
Abstract
Purpose:
To evaluate differences in the serum concentrations of cell adhesion molecules (CAMs) after retroperitoneal laparoscopic and conventional open radical nephrectomies for localized renal-cell carcinoma (RCC).
Patients and Methods:
A total of 62 patients with stage T1N0M0 RCC were randomized to either a retroperitoneal laparoscopic radical nephrectomy group (n=31) or an open group (n=31). Serum levels of soluble cluster of differentiation 44 splice variant 6 (sCD44v6), soluble intercellular adhesion molecule-1 (sICAM-1), soluble vascular cell adhesion molecule-1 (sVCAM-1), and soluble epithelial cadherin (sE-cadherin) were determined independently by enzyme linked immunosorbent assay (ELISA) preoperatively, and on postoperative days 1 and 5. In addition, follow-up results were compared.
Results:
On postoperative day 1, sCD44v6, sICAM-1, and sVCAM-1 levels increased significantly compared with preoperative levels in both groups (P<0.05). sE-cadherin levels decreased compared with preoperative levels in both groups without statistically significant differences (P>0.05). sCD44v6 levels in the retro-laparoscopy group were significantly higher than in the open group (P<0.05), while sICAM-1, sVCAM-1, and sE-cadherin levels showed no statistically significant differences between both groups (P>0.05). On postoperative day 5, all parameters in both groups were similar to preoperative values (P>0.05). Follow-up ranged from 7 to 18 months postoperatively in all 62 patients, with a 100% cancer-specific survival rate in each group.
Conclusion:
Although postoperatively higher serum concentrations of CAMs in both groups and significantly elevated sCD44v6 in the retro-laparoscopy group may be facilitated, the differences in CAMs between both groups are small and transient. Together with the similar follow-up results, this further supports previous studies that failed to show a difference in the oncologic outcomes between open and laparoscopic radical nephrectomy and provides a probable molecular mechanism.
Introduction
Interestingly, port-site metastases and local recurrences, although only occasionally observed, remain an unsatisfactorily explained phenomenon with laparoscopic cancer surgery. 8,9 A few experimental studies suggested that laparoscopic surgery promoted tumor growth and metastases, 10,11 while other investigators failed to confirm these experimental results in similar animal models. 12 The metastatic mechanism is complicated, and cell adhesion molecules (CAMs) may play an essential regulatory role in the process of metastatic spread and invasion of cancer cells. 9,13
Cluster of differentiation 44 splice variant 6 (CD44v6), intercellular adhesion molecule-1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1), and epithelial cadherin (E-cadherin) are the representative and most reported molecules involved in the cell-cell and cell-extracellular matrix interactions at tumor metastases. It has been reported recently that laparoscopy under CO2 insufflation can affect the serum concentrations of these CAMs. 14
A number of studies have tried to prove the metastatic mechanism of CAMs expressed in various human malignant cells and tissues, such as colorectal cancer, gastric cancer, malignant melanoma, breast cancer, and ovarian cancer, as well as their soluble forms in serum. 15 Little attention has been paid to CAMs in RCC, however, particularly after various surgical interventions. Thus, it is necessary and prudent to investigate whether laparoscopy influences the serum concentrations of CAMs.
In this study, we compared the alterations in the serum concentrations of sCD44v6, sICAM-1, sVCAM-1, and sE-cadherin after retroperitoneal laparoscopic and ORNs for localized RCC.
Patients and Methods
Study design
A total of 62 patients with stage T1N0M0 RCC admitted for surgical treatment between January 2009 and January 2010 were included in the study. The diagnosis of localized RCC was assumed when color Doppler imaging, enhanced CT, and/or MRI demonstrated renal masses. Two experienced radiologists and three senior urologists read the radiographic images carefully before patients' inclusion to minimize the possibility of benign masses.
Thirty-one patients were randomized to undergo retro-laparoscopic nephrectomy, and an additional 31 patients underwent the open retroperitoneal technique. Randomization was accomplished using closed envelopes prepared by a statistician, based on a computed randomization system. The primary clinical parameters recorded were demographic data, tumor information, duration of the operating procedure, estimated blood loss, duration of hospital stay, complications, and follow-up (Table 1). Consequently, all tumors removed were pathologically proven to be RCCs, and the information on pathologic subtype, pathologic stage, and Fuhrman grade is listed in Table 1.
