
Abstract
Background and Purpose:
Port-site hernias are rare complications that occur in approximately 1% of all laparoscopic surgeries. With the use of bladeless, blunt-tipped entry trocars, some surgeons have argued that not all port sites need fascial closure. Several cases of port-site hernia, however, have been reported recently with the use of bladeless trocars. This study evaluated the incidence of port-site hernias after robot-assisted radical prostatectomy (RARP) as we routinely closed the fascia of only the midline 12-mm port site.
Patients and Methods:
From 2006 to 2009, 498 patients with localized prostate cancer underwent RARP. Bladeless dilating trocars were used in all of our patients. Routinely, six ports were used: two 12 mm, three 8 mm, and one 5 mm. Fascial closure was performed only for the midline supraumbilical 12-mm port site.
Results:
In 498 cases of RARP, there were two port-site hernias (0.4%, 2/498). Both cases occurred at the midline supraumbilical 12-mm camera port site. No hernia developed at nonmidline port sites, including the lateral 12-mm port site.
Conclusion:
Trocar site hernias after RARP are rare. When bladeless dilating trocars are used, routine closure of fascia of non-midline 12-mm or smaller port sites is not necessary. Splitting the muscle and fascia without cutting likely renders routine closure of fascia unnecessary for nonmidline ports that are ≤12 mm.
Introduction
Compared with the cutting trocars, the blunt-tipped entry trocars cause a significantly smaller fascial defect. 5 Accordingly, the routine use of dilating trocars has been advocated by many surgeons to reduce the incidence of port-site hernias. More recently, some surgeons have argued that with the use of these noncutting trocars, all nonmidline port sites ≤12 mm do not need fascial closures. In this study, we report our experience of not closing the fascia after the use of bladeless trocars in robot-assisted radical prostatectomy (RARP).
Patients and Methods
From 2006 to 2009, 498 patients with localized prostate cancer underwent RARP by a single surgeon (IK) at the Cancer Institute of New Jersey. We retrospectively reviewed all cases of RARP after obtaining the approval from the University of Medicine and Dentistry of New Jersey Institutional Review Board. We used bladeless dilating trocars in all of the RARP cases. Routinely, six blunt trocars were placed using the standard technique: Two 12 mm, three 8 mm, and one 5 mm (Fig. 1). All disposable ports were Endopath® Xcel™ bladeless trocars (B5LT and B12 LT, Ethicon Endo-Surgery, Cincinnati, OH).
