
Abstract
Background and Purpose:
Laparoscopic radical prostatectomy (LRP) is an established treatment for patients with prostate cancer in selected centers with appropriate expertise. We studied our single-center experience of developing a LRP service and subsequent training of two additional surgeons by the initial surgeon. We assessed the learning curve of the three surgeons with regard to perioperative outcomes and oncologic results.
Patients and Methods:
Three hundred consecutive patients underwent a LRP between January 2005 and April 2011. Patients were divided into three equal groups (1–100 group 1], 101–200 [group 2], and 201–300 [group 3]). Age, American Society of Anesthesiologists score, preoperative comorbidities, and indications for LRP were comparable for all three patient groups. Perioperative and oncologic outcomes were compared across all three groups to assess the impact of the learning curve for LRP. All surgical complications were classified using the Clavien-Dindo system (CDS).
Results:
The mean age was 61.9 years (range 46–74 y). There was a significant reduction in the mean operative time (P<0.05), mean blood loss (P<0.05), mean duration of hospital stay (P<0.05), and duration of catherization (P<0.05) between the three groups as the series progressed. The two most important factors predictive of positive surgical margins at LRP were the initial prostate-specific antigen level and tumor stage at diagnosis. The overall positive margin rate was 27.7%. For pT2 tumors, the positive margin rate was 21%, while patients with pT3 tumors had a positive margin of 44%. For pT2 tumors, positive margin rates decreased with increasing experience (group 1, 27% vs group 2, 17% vs group 3, 19%). The incidence of major complications—ie, grade CDS score ≤III—was 4.6% (14/300).
Conclusion:
LRP is a safe procedure with low morbidity. As surgeons progress through the learning curve, perioperative parameters and oncologic outcomes improve. Using a carefully mentored approach, LRP can be safely introduced as a new procedure without compromising patient outcomes.
Introduction
Although there is no official screening policy for PCa in the United Kingdom (UK), the incidence of PCa has risen dramatically in the prostate-specific antigen (PSA) era. In 2008, there were 37,051 new cases of PCa diagnosed in the UK. 5 As a consequence of earlier detection, there has been considerable stage migration, and the majority of patients now present with clinically localized disease. 6 Many patients with clinically localized PCa now choose RP as their preferred treatment modality. The number of RPs performed in England and Wales has increased 19-fold from 164 in 1991 to 3070 in 2004. 7 In a study reported by Hanchanale and colleagues, 8 the number of RPs performed in England increased annually from 972 (1998 to 1999) to 3092 (2004 to 2005). During the same period, the number of LRPs increased from 2 to 257.
It is accepted that greater surgical experience is associated with improved functional and oncologic outcomes after RP. 8,9 With LRP, however, improvements in outcome seem to accrue more slowly than for open surgery. 9 The concept of a learning curve in LRP is well recognized (although less easy to define accurately). Normally, as the surgeon progresses through his or her learning curve, measurable outcomes such as operative time, conversion rates, blood loss, functional results, and surgical margin rates improve. It has been suggested that the learning curve for LRP plateaus at about 50 cases 10 ; however, Eden and coworkers 11 have described multiple learning curves with as many as 700 cases needed to reach a plateau for potency.
Introducing a technically difficult procedure such as LRP to a department where it has never been previously performed brings significant challenges. The most important issue is to protect patients from poor outcomes while the surgeon and his team progress through the learning curve and familiarize themselves with the technique. The British Association of Urological Surgeons (BAUS) has published guidelines on training and mentorship in LRP. 12 Further complexities arise when, having completed training in LRP, the lead surgeon facilitates service development within a department for training additional surgeons. The former lead surgeon becomes the mentor and trainer to another surgeon learning LRP. Here the unique challenge is to maintain safety and improve results and outcomes while mentoring a colleague through a new learning curve.
We present the results of the first 300 cases of transperitoneal LRP performed in our department by a team of three surgeons, focussing on perioperative outcomes, complications, and oncologic results.
Patients and Methods
Between January 2005 and April 2011, a total of 300 consecutive transperitoneal LRPs were performed in our unit by three surgeons. All patients had biopsy-proven adenocarcinoma of the prostate. Clinical data, prostate biopsies, and staging investigations (if indicated) were reviewed at the uro-oncology multidisciplinary team meeting.