GIT=gastrointestinal tract.
The primary end point of the study was the altered serum concentrations of CAMs in both groups of patients within 5 days postoperatively. The second end point was the difference in the serum concentrations of CAMs between the both groups. In addition, at the beginning of this research, we planned to keep close contact with the patients for 5 years to study the further results.
Ethical issues
The design and execution of this study was approved by the Hospital Ethics Committee, and written informed consent was obtained from every patient involved.
Exclusion criteria
Criteria for exclusion were as follows: History of infection in the retroperitoneal space, history of hormone replacement or immunosuppression therapy, and previous surgery or trauma to the lumbar region. Any evidence of an acute phase reaction, such as leukocytosis or various fever grades, was also considered an exclusion criterion. Indications for nephron-sparing surgery (NSS) are anatomic or functional solitary kidney; functioning opposite kidney that is affected by a condition that might impair renal function in the future; a peripheral renal tumor of up to 4 cm maximum diameter that was not close to the hilum with a healthy contralateral kidney. To prevent chronic kidney disease and its associated cardiovascular morbidity and potential mortality, the candidates for NSS were also not involved in this research, which meant the size of tumors more than 4 cm, and mass sizes below 4 cm, but located inside the kidney or adjacent to the hilum were considered for inclusion.
Operations and techniques
General anesthesia methods and a lateral decubitus position were applied in both groups. For open access, a 20-cm trans 12th rib lumbar incision was used according to standard surgical protocols without modification. Retro-laparoscopic operations were performed with a standardized technique using three trocars at the waist. A carbon dioxide pneumoperitoneum was established with an intra-abdominal pressure of 12∼15 mmHg throughout the operation. Electric and ultrasound scalpels were used to mobilize the kidney and Hem-o-lok was used to ligate the main vessels. After complete removal, the intact kidney with its perirenal fat and fascia was extracted in an entrapment bag through the 7-cm enlarged incision of the main trocar site, and one F14 drainage tube was secured through the 5-mm trocar site.
Laboratory assays
Five milliliters of venous blood were taken from each patient by peripheral venipuncture 1 day before the operation and on days 1 and 5 after the operation. After collection, the sample was cooled at room temperature for 30 minutes and centrifuged at 3000 g for 10 minutes. The serum from the upper layer of the centrifuged blood was separated and stored at −70°C until analysis. Serum sCD44v6, sICAM-1, sVCAM-1, and sE-cadherin concentrations were determined using commercially available enzyme-linked immunosorbent assay (ELISA) kits (Bender Med Systems, Vienna, Austria) according to procedures recommended by the manufacturer. Each serum sample was tested in duplicate. The sensitivity of the ELISA was 0.5 ng/mL for sCD44v6 and sICAM-1, 0.9 ng/mL for sVCAM-1, and 1.0 ng/mL for sE-cadherin.
Statistical analysis
Statistical analysis was performed using the SPSS software package (SAS Institute Inc., Cary, NC). The independent samples t test was used to compare means between two groups, and the chi-square test was used for enumeration data. Comparisons between the CAMs before and after surgery were performed according to the analysis of variance test (single factor factorial; one repeated measure). A value of P<0.05 was considered statistically significant. The power was set to 0.9.
Results
Patient characteristics in terms of gender, age, weight, body mass index, involved side of kidney, tumor size, Fuhrman grade, pathologic subtype, pathologic stage, procedure duration, and main complications were similar between the two groups (P>0.05). Two intraoperative complications were noted in each group, and one wound infection occurred in the open group. The retro-laparoscopy group had advantages over the open group regarding estimated blood loss (30.0±18.0 mL vs 156.4±45.7 mL; P=0.011), postoperative gastrointestinal tract restoration (18.7±8.4 hours vs 39.8±9.1 hours; P=0.035), time to ambulation (24.6±9.3 hours vs 47.7±10.2 hours; P=0.044), and duration of hospital stay after surgery (4.7±0.9 days vs 8.0±1.2 days; P=0.019) (Table 1).
