
Abstract

Introduction
The patient is a 28-year-old woman who has had recurrent urinary tract infections (UTIs) over the previous 2 years. These UTIs have typically manifested with symptoms of cystitis and were never associated with fever. Her primary care physician eventually referred her to a urologist. Her medical history and physical examination were unremarkable. A urinalysis was performed and found to be consistent with UTI; her urine culture ultimately grew >100,000 colonies of Escherichia coli.
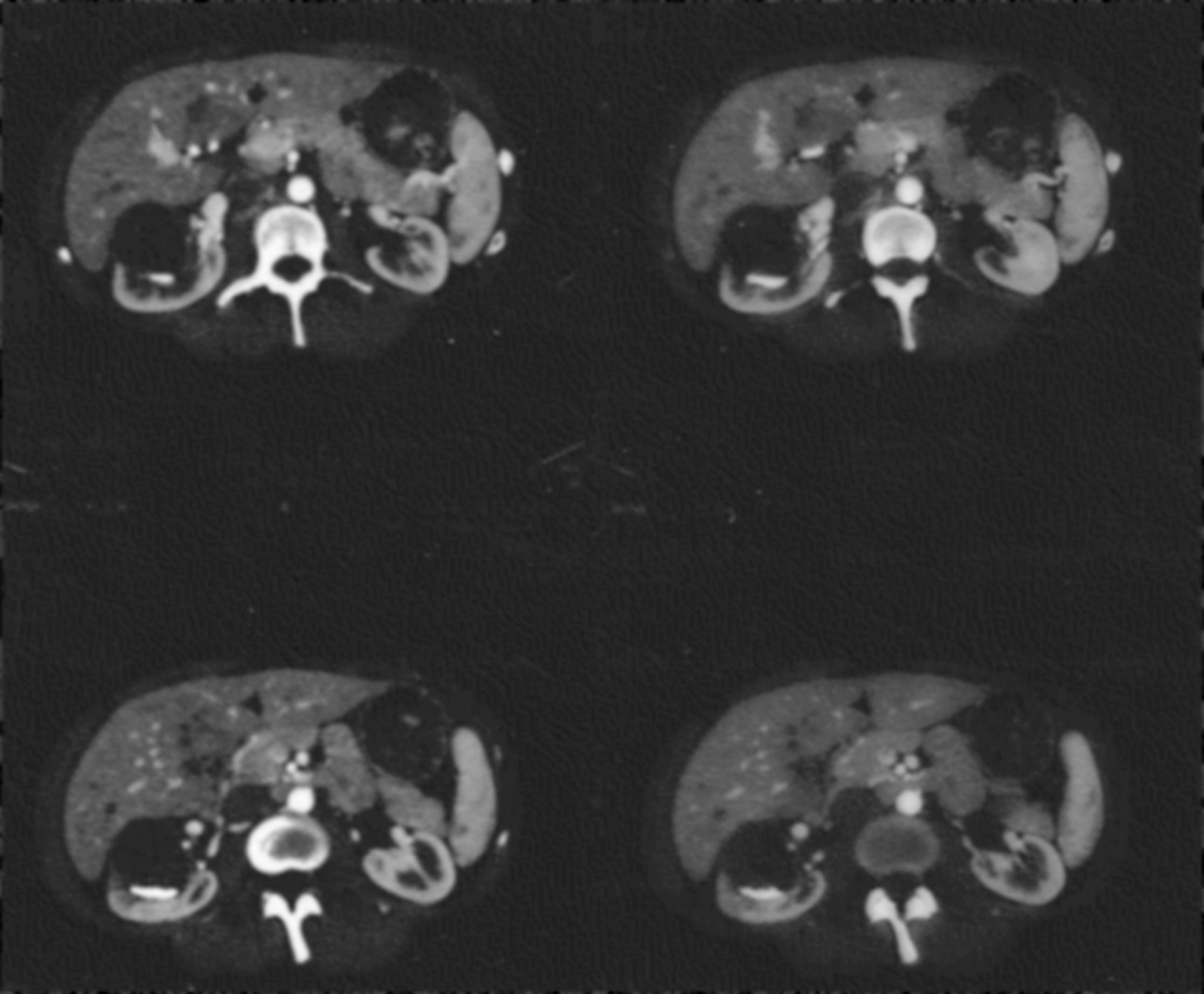
A CT scan was performed (Fig. 1).
