
Abstract
Background and Purpose:
Iatrogenic sphincter lesions are possible reasons for sphincteric incompetence and postprostatectomy urinary incontinence. The aim of this study was to identify early possible sphincter injuries as causes for urinary incontinence after radical prostatectomy by endoscopic evaluation of the anastomotic region.
Patients and Methods:
Among 374 patients who had undergone radical prostatectomy from 2005 to 2009 at our institution, we investigated patients with early postoperative urinary incontinence. Nineteen incontinent patients were identified with the symptomatic triad of early incontinence, reduced urinary flow, and post-void residual (PVR) volume after catheter removal. Patients were examined endoscopically, and the clinical effect of early suture removal in patients with sphincter penetration was evaluated.
Results:
Urethrocystoscopic evaluation revealed an isolated sphincter penetration as reason for early postoperative incontinence in 15/19 cases. The suture penetration was observed predominantly in the 3-degree (7/19) and 9-degree (8/19) positions and less frequently in the 12-degree (2/19) and 6-degree (2/19) positions. Four of (21%) 19 patients did show an additional sphincter transection. The penetrating sutures of the urethrovesical anastomosis were removed during the endoscopic procedure, and initial urinary incontinence could be corrected in all cases of isolated sphincter penetration.
Conclusion:
Early severe urinary incontinence, reduced urinary flow, and PVR volume after radical prostatectomy may indicate sphincter penetration by anastomosis sutures. In our patients, early transurethral punctual removal of the penetrating sutures could decrease the early postoperative incontinence rate.
Introduction
In accordance with this recommendation, damage to the nerve as well as direct muscle damages to the urethral sphincter may be a potential reason for postprostatectomy urinary incontinence. 5,6 They are rarely reported in current literature, however. In a recent study, 169 patients with postprostatectomy urinary incontinence representing different surgeons and different surgical techniques of RP have been endoscopically analyzed at our institution. 7 Two types of sphincteric defects have been described: A transection of the sphincter was seen in 65.1% of cases and a sphincter penetration by suture material in 46.2% of cases. A combination of both lesions was seen in 37% patients. Whereas transection of the sphincter is an irreversible damage, penetration of this muscle by suture material seems likely to result in a reversible functional disturbance, given that this condition is normalized early in the course.
Currently, urethrocystoscopy is not recommended as a standard postoperative procedure. According to the most recent European Association of Urology (EAU) guidelines on urinary incontinence, however, it is suggested as a supplemental tool within the two-stage assessment for diagnosis of complicated incontinence (including postprostatectomy incontinence). 8 Motivated by the results of the previous study, we hypothesized that an iatrogenic sphincter damage in terms of transection or penetration may result in early incontinence signs because of its relevant influence on the functional integrity of the muscle directly after surgery. The aim of this study was to identify early possible sphincter injuries as causes for urinary incontinence after RP. For this purpose. we endoscopically evaluated patients with severe early urinary incontinence symptoms after catheter removal after RP and searched for additional clinical signs possibly predictive for iatrogenic sphincter injuries.
Patients and Methods
Patients and surgical methods for RP
From 2005 until 2009, 374 open radical retropubic prostatectomies were performed by one surgeon at our institution. The ablative portion of the surgery was performed according to the modified technique for open RP as suggested by Walsh. 9 Preparation of the apical region as the most relevant step for oncologic and functional control followed recommendations by Graefen and coworkers. 10 The striated external sphincter is known to run circular and consists of fibers attached at the outside of the apex. The distal tip of the apex was exposed by pushing aside the fibers of the external sphincter, thus making it easily accessible for further incision of the urethra exactly at the end of the apex. Then, the vesicourethral anastomosis was established using four single-knot polyglactin sutures (coated Vicryl 0, UR-6, VC2594, Ethicon,® Somerville, NJ) in positions 12 degrees, 3 degrees, 6 degrees, and 9 degrees, respectively.
