
Abstract

Scientific Program for 29th World Congress of Endourology & SWL
Abstract Index
BR01: Basic, New Technology
Hrishi B. Joshi, UK
Iason Kyriazis, Greece
Markus J Bader, Germany
Yung K Tan, USA
Tatsuo Igarashi, Japan
Nuzhath Khan, UK
Kamran Ahmed, UK
Kamran Ahmed, UK
Prassannah Satasivam, Australia
Kapil Sethi, Australia
Ephrem O. Olweny, USA
Kurdo Barwari, Netherlands
Jan Colli, USA
Panagiotis Kallidonis, Greece
Aarond D. Benson, USA
BR02: Basic, Urolithiasis 1
Sutchin R. Patel, USA
Haresh Thummar, India
Rahim Taghavi, Iran
Haresh Thummar, India
Brian Duty, USA
Andrew Fuller, Canada
Haresh Thummar, India
Haresh Thummar, India
Maria Chiara Sighinolfi, Italy
Danny _ M Rabah, Saudi Arabia
Mohammad Reza Darabi Mahboub , Iran
Yoram Siegel, Israel
Alexander P. Duryea, USA
Fahimeh Kazemi Rashed, Iran
BR03: Basic, Robotic/Lap Surgery/Prostate/Female Urology/New Technology
Odysseas Andrikopoulos, Greece
Eric R. Taylor, USA
Jan Colli, USA
Jan Colli, USA
Janet L. Colli, USA
Kirk Tamaddon, USA
Kirk Tamaddon, USA
Aaron D. Benson, USA
Mohammad Reza Darabi Mahboub , Iran
George R. Schade, USA
Ju Hyun Lim, Korea
Ju Hyun Lim, Korea
Gideon Lorber, Israel
Gernot Bonkat, Switzerland
Philip G Smith, Australia
BR04: Basic, Urolithiasis 2
John WM Yuen, Hong Kong
Dirk Lange, Canada
Haresh Thummar, India
Ahmet A Sancaktutar, Turkey
Pankaj N Maheshwari, India
Iason Kyriazis, Greece
Dmitry Merinov, Russia
Carl Sarkissian, USA
Andy C.H. Won, Australia
Agnes J. Wang, USA
Eric R. Taylor, USA
Agnes J. Wang, USA
Agnes J. Wang, USA
Agnes J. Wang, USA
MP01: Less/Notes 1
Gang Zhu, China
Byong Chang Jeong, Korea
Jeffrey Woldrich, USA
yaqun zhang, China
Takatsugu Okegawa, Japan
Yuanhu Yuan, China
Ma Lulin
Gang Zhu, China
S Jeff Chueh, USA
Jeffrey Woldrich, USA
Zhang ShuDong, China
Kyung D Baik, Korea
Shogo Inoue, Japan
Steven M Lucas, USA
Ahsan Rao, UK
Jeffrey Woldrich, USA
MP02: Education & Simulators
Sashi S. Kommu, UK
Sashi S. Kommu, UK
Sashi S. Kommu, UK
Irene M. Tjiam, Netherlands
irene M. Tjiam, Netherlands
Sashi S. Kommu, UK
Samuel Bishara, UK
Sashi S. Kommu, UK
Sashi S. Kommu, UK
Nasser simforoosh, Iran
Jason Y Lee, USA
Jun Teishima, Japan
Benjie Tang, UK
Benjie Tang, UK
Thomas Johnston, UK
Irene M. Tjiam, Netherlands
Mahmoud Elfar, UK
Jason Y Lee, USA
Kenji Yoshida, Japan
MP03: Robotic/Lap Upper Urinary Tract 1
Stephen Faddegon, USA
Kurdo Barwari, Netherlands
Phillip M. Pierorazio, USA
Kurdo Barwari, Netherlands
Eric Barret, France
DA Payne, UK
Sashi S. Kommu, UK
Changjun Yin, China
Mohammed Haseebuddin, USA
Hitoshi Yanaihara, Japan
Ken Morita, Japan
Phillip M. Pierorazio, USA
Huang Yi, China
Huang Yi, China
Brian M. Benway, USA
Jeffrey K. Mullins, USA
Kwang T Kim, Korea
TETSUO FUJITA
Tae Hyo Kim
MP04: BPH laser 1
raman mehrzad, Sweden
Hoon Choi, Korea
raman mehrzad, Sweden
Christian Beck, Germany
Ming F Jiang, China
Kurt H Strom, USA
Motoo Araki, Japan
Steve W.H. Chan, Hong Kong
Motoo Araki, Japan
Hidekazu Yamamoto, UK
Alexander Bachmann, Switzerland
Malte Rieken, Switzerland
Alejandro Gonzalez, Mexico
Amanda S. J. Chung, Australia
Amanda S. J. Chung, Australia
Renu Eapen, Australia
Stavros Gravas, Greece
Ferdinando De Marco, Italy
Ming-Chak Lee, Australia
Malte Rieken, Switzerland
MP05: Urolithiasis 1
Aaron Woodall
Kyle Wood, USA
Mukul B. Patil, USA
Ming-Chak Lee, Australia
Thomas Knoll, Germany
Ben_H Chew, Canada
Stephania Olamendi, USA
Joseph Graversen, USA
Kyle Wood, USA
Luck Hee Sung, Korea
Jairam R. Eswara, USA
Jessica A Mandeville, USA
Mohummad Siddiqui, USA
Kyle Wood, USA
Kyle Wood, USA
Senthy V Sellaturay, UK
Thiruneelakandasivam Suntharasivam, UK
Mohummad Minhaj Siddiqui, USA
Ashok K. Hemal, USA
MP06: Robotic/Lap Upper Urinary Tract 2
Steven K. Huan, Taiwan, China
Akbar Nouralizadeh, Iran
Ashok K. Hemal, USA
Rahul J Sinha, India
Bruce L. Jacobs, USA
Ashok K Hemal, USA
Ashok K. Hemal, USA
Aniruddha Chakravarti, UK
Bakhman G. Guliev, Russia
MASATSUGU IWAMURA
Boris K. Komyakov, Russia
Chia-Da Lin, Taiwan, China
Panagiotis Kallidonis, Greece
Stephen Faddegon, USA
Tadahiro Isoyama, Japan
Steven M Lucas, USA
Vishwajeet Singh, India
Manar M Malki, UK
MP07: Less/Notes 2
Damien L. Smith, USA
Damien L. Smith, USA
ERNESTO III V. ARADA, Philippines
Chang Wook Jeong, Korea
ERNESTO III V. ARADA, Philippines
SHOGO INOUE
Xiaofeng Zou, China
Xiaofeng Zou, China
MASAYOSHI MIURA
Yoshio Sugino, Japan
Masaru Ogasawara, Japan
Sompol Permpongkosol, Thailand
Yeh Hong Tan, Singapore
Svetozar Subotic, Switzerland
YASUYUKI NAITOH, Japan
Ephrem O. Olweny, USA
MP08: Robotic/Lap Prostate 1
Kevin C. Zorn, Canada
Cheng-Che Chen, Taiwan, China
Eric Barret, France
Nishant Mishra, USA
Liu YuQing, China
Gregory Jack, Australia
Nadim Douaihy, Switzerland
Abhinav Khanna
Ryan Novak, MD, PharmD, USA
Eric Barret, France
Motoo Araki, Japan
Isaac Yi Kim, USA
Selcuk M Keskin, Turkey
Jennifer Yates, USA
David Albala, USA
David Albala, USA
MP09: New Technology/Imaging 1
John Lazarus, South Africa
John Lazarus
Jonathan K Makanjuola, UK
David A Rebuck, USA
Phillip M. Pierorazio, USA
Phillip M. Pierorazio, USA
Mohamed I Abdulmajed, UK
Nabi Ghulam, UK
Elias S. Hyams, USA
Davis P. Viprakasit, USA
Richard Johnston, UK
Bhaskar K Somani, UK
Kazutoshi Okubo, Japan
Sutchin R Patel, USA
Sutchin R. Patel, USA
Mohamad W. Salkini, USA
G. Zelichenko, Israel
MP10: Urolithiasis 2
Nadav Berkovitz, Israel
Bodo Knudsen, USA
Tracy P. Marien, USA
HITOSHI YAMADA, Japan
Brian R. Matlaga, USA
Brian R. Matlaga, USA
Milad A Hanna, UK
Bannakij Lojanapiwat, Thailand
Jangho Yoon, Korea
Abdulkader Alobaidy, Qatar
Abhijith D. Mally, USA
Shashikant mishra, India
Sung Yong Cho, Korea
Deok Hyun Han, Korea
MP11: Robotic/Lap Upper Urinary Tract 3 (Donor Nephrectomy)
Nasser I. Simforoosh, Iran
Kazuya Omoto
Jianfei Ye, China
Mohamed Etafy, USA
Steven M Lucas, USA
Steven M Lucas, USA
NAOHIKO FUKAMI
Nasser I. Simforoosh, Iran
Ashok K. Hemal, USA
Dan Magrill, UK
Jianfei Ye, China
Jianfei Ye, China
Milan Hora, Czech Republic
Qing_X Wang, China
Sapan Ambani, USA
Sashi S. Kommu, UK
MP12: Less/Notes 3
Bhaskar K. Somani, UK
Thomas Y. Hsueh, Taiwan, China
Zhang ShuDong, China
S Jeff Chueh, USA
Meng S Lim, Korea
Evangelos Liatsikos, Greece
Evangelos Liatsikos, Greece
Judy M. Choi, USA
Panagiotis Kallidonis, Greece
Fuminori Sato, Japan
S Jeff Chueh, USA
TAKAMITSU INOUE
Judy M. Choi, USA
Judy M. Choi, USA
Yong H Park, Korea
MP13: Robotic/Lap Prostate 2
Enrique Rijo
Johannes Hauser, Switzerland
Daniel T. Pucheril, USA
Ronald Cadillo-Chavez, USA
Hidefumi Kinoshita, Japan
Kyoko Sakamoto, USA
Mahmoud A. Abdel Hakim, Egypt
Kevin C. Zorn, Canada
Cassio Andreoni, Brazil
Yen-chuan Ou, Taiwan, China
Donna Owen, NP, USA
Ronney Abaza, USA
Humberto Martinez-Suarez, USA
Wisoot Kongchareonsombat, Thailand
Keisuke Hieda, Japan
Milos Brodak, Czech Republic
MP14: New Technology/Imaging 2
Jeffrey K. Mullins, USA
Qing_X Wang, China
Qing_X Wang, China
Matthias Franke, Denmark
Ravi Kulkarni, UK
Bong Hee Park, Korea
Damien L. Smith, USA
Myungchan Park, Korea
Joseph E. Fargusson, USA
Jonathan P. Heldt, USA
barbara c. gentile, Italy
Elias S. Hyams, USA
YASUO KAWANISHI, Japan
David M Albala, USA
Diana C Londoño, USA
Manickam Ramalingam, India
Peter J Gilling, New Zealand
Peter J Gilling, New Zealand
MP15: Prostate, Minimally Invasive Therapy/New Technology/Imaging 1
Christian_G Chaussy, Germany
Christian_G Chaussy, Germany
Roland F van Velthoven, Belgium
TOSHIYUKI CHINA
Stefan_FM Thueroff, Germany
Eric Barret, France
Toyoaki Uchida, Japan
MITSUHIRO SEKI, Japan
Giuseppe Simone, Italy
Eric Barret, France
Andre L. C. Abreu, USA
Kae Jack Tay, Singapore
George R. Schade, USA
Oleg V. Teodorovich
Nicholas R. Styn, USA
Agnes J. Wang, USA
MP16: Robotic/Lap Upper Urinary Tract 4
Ravi Munver, USA
Ravi Munver, USA
Fumiya Hongo
Jianfei Ye, China
Patricia J. Zondervan, Netherlands
Steven K. Huan, Taiwan, China
JIRO MACHIDA, Japan
Bhaskar K. Somani, UK
Elias S. Hyams, USA
Benjamin Lee, USA
Ilter Tufek, Turkey
Kenneth M Jacobsohn, USA
Ketul Shah, USA
Louis S Krane, USA
Louis S Krane, USA
Andre L. C. Abreu, USA
Ravi Munver, USA
MP17: Robotic/Lap Prostate 3
Kipp D. Voth, USA
Shahrokh F. Shariat, USA
Julien Renard, Switzerland
Dennis Gyomber, Australia
Allen Chang, USA
Gregory S Jack, Australia
Phillip M. Pierorazio, USA
Jeffrey Wilson, USA
Daniel T Pucheril, USA
Samuel H. Eaton, USA
Kelly A. Healy, USA
TAKAHIRO A. MRUYAMA
Sanket Chauhan, USA
Sanket Chauhan, USA
Sanket Chauhan, USA
MP18: PNL 1
wang yanbo, China
wang yanbo, China
Ming F Jiang, China
Ming F Jiang, China
ABDULKADER ALOBAIDY, Qatar
Mamun S Mahmud, Pakistan
Mario Sofer, Israel
Agnes J. Wang, USA
Agnes J. Wang, USA
Mario Sofer
Herman Fernando, UK
Kathryn F. Rzetelski-West, Australia
Razvan Multescu, Romania
Khaled Shahrour, USA
Samih Al-Hayek, USA
Khaled Shahrour, USA
Wen Zhong, China
Wen Zhong, China
MP19: Ureteroscopy 1
Bodo Knudsen, USA
zhihua Lu, China
W Finch, UK
Kelly A. Healy, USA
Joseph A. Graversen, USA
William J Finch, UK
roberto giulianelli, Italy
Jinsung Park, Korea
Liu YuQing, China
John M. Hollingsworth, USA
Julie M. Riley, USA
RavindraB Sabnis, India
Julie M. Riley, USA
Remzi Saglam, Turkey
roberto giulianelli, Italy
Guido Giusti, Italy
zhihua Lu, China
MP20: Less/Notes 4
Jae Hoon Chung, Korea
Stefan_FM Thueroff, Germany
Gang Zhu, China
Abai Xu, China
GAO XIN, China
Ma Lulin
Abai Xu, China
Dong Hyuk Kang, Korea
Changjun Yin, China
Toru Harabayashi
Vishwajeet Singh, India
HIDEO YUKI
Wahib E Isac, USA
BLAKE W MOORE, USA
Sanjeev Mehrotra, India
Granville L. Lloyd, USA
Abai Xu, China
MP21: Kidney, Urinary Tract, Endurology/New Technology
Xiao ChunLei, China
Paolo Puppo, Italy
Paolo Puppo, Italy
Vladimir Mouraviev, USA
KYOKO SAKAMOTO, USA
Jennifer K. Yates, USA
Ahmed Ghazi, USA
Seshadri Sriprasad, UK
Jennifer K Yates, USA
Jaime Tisnado, USA
Jaime Tisnado, USA
Sutchin R. Patel, USA
Cervando Ortiz, USA
Gabriel T. Schroeder, USA
Jairam R. Eswara, USA
Yung K Tan, USA
MP22: Transurethral Surgery Prostate and Baladder
John M. Hollingsworth, USA
John M. Hollingsworth, USA
Andreas Skolarikos
fernando rodriguez, Spain
Mohamed I Abdulmajed, UK
George R. Schade, USA
YOSHIKATSU NOJIRI, Japan
Anup Vora
Bogdan Geavlete, Romania
Heng-Jun Xiao, China
Bogdan Geavlete, Romania
Rajendra Nerli, India
Ponnambalam Chandrasekar, UK
Roberto Giulianelli, Italy
Bogdan Geavlete, Romania
Yuchuan Hou, China
wang yanbo, China
wang yanbo, China
MP23: PNL 2
Jorge Gutierrez, Mexico
Wei Xue, China
wang yanbo, China
wang yanbo, China
wang yanbo, China
wang chunxi, China
Mohammad M. Hosseini, Iran
Ming F Jiang, China
Brian Duty, USA
Joshua D. Wiesenthal, Canada
Zhou Xiangfu, China
Guido Giusti, Italy
Ada T NG, Hong Kong
Jan P. Jessen, Germany
Liu YuQing, China
Liu YuQing, China
Brian Duty, USA
Jan P. Jessen, Germany
MP24: SWL
Roberto Giulianelli, Italy
Dong Hoon Yoo
Gregory S Jack, Australia
Brian M. Benway, USA
R John D'A Honey, Canada
TORU SUGIHARA, Japan
Palle J. Osther, Denmark
Geert G. Tailly, Belgium
Michael Ordon, Canada
Mohamed Elkoushy, Canada
Maria Chiara Sighinolfi, Italy
Faqar Anjum, UK
Milad A Hanna, UK
Milad A Hanna, UK
Brian M. Benway, USA
Hyun Tae Kim
MP25: Female Urology/Pediatrics
Manickam Ramalingam, India
Sachiko Hongoh, Japan
Judy M Choi, USA
Judy M. Choi, USA
Bishoy A Gayed, USA
Yigit AKIN, Turkey
Paul Kokorowski, USA
Ramin Haghighi, Iran
Yoshiyuki Kojima, Japan
Svetozar Subotic, Switzerland
Eric D. Nelson, USA
Douglas E. Coplen, USA
Achim Lusch, USA
ramin haghighi, Iran
BARBARA C. B.C. GENTILE, Italy
Mitsuru Kajiwara
HIKARU TOMOE
MP26: Robotic/Lap Upper Urinary Tract 5
Mahmoud A. Abdel Hakim, Egypt
Shashikant Mishra, India
Rocco Papalia, Italy
HIDEO SAITO, Japan
Ephrem O. Olweny, USA
Rocco Papalia, Italy
Craig Rogers, USA
RYOICHI SHIROKI
Judy M. Choi, USA
Judy M. Choi, USA
Jong Jin Oh, Korea
Jong Jin Oh, Korea
Ke Liu, China
Ronald Cadillo-Chavez, USA
Ronald Cadillo-Chavez, USA
Wahib E Isac, USA
MP27: Adrenal
Alireza Aminsharifi, Iran
Koji Shiraishi, Japan
Changjun Yin, China
Christian Schwentner, Germany
Christian Schwentner, Germany
Yuchuan Hou, China
Shigeto Ishidoya, Japan
Rajendra Nerli, India
Elias S. Hyams, USA
Eduardo C. Landerer, Chile
Eduardo C. Landerer, Chile
TAKANOBU UTSUMI
TAKAYUKI KAMIGAITO
SEIYA HATTORI, Japan
Liu YuQing, China
OSAMU ISHIZUKA
MP28: Robotic/Lap Prostate 4
Catherine J. Chen, USA
Thomas Ahlering, USA
Ronald Cadillo-Chavez, USA
Oscar Schatloff, USA
Oscar Schatloff, USA
Oscar Schatloff, USA
Isaac Yi Kim, USA
Ravi Munver, USA
Sashi S. Kommu, UK
Zhang Fan
YOICHI MIZUTANI
Hidekazu Inui, Japan
MOTOTSUGU MURAMAKI
Ahmed Ghazi, USA
Xavier Hurtes, France
Motoo Araki, Japan
GAO XIN, China
Hideo Fukuhara, Japan
MP29: Ureter/Urothelial Cancer
Ben_H Chew, Canada
Michael A. Fargusson, USA
Jong-Wook Park, Korea
Gal Keren-Paz, Israel
Bakhman G. Guliev, Russia
Agnes J. Wang, USA
Ravi Kulkarni, UK
Ravi Kulkarni, UK
Marc L.J.E Paffen, Netherlands
zhihua Lu, China
zhihua Lu, China
ARAKI MOTOO
Chi-rei Yang, Taiwan, China
zhihua Lu, China
William Finch, UK
Xiao Bo, China
MP30: Ureteroscopy 2
Shinsuke Okada, Japan
Petrisor Geavlete, Romania
Faqar Anjum, UK
Xiao ChunLei, China
Ilter Tufek, Turkey
Daisuke Kudo
Ming F Jiang, China
wang yanbo, China
Roberto Giulianelli, Italy
Bhaskar K Somani, UK
Ryan_F Paterson, Canada
Bhaskar K. Somani, UK
Jessica A Mandeville, USA
Wen Zhong, China
Wen Zhong, China
Blake Hamilton, USA
MP31: Robotic/Lap Upper Urinary Tract 6
Steven M Lucas, USA
Cassio Andreoni, Brazil
Tsunenori Kondo, Japan
Cassio Andreoni, Brazil
TSUNENORI KONDO
Cassio Andreoni, Brazil
TOMOYUKI TATENUMA
Sashi S. Kommu, UK
Ketul Shah, USA
Kenneth M Jacobsohn, USA
Takashige Abe, Japan
Satoshi Otsubo
Louis S Krane, USA
Zhang ShuDong, China
Ahmet Tefekli, Turkey
Mohamad Salkini, USA
Tracy P. Marien, USA
MP32: Prostate, Minimally Invasive Therapy/New Technology/Imaging 2
KAZUYOSHI NAKAMURA, Japan
zhihua Lu, China
roberto giulianelli, Italy
Andre L. C. Abreu, USA
Satoru Muto, Japan
Ardeshir R Rastinehad, USA
Prasannah Satisvatam, Australia
zhihua Lu, China
Shoji Koga, Japan
Ponnambalam Chandrasekar, UK
Giuseppe Simone, Italy
Masahiro Inoue, Japan
Matthieu Durand
Mehmet Baykara, Turkey
Humberto Kern Laydner
Phillip Mucksavage, USA
Holger Gerullis, Germany
Holger Gerullis, Germany
MP33: BPH laser 2
Yoichi Kambara, Japan
Yohei Omori, Japan
KEISUKE SAITO
Shinobu Kato, Japan
Jessica A Mandeville, USA
Hidekazu Yamamoto, UK
Lukas Lusuardi, Austria
Jan Peter Jessen, Germany
Lluis Fumado, Spain
Gana Kugathasan, UK
HIROSHI KAMEOKA, Japan
Daisuke Obinata, Japan
TOSHIHIDE SHISHIDO, Japan
MP34: Urolithiasis/PNL/Ureteroscopy
Ravi Kulkarni, UK
Ravi Kulkarni, UK
HIROMASA SAKAMOTO, Japan
Palle J. Osther, Denmark
Khanh K. Nguyen, USA
Hillary J. Wagner, USA
Caleb Nelson, USA
Sutchin R Patel, USA
Damien L. Smith, USA
Behzad Feizzadeh Kerigh
Pavan Aluru, UK
Yuchuan Hou, China
Cheng-Huang Shen, Taiwan, China
Wansuk Kim, Korea
Wen Zhong, China
Alejandro Gonzalez, Mexico
UP01: Unmoderated Poster Session 1
Roberto Giulianelli, Italy
Kun-Lin Hsieh, Taiwan
Insang Hwang, Korea
Kamlesh B. Patel, India
HIROSHI FURUSE, Japan
HIDEHIKO HARA, Japan
AKIHIRO ITO, Japan
MANABU KATO, Japan
Yasuyuki Kobayashi, Japan
MASARU MORI, Japan
GO NAKAGAWA, Japan
KAZUO NISHIMURA, Japan
NOBUFUMI UEDA, Japan
HITOSHI YOKOYAMA, Japan
HIDENORI ZAKOJI, Japan
Elias S. Hyams
Sarfraz Ahmad, UK
Jae Young Choi, Korea
Masayuki Hagiwara, Japan
Naoki Itoh, Japan
Takashi Kasahara, Japan
Wei-Hong LAI, Taiwan
Yu-wei Lai, Taiwan, China
Nor Azhari Bin Mohd Zam, Singapore
Kazuhiko Nishi, Japan
Tae Hee Oh, Korea
Kazuya Omoto, Japan
Kazuya Omoto, Japan
Kazuya Omoto, Japan
Kazuya Omoto, Japan
Sung Hyun Paick, Korea
Ju Tae Seo, Korea
Yosuke Shimizu, Japan
Rahul J Sinha, India
Jhih Cheng Wang, Taiwan
Long Zhang, China
HIDEAKI MIYAKE, Japan
SHINSUKE HAMADA, Japan
TAIJI HAYASHI, Japan
DAISUKE ISHII, Japan
TAKESHI ISHIMURA, Japan
Noriyuki Ito, Japan
TATSUYA IWATA, Japan
NORITAKA KAMIMURA, Japan
TOMOYUKI KATO, Japan
SATORU KIRA, Japan
HIROSHI KITAMURA, Japan
SATOSHI KUROKAWA, Japan
KOJI MITA, Japan
YUKIO NAYA, Japan
MORIHIRO NISHI, Japan
MASAHIRO NOZAWA, Japan
KENJI OMAE, Japan
TAKEHISA ONISHI, Japan
YUJI SATOH, Japan
MIKIO SUGIMOTO, Japan
TOSHIO TAKAGI, Japan
SATOSHI TAMADA, Japan
YOSHIKAZU TSUJI, Japan
KAZUHIKO YOSHIDA, Japan
Byong Chang Jung, Korea
Seong Il Seo
HeeJo Yang, Korea
KOSUKE FUKAYA, Japan
KEITA MINAMI, Japan
YASUHIDE MIYOSHI, Japan
NISHIDA TAKESHI, Japan
Danielle Brooks, USA
Danielle Brooks, USA
Hyuk Jin Cho, Korea
Sung Hoo Hong, Korea
Michael Huang, USA
Gou Kaneko, Japan
Seung Hwan Lee, Korea
Takahiro Maeda, Japan
Sanjeev Mehrotra, India
Sanjay Mohan, USA
Enrique Rijo, Spain
Nusrat Shaikh, USA
Prasanna Sooriakumaran, USA
Abhishek Srivastava, USA
Chia-Cheng Su, Taiwan
Anup Vora, USA
Yota Yasumizu, Japan
RYOSUKE ANDO, Japan
MASAYUKI EGAWA, Japan
TAKESHI INAGAKI, Japan
Teruo Inamoto, Japan
AKIRA IRIE, Japan
KEIICHI ITO, Japan
KAZUMI KAMOI, Japan
SHINJI KUROSAKA, Japan
KOJI MITA, Japan
DAISUKE NAGATA, Japan
YUZO NAKANO, Japan
KENICHI TABATA, Japan
KIYOSHI TAKAHARA, Japan
WATARU TAKAHASHI, Japan
HIDEKAZU TAKIUCHI, Japan
KAZUSHI TANAKA, Japan
KEIICHI TOZAWA, Japan
NOBUO TSURU, Japan
SHINICHIRO WATANABE, Japan
TORU INOUE, Japan
NORIYASU KAWAI, Japan
Leonard S. Chuech, Taiwan
S Jeff Chueh, USA
YUTAKA FUJISUE, Japan
TETSUYA IMAO, Japan
Humberto Kern Laydner, USA
Akira Miyajima, Japan
TETSUO NOZAKI, Japan
Seng-Chen Wen, Taiwan
Late Breaking
MITSUHIRO SEKI, Japan
UP02: Unmoderated Poster Session 2
Shaobo Zheng, China
Lluis Fumado, Spain
Ji Lu
Luck Hee Sung, Korea
wang yanbo, China
aliasghar yarmohamadi, Iran
aliasghar yarmohamadi, Iran
MASATO DOBASHI, Japan
TAKAHIRO HARAGUCHI, Japan
Kenji Kawamura, Japan
SHIGEMASA KUDO, Japan
Minori Matsumoto, Japan
Roberto Giulianelli, Italy
hassan ahmadnia
Qihui Chen
Qihui Chen
Toru Kimura, Japan
Dong Hoon Lee, Korea
Jae Sung Lim, Korea
Subhasis Sengupta, UK
Kisik Shim, South Korea
Oleg V. Teodorovich, Russia
SHINGO MINAGAWA, Japan
HIROSHI IKEDA, Japan
KANYA KAGA, Japan
SEIICHI SAITO, Japan
TOSHIYA SHITARA, Japan
HIDEYASU TSUMURA, Japan
Ming-Chak Lee, Australia
Qihui Chen
Qihui Chen
Yii-Her Chou, Taiwan
janet colli, USA
Mantu Gupta, USA
Yoshiyuki Ishiura
Yeong-Chin Jou, Taiwan
Ryoichi Nakanishi, Japan
Sangtae Park, USA
Gauthier Raynal, France
Kisik Shim, Korea
Sergey Tadtayev, UK
Oleg V. Teodorovich, Russia
Cole W. Wootton, USA
NAOSHI ITAYA, Japan
Hiroki Ito, Japan
HIROAKI KAKINOKI, Japan
TORU KANNO, Japan
Takashi Kawahara, Japan
YASUHIRO NISHIYAMA, Japan
Satoshi Nishizawa, Japan
AKITAKA SUZUKI, Japan
MITSUHIRO TAMBO, Japan
Wai Man Chow, UK
Seok Heun Jang, Korea
Elea Monteferrante, UK
Jin Kyu Oh
Bongsuk Shim, Korea
Kazunori Haga, Japan
OSAMU ICHIYANAGI, Japan
AYUMU MATSUDA, Japan
KATSUTOSHI UEMATSU, Japan
Sri Sivalingam
Gyungtak (Mario) Sung, Korea
Wen Zhong, China
Mohsen Amjadi, Iran
Leonard S. Chuech, Taiwan
Ji Lu
Hiroya Mizusawa, Japan
Stanislav A. Naryshkin, Russia
Hao Zhang
Chuk M. Won, Australia
Taro Iguchi, Japan
Hassan Ahmadnia, Iran
Omar M Aboumarzouk, UK
Qihui Chen
Junichi Inokuchi, France
Ji Lu
Ji Lu
Sachin Malde, UK
Muhammad Moazzam, UK
GAUTHIER RAYNAL, France
Taimur T shah, UK
SHOHEI ISHIDA, Japan
SOJUN KANAMARU, Japan
RYOICHI MATSUO, Japan
JUNICHI MATSUZAKI, Japan
JUN MORITA, Japan
MASAO NAGATA, Japan
KIKUO NUTAHARA, Japan
KIYOTAKA OKA, Japan
RYOJI TAKAZAWA, Japan
HIDEYUKI TERAO, Japan
aliasghar yarmohamadi, Iran
Mitsuru Kajiwara, Japan
Mitsuru Kajiwara, Japan
Rajendra Nerli, India
ATSUSHI HAMANO, Japan
KENTARO MIZUNO, Japan
KIMIHIKO MORIYA, Japan
Omar M Aboumarzouk, UK
Sarfraz Ahmad, UK
Christian_G Chaussy, Germany
Wai Man Chow, UK
Joseph Graversen, USA
TH Karaolidis, Greece
Sachin Malde, UK
TERUO INAMOTO, Japan
YOSHIMASA JO, Japan
TERUYUKI OGAWA, Japan
MASAFUMI OYAMA, Japan
NORIHITO SOGA, Japan
Anup Vora, USA
Anup Vora, USA
Kazuyoshi Izumi, Japan
Tarik Esen, Turkey
nicha piyasoontrawong, Thailand
Leticia Ruiz, Panama
NORITAKA ISHITO, Japan
TAKUMA KATO, Japan
Yoshiyuki Matsui, Japan
YOSHIYUKI SHIGA, Japan
Dong Hyuk Kang, Korea
Jae Hoon Chung, Korea
Sangtae Park, USA
Sangtae Park, USA
Sangtae Park, USA
Fatih Altunrende, USA
Fatih Altunrende, USA
VP01: Robotic/Lap Bladder/Less/Notes
Gianmarco Isgro', Italy
Ken Nakagawa, Japan
Ronney Abaza, USA
Jeffrey P Wolters, USA
Fiona Wu, Singapore
Wing Hang Au, Hong Kong
Vineet Gauhar, Singapore
Sashi S. Kommu, UK
Takeshi Iida, Japan
Yao-Chou Tsai, Taiwan, China
BLAKE W MOORE, USA
Abai Xu, China
Jeffrey Woldrich, USA
Jeffrey Woldrich
Yong H Park, Korea
VP02: Robotic/Lap Adrenal and Kidney
Ahmed Ghazi, USA
Ahmed Ghazi, USA
Amr M. Emara, UK
Chie Onizuka, Japan
Chia-Da Lin, Taiwan, China
Fuminari Hanashima, Japan
Ryoko Sakata, Japan
Naoya Masumori, Japan
Edmund Chiong, Singapore
Narushi Yokota, Japan
Kazushi Tanaka, Japan
Salvatore Micali, Italy
Tracy P. Marien, USA
Bogdan Petrut, Romania
Amr M Emara, UK
Yi-Chia Lin, Taiwan, China
VP03: Prostate Diagnosis/Urotherial Cancer/Education
Sashi S. Kommu, UK
Sashi S. Kommu, UK
Jason Y Lee, USA
Kenji Yoshida, Japan
Robert M. Sweet, USA
Bogdan Petrut, Romania
Sashi S. Kommu, UK
Misop Han, USA
Ardeshir R Rastinehad, USA
Vladimir Mouraviev, USA
Saeed M Al-Qahtani, France
Bogdan Geavlete, Romania
Bogdan Geavlete, Romania
Jan P. Jessen, Germany
Mariaconsiglia Ferriero, Italy
VP04: Urolithiasis
Christian Bohris, Germany
Agnes J. Wang, USA
Hoang Duc David Nguyen, Vietnam
Yew-Lam Chong, Singapore
takahiko kobayashi, Japan
Raghuram Devarajan, UK
Shashikant Mishra, India
Steve K. Williams, USA
Viorel Bucuras, Romania
Francisco P. Daels, Argentina
YASUO KOHJIMOTO, Japan
remzi saglam, Turkey
Saeed M Al-Qahtani, France
Saeed M Al-Qahtani, France
RavindraB Sabnis, India
Roos Stuurman, France
VP05: Robotic/Lap/TUR Prostate
Chang Wook Jeong, Korea
Kevin C. Zorn, Canada
Abai Xu, China
Takahiro Yasui, Japan
Saeed M Al-Qahtani, France
Kazushi Tanaka, Japan
Vineet Gauhar, Singapore
Johannes Hauser, Switzerland
Amanda S. J. Chung, Australia
ERNESTO III V. ARADA, Philippines
HOANG DUC NGUYEN DAVID, Vietnam
Toshiya Shitara, Japan
Nouval Shahab, Japan
Anil Kumar Varshney, India
Anil Kumar Varshney, India
Kevin C. Zorn, Canada
VP06: Imaging/New Technology/Pediatrics
Yasushi Yoshino, Japan
Aaron P. Bayne, USA
Florin Nechita, Romania
Heng-Jun Xiao, China
Derya Tilki, Germany
Thmoas Knoll, Germany
Sashi S. Kommu, UK
Paolo Puppo, Italy
Hora Milan, Czech Republic
Phillip M. Pierorazio, USA
Shigeji Matsubara, Japan
Sashi S. Kommu, UK
Craig Rogers, USA
Sashi S. Kommu, UK
Hiroaki Aoki, Japan
Agnes J. Wang, USA
VS01: Laparoscopic Partial Nephrectomy
Federico Escobar Jaramillo, Colombia
Giuseppe Simone, Italy
Giuseppe Simone, Italy
Rocco Papalia, Italy
Juan A. Peña, Spain
Jorge Rioja, Spain
Taek Sang Kim, Korea
Rajesh K Ahlawat, India
Juan A. Peña, Spain
Juan A. Peña, Spain
VS02: Robotic Partial Nephrectomy
Nicholas P Vaughn, USA
Osamu Ukimura, USA
Philip J Dorsey, Jr., USA
Andre L. C. Abreu, USA
Craig G. Rogers, USA
Praneeth Vemulapalli, USA
Amr M Emara, UK
Ramakrishna Venkatesh, USA
VS03: Robotic/ Laparoscopic Prostate Surgery 1
Nobuyuki Hinata, Japan
Rene Sotelo, Venezuela
rene sotelo, Venezuela
Sanket Chauhan, USA
Oscar Schatloff, USA
Bogdan B Petrut, Romania
Hidetoshi Akita, Japan
Ahmed Ghazi, USA
VS04: Notes/Less 1
Chi Fai Kan, Hong Kong
Mahmoud A. Abdel Hakim, Egypt
Lance J. Hampton, USA
Mahmoud A. Abdel Hakim, Egypt
Mahmoud A. Abdel Hakim, Egypt
Rene Sotelo, Venezuela
Mahmoud A. Abdel Hakim, Egypt
VS05: Adrenal/Upper Urinary Tract
Manickam Ramalingam, India
Federico Escobar Jaramillo, Colombia
Ali-Asghar Zhumkhawala, USA
Kazuhiro Araki, Japan
Ataru Sazawa, Japan
Pietro Cozzupoli, Italy
CARLOS GONZALEZ-SATUE, Spain
Hitoshi Yanaihara, Japan
Mohammad Aslzare, Iran
VS06: Robotic /Laparoscopic Upper Urinary Tract Surgery 1
Mohammad Aslzare, Iran
Rajesh K. Ahlawat, India
Kamlesh B. Patel, India
Wendy Padilla, USA
Manickam Ramalingam, India
Manickam Ramalingam, India
Amr M Emara, UK
VS07: BPH,TUR,Female Urology
Shinobu Kato, Japan
Astushi Yoshimizu, Japan
Kurt H Strom, USA
Ming-Ying Yu, Taiwan, China
Caroline C. Carera, Switzerland
Federico Escobar Jaramillo, Colombia
Federico Escobar Jaramillo, Colombia
Nasser I. Simforoosh, Iran
VS08: Robotic /Laparoscopic Upper Urinary Tract Surgery 2
Benjamin R. Lee, USA
Jason Y Lee, USA
Juan A. Peña, Spain
Wendy Padilla, USA
Nicholas P Vaughn, USA
Ali Riza Kural, Turkey
VS09: Robotic/ Laparoscopic Prostate Surgery 2
John W. Davis, USA
Ali Riza Kural, Turkey
Federico Escobar Jaramillo, Colombia
Keita Takimoto, Japan
Gene O. Huang, USA
Juan A. Peña, Spain
Lance J. Hampton, USA
Enrique Rijo, Spain
VS10: Ureteroscopy / Endourology
Brian Duty, USA
Agnes J. Wang, USA
Gene O. Huang, USA
Carl Sarkissian, USA
Guido Giusti, Italy
olivier Traxer, France
Husain alenezi, Saudi Arabia
Kelly A. Healy, USA
Iqbal Shergill, UK
Kelly A. Healy, USA
VS11: Laparoscopic / Robotic Bladder Surgery
Rene Sotelo, Venezuela
Premsant Sangkum, Thailand
Bogdan B Petrut, Romania
manickam Ramalingam, India
Sarfraz Ahmad, UK
Manickam Ramalingam, India
Manickam Ramalingam, India
Shigehiro Soh, Japan
Sarfraz Ahmad, UK
Rene Sotelo, Venezuela
VS12: Notes/Less 2
Takeshi Sano, Japan
Xiaofeng Zou, China
Rihai Xiao, China
Sompol Permpongkosol, Thailand
Sompol Permpongkosol, Thailand
Chang Wook Jeong, Korea
Chang Wook Jeong, Korea
Gianmarco Isgro', Italy
VS13: Robotic /Laparoscopic Upper Urinary Tract Surgery 3
Rene Sotelo, Venezuela
Rajesh K Ahlawat, India
Agnes J. Wang, USA
Amr M Emara, UK
Oscar Schatloff, USA
Dmitry Perlin, Russia
Sung Yul Park, Korea
VS14: Pediatric Surgery/New Technology
Eric D Nelson, USA
Osamu Ukimura, USA
Masahiko Nakamoto, USA
Abbas Basiri, Iran
Stephen S. Yang, Taiwan, China
Judy M. Choi, USA
Bogdan B Petrut, Romania
Rakesh Khanna, USA
Kanji Nagahama, Japan
Juan A. Peña, Spain
VS15: Percutaneous Surgery
Shashikant Mishra, India
John Lazarus, South Africa
Yujiro Ito, Japan
James Borin, USA
Ho Man Tam, Hong Kong
Brian Duty, USA
David Hoenig, USA
Abbas Basiri, Iran
VS16: Robotic / Laparoscopic Pelvic Surgery
Manickam Ramalingam, India
Federico Escobar Jaramillo, Colombia
ahmed ghazi, USA
Mahmoud A. Abdel Hakim, Egypt
Johannes M. Hauser, Switzerland
Ali Riza Kural, Turkey
Ali Riza Kural, Turkey
Ravi Munver, USA
Razvan Multescu, Romania
VS17: Notes/Less 3
Jennifer Yates, USA
Tsai Yao-Chou, Taiwan, China
Xiaofeng Zou, China
Xiaofeng Zou, China
Xiaofeng Zou, China
Marek Roslan, Poland
Guoxi Zhang, China
Matthias Walter, Switzerland
BR01: Basic, New Technology
Department of Urology, University Hospital of Wales, Cardiff, UK
Introduction: There is a need for a reliable model for determining the permeation of therapeutic agents across urothelium in order to better predict in vivo intra-luminal drug delivery. Purpose:To develop An ex vivo model, (Franz diffusion cell type), to allow the relative permeation of a number of therapeutic agents across porcine bladder to be determined. Methods:Full thickness porcine bladder or excised porcine urothelium was mounted in a Franz diffusion cell and a formulation containing the therapeutic entity of interest applied to the donor chamber (basal side of the tissue). By sampling the receptor phase over a pre-defined period, the rate of permeation across the tissue could be determined. The tissue was also extracted to further understand the distribution of the drug in the model system. The viability of the tissue over the course of the experiment was evaluated in an assay investigating the co-permeation of a paracellular (sodium fluorescein) and a transcellular (propranolol hydrochloride) marker. Results:Permeation coefficients and tissue concentrations for a number of systems have been calculated based on assays performed using the Franz diffusion cell model. It was concluded that the barrier function of the urothelium remained viable over the course of the study since the relative permeation of the two markers remained unaltered. Conclusion:We describe the development of a model that will be useful in determining tissue concentrations achievable from clinically relevant dosage regimes. We expect it to aid in the development of sophisticated techniques for the controlled intraluminal drug delivery.
Department of Urology, University of Patras, Greece
Introduction: Parstatin, is a 41 amino-acid peptide that is cleaved from the proteinase-activated receptor-1 (PAR-1) during its activation by thrombin. Parstatin as well as its hydrophobic N-terminal part (parstatin 1-26) demonstrate cardioprotective properties in experimental models. Purpose: whether parastatin and parstatin1-26 attenuate renal ischemia reperfusion injury (RIRI) in a rat model.Methods: 106 male Wistar rats were examined. RIRI model included 45 minutes of bilateral renal ischemia, followed by 4 hours of reperfusion. The effects of Parstatin on RIRI were initially examined in 77 animals divided into 8 groups including sham (no ischemia), sham/parstatin (parstatin/no ischemia), control (vehicle pretreatment/ischemia), parstatin (pretreatment with 3, 10, 30 or 100μg/Kg parstatin/ischemia), scramble (pretreatment with a non-parstatin 41 aminoacid peptide/ischemia) and after (ischemia/administration of 30μg/Kg parstatin after ischemia). The effects of parstatin 1-26 were examined in 29 animals divided into 5 groups, including control (vehicle/ischemia), parstatin1-26 (pretreatment with 1, 10 or 100μg/Kg parstatin1-26/ischemia) and after (ischemia/administration of 10μg/Kg parstatin1-26 after ischemia). At the end of reperfusion period all animals were sacrificed and kidneys, urine and blood samples were examined for serum creatinine and BUN levels, Fractional Excretion of Sodium (FENa) and histopathology.Results: Administration of 10 or 30μg/Kg of parstatin before or 30μg/Kg after renal ischemia attenuated RIRI. Pretreatment with 10μg/Kg of parstatin1-26 attenuated RIRI as well. Conclusions: Parstatin and parstatin1-26 can preserve renal function in RIRI. A potential role of this molecule in clinical entities related to the phenomenon of RIRI is implied.
In-Vitro Assessment of Retropulsion and Fragmentation of Two Stand Alone, Handheld Lithotripsy Devices
Introduction: Probe velocity / displacement, retropulsion and fragmentation characteristics of the electromechanically driven EMS LithoBreaker and of the CO2 cartridge driven LMA Stonebreaker were compared. Material and Methods: Probe velocities and displacements were measured using high-speed photography. Retropulsion testing was conducted in an underwater set-up. The probes were projected against a led mass (0.98 g) placed in a 15 Fr horizontally mounted silicone tube. Retropulsion was determined by measuring the distance the mass was displaced. Fragmentation efficiency was assessed by measuring the number of shots required to break Bego Stone phantoms placed on a metal mesh into fragments smaller than 3 mm. Mean and standard deviation were computed for all groups and statistical analysis was performed (students t-test). Results: The Stonebreaker yielded the highest velocity of 22m/sec. followed by the LithoBreaker assembled with the hard probe guide of 14.1m/sec and the soft probe guide of 9.9m/sec. The maximum probe displacement for the Stonebreaker was 1.04mm and for the LithoBreaker 0.9mm versus 1.12mm (hard versus soft probe guide). The amount of shots for fragmentation was significantly higher for the LithoBreaker with hard probe guide with mean 21.5±5.29 and soft probe guide with mean 31.1±11.31 compared to the Stonebreaker with mean 11.2±2.65 for the softer Bego Stones, showing similar statistically significant results for the harder Bego Stones Conclusion: The LithoBreaker and the Stonebreaker produced comparable amounts of retropulsion and fragmentation of stone phantoms. The fragmentation characteristics of the mechanical lithotripter improved with the hardness of the probe support.
University of Texas Southwestern Medical Center
Introduction We developed a prototype magnetic tool for ureteroscopic extraction of magnetized stone particles and compared the efficiency of retrieval of magnetized COM stone particles with this prototype magnetic instrument vs. a conventional nitinol basket using a bench-top ureteroscopic simulator. Materials and Methods Human COM stones sized 1-1.5mm, 1.5-2mm and 2-2.5mm were successfully bound to iron oxide microparticles using previously described methodology. Several fragments of each size were implanted into the collecting system of a bench-top ureteroscopic simulator (Limbs & Things, Bristol, UK), and timed stone extraction (5 minute trials) was performed for each fragment size using either a backloaded 8F magnetic tool mounted on a 0.038-inch guidewire or a conventional basket. Median number of fragments retrieved per timed trial was compared for magnetic tool vs. basket using the Mann-Whitney U test.Results For 1-1.5mm fragments, median number of fragments retrieved was significantly higher for the prototype magnetic tool vs. the nitinol basket (9.5 vs. 3.5; p=0.03). For 1.5-2mm there was improvement but not statistically significant (9.5 vs. 4.5; p=0.19) and for 2-2.5mm fragments, median number of fragments retrieved was similar for each tool (6 vs. 6; p=1.0).Conclusion The use of prototype magnetic tools improved efficiency of retrieval of superparamagnetic stone particles sized less than 1.5mm. The magnetic tool profile decreased visibility more than the basket. With further development, this system has the potential to reduce retained residual fragments after ureteroscopic lithotripsy.
Division of Artificial System Science, Graduate School of Engineering, Chiba University, Chiba, Japan
Introduction: Laparoscopic surgeries, single port surgeries and NOTES are evolving to reduce the port. In this setting, small camera is considered to be advantageous to share restricted cavity of the access. In general, small cameras are assumed to have some drawbacks such as narrow and small view field and lack of depth cue, as well as its cost. We tested recently developed small camera and 2D-3D converting software whether it would be candidate for laparoscopic surgeries.Materials and Methods: A 3 mm sized camera system, PicoEndo, is kindly provided by Stevrin&Partners (Blekinge, Sweden). The camera, covering 120 degree of view field, captures video image with 160K pixels of resolution, and connected to PC directly without processor. 2D-3D converting software was developed to calculate distance between camera and the object from intensity of pixels, and then rotates the virtual 3D images to display two images with parallax in the 3D display. Five subjects had performed five-time rope passing test and five-pin drop test under 2D and 3D vision, and measured time for completion.Results: All five subjects had completed the tasks. In rope passing test and pin drop test, it took 1.3 and 1.1 minutes for 2D and 2.3 and 2.0 minutes for 3D vision, respectively. In 3D image, time-lag and motion blur are rather severe.Conclusions: Surgical maneuvering using small camera is feasible. 3D vision using monocular camera and software is also feasible, however, requires PC with high performance of processing.
King's College London University, London, United Kingdom
Introduction: Operating theatres are costly resources within healthcare systems where patient safety is paramount. The Productive Operating Theatre (TPOT) is a module based programme, designed by the National Health Service (NHS), to increase safety and efficiency of operating theatres. It aims to run the perfect operating list with improved team working, organisation, and safety; through multidisciplinary team meetings, checklists and briefings/debriefings.
Purpose: The aim of this comparative study was to evaluate improvements in efficiency by measuring time and cost savings before and after the introduction of TPOT in Urology operating theatres in Guys Hospital, London, UK.
Materials and Methods: TPOT was introduced in Urology operating theatres in September 2010. Theatre session start time and monthly overrun performance was measured from September 2010 to May 2011, during which 1365 patients underwent surgery. Potential savings in the cost of delay was calculated based on fixed overhead costs.
Results: Theatre session start time was improved with a 16-31% increase in the percentage of operating lists starting on time by 8.30am. Monthly overrun time was reduced by 64-74% from September 2010 (introduction of TPOT) to May 2011. There was a total reduction in monthly cost of delay ranging from 1,125 to 3,795 pounds.
Conclusions: The introduction of TPOT has enhanced efficiency in Urology operating theatres with improved theatre session start time and reduced overrun performance. The study is likely to instigate further research into operating theatre safety and efficiency; with findings being applicable to other high risk specialties.
Department of Urology, Guys Hospital, London, United Kingdom
Introduction: Patient safety in the operating theatre is highly reliant on effective communication and organisation. The Productive Operating Theatre (TPOT) programme has been designed by the National Health Service (NHS) with the aim of running the perfect operating list by improving team working, organisation, and safety.
Purpose: The aim of this study was to evaluate improvements in communication and efficiency following the introduction of TPOT in Urology operating theatres in Guys Hospital, London, UK.
Materials and Methods: Theatre session start time and monthly overrun performance was measured from September 2010 (the introduction of TPOT) to May 2011, during which 1365 patients underwent surgery. A semi-structured questionnaire was distributed to 54 post-operative patients returning for follow up after surgery.
Results: Theatre session start time was improved with a 16-31% increase in the percentage of operating lists starting on time by 8.30am. Monthly overrun time was reduced by 64-74% from September 2010 (introduction of TPOT) to May 2011. There was a total reduction in monthly cost of delay ranging from 1,125 to 3,795 pounds. High level of patient satisfaction was found regarding the quality and safety of care, staff communication with patients, organisation and efficiency.
Conclusions: The introduction of TPOT has improved theatre session start time and reduced overrun performance. There was high patient satisfaction regarding care, communication and organisation. The study is likely to instigate further research into operating theatre safety and efficiency; with findings being applicable to other high risk specialties.
Department of Urology, Guys Hospital, London, United Kingdom
Introduction: Operating theatres are costly resources within healthcare systems where patient safety is highly reliant on effective communication and organisation. The Productive Operating Theatre (TPOT) has been designed by the National Health Service (NHS) to increase safety and efficiency of operating theatres. It aims to run the perfect operating list with improved team working, organisation, and safety; via use of multidisciplinary team meetings, checklists and briefings/debriefings.
Purpose: The aim of this study was to evaluate patient satisfaction regarding the quality of care, communication and organisation following the implementation of TPOT in Urology operating theatres in Guys Hospital, London, UK.
Materials and Methods: TPOT was introduced in Urology operating theatres in September 2010. Following implementation, a semi structured questionnaire was issued to 54 post-operative patients returning for follow up after surgery. A total of 157 comments were coded by two independent raters and inter-rater reliability was measured.
Results: Results of the questionnaire showed a high number of positive comments regarding quality and safety of care/treatment (18); treatment/surgery (14); information given about care/treatment (14); staff communication with patients (12) and organisation and efficiency (12). Majority of negative comments were regarding environment/facilities including food/heating and staffing levels.
Conclusions: The introduction of TPOT has improved patient satisfaction in Urology; especially with regards to care, communication and organisation. Improvements may be made in facilities and staffing levels. The study is likely to instigate further research into operating theatre safety and efficiency; with findings being applicable to other high risk specialties.
Use of the Novel Technique of R.E.N.A.L. Nephrometry to Assess Surgical Decision Making at an Australian Tertiary Referral Centre
Introduction:Radical nephrectomy (RN) may lead to the development of chronic kidney disease and its complications. Consequently, elective nephron-sparing surgery (NSS) for suitable renal lesions has become widely advocated. Purpose:To examine recent trends in the utilisation of NSS at our centre; specifically, by applying R.E.N.A.L. nephrometry to assess the complexity of lesions for which surgery was undertaken.Materials and Methods:We performed a retrospective review of renal masses treated by surgery from January 2005 to December 2009, including 79 RN and 70 NSS. CT images were available for analysis in 50 patients within each group. Lesions were scored on the basis of their complexity using the R.E.N.A.L. nephrometry scoring system developed by Kutikov and Uzzo.Results:RN was performed for significantly larger lesions (68±9mm vs 29±2mm, P<0.05) of predominantly moderate- and high-complexity (12% low, 56% moderate, 32% high). NSS was primarily utilised for low-complexity lesions, but included 4 (8%) moderate complexity lesions in the final 2 years of the study. The use of NSS increased from 28.6% of cases in 2005 to 60.0% of cases in 2009, which mirrored the increase in the proportion of operations performed for low complexity lesions (22.2% low-complexity in 2005 to 70.6% in 2009, P<0.01 for trend). Conclusions:The utilisation of NSS at our institution increased over time and mirrored the incidence of low-complexity renal lesions. Practice at our centre reflects a shifting paradigm towards the preferential use of NSS for suitable renal masses.
Cobalt Preconditioning Reduces Renal Injury Prior to Temporary Ischemia in the Rat Model
Introduction: Renal preconditioning aims to trigger Hypoxia Inducible Factors (HIFs) to upregulate renoprotective genes and protect against ischaemic injury. Proven methods of preconditioning are cobalt stimulation and transient hypoxia (ischemic preconditioning). No previous study has compared these two techniques against each other in the kidney. Methods: 24 solitary kidney Sprague Dawley rats were divided into groups of 6 undergoing either a) control treatment, b) 30mg/kg subcutaneous cobalt chloride treatment for 24 and 6 hours pre-ischemia c) intermittent renal artery clamping (IC) of 5 minutes followed by 10 minutes reperfusion over 4 cycles, or d) a combination of both cobalt and IC. Following preconditioning, all rats underwent 40 minutes of renal artery clamping. All rats then underwent renal function tests for 7 days.Results: All rats demonstrated peaks in serum urea and creatinine between day 1 and 3, with return towards basal levels at day 7. Cobalt only treated rats had the lowest rise in serum urea and creatinine compared with the control group (p<0.005). Rats treated with intermitting renal artery clamping or in combination with cobalt treatment also had a lower rise in serum urea and creatinine than controls, but this was not significant. Whilst the control group had a 50% mortality rate, no rats in the preconditioning groups died (p<0.005).Conclusion: Individual Cobalt treatment offers greater protection against renal damage than IC or a combination of techniques. Development of similar hypoxia-mimetic agents that specifically target the prolyl hydroxylation pathway of HIF activation offer potential clinical benefits.
Comparison of Nonthermal Irreversible Electroporation (NT-IRE) to Thermal Irreversible Electroporation (T-IRE) for Kidney Ablation in a Porcine Model
Nonthermal irreversible electroporation (NT-IRE) was compared to thermal IRE (T-IRE) for renal ablation in a porcine model.
24 ablations were completed laparoscopically in 12 pigs using a Pulsed Power Generator (Ethicon Endo-Surgery, Cincinnati, OH), with survival for 24hrs, 7 days and 21 days post-ablation. A single modality was used for each animal. 4 ablations/modality were evaluated at each time point. Retrograde pyelography was used to assess for collecting system injury. Lesion size and pattern of injury were evaluated histologically.
Mean lesion sizes (cm) at 24hrs, 7 days and 21 days were 2.0 x 3.3, 1.2 x 2.4 and 0.7 x 1.3 respectively for NT-IRE; and 2.5 x 3.3, 2.2 x 4.1 and 1.9 x 2.7 respectively for T-IRE. NT-IRE lesions decreased in size over time and were significantly smaller than T-IRE lesions by 21 days (p=0.009). Urinary extravasation was more common with T-IRE. NT-IRE caused hemorrhagic necrosis acutely which resolved by 21 days; large blood vessels and extracellular matrix were preserved. T-IRE caused coagulation necrosis and significantly more inflammation than NT-IRE, which persisted at 21 days.
NT-IRE and T-IRE both resulted in successful renal ablation, but with distinct histological characteristics and significant size reduction observed for NT-IRE lesions by 21 days.
Department of Urology, Academic Medical Centre (AMC), University of Amsterdam, Amsterdam, the Netherlands
IntroductionTools to differentiate renal tumors pre-operatively are still lacking. Optical coherence tomography (OCT) is an imaging technique based on backscattered light intensity in depth, which is hypothetically lower in malignant tissue due to higher scattering by organelles/nuclei. PurposeTo assess the ability of OCT in differentiating renal tumors in an in-vivo setting.MethodsIn-vivo renal tumors and normal parenchyma OCT-images were obtained during nephrectomy (partial/radical) and cryoablation. When applicable, OCT-images of the interior of the tumor were obtained after extirpation(ex-vivo).As quantitative measurement, the attenuation-coefficient (mm−1) of OCT-images were assessed and compared between:-in-vivo renal tumor and normal renal parenchyma (per tissue-type (1) and per individual patient-analysis (2))-superficial and internal ex-vivo OCT-images of tumor (3).ResultsIn-vivo OCT was performed in 16 cases (11 RCC, 3 benign tumors, 1 non-diagnostic biopsy (lap. cryoablation) and 1 not-accessible tumor). 1.Median attenuation-coefficient of normal renal parenchyma (n=16) and tumor tissue (n=15) was 4.99 vs. 7.91mm-1 (p<0.001). 2.Median attenuation-coefficient compared per patient (using Wilcoxon SR-test in cases with both types of tissue available and confirmed pathology) were:-Normal parenchyma vs.RCC (11 cases): 4.97 vs. 9.21mm−1 (p<0.001)-Normal parenchyma vs.benign tumor (3 cases): 5.38 vs. 6.95mm−1 (NS)3.Ex-vivo superficial/internal OCT measurement was performed in 7 tumors. Median attenuation-coefficient did not differ significantly (10.02 vs. 9.21mm−1, NS).Conclusion Attenuation-coefficient of RCC differs significantly from that of normal renal parenchyma on in-vivo obtained OCT-images. Attenuation-coefficient of tumor-surface did not differ significantly from internal tumor suggesting that superficial OCT-measurement is accurate.
Tulane University Medical School, Department of Urology, New Orleans LA; USA
Introduction: Challenges in producing cold ischemia during laparoscopic partial nephrectomy have resulted in novel techniques being investigated for creation of renal hypothermia. Retrograde irrigation via a dual lumen catheter has been proposed to allow intrarenal circulation of agents and an alternative method to induce cold ischemia. Purpose: To compare efficacy and rate of hypothermia in two laparoscopic techniques (surface cooling versus retrograde cooling) in an off-clamp animal model. Materials and Methods: After Institutional Animal Use Committee approval, laparoscopic dissection was performed in four porcine kidneys. To perform retrograde cooling, the distal ureter was mobilized and cooling was performed via retrograde perfusion of ice cold irrigant through a double lumen ureteric catheter. For surface cooling, ice slurry was instilled though a laparoscopic port. Digital thermometer readings of cortical, medullary, and bowel temperatures were recorded for 600 seconds.Results: Using surface cooling, the average change in temperature was −2.62OF/min, to reach 67.5 OF, while retrograde cooling was −1.83 OF /min, to reach 76.30F. Medullary temperature change for retrograde cooling was −1.850F/min, to reach 67.20F, while surface cooling was −1.830F/min and reached a threshold temperature of 76.90F. Retrograde cooling provided more rapid total renal cooling, and provided significant medullary hypothermia, while the cortex remained slightly warmer. Surface cooling showed a different cooling pattern with the cortex cooling faster than the medulla.Conclusions: Both cooling techniques (surface and retrograde) were able to induce cold ischemia. Retrograde cooling was able to achieve a more rapid decrease in medullary temperatures compared to surface cooling.
Department of Urology, University of Patras, Greece
Inreoduction: Drug eluting stents (DES) proved to minimize neointimal hyperplasia in coronary vessels. Hyperplastic reaction is the most common unwelcome event related to the use of metal mesh stents in the ureter. Purpose: We evaluated the effect of zotarolimus eluting stent (ZES) in porcine and rabbit ureter.Methods: A ZES and a bare metal stent (BMS) were inserted by retrograde approach in each ureter of 10 pigs and 6 rabbits. Computerized tomography (CT) was used for the evaluation of porcine ureters and intravenous pyelography (IVP) for rabbit ureters. The follow-up included CT or IVP every week for 4 weeks (pigs) or 8 weeks (rabbits). Renal scintigraphies were performed prior to stent insertion and during the 3rd week. Optical coherence tomography (OCT) has been used for the evaluation of the luminal and intraluminal condition of the stented ureters. Histopathologic examination of the stented ureters embedded in glycol-methacrylate was performed.Results: Hyperplastic reaction was present in both stent types. BMSs in 7 porcine ureters were completely obstructed while porcine ureters stented with ZES had hyperplastic tissue which did not result in obstruction. Only 2 rabbit ureters stented by BMS were occluded. The function of obstructed stented ureters was compromised. The OCT revealed more severe hyperplastic reaction in the ureters stented by BMSs. Pathology examination revealed significantly more hyperplastic reaction in BMSs. Conclusion: ZESs in the pig and rabbit ureter were not related to hyperplastic reaction resulting in stent occlusion. These stents were related to significantly lower hyperplastic reaction in comparison to BMSs.
Single Institution Metal Ureteral Stent Experience: Series Update
Introduction: Metal ureteral stents are a relatively new version of a device with a long history of relieving ureteral obstruction. Our series has previously demonstrated short-term success and good tolerability of metal stents in both malignant (MUO) and benign ureteral obstruction (BUO).Purpose: We present our updated single institution experience with long-term metal ureteral stent placement.Methods: A retrospective analysis of patients undergoing metal ureteral stent placement between February 2008 and May 2011 was conducted. Data collected and reported includes patient age, gender, diagnosis/cause of obstruction, laterality, duration of indwelling metal stent, number of routine metal stent changes, complications, and early discontinuations of the metal stent.Results: Twenty-six patients have received placement of metal ureteral stents. With six patients receiving bilateral metal ureteral stents and eleven patients undergoing at least one stent exchange, a total of 48 ureteral units (UU) have been treated. All metal stents were placed to relieve ureteral obstruction due to ureteral stricture, ureteropelvic junction obstruction, or extrinsic obstruction. With a mean overall stent duration of 15.8 months, the overall stent failure rate was 6.3%, which was limited to two patients with MUO accounting for 3/12 (25%) UU in this group. There have been no intra-operative complications, persistent gross hematuria, or epidsodes of sepsis.Conclusions: Metal ureteral stents are effective and well tolerated in patients with either MUO or BUO. Annual stent exchanges make metal stents an appealing alternative for patients with chronic ureteral obstruction treated by indwelling ureteral stents.
BR02: Basic, Urolithiasis 1
Department of Urology, University of Wisconsin School of Medicine and Public Health, Madison WI, USA
Introduction: Previous porcine research has shown that a 5% hydroxyproline(HP) diet can lead to short-term hyperoxaluria. A gelatin diet has been shown to induce hyperoxaluria in humans. The purpose of our study was to determine if a HP or gelatin diet could induce long-term hyperoxaluria in the porcine model. Methods: A total of 18 gravid crossbred sows (Large White x Landrace) were randomly allotted into 3 treatment groups: 5%HP, 10%HP and gelatin diet. All sows were catheterized one day prior to starting treatment diet. Catheters were left in place for 5 days prior to being removed. Sows were re-catheterized for urine collections on days 11-12 and days 21-22. Urine was collected for each entire 24 hour period and urinary oxalate was determined by ion chromatography. Results: Urinary oxalate concentrations for all three diets peaked within the first five days of the diet. The sows fed the 5%HP, 10%HP and gelatin diets had an early peak in urinary oxalate concentration (mg/L) at day 2(158% increase), day 5(316% increase) and day 5(830% increase) respectively. The day 21-22 time points in all three diets demonstrated markedly increased urinary oxalate concentrations in comparison to baseline with some concentrations higher than the early time point peaks (Day 22: 5%HP=1906% increase, p=0.12; 10%HP=640% increase,p=0.02; Gelatin=501% increase,p=0.01). Conclusion: Although both the 10%HP and gelatin diets induce significant short and long-term hyperoxaluria in the porcine model, the gelatin diet is more cost-effective. The ability to induce long-term hyperoxaluria has important implications in establishing a porcine model for oxalate urolithiasis.
Guide Wireless PCNL: A Prospective Randomized Study
Introduction: PCNL remains the mainstay modality for large bulk renal urolithiasis.Placement of guide wire is the standard protocol. But its become little bit difficult to maintain guide wire in place while doing intrarenal manipulation and stone retrieval in small tract with sheath in place which requires lots of attention by assistant. Here we present our experience of PCNL without guide wire in situ while nephroscopy and compared it with wire in situ in prospectively.Materials and methods : We studied 40 patients in each group(group A wireless PCNL and group B PCNL with wire-standard PCNL) randomly selected and PCNL done by surgeon who has done more than 100 cases.We studied various parameters like age,stone bulk,pelviclyceal anatomy,puncture site,stone morphology,infection,operative time,intraoperative problems,tract size & numbers,blood loss, staging, stone clearance rate, need for other procedures,intraop and post operative complications and need for assistant, assistant comfort and surgeon comfort.Difficult pelvicalyceal anatomy, improper puncture tracts patients were excluded from this study.Result: In both the groups age,stone bulk,morphology,comorbidities, blood loss, tract size,number of tracts,stage were comparable.Assiatant comfort and surgeon comfort was significantly better in group A. Operative time was less in group A but statistically was not significant. There was no significant diffenerce in intraoperative or postoperative complications, stone clearance rate.Conclusion : In selected group of patients PCNL can be done with same efficacy without keeping guide wire in situ making more comfortable manipulations intraoperative for surgeon and assistant without affecting outcome after certain experience
Comparison of the Results and Complications Between Standard and Tubeless Percoutaneous Nephrolithotomy
Introduction: The purpose of this study was the evaluation of early elimination of nephrostomy tube-ureteral and bladder catheters on the results and complications of PCNL. Material and Methods: A total 138 patients with renal stone underwent PCNL. These patients was randomly divided into two groups. Both groups underwent PCNL likewise. At the end of procedure patients in control group underwent nephrostomy tube placement and for the patients in the other group nephrostomy was not used and the cutaneous incision was sutured. The incidence of hermorrhage, hematoma, urinary leakage, urinoma, hospital staying analgesic requarment and stone free rate were compared between two groups. Results: None of the patients needed for blood transfusion and no patient had perirenal hematoma as controlled by ultrasonography 3 day and 2 week after PCNL. 7 patients in the tubeless group had urine collection (3*4.5cm) that disappeared four weeks thereafter. Mean stone size was 28 mm in standard and tubeless group. Mean hospital stay in two groups was 2 and 3.5 days respectively. Mean analgesic requirement (pethedine) in two groups were 100 and 200 mg respectively. Overall stone free rate in both groups was 87% on the day after surgery and 93%, 3 months thereafter by conservative of management of residual fragment.Conclusion: Tubeless PCNL is safe and effective procedure and can decrease hospital stay and postoperative discomfort.
Upper Calyceal Percutaneous Nephrolithotomy (PCNL) Under Spinal Anesthesia: A Prospective Study
Introduction: Traditionally PCNL is being done under general aneshtesia which has its own morbidity and risk.test the suitability spinal anaesthesia forpercutaneous nephrolithotomy, a procedure hitherto performed undergeneral anaesthesia.Aim of our study is to compare Spinal Anesthesiawith General anesthesia in patients undergoing PCNL for upper calyceal puncture. Methods: Weperformed prospective study of 32 patients in each group of patientsundergoing PCNL at our institute Group A ; PCNL under spinal anesthesiaand grouop B under General anesthesia and studied various parameters.PCNLwas done in standard protocol.Nonco-operative patients were excluded.Results:The patients in the Spinal anesthesia group required lessintra-operative and post-operative analgesics, and both patients andendoscopists were better satisfied. Both groups were matched in age,stone burden,gender. There was no significant difference in both thegroups for parameters like operative time, intraoperative complications,pelvicalyceal aceess,bleeding, stone free rate or post operativecomplications. But cost was significantly less(10 time s at our hospital, 150Rs. VS 1600 Rs.) with group A apart from quick recovery from anesthesia,safe in high risk patients..Post operative pain was significantly less in group A. Post operative analgesic effect and respiration wassignificantly better in spinal group. Conclusion : This study demonstrates Spinal anesthesiais safe, reliable and as effective as GA but superior analgesia,at very lowcost without affecting outcome for patients subjected to percutaneousnephrolithotomy,with stable haemodynamics, good post-operative analgesiaand acceptable to patient and endoscopist satisfaction even in upper calyceal puncture
Supracostal Tubeless Percutaneous Nephrolithotomy: A Retrospective Cohort Study
Purpose: To evaluate the safety of tubeless percutaneous nephrolithotomy in patients undergoing supracostal percutaneous renal access.Materials and Methods: Between October 1999 and October 2010, 302 patients underwent percutaneous nephrolithotomy via a supracostal access tract. Two hundred and forty-eight (82.1%) patients had a nephrostomy tube placed at the conclusion of the case and 54 (17.9%) did not. The medical records of both cohorts were compared with regard to patient demographics (age, gender, body mass index, preoperative creatinine), operative characteristics (estimated blood loss, length of stay, treatment efficacy), and complication rates (overall, thoracic, hemorrhage requiring transfusion). Results: Patient demographics did not differ between the tubeless and nephrostomy tube groups. Estimated blood loss was significantly less in the tubeless patients (67 ml versus 123 ml; p=0.150). There was no difference in length of stay (tubeless 1.02 days versus nephrostomy tube 1.10 days, p=0.395). Treatment success was comparable between the two groups (tubeless 81.5% versus nephrostomy tube 77.8%; p=0.553). The overall complication (p=0.765) and blood transfusion (p=0.064) rates were equivalent. The incidence of chest complications was significantly higher in the tubeless (22.2%) group compared to the nephrostomy tube (10.9%) patients (p=0.024).Conclusions: Tubeless supracostal percutaneous nephrolithotomy was associated with less intraoperative blood loss and there was a trend towards fewer transfusions. However, the tubeless group experienced more chest complications, which calls into question the applicability of tubeless percutaneous nephrolithotomy in patients undergoing supracostal access.
Division of Urology, Department of Surgery, The University of Western Ontario, London, Ontario, Canada
Introduction - The efficacy and safety of percutaneous nephrolithotomy (PCNL) has been demonstrated in obese individuals, however there remains little data considering the outcomes of PCNL in super obese patients. Purpose - To assess perioperative and stone-related outcomes following PCNL in super obese patients. Materials and Methods - A prospective database captured data from 5803 patients treated with PCNL between November 2007 and December 2009. A multidimensional match of 97 super obese patients with those of normal weight was created using propensity score matching. Students T-test and Chi-square tests were used to assess for differences between the groups. Results - Ninety-seven patients with a BMI>40 were matched by stone characteristics with 97 patients of normal weight. The super obese population demonstrated higher rates of diabetes mellitus (43% vs 6%, p<0.001) and cardiovascular disease (56% vs 18%, p<0.001. Access was achieved more frequently by a Radiologist in the super obese group (19% vs 6%, p=0.016). Mean operative duration was longer in the super obese group (112±56 mins vs 86±44 mins, p<0.001). Stone free rates were lower in the obese group (66% vs 77%, p=0.071) with a resultant discrepancy in re-treatment rates (28% vs 12%, p=0.012). There was no significant difference in length of hospital stay or transfusion rate. Super obese patients were significantly more likely to experience a post-operative complication (22% vs 6%, p=0.004).Conclusions - PCNL in super obese patients is associated with longer operative duration, inferior stone free rates, higher rates of re-intervention and increased risk of peri-operative complications.
A Novel Technique for Large, Multiple Ureteric Stone: Antegrade Flush & Retrograde URS
Introduction : Large and multiple ureteric stone is still management dilemma especially in upper ureter and impacted.Due to stone belt region with poor socioeconomic condition we get so many large burden ureteric stone with renal insufficiency making its management tough. so using various techniques we developed our new technique for such type of urolithiasis management. Here we present our novel technique for management of upper ureteric stone.Materials and methods : We present this technique for endourological management for large burden ureteric stone in 64 cases. We do Percutaneous nephrostomy(PCN) placed preplanned and through PCN we do antegrade irrigation while doing retrograde URS and fragmenting stone with lithoclast. Advantage of antegrade irrigation is stone fragments do not migrate.Result: We performed this technique in 64 patients who had large, multiple ureteric stone of 1.3 cm to 3.2 cm. All stones could be cleared completely except two who required auxiliary procedure. seven patients required two staged procedure.eight patients had postoperative fever. None had any major complications. Out of 64 patients 55 had renal insufficiency so PCN could help in improving renal function.Conclusion: This Novel technique;Antegrade flush-Retrograde URS is effective, safe, cost effective modality for management for large burden ureteric stone.
Extrarenal Manipulations for Retropgrade Intrarenal Surgery(RIRS) Using Semirigid URS and Pneumatic Lithotripsy: A Novel Concept
IntroductionRIRS is the mainstay for small burden renal stone management when ESWL does not work. But the drawbacks associated with RIRS are unavailability, high initial and maintenance cost especially in developing world.Here we present our experience of RIRS using semirigid URS with some extrarenal manipulations making it more effective safe and feasible with low cost.MethodsWe have performed 154 cases of RIRS with semirigid URS with help of some manipulations from Nov 2008 to june 2011.Extrarenal manipulations like lifting kidney up, down , rotating it medially or laterally, movement of upper or lower pole, tilting table ipsilateral or contralateral side, making table head side up or down, tilting patient side by side, making respiration rate and depth controlled as per need,making irrigation slow or fast, use of suction, forced dieresis with diuretics etc.We studied various parameters.ResultsOut of 154 patients,91 has pelvic stone with upper calyceal stones in 61, middle calyceal stones in 58 cases, lower calyceal stones in 42 cases with favorable anatomy. With manipulations described above,we could clear stones in 134 patients( 86%).There was no major intraoperative complications except minor extravasation in one case.Operative time was 46+9 minutes. Four patients had post operative feverConclusionsExtrarenal manipulations for intrarenal surgery using semirigid URS and pneumatic lithotripsy is safe, effective strategy without compromising outcome with low cost.
Department of Urology, University of Modena and Reggio Emilia, Italy
Introduction: Encrustation is a frequent complication of indwelling-ureteral-stent. Purpose: chemical-mineralogical analysis of stents, with evaluation of risk-factors for encrustation. Methods: 28 patients submitted to ureteral-stent-removal were considered. Stents were previously positioned for urolithiasis(22), during management of non-metastatic urothelial-malignancies(4), after pyeloplasty(2cases). Mean indwelling time:57,1+/-7.4days. Analytic-procedure: quantification of encrustation was performed at both ends(6-10cm), heated at 70degrees for 12hours and then cooled. Stent-ends were located into 35ml-Becker with additional 10-ml of HNO3-0,7M. Beckers were submitted to ultrasound-bath for 45min and the so-obtained solution was bring to volume into 25ml-volumetric flask. The procedure was repeated up to reach constant weight. The degree-of-encrustation was calculated as weight-difference before and after chemical attack(mg/5cm). Calcium and magnesium were measured in this aqueous-solution with atomic-absorption-spectrophotometry whereas phosphate content was determined with colorimetry. Structural-mineralogical analysis with X-rays-diffraction was performed when separate rates of encrusted material were available. Results: mean weight of encrustation was 5,77+/-8,12 at the proximal- and 3,15+/-3,77 at the distal-end of the stent. In a linear-regression-model, the only variable significantly related to the burden of proximal-coil-encrustation was urolithiasis(p=0.042) whereas time-of-stent-permanence was insignificant(p=0.1). Among patients with urolithiasis, frequent-stone-formers presented more encrustation of the proximal end than patients at their first stone-episode(p=0.04). Stent encrustations reflect stone composition(p=0.00). Higher degree of encrustation at the distal-coil were related to urinary-infection(p=0.016) and age(p=0.07).Conclusion: The present study highlighted variables related to ureteral-stent-encrustation; furthermore, it seems to be the first one analyzing separately the two coils of the device. The so-obtained risk factors have to be considered when positioning a DoubleJstent.
Health Related Quality of Life in Ureteral Stone Patients: Post-Ureterolithiasis.
Ureteral stones disease is among the most painful and prevalent among urologic disorders that can substantially impact health-related quality of life (HRQoL). The aim of the study is to assess the QoL in patients with ureteral calculi after surgical intervention and identifying the most significant factors that could impact their QoL. The target population included two groups: post-lithotripsy patients and comparator group comprising healthy individuals selected from the general population. Both groups were matched for age and gender. The study continued through a period of 9 months. An observation period of 4-10 months following the last surgical intervention was applied before interviewing patients. Information regarding socio-demographics, medical data and presence of co-morbidities were recorded. The Medical Outcome Study Short-Form 36-item survey (SF-36) was used to assess HRQoL for both groups. Based on the SF-36 questionnaire, there were no significant differences between patients and healthy volunteers in the mean scores for eight of the HRQoL domains, except for pain and social functioning subscales. Patient's age, distal ureteral stones and ureteral stent, in addition to DM and low back pain appeared to significantly affect the HRQoL of patients. In conclusion, the promising end point in the management of urolithiasis is improvement of HRQoL. The results of the current study support the notion that urinary stone disease is not a life threatening disease and patients can return to normal life after surgical intervention. Prospective studies are warranted for elucidating the factors influencing HRQoL in ureteral stone patients to optimize patient care.
Preventing Retrograde Stone Displacement During Pneumatic Lithotripsy for Ureteral Calculi Using Lidocaine Jelly
Objectives:To assess the efficacy of lubricating jelly instillation proximal to the ureteral calculi during lithotripsy on the prevention of retrograde stone displacement and the stone-free rate Methods: 110 patient with ureteral calculi of less than 2 cm were randomized into 2 groups: jelly instillation (n=55) and controls (n=55). Ureteroscopy was performed using a 9.8F semirigid ureteroscope. A 5F ureteral stent was advanced beyond the stone. Lidocaine jelly (2 mL) was instilled, and lithotripsy was done with a Swiss Lithoclast. A 5F ureteral catheter was left in place for 24 hours, and patients were followed up at 24 hours with radiography of the kidneys, ureters, and bladder and at 2 weeks with sonography.Results: Both groups were comparable in terms of mean age and stone size. Stone or stone fragment migration occurred in 18.8% of the treatment group and 44.2 of the controls, statistically significantly different (P=0.009). The stone-free rate was 81.3 and 55.8 in the treatment and control groups, respectively. The rates did not improve after 2 weeks, and the difference was not statistically significant between the two groups (P=0.384). The mean operative time was also comparable between the two groups.Conclusion: Lidocaine jelly instillation proximal to the ureteral calculi during lithotripsy is an effective method to prevent retrograde stone displacement.
Endourology Assaf Harofe, University of Tell Aviv, Israel
Respiratory motion during SWL can move stones with each breath; this movement is not in line with the axis of the waves. Depending on respiratory rate, length of excursion, focal width and shock wave rate, the stone can be outside the focal zone 50% of the time. When the first SWL treatment fails, a patient may have to undergo more procedures. Accordingly, we design a prospective control study to examine the ability of bronchial blocker (BB) to improve the outcome. The procedure was performed under general anesthesia (GA), using BB, on patients (n=13) who had failed the first SWL treatment. The control group of patients (n=17) went the treatment under sedation. Successful outcome was stone free at 3 month follow up.The treatment duration was significantly more p=0.001 in the study group with no side effects. We found significant ( p=0.02) improved outcome with upper pole stones location. The success/failure in the study and control groups was 9/3 vs 10/7 with p=0.12. We conclude that in a small group of patients the addition of BB to SWL did not change significantly the outcome, larger group is needed.
Department of Biomedical Engineering, University of Michigan, Ann Arbor, MI, USA
Introduction
Previous work has demonstrated cavitationally-based pulsed ultrasound therapy (histotripsy) effectively comminutes model urinary stones, eroding them to fine debris<100-μm in size.
Purpose
Histotripsy was evaluated as a potential adjunct to conventional SWL procedures, with the hypothesis that synergistic interplay of the two modalities will yield faster and more complete stone comminution.
Materials and Methods
Model stones cast from Ultracal-30 gypsum cement were placed on a 2-mm mesh screen and treated with one of three therapies using a system built in-house (pictured): (1) Electrohydraulic SWL at a shock rate of 1-Hz; (2) Histotripsy at a pulse repetition rate of 100-Hz; (3) Simultaneous application of (1) and (2). Five stones were treated with each case, and time to complete comminution (all fragments<2-mm) was measured.
Results
Electrohydraulic SWL achieved complete stone comminution in 43.6±6.3 min/g. Statistically significant reductions in treatment time were observed for both histotripsy and the combined therapy, which produced complete comminution in 25.4±2.3 min/g and 16.7±3.2 min/g, respectively (p<0.001).
Conclusions
Cavitationally-based stone erosion with histotripsy shows potential as a means to augment traditional SWL, and it is likely that an optimized combination of the two modalities will lead to further enhancement of the comminution process.
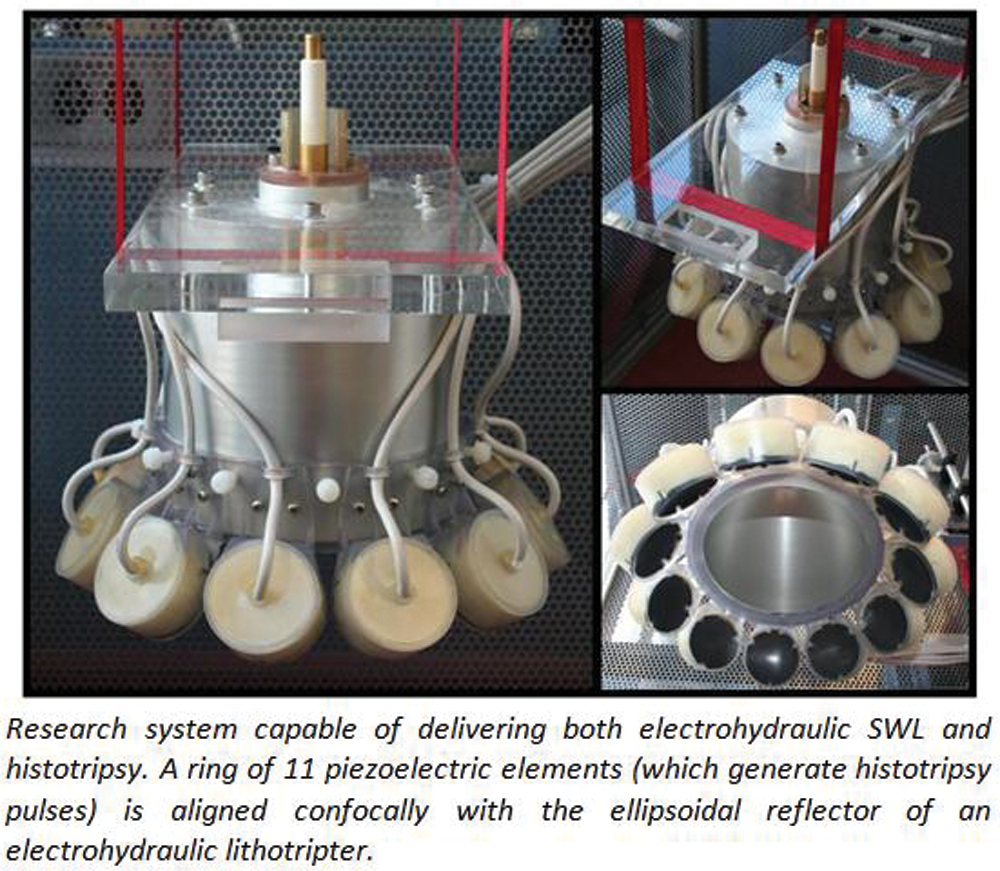
Incidence of Diabetes Mellitus After Extra Corporeal Shock Wave Lithotripsy in 15 Years Follow-Up
(Introduction: Following the recognition and practice of Extracorporeal Shock Wave Lithotripsy in 1982, numerous reports have been published to investigate its side effects but long term complications are still unknown. Purpose: to investigate the hypothesis that extra corporeal shock wave lithotripsy increases the incident risk of new onset diabetes mellitus. Studies have suggested that Extracorporeal Shock Wave Lithotripsy predispose to diabetes mellitus.Materials and Methods: we collected data from 307 patients treated with Extracorporeal Shock Wave Lithotripsy from 1991 to 1994. In 15 years fallow up we invited patients to check Blood Sugar.Results: The incidences of diabetes mellitus were increased to 8 percent after Extracorporeal Shock Wave Lithotripsy. The mean Fasting Blood Sugar was increased to 12 gram per decilitre. It was 15 percent in right side and 9 percent in left. And there wasnot any significant relationship between age, sex and BMI with increasing of Fasting Blood Sugar. Also the increase of Fasting Blood Sugar is more significant in intensities higher than 16 Kilowatts.Discussions: our findings suggest that Extracorporeal Shock Wave Lithotripsy treatment might associated with new onset of diabetes mellitus in 15 years follow up but more investigations are needed.)
BR03: Basic, Robotic/Lap Surgery/Prostate/Female Urology/New Technology
Department of Urology, University of Patras, Greece
Introduction: Phosphodiesterase type 5 (PDE5) inhibitors have been reported to induce ureteral smooth muscle relaxation in isolated human ureters. Nevertheless, the availability of human ureteral tissue for basic science studies is subjected to several limitations. Purpose: Porcine and sheep ureters were used as an in vitro model for ureteral contractility examination. The effect of vardenafil in this model was used to investigate whether it can reproduce human results and can be considered as a replica of human ureter for further pharmacological studies.Materials and methods: The ureters of 10 domestic piglets and 10 sheep were harvested. Isolated 5mm ureteral rings from 4 different parts of each ureter (ureteropelvic junction, upper, middle, lower) were placed in an organ bath and connected to a tension transducer to measure ureteral ring contractility. Basic ureteral contractility of each segment was documented. The ureteral rings were then exited using KCL, epinephrine and subjected to different doses of Vardenafil. Results: Basic ureteral contractility was found to follow different patterns between porcine and sheep ureter. Measured ureteral contractility was found to be depended to the level of the ureter from which ureteral ring had been obtained. Vardenafil was found to induce ureteral smooth muscle relaxation to both species. Non significant differences in ureteral response to Vardenafil were observed between different segments of the same ureter. Conclusions: Vardenafil induced smooth muscle relaxation to both porcine and sheep isolated ureteral rings. Porcine and sheep ureters can offer a useful tool for the in vitro examination of ureteral contractility.
Nephron Sparing Surgery without Renal Hilar Clamping
Introduction: Detection of incidental renal lesions has risen sharply. Most are small, <7 cm, sized lesions. During robotic or laparoscopic nephron sparing surgery renal hilar clamping is often employed. Unfortunately, there is no simple technique to cool renal parenchyma during laparoscopic surgery and longer warm ischemia times are associated with renal damage.Purpose: Analyze outcomes of patients undergoing laparoscopic and robotic partial nephrectomies without hilar clamping.Methods: A retrospective database of patients undergoing partial nephrectomy from 2003-2010 was reviewed. Small renal masses suspicious for malignancy were excised by conventional laparoscopic partial nephrectomy (LPN) or robotic-assisted laparoscopic partial nephrectomy (RALPN) without renal vessel clamping. Data from these clinical interactions was retrospectively collected and analyzed, which included patient age, pathologic diagnosis, operative time, surgical margins, serum creatinine change, EBL, post-operative hemoglobin change, transfusion rate, length of follow up, recurrences, and complications.Results: Twenty-nine patients underwent partial nephrectomy without renal hilar clamping. Fifteen were performed by LPN while 14 underwent RALPN. No intra-operative complications occurred and 6 (20%) post-operative complications occurred without any reoperation. The mean pre- and post-operative serum creatinine levels were 1.2 and 1.1. The mean hemoglobin change was −2.7(g/dL), with 3 (10.3%) patients requiring a blood transfusion. Of the masses, 72.4% were malignant with a mean size of 2.2cm. One positive margin occurred, but at a median follow up of 34 months there have been no recurrences.Conclusions: LPN with or without robotic assistance can be safely performed without hilar clamping in select patients providing renal functional protection.
Measuring the Protective Effect of Allopurinol Using Isoprostane After Renal Ischemia in an Animal Model
Introduction: Laparoscopic/robotic partial nephrectomy involves temporarily clamping the renal artery, making the kidney susceptible to ischemic damage. Isoprostane is a prostaglandin compound formed in vivo from free radical catalyzed peroxidation of archidonic acid independent of cyclooxygenase enzyme. Isoprostane represents one potential marker of oxidative injury. Purpose: To determine if renal interstitial isoprostane levels can quantitate renal damage secondary to warm ischemia. Another goal is to investigate allopurinol for renoprotective abilities. Previous studies have demonstrated transplant kidneys pretreated with allopurinol sustain less nephron damages from ischemia.Materials and Methods: A microdialysis probe was inserted into renal parenchyma of rats to allow continuous dialysis and collection of effluent for isoprostane levels. Following clamping of the renal vessels for predefined intervals (15, 30, 45, & 60 minutes) of ischemia, the interstitial effluent from the probe was collected and subsequently analyzed for isoprostane levels with and without allopurinol pretreatment.Results: Clamping of the renal artery and vein produced increases in isoprostane levels during the ischemic period and larger increases during reperfusion. Greatest damage was during 60 min clamp. When comparing isoprostane levels in rats which did not receive allopurinol, there were significant differences between the clamp and post clamp levels of isoprostane. Allopurinol demonstrated protection to the kidney from ischemic changes caused by clamping the renal hilum. Conclusions: Our data demonstrated that isoprostane levels are potential real-time markers of renal ischemia and reperfusion injury. We also found allopurinol administration demonstrated a trend toward renoprotective abilities in the hilar occluded kidney in this animal model.
Clamping Renal Artery Alone Improves Oxygen Reperfusion Over Both Artery and Vein: Quantitation Using Infrared Tissue Oximetry in Porcine Model.
Introduction: Near infrared tissue oximetry has been used quantify renal ischemia. Previous studies demonstrated a protective effect from clamping artery alone versus artery & vein during open partial nephrectomy; however this benefit has not been demonstrated with laparoscopy, possibly due to impaired venous outflow from pneumoperitoneum.Purpose: To evaluate oxygen saturation during arterial clamping alone, compared to artery & vein together, using infrared tissue oximetry. Materials and Methods: Infrared renal oximetry (ViOptixFremont, CA) measurements were obtained at baseline (prior to selective renal hilar clamping), every 30 seconds during warm ischemia (15 and 30 minutes trials) and for 10 minutes after unclamping the artery/vein versus artery alone of Yorkshire swines. A total of 120 oximetry readings were obtained for each of the 4 renal units.Results: Compared to renal artery and vein, clamping artery alone produced lower and faster decreases in tissue oxygen levels in both 15 and 30 minute clamp periods. Upon reperfusion, mean oxygen saturation increased statistically more quickly in the renal unit with only artery clamped, in both 15 and 30 minute experiments. In the recovery phase, maximum oxygen saturation levels were higher when artery was clamped alone versus artery and vein.Conclusions: Tissue oximetry analysis during renal arterial clamping alone demonstrated larger drops in tissue oxygen saturation and faster recovery of tissue ischemia compared to combined renal artery and vein clamping in porcine model. Further studies to correlate tissue oximetry to renal function recovery following hilar clamping during partial nephrectomy are underway.
Intrarenal Pressures Remain Low with Placement of a Dual Lumen Catheter for Retrograde Irrigation to Induce Renal Hypothermia.
OBJECTIVES: To determine whether placement of a 10F dual lumen catheter during retrograde irrigation produces a low pressure collecting system. To determine maximal flow rate while simultaneously maintaining intrarenal pressures less than 20mm H2O.METHODS: Ex vivo porcine kidneys underwent harvest, and a dual lumen ureteral catheter was placed within the ureter at the level of the renal pelvis. After attaching the manometer of a LifeTech Urovision JanusV (v.1,71.0) Urodynamics machine, pressure measurements (n=1080) were recorded at 1 sec intervals. Irrigant flow rates were initiated at gravity and subsequently increased at 10cc/minute increments to a maximum of rate of 100cc/minute. Consecutive one minute trials were recorded for each infusion rate.RESULTS: During retrograde infusion without a dual lumen catheter, every 10cc/minute rate increase resulted in an 8 cmH2O rise in intrarenal pressure. The maximum flow rate obtained was 20cc/minute before urinary extravasation or intrarenal drainage occurred. Maximum pressure obtained before urinary extravasation or collecting system perforation was 16 cmH2O. Placement of a dual lumen catheter within the renal pelvis allowed intrarenal pressures to remain less than 5 cmH2O, (when infusion rates were less than 80cc/minute). Maximum flow rate while maintaining pressures less than 20 cmH2O was 90cc/minute. Flow rates above 100cc/minute resulted in urinary extravasation. During gravity infusion, optimal drainage from dual lumen catheter was obtained.CONCLUSIONS: Using an ex-vivo porcine model, application of a 10F ureteral dual lumen catheter produced adequate retrograde drainage which resulted in low intrarenal pressures.
Time to Oncologic Proficiency in Robotic Radical Prostatectomy: Successfully Reducing the Learning Curve in a Multisurgeon Program
INTRODUCTION: Objective was to develop a multi-surgeon robotic surgery program allowing surgeons learning RALP to achieve proficiency without compromising cancer control during the learning curve.METHODS: We started with 10 surgeons. Three of the surgeons had completed an accredited fellowship in robotic surgery. These surgeons served as preceptors for the other surgeons. Surgery was undertaken in a step-wise fashion, with all surgeons completing more than 10 cases with the preceptor. Each RALP was performed was done so with one of the original 10 surgeons serving as primary assistant.We prospectively collected pathologic data, using margin status as a surrogate endpoint for cancer control.RESULTS: 1732 RALPs have been performed. Mean age is 59.3. Mean pre-operative PSA level is 7.2 (0.6-41). Mean Gleason score was 6.3 (5-10). All prostate specimens were reviewed by the same 3 pathologists at one institution. 1262 (78%) patients were pathologic stage pT2 and 470 (22%) of patients were pT3. The mean number of cases performed per surgeon is 99 (4-147). Surgical margin status was evaluated for the first 1200 cases by quartile (1st 300 cases, 2nd 300, 3rd 300 and 4th 300) and is as follows: For pT2: 24%, 14%, 13% and 11%; for pT3: 51%, 43, 21 and 25%, respectively per quartile. Complication rate (Clavien grade 3 and 4): 1.3%.CONCLUSIONS: We have demonstrated that an acceptable positive surgical margin status for RALP, as well as a low complication rate, can be achieved within a relatively short period of time, using a standardized preceptorship program.
Robotic Assisted Surgery Reduces Rectal Injury Rates in Radical Prostatectomy Patients
Introduction:Rectal injury can be a devastating complication for both patients and surgeons during radical prostatectomy. Our Goal was to compare rectal injury rates during radical prostatectomy for laparoscopic (LP) vs. robotic assisted radical prostatectomy (RALP). Methods:Our study is a retrospective review of rectal injury rates in men undergoing radical prostactomy. Between 2005-2008 our institution did a large volume of LPs. Starting August 2008 we developed a robotic surgery program and started to perfrom RALP procedures among 10 surgeons then expanding to 21 surgeons over a 2 year period with standardized, strict training approach for 21 attending surgeon staff. We reviwed the charts of the last 1000 LP and we compared those with our FIRST 1000 RALP patients. Rectal injury was defined as any lacertation that was through the mucosa and required primary repair or colostomy or resulted in fistula formationResults:For our LP group (N=1000): Mean age was 59.1. Mean pre-op PSA was 7.8 (.4-53). Mean Gleason score was 6.5 (5-10). 73% of were pathological stage pT2 and 20% were pT3. There were 12 rectal injuries (1.2%) in the LP group. For the RALP group (N=1000): Mean age is 59.3. Mean pre-operative PSA level is 7.2 (0.6-41). Mean Gleason score was 6.3 (5-10). 78% patients were pathologic stage pT2 and 22% of patients were pT3. There were 2 rectal injuries (0.2%) in the RALP groupConclusion:When comparing LP to RALP, Robotic surgery can lead to less rectal injury rates during prostatectomies.
Supracervical Robotic Assisted Laparoscopic Sacrocolpopexy and Robotic Hysterectomy as Treatment for Pelvic Organ Prolapse: Series Update
Objective: Supracervical robotic assisted laparoscopic sacrocolpopexy (SRALS) is a relatively new surgical treatment for pelvic organ prolapse that secures the cervical remnant to the sacral promontory. We present a series update on our experience with SRALS in the same setting as supracervical robotic assisted hysterectomy (SRAH).Methods: Women with vaginal vault prolapse and significant apical defects as defined by a Baden-Walker score of 3 or greater that had not undergone hysterectomy were offered SRALS in combination with SRAH. Chart review was performed to analyze operative and peri-operative data. Outcomes were compared to patients who underwent RALS without any other procedure.Results: From July 2005 through April 2011, 45 patients underwent RALS, including 19 patients who underwent SRALS. All SRALS were performed following SRAH in the same setting. Blood loss was negligible. Forty-three patients were discharged on postoperative day one. One patient in the RALS group had an apical recurrence, but none since the original series. There have been no recurrences in the SRALS group. Operative time was longer for SRALS as these procedures were performed in conjunction with SRAH.Conclusions: SRALS is effective to repair apical vaginal defects in patients with significant pelvic organ prolapse who have not undergone previous hysterectomy. The cervical buttress provides excellent support for the graft sutures and strength to the repair. Complications are few. Greater follow-up and numbers since the original series are helping to establish the role of this procedure in treatment of apical pelvic organ prolapse.
Evaluation Study Between Tension Free Vaginal Tape and Transobturator Tape in Treatment Stress Incontinence in Female
Objective: The aim of this study was to compare the efficacy of the TOT versus the TVT in women with stress urinary incontinence(SUI) with a median follow-up of 6 months.Methods: In This randomized clinical trial, eighty female patients with SUI were randomly allocated to TVT (n=40) or TOT (n=40). Preoperative and postoperative assessments included a validated Stress and Urge Incontinence Questionnaire,a 24-h pad test.The clinicopathologic parameters of the patients included age, body mass index, onset of incontinence, previous pelvic surgery, parity, delivery, type of anesthesia, operative time, hospital stay , catheter indwelling, postoperative complications and 1 ,3 and 6 months follow up of ICIQ.Results: Age was 52.02±0.88 for TVT and 52.27±7.34 years for TOT. The rate of the complications was similar two groups. Operative time (min) was 64.50±9.04 in TVT versus 64.00±9.48 in TOT (P=0.86), hospital stay (day) was 2.56±0.51 in TVT Vs 2.52±0.47 in TOT (p=0.76), catheter indwelling (day)was 1.88±0.41 in TVT Vs 1.55±0.47 in TOT (p=0.001). Before , 1 , 3 and months after intervention ICIQ was not significant between two group , although there was a non significant decearse of ICIQ in 3 and 6 months in TVT group Vs TOT group( p0.801 in 3 and 0.899 in 6 month). CONCLUSIONS: Our results evidence a similar efficacy and safety of TVT versus TOT procedure for female SUI, although catheter indwelling was significantly longer in TVT and in 6 months follow up, TVT procedure is non significantly more effective than TOT.
University of Michigan, Department of Urology, Ann Arbor, MI, USA
Introduction: Histotripsy is a non-thermal ablative focused ultrasound technology with potential future applications for prostate cancer focal therapy.Purpose: We used a novel prostate tumor model and evaluated the feasibility of treating prostate tumors with histotripsy.Methods: A total of 12 immunosuppressed (cyclosporine) canine subjects received transabdominal ultrasound guided intraprostatic injection of ACE-1 canine prostate cancer cells. Prostates were serially imaged with transrectal ultrasound (TRUS) to monitor tumor growth. Subjects were either treated as shams or with transabdominal histotripsy of the prostate targeting tumor implants and adjacent parenchyma using a 750 kHz piezoelectric ultrasound therapy transducer.Results: ACE-1 tumors were visualized on TRUS in all 12 subjects. Tumors demonstrated preferential growth in the prostatic capsule, fibrous septa, and periurethral fibrous stroma with significant desmoplastic reaction and areas of central necrosis on histology. Targeting of the tumor and histotripsy therapy was feasible with evidence of homogenization of normal parenchyma and tumor (see figure).Conclusion: This study provides preliminary data in a novel canine prostate tumor model suggesting a potential role for histotripsy in focal therapy for prostate cancer. Further studies are needed to better characterize the role of histotripsy in prostate cancer treatment and its effect on malignant potential.Funding: Departmental
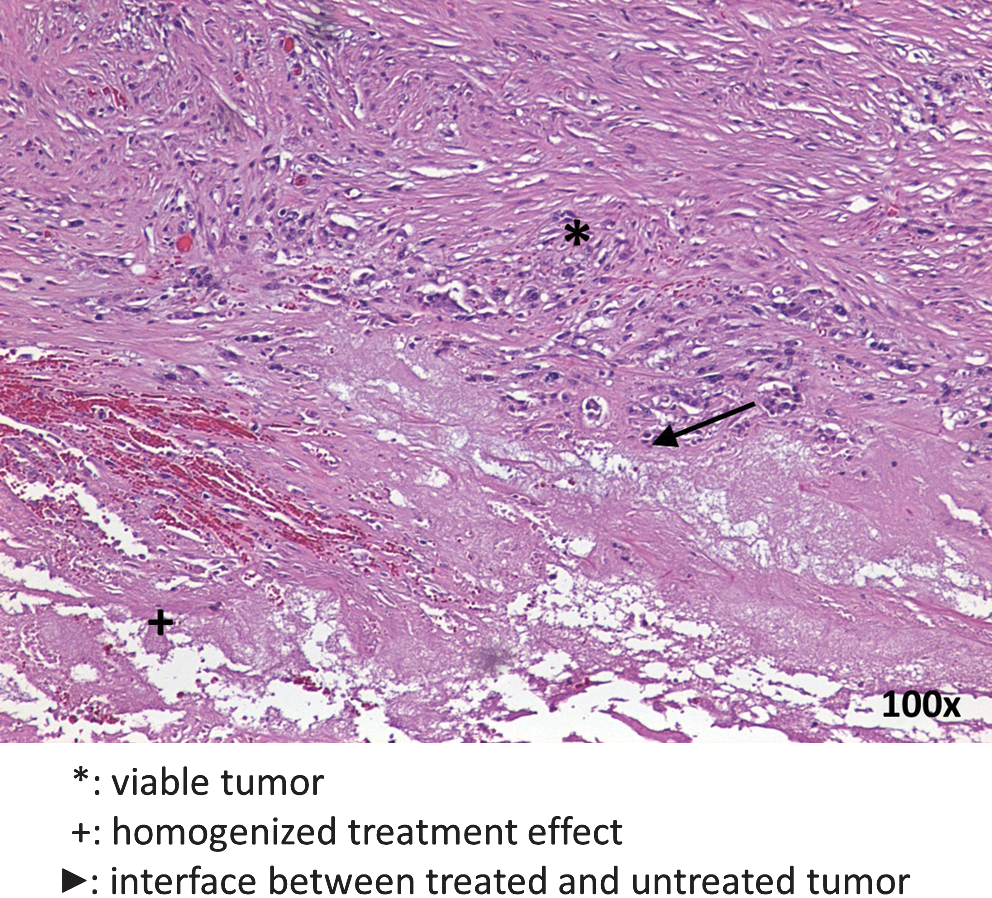
Departments of Urology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Purpose: To use a newly constructed, covered, retrievable, expandable nitinol stent with barbs to overcome the problem of stent migration associated with conventional covered prostatic expandable stents, as well as to prospectively evaluate the technical feasibility and clinical effectiveness of the stents in patients with benign prostatic hyperplasia.
Materials and methods: A covered retrievable expandable nitinol stent with four barbs was placed with use of an 18-Fr stent delivery system in seven consecutive patients with symptomatic BPH who had high operative risks. Patient age ranged from 62 to 83 (mean, 74) years. In cases in which the stent migrated it was replaced with a stent with 8 barbs. The stents were routinely removed 4 months after placement using a 21-Fr stent removal set.
Results: Stent placement was technically successful and well tolerated in six of the seven patients. The remaining patient needed a second stent placement after removal of the first stent. The stent with four barbs migrated into the urinary bladder in four patients (57%); three of these received a second stent with 8 barbs with good results, while the fourth did not need further treatment because his symptoms improved. Routine removal of the stent 4 months after placement was performed in three of the seven patients with good results.
Conclusions: Retrievable stents with eight barbs seem to overcome the problem of stent migration associated with conventional prostatic expandable stents. Our preliminary results suggest that stents with barbs are both feasible and effective in patients with benign prostatic hyperplasia.
Departments of Urology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Purpose: To prospectively evaluate the technical feasibility and clinical effectiveness of a newly constructed, covered, retrievable, expandable nitinol stent with 8 barbs in patients with metastatic prostatic cancer.
Materials and Methods: A stent 20mm in diameter when fully expanded and 20-50mm long was constructed from 0.01-inch-thick nitinol wires into a tubular configuration. To prevent stent migration, 4 barbs (2mm in length) were attached 5mm proximal to the distal (urethral) end of the stent and another 4 barbs to the middle body of the stent. To make the stent removable, two draw-strings were attached to the distal end of the stent crossing the lumen of the stent. The stent was placed with use of an 18-Fr stent delivery system in eight patients with symptomatic metastatic prostatic cancer.
Results: No technical failure or procedural complications occurred. All patients could void immediately after stent placement. Maximum urine flow rates and post-void residual volumes after stent placement were 5.6-10.2 mL/sec (mean, 8.2 mL/sec), and 5-45 mL (mean, 27 mL), respectively. Urinary incontinence occurred in five of the eight patients, which gradually improved. During the mean follow-up of 192 days (range, 21 to 553 days), the stent was removed in one patient because of stone formation 233 days after stent placement. The patient did not need further intervention because of improvement of the mass after stent removal.
Conclusioons: Our preliminary results show that the retrievable stent with 8 barbs seems to be both feasible and effective in patients with metastatic prostatic cancer.
Department of Urology, Hadassah Hebrew University Medical Center, Jerusalem, Israel
IntroductionDuring the past decade the incidence of sever infection following TRUS guided prostate biopsy has increased due to the emergence of resistant bacteria within the gut of patients, despite the use of prophylactic antibiotics. Antibacterial varnish coated dental implants are known to result in reduced infection rates. This varnish has yet to be tested in the field of Urology.PurposeAn in-vitro study assessing the possibility to reduce infection rates following prostate biopsy by coating the needle with a novel sustained, yet rapid release chlorhexidine varnish specifically modified for prostate biopsy.Materials and methodsA model of two layers of agar, of which one was pre infected with E. coli, separated by a non bacterial transmissible divider, simulating the environment of a prostate biopsy was developed. Biopsy needles were coated with the chlorhexidine-varnish and inserted multiple times into the model. The ability to reduce transmission of infection as well as to inhibit growth was assessed. Results were compared with a series of positive and negative control needles. ResultsA 100% reduction of infection transmission as well as a sustained inhibition of growth was observed when using the chlorhexidine-varnish coated needles compared with the control needles. ConclusionsThis in-vitro study represents a new strategy in infection control following prostate biopsy. The chlorhexidine-varnish coated needle resulted in decreased infection transmission as well as in growth inhibition. Further in-vivo studies are required. A new strategy of prophylactic antibiotics combined with varnish-coated needles should result in decreased infection rates following prostate biopsies.
Improved Detection of Microbial Suprapubic Catheter Colonisation by Sonication
AbstractINTRODUCTION AND OBJECTIVE: The spectrum of microbial suprapubic catheter colonization (MSCC) is unknown. The aim of this prospective sonication study was: (i) to assess the frequency of MSCC, (ii) to identify the responsible pathogens and (iii) to characterize the microbial diversity of MSCC.METHODS: A total of 177 suprapubic catheters from 102 patients were enrolled. Median indwelling time was 47 days (range 1-417 days). Sonication was performed in an ultrasound bath to dislodge adherent bacteria. The resulting sonicate-fluid was cultured and microorganisms identified. RESULTS: Sonicate-fluid culture (SFC) detected MSCC in 96.6%. A total of 422 microorganisms were identified; i.e., on average 2.5 microorganisms per colonised catheter. Fifty-four percent were gram-negative while 43% were gram-positive and 3% fungi, respectively. SFC observed single microbial growth in 13.6 % and multiple growths in 84.4 %. Enterobacteriaceae were most commonly isolated (38.2%), followed by Enterococcus spp. (22.5%) and Pseudomonas aeruginosa (8.5%). Escherichia coli (51.6%), Klebsiella pneumoniae (14.9%) and Proteus spp. (11.2%) were the most frequent detected pathogens within the group of Enterobacteriaceae. CONCLUSIONS: Microbial suprapubic catheter colonisation (MSCC) is common. Technical innovations to prevent MSCC associated UTI are most likely to be effective if they are based on a solid understanding of the pathogens involved. Therefore the detailed findings of our sonication study may be helpful to improve (i) the development of new biomaterials that reduce biofilm formation, (ii) the addition or impregnation of antimicrobial agents on catheter materials and (iii) the use of probiotics to delay or prevent MSCC and associated complications.
Urology Department, Royal Brisbane and Women's Hospital, Brisbane, Queensland, Australia
Introduction: Photoselective vaporization of the prostate (PVP) is an established treatment for bladder outlet obstruction due to benign prostatic hyperplasia. Three commercially available versions of PVP technology including the 80W potassium titanyl phosphate (KTP) laser, the 120W lithium triborate (LBO) laser and the more recent 180W LBO laser are available. Purpose: The objective of this study was to evaluate the impact of changes in PVP technology on the energy utilisation. Methods: The 80W KTP, 120W LBO and the new 180W LBO 532nm lasers were used for PVP. From March 2005 until March 2011 a database of PVP procedures performed by a single surgeon in Sydney, Australia was compiled. Prostate Volumes were measured pre-operatively. Lasing time and laser energy recordings were made intra-operatively. The data was analysed to define the mean energy used and the mean laser time, per prostate and per gram of prostate across the three versions of PVP technology. T-Test statistical comparisons were performed.Results: We analysed 99 80W KTP, 330 120W LBO, and 39 180W LBO laser procedures. Laser device data comparison, from 80W KTP to 120W LBO to 180W LBO, confirmed that mean laser time per gram of prostate decreased for all prostate volumes and mean energy used increased for almost all prostate volumes. T-Test comparisons showed statistical reductions in mean laser time per gram and increases in mean energy used.Conclusion: Our data shows that with new advances in laser technology, the energy used in resection increased, possibly providing a more efficient resection.
BR04: Basic, Urolithiasis 2
School of Nursing, The Hong Kong Polytechnic University, Hong Kong
Aim: To investigate how melamine affects renal tubular cells in culture for its damage, oxidative stress, inflammatory response and gene expression. Method: A two-compartment transwell culture model was used to establish intact monolayer of human tubular WT 9-12 cell line with tight junction. Crystallization of melamine cyanurate was allowed directly on the apical side of the monolayer to mimic the situations in the nephrons, and hence to study the cellular response.
Results: Direct cytotoxic effects were demonstrated in a concentration-dependent manner, whereby about 15-25% of the intact cells were injured by the physical contact of crystals formed by melamine and cyanurate at 1:1 and 99:1 (clinical relevant) ratios. Oxidative DNA damage, as measured in terms of 8-OHdG, only occurred in cells treated with 1:1 ratio. The exposure of melamine cyanurate mixture also induced the secretion of inflammatory cytokines include IL-5, IL-6, IL-8, and MCP-1, whereas the corresponding gene expression for such cytokines were revealed by the whole human genome 44K gene expression microarray. In addition to inflammation, cluster analysis of microarray results shown that genes involved in calcium-gated channels and zinc finger proteins were mainly affected by the crystals.
Conclusion: Unlike the lithiasis event involved in calcium oxalate and phosphate, long-term impact on the cells seems to be limited as melamine induces cell damage by physical means, evoking immune cells recruitment to site of injury.
The Stone Centre at Vancouver General Hospital, Department of Urologic Diseases, University of British Columbia, Vancouver, Canada
Purpose: Bacterial adhesion to and colonization of indwelling ureteral stents is believed to be promoted by the presence of a urinary conditioning film. We identified urinary conditioning film components on stents and determined their role in promoting bacterial adhesion and colonization. Methods: Polaris (Boston Scientific) and InLay stents (Bard) removed from patients, and stent pieces incubated in urine for up to 72 hours were analyzed for adherent proteins via Quadrupole Time of Flight Spectrometry. Stents Removed from Patients were incubated with Escherichia coli C1214 and Staphylococcus aureus Newman to determine bacterial adhesion in the presence of a conditioning film. Results: The most common proteins found on Polaris (n=24) and InLay (n=20) stents removed from patients included: Cytokeratins, Serum Albumin, Hemoglobin subunit alpha/beta, Uromodulin, Protein S100A9, Fibrinogen (alpha/beta/gamma chains), Vitronectin, and Apolipoprotein. Significantly less Polaris stents were found to contain Uromodulin (p=0.002) and Fibrinogen gamma chain (p=0.026) than InLay stentsIn temporal experiments with patient and control urine, keratins formed a base layer on the surface of stents, however stents incubated with patient urine also contained hemoglobin. When testing bacterial adhesion and colonization to conditioning film containing stents no increased effect of conditioning film deposition was found on bacterial colonization by uropathogenic bacteria. Conclusions: The conditioning film components of indwelling ureteral stents do not differ between stent types and patients, and the majority are known binding sites for bacteria. Despite this, conditioning films may not play a significant role in bacterial colonization and biofilm formation over time.
PCNL for Pediatric Complex Renal Calculi
INTRODUCTION: Treating complex renal calculi with large stone burden in pediatric population is a challenging task.PCNL remains the mainstay for large burden urolithiasis. We report our experience of PCNL monotherapy in managing such calculi. MATERIAL & METHODS:54 renal units treated with PCNL monotherapy were included. Average age of patients was 6.8 years ( 8 months to 16 years). There were 25 staghorn and 29 multiple complex calculi . Average size of calculus was 2.4 cm (1.2 cm to 3.8 cm). PCNL was carried out with USG &/or guided peripheral calyceal punctures, minimum tract dilatation (16Fr) use of pediatric slender nephroscope (18 Fr) and ureteroscope(8 fr). To achieve clearance, 3 tract required in 8 cases; 2 tracts in 19 and 1 tract in 18 cases. RESULTS: Complete clearance achieved in 52/54 units requiring single stage in 38 two stage in 12 three stages in 4 . Average Hb drop was1.8 gm%, nonee requiring transfusion except one. Average hospital stay was 5 days ( 3-13 days) . Post operatively 5 had minor urine leak from tract (only 1 required stenting); Pyrexia in 7 patients. CONCLUSIONS: We believe that with experience and alterations in standard technique of PCNL makes PCNL monotherapy, a safe, feasible and effective option for managing complex pediatric calculi. This also enables complete clearance with single hospital stay and minimum morbidity.
Treatment of Forgotten Ureteral Stents: How Much Does It Really Cost? A Cost-Effectiveness Study in 27 Patients
Purpose: Aim of study was to present costs of forgotten ureteral stents extraction so as to distract attentions of the urologists on this issue. Materials and Methods: Medical files of 27 accessible patients who referred to our clinics between 2001 and 2010 because of forgotten ureteral stent were retrospectively analyzed. The indwelling time of DJS was calculated from the time of its insertion. Costs related to radiological investigations, all invasive, and noninvasive interventions, duration of hospital stay, and medical treatments used were calculated. These estimations were based on 2010 prices determined by Turkey Ministry of Health. Results: Mean age of the patients was 31.2 (8-86 years) years. Mean indwelling time of ureteral DJSs was 36.7 months (14-84 months). Seventy-one (SWL, n=26; invasive/noninvasive interventions, n=32) procedures were applied for 27 patients. In 6 patients without incrustation, after a single session of SWL DJSs could be removed cystoscopically. A various combination of a multimodal therapy were used for other 21 patients. Total financial burden of 27 patients was 34300 US $. Cost of treatment was estimated to be 6.9-fold (1.8-21-fold) higher than an average timely stent extraction. Financial burden of the treatments increased in parallel with the duratin of the stent retention (p=0.001).Conclusion: Management of FUS is time consuming, difficult, complicated, risky, and costly. Threfore; financial burden, increased labour loss, and impaired quality of life brought by the application of these modalities must not be forgotten.
Retro-Renal Colon: is it an Acquired Anomaly?
Introduction: Retro renal colon (RRC) is considered one of the risk factors for colonic injury during percutaneous nephrolitotomy (PNL). An attempt was made to find if this is a congenital defect or an acquired anomaly?Method:Incidence of RRC was assessed in more than 1200 CT scans performed for non-urologic causes. Literature review was performed to look for colonic diseases like malignancies in RRC. A retrospective analysis was performed of 5 colonic injury instances that happened during PNL.Results:No case of RRC was found in review of the 1200 CT scans. There is no reference of any colonic disease in RRC in literature. All 5 patients who had a colonic injury had a long-standing large hydronephrosis that was initially drained by either a nephrostomy or a DJ stent. Colonic injury happened in the 2nd stage PNL. Our hypothesis:The colonic mesocolon lengthened over the gradually dilating obstructed kidney. Once the kidney was de-obstructed, the kidney reduced in size but the long mesocolon persisted. The colon with the long mesocolon dropped posterior to kidney forming a RRC. Conclusion:RRC is an acquired anomaly and not a congenital one.
Hemostatic Sealants in Percutaneous Nephrolithotomy: The Effect on Renal Drainage and Histology in an Experimental Porcine Study.
Introduction: Concerns that tubeless percutaneous nephrolithotomy (PCNL) is risky in case of a potential postoperative bleeding due to the lack of drainage, have lead to the introduction of methods of additional hemostasis of the nephrostomy tract including the use of hemostatic sealants. Purpose:In this work the midterm effects of hemostatic sealant application in the histology of the nephrostomy tract and the penetrated renal unit are assessed in an in-vivo study in pigs.Materials and Methods: Bilateral percutaneous access was established in 28 porcine renal units. At the end of the procedure 3 common hemostatic agents (Helisorb, Tachosil, Floseal) were randomly placed on the nephrostomy tracts. Computer tomography was performed on postoperative days 1, 15, 30 and 40 to access renal drainage. On postoperative day 40, all animals were sacrificed and both their kidneys and cutaneous parts of the nephrostomy tracts were harvested for histological evaluation.Results: Evidence of risk for drainage occlusion was revealed luckily avoided in all subjects but one in the Tachosil group. Significant histological lesions in the renal parenchyma were revealed in all cases of sealant application inside renal units. Observed histological reaction was not sealant specific and all three sealants could induce significant histological deterioration in the nephrostomy tract. Conclusions: The safeness of application of hemostatic sealants in PCNL must be reassessed focusing not only on the potential of such materials to occlude urinary drainage but on their effect on renal histology as well. Further investigation is considered necessary.
Efficiency of RIRS in the Staghorn Nephrolithiasis Treatment.
Introduction: Alternative treatments for staghorn nephrolithiasis are gaining in popularity, along with expanding the possibilities of modern endoscopic urology. Materials and Methods: To 34 patients with staghorn kidney stones was performed URS. The average size of concretions was 4.5 cm. To provide each URS we used UAC, semirigid and flexible ureteroscopes. After the operation, all patients drained by JJ- stent for 1 month. Results: At follow-up examination in 21 patients, there were no clinically significant residual fragments of stone. 9 patients underwent of ESWL about residuals. In URS of 2 men installing of UAC enclosure failed, so them was installed JJ- stent and after 1 week of passive dilatation performed a planned operation. Low efficiency of RIRS of men in 6 cases were caused by the impossibility of bringing housing to UPJ, which significantly reduced the destruction and removal of fragments of stone. The most significant complication of the method was the exacerbation of chronic pyelonephritis in 6 patients. Clinically significant bleeding in the perioperative period were noted. Conclusion: Thus, RIRS is quite effective and less invasive method of treatment of staghorn renal stones and allows 61% of patients completely free of residual stones. The lower risk of complications, the method is a reasonable alternative to PCNL. However, it must improve transurethral treatments for staghorn nephrolithiasis, which will in the future to resolve most issues related to complications and failures in the performance of conventional methods of treatment of such patients.
The Cleveland Clinic
Objective: To evaluate the safety of a novel ureteral occlusion device and compare its performance to other devices and guidewires.
Methods: The XenX (Xenolith Medical) was tested in an ex vivo porcine model to determine the percent denuded urothelium as a result of manipulation within the ureter, the capacity to prevent stone migration during laser lithotripsy, stent compatibility, and ability to be used for stent placement. Comparative evaluations of insertion forces and maneuverability were conducted in an in vitro ureter model with the XenX, Stone Cone (Boston Scientific), N-Trap (Cook Urological), HiWire (Cook Urological), Roadrunner (Cook Urological), and Sensor (Boston Scientific). Stone migration efficacy was conducted using a controlled distribution of stones in 4 and 10 mm silicone tubing with the XenX, N-Trap, and Stone Cone.
Results: The XenX was safely manipulated within the ureter, prevented significant particle migration during laser lithotripsy, and effectively placed stents. The N-Trap required the greatest force when attempting to navigate past a stone (p=0.0003), followed by the Stone Cone (p=0.009), with little difference among other devices (p=0.72). No differences were found for passing forces (p=0.061), time to pass (p=0.30), or number of attempts to pass stone (p=0.68). The XenX prevented the most stone migration, with more notable differences in 10 mm than 4 mm tubing.
Conclusion: Ex vivo evaluations hold promise for the XenX to be safely and effectively used during ureteroscopic procedures. Clinical evaluations are warranted to confirm the safety and performance of the XenX relative to other ureteral occlusion devices.
University of Sydney, Australia
Objective: Prostate cancer is the most common male urological malignancy in the developed countries. With our ageing population, prostate cancer will continue to be one of the major healthcare concerns because of the increasing incidence of prostate cancer with advancing age. We studied whether local treatments of the primary prostate cancer give palliative benefit to men who later develop castrate resistant prostate cancer (CRPC). Local treatments of primary prostate cancer are defined as radical retro-pubic prostatectomy (RRP) or external beam radiation (XRT). Methods: We reviewed the patient records in 5 different hospitals in Sydney, Australia and identified 263 men who have CRPC. Eligible patients were men who had progressive disease during androgen deprivation therapy with castrate levels of testosterone. Clinical and pathological data were reviewed and evaluated in Chi-square and relative risk to determine the relationship between previous local prostate treatment and complications secondary to local disease. The end point was complications and morbidity attributed to cancer progression locally (from the prostate). Results: Primary prostatic treatment by either RRP or XRT significantly reduces the incidence of local complications compared to no primary treatment (31.5% v 54.6% p<0.001). In addition, RRP demonstrated a significantly lower level of local complications compared to XRT ( 17.8% vs 46.7% p=0.003). The most common local complications were bladder outlet obstruction (34.2%) and ureteric obstruction (15.2%).Conclusion: This retrospective analysis supports the hypothesis that primary local prostatic treatment gives palliative benefit to men who later develop CRPC. RRP gives the greatest reduction in local complications.
Determination of Patient Radiation Dose During Ureteroscopic Treatment of Urolithiasis Using a Validated Model
IntroductionEffective dose is a way to relate absorbed radiation dose and risk of malignancy.Purpose We measured organ radiation dose rates and determined effective dose rates (EDR) during a simulated ureteroscopy (URS) using a validated model. We calculated the effective dose (ED) for ureteroscopyat our institution.Materials and MethodsAn anthropomorphic male phantom was placed on a fluoroscopy table and underwent a simulated URS. High sensitivity metal oxide semiconductor field effect transistors (MOSFET) dosimeters were placed at 20 organ locations and used to measure organ radiation doses. These dose rates were multiplied by their appropriate tissue weighting factor and summed to calculate the EDR. A retrospective review of patients undergoing ureteroscopy at our institution was performed. A total of 30 non-obese males with data on fluoroscopy time were included. The median ED was determined by multiplying the median fluoroscopy time by the EDR.ResultsThe skin entrance was exposed to the highest absorbed dose rate (0.3286 mGy/sec), followed by the small intestine (0.1882 mGy/sec) and gallbladder (0.1221 mGy/sec). The EDR for ureteroscopy was 0.024 mSv/sec. The median fluoroscopy time was 46.95 sec (12.9−298.8). The calculated median ED was 1.13 mSv (0.31 - 7.17). ConclusionFLuoroscopy used during ureteroscopy contributes to the overall radiation exposure in patients with nephrolithiasis. Non-obese males are exposed to a median of 1.13 mSv during ureteroscopy, similar to that of an abdominal/pelvic x-ray. Though more data is needed to determine clinical implications, urologists need to be aware and reduce patient radiation during URS.
Ocular Radiation Exposure in Urologic Practice
INTRODUCTION: Urologists are subject to radiation exposure during their work day. Safety precautions and judicious use of fluoroscopy minimizes undo radiation exposure. Eyes are highly radiosensitive but is often left unprotected. The typical sequela of radiation exposure to the eye is cataract formation. The minimum acute radiation dose required to initiate cataract formation is roughly 200rads (1 rad=1 rem) and the minimum fractionated long term dose is 250-650rads. Objective: Report radiation exposure received near 1 eye during common endourological cases.METHODS: Radiation badges were worn near the eye of 6 Urologists during endourologic procedures. Safety measures included; lead aprons and maximizing distances from the radiation source. No surgeon wore lead lined glasses. The procedures performed ranged from stent insertion to ureteroscopic lithotripsy or percutaneous nephrolithotomy. Radiation doses required to potentate formation of cataracts were calculated.RESULTS: 22 procedures were evaluated, including 13 ureteroscopic cases and 5 ureteral stent insertions. The mean dose received during these cases was 0.0246 (0.005-0.066)rads. Based on this and an average of 20 such cases per month it would take 42 years to reach the minimum threshold and 110 years to reach the maximal threshold for cataract formation. 4 percutaneous renal surgeries resulted in a mean dose of 0.00925 (0.004-0.018)rads. Based on 10 cases per month this would require 225 years to reach the minimal threshold.CONCLUSIONS: The eye is radiosensitive and often exposed during endoscopic cases. However, the lifetime exposure of Urologists would likely not necessitate safety precautions such as lead lined glasses.
Division of Urology, Duke University Medical Center, Durham, NC, USA
IntroductionPatients with nephrolithiasis are at increased risk for radiation exposure from computed tomography (CT) scans. The amount of radiation these patients are exposed to from a CT scan is poorly defined.PurposeTo measure organ specific radiation doses and determined the effective dose for a non-contrast CT abdomen/pelvis for the evaluation of nephrolithiasis performed at our institution.Materials and MethodsAn anthropomorphic male phantom was placed on a General Electric 64 slice VCT CT scanner. A non-contrast CT abdomen/pelvis was performed with the following settings: Tube voltage 120 kV, tube current 700 mA, pitch 1.375:1, noise index 17.5, images 80. High sensitivity metal oxide semiconductor field effect transistors (MOSFET) dosimeters were placed at 20 organ locations and used to measure organ radiation doses. The organ doses were multiplied by their tissue weighting factors and summed to determine the effective dose (ED).ResultsThe pelvic bone marrow was exposed to the highest absorbed dose (7.37 mGy), followed by the skin entrance (7.23 mGy) and bladder (6.60 mGy). The ED for the CT was 3.04 mSv. ConclusionRadiation from CT scans contributes to the overall radiation exposure for patients with nephrolithiasis. A non-contrast CT performed for the evaluation of nephrolithiasis results in an effective dose of 3.04 mSv. This is approximately equal to the radiation from 3 abdominal/pelvic x-rays. Accurate determination of ED enables patients and clinicians to make more informed decisions regarding CT imaging and allows calculation of cumulative ED in this at risk patient population.
Division of Urology, Duke University Medical Center, Durham, NC
IntroductionAcoustic Radiation Force Impulse (ARFI) imaging is a novel, ultrasound-based imaging that generates images of tissue stiffness. Purpose:To compare visualization of ureteral stones in B-mode, ARFI and CT in a phantom model.Materials and MethodsA conical Begostone phantom (7.5mm long with a 5.7mm base diameter) was placed in a 6.5 cm x 7 cm cylindrical gel phantom model. B-mode and ARFI imaging was performed using a Siemens VF7-3 transducer imaging at 5.3 MHz. CT was performed on a 64-slice GE scanner with settings of 120 kVp and 100 mA. Stone sizes were measured using both techniques. ResultsFigure 1 shows images of the stone phantom. The colorbar represents microns of displacement in the ARFI image. ARFI image demonstrates decreased displacement and decorrelation in and deep to the stone; these image features can be used to identify the stones even if they are isoechoic in the B-mode image. The length of the stone was 5 mm in B-mode and 7 mm in ARFI.ConclusionsThese results suggest that ARFI can significantly improve the sensitivity of ultrasound to detect small ureteral calculi. This may reduce the need for CT and radiation exposure in patients with nephrolithiasis.
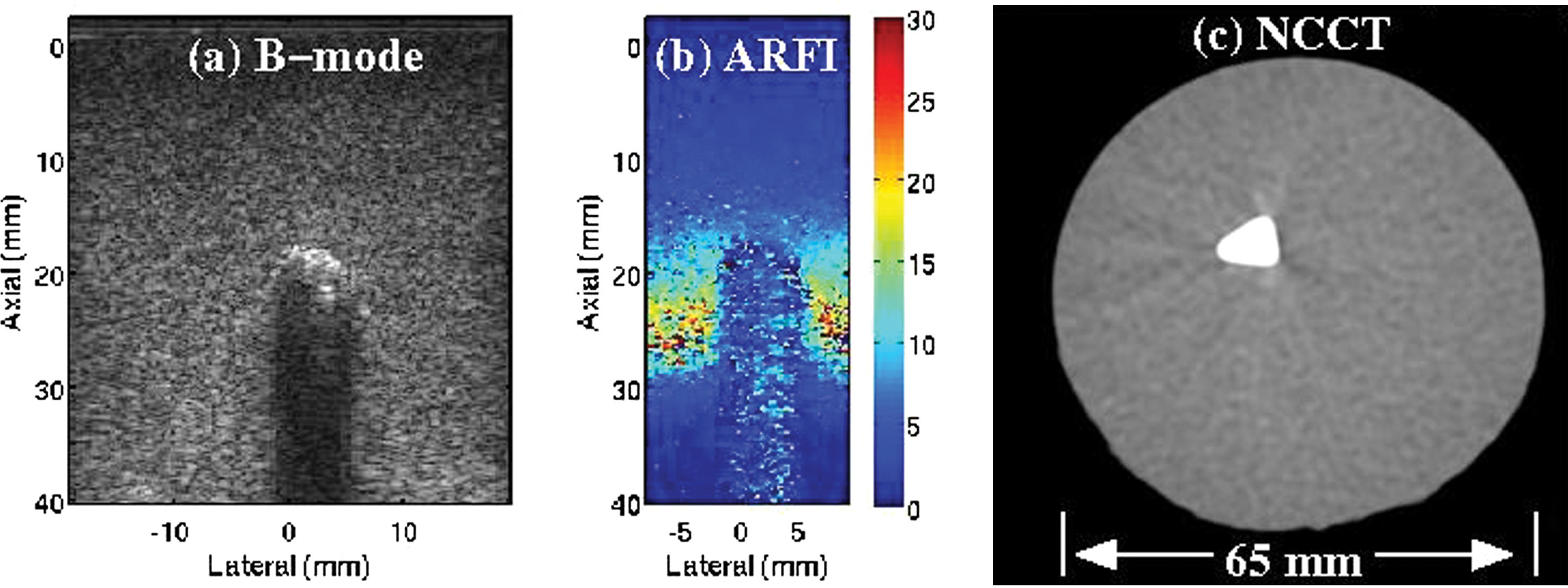
Organ Specific Radiation Dose Rates and Effective Dose Rates During Percutaneous Nephrolithotomy
IntroductionIt is difficult to determine actual radiation dose based on fluoroscopy time alone. PurposeWe determined organ radiation dose rates and calculated effective dose rates (EDR) during right and left percutaneous nephrolithotomy (PNL) using a validated phantom model.Materials and MethodsAn anthropomorphic adult male phantom was placed prone on an operating room table. Metal Oxide Semiconductor Field Effect Transistor (MOSFET) dosimeters were placed at 20 organ locations in the model. A portable C-arm was used to simulate a left and right PNL. Organ dose rate was determined by dividing organ dose by fluoroscopy time. The organ dose rates were multiplied by their tissue weighting factor and summed to determine EDR. ResultsThe EDR for a left sided PNL was 0.021 mSv/s and 0.014 mSv/s for a right sided PNL. The skin entrance had the highest organ dose rate during left and right PNL, 0.24 mGy/s and 0.26 mGy/s respectively. The stomach (0.07 mGy/s) and the gallbladder (0.12 mGy/s) were exposed to the second greatest amount of radiation on the left and right respectively. ConclusionThe effective dose rate is higher for a left sided PNL. Effective dose is a way to relate absorbed radiation dose and risk of malignancy. Further studies are needed to determine the long term implications of these radiation doses.
MP01: LESS/NOTES 1
Retroperitoneal Laparoendoscopic Single-Site Adrenalectomy
Introduction The feasibility, safety and advantages and disadvantages of retroperitoneal laparoendoscopic single-site surgery (LESS) need to be evaluated. Purpose To verify the safety and feasibility of applying retroperitoneal LESS adrenalectomy in the treatment of adrenal gland tumors. Materials and Methods From Sept. 2010 to May 2011, 6 patients underwent retroperitoneal LESS adrenalectomy. The mean patient age was 50 (23-71 yrs). The mean body mass index (BMI) was 25.1 kg/m2. There were 2 tumors in the left and 4 in the right. All operations were performed through retroperitoneal approch by using QudaPort (Olympus), tip filexible laparoscope with 0 degree lens (EndoEYE 5mm (LFT-VP), Olympus) and conventional laparoscopic instruments. We evaluated this technique in operative time, estimated blood loss, intraoperative complications, drainage time, post-operative pain score (VAPS), post-operative hospital stay and pathological results. Results 6 cases of LESS adrenalectomy were performed successfully without additional trocar added and conversion to standard laparoscopic or open adrenalectomy. The operative time was 111 (70-180 min), the estimated blood loss was 65 (5-200 m1), first post-operative day VAPS was 1.5 (0-3), post-operative drainage time was 2.1 (2-3 days) and post-operative hospital stay was 4.8 (3-6 days). No perioperative complication was observed. Pathological results showed 4 cases of adrenal cortical adenoma, 1 case of adrenal pheochromocytoma and 1 case of adrenal cyst. Conclusions Retroperitoneal LESS adrenalectomy is safe and feasilbe. The current known advantages of this technique are cosmatics and post-operative pain control.
Initial Experience with Laparoendoscopic Single-site Adrenalectomy for the Management of Pheochromocytomas
Background: To describe our initial experience and report the feasibility of laparoendoscopic single-site (LESS) adrenalectomy for the treatment of pheochromocytomas, comparing the perioperative outcomes to conventional laparoscopic adrenalectomy (LA).Methods: A total of 25 patients underwent LESS adrenalectomy or LA for clinically diagnosed pheochromocytoma between November 2008 and May 2011 at our institution. After exclusion of two patients with bilateral pheochromocytomas and four patients with tumors larger than 5 cm, 14 patients remained for analysis; seven patients were included in each group (LA group and LESS group). All clinical and surgical data of the LESS group, including tumor size, operative time, occurrence of intraoperative hyper- or hypotension, complications, and conversions, were compared to those of the LA group.Results: Preoperative parameters did not differ significantly between the two groups. There were two cases of conversion to conventional laparoscopic surgery in the LESS group. There were no significant differences in operative time, estimated blood loss, or hospital days between the groups. Intraoperative hypertension occurred once in the LA group and five times in the LESS adrenalectomy group. There was one case of postoperative hypertension that required medication. Other postoperative complications were not observed.Conclusions: LESS adrenalectomy for pheochromocytoma is technically feasible. However, care must be taken to minimize intraoperative hemodynamic events.
Feasibility and Efficacy of Retroperitoneal and Transperitoneal Laparoendoscopic Single-Site Adrenalectomy: Initial Experience
Introduction: By combining trocar sites and extraction incision, Laparoendoscopic Single-site Surgery (LESS) may provide less morbidity than traditional laparoscopy. Concerns continue about LESS for complex reconstructive and ablative procedures. Purpose: We examined our experience with LESS-adrenalectomy.Materials and Methods: Since 5/209, eight patients (4 M/4 F, mean follow up 10.9 months) underwent LESS-adrenalectomy. Umbilical or sub 12th rib single-site access were employed for transperitoneal or retroperitoneal LESS, respectively. LESS-adrenalectomy duplicated principles of laparoscopic adrenalectomy, with careful dissection of gland from surrounding tissues, control of the adrenal vein/accessory vessels, and intact specimen extraction. Demographics, perioperative, and postoperative data were recorded.Results: LESS-adrenalectomy (2-Left/6-Right, 3 transperitoneal/5 retroperitoneal) was successfully completed in all cases. One patient, transperitoneal, required placement of an accessory 5mm port. Indications were pheochromocytoma (4), Metastectomy (2), Adrenocortical Carcinoma (1), and Aldosteronoma (1). Median age was 55 years. Median Body mass index was 28.9 Kg/m2. Mean tumor size was 4.3 cm. Mean operative time was 165.7 minutes. Mean estimated blood loss was 110.7 mL. Median incision length was 3.5 cm. There was no significant difference between mean preoperative and discharge hemoglobin (g/dL) (13.7 vs. 13.4, p=0.673). Mean length of hospital stay was 44.6 hours, mean discharge pain score was 0.7, and median discharge morphine equivalents was 2 mg. There were no perioperative complications. Pathology confirmed negative margins in all. Conclusion: LESS adrenalectomy is feasible and safe, with reproducible and favorable perioperative and short-term outcomes in selected patients. Further study and comparison to multiport adrenalectomy is requisite.
Laparoendoscopic Single-Site Surgery Application in the Elder People with Any Urological Tumors
Objective To verify the safety and feasibility of applying laparoendoscopic single-site surgery (LESS) in the treatment of elder patients with urological tumors. Medthods From Aug. 2010 to March 2011 we had used LESS technique to treat 5cases of prostatectomy 3 cases of nephrectomy and 4 cases of adrenalectomy. Quadport was inserted through a transumbilical incision. Standard laparoscopic instruments and flexible tip 5mm laparoscope was used. Application of Quadport reduced the clash of instruments. Step by step performing surgery and avoiding blunt dissection reducing intraoperative bleeding is the cornerstone of success. We evaluated this technique in respects of operative time, estimated blood loss, intraoperative complications, drainage time, post-operative pain score (VAPS), post-operative hospital stay and pathological results. Results All the procedures in this group were completed successfully with LESS technique. There was no additional trocar added, no conversion to standard laparoscopic or open surgery. The operative time 192±76.7 min,estimated blood loss were 174.6±167.2ml. There was no severe intraoperative complication. The VAPS in the first post-operative day were 0.9±1.0.The drainage time were 3.5±1.7d,post-operative hospital stays were 7.9±3.4 d.There was no secondary bleeding or wound infection. Pathological results showed prostate cancer,renal cell carcinoma and adrenal adenoma. All the specimens in this group were surgical margin negative.
Initial Operative Experience Single-Port Retroperitoneal Laparoendoscopic Urological Surgery
Objectives: This study reports our early experience with single-port laparoscopic urologic surgery via the retroperitoneal approach. Patients and methods: Since April 2010, 23 patients have undergone single-port laparoscopic surgery for nephrectomy in 11 patients, and nephroureterectomy in 12 patients by an experienced laparoscopic surgeon. Results: The mean operative time for patients undergoing nephrectomy was 265.2 minutes, and 241.5 minutes for patients undergoing nephroureterectomy. The mean estimated blood loss (EBL) was 89.5 mL and 168.5 mL, respectively. No intraoperative or acute postoperative complications occurred. The mean length of hospitalization was 10.2 days and 11.5 days, respectively. No evidence of remote complications or compromised surgical outcomes was noted. When the single-port retroperitoneal laparoendoscopic surgery group was retrospectively compared with the group who had undergone standard retroperitoneal laparoscopic surgery, no significant difference was noted with respect to age, body mass index, EBL, operation time, or length of hospitalization. A significant difference in favor of the single-port retroperitoneal laparoendoscopic surgery group was noted with respect to the visual analog pain scale score at discharge (p=0.016). Conclusions: Although our results on retroperitoneal single-port laparoscopic surgery demonstrate that the technique is feasible with advanced skills and optimal instrumentation, further study is needed to determine the true benefits of the technique and the extent of its clinical application.
Laparoendoscopic Single-Site Surgery for Pyelolithotomy and Ureterolithotomy (Report of 24 Cases)
IntroductionLaparoendoscopic single-site surgery (LESS) might be desired as a primary or salvage therapy for some stones in upper urinary tract.Purpose: To evaluate the transumbilical LESS (U-LESS) for pyelolithotomy and ureterolithotomy. Materials and Methods A total of 24 patients with renal pelvic or ureteral calculi underwent U-LESS on 26 sides. Of them 10 were women and 14 were men. The calculi were found on left side in 9 cases, on right side in 13, and on both sides in 2. Renal pelvic calculi occurred in 2 cases, upper ureteral calculi in 22. In these patients, 4 patients had experienced unsuccessful extracorporeal shock wave lithotripsy (ESWL), 1 unsuccessful ureterolithotripsy (URL), 1 ureteral perforation during URL. Under general anesthesia, the patients were positioned in lateral decubitus with affected side elevated. Three 5- mm trocars were inserted into the abdomen cavity at the medial margin of umbilicus. The method for pyelolithotomy and ureterolithotomy was same as the standard laparoscopy.Results All procedures were successfully performed. The unilateral operative time was between 65 and 145 min with a mean of 80 min. The bilateral operative time was 205 and 160min, respectively. The intraoperative mean estimated blood loss was 30 ml (range 15 to 45 ml). There was no major complication during perioperation. During the follow-up (6 to 12 months), the incision at the umbilicus was not obvious, and no recurrent calculus and ureterostenosis was found. Conclusions The U-LESS for pyelolithotomy and ureterolithotomy was safe, feasible and cosmetic.
Laparoendoscopic Single-Site Surgery Radical Nephrectomy
Objective: To present our experience and assess the feasibility of Laparo-endoscopic single-site(LESS) radical nephrectomy.Patients and Methods: Since June, 2010, we have performed single-port laparoscopic radical prostatectomy in 10 patients clinically diagnosed with renal cell carcinoma. All procedures were performed through a single intra-umbilical X-cone port. The parameters analyzed were operative time, blood loss, intra- and post-operative complications and hospital stay.Results: LESS radical nephrectomy was successfully completed in nine patients. Conversion to a standard laparoscopic approach was necessary in one cases because of dense adhesions. The median (range) tumour size was 5.8 (3.7∼7.0) cm. The median (range) operating time was 207 (170∼271) min and the estimated blood loss was 114 (50∼450) mL. The median (range) hospital stay was 7(5∼9) days. There were no intra-operative and post-operative complications in 10 patients. Conclusions: LESS radical nephrectomy are technically feasible and reproducible in RCC patients if performed by surgeons with standard laparoscopic skills. A wider experience and longer follow-up are necessary to establish the role of this technique in treatment of RCC.
Techniques and Initial Experience of Laparoendoscopic Single-Site Radical Nephrectomy in One Center
Introduction The feasiblity, safty and advantages and disadvantages of laparoendoscopic single-site surgery (LESS) radical nephrectomy need to be evaluated. Purpose To verify the safety and feasibility of applying LESS radical nephrectomy in the treatment of kidney tumors. Medthods From Nov. 2010 to April 2011, we had used LESS radical nephrectomy technique to treat 3 kidney tumor cases, one right central 4.2 cm tumor and another two left lower pole 7.4 cm and 4.5 cm tumors by using QudaPort (Olympus), tip filexible laparoscope with 0 degree lens (EndoEYE 5mm (LFT-VP), Olympus) and conventional laparoscopic instruments. The standard laparoscopic transperitoneal nephrectomy technique was performed. We evaluated this technique in respects of operative time, estimated blood loss, intraoperative complications, drainage time, post-operative pain score (VAPS), post-operative hospital stay and pathological results. Results 3 LESS radical nephrectomy were completed successfully without additional trocar added and conversion to standard laparoscopic or open surgery. The operative time were 215, 230 and 170 min, estimated blood loss were 100, 100 and 150 ml. There was no severe intraoperative complication. The VAPS in the first post-operative day were 1, 2 and 2. The drainage time were 4, 3 and 2 d, post-operative hospital stays were 8, 10 and 8 d. There was no secondary. Pathological results showed that case No. 1 and 3 were renal clear cell carcinoma in pT1bN0M0 and case No. 2 was renal chromophobic cell carcinoma in pT2aN0M0, respectively. Conclusions LESS radical nephrectomy is a safe and feasible choice for the treatment of kidney tumors.
Feasibility, Advantages and Challenges of Retroperitoneoscopic LESS Nephrectomy
Objective: To evaluate the feasibility, advantages and to present the technical details of retroperitoneoscopic laparoendoscopic single-site surgery (LESS) nephrectomy Patients and Methods: Thirteen retroperitoneoscopic LESS nephrectomies (in 11 patients) have been completed for a variety of indications in a single center. The GelPOINT apparatus (Applied Medical) was used as an access platform through a 2.5 ∼ 5 cm flank incision. Except a bendable grasper and flexible vascular staplers all instruments used were conventional straight laparoscopic instruments. Peri-operative data were obtained for all patients including demographic data, operative indications, operative records, length of stay, complications, and pathologic analysis.Results: All retroperitoneoscopic LESS nephrectomy procedures attempted with the GelPOINTTM were completed successfully without complications. No extra working port was required for any case. Average operative time was 125 min and estimated blood loss (EBL) was 57 ml. Average length of hospital stay was 2 days (range: 1∼3). The mean narcotic used was 30 mg parental morphine sulfate equivalent. The mean visual analog pain scale score at discharge was 1.9 of 10 (range 0∼3). This single arm observation study is limited by small patient number and no control cohort.Conclusions: Retroperitoneoscopic LESS nephrectomy by using the GelPOINT apparatus as an access platform is feasible and safe, and provides adequate flexibility and spacing of port placements and acceptable operative outcomes. It is especially valuable for patients who need to keep peritoneal integrity or those with abnormal or obliterated peritoneal space.
Division of Urology, University of California San Diego, La Jolla, CA, USA
Introduction: Laparoendoscopic Single-site Surgery (LESS) may represent a further decrease in morbidity compared to multi-port laparoscopy (MPL). Concerns continue about LESS for complex procedures. Purpose: We compared LESS and MPL for radical nephrectomy and renal vein thrombectomy (RN-RVT).PATIENTS AND METHODS: Retrospective review of 6 patients who underwent LESS-RN-RVT (2-right/4-left) and 13 patients who underwent MPL-RV-RVT (7-right/6-left) between 1/2006-10/2010. LESS access was obtained by peri-umbilical incision through which all trocars were inserted. LESS-RN-RVT recapitulated steps of MPL-RN-RVT, including stapled renal vein thrombectomy and intact specimen extraction. Demographic factors/tumor characteristics, peri-operative variables, outcomes and complications were recorded and analyzed.RESULTS: All 13 MPL cases were successfully completed laparoscopically. All 6 LESS cases were successfully performed; one required insertion of a 5 mm port at a separate site. There were no significant demographic differences between the two groups. For LESS-RN-RVT and MPL-RN-RVT: Mean tumor diameter (cm) was 7.2 and 8.0 (p=0.437); mean operative time (min) was 161.8 and 153.8 (p=0.615); mean estimated blood loss (mL) was 141.7 and 176.9 (p=0.556). Mean pain score at discharge was significantly decreased in LESS-RN-RVT vs. MPL (1.2 vs. 2.8 p=0.02) and mean morphine equivalents (mg) was also significantly decreased for LESS (5.7 vs. 11.9, p=0.02). All had negative margins, without significant differences in complication/transfusion rates (p=0.943).CONCLUSION: In this well-matched comparison, LESS-RN-RVT is comparable to MPL-RN-RVT for select patients in terms of perioperative parameters and may confer benefit with respect to analgesic requirement. Prospective evaluation and longer-term assessment and follow-up are requisite.
Transumbilical Single-Port Laparoscopic Radical Nephrectomy by Homemade Device
Objectives: Aim of this study is to evaluate the efficacy and safety of transumbilical single-port laparoscopic radical nephrectomy by homemade device . Methods: The clinical data of laparoscopic radical nephrectomy performed from June 2010 to October 2010 in Peking University Third Hospital were analyzed retrospectively. 10 cases underwent transumbilical single-port laparoscopic radical nephrectomy (LESS) and 15 cases received retroperitoneal laparoscopic radical nephrectomy. Data on general presentation, tumor size, tumor location, operative time, blood loss, complications, Visual Analog Pain Scale (VAPS), postoperative hospital stay, pathological results were collected to compare between two groups. The LESS approach used our homemade single-site equipment(Fig),the kidney was dissociated after cut off the renal vessel and extracted through the umbilical incision. The retroperitoneal approach followed the standard surgical procedures, the specimens were removed from the extended incision. Results: All procedures were completed without conversion to open radical nephrectomy. Compare with traditional laparoscopic surgery, operative time and VAPS show significant difference in LESS group,and no difference was noted in other factors (P>0.05). There was no secondary bleeding, wound infection, intestinal obstruction, incision hernia and other severe postoperative complication. Conclusions: Transumbilical single-port laparoscopic radical nephrectomy is feasible, effective and safe. It gives a more mini-invasive and cosmetic option for young or female patients. The characteristics of lower-cost,more aesthetic,repeat use of the device appeared o be popularized.
Comparative Study on Operative Costs of Laparoendoscopic Single-Site and Conventional Laparoscopic Radical Nephrectomy for Localized Renal Cell Carcinoma
Introduction: No economic evaluation of laparoendoscopic single-site (LESS) and conventional laparoscopic radical nephrectomy (CLS) is available.Purpose: We aimed to assess and compare the economic burden of LESS and CLS for localized RCC.Materials and methods: A total of 20 patients (LESS n=10; CLS n=10) with cT1-2 RCC were enrolled in this prospective, randomized study. An economic evaluation was made to estimate all relevant costs and an incremental cost-effectiveness ratio (ICER) per improved postoperative recovery of the patients.Results: No significant differences were observed in patient characteristics, surgical outcomes, and pathologic outcomes. However, postoperative quality of recovery measured by QoR-40 scores was higher in the LESS group compared with the CLS group (173 vs. 146, p=0.037). Despite a higher cost of multichannel port and flexible laparoscopic instruments, the overall costs were comparable between LESS and CLS groups (5,079,224 vs. 4,868,990 Korean Won (KW), p=0.722). Also, the operating room costs, anesthesia costs, medication costs, lab costs, and room and board costs were not significantly different between two groups. The ICER per improved postoperative recovery of the patients was 7,508 KW using LESS.Conclusions: Despite all the challenges related with adoption of new technology, LESS radical nephrectomy showed comparable surgical outcomes and cost-effectiveness with CLS in patients with localized RCC.
Patient-Reported Cosmesis Outcomes Following Laparoscopic Adrenalectomy; LESS vs. Conventional Surgery
Introduction: Laparoendoscopic single site surgery (LESS) continues to gain prevalence in urology, with reported equivalent perioperative outcomes and superior cosmesis to conventional laparoscopic surgery (CLS).Purpose: The purpose of this study was to evaluate patient-reported satisfaction and cosmesis of LESS in comparison with that of CLS in Japanese.Materials and Methods: A total of 15 and 103 patients who underwent LESS and CLS between May 1996 and January 2011 were included in the study. Questionnaires inquiring about scar pain (0: not painful, 10: very painful), satisfaction (0: not satisfied, 10: very satisfied), and cosmesis (0: very ugly, 10: very beautiful) on the basis of a visual analogue scale that was sent to patients postoperatively. Results: Eleven (4 men and 7 women) and 51 (24 men and 27 women) patients who underwent LESS and CLS, respectively, responded. The mean follow-up times after surgery were 64.9 (range 18-181) and 11.4 (range 5-19) months for the CLS and LESS groups, respectively (p<0.01). There was no significant inter-group difference in age, male-to-female ratio, affected side, BMI, and blood loss. Insufflation time was significantly longer in the LESS group than the conventional group (229 vs. 191 min, p=0.03). There was no significant difference in pain (0.73 vs. 0.57, p=0.64), satisfaction (8.82 vs. 8.43, p=0.63), and cosmesis score (8.55 vs. 7.96, p=0.51).Conclusions: No significant difference was obtained in patient-reported cosmesis following LESS and CLS. Further evaluation is needed by longitudinal study to clarify whether LESS is superior to CLS in terms of cosmesis.
Analysis of Factors that Influence Patient Concerns for Cosmesis and Preference for LESS
Introduction: Laparoendosocopic single-site surgery (LESS) can potentially improve surgical cosmesis and recovery over standard laparoscopy (SL), though it is more challenging to perform.Purpose: To identify factors that influence patient concerns for various surgical outcomes and there subsequent preference for LESS.Methods: Patients followed after a laparoscopic procedure completed two surveys. First, patients rated the importance of pain, recovery time, cost, treatment success, scars, and complications (5-point Likert Scale). Additionally, they were asked their preference for LESS. The second survey assessed impact of scars on body image and cosmesis. Results: 79 patients (median age 54.8y, 65% male and 35% female) were treated for malignancy (53), donation (15), and benign indications (9). Treatment success (4.71±0.81) and complications (4.22±1.16) were most important, followed by pain (3.43±1.21) and convalescence (3.65±1.11), p<0.05. Cost was rated 2.68±1.38, and cosmesis was 2.22±1.13 (p<0.005). Cosmesis score increased in females (2.59±1.08 vs 2.02±1.12), patients under 50y (2.59±1.09 vs 2.02±1.12) and benign surgical indication, (3.33±1.12 vs 2.07±1.06), p<0.05. LESS was preferred in 30.4%, SL in 39.2%. Concern for cosmesis was associated with LESS preference (48.5% vs 17.8%, p=0.004). Female gender (38.5% versus 27.5%), younger age (35.7% versus 28.6%), and benign surgical indication (48.5% versus 17.8%) were associated with preference for LESS (p>0.05). On the body image scale, patients scored a mean 18.8±1.5 out of 20. Patients rated scar appearance 8.31±1.80 out of 10.Conclusion: Patients treated with laparoscopy were most concerned with success and complication. Preference for LESS was influenced by concern for cosmesis, gender, age, and surgical indication.
Department of Urology, Aberdeen Royal Infirmary, Scotland, UK
Introduction: New surgical techniques like NOTES and LESS help to decrease invasiveness of surgery. Our study analyses public preference, which will help us to establish the demand for such techniques and guide future resource allocation. Material and Methods: A questionnaire-based face-to-face study noting public preferences between different available surgical options were recorded along with their choices for new innovative techniques. It comprised of four questions based upon a hypothetical scenario of kidney disease (non-functioning and cancer). Patients were asked to rate the preference from 1 (most preferred option) to 4 (least preferred option) for open surgery, laparoscopic surgery, LESS and NOTES. Data was collected prospectively and analysed using statistical software. Results: A total of 500 participants took part in the study from variable backgrounds. Hypothetical scenario of kidney cancer:LESS and conventional laparoscopy were equally the most popular method (ranked 2.0 for both techniques). Open surgery and NOTES was the least preferred (ranked 2.78 and 3.22 respectively). When choosing only between LESS and NOTES only, 80% opted for LESS, 17.2% NOTES and 2.8% declined surgery. Hypothetical scenario of non-functioning kidney:LESS was most popular method followed by laparoscopy, open procedure and NOTES (1.89, 1.97, 2.94, 3.19 respectively).When choosing only between LESS and NOTES only, 76.6% opted for LESS, 19.2% NOTES and 4.2% declined surgery. Conclusion: LESS and conventional laparoscopy were the most preferred methods and NOTES was the least preferred technique. This shows general acceptance of the concept of virtually scar less surgery but without using the natural orifices.
Evolution of Single Institution Experience in Application of Laparoendoscopic Single-Site Surgery in Adult and Pediatric Urologic Surgery
Introduction: Adoption of Laparoendoscopic Single-site surgery (LESS) represents a further development of the minimally invasive surgical armamentarium for pediatric urology. Purpose: Review of evolution of adult and pediatric LESS at the University of California San Diego. Methods: Adult-LESS (A-LESS) commenced in 1/2009, followed by Pediatric-LESS (P-LESS) in 11/2009. Prior to initiation of P-LESS, pediatric urology proceeded with LESS-modified Society of American Gastrointestinal and Endoscopic Surgeons/Fundamentals of Laparoscopic Surgery curriculum in partnership with adult urology. A-LESS were performed by transperitoneal (56) and retroperitoneal (24) single-site approach with multiple trocars. P-LESS were performed by transperitoneal SILS port (Covidien). Demographics, intraoperative parameters, outcomes, and complications were recorded.Results: 80 A-LESS and 15 P-LESS were performed. A-LESS included 42 radical/19 partial nephrectomies, and 8 adrenalectomies. P-LESS included 7 unilateral/4 bilateral nephrectomies, and 1 ureteral reimplant. A-LESS included 1 conversion to open, multiport laparoscopy, or trocar placement at separate site. One P-LESS converted to open. Median age (years) for A-LESS was 62.5, and for P-LESS was 6. Median hospital stay (hours) for A-LESS was 60, and for P-LESS was 51.6. Median operative time (minutes) for A- and P-LESS were 154 and 183. Median discharge pain score for A-LESS was 1. Median pain score on post-operative day-1 for P-LESS was 2.2. Complications were noted in 6.3% A-LESS and 0 P-LESS.Conclusion: Adaptation of LESS technique with excellent, reproducible and comparable outcomes was achieved by collaboration between adult and pediatric urologic surgeons. Further investigation is requisite to determine ultimate utility of LESS in adult and pediatric urology.
MP02: Education & Simulators
STILUS Academic Research Group (SARG).
Introduction: The current recommended modality for the treatment of small renal tumours i.e. less than 4.0 cms includes partial nephrectomy (PN). Robot Assisted Partial Nephrectomy (RAPN) is an advanced platform for surgical extirpation of small renal tumours. However, there is a paucity of objective scoring systems of surgeon performance for feedback and governance of oncological and other outcomes. Purpose: To developed a system of direct observation with structured criteria to evaluate the surgical conduction of RAPN and to test the application and validity of the scoring system. Materials and Methods:20 cases of pre-recorded RAPN were each analysed by 2 mentors. Each mentor scored each case based on a 100 point scoring system comprising 25 key steps for RAPN (each step ranging 0 to 10). Steps included port placement, robot docking and safety checks in addition to the actual case. Additionally, a negative marking system based on a 50-point index scoring system was used such that technically unsound techniques were penalised heavily. The final scores independently submitted for each recorded case were analysed and compared. The system was then used to predict the experience of surgeon for 10 pilot cases. Results: There was no significant difference in the scores submitted by each of the 2 mentors for each of the cases observed. There was a strong correlation between overall score and seniority/experience of the performing surgeon. Conclusion: The scoring system was a reliable tool for assessing the performance of RAPN and accurately predicts the level of experience of the surgeon.
STILUS Academic Research Group (SARG). London. U.K.
Introduction: Training in advanced laparoscopic surgery using the robotic platform has inherent logistical and financial constraints placing demands on trainees and mentors. Purpose: To develop and test a novel model i.e. the CASCS technique with respect to its impact on optimising training time prior to embarking on the robotic console. Materials and Methods: Four prefellowship trainees in robotic urological surgery(PFTs) and 4 fellowship trainees(FTs) were followed prospectively for 18 months. The PFTs was put through the CASCS system and the FTs were allowed to continue as stipulated by the fellowship programme. CASCS is an abbreviation for skills acquired while performing one of four tasks i.e. [1] Camera driving and docking of robot [2] At hospital steeple chase exercised on ex vivo models [3] Scrub and first assistant at patient bedside [4] Courses/meetings and [5] Simulation training of at least 5 hours a week. At the completion of the 18 months follow-up period, participants were tested for specific skills including dry lab, wet lab and a formal written test. The PFT enrolled into the CASC arm performed the steps in an active and intense format. Result: There were no significant discernable differences in level of skill acquired nor written test scores between the PFTs and FTs. Tallies of overall costs showed that PFTs achieved the same level of skill as FTs at 25% of the cost of the latter. Conclusion: The CASC Technique is a simple, cost effective and potential way of optimising the prefellowship period for prospective robotic fellowship trainees.
Forced Gaze Control by Simultaneous Camera Drive and Target Task Narrows Skill Acquisition Curve
Introduction: Gaze analyses have shown that experienced surgeons spent significantly more time fixating the target locations than novices, who split their time between focusing on the targets and tracking the tools. We used the technique of subjecting laparoscopically naive trainees to perform basic laparoscopic tasks whereby they simultaneously guided the camera while performing the target task. Purpose: To test the impact of forced gaze control by simultaneous camera drive and target task on the skill acquisition curve. Materials and Methods: A laparoscopic box kit was fitted with a camera and solitary Port. In all, 24 candidates were enrolled and primed individually on basics of laparoscopy. Twelve novices were enrolled in this group (SCD) and 12 enrolled in the non-simultaneous camera drive group (NSCD). SCDs were required to perform specific tasks by adjusting the camera and instruments on a real time basis. After practice exercises, both groups were required to perform index tasks i.e. (A) needle drive through luminous hooks, (B) stacking 10 coins and (C) cutting a complex shape in a fixed paper. Times for task completion were tallied and compared to NSCDs. Gaze control was monitored in all by fitting them with an Applied Science Laboratories Mobile Eye gaze registration system. Results: Trainees from SCD were able to perform the index tasks (A) 1.8, (B) 1.7 and (T3) 2.8 times quicker than NSCD. Gaze control among SCD was better than NSCD. Conclusions: Forced gaze control by simultaneous camera drive and target task narrows skill acquisition curve.
Department of Urology, Catharina Hospital, Eindhoven, the Netherlands
Introduction: Today there is growing attention for training minimal invasive skills outside the operating room, because of ethical, legal and financial matters.Purpose: We developed and a evaluated a box training for basic laparoscopic urological skills (BLUS), partly abstracted from the Fundamentals of Laparoscopic Surgery, to determine its face, content and construct validation and to achieve standardization in training residents in urology.Materials and Methods: The BLUS consists of 5 basic laparoscopic tasks to train dexterity, depth perception, suturing, clipping and cutting skills. Fifty participants with different levels of laparoscopic experience performed the final BLUS training. Performance was measured on "time" by an observer and "quality of performance"by 2 urologists. A questionnaire was administered to measure the participants opinion regarding the usefulness of the BLUS for urology training. Results: Thirteen students, 20 residents and 17 urologists were included. Double-log-linear regression for all five tasks showed a significant effect (Effect Size (ES) range 0.55-0.82; p<0.01) of laparoscopic experience on performance time. Substantial correlations were found between experience and quality ratings (log linear regression ES 0.37; p=0.01). Usefulness of the BLUS model as a training tool for basic laparoscopic skills was rated 4.55 on a scale from 1 (=not useful) to 5 (=useful) (SD .58; range 3-5).Conclusion: This study indicates face, content and construct validity for the BLUS training. The training is considered appropriate for use as a primary training tool for an entry test or as part of a step-wise training programme for teaching urological laparoscopic skills.
Department of Urology, Catharina Hospital, Eindhoven, the Netherlands
Introduction: There is growing demand to assess surgical skills competency and define proficiency standards to safeguard quality of care.Purpose: To establish a defensible pass/fail score for the BLUS-assessment to set a baseline level of laparoscopic competency in the second year of the urological residency curriculum.Material and Methods: Cut-off scores to define BLUS-competency were defined according to the “contrasting group model” (fig.). Three referent groups were defined by their laparoscopic experience. Fifty participants (students, residents and urologists) were included. Performance was measured on "time" and "quality of performance". The cut-off scores were tested on the performance of 33 second year residents in urology.Results: Fifteen novices, 23 intermediates and 12 experts (>100 laparoscopic procedures) performed the BLUS-training. Cut-off scores were identified on the intersections; novice/intermediate (N/I) and intermediate/expert (I/E). The passing rates of 2nd year residents were 63,64% for N/I and 3,03% for I/E. Reliability of the assessment was 0.79 (Standard Error: 5.57) based on 2 examiners. Conclusion: This study showed reliability of the BLUS assessment and set a defensible pass/fail score for second year residents in urology on N/I level of competency with perspective on future development to acquire I/E level of competency.
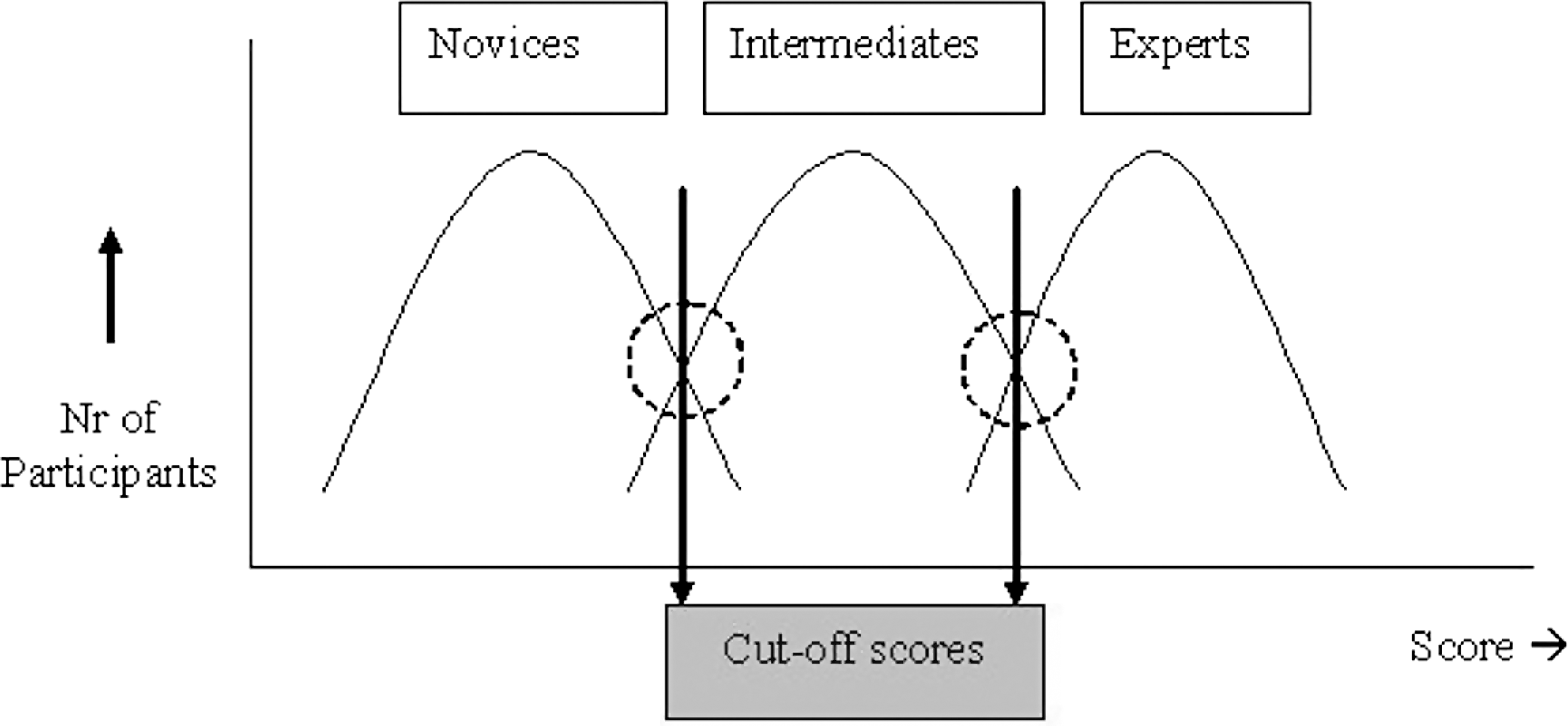
STILUS Academic Research Group (SARG). London. U.K.
Introduction: We previously devised and tested a grading system for continuum based laparoscopic skill acquisition using the dorsal vein complex ligation, vesicourethral anastomosis and laparoscopic partial nephrectomy (LPN) (Kommu et al.WCE 2009 & 2010). Purpose: To develop and test the continuum based approach for Extraperitoneal Robot Assisted Partial Nephrectomy (eRAPN).Materials and Methods: The grading system(Levels 1 to 5) was based on degree of resemblance to live human surgery. Level-1 Model was a basic model using styrofoam, Level-2 consisted of a sponge infused with red dye and secured in a liquid-tight fashion with polythene. Level-3 consisted of a bovine kidney procured from the butcher shop. Level-4 involved an animal model under anaesthesia. Two trainees who undertook basic level courses as deemed by the Royal College of Surgeons of England were enrolled. One trainee, was put through the continuum based model i.e. he was allowed to progress through the 4 Levels before reaching Level-5, the live human case. The other trainee was allowed to progress in the conventional route i.e. attending a dry lab, wet lab and then mentored live surgery. Time for the trainee to acquire the skill for competence as judged by expert laparoscopic surgeons was tallied and the progress monitored. Result: The trainee who used the continuum-based model was able to acquire competence at performing a LPN in the live human case 1.8 times quicker than the conventionally trained candidate. Conclusion: The continuum-based approach may provide a cost-effective and structured adjunctive tool for targeted skill acquisition for eRAPN.
STILUS Academic Research Group (SARG). London. UK.
Introduction: We previously developed and tested a grading system using continuum based skill acquisition for laparoscopic partial nephrectomy (LPN)[WCE 2008]. Purpose: To decipher construct, content and face validity of an ex vivo Continuum Based Level 3 Partial Nephrectomy Model(as described by Kommu et al.WCE 2008]. Material & Methods: The continuum based approach permits a LPN model to be graded into different Levels (i.e.1 to 5) based on degree of resemblance to live human surgery. Level 3 Model consisted of a bovine kidney procured from the butcher shop subjected to projection optics. Candidates were identified as novice (never involved with laparoscopy), intermediate (at least one case but less than 50 cases), and expert (50 or more cases). Each candidate performed LRP using the Level 3 Model. This was followed by a questionnaire assessing the model. Two experts reviewers assessed them using a validated tool. Results: Twenty candidates were enrolled (novices=8, intermediate=8, 4 experts). Experts scored higher overall than the other groups (p=0.0001). They were also shown to have better overall metrics than the other two groups. Experts rated the training model as near to live human case (median VAS 80/100) and overall rated the tools applicability/usefulness as 90/100 versus intermediates (100/100). Furthermore, in the intermediate subsection, the model was able to accurately predict between experienced fellow and beginning resident/registrar. Conclusion: The Continuum Based Level 3 Laparoscopic Partial Nephrectomy Model has been shown to have construct, content and face validity. It could supplement current training programmes and its utility should be explored further.
Utility of a Targeted Gaming Platform to Enhance Laparoscopic Skill Acquisition
Introduction: STILUS Academic Research Group (SARG) believes that laparoscopic skill acquisition is based on baseline inherent skills that could be enhanced by targeting key elements e.g. gaze control, concept of natural reality and forced exertion in hostile environment platforms. SARG developed a gaming platform prototype(EAGLE 1) to enhance laparoscopic urological skill acquisition. Purpose: To test the impact of a gaming platform on laparoscopic skill acquisition. Methods: Thirty candidates ranging 8 to 48yrs from all strata of society with no prior laparoscopic or video game experience were incorporated in the study. Ten were randomised to be primed on Eagle 1 (E1) and 10 randomised to be primed on a box kit (BK) and 10 were not primed (NP). Priming tasks were split into basic, intermediate and advanced. The basic practice tasks involved placing tiny beads into randomly lighting containers. The intermediate task involved tying 10 knots and the advanced task involved performing an anastomosis of two plastic tubular structures. All were tested on an index task, which involved cutting a complex shape on a premarked rubber sheet followed by stitching it over a template. Times for task completion and video analyses were tallied. Results: Time to target task completion was 3.8 quicker in E1 compared to BK. BK was 2.1 times quicker than NP. Metric scores were significantly higher in the E1 group compared to BK and NP. Conclusion: Utility of a purpose built gaming platform that targets gaze control and forced exertion in hostile environment platforms enhances laparoscopic skill acquisition.
STILUS Academic Research Group (SARG). London. UK.
Introduction: Optimal skill acquisition of the technique of dismembered pyeloplasty for ureteropelvic junction obstruction using the da Vinci® Robotic System is challenging and the live human case may not be the best platform for preliminary skills acquisition. Herein, we describe the construction of an ex vivo platform for skill acquisition in performing a pyeloplasty anastomosis using the da Vinci® Robotic System. Purpose: To describe the construction of a low cost ex vivo platform for skill acquisition in performing a pyeloplasty anastomosis using the da Vinci® Robotic System. Materials and Methods: The training module comprised of [a] the target task platform (TTP) and [b] the da Vinci® Robotic System. The target task was ex vivo continuous pyeloplasty anastomosis (CPA). The continuum based approach as previously described was used (Kommu et al. Journal of Endourology. October 2007: A1-A292). The grading system was for a target model of skill acquisition and was based on degree of resemblance to live human surgery graded Levels 1 to 5. Level-1 represented a basic model consisting of a tubular structure in the form of a balloon, Level-3 represented a fashioned ureteropelvis junction fashioned from supermarket chicken skin and Level-5 represented a live human laparoscopic pyeloplasty. Results: The platform was successfully constructed and applied for ex vivo steeplechase exercises. Conclusions: An ex vivo platform for skill acquisition in performing a pyeloplasty anastomosis using the da Vinci® Robotic System can be constructed with readily available over the counter materials at relatively minimal cost.
Laparoscopic Animal Surgery for Training without Scarifying Animals; Introducing the Rabbit as a Model for Infantile Laparoscopy.
Dept of Urology, University of California - Irvine
Background:Team-based simulation training (TBST) provides an opportunity to learn communication skills and prevent medical errors through experiential learning and deliberate practice. The OR is a high-stakes environment where effective communication is a key component to optimizing patient outcomes.Purpose:To assess the technical and non-technical skills of trainees during an OR-based TBST scenario. Methods:Urology and anesthesia residents were randomly paired to participate in a high-fidelity OR-based TBST scenario; laparoscopic renal vein injury (RVI) during radical nephrectomy. A surgical-task trainer used to simulate renal hilar dissection and a high-fidelity mannequin simulator were used to simulate 2 intra-operative events: vaso-vagal response to pneumoperitoneum and RVI during hilar dissection. Trainees were assessed on both technical performance (TP) and non-technical performance (NTP) during the simultaneous management of the patient by the urology and anesthesia resident.Results:Sixteen subjects were involved in the study and 93.8% felt that the simulated scenario was useful for intra-operative communication skills training. Urology resident level of training (LoT) correlated with EBL (p=0.022) and TP (p=0.004) but did not correlate with NTP as rated by both their anesthesia co-resident (p=0.127) and faculty experts (p=0.145). Anesthesia LoT correlated with NTP (p=0.036) but not TP (p=0.200). While urology residents consistently rated themselves higher on NTP (p=0.033) than did faculty, anesthesia residents did not differ in their NTP self-assessments (p=0.141).Conclusions:Residents felt that TBST involving a laparoscopic RVI scenario was useful for communication skills training. NTP did not correlate with urology resident LoT and urology residents often over-estimated their NTP.
Department of Urology, Graduate School of Biomedical Sciences, Hiroshima University, Hiroshima, Japan
Introduction: Although several institutions in Japan have introduced robot-assisted urologic surgery, the adaptability of individual surgeons to this technique has not been assessed. Purpose: The aim of the present study was to assess the adaptability of surgeons to robotic surgery by using the dV-trainer. Materials and Methods: Fifteen urological surgeons and 12 students were assessed using the dV-trainer. Nine of the urological surgeons had experienced more than 20 cases of laparoscopic surgery, and 5 of them were certified laparoscopic surgeons in this field. Each of the subjects completed a program consisting of 4 EndoWrist modules and 2 needle-driving modules, and repeated it several times. The performances of all subjects were recorded using a built-in scoring algorithm. Results: There were no significant differences in the initial score among the subjects, regardless of their characteristics, including experience of laparoscopic surgery. However, in the needle driving modules, after repeating the program, the scores of the certified laparoscopic surgeons became significantly better than those of the other subjects (after three times, p=0.0196, after four times, p=0.0336, respectively).Conclusions: Our data indicate that surgeons with experience of laparoscopic surgery may be more adaptable to the technique of robotic surgery.
department of urology, University of Dundee
Background:The human cadaver remains the gold standard for basic anatomic and surgical skills training. The Thiel embalming technique is not widely known, and therefore, little used. We describe a quality assessment of Thiel cadavers as a training model for the first British Association of Urological Surgeons approved advanced laparoscopic renal resection skills teaching course. Methods:Four trainee surgeons and four trained laparoscopic surgeons participated in an advanced laparoscopic renal resection training course that utilized Thiel cadavers. All participants completed a Likert 5-scale satisfaction questionnaire (1=strongly disagree; 2=disagree; 3=neither agree nor disagree; 4=strongly agree; 5=strongly agree) after their training session. Cadaveric tissue quality and the quality of the training session related to Thiel cadavers were assessed. Particular emphasis was placed on patient positioning, ease of trocars placement, preservation of tissue planes, pedicle dissection and quality of tissue preservation using this novel model. Results:Four participants rated the quality of the cadaveric tissue as excellent. The average score of quality of the Thiel cadaveric tissue was 4.5 by the participants. The quality of Thiel cadavers for laparoscopic nephrectomy was rated as 4.3 by faculty members. Two faculty members who had experience of teaching laparoscopic nephrectomy on fresh frozen cadavers commented that the Thiel cadavers were extremely life-like in comparison to frozen cadavers.
Cuschieri Skills Centre, Ninewells Hospital and Medical School, University of Dundee, Dundee DD1 9SY
Background:The tissue models remain invaluable for surgical skills training. Resemblance of tissue texture to normal, anatomical landmarks and quality of tissue are the essential for laparoscopic training tissue models. We describe quality assessment of calf models as a laparoscopic training model for advanced laparoscopic renal resection skills teaching course. Methods:Four trainee surgeons and four trained laparoscopic surgeons participated in a advanced laparoscopic renal resection training course that utilized calf-model for transperitoneal and retroperitoneal nephrectomy. All participants completed a likert 5-scale satisfaction questionnaire after their training session. Calf tissue quality and the quality of the training session related to this material were assessed. Particular emphasis was placed on anatomical landmarks, ease of trocars placement, preservation of tissue planes, pedicle dissection and quality of calf tissue.Results:Four urological trainees have used the calf model for the laparoscopic transperitoneal and retroperitoneal nephrectomy. In total the calf model had been given a mean score of 3.98/5. Conclusion:
Department of urology,Ninewells Hospital, Dundee,UK
Background: Laparoscopic training in Europe has become a challenge following European Working Time Directives (EWTD). Portable simulators could play an essential role in enhancing the skills acquisition, however there are not many randomised trials assessing their exact role. We present data from double blinded randomised controlled trial.Methods: 20 medical students with no prior laparoscopic exposure were assessed on fixed laparoscopic facility in skills laboratory using validated tools for basic laparoscopic skills. The skills were chosen by consensus between five experienced laparoscopic surgeons. They were randomised using computer generated random numbers into two groups, group one had access to portable simulator and group two did no. Group one practised for one hour each day for 3 weeks (14 hours in total). A log-book was maintained by an independent person ensuring training every day. At three weeks both the groups were re-assessed for skills acquisition using same validated tools. The exercises were recorded and scored by two experienced laparoscopic surgeons without knowledge about the randomisation. Statistical analysis was carried out.Results: There was significantly higher skills acquisition in all the laparoscopic skills such as dissection, cutting, retraction, suturing and instruments handling in the group 1 (with access to portable laparoscopic simulator. Except for time taken to complete task, quality of task performance was statistically significantly better in group 1 (p value 0.0937). Conclusions: Access to portable simulators enhances the skills acquisition and this facility should be made available as a part of surgical curriculum in the future.
Department of Urology, Catharina Hospital, Eindhoven, the Netherlands
Introduction: Training needs analysis is essential for development of simulator- based training. Endourological procedures are complex tasks, which consist of psychomotor and cognitive skills. Purpose: To design a simulator-based skills training for teaching the nephrostomy procedure according to Cognitive Task Analysis and 4C/ID model, which assumes that an effective training consists of four interrelated components: scenarios, supportive information, just-in-time-information, and part-task practice.Material and Methods: A semi-structured group interview was conducted among 8 expert urologists to identify all steps and sub-steps of the procedure (fig.). All sub-steps were classified as automatic or non-automatic. Different scenarios with increasing difficulty level were mentioned and error analysis was conducted. Results: The 4 components are integrated within the cognitive task analysis. Subtasks which were classified as automatic (i.e. bimanual dexterity) could be trained separately in a part-task practice until automatism has reached. Error analysis (i.e. haemorrhage) is highly suitable for just-in-time-information. The final result was a blueprint for training modules of increasing difficulty level.Conclusion: Training needs analysis according to CTA for the nephrostomy procedure results in identification of automatic and non-automatic psychomotor and cognitive skills. The final blueprint can be used by i.e. simulator developers. Collaboration between educationalists, urologists and simulator is recommended.
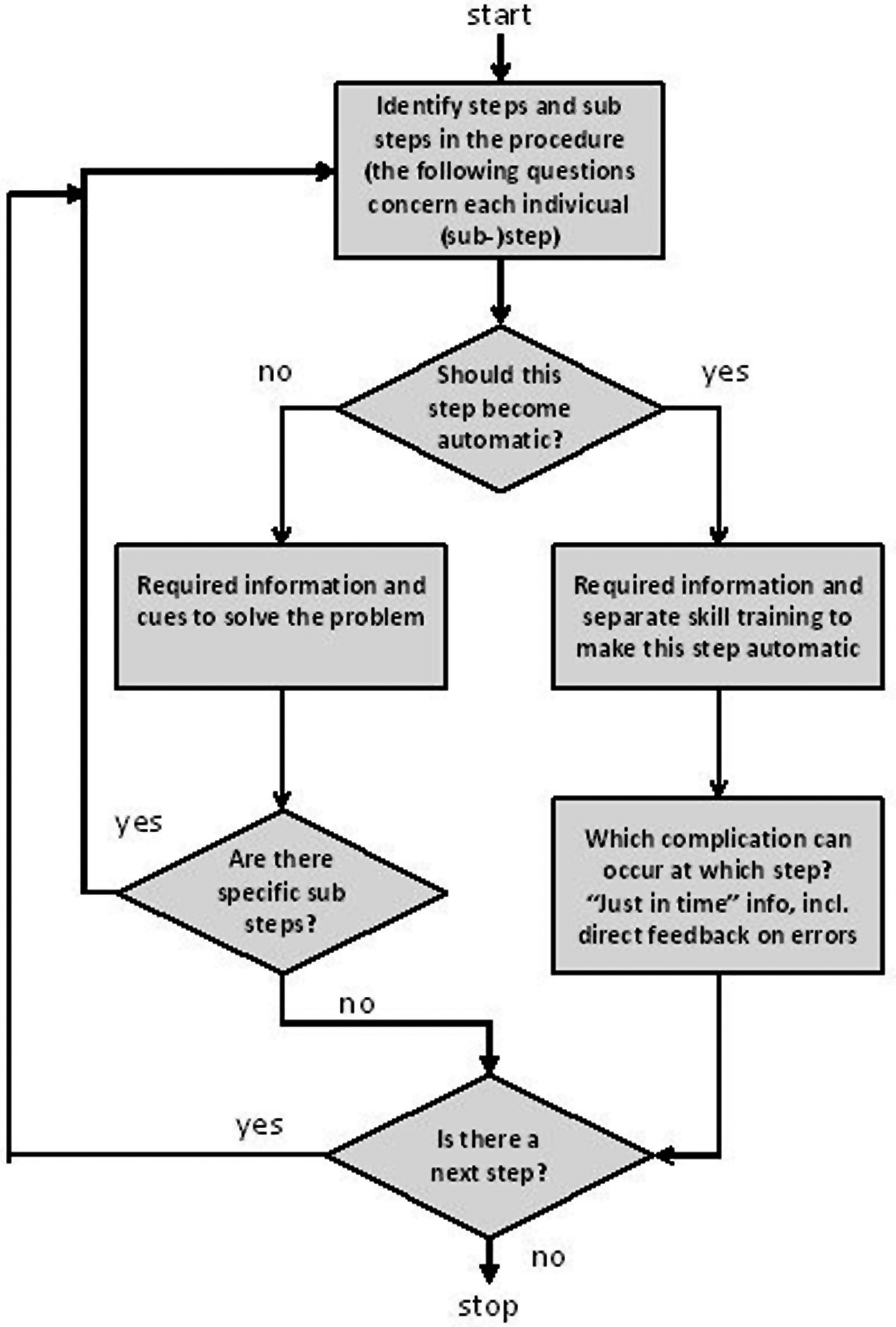
Urinary pH Measurement After Renal Obstruction. Can it be Used as a Marker for Recovery of Renal Function?
IntroductionUrinary tract obstruction impairs renal function and is often associated with a urinary acidification defect caused by diminished net Hydrogen ion secretion and or Sodium-Bicarbonate re-absorption. In animal modules, obstructed kidneys with urinary pH above 7.00 have significant reduction in creatinine clearance when compared with obstructed kidneys with urinary pH 7.00 or less. Regain of urine acidity is associated with recovery of renal function.Materials and methodsUrinary pH was measured on regular intervals for 10 days in 8 patients with obstructed kidneys following insertion of nephrostomy tube. Urinary pH was checked in bladder and nephorsotmy urine in 7 patients with unilateral obstruction and from both kidneys in one patient with bilateral obstruction. The eGFR for all patient with unilateral renal obstruction was more than 60. In patients with unilateral obstruction, the renal urine ph showed gradual acidification with mean pH at 10 days approaching mean bladder urine pH. Only one patient had MAG3 renogram following insertion of left nephrostomy This showed normal renogram with split renal function of 58-percent for left kidney and 42-percent. for right kidney.In the patient with bilateral obstruction, the renal pH showed gradual acidification with improvement of renal function detected by GFR 18-22.ConclusionAcidification of urine following insertion of nephrostomy is associated with improvement of the renal function. Regular measurement of urinary pH following relief of renal obstruction can be a reliable marker for return of renal function, especially in patient with normal renal function and obstructed unilateral kidney
Surgical Skills Acquisition Among Left-Handed Trainees: A Preliminary Study of Hand Dominance-Based Surgical Training
Background:Studies often report inferior surgical skills among left-handed trainees (LHT). Most training curricula and assessment methods, however, are right-handed (RH); which may place LHT at a disadvantage. Purpose:To evaluate the impact of a hand dominance-based curriculum on acquisition of suturing and knot tying skills among medical students.Methods:Students were randomized to either a left-handed curriculum (LHC) or RHC consisting of 1) an introductory video and 2) a two-hr instructor-led, hands-on session on suturing and knot tying. All instructional methods, instructors, and instruments were exclusively RH or LH for the RHC and LHC, respectively. Students were assessed on the performance of 2 suturing tasks, continuous running suturing (CRS) and instrument knot tying (IKT); both immediately and 2 weeks post-training.Results:A total of 19 students were enrolled (8 LHT, 11 RHT). Students randomized to a curriculum "in concordance" with hand dominance performed significantly better than those randomized to a "discordant" curriculum on both tasks (see Table). Within concordant and discordant groups, there were no significant differences between LHT and RHT. Conclusions:This preliminary study demonstrates that students participating in a training curriculum discordant with hand dominance may have inferior acquisition of suturing and knot tying skills.