All patients in group 1 were admitted the evening before surgery and received deep vein thrombosis prophylaxis with low molecular weight heparin and sequential elasticated compression stockings. Patients in groups 2 and 3 were admitted on the day of LRP. A phosphate enema was administered to empty the rectum. Prophylactic broad-spectrum antibiotics were administered at induction of anesthesia.
Intravenous induction of anesthesia was performed and maintained with an inhalational agent and an intravenous infusion of remifentanil. A nasogastric tube is not routinely inserted, but ranitidine may be prescribed as a premedication if there is a history of gastroesophageal reflux. A clear view of the face and vigilance in positioning are important preventive measures. The patient was transferred onto a nonslip gel mat on the operating table. Before this, a sheet was folded around a head pillow and then secured under the gel mat to stop the pillow from moving. A second gel mat was placed transversely across the table at midarm level. This was used to wrap over the patient's arms and under the torso to secure the arms during surgery. This configuration prevents the patient from slipping when in the steep Trendelenburg position and spreads the pressure across all contact points, rather than being focused at the shoulders. It is important to ensure that all intravenous cannulas are well padded to protect the skin, connections are secure, and fluid is running freely, because access is limited during surgery.
A five-port open (Hasson) access transperitoneal antegrade laparoscopic approach as described by Drs. Gaston and Piechaud 13 was used with the patient placed in a Trendelenburg tilt of 30 degrees. For patients with a PSA level ≥10 ng/mL and/or a primary Gleason score of ≥4, bilateral pelvic lymphadenopathy to the level of the bifurcation of the common iliac vessels was performed. A voice-controlled robotic arm (AESOP®) was used to control the camera. The primary surgeon stood to the left of the patient with a single assistant on the right. The Harmonic scalpel (ACE®) was used for the anterior dissection including the bladder neck. The posterior dissection was performed athermically with cold scissors and titanium clips to protect the rectum and neurovascular bundles from thermal injury. The Santorini plexus was ligated with 2-0 polyglactin before division. Sharp dissection with scissors was used at the apex. The urethrovesical anastomosis was performed using 3-0 poliglecaprone on a Visi-Black® needle in a continuous fashion over a 20F silicone catheter. Occasionally, if there was discrepancy in the size of the bladder neck, an anterior “tennis racquet” reconstruction was performed. The integrity of the anastomosis was tested by instilling 150 to 200 mL of physiologic saline into the bladder. A 15F Jackson-Pratt pelvic drain was inserted and placed on free drainage. The supraumbilical port was used to deliver the specimen. The 12-mm port sites were closed in layers.
The drain was removed when the output was <100 mL in 24 hours (usually postoperative day 1–2). The urethral catheter was removed after 3 weeks after cystography for the first 50 cases. For the subsequent 200 cases, the catheter was removed at day 10 without cystography. For the last 50 cases, the catheter was removed at day 7. After catheter removal, all patients were seen by the continence advisor and instructed in pelvic floor exercise technique. Patients who were potent preoperatively and who had undergone a nerve-sparing procedure were prescribed a phosphodiesterase (PDE) 5 inhibitor (sildenafil or taldafil) to facilitate rehabilitation of erectile function.
Perioperative data collected included length of operative time, weight of prostate specimen, estimated blood loss, transfusion rate, postoperative length of hospital stay, duration of catheterization, and positive surgical margin rates. All complications that occurred within the first 100 days of surgery were recorded, defined, and graded using the Clavien-Dindo system (CDS). 14 Patients were reviewed in clinic 6 weeks after surgery, every 3 months thereafter for the first year, and at 6-month intervals until year 5 with PSA measurements. Continence was defined as being pad free. Potency was defined as an erection sufficient for vaginal penetration with or without the assistance of a PDE5 inhibitor.
Before commencing LRP in our department, surgeon 1 (a proficient upper tract laparoscopic surgeon regularly performing laparoscopic nephrectomy, adrenalectomy, nephroureterectomy, pyeloplasty, and live-donor nephrectomy) visited a number of centers of excellence as an observer including the Cleveland Clinic, Institut Montsouris, Paris, and Clinique St. Augustine, Bordeaux. Subsequently, master classes and live demonstration cases were performed at our institution by international experts (Prof. Clément-Claude Abbou (France), Prof. Thierry Piéchaud (France), and Prof. Inderbir Singh Gill (United States). These experts jointly performed cases and provided mentorship.
