
Abstract
Purpose:
To evaluate the safety and cost-effectiveness of Hem-o-lok and metallic titanium clips for both renal arterial and venous control in laparoscopic nephrectomies.
Patients and Methods:
All patients who underwent laparoscopic nephrectomy from June 2000 to March 2011 in our center were included. Before July 2005, we used three medium-large titanium clips for safe control of renal vessels. After July 2005, we used two clips for renal artery control (one 10 mm Hem-o-lok clip and one medium-large titanium clip) and two clips for renal vein control (12 mm and 10 mm Hem-o-lok clips) in all cases. To prevent possible complications, we placed vascular clips 2 to 3 mm away from the aortic root of the renal artery underneath lumbar vessels. Episodes of clip failure were defined as intraoperative or postoperative hemorrhage or exploration because of clip failure.
Results:
This study included 1834 laparoscopic nephrectomies (1423 donor nephrectomies, 214 simple nephrectomies, and 197 radical nephrectomies). All arteries and renal veins were controlled by titanium and Hem-o-lok clips. One complication that was probably related to vascular clips (titanium and Hem-o-lok), however, involved a delayed hemorrhage from a pseudoaneurysm at the aortic root of the renal artery, which was repaired at exploration. No complication was clearly related to vascular clips. Using Hem-o-lok and titanium clips instead of vascular staplers resulted in $670 savings per operation.
Conclusions:
Hem-o-lok and metallic vascular clips applied properly by trained surgeons according to published safety measures provide a safe and considerable cost-saving option for vascular control in laparoscopic nephrectomy.
Introduction
The publication of two retrospective reports about Hem-o-lok (Weck Closure Systems, Research Triangle Park, NC) clip malfunction caused the manufacturing company to release a contraindication statement for the use of this clip in laparoscopic donor nephrectomy (LDN). 9,10 Nevertheless, other publications reported no serious complications with Hem-o-lok clips or fewer complications and similar mortality in comparison with staplers and metallic clips. 2,11,12 While the standard technique and method of choice for pedicle control during laparoscopic nephrectomy are yet to be established, the purpose of this article is to evaluate the safety and cost-effectiveness of Hem-o-lok and titanium clips (Pilling Titanium Clips, Karl Storz GmbH & Co. KG, Tuttlingen, Germany) in our 11-year experience with these devices for both renal arterial and venous control in laparoscopic nephrectomies.
Patients and Methods
This study entails all laparoscopic nephrectomies in our center from June 2000 through March 2011. Nephrectomies were performed by six experienced surgeons who have been active in advanced laparoscopic surgeries for more than 10 years in the Shahid Labbafinejad Medical Center. These operations included laparoscopic donor, simple, and radical nephrectomies. We used the four- or five-port intraperitoneal approach to explore the abdominal cavity. Our surgical protocol has been published. 6,13 The renal artery and vein were dissected off the surrounding tissues. For LDN in the left side, the renal artery was mobilized to the lateral border of the aorta to obtain a sufficient length for anastomosis, and the renal vein was dissected distal to the gonadal veins. For a right-sided LDN, the renal artery was clipped on the right border of the inferior vena cava (IVC), and the renal vein was dissected at its junction with the IVC with two extra-large Hem-o-lok clips as explained previously. 14
Our policy from June 2000 to July 2005 for safe control of the renal artery and vein has been to apply three medium-large metallic titanium clips as described previously. 15 When Hem-o-lok clips became available in our practice settings, we changed our policy in July 2005 to the use of Hem-o-lok clips as explained in the following discussion. 13 For double ligation of the renal artery, one 10-mm Hem-o-lok clip was applied over the vessel a few millimeters distal to the aorta, avoiding the proximal broad area of the renal artery, and a medium-large titanium clip was applied distal to the Hem-o-lok clip with a manual firing clip applier (Karl Storz). The closing pressure of the titanium clips was controlled by the surgeon's hand to ensure adequate tightness.