Cell adhesion molecules
Serum concentrations of sCD44v6, sICAM-1, sVCAM-1, and sE-cadherin measured before the surgery did not differ significantly between the two groups (P=0.941, P=0.922, P=0.871, P=0.940, respectively).
On postoperative day 1, both groups exhibited a noticeable increase in sCD44v6, sICAM-1, and sVCAM-1 levels (P<0.05), and the sCD44v6 level in the retro-laparoscopy group (353.5±51.2 ng/mL) was significantly higher than in the open group (238.1±48.3 ng/mL; P=0.047). There were no significant differences between the two groups in regards to sICAM-1 and sVCAM-1 levels (P=0.753, P=0.786). With respect to the sE-cadherin level, there was a moderate decrease in both groups one day after surgery (P>0.05) and although the concentration in the retro-laparoscopy group (1756.4±574.2 ng/mL) was lower than in the open group (1948.7±621.1 ng/mL; P=0.714), the difference was not significant.
On postoperative day 5, all the parameters in both groups returned to approximately preoperative levels (P>0.05) and no significant differences between the two groups were found (Fig. 1).
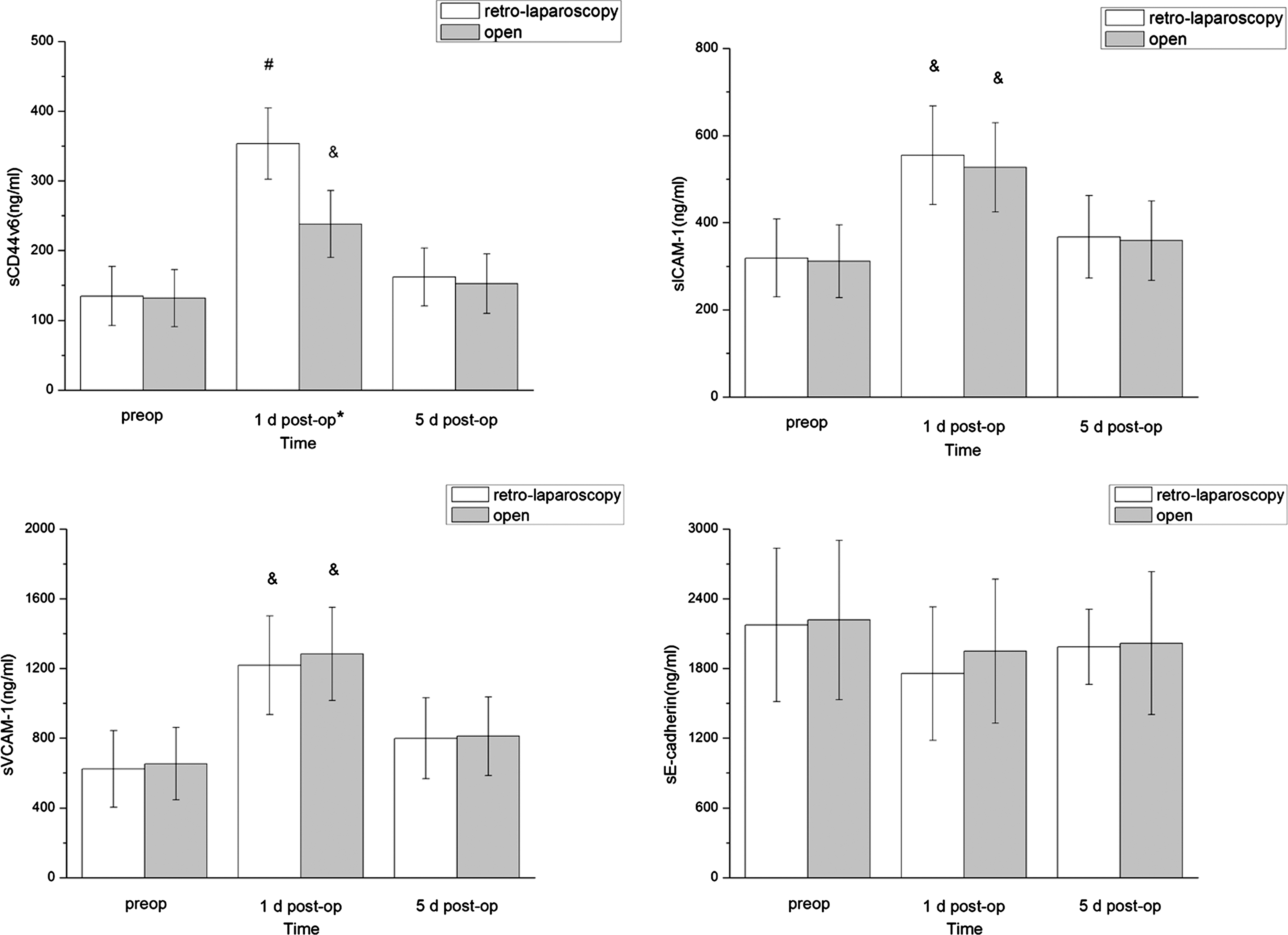
Variations in serum sCD44v6, sICAM-1, sVCAM-1, and sE-cadherin levels after retro-laparoscopic and open radical nephrectomies. & P<0.05, # P<0.01 compared with preoperative serum levels; *P<0.05 retro-laparoscopy vs the open procedure.