Kansai Medical University, Osaka, Japan
<Introduction> The dissection maneuver in laparoscopic surgery differs between expert and novice surgeons. This difference relates to the application of force on the instrument tip. The aim of our study was to analyze how surgeons apply force during a single stroke of a dissection maneuver.<Material and Methods>We developed a system to measure the force on the instrument tip. This system is capable of detecting vertical forces (VF) and horizontal forces (HF). Thirty participants were divided into three groups of surgeons: expert (n=10), intermediate (n=10), and novice (n=10). Participants performed a dissection task involving separation of an artery from surrounding fat in a dead porcine kidney using their dominant hand. Dissection skill was analyzed by the timing of the peak VF (TVF) and peak HF (THF) (TVF or THF [%]=time to peak VF or HF/whole dissection time). <Results> TVF of experts occurred at earlier timing compared with intermediates and novices (mean: experts, 39.9%±8.8%; intermediates, 51.3%±15.2%; novices, 63.7%±10.1%; P<0.05), while there was no significant difference in THF (P>0.05). <Conclusion> At the beginning of a dissection maneuver, experts applied VF with a small amount of HF. After the peak VF, HF was gradually applied with relaxation of the VF. By contrast, from the beginning, novices gradually applied VF and HF without relaxing either force. Intermediates applied an intermediate force between that of experts and novices.
MP03: Robotic/Lap Upper Urinary Tract 1
Tadalafil for Prevention of Renal Dysfunction Secondary to Renal Ischemia
Growing evidence suggests that phosphodiesterase 5 inhibitors may mitigate ischemia-related renal damage. We evaluated the role of tadalafil in renal function preservation during experimentally induced ischemia / reperfusion injury (IRI) in a solitary kidney porcine model.
Ten adult female pigs underwent left laparoscopic nephrectomy followed by a 1-week recovery period. They were then randomized to tadalafil vs. no treatment prior to cross-clamping the contra-lateral renal hilum for 90 minutes. The experimental group received 40 mg tadalafil in 2 equally divided doses, 12 hrs before and just prior to surgery. Serum creatinine for each animal was obtained just prior to ischemia induction (D0), and at days 1, 3 and 7 post hilar occlusion. Median creatinine at each time point was compared for the groups using the Mann Whitney U test.
Median serum creatinine at D0, measured after two doses of tadalafil, was significantly lower in the tadalafil group (1.9 mg/dl vs. 1.4 mg/dl, p=0.014). As expected, median creatinine for each group rose significantly on D1 (p=0.04 for each). Median creatinines following hilar occlusion at D1, D3 and D7, however, were not significantly different between groups.
In this porcine model, administration of perioperative tadalafil improves preoperative renal function, but it does not appear to mitigate ischemia/ reperfusion injury from hilar occlusion.
Focal Therapy in Renal Cell Carcinoma: Which Modality is Best?
Introduction: Thermal ablation of small renal tumours is an established treatment modality in selected cases. Major drawbacks of previously published reviews/meta-analyses is the heterogeneity of the series and the short-term oncologic follow-up.Purpose: To assess the best ablation technique and approach in renal tumours deemed suitable for ablation.Methods: A systematic PubMed-search through May 2011 was done. Publications not assessing oncological results, without specified results for biopsy-proven RCC, with a follow-up<36 month and not available in full-text English were excluded. To assess peri-operative complications we selected series exceeding 70 cases and comparative series among techniques.Results: Seven (3 RFA,4 cryoablation) and 16 original series met selection criteria for oncological- and complication assessment respectively. Since all studies were observational performing a meta-analysis was senseless.Mean follow-up for oncological series ranged from 53-95 months (caseload 18-55 patients). Recurrence-free survival ranged from 81-94% (RFA) and 84-100% (cryoablation).Mean reported time-to-recurrence was 16 (RFA) compared to 18 months (cryoablation). Metastatic-free survival ranged from 96-100% (RFA) and 89-100% (cryoablation) and cancer-specific survival ranged from 99-100% (RFA) and 89-100% (cryoablation). Initial failure rate was higher for the percutaneous approach compared to laparoscopy (5.3-11.5% vs. 1.0-6.7%). Overall complications and survival were comparable for percutaneous and laparoscopic approach.Major complication rate ranged 0-5.0% and 3.1-8.3% for percutaneous-and laparoscopic-approach respectively. Length of stay and patient convalescence was favourable for the percutaneous approach,regardless of ablation modality.Conclusion: Low-quality evidence shows that CA and RFA have similar acceptable oncologic outcomes and low major-complication rate. Initial failure is higher after percutaneous approach.
The DISSRM (Delayed Intervention and Surveillance for Small Renal Masses) Registry: Three Years of Observations
Introduction: The DISSRM Registry was opened January 1, 2009, enrolling patients with small renal masses (SRM) <=4.0 cm who chose intervention or active surveillance (AS).Purpose: To prospectively follow outcomes for patients with SRM electing AS or intervention.Materials and Methods: Patients were enrolled after consultation regarding AS versus intervention. Those electing AS were placed on an imaging protocol (CT, MRI or US) every 4-6 months for 2 years, then 6-12 months for 3 years. SF-12 questionnaires were completed at enrollment, 6 and 12 months, and annually thereafter.Results: At 36 months, 247 patients were enrolled; 159 (64.4%) electing intervention, 65 (26.1%) AS, and 15 (6.0%) crossed-over. Of the total population, 58.6% are men, 75.7% are Caucasian. In AS and intervention arms, median age was 72 and 61 (p<0.001), tumor diameter was 2.08 and 2.44cm (p<0.001) respectively. Mean SF12 at enrollment was 93.1 vs. 95.8 (p=0.2) and was not significantly different during follow-up. For those electing surgery, 126 (70.4%) underwent partial nephrectomy (PN), 23 (12.9%) radical nephrectomy and 29 (16.2%) cryoablation. Of the treated masses, 120 (67.4%) were RCC, 20 (11.2%) oncocytoma, and 11 (6.2%) AML. With a median follow-up of 15 months, two patients in each arm have died of causes unrelated to RCC. Three patients in the intervention arm progressed; two requiring repeat intervention, one developed diffuse metastases. Conclusions: Over 60% of patient with SRM selected intervention versus AS. 67% of masses removed were RCC. Progression free survival is excellent with short follow-up.
Penetration of Renal Mass Biopsy in the Global Urological Practice: A Survey Among Urologists
IntroductionThe vast increase in recent publications on renal mass biopsy (RMB) suggests an increased interest in the subject. PurposeTo assess the use of RMB in the current urological practice, including related factors such as indications and patterns in practice. MethodsThe link to a web-based questionnaire (www.surveymonkey.com) was sent to all registered e-mail addresses (±2000) of members of the Endourological Society in December 2010. The questionnaire contained 6 epidemiological questions, 10 regarding patterns of practice, one regarding the influence of literature and one on future techniques. Chi-square test (for trends) was used to assess statistical significant differences among categorical answers. ResultsIn total 190 respondents completed the survey of which 73% indicated to perform RMB "never" or "rarely" compared to 9% performing RMB in 25-100% of cases. 13% of respondents reported never to take a RMB. Of the latter, significantly lesser practice in university hospitals (6% vs. 20-30%, p=0.003).Main indications to perform RMB are still tumors in solitary/transplant kidneys and in metastatic disease. Lack of influence on clinical management and risk of false negatives were the main reasons not to perform biopsies. 61% prefers histological biopsies compared to 8% preferring cytological aspiration, 31% indicated to combine both techniques. Other tissue differentiation techniques (Optical Coherence Tomography, Raman-spectroscopy) are unknown for 65% of urologists ConclusionRMB is not yet applied widely in the urological practice, with academic urologists performing RMB less infrequently. Core biopsies are still preferred, although combined with cytological punctures by a considerable number of respondents.
Early Outcomes of LESS Nephrectomy Experience
Introduction: To present experience with LESS partial nephrectomy(PN) and LESS radical nephrectom(RN) in comparison to the corresponding conventional laparoscopic (CL) approach.Patients and Methods: A head-to-head comparison of 22 LESS nephrectomies (15 RN/7PN) with a control group of 22CL nephrectomies (15RN/7 PN) performed between January2009 to October2010. Classic laparoscopy and LESS: transperitoneal transumbilical approach with keyhole trocar placement and Gelpoint (Applied Medical) for access. A 5mm 30 degree-endoscope, CL instruments and SonoSurg ultrasonic scissors (Olympus*) were utilized. Comparisons regarding preoperative, peri-operative and immediate postoperative parameters. Results: With the RN analyses, LESS and CL cohorts were similar in age (71vs.68y,p=0.53) and tumor size (56vs.65.3mm,p=0.30). Intraoperative blood loss (133cc-LESSvs.72cc CL,p=0.58) and ORtime (LESS:120.5minvs.CL:120min,p=0.19) were comparable. Morphine use (LESS:29mgvs.CL:32mg,p=0.85) and length of hospital stay (LESS:5.2dvs.CL:6.2d,p=0.37) were similar. In the PN subgroup, no difference was noted in age (59.3y LESS vs.58.6y CL, p=0.93) and tumor size (28mmLESSvs.32.3mm CL, p=0.56). In 2/7 LESS-PN, a vascular clamping mean time of 32.5min. was recorded compared with 23.8min. for 6/7 CL-PN(p=0.35). Blood loss was similar (185.7ccLESSvs. 172.9ccCL,p=0.91). There was no difference when comparing operative time (109.3minLESSvs.140minCL, p=0.08). Morphine requirement (LESS32.8mgvs. CL58.9mg, p=0.29) and length of hospital stay (LESS 4.7dvs. 5.7d,p=0.16) were comparable. We verified 2 post-operative complications in LESS arm. One conversion to open surgery in the LESS arm was performed in one patient due to vascular stapling malfunctioning. No tumor recurrence has occurred in any of the patients in both arms.Conclusion: LESS approach is feasible for RN and in highly selected patients for PN.
Bristol Urological Institute
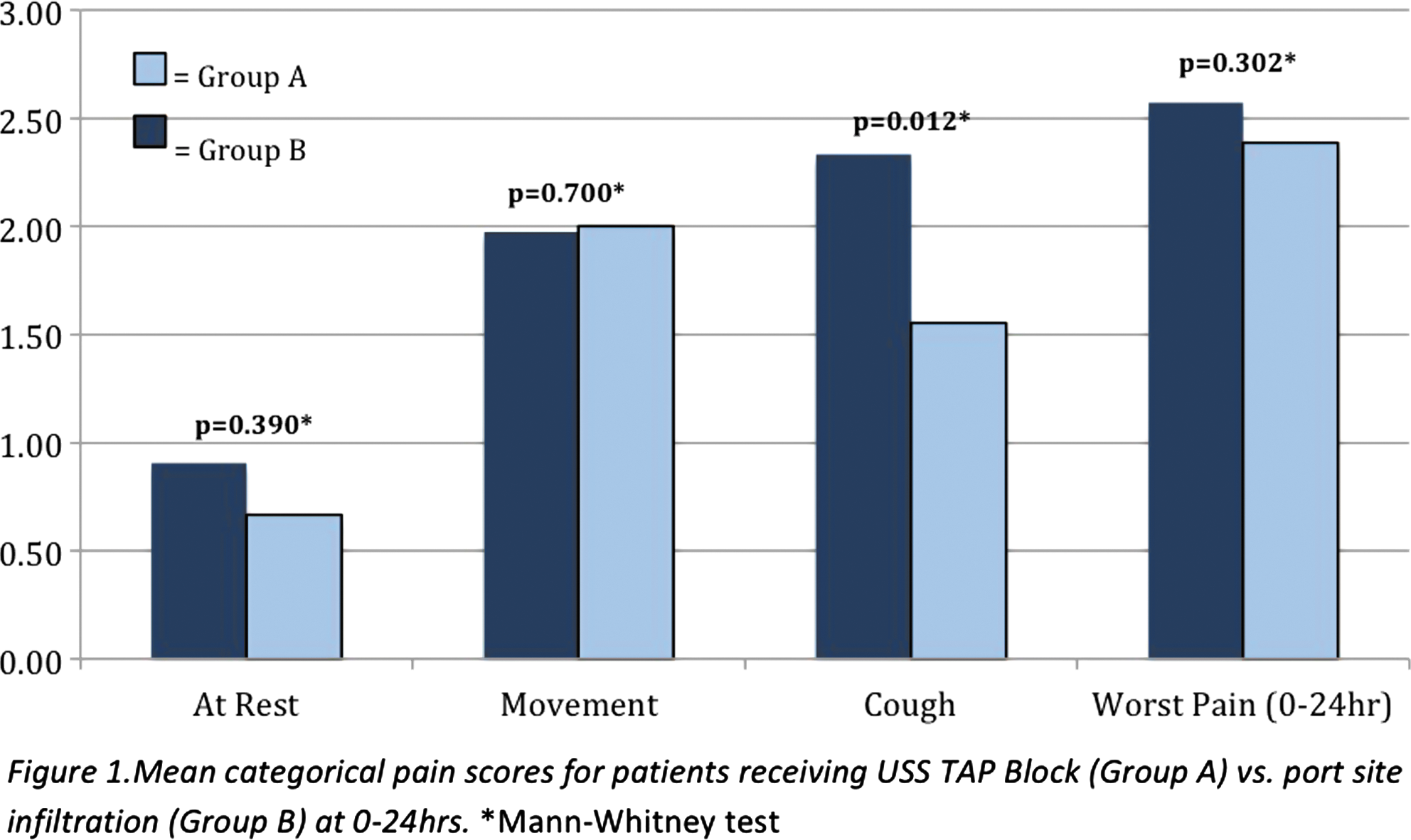
Blocking anterior abdominal wall nerve fibres however,did not effectively reduce pain on movement nor additional analgesia requirements.
A Stratification System for Predicting Patient Discharge Following Upper Tract Robotic Urological Surgery
Introduction: Postoperative hospital stay has a significant impact on health economic resources. With the advent of minimally invasive urological surgery, postoperative stay was purported to be reduced due to the inherent advantages of laparoscopy. However, following major upper tract urological surgery, there is still significant variation in hospital stay. There is currently no stratification system to predict patient discharge. Purpose: To develop and test a stratification tool to predict patient discharge following RANU, RAP and RAPN. Materials and Methods: Patients who underwent RANU, RAP and RAPN were identified. Their records were reviewed retrospectively. A proforma was devised to include 3 facets. Facet 1 involved Patient Health. This included ASA status and comorbid history. Facet 2 involved Home Patient Ambulatory Support (HPAS). This included presence of a friend/relative at home for support, home architecture including need for climbing stairs and infrastructure for summoning help e.g. availability of telephone. Facet 3 involved Nursing Support Services including geographical proximity to a district nurse. Each facet was scored for a minimum of 0 and a maximum of 10. Results: Patients who had a score of 20 or more had a greater than 90% chance of discharge the next day. Patients with a score of less than 10 were deemed unsuitable for discharge earlier than 48 hrs postoperatively. Conclusion: The stratification system accurately predicts likelihood of next day discharge following upper tract robotic urological surgery and could act as useful adjuncts to help with deciphering the suitability of patients for enhanced postoperative discharge.
Surgical Management of Renal Artery Stenosis Caused by Takayasu' Arteritis Using a Hybrid Laparoscopic Technique
Introduction: Takayasu's arteritis(TA) can cause renal artery stenosis and refractory renal hypertension. Percutaneous transluminal angioplasty (PTA) may fail in severe cases and surgical treatment is indicated.
Purpose: To evaluate the feasibility of laparoscopic application and efficacy of different types of vascular reconstruction in surgical treatment of renal artery stenosis.
Materials and methods: Seven patients with renal artery stenosis caused by TA were admitted. According to stenostic site and aortic condition, different types of vascular reconstruction were chosen for surgical treatment including two autotransplantations, four aortorenal bypass and one splenorenal bypass. Laparoscopic renal artery isolation and kidney mobilization were firstly performed. For bypass patients, hypogastric artery was harvested by laparoscopic approach while saphenous vein and spleen artery were dissected by open. Autotransplantation and arterial anastomosis were then performed through an open incision.
Results: Five patients had normal blood pressure postoperative and two required single-agent antihypertensive medication. Complications included lumbar artery injury and flank pain in each patient. Bypass operations had less operative time, less intraoperative blood loss and more rapid postoperative recovery than autotransplantation. The anastomosis was patent in all patients and none of re-stenosis occurred during the follow-up.
Conclusions: Laparoscopic dissection renal artery and harvesting hypogastric artery facilitate the complicated surgical procedure. Surgical treatment is effective in renal revascularization of TA patients. Aortorenal and splenorenal bypass provides higher efficiency compared to autotransplantation.
Division of Urology, Washington University School of Medicine, Saint Louis, MO
Purpose: We present our experience with long-term follow-up after laparoscopic cyst decortication (LCD) for autosomal dominant polycystic kidney disease (ADPKD), focusing on factors predictive of progression to end-stage renal disease (ESRD).Patients and Methods: Between August 1994 and December 2003, 37 ADPKD patients underwent LCD. 19 patients with at least 3 year follow up were included. Mean follow-up was 9.50 years (range 4.25−14.25). Renal function was evaluated using CKD-EPI creatinine-clearance formula. Hypertension was evaluated using the anti-hypertensive therapeutic index (ATI). Pain assessment was based on narcotic use. Patients in the ESRD group included those who underwent transplant, were on dialysis, or were preparing for dialysis.Results: 62.5% continued on narcotics after LCD. Recent ATI of 9.29 (stdev 8.13) was higher that pre-operative ATI of 4.25 (stdev 4.45) (p=0.04). 11 patients developed ESRD following LCD - 7 transplant, 2 dialysis, and 2 pre-dialysis. Characteristics of ESRD vs non-ESRD groups in the figure. Conclusions: Despite LCD,>50% of patients may continue to require narcotics. Recent ATI was significantly worse than preoperative ATI. Pre-op creatinine clearance is a strong predictor of progression to ESRD following LCD. The role of LCD in altering the natural progression to ESRD requires further investigation.
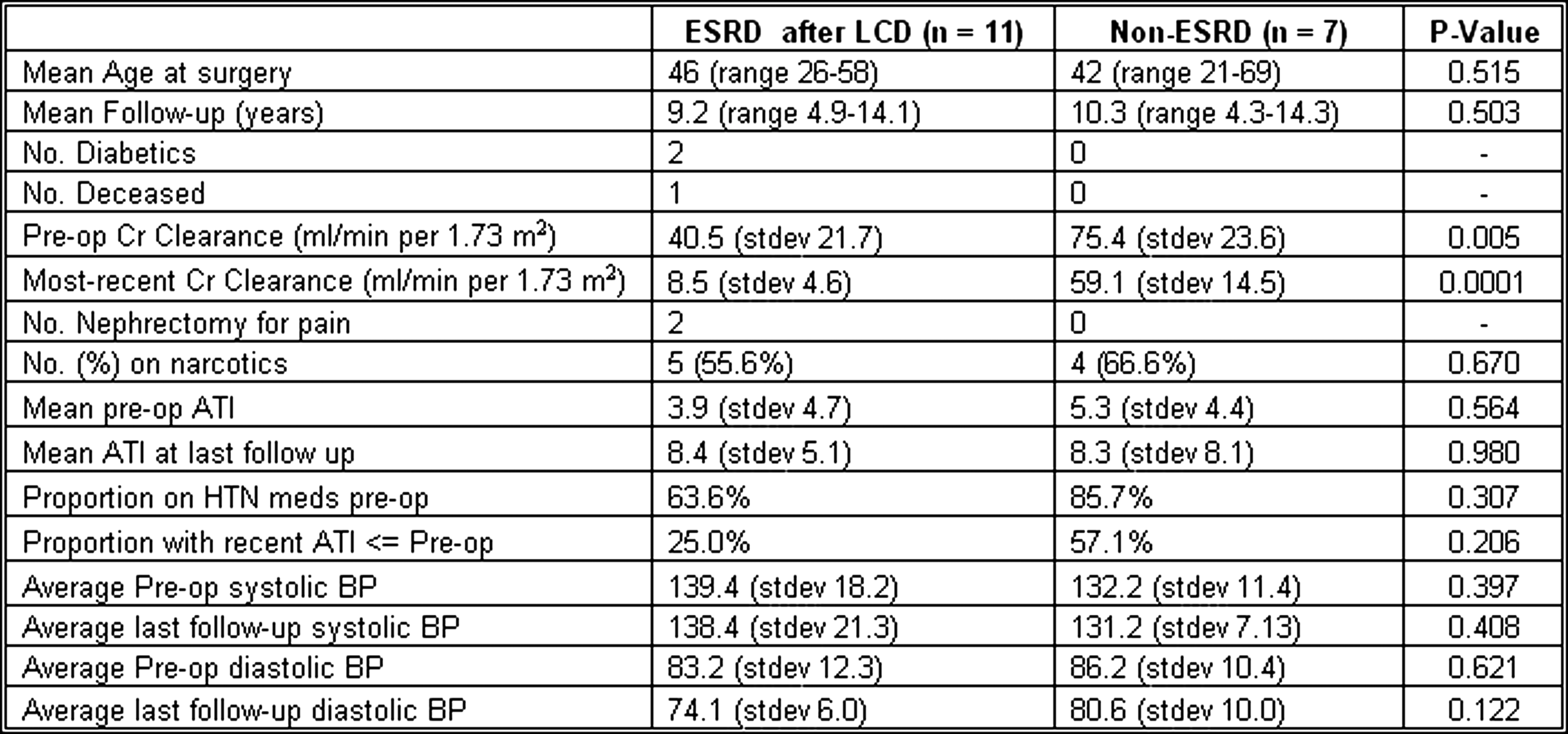
Department of Urology, Saitama Medical University, Saitama, Japan
<Introduction>Laparoscopic simple nephrecomy for atrophic kidney with severe infectious episode is thought to be difficult usually because of patient condition and severe adhesion around kidney. And, therefore, the key point to complete the procedure is probably depending on the indication and the skill, but it makes fair analysis difficult. In this presentation we analyzed perioperative parameters of this procedure, comparing to radical nephrectomy done by a single surgeon in same period.patient <Subjects> The first case of simple nephrectomy was done in November, 2007 for this surgeon. Therefore, cases of radical nephrectomy after this case were chosen for the comparison to simple nephrectomy cases. Simple nephrectomy was done for 12 case (all female). Average age and BMI were 63.5 years and 22.3. Radical nephrectomy was done for 41 cases in same period. <Result>Average time of pneumoperitoneum was 125.5±45.5 min in simple nephrectomy cases and 124.1±42.9 min in radical nephrectomy cases. Blood loss were 42.3±82.3 ml and 47.1±88.9 ml respectively. One converted case was recorded in radical nephrectomy group. There was no difference suggested in postoperative course and the length of hospital stay.<Discussion> In this recent years, skill of surgeons has progressed rapidly, which make complicated procedures possible. Skilled surgeons may propose laparoscopic procedure initially in any circumstances. From this report, even if simple nephrectomy for serious infectious episodes is supposed to be difficult to complete, experienced surgeons may manage same as radical nephrectomy.
The Department of Urology, Hokkaido University Hospital, Japan
Introduction: Peritoneal damage should be avoided at the nephrectomy in patients with end-stage renal disease treated by peritoneal dialysis (PD). Purpose: Feasibility to preserve peritoneal cavity in retroperitoneal nephrectomy in two PD patients. Surgical technique and peri-surgical PD procedure are evaluated. Patients and Methods: Thirty-six years old woman and 61 years old man underwent retroperitoneal nephrectomy due to renal tumors. Results: The former patient with 19 months PD treatment had bilateral renal mass (28 mm renal tumor in lower pole of left kidney and two aneurysmal tumors in middle of right kidney). She underwent staged retroperitoneal laparoscopic surgeries (left partial nephrectomy and right nephrectomy) uneventfully. Operation time was 217 and 105 minutes. Left renal cell carcinoma (RCC) (G1, pT1a) and right renal aneurysm (32 mm) were proven in pathology. The latter patient with 11 months PD treatment had a 29 mm of renal tumor in lower pole of left kidney. He underwent retroperitoneal laparoscopic nephrectomy uneventfully. Operation time was 140 min. Pathology of the tumor was RCC (G2, pT1a). PD was restarted 48 hours after the surgery in both patients without any troubles. Daily urine volume of former woman decreased from 600 to 300ml, that of latter man decreased from 2000 to 1300ml. She was converted to hemodialysis 6 months after surgery because of PD dysfunction (low clearance), while he is now maintained with PD 8 months after surgery. Conclusions: Retroperitoneal laparoscopic approach was beneficial for keeping perioperative PD procedure.
Laparoscopic Radical Nephrectomy for Large Renal Masses: Critical Assessment of the Perioperative and Oncologic Outcomes of T2a and T2b Tumors
Introduction: While laparoscopic radical nephrectomy (LRN) is the gold standard for the treatment of renal masses ineligible for nephron-sparing surgery, many surgeons prefer open RN for advanced or complex tumors. Purpose: To analyze the perioperative and oncological outcomes of large and complex tumors treated with LRN. Methods: 249 patients were identified in the Johns Hopkins Minimally Invasive Urologic Surgery Database (1994-present) who underwent LRN for large (>7cm) masses. Patient demographics, tumor characteristics and perioperative outcomes were compared among patients with tumors 7-10cm and>10cm using appropriate tests. The Kaplan-Meier method was used to determine cancer-specific (CSS) and recurrence free survival (RFS) and regression models were created to predict RFS.Results: Tumors were>7.0-10cm in 168 (67.5%) patients;>10cm in 81 (32.5%). Median follow-up was three years (range 0.5-16.2). Patients with tumors>10cm had a greater average blood loss (450 vs. 300cc, p=0.04) and were converted to open cases more often (13.6% vs. 3.0%, p=0.002). Length of stay, days to regular diet, blood transfusion rate and number/degree of post-operative complications were similar. In total, 57 (23.0%) patients experienced a complication; high-volume surgeons had fewer severe complications (Clavien 3-5; 39.5% vs. 62.5%, p=0.015). Of 199 patients with clinically localized disease, 7-year RFS and CSS was 59.6% and 89.3% respectively. In multivariable analysis, predictors of recurrence were clear cell histology, Fuhrman grade and tumor stage. pT2b disease was not a significant predictor of recurrence; PNE and RVI independently predicted RFS. Conclusions: LRN can have excellent outcomes for large (>7cm) and complex renal masses.
Major Vascular Injuries of Urologic Retroperitoneoscopic Operations
Purpose: We assessed vascular injuries of urologic retroperitoneoscopic operations and discussed the preventions and treatments of the complications. Methods: 1850 patients underwent retroperitoneoscopy for various renal ,adrenal and ureter pathology between January 2001 to May 2011.A total of three vascular injuries occurred, introoperative circumstances, preventions and management techniques were evaluated. Results: Case 1 was identified with vana caval half-transection by endo-gia during right laparoscopic radical nephrectomy,No special handing was given, the patient was followed two years with no sequelae.Case 2 was renal vein injury by titanium clip used to control lumbar vein during left partial nephrectomy, the renal vein was repaired by laparoscopic suture. Case 3 was abdominal aorta injury during the left ureterolithotomy, calcitication of aorta wall was incorrected idendified as ureter stone, immediate conversion to open operation was performed with no sequelae. Conclusions: Major vascular injury are uncommnon but serious complications,prompt judgement and repair are necessary.
Major Organ Injuries of Urologic Retroperitoneoscopic Operations
Purpose: We assessed organ injuries of urologic retroperitoneoscopic operations and discussed the preventions and treatments of the complications. Methods: 1850 patients underwent retroperitoneoscopy for various renal ,adrenal and ureter pathology between January 2001 to May 2011.A total of five organs injuries occurred, introoperative circumstances, preventions and management techniques were evaluated. Results: Case 1 was identified with duodenum injury five days later after right laparoscopic radical nephrourterectomy,repair of duodenum was performed by open operation.Case 2 was diagnosised pancreatic injury seven days later after left radic nephrectomy,conservative management with drainage of a pancreatic collection was successful. Case 3 was diaphragmatic injury during the left radic nephrectomy,repair of diaphragmatic was given intraoperation.Case4,5 was idendified as ureter injuries during operation of right kidney cyst, immediate conversion to open operation was performed with no sequelae. Conclusions: Major organ injury are uncommnon but serious complications,prompt judgement and managements are necessary.
Nephron-Sparing Surgery for pT3b Renal Cell Carcinoma in Patients with a Solitary Kidney
Robot-Assisted vs. Pure Laparoscopic Partial Nephrectomy: A Comparison of 200 Consecutive Cases
Introduction:Robot-assisted laparoscopic partial nephrectomy (RALPN) is an increasingly utilized surgical technique for small renal masses. There are few studies directly comparing perioperative outcomes of RALPN and laparoscopic partial nephrectomy (LPN). Purpose:To report our initial experience with RALPN compared to LPN.Materials and Methods: A retrospective review of the Johns Hopkins Minimally Invasive Urological Surgery Database identified 207 consecutive patients undergoing laparoscopic or robotic-assisted laparoscopic partial nephrectomy between 2007 and 2011 by a single surgeon. Patient demographics, pathologic, operative, and perioperative outcomes were compared between surgical techniques.Results: 102 and 105 patients underwent LPN and RALPN, respectively. Demographic data was comparable between groups. Patients undergoing RALPN had shorter warm ischemia times (15 min vs. 21 min, p<0.001), fewer cases with prolonged warm ischemia time (<30minutes) (3.8% vs. 12.7%, p=0.02), and equivalent operative times (165min vs. 180 min, p=0.19). The robotic group had less estimated blood loss (100mL vs. 200mL, p<0.001) but with similar transfusion rates. Tumor characteristics including nephrometry risk groups, median size, and pathologic stage were similar between groups. There was no difference in total perioperative complication rates although patients undergoing RALPN had significantly fewer high grade (Clavien 3/4) complications.Conclusions: Minimally invasive partial nephrectomy is associated with favorable perioperative outcomes and low morbidity. RALPN appears to be associated with favorable warm ischemia times and fewer serious complications when compared to LPN.
Comparison of Robot-Assisted and Open Partial Nephrectomy: Clinical Outcome and Complication Analysis
Introduction: There are few studies that have compared robot-assisted partial nephrectomy (RPN) with open partial nephrectomy (OPN). Purpose: The objective of this study was to compare the outcome of RPN and OPN perfomed by individual single surgeon.- Materials and Methods: We reviewed to compare RPN group of 67 patients with OPN group of 83 patients between April 2009 and June 2011 (26months). Results: There were no significant differences between the two groups with respect to age (p=0.107), sex (P=0.582), tumor size (P=0.256), tumor location (p=0.053), estimated blood loss (P=0.242) and change of estimated golomerular filtration rate (P=0.381). The length of hospitalization (2.97 vs 4.68 days, P<0.001) and use of postoperative analgesics were more favorable in the RPN cohort (P=0.037). The mean operative time (196 vs 126 min, P<0.001) and warm ischemia time (31 vs 27 min, P=0.032) was longer in the RPN group. Positive surgical margins was 1 for the RPN and 1 for the OPN groups (p=0.590). Complication rates were 15.7% and 14.9% in the RPN and OPN groups, respectively (P=0.901). Regarding RPN, complete obstruction due to ligation of renal pelvis and normal parenhymal excision leaving true mass were catastrophe.Conclusions: RPN could be a effective treatment option as a nephron-sparing surgery. But more careful approach are needed to avoid severe complication.
Benign Pathological Lesions After Laparoscopic Partial Nephrectomy in Preoperative Imaging Diagnosis of T1a Renal Cell Carcinoma
Introduction: Advancements in modern imaging techniques have increased the detection rate of asymptomatic renal tumors. It has led to the increasing use of nephron-sparing techniques, and may have resulted to the increasing incidence of benign pathological lesions. We here describe the incidence of benign pathological lesions after laparoscopic partial nephrectomy (LPN), and evaluated the predictive factors for such lesions in patients with preoperative imaging diagnosis of T1a renal cell carcinoma (RCC).
Materials and Methods: Between January 2000 and December 2010, 149 patients with clinical stage T1a RCC who had undergo partial nephrectomy (PN), were enrolled in this study. PN was carried out either open or laparoscopic approach. LPN was offered to tumor ≤ 3 cm in maximal diameter and>50% protruded tumor property. Open PN (OPN) was offered to tumor ≤ 4 cm in maximal diameter and not centrally located. The incidence of benign pathological lesions was evaluated.
Results: Seventy-seven patients (51.7%) were received LPN and 72 patients (48.3%) were received OPN. Benign pathological lesions were found in 13.0% of the LPN cohort, and 2.8% of the OPN cohort. Predictive factors were multivariate analyzed for benign pathological lesion, three parameters - age, gender, and LPN - proved statistically significant (P=0.0494, 0.0017, and 0.0066, respectively).
Conclusions: LPN was revealed significant predictive factor for benign pathological lesions. This result suggests that the possibility of correlation between exophytic tumor property and benign diagnosis in the incidence of benign pathological lesions after PN.
Prospective Comparison of en Bloc Hilar Ligation to Conventional Ligation During Laparoscopic Radical Nephrectomy for Early Renal Cell Carcinoma
PURPOSE: By evaluating the technical challenges encountered during 40 laparoscopic radical nephrecotmies, we have been able to modify the surgical technique to allow general urologists to effectively perform the procedure with minimal complications.DESIGN AND METHOD: A prospective protocol was performed on 40 patients who consecutively underwent laparoscopic radical nephrectomy. In 20 cases, the conventional technique was used, whereas in 20 cases the en bloc technique was used. Operating time, blood loss, transfusion requirements, intra- and postoperative complications, and the incidence of arteriovenous fistula (AVF) were documented. Follow-up included serial clinical evaluation and computed tomography angiogram at 3 months and repeated at 3-monthly intervals where indicated.RESULTS: Operative and postoperative parameters were improved in the en bloc group compared with the conventional group. In the en bloc group, the average operating time was 84 minutes and the average blood loss was scant. Postoperative complications were self-limiting and no patients developed post-nephrectomy AVF.CONCLUSION: The results of using the en bloc ligation technique for laparoscopic nephrectomy have been favorable in terms of operating time, risk to the patient, and surgeon's surgical preference. The risk of AVF formation after en bloc ligation of the renal pedicle was very low.
MP04: BPH Laser 1
Prevalence of Luts ed and bph; Apopulation Based Survey of Swedish Men
Background : Lower urinary tract symtoms (LUTS) and erectile dysfunction (ED) constitute a problem for the individual and a great burden for the society.The aim of this study was to investigate these problems in a cohort of swedish men but also try to correlate the findings to general health , coexisting morbidity and life conditions.Method : Qestionaries were sent to 3000 men(40-70 years) randomly selected.Qestions included IPSS , sexual function (IIES) demographic questions,Also health care seeking behavior was asked for.Socioeconomic status was registered.Results : LUTS was common also in younger men , 38% had IPSS above 8.There was a correlation between low socioeconomic status and high IPSS and Low IIES.37% reported IIES under 21.High IPSS was correlated to low IIES.A history of myocardial infarcton increased risk for LUTS and EDOnly 18 % had asked for medical advise for their problems.Study is ongoing and results preliminary at time for submission.Conclusions : LUTS and ED are common among middle aged men. Only 18 % had asked for medical advise for their problems.
Konyang Univ. Hospital, Gasoowon-dong, Seo-gu, Daejeon, Korea
Purpose: To compare the clinical therapeutic efficacy between finasteride and dutasteride as 5-alpha reductase inhibitor (5-ARI) in medical treatment of benign prostate hyperplasia.Materials and Methods: From 2007 July to 2010 July, 354 BPH patients with combination medication (alpha blocker and 5-ARI) were enrolled. These patients were classified into Finasteride medication group (F group) and Dutasteride medication group (D group). We initially checked total prostate volume(TPV), International Prostate Symptom Score (IPSS), quality of life score (QoL) , PSA, max flow rate (Qmax) and post-void residual urine (PVR). After at least twelve months of medication, we rechecked these clinical parameters and during medication, side effects related to medication were also recorded.Results: F group (n=129) and D group (n=225) showed no differences in baseline characteristics for age, TPV, IPSS, QoL scores and PSA . After medication, decreases in TPV were relatively higher in D group than F group (28.2 % vs 20.5 %). And decreases in PSA (43.6 % vs39.2 %), IPSS score (4.6 vs 3.5) were also higher in D group. There were no significant differences in QoL score, Qmax , PVR change and side effect between both groups.Conclusion: Dutasteride showed more efficacy in reduction of TPV, PSA and in symptomatic improvement by IPSS score than Finasteride. More large scale studies about the differences on clinical efficacy of finasteride and dutasteride are needed.
Prevalence of LUTS ED and BPH Apopulation Based Survey of Swedish Men Part 2 TRUL Flow Rate and pvr
Background:Lower urinary tract symtoms(LUTS) and erectile dysfunction(ED) constitute a problem for the individual and a burden for the society.The aim of this study was to investigate these problems in a cohort of swedish men and try to correlate them to coexisting diseases .3000 men(40-70 years) were randomly selected from natinal register.Demographic data registered.The participants answered questionaries( IPSS and IIES) and were investigated also with trul lab analyses flow rate and pvr.Results :Prostate size and psa increased with age.A correlation was found between high BMI and low IIES.We could not find a correlation between prostatic size and luts or ed or urinary flow rate.Study is ongoing and results preliminary at time for submission.Conclusions: LUTS and ED are common amomg middle aged men.There seems to be no correlation between prostatic size and flow rate, IPSS or ED.
Bipolar RF Thermotherapy for Chronic Prostatitis: 2 Years Follow Up
Introduction & Objectives:Chronic Prostatitis/Chronic Pelvic Pain Syndrome is a major health care burden which causes significant suffering to the.We are here reporting our results after 24 months follow up, using a minimal invasive treatment based on thermotherapy with the Tempro system (Direx-Initia).Material&Methods:We used Bipolar Radiofrequency Thermal Treatment with a protocol of 53,5 degrees Celsius for 60 minutes.All patients had symptoms at least 3 to 6 months, and have tried different drugs, without success.We have treated 60 relatively young patients, ages between 28 to 57 years (average 42 years). The mean prostate size was 40cc,out of which 33% were NIH Category II and 67% were Category IIIA. Results:37 Patients were available for follow at 24 months.Patients whose score decreased 50% or more were 18 (49%) and the ones that did not decreased 50% or more were 19 (51%). The mean Total CPSI Score improved from 23,4 to 14,0 (40%).Mean pain domain score improved from 12,1 to 5,7 (53%) and Quality of life domain score from 6,9 to 4,4 (37%).Conclusions:These results, with an overall success rate of 43% at 12 months and 49% at 24 months are very encouraging and show that results are maintained over this period of time.
2-Micron Continuous Wave Laser Vaporesection for the Treatment of Benign Prostatic Hyperplasia
Objective: To evaluate the safety and efficacy of 2 micron continuous wave laser vaporesection for the treatment of benign prostatic hyperplasia(BPH).Methods Fifty patients with obstructive BPH were treated with the revoLix 2 micron continuous wave laser vaporesection.the age ranged from 64 to 85 years with a mean of 71.5±5.2 years.mean prostatic volume was 75.0±15.0ml(ranged from 65 to 110ml).The operative time ,indwelling catheterization and operative complications were observed.The variables such as IPSS,QOL,Qmax,PVR were recorded and calculated pre- and post-operatively.Results The 2 micron continuous wave laser vaporesection was successfully performed on all the 50 patients with BPH.The mean operative time was 65±18.5 min.No significant bleeding was found during operation and no patients required blood transfusion.The average postoperative catheter time was 3.5±0.6 days.All cases were followed up for 6 months.IPSS and QOL score decreased from preoperative 26.8±4.5 and 5.1±1.1 to postoperative 5.4±1.8 and 1.2±0.6,respectively,Qmax increased from 5.9±2.2ml/s to 18.2±2.0ml/s,and PVR decreased from 126.5±65.3ml to 25.4±10.5ml.There were significant differences of these parameters between pre-and post-operation(P<0.01).No urinary incontinence occurred.Conclusion 2 micron continuous wave laser vaporesection of the prostate is a safe and efficient procedure in treatment of BPH,especially for those at advanced age or at high risk.
Division of Urology, University of Missouri, Columbia, Missouri, USA
Introduction and Objective: We present our experience and short-term results using the Evolve(TM) laser system as an in-office procedure under local anesthesia. Methods: Patients failing medical therapy and/or surgery underwent Evolve(TM) laser ablation in-office. American Urological Association Symptom Score (AUASS), maximum flow rate (Qmax), volumetric measurements, quality of life (QOL), and procedure success were investigated retrospectively. Results:40 consecutive patients with a mean age of 70.6±8.9 years, prostate volume was 42.6±15.3 mL underwent the procedure. Mean laser time was 23.9±6.7 minutes. Patients had a urethral catheter for a mean of 3.5±1.8 days. Intraoperatively, 2 patients had bladder spasms, 1 had pain during the procedure requiring re-injection of local anesthetic, and 1 had clonic leg spasms. 2 patients had long term post-op complications, 1 having prostatitis secondary to urinary tract infection and 1 patient with erectile dysfunction and incontinence. The mean AUASS decreased from 19.3 to 11.7 (p<0.01) and Qmax values increased from 11.1 to 19.6 ml/s (p<0.01) at 3 months to 2.3 years follow-up. Mean level of pain was 2 of 10 (max pain) during the procedure. Patient's QOL decreased to 1.5 from 3.6 (p<0.01) following procedure. 30 (91%) of the 33 patients reported the procedure as a success, 2 reported it as mixed, and 1 patient reported it as a failure. Conclusions: Evolve(TM) laser ablation is feasible, safe and efficacious as an in-office BPH treatement.
Department of Urology, Okayama University Graduate School of Medicine, Okayama, Japan
Introduction and Purpose: We evaluate the efficacy and safety of GreenLight HPS™ laser PVP for the treatment of benign prostatic hyperplasia (BPH) with different prostate volumes.
Materials and Methods: Based on the prostate volume measured by transrectal ultrasonography, patients were stratified into two groups: >=80 mL (group I) and<80 mL (group II). American Urological Association Symptom Score (AUASS), Quality of Life (QoL) score, maximum flow rate (Qmax) and post void residual (PVR) were measured preoperatively and at 1 and 4 weeks and 3, 6, 12, 18, 24 and 36 months postoperatively.
Results: 207 consecutive patients were identified (I: 57; II: 150). Among the preoperative parameters, there were significant differences (p<0.05) in the incidence of urinary retention (I: 24.6%; II: 7.3%), PSA (I: 4.5±2.7; II: 1.8±1.9 ng/mL), QoL (I: 4.2±1.1; II: 4.8±0.9) and prostate volume (I: 118.1±37.9; II: 48.5±15.5 mL), while AUASS, Qmax and PVR were similar (p>0.05). Significant differences (p<0.05) in laser utilization (I: 22.8±13.3; II: 10.4±6.4 minutes) and energy usage (I: 152.7±90.6; II: 70.9±44.8 kJ) were noted. Clinical outcomes (AUASS, QoL, Qmax and PVR) showed immediate and stable improvement from baseline (p<0.05) within each group, but no significant differences between the two groups were observed during the follow-up period (p>0.05). The incidence of adverse events were low and similar in both groups.
Conclusions: Our experience suggests that prostate volume has little effect on the efficacy and safety of GreenLight HPS™ laser PVP.
Bipolar Plasma Vaporisation of Prostate for Symptomatic Large Benign Prostatic Enlargement: Two-year clinical results
Vaporization of the prostate using bipolar high-frequency current applied to a novel mushroom-like electrode (Olympus, Germany) has recently been introduced. However, published studies on this technique only involved medium-sized prostates with at most 6-month follow-up.
To report the 2-year results of the Bipolar Plasma Vaporisation (BPV) technique in treating symptomatic large BPE.
From July 2008 to May 2011, 27 patients underwent BPV for symptomatic BPE in a prospective study. IPSS, TRUS prostate volume, Qmx and post-void residual (PVRU) were checked preoperatively. Postoperatively, they were evaluated at 3, 12, 24 and 36 months. Median follow-up was 22 months.
Intraoperatively, 3 patients required conversion to TURP (mechanical failure in 1 and slow progress in 2). There was no postoperative complication. At 3, 12 and 24 months, IPSS decreased from 20.5±7.7 preoperative to 11.6±8.6 (p=0.002), 14.1±12.5 (p=0.046) and 14.6±9.2 (p=0.138) respectively; prostate volume decreased from 92.8±42.8ml preoperative to 58.3±30.7 ml (p<0.001), 61.4±32.3ml (p=0.003) and 77.6±48.9ml (p=0.6); Qmx increased from 7.5±2.5ml/s to 11.1±3.6ml/s (p=0.009), 11.8±5.4ml/s (p=0.009) and 8.7±6.4ml/s (p=0.612); PVRU decreased from 137.8±68.3ml to 82.1±59.2ml (p=0.033), 90.3±83.1ml (p=0.241) and 132.7±102.6ml (p=0.499). Eight patients experienced deterioration of LUTS and required medical treatment at 15.6±9.1 month. Two patients experienced retention at 2 and 15 months. Three patients required re-operation at 15.7±7 months.
For large BPE, BPV resulted in clinical benefit that remained significant up to 12 months. Our cohort revealed with longer follow-up, the improvement in parameters seemed to be lost.
Department of Urology, Okayama University Graduate School of Medicine, Okayama, Japan
Introduction and Objective: GreenLight XPS™ laser PVP is a recently approved treatment option for lower urinary tract symptoms (LUTS) secondary to BPH. We review our perioperative experience using this technique.
Methods: We prospectively evaluated our initial experience with GreenLight XPS™ laser PVP. All patients who failed medical therapy underwent GreenLight HPS™ laser PVP (CW). All had American Urological Association Symptom Score (AUASS), Sexual Health Inventory for Men (SHIM) score, American Society of Anesthesiologists (ASA) risk score, serum prostate specific antigen (PSA), maximum flow rate (Qmax) and post void residual (PVR) determinations and volumetric measurements with transrectal ultrasonography. Transurethral PVP was performed using a GreenLight XPS™ side-firing laser system.
Results: 8 consecutive patients were identified, having a mean age of 73.0±12.1 years. The mean prostate volume was 67.5±16.4 mL and mean ASA score was 3.1±0.6. Mean laser time, operating time and energy usage were 5.9±3.0 minutes, 24.0±11.0 minutes, and 79.8±17.9 kJ, respectively. All were outpatient procedures with 6(75.0%) patients catheter-free at discharge. 1(12.5%) patient required catheter drainage for one week. 1(12.5%) patient developed a urinary tract infection. None had persistent hematuria>1 week or post-procedure irritative voiding symptoms. No bladder neck contractures or urethral strictures have been noted. Mean AUASS decreased from 24.6 at baseline to 7.3 and 6.9 at 1 and 4 weeks. Qmax and PVR values showed statistical significant improvement (p<0.05).
Conclusions: Our preliminary results suggest that GreenLight XPS™ laser PVP is safe, effective and efficient for the treatment of LUTS secondary to BPH. Continued follow-up is in progress.
King's College Hospital, London, UK
Introduction: We report the results of GreenLight 120W laser prostatectomy (GLL) with a minimum of one year follow-up in terms of urinary symptoms, energy usage and prostate volume reduction.
Methods: We prospectively evaluated patients treated with GLL HPS for LUTS in 7 International centres. Operation, hospitalization and catheterization times were recorded. Functional results, improvement of IPSS, Qmax, and postvoid residual (PVR), as well as Joules delivered were assessed at baseline, 3months and 12months.
Results: Of 257 patients, 162 (63%) had completed 12month of minimum follow-up at the time of submission. Median age was 66 (range 33-93years). Median operation time was 61.5min (range 9-201min) and median hospitalization was 20hrs (range 2 hrs-7 days); median catheterization times were 16hrs (range 2hrs-7days). No major complications were recorded. Mean prostate volume was 61.8g (±40.43g) and 36.3g (±22.08g)) at 1-year (p=0.0001). Mean PSA fell from 5.7ng/ml (±13.5ng/ml) to 3.3ng/ml (±6.5ng/ml) at 1 year (p=0.01). IPSS improved from 20.5 (±8.8) to 6.5 (±5.7) (p=0.0001), and QoL from 4.3 (±1.5) to 1.3 (±1.3)(p=0.0001). Maximum flow rate and PVR improved from 8.2ml/sec (±6.4ml/sec) and 215.9ml (±341.2ml/sec), respectively, to 19.7ml/sec (±10.2ml/sec) and 38.6ml (±78.6mls p=0.0001), respectively.
Conclusion: Prostate laser prostatectomy using the GreenLight HPS 120-W laser shows excellent results at 1 year follow-up, with significant improvement of IPSS, flow rate, PVR, PSA, prostate volume and QoL. Complications were few and minor.
Department of Urology, University Hospital Basel, University of Basel, Base, Switzerland
Objective: To evaluate safety and early results of the newest generation of Greenlight laser prostatectomy.Patient and Mehtod: Prospective consecutive data collection of patients treated with 180 W XPS laser prostatectomy at seven centres worldwide since June 2010. Indications for surgery based on practical and local recommendation and of the given AUA- or EAU guidelines. Patients receiving anticoagulants or those with a history of acute or chronic retention were included.Intervention: Photoselective vaporisation of the prostate with the 180 W GreenLight laser utilizing the MoXy fibre.Measurement: Subjective (e.g. IPSS) and objective parameters (e.g. Qmax, RV, side effects and complication rate) are presented with 3 mos. follow-up. Perioperative complication rate is presentedResults: Finally, 215 patients underwent XPS laser vaporisation with the MoXy fibre. Means were as follows: age 71±9 yrs.; prostate volume; preop. Qmax 8.5±4.0 ml/s, preop IPSS 20±7. About one forth of patients had a prostate size larger than 80ml. For a mean preop. prostate size of 68±42 ml on average 277±211 kJ energy were applied during a lasing time of 38±20 min. After 3 months results were as follows: Qmax 18±9ml/s; RV 45±85ml, IPSS 8±6 and prostate volume was 38±16ml. Perioperative complications were low. No severe complication or transfusion was reported.Conclusions: The 180 W XPS GreenLight is a new promising minimally-invasive treatment option for transurethral laser prostatectomy. It provides excellent safety and significantly easier handling of larger prostates. Perioperative complication rate is low, as know from previous GreenLight laser systems too.
Does an Increae in Power Lead to Improved Tissue Abaltion? Initial Clinical Results of the 180W XPS GreenLight Laser
Introduction:In vivo experiments demonstrate that the increased power of the 180W XPS GreenLight laser leads to a doubling of vaporization speed in comparison to predecessors. However, clinical data confirming this observation are scarce. Purpose:Comparison of vaporization parameters of the 180W XPS laser with the 80W and 120W laser. Material and Methods:Intraoperative data, complications and early postoperative results of the first 60 patients who underwent laser vaporization of the prostate with the 180W laser were compared with data from 60 consecutive patienst who underwent surgery with the 80W and 120W laser. Results:Age, PSA and prostate volume were comparable between the groups. Duration of surgery was comparable, however, application of energy was significantly higher in the 180W group (180W: 305±190 kJ; 120W: 188±128 kJ, p<0.05; 80W: 187±63 kJ, p<0.05). Furthermore, energy per prostate volume (180W: 5.3±2.8 kJ/ml; 120W: 3.0±1.4 kJ/ml; 80W: 3.9±1.3 kJ/ml) and energy per operation time (180W: 4.8±1.8 kJ/min; 120W: 3.0±1.3 kJ/min; 80W: 2.9±0.7 kJ/ml) were significantly (p<0.05) higher in the 180W group. The rate of intraoperative bleeding (180W: 8.9%, 120W: 13.2%, 80W: 4.4%) and capsule perforation (180W: 5.9%, 120W: 5.9%, 80W: 0%) were comparable with the 120W laser. 3 months postoperatively, all groups showed an improvement of voiding parameters and symptoms, the reduction of PSA was significantly higher in the 180W group.Conclusion: Our date confirm an increased tissue ablation with the 180W laser. However, a longer follow up is necessary to evaluate if the increased tissue ablation transfers into superior clinical results.
Green-Light Laser Photovaporization of Prostate, Comparison of Clinical Results Using 80 and 120-Watts Energy Systems.