The majority of our first 100 cases (group 1) were performed by surgeon 1 (Mr. N. Soomro) was assisted by surgeon 2 (Mr. G. Durkan). For the second 100 cases (group 2), surgeon 1 trained surgeon 2 in a modular fashion until surgeon 2 was competent in all steps of LRP. For the next 100 cases (group 3), surgeon 2 worked semi-independently of surgeon 1, who was available to provide assistance in particularly difficult cases. Both surgeons 1 and 2 mentored surgeon 3 (Mr. M. I. Johnson) during the last 50 cases in group 3. As per BAUS guidelines, before commencing LRP, surgeons 2 and 3 completed “dry” and “wet” laboratories, attended live demonstration master classes, attended a high-volume center of excellence as an observer (Clinique St. Augustine, Bordeaux), and had gained experience of upper tract laparoscopy.
Statistical analyses were performed using SPSS/PASWSTATISTICS Version 18.0, Chicago, IL. Demographic data are presented as mean±standard error. The Mann-Whitney test was used for quantitative variables, and the chi-square test was used for categorical variables. A P value of <0.05 was considered statistically significant.
Results
Preoperative parameters
All 300 patients were divided into three equal groups: Group 1 (cases 1–100), group 2 (cases 101–200), and group 3 (cases 201–300). The mean age at the time of surgery was 61.9 years (range 46–74 y), and the mean presenting PSA value at the time of diagnosis was 8.5 ng/mL (range 0.9–34 ng/mL). The preoperative parameters are summarized in Table 1.
PSA=prostate-specific antigen; ASA=American Society of Anesthesiologists; NS=non-significant; S=significant.
Operative parameters
The mean operative time for the whole cohort was 212 minutes (range 90–360 min). The mean operative time for group 1 was 231±55.6 minutes, group 2 was 204±49.2 minutes, and group 3 was 181±47.3 minutes (P<0.05). A scatter plot demonstrating the improvement in operative time through the series is shown in Figure 1. The mean intraoperative blood loss also reduced through the series; the initial mean blood loss in group 1 was 728±427.5 mL, group 2 was 536±384.6 mL, and group 3 was 511±353.7 mL (P<0.05).
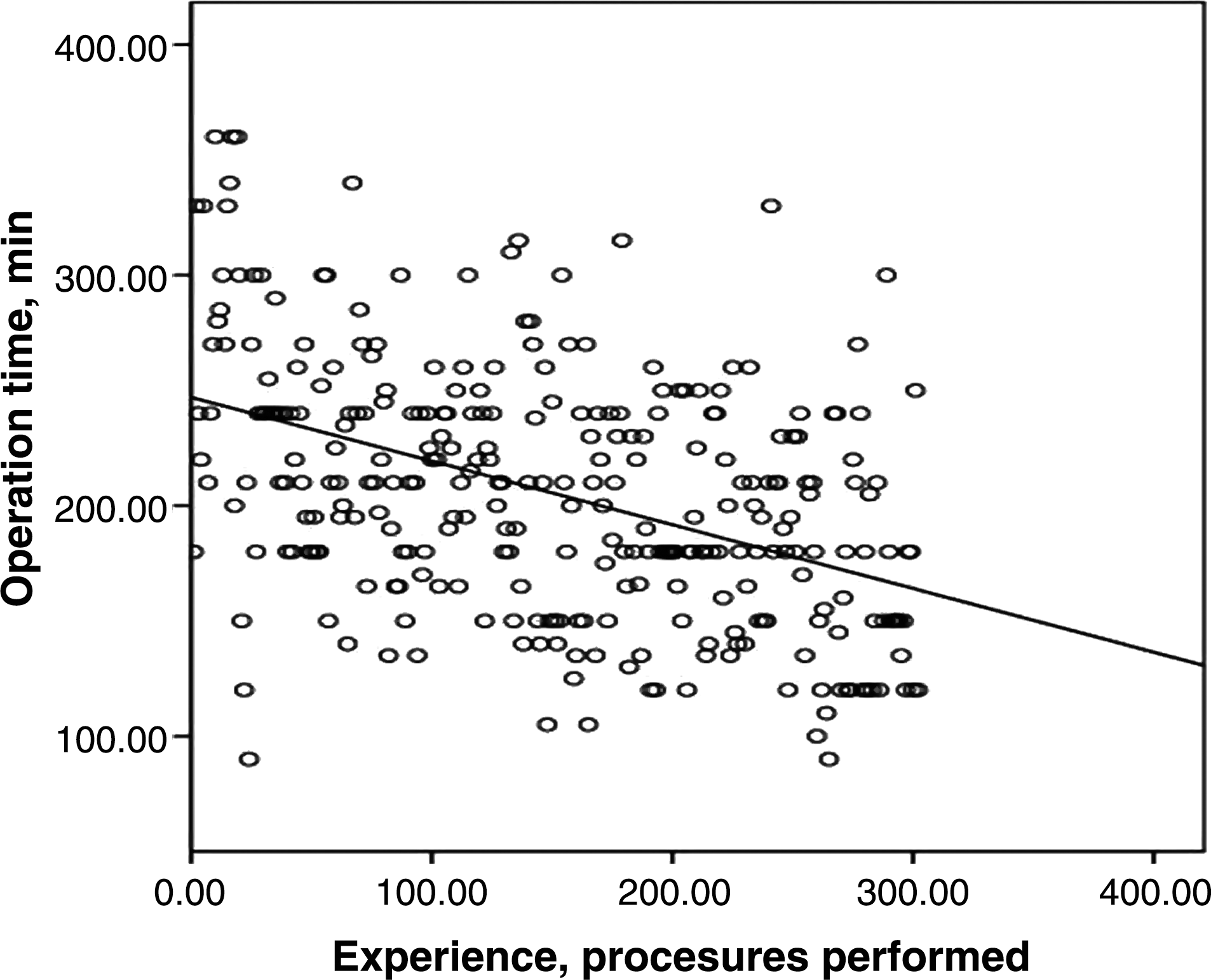
Scatter plot demonstrating the link between mean operative time and each group.
The incidence of intraoperative blood transfusion was 4.3% (13/300). The incidence of conversion to open surgery for the entire cohort was 1% (3/300). The reason for conversion was intraoperative hemorrhage (2) and difficulty with the urethrovesical anastomosis (1). One patient in group 2 had a rectal injury that was identified on table and repaired laparoscopically without conversion. The intraoperative parameters are summarized in Table 2.