Follow-up
The doctor and each patient remained in close contact. Both groups experienced the same follow-up duration (12.3±3.3 mos vs 12.1±3.0 mos; P=0.899), ranging from 7 to 18 months postoperatively for all 62 patients with a 100% cancer-specific survival rate. No clinical manifestations of any port site, wound, or distant metastases or local recurrence were observed, and objective auxiliary imaging examinations further demonstrated these results. At this time, there have not been any differences reported in the oncologic results for the two groups.
Discussion
Laparoscopy has been shown to be a safe and reliable technique to treat patients with various diseases, including malignancies. Besides milder pain, shorter convalescence, and improved cosmesis, it is even reported to provide better preservation of immunity. 16,17 Recent clinical trials in the United States and Europe have demonstrated that the recurrence and 5-year survival rates of LRN are identical to data obtained from open surgery. 5 –7 Thus, use of this minimally invasive technique in the surgical management of RCC should be theoretically safe and reliable in terms of the oncologic effect on the tumor compared with conventional surgery. 3,4 There have been no adequate researches, however, addressing the molecular mechanism for the equivalence until now.
Furthermore, probable oncologic risks of laparoscopic surgery in urologic carcinomas have been reported in several studies. 18,19 Specific worries about the pneumoperitoneum, tumor manipulation, and specimen extraction are addressed. Some experimental studies reported that laparoscopic surgery could promote tumor growth and metastases. 10,11 As to RCC, one of the greatest concerns is whether performing LRN under CO2 insufflation will enhance the possibility of metastases compared with the conventional open operation given that laparoscopy-related studies on metastases of RCC are lacking. Some CAMs were reported to be involved in the process of metastatic spread and invasion of cancer cells. 9,13 To make things clear, this study focused on the alterations of CAMs after either open or retro-laparoscopic radical nephrectomy.