Photoselective Vaporisation of the Prostate Using the 180W Lithium Triborate Laser
PVP has become an established surgical treatment for BPH. Since the recent introduction of the 180W LBO laser with its liquid cooled laser fibre, there has been little experience reported.
To evaluate the safety and efficacy of using the 180W LBO laser PVP and its liquid cooled laser fibre in the surgical treatment of BPH.
A retrospective analysis of prospectively collected data of all men treated by the 180W LBO laser between July 2010-May 2011 by a single surgeon was performed (n=57, median age 67 years, median prostate volume 70cc). Perioperative and functional outcomes were assessed at baseline, 3 months and 6 months post-operation.
Of 57 patients, 9 were in urinary retention and 20 were on antiplatelet/anticoagulant medication. Median operation time was 57 minutes, laser time 46 minutes, postoperative duration of catheterisation 13 hours, and duration of hospitalisation 18 hours. Functional outcomes at baseline, 3 months, and 6 months respectively were IPSS 20.5, 7.5, 4.5; QoL 4, 2, 1; Qmax 9.2, 25, 21.5; PVR 149.5, 31, 45. There was significant improvement in functional outcomes at 3 and 6 months (p<0.01). Eleven (19%) patients experienced a complication, of which 10 were Clavien grade I-III, 1 grade IV with posterior capsular perforation, and no grade V. Forty-eight (84%) men were able to be discharged home catheter-free within 24 hours.
Our early experience indicates that the 180W LBO laser PVP is a safe and efficacious treatment for men with BPH. Eighty-four percent of men who underwent this treatment went home catheter-free within 24 hours.
Photoselective Vaporisation of the Prostate in the Treatment of Men in Urinary Retention
Whilst PVP is used to treat BPH, there is little described about its performance in urinary retention.
To evaluate the efficacy and safety of PVP by HPS 120W LBO laser to treat men in urinary retention.
Retrospective analysis of prospectively collected data of all men in urinary retention who underwent treatment with 120W LBO laser PVP by a single surgeon from November 2006-July 2010 was performed (n=78, median age 71 years, prostate volume 91cc). Perioperative outcomes, and functional outcomes at baseline, 3 and 12 months postoperation were examined.
Patients managed preoperatively by urethral catheter (n=61) and SPC (n=5) were of greater age (8.2 years, p<0.05) and higher ASA scores (p=0.000, Fishers exact test mid p) than patients managed by ISC (n=12), but there was no difference in outcomes. Median operating time was 86 minutes, duration of catheterisation 13 hours, and duration of hospitalisation 18 hours. There was 1 Clavien grade III-IV complication, no grade V, and no requirement for blood transfusion. Fifty-three men (68%) were discharged home catheter-free within 24 hours. At baseline, 3 months, 12 months, median IPSS was 19, 7, 6; QoL 5, 1, 1; Qmax 6.1, 18.5, 22; and PVR 209, 52, 60 respectively. Paired data analysis demonstrated significant (p<0.05) improvement in functional outcomes.
PVP for urinary retention is not only efficacious and safe, but also associated with short duration of catheterisation, short hospitalisation, and can be used in anticoagulated men. Sixty-eight percent of men were discharged home catheter-free within 24 hours, and none required blood transfusion.
Photoselective Vaporisation of the Prostate (PVP) and Transurethral Resection of the Prostate (TURP) Have Similar Operative Times in Experienced Hands
Department of Urology, University Hospital of Larissa, Larissa, Greece
Introduction: Bipolar plasma vaporisation of the prostate with a mushroom-like electrode was recently introduced to achieve tissue vaporisation. In addition, men in retention represent a specific group of benign prostatic hyperplasia (BPH) patients that in general are at increased risk of perioperative morbidity and present a lower response to any treatment that resolves obstruction.Purpose: To evaluate the efficacy and safety of transurethral bipolar plasma vaporization of prostate in patients with retention due to BPH.Material and Methods: Overall, 26 patients were included in the study and underwent transurethral bipolar plasma vaporization of prostate (Olympus, Germany). Success rate, defined as the percentage of patients who regained their ability to void spontaneously, was the primary endpoint. International Prostate Symptom Score (IPSS), maximum flow rate (Qmax), and postvoid residual (PVR), were recorded at 3 months. Need for transfusion, difference in serum sodium concentration (pre- and post-operatively) and occurrence of any adverse event were also recorded to evaluate safety. Results: The success rate was 100% after removal of the catheter. Postoperatively, transient mild to moderate dysuria was seen in five patients. At 3 months mean IPSS was 8.1 (range 4-13) and mean Qmax 17.1 ml/s (12-23), while PVR was 55 ml (0-110). No patient required transfusion and there was not significant difference in sodium concentration. One patient experienced bladder neck stenosis.Conclusions: Our initial data with a short follow-up indicate that transurethral bipolar plasma vaporization of prostate seems to be effective and safe in patients in retention.
Department of Urology, Casa di Cura I.N.I., Grottaferrata, Italy
The light of diode lasers for the treatment of benign prostatic hyperplasia that operate on wavelengths in the near infrared is absorbed in both hemoglobin and water which leads to good hemostasis.
To assess the clinical value of the high power diode laser Dornier Medilas D UroBeam.
Since June 2008, the Dornier Medilas D UroBeam (Dornier MedTech, Wessling, Germany), operating at 940 nanometers and emitting a maximum power of 250 Watt in cw mode, was applied for treating BPH. Patients with prior prostate surgery were excluded. After operation, we saw the patients at 1, 3, 6, and 12 months.
In total, 98 patients were treated. 60 patients have reached 12 months of follow-up so far. Mean age of the patients was 73,8 years; pre-operative TRUS volume: 55,9 ml. 18/60 patients suffered from acute urinary retention, 46/60 were on alpha-blockers, and 26/60 were on anticoagulants when presenting for intervention. 2/60 patients experienced peri-operative bleeding. At 12 months, compared to pre-operatively, the mean maximum flow rate increased from 10,0 ml to 19,7 ml; mean IPSS dropped from 19,6 to 7,5; and mean post-void urine volume dropped from 82,4 ml to 25,5 ml.
The treatment of BPH with the high power diode laser in continuous wave mode at 250 W provides good clinical outcome regarding peri-operative bleeding and post-operative IPSS, maximal flow rate and residual urine in the follow-up of 12 months. Further studies with extended follow-up and patient numbers are needed to confirm these data.
Outcome of Incidental T1a & b Prostate Cancers in the PSA Era: Implications for Photo-Selective Vaporization (PVP) of the Prostate
Introduction: The advent of PVP has challenged the gold standard TURP for treatment of bladder outlet obstruction. However, despite advantages of reduced bleeding and hospital stay of these new laser procedures, there is the loss of prostate tissue examination, and therefore potential to miss an incidental prostate cancer diagnosis. The clinical outcome of these patients is not well described. Objective: To determine the clinical outcome of patients incidentally identified with prostate cancer by TURP. Materials and Methods: Histopathology records of all TURPs performed in a tertiary hospital from 1999-2009 were analysed retrospectively to identify incidental cases of prostate cancer. Patients known to have prostate cancer prior to TURP were excluded. Subsequent treatment, morbidity and mortality were recorded. Results: Of the 31 (4.1% of total TURP cases) new prostate cancer diagnoses, a Gleason score of 3+3 was the most common, reported in 10 patients (32.3%) whilst a score of 5+4 and 4+3 were found in 1 (3.2%) and 3 (9.7%) patients respectively. 8 patients subsequently received formal prostate biopsies and 4 (12.9%) had definitive prostate cancer treatment. Of the 3 patients who have since died (aged 72, 75, 87), one was due to metastatic bowel cancer and the cause of death in the other two patients is unknown. Conclusion: Although a small proportion of prostate cancer diagnoses would be missed in patients undergoing PVP, there is no significant improvement in the clinical outcome for the vast majority of patients; most likely reflecting the indolent and non-aggressive nature of early prostate cancer.
Department of Urology, University Hospital Basel, Basel, Switzerland
Introduction:Photoselective vaporization of the prostate (PVP) with the greenlight laser has emerged as a treatment alternative to transurethral resection of the prostate (TURP). Despite the widepread use of the technique longterm results of PVP in comparison to TURP are scarce. Purpose:Prospective non randomized comparison between PVP and TURP. Materials and Methods:200 patients who underwent PVP with the 80-W KPT-laser or TURP between 09/2002 and 12/2005 were compared. Micturition symptoms (IPSS, QoL), voiding parameters (peak urine flow, postvoid residue volume), PSA value and the reoperation rate were analyzed. Results: Mean patient age, prostate volume and operation time were comparable in both groups, whereas the length of hospital stay was shorter in the PVP group. After 60 months IPSS (p=0.005), QoL (p<0.01), peak urine flow (p<0.05) and postvoid residue volume (p<0.05) improved significantly after PVP while PSA-reduction did not meet significance. In the TURP-group, IPSS (p<0.005), QoL (p<0.005), postvoid residue volume (p<0.05) and PSA (p<0.005) deceased singificantly after 60 months , the increase in peak urine flow did not meet statistical significance. During follow-up one or more reoperations were necessary in 21% of the patients after PVP and in 7% after TURP (p<0.05) due to bladder neck sclerosis (4% vs. 1%), recurrent adenoma (14% vs. 5%) or urethral stricture (8% vs. 1%).Conclusions: Both techniques lead to an improvement of voiding parameters and micturition symptoms during long-term follow-up. However, the reoperation rate is significantly higher after PVP with the 80-W laser suggesting a lower tissue ablation capacity.
MP05: Urolithiasis 1
High-Risk Nephrolithiasis Predominates in Inner-City Populations- Population Based Study
Introduction:The Bronx represents a unique community with multi-ethnic diversity, low socioeconomic status, and a high incidence of metabolic syndrome. The 2009 American Community Survey documented 22.9% Caucasians, 35.4% African Americans, and 52% Hispanics and Latinos in the Bronx. Kidney stones are prevalent. Theres a paucity of population studies in this population. Purpose: To survey stone analysis in a contemporary PCNL population.Materials and Methods:Patients who underwent percutaneous nephrostolithotomy between June 2005 and August 2010 were retrospectively reviewed. Data amassed included stone analysis, stone composition, BMI, and comorbidities. 2-sided Students t-test used for analysis. Results:180 patients were included in our analysis. Mean age was 52 years. 72 male and 108 female patients were included. 98 of the patients were hispanic and 30% African American. 86 of the patient population were found to be obese BMI>25 and 36 had type II diabetes mellitus. Diabetic patients had a greater BMIthan non-diabetic patients p<0.05. A review of stone composition data demonstrated a predominance of calcium-oxalate-monohydrate stones in all ethnic groups-58%. Non-hispanic patients were found to have a significantly greater incidence of uric acid stones p<0.05.Conclusion:We have found an extremely high rate of predominantly calcium oxalate monohydrate stones in all population groups, with the highest rate among Hispanic and Latino patients. Hispanic patients undergoing PCNL appear to have a lower incidence of uric acid nephrolithiasis than other groups. Recognition of the preponderance of very dense stone composition in Bronx patients may help to guide most appropriate therapy for these patients.
Changing Stone Composition Profile of Children with Nephrolithiasis
Introduction: Adult patients with nephrolithiasis increasingly have calcium phosphate stones, especially those with recurrent disease. We hypothesized that similar trends may be present in children. Methods: We reviewed records of 179 patients managed from 1992-2010 (0.2 to 18 years old) for whom stone analysis data were available. We compared patients managed from 1992-2000 (P1) and 2001-2010 (P2). Results: Overall average age of manifestation did not differ between periods. Males comprised significantly higher proportion of patients developing stones during first decade of life, with male:female ratio 1.9:1. Contrastingly, females comprised significantly higher proportion of patients developing stones during second decade of life, with female:male ratio 1.7:1. Both trends were similar in P1 and P2. Higher percentage of patients had calcium oxalate stones (CaOx) in P1 compared to P2 (60%vs47%, p=0.0019). There was significant increase in percentage of patients having calcium phosphate stones (CaP) in P2 compared to P1 (27%vs18.5%, p=0.008). Twenty-seven patients had recurrent stones. Comparing composition of first and last stones of patients within this group demonstrated increase proportion of brushite stones (3.7% versus 11.1 %, p=0.04). 24 hour urine testing undertaken in 62 children with calcium containing stones (49 CaOx and 13CaP), with no statistically significant differences in urinary parameters of patients with CaOx stones compared with patients having CaP stones.Conclusion: An increasing number of children with kidney stones have CaP calculi. Brushite stones are more prevalent in children with recurrent stone events. The impetus of these shifts is not readily apparent and requires further investigation.
Quality Improvement and Clinical Outcomes of Nephrolithiasis in the Underserved Population
INTRODUCTION AND PURPOSE:LAC + USC Medical Center is the largest provider of healthcare in Los Angeles County, where 71% of patients are uninsured.Nephrolithiasis treatment had been mired in bureaucracy, scheduling delays and complications. In July 2009, a capital investment allowed development of a streamlined management process. We compare two management eras to determine whether a streamlined process and clinical integration impact healthcare quality and resource utilization.METHODS:In total, 254 charts were reviewed of patients undergoing surgery for nephroureterolithiasis. In Era 1, January 2007 to June 2009, 154 patients underwent stone surgery. In July 2009, a capital investment funded a dedicated OR, a standardized referral process, and integrated scheduling. In Era 2, the year following integration, 80 patients were treated. We compared patient demographics, stone size, and quality measurements (time to surgery, pre-surgical procedure rate, procedural complication rate, and number of healthcare encounters). Utilization measurements include number of prescriptions and pre-operative imaging. Clinical outcomes include surgical complication rate, stone-free rate, and secondary-procedure rate.RESULTS:We observed a decrease in average time to surgery, percentage of patients requiring pre-operative procedures, average number of procedures per patient and procedural complication rate (all p<0.01). Average number of pre-operative ER visits, clinic visits, prescriptions and pre-operative imaging studies all decreased (all p<0.01). Stone free rates were higher and secondary-procedure rates were lower for ureteroscopy than ESWL (p=0.02, p=0.047). CONCLUSIONS:Organizational integration in the management of nephrolithiasis provides an opportunity for improved clinical outcomes, enhanced quality of healthcare delivery, and reduced resource utilization.
Evolution of Stone Management in Australia
Introduction: The management of upper urinary tract stone disease has evolved significantly in the last three decades. The advent of shock wave lithotripsy and improvement in endoscopic equipment has brought about a paradigm shift in the way stones are now managed. Objective: To examine trends in the operative management of stone disease in Australia over the past 15 years. Materials and methods: The Medicare Australia and Australian Institute of Health and Welfare (AIHW) databases were used to determine the annual number of procedural interventions undertaken for stone disease. Results: In Australia over the past 15 years, the annual number of procedural interventions for upper urinary tract stones has increased, primarily due to the rising number of endoscopic procedures performed. Shock wave lithotripsy numbers peaked in the early 2000s but have since fallen, while open and percutaneous procedures have been in decline. Conclusion: There has been a significant increase in the use of ureteroscopy and pyeloscopy in Australia, however further studies are required to determine whether this trend is due to an increase in the incidence of stone disease, higher retreatment rate or a lower intervention threshold.
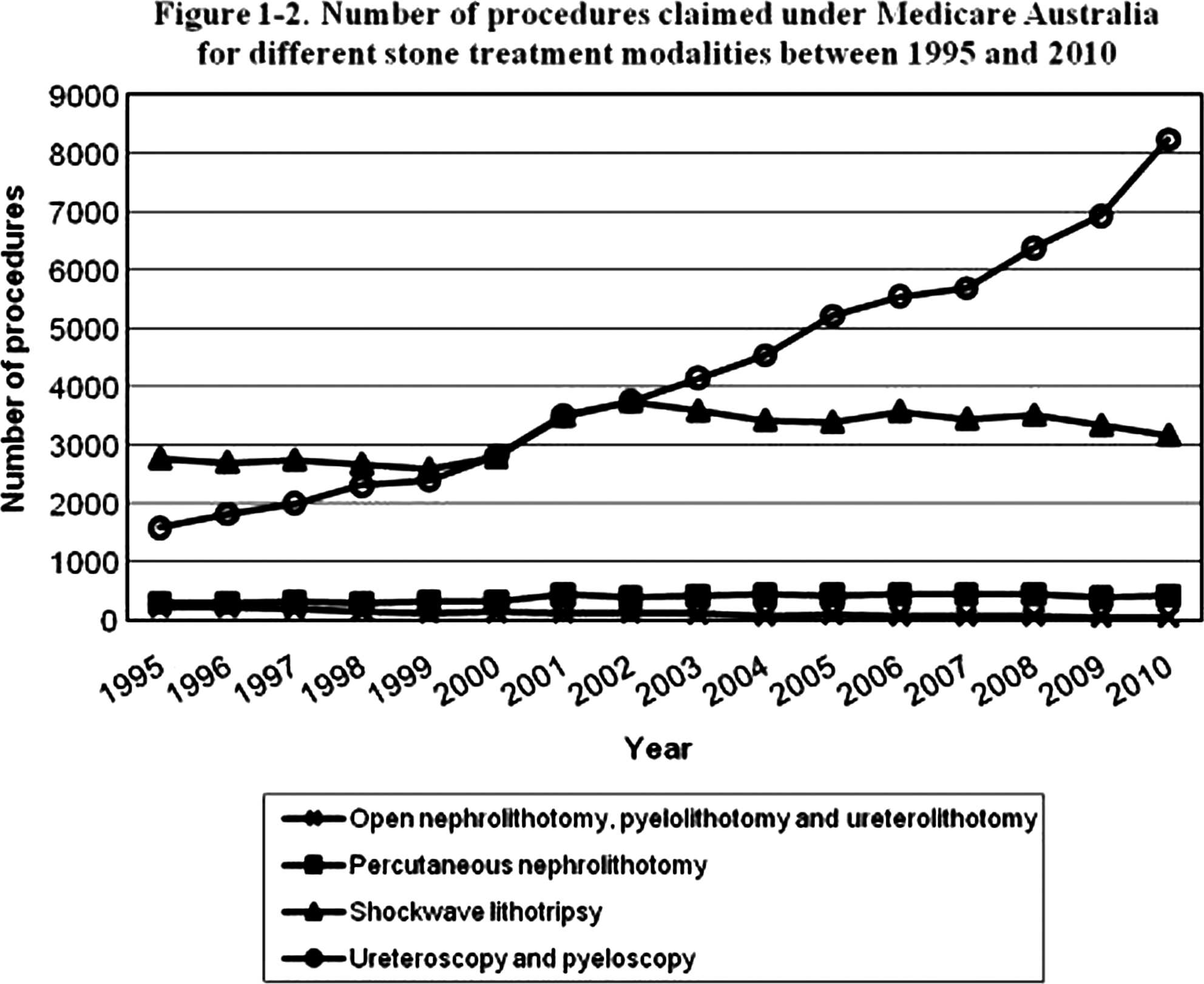
Department of Urology, Klinikum Sindelfingen, University of Tuebingen, Sindelfingen, Germany
Introduction: With the improvements in endourological techniques and optimized outcomes, metabolic evaluation and stone prevention became less important for many urologists. This international survey by the EAU sections for Urolithiasis (EULIS) and Uro-Technology (ESUT) aims to evaluate the current pattern of metabolic stone evaluation.Material and methods: An online survey was created and distributed through mailing lists. The questions to be answered included demographic data and information on interventional and metabolic concepts. Data collection started May 2011 and was closed July 2011. Results: 220 responders from Europe, Northern and South America, Arabia and Asia completed the survey. Average number of stone patients per urologist and year was 299.4 (total 52.697). 84.1% of the urologist believe that metabolic evaluation reduces stone recurrences and 72% assume cost-effectiveness. 89.2% perform metabolic evaluation, which is done by the urologist in 74.4%. The indication for further examination is based on risk profiles in 73.2%. Urine analysis is done by one 24h urine (62.1%), 31.4% perform two urine collections, while extensive protocols are rarely performed. Infrared spectroscopy is the method of choice for stone analysis, however, 39.3% were unsure about their methodology.Conclusion: Most international urologists perform metabolic evaluation. It is accepted that metabolic management reduces recurrences and is cost-effective. However, the standard of care is less clear. Only one third perform two urine collections, which is in contrast to current guideline recommendations. Almost half of the responders were not sure about the method of stone analysis. This illustrates the necessity of regular educational activities.
Targeted Intervention Versus Conservative Intervention for the Prevention of Kidney Stone Recurrence
Introduction: Conservative advice consists of increasing fluid intake, limiting protein, sodium and oxalate, and moderate calcium intake. Alternatively, performing two-24 hour urine tests can highlight specific metabolic abnormalities and targeted approaches such as selective dietary restriction, potassium citrate, or thiazide diuretics can be tailored. Conservative therapy is less costly, however not known if it is as effective as targeted therapy in preventing kidney stones.Purpose: We sought to compare conservative versus targeted preventative therapies.Materials and Methods: A retrospective chart review of patients from the Stone Centre at Vancouver General Hospital was performed involving 98 patients with recurrent metabolic stone disease, consisting of 24-hour urine collection while on a random diet and after dietary modification. Sex, age, body mass index (BMI), medical risk factors, anatomical risk factors, follow-up length, stone recurrences, and changes in volume, calcium, oxalate, citrate, sodium, and uric acid in the 24-hour urine samples were compared between targeted and conservative treatment groups.Results: There was no difference observed in urinary oxalate, calcium, or citrate between groups. Urinary sodium (p=0.014) and uric acid (p<0.001) increased for the targeted metabolic management. In the obese population, there was a significant increase in the urinary sodium (p=0.003) and volume (p=0.034) for the targeted treatment group. There was no difference in stone recurrence rates between groups with a mean follow-up of 6.8 months (p=0.391).Conclusions: From our results, both approaches in the management of patients at our centre have equal validity. More patients and further data analysis with longer follow-up are required.
Are 24 Hour Urine Samples Collected Prior to Stone Removal or with a Ureteral Stent in Place Still Reliable?
Background: Twenty-four hour urine samples collected for the management of stone disease are traditionally obtained 3-6 weeks after the patient has been cleared of all stones or ureteral stents. Purpose: We compared the results of 24 hour urine samples obtained before stone removal, with an indwelling ureteral stent and 3-6 weeks after stent removal. Methods: Thirty nine patients with radiographically confirmed stones were enrolled in a prospective study in which 24 hour urine samples were collected before stone removal, with a ureteral stent after stone removal and 3-6 weeks after stent removal. Only patients without infected urine or non-obstructing stones were enrolled in the study. All 24 hour urine samples were analyzed by Litholink Inc. Results: Thirty three patients had completed data at the time of analysis. The average time the ureteral stent was in place was 14.7 days (range 6-47 days). Eighty four percent of the stones retrieved were primarily calcium oxalate monohydrate. Twenty-four hour urine samples collected before stone removal, with an indwelling ureteral stent and 3-6 weeks after stent removal were not significantly different in any category except phosphorous (p=0.043). Conclusion: Twenty-four hour urine collection samples before the surgical removal of the stone or while the ureteral stent is in place appears to be as useful as urine obtained after stone or stent removal.
Twenty Four Hour Urine Parameters and Stent Encrustation: Can We Predict the Patients Who Are Prone to Encrustation?
Background: A recognized problem with ureteral stent placement is the variable level and rate of encrustation for different patients. Purpose: To determine what factors on a 24hr urine study are associated with stent encrustation in patients with urolithiasis. Materials and Methods: Thirty subjects undergoing urological surgery for urolithiasis with planned stent placement were consented into the study. Twenty four hour urine samples were obtained prior to treatment, after stone removal but with an indwelling stent, and 3-6 weeks after stent removal. Visualized stent encrustation was noted (yes or no) and dry weight of the stent was also obtained before and after removal. Results: Twenty-one subjects had complete data for analysis. Stents remained indwelling for an average 16.5 days (range 6- 47 days. Encrustation was visible in 4 patients. These subjects had significantly less urinary oxalate (p=0.038) and less phosphorous (p=0.026) in the urine collected with a ureteral stent and less phosphorous (p=0.049) in the post-stent removal sample compared to the subjects without visible encrustation. Pre-stent urinary parameters were not significantly different between the groups. Changes in the dried weight of the ureteral stent correlated significantly with pre-stent urinary pH (r=0.518, p=0.03). Conclusion: Urinary oxalate, phosphorous and pH may play a role in the encrustation of indwelling ureteral stents. More data is needed to determine if 24 hour urine parameters can be used to identify patients at risk for early encrustation.
Glyoxal Metabolism: A Novel Pathway in Endogenous Oxalate Synthesis
Introduction: Basic knowledge about oxalate formation is limited. This study aimed to demonstrate the hypothesized link between glyoxal, oxalate production, and diabetes mellitus. Methods: Three model systems were employed to test whether glyoxal metabolism results in oxalate synthesis: human liver lysates, HepG2 cells, and human red blood cells. Cells were incubated with varying concentrations of glyoxal over certain time periods. Glyoxylate, glycolate and oxalate were measured in these model systems. The effect of glutathione depletion on erythrocyte conversion of glyoxal to oxalate and glycolate was also studied.Results: In human liver lysates treated with increasing concentrations of glyoxal, there was linear increase in glyoxylate production. Human liver lysates treated with glyoxal were incubated with cofactors (NAD + or NADP+) and/or disulfiram (inhibitor of aldehyde dehydrogenase). Human liver lysates only converted glyoxal to glyoxylate in presence of NAD +, which was inhibited by disulfiram. As glyoxal concentrations increased in HepG2 cells, there was linear increase in glycolate and oxalate production, with significantly more glycolate produced. Incubating red blood cells with both glyoxal and menadione resulted in significantly more production of oxalate and decreased production of glycolate. Human erythrocytes cultured under hyperglycemic conditions yielded both glycolate and oxalate; normoglycemic conditions did not yield oxalate or glycolate. Conclusion: The conversion of glyoxal to glyoxylate likely by aldehyde dehydrogenase occurs in liver tissue. Glyoxal can result in oxalate formation in vitro. Under oxidative stress, an increased flux of glyoxal to oxalate formation occurs. Defining this pathway should provide novel insights into pathophysiology of calcium oxalate nephrolihtiasis.
Predictive Factors of Bacteriuria in Patients of Ureteral Calculi Who Visit Emergency Room
Objectwe assessed the possibility to progress APN in patients with ureteral calculi using emergency laboratory test. Materials and MethodsRetrospective chart review of 1,156 patients who visit emergency room (ER) was performed on all afebrile (<38C) patients with ureteral calculi between January 2007 and June 2010. Emergency laboratory test and urine culture were obtained at ER. Exclusion criteria were patients without laboratory test and with bilateral ureteral calculi (n=388). The impact of the above mentioned possible predictors on the presence of bacteriuria were evaluated by logistic regression analysis. Receiver operator characteristic (ROC) curve was generated for the comparison of the predictive powers of various predictors. ResultsOf the 768 patients, bacteriuria was found in 170 patients, and most common detected bacteria were E.coli (n=63). In unadjusted model, age, the presence of DM, leukocyte count, ANC, and the presence of pyuria were associated with bacteriuria. In adjusted model, age and ANC were significant factors (age: 1.003-1.029, P=0.016, ANC: 1.002-1.005, P<0.001). Ideal cufoff value for bacteriuria were 8,190/μl (sensitivity: 53%, specificity: 83%, 95 % confidence interval) and 54yrs (sensitivity:52%, specificity: 64%, 95 % confidence interval). The area under the ROC curve was significantly higher for ANC compared with age with 95% confidence interval (ANC: 0.709, age: 0.587, P<0.001). ConclusionANC (>8,190/μl) could be used to predict infection in afebrile patients with ureteral calculi. In those cases, antibiotics could be useful to protect bacteriuria.
Positive Stone Culture is Associated with Urosepsis After Endourological Procedures - An Update
Objectives: The purpose of this study was to determine how well urine and stone cultures are correlated with postoperative infection and the offending pathogen in patients treated for kidney stones.
Methods: 328 consecutive patients who underwent PCNL or ureteroscopy from July 2006- November 2009 were identified, all of whom had a stone culture obtained during surgery. All had a preoperative urine culture. 274 underwent ureteroscopy, and 54 PCNL. All patients had either negative preoperative urine cultures or antibiotics for 1-7 days prior to surgery. Stone fragments were obtained during the procedure and sent for analysis. The primary endpoint was urosepsis defined as postoperative fever requiring admission.
Results: Of 328 patients who had both urine and stone cultures, 11 (3%) were admitted for urosepsis postoperatively. 8/11 (73%) had positive stone cultures, while none had a positive preoperative urine culture. Overall, 96/328 had a positive stone culture, while only 3/232 with negative stone cultures were admitted (p=0.003). The urine culture obtained on readmission grew the same pathogen as the stone culture in 7/11 patients (64%) compared to 1/11 (9%) of preoperative urine cultures (p=0.02).
Conclusions: The pathogen causing infection had a higher correlation with the organism grown on stone culture than the preoperative urine culture. The patients who developed urosepsis did so despite preoperative antibiotics, and the pathogen grown on the preoperative urine culture was different from that seen post operatively. These results suggest that stone culture is more effective than preoperative urine culture for determining treatment of urosepsis.
IU Health Physicians - Urology
Introduction: Voided urine culture is performed routinely in most patients undergoing surgical treatment of stones. There is mixed data regarding correlation between positive urine and stone cultures. Purpose: To examine the correlation between positive urine culture and positive stone culture.Methods: We retrospectively reviewed data from patients in our IRB-approved database that underwent percutaneous nephrolithotomy (PNL) between April 1999 and May 2009. Of 931 consecutive patients, 548 (58.9%) had intra-operative stone culture data. Among these, 498 (90.1%) had preoperative urine culture data. For each patient, the results of stone culture were compared to the pre-operative urine culture.Results: 205 of the 498 patients (41.2%) had positive stone cultures. In patients with positive stone cultures, 153 (74.6%) had positive pre-operative urine cultures. Thus, 25.4% of patients with positive stone cultures had negative pre-operative urine cultures. In patients with positive stone culture and positive urine culture, the urine culture was in agreement with stone culture in 58% of cases. 231 out of 498 patients (46%) had positive pre-operative urine cultures, and of these patients 83 (35%) had negative stone cultures.Conclusions: Pre-operative urine culture is not a highly sensitive tool for identifying infected renal calculi, with a greater than 25% false negative rate. Moreover, bladder urine cultures do not reliably predict the organism present in the infected stone, with more than 40% discordance between bladder and stone cultures. These results support the routine collection of stone samples for culture during PNL, to insure that infections are accurately identified and treated.
Prospective Interventional Trial of Calcium Carbonate Supplements on Hyperoxaluria in Stone Formers
Introduction: Hyperoxaluria is a well known risk factor for recurrent nephrolithiasis. The magnitude of effect of calcium on hyperoxaluria has not been well characterized. The aim of this study was to assess the effect of calcium carbonate supplements to decrease urinary oxalate secretion.
Methods: IRB approval was obtained for this prospective interventional study. From June 2010 to July 2011, 21 patients with hyperoxaluria were prospectively treated. The patients were provided with calcium carbonate pills with 1000mg elemental calcium and no vitamin D and instructed to take these with lunch and dinner. Repeat 24-hour urinalysis using Litholink were performed at 4-6 weeks after the initiation of the calcium.
Results: Compliance with the intervention and follow-up was 71%. Amongst patients that submitted repeat 24-hour urine collections, the urinary oxalate secretion decreased by a mean of 7.1 mg/day (IQR−1 to−15, p=0.002) from a mean of 49.1 to 42.6mg/day. The supersaturation of calcium oxalate similarly decreased from a mean of 9.0 to 5.3 for a mean decrease by 41% (p<0.001). No statistically significant change was seen in urinary calcium and citrate secretion, or urine pH and volume. The mean secretion of urinary calcium actually decreased from 272 to 216 mg/day although this change was not statistically significant (p=0.2).
Conclusions: This analysis suggests that calcium carbonate supplements taken with meals is an effective intervention for decreasing urinary oxalate concentrations in patients with a history of nephrolithiasis and hyperoxaluria.
The Effects of Dietary Calcium and Oxalate on Urinary Parameters
Introduction: Diet influences development of calcium oxalate kidney stones. We hypothesized that an imbalance in dietary calcium and oxalate might impact urinary oxalate excretion. Methods: An IRB-approved study was performed where normal, non stone-forming adults (8 females, 2 males) consumed controlled diets with daily oxalate and calcium contents of 750 mg and 1000 mg, respectively. In one diet, calcium and oxalate were equally balanced between all 3 meals (333 mg and 250 mg). In the other, oxalate and calcium intake were imbalanced over breakfast (20mg, 400mg), lunch (20mg, 400mg), and dinner (710mg, 200mg). The diets were consumed for 1 week and fractionated urine specimens collected on the last 4 days. Washout was at least one week between diets.Results: Oxalate excretion, calcium excretion, and estimate of urine supersaturation with calcium oxalate (CaOx TI) were similar between the balanced and imbalanced diets when comparing 24 hr values. There were differences during fractional collections. In 1 pm to 6 pm collection, oxalate excretion, calcium excretion, and CaOx TI were statistically different between the diets. Urinary oxalate was 28.06 vs 16.74, respectively (p<0.01). Calcium excretion was 83.11 vs 110.21 (p<0.04). CaOx TI was 0.617 vs 0.518 (p<0.04). In 6pm to 11 pm collections, only calcium differed (71.27 vs 107.16, p<0.02). In 11 pm to 8 am collection only calcium differed (55.00 vs 41.79, p<0.02). Conclusion: These results highlight the dynamic interplay between dietary calcium and oxalate, indicating that there may be limited stone risk associated with dietary imbalances of calcium and oxalate.
Equilibration of Urinary Oxalate Excretion and Fecal Oxalate During Periods of Regulated Oxalate Intake
Introduction: Controlled diets are the gold standard to assess excretion of urinary analytes. We assessed impact of gut colonization with Oxalobacter formigenes (OxF) on urinary oxalate excretion during different periods of oxalate consumption to evaluate equilibration of urinary oxalate excretion.Methods: 23 non stone-forming, healthy adults were enrolled: 11 OxF colonized (C) and 11 OxF non-colonized (NC). Diets were consumed for 7 days over 3 consecutive weeks: 50 mg oxalate/1000 mg calcium, 250 mg oxalate/1000 mg calcium, and 750 mg oxalate/1000 mg calcium. Fluid consumption was regulated and ratios of calcium to oxalate per meal were similar. 24 hour urine specimens were collected daily. Results: No significant differences existed in urinary oxalate excretion on the last 6 days of each diet during all sequences (not influenced by colonization status.) When dietary oxalate increased from 250 mg to 750 mg and calcium maintained at 1000 mg, 1 day was required for urinary oxalate equilibration (p<0.04). Comparison of first day on lower oxalate diets (50 mg and 250 mg) to average of last six days did not demonstrate any statistical significance. Upon stratifying subjects based on OxF colonization only lowest oxalate diet (50mg) in C individuals required 1 day for mean urinary Ox/Cr to equilibrate (p<0.02) whereas equilibration was immediate for all other sequences in C and NC subjects. Conclusion: Limited time is needed for normal subjects to achieve equilibration of urinary oxalate excretion when dietary oxalate and other nutrients are controlled. OxF colonization has limited influence on this.
A comparative Study of Risk Factors for Stone Formation, Stone Characteristics and Management in Morbidly Obese and Non-Obese Patients.
Introduction and Objectives:Obesity is associated with the metabolic syndrome and renal stone formation.Our objective was to compare the risk factors, stone characteristics and ureteroscopic treatment outcomes between morbidly obese and non-obese patientsMethod:We conducted a retrospective study of 317 patients, undergoing 446 ureteroscopic laser stone ablation procedures. Patients were classified into two groups: BMI>35 (mean 40.1) - morbidly obese, n=63; BMI<35 (mean 27.7) - control, n=254.We compared the prevalence of radiopaque to radiolucent stones, stone size, metabolic risk factors, effectiveness of ureteroscopic laser stone ablation, and complication rates.Results:Radiolucent (uric acid) stones were significantly more prevalent in the morbidly obese group (26 / 36 patients, 42%) as compared to the non-obese control group (30 / 211 patients, 12%). Radiolucent stones were also significantly more prevalent in patients with the metabolic syndrome (46% vs 16%) and those with hyperlipidaemia (34% vs 15%). Diabetes and hypertension were not significant risk factors. Comparing morbidly obese and control patients: mean stone size (9.7 and 10.1 mm), stone clearance after repeated procedures (95.9 % and 93.8 %), and complication rates (3.23 % and 1.87 %) were all equivalent.Conclusions:Our study shows that radiolucent (uric acid) stones have a significantly higher prevalence in morbidly obese and metabolic syndrome patients. We also show that flexible ureteroscopic laser stone ablation is equally effective and safe in morbidly obese patients.
Metabolic Evaluation of High Risk Stone Formers. Who and What are We Treating?
European guidelines recommend that high risk stone formers should undergo a specific metabolic evaluation to enable individualised prevention of stone recurrences and complications. We present our experience of a regional multidisciplinary metabolic stone clinic where patients see a renal physician, urologist and biochemist.
We retrospectively reviewed 150 new patients. All underwent full metabolic assessment. Referral indication, metabolic abnormality and initiated treatment plans were identified.
Median age 41yrs (range 14-79; M:F 2.4:1). Median weight 69.4Kg (range 46.5-129Kg). Median blood pressure was 129/84 mmHg, 38% of patients were hypertensive, of whom 40% were treatment naïve.
Referral indications were: recurrent stone formation (38%), stone disease with positive family history (21%), early onset stone formation (21%), diseases associated with urolithiasis (10%), others (10%).
All patients were issued with fluid and dietary advice. Of patients with abnormal metabolic evaluation 66% had additional treatments. Urinary alkalinizing agents (53%), thiazide diuretic (29%), antihypertensives (15%), parathyroidectomy (1.5%) and/or allopurinol (1.5%).
In our clinic, a metabolic diagnosis was made in 66% of high risk stone formers referred. Specific treatment was subsequently initiated in 66% of these patients. This highlights the importance of managing this group of patients within a dedicated metabolic stone clinic.
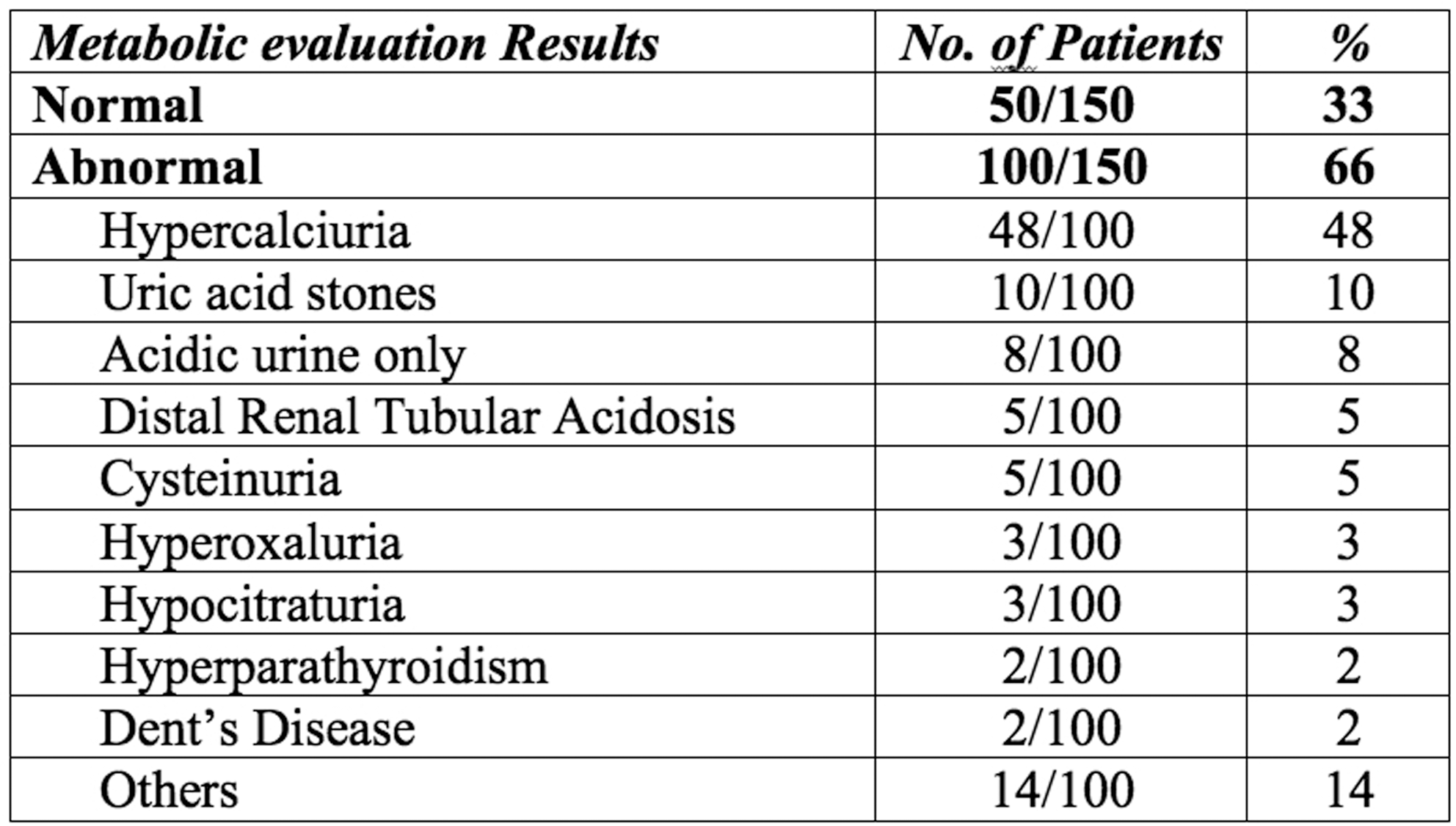
Changes in Stone Composition in Repeat Stone Formers
Background: First-time stone formers have a 50% risk of recurrence within the subsequent 10 years. Little is known regarding the composition of recurrent stones. This project examined stone composition in recurrent stone formers.
Methods: A medical record review of 270 patients was performed who had repeat stone analysis between 2003 and 2010. The same laboratory analyzed all these stones, Stones were characterized into four categories (uric acid stones, infected (struvite) stones, calcium stones, other (Cystine and xanthine)).
Results: A total of 270 patients and 734 stones were analyzed. A majority of the stones, 70% (513) of the analyzed stones, were of mixed composition and 30% (221) of the stones were 100% of one composition. Out of the patients reviewed, 16% (44) patients had changes in stone composition with subsequent stones at a mean time of 26 months. Uric acid stone formers were most likely to show stone change with 43% of subsequent stones of another type. Infected stone formers demonstrated a stone change in 33% of subsequent stones. Calcium stone formers had a stone change in only 8% of subsequent stones and the other category showed changes in type in 13% of cases (p<0.05).
Conclusion: Stone composition does change over time in a significant proportion of patients. In such cases, an adjustment in therapeutic modality may be necessary to treat those patient's stones. This study supports the use or repeat stone analysis in patients that form uric acid or struvite stones in order to provide optimally focused treatment.
Gas-Containing Renal Stones: Management of a New Cluster of Cases
INTRODUCTION:Gas-containing renal stones are a rare entity, with only four cases previously reported. We present four additional patients managed at our institution over a 2-year period.PURPOSE:We describe the clinical presentation, successful management, comorbidities, and microbiology of four cases of gas-containing renal stones.MATERIALS & METHODS:We reviewed the record of our four patients as well as the world literature on gas-containing stones. RESULTS:Our patients are all premenopausal females, have a majority calcium phosphate stone composition and evidence of ipsilateral urinary stasis. Clinical presentations included mild flank pain 3 patients and frank urosepsis in another. Three patients were rendered stone-free with percutaneous nephrostolithotomy while the other was treated with robotic extended pyelolithotomy. Comorbidities were present in all patients including diabetes, recurrent nephrolithiasis, gouty diathesis, hypocitraturia, hyperoxaluria, and hypercalciuria. Urinary E. Coli was isolated from three patients while Staph and Strep were present in the other. Review of the literature also suggests likely contributing factors to gas-containing stone formation include urinary stasis, metabolic mineral derangement, and diabetes. CONCLUSIONS:Gas-containing stones are a rare entity that may be increasing in prevalence. The clinical course of such patients mimics that of other infectious stones.

MP06: Robotic/Lap Upper Urinary Tract 2
Division of Urology, Department of Surgery, Chi Mei Medical Center
Retrocaval ureter is an uncommon venous anomaly in which the right ureter courses posterior to the inferior vena cava. Retrocaval ureter results from persistence of the posterior cardinal venous system that anomalously forms the inferior vena cava, and subsequently courses anterior to the ureter for a variable distance. This can resulted in varied degrees of ureteral obstruction, and surgical intervention is often indicated.We present two cases of retrocaval ureter featuring retroperitoneoscopic technique treatment using intracorporeal suture of the ureteral stumps. Surgical time was 80, 60 minutes, and the anastomosis was performed in 40, 30 minutes. There were no intra- or postoperative complications, and the patients were discharged from hospital on the third and second postoperative day. We conclude that this laparoscopic treatment of retrocaval ureter with retroperitoneal approach is feasible and easier to identify vena cava. The working space is not limited for intracorporeal suture.
Laparoscopic Transperitoneal Pyelolithotomy for Management of Staghorn Renal Calculi
Improved Outcomes of Surgeon Controlled Robotic Pyelolithotomy with Careful Patient Selection
INTRODUCTION:Robotic extended pyelolithotomy (REP) with concomitant upper tract reconstructive surgery such as pyeloplasty is well described. However, pure REP remains uncommon with only 26 patients in the literature. Reported stone free rates have ranged from 75-93% with average operative times up to 354 minutes. Prior studies have therefore suggested REP is best suited to patients with an extra-renal pelvis and minimal calyceal stone burden. We applied such criteria to seven cases of pure REP in effort to meet or improve upon outcomes. PURPOSE:To describe the perioperative course of seven carefully selected patients undergoing REP.MATERIALS & METHODS:We reviewed the record of seven patients undergoing pure REP at our institution from 6/2009 until 6/2011 to characterize stone burden, stone clearance, operative times, blood loss, and adjunctive procedures. RESULTS:All patients underwent stented transperitoneal REP without open conversion, perioperative transfusion, or flexible endoscopic techniques. The average patient was 49 years old, ASA class 2, with a BMI of 25. Average stone size was 2.97 cm (range 1.2-5.8) and average stone density 1163 Hounsefield units. Stone clearance rate was 100%. Average procedure time was 128 mins (range 101-183), average console time 65 mins (range 48-92), average estimated blood loss 40mL (range 10-100), and average length of 2.4 days (range 1-3).CONCLUSIONS:Robotic extended pyelolithotomy is a safe, highly efficacious, and highly efficient means of managing large renal stones when careful selection criteria are applied.
Prospective Randomized Comparison of Transperitoneal Laparoscopic Ureterolithotomy Versus Retroperitoneoscopic Ureterolithotomy for Proximal and Mid-Ureteric Stones
Aim: Prospective randomized comparison of transperitoneal laparoscopic ureterolithotomy versus retroperitoneoscopic ureterolithotomy for proximal and midureteric stones Material & Methods: Between September, 2009 to April, 2011; 36 patients of proximal and midureteric stones were included in the study. The patients were divided in two groups on the basis of 1:1 randomization. Patients with proximal and mid-ureteric calculi, more than 1 cm in size were included. Group I consisted of patients who underwent transperitoneal laparoscopic ureterolithotomy while group II consisted of patients who underwent retroperitoneoscopic ureterolithotomy. The intraoperative and postoperative parameters were compared e. g. operating time, blood loss, intracorporeal suturing time, visual pain analog score and total hospital stay. p value less than 0.05 was considered significant on statistical analysis.Result: The difference in the visual pain analog score and mean dose of tramadol for pain was significant on statistical analysis between the two groups. Hospital stay was more in group I and was significant on statistical analysis.Conclusion: Transperitoneal laparoscopic ureterolithotomy is associated with more pain, higher dose of analgesic requirement and longer hospital stay in comparison to retroperitoneoscopic laparoscopic ureterolithotomy.
Department of Urology, University of Michigan, Ann Arbor, USA
Introduction: Minimally invasive pyeloplasty is an effective treatment option for ureteropelvic junction obstruction. However, trends in its adoption are largely unknown. Purpose: To characterize the utilization of minimally invasive pyeloplasty compared to open pyeloplasty and evaluate patient-level factors that may be associated with its use.Materials and Methods: Using Florida data from the State Inpatient Database, we identified adults (i.e., 18 years or older) who underwent either an open or minimally invasive pyeloplasty between 1998 and 2006. We then examined trends in utilization as well as associated patient characteristics, including age, gender, race and insurance status, using chi-square analysis. Associations between minimally invasive pyeloplasty and patient-level characteristics were evaluated using multivariable logistic regression. Results: During this period, 76% and 24% of patients underwent an open versus minimally invasive pyeloplasty, respectively. Rates of minimally invasive pyeloplasty increased approximately 300% while rates of open pyeloplasty decreased 42% (p<0.01) (Figure). Among patient characteristics, those with private insurance had nearly twice the odds of receiving a minimally invasive pyeloplasty than those with non-private insurance (OR 1.82; 95% CI, 1.16-2.84). Conclusions: Although open pyeloplasty is still more common, the adoption of minimally invasive pyeloplasty is increasing, potentially more among patients with private insurance.

Surgeon-Controlled Robotic Revision Pyeloplasty is Highly Efficacious and Negligibly More Complex Than Primary Surgery.
INTRODUCTION:Robotic pyeloplasty has shown excellent functional results in the primary setting with short-term success rates of 83-96%. Results of robotic pyeloplasty for revision surgery are also encouraging, but it remains unclear if revision procedures are significantly more complex. PURPOSE:To compare perioperative and functional outcomes of primary versus revision robotic pyeloplasty.MATERIALS & METHODS:The records of 74 consecutive patients undergoing robotic pyeloplasty for uretero-pelvic junction obstruction (UPJO) were reviewed. Eight cases of revision pyeloplasty were compared to 66 cases of primary surgery in terms of operative time, blood loss, length of stay, and success rate. RESULTS:Success of revision surgery was 87.5% versus 96.97% for primary. No patients in either group required open conversion. Estimated blood loss for revision was 51mL versus 39 mL for primary. Average operative time for revision was 153 minutes versus 139 for primary. Median length of stay was 2 days in each group, while average length of stay was 2.13 days for revision versus 1.7 days for primary. None of these differences reached statistical significance. CONCLUSIONS:Revision robotic pyeloplasty does appear more complex that primary surgery as it was associated with longer operative times, increased blood loss, longer hospitalization, and lower success rate. However these differences are small, statistically insignificant, and likely clinically irrelevant.
Prior Management with Ureteral Stenting Does not Affect Outcomes of Surgeon-Controlled Robotic Pyeloplasty.
INTRODUCTION:Many patients referred for consideration of robotic pyeloplasty have been previously managed with ureteral stents, which are associated with peri-ureteral inflammation and fibrosis and may make pyeloplasty more difficult. It remains unclear whether prior management with ureteral stenting affects subsequent robotic pyeloplasty. PURPOSE:To compare perioperative outcomes of patients undergoing robotic pyeloplasty who were previously managed with ureteral stenting to those without prior stents.MATERIALS & METHODS:The records of 74 consecutive patients undergoing robotic pyeloplasty were reviewed. Twenty-four patients previously managed with ureteral stents were compared to 50 patients without prior stents in terms of success rate, operative times, blood loss, and perioperative complications. Additionally, patients previously stented were divided into a short term group (less than 90 days) and compared to those stented long term (greater than 90 days). RESULTS:Pyeloplasty was successful in 92% of previously stented patients versus 94% without prior stents. Previously stented patients had equivalent operative times and blood loss to those not previously stented. Patients in the short term group were stented on average 38 days versus 330 days for the long term group, but had equivalent operative times, blood loss, and lack of complications.CONCLUSIONS:Prior management with short or long term ureteral stenting does not significantly affect the complexity, morbidity, or success of robotic pyeloplasty.
Default Approach to Daycase Upper Tract Urological Surgery: Experience of First 80 Cases in a Single UK Tertiary Referral Center
Introduction: As minimally invasive surgery continues to evolve exponentially and incur higher capital investment in equipment, the challenge from a health economics viewpoint is emerging to enhance recovery and reduce length of hospital stay. Laparoscopic nephrectomy and pyeloplasty is the default expectation in our organization. Purpose: To evaluate the feasibility, safety and economic implications of implementing a daycase surgery policy for Laparoscopic upper tract surgery in the UK setting. Materials and Methods: Inclusion criteria was clinically fit (i.e. ASA Grade 1-2) patients who were well motivated, had good support at home and had access to well trained community nurses. A protocol permitted patients to contact the urological team. Postoperatively, all patients were given a questionnaire analysis to tally their experience. A preliminary costings analysis was completed. Results: Forty patients had laparoscopic pyeloplasty (LP), of which 36(12 to 67 years) were listed with intent for daycase procedure. All planned daycases were discharged on the day of surgery with a median operative time of 178mins and mean postoperative stay of 249mins (100 to 372 min). There were no open conversions or readmissions. Forty patients had successful daycase Laparoscopic Nephrectomy (LN). Twelve percent(3/25) had minor postoperative complications. From evaluation of the questionnaires, all but two patients stated they would prefer to have their procedure done as a daycase. Cost of daycase procedure was 15-30% less than non daycase procedure depending on length of stay. Conclusions: Laparoscopic upper tract surgery can be undertaken safely on a planned daycase setting in selected groups of patients.
Laparoscopic Pyelolasty: A Single Centre Experience
Introduction. Laparoscopic pyeloplasty (LP) is minimally invasive management option for ureteropelvic junction obstruction (UPJO) .Purpose. To determine the safety and efficacy of LP.Materials and methods. Since October 2009 to April 2011, 46 patients with UPJO underwent transperitoneal LP. All patients presented a primary UPJO. The mean age was 34 years (range 22 to 54), and of the 29 women and 17 men, 29 presented UPJO on the right side and 19 on the left side. All patients were subject to a preoperative evaluation including renal ultrasonography, diurethic renography and intravenous urography or CT scan that revealed the presence of severe hydronephrosis. Stones were detected in the renal pelvis in 6 patients. Results. No conversions were needed. The mean operative time was 125 minutes (range 95 - 210 min), blood loss was 40 ml (range 20 - 100 ml), and the mean postoperative duration of stay was 5,7 days (range 3 - 10 d). No intraoperative complications have occured. Crossing vessels were noted in 21 patients. Anastomotic leakage occured in 3 patients and was successfully treated by conservative treatment. A persistent UPJO was detected in three patients and was treated by transurethral endopyelotomy in two cases and by performing an open pyeloplasty in one case. A mean follow-up period was 18 months (range 6 to 28) and demonstrated a 93,5% success rate.Conclusions. LP is an effective method of treatment for UPJO, with a high overall success rate, a short inpatient stay, and negligible incidence of early complications.
Department of Urology, Kitasato University School of Medicine, Sagamihara, Japan
Introduction: A long-term outcomes and the stability of efficacy of laparoscopic pyeloplasty (LPP) were investigated.
Patients and Methods: Between October 1999 and December 2010 we preformed LPP on 125 ureters in 119 patients presenting with symptomatic hydronephrosis and/or asymptomatic cases with progressively loosing renal function. We performed dismembered Anderson-Hynes pyeloplasty, Fenger plasty, Y-V plasty in 108 (86.4%), 15(12.0%), 2 (1.6%) ureters, respectively. All procedures except for 1 were carried out transperitoneally.
Results: The procedure was completed successfully in all cases. Crossing vessels were noted in 57 of 125 ureters (45.6%). Median operative time and estimated blood loss were 200 minutes and 20 ml, respectively. Intra- and postoperative complications categorized as Clavien grade II or more were noted in 11 patients (8.9%). A total of 120 ureters (96%) demonstrated an improvement of hydronephrosis and/or disappearance of obstructive pattern on diuretic renography during a median follow up of 45 (5-146) months. Improvement of the hydronephrosis was still observed in some cases even after 2 years postoperatively. In contrast, progression of hydronephrosis due to re-obstruction was not noted after 1 year follow up.
Conclusion: Although the procedure requires advanced laparoscopic skills, the present study demonstrates that the result of LPP is equivalent to the conventional open procedure and its efficacy seems to be stable for long term. Laparoscopic pyeloplasty may be a valuable and less invasive alternative to open pyeloplasty for ureteropelvic junction obstruction.
Laparoscopic Pyeloplasty: Predictors for Failure
Introduction. Laparoscopic pyeloplasty (LP) is a standart method of treatment for UPJO. Some factors have been considered in relation to success of LP.Purpose. To determine spesific predictors for failure of LP.Materials and Methods. We reviwed 34 patients who underwent LP by a single surgeon from October 2009 to January 2011. We have evaluated such parameters as age, body mass index, presence of crossing vessels, operative time, estimated blood loss, method of drainage and postoperative complications. Long-term results were characterized as success, equivocals (symptoms without obstruction by diurethic renography) or failure (symptoms with obstruction).Results. There were 24 success, 7 equivocals and 3 failures. 18 patients had crossing vessels, of which all were transposed. Failures had non-significantly increased operative time in failures versus successes (206 min vs. 186, p=0.145) and method of drainage. There was significantly anastomotic urinary leakage and more blood loss in failures versus the successes (170 ml vs. 56,8, p=0.004).Conclusion. Age of patients, BMI, crossing vessels and methods of drainage were not a prognostic variable. Operative time and blood loss increased in failures. Anastomotic urinary leakage was predictor for failure of LP.
Surgical Outcomes of Mini-Laparoscopic Pyeloplasty
Introduction: Laparoscopic pyeloplasty for correction of ureteropelvic junction obstruction (UPJO) is comparable to open pyeloplasty in success rates. Experience with mini-laparoscopic pyeloplasty (mini-LPS) however remains limited. Purpose: To reoprt the surgical outcomes of mini-LPS pyeloplasty for UPJO.Materials and Methods: The hospital records of patients undergoing mini-LPS pyeloplasty between August 2005 and September 2010 are retrospectively reviewed. Surgical indications are UPJ stenosis with symptoms and obstructive uropathy which was prooved by DTPA. For the patients not older than 5 years old, we use 3 trocars of 3mm; for those who are older than 5 years old, one 5 mm trocar for telescope and a pair of 3mm trocars for instruments are applied. The post-operative outcomes are evaluated by symotoms, renal sonography, or DTPA.Results: 11 patients are included and the mean age is 17.9 (0.5-33) years. 10 patients underwent dismembered pyeloplasty and one received Foley Y-V pyeloplasty. The mean operation time was 265 (150-480) minutes. Mean hospital stay is 5.5 (3-10) days. One patient has urosepsis after operation, and one suffered from oliguria and acute pyelonephritis after removal of JJ stent. The two patients were managed with medical treatment succesfully. At a mean follow up of 23.3 (2-59) months, all patients demonstrated improvement of symptoms and drainage on DTPA or a decrease in the grade of hydronephrosis on sonography. The success rate was 100%. Conclusion: Our series of patients undergoing mini-LPS pleloplasty have high success rate. We consider this our primary technique for surgical correction of UPJO.
Department of Urology, University of Patras, Greece
Purpose: To present our initial clinical experience with the use of Quill self-retaining suture (SRS) (Angiotech Pharmaceuticals, Reading, PA) in laparoscopic dismembered pyeloplasty.Patients and methods: Totally, 4 patients (3 male/1 female) were treated by two expert laparoscopic surgeons for UPJ obstruction. During the procedure a single 4/0 Quill SRS was used for the anastomosis. The anastomosis was created with continuous suturing which approximated the spatulated ureter to the renal pelvis. Knotless laparoscopic suturing was proved fast and easy providing proper watertight sealing of the anastomosis. Peri-operative data were recorded. The ureteral stent was removed on the 30th postoperative day and retrograde pyelography was performed. Ultrasound investigation was repeated 4 weeks after the removal of stent and 6 months after the procedure. Results: Average patient age was 33.5 years (range 28-42), average Body Mass Index (BMI) was 26.3 (range 23.2-29.1) kgr/m2 and average operative time was 108 (98-122) min. Blood loss was minimal with 150ml to be the higher loss. All cases were discharged on post-operative day 3. During the ureteral stent extraction on post-operative day 30 a retrograde pyelography revealed the presence of ureteral stenosis at the level of ureteropelvic anastomosis in 3 patients. Successful management of the UPJ obstruction was observed in only patient. Conclusion: Knotless intracorporeal laparoscopic suturing using Quill SRS was proved fast and efficient. Nevertheless, Quill SRS should not be used for the reconstruction of the upper urinary tract during pyeloplasty due to the recurrence of stricture.
Minimally Invasive Treatment of UPJO in Horseshoe Kidneys: A Case Series
Horseshoe kidney is a common renal anomaly associated with uretero-pelvic junction obstruction that can impair renal function. With improved MIS techniques, laparoscopic and robotic treatment approaches will soon become more common. To date, however, only 3 small series have been reported in horseshoe kidneys.
To report our outcomes of MIS treatment of UPJO in a horseshoe kidney, including two cases of laparoscopic single incision surgery.
We performed a retrospective chart review of patients undergoing MIS pyeloplasty between March 2000 and March 2010 at our center. Seven patients were treated, but two patients were excluded due to inadequate followup. We evaluated perioperative outcomes and postoperative renal function.
Two patients underwent laparoscopic LESS pyeloplasty, while the remaining three were treated with a traditional laparoscopic approach. The mean age was 32 years, with a mean followup of 26±14 mos. The mean OR time was 170±49 mins with a mean blood loss of 39±15 ml. The mean preoperative differential function on renogram was 58±12%. No statistically significant decline in differential function was observed up to 30 months of followup.
This series provides support for the safety and efficacy of both the multi-incisional and LESS techniques for the treatment of UPJO in horseshoe kidneys.
Hydronephrosis Improves Slowly After Retroperitoneal Laparoscopic Dismembered Anderson-Hynes Pyeloplasty: A Longitudinal Analysis
INTRODUCTION: Laparoscopic pyeloplasty is considered a new gold standard for the treatment of ureteropelvic junction obstruction (UPJO). However, the evaluation of this technique is difficult, because patient postoperative improvement is reported to be variable. PURPOSE: We evaluated the improvement of hydronephrosis longitudinally after retroperitoneal laparoscopic dismembered Anderson-Hynes pyeloplasty for patients with UPJO. METHODS: Fourteen patients underwent retroperitoneal laparoscopic dismembered Anderson-Hynes pyeloplasty at our institute between January 2006 and March 2011. The ureteral stent was removed at 4 weeks after surgery. Hydronephrosis was assessed by ultrasound and intravenous pyelography at 3, 6, 12, 18, and 24 months after pyeloplasty. The degree of hydronephrosis was classified according to Ellenbogen's classification. RESULTS: The mean follow-up time was 18 months. Preoperative hydronephrosis was diagnosed as grade 2 and grade 3 in 7 patients each. The postoperative improvement of hydronephrosis by one grade was 64%, 100%, 100%, and 100%, at 3, 6, 12, and 24 months, respectively. The improvement of hydronephrosis by two grades was 0%, 18%, 33%, and 40%, at 3, 6, 12, and 24 months, respectively. In most cases, hydronephrosis was still improving even 12 months after pyeloplasty. CONCLUSIONS: Improvement of hydronephrosis after laparoscopic pyeloplasty is relatively slow. Although hydronephrosis had not begun to improve in 36% of patients at 3 months, all cases showed improvement at 6 months after surgery. Therefore, clinicians should wait to assess the effectiveness of laparoscopic pyeloplasty until 6 months after surgery.
Department of Urology, Indiana University School of Medicine, Indianapolis, IN
Introduction: During dismembered pyeloplasty, posterior transposition of crossing vessels has often been routine, but may not be indicated for all patients. Purpose: To compare outcomes of patients in whom vessels were transposed posteriorly versus those that were not during laparoscopic or robotic pyeloplasty.Methods: 487 cases from 15 centers had details regarding intraoperative crossing vessels. Posterior transposition was defined as moving the vessels posterior to the anastamosis. Cases performed without posterior transposition were either not transposed or transposed superiorly. Subjective failures were defined as unchanged or worsened pain. Radiographic failures were defined as worsening T1/2 or hydronephrosis. Results: 261/487 cases had crossing vessels. In these 261 patients, 95 had posterior transposition, 129 did not, and 37 were unknown. Patients who underwent posterior transposition versus those that did not were similar in median preoperative T1/2 (30min for both) and differential renal function (42%, IQR=18, versus 40%, IQR=20, p=0.432). Operative time was 225min (IQR=147) for posteriorly transposed cases and 215min for nontransposed cases (IQR=126), p=0.572. Subjective failures occurred in 4.5% posterior transposition and 5.0% without (p=0.99), while obstruction recurred in 5.9% posterior transposition and 3.8% without (p=0.721). Urine leak occurred in 4 posterior and 3 nonposterior, p=0.505. Secondary procedures were required in 5.3% posterior transpositions and 6.2% without posterior transposition, p=0.767.Conclusion: Transposition of crossing vessels posteriorly during dismembered pyeloplasty should be tailored to individual anatomic factors rather than performed as a standard.
Prospective Randomized Comparison of Transperitoneal Versus Retroperitoneal Laparoscopic Pyeloplasty for Primary Ureteropelvic Junction Obstruction.
Aim: Prospective randomized comparison of transperitoneal versus retroperitoneal laparoscopic pyeloplasty for primary ureteropelvic junction obstruction.Material & Methods: In a prospective study between September, 2009 to April, 2011; 42 patients of primary ureteropelvic junction (UPJ) obstruction were randomized for laparoscopic pyeloplasty; Group I consisted of patients undergoing transperitoneal pyeloplasty while group II were subjected to retroperitoneal pyeloplasty. The groups were compared for total operating time, intracorporeal suturing time, visual pain analog score (VAS), paralytic ileus and the duration of hospital stay. The patients were followed by ultrasonography at 3 months and DTPA scan. Two patients in each group had surgical failure at a median follow-up of 14 months. p less than 0.05 was considered significant for statistical analysis. Results: Total operating time and intracorporeal suturing time were higher in group II and significant on statistical analysis. Pain score was significantly higher in group I. Hospital stay was higher in group I. Paralytic ileus was significantly higher in group I.Conclusion: Total operating time and intracorporeal suturing time are significantly higher in the retroperitoneal group while paralytic ileus and total hospital stay are significantly higher in the transperitoneal group. Surgical success rate is equal in both the groups.
Conservative Management of Pelvi-Ureteric Junction Obstruction (PUJO): is it Appropriate and if so How Long is Follow-Up Needed?
IntroductionAlthough most PUJO is probably congenital, it often presents later in life. PUJO can be diagnosed during investigation of urological symptoms, or imaging for other reasons. In patients without indication for intervention, it is unclear how long they should be followed up, and how often renography should be performed.MethodsA retrospective notes review was performed of 214 patients who underwent 2 or more renograms within the period 1998 - 2009. 164 were excluded due to early intervention or absence of PUJO. Results50 suitable patients were identified, 34 female and 16 male. Mean age was 55.12 years. The mean follow up was 51.7 months. The mean number of renograms performed per patient was 4. 10 patients deteriorated and required intervention, 6 patients had symptomatic and renographic deterioration, 1 patient had only symptomatic deterioration. Only 3 patients had just asymptomatic renographic deterioration. Mean time from diagnosis to deterioration was 55.6 months. Patients who deteriorated after two years of follow up were all symptomatic. 9 out of the 10 patients who deteriorated were female. 8 patients underwent laparoscopic pyeloplasty, 1 patient underwent nephrectomy and 1 patient required nephrectomy but was unfit.ConclusionIn this cohort 20% of patients deteriorated and required surgical intervention. Mean follow up from diagnosis to deterioration was 55.6 months but was up to 11 years in one patient. Our study suggests that stopping renographic follow up at 24 months would be safe. Larger studies to elucidate this further are required.
MP07: LESS/NOTES 2
Hybrid Transureteral NOTES Nephrectomy: A Survival Study in the Porcine Model
Introduction: Natural orifice approaches for nephrectomy have included access via the stomach, vagina, bladder, and rectum. Recently, the feasibility of using the ureter as a natural orifice for NOTES nephrectomy has been demonstrated in a non-survival model.
Purpose: To assess the outcomes of transureteral laparoscopic NOTES nephrectomy in a survival porcine model.
Materials and Methods: Three 45-kg female farm pigs underwent transureteral nephrectomy in the lithotomy position. After placement of a guidewire into the left ureter, a bariatric laparoscopic trocar was used to intubate the left ureter. A needlescopic port was placed transabdominally to facilitate in situ morcellation. The kidney was morcellated using a bipolar sealing device and extracted via the ureter using the housing of a bariatric stapling device. The ureteral orifice was closed with a laparoscopic suturing device. The bladder was drained by a council-tip catheter for 12 days post-operatively. Pigs were euthanized on post-operative day 21.
Results: All surgeries were successfully completed with no intra-operative complications (Table 1). One instance of post-operative clot retention was managed by replacing the catheter.