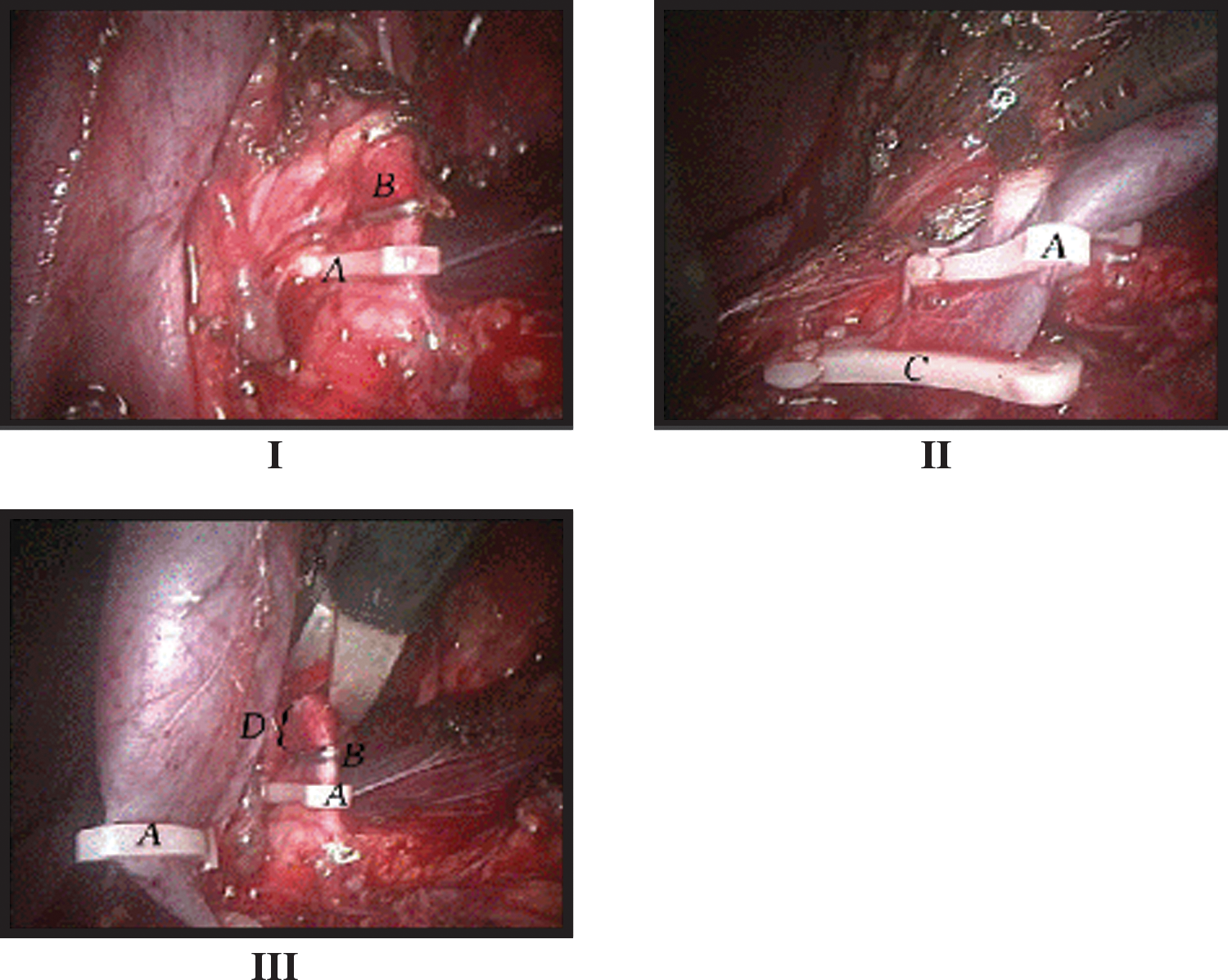
We opted to use two different types of clips and mechanisms in controlling the renal artery, which has a higher pressure than the renal vein. After ensuring safe control of the renal artery, the renal vein was controlled by placing one 12-mm and one 10-mm Hem-o-lok clip (Fig. 1).