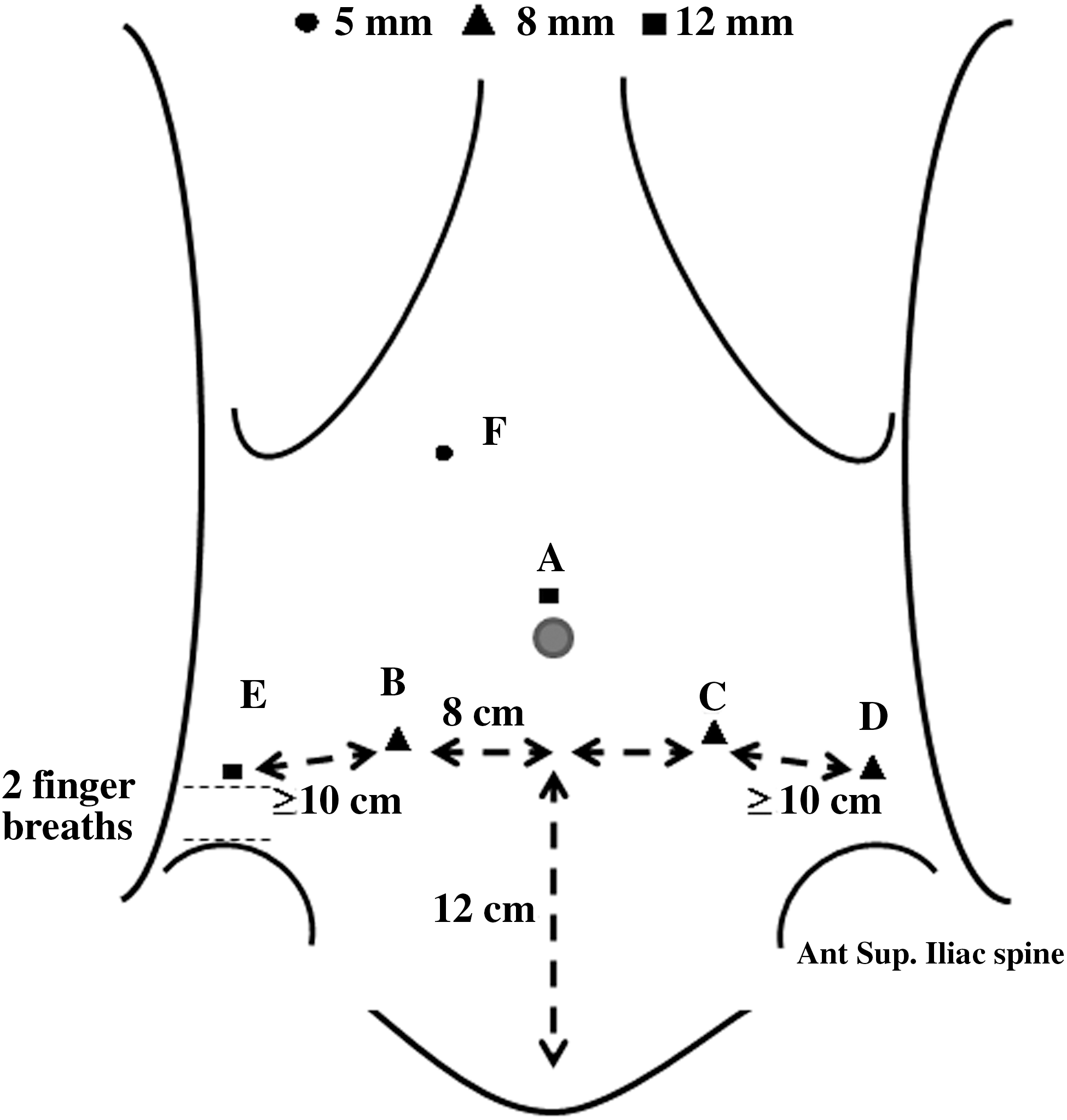
Trocar placement for robot-assisted radical prostatectomy:
Robotic ports were inserted using the nondisposable blunt tip obturators. The 12-mm midline camera port was placed just above the umbilicus; three 8-mm trocars were placed in the left and right lower quadrant just lateral to the rectus muscle; another 12-mm port was placed in the right lower quadrant of the abdomen two finger breadths superior to the anterior superior iliac spine and 10 cm lateral to the 8-mm port; and one 5-mm port was placed in the right upper quadrant. The precise locations of all trocar sites were determined after insufflating the peritoneal cavity to 20 mm Hg.
At the end of the procedure, the specimen was removed by extending the midline supraumbilical incision vertically. Subsequently, fascia was closed only for the midline supraumbilical 12-mm port site using the delayed absorbable polydioxanone suture in a running manner. Needles were placed to close both the fascia and peritoneum simultaneously. Routinely, no drains were placed. In nine patients, drains were inserted through the 12-mm right lateral port site because a bladder neck tailoring was necessary. After RARP, all patients were evaluated for port-site hernias on patient complaints or suspicious physical examination. Subsequently, CT scan confirmed trocar-site hernias before repair.
Results
This study evaluated 498 consecutive patients who underwent RARP between 2006 and 2009. Fascia was closed only for the midline 12-mm port site. The median patient age was 59.0 (range 36–82) years; the median patient body mass index was 27.9 (range 18.4–46.5); the median operating room time was 195 (range 100–540) minutes; and the median follow-up time after RARP was 18 (range 3–48) months. The transperitoneal approach was used in all RARP. Of the 498 cases, two had port-site hernias (0.04%, 2/498). Both occurred at the midline supraumbilical 12-mm camera-port site (Table 1, Fig. 2). No hernia developed at nonmidline port sites, including the lateral 12-mm port site.
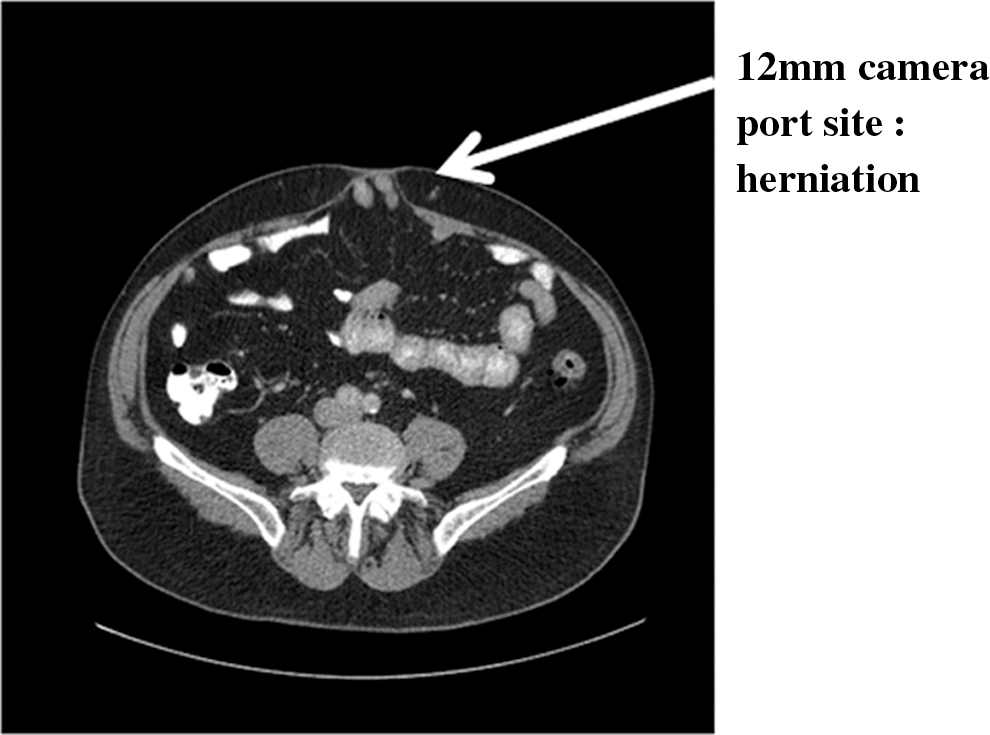
Supraumbilical port-site hernias. All hernias occurred at the midline 12-mm camera ports.