Conclusions: This study demonstrates the feasibility of a transureteral approach to nephrectomy in the survival porcine model. This technique promises to decrease the invasiveness of NOTES nephrectomy.
Cosmetic Impact of Needlescopic Ports and Placement Techniques Upon Scarless Surgery in a Porcine Model
Introduction: LESS and NOTES procedures aim to provide scarless cosmesis. In an attempt to simplify these technically challenging procedures, surgeons may employ accessory needlescopic ports. The cosmetic impact of these additional ports, however, has not been determined.
Purpose: To characterize the cosmetic impact of a 2 mm needlescopic port and to evaluate 4 different methods for creating these incisions.
Methods: In the porcine model, 45 2x2 cm boxes were tattooed onto the abdominal wall and randomized to 4 different incisional techniques: incision with a #11 blade, a no-scalpel vasectomy tool, a veress needle, or electrocautery. A fifth group with no incision acted as a control. All ports were left in place for 2 hours and mobilized in a uniform manner in all dimensions to mimic the forces experienced during laparoscopic surgery. Incisions were closed with adhesive skin glue and assessed 4 weeks post-operatively by a blinded plastic surgeon using the Vancouver Scar Scale (VSS).
Results: See Table 1.

Conclusions: A 2 mm needlescopic port has minimal impact upon overall cosmesis; only 50% of incisions were identified. Techniques used to make needlescopic incisions significantly impacts post-operative cosmesis, with the no-scalpel technique being least likely to leave an identifiable scar.
Do More Acute Angles Between Straight Instruments Used During Laparoendoscopic Single Site Surgeries Significantly Prolong Laparoscopic Suturing and Knot-Tying Time?
Introduction: Laparoscopic suturing and knot-tying is challenging, when performed in Laparoendoscopic Single Site (L.E.S.S.) Surgeries using straight non-articulating needle-drivers and graspers, because of the more acute angles between them.Objective: To determine if more acute angles between straight non-articulating instruments significantly prolong laparoscopic suturing and knot-tying time.Methodology: Six urologists, with different laparoscopic skill levels, performed time-exercises making five sutures and tying three knots in 2-cm incision with 3-O Polyglycolic acid with HR26 needle inside Home-made Laparoscopic Suturing and Knot-Tying Angle-Trainer. Straight non-articulating laparoscopic needle-drivers and graspers, at instrument-angles between them of 15-degrees, 25-degrees and 45-degrees respectively, were used. Zero-degree laparoscopic telescope was placed between instruments and at 135-degrees and 90-degrees sutured-object position. Results: Suturing and knot-tying time were: 1046 seconds (range: 698-1454) at 15-degrees instrument-angle and 135-degrees object-position; 785 seconds (range: 487-1313) at 25-degrees instrument-angle and 135-degrees object-position; 744 seconds (range: 480-1128) at 45-degrees instrument-angle and 135-degrees object-position; 929 seconds (range: 360-1576) at 15-degrees instrument-angle and 90-degrees object-position; 736 seconds (range: 345-1325) at 25-degrees instrument-angle and 90-degrees object-position; 695 seconds (range: 408-1157) at 45-degrees instrument-angle and 90-degrees object-position. Using Wilcoxon Signed Rank Test, suturing and knot-tying time were significantly longer (p=0.0061) at 15-degrees instrument-angle compared with 25-degrees instrument-angle and at 15-degrees instrument-angle compared with 45-degrees instrument-angle. No significant difference (p=0.1167) in suturing and knot-tying time at 25-degrees instrument-angle compared with 45-degrees instrument-angle.Conclusion: The more acute 15-degrees angle between straight non-articulating instruments in L.E.S.S. surgeries, compared to 25-degrees instrument-angle and 45-degrees instrument-angle, significantly prolongs laparoscopic suturing and knot-tying time.
The Joint Force of First Generation Articulating Instruments for LESS is not Enough
With the increased understanding of the LaparoEndoscopic Sing-site Surgery (LESS), several problems associated with instruments became apparent. Current articulating instruments do not seem to fulfill the articulating and sustaining forces required.
To measure and evaluate a sustaining force of the joints in the first generation articulating instruments for LESS.
The articulating instruments adopted in this experiment were Laparo-Angle™(Cambridge Endoscopic Devices Inc., USA), RealHand™(Novare Surgical Systems Inc., USA) and Roticulator™(Covidien Inc., USA). We measured the angle of flexible forceps joints of several commercial instruments in proportion to the articulating force using push-pull gauge. Two configurations of fixed position were predetermined as a neutral position and fully refracted position of the instruments.
Straining forces to bend through 30 degrees were only 7.0 and 5.9 N in Laparo-Angle™ and RealHand™ respectively. Furthermore, sustaining forces keeping the position in fully refracted state were only 2.1, 1.8 and 1.7 N respectively. The usual range of force required for laparoscopic surgery is approximately 20 N. Compare to this requirement, sustaining force of the joints in the first generation articulating instruments were fairly insufficient.
Joint force of the recent articulating instruments for LESS is not enough for usual operation. The improved articulating instruments having more sustaining force should be developed to meet surgeons' requirements. '
A Home-Made Acute Angle Trainer for Laparoscopic Suturing and Knot-Tying Practice-Exercises Using Standard Straight Instruments Before Performing L.E.S.S. Surgeries
Introduction: Laparoscopic suturing and knot-tying practice-exercises are helpful before performing renal, ureteral and pelvic Laparoendoscopic Single Site surgeries using straight instruments with acute angles between them.Purpose: To present a home-made acute angle trainer for practice-exercises in laparoscopic suturing and knot-tying using standard straight instruments.Methods: An acute angle trainer was fabricated from readily available household and art materials. Laparoscopic suturing and knot-tying practice-exercises making five sutures and three knots after first suture were performed on 2.0cm long midline incision of 2.5cm x 5.0cm penrose drain using 20cm long 3-O Polyglycolic acid suture with HR26 needle.Results: Practice-exercises on the home-made acute angle trainer were performed in two series. First series of practice-exercises performed in 135-degrees position of penrose drain to 10mm telescope axis with straight 5mm needle driver and grasper/needle driver at 45-degrees, 25-degrees and 15-degrees angles between instruments consecutively. Second series of practice-exercises performed in 90-degrees position of penrose drain to 10mm telescope axis with straight 5mm needle driver and grasper/needle driver at 45-degrees, 25-degrees and 15-degrees angles between instruments consecutively.Conclusion: A home-made acute angle trainer is feasible and useful in practice-exercises before performing laparoscopic suturing and knot-tying in Laparoendoscopic Single Site surgeries using standard straight instruments.

Patient-Reported Cosmesis Outcomes Following Laparoscopic Adrenalectomy; LESS vs. Conventional Surgery
Introduction: Laparoendoscopic single site surgery (LESS) continues to gain prevalence in urology, with reported equivalent perioperative outcomes and superior cosmesis to conventional laparoscopic surgery (CLS).Purpose: The purpose of this study was to evaluate patient-reported satisfaction and cosmesis of LESS in comparison with that of CLS in Japanese.Materials and Methods: A total of 15 and 103 patients who underwent LESS and CLS between May 1996 and January 2011 were included in the study. Questionnaires inquiring about scar pain (0: not painful, 10: very painful), satisfaction (0: not satisfied, 10: very satisfied), and cosmesis (0: very ugly, 10: very beautiful) on the basis of a visual analogue scale that was sent to patients postoperatively. Results: Eleven (4 men and 7 women) and 51 (24 men and 27 women) patients who underwent LESS and CLS, respectively, responded. The mean follow-up times after surgery were 64.9 (range 18-181) and 11.4 (range 5-19) months for the CLS and LESS groups, respectively (p<0.01). There was no significant inter-group difference in age, male-to-female ratio, affected side, BMI, and blood loss. Insufflation time was significantly longer in the LESS group than the conventional group (229 vs. 191 min, p=0.03). There was no significant difference in pain (0.73 vs. 0.57, p=0.64), satisfaction (8.82 vs. 8.43, p=0.63), and cosmesis score (8.55 vs. 7.96, p=0.51).Conclusions: No significant difference was obtained in patient-reported cosmesis following LESS and CLS. Further evaluation is needed by longitudinal study to clarify whether LESS is superior to CLS in terms of cosmesis.
Application of Embryonic Natural Orifice Transumbilical Endoscopic Surgery in Urology: with A Report of 115 Cases
Introduction Embryonic natural orifice transumbilical endoscopic surgery (E-NOTES) has emerged as an attempt to further enhance cosmetic benefits and reduce morbidity of minimally invasive surgery. Purpose We describe the clinical experience of E-NOTES in our center, and evaluate its feasibility, safety and efficacy.Materials and Methods One hundred and fifteen consecutive patients, including 67 males and 48 females, were subjected to E-NOTES in our center. Of the patients, there were 3 adrenal tumors, 29 renal cysts, 1 polycystic kidney, 1 renal tuberculosis, 5 ureteropelvic junction obstructions, 5 renal carcinomas, 15 non-functioning kidneys, 2 duplex kidneys, 2 renal pelvic calculi, 22 ureteral calculi, 3 cryptorchidisms, and 27 varicoceles. Under general anesthesia, the patients were positioned in lateral decubitus with affected side elevated, except the patients with cryptorchidism and varicocele, who were placed in the Tredelenburg position. The operation was same as that of standard laparoscopy. ResultsAll the 115 procedures were successfully performed without conversion to open surgery. Only one patient with right renal carcinoma, were converted to undergo standard laparoscopy because of persistent blooding. The mean operative time were 93 mins, 165 mins, 133mins, 148mins, and 80 mins for adrenalectomy, simple nephrectomy, radical nephrectomy, pyeloplasty, and pelvic or ureterolithotomy, respectively. The mean blood loss was 117ml. There was no major complication occurred. The follow-up of 6-12 months showed satisfactory short-term results, with hidden umbilical scar. Conclusions E-NOTES appears to be a feasible and reproducible surgical technique. It would lead to less injury, rapid convalescence, and improved cosmetic results.
A Novel Approach for Embryonic Natural Orifice Transumbilical Endoscopic Surgery (E-NOTES) Using Conventional Laparoscopic Instruments in Urology
Introduction The laparoscope and instruments continuously interfere with each other during embryonic natural orifice transumbilical endoscopic surgery (E-NOTES). Purpose To report our initial experience with suprapubic-assisted E-NOTES using conventional laparoscopic instruments in urology, and evaluate its feasibility, safety and efficacy.Patients and Methods Seventy nine patients were subjected to suprapubic-assisted E-NOTES. The procedures included adrenalectomy (N=6), renal cyst excision (N=3), nephrectomy (N=33), nephroureterectomy (N=1), nephron-sparing surgery (N=1), heminephroureterectomy (N=2), pyeloplasty (N=5), pyelolithotomy (N=4), and ureterolithotomy (N=25). The patient was secured on the operating table in lateral decubitus with affected side elevated 70 degree. One 5- and 10-mm (or two 5-mm) trocars were inserted at the umbilical edge. A 10-or 5-mm trocar was inserted into abdominal cavity below the pubic hairline. Our technique for the suprapubic-assisted E-NOTES is similar to that of the standard laparoscopy. Some bigger specimens were removed after the incisions below the pubic hairline were enlarged. Results The 79 procedures were all successfully performed. The median operative time was 81, 106, 91, 141, and 83 minutes, and estimated blood loss was 61, 213, 115, 76, and 53 mL for adrenalectomy, simple nephrectomy, radical nephrectomy, pyeloplasty, ureterolithotomy, respectively. The mean follow-up of 5.2 (range 1 to 11) months showed hidden umbilicus scar. The scar below the pubic hairline was not detectable because of the covering of the pubic hairs. Conclusions Suprapubic-assisted E-NOTES appears to be feasible, safe and effective. It would not only lead to improved cosmetic results, but decrease the difficulty of operation.
Department of Urology and Renal Transplantation, Sapporo Hokuyu Hospital, Sapporo, Japan
Objectives: We report our clinical results of retroperitoneoscopic diagnostic lymphadenectomy for cases suspected of malignant lymphoma. Methods: Five cases with paraaortic or paracaval enlarged lymph nodes without any surface lymphadenopathy were included in this study. Four cases were for initial diagnosis and 1 case was for recurrent disease. Three-port surgery was done for 4 cases and single-port surgery was done for the last case. The most accessible lymph node of more than 1cm in diameter was excised. A case with renal cancer underwent radical nephrectomy at the same time. Results: Operation time was 81 min in average and blood loss was trace amount in the all cases. Final pathology was malignant lymphoma in 4 cases and metastatic cancer in 1 case. Although there was no intraoperative complications, the first patient who underwent chemotherapy immediate after the surgery presented with a gigantic retroperitoneal lymphocele. Thereafter, we routinely apply fibrin glue before closure for the patients who are planned for immediate chemotherapy. All the cases recovered ambulation and feeding on the next day. Conclusions: Reteroperitoneoscopic lymphadenectomy is a minimally-invasive procedure feasible for the patients who require a large biopsy specimen and immediate induction of chemotherapy. Care must be taken for development of lymphocele due to the delay in wound healing associated with chemotherapy.
A Case of Extraperitoneal Laparo-Endoscopic Single-Site Biopsy of External Iliac Lymph Node
Introduction: Recently, Laparo-Endoscopic Single-Site (LESS) surgery has gained interest as minimal invasive surgical technique. In this report we present a case of external Iliac lymph node biopsy in which LESS surgery was useful.Purpose: To report the clinical experience with extraperitoneal laparo-endoscopic single-site (LESS) biopsy of external Iliac lymph node.Materials and Methods: A 61-year-old man was incidentally found to have multiple lymph node swellings during his therapy for hepatitis type C. To diagnose and make a treatment plan, LESS external Iliac lymph node biopsy was planned. A 3cm U-shaped transverse incision was made just under the umbilicus. The preperitoneal space was created and the SILSTMport was inserted. One swelled external iliac lymph node was dissected and removed using a 5mm flexible endoscopy, LigaSure VTM, EndoPathTM and an articulated grasper. The specimen was extracted by using Endocatch GoldTM through 10mm port.Results: The procedure was completed in 140min (endoscopic time was 90min). There were no intraoperative or postoperative complications, and the blood loss was minimal. The pathological diagnosis was nodular lymphocyte predominant Hodgkin lymphoma (NLPHL).Conclusions: LESS external iliac lymph node biopsy is feasible and safe, and provides some useful information for the diagnosis.

Laparo-Endoscopic Single-Site Surgery for Pyourachus is a Safe and Minimally Invasive Surgery.
Introduction : We performed LESS for pyourachus. There are few reports on LESS for urachal remant.
Purpose: There are a few small fascial injuries in laparoscopic surgery so we believed return to everyday life would be faster. Furthermore, considering cosmetics, we decide to perform a LESS operation instead of a regular laparoscopic surgery.
Materials and Methods: Under general anesthesia, the patient was in supine position. 5 cm above the navel, in the central abdominal region, a 2cm incision was made, and Covidien SILS Ports was placed, a 5mm camera, Covidien flexible forcepts, and flexible scissors and LigaSure were used. We put pressure on the navel with a probe and confirmed its position, and right below the navel we did a ligature with a Hem-o-lok. Once the dissection was completed, we could preserve the umbilical region. The operation took 98 minutes and there was no bleeding at all.
Results: The post operative development was good. The operation wound was small, and there were no signs of complications such as surgical site infection or port hernia. On the first postoperative day, the patient could eat and on the third postoperative day the patient could leave the hospital.
Conclusions: LESS for pyourachus it is basically a safe, minimally invasive surgery. It is the best choice and can be actively introduced as an operative method for a urachal remmant.
Laparo-Endoscopic Single Site (LESS) Management of Kidney Diseases
PurposeTo present our experience with Laparo-Endoscopic Single Site (LESS) management of kidney diseases.Materials and MethodsFrom September 2008 to June 2011, 35 patients underwent single port transumbilical laparoscopic surgery: nephrectomy for a nonfunctioning kidney (12 cases) and cancer (6 cases), cyst decortications for symptomatic renal cyst (13 cases), redo-dismembered pyeloplasty with previously failed laparoscopic surgical repair (1 case), and renal radiofrequency ablation ( 2 cases) respectively. Patients underwent surgery through a single 2-cm infraumbilical incision with many types of single port. ResultsMean patient age and BMI were 60 years and 23.75 kg/m2, respectively. Mean operating time was 167.7 min. LESS was a possible and safe approach in 85.8 % of patients. All LESS cyst decortications and redo-pyeloplasty were completed without major complications or conversion to open surgery. However, there was 1 case of each LESS cyst decortication and pyeloplasty requiring an additional 3-mm port for suturing due to bleeding and an instrument error, respectively. For LESS nephrectomy, two (28.6 %) with higher waist circumference were converted to standard laparoscopic nephrectomy due to failure to progress. One post operative complication of incisional hernia occurred in a patient with chronic bronchitis and asthma.ConclusionsLESS for the management of kidney diseases is an effective and safe treatment option with selected patients and experienced surgeon.
LESS Nephrectomy and Nephroureterectomy - Early Experience in Singapore
Introduction: Single Port or LaparoEndoscopic Single Site (LESS) Surgery has been developed as anew mode of minimally invasive surgery.Purpose: We describe our initial experience of LESS nephrectomy and nephroureterectomy.Materials and Methods: Eleven patients were included in the study. The indications for surgery werekidney cancer , hydronephrotic non-functioning kidney and renal pelvic urothelial tumor . Thepatient demographics, peri-operative parameters and pathology results were recorded.Results: The patients underwent single port/ LESS nephrectomy (10) and nephroureterectomy (1)respectively, using the TRIPORT Access System (Olympus) or the X cone (Storz) inserted through a transumbilical incision.Nephrectomy was performed successfully in 9 patients. In the nephroureterectomy patient withrenal pelvic tumor, open lower ureterectomy was performed, upon completion of single portnephrectomy. The average operative time was 3 hours. One patient requiredconversion to open surgery due to bleeding during nephrectomy.Conclusions: Single port/ LaparoEndoscopic Single Site (LESS) Surgery is feasible, potentiallyoffering better cosmesis and faster recovery due to smaller wound. However, it is technicallychallenging and may require conversion to standard laparoscopic or open technique occasionally.
First Swiss Experience with Laparo-Endoscopic-Single-Site Surgery (LESS) and Retroperitoneoscopic-Single-Site Surgery (RESS)
Introduction: To evaluate feasibility and compare outcome of Laparo-Endoscopic Single Site Surgery (LESS) and Retroperitoneoscopic single-site surgery (RESS).Material & Methods: Since 2010 we performed LESS and RESS surgery for a selected patient population (LESS n=9, RESS n=2): 4 nephrectomies, 3 renal cyst marsupializations, 2 varicocele operations, 1 partial nephrectomy and 1 diagnostic LESS were performed.Results: The intraoperative and postoperative course was uneventful, except one SILS-port defect while performing renal cyst marsupialization. Only one conversion from the RESS technique to conventional retroperitoneoscopic technique was necessary in a case of nephrectomy. The average operative time was 171 min (range=105-285min), blood loss was 104.5ml (range=0-300ml). The average hospital stay was 5 days (range=2-7 days).Conclusion: As described recently in the literature, single-site surgery is a minimally invasive technique with comparable feasibility and results to the conventional laparoscopic technique. Even in highly difficult surgical procedures like partial nephrectomy, we could prove the feasibility. Long-term data are lacking so far and have still to confirm the safety and oncological outcome of this new minimal invasive technique.
Sixteen Pyeloplasty Patient Cases Who Underwent Laparoendoscopic Single Site (LESS) Surgery
Purpose: We have quickly adopted laparoendoscopic single-site surgery (LESS) for pyeloplasty cases to treat adults as well as children. The results of 16 cases (8 pediatric cases) who underwent LESS pyeloplasty was reported.Methods: A total of 16 LESS pyeloplasty cases (8 pediatric cases) performed in our clinic since 2008 entered this study. As a control group, 16 age-matched laparoscopic pyeloplasty cases performed in our clinic were compared. Results: The mean age of the patients was 20.8 years (range1-56 years). Mean operative time was 261 minutes. Regarding the eight pediatric patients, the mean age of the patients was 4.6 years (range1-10 years). Mean operative time was 255 minutes. As for the eight adult patients, the mean age of the patients was 37.1 years (range16-56 years). Mean operative time was 267 minutes. Mean operative time of the control group was 246 minutes. It was 221 minutes for the pediatric patients and 271 minutes for the adult patients. There was no significant difference in the operative time between the control group and the LESS group for both adults and children (Total P=0.5, Children P=0.25, Adults P=0.91). Blood loss was minimal and no intraoperative and postoperative complications were observed. Oral intake started 1.5 days after operation. Conclusion: This method is less invasive laparoscopic procedure and is considered to be highly effective for adult patients as well as pediatric patients. Being cosmetically highly favorable, in the future, this procedure will likely be further developed as a scar-less surgery.
Perioperative Comparison of Robotic-Assisted Laparoendoscopic Single-Site (R-LESS) Pyeloplasty with Conventional LESS (C-LESS) Pyeloplasty
We compared our perioperative experience with robotic LESS (R-LESS) pyeloplasty, performed using the da Vinci Si™ robotic surgical system, to conventional LESS (C-LESS) pyeloplasty.
Between Mar 2009 and June 2011, 10 patients each underwent R-LESS and C-LESS pyeloplasty. Demographic, clinical, intra- and perioperative outcomes for each group were compared. All patients presented with symptomatic UPJ obstruction. Trans-umbilical access was obtained using three 5-mm trocars (4/10) or a GelPOINT™ device (Applied Medical, Rancho Santa Margarita, CA) (6/10) during C-LESS, vs. the GelPOINT™ solely during R-LESS pyeloplasty. Antegrade stent placement was performed during C-LESS, while pre-operative cystoscopy with stenting was performed for R-LESS.
Age, gender distribution, BMI, and proportion with prior abdominal surgery were similar for the groups. During C-LESS, an additional 3-mm lateral instrument was required during the anastomosis, and conversion to conventional laparoscopy was required in two cases, both in contrast to R-LESS. Mean operative time was longer for R-LESS (226 vs. 188 min; p=0.007). One Clavien grade 3a postoperative complication occurred in the R-LESS group, compared to two for the C-LESS group.
In our initial experience, R-LESS improves ergonomics (particularly the anastomosis) during single-site pyeloplasty with comparable perioperative outcomes to C-LESS pyeloplasty. Modestly longer operative times were likely attributable to the additional step of cystoscopy and stent placement.
MP08: Robotic/Lap Prostate 1
University of Montreal Hospital Center, Cancer Prognostics and Health Outcomes Unit, Montreal, Canada, 2Vattikuti Urolology Institute, Henry Ford Health System, Detroit, MI, USA
Introduction:Race represents an established barrier to healthcare access. We examined whether race affects the rate of use of MIRP in a population-based sample of American men.Methods:Within the Health Care Utilization Project Nationwide Inpatient Sample(NIS) we focused on patients in whom MIRP and ORP were performed between 2001-2007. Multivariable logistic regression analyses further adjusted for age, baseline Charlson-Comorbidity-Index(CCI), annual hospital volume tertiles(AHV) and hospital academic status.Results: Overall,we identified 3581 MIRP(5.5%) and 61567 ORP(94.5%) men after exclusion of 24822 for whom race-information was unavailable. Among MIRP patients, 18.4% were non-Caucasians vs 21.1% for ORP (p<0.001). The proportions of non-caucasian patients treated with MIRP were 19.1,10.7,17.8,13.6,23.0,19.9 and 18.6% respectively from 2001 to 2007 (p=0.1) vs 20.2,21.6,21.8,20.9,20.7,22.4 and 21.9% respectively in ORP treated patients during the same study years(p=0.01,increase of 1.2% per year). In multivariable-analysis for prediction of MIRP status, non-caucasian race failed to reach independent predictor status (odds ratio [OR]:0.9,p=0.2). All analyses were then repeated to compare African-Americans to other patients. Of patients treated with MIRP, 8.6% were African Americans vs 11.5% for ORP (p<0.001). The proportions of African American patients treated with MIRP were 4.1,4.0,6.4,8.0,7.5,11.4 and 8.6%,respectively from 2001 to 2007(p=0.004, increase of 3.8% per year) vs 11.3,11.5,11.8,12.3,10.5,11.4 and 11.8% respectively in ORP treated patients during the same study years p=0.9). In multivariable analysis for prediction of MIRP status,African-American achieved independent predictor status (OR: 0.81, p=0.001). Conclusions:Our results indicate that in the United States non-caucasians have equal access to MIRP. Conversely, African-American may have unequal access to MIRP according to the NIS.
Malfunction of da Vinci Robotic Surgery in Urology
Introduction:da Vinci robotic system has been applied to many fields of surgery, especially in Urology. The benefits of minimal invasion and precisely performance increase the popularity.
Purpose:However, malfunction of this system is rarely reported, which may result in variable outcomes. The reliability and safety were concerned. We analyze the malfunction of surgeries in Urology of our cases, and provide the possible solutions for such situations.
Materials and Methods: Since Dec 2005 to April 2010, 400 patients underwent da Vinci robotic urologic surgeries in our hospital. These surgeries were performed by the 3rd da Vinci robot. Malfunction of this system happened in 14 cases. We analyze these cases by the period, procedure, types of malfunction, and management.
Results: There are 14 cases (3.5%) from 400 encountering malfunction of this system. Five (1.25%) happened before surgery and the other nine (2.25%) happened during intra-operative period. Operative procedures include radical prostatectomy (most), partial nephrectomy, nephroureterectomy and radical cystectomy, and partial cystectomy. Malfunctioning component include 10 for joint malfunction (71.4%), 1 for optical system (7.1%), 1 for power system (7.1%); 1 for endoscopic instrument (7.1%); and 1 for software system (7.1%). Four cases were nonrecoverable (critical) failure (1%), and ten cases (2.5%) were recoverable failure.
Conclusions: da Vinci robotic surgery in Urology is extremely reliable. Malfunction of this system is rare (3.5%). Risk of critical failure of da Vinci robotic surgery is very low. How to manage mechanical failure in da Vinci surgery is the key to benefit for patients.
Final Pathology Upgrade of Patients with Low Risk Prostate Cancer Treated with Radical Prostatectomy
Introduction To evaluate the final pathologic characteristics of surgically treated low risk prostatic carcinoma(PCa).Material & Methods Prospective data were collected for men who underwent laparoscopic radical prostatectomy between May1998 - October2008. Preoperative low risk was defined as: PSA less than 10 ng/ml,biopsy Gleason score 3+3 or less and no palpable nodules. Upgrade was defined as pT3 disease and or Gleason score 7 or greater in final specimen. BCR was defined as serum PSA more than 0.2 ng/ml and rising or start of secondary therapy. Kaplan Meier curves and Cox regression analysis was used to estimate predicting factors.Results A total of 846 patients with PLR underwent LRP. Of these, 342(40%) patients were upgraded (Gleason more than 3+4(n=300-35%) or pT3 disease(n=79-9%). Total number of biopsy cores did not impact the proportion of patients upgraded(P=0.5). Number of positive cores was a significant predictor of pathologic upgrade(p=0.02). Percentage of positive cores more than 15% was verified as predictor of pathologic upgrade(233/513(45%) patients more than 15% vs.106/322(33%) patients less than 15%. In multivariate logistic regression analysis, greater age, presence of 2 positive cores and smaller prostate gland were significant predictors of pathologic upgrading. BCR free survival curves for patients with more or equal10 biopsy cores (n=385) did not show any differences in between patients with pathologic low risk disease (pT2, Gleason 3+3) and those who were upgraded (pT3 and or Gleason 7).Conclusions Nine to 35% of patients eligible for active surveillance whom underwent LRP showed high risk of recurrence features in final pathology.
Department of Urology, New York Presbyterian Hospital, Weill Cornell Medical College, New York, USA
INTRODUCTION AND OBJECTIVES: We report the oncologic outcomes of patients undergoing robotic radical prostatectomy (RARP) using a risk-stratified approach based on layers of periprostatic fascial dissection.
METHODS: From December 2010 to June 2011, 1,304 men underwent RARP performed at our institution using a risk-stratified approach. 4 grades of nerve sparing (NS) were adopted as such: Grade 1-Incision of Denonvilliers and prostatic fascia is made just outside the prostatic capsule; Grade 2-Incision through the Denonvilliers (leaving deeper layers on the rectum) and lateral pelvic fascia (LPF) is taken just outside the layer of veins of the prostate capsule; Grade 3-Incision is taken through the outer compartment of LPF removing the prostatic fascia while leaving behind the levator fascia; and Grade 4-Here, we perform wide excision of the LPF (prostatic and levator fasciae) and Denonvilliers fascia. Selection into this risk-stratified approach was based on DAmico risk group where DAmico low risk received Grade 1 NS, intermediate received Grade 2 NS, and high risk received either Grade 3 or 4 NS. We reviewed radical prostatectomy specimen characteristics on final pathology.
RESULTS: Nerve sparing data was available on 1,187 patients. Surgical margin positivity (PSM) in Grade 1, 2, 3, and 4 were 8.3%, 7.4%, 7.3%, and 18.9%, respectively (p=0.086), with overall PSM of 7.9% for the whole cohort. Extraprostatic extension (EPE) occurred in 7.6%, 16.6%, 36.2%, and 54.1% for Grades 1 to 4, respectively (p<0.001).
CONCLUSIONS: Our risk-stratified approach to nerve-sparing robotic prostatectomy based on likelihood of EPE, minimizes margin positivity.
Close Surgical Margin (CSM) After Laparoscopic Radical Prostatectomy is an Independent Predictor of Biochemical Recurrence
OBJECTIVE: To evaluate the impact of CSM on the long-term risk of biochemical recurrence following laparoscopic radical prostatectomy.METHODS: We identified 164 consecutive patients who underwent laparoscopic radical prostatectomy for localized prostate cancer in our institution from 2004 to 2008. In 96 of these patients, associations between margin status, Gleason score, pathological stage, pre-operative PSA, prostate weight, and age with the risk of biochemical recurrence were examined.RESULTS: Seventy-four of 96 patients (77%) had negative margins. Of these patients, 17 (23.0%) had CSM. In the group with PSA recurrence, median time to recurrence was 28.5 months. In the group without recurrence, median follow-up was 45.6 months. Cumulative recurrence-free survival differed significantly among the three types of margins (positive, negative and close) (p<0.001). On multivariate analysis, CSM constituted a significant, independent predictor of recurrence (HR 2.27 95%CI 1.12-4.86). Gleason score and positive margins were the strongest prognostic factors.CONCLUSIONS: In this cohort, CSM were independently associated with a twofold risk of postoperative biochemical recurrence. Further evaluation of the clinical significance of CSM is indicated, as they might be an indicator of local recurrence and of relevance when considering salvage therapy.
Pathologist is an Independent Predictor of Positive Surgical Margin Rates
INTRODUCTION: We analyzed 13 heterogeneous surgeons in regards to factors affecting their positive surgical margins (PSM).METHODS: We captured 100% of the procedures performed by 13 independent surgeons and analyzed their surgical margin rates. Binary logistic regression was performed with PSM as an endpoint. Surgeons performing <10 cases were excluded from the analysis. RESULTS: 1575 patients underwent RALP between August 2005 and August 2010 on a shared da Vinci Surgical system. Surgeon volume ranged from 21 - 396 cases. Factors affecting PSM are shown in Table 1. PSM rates reported by 4 independent pathologists varied (range 14−28% PSM rate). The significance remained after controlling for surgeon variation (p<0.05).CONCLUSIONS: In addition to the known risk factors such as PSA and stage, we found that choice of surgeon, and choice of pathologist influenced margin rates. Patient obesity and procedure time had no effect on margin status in our model.

Department of Urology, Geneva University Hospital
INTRODUCTIONAim of this study is to present oncologic and functional outcomes of Robot-assisted radical prostatectomy (RARP) for localized prostate cancer with a 2 year follow-up. MATERIAL AND METHODS146 patients were included. Histologic analysis of the specimens included presence and localisation of margins. Positive margins were categorized as focal (1-3 mm long on a single slide) or extensive (>3mm). Urinary continence and erectile function were measured pre and postoperatively, excluding older than 65 patients with preoperative ICS1>1 or IIEF-5<23, or that did not undergo nerve sparing procedure. RESULTSOverall positive margin rate was 23%, of which 52% were focal. Margin rate in pT2 tumors was 16%, 44% being focal. In pT3 tumors, 35% of patients had positive margins, but 3 quarters were focal. Mean ICS1 scores were 3/23 at 1 year and 2.8/23 at 2 years. Mean ICS2 score was 2.4/12 after 1 and 2 years. 74% were pad free after the first postoperative year. When patients wearing a safety pad were considered continent, continence rate reached 85% . Merely 8% of patients wear>1 pad/day after 1 and 2 years.After unilateral nerve sparing procedures, mean IIEF-5 was 13.2/25 (1-24) at 1 year, 21/25 (17-25) at 2 years. After bilateral nerve sparing, mean IIEF-5 were 12.3/25 (1-22) at year 1, 18.3/25 (5-24) at year 2. Transfusion rate was 1%. CONCLUSIONOncological and functional outcomes of the first 146 RARP was satisfactory. Ongoing assessment of this series entailing now 300 patients may outline a learning curve effect.
Department of Urology, NewYork-Presbyterian Hospital, Weill Cornell Medical College, New York, NY
OBJECTIVES: We wanted to investigate preoperative predictors of pT3 disease and 3-year BCR as well as the influence of nerve sparing and positive surgical margin status on 3-year BCR rates.
METHODS: 774 patients who underwent RARP at our institution and had at least 3 years follow up were included for analysis of BCR and pT3 rates. BCR was defined as a postoperative PSA>0.2 ng/ml and pT3 by evidence of extraprostatic extension in surgical pathology. Multivariable logistic regression models were used to develop the pT3 and BCR predictive nomograms. The predictive accuracy of the models was assessed in terms of discrimination and calibration.
RESULTS: All nomograms discriminated well between patients that recurred and those that did not (bootstrap corrected c-indices of 0.732, 0.766, and 0.806 for nomograms 1, 2, and 3, respectively). Nomograms 1 & 2 were well calibrated, but nomogram 3 over-predicted the probability of biochemical recurrence in patients at>30% risk.
CONCLUSIONS: Our nomograms have good predictive ability to differentiate between RARP-treated patients that exhibit extraprostatic extension (pT3 disease) and biochemical recurrence by 3 years from those who do not. Adding nerve sparing and surgical margin status further improved discriminatory ability for BCR at the expense of over-prediction for patients at high risk. These nomograms may be used to counsel patients on their likelihood of extraprostatic extension and guide the use of nerve sparing and the management of positive margins in RARP.
Do Nomograms Accurately Predict Nodal Positivity with Extended Lymphadenectomy for High-Risk Prostate Cancer?
Introduction: Nomograms are often used before prostatectomy to predict likelihood of nodal involvement and determine need for lymphadenectomy. Commonly-used nomograms are not based on extended pelvic lymph node dissection (ePLND) and may therefore underestimate lymph node positivity (LN+) in higher-risk patients. Objective: We assessed the predicted versus actual LN + rate after ePLND during robotic prostatectomy. Methods: All robotic prostatectomy procedures with ePLND performed by a single surgeon (RA) between February 2008 and December 2010 were reviewed. Indications for ePLND included PSA>/=10, Gleason>/=8, stage>/=cT3a, and/or>50% of biopsied tissue involved by tumor. Predicted LN + was calculated from pre-operative characteristics using Partin and MSKCC nomograms and compared with observed LN + on pathology. Patients were stratified by nomogram-predicted risk for LN + of<5%, 5-10%, and>10%. Results: A total of 155 patients underwent ePLND with median PSA of 6.9ng/mL (1-114.5ng/mL). Overall mean yield was 15 nodes with LN + identified in 38 patients (24.5%). Sufficient clinical data were available for 135 patients for Partin and 130 patients for MSKCC nomogram calculations. The median Partin and MSKCC nomogram-predicted rates of LN + were both 6%. For Partin nomogram-predicted probability of LN + of<5%, 5-10% and>10%, observed LN + rates were 12.5%, 28.6%, and 31.8%, respectively. For MSKCC nomogram-predicted probability of LN + of<5%, 5-10%, and>10%, observed LN + rates were 10.9%, 25.5% and 35.1%, respectively. Conclusions: Commonly-used nomogams underpredicted nodal disease in higher-risk prostate cancer patients undergoing ePLND. Nomograms should be used with caution in these patients to avoid potentially inappropriately omitting lymphadenectomy.
The Institut Montsouris
Introduction an purposes To estimate the positive surgical margin learning curve. Material & Methods We evaluated our prospectively collected robotic prostatectomy database and estimated the positive surgical margin rate trend over the last 10 years, for the entire population, according to risk groups and pathologic stage. Prostatectomies were performed by one of 4 surgeons (300 laparoscopic prostatectomies experience). Risk groups were defined as DAmicos 2001. Intermediate and high risk patients were analysed together. We estimated proportions of PSM by year and generated trend curves estimating R2 coefficient.Results From May 2000 through August 2010, 795 patients with localized prostate cancer were treated with robotic radical prostatectomy. The median age was 62 years (Interquartile range, IQR: 57,65), BMI was 25 (23, 27), and PSA was 6.7 (5.2, 9). Overall, 34% had palpable nodule (n=279), 2% had biopsy Gleason 8-10, 31% Gleason 7 and 67% Gleason 6 or less. PSM were identified in 18% (n=146), 15% pT2 and 28% pT3a-b. The proportion (n) of PSM by risk Group was: Low Risk, 17%(75), Intermediate Risk,19%(60) and High risk, 24%(9). XY graphs show PSM trends overall (R2=0,498), Low risk (R2=0,429), intermediate and high risk (R2=0,399), pT2 (R2=0,577) and pT3 ( R2=0,009).Conclusions: We observed a decreasing trend in PSM in pT2 patients with low risk features, particularly after around 100 cases; however, we failed to observe such a trend in pT3 patients even after having performed 189 such cases.
Department of Urology, Okayama University Graduate School of Medicine, Okayama, Japan
Introduction and Purpose: Discrepancy between Gleason grade on TRUS biopsy and final pathology may impact management disposition of clinically localized prostate cancer. We review the findings in our cohort of RALP patients.
Materials and Methods: Consecutive patients who underwent transperitoneal RALP by a single surgeon (CW) were reviewed. Using an anterior approach, a bladder neck sparing procedure was preferentially performed. TRUS guided biopsy specimens and final prostate pathology were compared.
Results: 233 consecutive patients were identified. The mean number of biopsy cores sampled was 11.3±5.1. Clinical stage included 210 (90.1%) T1c and 14 (6.0%) T2a, having a mean Gleason score of 6.5±0.8. 195 (83.7%) had bilateral, 20 (8.6%) had unilateral and 18 (7.7%) did not undergo nerve sparing prostatectomy. 2 (0.8%) pTx, 34 (14.6%) pT2a, 13 (5.6%) pT2b, 144 (61.8%) pT2c and 40 (17.2%) pT3 cancers were reported, having a mean prostate volume of 44.8±12.7 mL. The mean Gleason score was 6.5±1.0. 34 (14.6%) patients had positive surgical margins. Upgrading on final pathology occurred in 30 (12.9%), downgrading in 35 (15.0%) and 168 (72.1%) prostate specimens remained unchanged. The independent variables of preoperative age, BMI, digital rectal examination, PSA, TRUS volume, Gleason score, number of positive biopsy cores and final pathology were not predictive of whether pathologic upgrading or downgrading would occur.
Conclusions: Our incidence of pathologic upgrading and downgrading following RALP is consistent with that reported in the literature. Whether a TRUS guided biopsy specimen will change on final pathologic evaluation appears to be difficult to predict preoperatively.
Section of Urologic Oncology Section and Dean and Betty Gallo Prostate Cancer Center, The Cancer Institute of New Jersey/Robert Wood Johnson Medical School, New Brunswick, NJ, USA
Introduction: Positive surgical margin (PSM) is an important prognostic factor of biochemical recurrence following radical prostatectomy.Purpose: This study evaluated the prognostic significance of PSM according to the pathological stage and Gleason score in patients with localized prostate cancer who elected radical prostatectomy as the primary therapy.Materials and Methods: We reviewed 498 prostate cancer patients who underwent a robot-assisted radical prostatectomy (RARP) without any adjuvant therapy between 2006 and 2009. Median follow-up was 21 months. Biochemical recurrence was defined as two consecutive rises in PSA above 0.2 ng/ml.Results: Overall, PSM rate was 13.6% (68/498) and men with PSM had a significantly higher risk of post-operative PSA recurrence (19.1%, 13 of 68 patients ) (p=0.014). When these patients were stratified by pathological stage, biochemical recurrence rate in pT2 and pT3 patients with PSM were 8.8% (3/34) and 29.4% (10/34), respectively. Biochemical recurrence-free survival (RFS) did not differ between the margin-positive and negative group in patients with pT2 disease (p=0.078). However, in patients with pT3 disease, PSA recurrence rate was significantly higher in men with PSM (HR=2.3∼3.3 fold, p<0.05). Similarly, the biochemical relapse rate was significantly higher in men with Gleason score >=8 when compared to those with Gleason score <=7 (HR=7.59 fold, p=0.016). Conclusions: Overall, PSMs are associated with an increased biochemical recurrence rate. However, in men with pT2 disease, surgical margin status did not portend worse outcome. These results suggest that adjuvant therapy may not be necessary in men with PSM and organ-confined prostate cancer.
The Department of Urology, Acibadem University, Istanbul, Turkey
Introduction: Pelvic lymph node dissection (PLND) is the most reliable method for detection of lymph node metastasis. In this study, data of the patients who underwent robot-assisted radical prostatectomy (RARP) with or without PLND were compared.Material and Methods: Between March 2005 and July 2011, 300 patients underwent RARP and 176 RARP + PLND. In PLND group, 11 patients (of the first 70) underwent standard and 165 extended PLND. Comparative data is presented in Table-1Results: On average, in standard PLND group, 4 (2-6) and in extended PLND group 15 (7-47) lymph nodes were removed. In standard PLND group and extended PLND group, lymph node positivity was 9.0% (1/11) and 12.7% (21/165), respectively. Mean PSA and positive surgical margin (PSM) rate were 11.8 ng/ml and 45% and 9.8 ng/ml and 11.1% for lymph node metastasis (+) and (-) patients, respectively. Among PSM patients, pT3 rate was 8/9(88.8%) and 12/18(66.6%) for lymph node metastasis (+) and (-) patients, respectively.Conclusion: Extended PLND can be safely performed during RARP with acceptable complication rate and blood loss. The yielded number of the lymph nodes is equal to the open series. Length of hospital stay is longer in PLND group while complication rates are similar.
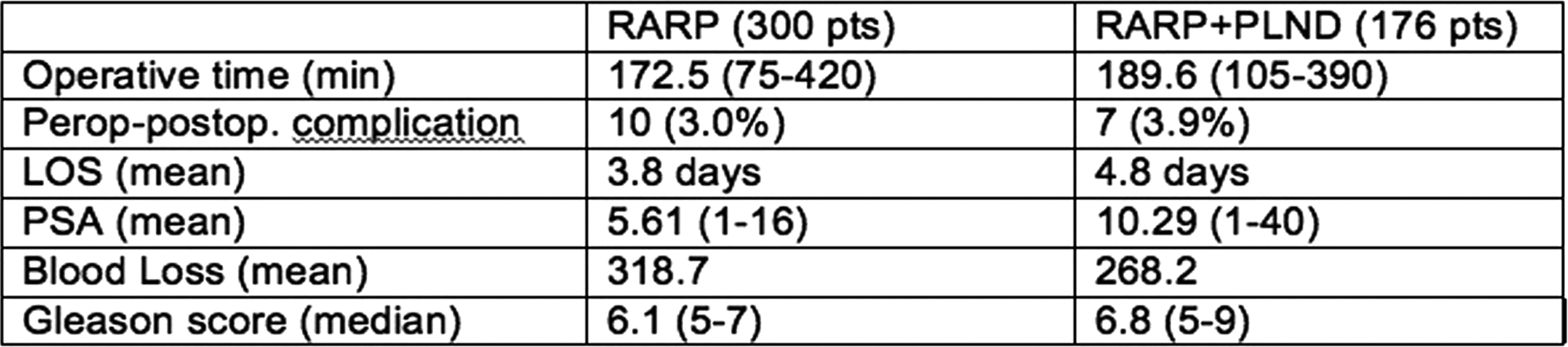
Hackensack University Medical Center
Introduction and Objectives:Prostate median lobe enlargement can be technically challenging during robot-assisted laparoscopic radical prostatectomy (RALP). We investigate whether the presence of a median lobe on preoperative cystoscopy increases the incidence of positive surgical margins (PSM).Methods: The operative records of two surgeons at our institution performing RALP between 2004 and 2009 were reviewed. All patients underwent preoperative office cystoscopy, and the presence (median lobe, or + ML) or absence of a median lobe (NML) was recorded. Results:A total of 490 patients were included in the review, including 394 patients without an enlarged median lobe and 96 patients with an enlarged median lobe. The overall rate of extracapsular extension (pT3) was 11.8%. The PSM rate was 20.8% in the + ML group and 23.4% in the NML group. The preoperative PSA and prostate sizes were similar in each group, while the operative time in the + ML group was higher than the NML group.Conclusions:There was no difference in the PSM rate in patients with and without an enlarged median lobe on preoperative cystoscopy. Preoperative cystoscopy may improve the surgeons ability to tailor the bladder neck dissection and thus prevent inadvertent incision into the median lobe.
Associated Medical Professionals
Objective: We attempted to identify factors associated with Positive Surgical Margins (PSM) and their location during RALP.Methods: Records of patients undergoing RALP between 2003-2009 were retrospectively reviewed. We collected demographic data cumulative surgical experience, clinical (PSA levels, biopsy Gleason sums), nerve-sparing technique, and pathological variables including stage, Gleason sums, prostate weight, status and location of the surgical margins. Multivariate regression models were constructed to identify factors associated with PSM at prostate apex, periphery, proximal and all locations.Results: A total of 560 patients were analyzed. Median age was 60.1, 19% were African-Americans, median BMI was 28.1, PSA levels were 5.3 (3.9-7.1ng/mL) and mean prostate weight 45.2. Gleason sums were as follows: less than 6 in 42.5%, 7 in 53.4% and greater than 7 in 3.1%. Overall, PSM were reported in 130 (23.2%), including 58 (44.6%) apical, 81 (62.3%) peripheral and 20 (15.4%) proximal. Overall rate of PSM was associated with surgical experience, PSA, prostate weight and Gleason sums. Apical PSM were independently associated only with surgical experience. Peripheral PSM were associated with PSA, stage, Gleason sums, prostate weight. Finally, proximal margin status showed an association with PSA levels only.Conclusions: Apical margin status is significantly and independently associated only with surgical experience, whereas peripheral, proximal and overall PSM are largely associated with inherent disease biology (grade, PSA levels etc.). This emphasizes apical margin status as an indicator of surgical expertise with RALP. Improvement of oncological outcomes could be achieved as future experience is gained with RALP.
Associated Medical Professionals
Background: The risk factors for prolonged operative time (OT) during robot-assisted laparoscopic radical prostatectomy (RALP) have not been studied.Objective: To determine risk factors for prolonged OT during RALP.Design, Setting, and Participants: Retrospective review of patient records undergoing RALP between 2003 and 2009.Measurements: The following variables were recorded: age, race, body mass index (BMI), prior abdominal surgery, nerve-sparing technique, lymph nodes dissection, pathological stage, cumulative surgical experience with RALP since introduction of RALP, prostate weight and OT calculated skin-to-skin by the anesthesiologists. Prolonged OT was defined as the upper quintile (20%) according to the distribution. Multivariate regression model was generated to assess potential predictors of prolonged OT. Results and Limitations: Overall 523 records were retrieved. Caucasians accounted for 77.8% of the cohort. Median age was 60.3,median BMI 28.1, prostate weight 46.0. Eighty-six (16.4%) patients had prior abdominal surgery, lymph nodes dissection (LND) was performed in 341 (65.2%) and nerve sparing (NS) was done in 310 (59.3%) cases. Median OT was 175 (IQR 146-220 min). Prolonged OT was set at greater than 230 min, thereby 105 (20.1%) records were classified as such. On multivariate analysis, cumulative surgical experience with RALP, NS, and prostate weight were independent predictors of prolonged OT. In addition, the definition of prolonged OT is based purely on statistical parameter distribution and was not correlated to potential outcomes. Conclusions: Larger prostates are associated with longer OT and this effect is maintained independently of cumulative robotic experience that represents another independent factor in determining OT.
MP09: New Technology/Imaging 1
The AirScope: A Novel Wireless Laparoscope
IntroductionThe modern laparoscope relies on Hopkins glass rod lenses and a fibre-optic light source with a camera and external cables. We aimed to assess the feasibility of developing an experimental prototype of a wireless laparoscope.MethodDesign requirements were defined to mimic a 10mm adult laparoscope. An 8mm camera (CMOS) was used which delivered standard TV resolution at an image refresh rate of 25Hz. A wide-angle lens and focusing mechanism was designed. Illumination was achieved using miniature LEDs. 2.4GHz wireless transmission with adequate range was required. A wireless receiver on a standard computer with off the shelf image processing software was used. A rechargeable battery powered the system.ResultFlicker-free invitro wireless video transmission was achieved. The unit is waterproof and allows gas or chemically sterilisation. Its weight is 78 grams compared with more than 1000 grams of a typical 10mm laparoscope, camera and fibre-optic setup. Drawbacks included reduced resolution as compared to HDTV quality on some commercial cameras.ConclusionThis prototype demonstrates improved ergonomic maneuverability and reduced weight.

3D Endocam: Preliminary Report of a Novel Stereoscopic Laparoscope.
IntroductionLaparoscopy (non-robotic) relies on 2 dimentional video feedback. This 2D field-of-view reduces surgical performance particularly when complex suturing is required. PurposeStereoscopic 3D visualisation holds the promise of enabling the surgeon to attain a greater appreciation and handling of tissues by improved depth perception.Materials and MethodsInitially a prototype involved the manufacture of a traditional 15mm laparoscope that incorporated miniature digital cameras and a LED light source. Various commercially available stereoscopic rendering software packages and methods for stereoscopic display were explored. ResultsThis preliminary report describes the construction of the prototype. We report that a dense stereoscopic image is obtained with our chosen rendering software and autostereoscopic display. Conclusion Stereoscopic laparoscopy undoubtedly holds promise for reducing patient morbidity and providing the surgeon with greater appreciation of the operative field via 3D visualisation. Future proof of concept will be the successful performance of a porcine nephrectomy.
Department of Urology , Kings College Hospital NHS Trust, London, UK
Despite demonstrated benefits for patients the adoption of minimally invasive surgery relies on a learning curve restricted by a two-dimensional vision. Current laparoscopic and robotic stereoscopic systems provide an unnatural albeit improved three-dimensional viewing. We propose a 3D imaging system producing images that are true optical models.
To address the eye fatigue and headaches caused by stereoscopy after prolonged use in operations as it requires users to focus onto the plane of the screen while their eyes are converging to a point in space.
We have developed proof of concept cameras and display models (fig.1). The proposed 3D imaging technology allows natural accommodation and convergence to accomplish stress-free viewing.

We display on a poster a ground-breaking 3D image relevant to minimally invasive urology without the need for 3D eyeware. We are developing a laparoscopic prototype and algorithms required to convert DICOM data from CT, MRI and US into 3D images on flat screen.
Our application to the medical field of this emerging technology will revolutionize the visualization spectrum from diagnosis, to staging investigations, simulation training and we believe will add a new dimension to augmented reality in minimally invasive surgery.
Trajectory Image-Guided Percutaneous Renal Cryoablation in a Porcine Model: A Pilot Study
Introduction: Traditional CT-guided localization for percutaneous ablative procedures often requires large amounts of radiation exposure, and does not provide true realtime imaging. Purpose: To assess the technical feasibility and safety of trajectory image-guided percutaneous renal cryoablation in a porcine model. Methods: 5pigs were used(10kidneys). Image-guided localization was performed using The O-Arm and StealthStation TREON System (OASSTS, Medtronic,USA) utilizing a bone anchored tracking frame. Specific areas of each renal unit were targeted and satisfactory targeting was determined utilizing both gross analysis and histopathologic confirmation of appropriate treatment on necropsy.Results: Results of individual treatments are displayed in the table. All treatments were successfully localize based on correlation between planned treatment location and analysis of location of treatment on necropsy. Mean total treatment time was 57.85 minutes. The mean cryoablation lesion diameter and depth (from the level of the renal capsule) was 40.1 and 17.8 mm, respectively. Conclusion: The OASSTS provides excellent real-time localization for cryoprobe placement, with decreased radiation exposure to the operator and patient. Further studies need to be done to assess efficacy in treatment of tumors prior to adoption in clinical practice.
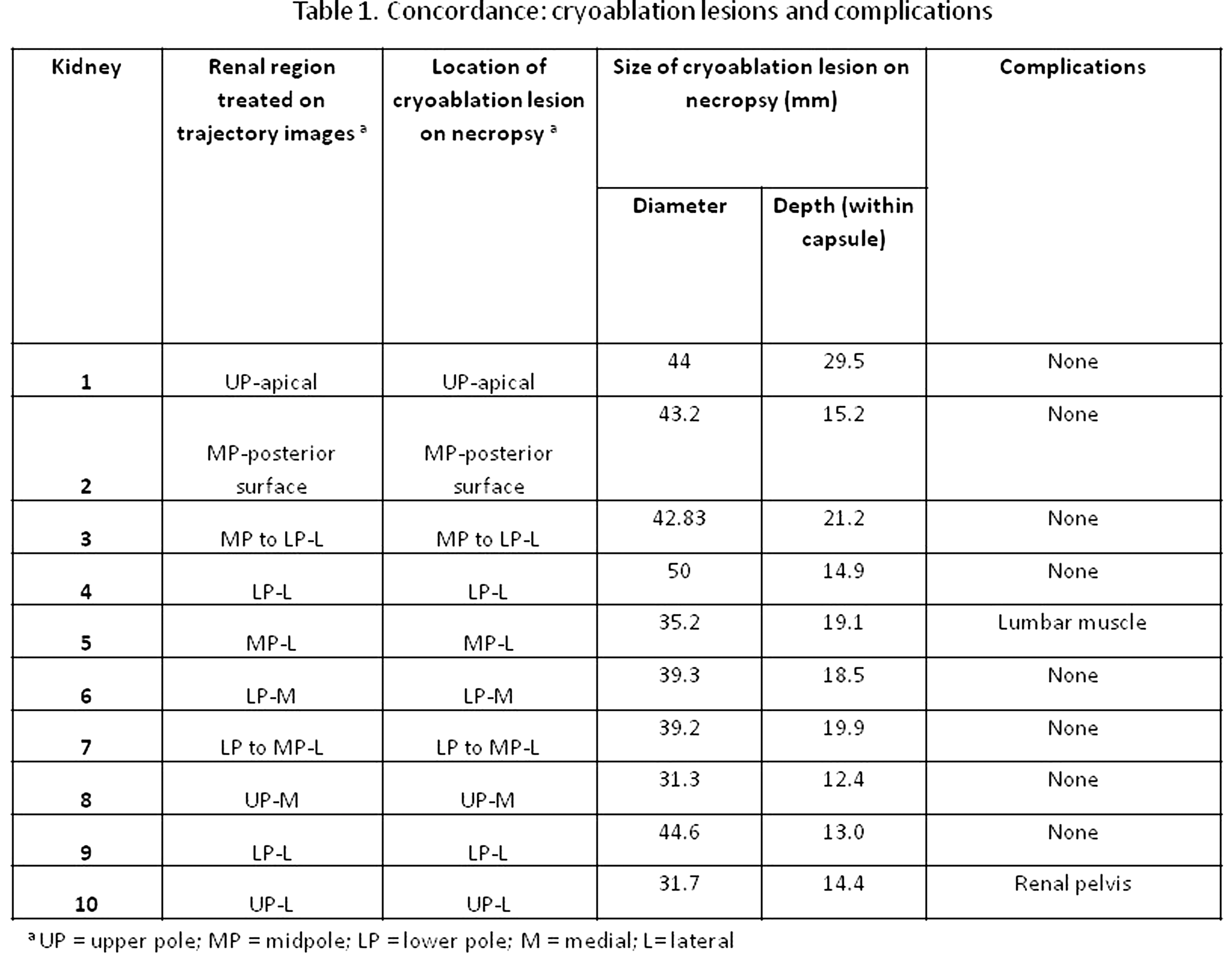
James Buchanan Brady Urological Institute, Johns Hopkins University
Introduction: Laparoscopic partial nephrectomy (LPN) can be technically challenging and relies on resection without visible landmarks (especially when tumors are endophytic) in a limited field of view. Advances in intra-operative imaging, navigation and registration with preoperative imaging may improve the safety, applicability and dissemination of LPN and related surgeries. Purpose: To describe the creation and use of renal phantoms for the use in image-guided LPN. Methods: Ex-vivo phantoms (animal tissue preparations exhibiting structures resembling actual in-vivo conditions) were based on porcine kidneys (extracted shortly after exitus). Kidneys were partially treated with CT contrast agent via artery and ureter (5% suspension of TiO powder (5m) in agar solution), and embedded in a stabilizing porcine gelatin mold. Fiducials were inserted into the phantoms to facilitate later registration. Pseudotumors were created with radiofrequency ablation and alginate injection. Using a novel system based on 3D-US elasticity imaging (EI) registration with CT imaging, pseudo-tumor containing phantoms were tested for ability to identify, register and track tumors for intra-operative motion tracking. Results: Renal parenchyma, blood vessels, the collecting system, pseudo-tumors and fiducials were visualized using CT and US. With high quality, robust strain imaging (through a combination of parallelized 2D-EI, optimal frame pair selection, and optimized palpation motions), kidney tumors that were previously unregistrable or sometimes even considered isoechoic with conventional B-mode ultrasound were imaged reliably. Conclusions: Porcine-based renal phantoms with tumor models are easily produced, viewable in US and CT imaging and are the foundation of markerless mutual-information-based registration and intraoperative tracking.
James Buchanan Brady Urological Institute, Johns Hopkins University
Introduction: Laparoscopic partial nephrectomy (LPN) can be technically challenging and relies on resection without visible landmarks (especially when tumors are endophytic) in a limited field of view. Ultrasound elastography can discriminate and classify lesions in a number of tumor models. Purpose: In order to improve the safety, applicability and dissemination of LPN and related surgeries, a real-time image-guided intervention system was created using 3D elastic imaging (EI) registered to preoperative CT. Methods: The strain computation process of 3DEI is optimized using dynamic programming algorithms and electromagnetic tracking of the US probe to create a 3D volume reconstruction with few low-quality frames. EI stiffness values are registered to CT density information using Mattes Mutual Information as the metric for registering two distinct modalities. Three landmarks are chosen in US and CT and registered via optimization algorithms. The tumor is outlined on 2D imaging by the user, then scaled and stored into 3D by the navigation part of the system. Using electromagnetic (EM) sensors in the porcine-based and synthetic kidney tumor phantoms, US probe, laparoscope and instruments, a 3D tumor is overlaid into the live video stream. Results: Registration of the volume of interest was complete in 5-10 seconds for three translational degrees of freedom. With high-quality, robust strain imaging, kidney tumors were imaged reliably in an interventional setting. Using EM sensors, real-time motion tracking was achieved. Conclusions: Through real-time elastrography, fast 3DEI/CT registration and intraoperative tracking, kidney tumors could be located and tracked in a phantom model for laparoscopic partial nephrectomy.
Diagnostic and Clinical Value of Post-PCNL Nephrostogram
Introduction:Nephrostomy tube insertion after Percutaneous Nephrolithotomy (PCNL) is commonly used in current practice. Post-PCNL nephrostogram (PPN) is then performed, to exclude post-operative complications. Purpose:We critically reviewed diagnostic and clinical value of performing PPN at our institution. Materials and Methods: We performed a retrospective radiological and case note review of all patients (n=105) at our institution who had undergone unilateral PCNL and nephrostomy insertion, for stone disease, between January 2006 and May 2011. Demographic data on patients and clinico-radiological outcomes of PPN were assessed. Results: The average patient age was 56 years (25-95); 53 males (50.5%) and 52 females (49.5%). PPN (Left, n=57; Right, n=48) was performed on all patients on median post-operative day 3 (1-5). 78 out of 105 PPNs (74.3%) were deemed satisfactory, with free drainage, and nephrostomy tube was removed uneventfully. Repeat PPNs were obtained in the remaining 27 patients (once, n=18; twice, n=6; thrice, n=3) and nine cases required antegrade ureteric stenting. Subsequently, only 2 of these patients actually had confirmed ureteric stone on retrograde studies requiring ureteroscopic stone extraction, the remainder had obstruction due to clot/oedema. There were no significant differences in outcomes in males and females, or related to laterality of PPN. Conclusion: Unsatisfactory initial PPN was only detected in a quarter of cases, but resulted in a change in clinical outcome. Overall incidence of patients requiring antegrade ureteric stenting was found to be remarkably low.
Clinical and Population Sciences & Education Division
Introduction
We undertook a systematic review of studies examining the usefulness of Image Guided Biopsy (IGB) for in indeterminate and small renal masses. We investigate the methodological difficulties in conducting the systematic review and provide recommendations for quality improvement in future studies evaluating IGB.
Methods
We included 36 studies that enrolled adults with suspected renal masses on imaging, and measured one or more of the following outcomes:
Diagnostic accuracy of image-guided biopsy compared to final histopathological outcome following surgical procedure or follow-up imaging for at least 5 years.
Improvement of diagnostic accuracy using additional or adjunctive histopathological techniques.
Adverse events.
The index test was IGB: ultrasound, computerised tomography, or magnetic resonance imaging. The reference standard was histopathology of the final specimen (radical nephrectomy or nephron sparing surgery), or at least five years follow-up of imaging results. Study quality was examined using a validated checklist.
Results
The studies were poorly reported; and had problems with several methodological features:
Less than optimal follow-up for determining change in a mass identified by biopsy;
Failure to independently outcome assess, spectrum bias;
Unclear reporting of withdrawals;
Dissimilar comparisons; and
Conclusions based on premature follow-up.
Because they were poorly conducted, the usefulness of IGB for renal masses remains unclear.
Conclusions:
The methodological scrutiny of studies reporting on image guided biopsies in small renal masses showed many flaws and forms the basis of recommendations for future areas of improvement in conducting and reporting of studies on this topic.
Brady Urological Institute, Johns Hopkins Hospital
Introduction: Patients with acute flank pain or kidney pain are most commonlyevaluated in the emergency department (ED) with computed tomography (CT). Atpresent, our understanding of the radiographic practice patterns in the emergencyimaging of flank pain is limited. We performed a study to characterize the utilization ofconventional radiography (X-ray), ultrasound (US), and CT in the ED evaluation ofpatients with acute flank pain.Materials and Methods: A retrospective cross-sectional analysis of ED visits using datafrom the National Hospital Ambulatory Medical Care Survey (2000-2008) wasperformed. Specific visits for a complaint of either flank pain or kidney pain were furtheranalyzed.Results: Over the time period studied, there was a significant increase in the utilizationof CT (p<0.0001), a significant decline in the use of X-ray (p=0.035), and the utilizationof US remained stable (p=0.803). Over that same time period, the proportion ofpatients with flank pain who were diagnosed with a kidney stone remained stable, atapproximately 20% (p=0.135). Conclusion: Between 2000 and 2008, there was a significant increase in the utilizationof CT in the emergency evaluation of patients with flank pain.
Division of Urology, University of North Carolina, Chapel Hill, USA
ABSTRACT WITHDRAWN
Department of Urology, Addenbrooke's Hospital, Cambridge, UK
IntroductionStone size can be measured in various ways with maximum diameter on X-ray KUB traditionally used. 3D cross-sectional imaging and reconstructive software allows for rapid assessment of stone volume. Stone volume may be helpful in predicting treatment outcome for renal stones. We assessed the relationship between maximum diameter on plain film, surface area on plain film and maximal diameter on a single CT slice compared to 3D software reconstructed volume.Methods100 stones with both X-ray KUB and CT scan (1-2mm slices) were reviewed. Staghorn stones were excluded. Stone volume and surface area were calculated using software designed to measure irregular shaped ellipsoids. Correlation coefficients between all measured outcomes were compared. Stone volumes were analysed to determine the average "shape" of the stones. Results Maximum diameter on X-ray KUB ranged from 3 - 48mm, surface area from 6.88 - 1478 mm2, CT scan diameter from 3 - 48 mm and volume from 14.15 - 36760 mm3. Smaller stones trended towards prolate ellipsoid (rugby-ball shaped), stones between 8 - 15mm towards oblate ellipsoids (disc shaped) and stones over 15mm towards scalene ellipsoids. Stone maximal diameter and surface area on plain film were well correlated and estimated stone volume with similar precision. ConclusionThe average shape of renal stones changes with maximal diameter. No single equation for estimating stone volume can be recommended. As maximal diameter changes, there is poor correlation with stone volume. We recommend that research looking at stone clearance rates should use CT reconstructed stone volumes.
Additional Findings on CT KUB Done for Renal Colic: Are We Opening a Pandoras Box
Introduction: We aimed to evaluate the rates of stone disease and the presence of any additional pathology on routine CT KUBs.Material & Methods: A review of 404 consecutive cases of suspected acute renal colic was undertaken. Data was collected on patient demographics, size and site of stone, presence of contralateral (non-symptomatic side) calculus disease, additional urological or non-urological pathology and its clinical relevance. Results: 404 patients had CTKUB (mean age: 50 years), with 239 males and 165 females. Ureteric stone was found in 58 (14%), with renal stones in 85 (21%) and combined ureteric and renal stones in 39 (10%) patients. Contralateral asymptomatic renal stones were seen in 75(19%). Apart from stone disease, additional findings were picked up in 264 (65%) patients. Of these, urology specific pathology was found in 85 (21%) patients and non-urological pathologies were seen in 113 (28%) patients. Clinically relevant non-calculus pathologies were found in 107 patients (26%) (Table 1). Conclusions: CT KUB pick of additional pathologies can lead to the diagnosis and treatment of other pathologies in the absence of stone disease. Our findings confirm the importance of the use of CT KUBs for accurate diagnosis in all patients presenting with acute renal colic.
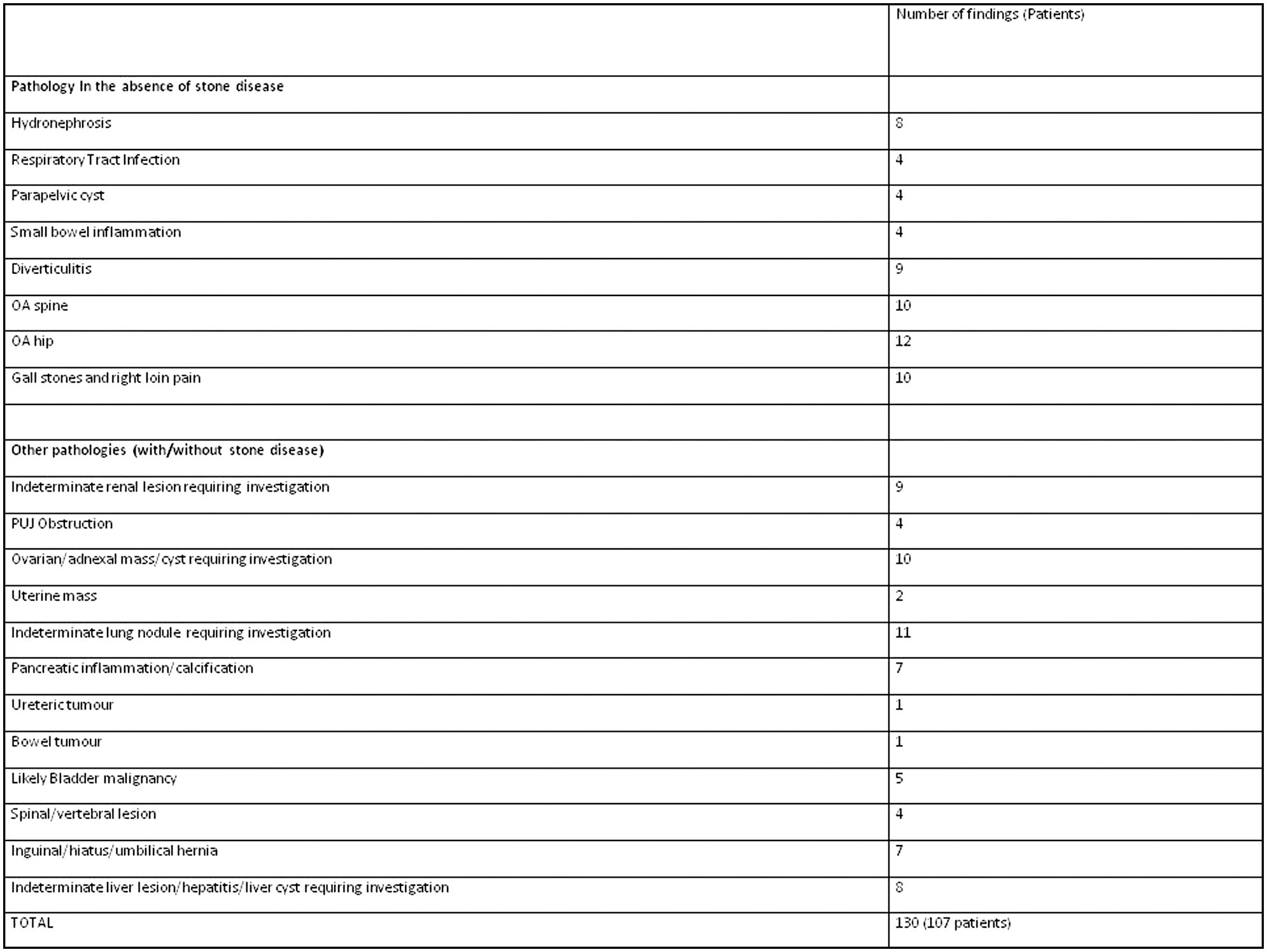
Department of Urology, Kyoto University Graduate School of Medicine, Kyoto, Japan
Introduction
Hardness of perirenal fat tissue sometimes bothers surgeons during laparoscopic renal surgery. The purpose of our study is to investigate the possibility of prediction of hardness of perirenal fat tissue using preoperative CT images.
Methods
Thirteen patients who underwent laparoscopic partial nephrectomy for renal tumor or donor nephrectomy were enrolled in this study. We reviewed intraoperative movies recorded on DVDs, and classified the hardness of fat tissues into three grades, "soft", "intermediate", and "hard". We measured pre-contrast CT attenuation values within circular regions of interest created in the perirenal fat tissue. Standard deviation (SD) of the CT attenuation values was calculated per individual patient for measurement of those variances and used as an indicator for heterogeneity of fat tissue. The correlations between average or SDs of CT attenuation values and grade of hardness were statistically analyzed.
Results
Average CT attenuation values (Hounsfield Units)/SDs of fat tissues in groups of patients with soft (n=5), intermediate (n=4) and hard (n=4) fat tissue were −89.7/15.2,−107.0/13.4 and −94.2/19.5, respectively. These CT attenuation values were not statistically different among three groups. Although the SDs of CT values were not statistically significant among three groups, there was a tendency that SDs in patients with hard fat tissue is slightly higher than those in other groups.
Conclusions
According to our preliminary experience, prediction of hardness of fat tissue seems difficult based on CT attenuation values. Further investigation in a larger patient population is required, especially in a viewpoint of SD of CT attenuation values.
Department of Urology, University of Wisconsin School of Medicine and Public Health, Madison WI, USA
Introduction: Automated volume measurement of renal calculi of non-contrast computed tomography (CT) may be preferable for the serial assessment of stone burden. The aim of this study was to compare the reproducibility of automated volume measurement to manual linear measurement using same-day supine and prone CT series. Methods: Fifty consecutive adults (mean age:56.4 years) with renal calculi identified during CT colonography screening comprised the patient cohort. The largest stone per patient was assessed treating the supine and prone CT series as mutual controls. Automated stone volume was derived using a coronary calcium scoring tool(Ziosoft). Maximum axial lengths for each index stone were manually measured by 3 board-certified radiologists. Supine-prone reproducibility for automated volume was compared with intra-observer supine-prone manual linear measurement. Inter-observer variability for manual linear measurements of the same supine or prone series was also assessed. Results: Mean linear size and volume of the 50 index calculi was 4.5±2.7 mm(range 1.8-16 mm) and 141.7±456.1 mm3, respectively. Mean supine-prone error for automated stone volume was 16.3% compared with an average uni-dimensional intra-observer error of 11.7% for manual axial measurement. Inter-observer linear error for the same CT series averaged 26.3%, whereas automated volume measurement of the same series did not vary. Conclusion: Automated non-contrast CT renal stone volume is more reproducible than manual linear size measurement and avoids the often large inter-observer variability seen with manual assessment. Because small linear differences correspond to much larger volume changes, automated volume measurement may be an improved clinical parameter for following renal stone burden.
Department of Urology, University of Wisconsin School of Medicine and Public Health, Madison WI, USA
Introduction: Hydrodissection with 5% dextrose in water or sterile water used to displace organs near the tumor prior to ablation can lead to difficulty in differentiating the fluid from the isodense surrounding structure. We describe our experience using 5% dextrose in water and 1% iodinated contrast to hydrodissect colon, pancreas and ureter prior to percutaneous renal cryoablation. Methods: We reviewed all percutaneous renal cryoablations performed at our institution from 2003-2010 for patients undergoing hydrodissection prior to ablation. Hydrodissection was performed with placement of a 20-gauge 15 cm introducer needle into the retroperitoneum followed by infusion of iodinated contrast solution between the kidney and the adjacent organ under CT guidance. Results: Of the 101 percutaneous renal cryoablations performed at our institution, 8 patients underwent hydrodissection using an iodinated contrast solution. Mean patient age was 62 years. Mean tumor size was 3.1±1.2cm. The organs displaced included colon(n=5), small bowel(n=1), pancreas(n=1) and in one case both the colon and ureter were displaced. The average displacement of all organs from the kidney was 2.7 cm(range 2.2-3.5cm). Mean volume of fluid for hydrodissection was 389 mL. Mean attenuation of hydrodissection fluid was 305 HU compared to a mean of 48 HU for the kidney. There were no complications and no injuries to any adjacent structures. No recurrences were noted on follow-up imaging with a mean follow-up of 5.4 months. Conclusions: The injection of iodinated contrast allows for safe mobilization and differentiation of adjacent organs from the renal tumor and parenchyma leading to potentially safer cryoablation.
Comparison of Radiographic and Pathologic Sizes of Renal Tumors in Patient Suitable for Robotic Partial Nephrectomy.
PURPOSE: Patients with renal masses may be selected for nephronsparing approach based on the tumor size. We compared the difference in size between kidney tumors seen on preoperative CT scan with the actual size of the removed specimen in patients presented to our institute.METHODS:A total of 68 patients underwent nephron sparing surgery for renal mass. The size of the mass, the location of the mass, bilateral masses, preexisting medical condition (diabetes mellitus, hypertension, renal impairment) were the criteria for selecting these patients for partial nephrectomy. The preoperative size of the mass measured by CT scan was compared to the post operative pathological actual size.RESULTS: The mean age of the patients was 62.4 years (ranging from 23 to 85). 42 patients underwent robotically assisted partial nephrectomy and the rest had traditional open partial nephrectomy. The mean radiologic size of the tumors was 3.8 cm (ranging from 2.2 to7), however the actual pathologic size was 3.4 cm (ranging from 1.8 - 6.3). There was statistically significant downsizing of the tumor from the radiologic estimate to the pathologic measurement (P<0.02). Factors such as age, gender, body mass index, tumor stage, tumor grade, surgical approach and tumor location were observed to have no significant impact on differences observed between radiographic and pathologic tumor size.CONCLUSIONS: The actual size of the kidney tumor is usually overestimated with the CT scan. This should be considered especially when considering patients for nephron sparing surgery.
Department of Urology, Hadassah University Medical Center, Jerusalem, Israel.
Evaluation of upper urinary tract obstruction is often performed by visual monitoring of sequential fluoroscopic imaging to estimate the clearance of contrast media from the renal pelvis. However, the diagnostic accuracy of this method is debated due to its subjectivity. The purpose of this study was to develop a computerized method for quantitative evaluation of the upper urinary tract clearance rate, using conventional fluoroscopic images. 25 patients after percutaneous nephrolithotomy (PCNL) were examined. All were considere non-obstructed. The patients underwent follow-up nephrostogram , and the quantitative information obtained was normalized by a phantom attached to the patients. The proportion of the amount of contrast media in the renal pelvis was analyzed, using densitometric methods. Clearance was measured using time dependence curves of the radio-density in the renal pelvis, in arbitrary units (a.u.) . Normal clearance showed, exponential decay, with a correlation coefficient of 0.94±0.02 for the regression fitting curve. The integrated radio-density of the contrast media was found to decrease at rate of 6±3 a.u. per minute, and the area of the contrast agent in the renal pelvis decreased by 5±2 a.u. per minute. It was concluded that this method could provide a quantitative estimation of the degree of upper urinary tract obstruction using only the initial measurement phase of a routine urological modality.
MP10: Urolithiasis 2
Departments of Radiology, Assaf Harofeh MC, Tel Aviv University, Israel.
Purpose: To view ureteral stones in 3 planes of measurement and look for a trend in stone location and shape.Materials and Methods: From 2007 to 2010, we collected all patients with acute renal colic and ureterolithiasis diagnosis on non-contrast CT (NCCT). The proximal vs. distal location of impaction, delineated by iliac vessels, was noted and stone dimensions were measured in 3 planes (axial, coronal and sagittal). The shape of the stone, as expressed by the maximal difference in dimension, was recorded as both an absolute value and as a relative change (percentage). Results: There were 137 patients average age 55 years. Seventy two stones were proximal and 65 distal. Comparing proximal stones vs. distal, no significant difference was found in age or side of impaction. Proximal stones were larger than distal for each plane (axial, p=0.01; coronal; p=0.0001; sagittal, p=0.00002). Increasing age correlated with larger stones for all planes (axial, r=0.23, p=0.006; coronal, r=0.22, p=0.008; sagittal, r=0.26, p=0.002). Multivariate analysis found both location and age independently correlated with increased size (p=0.0001 and p=0.003, respectively). Elongated stone shape was associated with proximal stones, as compared to distal stones (p=0.004 and p=0.004, respectively), and correlated with increasing age (r=0.18, p=0.04). Conclusion: Proximal stones are more likely to be larger and elongated compared to distal stones. Size of stone tends to increase with patient age. These observations are independent of each other.
Ball-Tip Holmium:Yag Optical Fiber
Introduction: We test the hypothesis that a ball-tipped fiber allows for safer passage through a ureteroscope in a deflected configuration.Methods: A 240 microm optical laser fiber with a ball-tip was passed through the channel of seven ureteroscopes. Measurements recorded: Pre- and post-visual assessment of the screen image, resistance to passing fiber in a 180 degree and maximally deflected configuration (Scale 1- 5), visualization of aiming beam, visualization of stone before and during ablation. Results: SCOPE OPTICS PRE POST RESISTANCE TO FIBER PASSAGE: 180 RESISTANCE TO FIBER PASSAGE: FULLY DEFLECTED Wolf Viper No damage No damage 2, 2, 2 2, 2, 2 Stryker U-500 N/A N/A 2, 4, 4 3, 4, 4Olympus URF-V #1 No damage No damage 1, 2, 2 2, 2, 2 Olympus URF-V #2 No damage No damage 3, 2, 2 2, 1, 2 Olympus URF-P5 No damage No damage 2, 2, 2 2, 2, 2 ACMI DUR-8 Elite No damage No damage 3, 4, 3 3, 4, 3 Storz Flex-X2 No damage No damage 1, 1, 1 1, 1, 1 Conclusion: The ball-tipped fiber passed through all scope channels but required greatest force in the two ureteroscopes that had active secondary deflection (DUR-8 Elite, U-500).

Metabolic Factors Associated with Adult Ureteropelvic Junction Obstruction (UPJO) and Nephrolithiasis
INTRODUCTION: There have been relatively few investigations regarding the etiology of kidney stone in adult UPJO. Both urinary stasis and metabolic abnormalities may be contributing factors. PURPOSE: To determine the incidence and to identify factors associated with stone disease and UPJO.METHODS: A retrospective chart review was performed on all patients (n=120) undergoing robotic pyeloplasty for UPJO from 2003-2010. RESULTS: 13.4% were identified with concurrent stone disease on the ipsilateral side of the UPJO. When the UPJO kidney did not have stones, the contralateral kidney had stones in 4.2% of cases. There were no cases of bilateral calculi. Patient characteristics are presented in Table 1. The predominant stone composition was calcium oxalate (66.7%). 24 hour urine collections were available for six patients; the two most common findings were hyperoxaluria (66.7%) and hypercalciuria (50%). Four patients developed recurrent stones. CONCLUSIONS: Patients with UPJO also have metabolic abnormalities predisposing them to nephrolithiasis and will likely benefit from metabolic evaluation and treatment.
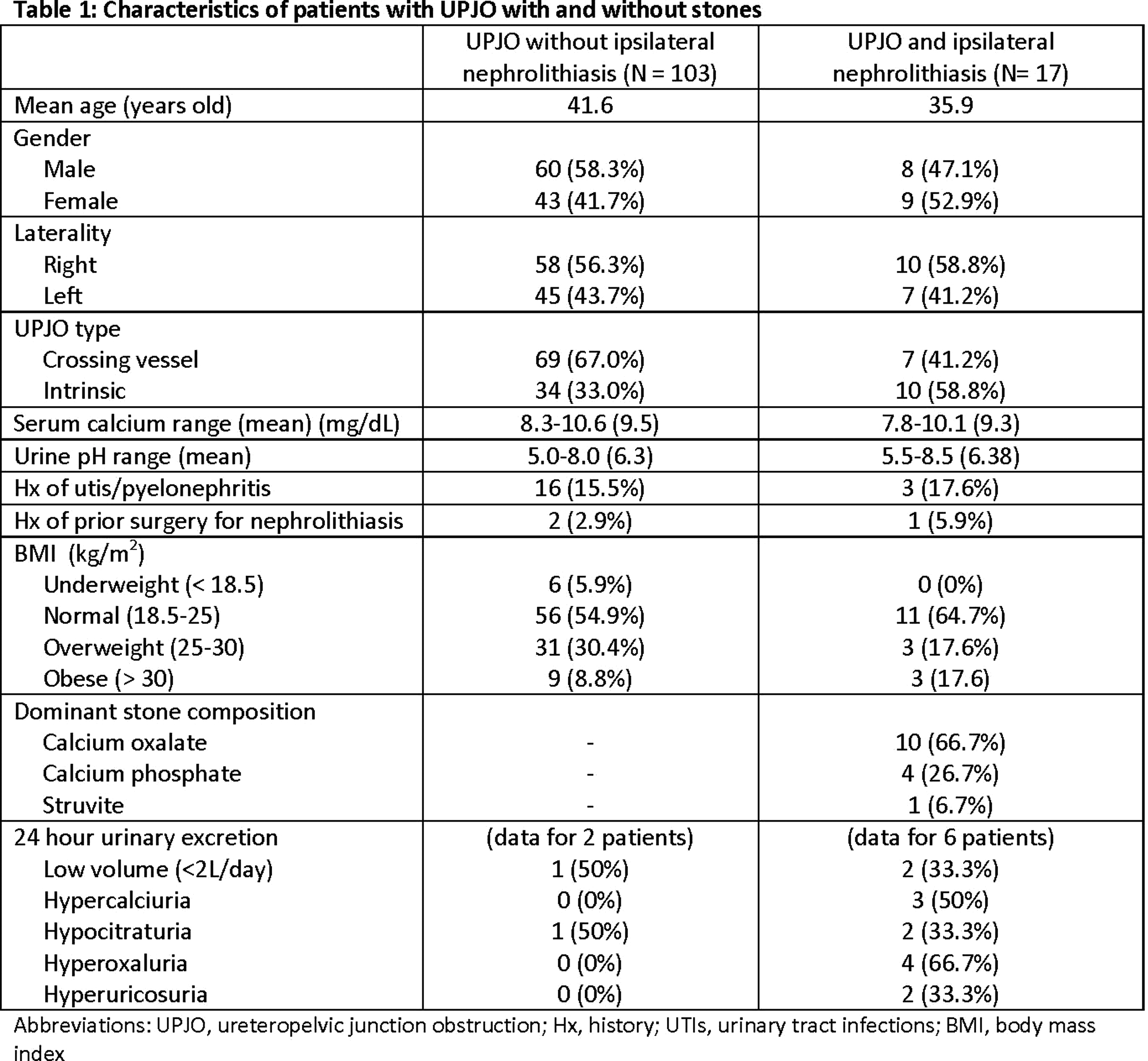
Clinical Course of Small Renal Stones Observed Over 5 Years
Purpose: Small renal stones(<5mm ) are asymptotic and out of the indication of surgical treatments. So the patients are recommended to visit the office when they have some symptons such as pain or hematuria. We aimed to assess the re-growth rate to discuss the need of regular visits. Materials and methods: 171 patients who had had small renal stones (<5mm ) were checked with ultrasonography more than 5 years later. We evaluated them to assess the re-growth rate and the diminish rate.Results These patients had 2.49 stones in average and the mean diameter of the stones was 3.24mm. 130 patients (76.0%) have experienced increase in number or size of the stones and 66 (38.6%) needed surgical treatments such as ESWL or TUL. On the other hand, the stones of only 22 patients have decreased or diminished.Conclusions: Due to the high re-growth rate, most of the patients who have small renal stones should be followed with regular visits.
James Buchanan Brady Urological Institute, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA
Objective: To compare clinical outcomes of patients with ureteral or renal stones treated with ureteroscopy(URS), shockwave lithotripsy(SWL, both HM3 and non-HM3) and percutaneous nephrolithotomy(PNL). Methods: A systematic literature search identified randomized controlled trials(RCTs) of treatment for distal ureteral stones (6 studies), proximal ureteral stones (4 studies) and renal stones (3 studies) published between 1995-2010. We used meta-analytic techniques to calculate overall stone free, retreatment, and complication rates.Results: Based on the RCTs evaluated, treatment of distal ureteral stones with semi-rigid URS showed a 55% greater probability (pooled relative risk(RR)=1.55; 95% CI 1.13-2.56) of being stone free at the initial assessment than treatment with SWL. Patients treated with semi-rigid URS were also less likely to require retreatment than those treated with SWL (non-HM3) (RR=0.14; 95% CI 0.08-0.23). The risk of complications was no different between the two treatment modalities. Of the four RCTs identified for proximal ureteral stones, only two studies evaluated flexible URS, and both focused specifically on the treatment of "large" stones 1.5cm or greater, limiting their clinical relevance. The degree of heterogeneity among the studies evaluating renal stones was so great that it precluded any meaningful comparisons. Conclusion: Semi-rigid URS is more efficacious than SWL for distal ureteral stones. There are no relevant RCTs for flexible URS treatment of proximal ureteral calculi of a size commonly encountered in the clinical setting. Taken all together, the comparative effectiveness of URS and SWL for proximal ureteral and renal calculi is poorly characterized, with few meaningful published studies.
James Buchanan Brady Urological Institute, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA
Objective: To evaluate the cost-effectiveness of treatment of ureteral/renal stones comparing ureteroscopy(URS), extra-corporeal shockwave lithotripsy(SWL), or percutaneous nephrolithotomy(PNL). Methods: A systematic literature search identified studies evaluating treatment for adult ureteral and renal stone patients published between 1994-2010. For inclusion, studies needed to report stone free rate(SFR) and cost for at least two therapies. Results: Nine studies were identified, with 3 comparing distal ureteral stones, 3 comparing proximal stones, 1 comparing any ureteral stone, and 2 comparing renal stones. Eight studies had an observational design, and 1 study was a data-synthesis using decision modeling techniques. For the studies comparing costs and SFR of URS versus SWL for distal ureteral stones, 2 found URS had higher stone free rates as well as lower costs; 1 study, which included both mid and distal ureteral stones, found URS also had greater SFR but costs were higher than with SWL. Two of the studies comparing URS versus SWL for proximal stones found URS had a higher SFR and lower costs; one study found URS had a higher SFR but also higher costs. A study evaluating any ureteral stone showed greater SFR and lower costs with URS relative to SWL. Studies evaluating SWL versus PNL and URS versus PNL for renal stones showed both higher costs and higher SFR with PNL.Conclusion: Despite the great heterogeneity and limited quality of available cost-effectiveness evaluations, the majority of studies demonstrated URS was more favorable than SWL for treatment of ureteral stones for both SFR and cost.
Urology Department, Charing Cross Hospital, Imperial College Healthcare NHS Trust, London, UK
Purpose:To show the effect of Tamsulosin in the treatment of lower ureteric stones (up to 6mm.)Materials & Methods: Prospective study for 3 years on adult patients presented to our unit with lower ureteric stones up to 6mm. (72 Pts.) (Group I) The result was compared with similar group of patients who presented during the previous 3 years (61Pts.) (Group II) Both groups had the same treatment regime, except using Tamsulosin in Group I. Patients were reviewed and if the stone persisted for more than 3 weeks; one ESWL session was given. ESWL was repeated if the stone or significant fragment persisted for more than another 3 weeks. If no clearance; Pts underwent ureteroscopy.Patients were assessed regarding; severity and frequency of pain, use of analgesics Stone expulsion, the need for ESWL or endoscopic intervention. Results(see Table) Conclusions:A conservative approach using Tamsulosin should be considered as the first option for non-obstructing distal ureteric stones up to 6mm. in sizeTamsulosin enhances the passage of small lower ureteric stones and reduces the time needed for stone expulsion and cut down intervention.

