera attached to the endoscope that can detect the near infrared light fluoresced from the ICG molecule (approximate wavelength of 830 nm). The raw imaging output of this system is a grayscale image, with increasing amounts of fluorescence appearing brighter. A composite image (white light and NIRF) is also created, which includes a computer-generated green color corresponding to the degree of fluorescence seen on the grayscale images. This allows real-time viewing of white light and NIRF images simultaneously. During robotic procedures, the NIRF scope was inserted by the bedside assistant through a 12-mm port, with images displayed in the operating room on a separate monitor.

The Endoscopic SPY Imaging System.
ICG was diluted to a 2.5 mg/mL solution immediately before each case and was administered in discrete boluses intravenously by the anesthesia team as directed by the surgeon. Up to 7.5 mg of ICG was administered at a time, with additional amounts given as needed to obtain optimal fluorescence. The total doses of ICG ranged from 5 mg to 25 mg. Partial nephrectomy procedures were performed using standard techniques for LPN and RALPN. The kidney and renal hilum were dissected from surrounding tissues, and ICG was administered before arterial clamping. NIRF imaging was performed before clamping to assist with scoring of the tumor margin, as well as during tumor resection. Pathologic examination of all specimens was performed to correlate tumor histology with intraoperative findings.
Results
Table 1 lists the patient demographics, tumor characteristics, operative parameters, pathologic data, and outcomes. Seventeen patients underwent RALPN and the remaining 2 underwent pure laparoscopic partial nephrectomies. Mean radiographic tumor size was 3.0 cm (range 0.8– 5.9 cm) with a mean nephrometry score of 7.7 (range 4–10). One patient did not undergo renal arterial clamping. The mean warm ischemia time for the other 18 patients was 21.7 minutes (range 8–37). The patient with a warm ischemia time of 37 minutes had inadequate arterial control with a single bulldog clamp, and extra time was necessary to gain necessary vascular control (this patient was also the outlier for estimated blood loss with 1200 mL). There were no conversions to open surgery or radical nephrectomy.
One patient had negative margins on frozen section with focally positive margins at final pathology results.
One patient needed reexploration for postoperative bleeding.
EBL=estimated blood loss; GFR=glomerular filtration rate; ICG=indocyanine green.
On final pathology results, 13 patients had malignant lesions, including 10 conventional (clear-cell) and 3 chromophobe renal-cell carcinomas. The tumor margin demarcation was most apparent with NIRF imaging when the lesion studied was either hypofluorescent or hyperfluorescent (Fig. 2). All 13 malignant lesions were hypofluorescent compared with the surrounding normal renal parenchyma during intraoperative NIRF imaging (Fig. 3). The differentiation between tumor and normal kidney was easier to distinguish for more exophytic lesions with less parenchyma overlying them. For endophytic tumors, the hypofluorescent nature of the tumor was better appreciated once resection had commenced. The six benign tumors included three benign cysts, two angiomyolipomas, and one oncocytoma. Two of the benign cysts appeared hyperfluorescent and one was isofluorescent compared with surrounding parenchyma. The oncocytoma and one of the angiomyolipomas were isofluorescent compared with the adjacent tissue, while the second angiomyolipoma had prominent vessels that were strongly hyperfluorescent. All tissue margins were negative with the exception of one patient, whose intraoperative frozen section margins were called negative but final pathology results revealed a focally positive margin.