After double ligation of the renal artery and vein, the vessels were divided and the whole procedure was completed routinely. We defined clip failure as intraoperative or postoperative hemorrhage because of failure of the clip to prevent hemorrhage after its placement, necessitating open conversion, or as postoperative reexploration because of cardiovascular instability with findings consistent with clip failure.
Results
A total of 1834 laparoscopic nephrectomies were performed in our institution from June 2000 through September 2010. These include 1423 LDNs, 214 simple nephrectomies, and 197 radical nephrectomies. Of these, 1555 operations were on the left side and 279 were on the right side. The considerable preponderance of left operations is because of the high volume of LDNs in this series (78%), which were performed primarily on the left side (92%). In 962 cases, renal vessels were controlled by Hem-o-lok and titanium clips (our current practice as explained above) in 461 cases; renal vessels were controlled by titanium clips. There were no cases of clip dislodgement or slippage during the operations. Patients with renal mass were followed using a long-term standard program, and we did not notice any complications related to using clips. Kidney donors were followed for 3 months after operation.
We encountered one case of arterial bleeding 27 days postoperatively. The patient was a 23-year-old, healthy, left living donor who underwent our recent method of renal vascular control (titanium clips and Hem-o-lok). He presented 10 days after nephrectomy with weakness, dizziness, and low blood pressure and underwent exploration for a possible diagnosis of internal hemorrhage. During operation, an old hematoma was encountered, but no active bleeding was observed. Two weeks later, he presented again with tachycardia and pallor. Abdominal sonography revealed free fluid in the lower abdomen and a 10 cm×8 cm heteroechoic mass in the left renal bed. The patient was immediately explored, and active bleeding was observed proximal to a clipped area from an aneurismal dilation at the aortic root of the renal artery, which was repaired. At discharge, the patient was in a normal condition, and no further events were observed in follow-up.
Discussion
Even though most centers were using vascular staplers when we started laparoscopic nephrectomy, we opted to use clips instead of staplers for the renal artery and vein because clips had several advantages, including simplicity of application, ability to obtain a greater length of donor vessels, and lower cost. Use of staplers was reported to be associated with the risk of device malfunction, especially in the presence of previously applied clips for control of gonadal and lumbar veins, shorter vessel length, which may lead to a donor kidney with multiple arteries, 1,11 and mortality. 2 Most failures from staplers were categorized as missing, malformed, or missing staple line, failure to release from tissue, or firing problems, resulting in open conversion or intraoperative hemorrhage.