Postoperative parameters
The mean length of hospital stay for the entire cohort was 4 days (range 2-21). Patients in group 3 had a significantly shorter hospital stay than patients in group 1 (5.2±3.3 days vs 3.2±1.2 days, P<0.05). The mean duration of catheterization improved from 19.5±15 days in group 1, 11.4±5.1 days in group 2 to 9.9±5.2 days in group 3 (P<0.05). The postoperative parameters are summarized in Table 3.
Postoperative complications
All complications that occurred within the first 100 days of surgery were recorded, defined, and graded using the CDS (Table 4). 14 The complications were classified from grade I to V. Grade I, need oral medication/bedside care; grade II, required intravenous therapy, enteral feeding, or transfusion; grade III, required intubation, interventional radiology, or reoperative intervention; grade IV, required organ resection or resulted in chronic disability; and grade V, death.
ITU=intensive therapy unit; TPN=total parenteral nutrition; ATN=acute tubular necrosis.
The overall incidence of postoperative complications was 17.3% (52/300). The incidence of minor complications (grade I–II) was 12.6% (38/300). The incidence of major complications (grade III–V) was 4.6% (14/300). The complication rates for each group are summarized in Table 4.
Six (2%) patients underwent reoperation. These included four emergency laparotomies for postoperative hemorrhage and two cases in which a large urinoma from an anastomotic leakage necessitated open drainage. The incidence of unplanned admission to intensive care was 1% (3/300). These incidences were for an acute postoperative myocardial infarction (1), pneumonia (1), and acute renal failure necessitating hemodialysis (1). The patient who needed hemodialysis had a single kidney with a background of chronic renal impairment. The rates of anastomotic leakage significantly improved after the first 50 cases performed.
Final histology and positive surgical margin status
The histology results for all cases were reported using the 2002 Tumor-Node-Metastasis classification. The incidence of pT2 tumors was 71.6% (215/300), pT3 tumors 26.6% (80/300), and pT4 tumors 1.6% (5/300). Positive surgical margin (PSM) rates improved across the three groups with progression through the series. The incidence of PSM in group 1 was 32%, group 2 was 27%, and group 3 was 23% (P=0.36). The final histology results and positive margin rates are summarized in Table 5.
PSM=positive surgical margin.