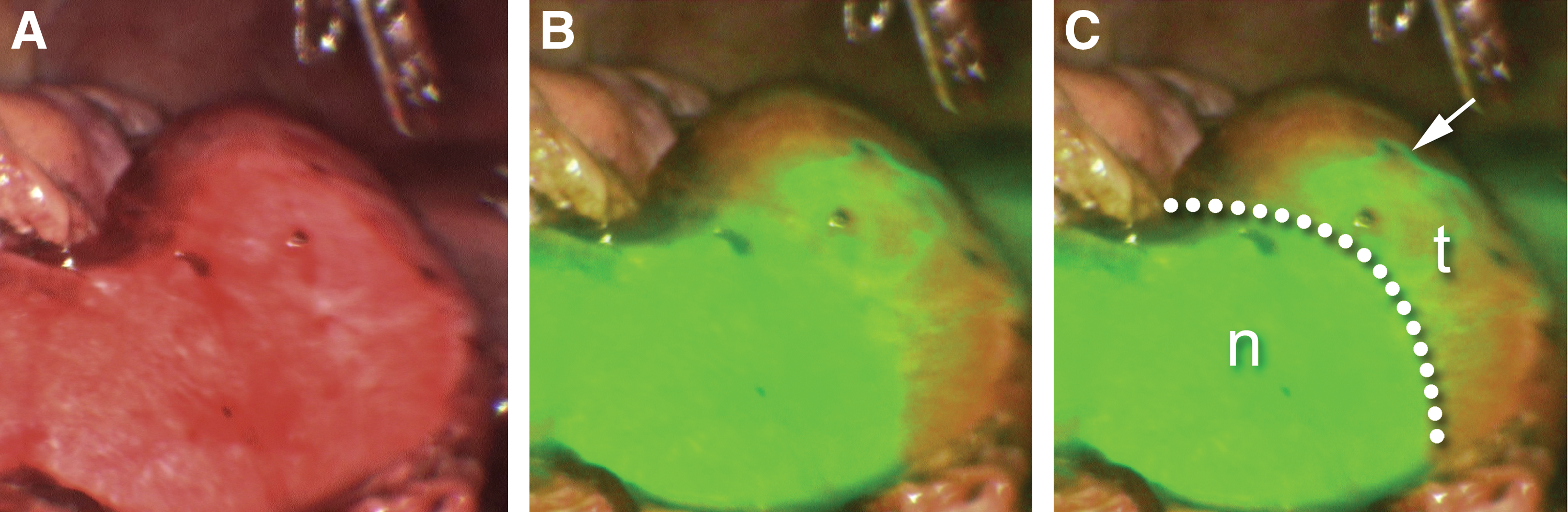
White light and near infrared fluorescence (NIRF) imaging. Traditional white light imaging demonstrates an indistinct margin between tumor tissue and normal kidney
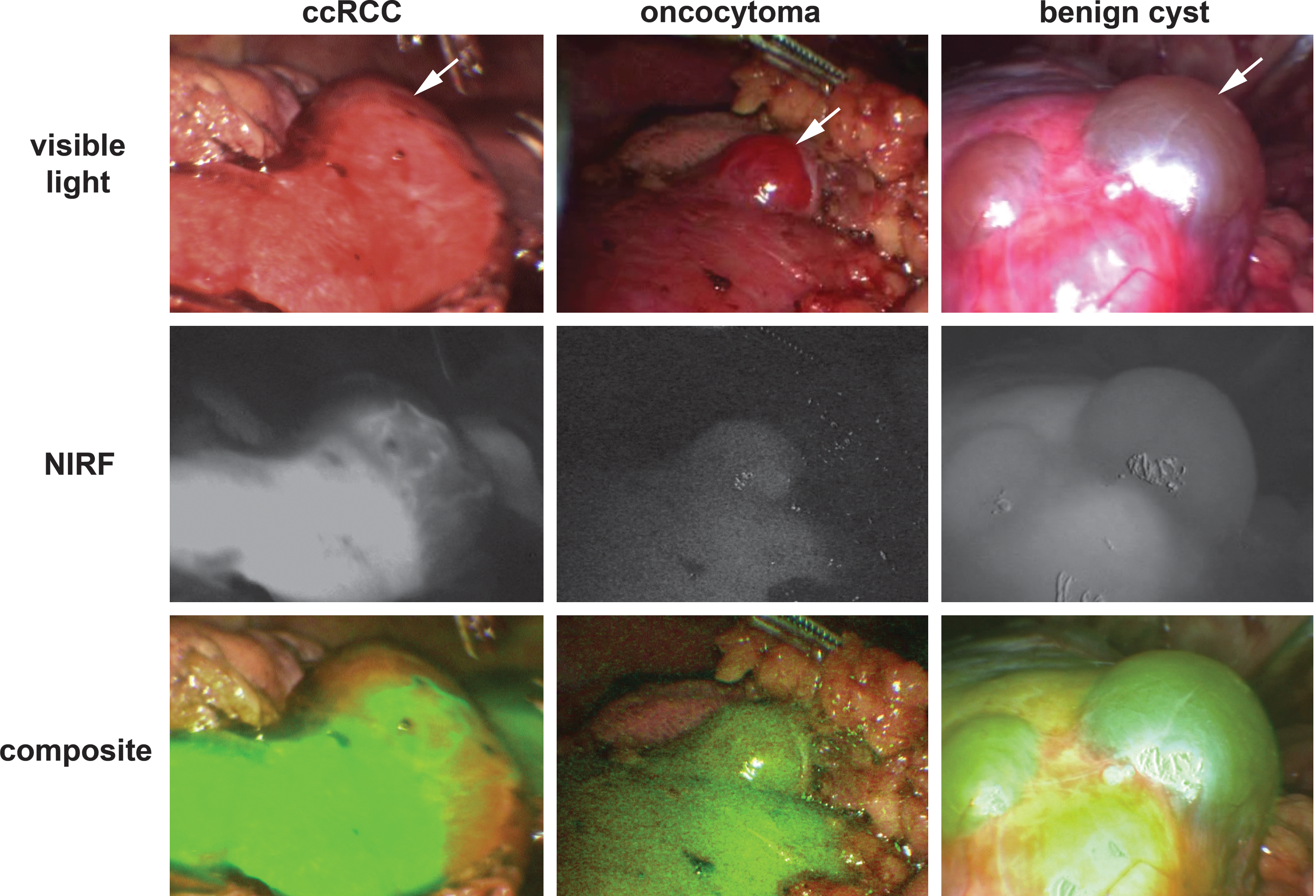
White light, near infrared fluorescence (NIRF) only, and composite imaging of different tumor histologies. The typical NIRF imaging characteristics of clear-cell renal-cell carcinoma (ccRCC), oncocytoma, and benign cysts are demonstrated. The ccRCC is seen to be hypofluorescent compared with surrounding parenchyma, oncocytoma is isofluorescent, and benign cysts appear hyperfluorescent.
There were no adverse events related to ICG injections either intraoperatively (as assessed by anesthesia based on vital signs and respiratory dynamics) or postoperatively (such as rash, itching, or hepatic dysfunction). One significant postoperative complication occurred in a patient who underwent an uneventful RALPN procedure. This patient was found to be bleeding in the postanesthesia care unit (as assessed by drain output and hemodynamics) and was taken back emergently to the operating room for open exploration. One of the Hem-o-lok clips used during the renorrhaphy had come undone, and the cut surface of the kidney was bleeding. This was controlled with reinforcing renorrhaphy sutures and the patient subsequently did well.
Discussion
Many of the recent advancements in surgical technology have involved surgical instruments, such as the multiwristed capabilities of the robotic surgical systems. Until very recently, however, intraoperative imaging had not progressed much beyond magnification to assist the surgeon with very fine dissections. Even the three-dimensional high-definition imaging available in robotic surgery (a significant advancement over the two-dimensional view of traditional laparoscopic surgery) affords only a traditional white light view of the operative field. With the increased utility of LPN and RALPN, the ability of the surgeon to use the sense of touch to discriminate