Postoperative continence assessment
On postoperative day 8, before catheter removal, cystography was performed to evaluate the urethrovesical anastomosis for impermeability. For this purpose, the bladder was filled with contrast medium, and the catheter was removed. Subsequently, the patient was asked to remain in a standing position and was observed by the examining physician. When a continuous dropping of urine during at least 2 minutes was observed and the patient was not able to successfully perform the stop-test, he was scheduled for further investigations and endoscopic evaluation on the next day. After catheter removal, the patient was asked to keep in a reclined position in bed for 3 to 4 hours to guarantee a sufficient voiding volume for subsequent urinary flow examination and postvoid residual (PVR) quantification. A repetition of the urinary flow examination and PVR quantification by ultrasonography were performed at the earliest 4 hours after catheter removal and repeated at least three times when the results were suspicious.
Endoscopic suture removal
The indication for endoscopic evaluation was initially given exclusively based on the clinical observation of continuously dropping urine after catheter removal. In addition, we measured urinary flow rate and residual bladder volume. During the course of the study we noted that those incontinent patients presented reduced urinary flow of <10 mL/s and a residual bladder volume of ≥50 mL; thus, we extended the inclusion criteria for those values.
All early incontinent patients (19/19) with this symptomatic triad underwent urethrocystoscopy the day after diagnosis. After identifying a sphincter penetration by suture material, we removed the culprit suture material endoscopically using a 45-degree Turner Warwick needle (Surg Master 0.9 NaCl, Olympus GmbH, Hamburg, Germany) (Fig. 1). For the initial three cases, we removed the sphincter penetrating suture as well as any visible suture material. With increasing expertise in assessing the fresh anastomotic region, however, we deleted the penetrating sutures only as we got more experienced to distinguish them from nonpenetrating sutures. On average we deleted two sutures (range 1–4) in the 19 patients.
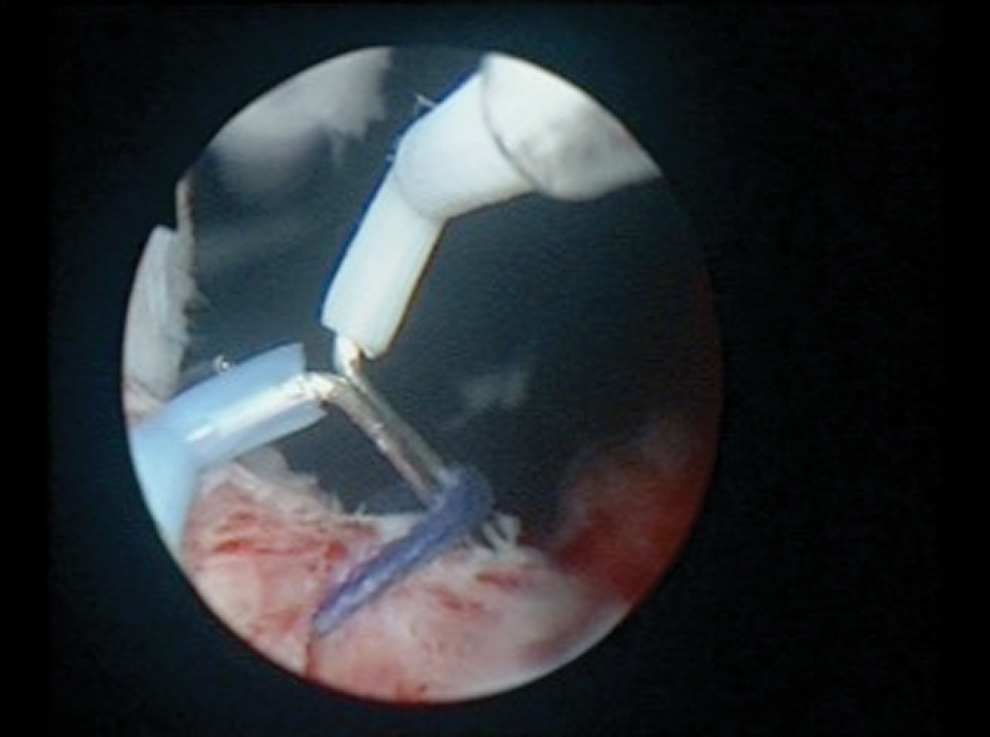
Endoscopic view of penetrating suture in 6-degree to 9-degree positions. Removal of the suture is executed with a Turner Warwick needle.