Soluble circulating forms of CAMs can be shed by cancer cells as well as by peripheral blood mononuclear cells, endothelial cells, and fibroblasts. Changes in the concentrations of soluble circulating CAMs, including sE-cadherin, sICAM-1, sVCAM-1, and sCD44v6, have been reported to alter the progression, invasiveness, and metastatic potential of various carcinomas in many clinical and experimental studies. 15,20,21 E-cadherin has been reported to have a major function in cell-cell adhesion processes, mediating the adhesiveness and integrity of different epithelial cell formations. 22 Shiozaki and associates 23 reported that loss of expression and/or abnormal function of this molecule could initiate tumor invasion and metastases because E-cadherin may prevent the possible detachment of tumor cells from the primary focus. ICAM-1 mediates the adhesion of circulating cells to the intravascular endothelium and the following extravasation. 13 Thus, high concentration of ICAM-1 is believed to promote the adhesion of circulating tumor cells to the endothelium. 13 VCAM-1 is involved in the adhesion of white blood cells to the endothelium and is relevant to tumor growth and angiogenesis. 24 Changes in the concentration of CD44 are reported to be associated with increased tumor spread and metastases. The CD44 variant exon v6 has been described as more frequently expressed in many cancers than the variant exons v3–5, v7–10. 15
With respect to RCC, Ohno and colleagues 25 found that elevated levels of ICAM-1 measured in the serum of RCC patients were negatively associated with patient survival and could be a pretreament predictor of overall survival. The sICAM-1 levels were found to be higher in metastatic tumors. Vasselli and coworkers 26 identified VCAM-1 as a prognostic biomarker. High concentrations of this CAM predicted for better overall survival in both clear-cell and papillary cancers, suggesting that VCAM-1 may generally indicate tumor cells with lower metastatic potential. 27 Loss of E-cadherin was reported to be relevant to RCC progression. 28 Gilcrease and colleagues 29 suggested that the splitting product CD44v6 from the standard form CD44s might correlate with RCC progression and recurrence. All these studies above support that molecular features of CAMs could be used to explain metastatic behavior of RCC. 27
In this study, we investigated whether the serum concentrations of CAMs were changed after retroperitoneal laparoscopic nephrectomies and ORNs for localized RCC, particularly in the narrow retroperitoneal space under CO2 pneumoperitoneum. With identical clinical/pathologic tumor-node-metastasis (TNM) stages, pathologic subtype, and Fuhrman grades, there were no significant differences in preoperative serum sCD44v6, sICAM-1, sVCAM-1, and sE-cadherin concentrations between the two groups.
On postoperative day 1, both groups exhibited a marked increase in sCD44v6, sICAM-1, and sVCAM-1 levels (P<0.05) and a moderate decrease in sE-cadherin (P>0.05). The results imply that variations in serum CAMs can be regulated by shedding into the bloodstream during and after operative manipulation, and surgical trauma and inflammatory reactions could be contributing factors. Moreover, significant elevations in sCD44v6 levels were observed in the retro-laparoscopy group. It is not clear yet for the elevated sCD44v6 levels; however, CO2 pneumoperitoneum could be a promoting factor.
On postoperative day 5, all the levels of serum CAMs in both groups returned to approximately preoperative levels (P>0.05), inferring that the durations of the altered serum CAMs levels after either type of surgery were not long lasting.
From a biologic viewpoint, the negative impact of a sustained positive pressure CO2 pneumoperitoneum is somewhat debatable and the risks of laparoscopy remain hard to clarify. Superficially, elevated concentrations of CD44v6 seem to be associated with an increased metastatic potential and a poorer prognosis in patients with various carcinomas. 30 In this study, a transient increase in sCD44v6 levels was noticed in the retro-laparoscopy group; nevertheless, it is difficult to evaluate what adverse influences may have been exerted on the potential metastases. Subsequently, equal short- to medium-term follow-up results were achieved in both groups without the occurrence of any metastases or recurrence. Based on these results, it is possible that preserved immune function after laparoscopic surgery may offset some adverse effects of CAMs when their elevations are altered just for a limited time. 31,32 Theoretically, this study further supports the existing clinical data and explains the possible reason why identical consequences could be achieved after both surgeries in the literature.
First of all, this study was more descriptive than conclusive. Moreover, the number of RCC patients involved was small and follow-up of the patients was too short. Therefore, it is difficult to completely clarify a substantial conclusion according to the information above. Notwithstanding these limitations, this study provides a base for the following advancement in this area. Longer follow-up results and further studies with a larger number of patients and higher TNM stages are needed in our future work to elucidate the role of CAMs in RCC patients who undergo retroperitoneal LRN.
Conclusion
Although postoperatively, higher serum concentrations of CAMs in both groups and significantly elevated sCD44v6 in the retro-laparoscopy group may be facilitated, the differences in CAMs concentrations between both groups are small, transient, and almost coordinative. Together with the similar follow-up results, this further supports previous studies that failed to show a difference in the outcomes between ORN and LRN, justifies the oncologic reliability of laparoscopy for RCC, and provides a probable molecular mechanism.
Footnotes
Acknowledgments
This program was supported by the National Natural Science Foundation of China (Grant No.30901484 and No.30973013/H0513).
We thank Lan Zheng, M.D. and Shuang Zhang, M.D. for their expert technical assistance.
Disclosure Statement
No competing financial interests exist.