subtle differences between types of tissue has diminished. Therefore, we believe that there is significant potential for improvement in terms of available intraoperative imaging technology. Certainly, not all procedures will need advanced imaging techniques, and many small renal masses have been removed without imaging adjuncts. With the migration towards larger, more complex tumors being removed with minimally invasive techniques, however, the need for better imaging is likely to grow.
Different types of intraoperative imaging modalities are currently under investigation for their usefulness during nephron-sparing procedures. The eventual goals of such technology would be to use preoperative and intraoperative imaging modalities to literally “cut on the dotted line.” Altamar and colleagues 18 have made initial forays into image-guided kidney surgery, whereby preoperative information obtained from CT and laser scanners is reconstructed in three dimensions and compared with intraoperative spatial information using robotic instruments. Ukimura and Gill 19 described several imaging-assisted surgical techniques, including the fusing of intraoperative ultrasonographic images or preoperative cross-sectional images with laparoscopic instruments outfitted with optical sensors to provide a real-time overlay of the area of interest in an operative field. They demonstrated real-time color-coded safety zones around the tumor based on the distance away from its margin, which actively change with the field if the camera or tissue are moved. Teber and associates 20 also reported on augmented reality during partial nephrectomy, whereby three-dimensional reconstructions of regional anatomy based on preoperative imaging are overlaid onto real-time surgical image acquisitions. The common goal of these improved intraoperative imaging techniques is to provide surgeons with more anatomic information than they can obtain with the naked eye, so that oncologic principles are maintained while maximizing safety to surrounding structures.