The average operative time for the entire endoscopic surgical procedure was 11 minutes (range 5–17 min). After the endoscopic intervention, patients were supplied with a transurethral catheter for 1 day. After removal of the catheter, we repeated the initial examinations with the addition of cystography to show integrity of the anastomosis after suture removal. The work flow used successfully in this study is shown in Table 1.
Results
Median age of the 374 patients who underwent retropubic RP with extended inguinal lymphadenectomy at our institution was 67 years. Follow-up was 28.5 months; mean operative time was 72 minutes (range 48–120 min). Oncologic results were as follows: Tumor classification of the entire group revealed a histopathologic distribution of pT2a in 10/347 (3%) patients, pT2b in 13/347 (4%) patients, pT2c in 212/347 (61%) patients, pT3a in 69/347 (20%) patients, and pT3b in 41/347 (12%) patients. Analysis of the respective lymph node status revealed pN0 in 345/347 (99.6%) patients and pN1 in 2/347 (0.6%) patients. With regard to local tumor control, our results indicated R0 status in 100% and 95% of all pT2a/b and pT2c patients, respectively, whereas in patients with locally advanced tumor stages (pT3a,b; n=110) negative resection margin (R0) was only achieved in 75% (83/110). Postoperatively, patients needed a transurethral urinary catheter for an average of 8.7 days (range 8–10 days ).
Among this entire patient cohort, we identified 19/374 (5%) patients who did show early incontinence signs after catheter removal and therefore underwent endoscopy. These patients presented the combined symptom triad (incontinence, reduced urinary flow rate, and elevated PVR). Table 2 shows the results of urinary flow and PVR by ultrasonography after catheter removal for this patient subgroup. During endoscopy in these 19 patients, sutures were visible in all cases. With increasing expertise, however, the penetrating sutures could be safely distinguished from the majority of visible sutures that could be identified clearly at the urethrovesical anastomosis attaching the urethra to the bladder neck without functional relation to the external sphincter.
After catheter removal, early incontinent patients underwent uroflow and ultrasonographic examinations. The table displays the respective values; examinations were repeated three times when initially suspicious (uroflow below 10 mL/sec, residual bladder volume ≥50 mL).
PVR=postvoid residual.
In 79% (15/19) of the patients, exclusive sphincter penetration by suture material was detected. The area of penetration was characterized by the endoscopic impression of a punctually packed sphincter with peripheral edema. When provoking sphincter contraction, distinctively reduced contractility was observed in the area of suture penetration whereas the remainder of the sphincter did show normal functionality. The endoscopic impression of the penetrated sphincter was as of an ellipsoid, distorted muscle (in the direction of suture penetration) with abrogated rotundity resulting in a mechanic constriction (Fig. 2).