BMI=body mass index.
Discussion
This study evaluated the incidence of incisional hernias after the use of bladeless trocars in RARP as the fascia of all port sites was not routinely closed. Currently, most laparoscopic surgeons use bladeless radially expanding trocars (bladeless trocar). Although there are multiple reasons for the popularity of these bladeless trocars, many surgeons cite less damage to tissues and decreased risk of abdominal organ injuries during laparoscopic surgery. 6
Multiple investigators have examined the clinical outcome of nonfascial closure techniques with bladeless trocars; the results suggest that bladeless trocars do not necessitate routine fascial closure at the end of the surgery, including the 12-mm ports. 7 –11 Rubenstein and associates 8 reported no incisional hernia when the authors did not close the fascia of 12-mm bladeless trocars in 112 locations in the upper and lower abdomen, upper and lower quadrant, midline, pelvis, and umbilicus. In a retrospective study, Siqueira and colleagues 9 reported no hernias involving bladeless 12-mm port sites located at the lateral border of the rectus muscle in 70 transperitoneal live-donor nephrectomies. In addition, a prospective randomized study found no port-site hernia in a nonfascial closure group. 10 Based on this body of evidence, we chose not to close the fascia except for the midline supraumbilical port site. The results revealed no incidence of incisional hernia at the all nonmidline trocar sites—including the 12-mm lateral port site.
Whether to close the fascia when using bladeless trocars remains controversial. Several cases of port-site hernia with bladeless trocars have been reported. 12 –14 Two port-site hernias were reported after donor nephrectomies using bladeless trocars. 13,14 Chiong and coworkers 12 reported seven (0.66%) cases of port-site hernia in urologic surgery. Of 1055 cases using bladeless trocars, port-site hernias involving the 12-mm right lower quadrant port site were identified in 0.9% of RARP cases. When we compared the exact location of the lateral 12-mm port sites to published studies, our location was significantly further lateral.
Many factors lead to the formation of port-site hernias: Mechanical factors (trocar type and size); site of specimen extraction; preoperative risk factors (diabetes, obesity, malnutrition, and smoking); and perioperative factors (trocar direction, wound infection, operative time, use of drain, and port location). Recently, it has been reported that a transverse incision at the midline trocar site decreased the incidence of incisional hernia from 5.3% to 0.6%. 3 Indeed, the increased risk of herniation through the midline incision may be because of the lack of muscular abdominal wall layers. In addition, the site of prostate extraction will likely influence the incidence of incisional hernias because extension of the incisions is usually necessary to remove the prostate. Accordingly, in centers at which extractions occur through the lateral port site, we recommend that the fascia be closed.
Notwithstanding, obese patients are at increased risk of port-site hernias because it is very difficult to find the fascia, and the intra-abdominal pressure is elevated. 15 In our cohort, 81.3% of the patients were overweight or obese, and 30 (6%) patients had a BMI >35. In addition, 21 (4%) patients had diabetes mellitus, abused alcohol, or were heavy smokers. The two cases of incisional hernias occurred in obese patients.
The precise reason for the absence of hernias involving the lateral port sites in our series remains unclear at the present time. One possibility is that drains were not routinely placed. At our institution, drains are placed only when bladder neck tailoring is needed. In the current study, this occurred in only nine patients. As an alternate possibility, we have noticed that the 12-mm port site over the right lower quadrant ultimately ends up below the anterior superior iliac spine. Therefore, the lack of trocar site hernias over the 12-mm lateral port sites in the present study may be because of the caudad movement of the skin, peritoneum, and muscles after inflation and deflation in RARP (Fig. 3).