The safety of Hem-o-lok clips for laparoscopic nephrectomy was initially attested in several publications. 3 –6,13 Later reports based on surveys of United States (U.S.) transplant surgeons 10 and the U.S. Food and Drug Administration Manufacturer and User Facility Device Experience (MAUDE) database, however, challenged the safety of Hem-o-lok clips by declaring two mortalities and eight cases of reexploration because of late device malfunction. 9,16 The survey of U.S. transplant surgeons reported 12 cases of arterial hemorrhage when Hem-o-lok clips were used. In this study, however, a substantial proportion of surgeons (36%) had no previous formal training in LDN. 9 This survey also was retrospective and subject to recall and response bias, 11 nor did the authors evaluate the relationship of failure with surgeons' experience. 8 The report from the MAUDE database did not differentiate between device failure and user error. 8 On the other hand, similar to the Hem-o-lok mortalities, two previously published cases of mortalities extracted from the MAUDE database were associated with staple malfunction. 2
Despite the aforementioned reports and the resultant contraindication statement for the use of Hem-o-lok clips for LDN, many surgeons still use Hem-o-lok clips as well as titanium clips, which are also contraindicated for LDN by the manufacturer 11 (probably because of legal consequences). Surveys of U.S. transplant surgeons have shown that 56% of them prefer to use a stapler and 28% prefer Hem-o-lok clips for LDN. A recent multi-institutional report including 1695 donor nephrectomies reported no episode of clip failure. 8 Furthermore, new analysis of the U.S. MAUDE database reported a higher rate of complications associated with staplers than with Hem-o-lok clips. 11 The failure rate with staplers was estimated at approximately 3.0%, while this rate for Hem-o-lok clips was 1.7%. 11 In addition, another retrospective comparative trial reported higher safety with the use of Hem-o-lok clips in comparison with staplers. 12
In the current study, we reported 1834 nephrectomies from one center within 11 years. To the best of our knowledge, this is the largest series in which renal arteries and veins were all controlled by Hem-o-lok or titanium clips. As indicated previously, we controlled all renal veins with Hem-o-lok or metallic clips while in other large series, 8 a great proportion of the renal veins was controlled with staples. We think that the application of vascular clips is both safe and cost-effective for renal pedicle control, which is discussed in the following sections.
In this series, only one complication was probably related to vascular clips (titanium and Hem-o-lok). We thought that the formation of a pseudoaneurysm could result from placing a Hem-o-lok clip too close to the aorta, causing minimal abrasion of the arterial wall in the proximal wider root of the renal artery. After this event, as explained in the Methods section, we placed the Hem-o-lok clip a few millimeters away from the renal artery root on the aorta, and we tried not to denude the artery or vein. We did not observe any case of clinical complications because of pseudoaneurysm in the following 938 LDNs.
As indicated, the surgeons of the current series all had previous experience in laparoscopic surgeries. In all LDNs, dissecting renal vessels, applying clips, and dissecting vessels were performed by experienced urologic surgeons (N.S. and A.B.), but in cases of other laparoscopic nephrectomies (radical and simple), urology fellows performed the above procedures under supervision of experienced surgeons. Therefore, by observing the number of radical and simple nephrectomies (N=411), one can conclude that applying Hem-o-lok and titanium clips can be safe even in an educational settings if the following safety measures are adhered to.
We previously reported our method for safe vascular control in LDN,
13
which includes the following hallmarks: Using clips with different mechanisms of action for control of the renal artery (Hem-o-lok and titanium) with higher pressure and using a manual clip applier to close metallic clips; applying two clips for safe control of renal vessels; sparing 2 to 3 mm of the renal artery/vein distal to the clips; and applying Hem-o-lok clips a few millimeters away from the aortic root of the renal artery to avoid a probable risk of pseudoaneurysm
Another great advantage of using vascular clips (Hem-o-lok and titanium) is their great cost-effectiveness in comparison with staplers, which is a major concern in the current economic crisis, especially for developing countries. The lower cost of Hem-o-lok clips has been attested in previous publications. 4,17,18 In this series, application of Hem-o-lok and titanium clips according to our recent method (see Methods) cost $20 per donor while using an Ethicon vascular stapler would have cost $690. This added up to a savings of 1.2 million dollars in our laparoscopic nephrectomy series. Considering an annual laparoscopic nephrectomy rate of about 10,000 in the United States in 2002 19 and an expected doubling of the proportion of laparoscopic operations in the following years, 20 an estimated 20,000 laparoscopic annual nephrectomies are performed in the United States. If the 60% of laparoscopic surgeons who prefer to use staplers change to using vascular Hem-o-lok and titanium clips instead, 11 approximatley 8 million dollars a year would be saved in the United States.
Conclusions
The current series adds evidence to the safety and cost-effectiveness of Hem-o-lok and titanium clips for vascular control in laparoscopic nephrectomy, including donor nephrectomy, when applied by trained surgeons and according to published safety guidelines.
Footnotes
Disclosure Statement
No competing financial interests exist.