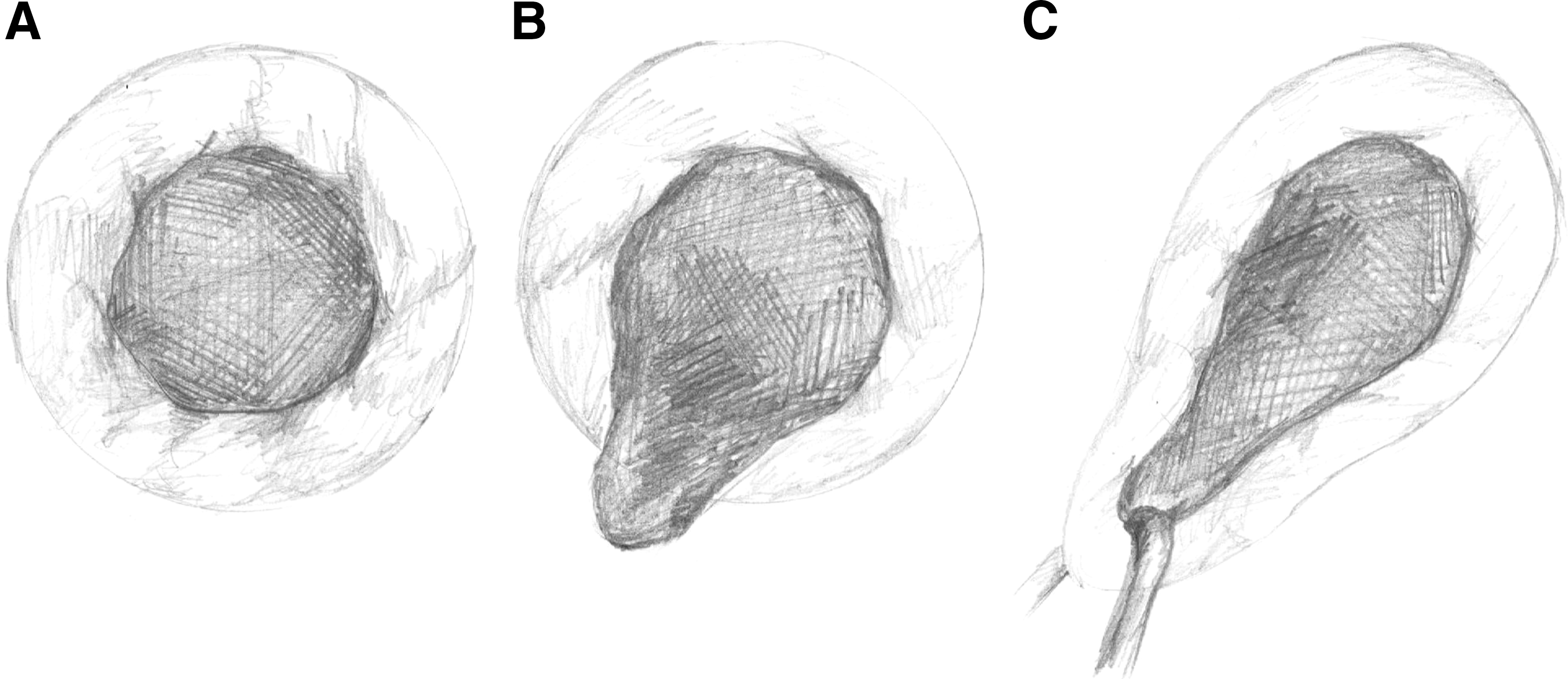
Sphincter alterations and endoscopic appearance. The observed sphincter alterations were predominantly visible under contraction.
The suture penetration was observed predominantly in the 3-degree (7/19) and 9-degree (8/19) positions; in two cases each, we could see the penetration in the 12-degree (2/19) and 6-degree (2/19) positions. Twenty-one percent (4/19) of patients did show additional sphincter injury in terms of transection. These four concomitant sphincter transections were seen in the lower circumference; the respective sphincter penetrations in those four patients were detected in the 3-degeee (2/4) and 9-degree (2/4) positions.
Endoscopically, the transections presented as a fresh gaping wound in the sphincter fibers (Fig. 2). When provoking muscle contraction, no contractility at all could be detected in the transected area of the muscle, whereas the region with suture penetration impressed as previously described. Because the combination of both damages was seen in close local relationship in those four patients, the functional disintegrity was considerably higher than in the patients with single sphincter penetration only. However, we removed the penetrating suture also in those four cases.