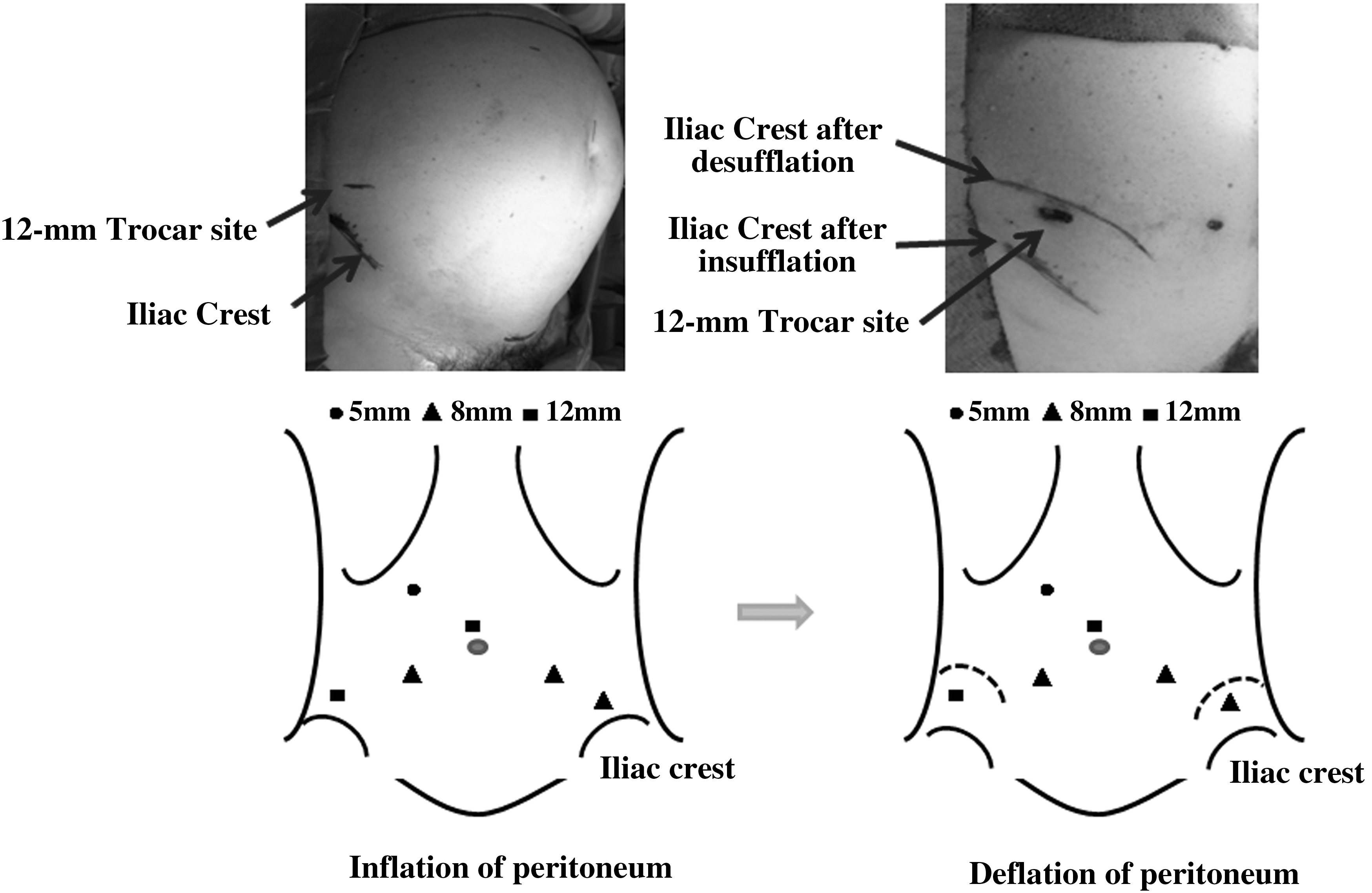
Movement of the skin, abdominal muscles, and peritoneum after inflation and deflation of the abdomen. The dotted line shows the changes after deflation.
Asymptomatic or subclinical hernias could have been missed in this study because we do not routinely obtain follow-up imaging studies. Another criticism of this study is that the analysis was completed retrospectively. Nevertheless, this study is valuable in that the sample size is very large.
Conclusion
Trocar-site hernia after RARP in our series was rare. When bladeless dilating trocars are used, routine fascial closure of nonmidline 12-mm or less port sites is not necessary. Marking the trocar sites after insufflation and splitting the muscle and fascial layers without cutting likely renders routine fascial closure unnecessary in nonmidline ports that are ≤12 mm.
Footnotes
Disclosure Statement
Isaac Kim is a consultant for Baxter Inc. and Amgen Inc. No competing financial interests exist for the other authors.