Efficacy of Tamsulosin 0.4 mg in Relieving of Double-J Stent-Related Symptoms: A Randomized Controlled Study
Objectives. To evaluate the efficacy of tamsulosin in improving double-J stent related symptom , and quality of life in patients with indwelling double-J ureteral stents.Methods. A total of 42 pateints, 15 men and 27 women with ureteral stents placement after ureteroscopy, percutaneous nephrolithotomy and balloon dilatation, were prospectively randomized into two groups. Group I included 21 patients who received 4 mg of tamsulosin, once daily for 4 weeks, and group II consisted of 21 patients as the control group . All patients completed International Prostatic Symptom Score (IPSS), quality of life and SF-36 questionnaires at 2 weeks and 4 weeks post double-J stent placement.Results. Of IPSS, the irritative symptom at 2 weeks was 5.48 and 7.81 for group I and group II, respectively (P=0.044). At 4 weeks the irritative symptom was significantly less in group I, P<0.001. At 2 weeks and 4 weeks, obstructive symptom were significantly less in group I (P<0.001, P=0.003, respectively). Of 8 domains of SF-36, role limitation due to physical health and bodily pain were significantly better in group I (tamsulosin group) at 2 weeks and 4 weeks. General health was significantly better in group I at 2 weeks. No serious side effect of tamsulosin was found in all patients of Group I.Conclusion. Tamsulosin improved both subset of stent-related urinary symptoms, as irritative and obstructive symptoms, and quality of life in patients who were inserted wih ureteral stent without increasing of side effect.
Is Routine Post-Operation Double-J Stent Needed After Percutaneous Nephrolithotomy?
INTRODUCTION AND OBJECTIVES: The percutaneous nephrolithotomy may leave small stone particle causing ureteral obstruction and cause renal bleeding. Doube-J stent insertion may reduce this complication at th end of procedure. The objective this study is usefulness or harmness of dougle-J stent.
METHODS:
From May 2010l to July 2011, 36 cases with kidney stones degerent in size & locations, were perated by PNL with double-J stent (gourp1) or without double-J stent (gourp2). Group 1 consists of 12 cases, 8 male and 4 female. Group 2 consists of 24 cases, 16 male and 8 female. Both groups compared from the point of post PNL complications, without using tissue sealants or tract cauterization.
RESULTS:
We achieved stone free rate in 33 patients (91.7%) and residual stone in 3 patients (8.3%) took two ESWL and one observation. Post PNL complication with double-J stent of hematuria more than 48hrs 3 cases (25%), leakage or urine 2 cases (16.7%). As regard more in Group 2 without double-J stent, pericathete urine leakage in 8 cases (33.3%), hematuria more than 48hrs 1 cases (4.2%).
CONCLUSIONS:
Post PNL complications are reported everywhere with different incidence. Althouth PNL c double-J decrease the urine leakage and perinephric urinoma incidence, but persistent hematuria make hospital stay longer than without double-J gourp.
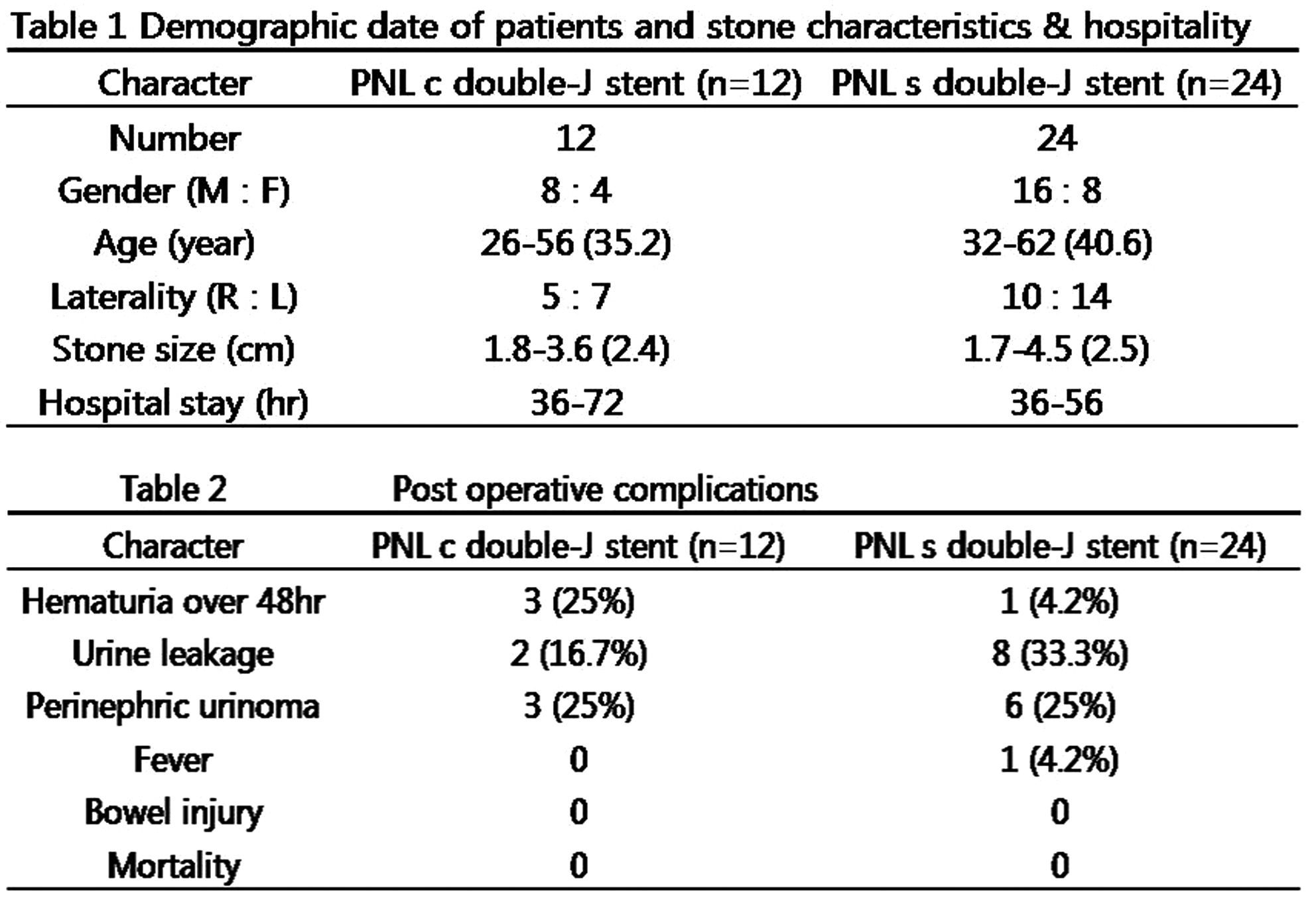
Efficacy of Tamsulosin in the Management of Lower Ureteral Stones: A Randomized Double-Blind Placebo-Controlled Study of 100 Patients
ABSTRACT WITHDRAWN
To Treat or Not to Treat: The Randalls Plaque Dilemma
Purpose:While Randalls Plaque was initially identified over 60 years ago, it is still largely unknown whether there is any benefit to endoscopic removal of these plaques in patients with flank pain. We speculated that these plaques might contribute to flank pain via obstruction at the microtubule (collecting duct) level.Materials and Methods:We retrospectively reviewed the kidney stone database of a single pediatric and adult urologist to identify patients who were endoscopically treated for Randalls Plaque in the absence of free urinary calculi between July 2007 and January 2011. Success was defined as the patients being pain free upon last follow up. Results:Among 175 patients who had endoscopic treatment for nephrolithiasis, there were 17 procedures to treat Randalls plaque. Ureteroscopic laser lithotripsy of Randalls plaque in the absence of free urinary calculi was performed 12 times in 10 patients, including 8 unilateral and 2 bilateral procedures. Mean±SD patient age was 23±10 years. Five patients (50%) were pain free at 11±8 months. Conclusions: Endoscopic treatment of Randalls Plaques may be offered to symptomatic stone patients as a treatment modality. Patients should be counseled on the 50% success rate in this clinical scenario. Long-term studies are needed to determine the duration of such benefit.
Renal Deterioration Index: Prognostic Indicator for Post Treatment Outcome of Obstructive Urolithiasis.
Background: Patients presenting with varying severity of obstructive urolithiasis behave differently after the treatment. Some recover while others progress to CKD V.Objective: To objectively quantify which categories of patient would progress to renal failure following treatment for obstructive urolithiasis. Material and methods: A prospective analysis of 167 patients with renal failure due to bilateral nephrolithiasis who were treated and subsequently followed for at least 1 year was done. All patient had pre-operative placement of percutaneous nephrostomy tube for at least 5 day prior to urolithiasis treatment. Multiple logistic regression analysis of affecting parameters such as age, hemoglobin, serum bicarbonate, urine culture, combined maximum cortical width and GFR at presentation, co-morbidity and GFR at 5days post bilateral PCN was done. A Renal deterioration index (RDI) was constructed based on scores assigned to varying severity of multivariate significant factors. Results: 48(28.7%) patients progressed to CKD stage V at 1 year follow up. Combined cortical width (p<0.001), proteinuria (p=0.009), positive urine culture (p=0.0036) and GFR at 5 days post bilateral PCN (p=0.03) were statistically significant factors affecting renal deterioration on multi-variate analysis. RDI has high sensitivity, specificity, positive and negative predictive value (AUR=0.924) for predicting renal functional outcome. Combining these parameters in a prediction table yielded RDI score more than 12 being associated with high odds risk of renal deterioration.Conclusion: RDI more than 12 is associated with renal deterioration after appropriate treatment of bilateral obstructive urolithiasis.
The Role of Flexible Cystoscopy in Laparoscopic Stone Surgery- A Single Surgeon Experience
Purpose: To investigate the usefulness of flexible cystoscopy in performing laparoscopic stone surgery of a single surgeon experienceMethods: A retrospective analysis was performed in 71 patients with complex renal stones or large and impacted proximal ureter stones. Patients underwent laparoscopic pyelo- or ureterolithotomies with or without concomitant calyceal stone removal by using flexible cystoscopy. Operative success was defined as no residual stone in the intravenous pyelogram at 12 weeks postoperatively. Surgical outcomes and significant predictors in the determination of operative success were analyzed.Results: Mean age was 54.7±13.7 years, 53 males (74.6%) and 18 females (25.4%) were included. Mean maximal size of stones was 19.4±9.4 mm. Mean operative time was 139.0±63.7 min. Stones were completely removed in 61 cases (85.9%) and no further ancillary treatment was needed to remove the residual stones in 7 cases (9.9%) because they were too small to be removed. The risk of residual stones was higher during surgery for complex renal stones than ureter stones with borderline significance (OR=5.4, p=0.086). Multivariate analysis showed that complex renal stones had a higher risk of the presence of residual stones than ureter stones and that the use of flexible cystoscopy can reduce the risk of the residual stones.Conclusions: The use of flexible cystoscopy was more useful in the patients with complex renal stones during performing laparoscopic stone surgery to maximize stone clearance rates.
Initial Experience with Laparoendoscopic Single-Sitenephrolithotomy for Caliceal Diverticular Calculi
Introduction: Although percutaneous nephrolithotmy is a standard treatment for caliceal diverticular calculi, laparoscopic nephrolithotomy is accepted as an alternative for selected cases. However, there is few data for laparoendoscopic single site nephrolithotomy (LESS-LN). Purpose: We described our initial experience with LESS-NL for caliceal diverticular calculi.Materials and Methods: Seven patients who underwent LESS-NL for caliceal diverticular calculi were evaluated. Five of them were performed by transumbilical LESS and 2 by retroperitoneal LESS. Additional 2mm trocar was used in 3 cases. Intraoperative ultrasould was used (4 cases) and the mean warm ischemic time was 35 mins (15-29) in 3 cases. In all cases, noncontrast computerized tomography was performed on postoperative day 1. Complications according to modified Clavien-Dindo classification were assessed. Results: The median patient age was 52 years (31-64). The median size of diverticulum was 26mm (17-58) and the median thickness of thinnest diverticular wall was 2.6mm (1.1-7.9).The perioperative outcomes were shown in Table 1. There were 2 cases of grade I complications (self-limiting fever) and no solid organ injury, urinary leakage, and perirenal hematoma .Conclusions: In our initial series, LESS-NL was performed safely for calyceal diverticular calculi. LESS-NL seems to be considered as an alternative to conventional laparoscopic nephrolithotomy.

MP11: Robotic/Lap Upper urinary Tract 3 (donor nephrectomy)
Long Term Graft Function in a Randomized Clinical Trial Comparing Laparoscopic Versus Open Donor Nephrectomy.
Objective: To evaluate and compare long term graft and recipient patient survival in kidney transplantation from LDN with ODN.Patients and method: The original study, including 100 cases of LDN and 100 cases of ODN was performed between July 2001 and September 2003. Median follow up of recipients in this study was 6.4 years (1-9.3 years: SD=2.6). 156 patients had follow-up greater than 5 years. The present study is a longer follow up of the previous randomized clinical trial (RCT), comparing patient and graft survival in recipients of LDN and ODN.Results : The mean duration of kidney warm ischemia time (WIT) was 8.7 min for LDN and 1.8 min for ODN. There were no significant difference in 5 year graft survival in LDN and ODN group (89.5% and 84.3% respectively; P=0.96). Also there were no differences in the occurrence of delayed graft function (DGF) in LDN and ODN group (8 and 11 patients, respectively P=0.135). There was a significant difference in 5 year graft survival between recipients with history of DGF and those without DGF (63.2% and 89.7%, respectively P=0.04). Despite Longer WIT in LDN (8.69 vs 1.87, p=0.0001), WIT did not reflect in graft outcome in long term follow up.Conclusion: DGF leads to worse graft outcome, both in LDN and ODN with no difference in either group. There is no relationship between WIT up to 17 min and long term graft outcome.
Impact of Right Nephrectomy on Long-Term Outcomes in Retroperitoneoscopic Live Donor Nephrectomy.
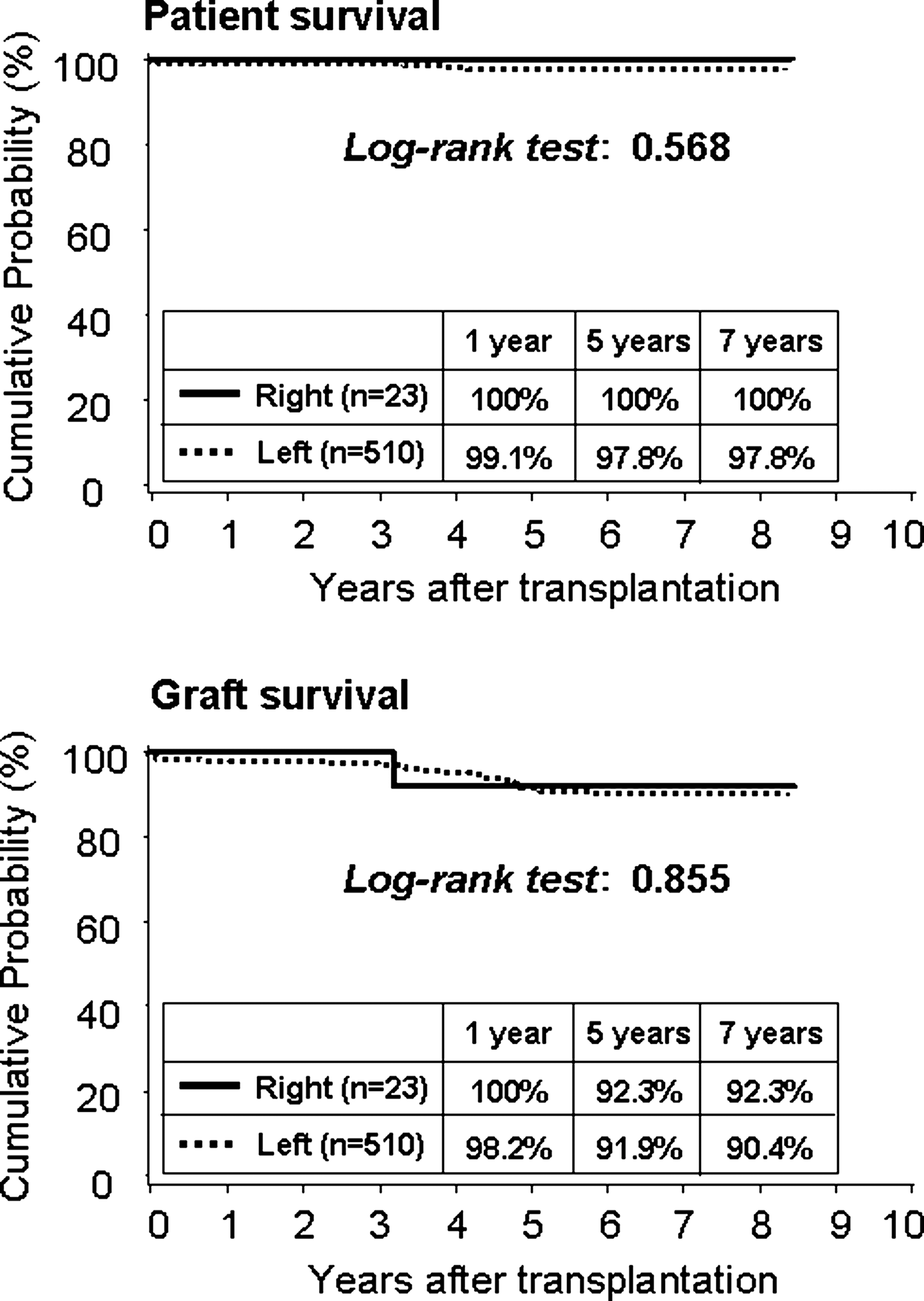
Learning Curve of Retroperitoneal Laparoscopic Live Donor Nephrectomy
Introduction: The learning curve period for RPLDN is still unclear because of the limited sample in the published studies.Objective: To evaluate the efficacy and explore the learning curve of our modified retroperitoneoscopic live donor nephrectomy.Methods: From December 2003 to June 2010, 158 consecutive retroperitoneoscopic live donor nephrectomies were carried out at our institution. All the donors who underwent RPLDN were separated into 4 groups in consecutive sequence to explore a learning curve. Group 1-3 were composed of consecutive 40 cases respectively and group 4 the last 38 cases. The renal artery and vein were controlled with two plastic locking clips at proximal ends.Results: The mean operation times were 160.5, 116.9, 101.4 and 100.5 minutes in group 1-4( group 1 vs group 2, 3 or 4, P less than 0.01 ). The estimated blood losses were 88.8, 73.0, 69.3 and 40.3ml in group 1-4( group 1 vs group 4, P less than 0.01). Post-operative hospital stays were 7.8, 6.9, 6.6 and 5.2 days in group 1-4( group 1 vs group 4, P less than 0.05 ). 8 donors and 7 grafts suffered from complications. Complication rates were 22.5%, 7.5%, 5.0% and 2.6% in group 1-4(group 1 vs group 3 and 4, p less than 0.05). Postoperative pain management and postoperative verse preoperative renal function changes of renal donors and recipients. Conclusion: Our modified retroperitoneoscopic live donor nephrectomy could be a safe and efficient alternative with a learning curve of about 40 cases.
Comparison of Renal Function Following Donor Nephrectomy Versus Radical Nephrectomy for Renal Tumor
Abstract Withdrawn
Removing the Smaller Kidney may Aid Early Renal Recovery in Laparoscopic Donors with Minimal Effect on Recipient Outcomes.
Introduction: The ideal kidney donation maximizes recipient kidney function without detriment to donor renal function.Purpose: To determine the impact of selecting the smaller kidney on laparoscopic donor and recipient renal function.Methods: Consecutive laparoscopic donors and recipients from 2002-2011 were reviewed. Volume measurement on CT began in October 2007. Discrepancies>5% prompted removal of the smaller kidney. Donor and recipient outcomes prior to volume selection (group 1) were compared to those selected by volume (group 2). Results: 149 donations in group 1 were compared to 102 in group 2. In Group 2, 63 (62.4%) had significant size discrepancy (median difference: 23ml, IQR=12.5). Median donor renal function for groups 1 and 2 were 57.4 (IQR=14.7) versus 60.3ml/min/1.73m2 (IQR=17.2), and 59.4 (IQR=16.1) versus 63.2ml/min/1.73m2 (IQR=19.9), at 1mo (p=0.012) and>3mo (p=0.115). In group 1, 38/71 (53.5%) at>3mo had renal function<60ml/min/1.73m2, compared to 21/56 (37.5%) in group 2, p=0.072. When<47.5% total renal volume was removed, median renal function at 1mo was 64.5 (IQR=19.2) versus 60.2ml/min/1.73m2 for larger proportions (p=0.394). Median recipient renal function at 3mo was 52.1 (IQR=36.3) and 57.6mlmin/1.73m22 (IQR=29.0) for groups 1 and 2, p=0.140. Postoperative oliguria occurred in 8/149 (5.4%) in group 1 and 3/102 (2.9%) in group 2, p=0.338. At last follow-up, 85% Group 1 kidneys (median follow-up: 34mo) and 97% Group 2 (median follow-up: 5mo) were functioning. Conclusion: Size discrepancy was common in donors. Donating the smaller kidney slightly improves early renal function of donors without impacting recipient outcomes.
Renal Transplantation, when Compared to Dialysis, Improves Recovery Following Laparoscopic Native Nephrectomy
Introduction: While renal tranplantation confers many benefits, it is unclear whether perioperative outcomes of laparoscopy are improved.Purpose: To compare laparoscopic nephrectomy in patients without end stage renal disease (control) to those on dialysis and those with functioning transplants. Methods: Consecutive laparoscopic nephrectomies performed by a single surgeon from 2003-2010 were categorized into three groups: control, dialysis, and transplant. Intraoperative and postoperative outcomes were compared using Kruskal-Walis and chi-square tests. Results: 240 cases were performed (147 control, 22 dialysis, 71 transplant). Median age was higher in the control (59.0y, IQR=22.0) than for dialysis (51.5y, IQR=17.4) and transplant patients (51.8y, IQR=12.9), p=0.001. Bilateral nephrectomies were performed in 1.4% control, 40.9% dialysis, and 49.3% transplant patients (p<0.001). Median operative time was 3h for each group, comparing only unilateral cases . Blood loss for the control, dialysis, and transplant groups was 50ml (IQR=70), 100ml (IQR=250), and 100ml (IQR=100), p<0.001. Intraoperative transfusions were required in 4.8% control, 9.1% dialysis, and 0 transplant patients (p=0.085). Intraoperative complications occurred in 8.8%, 9.1%, and 8.5% (p=0.994), while open conversion occurred in 0.7%, 9.1%, and 0, respectively. There were postoperative complications in 18.4% control, 45.5% dialysis, and 33.8% transplant patients (p=0.004). Grade 3 or higher complications were seen in 2.0% controls, 9.1% dialysis, and 1.4% transplant patients, p=0.001. Median hospital stay was 2.0d (IQR=1.0), 3.5 (IQR=5.3), and 3.0 (IQR=1.9) for control, dialysis, and transplant patients (p=0.003).Conclusion: Presence of renal failure added morbidity to laparoscopic nephrectomy, but postoperative recovery was improved following transplant relative to dialysis.
Department of Urology, Fujita Health University
Purpose: Laparoscopic donor nephrectomy (LDN) has been the preferred method for removal of kidney in living renal transplantation. Advantages for the donors included a quicker recovery, a shorter hospital stay and decreased postoperative pain compared to traditional open donor nephrectomy. We reviewed our 31 cases of LDN. Methods: Since June 2005, 31 cases of LDN performed hand-assisted retoroperitoneoscopic approach in our institution. The patients were placed in lateral decubitus position. The lower abdominal pararectal incision was made on nephectomy side. The Camera port and Two 12 mm ports were placed on middle, anterior and posterior axillary line, respectively. Results: Laparoscopic donor nephrectomy was carried out 31 patients including 10 males and 21 females. The median age of donors was 57 years. The side of nephrectomy was 30 cases on left and one on right. The median operating time, warm ischemic time and blood loss were 250 min, 4 min and 210 ml, respectively. All cases completed without open conversion or blood transfusion. The median length of stay after operation was 8 days. No cases developed complications after LDN. Immediate graft function occurred in all cases and the median lowest S-Cr in recipients was 1.1 mg/dl. Conclusions: Hand-assisted retroperitoneoscopy in living-donor nephrectomy appeared to be safe and lead to minimal invasion as well as excellent graft function.
Vascular Clips are Safe for Arterial and Venous Control in Laparoscopic Nephrectomy: Single Centre Experience with 1834 Laparoscopic Nephrectomies
Surgeon-Controlled Robotic Nephroureterectomy with Bladder Cuff Excision (RNUB) for Upper Tract Urothelial Carcinoma: Initial Experience in 20 Patients.
INTRODUCTION:Surgeon-Controlled Robotic Nephroureterectomy with Bladder Cuff Excision (RNUB)is a technique for treatment of upper tract urothelial cancer that offers advantages of minimally invasive surgery without the need for concomitant cystoscopic manipulation. However there is paucity of literature on the oncological efficacy and perioperative morbidity of this procedure. PURPOSE:To report our experience with RNUB in our first 20 consecutive patients with regards to peri-operative morbidty and oncologic outcomes.MATERIALS & METHODS:An institutional approved prospective database was reviewed to identify patients who underwent RNUB between 2008 and 2010. Patient demographics, imaging, operative data, pathologic results, complications and follow-up data were reviewed. RESULTS:There were 6 women and 14 men with ages 51-87 who underwent RNUB. A transperitoneal approach using a four arm robot was utilized in all cases without changing patient position or re-docking. Median OR time was 206 minutes, blood loss was 100 ml, and hospital stay was 2 days. There were no immediate perioperative complications. Retroperitoneal lymph node dissection was additionally performed in 10 patients with median removal of 9 lymph nodes. Follow up ranged from 4-29 months with bladder cancer recurrence in 4 patients, 3 of which were low stage and managed transurethrally while 1 patient progressed to muscle-invasive disease managed with robotic cystectomy. One patient developed metastatic disease to the abdominal wall treated with adjuvant chemotherapy. CONCLUSIONS:RNUB is a safe and clinically viable technique for managing upper tract urothelial carcinoma. As with any new oncologic procedure, longer term outcomes are necessary to verify durable efficacy.
Endoscopic Circumferential Mobilisation of Distal Ureter in Robot Assisted Laparoscopic Nephroureterectomy: A Safe Option
Introduction: There have been concerns in the literature regarding the oncological safety of the traditional "rip and pluck" technique for radical nephroureterectomy. The advantages that it offered in decreasing surgical insult had to be balanced against the risk of local tumour recurrence and seeding of tumour cells from the urinary tract into the operative field. Purpose: To evaluate the oncological safety of adoption of the principles of this technique using robot assisted laparoscopic nephroureterectomy. Materials and Methods: Our technique of robot assisted laparoscopic nephroureterectomy involved a four-port dual positioning system. Post operatively patients were recruited into ODMIT-C or received single dose intravesical Mitomicin upon catheter removal on day 10. Data on 46 patients was collected prospectively with follow up of up to 5.5 years (median 36 months). Results: Thirty-one patients had histologically confirmed Transitional Cell Carcinoma (TCC) of which 16 were Stage pT3. There was one case that developed recurrence along the surgical tract. Five patients developed subsequent bladder tumours. Four patients subsequently died from metastatic TCC. There was 16% intravesical recurrence rate compared with 17% reported from ODMIT-C. There was a 3% local recurrence rate overall and a 75% 3 year survival for Stage T3 disease. Conclusion: Endoscopic circumferential mobilisation of distal ureter in robot assisted laparoscopic nephroureterectomy is oncologically safe and has similar outcomes when compared to series describing formal open excision of the ureteric orifice.
Comparative Outcomes Following Retroperitoneoscopic Bilateral verses Unilateral Nephroureterectomy for de Novo Upper Tract Urothelial Carcinoma after Renal Transplantation
Introduction:De novo malignancies are long term complications for organ transplant recipients.De novo urothelial carcinoma may lead to deaths of recipients with a functioning allograft. Objective: To present the treatment strategies and pathological outcomes of de novo UT-UC after renal transplantation.Methods:Thirty-one renal transplant recipients underwent retroperitoneoscopic bilateral or unilateral nephroureterectomy for de novo UT-UC after renal transplantation at our institution from June 2002 to December 2009. They were separated into two groups: Group 1 was consisted of 15 patients who underwent unilateral nephroureterectomy with ipsilateral bladder cuff resection and Group 2 was consisted of 16 patients who underwent simultaneous or subsequent nephroureterectomy with bilateral bladder cuffs resection. Results:The mean follow-up was 25.5 months in all, 22.8 months in Group 1 and 28.1 months in Group 2. Mean size of tumors in Group 1 was significantly larger than Group 2 (p=0.008). Mean operative time in Group 2 was significantly longer than Group 1 (p=0.002). Concomitant bladder tumors were found in 9 patients preoperatively. The median survival time in Group 1 was 22.3 months, whereas longer than 50 months in Group 2.Goup 2 showed better prognosis than Group 1 in overall survival(p=0.026). Conclusions:Retroperitoneoscopic bilateral nephroureterectomy was associated with better overall survival compared with unilateral nephroureterectomy. It is recommended that patients with invasive tumor (stage greater than T2, or node greater than N1) should be treated with bilateral nephroureterectomy for de novo UTUC after renal transplantation even if there was no evidence of bilateral de novo UTUC.
Comparative Study after Retroperitoneal Laparoscopic Radical Nephroureterectomy with Various Forms of Bladder Cuff Control: Single-Center Experience with 135 Cases
Introduction: The management of the distal ureter and ipsilateral bladder cuff remains controversial and challenging in retroperitoneoscopic radical nephroureterectomy.Purpose: We compare results following retroperitoneal laparoscopic nephroureterctomy for upper tract urothelial carcinoma using 3 forms of bladder cuff control.Methods: 135 patients with upper tract urothelial carcinoma underwent retroperitoneal laparoscopic nephroureterectomy between December 2002 and June 2010. Group A (n49): open iliac dissection with specimen retrieval from this original incision; Group B (n35): transurethral resection of bladder cuff with retrieval from the iliac incision and Group C (n51): transurethral resection of bladder cuff with retrieval from the lumbar incision (modified “pluck” technique).Results: The mean age was 64.5 years. Median followup was 36 months. Median survival time of Group A 211; C was 39, 34 and 32 months, while there was no difference between these three groups. Recurrence developed in 23% and 6%of cases in the bladder at a median of 6 months and retroperitoneum at 9 months. Overall survival was associated with bladder recurrence (p 0.03), upper tract urothelial carcinoma stage (p 0.01) and lymph node involvement (p 0.04). But overall survival was not associated with bladder cuff excision method (p 0.09).Conclusions: With enough experience, either open dissection or transurethral resection of distal ureter and bladder cuff is good alternative.
Department of Urology, University Hospital, Plzen, Czech Republic
Introduction: We present complete laparoscopic nephroureterectomy (CLNUE) with intravesical lockable clip (WILC).Materials, methods: 1/2010-5/2011, 12 patients were indicated to CLNUE-WILC. First step is transurethral excision of ureterovesical junction with Collin knife deeply to the paravesical fat tissue. From the suprapubic region, 5 mm port is introduced in the urinary bladder. Stump of the ureter is grasped with biopsy forceps and on the end of ureter Hem-o-lok clip size ML (applicator 5mm). Patient is rotated to the flank position and standard laparoscopic nephrectomy is performed. Only ureter is not divided and it is liberated completely. Clip on the distal ureter if proof of completion of ureterectomy. In one more case, endoscopic phase was followed by translumbal NUE (not included in study).Results: The mean time was 156 (115-200) min, blood loss 100(0-200) ml. In four cases (33percentage) application of clip failed and CLNUE were finished with non-occluded ureter. There was only one complication: one patient died for heart failure in day of operation. The mean hospital stay was 8.7 (6-14) days. Follow-up is known in all patients - mean 8.6(1-17) months. Conclusion: CLNUE is fast and safe surgery. Disadvantages are following: need of changing of position, two method (endoscopy and laparoscopy), risk of inability to apply clip, unclosed defect of urinary bladder. In spite of these facts, we continue using this method. We hope the failing of methods was due to insufficient experience. Endoscopic phase can be followed with open NUE as well.Work supported by MSM0021620819.
Long-term Results of Retroperitoneoscopic Nephroureterectomy for T2 Upper Urinary Tract Transitional Cell Carcinoma in China
Introduction: For Ta or T1 Upper Urinary Tract Transitional Cell Carcinoma(UTCC), retroperitoneoscopic nephroureterectomy (RNU) may be a overtreatment. Open nephroureterectomy (ONU) usually performed on T3 or T4 UTCC. Objective: To compare the long-term clinical outcomes of RNU and ONU for T2 UTCC. Methods: Clinical data on 46 patients who underwent RNU were retrospectively compared with those on 51 who underwent ONU for upper urinary tract transitional cell carcinoma. Results: There is no significant difference in the operation time, but the intraoperative estimated blood loss and postoperative hospital stay in the RNU group showed significant advantages. The median follow-up period was 25.6 months.The 3-yr overall survival rate and 3-yr disease special survival rate in the RNU group was 63.8% and 81.7%, respectively. In the ONU group, the 3-yr overall survival rate and 3-yr disease special survival rate was 72.9% and 89.3%, there is no difference between the two groups. The 3-yr recurrence free survival rate in the RNU group was 65.7%, and 70.6% in the ONU group(p>0.05). The 3-yr intravesical recurrence free survival rate was 76.2% and 81.1% in the two groups, respectively, and no difference was observed. Conclusion: Compared with open surgery, retroperitoneoscopic nephroureterectomy for T2 is a safe, minimally invasive and effective procedure. The two modes of operation share the same long-term result.
Matched Comparison of Robotic versus Laparoscopic Nephroureterectomy: A Single Institution Experience
Introduction: Robotics has diffused rapidly in urologic oncology, and its role for prostatectomy is well established. The utility of robotic management of upper tract urothelial carcinoma (UTUC) has yet to be proven. Purpose: We compare our institution's initial robotic-assisted nephroureterectomy (RAN) experience with a well-established history of performing hand-assisted laparoscopic nephroureterectomy (HLN) to treat UTUC.Methods: We analyzed patients via a minimally-invasive renal surgery database. Patients (n=20) who underwent RAN from 4/2009 to 4/2011 were matched by tumor stage and age (+/- 10 years) to those who underwent HLN. Results: Mean operative time (300 v. 249 minutes) and estimated blood loss (380 v. 227 ml) were significantly higher with RAN than HLN, with no need for transfusion and no difference in perioperative complications. Lymph node dissection was performed more frequently with RAN (60% v. 25%), with the average node count being significantly greater (9.5 v. 4.2). After a mean follow up of 7.2 months for RAN and 19.9 months for HLN, no significant difference was seen in the rate of bladder (31% v. 26%), distant (25% v. 20%), or time to recurrence (8 months v. 18 months). Conclusion: Our RAN experience is associated with higher operative time and blood loss which may be explained by our more frequent use of node dissection, robot repositioning, and/or initial learning curve. Lymph node dissection was more frequently performed with greater average node counts with RAN, reflecting our historic HLN practice pattern. Our initial experience with RAN is encouraging but requires further evaluation.
Robotic Nephroureterectomy: A Valid Option for the Management of Upper Urinary Tract Transitional Cell Carcinoma
Introduction: Nephroureterectomy is the gold standard for management of upper urinary TCC. Laparoscopic and Robot Assisted approaches have been have been the mainstay in some specialized centres. Purpose: To evaluate our experience and outcomes in the Robotic Assisted approach for nephroureterectomy. Patients and Methods: All procedures were initiated with a cystoscop. Using the Collins wire knife TUR electrode we endoscopically release the ureteric opening from the bladder till the extravesical fat is visualized. All patients are then positioned such that a transperitoneal approach to the kidney is achieved. The robot is then docked followed by dissection of the ureter down to the extravesical fat disconnecting it from the bladder. The bladder defect is secured with extravesical closure. Perioperative and oncological outcomes were prospectively collected.Results: Fifteen patients were treated using this approach in our centre since March 2010. Mean age 65.2 years, postoperative pathology proved TCC in 13 patients (T1a-T3) and two patients diagnosed with RCC. Average operative time 221.5 min and 26 mls mean blood loss; none of the patients were converted to open. Average post operative stay was 2.4 days with median Clavien Dindo classification of 1. Early follow up figures revealed no recurrence. Conclusion: Robot Assisted nephroureterctomy is techniqually feasible with early recovery and hospital discharge. It provides comparable postoperative and oncological outcomes at short term follow up to the standard open technique.
MP12: LESS/NOTES 3
STILUS Academic Research Group (SARG). London. UK
Introduction: Laparoendoscopic single-site surgery (LESS) has been increasingly used in the management of a variety of urological conditions. Purpose: To decipher the current global outcomes of LESS in urology by means a systematic review of literature. Material & Methods: We searched MEDLINE, PubMed and the Cochrane Library from January 2006 to June 2011 for results of LESS in Urology. Inclusion criteria were all English language articles reporting on more than 10 patients. Data was extracted on the outcomes and complications reported in the literature. Results: A total of 10 studies (2 RCT, 5 prospective and 3 retrospective) reported on 1601 patients. The procedures included simple nephrectomy(231), radical nephrectomy(216), partial nephrectomy(220), donor nephrectomy(129), cyst decortications(145), pyeloplasty(118), adreanalectomy(62), nephro-ureterectomy(33), ureterolithotomy(62), varicocoelectomy(48) and other procedures(337). Of these (247, 15% were done robotically. The mean age was 49 years (1-89 years) with a male:female ratio of 718:708. The mean BMI, operating time, blood loss and hospital stay was 25 (17-52), 180 min (60-440 min), 119 ml (25-1850 ml) and 3 days (1-22 days) respectively. Conversion to open surgery and conventional laparoscopic surgery was in 24 (1.4%) and 225 (14%) cases respectively. There were 54 (3.3%) intra-op complications (Vascular injury n=26, Bowel injury n=10, Splenic injury n=4, Diaphragmatic injury n=7 and others n=7). There were 140 (8.7%) post-operative complications of which 33 (23%) were Clavien grade 3 or 4. Conclusion: LESS is feasible and safe with outcomes and complications similar to conventional laparoscopic urological surgery.
Department of Surgery, Taipei City Hospital zhongxiao branch, Taipei, Taiwan
Introduction: Peritoneal dialysis is one of the treatment options for patients with end stage renal disease. The success of peritoneal dialysis depends greatly on the adequate insertion of peritoneal dialysis catheter. Herein we report of 2-year experience in laparoendoscopic single site peritoneal dialysis catheter insertion.Patients and Methods: From November 2009 to June 2011, total 28 patients were enrolled into this study. All procedures were finished under laparoscopic guidance using one 10mm trocar or/with one additional 5 mm trocar via one periumbilical incision. The mean followup period was 15 months.Results: The mean operative time was 34 minutes (range 25 to 90 minutes). There were 6 patients received laparoscopic adhesionlysis concomitantly. The incidence of perioperative complication was 3.57% (1/28). There was no catheter outflow failure rate in our series. The incidence of conversion to hemodialysis due to peritonitis was 7.14% (2/28). The 6-month and 1-year catheter survival rate was 94% and 80% respectively. The incidence of catheter migration was 7.14% (2/28).Conclusion: Laparoendoscopic single site peritoneal dialysis catheter insertion is a safe and feasible technique with low complication rate and high 1-year catheter survival. A prospective large scale study is required for further elucidation regarding the long term outcome of this technique.
Application of a Novel Homemade Device in Transumbilical Laparoendoscopic Single-site Surgery: Single Center Experience
OBJECTIVES: Aim of this study is to evaluate the feasibility of a novel homemade single-port device and present a single center cumulative experience with LESS. METHODS: The clinical data of LESS performed from June 2010 to May 2011 in our hospital were analyzed retrospectively. Our homemade single-port equipment is composed of polycarbonate cone device and a 6F sterile surgical glove . The shape of the posterior outer edge is spiral, which can be fixed in the incision and will not be prone to prolapse from the incision. The thumb, middle, and ring fingers of the glove were implanted and fixed with 12mm,10mm and 5mm diameters trocar respectively. RESULTS: We have implemented our homemade single-port device for 14 cases of radical nephrectomy, 15 cases of modified radical cystectomy, 12 cases of renal cyst resection, 3 cases of non-functional kidney resection and one patients with adrenal cyst.. None was converted to traditional three-port procedures, but radical cystectomy and right nephrectomy need one or two trocar plus. There was no secondary bleeding, wound infection, intestinal obstruction, incision hernia and other severe postoperative complication. CONCLUSIONS: Our homemade single-site device offers the advantages as follows: it can be made simply and used repeatedly; no additional fees were charged for the device; trocar position can move freely without restrictions; different trocars can be replaced freely for different surgery; the outer edge of device is spiral which can be fixed into the incision.
Why Insisting on “Single Incision”? “Hybrid” use of Single-Site Apparatus in Laparoscopic Partial Nephrectomy- Change of Mind-Set.
Introduction: Very few urologists are able to routinely perform LESS partial nephrectomy (PN). Conventional laparoscopic PN (LPN) usually employs 4∼6 ports for a variety of instruments, with one of them finally extended to accommodate specimen extraction. We report a novel application of single-port apparatus for "Hybrid" LPN and LESS PN. Methods: Five patients with an organ-confined renal tumor underwent LESS LPN. The operation started by making a 3-4 cm vertical para-rectus incision around umbilicus, and a GelPoint (Applied Medical) apparatus was setup. A 30 degree laparoscope was inserted through a trocar at the GelPoint. Then two 5mm standard ports were inserted at ipsilateral subcostal margin and lateral abdominal wall as standard LPN; further assistant instruments for graspers, suction devices, application of temporary vascular clamps, insertion of suture materials and hemostatic bolters, LaproTye applications, and retrieval bag were carried through 2-3 ports mounted on the GelPoint. Specimen was removed through the GelPoint incision.Results: All operations were performed successfully without intraoperative complications or blood transfusion. No further port was created besides those 3 mentioned. Average EBL was 139 mL, and the median operative time was 229 minutes. Pathological examination revealed 4 renal cell carcinomas with negative margins, and 1 hemorrhagic cyst. No recurrence has occurred in median followup of 9 months.Conclusions: Applying a single-port apparatus to "hybridize" with standard LPN effectively reduced the total number of port wounds to 2 plus one small GelPoint incision while preserving the dexterity of standard LPN for excision and reconstruction.
Operative Outcomes Of Conventional Vs Single-Port Robot-Assisted Partial Nephrectomy For Renal Masses More Than 4 Centimeters.
IntroductionThe use of laparoscopic partial nephrectomy (LPN) for renal masses larger than 4cm is increasingly being practiced in centers with advanced laparoscopic expertise. Robot-assisted laparoscopic partial nephrectomy (RALPN) overcomes many of the technical hurdles of LPN. With experience, RALPN can be combined with novel single-port access technique to reduce wound site related complications while still achieving the benefits of renal preservation. Purpose:We compare the outcomes of RALPN for renal masses larger than 4.0 cm performed by conventional or single-port access techniques.Materials and Methods:Nineteen consecutive cases of single renal masses larger than 4.0cm were performed by a single surgeon. Seven (7) cases using conventional RALPN from November 2007 to March 2009 and 12 cases using single-port RALPN (SP-RALPN) from May 2009 to July 2010 were assessed. One case of SP-RALPN was converted to open partial nephrectomy due to technical difficulties. Operative outcomes of the successful cases were compared using the Mann-Whitney U and Chi-squared test.Results: (table)Conclusion:SP-RALPN is a feasible and novel evolution of conventional RALPN. The short-term oncologic and renal function outcomes are comparable between the two techniques. Its role is dependent on surgical expertise and long-term follow-up is needed to assess its viability.

Department of Urology, University of Patras, Greece
Introduction and Purpose: We report the experience of two academic institutions in single site urologic surgery (SPS).Methods: 101 patients were treated by single site laparoscopic surgery for various indications. The performed procedures included 42 nephrectomies (32 radical and 10 simple), 11 cyst deroofing, 14 pyeloplasties, 3 partial nephrectomies, 14 bladder diverticulectomies, 3 radical prostatectomies, 4 nephropexies and 10 TEP hernia repairs. The procedures were performed by the use of Triport/Quadport (Olympus, Germany), Endocone/X-cone (Karl Storz, Germany) and Gelport/Gelpoint (Applied Medical, USA) in combination with articulating, pre-bent and conventional laparoscopic instruments depending on the availability of the equipment. Perioperative data were prospectively collected. Postoperative pain, analgesic medication requirements, Convalescence time and return to duties period were also recorded.Results: Special selection of cases for the performance of SPS was not performed. The SPS cases represented a small portion (approximately 10%) of the total number of laparoscopic performed at the participating institutions. Conversion to open surgery never took place. An additional laparoscopic instrument was used in 42 cases. In 35 cases, a 3mm instrument was inserted while a 5mm trocar and instrument was used in 7 cases. These instruments were used for liver retraction in the right nephrectomy cases, for suturing in reconstructive procedures and for assistance in complications or difficult cases. Operative time ranged between 45min and 243min. Blood loss, postoperative pain and requirement for analgesia was minimal.Conclusion: SPS procedures are feasible, safe and could be performed on an extended scale representing significant portion of the urological laparoscopic surgery.
Department of Urology, University of Patras, Greece
Introduction: The conventional laparoscopic surgery is now paving way to the new technologies including robotic and Laparoscopic Single Site Surgery (LESS). Purpose: We present our updated experience on LESS Radical Nephrectomy (LESS-RN).Patients and methods: The data from patients undergoing LESS-RN in our two institutions was reviewed along with various clinical and pathological parameters. Results: Between 2008 and 2011, 42 LESS-RN were performed (right=22, left=20) with mean (range) age and BMI of 63.7(33-86)y and 25.1kg/m2 respectively. In addition to the instruments in the single port, one extra 3mm needle scopic instrument was required in 19 patients ( right=17, left=2).In three patients, two additional 5 mm trocars and instruments were required. None required open conversion. The recorded adverse events include one bowel injury (intraoperative closure without the need for stoma), one postoperative bleeding requiring blood transfusion, one prolonged ileus and one deep venous thrombosis. The resected specimens revealed pT1a (n=3), pT1b (n=33), pT2 (n=4) and pT3b (n=2) tumors. The finding of pT3b was incidental rather than planned procedure. None of the patients had positive margins.Conclusion: LESS-RN has proven to be feasible and safe. Beyond cosmesis, further advantages of this approach needs to addressed by randomised trials.
Robotic-Assisted Laparoscopic Repair of Ureteral Strictures and Iatrogenic Ureteral Injuries in 15 Consecutive Patients.
INTRODUCTION: Robotic surgery has become a well-established technique for addressing congenital UPJ obstructions, although few studies have reported its role in treating ureteral injuries or acquired strictures. PURPOSE: We review our experience with robotic-assisted laparoscopic reconstruction of the proximal, mid, and distal ureter. METHODS: We retrospectively reviewed records from patients who underwent robotic-assisted laparoscopic ureteral reconstructive surgery by a single surgeon over a 2-year period. Pyeloplasties (n=33) were excluded. RESULTS: 15 patients underwent robotic-assisted laparoscopic ureteral reconstruction. Mean age was 47.9 years and BMI was 32.4 (range: 22.7-44.3). 33.3% had undergone a previous repair by another surgeon. Indications included high-grade ureteral stricture (n=7: ureterolithiasis, chemo-radiation, congenital megaureter, tumors, and retroperitoneal hematoma), partial transection (n=3: hysterectomy and ureteroscopic avulsion), and complete transection/obstruction (n=5: gynecologic surgery, sigmoidectomy, and prostatectomy). Median delay after diagnosis was 4 months (0 days-4.75 years). Two occurred in the upper, three in the mid, and ten in the distal ureter. Procedures included: robotic ureteroureterostomy (n=5), ureteroneocystostomy (UNC; n=4; including a tailored reimplant), psoas-hitch UNC (n=5), and complicated ureterolysis (n=1). There were no intraoperative complications or open conversions. Mean operative time was 278.9 min, EBL was 151.4 ml and hospital stay was 3.2 days. Mean follow-up was 312 days. 93.3% continued to do well post-operatively, although one patient ultimately underwent a laparoscopic nephrectomy for a poorly-functioning kidney. CONCLUSIONS: The current series demonstrates the versatility, efficacy, and safety of the robotic approach for complex ureteral reconstructive surgeries.
Department of Urology, University of Patras, Greece
OBJECTIVE: To present the technique of hybrid NOTES (Natural Orifice Transluminal Endoscopic Surgery) Transvaginal nephrectomy. METHODS: 5 female patients were submitted to hybrid transvaginal nephrectomy for tumor (n=4) and non-functioning renal unit (n=1). The procedure was performed by Gelpoint (Applied Medical Resources Corporation, California, USA) or Endocone (Karl Storz, Tuttlingen, Germany) or Quadport (Advanced Surgical Concepts, Wicklow, Ireland) multi-instrument ports inserted through an umbilical and vaginal incision. A 30 degree lens extra long camera and combinations of conventional laparoscopic and pre-bent instruments were used. Specially designed extra-long pre-bent and straight instrumentation was found particularly useful for manipulations performed through the vagina. Several peri-operative parameters were recorded prospectively. RESULTS: Four patients underwent radical nephrectomy for tumors with an average diameter of 6.25cm (range 5.5-7.5cm). Average operative time was 128min (range 100-190min). Estimated blood loss ranged between 50 and 150ml (average 90ml). Intraoperative complications were not observed while postoperatively one of the patients suffered by fever of unknown origin treated with antibiotics. Average hospital stay was 3.4 days (range 3-5). Positive surgical margins were not detected in any of the malignant specimens. CONCLUSION: Hybrid NOTES transvaginal nephrectomy is a feasible and safe alternative to standard laparoscopic nephrectomy for selected patients. Several difficulties arising from limitations in current instrumentation have been addressed by the use of extra-long pre-bent instruments. However, larger clinical studies and careful patient selection are required.
Laparoendoscopic Single Site Surgery. Our Experience.
INTRODUCTION and OBJECTIVE: Laparoendoscopic single site (LESS) surgery has been developed and rapidly indicated for urological diseases. Nevertheless, LESS surgery is still recognized as a technically complex procedure, and only limited institutions reported some series of LESS surgery to date. We present our experience of LESS surgery, and discuss the feasibility of this technique. METHODS: Thirty patients underwent LESS surgery for urological disease in our institution. The single peri-umbilical incision and multiport technique was used for initial 7 cases. In the other 23 patients, the GelPort or SILS port was used as an access platform. The LESS surgeries included nephrectomy (n=3), radical nephrectomy (n=7), nephroureterectomy (n=6), donor nephrectomy (n=8), and adrenalectomy (n=6). The perioperative outcome of these 30 patients was evaluated retrospectively.RESULTS: The LESS surgery was successful in 29 patients, but only one patient, who underwent left radical nephrectomy, required open conversion and blood transfusion because of splenic injury. Perioperatively, there were no major complications or transfusion in other 29 cases. Median operative time was 148, 211, 470, 302 and 179 minutes, and blood loss was 55, 50, 470, 210 and 5 ml in nephrectomy, radical nephrectomy, nephroureterectomy, donor nephrectomy and adrenalectomy, respectively. Median warm ischemic time in donor nephrectomy was 3.9 min (range, 2.5 to 11.5). CONCLUSIONS: LESS procedure is suggested to be a feasible and safe technique for major urological disease in medium-scale hospital. Nevertheless, we cannot conclude the efficacy of this procedure, and the further evaluation of this technique is mandatory.
Safety and Technical Considerations of Laparoendoscopic Single Site (LESS) Live Donor Nephrectomy in a Small-volume Transplant Center
OBJECTIVES: To discuss how to perform LESS live donor nephrectomy (LDN) safely in a center with limited case number. Laparoscopic LDN is usually performed through a hand-assisted manner or a 3-port pure laparoscopic technique besides a retrieving peri-umbilical or Pfannenstiel incision.METHODS: The GelPort device was used as the LESS platform and setup at a 5 cm peri-umbilical midline incision. Three to 4 ports inserted through the gel-cap achieved triangulation to perform LESS-LDN. Before hilar vessels ligated with Endo TA staplers, an EndoCatch-II was inserted through gel-cap separately to bag the kidney and harvest longer pedicle. The kidney was removed through the LESS incision.RESULTS: LESS LDN was successfully performed in 10 patients without standard laparoscopic or open conversion. No extra instruments through separate wounds other than the LESS incision were used. The median operative time was 310 minutes with a median warm ischemia time of 3.5 minutes. Median hospital stay was 2 days and the median visual analog pain score was 4/10 at discharge and 2/10 at 2 weeks. All of them were back to original daily activities in 2 weeks post-operatively. None of the patients received transfusions perioperatively and none had peri-operative complications.CONCLUSIONS: LESS LDN using the GelPort device as the access platform offers the benefits of improved cosmesis over the standard laparoscopic donor nephrectomy, and provides an easy conversion potential in case of difficulty. Prospective randomized trials are needed to compare the postoperative pain levels and the degree of satisfaction.
Department of Urology, Akita University School of Medicine, Akita, Japan
Background: Laparo-Endoscopic Single-Site (LESS) surgeries may improve cosmesis of renal transplantation donors. However, this procedure requires utilization of the specialized instruments with adversity of the surgical technique which could be cause of increased morbidity. We performed a new procedure of LESS plus one trocar donor nephrectomy (LEPODN) in order to utilize only the standard instruments and achieve good cosmesis. Patients and Methods: From October 2010 to June 2011, a total of 11 donors of the living renal transplantation underwent LEPODN. Median age and preoperative creatinine clearance were 59 (38-76) and 109.7 mg/min (73.3-162.2). The GelPort® was loaded at a 5-6 cm para-rectus incision at a level of umbilicus. 12mm camera trocar, 12mm left-hand working trocar and 5mm assistant trocar were placed through the GelPort®. A subcostal 5 mm right-hand working trocar was additionally placed. Graft kidney was extracted by the GelPort® using the Endo Catch II Bag. 19Fr drain was placed at the 5 mm right-hand working trocar.Results: Median operative time, bleeding, and warm ischemic time were 231 minutes (162-285), 25 ml (0-191), and 255 seconds (140-498), respectively. Median one month postoperative serum creatinine concentration was 0.86 mg/dl (0.5-1.65). Delayed graft function due to postoperative heart failure was occurred in one patient. Conclusion: LEPODN was feasible and can be performed utilizing only the standard instruments with addition of subcostal 5 mm right-hand working trocar. LEPODN can be performed by the surgeons with experience of conventional urologic laparoscopic surgery, with minimum morbidity, good graft function and good cosmesis.
Exploring the Early Learning Curve of Laparoendoscopic Single-Site (LESS) Donor Nephrectomy: A Comparison to the Standard Multi-Site Laparoscopic Approach.
INTRODUCTION: Laparoendoscopic single-site (LESS) donor nephrectomy is gaining popularity as a means to harvest kidneys for transplantation, despite being technically more challenging than standard or hand-assisted laparoscopic donor nephrectomy. PURPOSE: We compare outcomes of patients undergoing standard laparoscopic and LESS donor nephrectomies in a single-surgeon series. METHODS: A retrospective analysis was performed based on medical records of patients undergoing standard laparoscopic and LESS donor nephrectomies from 2006-2011 by a single surgeon. RESULTS: 165 patients underwent donor nephrectomies, 109 via the standard laparoscopic approach and 56 via the LESS approach. 29.4% had multiple arteries in the standard laparoscopic group, versus 25% in the LESS group (p=0.557). There were no differences between groups regarding age, sex, or BMI. The mean extraction site size for the LESS group was 5.21cm, versus 7.44cm in the standard laparoscopic group (p<0.001), and mean estimated blood loss (EBL) was less in the LESS group (56.2ml vs. 6.3ml; p<0.001). Operative time, warm ischemia time, length of hospital stay, complication rates, and change in donor glomerular filtration rate did not differ between groups. CONCLUSIONS: This is a large single-surgeon series comparing perioperative outcomes of patients undergoing standard laparoscopic and LESS donor nephrectomies. The LESS approach was found to be safe and efficacious compared to the standard laparoscopic approach. Operative time for LESS was similar to standard laparoscopic surgery and did not change significantly over the first 55 cases. For surgeons experienced with standard laparoscopic donor surgery, transitioning to the LESS approach appears to have a relatively short learning curve.
Scott Department of Urology, Baylor College of Medicine, Houston, Texas, USA
INTRODUCTION: Multiple renal arteries can present a challenge for surgeons performing laparoscopic donor nephrectomy for renal transplantation. PURPOSE: We reviewed our experience with multiple renal arteries in patients undergoing standard laparoscopic (SL) and laparoendoscopic single-site (LESS) donor nephrectomy. MATERIALS AND METHODS: A retrospective analysis on medical records of patients undergoing SL and LESS donor nephrectomy from 2007-2011 by a single surgeon was performed. Corresponding recipient data was also analyzed. RESULTS: 153 patients underwent donor nephrectomy (98 SL, 55 LESS). Of these, 27.4% (n=42) had multiple renal arteries. 36 patients had two renal arteries (24 SL, 12 LESS), 4 had three renal arteries (2 SL, 2 LESS), and 2 had four renal arteries (2 SL). There was no significant difference in sex, BMI, estimated blood loss, or hospital length of stay, with regard to number of renal arteries. Surprisingly, operative time was not significantly extended by the presence of multiple renal arteries (p=0.69). Warm ischemia time (WIT) did increase slightly with greater numbers of renal arteries (1 artery-4.6min, 2 arteries-5.1min, 3 arteries-6.3min, and 4 arteries-7.0min). The number of donor renal arteries did not significantly affect conversion rates, intra-operative complication rates, post-operative changes in donor glomerular filtration rate (GFR), or recipient graft survival. CONCLUSIONS: Although multiple renal arteries were associated with slightly increased WIT, donor and recipient surgical outcomes were unaffected. Patients with multiple renal arteries should not be excluded from laparoscopic renal donation using either the SL or LESS approaches.
Prospective Randomized Controlled Trial of Laparoendoscopic Single-Site Versus Conventional Laparoscopic Radical Nephrectomy for Localized Renal Cell Carcinoma
Introduction: The safety and efficacy of LESS for renal cell carcinoma RCC has not been clearly demonstrated.Purpose: We aimed to present preliminary data from a prospective randomized controlled trial of LESS versus conventional laparoscopic radical nephrectomy (CLS) for localized RCC.Materials and methods: Patients with cT1-2 RCC were randomized to LESS (n=10) or CLS (n=10). Short-term outcomes assessed were surgical reults, postoperative pain, and quality of recovery measured by QoR-40.Results: No significant differences were observed in operative time (128.6 vs. 117.2 min, p=0.689), blood loss (95.0 vs. 80.5 ml, p=0.280), hospital stay (3.4 vs. 2.4 days, p=0.202), analgesics requirement (84.4 vs. 65.0 mg, p=0.747), and complication rate (37.5 vs. 30.0 %, p=1.000) between the LESS and CLS groups. Postoperative pain at postoperative day 1 (5.1 vs. 5.3, p=0.464), 2 (4.2 vs. 4.2, p=0.705), and 3 (3.6 vs. 3.5, p=1.000) was not different between two groups. Postoperative quality of recovery measured by QoR-40 scores was higher in the LESS group compared with the CLS group (173 vs. 146, p=0.037). In the LESS group, improved QoR was observed in the QoR-40 dimensions of emotional state (39.8 vs. 31.1, p=0.007), and pain (31.5 vs. 26.1, p=0.012), but, not in physical comfort (50.9 vs. 44.3, p=0.162), psychological support (31.4 vs. 26.6, p=0.061), and physical independence (19.9 vs. 17.7, p=0.448).Conclusions: Preliminary results from this prospective trial showed that LESS could be a safe and effective treatment option for localized RCC with equivalent surgical outcomes and improved postoperative quality of life compared with CLS.
MP13: Robotic/Lap Prostate 2
Department of Urology, Autonomous University of Barcelona, Hospital del Mar, Barcelona, Spain
Outcome of Inguinal Herniorrhaphy Performed During Robotic Assisted Radical Prostatectomy.
Introduction: Inguinal hernias are found in 5 to 33% of men who undergo a surgical treatment of prostate cancer. In order to avoid another procedure it can be treated simultaneously. Purpose: In this study, we review our experience of herniorraphy performed simultaneously with Robotic assisted laparoscopic radical prostatectomy (RALP).Materials and Methods: The records of all patients operated by RALP since November 2007(n=218) were scrutinized in order to depict simultaneous herniorraphy. Peri-operative features included hernia repair time, mean hospital stay as well as occurrence of short and long term complications linked to the repair (mesh infection, hernia recurrence) were assessed.Results: From November 2007 to June 2011, 218 RALP were performed at our institution. 25 patients (12 %) had simultaneously an inguinal hernia. Mean follow up was 23 (1-42) month. In 21 cases (84 %) the diagnosis was pre-operative, and in the 4 remaining (16 %) per-operative. Nineteen patients had a direct hernia, 4 an indirect hernia and 1 a mixed hernia. Mean hernia repair time was 24 (5-42) minutes. No differences were observed in terms of hospital stay in compare to the 193 RALP without. No complication related to the herniorrhaphy was encountered during hospital stay and none of the 25 patients with hernia repair reported inguinal or scrotal pain. One recurrence (4%) was diagnosed on clinical examination 10 month after RALP and needed a secondary open repair.Conclusion: Inguinal herniorrhaphy during RALP is feasible, efficient and deprived of comorbidities, although this procedure is performed in a sterile-contaminated environment.
Jefferson Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania
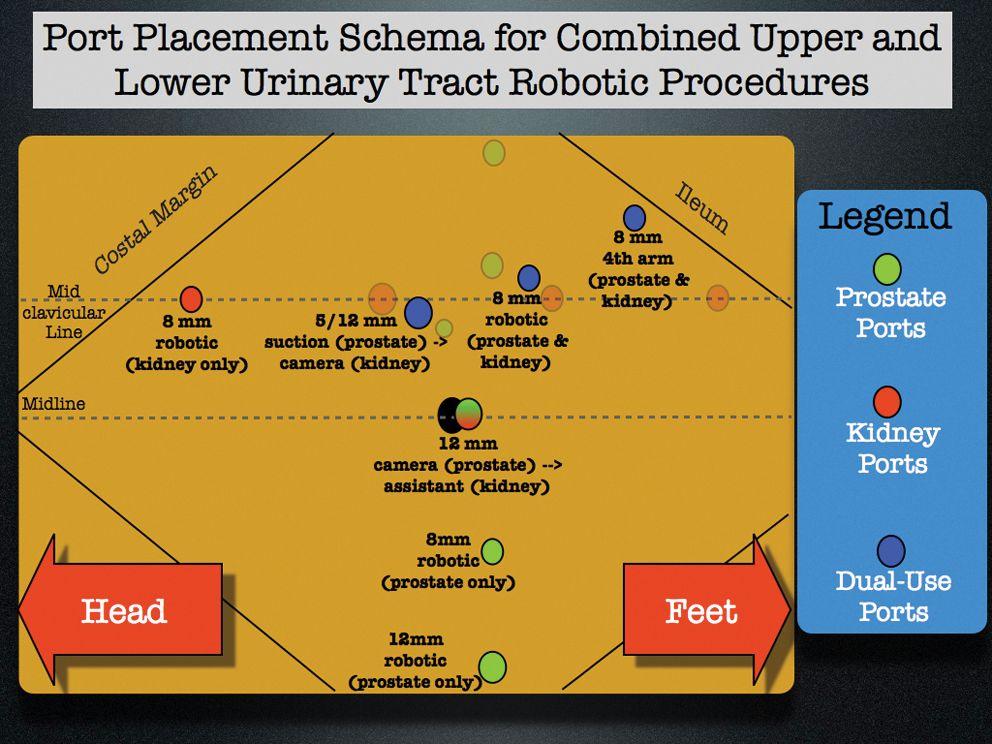
Bloodless Surgery for Jehovah Witnesss Patients: Our Initial Experience in Major Robotic Urologic Procedures
INTRODUCTION: Although numerous bloodless surgery techniques for Jehovah,s Witness (JW) patients have been reported, the literature is limited to mostly case reports or small case series. Since 2000, the rapid adoption of robotic surgery has enabled many patients to undergo complex minimally invasive surgery in lieu of open surgery. This rapid adoption of robotic surgery has been most notable in urology, however this adoption has not been reflected amongst JW patients in the literature. We review our center,s robotic urologic surgery experience in JW patients.MATERIAL AND METHODS: From November 2008 to April 2011, we reviewed all bloodless medicine patients that underwent robotic-assisted laparoscopic procedures by a single urologic surgeon (DE). Peri-operatively, all patients were co-managed with an established Bloodless Medicine team. We retrospectively analyzed peri-operative and blood management outcomes. RESULTS: Within a 29 month period, 27 patients underwent a major robotic urologic operation. Robotic prostatectomy (N=19; 5 had a concomitant procedure), partial nephrectomy (N=4), pyeloplasty (N=1), cystectomy (N=2), modified template retroperitoneal lymph node dissection (N=1). Intraoperative cell salvage was not used in any cases. One patient required postoperative Epoetin and one patient consented to a postoperative blood transfusion. One patient who was discharged on Clopidogrel postoperatively, died after profound epistaxis. CONCLUSIONS: Our center,s experience shows that a comprehensive robotic urologic surgery program is feasible in JW patients. Specialized robotic centers may offer expanded surgical indications for JW patients that may not be conventionally available elsewhere.
Influence of Education and Training for Young Surgeons on Practice of Laparoscopic Prostatectomy
Background; Education and practical training are very important for the young surgeons. After they learn the surgical skill by dry training box and/or animal lab and they experienced laparoscopic surgery as assistance in a surgical team. After that, young surgeons would have an opportunity to perform some procedures of laparoscopic surgery. So in each laparoscopic surgery there would be substantial time to consume for the practice for young surgeons.
Objectives; We evaluated the peri-operative data of laparoscopic prostatectomy to clarify the influence of education and practical training by young surgeons.
Methods; From March to September 2011, we participated in the clinical trial about laparoscopic radical prostatectomy. In this period, 3 expert surgeons complete the consecutive 44 operations without changes of the surgeons for training (group 1). Peri-operative data of this period was compared with that of 44 operations matched by nerve sparing and lymph node dissection from June 2010 to March 2011, in which young surgeons performed some procedures during operation.
Results; Nerve sparing and lymph node dissection were performed in 12 and 9 of 44 operations in each group. Prostate weight were 30.7 g (group 1) and 34.5 g (group 2). Average operation time was significantly longer in group 1 (255 min vs 187 min) (p < 0.001). Average blood loss including urine was significantly more in group 1 (773 ml vs 601 ml) (p < 0.001).
Conclusion; We demonstrated that we usually spent approximately one hour for education and practical training for the young surgeons in each laparoscopic prostatectomy.
A Progressive Training Program in Robotic-Assisted Laparoscopic Prostatectomy: Comparative Outcomes within a Veterans Affairs Population
Introduction: We sought to determine if surgeons participating in a progressive training program in robotic-assisted laparoscopic prostatectomy had similar perioperative outcomes. Methods: 90 robotic-assisted laparoscopic prostatectomies were successfully performed, under the auspices of a progressive training program. A single experienced robotic surgeon provided extended mentorship during the first 30 cases for a novice robotic surgeon. The initially novice surgeon went on to amass her own case series during the following 30 cases. In the last 30 cases, she was then the senior mentor for urology residents, operating as the primary surgeons. Independent t-test, Chi2, ANOVA, and Kruskal-Walls tests compared the demographics and operative outcomes in these patient populations.Results: The patient populations (n=30) were similar in age (p=0.867), clinical T-stage (p=0.247), and D'Amico Risk Group (p=0.076). The last 30 patients had a highest median (IQR) preoperative PSA, 8 (5-12.8, p<0.001) and the largest prostates, 47.8 grams (35.8-62.9 grams, p=0.044). Estimated blood loss (p=0.568), rate of blood transfusion (p=0.129), length of hospital stay (p=0.075), pathologic T-stage (p=0.357), and rate of positive margins (p=0.812), were comparable in all groups. There was no statistically significant difference in mean scores for pad use, pad dampness, satisfaction with sexual and urinary recovery or SHIM score between experienced and novice groups at twelve months. (all p>0.05).Conclusion: Using this model of progressive training, perioperative outcomes of surgeons, trained under the tutelage of a relatively new robotic mentor, are similar to the outcomes of surgeons trained directly by an experienced robotic mentor.
Less Radical Prostatectomy
INTRODUCTIONLaparoscopic radical prostatectomy has become the gold standard for treatment of prostate cancer in many centers world wide. LESS is a rising star in the world of laparoscopic surgery.PURPOSETo present our first case of pure laparoendoscopic single site radical prostatectomyPATIENTS AND METHODSOne patient underwent LESS radical prostatectomy using SILS port that was inserted through a 20-30-mm umbilical incision. PSA was 8.7gm/dl.Gleason score was 3+3. The whole gland size was 57 gm.RESULTS Patients age was 63 years old. Operative time was 287 min. Blood loss was 350.Hospital stay was 2 days. Visual analogue pain score was 2/10. No need for analgesic use in the early post operative period. The procedure was completed successfully without need for additional ports .Articulating instruments were used. Uretheral catheter was removed on tenth day. P.O pathology reveal prostate adenocarcinoma gleason 3+3 with negative surgical margin.P.S.A was 0.04 six weeks after the procedure.CONCLUSIONLESS radical prostatectomy is a technically challenging procedure whoever a large number of cases is needed to point out its role in management of prostate cancer cases.
University of Montreal Hospital Center, Cancer Prognostics and Health Outcomes Unit, Montreal, Canada
Introduction:RP outcomes should not differ between privately insured and other patients after adjustment for confounding variables. Methods:Within the Health Care Utilization Project Nationwide Inpatient Sample(NIS) we focused on RPs performed within the 5 most contemporary years(2003-2007). We tested the rates of homologous blood transfusions, extended length of stay, as well as intraoperative and postoperative complications, stratified according to institutional academic status.Multivariable logistic regression analyses further adjusted for age, race, Charlson Comorbidty Index (CCI), hospital region, annual hospital caseload (AHC) and institutional academic status.Results: Overall, 62070 private insurance/Medicaid/Medicare/Self-pay RPs were identified. Of those, private insurance accounted for the majority of cases(n=41312, 66.5%), followed by Medicare (n=18759), Medicaid(n=1096) and self-pay(n=903).Privately insured patients had a lower CCI, were less frequently Caucasians than other patients and were also more often treated at academic institutions with high AHC. Private insurance RPs were associated with fewer homologous blood transfusions, fewer intraoperative and postoperative complications, lower rates of hospital stay above the median, as well as decreased in-hospital mortality than other patients.In multivariable analyses, Medicaid RPs were associated with increased blood transfusion rates (OR=1.39), LOS beyond the median rates (OR=1.48) and in-hospital mortality rates (OR=8.43) compared to private insurance RPs. Similarly, Medicare RPs were associated with increased blood transfusion rates (OR=1.21), postoperative complication rates (OR=1.15) and length of stay beyond the median rates (OR=1.25). Finally, self-pay RPs were associated with increased blood transfusion rates (OR=1.35).Conclusions:Even after adjusting for confounding factors, private insurance RPs are invariably associated with better outcomes than their public insurance or uninsured counterparts.
Surgical and Oncological Outcomes in the Learning Curve of Four Approaches for Radical Prostatectomy: Perineal, Retropubic, Laparoscopic and Robotic.
Introduction There are still controversies regarding the best approach for radical prostatectomy.Purpose: to compare four groups of patients treated by different approaches of radical prostatectomy. Material and Methods: a prospective database of four consecutive series of radical prostatectomy surgeries for prostate cancer: perineal (PRP), retropubic (RRP), pure laparoscopic (LARP) and robotic (RARP) was analysed. Collected operative data included surgical time, anesthesia time, estimated blood loss, transfusion rate, hospital stay and histological evaluation.Results: A total of 160 patients (40 patients in each group) were included in the present series, all with clinical localized prostate cancer. Perioperative data revealed a statistically significant lower surgical time and anesthesia time for RARP (p<0.05.). Estimated blood loss were significant lower for RARP and PRP (220cc and 240 cc) in comparison to LRP and RRP (600 cc and 1080 cc) (p<0.05). Transfusion rate was 0% for both RARP and PRP whereas RRP and LRP revealed 17.5% and 7.5%, respectivelly. Hospital stay revealed to be significant lower in the RARP when compared to the other groups (p<0.05). Positive surgical margins rate was significant higher in the RRP group (30%) versus 15%, 12.5% and 17.5% for RARP, LRP and PRP, respectivelly. There were no differences regarding complications. Conclusions: RARP presents a safe initial learning curve with even better results when compared to other techniques. However randomized controlled trials are necessary before definitive conclusions are made and are strongly recommended in order to achieve the best patient health care provision.
Division of Urology, Department of Urology, Taichung Veterans General Hospital
ABSTRACT Purpose: Precise apical dissection of the urethra significantly ameliorates the apical positive surgical margin (PSM) rate in patients undergoing robotic-assisted radical prostatectomy (RARP). To analyze the feasibility of retro-apical transection of the urethra during RARP performed in Asian population.Materials and Methods: Eighty consecutive patients with clinically localized prostate cancer received RARP performed by a single surgeon. Patients received retro-apical (Group 1) or anterior-apical (Group 2) urethral transaction during RARP. We recorded preoperative clinical characteristics and measured bone pelvic parameters and prostate apex shape on magnetic resonance image (MRI). Operative parameters were compared between groups and pathological outcomes assessed. Results: Of patients, 75% were in Group 1 and 25% in Group 2. Bone pelvic parameters and apex shape were similar between groups. Group 2 had significantly higher preoperative body mass index (BMI) than Group 1 (27.43 vs 23.50, pless 0.001) and significantly higher prostate weight than Group 1 (52.00 vs 36.55g, p less 0.05). More of those in Group 2 than Group 1 received previous transurethral resection of the prostate (TURP, 25% vs 1.67%, p=0.003). Tumour volume in Group 2 was significantly higher than in Group 1 (15.17 vs 8.10 ml, p=0.049). The incidence of retro-apical transection of the urethra was 62.5% and 82.5% in the initial 40 cases and subsequent 40 cases, respectively (p=0.02).Conclusions: Large BMI, larger prostate and previous TURP, but not bone pelvic parameters or apex shape, may hinder retro-apical transection of the urethra.
Total Avoidance of Intravenous and Oral Narcotics after Robotic Prostatectomy
Introduction: Evidence of decreased pain with robotic prostatectomy (RP) has been sparse despite expectations of minimally-invasive surgery. Objective: We hypothesized that the low pain level associated with RP could allow complete narcotic avoidance and evaluated ability to manage pain with non-narcotic analgesics alone. Methods: We instituted a strategy of oral and intravenous narcotic avoidance after RP. The strategy and benefits were explained to patients and nursing staff, and intravenous NSAID therapy and oral acetaminophen were routinely given with even oral narcotics only if requested. Narcotic use in the hospital and the first week after surgery were recorded prospectively. Results: Outcomes for the initial 100 consecutive RP patients were evaluated. Mean patient age was 60yrs (44-75yrs) with mean BMI of 30kg/m2 (21-45). All received intravenous NSAID except one with renal insufficiency and one who wanted only acetaminophen. No patient required intravenous narcotics, and 62% of patients also required no oral narcotics. Of these, only one took any narcotic tablets at home (1 tablet). Of 38 patients who requested oral narcotic in the hospital, 12, 8, and 18 required 1, 2, or>2 oral narcotic tablets, respectively. Only 6 of these used any narcotic tablets at home (maximum 3 tablets). Therefore, overall only 8% used any narcotic tablets at home. All ambulated the day of surgery and 99% were discharged on the first postoperative day with only one experiencing ileus requiring longer hospitalization. Conclusions: Total avoidance of narcotics is possible in most RP patients with rare need for oral narcotics after discharge.
Quality and Outcomes of Robotic Lymphadenectomy for Prostate Cancer in Obese and Morbidly Obese Patients
Introduction: Robotic prostatectomy (RALP) is feasible in obese patients with body mass index (BMI)>30kg/m2, but possibly with increased operative times and complications. We offer RALP regardless of weight and routinely perform pelvic lymph node dissection (PLND). Objective: We assessed ability to perform PLND in obese and morbidly obese patients (BMI>40kg/m2) by evaluating nodal yield and positivity. Methods: We reviewed 1000 RALP procedures by a single surgeon (RA) between February 2008 and May 2011. Extended PLND was performed for high-risk cancers and limited PLND in all others. Outcomes were compared for BMI<30, 30-39, and>40kg/m2. Results: Mean BMI among all patients was 30kg/m2 (18-52kg/m2) with 525 of BMI<30kg/m2, 430 obese, and 45 morbidly obese and no difference among groups in proportion of high-risk cancers. Mean total operative time was 149min, 159min, and 176min for normal, obese, and morbidly obese patients, respectively (p<0.05). Estimated blood loss was 106mL, 128mL and 148mL (p<0.05) with transfusion rate of only 0.5% and none in the morbidly obese group. Mean hospitalization was 1.0d in all three groups. Mean nodal yields were 9.2, 9.8, and 10.8 nodes for normal, obese and morbidly obese patients (p=NS). Extended PLND was performed in 15%, 17%, and 16% with mean yields of 16.4, 15.6, and 18.7 nodes, respectively (p=NS). Node positivity was identified in 5.1%, 6.5%, and 11.1% (p=NS). Complications of PLND occurred in 1.3%, 2.3%, and 4.4%, which were mostly symptomatic lymphoceles. Conclusions: Robotic PLND can be performed with equal efficacy in obese and morbidly obese patients.
Effect of Median Lobes on Perioperative Outcomes and Urinary Function After Robotic Prostatectomy
Introduction: Enlarged median lobes (ML) may affect perioperative and urinary function outcomes after robotic prostatectomy (RP). Objective: We assessed ML incidence among our patients and compared their outcomes to patients without ML. Methods: We reviewed 632 RP by a single surgeon with at least three months of follow-up. Urinary function was assessed by questionnaires. Results: ML was identified in 134 patients (21.2%). Mean age was higher in ML patients (62.2yrs vs. 60.7yrs, p=0.03) as was gland size (68.2g [34.7-160g] vs. 53.2g [20.1-257.9g], p<0.05). Mean blood loss was higher in ML patients (128.5mL vs. 115.3mL, p<0.01), but only one ML and 2 non-ML patients required transfusion. There was no difference in mean operative time (150.5min vs. 145.7min, p=0.10), mean hospitalization time (1.01 vs. 1.02 days, p=0.94), or need for bladder neck reconstruction (3% vs. 2.4%, p=0.71). A JP drain was not used in any ML patients and was used in 5 (1%) non-ML patients. Median catheterization time was 6.0d in both groups, but mean catheterization time was longer in ML patients (6.3 vs. 5.6d, p=0.01). Preoperatively, ML patients had higher mean AUA-Symptom Score (12.5 vs. 9.7, p<0.01) but were similar to non-ML patients at 3 months (8.0 vs. 9.1, p=0.10). At 3 months there was no difference in urinary frequency, nocturia episodes, or urgency, and self-reported continence (0-1 pads/day) was achieved in 77% of ML patients and 70.4% of non-ML patients (p=0.26). Conclusions: Presence of ML did not greatly impact perioperative outcomes with no difference in urinary function at 3 months.
Comparison of Extraperitoneal Laparoscopic Radical Prostatectomy and Open Retropubic Radical Prostatectomy at Ramathibodi Hospital, Thailand : A Retrospective Review
Objective: To compare outcomes of open radical prostatectomies (O-RP)and laparoscopic radical prostatectomies (LRP), focusing on operative time, blood loss, length of hospital stay, time to drain removal and surgical margin status. Materials and Methods: We reviewed the medical histories of 173 patients treated for prostate cancer by radical prostatectomy in at Ramathibodi Hospital between January 1997 and August 2010. Eighty-one patients were treated with O-RRP and 52 were treated with E-LRP.Forty cases were omitted from the study due to incomplete data. The following data were collected and compared between treatments: operative time, blood loss, length of hospital stay, time to drain removal and surgical margin status.Results: Estimated blood loss was significantly lower in the E-LRP group (median=600 ml, range=50-4000 ml) than in the O-RRP group (median=2000 ml, range 200-7500 ml) (p<0.001). The length of hospital stay in the E-LRP group (median=8 days, range=4-27 days) was significantly shorter than in the open group (median=11 days, range=5-37 days) (p<0.001). There were no significant differences between operative times, times to drain removal or surgical margin statuses.Conclusion: The study shows that patients who underwent E-LRP experienced less blood loss and shorter hospital stays than patients who underwent O-RRP.
Uefulness of V-Loc™180 During Laparoscopic Radical Prostatectomy
Introduction: Although laparoscopic radical prostatectomy (LRP) has spread widely in Japan, to improve the technique of vesicourethral anastomosis is still very important theme.Purpose: The aim of the present study is to elucidate the utility of a novel technique of self-cinching anastomosis using a barbed and looped suture, V-Loc™180, during LRP.Marerials and Methods: 6 consecutive patients underwent LRP for clinically localized prostate cancer using V-Loc™180 absorbable barbed suture during vesicourethral anastomosis. Duration of each steps in LRP and postoperative catheterization were compared with those in other 6 consecutive patients who underwent LRP by the same surgeon using Biosyn™. Results: There was no difference between charecteristics of these two groups. Duration of vesicourethral anastomosis using V-Loc™180 was significantly shorter than that using Biosyn™ (median; 25min, 35min, respectively; p=0.009). There was no significant difference between these two groups in pneumoperitoneum time(median; 167min, 187min, respectively; p=0.591), operative time(median; 200min, 206 min, respectively; p=0.458) and duration of postoperative catheterization (median; 7, 6, respectively; p=0.104). There was no severe adverse event using V-Loc™180.Conclusions: The results of this study demonstrate that V-Loc™180 can be one of the feasible option in vesicourethral anastomosis.
Laparoscopic and Retropubic Radical Prostatectomy, Single Center Experience
IntroductionLaparoscopic radical prostatectomy is alternative method retropubic radical prostatectomy.PurposeThe aim of this study was a comparison of laparoscopic and retropubic radical prostatectomy carried out in our center.Materials and Methods There were evaluated 225 patients who underwent radical prostatectomy in period January 2008 to April 2011. The retropubic prostatectomy (RRP) was performed in 125 patients and extraperitoneal laparoscopic (LRP) in 100. The surgical results and complications with functional and preliminary oncologic results were evaluated.Results The median follow-up was 14 months. The mean age was 62 years, median PSA was 9 ng/ml and Gleason sum 7. Both cohorts were comparable in demographic and oncologic parameters. The results are shown in table 1. ConclusionsLaparoscopic extraperitoneal radical prostatectomy is a suitable minimally invasive alternative method to the open retropubic prostatectomy. The duration of a surgery was initially longer. The blood loss is significantly lower, functional and preliminary oncologic results are similar. Laparoscopic approach allowed short recovery.
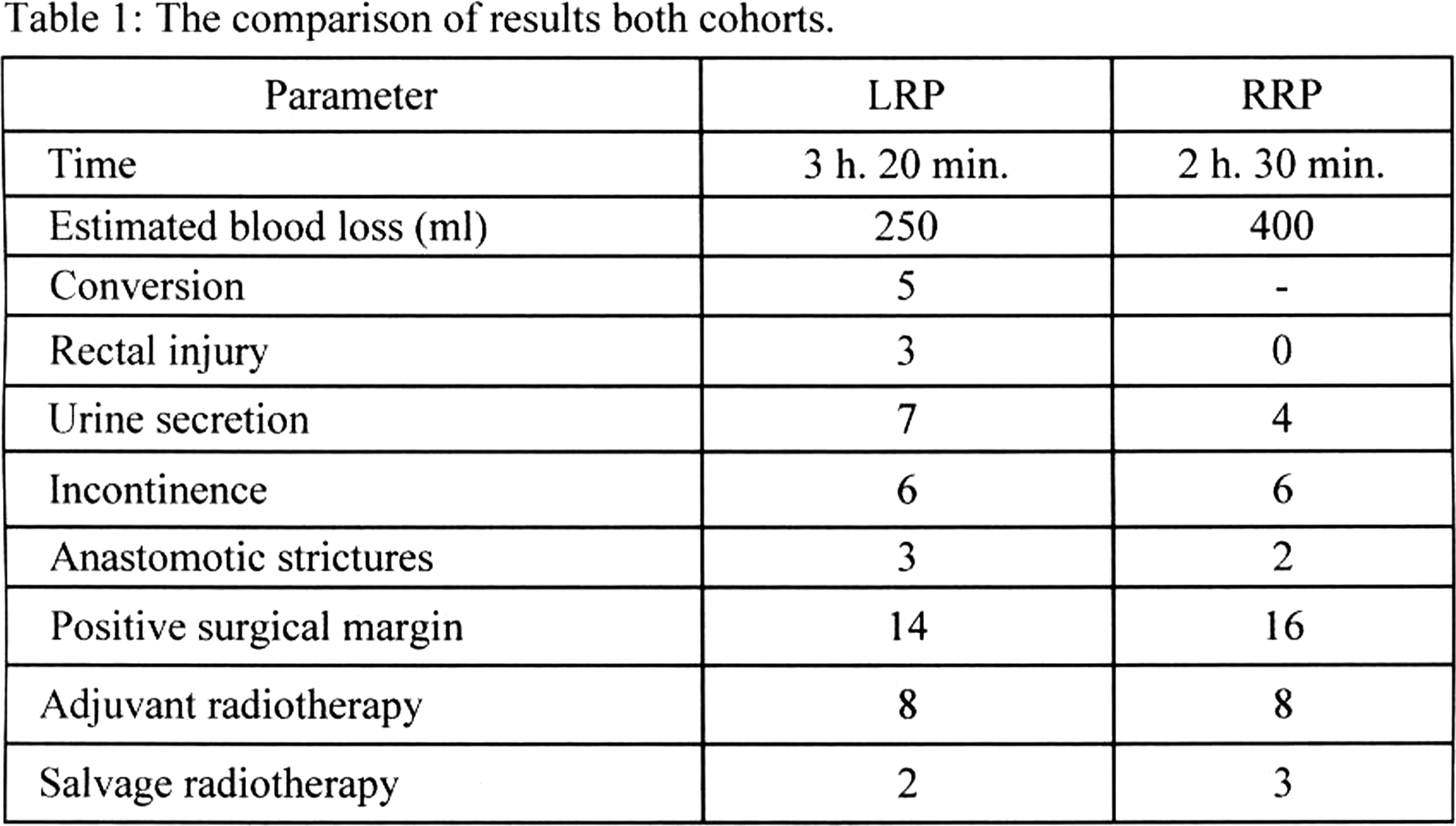
MP14: New Technology/Imaging 2
Lymphangiography with or without Sclerotherapy: A Novel Technique for the Treatment of Refractory Chylous Ascites Following Urological Surgery
Introduction:Prolonged lymphatic leak and chylous ascites can be a devastating complication following retroperitoneal surgery. Patients refractory to standard conservative measures can become debilitated by discomfort and malnutrition. Lymphangiography (LAG) ± sclerotherapy are options for the localization and management of refractory lymphatic leaks.Purpose:We report the outcomes of a small series of patients with refractory chylous ascites following urologic surgery treated with lymphangiography ± sclerotherapy.Materials and Methods:Retrospective review revealed three patients who underwent lymphangiography for prolonged lymphatic leak following urological surgery. Contrast material is injected slowly into a lymphatic vessel on the dorsum of the foot and serial imaging is used to capture the location and degree of lymphatic leak in order to guide definitive treatment. Demographic and clinical details were collected and are reported.Results:Three patients were identified from 2005-2008 (1 following donor nephrectomy and 2 following retroperitoneal lymph node dissection). All patients presented with abdominal distension within 30 days of surgery. Traditional conservative measures failed in all patients. Lymphangiography localized all leaks (renal hilum, paraspinal, and retrocaval). One patient elected for successful surgical repair after localization. The remaining 2 patients resolved immediately following LAG; one of these patients underwent percutaneous doxycycline sclerosis. With over 1 year of follow up there have been no recurrences or long-term sequelae.Conclusions:Lymphangiography is a valuable management option for the rare patient with chylous ascites refractory to conservative therapy. Prompt resolution of prolonged chylous ascites following lymphangiography should encourage its use in such difficult cases.
The Fabrication and Properties of Co-polymer Poly(lactic-co-glycolic acid) Ureteral Stent By Electrospinning
Objective: The present study was designed to discuss the feasibility of the fabrication of co-polymer poly (lactic-co-glycolic acid) (PLGA) ureteral stent by electrospinning and evaluate its degradable properties in vitro. Methods: After synthesizing of different ratio of PLGA, the electrospinning technique was used to fabricate the ureteral stent. The morphology was investigated by scanning electron microscope. The stent was cut into pieces which were immersed in the urine to evaluate its degradability. The morphology, residual weight rate and molecular weight were investigated in each observation point. Results: The stent had the nanostrcuture, and the morphology of the stent can satisfied the demand of a degradable stent. The residual weight rate curve of different ratio of PLGA was close to a straight line. The polymer containing a 50:50 ratio of lactic and glycolic acids was hydrolyzed within 6 weeks, which was much faster than those containing higher proportions of either of the two monomers. An 80:20 ratio of PLGA was degraded completely within 8 weeks, and PLGA (70:30) samples were observed to collapse at the tenth weeks. The decrease of molecular weight was apparently in the early stage, and was slow down in the later stage. Conclusion: The properties of PLGA (50:50) and PLGA (80:20) ureteral stent which fabricated by electrospinning technique can fully satisfied the demand of a degradable stent.
The Fabrication and Properties of Co-polymer Poly(lactic-co-glycolic acid) 80:20 Tubular Urethral Scaffold By Electrospinning
Objective: The present study was to discuss the feasibility of the fabrication of co-polymer poly (lactic-co-glycolic acid) (PLGA) 80:20 tubular urethral scaffold by electrospinning and evaluate its properties. Methods: PLGA(80:20) was dissolved in chloroform to form solutions with concentrations varying from 3% to 6%.The electrospinning technique was used to fabricate the tubular urethral scaffolds.Fiber diameters, aperture, porosity and mechanical properties were compared between various concentrations. Results: The concentration of 6% failed for high concentration. The scaffold was 4 cm long and with an inner diameter of 3.0 mm and an outside diameter of 4.0 mm. The fiber diameter was thicken with the increasing of the concentrations(p<0.05). The average aperture of three concentrations of PLGA were 7±4um, 13±7um, 32±13um, respectively(p<0.05). The porosity of 3% PLGA was close to 79%, and 5% PLGA was up to 90%, a significant differences was observed(p<0.05). The mean stress at break of the three concentrations of PLGA were 2.37±0.15MPa, 1.97±0.07MPa , 1.75±0.11MPa, respectively, the mean stress at break of 3% PLGA was significantly higher than that of the concentration of 4% and 5%(p<0.05), while no differences was observed between 4% PLGA and 5% PLGA (p>0.05). Conclusion: The properties of 5% PLGA (80:20) urethral scaffold which fabricated by electrospinning technique can fully satisfied the demand of a degradable urethral scaffold.
Department of Urology, Hospital Littlebelt, Fredericia, Denmark
Introduction:The MemokathTM051 (PNN Medical, Denmark) is a thermo-expandable ureteral nitinol stent and is designed for the long-term management of chronic ureteral strictures. Purpose:The aim of the present study was to evaluate the use of the MemokathTM051-stent in the treatment of chronic ureteral strictures due to retroperitoneal and periaortal fibrosis.Materials and Methods:In this retrospective study we included a total of 35 patients with ureteral strictures due to periaortal or retroperitoneal fibrosis. The Follow-up included KUB and renography. Results:The stenting procedure was usually easy and without serious complications. The average indwelling time of an individual Memokath was 26 months (range 8 days - 114 months). Migration occurred in 16 % of cases. Incrustations were seen very seldom. Stent removal was easy and could be done retrograde in all cases.Conclusion:The MemokathTM051-stent seems to be especially well suited for long-term treatment of chronic ureteral strictures due to periaortal or retroperitoneal fibrosis without the high rate of side-effects of JJ-stenting.
Duel Expansion Memokath 051 Stent in the Management of Ureteric Strictures: An outcome Analysis
Introduction: Memokath 051 has been effective in the management of ureteric strictures. However, migration has been reported especially in benign strictures. We present out results with this modified device which is expected to prevent this complication.Material and Methods: Fifteen Memokath051 duel expansion stents were inserted in 10 patients with ureteric strictures between 2003 and 2011. In two patients, stricture was caused by malignancy, 8 had benign recurrent strictures. Sticture length varied from 1.5 to 5 cm (median 2 .5 cm). Stricture was in the lower 1/3rd ureter in 7 patients, middle 1/3rd in 1, at PUJ in 1 and at the uretero-ileal anastomosis in 1. Conventional insertion technique was used. Follow-up included IVU, renal function tests and MSU.Results: Upper tract decompression was achieved in all patients. Three patients currently have functional stents with a mean follow up of 20 months (2 to 43 months). One patient had died with malignancy with functional stent. Stent migration resulting in recurrence of obstruction was detected in 5 patients. The migration was always proximal. The period of migration varied between 6 months to 3 years. Encrustation necessitated removal of one stent in the patient with ileal conduit. Successful re-insertion was achieved in all cases.Conclusions: This modified version of the Memokath 051 ureteric stent offers a good functional result but is not free from migration. The study is limited to a small number of patients.
Department of Urology, Samsung Medical Center
IntroductionTo investigate the clinical efficacy of novel covered self-expandable dual-layered metallic mesh stent(CEdMS) in patients with ureteral obstruction.Material and methodsTwenty four patients(34 ureter units) underwent a novel CEdMS(Niti-S™, TaeWoong Medical, Korea) placement from December 2009 to Jan 2011. Indications of stent placement were malignant ureteral obstruction with advanced cancer, D-J stent malfunction and/or severe D-J stent irritations and/or severe pain during periodic change. Urinalysis, blood biochemistry and diuretic renogram was evaluated every 3 months. Primary success was defined as no obstruction after primary insertion and final success as no obstruction without any intervention except additional CEdMS insertion.ResultsThirty two units were evaluable. Mean age was 55yrs(35-78) and follow up period was 5mos(1-10). Mean ureteral stricture was 9.8cm(1-20.5). The most common indication of CEdMS was D-J stent malfunction(70.5%). Primary success was 66%(21cases) and final success was 75% (24 cases). The cause of failure was tumor progression to additional ureteral segment(4) and obstruction by bladder invasion(4). All failed cases needed percutaneous nephrostomies. Eighteen of 22 patients(82%) experienced final success. Most common complication was abdominal pain(6), followed by gross hematuria(2), acute pyelonephritis(1), persistent lower urinary tract symptoms(1), and downward migration(1). There was no case of transfusion, urinary leak and extraureteral migration.Conclusions In this preliminary data, CEdMS showed good success rate even for D-J stent resistant malignant ureteral obstructions. CEdMS could be performed safely with low migration rate in short-term follow up. CEdMS could be considered as an option for malignant ureteral obstruction with advanced primary cancer.
Comparing Stone Attenuation In Low-Dose and Conventional Noncontrast Computerized Tomography
Introduction: Noncontrast computerized tomography (NCCT) is the radiographic modality of choice for detecting stones and is able to provide Hounsfield Units (HU) to assist in identifying stone type. Many centers are developing low-dose CT stone protocols as they can detect stones with high sensitivity and specificity; however, it is not known whether these protocols are equally effective in determining the HU stone density.
Purpose: To determine if there is a difference in attenuation measurements when comparing low-dose radiation and conventional CT scans.
Materials and Methods: In this prospective randomized study, 7 mm calcium oxalate stones were placed into random locations in the ureter in 3 human cadavers. NCCT was performed for each stone configuration using different mAs radiation settings ranging from 5 to 140 mAs. The average attenuation levels were measured in an identical manner for each stone to determine the stone density at each mAs setting.
Results: Median attenuation levels of the 133 observed stones were 614 HU at 5 mAs, 674 HU at 7.5 mAs, 681 HU at 15 mAs, 669 HU at 30 mAs, 670 HU at 50 mAs, 674 HU at 70 mAs, and 667 HU at 140 mAs. The differences in median attenuation levels were not significantly (p=0.998) different from each other at the selected radiation settings. Increasing attenuation variability was noticed as the radiation dosage decreased; however, this trend was not significant (p=0.411).
Conclusion: When determining stone composition and density, measuring stone attenuation in low-dose CT is as reliable as measuring stone attenuation in conventional computerized tomography.
Predicting Factors for the Spontaneous Passage of Ureteral Calculi: Impacts of the Stone Size as Measured on Thin-slice CT
Introduction: KUB provides only 2-dimensional, stone size information corresponding to coronal section CT, whereas CT provides 3-dimensional information including anteroposterior diameter (APD). Purpose: We studied the size correlation of radiopaque stones on KUB and CT and analyzed predictive factors for spontaneous passage during conservative treatment.Materials and Methods: Of 1,694 patients, who underwent both KUB and 2-mm, thin-slice stone CT, 117 with ureteral stones and follow-up imaging studies were included. Stone dimensions analyzed included transverse diameter (TD) and craniocaudal length (CL) on KUB, APD and TD on cross-sectional CT imaging, and CL on CT estimated by slices with visible stones.Results: The median patient (range) age was 54 years (4-82). Fifty-seven (48.7%) stones were located in the upper ureter above the sacroiliac joint. The median stone size measured on KUB was 4.2 mm (2.0-13.4) for TD and 5.3 (2.2-19.3) for CL. The median size measured on CT was 5.0 (2.6-15.0) for TD and 6.0 (2.5-21.0) for CL, both being significantly larger than measured on KUB (p<0.001, respectively). Median APD on CT and not measurable by KUB, was 5.3 (2.1-15.7) which was the largest dimension in 29 patients (24.8%). In 41 patients (35.0%), stones passed spontaneously, during a median 12 days (1-83). On multivariate analysis, only APD (HR 6.87; 95% CI 2.0-23.3; p=0.002) was an independent factor to predict spontaneous passage.Conclusions: Stone dimensions estimated by thin-slice CT were larger than those determined by KUB. APD on thin-slice CT is an independent factor predicting the likelihood of spontaneous passage.
Department of Urology, Loma Linda University, Loma Linda, CA, USA
Introduction: Stone burden is often determined using two-dimensional measurements on computed tomography (CT) scans. Studies suggest that stone volume may be a more accurate index of measurement. Previously, stone volumes have been measured by counting voxels or measuring circumferences which can be time consuming and cumbersome. OsiriX software allows for three-dimensional measurements to be taken quickly and easily.
Purpose: To compare stone volumes measured by water-displacement with stone volumes calculated with OsiriX software.
Materials and Methods: CT imaging was performed of 124 urinary stones, ranging from 5.58 to 31.42 mm in size, placed within kidneys in a female human cadaver. OsiriX imaging software with the NMSegmentation plug-in was used to calculate stone volume. OsiriX volumes were then compared with water-displaced volume to determine accuracy of measurement. Statistical analysis was conducted using repeated measures ANOVA and least square means analysis (α=0.05).
Results: For stones>1 mL, OsiriX calculated renal calculi volumes with 4.17%, 4.89%, and 5.58% median error for 1.25, 2.5, and 5 mm slice thicknesses, respectively. For stones<1 mL, there was a significant difference (p<.001) in mean error using 5 mm cuts (40.8%) compared to 1.25 mm (24.2%) and 2.5 mm cuts (30.1%). The average time of stone volume determination was 10.25 s.
Conclusion: Stone volume can be accurately calculated using OsiriX for stones>1 mL; however, it is less accurate when evaluating stones<1 mL. For larger stones, this three-dimensional volume calculation could prove to be a powerful clinical and research tool to allow standardization of stone volumes.
Department of Urology, Loma Linda University, Loma Linda, CA, USA
Introduction: Patient body weight has been shown to affect the radiation dose required for computed tomography (CT) scans. The accuracy of low-dose CT protocols, which deliver less ionizing radiation compared to conventional CT for individuals of average body habitus, has not yet been determined for patients in the extremes of weight.
Purpose: To evaluate the effect of body weight when using low-dose protocols to detect ureteral calculi.
Materials and Methods: Three cadavers of increasing weight (55-kg, 85-kg, and 115-kg) were prepared by inserting 721 calcium oxalate stones (range: 3-7 mm) in 33 random configurations into urinary tracts and scanned using a GE LightSpeed at 7 radiation settings. An independent review by a blinded radiologist was conducted to generate ROC curves, with areas under the curve compared using a one-way ANOVA (α=0.05).
Results: Diagnostic accuracy was significantly lower in both the low and high weight cadavers compared to the medium weight cadaver at 5 mAs (p<0.001) and 7.5 mAs (p=0.048) (Figure 1). Differences in accuracy at radiation settings >=15 mAs were not significant.
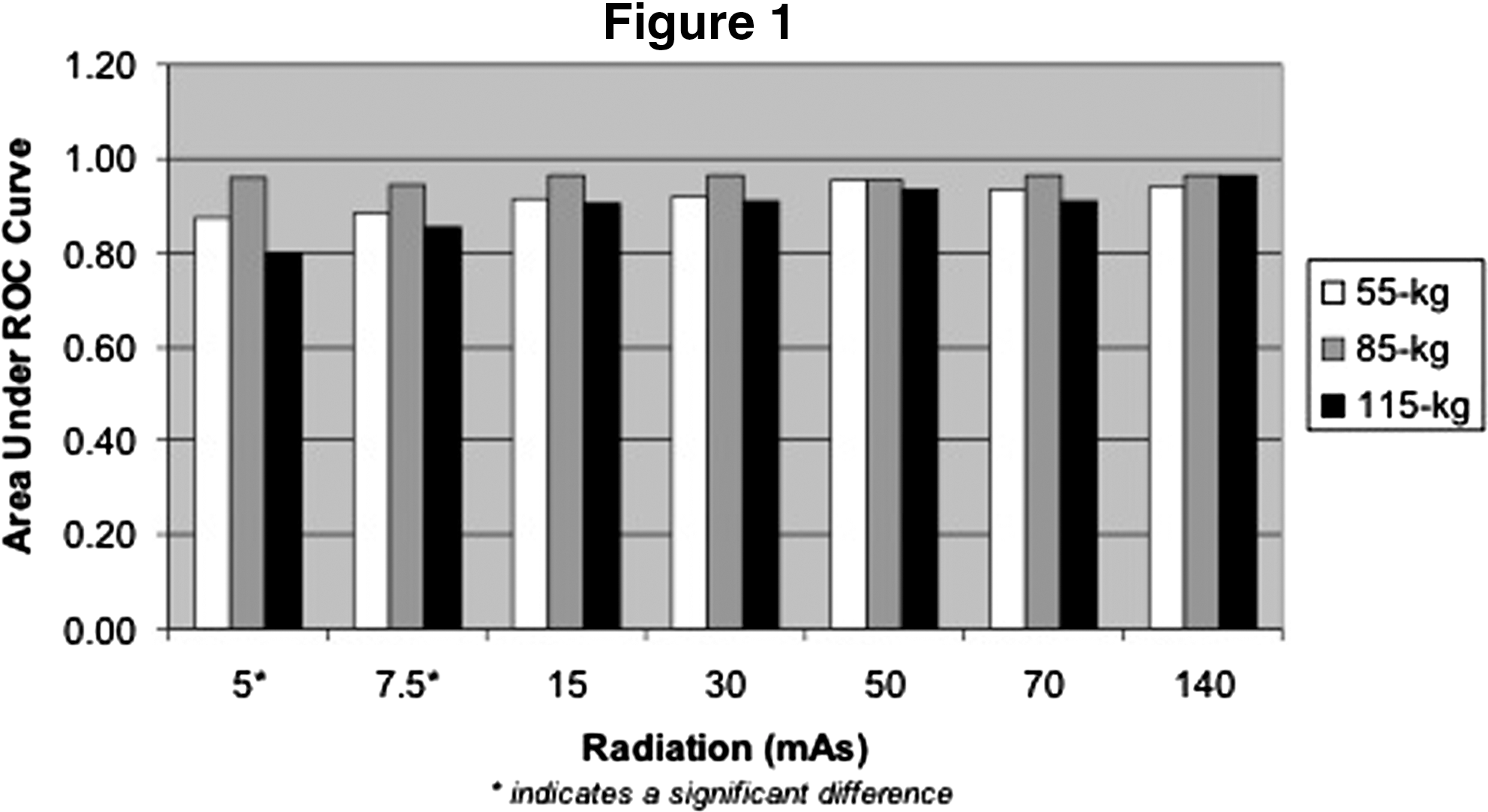
Conclusions: Extremely low-dose protocols may interfere with stone detection in underweight and overweight patients. Slightly higher radiation levels may be required in these patients.
No Invasve Urodynamics: Our Experience
OBJECTIVES: Troublesome voiding lower urinary tract symptoms (LUTS) are a common problem in men and a multitude of methods have been applied to assess lower urinary tract symptoms (LUTS). Pressure flow studies still remain the gold standard for assessing bladder outlet obstruction. In this study we evaluate the clinical and urodynamic features in men with LUTS and to determine non-invasive parameters for predicting bladder outlet obstruction (BOO). We performed a non-invasive test to categorize voiding dysfunction in men complaining of lower urinary tract symptoms (LUTS) - the penile cuff test.METHODS: A total of 67 patients with lower urinary tract symptoms underwent simultaneous invasive urodinamics pressure flow studies with bladder and abdominal catheter and noninvasive pressure flow studies with penile cuff. Average age was 60.5 years. We performed the test involves the controlled inflation of a penile cuff during micturition to interrupt voiding and estimate isovolumetric bladder.RESULTS: In 67 patients in invasive urodinamics study 22 was no obstructed, 17 was mild obstructed and 28 was severe obstructed. In the penile cuff test there was correspondence in 87%.CONCLUSION: Non-invasive methods that measure isovolumetric bladder pressure by interrupting the urinary stream can reproducibly measure pressure and urinary flow, but are unable to determine the effects of abdominal straining during voiding and give no insight into urine storage symptoms. Also failed to differentiate obstruction from ipocontrattility detrusorial. However it is a simple test, non-invasive and good predictionto the diagnosis and treatment planning of men with LUTS.
Incidence of Patient Safety Indicators for Three Minimally Invasive Urologic Surgeries: An Analysis of the National Inpatient Sample
IntroductionPatient safety has become a central issue in healthcare quality. Patient safety indicators (PSIs) have been developed to identify potentially preventable adverse events that compromise patient safety. We examined the prevalence of PSIs in patients undergoing commonly performed laparoscopic/endourologic procedures: laparoscopic nephrectomy (LN), laparoscopic prostatectomy (LP), and percutaneous nephrolithotomy (PNL). MethodsWe examined the 2008 Nationwide Inpatient Sample (NIS) from the Healthcare Cost and Utilization Project, which contains discharge data from 1,056 hospitals in 42 states. Subjects were identified by ICD-9 coding: LN (5552, 5553 or 5554 with 5421 or 5451), LP (1742 with 605), and PNL (5504, and 5503 with 5521). PSIs were identified and descriptive analyses were performed. RESULTSSee Table 1 for PSI incidence among the 3 procedures. Subjects undergoing LP were significantly older than those undergoing LN or PNL. Mortality was significantly higher in LN (0.6%) compared with PNL (0%) and LP (0%) (p=0.0002). CONCLUSIONSThe prevalence of PSIs among patients undergoing minimally invasive urologic surgeries is low. Future efforts to identify more meaningful indicators of care quality for minimally invasive urologic surgery are welcome, as the urologic community continues to focus on the preventability of adverse events.
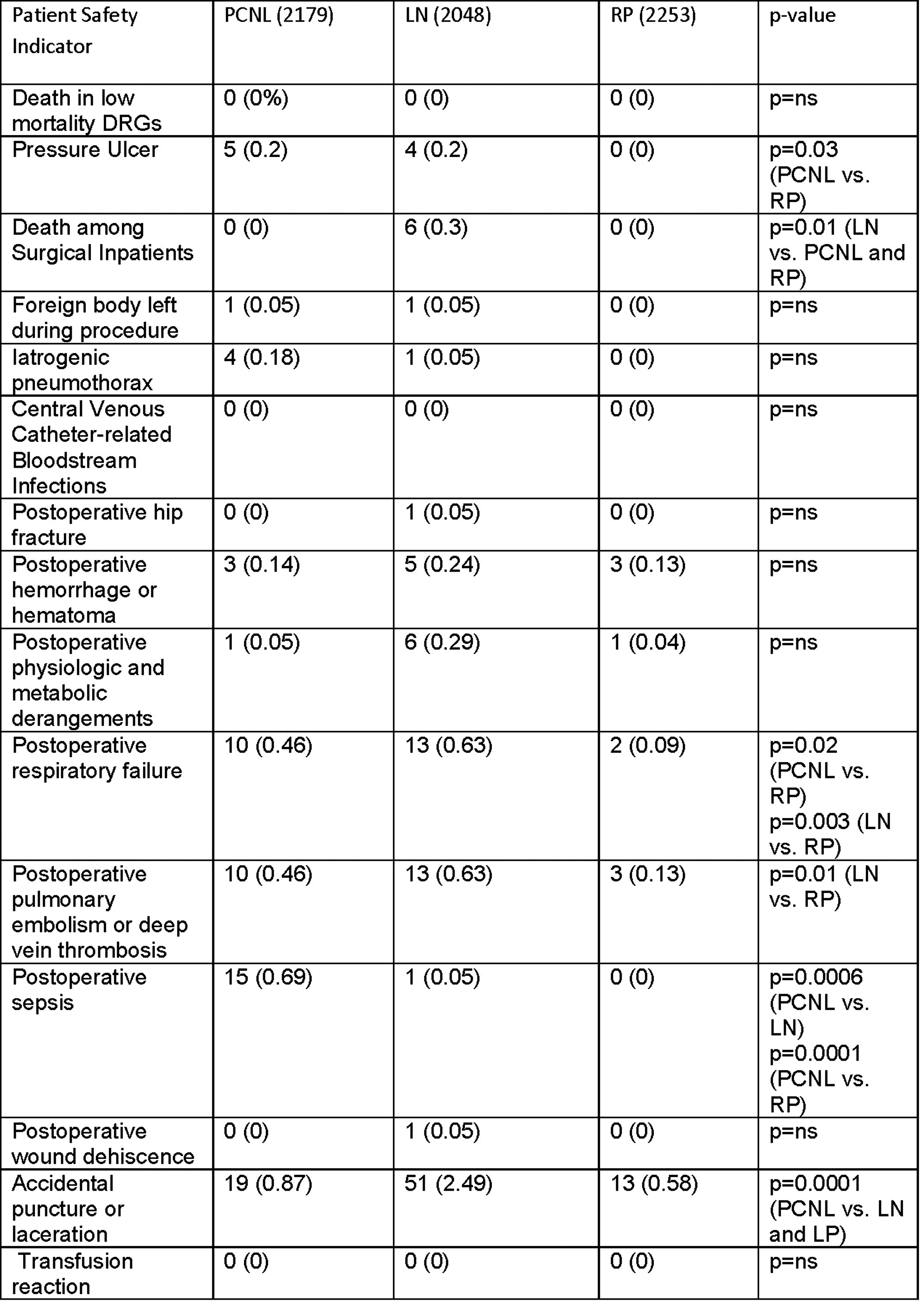
Significance of Virtual Cavernoscopy in the Diagnosis of Penile Venous Leakage
Virtual cavernoscopy is one of the most useful modalities in the diagnosis of erectile dysfunction. We compared the characteristics of virtual cavernoscopy and 3D CT cavernosography. The subjects were 45 patients with suspected organic erectile dysfunction. After the written informed consent, we performed pharmaco-dynamic infusion cavernosometry and cavernosography with a CT scanner. Drainage veins in each case were evaluated using both virtual cavernoscopy and 3D CT cavernosography. Virtual cavernoscopy showed drainage to the deep dorsal vein in 14 cases. However, this modality was not able to diagnose the patency of the vein at the base of the penis. Compared with this, 3D CT cavernosography revealed the deep dorsal vein at the body of the penis in 31 cases. Regarding the patency of this vein at the base of the penis with this method, 14 cases out of 31 showed narrowing, 11 showed complete blocking, and 6 showed patency. Leakage via crural veins was equally depicted in 15 cases with both methods. Virtual cavernoscopy showed leakage, including the origins of the veins, via cavernous veins in 33 cases. 3D CT cavernosography showed leakage via cavernous veins in 23 cases, but could not show the origins of all the veins. Virtual cavernoscopy is not suited for the diagnosis of deep dorsal vein leakage. On the other hand, in the diagnosis of the cavernous veins, virtual cavernoscopy is superior to 3D CT cavernosography. In conclusion, When diagnosing the penile venous leakage, we recommend utilizing both virtual cavernoscopy and the 3DCT cavernosography.
Associated Medical Professionals
Background: This study evaluated the safety and hemostatic effectiveness of a tranexamic acid- and aprotinin-free fibrin sealant versus an absorbable hemostat in soft tissue during elective retroperitoneal or intra-abdominal surgery.Materials and Methods: This randomized, active-controlled, multicenter study enrolled patients who were undergoing elective retroperitoneal or intra-abdominal surgery and required adjunctive hemostatic measures at the target bleeding site (TBS).Patients were randomized (time=0 minutes) to receive fibrin sealant or absorbable hemostat. The primary endpoint was the absence of bleeding at the TBS at 10 minutes. Secondary endpoints included the absence of bleeding at 4 and 7 minutes and the incidence of treatment failure (bleeding at 10 minutes or brisk bleeding requiring additional hemostatic measures), and the incidence of complications potentially related to bleeding. Adverse events were assessed.Results: Patients (N=124) were randomized to receive fibrin sealant (n=62) or absorbable hemostat (n=62). A higher percentage of patients who received fibrin sealant versus absorbable hemostat achieved hemostasis within 10 minutes (95.2% vs 82.3%; 95% CI, 1.02 to 1.35) and also at 4 (74.2% vs 54.8%; 95% CI, 1.04 to 1.80) and 7 (90.3% vs 77.4%; 95% CI, 1.00 to 1.39) minutes. A lower incidence of treatment failure was observed for patients receiving fibrin sealant. Similar incidences of adverse events and complications potentially related to bleeding were observed.Conclusions: This tranexamic acid- and aprotinin-free fibrin sealant is safe and effective for achieving hemostasis in soft tissue during elective retroperitoneal or intra-abdominal surgery. Trial registration: ClinicalTrials.gov, NCT00307515,
Urology Department, Los Angeles Medical Center, Kaiser Permanente, Los Angeles, California, USA
INTRODUCTION AND OBJECTIVES: Percutaneous renal needle biopsy is gaining relevance and reemerging in clinical decision-making as the approach to management of renal masses is evolving. We intended to characterize renal biopsy results in order to assess the accuracy of renal biopsy for predicting tumor histologic subtype and nuclear grade, and to illustrate the role of renal biopsy in surgical versus nonsurgical management.METHODS: A retrospective chart review was performed of patients that underwent percutaneous renal biopsy of a solid renal mass from 01/2005 to 12/2009. Patients were stratified by size of renal mass, comparing SRMs to larger renal tumors. Initial biopsy results including tumor histology and nuclear grade were evaluated and related to post-operative pathology specimens when surgery was performed.RESULTS: The study included 126 patients (129 renal units with 132 biopsies). 63 patients (50%) ultimately underwent surgery(23 partial and 40 radical nephrectomies). The overall sensitivity for detecting cancer (verified by final pathology) was 75.4% with 100% specificity. The PPV for patients who underwent surgery was 100% and NPV of 11.7%. When evaluating factors associated with renal biopsys accuracy of predicting cancer, larger tumor size had an adjusted odds ratio of 2.20(0.547, 8.878, 95% CI) and increasing number of biopsy samples>3 had an adjusted odds ratio of 2.50(0.586, 10.694, 95% CI).CONCLUSIONS: Percutaneous renal needle biopsy in the modern era has respectable sensitivity, excellent specificity and good concordance with final pathology. This modality can assist in clinical decision-making for renal masses, particularly for SRMs, as treatment options are expanding.
PSG Institute of Medical Sciences and Research, Coimbatore, India
Laparoscopic procedures are replacing almost all abdominal open procedures. Sometimes minor disturbances hinder the progression of surgery. One such hindrance is the constant slipping of the trocar within and outside the abdominal cavity. This movement and repositioning can consume considerable operative time. Fixing the trocar with sutures is usually done with some benefit. Apple trocar with ridges can also act as a self retaining trocar. We present a couple of ideas to prevent constant migration of the trocar. The first one is to use a cut finger stall of the glove and winding it over the trocar tightly. The glove ring in turn may be sutured with the skin to have a tight hold to the abdominal wall. The other idea is to fasten a nut and bolt around the trocar and fixing the skin with the bolt. This gives better hold of the port with the abdominal wall. These innovations reduce the operative time and frustration of the laparoscopic surgeon.
A Randomized Single-Blind Comparison of the Cost-Effectiveness of Tristel Fuse and Cidex OPA for use with Flexible Cystoscopes.
Introduction: The effectiveness of Tristel Fuse was compared with Cidex OPA for high-level disinfection of flexible cystoscopes. The clinical and microbiological efficacy, safety, cost-effectiveness and ease-of-use were compared.Methods and Materials: A randomized single-blind study comparing the high level disinfectants Tristel Fuse (Chlorine Dioxide) as a soak and Cidex (ortho-Phthalaldehyde; 1,2 benzenedicarboxaldehyde) using an automated reprocessor. Participants were blinded to the disinfectant used on the flexible cystoscope prior to use. All patients had a negative mid-stream urine (MSU) at baseline, no symptoms of UTI on the day of investigation, no recent antibiotic use or current indwelling urinary catheter. Patients who underwent a cystoscopic biopsy during the procedure were excluded. MSU analysis before and 3-5 days after, cystoscope and equipment cultures were performed. The Urogenital Distress Inventory (UDI 6+2), AUA and QoL scores were performed before and after cystoscopy, ease-of-use assessments and a full cost analysis were also done.Results: A total of 180 participants were randomized 1:1. The mean age overall was 72.1 years, 17% were females and 57% of procedures were performed for bladder tumor surveillance. The MSU was positive in 5.4% of patients in each group and 29% (Tristel) vs. 20% (Cidex) of patients had urinary leucocyturia (p=ns) post-procedure. The turnover (minutes per cycle) was 7.5 (Tristel) vs 26.7 (Cidex). The cost per disinfection was USD11.2 (Tristel) vs. USD75.8 with fixed costs of USD4,553 (Tristel) vs USD57,543 (Cidex).Conclusions: Tristel Fuse appears to be more cost-effective than Cidex OPA for high-level disinfection of flexible cystoscopes.
Tauranga Hospital, Tauranga, New Zealand
A novel urine test which quantifies 5 RNA transcripts (using multiplex qRT-PCR technology) was studied in a multi-center prospective clinical trial. A linear regression algorithm was used to generate a single patient score from the data which was compared to voided cytology and both the NMP22 BladderChek and NMP22 ELISA assays. This preliminary study comprised 467(56 with TCC) patients presenting with gross haematuria. The assay had an overall sensitivity of 84% for TCC at a prescribed specificity of 85%.100% of stage T1, T2 and Tis tumours, 77% of Ta tumours and 96% of all high grade tumours were detected.
MP15: Prostate, Minimally Invasive Therapy/New Technology/Imaging 1
Harlachinger Krebshilfe e.V. am Klinikum Harlaching, Muenchen, Germany
INTRODUCTION: 146 PCa patients (T3-4,N0,M0)were treated since 2001 with TURP & HIFU. Efficacy and side effects were analyzed during a max. follow up of 9 years. METHODS: Only patients without previous androgen deprivation therapy (ADT) were included in this prospective, monocentric study. Three groups were established: A): initial PSA: below 20(n=89); B): initial PSA: 21-50 (n=39); C): initial PSA more than 50 ng/ml (n=18). Mean follow up was 3 years (0.3-9), staging: T3: 90%, T4: 10%, age: 70 (49-84). Mean initial PSA was 26.5 ng/ml (0.6-211). mean PSA at HIFU was 12.4 ng/ml (0-131). Short term ADT less than 3 months in 38% (62% had no ADT at all). Single HIFU treatments with mean 662 HIFU lesions applied in 111 min. After HIFU ADT was discontinued.RESULTS: mean follow up time 36 (4.4-108) months. Median PSA Nadir: 0.28 ng/ml, time to Nadir: 2.5 months. Last PSA 1.1ng/ml: of those were 77% below 10 ng/ml and 5% more than 50 ng/ml. Last PSA after 2 years was in 93 % still below initial PSA levels. Median PSA velocity was 0.26 ng/ml/year: A): 0.14, B): 0.5, C): 0.93 ng/ml. Follow up period without ADT: 95.9%.CONCLUSION: TURP & HIFU ablation in this T3-4,N0,M0 PCa cohort of 146 patients resulted in a PSA Nadir of 0.28 ng/ml and a median PSA velocity of 0.26 ng/ml/year. Until a mean follow up of 3 years 96 % of the patients remained without ADT .Source of Funding: Harlachinger Krebshilfe e.V. and Lingen foundation.
Harlachinger Krebshilfe e.V. am Klinikum Harlaching, Muenchen-Germany
INTRODUCTION: Earlier onset of androgen deprivation therapy (ADT) and longer overall patient survival lead to an increase of patients with biochemical PSA relapse under ADT. In this prospective monocentric study the effect of early local tumor ablation of castration refractory prostate cancer (CrPCa) with HIFU was analyzed. MATERIAL & METHOD: 56 patients with locally, non-metastasized, biopsy proven PCa with triple PSA increase under permanent (min. 2 years) ADT were included in the study: median age was 74 (55-88). Staging: T2: 29%, T3-4: 71%; median Gleason: 7.5 (4-9); N0/M0; Permanent ADT before: 5.1 years; median PSA at HIFU 13.8 ng/ml. Robotic HIFU after TURP was performed under spinal anaesthesia in one session using Ablatherm (EDAP-TMS, Lyon) at 3 MHz. Efficacy and side effects have been analyzed with a follow-up of max. 9.5 years. RESULTS: Efficacy: median PSA Nadir: 0.9 (0-69) ng/ml: of those 71% less than 4ng/ml and 10% less than 20mg/ml. Time to Nadir (months):median 1.7(0.3-8.6). median PSA reduction was 84%. Mean follow up time was 26 months; lLast PSA:median 4.9 ng/ml. Survival rate was 66% at a mean time of 27 months. 34% of the patients died during follow-up: 11% were PCa related, 18% not PCa related, 5% unknown. CONCLUSION: TURP & HIFU in CrPCa reduced PSA by 84% and resulted in a median PSA velocity of 2.95 ng/ml/year. 1/3 did not receive further ADT. 2/3 of the patients were still alive after a follow up of 2 years and had a PSA below PSA at treatment onset.
High Intensity Focused Ultrasound (HIFU) Allows Control of Unilateral Prostate Cancer: Pilot Study with two Years of Median Follow-UP.
Early detection of prostate cancer (PCa), yields 15% of unilateral disease also detected by 3T multimodal MRI. HIFU thermo-ablation is accepted as valid alternative to standard therapies. Since 2007, 32 patients bearing unilateral PCa, shown by Ultrasound guided biopsies and 3T MRI, were selected for HIFU hemi-ablation with Ablatherm of EDAP company. In one procedure, under spinal anaesthesia, HIFU thermoablation combines with ipsilateral TUR to avoid acute retention and sloughing. Median age of patients, gleason and PSA are 71 years, score 6 and 5.7ng/ml respectively. The treated volume is 58.8% of 29.5cc median prostatic volume. Median 3 months PSA nadir is 0,92ng/ml. Phoenix criteria (nadir + 2) indicated four rebiopsies; localized PCa of non treated area was found in 2/4. PCa progression within six months, occurred in two understaged patients.With 25 months median follow-up, 28/32 patients show no evidence of disease (87.5%). Two cases (6%) showed transient grade I incontinence. Potency is preserved in 6/8 patients without previous dysfunction. Low and intermediate risk PCa with small volume and unilateral index lesion, assessed by biopsies and by multimodal MRI, can be adequately destroyed by HIFU. Thereafter active surveillance monitorizes PSA after an individual 3 months nadir taken as reference for new biopsies.Zonal HIFU allows local control of unilateral PCa, avoiding costs and side effects of standard treatments, delaying the expenses of chronic ADT; it minimizes specific side effects of HIFU, respects continence in all patients and potency when present. These encouraging results deserve larger prospective studies.
Department of Urology, Teikyo University, Schoo; of Medicine, Tokyo, Japan
Introduction: HIFU is an emerging treatment for patients with localized prostate cancer. Purpose: To investigate the parameters that predict local recurrence or residual disease after HIFU therapy for localized prostate cancer. Materials and Methods: This study included 61 patients with histologically and clinically confirmed localized prostate cancer who underwent HIFU using the Sonablate™ 500 (Focus Surgery, Indianapolis, IN, USA) as primary therapy. The median post-HIFU follow-up period was 52 months (range, 9-76 months). Prostate-specific antigen (PSA) and its derivatives were measured before and after HIFU. Patients underwent prostate biopsy at 6, 12, and 24 months after HIFU. 1H-MRS was conducted prior to the biopsy procedure, and any region in which the [choline + creatine]/citrate ratio was greater than 1.07 was considered positive for cancer. Logistical analysis was performed using clinical and pathological parameters to predict the positive biopsies. Results: The rate of negative biopsy after HIFU therapy was 81.0%, and the rate of negative 1H-MRS was 66.7%. Chi-square test showed that pre- and post-HIFU PSA levels, PSA velocity, treatment outcome as assessed by Phoenix/ASTRO criteria, and positive 1H-MRS were significant parameters for predicting positive biopsies. Multivariable logistic regression analysis using these five significant parameters demonstrated that positive 1H-MRS was the only significant predictive factor for positive biopsies (X2=6.847, p=0.009). Conclusions: 1H-MRS is a useful noninvasive diagnostic modality to evaluate recurrence or residual disease after HIFU.
Harlachinger Krebshilfe e.V. am Klinikum Harlaching, Muenchen-Germany
INTRODUCTION: PSA Nadir is a strong surrogat parameter for success after HIFU therapy of localized prostatic cancer (PCa). Three therapeutic options are available in HIFU therapy: HIFU only, TURP and HIFU in one session, and TURP one month before HIFU. We compared these different strategies in regarding their influence on PSA Nadir. MATERIAL & METHOD: The prospective Harlaching HIFU Database (n=2.300, since1996) was used as data source for analysis. 3 patient cohorts (T1-2, N0, M0)were analyzed: A)1998-2000 (treatment with HIFU only), B) 2001-2004: (treatment with TURP & HIFU), C) 2005-2010: (treatment with TURP 1 month before HIFU),evaluable T1-T2 patients for group A:153 / B:312 / C:212, none of the patients had any pretreatment. We analyzed prostate volume and PSA at diagnosis before TURP/HIFU and after HIFU therapy. RESULTS: Prostate volume (cc) median in group A:19 / B:35 / C:37. PSA at diagnosis (median)group A:10 / B:8 / C:7,1.Resected volume in group A:0% / B:40% / C:49%. Prostate volume at HIFU in group A:19 / B:21 / C:19.5. PSA at HIFU (median)in group A:6 / B:5.9 / C:5.4. PSA Nadir (median)in group A:0.8 / B:0.06 / C:0.06. Prostate volume final (cc)(3 months after HIFU treatment), group A:10 / B:7 / C:5. CONCLUSION: Minor PSA decrease before HIFU is caused by debulcking TURP. PSA Nadir below 0.1 ng/ml in HIFU monotherapy shows the efficacy of HIFU at 3 MHz. Further decrease of PSA Nadir in cohorts B and C is caused by radically debulcking TURP and development in HIFU technology. Besides that there was a significant decrease in side effects in these two groups.
The Institut Montsouris
Introduction & purpose.To report long term oncologic outcome of HIFU-Ablatherm in patients with localized prostate cancer with more than five years of follow-up.Material & Methods.From January 1996 to October 2010, 528 patients with localized PCA have been treated in our institution. Out of these, 260 have achieved more than five years follow-up and were considered in this study. Recurrence defined as PSA nadir + 2 (Phoenix definition) or positive biopsies or secondary treatment patterns. Disease-free survival (DFS) was estimated with Kaplan-Meier curves.Results. We identified 255 patients with more than 5 years of follow-up. The mean follow-up was 7.2 years(12.3 years). The median age at time of treatment was 73 years(51-84), median PSA 7,7 ng/ml(1.1-44), median prostate volume 37g(15-70) and median Gleason score 6 (6-9). Stratification according to DAmicos risk group was low, intermediate, and high in 117(46%), 128(50%) and 10(4%) of patients, respectively. The median PSA nadir was 0,8 ng/ml(0-45) with a median time to nadir of 11.4 weeks(0.1-26.1). Control biopsies were available in 143(56%) patients within 1 year of HIFU therapy and 79(55%) were reported as negative at 12 months. Recurrence free survival rate at 5 yr was 73%. Secondary therapy free survival rates were 84%, 72%, and 45%(p=0.001) for low-, intermediate-, and high-risk patients, respectively. 43 (17%) patients received re -treatment with HIFU. Ninety percent of patients presented with grade 1 complications (dysuria).Conclusions. Adequate local control and recurrence free survival achieved with HIFU at a long term follow-up are circumscribed for low risk patients.
The Department of Urology, Tokai University Hachioji Hospital, Hachioji, Japan
Objective: To report on the long-term results of high-intensity focused ultrasound (HIFU) in the treatment of localized prostate cancer.Materials and Methods: Seven hundred and fifty-three men with stage T1c-T3N0M0 prostate cancer treated with Sonablate® (SB) devices were included. All patients were followed for more than 2 years. The patients were divided into two groups: in the Former group, 421 patients were treated with SB200 and 500 from 1990 to 2005; in the Latter group, 332 patients were treated with SB 500 ver. 4 and TCM from 2005 to 2009. Biochemical failure was defined according to the Phoenix definition (PSA nadir + 2 ng/ml). Results: The mean age, PSA and follow-up period in the Former and Latter groups were 68 and 67 years, 11.3 and 9.7 ng/ml, and 49 and 38 months, respectively.The biochemical disease-free rate (BDFR) in the groups at 5 years was, respectively, 67% and 53%, and was 50% at 10 years in the Former group (p<0.0001). The BDFR in patients in the low-, intermediate-, and high-risk groups in the Former group at 10 years were 48%, and 43% and 40%, respectively (p<0.0001). The BDFR in patients in the low-, intermediate-, and high-risk groups in the Latter group at 5 years were 83%, 76%, and 42% (p<0.0001). The negative prostate biopsy rate in the Former and Latter groups was 81% and 93%, respectively.Conclusions: HIFU therapy appears to be minimally invasive, efficacious, and safe for patients with localized prostate cancer, particularly those with low- and intermediate-risk cancer.
The Correlation Between Clinical Outcomes and Some Parameters in Patients with Localized Prostate Cancer after High-Intensity Focused Ultrasound Treatment
ABSTRACT WITHDRAWN
“Regina Elena” National Cancer Institute of Rome
Introduction: We report results of a single-centre preliminary experience with salvage cryoablation for radio-recurrent prostate cancer. Materials and Methods: Between January 2009 and January 2011 24 consecutive patients with local recurrent prostate cancer (positive biopsy and negative imaging underwent cryoablation. Kaplan-Meier analysis was performed with biochemical failure and with local recurrence.Results: Data from 24 patients with a minimum follow-up of 6 months were analyzed. Median patient age was 73 years (IQR 70-76).Seventeen patients had increasing PSA levels before treatment and none of these discontinued treatment after cryoablation.Pretreatment median PSA level was 4.11 ng/mL (IQR 1.33-5) in patients not receiving androgen deprivation treatment (ADT) and 3.13ng/mL (IQR 1.13-6.11) in patients receiving ADT. Mean Gleason score in patients not receiving ADT was 7.4 (range 6-9). According to Phoenix criteria 24-mo biochemical recurrence free survival (BRFS) rate was 56%, while 21-month BRFS rate was 65.6% in patients without ADT and 57.6 in patients receiving ADT. According to ASTRO criteria 24-mo BRFS rate was 53.6%, while 21-mo BRFS rate was 80% in patients without ADT and 60% in patients receiving ADT. Local recurrence was proved by biopsy in 2 out of 6 patients. The incontinence rate was 20%. The rectal fistula rate was 4% and 12.5% of patients underwent TURP to remove sloughed tissue.Conclusions: Salvage cryoablation is an effective treatment for locally recurrent disease, but the risk of nodal metastasis in patients with increasing PSA levels receiving ADT despite preoperative negative imaging may be underestimated.
Focal Therapy of Prostate Cancer: Initial Experience with Cryotherapy.
Objective: To assess outcomes of cryotherapy for focal treatment (CFT) in prostatic carcinoma (PCa).Methods: Prospective study in patients with localized-PCa. Inclusion criteria: PSA less than 10ng/ml, clinical-stage less than T2c, prostatic biopsy(PB) with at least 20-cores harboring only unilateral invasion with less than 33% involvement of the PB and/or less than 50% of the length of BP; absence of Gleason grades 4-5 and MRI findings excluding extraprostatic disease. Treatment was deployed under echo-guided monitoring with transperineal needle placement on the affected lobe: two freezing cycles interspersed with 2 passive warming cycles. Post-operative PSA, IPSS, IIEF5 and complications were assessed at 3, 6 and 12 months. MRI and systematic biopsies were performed at 12 months post-operation. Criteria for failure were the presence of cancer on control PB in the treated area and/or biological recurrence (Phoenix criteria).Results: From April-2009 to April-2010, 30 patients, mean age 66 years(52-77) were treated (right:17cases;left:13cases). Preoperative characteristics: mean PSA=6.6ng/ml(3.1-9.8, mean prostate volume=51gr(29-104). Mean IPSS was 10(2-21) and mean IIEF5=14(1-24). Postoperatively, mean PSA at 3, 6 and 12 months were 3.3ng/ml, 4.2ng/ml and 3.4ng/ml, respectively. Treatment-related complications: urinary acute retention: 5 cases(16%) and perineal hematoma: 11 cases(36%). At one year of follow-up, PB were positive on the side treated in 6 cases(20%) and in 3 cases(10%) contralaterally. Biochemical recurrence was verified in 4 cases(13%). At a 3 Months of follow-up, mean IPSS was 8 (2-20) and mean IIEF5 was 11(0-24).Conclusion: CFT for localized-PCa seems an aceptable treatment with limited morbidity in selected population.
USC Institute of Urology, Keck School of Medicine, University of Southern California Los Angeles, California, USA.
PURPOSE: We report 8 years experience of oncologic and functional outcomes with primary focal cryotherapy for prostate cancer. METHODS: Over an 8 years period (09/2002 to 10/2010), prostate focal cryoablation was performed in 75 carefully-selected men with unilateral low-intermediate risk cancer. All patients underwent re-biopsy at entry with sextant protocol plus Doppler US-targeted biopsy. Median age was 64 yrs, PSA 5.8 ng/ml, prostate volume 38 cc. Percentage of cancer cores of index lesion was 40% (3-95), and Gleason score 6 (n=30; 40%) or 7 (n=45, 60%). Follow-up comprised PSA (3-6 monthly), follow-up biopsy (6 or 12 months, and then, yearly or indicated), and validated questionnaires. RESULTS: Median follow-up is 3.6 years (1-8). To date, among the followed-up 71 men, no patient died or developed metastases. Positive biopsies in follow-up: treated lobe (n=1; 1.8%), untreated lobe (n=11; 20%). Of the 12 men with positive biopsies, 75% (9/12) were followed with active surveillance (n=7) or repeat focal cryoablation (n=2); 2 progressed to radical therapy and 1 had hormonal therapy. PSA kinetics at 3, 6, 12, 24, and 36 months: Mean PSA were 1.4, 2.0, 2.0, 2.8, and 1.3 ng/ml, and 1.7, 1.9, 2.5, 2.7, and 2.5 ng/ml, in men with positive and negative biopsy, respectively. 1 year functional data: Continence rate: 100%. Sexual intercourse rate: 86% in pre-operatively potent men. CONCLUSIONS: 75 selected patients underwent primary focal cryoablation of low-intermediate risk unilateral prostate cancer, diagnosed by sextant plus Doppler-targeted biopsy. At up to 8 years following, oncologic and functional outcomes were encouraging.
Department of Urology, Singapore General Hospital, Singapore
Introduction:Active surveillance for low-risk prostate cancer is hindered by substantial drop-out due to fears of under-staging and missed opportunity for cure. An effective treatment with low morbidity commensurate with low risk of the disease is needed. MRI-guided Focus Ultrasound (MRgFUS) involves focal therapy with sonication guided by MR-quality anatomical definition and real-time MR thermometry. We report our initial experience using a transrectal MRgFUS transducer to treat the prostate.
Methods:Patients with untreated low-risk prostate cancers were selected including those with PSA<10 ng/dl, Gleason score <=6, maximum of two lesions<10mm each on mapping biopsy and no contraindications to MR. IRB approval was obtained.
We report on 9 patients treated in Singapore, out of 20 treated in Singapore, Russia, Italy and India. Under regional/general anesthesia, the transrectal probe was inserted. MR localization of targets and background thermometry was performed. The treatment area was planned excluding critical areas from the beam path. Target areas were sonicated under real-time thermometry monitoring. A final contrast-enhanced MR was performed.
Results:All patients experienced minimal discomfort and voided normally the next day. No prolonged retention or significant hematuria was observed. Post-operative IPSS and IIEF returned to base-line within weeks. PSA trended downwards or remained stable. Immediate contrast-enhanced MR demonstrated non-perfused areas corresponding to targeted areas. Interval MR imaging showed initial expansion of the areas followed by shrinkage. The first patient reaching 6 months had a negative repeat biopsy.
Conclusion:Heretofore, the treatment is safe with minimal morbidity. Initial efficacy demonstrated by MR non-perfusion will be further confirmed by biopsy.
University of Michigan, Department of Urology, Ann Arbor, MI, USA
Introduction: Histotripsy is a non-invasive focused ultrasound technology capable of producing a TURP like defect in a canine prostate model. However, the necessity of homogenizing the urethra is unclear. Purpose: We evaluated the local bioeffects following urethral sparing prostate histotripsy. Methods: Histotripsy was performed on 10 canines using a focused 750 kHz piezoelectric ultrasound transducer targeting the prostatic parenchyma while avoiding the urethra. Cystoscopy was performed immediately post-op (POD0) and on POD 3, 7, 14, 28 and 56. Ultrasound surveillance was performed on POD 0, 7, 14, 28, and 56. Four, two, and four subjects were euthanized acutely, at 1 week, and at 8 weeks, respectively, with confirmatory histology. Results: Urethral preservation was successful in 8/10 subjects. Among subjects euthanized at 8 weeks, prostate volume had decreased from 23.3 cc before treatment to 20.4 cc at 8 weeks. Gross examination revealed intact smooth-walled treatment cavities containing simple fluid with minimal cellular debris. Histology demonstrated complete urothelialization of cavities with minimal focal inflammation (see figure). Conclusions: Urethral sparing prostate histotripsy is feasible, resulting in small volume reduction and simple treatment cavities by 8 weeks. Further studies are needed in humans to evaluate the clinical utility of urethral sparing. Funding: NIH K08DK081656