After removal of the penetrating suture and subsequent provocation of sphincter contraction, the formerly penetrated area remained still noncontractile; indeed, the described abrogated rotundity seemed to decrease and the previous nonfunctional area in the periphery of the penetration did show discrete signs of increased contractility, suggesting an ongoing recovery. After catheter removal 24 hours postintervention, we repeated the initial examinations (uroflow and bladder ultrasonography) with the addition of cystography to show integrity of the anastomosis after suture removal. In only two patients with exclusive sphincter penetration, we got permission to repeat postinterventional cystoscopy. In both cases, the previously seen sphincter alteration was regressive, and the muscle exhibited signs of functional and orthotopic recovery. All remaining patients denied permission for additional cystoscopy.
The residual volume decreased in all cases; the respective urinary flow rate increased within a short-term follow-up period of 4 weeks. All treated patients with sphincter penetration only were continent after the procedure and remained continent at the second follow-up after 6 months. From the four patients with combined sphincter damage who did not benefit from the endoscopic suture removal, two patients were treated successfully by autologous transplantation of muscle derived cells. 11 The two remaining patients received an artificial sphincter system.
As a major complication, we observed in one patient a discontinuation of the urethrovesical anastomosis after suture removal. This patient (second patient in this series) had shown an isolated sphincter penetration and had all four visible sutures removed during the endoscopic procedure. Because the complication occurred directly after suture removal, we were able to manage it promptly. We visualized the urinary bladder via percutaneous access and subsequent cystography. A wire was placed into the bladder/bladder neck (antegrade). Then a catheter was introduced endoscopically to the disconnected bladder (retrograde) via this wire, and the bladder was reattached to the urethra. The catheter remained in place for 4 weeks; after cystography and catheter removal, the patient was continent for the remainder of the follow-up.
Discussion
Current literature provides wide ranges of postprostatectomy urinary incontinence rates, presumably related to the unknown influence of the operating surgeon. 12 Critical self-evaluation following currently accepted guidelines and constructive reporting of possible pitfalls that could lead to postprostatectomy incontinence will likely help to better understand clinically significant causes for this complication.
Several more or less complicated questionnaires have been developed for assessment of urinary incontinence. Among those, the very simple and short International Consultation on Incontinence Questionnaire—Short Form, recommended by the EAU, seems to be a valuable tool for daily practice. 13 Unfortunately, those standardized systems for follow-up and documentation of postoperative continence features are seldom used when many patients are cared for by office-based urologists. Thus, evaluation and, more so, reporting of surgical outcome regarding postprostatectomy incontinence is often dependent on the particular (scientific) interest of the respective surgeons.
Our center is specialized in diagnosis and treatment of urinary incontinence in men, with particular focus on the treatment of patients with refractory postoperative stress urinary incontinence from damage of the urethral sphincter using autologous skeletal muscle-derived cells. 11 We recently identified two major types of sphincter defects among patients with assumed iatrogenic postprostatectomy urinary incontinence: A transection of the sphincter in 65.1% of cases and a sphincter penetration (most likely during the placement of the suture) in 46.2% of cases. A combination of both damages was seen in 37% patients. These results were based on the evaluation of 169 negatively selected incontinent patients representing four surgical techniques and at least 28 different surgeons in Germany. 7
The data presented here show the experience of 374 patients operated on by a single surgeon over 5 years, using the same retropubic approach. Clinical observation of the patients after catheter removal and early cystoscopic evaluation are the main pillars of this investigation. We identified 19 patients among 374 with early postoperative incontinence, corresponding to an initial incontinence rate of 5.1%. Interestingly, these patients with early postoperative incontinence presented with a coincidentally augmented PVR and a significant obstructive urinary flow rate.
