
Abstract
Background and Purpose:
Protease inhibitors, specifically indinavir, have historically been implicated as a cause of nephrolithiasis in the human immunodeficiency virus
Patients and Methods:
We retrospectively reviewed HIV-positive patients currently receiving HAART treatment in whom image proven kidney and/or ureteral urolithiasis developed, between 1998 and 2010. A detailed analysis of patients' current treatment, surgical intervention, and metabolic studies was performed.
Results:
A total of 436 HIV-positive patients were included and 46 (11%) patients had nephrolithiasis. Each patient included in this study was receiving nonindinavir-based antiretroviral therapy. There were 41 men of whom 36 were Caucasian. Eleven (24%) patients underwent 24-hour urine collections with 11 metabolic abnormalities identified. Stone analysis was available for seven patients (four calcium oxalate monohydrate, one cystine, one uric acid, and one atazanavir).
Conclusions:
We report the largest series of nephrolithiasis in an HIV population since the introduction of HAART and highlight not only the similar prevalence of nephrolithiasis to the non-HIV population but also the lack of consistent comprehensive metabolic evaluations in HIV patients with recurrent nephrolithiasis.
Introduction
We therefore sought to identify the prevalence of nephrolithiasis in the HIV-infected patient population on nonindinivar therapy (HAART) at our institution and describe the different aspects of nephrolithiasis in this contemporary cohort, such as medical and surgical treatment, stone analysis, and underlying metabolic urinary abnormalities.
Patients and Methods
Between January 1998 and January 2010, HIV-positive patients >18 years old receiving nonindinivar HAART-based treatment were identified through a retrospective review of our institution's electronic health record at the University of California San Diego Health System with Institutional Review Board approval. A list of all HAART and their respective kidney stones that were evaluated in our database is demonstrated in Table 1. We intentionally excluded any patient with a history of nephrolithiasis to determine prevalence of kidney stone disease after administration of HAART. All patients with image-documented calculi in the kidneys and/or ureters were included for analysis.
Genitourinary history, distinct renal colic episodes, including medical and/or surgical treatment, and antiretroviral therapy were retrieved. Serum electrolytes, urinalysis with microscopy, urine culture, stone analysis, and 24-hour urine collections were documented. The primary insurance carrier was used for purposes of analysis, because the company (Dianon Systems, Shelton, CT) that processes our 24-hour urine collections only bills the primary insurance carrier. Descriptive statistics and analysis of variance were used with statistical significance set at P<0.05.
Results
A total of 436 HIV-positive patients were identified and 46 (11%, 95% confidence interval 9–15%) of these demonstrated image-proven kidney and/or ureteral urolithiasis. Mean age was 54 years (range 34–78 y), and mean body mass index was 27 (range 22–35). Patient demographics are shown in Table 2. None of the patients were instructed to stop HAART after diagnosis of nephrolithiasis. In the vast majority of cases, CT urography was the imaging modality (n=39, 85%), whereas ultrasonography alone (n=5, 11%) and plain kidneys-ureters-bladder radiography alone (n=2, 4%) were less commonly used. Mean time of patients with a HIV diagnosis was 24 months (range 12–36 mos), and mean time to nephrolithiasis diagnosis while receiving HAART was 13.5 months (range 9–18 mos) (P<0.05).
Only the primary insurance is listed and used for the purposes of this study.
The characteristics of the stones, including their treatment, are listed in Table 3. Mean stone size was 8 mm (range 2–24 mm±2.8 standard deviation). Seven subjects had multiple kidney calculi (≥2), and only one had bilateral kidney calculi. Ureteral obstruction secondary to obstructive ureteral calculi developed in 30 patients. A total of 23 patients had kidney calculi, 28 had ureteral calculi, and 42/46 were symptomatic—among these, 10 patients underwent shockwave lithotripsy (SWL), 13 underwent ureteroscopy/lithotripsy, and 23 were treated with medical expulsive therapy with spontaneous passage of stones. Two patients needed repeated surgery, including one SWL and one ureteroscopy/lithotripsy. Despite the immunocompromised status of these HIV-positive patients, there were limited complications as a result of treatment for nephrolithiasis. These complications included urinary tract infection (3) and cystitis (2) that was treated with outpatient oral antibiotics. The third patient had sepsis after ureteroscopy/lithotripsy despite a preoperative negative urine culture. He recovered without sequelae.
SD=standard deviation; CT=computed tomography; KUB=kidneys, ureters, and bladder.