Department of Endoscopic Urology, Russian Medical Academy of Postgraduate Education, Moscow, Russia
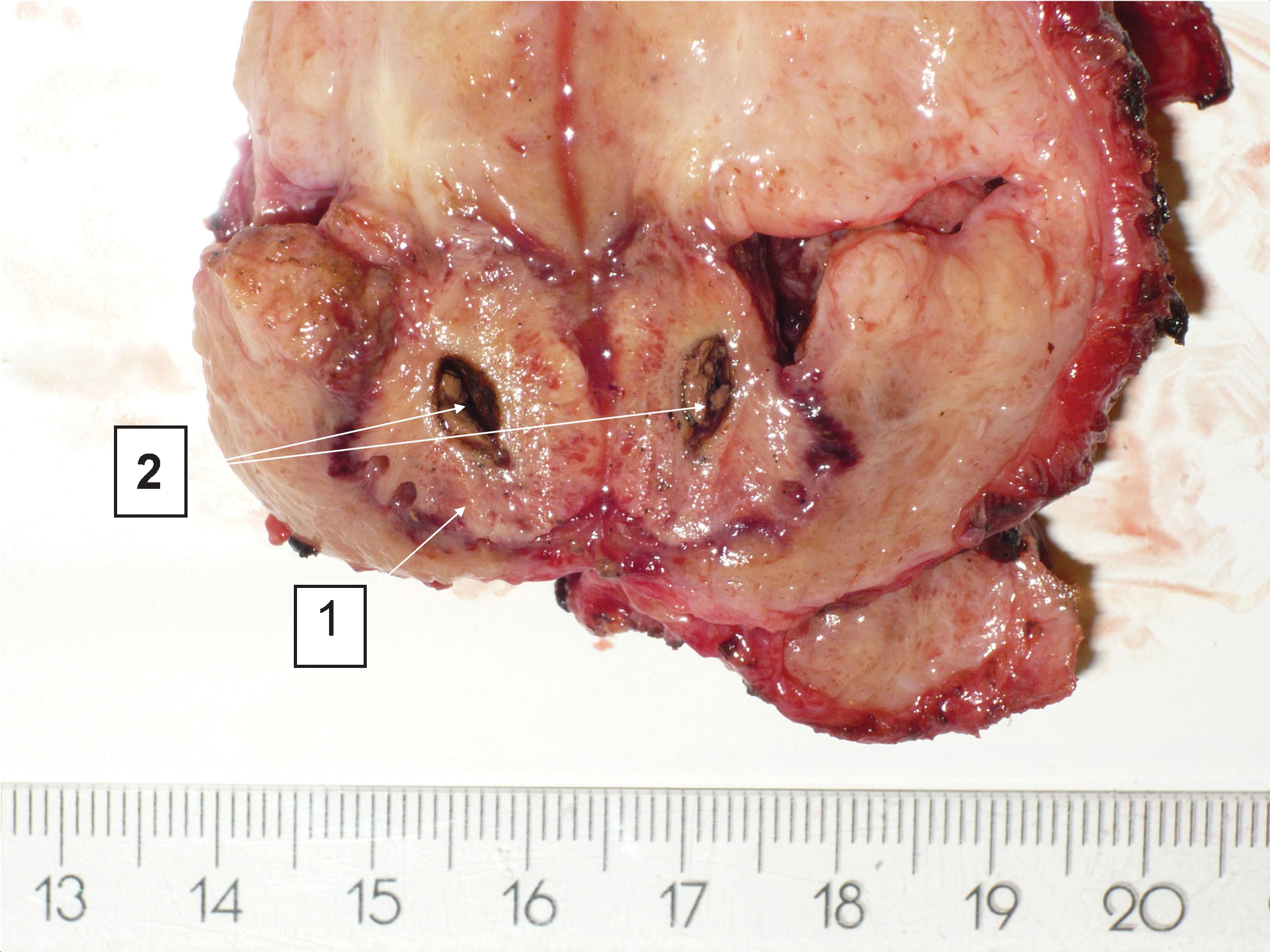
University of Michigan, Department of Urology, Ann Arbor, MI
INTRODUCTION: Histotripsy is a non-invasive, non-thermal, pulsed ultrasound (US) technology that produces targeted mechanical tissue fractionation. Feasibility of histotripsy ablation of normal renal tissue, and renal implanted VX-2 tumor has been previously demonstrated. PURPOSE: To evaluate the metastatic potential following histotripsy treatment of renal implanted VX-2 tumors by quantifying lung tumor metastases.MATERIALS AND METHODS: VX-2 tumor was implanted into 28 New Zealand White rabbits left kidney. Thirteen days following implantation, 20 rabbits were treated with histotripsy while 8 remained as controls. Twenty-four hours post-treatment, all rabbits underwent left nephrectomy. All subjects were euthanized on day 19, and lungs were harvested and processed for histopathologic inspection. Two lung, whole-mount, coronal sections were counted for metastatic foci to calculate total metastases and metastatic density.RESULTS: Viable tumor was present in all 28 implanted rabbits identified on histology. Tumors were localized in 19 of 20 treatment subjects with US prior to treatment. Histology confirmed fractionation of tumor in all treatment rabbits. There was no difference in total lung metastases (p=0.29) or metastatic density (p=0.22) between treatment and control rabbits (88.7 vs. 72.5; 8.9 mets/cm2 vs. 7.0 mets/cm2).CONCLUSIONS: Histotripsy of renal implanted VX-2 using an in-vivo rabbit model did not produce a statistically significant increase in number or density of lung metastasis. Further investigation of histotripsy ablation of solid malignancy is warranted to confirm these initial results using this VX-2 model and in less aggressive tumor models.
Division of Urology, Duke University, Durham, North Carolina, USA
Objectives: The EMS Swiss Lithobreaker is a new, portable, electro-kinetic lithotripter. We compared the tip speed and displacement characteristics of the pneumatic LMA Stonebreaker™ with the Lithobreaker and using in vitro models of percutaneous and ureteroscopic stone fragmentation.
Methods: The probe tip was aligned to occlude a laser beam aimed at a photo detector. Thirty displacement and velocity profiles were measured for 1mm and 2mm probes. For the percutaneous model, 2mm probes fragmented BegoStone phantoms until the fragments passed through a mesh sieve. The number of impulses and time required to clear each stone were recorded. The ureteroscopic model utilized 1mm probes and compared the Stonebreaker, Lithobreaker, and a 200μm laser fiber (Boston Scientific Flexiva™). BegoStone phantoms were placed into silicone tubing to simulate the ureter; clearance was defined as fragments passing by a narrowing in the tubing. Four trials were conducted with each lithotrite.
Results: For both 1mm and 2mm probes, the Lithobreaker had significantly higher tip displacement and slower tip velocity, p<0.01. In the percutaneous model, the Lithobreaker required an average of 484 impulses over 430s to fragment one BegoStone, while the Stonebreaker required an average of 29 impulses over 122s to fragment one stone. Ureteroscopically, the mean clearance time was 157s for the Lithobreaker, 531s for the Stonebreaker, and 253s for the laser.
Conclusion: These findings suggest that the EMS Swiss Lithobreaker may be better suited for treatment of ureteral stones. Further clinical studies are being conducted to assess the utility of this device.
MP16: Robotic/Lap Upper urinary Tract 4
Hackensack University Medical Center
Introduction and Objective:The optimal role for the robot-assisted renal surgery has not been defined. Advances in experience is resulting in an increasing interest in robotic nephron-sparing surgery. We report on a collaborative multi-institutional experience with robot-assisted partial nephrectomy (RAPN) at 25 institutions.Materials and MethodsA retrospective review of all consecutive robot-assisted partial nephrectomies was performed at 25 institutions. Of 33 primary surgeons, 79% had advanced training in minimally invasive/endourology (80%) or urologic oncology (20%) fellowships. Surgeons had a collective experience of more than 2500 laparoscopic partial nephrectomies. Demographic and perioperative data were prospectively collected and analyzed. ResultsA total of 1269 patients that underwent RAPN were evaluated. Mean patient age was 58.5 years (range 20-86) and included 61% men/39% women. Procedures were performed on the left (49%)/right (51%) kidney. Mean operative time was 203 min (range 71-447) and warm ischemia time was 25.2 min (range 6-77. Estimated blood loss was 184 mL (range 5-2800) and the mean hospital stay was 2.6 days (range 1-89). Mean tumor size was 3.1 cm (range 0.5-10) and 96% of the specimens had negative surgical margins. The overall complication rate was 15.7%.ConclusionsRobot-assisted laparoscopic partial nephrectomy is being performed by surgeons with various levels of expertise. The benefits of robotic-assistance for experienced laparoscopic renal surgeons remain to be determined, and selection of the approach for partial nephrectomy is dependent on surgeon comfort. We report on our initial experience and will continue to report our ongoing evaluation with robot-assisted partial nephrectomy.
Complications of Robot-Assisted Partial Nephrectomy: Multi-Institutional Experience from the Robot-Assisted Partial Nephrectomy Integrated Database (Rapid) Study Group
Introduction: Laparoscopic partial nephrectomy (LPN) is underutilized for small renal masses. The introduction of the da Vinci Surgical System has led to an increasing interest in evaluating this technology for LPN. With adoption of this technology, complication rates require assessment. Purpose: We reviewed our multi-institutional experience with robot-assisted partial nephrectomy (RAPN) and report on our complications with adoption of this technology. Materials and Methods: A retrospective review was conducted of robot-assisted partial nephrectommies performed at 25 institutions. Procedures were performed by surgeons with extensive experience in performing laparoscopic and robotic renal surgery. Perioperative complications and management were recorded and analyzed. Complications were classified according to the Clavien classification of surgical complications.Results: Of a total of 1269 patients that underwent RAPN, 51 intraoperative complications and 148 postoperative complications were recorded for an overall complication rate of 15.7%. The most common complication was bleeding or hemorrhage 47 (3.7%). A total of 16 conversions to a pure laparoscopic, hand-assisted laparoscopic, or open approach to partial or radical nephrectomy were recorded for a variety of indications. Complications were directly associated with higher R.E.N.A.L. nephrometry scores.Conclusions: Robot-assisted laparoscopic partial nephrectomy is gaining the attention of novice and advanced laparoscopic surgeons. Advances in robotic technology, such as second and third generation robotic systems, and new robotic instrumentation may facilitate the adoption of RAPN. The early learning curve and more complicated cases may be associated with an increased complication rate. Complications can be successfully managed when recognized in the intraoperative or postoperative setting.
Laparoscopic Partial Nephrectomy. Experience in 130 Cases.
Objectives: Laparoscopic partial nephrectomy (LPN) is one of the treatment for better preservation of renal function compared with radical nephrectomy. We describe recent surgical technique. Material and methods: Between 2001 and 2011, 130 LPN procedures were performed in our institute. Retroperineal or intraperitoneal approach was selected on the dependent of tumor location and size. Our technique for partial nephrectomy involved transient clamping of the renal artery and vein without surface cooling (warm ischemia), followed by cold endoscopic shear excision of the tumor with adequate margins. Control of transected intrarenal blood vessels and pelvicaliceal repair were achieved with an initial central running stitch. Subsequent parenchymal reconstruction involved parenchymal mattress sutures tied over a bolster. Thus, the entire renal repair was performed in the ischemic kidney with the hilar vessels clamped. Polyglycol acid sheet (Neoveil) with fibrin glue (Bolheal ) was used for covering the wound. Results: In all cases, warm ischemia time was 31.2 min and intra operative bleeding loss was 171cc. In recent 36 cases, warm ischemia time was 30.2 min and intra operative bleeding loss was 174cc.Conclusions: We have treated 130 cases of small renal tumor with LPN. With experience these tumors are successfully treated, preserving more renal function with shorter warm ischemia time, while achieving low complication rate and excellent short-term oncologic outcome.
Short Learning Curve of Retroperitoneal Laparoscopic Nephron Sparing Nephrectomy: Single Center Experience with Low Volume of Patients
Introduction: Retroperitoneal laparoscopic nephron-sparing nephrectomy is difficult surgery because of limited working space and demanding techniques.Objective: To evaluate the efficacy of retroperitoneal laparoscopic partial nephrectomy (RPPN) in a single center with low volume of patients.Patients and methods: 86 RPPNs were performed between January 2006 and May 2010. After the three-port retroperitoneoscopic approach was established, the perirenal fatty tissue was circumferentially mobilized by harmonic scalpel. Care should be taken to leave 2-cm-thicness fatty tissue around the tumor. After the renal artery was blocked, the tumor with 0.5 cm normal renal parenchyma around was sheared with scissors laparoscopically. Intermittent suture was performed 0.5-1 cm away from the edge of the incision with absorbable stitch in laparoscopy. The suture of the renal pelvis was recommended when part of it was removed.Results: All of the 86 RPPNs were carried out consecutively and successfully. The mean operation time and warm ischemic time was 141.2 and 25.6 minutes. The mean blood loss was 163.0 ml. No open conversion was required. None of the donors encountered major complication which needed re-operations. With a follow-up period of 3 months to 5 years, 1 of the patients developed impaired renal function and all of them still survived.Conclusions: With a short learning curve, retroperitoneal laparoscopic partial nephrectomy might be a safe and feasible alternative for some well-trained urological surgeons.
Department of urology Academic Medical Center (AMC), University of Amsterdam, Amsterdam (the Netherlands)
Purpose: To assess the efficacy of the barbed suture in partial nephrectomy (PN) in the peri-operative period.Material and Methods: A paired matched comparison between patients who underwent a PN, either open or laparoscopic with and without barbed suture were performed. Cases were matched for PADUA score, approach (laparoscopic or open) and the center where surgery was performed. We enrolled 31 consecutive patients who underwent PN for renal tumors with V-Loc® barbed suture in two clinics in Europe. Perioperative outcomes included warm ischemia time, changes in Hemoglobin (Hb), changes in estimated Glomerular Filtration Rate (eGFR) and perioperative complications (postoperative complications according to Clavien classification). Results were compared with a matched control group of 31 patients that received a conventional parenchyma and capsular suture with Vycril. Results: The number of peri-operative complications was statistically significant lower in the barbed cohort 6.5% versus 22.6% in the non-barbed cohort. Mean ischemia time was 19.6 minutes (SD 7.5) in the barbed suture group vs 21.8 minutes (SD 9.5) in the conventional suture group. There were no significant differences between groups for postoperative changes in creatinine, eGFR and Hb. Limitations of this study include the absence of randomization and the relative small sample size. Conclusions: Barbed suture can be safely used during PN. It reduces significantly the number of perioperative complications. Our study suggests that although not significant some benefit may be gained in terms of warm ischemia time.
Division of Urology, Department of Surgery, Chi Mei Medical Center
Purpose: In recent years, laparoscopic partial nephrectomy has gained popularity in treating benign and malignant renal diseases, and is usually performed via the transperitoneal or retroperitoneal approach. Retroperitoneal laparoscopy, by providing direct access to the retroperitoneal cavity, is an interesting approach to urological surgery. Retroperitoneoscopic surgery has proven advantages in reducing postoperative pain, hospital stay, and early return to work. We report our experience with retroperitoneal laparoscopic partial nephrectomy. Materials and Methods: Between January 2004 and December 2010, 74 renal peripheral masses were performed by retroperitoneal partial nephrectomy in our institute. These patients were placed in the lateral decubitus position and 3 trocars were used. The retroperitoneal working space was created by digital dissection and was completed by insufflation without balloon dissection. En bloc control of the renal artery was achieved with elastic vessel loop to allow cold knife excision of the renal mass and laparoscopic intracoporeal suture to repair collecting system. Results: The average operating time is 92 minutes (range 50 to 180). Average tumor size was 35 mm (range 60 to 15). Average hospital stay was 4.5 days (range 3 to 14). Average blood loss was 200ml (range 50 to 800). Postoperative analgesic requirements were moderate. Conversion to open surgery was not necessary. The median follow-up period is 30 months, there was no tumor recurrence. Conclusion: Retroperitoneoscopic partial nephrectomy has demonstrated to be technically feasible, with low morbidity. The vessel loop is cheap and user friendly. Pedicle control with a simple tool, vessel loop, was an efficacious procedure.
Influence Factors of Postoperative Renal Function over a year period in Laparoscopic Partial Nephrectomy
Purpose To clarifies the influence factors of postoperative renal function over a year period in laparoscopic partial nephrectomy(LPN). Materials and Methods Off the 118 LPNs performed from January 2006 to September 2010, 5 patients by retroperitoneal approach underwent renal surface cooling with the slush ice, and 113 patients by transperitoneal approach underwent retrograde intracavitary cold saline perfusion. For both groups, the LPN was done by occluding renal artery or pedicle with bulldog clamp. The serum creatinine, eGFR(estimated glomerular filtration rate) and d-eGFR=(postoperative-eGFR-preoperative-eGFR)/preoperative-eGFR*100% were evaluated between two groups. As the influence factors to 1 and 12 months postoperative eGFR value, following were analyzed; body mass index, age, hypertension, diabetes, heparin injection, manitol injection, cooling methods, bleeding volume, ischemic time, renal artery vs pedicle clamping, tumor size, and preoperative renal function. The postoperative renal function was also evaluated according to the length of ischemic time. Result The renal function 12 months after surgery was influenced by age, ischemic time and preoperative eGFR value, and 1 month was also affected by the same factors as well as heparin and mannitol injection. There were no significant differences among postoperative renal functions according to the length of ischemic time except d-eGFR value 1 month after surgery. Conclusion The heparin and manitol injection were effective on recovery of renal function in 1 month after surgery. The age, ischemic time and preoperative renal function were important factors influencing renal function over a year period.
Outcomes of Robotic Assisted Partial Nephrectomy (RAPN): Systematic Review and Critical Evaluation
Introduction: Robotic Assisted Partial Nephrectomy (RAPN) is one of the established modes of performing minimally invasive nephron sparing surgery for small renal masses (4 cm or less). With its recent uptake there has been an interest in the outcomes using the robotic platform. Purpose: To critically evaluate the outcomes of RAPN via a systematic review of literature. Material & Methods: We searched MEDLINE, PubMed and the Cochrane Library from January 2006 to June 2011 for results of RPN. Inclusion criteria were all English language articles reporting on more than 50 patients. Data was extracted on the outcomes and complications reported in the literature. Results: A total of 8 studies(4 prospective & 4 retrospective) reported on 1152 patients. The mean age was 60 years(18-88 years) with a male:female ratio of 575:394. The mean operating time, ischemia time, blood loss and hospital stay was 189 min(52-472 min), 22 min(10-53 min), 185 ml(10-2200 ml) and 3.3 days respectively. A positive surgical margin was seen in 28 patients(2.6%, 7 studies). Conversion to open surgery and conventional laparoscopic surgery was in 17 and 3 cases respectively. There were 7(0.6%) intra-op complications (Vascular 3,Bowel tear 1,Splenic tear 1,Liver tear 1 and death from MI 1). There were 99(8.6%) post-op complications including bleeding 28 (2.4%), ileus 5(0.4%), PE/DVT 14(1.2%), urine leak 15(1.3%), pseudoaneurysm 3, not mentioned 15 and other complications were seen in 19 patients. Conclusion: Robotic partial nephrectomy is feasible and safe with outcomes and complications similar to laparoscopic and open partial nephrectomy.
A Comparative Cost Analysis of Robotic-Assisted vs. Traditional Laparoscopic Partial Nephrectomy
Introduction:Robotic-assisted laparoscopic partial nephrectomy is supplanting traditional laparoscopy as the technique of choice for minimally invasive nephron-sparing surgery. This evolution has resulted from potential clinical benefits, as well as proliferation of robotic systems and patient demand for robotic surgery. We sought to quantify the costs associated with use of robotics for minimally invasive partial nephrectomy (MIPN).Methods:A cost analysis was performed for 20 consecutive RPN and LPN patients at our institution from 2009-2010. Data included actual perioperative and hospitalization costs as well as professional fees. Capital costs were estimated using purchase costs and amortization of two robotic systems from 2001-2009, as well as maintenance contract costs. The estimated cost/case was obtained using total robotic surgical volume during this time period. Total estimated costs were compared between groups. A separate analysis was performed assuming "ideal" robotic utilization during a comparable time period.Results:RALPN had a cost premium of + $1066/case compared with LPN, assuming actual robotic utilization from 2001-2009. Assuming "ideal" utilization during a comparable time period, this premium decreased to + $334; capital costs per case decreased from $1907 to $1175. Tumor characteristics, OR time, and length of stay were comparable between groups.Conclusions:RALPN is associated with a small-moderate cost premium depending on assumptions regarding robotic surgical volume. Saturated utilization of robotic systems decreases attributable capital costs, and makes comparison with laparoscopy more favorable. Purported clinical benefits of RPN (e.g. decreased warm ischemia time, increased utilization of nephron-sparing surgery) require further study and may have cost implications.
Partial Nephrectomy for Clinical T1 Renal Tumors: Comparison of Intermediate Outcomes of 284 Robotic, Laparoscopic and Open Approaches
PURPOSE: To compare the surgical outcomes of open, laparoscopic, and robotic partial nephrectomy of T1 renal tumors.METHODS: After Institutional Review Board approval, a retrospective chart review was performed for 284 patients who underwent partial nephrectomy at Tulane Medical Center between 1999 and 2011 (31 open, 148 laparoscopic, and 105 robotic). Age, sex, race, tumor side, tumor size, operative time, blood loss, ischemia time, pathologic grade and stage, and hospital stay were compared. RESULTS: Open, laparoscopic, and robotic groups were comparable regarding age, sex, tumor size, and tumor side. Operative time and blood loss were significantly higher in open group compared to laparoscopic and robotic groups. Ischemia time (19.5 min) and length of stay (2.4 days) in robotic group was significantly lower than open and laparoscopic groups (30.0 and 37.7 min, 4.2 and 3.7 days, respectively. Surgical margins were positive in 8/148 (5.4%) patients in laparoscopic group, 1/31 (3.2%) in open group, and 6/105 (5.7%) in robotic group (p=0.04). In follow-up, (range 6-96 months), no patient with positive surgical margin developed recurrence. Final pathology demonstrated renal cell carcinoma in 83.3%, benign disease (angiomyolipoma, oncocytoma) in 11.1%, and cystic disease in 5.6%. Pathologic nuclear Fuhrman grade in renal cell carcinoma patients were: grade 1 (12.3%), grade 2 (71%), grade 3 (15.2%), and grade 4 (1.5%). CONCLUSION: Robotic partial nephrectomy had shorter ischemia times and length of stay compared to open and laparoscopic approaches. Robotic assisted and laparoscopic partial nephrectomies have shorter operative times and blood loss compared to open partial nephrectomies.
Urology Department, Acibadem University, Istanbul, Turkey
Introduction: Robot-assisted partial nephrectomy (RAPN) is a promising, minimally-invasive method for treatment of small renal masses. The technique necessitates completion of a learning curve for optimal results.Purpose: To evaluate the effect of learning curve on perioperative parameters in robotic partial nephrectomy patients.Materials and Methods: Between April 2008 and May 2011 32 patients underwent RAPN operation at our institution by a single surgeon with extensive prior robotic experience. Perioperative parameters of the initial 16 patients (group-I) were compared with the last 16 patients (group-II). Transperitoneal approach was used in all patients.Results: The mean pathological tumor size was 31.8 (12-52) cm. The mean operative and warm ischemia time was 161 and 24 minutes in group I and 132 and 20 minutes in group-II, respectively. Estimated blood loss was 262 ml in group-I and 153 ml in group-II. Histopathological examination revealed renal cell carcinoma in 14 patients in group-I while all patients had renal cell carcinoma in group-II. There were 1 oncocytoma and 1 calcified benign lesion in group-I. No patients had positive surgical margins in both groups. There were two Clavien grade III and one grade I complications in group-I and one Clavien grade-II complication in group II. The patient with Clavien grade II complication in group II had 2 units of blood transfusions.Conclusions: Completion of the learning curve provides optimal perioperative results in RAPN operations. Prior robotic experience enables a more secure learning curve.
Routine Surgical Drain Placement is Unnecessary in Patients Undergoing Robotic Partial Nephrectomy
Introduction: Routine drainage of the surgical site is the standard of care following partial nephrectomy for solid renal masses by any approach in order to drain any urine leak or hemorrhage. Robotic partial nephrectomy (RPN) offers the potential of decreased blood loss, improved vision and a meticulous renorrhaphy compared to open or conventional laparoscopic approaches potentially eliminating the need for drain placement following repair.Purpose: Here we evaluate the safety and feasibility of drainless RPN.Materials and Methods: Following institutional review board approval we reviewed the charts of all patients undergoing robotic partial nephrectomy at our institution from August 2008 until September 2010. All patients underwent robotic partial nephrectomy using a 3 or 4 arm approach with the daVinci Surgical System (Intuitive Surgical, Sunnyvale, CA). Collecting system entry was repaired primarily and renorrhaphy was performed using a sliding hem-o-lok technique. All patients had abdominal imaging between 6 weeks and 3 months postoperatively.Results: 73 patients underwent RPN. Mean patient age, tumor size, warm ischemia time, BMI and length of stay were 58 years, 2.8 cm, 30.1 and 2.4 days. 23 patients received formal collecting system repair. Surgical drains were placed in 10 of the first 18 patients initial patients and then this process ceased. There were no clinically detectable postoperative urine leaks or hemorrhages.Conclusions: Routine drainage of the surgical bed is unnecessary in patients undergoing RPN. Decreasing drain usage may lead to less postoperative pain and shorter hospitalization.
Clinical Pathway for Discharge on Postoperative Day one After Robotic Partial Nephrectomy
INTRODUCTION: A potential benefit of minimally-invasive surgery is reduced hospitalization, but published lengths of stay after robotic partial nephrectomy (RPN) have not been significantly less than after open surgery. OBJECTIVE: We use a clinical pathway targeting discharge on postoperative day (POD) one after RPN and analyzed results. METHODS: We reviewed all RPN by a single surgeon (RA) since beginning our clinical pathway. The pathway comprises ambulation and clear liquids the night of surgery. Intravenous narcotics are avoided. No stent is used and closed suction drains are avoided. The Foley catheter is removed and regular diet started POD#1 before discharge. The pathway was not modified regardless of complexity of RPN. RESULTS: A total of 113 RPNs were performed in 104 consecutive patients. Two had solitary kidneys, and seven underwent multiple (2-4) RPNs. Mean tumor size was 3.4cm (1.6-9.8cm). All were performed transperitoneally with 18 hilar tumors, 10 with segmental artery clamping, 21 off-clamp, and 41 with early unclamping. Warm ischemia time was 12.1min (0-30.0min). Mean preoperative and discharge creatinine were 0.89mg/dL (0.43-2.79) and 1.14mg/dL (0.57-2.93). All patients ambulated POD#0, and none required IV narcotics. A JP drain was avoided in 96 (92%) with only 2/104 (2%) experiencing minor urine leaks. Only 2 (1.9%) required transfusion. Ninety-eight (94%) were discharged on POD#1, of which only 6 (6%) were readmitted within 30d. CONCLUSIONS: Discharge on POD#1 is feasible in most RPN patients. Readmission rate was low, indicating that longer admissions may not prevent complications when patients meeting discharge criteria go home on POD#1.
Complications in a Single Surgeon Series of Surgeon Controlled Robotic Partial Nephrectomy
Introduction: Surgeon controlled robotic partial nephrectomy (RPN) has become an increasingly popular management option for patients with small renal masses. As this technology has disseminated from the academic centers to other institutions, the expected complications and management of these should be described. Purpose: To identify common surgical and medical complications of patients undergoing RPN. Materials and Methods: We queried a prospectively maintained institutional review board approved database of 160 patients who underwent RPN by a single surgeon between March 2008 and June 2011 to identified all patients who deviated from routine postoperative course (Discharge post op day two from surgical floor) within 30 days of surgery. Complications were graded according to the Clavien classification and divided into either surgically related or medical complications. Results: Overall, 33(21%) of patients had any complication. The majority of these were minor complications (19 Clavien I/II) and none had any significant sequelae. 6(4%) major medical complications occurred, all of which required ICU monitoring and were mostly cardiac related(4). All of these patients had significant cardiac comorbidities preoperatively. 8(5%) were major surgical complications which required bladder clot evacuation(2), angioembolization of bleeding renal vessel(2), percutaneous drain placement(2), thoracostomy placement(1).Conclusions: RPN can be performed safely in patients small renal masses with small masses. While some major complications do occur, most complications occurring from this procedure are minor and do not have long term adverse patient consequences.
Prediction of Complications Using Published Scoring Systems for Patients Undergoing Surgeon Controlled Robotic Partial Nephrectomy
Introduction: Surgeon controlled robotic partial nephrectomy(RPN) has become an increasingly popular management option for patients with small renal masses. Several scoring for grading renal masses and potential perioperative complications have been proposed however these have not been validated in multi-institutional trials. Purpose: To evaluate previously published renal mass scoring systems and their ability to predict adverse perioperative outcomes.Materials and Methods: We queried a prospectively maintained institutional review board approved database of 160 patients who underwent RPN by a single surgeon between March 2008 and June 2011 to identified all patients who deviated from routine postoperative course(Discharge post op day two from surgical floor)within 30 days of surgery. Complications were graded according to the Clavien classification. Nephrometry and PADUA scores were graded and differentiated into low, medium or high risk based on publications. Results: 15 patients could not have scoring performed. Overall, 33(21%)of patients had any complication. The majority of these were minor complications(19 Clavien I/II) and none had any significant sequelae. Table 1 outlines complications based on scored groupings. No values were statistically significant in comparing cohorts.Conclusions: Nephrometry or PADUA scoring did not increase ability to identify patients at risk for adverse perioperative events in the present series.

Clamp Versus Unclamped Robotic Partial Nephrectomy.
Purpose: To compare peri-operative outcomes between clamped and unclamped robotic partial nephrectomy (RPN). Patients and Methods: We analyzed data on 21 patients undergoing unclamped RPN and compared to 21 patients undergoing clamped RPN that were matched for tumor size and baseline estimated glomerular filtration rate (eGFR). Our technique of unclamped RPN included renovascular micro-dissection and superselective neurosurgical micro-bulldogs clamp of specific feeding tumor vessels. For RPN clamped, the hilar clamping included artery alone or artery and vein (en block) clamp. Results: Both groups were matched in terms of age (62.2 vs 59.6 years, p=0.4), tumor size (2.9 vs 3.4 cm, p=0.06), C-index (2.8 vs 2, p=0.06), R.E.N.A.L. score (6.8 vs 7.8, p=0.12), and baseline serum creatinine (SCr) (0.9 vs 1.1, p=0.13) for clamp vs unclamp, respectvely. There were no conversions to open surgery or radical nephrectomy. Mean operating time was 254 vs 291 minutes (p=0.12), estimated blood loss was 195 vs 239 ml (p=0.22) and warm ischemia time was 18 vs zero minute (p=0.0001) for clamped and unclamped RPN, respectively. There were 2 complications in each group. Postoperatively, mean SCr and eGFR were 0.9 vs 1.2, p=0.14 and 83 vs 67, p=0.32 for clamp vs unclamp RPN, respectively. All tumor margins were negatives. Conclusions: Unclamped RPN is safe and feasible. A matched comparison with early unclamping reveals equivalent operative time, blood loss and complication rates. Even though there was no renal function advantage in this small retrospective comparison, it removes warm ischemia as a contributing factor in postoperative renal dysfunction.

Comparison of Selective Arterial Clamping and Non-Arterial Clamping: Results from the Robot-Assisted Partial Nephrectomy Integrated Database (Rapid) Study Group
Introduction and Objectives:During partial nephrectomy, selective arterial clamping or performing the procedure without arterial clamping can offer a renoprotective effect by reducing warm ischemia time. We describe the outcomes of a multi-institutional series of patients undergoing robot-assisted partial nephrectomy (RAPN) with either selective arterial clamping or without arterial clamping.Methods:A collaborative multi-institutional database of prospectively collected data from 23 institutions was reviewed. Patients undergoing RAPN with selective arterial clamping or without arterial clamping were identified. The operative variables and perioperative outcomes were assessed. Results:A total of 108 (11.1%) of 970 consecutive robot-assisted partial neprhectomies were performed without arterial clamping or selective arterial clamping. Total arterial clamping was not required in any of the non-arterial or selective arterial clamping procedures. In the non-arterial clamping (n=83)/selective arterial clamping (n=25)/total arterial clamping (n=862) groups, the clamp time (min) was 0/18.6/26.3 respectively. The mean tumor size (cm) was 2.8/2.6/2.9, mean operative time (min) was 179/183/201, estimated blood loss (mL) was 210/242/216, and final pathology positive margin rates were 2.4%/4%/4.6% respectively. These values were not statistically significant. Bleeding complications in the three groups were 4.8%/0%/1.7%.Conclusions:Robot-assisted laparoscopic partial nephrectomy with selective arterial clamping or without arterial clamping is feasible. The bleeding complication rate was highest in the non-arterial clamping group, however the positive margin rate is not significantly higher than in patients undergoing RAPN with selective or total arterial clamping.
MP17: Robotic/Lap Prostate 3
Comparison of Imaging Studies Following Transperitoneal and Extraperitoneal Prostatectomy
Introduction: The rates of abdominal imaging following a transperitoneal radical prostatectomy (RP) or extraperitoneal RP procedure are unknown. Purpose: To investigate the rates of abdominal imaging and subsequent interventions following transperitoneal or extraperitoneal RP modalities. Materials and Methods: The Johns Hopkins RP Database was queried for patients who had undergone Robotic-assisted laparoscopic radical prostatectomy (RALRP), radical retropubic prostatectomy (RRP), and extraperitoneal laparoscopic radical prostatectomy (LRP). Using a prior pilot study which demonstrated a 7% rate of abdominal imaging (CT or x-ray) within 30 days of RALRP, 250 trans- and extraperitoneal patients were needed to detect a 3.5% difference in abdominal imaging based on modality. Appropriate comparative tests including ANOVA were used to determine differences in rates of abdominal imaging among groups.Results: 257 RALRP, 257 RRP and 194 consecutive LRP were identified working backward since March, 2011. 36 patients underwent imaging studies: 10 (3.9%) RRP, 19 (7.4%) RALRP, and 7 (3.6%) LRP. A total of 33 CT and 80 AXR, with the average day of first image 7 days post-operatively (range 0-30). Patients undergoing RALRP had a greater incidence of imaging when compared to extraperitoneal LRP and RRP (p=0.03). The most common finding on imaging was ileus or bowel obstructive patterns in 15 patients, 8 vesicourethral anastamotic leaks, one large pelvic hematoma and 13 patients had findings consistent with normal post surgical changes. Conclusions: RALRP is associated with an increased rate of abdominal imaging within 30 days of surgery when compared to extraperitoneal approaches.
Department of Urology, New York Presbyterian Hospital, Weill Cornell Medical College, New York, USA
INTRODUCTION AND OBJECTIVES: Extraprostatic extension (EPE; pT3a disease) and seminal vesicle invasion (SVI; pT3b disease) are established features of biologically aggressive prostate cancer. We compared the oncologic effectiveness of ORP versus LRP versus RARP in a large international, multicenter cohort of pT3 patients.
METHODS: 22,403 patients with prostate cancer underwent ORP (n=10,092), LRP (n=7,873), or RARP (n=4,438) from January 2000 onwardsin 15 institutions by 40 surgeons. 4,712 (21%) patients had EPE and 1,722 (7.7%) had SVI on final pathology. The BCR rates of ORP, LRP, and RARP were compared and multivariable Cox proportional hazard regression analysis was performed to identify independent predictors of BCR.
RESULTS: In the pT3a group, 73.3% of ORP patients remained free of BCR compared to 78.1% of LRP and 91.2% of RARP patients. Multivariable Cox proportional hazard regression analysis identified peroperative PSA, surgical margin positivity, RP Gleason sum 7, RP Gleason sum ≥ 8, and RARP as independent predictors of BCR (1.02, 1.53, 2.03, 4.97, 0.56). In the pT3b group, 42.9% ORP patients remained free of BCR as compared to 52.5% of LRP and 79.5% of RARP patients. Multivariable Cox proportional hazard regression analysis identified preoperative PSA, surgical margin positivity, RP Gleason sum ≥ 8, LRP, and RALP as independent predictors of BCR (1.00, 1.63, 2.50, 1.22, 0.61).
CONCLUSIONS: RARP appears at least non-inferior to ORP and LRP in the management of men with pT3a or T3b prostate cancer.
Advantage of Barbed Sutures for Vesico-Urethral Anastomosis during Da-Vinci Radical Prostatectomy
Introduction:During Da Vinci radical prostatectomy (PRDV), urethro-vesical anastomosis is performed with running sutures whose tension needs to be constant to achieve a waterproof reconstruction. New “barbed” sutures which prevent loss of running suture tension have recently been available. We assess their efficacy in comparison to classical sutures.Methods:All patients treated by PRDV with the use of barbed (V-locTM180) sutures were included. Each anastomosis entailed 2 half running sutures with posterior reconstruction, performed by 3 different operators. Waterproofness was verified performing cystography on postop day 10 before catheter removal, and in case of leakage at time of catheter removal. We compared these cases to a group of patients previously operated with classical sutures We analyzed operative and anastomosis time as well as time to catheter removal and the presence of urinary leakage.Results:44 patients underwent PRDV using V-locTM180 from June 2010 to March 2011.One patient (2.3%) presented leakage requiring bladder catheterization for 20 days. Of the 44 patients of the control group, 3 (6.8%) showed leakage requiring catheterization for a mean 21.3 days (20-22). All other had catheter removal at 10 post-operative days without complications. Mean anastomosis time was significantly shorter in the V-locTM180 group (24.4 versus 30 minutes ;p=0.01). No significant difference was found in terms of urinary leakage (p=0.39) nor operative time (p=0.45).ConclusionThe use of barbed sutures during PRDV reduces significantly anastomosis time and allows a reduction in urinary leakage from 7 to 2%, This has led us to renounce to postop cystographic control.
Robotic Prostatectomy Learning Curves- An Independent Analysis of 13 Unrelated Surgeons over 5 years
OBJECTIVES: A prospective database of robotic assisted laparoscopic prostatectomy (RALP) procedures was established to evaluate outcomes. METHODS: We used logistic regression and weighted means to establish learning-curve models using positive surgical margins (PSM) as surrogates for learning curve outcome.RESULTS: 13 surgeons performed 1575 cases. The overall PSM was 20%. pT2 and pT3 PSM rates were 13.6% and 38.7% . While surgeons showed significant variability in PSM rates, all had similar shaped “learning curves””. An individual surgeon's rate of improvement in PSM was statistically no different in their initial 25 cases compared to the 2nd 25 cases (p=0.808). However, when the rate of improvement in the 1st 50 cases was compared to the 2nd 50 cases, there was a significant improvement in PSM (p 0.00001). This implies the major transition point occurs between cases 25 to 50. Using logistic regression there was a 76% greater likelihood of PSM in the 1st 25 cases compared to subsequent cases. This risk was not apparent when the 1st 50 cases were compared to subsequent cases, again implying a rate of change transition (learning-curve) between cases 25 - 50.CONCLUSIONS: Our surgeons have different incidences of PSM, however the time frame in which reach their individual plateau is similar. A surgeon's PSM improvement rate significantly improves between cases 25 to 50 on average. After 50 cases, PSM rate may improve however the rate of improvement is not statistically significant and eventually plateaus. The absolute PSM rate achieved appears to be a function of the individual surgeon.
The Learning Curve of Laparoscopic Versus Robotic Trained Surgeons During Implementation of a Robotic Prostatectomy Program
Introduction: Currently there is a paucity of data on the results of laparoscopically (LS) versus robotically trained surgeons (RS) for robotic assisted laparoscopic prostatectomy (RALP). Purpose: We report our experience with a community-based RALP program involving only LS and RS. We compare their learning curves. Materials and Methods: Between 8/2008 and 9/2010, a total of 969 consecutive RALPs were performed at our institution by 4 RS and 4 LS. We recorded preoperative clinical data, intraoperative logistics, and pathologic outcomes. Positive surgical margin rate (PSMR) was used as a surrogate for defining mastery of RALP technique. Data were analyzed with chi-squared test and multivariate analysis. Results: A total of 969 patients were enrolled. The RS group performed 420 RALPs and LS group performed 549 RALPs. There was no significant difference in perioperative clinical parameters. Individual LS approximated RS after 40 cases. LS group approximated RS group after 300 cases. There was a significant difference in the total prostatectomy time and PSMR: RS 27.8%, LS 19.9%. Conclusions: RS group has better initial outcomes compared to LS group. However, the two groups equaled during our observation period. This study is applicable to a community practice model where multiple urologists are granted robotic privileges.
Effect of Surgeon Training, Volume, and Specialty on Surgical Margin Rates following Robotic Prostatectomy
INTRODUCTION: A prospective database captured 100% of robotic-assisted laparoscopic prostatectomies (RALP) performed on a shared da Vinci Surgical Systems in Melbourne, Australia. Individual surgeon's positive surgical margins (PSM) rates were analyzed.
METHODS: 13 independent surgeons transitioned from active open and laparoscopic practices into RALP and were monitored over 5 years. None had prior RALP training in the form of RALP fellowship or residency training. 1575 RALP cases were analyzed for PSM. Multivariate modeling was performed to control for PSA, Grade, Stage, and date of surgery.
RESULTS: Surgeon volume ranged from 21 - 396 cases, mean 131 cases. Individual surgeon results varied significantly (pT2 PSM range=2-22%; pT3 PSM range=19-55%). Surgeons with laparoscopic training, >100 case experience, or >2.5 yrs experience did not outperform their counterparts in this analysis (Figure 1).
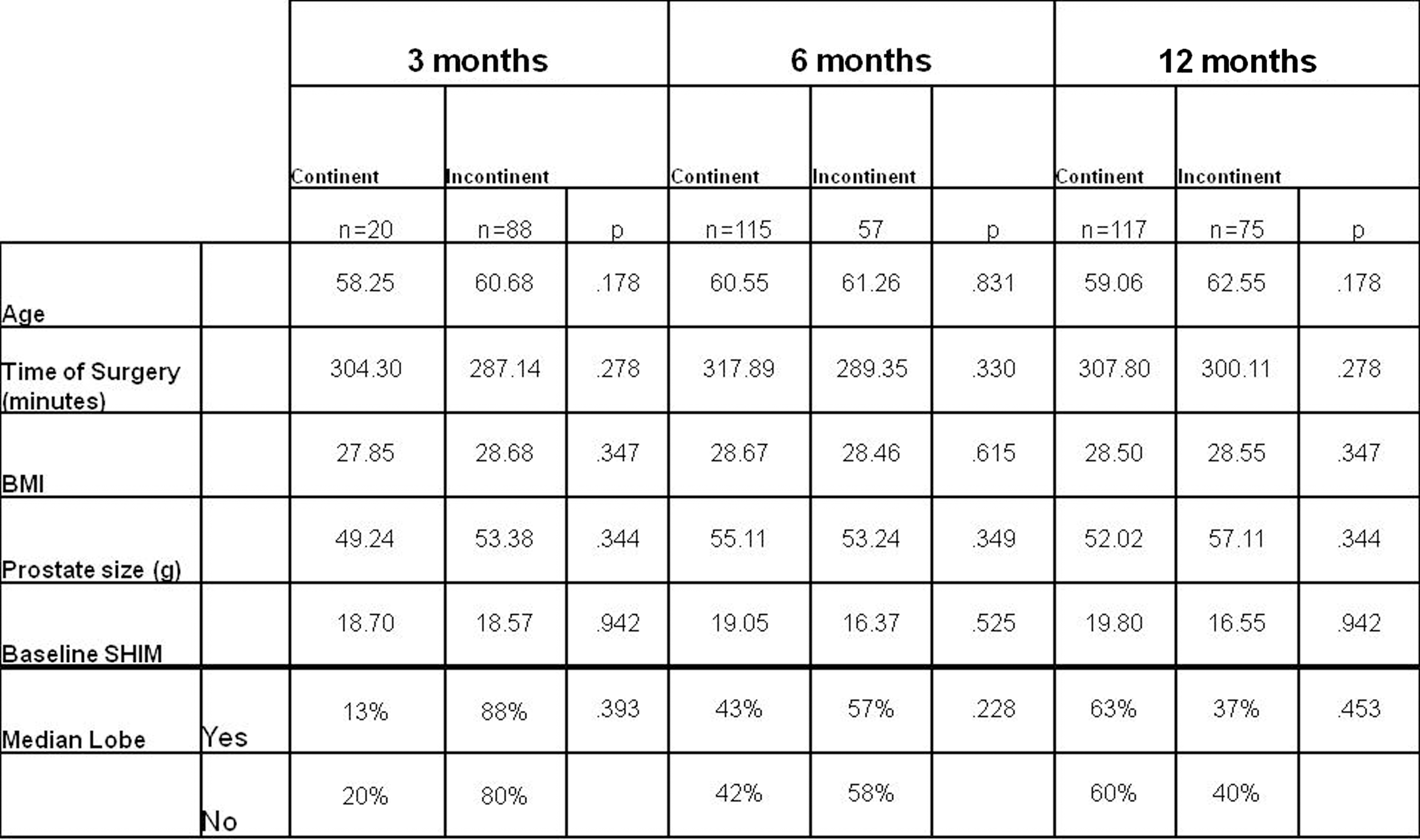
CONCLUSIONS: Individual surgeon's PSM rates are highly variable and multi-factorial and cannot be attributed to surgical background or surgical experience alone in this limited study.
Open versus Minimally-Invasive Radical Prostatectomy for High-Risk Prostate Cancer
Introduction: The ideal treatment for high-risk prostate cancer (HRPC: PSA>20ng/mL, >=cT2c, Gleason 8-10) is not well-defined. Population-based studies indicate that surgical margin rates and use of adjuvant and salvage therapy are greater in minimally-invasive radical prostatectomy (MIRP). Purpose: To analyze the perioperative and short-term oncological outcomes of men undergoing open and MIRP for HRPC.Methods: 913 patients with HRPC were identified in the Johns Hopkins RP Database since the inception of MIRP at this institution (2002-2011); 743 (81.4%) underwent open RP, 105 (11.5%) robot-assisted laparoscopic RP (RALRP) and 65 (7.1%) laparoscopic radical prostatectomy (LRP) for HRPC. Appropriate comparative tests were used to evaluate patient and prostate cancer characteristics.Results: Age, biopsy and pathological Gleason sum were similar among all groups (p>0.06). Median pre-operative PSA was 6.7, 6.4 and 6.7 in men undergoing RP, RALRP and LRP, respectively (p=0.011); 10.6%, 9.3% and 24.2% of men were >=cT2c (p=0.02); 33.3%, 34.3% and 53.8% had organ-confined (pT2) disease at RP (p=0.007); and median year of surgery was 2006, 2008 and 2006 (p<0.001). Overall surgical margin rate was 29.4%, 34.3% and 27.7% (p=0.52) and 1.9%, 2.9% and 6.2% (p=0.39) for pT2 disease. Rates of adjuvant radiation treatment were 8.1%, 2.9% and 13.8% (p=0.035); rates of overall additional androgen deprivation treatment were 13.1%, 3.8% and 4.6% (p=0.018) at mean follow-up of 3.0 years (1-8 ).Conclusions: At an experienced center, MIRP is comparable to open RP for HRPC with regard to surgical margin status, adjuvant radiation and short-term salvage hormones.
Should Patients with Glaucoma be Offered Robotic Prostatectomy?
Introduction: Steep Trendelenburg positioning is used during robotic prostatectomy (RP). Due to resulting head and neck edema and demonstrated increased intraocular pressures (IOP) during RP, surgeons or anesthesiologists may deny glaucoma patients the option of RP. Objective: We reviewed our RP experience in patients with glaucoma or ocular hypertension (OH). Methods: A prospective database of 1025 RPs performed since February 2008 by a single surgeon (RA) was reviewed. Patients with glaucoma or ocular hypertension were instructed to obtain ophthalmologic clearance preoperatively. Intraoperative fluids were restricted to 1 liter even in unaffected patients. Results: Two glaucoma patients during the study period were unable to obtain ophthalmology clearance and opted for open prostatectomy leaving 25 affected patients undergoing RP, including 23 with glaucoma and 2 with OH. Mean operative time was 154min (108-266min) with all undergoing lymphadenectomy with mean yield of 11 nodes. Trainees performed any portion of the procedure at the console in 13 patients (52%). Mean BMI was 31kg/m2 (23-44kg/m2). No patient experienced any changes in vision or other ocular complications. Among patients without glaucoma, mean operative time was 155min, and mean BMI was 30kg/m2. Estimated blood loss was 122mL (50-200cc) for patients with glaucoma or OH and 118mL (10-400cc) for those without. Conclusions: RP was safely performed in patients with a history of glaucoma or OH without perioperative ocular complications. While IOP rises during RP, the absence of clinically evident sequelae does not support a practice of routinely denying RP to patients with glaucoma or OH when optimized perioperatively.
Jefferson Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania
Predictors for Incontinence Following Robotic Assisted Laparoscopic Prostatectomy
Introduction: Good predictors for return of continence following robot assisted laparoscopic prostatectomy (RALP) have not been well established.Purpose: We analyzed our cohort of patients undergoing RALP to determine predictors for return of continence.Methods: All patients undergoing RALP from January 2007 to June 2009 were identified. Numbers reported include only those patients who completed questionairres regarding outcomes. We assessed preoperative and intraoperative parameters including BMI, Age, AUA symptom score, SHIM, median lobe, prostate size, and operative time (as surrogate case difficulty). Post-operative incontinence was determined based on patient surveys collected prospectively measuring presence or absence of any urinary leakage, and pad use. The presence of incontinence was defined as any pad usage, or report of any leakage of urine. Results: Findings are reproduced in Table 1. None of the examined parameters were found to be significant predictors of incontinence. The above parameters were also examined using a relaxed cutoff of>1 pad per day to define incontinence, and while overall measured continence rates were higher, no differences in the above parameters were noted within our cohort. Conclusions: Better prognostic factors need to be identified to help predict those who may have a worse functional outcome following RALP.
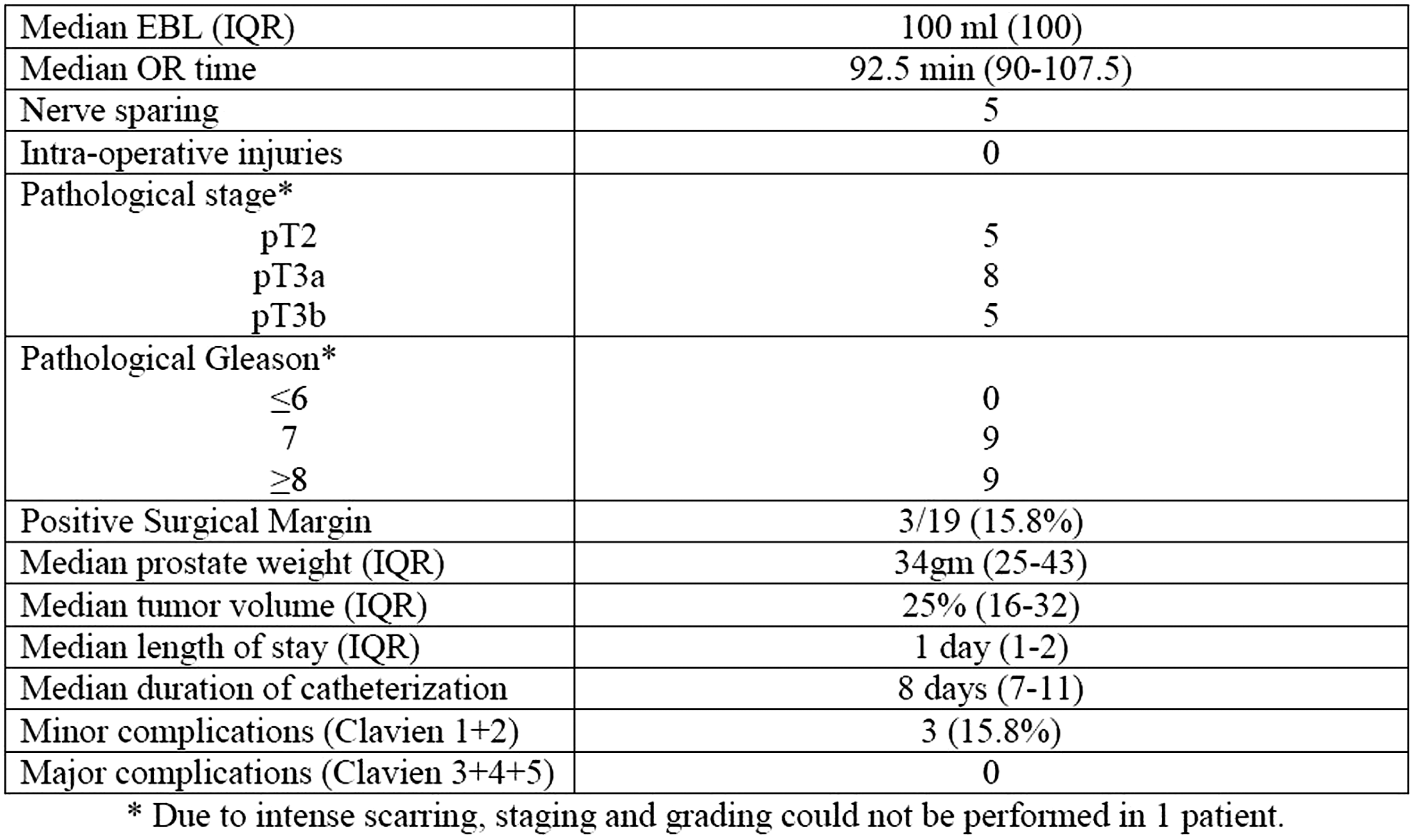
Transperitoneal Robotic-Assisted Laparoscopic Prostatectomy with Concomitant Repairs: Our 5 Year Institutional Experience
Introduction: Robotic-assisted laparoscopic prostatectomy (RALP) has gained increasing acceptance in the surgical management of prostate cancer. Purpose: To assess the efficacy and safety of performing RALP concurrently with other urological and/or general surgery procedures. Materials and Methods: From October 2005-February 2011, transperitoneal RALP procedures were performed by 2 surgeons (EJT, CDL) and prospectively recorded. We retrospectively reviewed our robotic database to identify patients who simultaneously underwent additional procedures (RALP+) under the same general anesthetic. Demographic and perioperative data were compared between RALP only and RALP + patients. Statistical analysis was performed with t-test to compare these 2 groups.Results: Over a 64 month period, 820 RALP were performed at our academic tertiary care hospital. Of these, 60 patients (7.3%) underwent 68 concurrent procedures. This included 30 inguinal hernia repairs with mesh (3 bilateral), 29 umbilical hernia repairs, and 6 other (2 hydrocelectomies, 2 incisional hernia repairs, 1 radical orchiectomy, 1 laparoscopic radical nephrectomy). Mean age (59.1 vs. 59.7 years) and mean BMI (28.4 vs. 28.6 kg/m2) were comparable between RALP only and RALP + patients, respectively (p>0.05). No significant differences in perioperative outcomes were observed between the 2 groups. Mean EBL (204 vs. 210 cc) and mean LOS (1.9 vs. 1.5 days) were also similar (p>0.05). No intraoperative or postoperative complications occurred secondary to the additional procedure(s) performed concurrently with RALP. At last follow-up, no hernia recurrences were noted.Conclusions: Concurrent procedures, particularly inguinal and umbilical hernia repairs, may be safely and effectively performed at the time of RALP with durable outcomes.
Robotic-Assisted Laparoscopic Radical Prostatectomy:64 Cases at Fujita Health University.
OBJECTIVE: We report the operative details and functional outcome of robotic-assisted laparoscopic radical prostatectomy (RALP) performed at our institution. METHODS: From August 2009 to June 2011, 64 consecutive patients underwent RALP at our institution. Prostatectomy is a transperitoneal antegrade approach, leading the dissection on the lateral border of the bladder neck following the seminal vesicle dissection. The urinary tract reconstructive procedure included an anterior as well as a posterior reconstruction after prostatectomy (total reconstruction). RESULTS: Median age was 64 (50-73) years and prostate-specific antigen (PSA) was 7.3 (4.0-57.1) ng/mL. Median operative time was 3 hours 18 minutes (console time was 2 hours 45 minutes) and median blood loss (EBL) was 150 (10-800) mL. Median weight of removed specimen was 38 (20-117) g. No case of conversion to open laparotomy or homologous blood transfusion during surgery were noted. Serious adverse event was one case that required colostomy with delayed perforation of sigmoid colon. Positive surgical margin rates for pT0, pT2 and pT3 disease was 0 (0/2), 24 (12/51), 45 (5/11)%, respectively. Urinary continence rate (safety pad 1/day) after surgery for one month was 55 (32/58)%. CONCLUSIONS: RALP by da Vinci is a safe and feasible surgical modality for prostate cancer and will have health-related quality-of-life benefits for the patients.
RARP in Patients with a History of Endoscopic treatment for BPH: A Propensity Score Based Matched-Pair Analysis.
Introduction:The purpose of this study is to determine whether previous prostate surgery has adverse effect on the perioperative, histopathological and functional outcomes of RARP Materials and Methods:We retrospectively identified 42 patients (Group 1) who had a history of endoscopic prostate surgery for the treatment of BPH. Propensity score matching was performed to generate a control Group 2. The peri-operative, histo-pathological and functional outcomes were compared between these groups.Results:Both the groups were comparable in terms of age , BMI , PSA , preoperative SHIM score and AUA-SS . The OR time was significantly increased in group 1 as compared to group 2 (Median 77.5 vs 75 min; p=0.02). There was no statistically significant difference in terms of length of stay , PSMs ,duration of catheterization and complication rates.The continence rates at 1, 3,6,12 and 18 months after catheter removal for Group 1 were 48.8%, 79.5%, 83.8%, 86.2% and 86.4% respectively for Group 1 while for the matched group, these rates were 45.2%, 69%, 78.9%, 89.7% and 90.5% respectively. The potency rates (SHIM>17 and nerve sparing) at similar intervals were 27.3%, 42.9%, 65%, 76.5% and 76.9% respectively for group 1 and 32%, 52%, 69.6%, 77.8% and 83.3% respectively for Group 2. The difference was not statistically significant at any point of time for either continence or potency outcomes Conclusion:Although the OR time is higher, the PSM rates, complication rates, histo-pathological and functional outcomes are comparable to those patients who have no prior prostate surgery.
Salvage Robot Assisted Radical Prostatectomy: Single Surgeon Experience
Objective: The objective of this study is to report the peri-operative, functional and early oncological outcomes of salvage Robot Assisted Radical Prostatectomy (sRARP) for radio-recurrent prostate cancer.Methods:We identified 19 patients who underwent sRARP for radio-recurrent prostate cancer by a single surgeon (VRP) between July 2002 and October 2010. RT consisted of External beam RT (XRT) in 9 cases, brachytherapy (BT) in 7 cases), BT + XRT in 2 cases and proton beam therapy (PBT) in one case. Biochemical failure was defined according to the ASTRO criteria as a PSA of>2.0ng/ml over the absolute nadir. Continence was defined as the use of no pads after surgery and potency was defined as erections adequate enough for penetration, with or without the use of PDE-5 inhibitors. Biochemical recurrence (BCR) was defined as a PSA of>0.2ng/ml after sRARP.Results:Please see table Conclusions:RARP is a technically challenging, but feasible procedure. Common side effects include delayed healing of urethro-vascular anastomosis leading to prolonged catheterization. Careful patient selection, extensive counseling regarding possible side effects of procedure, and intra operative proctoscopy are the key features while performing sRARP.
Peri-operative outcomes and Positive Surgical Margin rates in a single surgeon series of 4000 Robot Assisted Radical Prostatectomies.
Objective:Robot Assisted Radical Prostatectomy (RARP) is a rapidly evolving minimally invasive treatment modality for clinically localized prostate cancer. We analyze the lessons learned over 4000 cases by a single surgeon and report the peri-operative outcomes of the procedure. Methods:After IRB approval at each of the three institutions, we prospectively analyzed 4000 consecutive cases of RARP. All cases were performed via a 6 port trans-peritoneal technique. The peri-operative outcomes and histopathological outcomes including the positive surgical margin rates have been reported. The complications were classified according to the Dindo modification to the Clavien grading system. Clavien grade 1 and 2 were classified as minor complications which required no surgical intervention while Clavien grade 3 and 4 were classified as major complications.Results:See tableConclusion:RARP is a safe treatment option for prostate cancer, and our study demonstrates encouraging complication rates. Most of these complications are minor complications requiring no surgical intervention. The most common complication before discharge from hospital is bleeding requiring blood transfusion and ileus; while those after hospital discharge are anastomotic leak and acute urinary retention.