The patient is a 28 year old female who has suffered from recurrent urinary tract infection (UTI) over the previous two years. These UTIs have typically manifested with symptoms of cystitis and were never associated with fever. Her primary care physician eventually referred her to a urologist. Her past medical history and physical examination were unremarkable. A urinalysis was performed and found to be consistent with urinary tract infection; her urine culture ultimately grew >100,000 colonies of E. coli.
Expert Opinions
No. 1
The patient should be questioned about risk factors for recurrent UTIs: Poor fluid intake, infrequent voiding, constipation, association with coitus. We would start by treating her in a conservative fashion: Increasing fluid intake, regular voiding, and daily bowel movements. She may benefit from one dose of postcoital antibiotics if the UTIs are associated with sexual intercourse. 2 Self-start therapy with an appropriate antibiotic, such as oral nitrofurantoin 100 mg twice daily for 7 days at the start of any symptoms (urine cloudiness, foul-smelling urine, or dysuria) in addition to a standing order for a urine culture, should be offered to the patient as well. 3
After conservative management for 6 months, reevaluation about the frequency and precipitating factors for UTIs should be evaluated. If there is a definite cause for the infections, such as dehydration, sexual intercourse, or constipation, then targeted therapy to remedy these situations should be continued. If the UTIs recur but without any known precipitating cause, one would consider therapy for the caliceal diverticulum with the caveat that the patient's recurrent UTIs may continue despite treatment of the diverticulum. Certainly, there have been case reports of infections occurring from and within caliceal diverticuli, 4,5 but this current patient's lack of symptoms would tend to favor the diagnosis of recurrent UTIs over infections related to caliceal diverticulum.
If treatment is to be considered for the caliceal diverticulum as a cause of the infections, the patient must be counseled appropriately and understand that the infections may continue to occur even if the diverticulum is treated. Treatment options for diverticuli involve percutaneous nephrolithotomy with ablation, ureteroscopy with laser incision of the stenosed infundibulum, 6 or laparoscopic partial nephrectomy of the diverticulum. 7 The usual treatment of choice is the percutaneous approach in which the puncture is made directly into the diverticulum with or without ballooning open the stenosed infundibulum so that the diverticulum may drain into the rest of the collecting system. 7 Ablation using a resectoscope and roller ball electrode should result in ablation of the caliceal diverticulum. The main limitation to the percutaneous approach is that it is not good for accessing anterior calices. Tracts can be made into anterior calices, but traverse many major blood vessels and increase the risk of bleeding.
In this case, the caliceal diverticulum is very anterior with little or no overlying parenchyma. The best approach for treatment would be a laparoscopic decortication of the diverticulum, 7 an operation that is similar to that originally described for large symptomatic renal cysts. 8 In the operating room, a ureteral catheter should be placed via flexible cystoscopy so that methylene blue may be administered to identify the internal os for fulguration once the diverticulum has been marsupialized. Then the patient should be placed in the lateral decubitus position with the table flexed. Standard three-port placement to access the kidney should be obtained.
Standard dissection and clamping of the vessels (as for partial nephrectomy) are typically not necessary, because there is very little or no overlying parenchyma. The Gerota fascia overlying the kidney is removed, and the edges of the diverticulum are identified. Laparoscopic ultrasonography may be of benefit to identify the edges of the diverticulum. The middle of the diverticulum may be entered and the fluid removed by suction. Using the harmonic scalpel or some form of heat cautery method, the edges of the diverticulum are removed. Cauterization of the inside of the diverticulum is not necessary, 9 because it may cause injury to deeper vessels and result in bleeding. A surgical drain is left through one of the 5-mm ports as well as a Foley catheter in the bladder; both will be removed before the patient is sent home.
A laparoscopic assisted percutaneous nephrolithotomy has also been described in the literature for anteriorly located caliceal diverticuli. 10 Basically, laparoscopic methods are used to take down the colon along the white line of Toldt, and a more anterior puncture can be made directly into the anterior caliceal diverticulum. This method prevents the percutaneous tract from traversing bowel.
Follow-up will consist of urine cultures and a CT-intravenous pyelography and/or ultrasonography within 3 to 6 months to evaluate the caliceal diverticulum. The radiologic tests, however, are not the most important metric to measure postoperatively: The best measure of success will be the reduction or elimination of UTIs in this young patient. Should the UTIs recur, it is important to have counseled the patient preoperatively, and general and/or directed measures to reduce these infections may be needed.