Only eleven (24%) patients underwent 24-hour urine collections. Among these 11 patients, 10 had urinary abnormalities detected in their 24-hour urine collection including hypocitraturia, hypercalciuria, hyperuricosuria, hyperphosphaturia, or hypernatriuria (Fig. 1). Hypercalciuria (35%) and hypocitraturia (29%) were the two most common urinary abnormalities identified, followed by hypernatriuria (18%), hyperuricosuria (12%), and hyperphosphaturia (6%). The mean urinary pH among this group of patients was 6.2. These patients had varied insurance coverage: five had Medicare, three had private, two had Medi-Cal, and one was uninsured. The insurance coverage among the 35 patients who did not undergo 24-hour urine collections also varied: 16 had Medicare, 12 had Medi-Cal, 6 had private, and 2 had Ryan White. Twenty-four patients had a history of recurrent nephrolithiasis, but only four of these patients underwent a comprehensive metabolic evaluation.
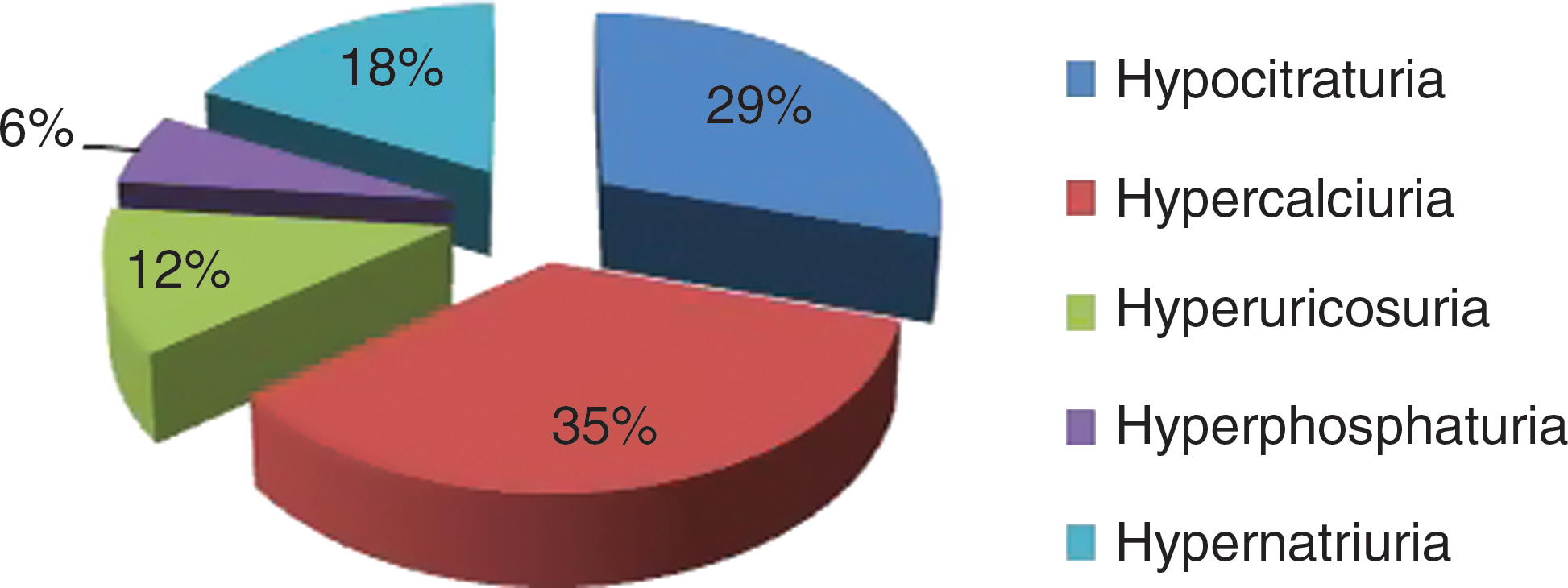
Details of the etiology of nephrolithiasis among patients who underwent 24-hour urine collection.
Seven (14%) patients underwent chemical analysis of the urinary calculi: Four had calcium oxalate monohydrate, one had cystine, one had uric acid, and one had an atazanavir metabolite stone. In addition, six patients had a family history of urolithiasis.