Advanced tumor stage (pT3/4) and PSA levels >10 ng/mL at diagnosis are associated with significantly higher rates of PSM (P<0.01, 0.044, respectively). The overall PSM rate for our series was 27.3% (82/300). On comparing the three consecutive groups, the PSM rates were 32% (group 1), 23% (group 2), and 27% (group 3), respectively. There were a far higher number of pT3 tumors in group 3 than in groups 1 and 2, however. Using the D'Amico classification, 15,16 we stratified the cases into low, intermediate, and high risk. PSM rates increased across risk groups but fell with progression through the learning curve (Table 6). This was despite a significant increase in the incidence of high-risk tumors in group 3 compared with groups 1 and 2.
PSA=prostate-specific antigen; PSM=positive surgical margin.
The most common location of PSMs in our series was at the apex (65%). As per the TNM classification T4 tumors were those where the bladder neck was involved. Our PSM rates in group 3 are acceptable when compared with LPR. 17 We continue to strive to have a 0% rate of PSM in all patients as does every urologist performing an RP.
Continence and potency
At a mean follow-up of 23.47 months (range 0.4–88 mos), 78.3% (235/300) of patients were completely dry (pad-free); 11.6% (35/300) of patients wore between 1 to 2 pads/d and 7.3% (22/300) wore 3 to 4 pads/d. Three percent (8/300) of patients had an artificial urinary sphincter placed during the course of the series. Among these eight patients, three were from group 1, four from group 2, and one from group 3 (P=NS).
Erections satisfactory for vaginal penetration and intercourse were present in 152 (51%) patients. Of these, 52 had spontaneous erections and 100 could achieve erection with a PDE5 inhibitor. A further 32 patients used intracavernosal alprostadil injections to achieve erection and 1 patient used a vacuum pump device. Five (1.6%) patients opted to have a penile prosthesis inserted. The remaining 110 patients have erectile dysfunction but do not find this distressing and have not pursued further treatment.
This information was on the basis of the Male Lower Urinary Tract Symptoms, Sexual Health Inventory for Men, and Evaluation of Health-Related Quality of Life.
Discussion
Driven partly by innovation and partly by patient demand, surgeons continue to seek less invasive ways to perform RP. Improved technology and instrumentation have facilitated progress in LRP and made it more reproducible. LRP, however, remains a challenging procedure for the novice pelvic laparoscopist and has a steep learning curve. The theoretical concept of a learning curve—ie, the experience a surgeon needs to amass before reaching a plateau with regard to oncologic and functional outcomes—has been described in the recent literature with regard to LRP. 18,19 Most contemporary publications of LRP are single surgeon series. Our series, however, reports the relatively early outcomes for three surgeons working in mentorship together to develop LRP in a single institution.
In a recent comparison of surgeon background experience, Frede and associates 19 were able to show that experience in open prostatectomy was not essential to perform LRP; indeed for the surgeons with previous laparoscopic experience, the “learning curve” was shorter, but then this may have been influenced by mentorship from already established pelvic laparoscopists. Vickers and colleagues, 9 elaborated on this point further by commenting that one of the reasons for a shorter learning curve for surgeons with no or limited open RP background is that they do not compare the anatomy or technical steps of open RP while performing LRP. Eden and coworkers 11 describe the concept of a number of different learning curves for PSM rates, continence, and potency. If there is more than one surgeon in a department performing the same procedure and if there is a high throughput of cases, it should be possible to safely train more surgeons with resultant shorter leaning curves. The learning curve in this sense pertains mostly to perioperative parameters such as operative time, blood loss, and positive margins, in addition to complications in the first instance and oncologic outcomes subsequently.
It is now advocated that about 60 LRP cases are needed to facilitate independent operating with acceptable outcomes for surgeons with previous laparoscopic experience. 20 –23 Further improvements in operative, oncologic, and functional outcomes can be seen up to about 300 cases. 21 –23 All cases present their own unique challenges. Diversity among surgeons in terms of experience and skill further clouds the number of cases needed to perform LRP independently and safely with acceptable oncologic and functional outcomes–the learning curve. At best, these learning curve numbers constitute a general guideline rather than rigid dogma.
In our series, the first surgeon was an experienced upper tract laparoscopist. After mentoring from expert pelvic laparoscopic surgeons, he performed the procedure independently, assisted by surgeon 2. After 50 cases, he began training surgeon 2 who was an experienced open radical prostatectomist and had some upper tract laparoscopy experience. The data from group 2 indicate that the overall results continued to improve despite the training of a second surgeon. In group 3, a third surgeon began training when the combined experience of surgeons 1 and 2 exceeded 200 LRP cases. Our experience shows the feasibility of training new surgeons in LRP at a relatively early stage without compromising oncologic outcomes or complication rates. Careful support and mentorship allowed dissemination of this complex technique within our department while operative times, blood loss, and complication rates all fell.