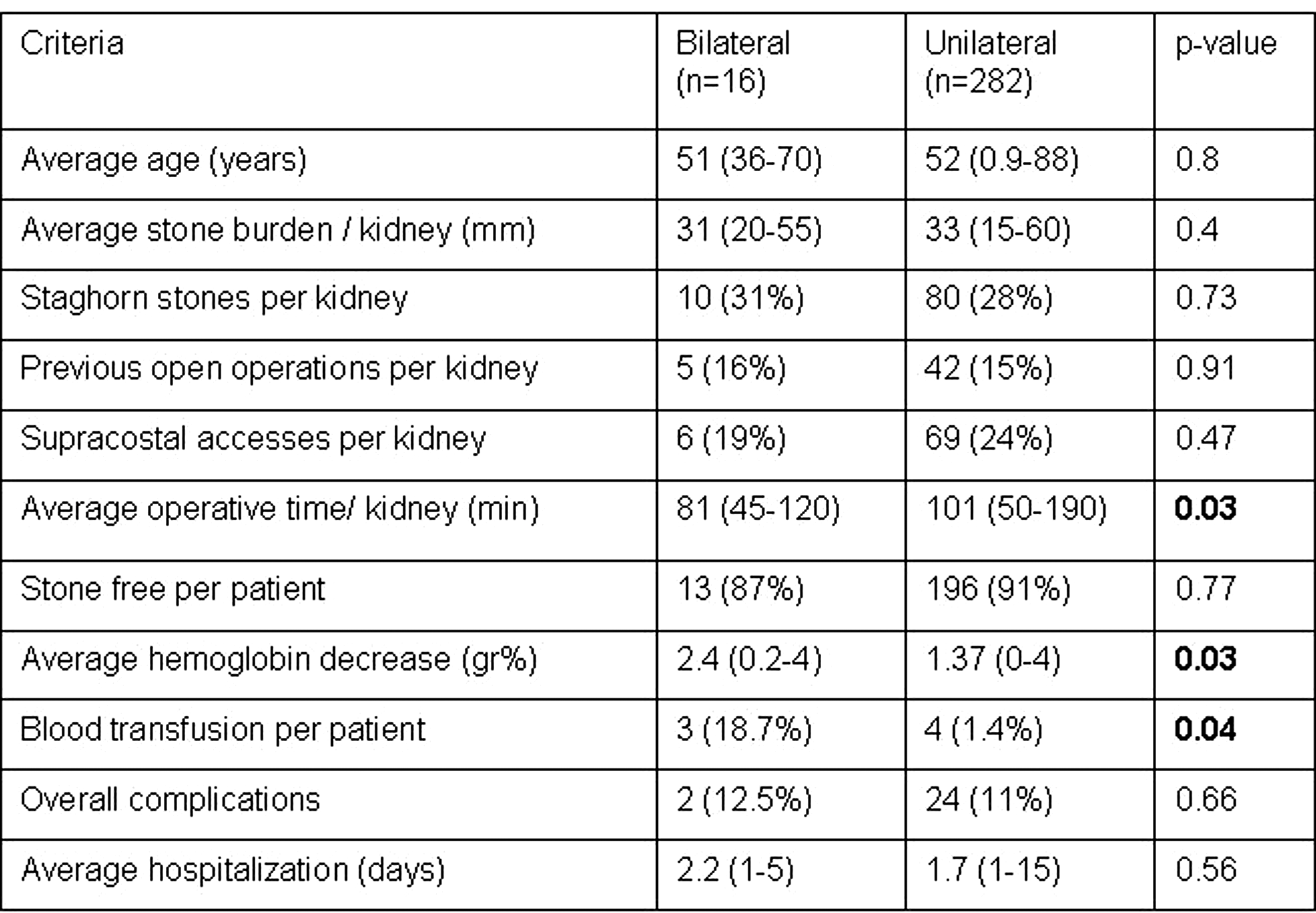
MP18: PNL 1
The Safety and Efficacy of Percutaneous Nephrolithotomy with Supracostal Approach in the Treatment of Renal Stones
[Purpose] To evaluate the safety and efficacy of percutaneous nephrolithotomy with supracostal approach in the treatment of renal stones in a single center data .[Materials and methods] A retrospective chart review of 485 renal calculi patients who underwent ultrasound-guided PCNL from March 2004 to May 2011 in the first hospital of Jilin university was performed. Supracostal approach was 88 cases and infracostal approach was 397 cases. The indications of supracostal approach in our study were staghorn stones, complex inferior calyceal stones, stones in the upper calyx or the upper ureter. All punctures were made by the urologist under ultrasound-guided in the prone position. All supracostal choice were between 11th and 12th rib. The operative time, success rate, puncture times, hospital stay, and complications were evaluated.[Results] there were no difference between the two group in operative time, puncture times and hospital stay. Success in the supracostal group (90.2%) was not statistically different from the infracostal group (93.9%), P>0.05. Overall complication rates across groups was low (11.6%), with a significant difference in complications between the supracostal and infracostal puncture groups across Clavien grades, P<0.01. [Conclusions] The supracostal approach was found to be safe as well as effective, with acceptable complications. It gives high stone clearance rates with acceptable morbidity rates and should be attempted in selected cases.
Which Factors may Affect Urinary Leakage Following Ultrasound-Guided Percutaneous Nephrolithotomy?
[Purpose] To evaluate the factors that may affect urinary leakage following ultrasound-guided percutaneous nephrolithotomy (PCNL).[Materials and methods] A retrospective chart review of 420 renal calculi patients who underwent ultrasound-guided PCNL from March 2004 to May 2010 in the first hospital of Jilin university was performed. The factors that may result in urinary leakage after surgery were analyzed as categorized into four groups according to individual variables (sex, age, body mass index); stone burden; renal factors (previous surgery, extracorporeal shock wave lithotripsy history, presence of hydronephrosis); and surgical features (access number, presence of nephrostomy catheter). These data were compared for the presence and duration of urinary leakage.[Results] There was no statistically significant correlation between individual factors and both the presence of leak (POL) and the duration of leak (DOL) (P>0.05). Among renal factors, only presence and degree of hydronephrosis was significantly correlated with POL (P<0.001) and DOL (P<0.001). The mean cumulative stone burden neither had impact on POL nor correlated with DOL (P>0.05). Among surgical factors, there was no statistically significant difference about the number of puncture times. Using an internal ureteral stent significantly decreased incidence of POL and DOL (P<0.001). DOL increased with catheter diameter and stay time (P<0.05).[Conclusions] Several factors can lead to urinary leakage following ultrasound-guided percutaneous nephrolithotomy. Precautions may also be simple if these factors are considered preoperatively.
Variables That Influence Bleeding During Percutaneous Nephrolithotomy
Objective: To investigate variables that influence bleeding during percutaneous nephrolithotomy (PCNL). Methods: The records of 249 PCNL procedures that were performed by a single surgeon were retrospectively analyzed.The patientand stone-related factors,including age,sex, hypertension,and diabetes,history of ipsilateral renal procedures, stone type,degree of hydronephrosis, preoperative hemoglobin level;operative factors,such number and size of accesses and operative time werei nvestigated. Univariate analyses and multivariate stepwise regression analyses were used for statistical assessment. Results: The overallblood transfusion rate was 7.8%. The average Hb drop after PCNL procedures were 11.2g/L. During the univariae analyses, the number of accesses, the size of accesses, stone type,diabetes, and operative time were the most important factors for blood transfusion requirement. Multivariate stepwise regression analyses showed that there was an association between diabetes, operativetime, number of accesses, size of accesses and stonetype with the decrease in hemoglobin levels and transfusion rate. No correlation between surgical experience and decrease in hemoglobin levelas well as blood transfusion necessity was found. Conclusions: Depending on the results achieved by univariate analyses and multivariate stepwise regression analyse, multiple access tracts, big access, staghorn calculi, presence of diabetes and long operativetime,but not surgical experience, significantly increased bloodloss during PCNL.
The Safety and Efficacy of Ultrasound-Guided Minimally Invasive Percutaneous Nephrolithotomy for the Patients with Complicated Upper Ureteral Calculus
Purpose: The purpose of the study was to evaluate the safety and efficacy of ultrasound-guided minimally invasive percutaneous nephrolithotomy(mini-PCNL) for the patients with complicated upper ureteral calculus. Methods: We retrospectively analyzed the clinical data of forty-eight patients with complicated upper ureteral calculus, all of whom had undergone ultrasound-guided mini-PCNL, including the operative duration, the stone-free rate, the retention time of nephrostomy tube, the average postoperative hospital stay and the complications after the surgery. Results: In all the 48 cases, the 16F nephrostomy tract was established and the calculus were cleared successfully in one stage. The average operative time was 24 minutes, the average estimate intraoperative blood loss was 60ml. The stone-free rate is 100% according to the ultrasonography or KUB after the surgery. There were no complications such as bleeding, the damage to pleura or intestines. Conclusions: As the preferred treatment of complicated upper ureteral calculus, ultrasound-guided mini-PCNL is a safe and effective procedure.
Percutaneous Nephrolithotomy: Critical Analysis Ofunfavorable Results
ABSTRACT WITHDRAWN
Does Early ESWL Following PCNL Lead to Trapped Stones in the Tract: Myth or Reality?
Bilateral Same Session Tubeless Percutaneous Nephrolithotomy without Preopative Exclusion Criteria
Purpose: To assess the outcome of bilateral tubeless percutaneous nephrolithotomy (TPNL) performed without preoperative exclusion criteria. Materials and Methods: Starting with 2004, 298 patients with renal calculi underwent TPNL under general anesthesia. Bilateral same session TPNL was performed in 16 (5.4%) patients. Large stone burden, previously operated kidneys, anatomic anomalies, complex and staghorn stones, multiple accesses and long operative time were not considered exclusion criteria. Results: See table. Conclusions: Bilateral same session TPNL without preoperative limitations appears to be feasible, safe and efficient. The significant less operative time per kidney in the bilateral TPNL group is probably explained by the time spared with single positioning and preparation for both kidneys. Patients should be aware that the bilateral approach carries an increase postoperative transfusion rate in comparison to unilateral procedures. The bilateral approach may have potentially advantages in the suitable patients and should be further evaluated in larger series.
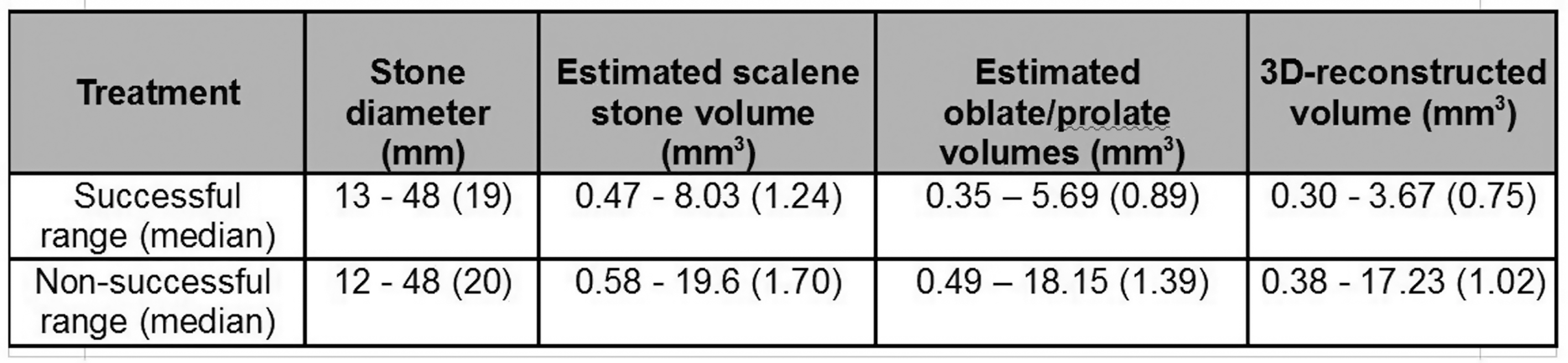
Division of Urology, Department of Surgery, Duke University Medical Center, Durham, NC, USA
Introduction: Urosepsis, usually marked by fever, is a serious complication following percutaneous nephrolithotomy (PNL). Despite different intracorporeal lithotrites used today, data are lacking on fever risk stratified by lithotrite type. Purpose: To compare risk of post-PNL fever from different lithotrites. Materials and Methods: The Clinical Research Office of the Endourological Society (CROES) PNL database is a prospective, multi-institutional, international PNL registry. Of 5803 total patients, 4968 received pre-operative antibiotics, had complete information, and were included in this analysis. Lithotrites assessed included no fragmentation (NF), ultrasound (US), laser (LA), pneumatic (PN), and combination ultrasound/pneumatic (CUP). Fever risk was estimated using multivariate logistic regression adjusting for diabetes, steroid use, history of positive urine culture, presence of staghorn calculi, pre-operative nephrostomy, stone burden, and lithotrite. Results: Overall fever rate was 10%. PN lithotrites were used in 43% of the cohort, followed by US (24%), CUP (17.3%), NF (8.4%), and LA (7.3%). Fever rates were no different between patients who underwent NF or fragmentation (p=0.117), nor among patients when stratified by lithotrite (p=0.429). On multivariate analysis, fragmentation was not significantly associated with fever (Odds Ratio [OR] 1.17, p=0.413), while diabetes (OR 1.32, p=0.048), positive urine culture (OR 2.08, p<0.001), staghorn calculi (OR 1.80, p<0.001), and nephrostomy (OR 1.65, p<0.001) increased fever risk. Fever risk was no different among lithotrites, relative to PN (p>0.128). Conclusion: Risk of post-PNL fever was no different among the various lithotrites used in the CROES PNL study. However, diabetes, staghorn calculi, and nephrostomy tube all increased fever risk.
Division of Urology, Department of Surgery, Duke University Medical Center, Durham, NC, USA
Introduction: Stone-free rates after percutaneous nephrolithotomy (PNL) are determined by computed tomography (CT), ultrasound (US) or abdominal/pelvic x-ray (KUB), which have different sensitivities for detecting stones. Purpose: To compare stone-free rates after PNL stratified by imaging modality. Materials and Methods: The Clinical Research Office of the Endourological Society (CROES) PNL database is a prospective, multi-institutional, international PNL registry. Of 5803 total patients, 3539 with measurable stone burden,<11 stones, and complete data were included for analysis. Multivariate logistic regression estimated odds of stone-free status with adjustment for stone count, stone burden, lithotrite, puncture site, and imaging modality. Results: Overall stone-free rate was 83%. KUB was used in 74% of patients to verify stone-free status, followed by US (15%) and CT (11%). CT usage conferred lower stone-free rates compared to US and KUB (68.2, 84.8, and 84.8%, respectively; p<0.001) and higher retreatment rates (19.1, 5.7, and 9.2%, respectively; p<0.001). Multivariate analysis showed CT usage was significantly associated with lower odds of stone-free status (Odds Ratio [OR] 0.36, p<0.0001) relative to KUB. Other predictors of stone-free status included higher stone counts (OR 0.76, p<0.0001), multiple puncture sites (OR 0.50, p=0.0002), and use of ultrasound (OR 0.64, p=0.0006), laser (OR 0.66, p=0.038), or combination ultrasound/pneumatic (OR 0.72, p=0.015) lithotrites relative to pneumatic. KUB did not predict stone-free status any differently than US. Conclusion: CT usage after PNL is more sensitive to detect stone remnants compared to other modalities. Standardization of follow-up imaging after PNL is important to compare results reported in the literature.
Percutaneous Nephrolithotomy Combined with Other Surgical Interventions
Aim: To assess the feasibility of performing percutaneous nephrolithotomy (PNL) combined with other operations during the same operative session.Materials and Methods: The study group comprised 24 candidates for PNL presenting with concomitant other surgically correctable comorbidities. Patients operated concomitantly for different sites of urolithiasis (e.g. cystolithotripsy, contralateral ureteroscopy and PNL) were excluded. The operating time, technical feasibility, operative success, complications, hospital stay, and patient satisfaction were analyzed. Results: Patients' average age was 52 (range 21-81). The average stone diameter was 35 mm (range 15-60) and 9 (38%) patients presented with staghorn stones. Tubeless PNL was performed in 15 (63%) cases. PNL was combined with: radical retropubic prostatectomy (n=2), laparoscopic (n=1) and open (n=1) contralateral nephrectomy, suprapubic prostatectomy (n=2), transurethral resection of prostate (n=2), repair of inguinal hernia (n=5), parathyroidectomy (n=3), hydrocelectomy (n=3), percutaneous gastrostomy (n=1), laparoscopic cholecystectomy (n=1), fixation of hip fracture (n=1), excision of lipoma of thigh (n=1), wedge excision of lung tumor (n=1). There were no complications. The average hospital stay was 5 days (range 1- 6). The duration of hospitalization was related to the more complex operation; combining the procedures did not prolong it. The average follow-up was 47 months (range 3−84). Conclusions: Our results support the concept of performing simultaneous PNL and other operations during one surgical session. This approach obviates the need for repeated anesthesia, reduces patient inconvenience, the psychological stress related to multiple operations, and the total hospital stay.
Results of a Modified Technique of Tubeless PCNL
Introduction:Tubeless PCNL has been propagated as a procedure without a nephrostomy drain. Clayman (2009) described a technique using Floseal with a retrograde balloon occlusion catheter to seal the tract. A double J stent is used for internal drainage. Purpose: To present our case series of patients who underwent PCNL with a modified technique using an antegrade Fogarty balloon for occluding the pelvi-calyceal system and deployment of Floseal as a tract sealant. Materials: Data of patients who underwent tubeless PCNL were reviewed retrospectively with respect to patient demographics, stone burden, stone-free outcome, length of stay, transfusion rate and complications. The analgesic requirements were compared with a cohort of 50 standard PCNLs. Results: Thirty four (27 male and 9 female) patients underwent tubeless PCNL between November 2007 to April 2011. The median age was 47 years. The mean stone burden was 2.1cm. Nineteen percent had staghorn calculus. The median length of stay was 3 days. No patient required peri-operative transfusion with a mean drop in haemoglobin of 1.51gm/dL. Post-operative pyrexia developed in 12.5% of cases and settled with antibiotics. Seventy six percent were rendered stone free, while the rest had ancillary procedures. The average analgesic requirement in the post-operative period was 44.8mg morphine and 167.5mg diclofenac equivalents respectively. This compared favourably with standard PCNLs (92 and 340mgs of morphine and diclofenac equivalents respectively).Conclusions: Antegrade tract closure for tubeless/ nephrostomy free PCNL is a modification associated with low morbidity, reduced hospital stay and lower analgesic requirements.
Initial Experience of Modified Supine PCNL in a peripheral hospital.
INTRODUCTIONPCNL is a traditionally performed in a prone position. This has significant anaesthetic ramifications and is time-consuming. Recently, approaches including modified supine positions have been described. Additional benefits of these positions include treating ureteric calculi simultaneously, thereby avoid additional operations and decreased operating time. Despite these benefits, it is not common practice in Australia due to lack of training.PURPOSEOur purpose is to determine whether the larger trial data available is applicable to a peripheral hospital and a urologist new to this technique.MATERIALS AND METHODSBetween March to July 2011, 15 consecutive patients with renal and/or ureteric calculi were treated with a modified supine PCNL performed by a single surgeon. These were his first 15 PCNL performed in a modified supine position. Data was collected prospectively.RESULTSAverage age of patients was 48 years (range 19-78). Median length of stay is 2.5 days (range 1-8). Average operating time is 90 minutes (range 55-151). 20% of patients presented with concurrent ureteric calculi which were treated simultaneously. 1 patient was converted to prone position. 1 patient had post-operative haemorrhage requiring blood transfusion. This patient had CT angiogram which did not demonstrate any active bleeding. There were no other complications. CONCLUSIONSModified supine PCNL is a technique which is able to be performed by urologists new to this technique. There are many additional benefits compared to traditional PCNL including decreased operating time, treatment of ureteric stones and anaesthetic benefits. This makes it an attractive technique for all urologists to learn.
Lessons Learned after 3000 Percutaneous Procedures for Urolithiasis
Introduction: Percutaneous nephrolithotomy is nowadays routinely performed in many centers. Purpose: To evaluate methods to improve results on large series of patients.Materials and Methods: During the last 9 years, in our department were performed 3071 percutaneous procedures for lithiasis. The technical tricks used for solving procedural problems were represented by: supplementary puncture and displacement of the calculus, basket removal of calculi migrated into the ureter, dye or air instillation through the ureteral catheter, lumbar palpation to modify renal position and usage of the flexible endoscopes.Results: A single supplementary access traject was performed in 93 cases, 2 supplementary trajects in 58 cases and 3 supplementary trajects in only 14 cases. The displacement of the calculus was applied in 52 cases using the needle, a jet of saline under pressure or the percutaneously inserted ureteroscope in 2 cases. The use of flexible endoscopes improved the stone-free rate in 123 cases. Accidentally lost percutaneous trajects were renegotiated after metilen blue or air instillation through the ureteral catheter in 44 cases. Stone fragments migrated into the ureter were extracted using a basket in 54 cases, the flexible endoscopes in 35 cases or pushed up jets of saline under pressure injected through the ureteral catheter. Lumbar palpation allowed the repositioning and extraction of migrated fragments in 54 cases.Conclusions: Technical tricks improved the stone-free rate in a significant number of cases. Their appliance increases proportionally with the surgeon experience, but they must be performed with caution, due to the possible associated morbidity.
Shockwave Lithotripsy is Associated With Improved Outcome of Single-Tract Percutaneous Nephrolithotomy
PURPOSE: To evaluate the efficacy of single tract percutaneous nephrolithotomy (sPCNL) and investigate the preoperative predictive factors associated with stone clearance after sPCNL.Methods:A retrospective review of 351 cases of sPCNL performed at a single institution by one of two endourologists between January 2000 and March 2010 was performed. The primary outcome evaluated was stone free rate (SFR) as assessed immediately following either initial procedure or second-look nephroscopy performed on post-operative day two. Preoperative patient and stone factors including age, sex, body mass index, preoperative hematocrit and creatinine, previous surgical history, comorbidities, renal anomalies, stone size, shape, location, and history of any previous treatment to the active stone burden were included in univariate analysis. Significant factors on univariate analysis were then included in a logistic regression multivariate analysis.Results:SFR following either initial procedure or second-look nephroscopy was 76%. On univariate analysis, rising preoperative creatinine, hypertension, increasing stone diameter, complete staghorn stone, presence of stones in the upper pole and absence of prior SWL were associated with lower SFR. Stone size, presence of stones in the upper pole, and prior SWL for the active burden were independent predictors of SFR on multivariate analysis. ConclusionsPCNL is an efficient procedure to clear renal stones, especially when used in conjunction with routine second-look nephroscopy. SWL performed prior to PCNL is associated with improved stone clearance even after adjusting for size and location. The role of SWL prior to PCNL warrants further prospective investigation.
Percutaneous Nephrolithotomy and Staged Ureteroscopy for Kidney Stones Between 2 and 4 Centimeters: Comparative Effectiveness
INTRODUCTION: Historically percutaneous nephrolithotomy (PCNL) has been the primary treatment for>2cm stones. However, staged ureteroscopy (SURS) has increasingly been utilized. This study evaluates PCNL and SURS to determine the comparative effectiveness in treating stones 2- 4 centimeters in diameter.PATIENTS AND METHODS: With IRB approval, all PCNL patients charts who met criteria with stones between 2 and 4 centimeters were reviewed from 2000 through 2010. Theses were compared with SURS patients who met the same criteria from 2005 through 2010. RESULTS: A total of 254 patients were reviewed. 207 patients underwent PCNL and 47 underwent SURS. Average BMI was 29.9 vs. 35.9 for PCNL and SURS respectively. Average procedure length for PCNL was 138 minutes with a complication rate of 19.2% and average hospital length of stay (HLOS) was 2.6 days. A second look procedure was required in 31% of PCNL patients with a stone-free rate of 91.8%. The average procedure length for SURS was 130.5 minutes (p=0.44) with a complication rate of 2.1% and only 3 patients needed to stay overnight in hospital. 13% required only one procedure and 80.9% of SURS patients were stone-free. CONCLUSIONS: PCNL can be performed with a higher rate of success when compared with SURS for 2-4 cm stones. However, PCNL resulted in a higher rate of complication and longer HLOS, suggesting SURS should be considered as an alternative treatment in the appropriate patient.
Predictors of Complications of Single-tract Percutaneous Nephrolithotomy
INTRODUCTION: Single-tract percutaneous nephrolithotomy (sPCNL) is assumed to have fewer complications than multi-tract PCNL. Our objective is to evaluate the complications of sPCNL and investigate the preoperative factors which are associated with significant complications of sPCNL.METHODS: A retrospective review of 351 cases of sPCNL (January 2000-March2010) was performed at our institution. High Clavien grade (grades III-V) complications were the primary outcome. Preoperative patient and stone factors such as age, sex, BMI, preoperative hematocrit and creatinine, previous surgical history, comorbidities, renal anomalies, stone size, shape, location, and history of any previous treatment to the active stone burden were included in univariate analyses. Significant factors on univariate analyses were then included in a multivariate logistic regression model analysis.RESULTS: There were 67 (19.1%) complications with low grade (Clavien grade I and II) complications comprising around 12.8% and high grade complications were only 6.3%. Transfusion rate was only 1% and there was no perioperative mortality. Univariate analysis shows that solitary kidney and intercostal punctures had more high-grade complications while subcostal or lower pole punctures had fewer severe complications. Multivariate analysis of these factors showed that solitary kidney and subcostal access were the only significant factors.CONCLUSIONS: sPCNL is a safe procedure. Patients with a solitary kidney have a higher complication rate. Subcostal access is associated with lower risk of complications. Stone diameter and staghorn stones are not significant predictors of having high grade complications. Further prospective comparison between staged ureteroscopy, multiple-tract PCNL and sPCNL in solitary kidney patients should be done.
Department of Urology, the first affiliated hospital of Guangzhou Medical College, Guangzhou, China
Introduction and purpose: To evaluated the effects of previous failed repeated extracorporeal shockwave lithotripsy(SWL) on the performance and outcomes of subsequent percutaneous nephrolithotomy (PCNL).Material and Methods: 24 patients with a history of failed repeated SWL (group 1) on the same kidney unit were compared with 30 patients submitting to PCNL as their first treatment choice (group 2). Patients demographics, stone characteristics, operative findings, including operative time, time to establishing percutaneous tract, time to extract stone fragments, success rate, need for auxiliary treatments, and complications were documented in detail and compared in the two groups.Results: Group 1 and 2 had comparable patients demographics and stone characteristics. Time consuming for establishing percutaneous tract (7VS8min), extracting stone fragments(51 VS 48min), total operative time(74 VS 65min), and major complications did not differ significantly in the two groups(16.7% VS 20%). The stone complete free rates were 75.0% and 83.3% in group 1 and group 2, and the rates of residual fragments less than 4mm were 8.3% and 10%,respectively.Conclusions: Previous failed repeated SWL did bring much difficulty in the procedures of stone fragments extracting in few cases, while PCNL can be performed safely in patients with a history of repeated SWL without a higher risk of complications and with a success rate similar to that of PCNL in patients with no previous SWL intervention.
Department of Urology, the first affiliated hospital of Guangzhou Medical College, Guangzhou, China
Introduction and Purpose:Tubeless PCNL in select patients has been demonstrated to decrease postoperative discomfort and improve patient satisfaction without compromising safety, several methods was carried to ensure the safety of this technique. A nobel tubeless mPCNL technique was carried out in this series.Material and methods:17 consecutive cases underwent single access tubeless mPCNL was enrolled. After 16Fr percutaneous tract established with fascial dilators, mPCNL with ureteroscope was carried. Efflux from the sheath at the end of the procedure was clear. The tract was inspected with ureteroscope visualization for any bleeding during the gradual withdrawal of the sheath. No nerphrostomy tube or JJ stent was placed.Results:17 access tracts were established in these cases, no second-look procedures was needed. The mean operating time was 46 minutes, ranged from 33 minutes to 62 minutes. The duration of hospitalization was 3.2 days (range 3 to 6 days).Complete stone clearance was achieved in 16 cases (16/17,94.1%) in a single session.1 case had residual calculi with the size of 5mm in the lower pole. Blood loss was 120ml(90-270), no patients required blood transfusion. 3 patients (3/17, 17.6%) with a postoperative fever of 38.5 centi-degree or greater. Conclusions:Tubeless mPCNL using a little percutaneous tract was safe and well tolerated without associated morbidity.
MP19: Ureteroscopy 1
The Ohio State University Medical Center, Columbus, OH
(Introduction: We determined the performance characteristics of a non-tapered, single-use 240 micron fiber Flexiva Boston Scientific, Natick, MA), during both clinical use and in a bench-test model.Methods: One hundred fibers were used in 100 consecutive procedures. Pulse energy, frequency, and total energy were recorded. The amount of fiber burn back from the tip was measured. Following their use in clinical cases, the fibers were evaluated for energy transmission in both straight and 180 bent configuration with settings of 400 mJ at 5Hz. Failure threshold was evaluated by bending the fibers to 180 with an initial bend radius of 1.25 cm. The laser was activated with a setting of 1200 mJ at 10Hz for 30 seconds. If the fiber did not break, the radius was reducing in 0.25 cm increments and the testing repeated.Results: The mean energy transmitted was 451 mJ and 441 mJ in a straight and 180 bend configuration. 80% of fibers transmitted at least 400 mJ; 13% of fibers fractured at a bend radius of 0.5 cm with energy transmission. No fibers failed at larger bends. During clinical use, fiber tips burnt back an average length of 1.664 mm, but the amount of burn back was highly variable. No fibers fractured during clinical use.Conclusion: Fiber performance between fibers was consistent in terms of energy transmission and resistance to fracture. Fiber burn back showed variation amongst the fibers. The lack of fiber fracture during clinical use may reduce the risk of flexible endoscope damage.
A Logistic Analysis for the key factors related to Success of Holmium-Laser Ureteroscopic Lithotripsy
Introduction: Holmium-laser ureteroscopic lithotripsy(URSL) is the first choice for patients who had stone desease in ureter.Purpose: To define the factors related to success of holmium-laser ureteroscopic lithotripsy.Materials and Methods: To retrospectively reviewed 265 patients who underwent holmium-laser ureteroscopic lithotripsy from January 2006 to July 2009. Plain films and/or ureter CT scan were taken postoperative immediately and one month later. Stone size, numbers, location, size of fragments, impaction, ureter stenosis, total renal function, ipsilateral renal function, degree of hydronephrosis, operation time, volume of postoperative fluid infusion, using diuretic medicine postoperatively, time of ambulation, ESWL history, surgeons experience were included in logistic regression analysis. Results: The stone free rate was 56.1%. According to logistic regression analysis results: total renal function (OR=1.944, 95%CI:1.140-3.315), ipsilateral renal function (OR=0.654, 95%CI: 0.367-1.165), operation time (OR=0.594, 95%CI:0.343-1.031), numbers of stones (OR=0.171, 95%CI:0.052-0.561), location of stone (OR=3.582, 95%CI: 2.008-6.389), size of fragments (OR=0.623, 95%CI: 0.352-1.103), using diuretic medicine postoperatively (OR=0.393, 95%CI: 0.118-1.309) were significant factors related to the success of URSL.Conclusions: total renal function, ipsilateral renal function, operation time, numbers of stones, location of stone, size of fragments, using diuretic medicine postoperatively will be the predictive factors for the success of Holmium-laser ureteroscopic lithotripsy.
What should we measure? Predicting Outcomes with Flexible Ureteroscopy for Large Renal Stones
Introduction
Predicting stone surgery outcome is important for patient counselling. We compared stone diameter, estimated stone volume and computer generated 3D-reconstructed volume in predicting treatment success for renal stones>10mm with flexible ureteroscopy (fURS) and holmium laser fragmentation.
Methods
Renal stones>10mm treated with fURS and pre-operative CT (2mm slices) were identified. Stone diameter was measured in 3 planes and volume estimated using a generalised scalene ellipsoid formula,specialized oblate/prolate ellipsoid transformations previously validated within our department and computer generated 3D-reconstructed volume. Success was defined as no fragments>2mm on plain X-ray at follow-up.
Results
47 patients were identified. Overall treatment success was 26/47=55.3%. Univariate analysis revealed 3D-reconstructed stone volume most accurately predicted treatment outcome. Correlation coefficients between generalised scalene estimated volume and 3D-reconstructed volume were r=0.80 for successful and r=0.77 for non-successful treatments. Improved correlation was seen when substituting the generalised-scalene formula for specialised oblate/prolate ellipsoid transformations r=0.89 and r=0.85 respectively.
Conclusion
Stone diameter, estimated volume and 3D-reconstructed volume can predict treatment outcome. A general scalene ellipsoid formula appears to over-estimate volume. Oblate and prolate ellipsoid equations had better correlation to 3D-reconstructed stone volume, which most accurately predicts fURS outcome for stones>10mm.
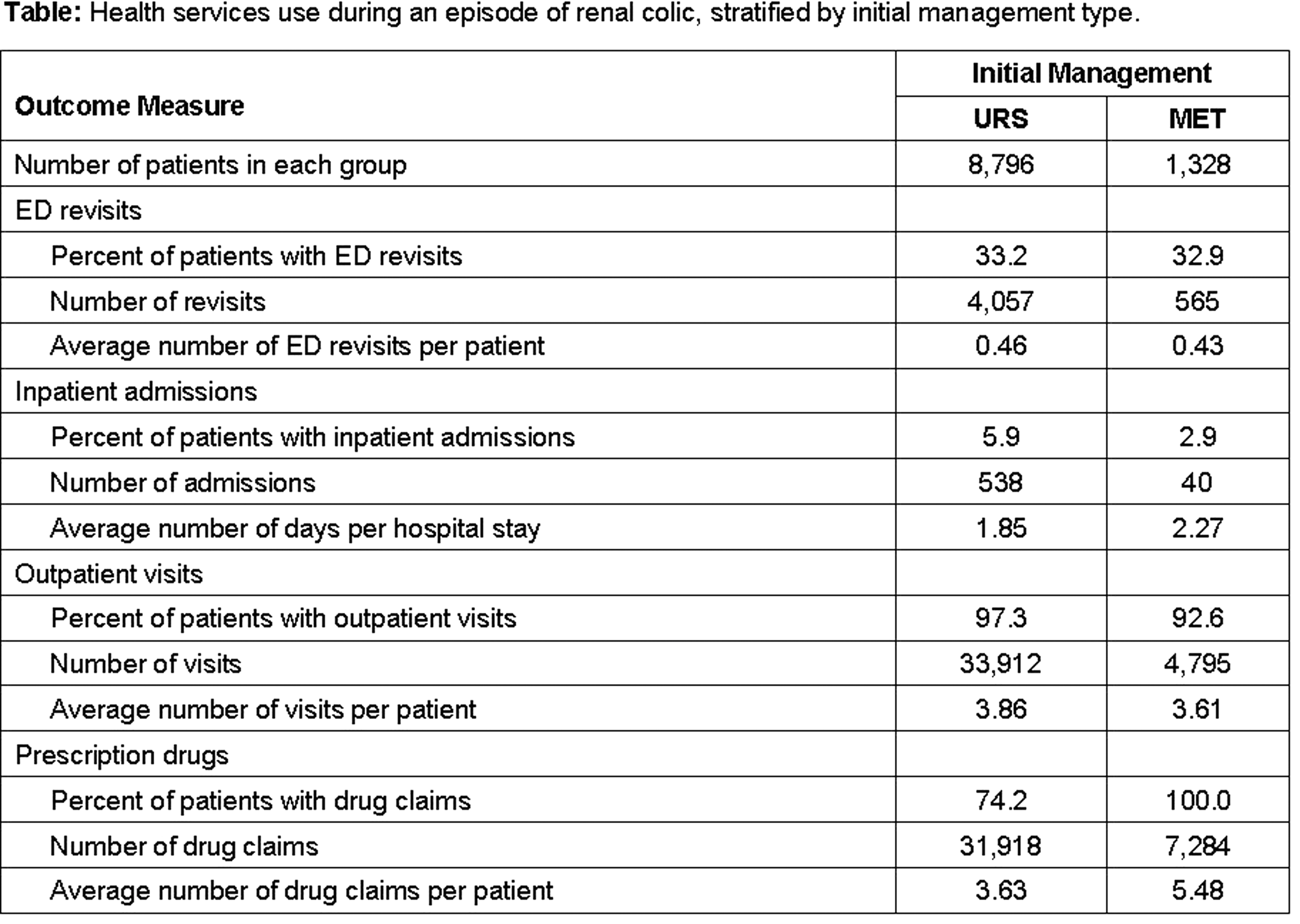
Retrograde Ureteroscopic Management of Upper Tract Stone Burdens >2 cm
Introduction: Advances in flexible ureteroscope design and accessory instrumentation have allowed more challenging cases to be treated ureteroscopically. Typically, large upper urinary tract stone burdens are managed via a percutaneous endoscopic approach. Purpose: To evaluate our experience with ureteroscopy for the management of upper tract stone burdens >2 cm. Materials and Methods: We retrospectively reviewed all ureteroscopy cases between 8/2007 and 3/2011 performed by a single surgeon (DHB) at an academic tertiary care institution. The stone database identified those patients with ureteral and/or renal stone burdens at least 2 cm managed with a retrograde ureteroscopic approach. Small diameter rigid and/or flexible fiberoptic ureteroscopes were used in combination with holmium laser (200 or 365 micron fiber) ±electrohydraulic lithotripsy. Patient demographics, intraoperative data, and postoperative outcomes were evaluated. Results: Over a 43 month period, a total of 55 patients (23 males, 32 females) underwent a total of 67 procedures for large initial stone burdens >2 cm. Mean patient age was 58.5 years (22-84). Mean number of procedures per patient was 1.2 (1-5). Stone laterality included right 26, left 22, and bilateral 7. Mean length of stay was 0.6 days. All stones were treated with holmium laser lithotripsy ±electrohydraulic lithotripsy (8). Stone size was a significant predictor of stone-free rate. Conclusions: Retrograde ureteroscopic lithotripsy is safe and efficacious for the management of large upper tract stone burdens >2 cm. Total stone burden is a reliable predictor for the need of a staged procedure.
Department of Urology, Columbia University Medical Center, New York, USA
Introduction: Balloon expendable ureteral access sheath (BEUAS) utilizes radial dilation mechanism for sheath placement. Earlier prototypes experienced significant rates of mechanical failure due to balloon rupture. Purpose: We aimed to assess performance of a redesigned BEUAS and compare it to that of a standard ureteral access sheath (SUAS). Materials and Methods: The BEUAS is both an access sheath and a balloon dilating device. The sheath is deployed under fluoroscopic guidance as a 9.5 Fr catheter. Using high pressure syringe, the inner balloon is expanded. The balloon is deflated and withdraw leaving 12Fr inner/15Fr outer sheath. Patients undergoing flexible ureteroscopy for lithotripsy were prospectively randomized into SUAS and BEUAS groups. Endpoints assessed included:time for sheath placement, rates of placement failures, ease of insertion, and stone free rate.Results: The median age was 48 years(range 19-82) and was not different between the groups. Mean OR time was 76.3 and 79.9 minutes (p=0.81) for the SUAS and BEUAS groups, respectively. Mean time for sheath placement was 132 and 160 seconds (p=0.43) for the SUAS and BEUAS groups. There were two sheath placement failures in each group. BEUAS was rated as "easy to insert" more frequently than SEUAS (80% vs 63%), and there was no difference with respect to stone free rates (p=0.2) between two groups. There were no complications in either group.Conclusions: Use of BEUAS for flexible ureteroscopy is safe and effective. It compares favorably to standard access sheaths, and was rated as easy to insert in the majority of cases.
Flexible Ureteroscopy for Renal Stones>1cm - the Method of Choice?
Introduction European guidelines do not currently recommend flexible ureteroscopy (fURS) as first line therapy for renal stones>1cm. We present our experience with fURS and holmium laser fragmentation for these stones.Materials and MethodsA retrospective review of patients treated since 2005 was carried out. Stone size was calculated using the longest axis of the stone at preoperative CT scan. Treatment success was defined as stone-free or fragments<2mm visible on X-ray KUB.Results66 patients had 71 treatments. Overall success was 57.6%. Mean stone size±SD was 23.3±8.4mm Treatment success was higher for stones<25mm compared with stones>25mm (68.2% vs. 36.4% p=0.009). 5 patients required repeat fURS for treatment success. Treatment success was dependant on stone location. Success rates for renal pelvis, upper pole, interpolar and lower pole was 80%, 58.3%, 66.7% and 34.6% respectively. Lower pole success rates were inferior to other stone positions (p=0.009). Mean upper pole stone size successfully treated was greater than other stone positions (28.71mm vs.20.12mm, p=0.003), and as a consequence renal pelvis and interpolar treatment success appear superior.ConclusionsRenal stones>1cm can be successfully treated with fURS and holmium laser fragmentation. Success rates of ∼70% are achievable for stones<25mm, usually after a single treatment. Success rates for stones>25mm with fURS are inferior and may require repeat treatment. Lower pole stones have inferior treatment outcomes compared with other renal positions and other treatment modalities should be considered where possible.
Villa Tiberia Experience in the Treatment of Renal Stones with Retrograde Intrarenal Surgery (RIRS)
INTRODUCTIONAim of this study is to show the results of Retrograde Intrarenal Surgery(RIRS) carried out with flexible URS for kidneystones in an our department.MATHERIALS AND METHODS68 patients were treated between January2008 and January2011. Variables and data analyzed included case load number, preoperative and postoperative imaging, stone burned, anesthesia(general or spinal), access location and size, operation time, JJ stenting or not;complication rate, the percentage of endoscopic second look and hospital stay.RESULTSPreoperatively, in 59 pts diagnosis was made with CT KUB scan, whereas in the follow-up 44 used CT KUB scan, while 19 pts kidney ultrasonography; X-ray and ultrasound only 5 pts. Mean stone burned was 2,05+0,56 cm;. General anesthesia was induced in 53 pts;In 32 pts the stones was in the lower pole, in 23 pts in the medium and in 13 pts;in the higher pole kidney;4 patients underwent ureteral ostium dilation. Operative time was 52+37 minutes. In 42 pts a single procedure resulted effective, thus 38,3% of patients were treated with RIRS plus ESWL (20,5% one ESWL, 17,6% multiple ESWL) .In 58 pts we placed a JJ stent. No blood transfusion but haematuria in 5 pts,;pain in 2 pts and urosepsis in 1 patient. Mean hospital stay was 2,8+1,9 days.CONCLUSIONSThe high success rates, relatively low morbility, short operative time and short hospital stay confirmed, in our experience, that RIRS with flexible ureteroscope is a;good choise of treatment for patients affected by intrarenal stones.
Department of Urology, Eulji University College of Medicine, Eulji University Hospital, Daejeon, Korea
Purpose: We prospectively examined patient satisfaction with treatment outcomes in patients treated with shock wave lithotripsy (SWL) and ureteroscopic lithotripsy (URL) for ureteral stones (US). Methods: From June 2009 to June 2011, we evaluated 160 consecutive patients who underwent SWL (n=65) or URL (n=95) for a single radiopaque US. Stone-free rates (SFRs), defined as no visible fragment on KUB, complications and patient satisfaction were compared. Patient satisfaction was examined through specifically tailored questionnaire which includes overall satisfaction (5 scales), 4 domains (pain, hematuria, voiding symptom and recovery to routine performance status), and willingness to retreatment. Results: The SFRs after the first, second, third and>4th sessions SWL were 61.5%, 81.0%, 93.5%, and 95.2%, respectively. The SFR after URL was 100%, which was significantly better than SFRs of the third sessions SWL (p=0.023). Complications were comparable in the two groups, except that gross hematuria lasting for>48 hours and febrile urinary tract infection was relatively more common after URL than SWL. While overall satisfaction was similar, satisfaction in hematuria, voiding symptom and recovery to routine performance status were significantly better in the SWL group than URL group (all p<0.05). For retreatment, 64.6% of SWL and 51.6% of URL group had willingness to the same treatment method (p=0.102).Conclusions: While overall patient satisfaction was comparable between the SWL and URL groups, satisfaction of SWL group was better than URL in 3 domains. Our results indicate that besides objective treatment outcomes, patient subjective satisfaction should be considered in counseling treatment methods for US.
A Comparative Matched-Pair Study Between Shock Wave Lithotripsy and Ureteroscopy For Proximal Ureteral Calculi
OBJECTIVE: To use a matched-pair analysis design to compare the safety and efficacy of shock wave lithotripsy (SWL) and ureteroscopy (URS), regarding whether SWL or URS is the best management of upper ureteral calculi.METHODS: We reviewed the records of patients with a single radiopaque upper ureteral stone treated by URS or SWL from January 2005 to December 2008. SWL was performed as an outpatient procedure using the electromagnetic lithotripter. URS was performed using an 8F or 9.8F semirigid ureteroscope. Intracorporeal lithotripsy with pneumatic or holmium laser energy was used when needed. A matched-pair analysis was performed using 3 parameters (sex, stone size, and degree of hydronephrosis). The success rates, retreatment rates, auxiliary procedures, and complications were compared in each group.RESULTS: A total of 458 patients were treated for upper ureteral stones. Forty-eight matched pairs were identified and compared. The success rate was 83.3% (40/48) for SWL vs 89.6% (43/48) for URS (P=0.08). The retreatment rate was significantly greater in the SWL group than in the URS group (54.2%, 26/48 vs 6.3%, 3/48 respectively; P<0.001). The need for auxiliary procedures was equal in both groups (10.4%, 5/48). The complication rate was 12.5% (6/48) in the URS group and 4.2% (2/48) in the SWL group (P<0.05).CONCLUSIONS: SWL and semirigid URS are highly effective in the treatment of proximal ureteral stones (<20 mm). The results of our study showed that SWL was safer and less invasive, but that URS was more effective and resulted in a lower retreatment rate.
Early Surgical Intervention versus Medical Expulsive Therapy for Renal Colic
Introduction: The benefits of medical expulsive therapy (MET) over active stone removal for management of renal colic may be mitigated by increased health services use among patients awaiting stone passage. Purpose: To compare the effectiveness of early surgical intervention with a strategy of MET and conservative care for patients with urinary stone disease. Materials and Methods: Using claims data (2002-2006), we identified patients with renal colic. We determined whether each patient received early (i.e., within 3 days of diagnosis) ureteroscopy (URS) versus a trial of MET. We followed patients for 6 weeks and measured their frequency of emergency department (ED) revisit, inpatient admission, outpatient visit, and prescription fill. We assessed total episode payments made on their behalf. Results: Patients managed with MET had fewer inpatient admissions (P<0.001) and outpatient visits (P=0.001), but more prescription fills (P<0.001) than those who underwent early surgery (Table). Compared to active stone removal, conservative care was associated with lower payments for ED (U.S. $2,210 versus $4,325, P<0.001) and outpatient care ($3,080 versus $4,829, P<0.001); however, drug costs were higher ($274 versus $219, P=0.001). Conclusions: Regarding resource utilization, MET with eventual URS, if needed, appears more effective than early URS for treatment of renal colic.
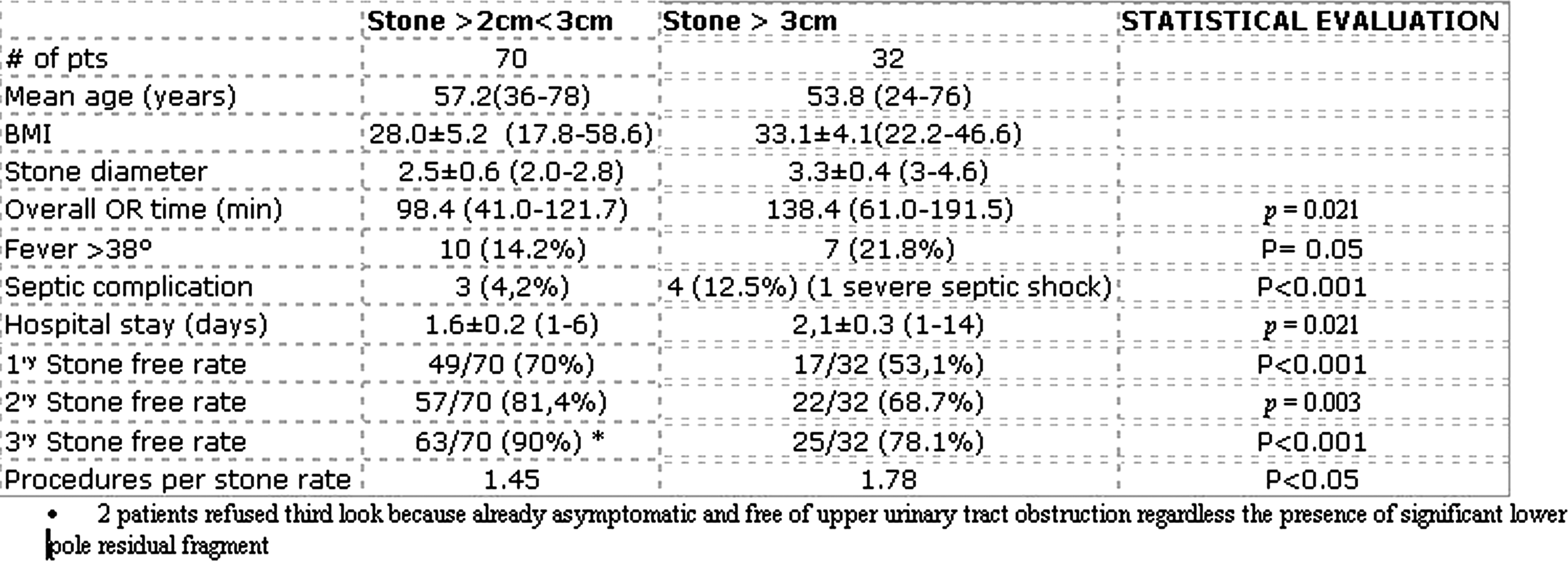
Cost and Clinical Outcomes of Percutaneous Nephrolithotomy vs. Ureteroscopy
Introduction: Percutaneous nephrolithomy (PCNL) and ureteroscopy (URS) are common procedures for managing large renal calculi. Stone clearance and cost were compared between PCNL and URS for 1.5-3.0 cm stones.Materials: Records of patients who underwent PCNL or URS for 1.5-3.0 cm renal stones from 2005 to 2009 were retrospectively reviewed. The URS group was divided into pre-stented URS (SURS) defined as ureteral stents placed at least 2 weeks before definitive treatment and non pre-stented URS (NSURS). Number of procedures, stone clearance rates and total costs (direct and indirect) were analyzed. Cost was calculated for each patient.Results: There were 160 PCNL, 22 SURS and 15 NSURS patients. Overall PCNL vs. SURS was equal ($16,258 vs. $15,175, p=0.59), both significantly less than NSURS at $30,051 (p=<0.001). Stones 1.5-2.0 cm demonstrated no difference among PCNL, SURS and NSURS costing $16, 549, $14, 365 and $19, 843 respectively. The average number of procedures for each group was 1. Stone clearance rates were 73%, 100% and 20% for PCNL, SURS and NSURS respectively. Stones 2.1-3.0 cm showed similar costs between PCNL and SURS ($16,057 vs. $21,972, p=0.263), both less than NSURS ($31, 212, p=<0.001). Average number of procedures was 1 for PCNL vs. 2 for both URS groups with stone clearance rates of 76%, 100% and 0% for PCNL, SURS and NSURS respectively. Conclusion: For stones 1.5-2.0 cm, SURS should be offered as first line therapy, while PCNL is superior for 2.1-3.0 cm stones due to decreased health care costs and re-operative rates.
Treating renal calculus 1-2 cm size with miniperc or RIRS; A prospective comparative study.
Introduction and objective: We planned a prospective comparative case control designed study aiming to compare miniperc and RIRS for renal calculus of size 1 to 2 cm.Material and methods:A total of 64 cases (32 in each arm) underwent miniperc and RIRS during the study period March 2009 and April 2011. The primary and secondary outcome objective were stone free rate and retreatment rate, complications, OR time, patient visual pain scores, analgesic requirement, hemoglobin drop and hospital stay, respectively.Results:Baseline demography was similar in each group. Miniperc and RIRS had stone clearance rates of 100% and 96.88%, respectively. One patient of the RIRS group required retreatment at 1 month. Hospital stay (0.24), Intraoperative (0.99) and post-operative complications (0.60) were similar in both groups. OR time (0.003*) was lesser in miniperc group. Hemoglobin drop (<0.0001*), patient pain VAS score (<0.0001* each) at 6, 24 and 48 hours and analgesic requirement (0.003*) was less in the RIRS group. 5 vs 27 patient required double J stent removal at 1 month follow up.Conclusion: The stone clearances in both the modalities are high and complications low. RIRS requires larger OR time but is associated with favorable pain scores and lesser hemoglobin drop.
Staged Retrograde Endoscopic Lithotripsy as an Alternative to PCNL: An Update
INTRODUCTION:Although percutaneous nephrolithotomy remains the gold standard for >2 cm renal calculi, staged retrograde endoscopic lithotripsy (REL) has gained acceptance as an alternative. We previously reported 23 patients who had undergone staged REL between 2003 and 2006. We now present our updated experience.METHODS:Medical records of patients who underwent staged REL by fellowship-trained endourologists between 2006 and 2010 were retrospectively reviewed. Successful therapy was defined as no residual fragments >2 mm.RESULTS:Forty-eight additional patients underwent staged REL for renal calculi. Patients in the updated cohort were more likely to be obese (BMI>30, 63% vs. 30%, p=0.01) with 31% morbidly obese (BMI>40) and fewer had a previous failed procedure (21% vs. 61%, p<0.05). Two patients underwent staged REL for an inability to establish percutaneous access (4%). Mean calculated stone volume was 7416 mm3 in the updated cohort. More patients progressed to second-stage operations (90.7% vs. 47.8%, p<0.001); nine (19%) required three or more. Stone-free rates were similar between groups (74.1% vs. 73.9%, p=1.0). In the 14 patients of the updated cohort with residual stone, five (36%) were due to an inability to deflect the ureteroscope to the lower pole. Linear stone burden >40 mm and stone volume>15,000 mm3 were associated with treatment failure.CONCLUSIONS:Our combined series of 71 patients represents the largest reported experience of staged REL. Patients with unilateral stone burden <4 cm and significant comorbidities should be counseled that REL provides stone-free rates greater than 70% but may require two or more operative sessions.
Medicana International Ankara Hospital, Department of Urology, Ankara, Turkey
Introduction: As a result of the improvements of flexible ureterorenoscopes FURLAS (Flexible Ureterorenoscopic Lasertreatment), with wellknown name RIRS (Retrograde Intrarenal Surgery) became a widespread treatment method for intrarenal stones. Desai described a custom made 14F Remote Catheter Control system in 2008. We presented a novel robotic device in EAU and AUA meetings of 2011 which controls remotely all functions of the commercially available ureterorenoscopes. Purpose: In this study we studied the effectivity and advantages of robotic flexible ureterorenoscopic treatment of the kidney stones.Materials and Method: We evaluated 21 patients with intra renal single stone, without ureteral obstruction. Although we could use all of the commercial devices and disposable flexible ureterorenoscope, we used 7,5F Storz Flex- X2 Flexible Uretero Reno Scope (FURS). After insertion of access sheath, we introduced the FURS manually and connected it to the robot. We recorded the time for connection and time for fragmentation. We scaled the remote control of functions. Results:Mean stone size was 19mm. (9-38mm). We remotely controlled all functions of FURS including rotation, deflection and the movement of laser fiber. We remotely adjusted the flow rate of the irrigation fluid from the control panel. We fragmented the stones while seated, outside of the radiation zone. After three month, stone free rate was 93%. Mean fragmentation time was 34min. The mean connection time of FURS to the robot was 1.3 minutes. Conclusion:Remote robotic control of the commercial flexible ureterenoscope provides the treatment of kidney stones, while seated, outside of the radiation zone.
Ureteroscopy: Role of Post-Operative Renal Ultrasonography
im of this study was to evaluate the use of rUS following ureteroscopy.MATERIALS & METHODSFrom March 2005 and October 2010 368 patients underwent semirigid or flexible retrograde ureteroscopy. We retrospectively reviewed all ureteroscopies performed by four surgeons and checked preoperative, intraoperative and postoperative details of each case. Average age was 42+11 years; 59,7% male and 40,3% female. Average stone size 13,9+5,6 mm (7 to 26 mm). The main broken stone was found in lower-medium ureteral tract (45,6%), followed by upper ureteral tract (27,7%), renal pelvis (12,5%), lower calices (7,3%) and upper calices (4,07%). Average operative time was 55 min (15; 130 min). All patients underwent a rUS follow-up protocol after 1 months.RESULTSPostoperative renal ultrasound was performed at a mean time of 54 days. Of 368 patients performing follow up 320 (78,2%) did not experienced ipsilateral flank pain. Of 34 (9,23%) patients having sonographic demonstration of hydronefrosis, 19 (5,16%) were asymptomatic and 15 (4,07%) experienced ipsilateral flank pain. There was no statistically significant difference between the asymptomatic and the symptomatic groups with respect to the need of further surgery. Postsurgical hydronefrosis detection rate in asymptomatic patients was one each 18 renal ultrasound.CONCLUSIONSRenal ultrasound (rUS) after 1 month ensures appropriate detection of asymptomatic hydronephrosis and should be considered a must during the post-operative follow-up.
Three cm is the cut off to maximize the outcomes of RIRS for renal calculi larger than 2 cm
Introduction: In the last few years, retrograde approach to renal calculi is becoming a reasonable treatment option even for renal stones larger than 2 cm and it is gaining quite large popularity among urological community. The objective of this study is to assess the stone size limit which is advisable not to extend the indication for RIRS beyond in order to maximize its outcome. MM: Since April 2006, 102 patients affected with renal stones larger than 2cm have been treated with RIRS. Patients have been divided in 2 groups being the diameter of 3 cm the cut off.Results: Results are reported in table 1. Conclusion: According with other reports in the literature, it is reasonable to consider RIRS a viable alternative to PCNL in case of renal stones larger than 2 cm. Nevertheless, our results demonstrate that 3 cm should be considered the cut off limit in stones diameter beyond which septic complications, stone free and procedures per stone rate is significantly compromised. As such, except for those cases where contraindications are present, in case of renal stones larger than 3 cm PCNL performs significantly better and should still be considered the procedure of choice.
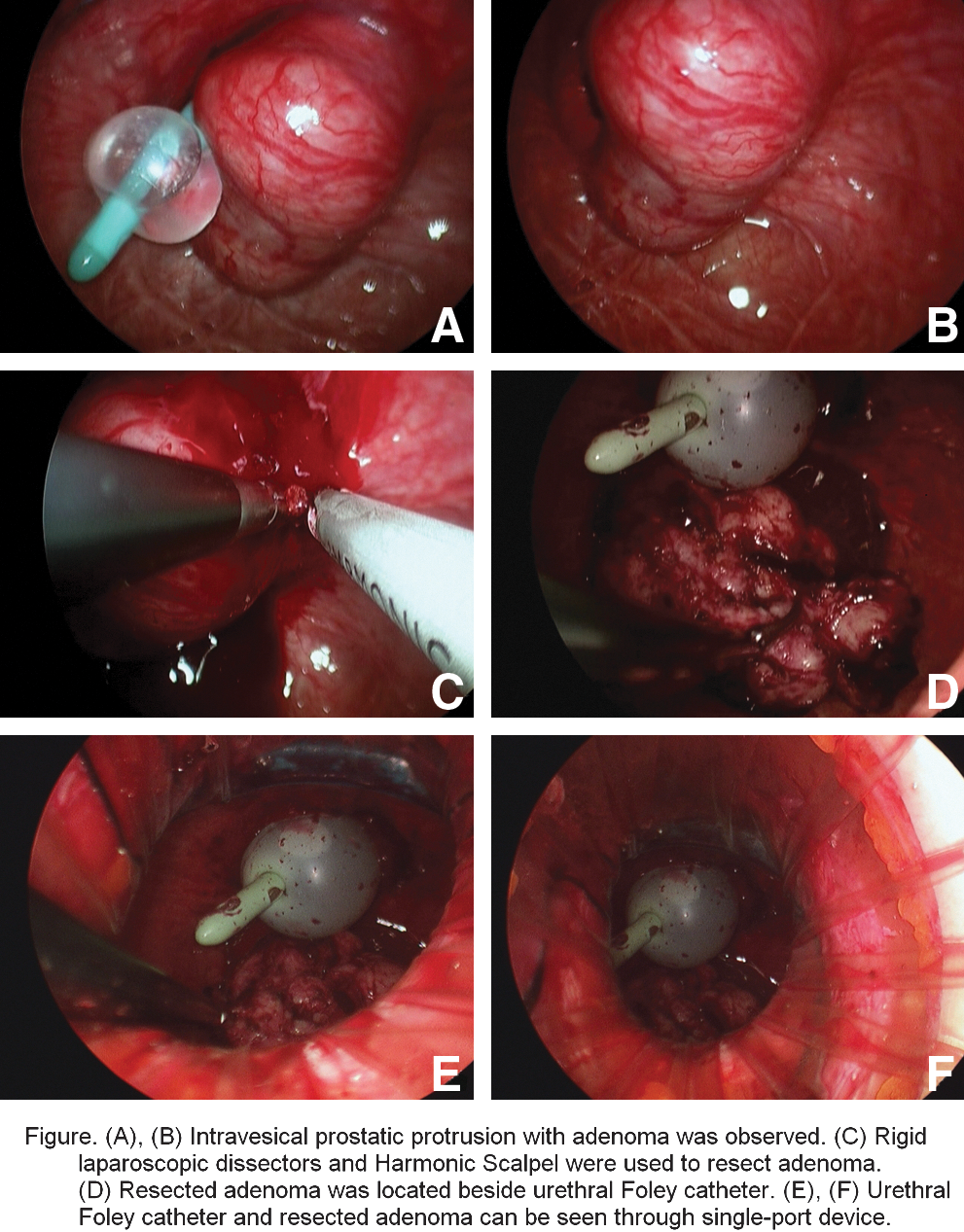
The treatment of proximal ureteral stone: percutaneous nephrolithotomy or ureteroscopic lithotripsy, which one is better?
Introduction: Percutaneous nephrolithotomy(PCNL) or ureteroscopic lithotripsy(URSL) have their own merits respectively for the treatment of proximal ureteral stones. The optimal treatment for the proximal ureteral stone remains controversial. Purpose: To compare the outcomes of PCNL and URSL for proximal ureteral stones with stone clearance rate(SCR)and complications. Materials and Methods: We retrospectively reviewed total 87 patients who had proximal ureteral stones. 41 patients treated with PCNL and 46 patients treated with URSL from January 2006 to April 2011. Pre- and postoperative plain films and/or ureteral CT scan were performed. Average follow-up were 1 month. SCR, perioperative data, complications were compared between two groups. Results: Stone burden in the PCNL and URSL group were 160.2±46.1 mm2 and 142.3±39.8 mm2 (p<0.05) respectively. The SCR was 80.5% (33/41) in PCNL group and 76.1% (35/46) in URSL group(p%gt0.05). Operation time was 40±16 minutes in PCNL group and 34±16 minutes in URSL group(p>0.05). Hospital-stay of PCNL group were 5.5±2.7 days and that of URSL group were 3.4±2.1 days(p<0.05). Two patients had sepsis in PCNL and URSL group respectively. Two patients received blood transfusion and four patients had renal pelvic perforation in PCNL group. Nine patients received ESWL for stone migrated into renal pelvic in USRL group. Conclusions: shorter hospital stay and less complications in group of patients who treated with URSL, but patients in this group would have higher risk of stone migration and more chances of secondary ESWL.
MP20: LESS/NOTES 4
Department of Urology, Hanyang University College of Medicine, Seoul, Korea
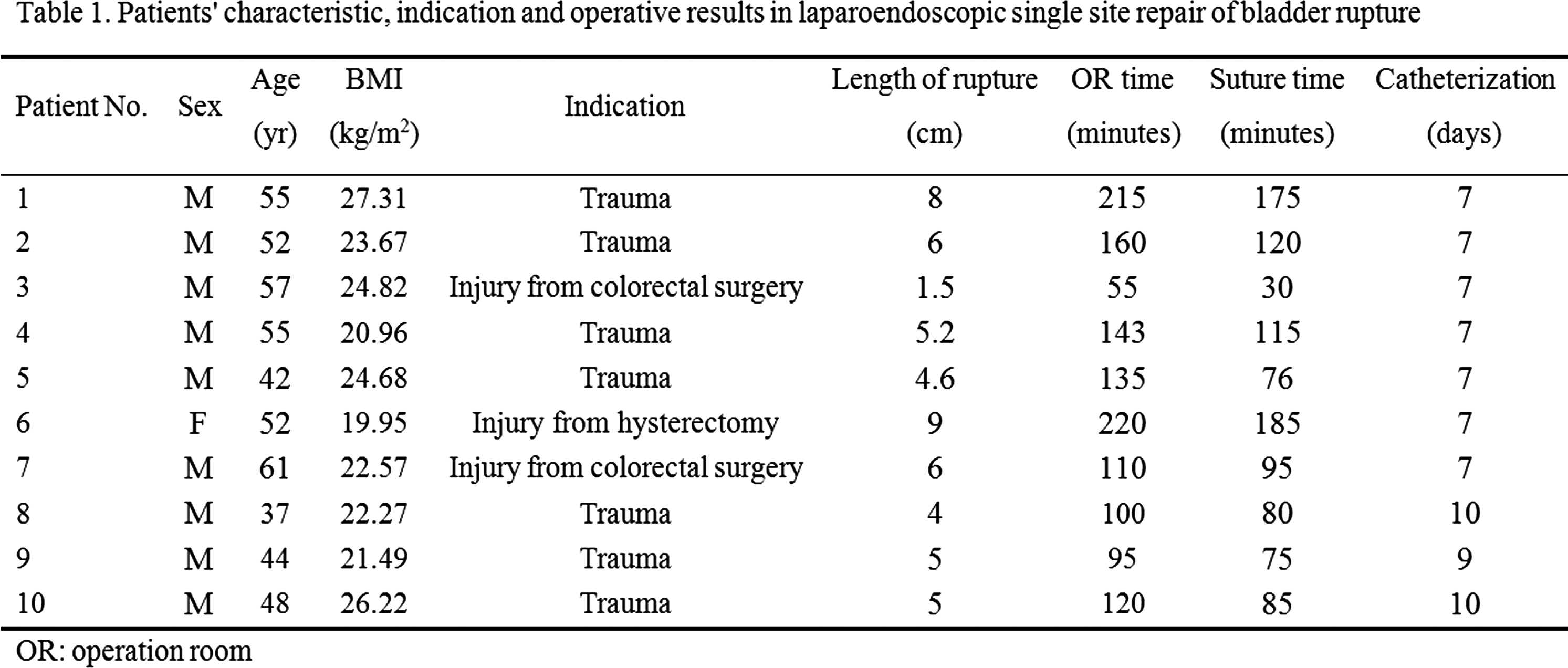
Harlachinger Krebshilfe e.V. am Klinikum Harlaching, Muenchen-Germany
OBJECTIVE: Up to 8% of patients, who undergo TURP/adenomectomy for BPH show in histology unexspected PCa. These patients need cancer therapy. In a prospective, monocentric study, we treated patients after TURP with HIFU as a definitive local therapy.MATERIAL AND METHODS: Since 2000 65 patients with incidental PCa were treated with robotic HIFU. Median (*) age was 70 (57-87), initial PSA was 4.9 (1-32), prostatic volume 39 cc (16-130), *20 gr (1-95) had been resected by TURP. Histology showed *5% (5-50%) positive chips with a Gleason of 5 (3-9). We used robotic Ablatherm integrated imaging, (EDAP-TMS, Lyon) in a single session. RESULTS: PSA Nadir of *0.07 (0-3.67) after *1.8 (0.7-5.9) months, including 62% with less than 0.1 / 81% withless than 0.5 ng/ml). PSA of *0.13 (0-8.3)was equivalent to a PSA velocity of *0.01 ng/ml/year after a mean follow up of 48 months (3-110) was registered.Follow up showed in 45% intermediate secondary obstructions caused by necrotic tissue or bladder neck stenosis. Other long term side effects were mild: intermediate urinary stress incontinence Grade I (11%) and UTI (14%). CONCLUSION: PSA Nadir of *0.07 ng/ml as well as a PSA velocity of *0.01 ng/ml/year indicate that HIFU can be used as a curative therapy for patients with incidental PCa. The psychological burden of patients who are confronted either with untreated cancer disease in cases of wait & see or with fear of significant side effects in cases of radical surgery or radiation can be avoided by this non invasive, transrectal, single session therapy.
Laparoendoscopic single-site radical prostatectomy with conventional instruments
Introduction The feasiblity and safty of laparoendoscopic single-site radical prostatectomy (LESS-LRP) with conventional instruments has not been properly demenstrated and need to be furter evaluated. Purpose To verify the safety and feasibility of applying LESS-LRP in the treatment of prostate cancer. Materials and Medthods From Sept. 2010 to May. 2011, we had used LESS-LRP treated 5 prostate cancer patients. The mean patient age was 74.8 (74-76 yrs). The mean body mass index (BMI) was 24.3 (19.5-32.2 kg/m2). The LESS-LRP was preformed through extra-peritoneal approach by using QudaPort (Olympus), tip filexible laparoscope with 0 degree lens (EndoEYE 5mm, Olympus) and conventional laparoscopic instruments. We evaluated this technique in operative time, estimated blood loss, intraoperative complications, drainage time, post-operative pain score (VAPS), pathological results and post-operative PSA levels. Results All procedures of the 5 cases were completed with LESS-LRP without additional trocar added and conversion to standard laparoscopic or open radical prostatectomy. The operative times for LESS-LRP were 249 (190-305 min), estimated blood loss were 320 (100-500 ml). There was no severe intraoperative complication. The drainage times were 4.8 (2-7 d), and the first post-operative day VAPS was 0.8 (0-3). There were 3 cases in pT2aN0M0 and 2 cases in pT2cN0M0. Surgical margins were all negative. The post-operative PSA was less than 0.02 ng/ml in all the cases. 4/5 cases were complete dry and 1/5 case was with 1 pad/day and improving. Conclusions LESS-LRP is feasible and safe. It can be an option for the treatment of prostate cancer.
Laparoendoscopic single-site extraperitoneal radical prostatectomy: Chinese experience
Transvesical Single-port Laparoscopic Radical Prostatectomy: 20 cases report
- Introduction The insufflated bladder might actually provide an optimal portal of access to the prostate and a direct in-line exposure of the prostate and relevant peri-prostatic anatomy. The transvesical approach obviates the need for mobilizing the bladder and dissecting the prevesical space, and might further reduce the risk of incontinence after radical prostatectomy.- Purpose To present the experience of transvesical single-port laparoscopic radical prostatectomy (TVSLRP). - Materials and Methods From June 2010 to July 2011, 20 patients with organ confined prostate cancer at low risk ( PSA <10 ng/ml; Gleason Score <6; T1b or T2a) underwent TVSLRP. A Quadport ® was deployed percutaneouly into the bladder to establish pheumovasicum through a 4-cm bladder incision. All the operative procedure including incision of the posterior bladder neck, dissection of the seminal vesicles and vas deferens, ligation of prostatic pedicles, preserving of neurovascular bundles, apical dissection, urethral transection, and urethro-vesical anastomosis, were performed transvesically and laparoscopically. - Results All cases were completed successfully, without conversion to standard laparoscopic approach. The total operative time was 75-180 min, the mean operative time was 105 min. The blood loss was 75-500ml, and no blood transfusion was required. The total hospital stay was 12-25 days. The Foley catheter was removed 9-16 days after surgery. No intraoperative complications occurred. No patient had positive margins. All the patients regained continence well after catheterization. - Conclusions TVSLRP under pneumovesicum is technically feasible and available for cases with early stage of prostate cancer.
Laparoendoscopic Single-Site Surgery Radical cystectomy
Objective: To present our experience and assess the feasibility of Laparo-endoscopic single-site(LESS) radical cystectomy.Patients and Methods: Between November 2010 and April 2011, 10 selected patients underwent LESS radical cystectomy for pathological diagnosed muscle-invasive bladder cancer. All procedures were performed through a single intra-umbilical X-cone port. A 5-mm port was inserted in the anterior axillary line to aid in tissue retraction and lymph-node dissection. Lymphadenectomy was performed using an extended template up to the aortic bifurcation. The parameters analyzed were operative time, blood loss, intra- and post-operative complications and hospital stay.Results: LESS radical cystectomy with bilateral pelvic lymph node dissection was successfully completed in 10 patients. All patients underwent extracorporeal urinary diversion by way of extension of the umbilical port site. The median (range) operating time was 336 (251∼492) min and the estimated blood loss was 246 (100∼500) mL. The median (range) hospital stay was 10.7(7∼18) days. The post-operation pathologic test showed negative margins and negative lymph node involvement in all patients. There were no intra-operative complications in 10 patients, though there was one postoperative case of ilues in neobladder patients.Conclusions: LESS radical cystectomy is technically feasible in select patients with invasive bladder cancer if performed by surgeons with standard laparoscopic skills. A larger cohort with long-term follow-up is necessary to validate our results and establish the role of this technique in treatment of invasive bladder cancer.
Laparoendoscopic single-site radical cystectomy:Chinese experience
Department of Urology, Hanyang University College of Medicine, Seoul, Korea
Pure-Laparoscopic Orthotopic Ileal Neobladder During Radical Cystectomy
Introduction: With development of laparoscopic techniques, Pure-intracorporeal urinary reconstruction may provide smaller incision and comparable surgical outcomes.
Purpose: To study the feasibility and efficiency of pure-laparoscopic orthotopic ileal neobladder during radical cystectomy.
Materials and methods:Six patients(3 male and 3 femal) with bladder cancer received laparoscopic radical cystectomy with intracorporeal orthotopic ileal neobladder. The pelvic lymphadectomy was done followed by total cystectomy. A 40cm ileal segment was chosen for urinary reservoir. Anastomosis staplers was applied for harvesting ileal segment and recovery of ileal continuity. The lowest position of ileal segment was anastomosed to posterior urethra by running suturing. Then antimesenteric ileal wall was incised with proximal 10cm ileum saved for anastomosis with bilateral ureter. Bowel loops was rearranged in a U shape and ileal plate was sutured to formed reservoir. Ureter stent was taken out through urethra in female and abdomen incision in male.
Results: All procedures were successful without open conversion and major intra/post-operative complications. Mean total operative time was 350min. Mean during for urinary diversion was 190min. Intraoperative blood loss was 500ml and one case received blood transfusion. Mean bowl movement occurred on 3 days and all patients have fluid diet on 5 days. Ureteric stent was kept for 7-10days and catheter was removed on 18-21 days. All patients have continence on discharge.
Conclusions: Pure-laparoscopic orthotopic ileal neobladder during radical cystectomy is feasible with the premise of laparoscopic skills.
Perioperative Results of Laparoscopic Radical Cystectomy
Radical cystectomy is the gold standard for the treatment of invasive bladder cancer. However, perioperative morbidity is not low.PATIENTS AND METHODS. Since December 2009 we performed 23 laparoscopic radical cystectectomy in 14 men and 9 wemen, median age 76 years. A 5-trocker transperitoneal approach with supraumbilical camera port was applied. Following laparocopic extended pelvic lymphadenectomy and antegrade dissection of bladder, an ileal neobladder and conduit was constructed extracorporeally in 10 and 11 patients. RESULTS. Laparocopic cystectomy was completed in 21 patients, whereas a conversion was required in 2 patients due to T4 disease. Median operative time was 355 min, blood loss was 570 mL and blood transfusion rate was 28%. Median time for lymphadenectomy was 107 min, for cystectomy 84 min, and for construction of neobladder or conduit 159 min. Patients begun food intake in POD 5. There was no perioperative mortality. Major complication (Clavien G3<) was seen in 3 patients (14%). CONCLUSION. Laparoscopic radical cystectomy is a feasible procedure with low blood loss and early bowel recovery. To determine the oncologic outcome long-time follow-up will be necessary.
Laparoscopic Repair of Supratrigonal Vesicovaginal Fistulae - Experience of a Tertiary Care Center in North India.
Aim: To present our experience of laparoscopic repair of supratrigonal vesicovaginal fistulae and their follow-up.Material & Methods: From September, 2009 to April, 2011; we treated 10 patients of supratrigonal fistulae by laparoscopic repair. Obstetric fistula was present in 6 and gynecologic fistula in 4 patients respectively. Single supratrigonal fistula was present in 8 patients while 2 patients had two fistulae lying side by side in the supratrigonal region. Transperitoneal transvesical laparoscopic repair with interposition graft was performed. In two patients, open conversion was opted for. Vaginal opening was closed in single layer (interrupted sutures) while cystotomy was also closed as single layer (continuous suture) with by 3-0 polyglactin. Omentum was used as interposition flap in all the cases except in one in whom the posterosuperior vesical fold of peritoneum was used. Urethral catheter was removed after 3-4 weeks following cystogram.Result: Mean fistula size was 1.2 cm (range 8 mm to 2.5 cm). Open conversion was resorted to in 2 cases; one had excessive carbon dioxide retention and cardiac arrhythmia while in another, suture needle was lost in peritoneal cavity (recovered following laparotomy. All patients are continent following the catheter removal. Conclusion: Laparoscopic repair of supratrigonal vesicovaginal fistula is effective minimally invasive treatment with good outcome.
Laparoscopic Radical Cystectomy : Our Experience of 42 Patients
Objective: We report our experience with laparoscopic radical cystectomy(LRC) for localized bladder cancer unfit for bladder preservation in 42 patients.Methods: Between October 2004 and July 2011, 34 men and 8 women aged from 28 to 91 years (mean 70) underwent LRC. Retrospectively, the operative and oncological outcomes were compared with those of historical controls undergoing open radical cystectomies in our institute (n=30).Results: The median follow up is 35 months (range 1 – 80). The median operative time is 508 min (range 230 – 727). The median blood loss is 735 ml (range 20 – 9980). Urinary diversions were performed in 40 patients. Postoperative complications were observed in 14 patients and 2 patients were required surgical treatment. Paralytic ileus occurred in 4 patients, but the number of paralytic ileus in LRP group was less than that of open radical cystectomy(ORC). Median estimated blood loss was lower than ORC. Mid term oncological result is comparable.Conclusions: LRC seemed to be a less invasive and feasible technique for invasive bladder cancer, but this procedure has not yet matured to promise the long-term oncological outcome. Further investigation is needed to answer this question.
Robotic Ureteroneocystostomy: a Comparison to the Open Procedure
Introduction and objective:Robotic ureteroneocystostomy (RUNC) can be used for treatment of stricture disease, cancer, or iatrogenic injury. Herein we compare perioperative outcomes for RUNC and without use of psoas hitch and boari flap to open ureteral reconstruction (OUR).Methods: We identified 26 patients who underwent RUNC at our institution from 2007-2010 and 33 patients who underwent OUR from the period of 2000-2010. Data was collected retrospectively including preoperative demographics, perioperative data, and clinical and radiographic follow-up. Results: No significant difference was noted in terms of age (p=0.9), BMI (p=0.3) and American Society of Anesthesiologists score (p=0.4) between the 2 groups. OUR procedures were performed with a shorter median operative time (229 vs. 267min., p=0.04). RUNC patients had shorter hospital (3.5 vs 5 days) (p=0.0004), less narcotic requirements in morphine equivalents (82 vs 318) (p=0.0001) and less estimated blood loss (100 vs 275 mls) (p=0.0001). One patient in the robotic cohort required additional procedures, and radiographic success was noted for all patients. In the open surgical group one patient had a wound dehiscence and needed reoperation and another patient had persistent pain, radiographic evidence of obstruction, and a nephrostomy tube was placed. Conclusion: Robotic ureteroneocystostomy provides excellent outcomes with shorter hospital stay and less narcotic pain requirement when compared to the open procedure. Advantages of the robotic platform for dissection and suturing are quite useful for complex minimally invasive reconstructive procedures.
Intracorporeal Robotic-assisted Laparoscopic Ileovesicostomy
Introduction:
Ileovesicostomy is a long-term surgical management option for patients with neurogenic bladder who have failed medical or other conservative therapies.
Purpose:
The purpose of this retrospective study is to report our initial experience with robotic-assisted completely intracorporeal ileovesicostomy. Potential benefits with this technique compared to ileovesicostomy with extracorporeal bowel anastamosis include smaller incisions, quicker return of bowel function, decreased wound infections and fewer incisional hernias.
Materials and Methods:
A retrospective review between April 2010 and May 2011 identified all patients who underwent a robotic-assisted ileovesicostomy at our institution. Preoperative, intraoperative and postoperative data, including functional outcomes with a minimum of 3 months follow-up, were analyzed. All bowel work was completed intracorporeally except for stoma maturation at the end of the procedure.
Results:
Four robotic-assisted ileovesicostomies were performed between April 2010 and May 2011. The mean patient age was 49.3 years and mean BMI was 26.8. Pre-operative urinary dynamic studies revealed elevated detrusor pressure or limited bladder capacity. Patients were unable to perform intermittent catheterization for bladder management. Average EBL and operative time were 131.3 mL and 289.5 minutes respectively. No intra-operative complications occurred. Bowel function, defined as flatus, returned on average 3.3 days after surgery and the average length of stay was 6 days. Mean follow-up time was 8 months. One patient had continued urethral incontinence after surgery that was successfully treated with placement of a suburethral sling.
Conclusions:
The first four cases of a completely intracorporeal robotic-assisted ileovesicostomy were successfully completed without open conversion and without major complication.
Robotic Extravesical Reimplantation for Lower Ureteric Strictures.
Material and methods: We retrospectively ananlysed 6 patients who underwent robotic ureteric reimplantation for lower ureteric strictures for various causes between may 2009 and april2010.Results: Average age of patient was 40 years there were 5 male and 2 females. Average operative time was 242 mins. Patients required an average of 150 mg of morphine equivalents post operatively. Patients were on full oral without any IV fluids at an average of 42 hours posts operatively and technically could have been discharged at that time. There were no intraoperative complications and only few minor post operative complications like conjunctival irritation and uti. Average hospital stay was 6.66 days. Average follow up after DJ removal was 3 months in 6 patients and awaited in 1 patient. All surgeries were performed by 1 surgeon except the last case. Operative time has come down from 245 min in the first case to 165 minutes in the last case of the more experienced surgeon. The video demonstrates the point of technique in robotic assisted ureteric reimplantation and also compares the same with conventional laparoscopic ureteric reimplantation done at our institute.Conclusions: Robotic ureteric reimplantation is a feasible procedure with good short term results .It combines the advantages of both laparoscopy and open surgery. With instruments with 5 degrees of freedom 3 d vision, reconstructive procedures can be performed with greater accuracy.Albeit after a small learning curve in a previously experienced laparoscopic surgeon.
Complex Robotically Assisted Pelvic Surgery in the Setting of Prior Ostomy
Contemporary laparoscopic surgery requires the development of a safe and adequately insufflated working space. It has been estimated that the North American ostomy population alone is between 750,00 and 1 million patients, but the feasibility of robotically assisted surgery in these patients has not been assessed.The anatomic alterations associated with ostomy can pose a significant challenge to laparoscopic surgery: adhesions may complicate entry into the peritoneal cavity and hamper development of adequate working space. Laparoscopic navigation in the setting of a bowel segment affixed to the anterior abdominal wall may be complex, especially given the need for appropriate relative geometry of visual and working port placement. We present an initial series of 5 patients who safely underwent robotically assisted complex pelvic surgery in the setting of prior ostomies. MATERIALS AND METHODS:5 patients were identified that had prior abdominal-wall ostomies and indications for surgery (Table 1).RESULTSResults are presented in Table 1. CONCLUSION:Robotically assisted laparoscopic surgery can be safely and successfully undertaken in the setting of prior ostomy with acceptable operative times, no additional morbidity and excellent outcomes. This series represents an useful step in the continued expansion of indications for laparoscopic surgery.
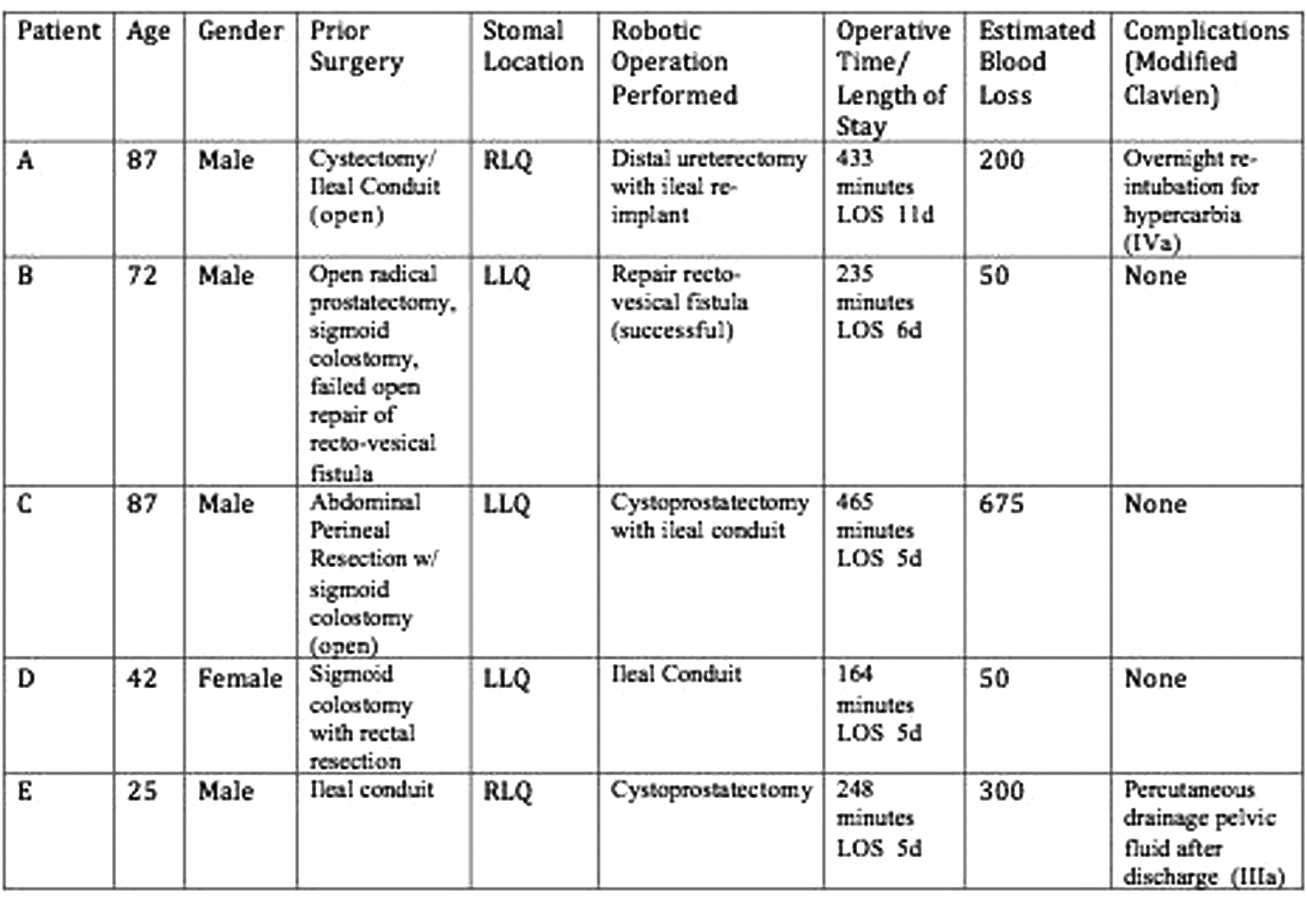
Laparoendoscopic Single-Site Assisted Transsexual Surgery
MP21: Kidney, Urinary Tract, Endurology/New Technology
Percutaneous Nephroscopy Combined With Fiber Cystoscopy For Treatment Of Renal Transplant Ureterovesical Anastomotic Stenosis
Objectives: Explore the feasibility of percutaneous nephroscopy combined with fiber cystoscopy in the treatment of renal transplant ureterovesical anastomotic stenosis.Material and Methods: A 40-year-old women received allograft renal transplantation because of the chronic renal failure. MRI showed pyelocaliectasis and ureterectasia, ureterovesical anastomotic stenosis. She received two stages operation. During stage I, percutaneous nephrostomy was implemented. F14 balloon nephrostomy tube was placed into it for two weeks.During stage II, Imbedding the channel under guided wire. Overlapping metal dilator expanded the channel to F24 wide. We inserted the fiber cystoscopy(F16, Olympus, Japan) along with the channel to locate the uroteropelvic junction, then went down to the bottom of ureter until. Then insert the ureteroscopy( F8/9.8 WOLF, Germany) transurethral access to the bladder. Shut one side light source of endoscopy, located the position with contralateral bright spots,cut the mucosa with flexible electrode.An guide wire was introduced into it followed by the dilator to expand the channel to F14 wide gradually. An 12F ureteral stent was retended at the end of operation.Results: The peration cost 90 minutes and got off the ground, the daily urine output was 2000 to 2500ml when the nephrostomy tube removed. Serum creatine fell down to 143umol/L two days later. After 3 monthes follows-up, the patients recoverd well.Conclusions: The use of percutaneous nephroscopy combined with fiber cystoscopy in treatment of renal ureter bladder anastomotic stenosis is effective. Endoscopic technique can be more easily to reach the operative site which is definitely improve the success rate of surgery.
Is it Possible to Avoid Second TUR in High Grade Bladder Cancer after a First TUR Performed in NBI Modality?
Second TUR is a standard treatment of newly diagnosed high grade non muscle invasive bladder cancer. We identified a cohort of 45 patients submitted to second TUR who were randomized to NBI, 26 subjects, or standard, 19 subjects, first TUR in a clinical trial registered with the code NCT0100421. Second TUR was performed in the same modality of the first TUR. Overall 11 patients had residual/recurrent cancer (24%), 5 (19%) in the NBI group and 6 (31%) in standard group (p 0.548 Yates-corrected chi-square); particularly 9/11 (4 pure Cis, 1 concomitant Cis) cases carried high grade cancer. Regarding detection rate, 153 and 114 overt or suspect lesions were retrieved in the NBI and in the standard group of which 15(10%) and 9 (8%) were respectively positive (p 0.746 Yates-corrected chi-square). Therefore 15 cancerous lesions were identified in 5 patient, 3 lesions per patient, in the NBI group and 9 lesions in 6 patient, 1.5 per patient, in the standard group (p 0.21 unpaired Student T-test). Given the consistent rate of positivity of second TUR in both groups, present data do not support to avoid second TUR in patient submitted to TUR of newly diagnosed high grade bladder cancer irrespective of the modality used. Nevertheless the trend is towards less incidence of residual/recurrent cancer in the NBI group which indeed detected more cancerous lesions per patient.
NBI TUR Improves the Detection rate of Bladder Cancer and Leaves the Bladder more Receptive to the BCG Topic Treatment
BCG is the standard treatment to improve recurrence rate of high risk non muscle invasive bladder cancer. We identified a cohort of 42 patients submitted to BCG topic therapy who were randomized to standard, 18 subjects, or NBI, 24 subjects, TUR in a clinical trial registered with the code NCT0100421. The 2 groups have similar clinical and pathological characteristics. Median follow up is 11 months, range 1 to 19. Overall, 64 lesions were accounted, respectively 45 in the NBI group (1.875 lesions per patient) and 19 in the standard group (1.06 lesions for patients). 11 (26%) of the subjects experienced a recurrence at a median time of 6 months, 3 in the NBI group (12.5%) and 8 (44%) in the standard group (Yates corrected qui square p 0.048). The number of lesions identified in the NBI group was greater even if it does not reach the statistical significance (p 0.57 unpaired Student T test). However the increased detection translates in a bladder more receptive to BCG and consequently in a lower recurrence rate.
The Multisequence MRI is a Highly Accurate for Staging Bladder Cancer
Introduction: Multisequence MRI is rarely used as a staging tool in bladder cancer. We explored a feasibility of preoperative multisequence MRI including T1 and T2 weighted images, pre- and post-contrast 3-D imaging, and diffusion weighted imaging to stage bladder cancer. Material & Methods: Between 2009 and 2011 25 patients with bladder cancer underwent multisequence MRI with a 3T device (Signa GE Medical Systems, Milwaukee, WI). Statistical analysis using chi-square was performed to define correlation between imaging and pathology data to distinguish non- from muscle invasive cancer and to assess pelvic lymph nodes status.Results: The multisequence MRI was able to correctly stage bladder cancer in all 12 cases as validated by pathology assessment of tissue removed by TURBT or specimens after cystectomy. T1 weighted images in the axial or coronal plane provided a high resolution visualization of the pelvis and lymph nodes. T2 weighted images in all three orthogonal planes revealed information on structure and delineation of detrusor muscle. Pre and post contrast 3-D imaging and diffusion weighted imaging allowed exact volumetric acquisition, enabled multiplanar reformatting and demonstrated tumor enhancement.Conclusion: The results of this pilot trial demonstrated a high accuracy of multisequence MRI for staging of bladder cancer. Large-scale clinical studies are currently underway to further provide proof of concept.
SAN DIEGO VA MEDICAL CENTER
INTRODUCTION:Nodal status is important in bladder cancer. Tilmanocept, or DTPA-mannosyl-dextran, or Lymphoseek has the advantage of specificity to lymph nodes and has been used for sentinel lymph node (SLN) mapping. PURPOSE:Our study was to evaluate the feasibility of porcine model to perform transurethral cystocscopic injection of Lymphoseek.METHODS:Six adolescent female pigs were anesthesthetized. The Lymphoseek was injected into the bladder mucosa through flexible cystoscope. Fifteen minutes after the injection, the lymph nodes at the aortic bifurcation, bilateral common iliac, external iliac and obturator areas were removed to simulate the lymph node dissection during cystectomy in human. The nodes were considered to be positive, or were SLN, if the radioactivity was 4 times the background using the hand held gamma counter probe. The precent-of-injected dose was calculated by assaying each excised lymph node using standard gamma well counter. RESULTS:Four pigs underwent successful injection of the mixture into the bladder wall. At least 1 SLN was recovered from each animal with successful injection of Lymphoseek into the bladder wall. None of the 2 pigs with unsuccessful injections had SLN. The mean (SD) count rate of the hand-held gamma detector and the mean (SC) percent-of-injected dose for SLN were 7,383±9153 and 0.32±0.25 %, respectively.DISCUSSIONS:At least 1 SLN was detected in pigs with injection and no SLN in pigs without the injection. Porcine model for transurethral cystoscopic injection of Lymphoseek is a viable model for the study of SLN mapping in bladder.
Hackensack University Medical Center
Introduction and Objectives:Nephron-sparing surgery has become the standard of care for small renal cortical neoplasms. We report the minimally-invasive management and outcome of urinary fistulae after open partial nephrectomy (PN).Methods: The operative records of a single surgeon performing open PN were reviewed. Patients with clinical evidence of a urinary leak were identified. Clinical evidence of a urinary leak included drain output greater than 40 mL per shift or drain creatinine more than twice serum creatinine. The incidence of spontaneous resolution of the urinary fistulae and the need for intervention to manage the fistulae was recorded.Results:A total of 179 patients that underwent open PN were included for review. The incidence of urinary fistula was 12.8% (N=23). Only 5 of these patients (22%) required ureteral stenting, while the remaining 78% of urinary leaks resolved with prolonged JP drainage. Percutaneous drain placement or open exploration was not necessary in any case. The majority of the ureteral stents were placed early in the PN series. Conclusions:The incidence of urinary fistula after open PN is low, occurring in 12.8% of patients in this study. Of those patients with clinical evidence of urinary leakage after PN, 78% resolved spontaneously without the need for intervention. The success rate of minimally-invasive treatment of urinary fistulae with ureteral stent was 100%.
Robot assisted laparoscopic repair of gynecological iatrogenic lower urinary tract injuries.
Introduction: It is estimated that between 50% and 80% of all surgical complications involving the LUT are associated with gynecologic surgery, as a result of the anatomic proximity of the reproductive and lower urinary tracts (LUT). Most injuries are managed in a delayed fashion through a standard open surgical approach due to associated severe scarring. We present our experience with robot assisted management of immediate and delayed gynecological iatrogenic LUT injuries.Materials and methods: Form December 2006 to April 2011, 13 females were diagnosed with iatrogenic LUT injuries following gynecological surgery and repaired via a robot assisted approach. Patient demographics are summarized in table 1. Results: All 13 cases were successfully completed robotically without any conversions. Mean operative time and blood loss was 165.8 minutes and 51.5 ml. Patients were discharged with no major perioperative complications at an average hospital stay of 2.7 days. A mean follow-up of 7.46 months, showed no cases of urine leakage or urinary tract obstruction.Conclusion: Advances in technology, experience, and familiarity with robotic surgery are enabling repair of LUT injuries via a robot assisted approach to be an effective and safe option consistent with the principles of open repair.
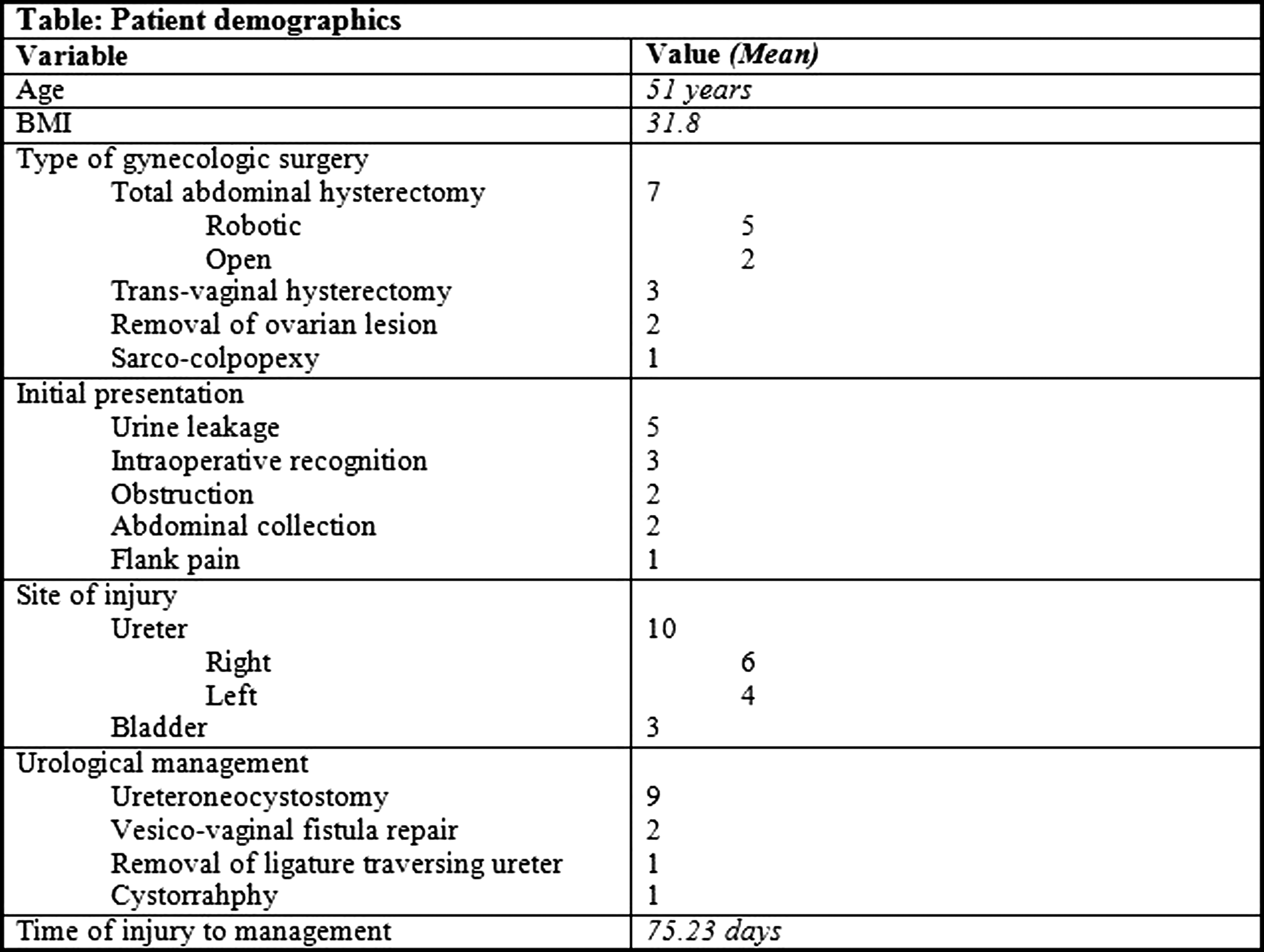
The Department of Urology, Darent Valley Hospital, Dartford, Kent, U.K
Management of upper tract problems (UTPs) is technically difficult in patients who have had cystectomy and have ileal conduits or neobladders. We present our experience of these challenging cases.Methods: In this multicentre study, 44 patients who following cystectomy, developed UTPs over the 5 years were studied. Six patients had Studer neobladder and 38 had an ileal conduit. The median time taken for the development of UTPs after cystectomy was 3 years (1-6 years) and their median age was 71years (51-84). Routine follow up imaging picked up UTPs in 28 asymptomatic patients and the rest presented with loin pain or renal impairment. Significant stone burden was present in the kidney or upper ureter in 22 patients. Ureteric and renal pelvic tumours were seen in 5 and strictures of the uretero ileal/ureteric- neobladder anastomosis were seen in 15 patients. Results: All 23 stone cases were treated with PCNL. Four of the five renal pelvic/ureteric tumours were treated with percutaneous nephro-ureteroscopic holmium laser ablation. Fourteen of the anastomotic strictures were treated with holmium laser endoureterotomy. Three patients required open surgery: one for removal of stent that slipped into Studer Chimney and two required nephroureterctomy with reformation of ileal conduit for ureteric and anastomotic recurrences. Nine patients undergo annual stent changes and three patients died of metastasis. Overall 93.2% (41/44) of patients were managed successfully.Conclusion: Although UTPs in this select group is difficult to manage, our experience illustrates that majority of these problems can be dealt with using endourological techniques achieving satisfactory results.
Hackensack University Medical Center
IntroductionUreteral complications after renal transplantation are often managed via percutaneous renal access. Retrograde endoscopic access, while technically challenging, can offer a less morbid treatment option.PurposeWe describe a contemporary series of patients undergoing retrograde management of ureteral complications after renal transplantation.Materials and MethodsThe records of patients presenting with ureteral complications after renal transplantation were reviewed. Those patients who underwent attempted retrograde management of the complication were included in the analysis. All patients had undergone Lich-Gregoir ureteral reimplantation at the bladder dome.ResultsA total of 8 patients underwent 19 retrograde endoscopic procedures to manage ureteral pathology, including hydronephrosis, ureteral stricture, and migrated ureteral stent. The success rate of the 19 procedures was 74%. In 2 cases, the stent would not pass over an appropriately positioned wire, and in 2 cases the wire would not pass beyond the distal ureter. In 10 of the successful procedures, a Berenstein angiocatheter was utilized. The success rate appeared to increase over time, with the most recent 5 attempts at retrograde access successful. ConclusionsRetrograde endoscopic management of ureteral complications after renal transplantation is feasible and offers a less morbid treatment option. In our experience, the Berenstein angiocatheter was a valuable tool for accessing the transplant ureteral orifice. The success rate of attempted retrograde ureteral access improved with experience.
The role of interventional radiology in the management of complications of renal transplantation-A comprehensive review
OBJECTIVES: Renal transplantation, the definitive and curative management for patients with end-stage renal disease, is effective, safe, and widespread, and being performed in more institutions. Therefore, as more transplants are done, more associated problems and complications are found. Our institution is pioneer in renal transplantation in USA and world. Therefore, we have acquired a vast experience on the management of its complications. METHODS: Few comprehensive reviews are available. Therefore, we review our experience in the IR management of most complications including (a) vascular and (b) non-vascular. Vascular: PTA of renal artery stenoses, stenting of renal arteries, arterial and venous thrombolysis, placement of filters in the IVC and iliac veins, embolization of AVFs secondary to kidney biopsy. Non-vascular: Percutaneous nephrostomy, internal and external urinary drainage, dilatation of pelvic and ureteral strictures, stenting of ureters, drainage of lymphocele and other fluid collections, needle aspiration and core biopsies, and others. RESULTS: Most, if not all procedures, are successful in managing all the minor and major complications listed above. CONCLUSIONS: The IR are one the most important members of the team managing renal transplant complications. The IR procedures are simple, quick, safe, effective and cost-effective. Surgery with its attendant morbidity must be avoided, if possible. The IRs must be available 24 hours a day, 7 days a week. Every effort must be made to salvage a transplanted kidney as the shortage of organs for transplantation is critical in our country.
MCV Hospitals/VCU Medical Center
OBJECTIVES: Each year 200 new patients with ESRD per 1,000,000 people in USA. Population at risk is 50-60,000 patients. Patients are managed with hemodialysis (HD) via arteriovenous fistula (AVF), peritoneal dialysis or central catheter and with a renal transplant. Critical shortage of organs and many patients are not candidates for transplant. Complications are common. Our institution pioneered in the world in renal transplantation, with vast experience in management.METHODS: IR plays very important role in management of patients with ESRD with two main types of interventions: (A) Management and maintenance of complications of HD accesses - AVF and central and peritoneal dialysis catheters; (B) Management of complications of renal transplantation. Complications: (a) vascular, (b) urologic, and (c) iatrogenic. We illustrate IR management with many examples of most events. The dual role of IR in insertion of central and peritoneal catheters and in management of complications associated with central catheters and AVF (both native and with graft) illustrated with many examples.RESULTS: All IR procedures are safe, quick, successful, and cost effective in long-term maintenance of patients with ESRD.CONCLUSIONS: IR plays an important role in the management of patients with ESRD with: (A) Insertion of central and peritoneal catheters for dialysis; (B) Management of complications of central catheters; (C) Management of complications of renal transplantation; (D) Management of complications of AVF. IR must be ready and available in all institutions performing renal transplantation, placement of AVF and insertion of central and peritoneal catheters for dialysis in patients with ESRD.
Ablation of Small Renal Masses: Practice Patterns at Academic Institutions in the United States
Introduction: With the increasing use of cross-sectional imaging, the incidence and detection of small renal masses has increased in the United States. We aimed to determine the current practice patterns at academic institutions in the use of ablative technologies for the management of small renal masses. Methods: Mail surveys were sent to 124 academic institutions in the United States. The survey consisted of 12 questions pertaining to the institutional use of ablation technology for treatment of small renal masses and the role of the urologist in evaluation and treatment. Results: The overall response rate was 52%(64/124). Ablation was offered by all of the responding academic centers. Specific modalities included: percutaneous cryoablation(75%), percutaneous radiofrequency ablation(RFA)(52%), laparoscopic cryoablation(83%) and laparoscopic RFA(19%). Eighty eight percent of institutions performed 1-5 ablation procedures each month. Percutaneous ablation procedures were performed by a radiologist alone (43%) or by a combined approach with both urologist and radiologist present (45%). In combined procedures, the urologist role included: present at the time of ablation (59%), placed the ablation probes (32%), was responsible for the post-operative care (98%). Pre-ablative biopsy of the mass was performed at 89% of academic institutions with the biopsy being performed prior to the day of the procedure in only 19% of responding institutions. Conclusions: Ablative technologies are widely utilized for the treatment of small renal masses at current academic institutions with urologists participating in the ablation procedure in half of the institutions. While pre-ablation biopsy is common, pathology is rarely known prior to ablation.
Ex-Vivo Model for Renal Fracture in Cryoablation
Introduction: Renal fracture is a recognized complication of cryoablation, comprising as many as 4% of the complications reportedpurpose : to demonstrate the formation of fractures due to cryoablative therapy in a controlled model. Methods: Endocare Perc-17 (1.7 mm) and Galil 17 gauge IceRod (1.47 mm) probes were selected because of similar diameter and reported ice ball size. The ex-vivo model used here is a kidney obtained at the supermarket. They are provided without the renal capsule, but this is not needed. The kidneys were subsequently bivalved. The cryoprobes are inserted running and just underneath the cut surface, entering the lateral surface of the kidney directed towards the medial surface of either upper or lower pole, avoiding the major calyces and involving the most parenchyma. Freeze-thaw-freeze cycles of various durations were performed. The probes were frozen individually and parallel 20 or 25 mm apart. Results: Fracture formation was only observed with the Endocare probes, with single or parallel freezes. No fractures were noted in the IceRod freezes. Evidence of fracture included popping sounds noted during thaw and visible cracks that became evident during the phase of second freeze (Figure 1). Cracks were noted to extend from the probe through parenchyma. In multiple probe freezes the intervening zone between the two ice balls has the smoother ice and the fractures that appear there originate at either probe and extend through this area. Conclusion: The bivalved ex-vivo kidney is an inexpensive, representative and demonstrative model for study of fracture during cryoablation.
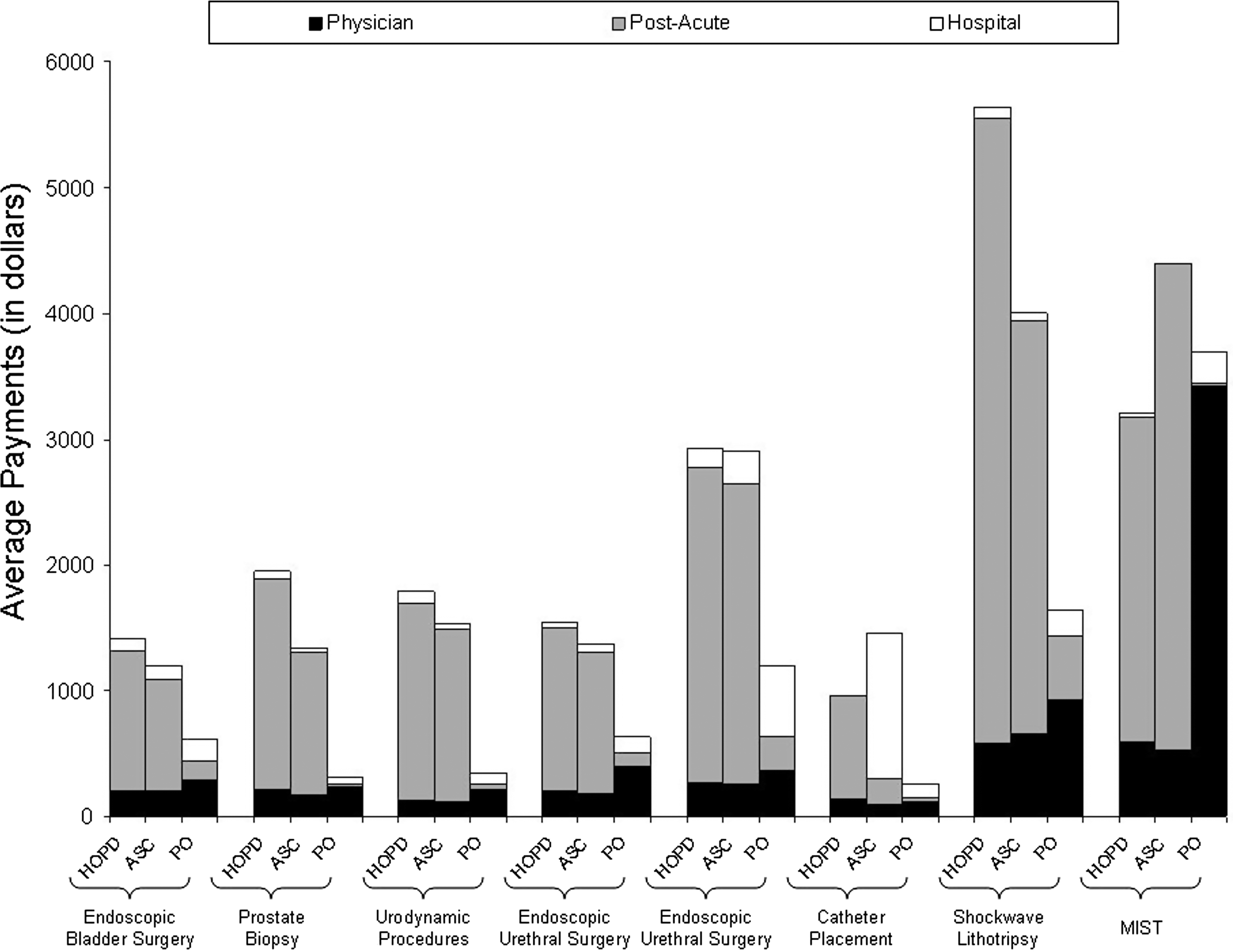
Department of Urology, Loma Linda University, Loma Linda, CA, USA
Introduction: Percutaneous radiofrequency ablation (RFA) and percutaneous cryoablation (cryo) are alternatives to surgical therapies in the treatment of small renal masses. These treatments require image guidance, most commonly computed tomography, which may subject patients to high radiation exposures. There have been no previous studies examining the radiation doses received by patients treated with RFA and cryo.
Purpose: To analyze and compare the radiation exposures associated with RFA and cryo.
Methods: A retrospective review was performed of patients undergoing RFA or cryo between 2004 and 2010. Fifty-six patients with solitary renal tumors<4.0 cm who were treated with either one of the ablative techniques were identified. The length of the procedures and radiation dose were measured. Data was analyzed using independent samples t-test and Pearson Chi-Square.
Results: The mean procedure time for RFA and cryo was 61.4 and 89.4 minutes, respectively (p=0.001). The mean number of CT scans between RFA and cryo was 10.9 and 16.4, respectively (p=0.002). The mean DLP (mGy-cm) for RFA was significantly smaller than the DLP for cryo using the two-sample t-test for unequal variances (p=0.03). The effective doses of the ablative therapies in our study are 23.4 mSv for RFA versus 38.2 mSv for cryo.
Conclusion: Cryoablation resulted in significantly more radiation exposure, longer procedure times, and a greater number of CT scans than RFA. Patients undergoing both percutaneous RFA and cryo are exposed to significant radiation exposures during treatment, and this factor must be considered when selecting ablative strategies in young patients.
Department of Urology, Massachusetts General Hospital, Boston, MA, USA
Introduction: Radiofrequency ablation (RFA) is an effective means of renal tumor ablation. The ablation of masses adjacent to the ureter risks ureteral injury and stricture, however, placement of a ureteral catheter and retrograde pyeloperfusion with dextrose 5% in water (D5W) has been used to reduce ureteral injury.
Methods: From 2005-2010, 46 patients (52 ablations) underwent pyeloperfusion to protect the ureter. Patients were selected for pyeloperfusion during RFA if the tumor was located within 1.5cm of the ureter. Pyeloperfusion was performed by insertion of a 5Fr ureteral catheter and instillation of D5W. Tumors were classified as central, exophytic, or mixed according to the Gervais classification system.
Results: 52 ablations with pyeloperfusion were performed in 46 patients with a complete response rate of 87%. Median tumor diameter was 3.3 cm. 14 /46 (30%) patients had major complications, but only 2 patients (4%) developed ureteral stricture managed with ureteral stenting. 5 patients (10%) had significant hematuria, 2 (4%) had urinomas requiring IR drainage, and 1 had a pseudoaneurysm requiring angioembolization. Notably, 2 patients (4%) had delayed abscesses: 1 patient underwent IR drainage of the abscess, and 1 underwent nephrectomy for what was thought to be recurrent tumor, but was found on pathology to be a delayed abscess with no evidence of malignancy.
Conclusions: RFA for renal masses is generally well-tolerated. Pyeloperfusion for ablations adjacent to the ureter led to only 2 ureteral strictures but also 2 delayed abscesses. Our complication rate is slightly higher than that of other contemporary RFA series.
UT Southwestern Medical Centre, Texas, USA, 2Yung Khan Tan
Purpose:The traditional management of the enhancing small renal mass (SRM) is surgical extirpation. Tumor ablation is now an alternative minimally invasive approach with published series appropriately emphasizing outcomes for the renal cell carcinoma subset of treated tumors. The long term outcomes of incidentally ablated benign tumors and their appropriate follow-up is unknown. As such, we reviewed our 10 year experience with radiofrequency ablation (RFA) in the treatment of the incidental benign SRM.Materials and Methods A review of our database of small renal masses treated with temperature-based radiofrequency ablation was carried out between 2001 and 2011 and cases with a benign histology were included in the study. A total of 315 enhancing small renal masses were treated of which 47 were biopsy-confirmed benign lesions. ResultsOf the 47 benign SRMs, 32 were treated percutaneously and 15 laparoscopically. Biopsy histology was angiomyolipoma(10) and oncocytoma(37). Median tumor size was 2.1 cm (range 1 - 3.6) and the mean followup was 45.2 +/- 30.5 months. There were no recurrences and all lesions required only one treatment session. There was a clinically insignificant increase in creatinine post procedure (0.08 mg/dl). There was one procedure-specific complication: ureteropelvic junction obstruction.ConclusionThe small benign renal lesion can be efficaciously treated with a single RFA treatment session. Long-term follow-up imaging is not required if successful ablation is determined at the initial post-treatment cross-sectional imaging study. Whether RFA for symptomatic or clinically significant benign SRMs can be offered as alternative to surgery remains to be determined.
MP22: Transurethral Surgery Prostate and Baladder
Department of Urology, University of Michigan, Ann Arbor, USA
Introduction: Delivery of outpatient surgical services within a hospital infrastructure designed and maintained for inpatient care has possible implications for payers.Purpose: To compare episode payments for procedures that can be performed in multiple ambulatory settings.Materials and Methods: Using national Medicare data (1998-2006), we identified elderly beneficiaries who underwent one of 22 common urologic procedures. We then measured total and component (hospital, physician, and post-acute care) payments from the date of surgery to 30 days after the index procedure. Finally, we compared adjusted payments across ambulatory care settings [hospital (HOPD) versus surgery center (ASC) versus physician office (PO)] using multivariable regression.Results: Variation exists in average total payments around outpatient surgical episodes, from U.S. dollars (USD) 253 for urethral dilation in the PO to USD 5,642 for HOPD-based shockwave lithotripsy. Exclusive of endoscopic ureteral surgery and microwave therapy for prostate enlargement, ASCs were associated with lower adjusted total payments than HOPDs, but the absolute magnitude of this difference was substantially smaller than that between HOPDs and POs (Figure). Post-acute care was the biggest driver of average total payments. Conclusions: These data support policies that encourage the provision of outpatient surgical care in less resource-intensive settings.
Department of Urology, University of Michigan, Ann Arbor, USA
Introduction: Cost-efficiency gains from moving procedures to ambulatory surgery centers (ASCs) and the physician office (PO) may be mitigated if the surgical quality at these facilities is not comparable to that of the hospital (HOPD).Purpose: To assess short-term morbidity and mortality across ambulatory settings.Materials and Methods: Using Medicare claims (1998-2006), we identified elderly beneficiaries who underwent common outpatient urologic procedures, including transurethral surgery. After determining the facility where each procedure was performed, we measured 30-day mortality, admissions, and complications. We fit logistic models to evaluate the association between an adverse event and the type of ambulatory setting.Results: There was an increase in the frequency PO-based procedures, reflecting a shift in care away from HOPDs. Compared to patients treated in ASCs and POs, those at HOPDs tended to be older and less healthy. Patients treated in POs (versus HOPDs) experienced fewer postoperative complications; however, PO-based surgery conferred three-fold higher odds of being admitted on the day of the procedure (OR, 3.34; 95% CI, 2.30-4.85). With case-mix adjustment, the probability of any adverse event was low across all ambulatory settings (Figure). Conclusions: These data indicate that small, but measurable variation in surgical quality exists across ambulatory settings.
Second Urology Department, Sismanogleion Hospital,University of Athens, Greece.
INTRODUCTIONThe diagnostic value of photodynamic diagnosis (PDD) with the use of 5-ALA has been well documented. Hexaminolevulinate (HAL) is a more lipophilic ester of 5-ALA that has been shown to provide better selectivity and brighter fluorescence with much smaller concentration and installation time.PURPOSE To evaluate the diagnostic efficacy of HAL compared to white light cystoscopy in our clinical practice.MATERIALS AND METHODSSample included of 49 patients with clinical suspicion of non-muscle-invasive bladder cancer (NMIBC) that underwent endoscopic control with white light and HAL-induced photodynamic cystoscopy. Detection rate of the two methods of cystoscopy were compared. In addition, the impact of HAL-PDD in modifying treatment was evaluated.RESULTSDetection rate of PDD was 99.1 % while for normal cystoscopy was 74.5%. PDD and WL had a false-positive rate of 18.1% and 15% respectively. In 12 patients (25.5%) HAL fluorescence revealed lesions that proved to be malignant and would have been missed with WL.Most importantly, in 5 patients (11%) the additional malignant lesions that were found by HAL PDD resulted to a different therapy scheme. Namely, in two patients the diagnosis of CIS leaded to BCG intravesical installations instead of epirubicin. Also, in 3 patients that were thought to have only solitary tumours, additional lesions were revealed and consequently epirubicin installations were indicated due to the tumour multiplicity. CONCLUSIONSHexaminolevulinate fluorescence cystoscopy provided significant aid in the diagnosis of NMIBC in our clinical practice and had a decisive clinical impact in 11% of patients
Safety and Efficacy Evaluation of Botulinum Toxin Type A in 100 Patients with Detrusor Overactivity
Introduction: BTX-A is a neurotoxin derived from Clostridium botulinum. BTX-A has been used mainly in situations associated with muscle hyperactivity. In urology, BTX-A has been essentially directed to the treatment of refractory detrusor overactivity (DO).Material and Methods: retrospective study of 100 patients with urodynamic diagnosis of DO refractory to anticholinergic treatment. The primary outcomes were 24-hr voiding frecuency, average voided volume, incontinence and urgency. Secondary variables: OAB-q scores, adverse events, and urodynamic parameters. The dose of BTX-A was 100units in idiopathic, 200units in diabetic,and 300units in neurogenic.The procedure was performed with rigid cystoscope under local anesthesia in women and spinal anesthesia in men. Twenty intra-detrusor punctures were carried out in each patient avoiding the trigone. All patients were assessed at 2 weeks, 2, 4, 6 and 9 months.Results: 51 had idiopathic and 39 neurogenic DO, 68 women and 32 men. Mean age 63 years old. There was a significant decrease in daytime and nighttime urinary frequency from the second week post-injection, and a decreased number of leaks and pads per day.As for the subjective point of view, 50% reported complete improvement and the remaining 50% partial improvement.An increase in maximum cystometric capacity was seen. No involuntary contractions were observed in 30% of patients. Conclusions: BTX-A injection provides significant clinical benefit, especially those who are refractory to anticholinergic. It is a minimally invasive procedure and well tolerated with few adverse effects. Thus, BTX-A is presented as an option to consider and a promising risk-benefit ratio.
Flexible Cystoscopy Removal of Ureteric Stent and Pain Scores: A case-controlled study
Introduction: Flexible cystoscopy removal of a ureteric stent (FCRUS) is usually performed in the outpatient setting and may be a potentially painful procedure, but no previous studies have formally assessed this hypothesis. Purpose:We performed a case-control study to assess the degree of pain, and to assess patient experience during FCRUS. Patients and Methods: Prospectively, 21 patients who underwent FCRUS under local anaesthesia were compared with 21 age-matched, controls having diagnostic flexible cystoscopy only. Following the procedure, each patient completed a 10cm Visual Analogue pain score, for overall pain, pain on gel instillation, insertion of flexible cystoscope, and finally, actual removal of the ureteric stent and /or the cystoscope. Further data on patient experience and perception of the procedure was also obtained. Results: No significant difference was observed in the average pain score, of the procedure overall, gel instillation, and on scope insertion between case and control arms. However, actual removal of stent was significantly more painful (n=3.2, range:1-7) than removal of the cystoscope in control group (n=1.4; range:1-4). More patients preferred analgesia before FCRUS (n=11; 52.4%) than in controls (n=2;9.5%). Four patients (19%) requested future FCRUS to be performed under general anaesthetic, compared to nil in the control arm, due to the pain experienced. Conclusion:This is the first study to demonstrate that FCRUS is a potentially painful procedure. Pain scores on actual removal of stent are significantly greater than in controls, and patients are more likely to prefer analgesia prior to this procedure, as compared to controls.
University of Michigan, Department of Urology, Ann Arbor, MI, USA
Introduction: Histotripsy is a non-invasive focused ultrasound technology that induces acoustic cavitation to mechanically homogenize targeted tissues. The prostatic urethra is more resistant to histotripsy homogenization than glandular prostate. Purpose: We established dose thresholds to reliably achieve urethral fragmentation to facilitate drainage of treated adenoma. Methods: Prostatic histotripsy was performed on 17 canines using a focused 750 kHz piezoelectric ultrasound transducer targeting a transverse line across the urethra with doses ranging from 3,000-100,000 pulses/mm. On postoperative day (POD) 0, 1, 3, 7, and 14 the prostatic urethra was assessed endoscopically for damage. Findings were confirmed with histology. Results: A total of 33 treatments were delivered to 17 prostates (1-3 treatments/prostate dependent on size) of mean volume 20.6±6.0 cc. On endoscopic assessment, urethral homogenization was apparent in 0/6 (0%), 2/4 (50%), 11/13 (85%), 5/6 (83%), and 6/6 (100%) by POD14 when doses of</=3,000, 12,500, 25,000, 50,000, and 100,000 pulses/mm were applied. Higher doses produced macroscopic urethral disintegration sooner (see table). Conclusion: Delivering a dose>/=25,000 pulses/mm in a single stripe of urethra produces reliable urethral homogenization. Further studies are needed to optimize whole gland histotripsy treatment. Funding: NIH K08 DK081656
National Center for Geriatrics and Gerontology
Purpose: We examined the relationship between frequency of the hemorrhage after TURP and manufacturer of the electrosurgical units.Object: A Japanese nationwide survey of perioperative management of transurethral surgery for BPH was carried out between 2007 and 2009, assisted by Japanese Society of Endourology. An additional investigation about the surgical apparatus was done in 2010 and we got replies from 81 institutes. The conventional TURP was performed in 3355 men in 72 hospitals.Result: Electrosurgical units made by the company A, B, C and D was used at 12 (598 patients), 28 (658), 13 (1285) and 9 (339) institutes (group A to D, respectively). Four hundred seventy-five patients in 10 institutes were excluded because of use of the other electrosurgical units. Significant differences were seen about age, preoperative urinary tract infection, preoperative urethral catheter, prostate volume, experiences of operator, surgical duration, resection weight, and the incidences of TUR syndrome, heterologous blood transfusion and autologous blood transfusion. The catheter blockage caused by the postoperative hemorrhage was significantly less frequent in group A (0.7%) than in group B (4.7%), in group C (3.3%) and in group D (4.2%). Multivariate analysis revealed that the risk factors of the catheter blockage were prostate volume, continuous irrigation during the surgery and manufacture of the electrosurgical units.Conclusion: Although there were differences in the patient background, surgical duration, and resected weight among the groups, it is thought that the hemostatic capability of the electrosurgical units made by the company A might be excellent.