Discussion
We believe this is the first article to report both the prevalence and etiology of nephrolithiasis in an HIV-positive cohort of patients taking no indinavir in the HAART era. Despite the recent shift toward less lithogenic HIV therapy, the 11% prevalence of nephrolithiasis in our cohort still exceeded that of the non-HIV population (5.2%). 2,3 Similar to previous reports, our study confirms that HIV patients share an equal risk of nephrolithiasis that is not necessarily related to indinavir-based therapy. 4 The medications in this study included PIs, but only one stone analysis demonstrated evidence of a PI-contained calculi. These findings are of critical importance, because it demonstrates that HIV-infected patients are at an equal risk for nephrolithiasis, which ultimately significantly contributes to the annual United States healthcare expenditures. 5
Medical management is the foundation of kidney and/or ureteral calculi prevention, with algorithms dependent on both serum studies and 24-hour urine studies as the cornerstone of a comprehensive metabolic evaluation. Unfortunately, both previous reports and our current study document low utilization of the 24-hour urine study in the evaluation of nephrolithiasis. Recurrence rates in non-HIV patients are 50% over 5 to 10 years, while medical management can identify specific urinary abnormalities in approximately 97% of analyses, potentially reducing recurrence rates. 6
More than half of our patients had recurrent nephrolithiasis and may well have benefited from medical intervention as a preventative measure. Furthermore, more than half of our cohort needed surgical intervention with its attendant risks and financial burden to an already diseased population. These findings add credence to performance of a comprehensive metabolic evaluation as a means of reducing risk of recurrent nephrolithiasis. Generally, the evaluation for nephrolithiasis in the HIV patient should be no different from that of the non-HIV patient. Stone analysis, however, is particularly useful, because it discriminates metabolic stone from drug-induced stone and subsequently reinforces the utility of a metabolic evaluation when a metabolic component exists in the stone analysis. A metabolic evaluation should also be considered, especially if a stone analysis is not available or if there is a history of recurrent metabolic stone disease.
We suspect that poor utilization of 24-hour urine studies is most likely because of one of four possibilities: (1) provider decision to recommend nonoperative therapy (increase fluid intake, decrease salt and protein) in low-risk nephrolithiasis formers or first-time nephrolithiasis formers; (2) provider disbelief in the utility of the comprehensive metabolic testing and evaluation; (3) poor patient compliance in undergoing this testing; or (4) insurance obstacles. Regarding the latter, we discovered a proportion (6%) of HIV patients were not eligible for 24-hour urine studies because of their specific federal insurance, the Ryan White program, which only reimburses this specific test on a case by case basis. Our data, however, do not support the supposition that insurance is an obstacle to metabolic evaluation.
The prevalence of nephrolithiasis is estimated to be 3% to 22% for HIV-positive patients receiving indinavir. 2,4,7 –10 Indinavir is a PI of which approximately 20% is not metabolized and is excreted by the kidneys. Indinavir is most soluble at pH<5, and therefore it tends to precipitate in alkaline urine. Hence, indinavir calculi typically tend to be radiolucent but may act as a nidus for the formation of kidney and/or ureteral calculi containing calcium oxalate and phosphate, which are radiopaque. 2,11 –13
The newer antiretroviral therapies in the form of HAART have made a significant impact on the morbidity and mortality of patients with HIV infection. Antiretroviral drug resistance can develop rapidly through mutations; therefore, a combination of at least three drugs from at least two different classes is now used, coined HAART. Two NRTIs are usually combined with either NNRTIs or a PI. The primary aim of HAART is to suppress a viral load below detectable levels, and thereby increase the CD4 cell count and decrease morbidity and mortality. 9,10 Reports of kidney calculi made of a degraded PI other than indinavir exist with atazanavir, however. 14 –18 In addition, nephrolithiasis case reports associated with nonindinavir-based HAART exist (Table 4).
NRTIs=nucleoside reverse transcriptase inhibitors; PIs=protease inhibitors.
Notwithstanding the risk of PI composed stones, we report a risk of nephrolithiasis in HIV patients that mimics the non-HIV population. We acknowledge the limitations/bias of this retrospective study, which limits data collection, such as missing data. In addition, we acknowledge that certain medications such as thiazide diuretics may affect kidney stone formation, and therefore our analysis may underestimate the true prevalence, because we did not collect this information. The patient sample was derived from an academic referral center, and therefore our conclusions are not as generalizable as a population-based study would offer.
Conclusions
We report the largest series of nephrolithiasis in an HIV population since the introduction of HAART and highlight the lack of consistent comprehensive metabolic evaluations in HIV patients. This study suggests that the contemporary population receiving HAART appears to have a significant risk of nephrolithiasis and that comprehensive metabolic evaluation should be considered, especially where there is evidence of a metabolic component to kidney stone formation.
Footnotes
Disclosure Statement
No competing financial interests exist.