We continue to strive to provide training for specialist registrar and consultants in our center to enhance dry laboratory laparoscopic skills in uro-oncology. Our center has a laparoscopic cadaveric laboratory, the first and only one of its kind in the UK (Newcastle Surgical Training Center,
Longer follow-up is needed to evaluate the oncologic efficacy and recurrence rates after LRP. It is probable that PSA failure and disease recurrence after LRP reduces with improved surgical experience. 7 As our experience with LRP increased, we were able to offer the technique to more patients with high-risk PCa while reducing PSM rates. Functional outcomes were evaluated subjectively during follow-up in the outpatient clinic rather than objectively with validated questionnaires. Pad-free rates were 78.3% (235/300) while a further 35 (11.6%) men wore only 1 to 2 pads/d. Only 1.6% needed an artificial sphincter. Satisfactory potency was reported in 51% (152/300). Unfortunately, the number of men with preexisting erectile dysfunction before LRP was not recorded, so our potency rates are probably slightly higher. It is encouraging that our functional outcomes are close to those reported by other major centers. 13
Close cooperation with our anesthesia colleagues was vital in developing a safe LRP service. LRP is a relatively long procedure necessitating steep Trendelenburg positioning (>30 degrees) and CO2 pneumoperitoneum that can impact adversely on normal physiology. Careful patient selection and attention to detail are key to achieving a good outcome. Venous congestion in the head can give erroneous readings if the pulse oximeter is placed on the pinna. 24 The increase in dead space can lead to an increase in arterial-alveolar gradient for CO2. The study by Kalmar and colleagues 25 found that the end-tidal CO2 (ETCO2) measurement can be approximately 1.41 KPa lower than arterial pCO2 after 2 hours in the Trendelenburg position. Tidal volumes and respiratory rate need to be increased to prevent hypercarbia and respiratory acidosis. Intracranial pressure (ICP), cerebral blood flow, and intraocular pressure (IOP) increase in the Trendelenburg position. A rise in PaCO2 further increases ICP and IOP. 26 Surgical duration and ETCO2 are significant predictors of increased IOP in the Trendelenburg position. Maintaining PaCO2 within normal limits is important to prevent potentially devastating rises in ICP and IOP. 27 The use of dexamethasone 8 mg as part of our postoperative nausea and vomiting protocol may have some benefit, although there is no evidence to support this.
We do not routinely monitor central venous pressure, but use an esophageal Doppler to guide fluid and vasopressor administration to maintain cardiac output and blood pressure. Fluid restriction decreases urine production to facilitate a dry operative field. It may also reduce the amount of facial and cerebral edema. It is difficult to accurately monitor urine output and blood loss in these patients, because suction from the abdomen will contain a variable mixture of blood, urine, and wash. Not all fluid will be evacuated into the suction bowls. Regular Haemoglobinometer measurements are useful if excessive blood loss is suspected. 28 Renal perfusion decreases because of a combination of raised intra-abdominal pressure (IAP) and activation of the renin, aldosterone, and angiotensin systems. This is associated with a decrease in urine production and a concomitant deterioration in renal function. Minimizing IAP, duration of surgery, and ensuring adequate cardiac output help preserve renal function. 29 Particular care is needed in patients with a solitary kidney and/or chronic kidney disease to maintain adequate renal perfusion and avoid acute tubular necrosis. Despite these profound physiologic derangements, hemodynamic and pulmonary variables can be kept within safe limits, and LRP is well tolerated by patients. 25
As the series progressed, patients with intermediate-risk cancer—ie, Gleason 7, PSA <20, and T2c+suspicious T3a on preoperative MRI scan—were included in the series. In the department, currently all patients are initially offered a nerve-sparing LRP. The only reason why patients are offered an open RP include T3b disease (seminal vesicle) involvement, high-risk prostate volume (ie, Gleason 8/9), salvage prostatectomy after previous radical radiotherapy, body mass index >35, or patient choice to pursue an open RP.
Conclusion
LRP is a challenging procedure with a significant learning curve. Parameters such as operative time, blood loss, transfusion rates, length of stay, and positive margin rates improve with increasing experience. With appropriate support, training and mentorship LRP can be taught to other surgeons while continuing to improve outcomes for patients.
Footnotes
Disclosure Statement
No competing financial interests exist.