Near infrared imaging of intravenously injected ICG has several characteristics that make it a promising imaging adjunct during partial nephrectomy. ICG appears to be transported into the proximal tubule cells of normal renal parenchyma, while renal-cell carcinomas do not take up ICG, perhaps because of loss of a cell membrane transporter. 21 This provides a stark visual contrast between tumor tissue and normal parenchyma when imaged with NIRF light. In addition, the angiographic properties of ICG can be very useful for renal vasculature identification and control. Perhaps even more important, the highly vascular nature of the kidney can be used to monitor segmental perfusion deficits with NIRF imaging of ICG after renal hilar clamping—a segmental vessel can be clamped, ICG administered, and the regional perfusion deficit in the kidney can be readily identified. This allows confirmation that the area containing the tumor is ischemic, so that resection can occur in a bloodless field while maintaining perfusion to the remainder of the kidney. ICG is nonnephrotoxic and can therefore be used in patients in whom contrast-enhanced axial imaging is contraindicated.
In the current study, tumors appeared to have fluorescent properties that were fairly consistent based on histology. Most importantly, all of the malignancies were hypofluorescent compared with surrounding normal parenchyma. This provided a stark contrast that improved the confidence of the surgeon that the appropriate tumor margin had been identified. The benign lesions were all iso- or hyperfluorescent. It is possible that an intraoperative imaging modality similar to this one will eventually be able to accurately discriminate benign from malignant lesions, thereby obviating resection, but further study is needed. We believe, however, that the immediate future of this technology lies in the ability to monitor perfusion deficits and accurately identify the tumor margin during LPN and RALPN. This may not be necessary for all cases, but will likely be helpful during complex procedures where improved imaging could potentially lead to decreased ischemia time and blood loss. An additional advantage of the current system is that it can be used during both laparoscopic and robotic procedures, thereby improving the overall cost effectiveness.
There are several potential limitations of this pilot study. Three different surgeons each performed these procedures on a limited number of patients. More than one surgeon was present for the imaging portion in most cases, however. In addition, although surgical technique may differ slightly between surgeons, the imaging needs little operator involvement, and the images created did not appear to be different among the different surgeons. We did not have the ability to objectively quantify the relative degrees of fluorescence of the tissues that were being observed. Therefore, subjective determinations of qualitative fluorescence characteristics were necessary. Although exact measurements of fluorescent intensity may prove useful in situations with subtle differences between tissue types, the differences in relative fluorescence that we observed were quite obvious to the naked eye.
All patients underwent NIRF imaging of the kidney surface before arterial clamping, but its use at other times (such as during tumor resection) was variable. In one notable case (an outlier in terms of estimated blood loss and warm ischemia time), we did not use NIRF imaging after arterial clamping. Had this been done, it is likely we would have discovered the area around the tumor was not adequately ischemic because of an accessory renal artery.
Patients undergoing NIRF imaging were not compared with similar cases using only white light imaging, which would be necessary to demonstrate better outcomes with this technology. This was primarily a feasibility study designed to evaluate the fluorescence properties of renal tumors and efficacy of this technology. Comparison studies will likely be performed in the near future as use of this technique increases.
Conclusions
NIRF imaging of intravenously injected ICG can be safely used during pure LPN or RALPN. Malignant renal tumors were visualized as hypofluorescent compared with the surrounding normal renal parenchyma. Benign lesions were isofluorescent or hyperfluorescent compared with adjacent kidney tissue. Further study will be necessary to prove better outcomes are possible when this technology is used in selected cases.
Footnotes
Acknowledgments
The authors would like to thank Betty Smith for her assistance with the study preparation and Institutional Review Board approval process.
Disclosure Statement
Partial research funding was provided by Novadaq Technologies, Inc., Missisaugua, Ontario, Canada.