The initial postoperative incontinence rate was reduced to 1.1% after successful endoscopic removal of the sphincter-altering sutures. Both rates are in the range of described high postoperative continence rates between 91% and 98% reported for high-volume centers with small numbers of surgeons. 14,15
The oncologic status of the 19 patients with sphincter damage is reflective of the entire RP collective of our institution. We performed prostatectomy predominantly in patients with intermediate risk/high risk prostate cancer. Apex preparation, however, was performed extensively in all cases, because suboptimal apical dissection resulting in positive resection margins should always be avoided when trying to preserve the sphincter. Although it is strongly recommended to preserve as much as possible of the circumferential muscle, rhabdosphincter fibers, its fascial attachments, and the autonomic and somatic nerve supply during dissection of the apex region, 16 the extensive apex preparation in our series may be the most probable reason for transection or sphincter penetration during placement of the suture. It seems to occur independently from the aggressiveness of the tumor.
Until recently, few reports exist about endoscopic evaluation of the sphincter region in postprostatectomy incontinent patients. The invasive and probably disturbing urethrocystoscopy is not recommended as a standard postoperative procedure to evaluate postprostatectomy incontinence. It is suggested, however, for complicated cases of urinary incontinence within the two-stage assessment for diagnosis by the EAU guidelines. 8 Our data suggest that some postprostatectomy incontinent patients may be detected early in the postoperative course by the symptomatic triad of early incontinence, reduced urinary flow rate and elevated PVR, which are indicative of sphincter penetration. In addition, this group of patients seems to benefit from early endoscopic evaluation and suture removal because this sphincter damage seems to be still reversible at that stage.
Without doubt, assessment of urinary flow immediately after catheter removal in incontinent patients may be difficult because those patients may have problems building up a sufficient volume in the bladder to adequately perform this test. In this study, the mean voiding volume was 110 (100–170) mL, whereas the mean PVR was 60 (50–110) mL; thus, reduced voiding volume may have negatively altered the urinary flow in the patients. This has to be critically taken into account when analyzing the symptomatic triad described here. This symptomatic triad, however, has to be further investigated in higher numbers of patients with regard to reproducibility.
Finally, the decision to have a patient undergo cystoscopy was mostly triggered by the clinical observation of a continuously dropping urine and negative stop-test directly after catheter removal and the grade of incontinence that was evaluated by pad test (at least 5 pads per day) and individual description by the patient. The additional data of reduced flow and increased PVR were coincidentally observed as side effects of this incontinence situation. In our entire prostatectomy cohort, those 19 patients were the only ones with those signs of incontinence after catheter removal.
Urethrocystoscopy is of crucial importance for this early diagnosis. In the 15 patients with isolated sphincter penetration, early removal of the sutures resolved early urinary postprostatectomy incontinence. It seems plausible that penetration of the sphincter by a suture results in affected integrity and functionality of this muscle. Whereas transection of the sphincter is an irreversible damage, penetration of this muscle by suture material seems likely to result in a reversible functional disturbance, given that this condition is normalized early in the course, as done in this study. It seems plausible that simple and punctual removal of the confining suture may lead to recovery of functional integrity of the sphincter and consecutively to recovery of continence. This could be shown endoscopically in two patients in this study and, although not cystoscopically proven, the recovered incontinence in the remaining patients with isolated sphincter penetrations highly suggests functional recovery of the sphincter as well.
When this suture removal is not performed or delayed, however, scar tissue formation is likely to occur, and the initially reversible damage becomes irreversible. Although the precise etiology of postprostatectomy urinary incontinence has not been completely understood until now, it is commonly accepted that it can be a result of sphincteric incompetence or/and bladder dysfunction. Thus, our data causing a damaged sphincter responsible for incontinence are in accordance with this theory. Moreover, it is not a surprise that the observed sphincteric incompetence from muscle damage occurs early in the course, even directly after catheter removal, because the sphincter may transiently lose relevant parts of its functional integrity, as shown here. Of course, incontinence may alter in the clinical course from worsening to improving.
We cannot give exact information about the number of incontinent patients in our entire prostatectomy cohort because follow-up of all patients was limited. Normally, patients after RP are seen by office-based urologists, reducing the possibility to have continuous data about mid- and long-term follow-up regarding functionality after RP. The reported 19 patients were the early incontinent patients of our cohort; the number of patients classified incontinent grade I–III in the longer follow-up are not known. In the long term, postprostatectomy incontinence develops toward a more complex appearance with concomitant causative factors such as as urethral strictures, urodynamic alterations. The aim of this study was to show very early and possible reasons of sphincteral disturbance; thus, it is not a surprise that we did not observe relevant urethral strictures 8 days after RP directly after catheter removal.
We consider it crucial, however, to identify patients who show symptoms of early incontinence and to subsequently subject them to endoscopic evaluation, as done here. Otherwise, those patients get lost to immediate functional follow-up and a possibly curable sphincter disturbance as suture penetration turns from reversible to irreversible.
Our rate of 5% incontinent patients early after surgery remains realistic. It could be argued that the present data show a systematic error of a particular surgeon. Obviously, these patients had the same common iatrogenic sphincter damage during RP. This damage reflects a certain complexity in the previous surgery that led to this sphincter disturbance. As we have shown previously in a negatively preselected group of 169 incontinent patients after RP, sphincter penetration had a relevant impact on functional outcome during RP, independent of the surgeon or the surgical technique. 7 We can only assume that without suture removal, the 15 patients would not have regained their continence. Moreover, as a main conclusion, we could show that the effect of an isolated sphincter penetration is reversible and can be cured when diagnosed in a timely fashion.
Our intention was to emphasize the value of endoscopic inspection of the anastomosis in the early and midterm follow-up of incontinent patients after RP. Therefore, the described symptomatic triad and the subsequent endoscopic evaluation/suture removal could be a problem handling approach for detection and therapy of early incontinence after RP. Suture removal could be performed easily, and the anastomosis remained sufficient in 18/19 cases. In one patient, who was among the first patients treated in the reported cohort, we observed a major complication as a discontinuation of the urethrovesical anastomosis resulting in bladder dislocation/cranialization after the removal of four sutures (one penetrating suture, three additionally visible sutures). The complication could be managed immediately and did not lead to permanent damage. With ongoing experience, we limited the number of removed sutures to a maximum of two and subsequently experienced no further complications.
This study has several limitations. Being a clinical observation, it is neither a prospective nor a controlled investigation. The patient number is small, and no preoperative urinary flow rates were obtained for comparative purposes. The study was a retrospective observation, and we did not have asymptomatic patients undergo cystoscopic evaluation as a control group because this examination may be disturbing and would not have been justified in patients without symptoms within the early postoperative course after RP. In addition, for the same reason, only two of the 19 investigated patients accepted postinterventional recystoscopy after suture removal.
As the sphincter penetration was endoscopically very obvious and the consecutive functional disturbance seemed very likely in all cases, we did not see a reason for a subsequent urodynamic evaluation. Thus, although very unlikely to be causative of the incontinence in our patients, bladder outlet obstruction and bladder overactivity have not been excluded as theoretical major contributors to incontinence. In further prospective investigations. those parameters should definitely be investigated.
In our opinion, we present important observations that seem to follow a defined pattern of clinical signs. Further, comparable investigations and observations by other surgical centers may help to critically evaluate the value of the presented results. Therefore, endoscopic evaluation of early postprostatectomy urinary incontinence should be encouraged. The key is to identify the appropriate patient who has high probability of showing sphincter penetration and who would benefit from a minimally invasive procedure with potentially high impact on the postoperative course and quality of life.
Conclusion
The combination of early urinary incontinence, decreased urinary flow, and PVR can be used as an indicator for sphincter penetration by anastomosis sutures as cause for urinary incontinence. Intensive clinical observation and early cystoscopic evaluation of the sphincter/anastomosis region may help to detect this functional disturbance and avoid irreversibility. Transection and removal of the sutures may be easily performed and seem to decrease postprostatectomy incontinence rates.
Footnotes
Acknowledgments
This article is dedicated to Prof. Dr. Günther Wiedemann on the occasion of the 10th meeting of the North German Cytostatic Workshop-South, September 9–10, 2011.
Disclosure Statement
No competing financial interests exist.