Georgetown University Hospital
Purpose: Open suprapubic simple prostatectomy is the treatment of choice for symptomatic, large volume BPH. While series of robotic-assisted simple prostatectomies have been reported, they are limited to medium-size prostates that may be amenable to transurethral treatments. We report our multi-institutional experience and outcomes with robotic-assisted simple prostatectomy for glands (>100gm).Materials/Methods: From August 2009 to May 2011, 13 robotic simple suprapubic prostatectomies were performed in patients with symptomatic large volume BPH (mean volume on transrectal ultrasonography 163cc). An essential aspect of our technique included use of use of a laparoscopic/robotic tinaculum grasper to aid in retraction of adenoma during dissection.Results: Mean operative time was 179 minutes (range 900 to 270), blood loss was 219 ml (range 50 to 500), hospital stay was 2.7 days (range 1 to 8), and foley catheter duration was 8.8 days (range 5 to 14). Mean specimen weight on pathological examination was 127 gm (range 100 to 165). Intraoperative complications included an introaperative leak in one patient and failure to progress with abortion of case in another. No patients required blood transfusions. All patients were followed for at least 4 months and significant improvement from baseline was noted in the international prostate symptom score (preoperative vs postoperative 18.1 vs 5.3, p<0.001) and the maximum urine flow rate (preoperative vs postoperative 4.3 vs 19.0 cc per minute, p<0.001).Conclusions: Minimally-invasive robotic simple prostatectomy is techincally feasible in patients with large volume (>100gm) BPH and is associated with significant improvement in obstructive urinary symptoms.
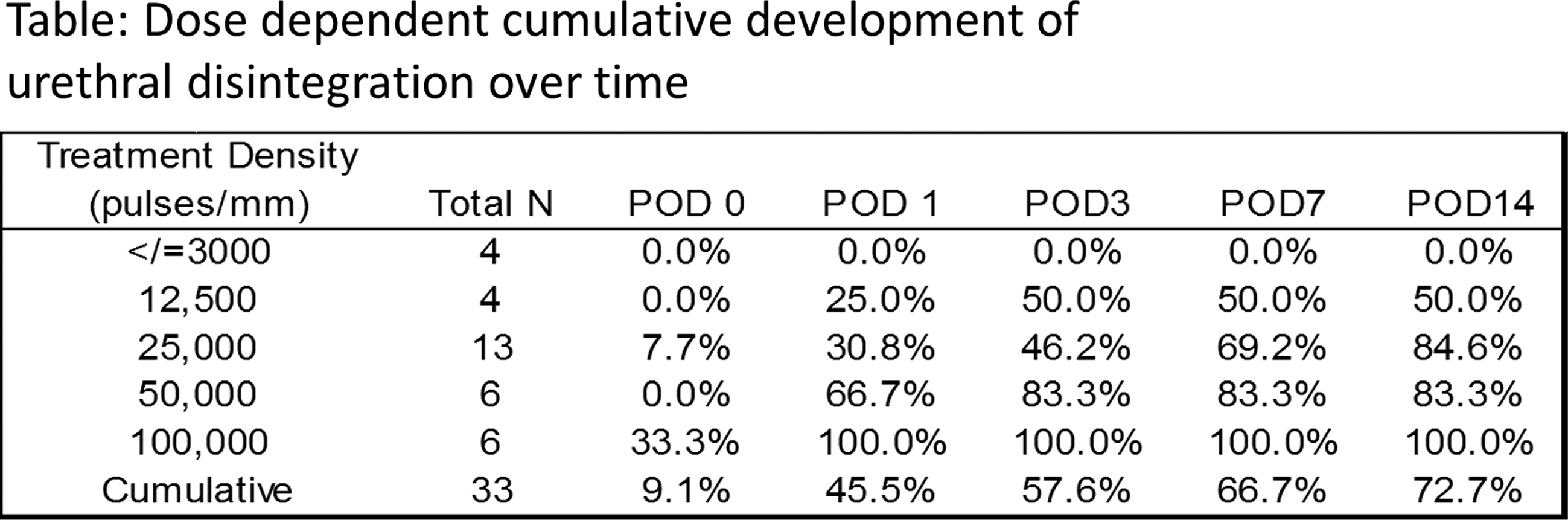
Bipolar Plasma Vaporization versus Monopolar and Bipolar TURP: Results of a Prospective, Randomized, Long Term Comparison
Introduction: A prospective, long term, randomized comparison between the bipolar plasma vaporization (BPV), monopolar and bipolar TURP was performed.Purpose: The study aimed to evaluate the surgical efficacy, complication rate and follow-up results of the 3 methods.Materials and Methods: A total of 510 BPH patients with Qmax under 10 ml/s, IPSS over 19 and prostate volume between 30-80 ml were enrolled. All cases were evaluated preoperatively and during 18 months after surgery by IPSS and Qmax.Results: The mean operation time, catheterization period and hospital stay were significantly shorter for BPV patients (39.7 versus 52.1 and 55.6 minutes; 23.5 versus 46.3 and 72.8 hours; 45.6 versus 74.4 and 100.8 hours). The mean hemoglobin drop, intraoperative bleeding and capsular perforation rates were significantly reduced in the BPV series (0.5 versus 1.2 and 1.6 g/dl; 1.8% versus 8.2% and 13.5%; 1.2% versus 7.1% and 9.4%). The rate of irritative symptoms was similar in the 3 study arms. The BPV group emphasized significantly superior follow-up parameters concerning IPSS and Qmax (table 1).Conclusions: BPV represents a valuable endoscopic alternative for BPH patients, with superior efficacy, satisfactory complication rate and improved long term follow-up parameters by comparison to monopolar and bipolar TURP.

Management of Postoperative Delirium Following Transurethral Resection of the Prostate with Geriatric Patients
Introduction: Postoperative delirium is adverse events that occur frequently in geriatric patients. The pathogenesis of it is incompletely understood. It often appears to emerge cognitive decline or delirium after transurethral resection of the prostate (TURP). This study was to describe the risk factors and how to treat it.Aims: To investigate the risk factors and the management of postoperative delirium following TURP in the geriatric patient with benign prostatic hyperplasia (BPH). Methods: The clinical data of 1078 BPH patients receiving TURP in our clinic were reviewed. There was no cognitive impairment or psychiatric diseases before surgery in all patients. Cognitive functions were examined by psychologist after TURP. TUR syndrome and other disturbance of consciousness due to systemic diseases or serum electrolyte imbalance were excluded. Results: 13 patients appeared to be postoperative delirium during 10 to 48h after TURP. All 13 patients are more than 60 years old. Of them, 3 patients are in 60 to 70 years old, 7 cases in 70 to 80, and 3 patients are more than 80 years old. The incidence of it is respectively 1.2%, 4.8%, and 5.5%. One patient presented sleep-disorder slightly and was cured by injecting diazepam. Delirium remitted or disappeared after 6 to 24 hours by intramuscular injection of haloperidol in the other 12 patients. Conclusions: Advanced age is an important risk factor for postoperative delirium due to TURP. Pharmacologic therapy with haloperidol is usually conducted to control symptoms and may be very useful to treat it.
Bipolar Plasma Vaporization of Secondary Bladder Neck Sclerosis: A Prospective, Randomized, Long Term Comparison with the Standard TUR
Introduction: A prospective, randomized comparison between bipolar plasma vaporization (BPV) and monopolar transurethral resection (TUR) in cases of secondary bladder neck sclerosis (BNS) was performed.Purpose: The trial aimed to assess the therapeutic efficiency, overall safety and postoperative results of this new technique. Materials and Methods: A total of 60 patients with BNS secondary to TURP (41 cases), to adenomectomy (14 cases) and to radical prostatectomy (5 cases) were enrolled in 2 equally numbered study arms. The inclusion criteria consisted of Qmax under 10 ml/s and IPSS over19. All patients were evaluated preoperatively and at 1, 3, 6 and 12 months after surgery by IPSS and Qmax. Results: The mean operative time, catheterization period and hospital stay were significantly reduced in the BPV series (16.5 versus 27 minutes, 18 versus 46.5 hours and 34.5 versus 73 hours). Capsular perforation only occurred in 2 cases of the TUR group, while the rate of irritative symptoms was similar in the 2 series (13.3% versus 16.7%). The 1, 3, 6 and 12 months follow-up emphasized superior improvements in the BPV group by comparison to the TUR series in terms of IPSS (3.4 versus 6.3, 3.6 versus 6.5, 3.7 versus 6.8 and 3.9 versus 7.2, respectively) and Qmax (23.8 versus 21.1 ml/s, 23.7 versus 20.6 ml/s, 23.4 versus 20.7 ml/s and 23.2 versus 20.1 ml/s, respectively). Conclusions: BPV represents a valuable endoscopic alternative for secondary BNS, with superior efficacy, satisfactory safety profile and significantly improved follow-up parameters by comparison to standard TUR.
Initial Experience with Turis Plasma Vaporization of Prostate
Introduction: Over the years, TURP (Transurethral resection of Prostate), as a treatment modality for obstructing BPH (Benign Prostatic hypertrophy), has gained popularity throughout the world. It is now considered the gold standard for the surgical management of BPH. The TURis plasma vaporization electrode does not cut off tissue with a loop, but energetically vaporizes the tissue with a small button electrode. We report our data from our randomized clinical trial comparing monopolar transurethral resection of prostate with plasma vaporization of prostate in saline.Materials and Methods: Patients presenting with urodynamically proved infra-vesical obstruction secondary to enlarged prostate and needing transurethral resection for relief of symptoms were randomized to undergo either standard monopolar TURP or TURis plasma vaporization. Resection time, prostate volume, catheter time, hospital stay, change in haemoglobin and serum sodium were properly recorded and analyzed. Results: During the period Sept 2010 to March 2011, 64 patients underwent standard monopolar TURP and 69 patients underwent TURis plasma vaporization. The age of the patients , mean prostate volume and preoperative Hb was similar in both the groups . There was no significant change in post-operative Hb and sodium levels following TURis plasma vaporization . There was significant change in Hb as well as serum sodium levels following standard TURP in patients whose prostate volume was>or equal to 40 cc.Conclusions: TURis plasma vaporization of prostate is safe and not associated with significant changes in post-operative Hb and sodium values.
A Prospective Randomised Study between Transurethral Vaporisation using Plasmakinetic Energy and Transurethral Resection of Prostate: 8 Years Follow-Up
Introduction: A prospective randomised study was conducted to evaluate the safety and efficacy of Plasmakinetic energy (Gyrus electrosurgical system) that produces vaporisation of tissue immersed in isotonic saline against standard transurethral resection of the prostate in the treatment of benign prostatic hyperplasiaMaterials and methods: Randomisation was commenced in October 1998 with ratio of 2:1 (Plasmakinetic: TURP). Seventy six (22 with retention of urine) has been enrolled in this study with age ranging between 50 to 82 (mean 70.1) years and prostatic weight 20 to 105 (mean 48.3) grams. Intra operative parameters were operating time, blood loss (Haemocue B haemoglobin system), fluid absorption during TURP by using ethanol glycine by alcoholmeter (saline was used during vaporisation), serum sodium and haemoglobin. Results: Operative duration was similar in both the groups. There was no significant difference in pre and post-operative sodium and creatinine. Mean blood loss in plasmakinetic group was 251ml (range 49-1000) and TURP group 497ml (range50-1750). Fluid absorption in TURP group was less than 500ml. One patient in plasmakinetic group had prolonged catheterisation for 5 days, 3 patients had mild stress incontinence lasting three months and 2 patients required TURP (4%) in 8 years. In the TURP group 1 patient required TURP (4%) in 8 years. There was significant improvement in I-PSS, Quality of Life score and uroflow which was comparable in both groups.Conclusion: Plasmakinetic vaporisation produced reduced intra operative bleeding and has no risk of TUR syndrome due to saline irrigant.
Randomized Study on Endoscopic Gyrus Vs Open Surgery for over 100 GR Prostate
INTRODUCTION The aim of this study is to compare the clinical efficaciousness of Gyrus Plasma Kinetic technique versus OPSU in the treatment of voluminous BPH.MATERIALS and METHODSFrom January to June 2003, 140 patients with voluminous BPH, were randomized in 2 groups underwent bipolar TURP or OPSU. Prostate volume was measured by ultrasonography. All patients underwent a pre and postsurgical evaluation after one month, each 3 months for one year and annually with uroflowmetry, assessment of PVR and PSA; symptoms were determined by IPPS, IEFF-5, QOL. Hb values, catheterization periods, the length of hospitalization and the eventual hemotransfusions and complications were also valued. RESULTS: Average age of the patients was 67,5 yrs. Medium follow-up 81 months. In both groups, statistically significant increment in Qmax and Qave baseline and a reduction of the RPM and PSA. At one month, datas concerning patients, treated with traditional OPSU were better, but equal from the third month onward. In Gyrus group shorter periods of catheterization and hospitalization, minor degrees on Hb values, no post-surgical hemotransfusions. A case of death in open surgery group because of thrombosis. Second look in 8 patients of the OPSU group versus 2 of the Gyrus group. CONCLUSIONSComparing to open surgery, endoscopic bipolar resection of prostate offers same clinical results but it guarantees a minor post-surgical hospitalization and catheterization periods with less complications rate
NBI Cystoscopy and Bipolar Plasma Vaporization Versus Standard Cystoscopy and Monopolar TURBT in Cases of Large Non-Muscle Invasive Bladder Tumors
Introduction: A prospective, randomized comparison between narrow band imaging (NBI) cystoscopy associated with bipolar plasma vaporization (BPV) and standard white light cystoscopy (WLC) and monopolar TURBT was performed.Purpose: The study aimed to evaluate the diagnostic accuracy, surgical efficacy, Re-TUR and long term recurrence rates of the 2 approaches in cases of large bladder tumors.Materials and Methods: A total of 220 patients with bladder tumors over 3 cm were included in the trial based on ultrasonography, CT and flexible WLC. WLC, NBI cystoscopy and BPV were performed in one arm and WLC and TURBT in the second one. All NMIBT patients underwent standard Re-TUR at 4 weeks and follow-up urinary cytology and WLC at 3, 6, 9 and 12 months.Results: In the NBI-BPV series, the CIS, pTa and overall tumors detection rates were significantly improved for NBI cystoscopy (94.6% versus 67.6%, 93% versus 82.4% and 94.9% versus 84.3%). The catheterization period and hospital stay were shorter in the BPV arm. The obturator nerve stimulation, bladder wall perforation, mean hemoglobin drop and postoperative bleeding rates were significantly reduced for BPV. The overall and primary site Re-TUR residual tumors rates were lower for NBI-BPV (6.3% versus 17.5% and 4.2% versus 13.4%). The one year recurrence rate was significantly reduced in the NBI-BPV group (7.9% versus 17.8%). Conclusions: NBI cystoscopy significantly improved the diagnostic accuracy while BPV emphasized superior efficacy and reduced complication rate. This approach provided a lower Re-TUR residual tumors rate and a reduced one year recurrence rate.
Transurethral Partial Cystectomy for the Muscle-Invasive Bladder Cancer with 2-Micron Laser (a Report of 8 Cases)
Objectives To investigate the safety and efficacy of transurethral partial cystectomy with 2-micron laser for muscle invasive bladder cancer. Methods 8 cases of muscle invasive bladder cancer, which were confirmed by cystoscope and CT studies, were treated by RevoLix 2 microns laser surgery system between January 2011 and June 2011. 4 cases were male and 4 were female, mean age was 69 years old. All the bladder tumor were solitary, with diameter ranged 1.8-3cm. The final diagnosis was confirmed to be urothelial carcinoma with stage T3 by the postoperative pathological studies. All cases were treated under continuous epidural anesthesia. 2-micron laser were used for transurethral tumor resection. It was required that the depth of cutting surround tumor should include the whole bladder wall. The bladder tumor tissues were harvested and sent to pathological studies.Results The mean operation time was 25 minutes, ranged from 12 minutes to 40 minutes. The duration of hospitalization was 2.5 days. There were no complications in this study.Conclusions 2-micron laser transurethral partial cystectomy was feasible for single muscle invasive bladder cancer. A long-term follow-up should be launched to evaluate the long-term effect of this technique.
2-Micron Laser Transurethral Resection of Repeated Recurrence of Multiple Non-Muscle Invasive Bladder Tumors (Report of 23 Cases)
[Introduction] the patients with repeated recurrence of non-muscle invasive bladder cancer should underwent radical cystectomy. But for senior patients and the patients who can not tolerate radical cystectomy surgery, palliative resection of bladder tumor is one of the appropriate treatments. [Purpose] To evaluate the safety and efficacy of RevoLix 2 micron laser transurethral resection of repeated recurrence of multiple non-muscle invasive bladder tumor(RRMNMIBT).[Materials and methods] We retrospectively analyzed 23 patients in our hospital from May 2010 April 2011 conducted by transurethral resection RevoLix 2 micron laser treatment of RRMNMIBT patients. Average relapse frequency was 4 (2 ∼ 12), Average age was 74 years (68 years to 95 years), patients with a history of cardiac stent were 16, and the remaining patients had varying degrees of hypertension, diabetes, coronary heart disease, stroke and history of cerebral hemorrhage.[Results] The tumor number was 3 ∼ 95 and mean operative time was 22min (8min ∼ 48min). All patients had no intraoperative obturator nerve reflex, no bladder perforation and no blood transfusion. Indwelling Foley catheter was placed about 1 ∼ 3d and there were no bladder irrigation. All patients were able to get postoperative pathology specimens and pathology results in 18 patients were non- muscle invasive bladder cancer (high level), the other 5 patients were muscle invasive bladder cancer (high level).[Conclusions] For senior patients and the patients who can not tolerate radical cystectomy surgery with RRMNMIBT, transurethral RevoLix 2 micron laser surgery is effective, safe and reliable.
Preliminary Clinical Study of 2-Micron Laser Transurethral Resection of Ureteral Cancer (Report of 8 Cases)
[Background] The patients with ureter cancer should undergo ureter cancer radical surgery, but for the patients with ureteral cancer who can not tolerate radical surgery, palliative transurethral ureteral resection of the tumor is an optional treatment.[Objective] To evaluate the efficacy and safety of RevoLix 2 micron laser transurethral resection of ureteral tumor.[Methods] We retrospectively analyzed 8 patients conducted by transurethral resection RevoLix 2 micron laser treatment of ureteral tumors in our hospital from March 2010 to December 2010. The average age was 72 year, among them, the patients with a history of cardiac stent was 5, and all patients had varying degrees of hypertension, diabetes, coronary heart disease, history of cerebral infarction or cerebral hemorrhage.[Results] The ureteral tumor length was about 1cm ∼ 3cm. mean operative time was 16min (8min ∼ 35min). All patients had no ureteral perforation and ureteral stripping and no blood transfusion cases occured. Conventional indwelling double-J tube was placed and it would be pulled out four weeks post-operation in the outpatient. All patients could get postoperative pathology and the pathology results of four patients were non-muscle invasive ureteral cancer (low level), three were non-muscle invasive ureteral cancer (high level), one was muscle invasive ureteral cancer (high level). All patients were followed about 3 months to 6 months and no tumor occured.[Conclusion] For the patients with ureteral cancer who can not tolerate radical surgery, palliative transurethral resection of RevoLix 2 micron laser is effective, safe and reliable during short-term follow-up.
MP23: PNL 2
Instituto de Endourologia, Centro Medico Puerta de Hierro and Nuevo Hospital Civil, Universidad de Guadalajara, Guadalajara, Mexico
INTRODUCTION Despite antibiotic prophylaxis, fever secondary to a urinary tract infection remains one of the most common sequelae of percutaneous nephrolithotomy (PCNL).PURPOSETo review the incidence of UTIs and to assess the risk factors associated with the occurrence of post-operative fever among PCNL patients.MATERIALS AND METHODSBetween 2007 and 2009, 5803 consecutive PCNL patients were treated over a 1-year period at one of 96 centers participating in the PCNL Global Study. Pre-operative bladder urine culture and post-operative fever (>38.5 degrees celsius) were assessed. RESULTS A total of 865 (16.2%) patients assessed had a positive urine culture; Escherichia coli was the most common micro-organism found, being present in the urine of 350 patients (6.5% of sample). Of the patients with negative pre-operative urine cultures, 8.8% developed a fever post PCNL, in contrast to 18.2% of patients with positive urine cultures. Fever developed more often among patients whose urine cultures consisted of Gram-negative micro-organisms (19.4-23.8%) versus those with Gram-positive micro-organisms (9.7-14.5%). Multivariate analysis indicated that a positive urine culture (odds ratio [OR]=2.12, C.I [1.69-2.65], staghorn calculus (OR=1.59, C.I[1.28-1.96]), preoperative nephrostomy (OR=1.61, C.I [1.19-2.17]), lower patient age (OR for each year of 0.99, C.I [0.99-1.00]), and diabetes (OR=1.38, C.I [1.05-1.81]) all increased the risk of post-operative fever. CONCLUSIONS Approximately 10% of PCNL-treated patients develop fever in the post-operative period despite receiving antibiotic prophylaxis. However, the risk of post-operative fever is increased in the presence of a positive urine bacterial culture, diabetes, staghorn calculi, and a pre-operative nephrostomy.
Renji Hospital, Shanghai Jiaotong University, School of Medicine, Shanghai, China
IntroductionThe technique of PCNL is the preferred first-line therapy for large renal stones.PurposeThe study compared stone characteristics and outcomes in patients with large renal calculi treated with PCNL in the CROES Global Study.Materials and MethodsTwo statistical analyses were undertaken; one comparing large renal stones on size and the other on renal location (pelvic or upper-, mid- or lower-calyceal). Surgical outcomes were compared between groups. Fitness for surgery was assessed using ASA scoring system. Severity of post-surgical complications was graded using the modified Clavien classification system. ResultsOf 1448 stones, 1202 (83%) were 20-30 mm, 202 (14%)>30-40 mm and 44 (3%)>40-60 mm in size. The majority of large stones were located in the renal pelvis (73%). Statistically significantly lower stone free rates, higher rates of post-operative fever and greater levels of blood transfusion were seen with increased calculus size. As ASA score increased, so the proportion of large stones located in the calyces increased. At ASA score III, the proportion of large stones located in the calyces (13.5%) was over twice that of stones located in the renal pelvis (5.7%). Generally, more patients with large calyceal than pelvic stones had post-operative complications across the range of Clavien scores from I to IIIB. ConclusionsCalyceal location was associated with decreased fitness for surgery and increased risk of post-operative complications than renal location. Alternative approaches to the management of large calculi, especially those within the calyces, may be needed.
Percutaneous Nephrolithotomy in Patients with Solitary Kidney (Report of 12 Cases)
[Purpose] To evaluate percutaneous nephrolithotomy (PCNL) in the patients with solitary kidneys. We present our experience with percutaneous nephrolithotomy (PCNL) in treating 12 patients in a solitary kidney to determine short-term renal functional results.[Material and methods] We retrospectively reviewed the records of 12 patients with renal staghorn calculi in a solitary kidney treated with PCNL. 10 patients were functional solitary kidney and 2 patients were anatomy solitary kidney. Demographic data, number of accesses, location of accesses, hemoglobin values, and complications were studied. Serum creatinine, systolic and diastolic blood pressure, new onset hypertension, and kidney morphology were determined preoperatively and postoperatively at 1 month and 12 months. [Results] Male to female ratio was 5:1 and mean age was 46.5 years (range 29-54). Among them, 10 patients required a single standard tract, while 2 needed a single standard tract and a micro-tract. The complete stone clearance rate was 91.7% (11/12) after the first stage. And one patient required extracorporeal shock wave lithotripsy (SWL). A double-J catheter was inserted in all patients and it was removed post-operation 4 weeks. No severe complications occurred in all patients and no blood transfusion events took place. We demonstrated a significant improvement in creatinine levels from preoperatively to 12 months follow-up. The number of patients with hypertension before PCNL was 3 and by the end of follow-up there was no new onset hypertension.[Conclusion] PCNL is not only effective but is also safe in the solitary kidney with staghorn calculi.
Percutaneous Nephrolithotomy in Patients with Spinal Deformities (Report of 8 Cases)
[Purpose] To evaluate the efficacy and feasibility of percutaneous nephrolithotomy (PCNL) in patients with spinal deformities. [Patients and methods] We retrospectively reviewed the records of 8 patients with spinal deformities underwent PCNLs from March 2004 to May 2010. Preoperative investigation of the respiratory function and evaluation of anatomy by intravenous pyelography and CT spiral scan were performed in all patients. All patients were in a prone position during PCNL. US-guided fluoroscopic adjusted percutaneous puncture of the desired calix was performed in all patients. Demographic data, number of accesses, location of accesses, hemoglobin values, and complications were studied.RESULTS: Male to female ratio was 3:1 and mean age was 39.5 years (range 22-48). Among them, 5 patients required a single standard tract, while 3 needed a single standard tract and a micro-tract. A double-J catheter was inserted in all patients and it was removed post-operation 4 weeks. Of them, no patients encountered septic shock. 1 patient needed blood transfusion. The complete stone clearance rate was 75% (6/8). And 2 patients required extracorporeal shock wave lithotripsy (SWL). At the 3-month follow-up, the overall stone-free rate was 87.5% (7/8).CONCLUSION: PCNL in patients with spinal deformities is challenging. Accurate preoperative evaluation of the anatomy and respiratory function and a precise preoperative planning are compulsory. Prone position may offer a wider space for percutaneous access. And so, the complete stone clearance rate is acceptable. Combination therapy with SWL after PCNL improves stone-free rates
Renal Access by Urologist versus Sonographer During Percutaneous Nephrolithotomy
[Purpose] To evaluate the percutaneous access outcomes and complications following percutaneous nephrolithotomy (PCNL) that was obtained by urologist or sonographer at a single academic institution.[Materials and methods] A retrospective chart review of 420 renal calculi patients who underwent ultrasound-guided PCNL from March 2004 to May 2010 in the first hospital of Jilin university was performed. Patients were stratified according to percutaneous access by urologist (group 1) or a group of sonographer (group 2) in 105 and 315 patients, respectively. A predicted access difficulty score was calculated using demographic, stone, and operative variables. Percutaneous access complications and stone-free rates were compared between groups.[Results] Use of multiple access tracts (3.2% vs 4.4%; P=0.67), mean stone diameter (4.3±1.7 cm vs 4.6±2.1 cm; P=0.65), and mean access difficulty parameters were comparable between groups. The percentage of staghorn calculi (25% vs 28%; P=0.69) and number of obese (body mass index>30) patients (32% vs 36%; P=0.85) were also comparable between groups 1 and 2. The complication rate was the same in the two groups (8.2% vs 7.5%; P=0.59). The overall stone-free rate was the same too in the two groups (93.5% vs 91.8%; P=0.32). Sonographer-obtained access could not be used in 12.8% of patients, necessitating additional access tract placement at the time of surgery.[Conclusions] Access obtained by Sonographer often is not adequate for PCNL. Urologist-obtained access is safe and effective for PCNL.
Post-Percutaneous Nephrolithotomy Septic Shock and Severe Hemorrhage: A Study of Risk Factors
Objectives:We identified the risk factors predicating septic shock and severe hemorrhage due to percutaneous nephrolithotomy (PCNL).Patients and Methods: 420 renal calculi patients who underwent ultrasound-guided percutaneous nephroscope/ureteroscope holmium laser lithotripsy procedures from March 2004 to May 2010 in the First Hospital of Jilin University were retrospectively reviewed. We tested the characteristics of pre-hospitalization urine white cell count, stone position, kidney morphology, calculus diameter, puncture times, operation time and operation method.Results: Of 420 patients, 10(2.4%) encountered septic shock and 4(1%) had severe hemorrhage. Significant risk factors for infectious shock were urine white cell count (WBC) in pre-hospitalization and operation time. Significant risk factors for severe bleeding were kidney morphology and puncture times. In coherent with septic shock, the patients with operation time more than 90 minutes were easier to confront sever renal bleeding(P=0.017). In conflicting with septic shock, the risk of encountering severe renal bleeding for patients by nephroscope was higher than those by ureteroscope(P=0.045). Conclusions:The mutual risk factor for septic shock and severe hemorrhage of PCNL was operation time. Positively pre-operation anti-inflammatory therapy could reduce the possibility of septic shock after PCNL. The patients with no-hydronephrosis in pre-operation were easier to confront severe renal bleeding. Reducing the intra-operational puncture time could cut down the probability of post-PCNL severe hemorrhage. Whether encountered septic shock or not was no significant with the crudeness or fineness of passage. However, comparatively gross nephroscope passage was easier to result in severe renal bleeding.
Radiation-Free Percutaneous Nephrolithotomy(PCNL) in Pregnancy
IntroductionUrolithiasis during pregnancy is a clinical dilemma due to potential risks for mother and fetus.Management of these patients needs a multidisciplinary approach including urologist,obstetrician,anesthesiologist,radiologist and perinatalogist. PurposeWe repot our experince of PCNL in pregnancy under ultrasound guide compeletely.Materials and MethodsOur cases were 9,14 and 12 weeks pregnant women who referred by her obstetrician because of fever,urinary symptoms, several episodes of severe right flank pain and gross hematuria.all were in second pregnancy and had history of renal stone.One of them had history of one session PCNL of left kidney 2 years ago.Ultrasonography(US) revealed normal alive fetus,2 right and one left side severe hydronephrosis and multiple stones measuring 7 to 21mm,largest one in ureteropelvic junction causes obstruction.Patients refused any temporary procedure such as jj stent or percutaneous nephrostomy and even abbreviated excretory urography,compeleted and signed consent for PCNL with US guide.So,second US performed by an expert radiologist and underwent PCNL with US guide. ResultsAll were Stone-free in sonography 2 weeks after operation . No any complication in perioperative period.They are symptom-free ,with good condition of their babies,4 and 7 months old and 15 weeks alive fetus, respectively, now. ConclusionsPCNL with guide of US seems safe and effective modality for large symptomatic stone during pregnancy without any radiation to mother or fetus.
The Safety and Efficacy of Minimally Invasive Percutaneous Nephrolithotomy in Elderly Patients with Proximal Ureteral Stones
Objective: The present study was designde to compare the safety and efficacy of minimally invasive percutaneous nephrolithotomy(MPCNL) in elderly patients with proximal ureteral stones. Methods: Clinical date on 108 elderly patients who underwent ureteroscopic lithotomy(URL) were retrospectively compared with those on 35 who underwent MPCNL for proximal ureteral stones, including patient demographic date, perioperative indexs and clinical outcomes. Results: There were no significant difference in age, sex ,stone size and comorbidities in the two groups. In the comparison of intraoperative parameters in the two groups, there is no significant difference in the operative time(48.3±11.4min vs 59.4±14.2min, P>0.05). Comparision of postoperative parameters showed that the postoperative hospital stay were shorter in the URL group than in the MPCNL group(P<0.05). The overall complication rate had no differences between the URL group (11.2%) and MPCNL group(10.3%) (P>0.05). The stone-free rate in the URL group was 67% ,while 97% in the MPCNL group, the differences was significant (P<0.05). Conclusions: For the elderly patients with proximal ureteral stones, MPCNL can be a safely and effective procedure.
Anatomical Variation between the Prone, Supine and Supine Oblique Positions on Computed Tomography: Implications for Percutaneous Nephrolithotomy Access
Purpose: To determine anatomical variations between the prone, supine, and supine oblique positions that are likely to impact percutaneous renal access. Materials and Methods: Twenty patients underwent computed tomography urograms in the supine and prone position. Twenty patients underwent supine oblique and prone scans. Mean nephrostomy tract length, maximum access angle and anterior-posterior renal position were calculated. Results: Mean nephrostomy tract length was shorter in the prone position (82.6 mm right kidney, 85.4 mm left kidney) compared to the supine position (108.3 mm right kidney, p<0.001; 103.7 mm left kidney, p<0.001). Prone tract length was also shorter than supine oblique tract length (86.1 mm vs 96.5 mm; p=0.048). Mean maximum access angle was significantly greater (p=0.018 right kidney; p=0.007 left kidney) in the prone position (right kidney 99.7 degrees, left kidney 104.0 degrees) compared to the supine position (right kidney 87.7 degrees, left kidney 89.4 degrees). The same held true for the prone compared to the supine oblique position (75.8 degrees vs 58.7 degrees; p=0.004). No difference was noted in anterior-posterior renal position between the supine and prone positions (20.3 mm vs 26.7 mm; p=0.094) or supine oblique and prone positions (22.8 mm vs 15.6 mm; p=0.45).Conclusions: The prone position is associated with a significantly shorter nephrostomy tract length and more potential access sites, which may improve ease and safety of percutaneous renal access.
The Relative Renal Anatomy in the Prone-Flexed Position for Percutaneous Nephrolithotomy: A Proof of Concept for our Modified Position
Introduction :The study presents the anatomical basis for our position modification for percutaneous nephrolithotomy and demonstrates why the prone-flexed position facilitates percutaneous renal access and potentially minimizes its morbidity.Methods:Reconstructed abdominal-pelvic triphasic computed tomography was conducted on 16 patients in the prone and prone-flexed positions. The trajectory of nephrostomy access was virtually positioned at a 30 degree angle off the vertical axis lateral to the paraspinal muscles.Results:In the prone-flexed position, the left kidney was displaced lower than the right in 92.3% of cases, such that it would have lowered an upper pole puncture from above the 11 th rib to one above the 12th rib in 5 of 11 patients (45.5%). For lower pole punctures, the right and left kidneys were significantly lower (11.6 mm and 9.8 mm, respectively), p<0.001. The prone-flexed position moved the kidney further from the adjacent organs (the planned trajectory was 13.6 degrees further away from the liver and 11.3 degrees further from the spleen (both p<0.001). In the prone-flexed position, the mean angle of trajectory of a rigid nephroscope from an upper pole puncture into the lower calyx was 101.3 degrees, whereas from a lower pole puncture into an upper pole calyx was 96.1 degrees (p<0.01). Conclusions:The prone-flexed modification shortens the skin-to-kidney distance, lowers the kidneys in relation to the ribs minimizing supracostal punctures, moves the liver and spleen away from potential punctures and flattens the natural lumbar lordosis facilitating the instrumentation from a lower pole puncture.
Supine-Lithotomy versus Prone Position in Minimally Invasive Percutaneous Nephrolithotomy for Upper Urinary Tract Calculi
Objective: To compare operative time, safety, and effectiveness of minimally invasive percutaneous nephrolithotomy(MPCNL) in a new supine-lithotomy versus prone position in a prospective randomized trial.Methods: 109 patients (74 men, 35 women; mean age, 44.6 yr) were prospectively enrolled and randomly divided into group A (53 patients, supine-lithotomy position) and group B (56 patients, prone position). The MPCNL procedures were performed under the guidance of real-time grayscale ultrasound system. The preoperative characteristics, intraoperative and postoperative parameters were analyzed.Results: The two groups were comparable in male-to-female ratio, age, body mass index (BMI), American Society of Anaesthesiologists (ASA) score,stone location and stone size. All patients were successfully operated, and there was no conversion to open surgery. There was no significant difference between the two groups in stone-free rate, mean blood loss, number of access tracts, calyx puncture, mean hospital stay and complications. But the operative time was significantly shortened in supine-lithotomy position (group A, 56±15 min vs. group B, 86±23 min, p<0.001).Conclusions: The efficacy and safety of supine-lithotomy position for MPCNL were similar to the prone position, but the supine-lithotomy position shortens significantly operating room time. The supine-lithotomy position should be a choice to perform MPCNL.

PCNL: Prone or Supine?
Introduction: In the last decade supine position during PCNL has gained large acceptance among European urological community. Nevertheless it has not yet been demonstrated a clear superiority of one technique over the other. The aim of this retrospective study is to compare operative time, safety, and effectiveness of PCNL in supine versus prone position .MM: Since June 1999, a total of 512 PCNLs has been carried at our Stone Center. Among them, 344 has been carried out in prone position while 168 in supine position Results: Results are reported in table 1 Conclusions: Results do not differ significantly between these 2 series in terms of blood loss, transfusions, complications and stone free rate and hospitalization. On the counterpart, PCNL in supine position reduces invasiveness of percutaneous surgery in terms of shorter operative time and convalescence likely due to the higher rate of tubeless procedures together with a lower number of tracts and 2nd look per case. These data failed to demonstrate a clear superiority of supine over prone position during. Nevertheless, we believe that even though it is not mandatory for any endourologist to adopt the supine position, this position is definitely here to stay.
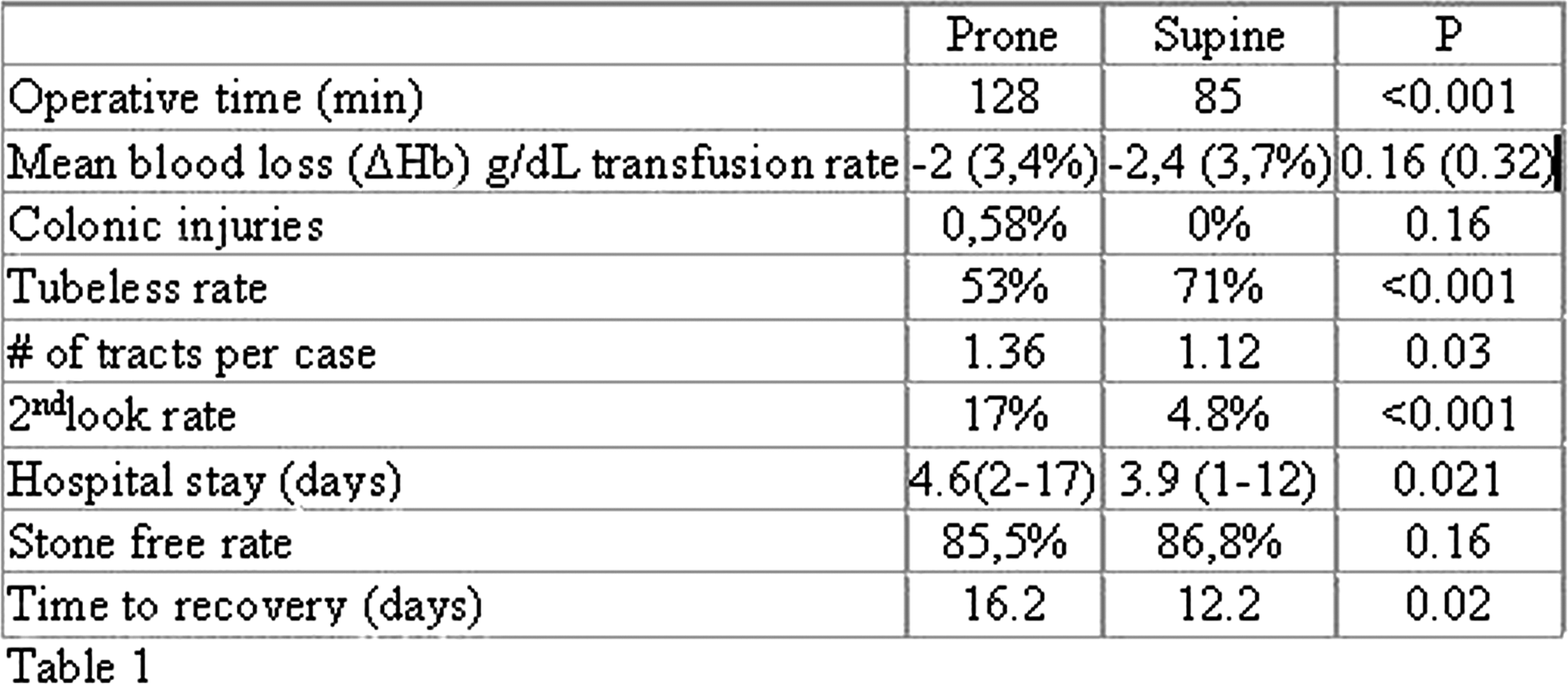
PCNL Trajectory to Predict Success in Supine PCNL: A Novel Concept
Introduction Supine PCNL confers certain advantages over prone. Access parameters change with positioning. Supine position limits maneuverability of instruments, limiting access to upper & mid-pole stones. We aim to determine predictive factors for success of supine PCNL through road-mapping of PCNL trajectory.Material&methodConsecutive patients undergoing PCNL from July-Dec2010 were recruited. Choice of position was made by surgeon. Tracts were performed under USG & fluoroscopy. Distances and angles were measured intra-operatively with rigid and flexible nephroscope, and correlated with pre-operative imaging.Results 19 patients underwent PCNL(13supine, 6prone) Stone load was comparable in both groups. Overall stone clearance after single PCNL was 74%. Regardless of abdominal thickness and approach, all lower pole and renal pelvic stones were reached with mean-excursion of 140 mm in supine & 105 mm in prone position. Mean-entry angle was 59 for supine, and 35 for prone.In supine PCNL, the upper pole was reached in 4 of 11 tracts, with mean-excursion of 172mm & entry angle of 33. Similarly, 2 of 11 supine PCNL reached middle pole. Conversely, all prone PCNL tracts reached upper & middle pole with decreased excursion & angle. ConclusionPCNL in prone position can reach renal pelvis and 3 poles via lower pole puncture. PCNL trajectory may be a tool to predict success in supine PCNL by estimating chance of reaching mid & upper pole. Skin to upper pole distance larger than 185mm and entry angle more than 48 degrees decrease chance of upper pole access.
Conventional-PNL vs Mini-PNL: Complication Classification According to a Modified Clavien Grading System.
Treatment of calyceal diverticular calculi on minimally invasive percutaneous nephrolithotomy: a report of 24 cases
OBJECTIVE: To assess the safety, feasibility and the curative effect of treatment with minimally invasive percutaneous nephrolithotomy (MPCNL) in calyceal diverticular calculi. METHODS: A restrospective investigation was going on 24 cases of calyceal diverticular calculi, who were treated with minimally invasive percutaneous nephrolithotomy from February 2005 to May 2008. In all cases stone were removed using a direct approach and diverticular infundibulum was incised by Holium laser. Trans-diverticular percutaneous drainage was maintained 7 days, and trans-diverticular ureteral stent was removed 3 months after operations.RESULTS: Of 24 cases, 100% stone-free rate was achieved using one-stage minimally invasive percutaneous nephrolithotomy. The average opertion time and hospital stay were (65.5±28.1) min (range 55-110) and (5.7±2.5) d. (range 4-8). One case with infectious diverticular calculi occurred postoperative hyperpyrexia and recovered after antibiotics therapy, and no major complications were noted in the other patients. On the 3rd day after operations, the mean reduction in blood hemoglobin concentration was (18.1±11.7) g/L (range 9-35). All of patients were not found recurrance of diverticular calculi at average followup (45.6±7.6) months (range 36-60).CONCLUSIONS: Minimally invasive percutaneous nephrolithotomy is safe and effective treatment for calyceal diverticula calculi with high stone free rate, short hospitalization stay, and low incidence of introoperative and postoperative complications.
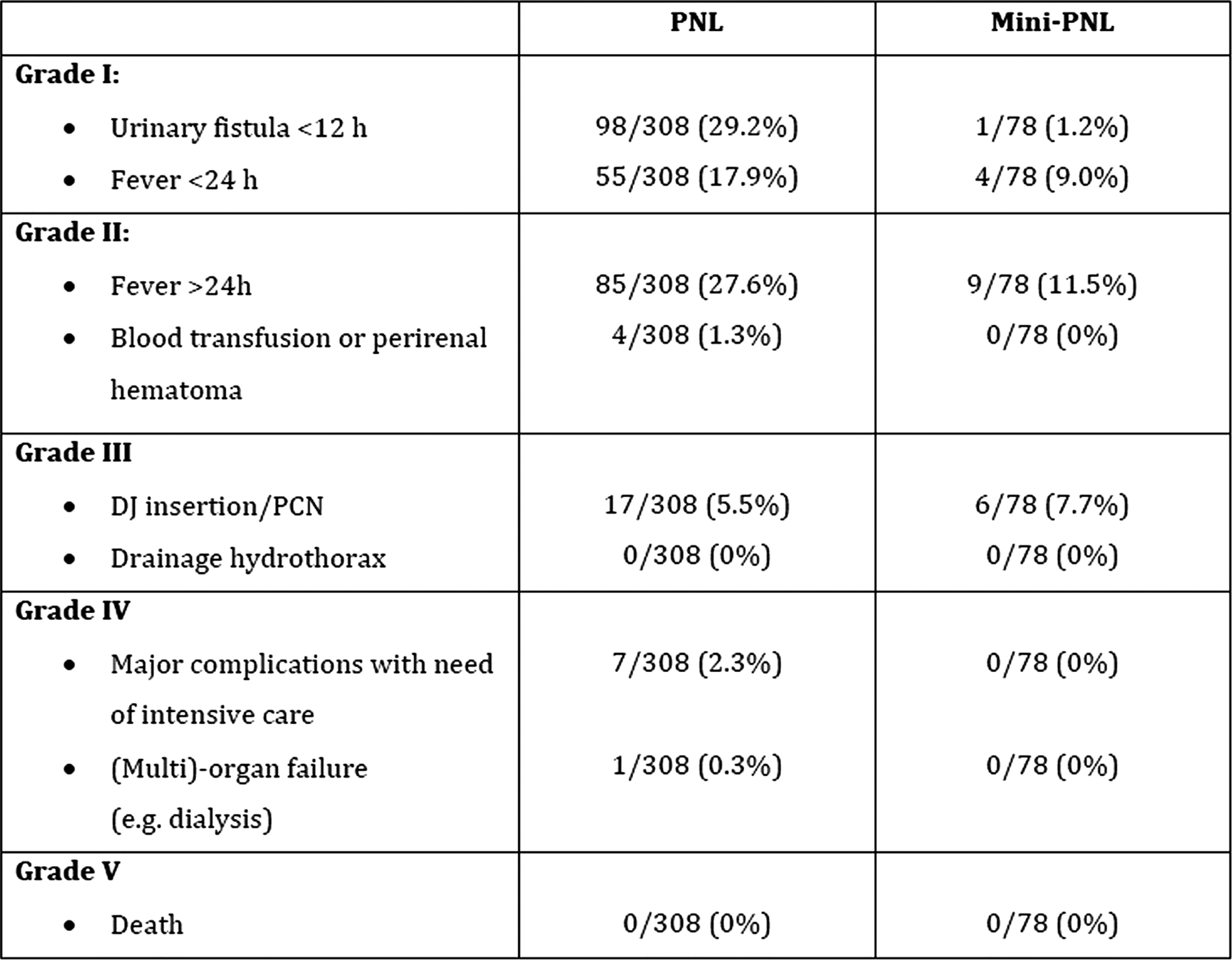
The Comparison between Minimally Invasive Percutaneous Nephrolithotomy and Retroperitoneal Laparoscopic Ureterolithotomy for Impacted Upper Ureteral Calculi
OBJECTIVE: To compare the efficacy and security between minimally invasive percutaneous nephrolithotomy (MPCNL) and retroperitoneal laparoscopic ureterolithotomy (RLUL) for impacted upper ureteral calculi. METHODS: A total of 76 patients with unilateral impacted upper ureteral calculi accompanied by hydronephrosis were included in this study, of whom 47 patients received MPCNL (MPCNL Group), and the other 29 patients received RLUL (RLUL Group). And the stone clearance rate, the incidence of operative complication was statistically analyzed. RESULTS: The mean operation time of RLUL (94.2±20.7)min was significantly longer than that of MPCNL (61.7±24.6)min (P = 0.001). The MPCNL Group got a stone clearance rate on the 3rd day after operations as 93.62% (44/47), without significant difference to that of RLUL Group as 100.0% (29/29) (P=0. 521). As compared with the RLUL Group, the MPCNL Group showed a significantly higher mean reduction in blood hemoglobin concentration on the 3rd day after operations, as (8.7±4.2)g/L vs. (3.7±1.9)g/L (P=0.007). The incidence of postoperative hyperpyrexia (T>38.5) between two groups showed no significant difference (8.51% vs 3.45%, P=0.611). And the incidence of postoperative urine leakage of RLUL Group was 3.45% (1/29), showed no significant difference with that of MPCNL Group (0.0%). CONCLUSIONS: MPCNL and RLUL showed satisfactory availability and security for management to impacted upper ureteral calculi, and RLUL meant less blood loss but more operation time needed. So for impacted upper ureteral calculi, RLUL can be considered available to skilled urologists in advanced hospitals.
Medical Malpractice in Endourology: Analysis of Closed Cases from the State of New York
Purpose: Medical malpractice indemnity payments continue to rise resulting in increased insurance premiums. We review closed malpractice claims pertaining to endourologic procedures with the goal of helping urologists mitigate their risk of lawsuit. Materials and Methods: All closed malpractice claims from 2005 to 2010 pertaining to endourologic procedures filed against urologists insured by the Medical Liability Mutual Insurance Company of New York were reviewed. Claims were reviewed for plaintiff demographics, medical history, operative details, alleged complication, clinical outcome and lawsuit disposition. Results: Twenty-five closed claims involved endourologic operations. Ten of the 25 cases were closed with an indemnity payment. The average payout was $346,722 (range $25,000 to $995,000). Sixteen plaintiffs were woman. Mean plaintiff age was 51.4 years. Cystoscopy with ureteral stent placement/exchange resulted in 13 lawsuits, ureteroscopic lithotripsy 8, percutaneous stone extraction 2, and shock wave lithotripsy 2. Seventeen malpractice suits were for alleged operative complications. Failure to arrange adequate follow-up was implicated in four cases. Error in diagnosis and delay in treatment was alleged in three claims.Conclusions: Urologists are not immune to the current medical malpractice crisis. Endourology and urologic oncology generate the greatest number of lawsuits against urologists. Most malpractice claims involving endourologic procedures result from alleged technical errors. Therefore, careful attention to surgical technique is essential to reduce the risk of malpractice litigation.
Flexible Ureterorenoscopy Compared to Mini-PNL for Solitary Renal Calculi of 1-3 cm Size

MP24: SWL
Treatment of Uretero-Pelvic Stones: Laser Ureteroscopic Lithotripsy and ESWL
INTRODUCTION Management of impacted uretero-pelvic (UP) stones remains challenging. We first performed retrograde endoscopic treatment for impacted UP stones (both in pelvis and proximal ureter), then the residual escaped stone fragments were treated by ESWL. MATERIALS & METHODS We analyzed the patients medical records between March 2005 and December 2010. A total of 12 patients with impacted UP stones, larger than 1 cm, after ESWL failing, were enrolled in this study. First endoscopic retrograde treatment was performed using a semirigid ureteroscope 7/9F and Holmium laser lithotripsy in general anesthesia on an in-patient. The day after the endoscopic procedure, ESWL was performed on the residual escaped stone fragments on an outpatient clinic using Dornier Compact Delta II lithotripter. The mean numbers of ESWL treatments were 1,2. Successful outcome was defined as: patient stone-free on radiography and renal ultrasounds (r US) 1 month after the treatment RESULTS Average stone diameter was 15,0 mm. All patients first underwent retrograde endoscopic holmium laser lithotripsy and then ESWL. Overall stone free rate was 100%. There were no significant complications CONCLUSIONS Impacted kidney stones require immediate attention to avoid the risk of infection or more severe kidney damage. Ureteroscopic holmium laser lithotripsy and ESWL are usually reserved to complex proximal ureteral stones-impacted calculi who failed other stone removal procedures, in marked dilatation of renal collecting system and in large stone.
Comparison of ESWL and URS after ESWL Failure in Patients, and Factors Contributing to the Failure of ESWL
Purpose: There is lack of data investigating the factors predicting the failure of ESWL treatment. The aim of this study was to identifying the factors affecting the failure of ESWL treatment, by analyzing ESWL and URS after ESWL treatment failure patients.Materials and Methods: Between January 2004 and July 2010, a total of 90 patients were reviewed. They were divided into two treatment groups: group A (n=50), who underwent ESWL for ureter stones, and group B (n=40), who received URS after ESWL because inadequate fragmentation was observed after three sessions per week. The patients' characteristics, such as sex, age, body mass index (BMI), and stone size, location, degree of hydronephrosis, and whether there was recurrence or only a single episode were reviewed. The impact of the possible predictors of ESWL failure was evaluated via multivariate analysis.Results: The univariate analysis showed that the obesity and stone size, location, and degree of hydronephrosis were significantly different between the two groups (p<0.05). On multivariate analysis, factors affecting to the ESWL failure were obesity (BMI>25 kg/m2; OR=3.5, 95% CI: 1.1-11.0), size (>1 cm; OR=10.5, 95% CI: 3.0-36.2), location (mid-ureter; OR=8.49, 95% CI:1.5-45.7), and hydronephrosis (severe; OR=12.3, 95% CI:1.9-79.5).Conclusions: A more-than-1.0-cm-diameter stone, location in the mid-ureter, and severe hydronephrosis were found to be significant predictors of ESWL failure for ureter stones. Thus, the stone size, location, and degree of hydronephrosis should be considered when making a decision regarding the treatment of ureter stones.
ESWT versus 16-Dot Plication for Peyronie's Disease
Introduction: We compared outcomes following ESWT and corporal plication for men with moderate Peyronie's disease.
Methods: SHIM, QOL and post-op results were reviewed for all patients undergoing surgery for Peyronie's disease at our institution between Jan 2009 and Jan 2011. ESWT was performed with a Stortz Duolith SD1, 0.25mJ, 3000 shocks weekly, for 3-12 treatments.
Results: 18 patients underwent ESWT and 12 underwent plication. Mean curvature decreased from 45 to 30 degrees; and 60 to 0 degrees respectively. 2/3rds of patients reported mild to moderate satisfaction following ESWT, and no patients were unhappy. Corporal plication provided high level of satisfaction in 2/3rds of patients, but at the risk of dissatisfaction in 1/3 of patients.
Conclusions: ESWT can be considered as a first line surgical therapy for Peyronie's disease in select patients due to its mild benefit and minimal downside.
Ten Years of Shockwave Lithotripsy: The Washington University Experience 1999-2009
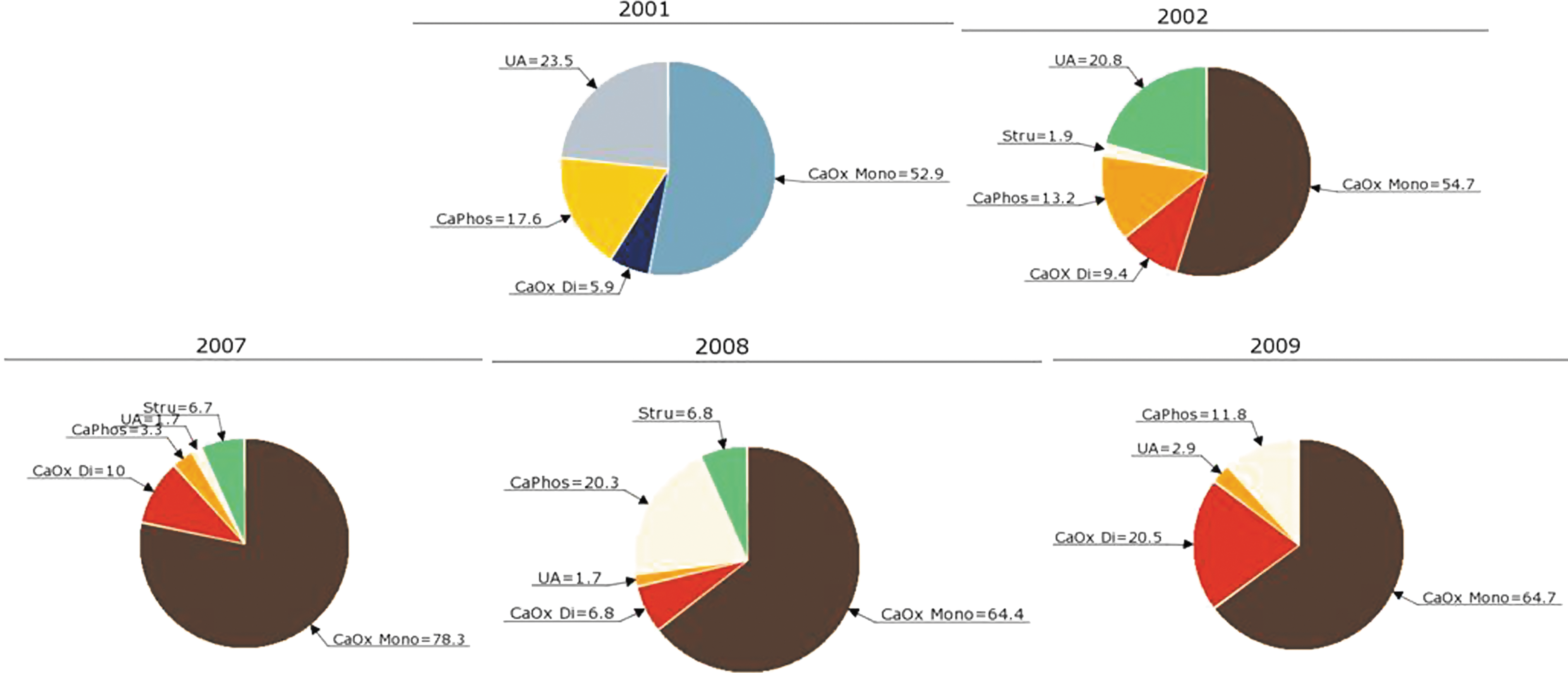
A Prospective Study Examining the Incidence of Bacteriuria and Urinary Tract Infection Post-Shockwave Lithotripsy
Introduction & Objective:Controversy exists over the need for antibiotic prophylaxis prior to shockwave lithotripsy (SWL). The AUA,s Best Practice Policy Statement uses level 1A evidence to indicate universal antibiotic prophylaxis, whereas the EAU,s Guidelines cites level 1A evidence to indicate prophylaxis only for patients with urinary drainage tubes, ureteral stents or infected stones. This prospective study evaluates the use of targeted antibiotic prophylaxis in patients undergoing SWL.Methods:Over a three-month period, patients undergoing SWL for urolithiasis were enrolled. All patients underwent urine dipstick, microscopy and culture prior to SWL. A urine culture was performed 3 days post-SWL if patients did not undergo antibiotic prophylaxis, or 2 days after finishing their course of antibiotic prophylaxis. All patients completed a survey documenting fevers or urinary symptoms post-treatment.Results:526 patients were enrolled. Only 3 (13.0%) of the positive urine cultures taken prior to SWL were both leukocyte and nitrite positive on urine dipstick, whereas 17 (54.8%) of the positive urine cultures were both leukocyte and nitrite negative on dipstick. 10 (2.2%) patients were administered antibiotic prophylaxis (6 of which had ureteral stents), and 14 (2.7%) were given antibiotics post-treatment. Post-SWL, only 1 (0.2%) patient developed a urinary tract infection (UTI) and 4 (0.8%) patients developed asymptomatic bacteriuria.Conclusions:The rates of UTI and asymptomatic bacteriuria following SWL are extremely low (<1%) with targeted antibiotic prophylaxis. This prospective study questions the need for universal antibiotic prophylaxis prior to SWL and for antibiotic prophylaxis in patients undergoing SWL with indwelling ureteral stents.
Department of Urology, Shintoshi Hospital, Iwata, Japan
Introduction: Previously we compared three types of shock wave generators (electrohydraulic, electromagnetic and piezoelectric types), using The Diagnosis Procedure Combination (DPC) database; an inpatient administrative claim database in Japan and revealed that piezoelectric type and high hospital volume (HV) were associated with significantly low incidence of renal hemorrhage (OR, 0.13 and 0.48, respectively). HV is an annual operative caseload. Toward further investigation, we assessed how focal size and F2 angle affects the incidence of renal hemorrhage.Methods: We collected 22,414 patients who underwent ESWL for urolithiasis from July to December, 2006-2008. The lithotripters in each hospital were identified from a Japanese medical device magazine, or an online search. Results: Seventy-five renal hemorrhages were identified (0.51% and 0.14% in kidney and ureteral stones, respectively). Multivariate logistic regression analysis resulted in no significant frequency of renal hemorrhage among focal size (large (>100mm3) vs. small, p=0.844) and F2 angle (wide (>70 degree) and narrow, p=0.395).High HV (≥140/yr) still remained as a significant risk reducer (vs. low-(≤70/yr), OR=0.49).Acknowledgments: The DPC database was funded by a Grant-in-Aid for Research on Policy Planning and Evaluation from the Ministry of Health, Labour and Welfare, Japan (Grant number: H19-Policy-001)
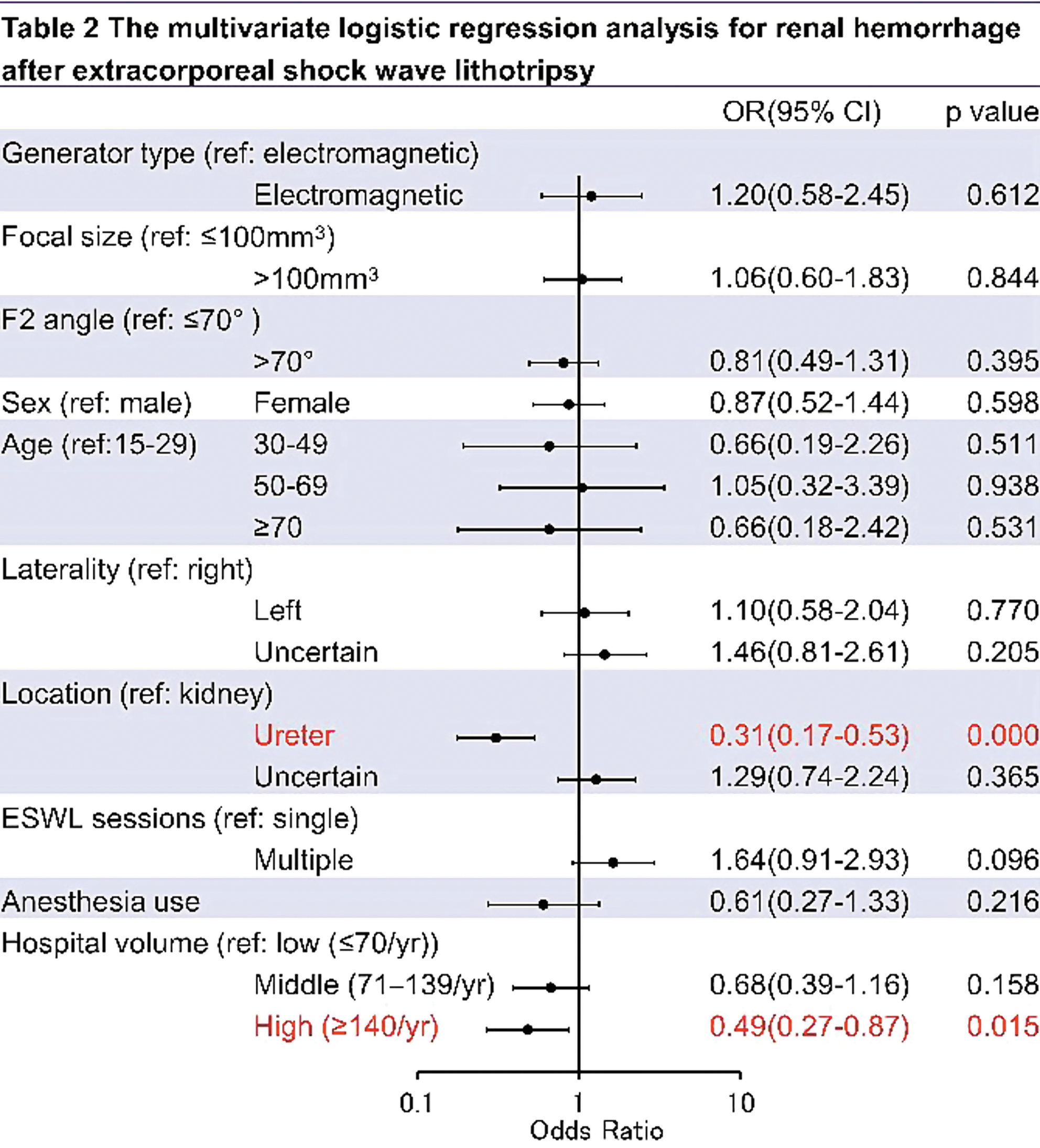
Treatment of inhomogeneous cystine stones with SWL is highly effective
Introduction. Cystine stones are generally accepted as being SWL resistant. In vitro studies have shown that cystine stones appearing homogeneous by CT required 61 percent more SWs for comminution than did stones showing regions of low X-ray attenuation (inhomogeneous stones). These findings demonstrate the possible feasibility of using CT to identify cystine stones that will be susceptible to SWL. Objective. The objective of this study was to evaluate in vivo outcome of SWL in patients with inhomogeneous cystine stones. Material and method. 7 patients with known cystinuria were found to have inhomogeneous kidney stone on multislice CT scans. The internal structure of the stones was evaluated on the bone window of the CT scan using magnification, and all stones showed void regions of low X-ray attenuation. The 7 patients (aged ranged from 3 to 84 years) were treated with SWL (Storz Medical Modulith SLX F2) for 15 individual stones. Stone size ranged from 7 mm to 12 mm. Results. Complete fragmentation was observed at treatment in all but one stone (93.3 percent). The treatment result was confirmed by non-contrast CT or IVP. The only failure was subsequently treated by retrograde intrarenal surgery (RIRS). Conclusion. Treatment of inhomogeneous cystine stones with SWL is highly effective. Patients with cystine stones suitable for SWL can be selected by the appearance of the stone on CT.
Preliminary Experience with the High Penetration EMSE 220F-XXP HP.
Introduction :In a short period (26/05/2010 - 04/03/2011) we evaluated a high penetration (HP) version of the existing EMSE 220F-XXP on our Dornier Lithotripter S.The EMSE 220F-XXP HP distinguishes itself from the standard EMSE 220F-XXP with a smaller aperture angle, a larger focus (89 mm x 6 mm vs 63 mm x 5 mm) and a treatment depth of 170 mm (vs 150 mm).Purpose :To investigate the performance of the EMSE 220F-XXP HP which was designed to better treat obese patients.Material and Methods :In this series a total of 162 patients (114 renal and 48 ureteral stones) with a BMI ranging from 19.3-36.3 (mean 26.3) was treated.Mean stone size was 67.4 mm2.Results :As compared to the EMSE 220F-XXP both mean number of SW (1521 vs 2368) and mean energy level (7 vs 10) were significantly lower.Overall treatment results were largely comparable to the EMSE 220F-XXP : retreatment rate 18.5%, total auxiliary procedure rate 9.9%, SFR 87.0%, EQ 68.No SW-related complications were encountered.Conclusions :The Dornier EMSE 220F-XXP HP offers two improvements:- improved treatment depth : obese patients!- excellent results with a significantly lower total energy Both retreatment rate and auxiliary procedure rate were slightly higher than with the EMSE 220F-XXP however. By delivering slightly higher total energy results no doubt still can be improved.
A Comparison of Extracorporeal Shockwave Lithotripsy with an Electrohydraulic Unit vs. an Electromagnetic Unit
Introduction and Objective: Several studies comparing electrohydraulic and electromagnetic lithotripters have shown mixed results. Our objective was to evaluate the effectiveness of a new electromagnetic lithotripter compared to our previous electrohydraulic lithotripter.Methods: We compared 100 patients treated with the Philips Lithotron Ultra electrohydraulic lithotripter with 100 patients treated with the Storz Modulith SLX F2 electromagnetic lithotripter. The outcome measured was stone free rate and success rate at 2 weeks and 3 months. Success was defined as being either stone free, having residual sand or an asymptomatic fragment<4mm on KUB x-ray. Results: The two groups were comparable in terms of stone size, location and density, BMI, presence of a stent and skin-to-stone distance. Univariate analysis showed no difference between the two groups for stone free or success rate at 2 weeks and 3 months. There was no difference in the complication rate and need for ancillary procedure between the groups. On average a significantly fewer number of shocks were administered with the Storz unit (p=0.02). Logistic regression, adjusting for stone size and location, BMI and presence of a stent showed no effect for type of lithotripter. Stone size (p=0.002) and presence of a stent (p=0.025) were the only significant predictors of stone free rate at 3 months in this model. Conclusion: The Phillips Lithron Ultra and Storz Modulith SLX F2 had equivalent stone free and success rates at 2 weeks and 3 months. However, the Storz Modulith demonstrated more efficient fragmentation as fewer shocks were administered.
Impact of Radiological Technologists on the Outcome of Shock Wave Lithotripsy
Purpose: To evaluate the correlation of radiological technologists (RTs) and the outcome of Shockwave Lithotripsy (SWL) in terms of fluoroscopy time, fragmentation rate and stone-free rate. Methods: A retrospective review of a prospectively collected database of 601 SWL treatments between June 2009 and March 2010 was performed. Patients with radiolucent stones were excluded. SWL was done by 6 RTs with different levels of experience. Follow up was available for 534 treatments. Multivariate analysis was performed. Results: RTs (A-F) performed 144, 109, 118, 58, 57, and 48 SWL sessions, respectively. There was no statistical difference among RTs in terms of mean stone size or stone location. In comparison with other RTs, RT A had significantly lower mean fluoroscopy time of 129 seconds (95% CI:120.8- 137.3) (p<0.001), higher stone-free rate (75.7%) (p=0.035), and stone fragmentation rate after a single SWL session (82.6%) (p=0.004). After correcting for stone size and location, fluoroscopy time (p<0.001), fragmentation rate (p=0.002), and stone-free rate (p=0.04) maintained their significance. When comparing the top 3 RTs performing>100 SWL sessions, RTs B and C had significantly higher fluoroscopy time compared with RT A [OR (95%CI): 1.84(1.38- 2.45); p<0.001 and 2.67 (2.00- 3.57); p<0.001], respectively. After correcting for stone size and location, RT B had significantly lower fragmentation rate when compared with RT A [OR (95%CI): 0.21(0.05-0.86), p=0.03]. However, there were no significant differences among the top 3 RTs in terms of stone-free rates.Conclusions: RTs significantly differ in fluoroscopy usage and stone fragmentation rate.
Maximum and Ideal Number of SWL Sessions: An Outdated Concept?
Introduction: extracorporeal-shock-wave-lithotripsy(ESWL) represents the non-invasive-treatment of urolithiasis, and can be repeated in case of failure. However, an ideal number of sessions before changing therapeutic modality has never been defined. Purpose: to assess if the concept of number of sessions can be considered as a reliable marker to evaluate ESWL-effectiveness. Methods: We retrospectively considered in a randomized-fashion clinical-data of 106 patients submitted to ESWL(DoLiS XXP) for calcium-oxalate-stones. Patient-age, stone-size and location, number of sessions, shock-waves per session, global number of shock-waves for patient, global accumulated-energy/patient, energetic-level (mJ), stone-free condition were considered. Data were analyzed with logistic-regression, non-parametric-tests(SPSS12).Results: 70patients (GroupA) were submitted to a single ESWL-session; the remaining patients (GroupB) underwent more-than-2 sessions (mean: 2,3 +/-0,67). Stone size was 9,37+/-3,3 mm in GroupA, 10,33 +/-4,2 in GroupB(p=0,2). Stone location and age did not differ significantlys.From a logistic-regression-model, stone location was associated to stone-free condition (p=0.072). However, among treatment-characteristics, accumulated-energy and global shock-wave amount per patient were the variables predictive of stone-free-status (p=0,028 and p=0,01,respectively). The number of sessions(p=0.8) and energetic-level(p=0.56) were statistically-insignificant.Conclusion: the number of ESWL-session is a concern often afflicting the physician. Such variable also defines the effectiveness-quotient (EQ) of ESWL-procedure. However, sessions may differ in both number of shock-waves and/or energy level, and the use of third-generation lithotriptors or pain influence those variables. In this perspective, the concept of number of ESWL-sessions seems to be overcome by overall-shock-waves/per patient or global accumulated-energy, that better define the whole energy applied to the stone and to the kidney unit.
New Dual Electromagnetic Shock Wave Lithotripter in the Management of Upper Urinary Tract Calculi under Analgesia.
Introduction:Urinary calculi are one of the most common urological disorders. Extracorporeal Shock Wave Lithotripsy (ESWL) is still considered the standard of care to treat upper urinary tract calculi. We present our experience at our stone centre with the new dual head electromagnetic lithotripter (Duet, Direx).Methods:138 patients were included in this prospective study from June 2009 to September 2010. All patients had 3000 shock waves at 120 shocks per minute under analgesia (Pethidine 75 mg IM, Diclofenac 100 mg PR & Paracetamol 100 mg PO) only. They were reviewed in 4-6 weeks with a plain X-Ray KUB. Results:Of the 138 patients studied, the male: female ratio was 95:43. The mean age was 35.4 years. Five patients had lithotripsy in the mono (single head) mode and the rest 133 had dual head lithotripsy. 108 patients had one session, 25 had two sessions and 5 had 3 sessions of lithotripsy. The mean stone size was 8.8 mm (range 5-20 mm). The stone distribution was upper calyx 22 (16%), middle calyx 14 (10%), lower calyx 79 (57%), renal pelvis 21 (15%) and upper ureter 2 (1%). The stone free rates werea. 5-10 mm=94/111=85%b. 10-15 mm=16/22=73%c. 15-20 mm=4/5=80%The overall stone free rate was 83%. Conclusion:The dual head electromagnetic lithotripter is safe and efficacious in treating upper urinary tract calculi. Patients benefit from effective treatment with the advantage of potentially reduced kidney damage and reduced analgesic requirement.
Urology Department, Charing Cross Hospital, Imperial College Healthcare NHS Trust
Purpose: to compare the efficacy of Piezoelectric and electromagnetic lithotripters in the treatment of Lower ureteric stones.Materials & Methods: Retrospective study of patients underwent ESWL to lower ureteric stones in our unit during the last 6 years. (Group I) 99Patients had ESWL by piezoelectric Lithotripter (Wolf Pizolith 2501) (Group II) 107patients had ESWL by electromagnetic Lithotripter (Storz SLX F2)Both groups were treated in prone position. Stone was localized initially by fluoroscopy Patients were reviewed after 3 weeks, if the stone or a significant fragment persisted for more than 3 weeks; further ESWL session was given. If the stone showed no fragmentation after 2 ESWL sessions; ureteroscopy was performed Patients were assessed regarding; stone fragmentation and clearance, the need for further ESWL or endoscopic intervention.Results: (see table)Conclusions:ESWL is an effective treatment for lower ureteric stonesElectromagnetic lithotripters have lower retreatment and higher success rate in comparison with piezoelectric lithotripters.
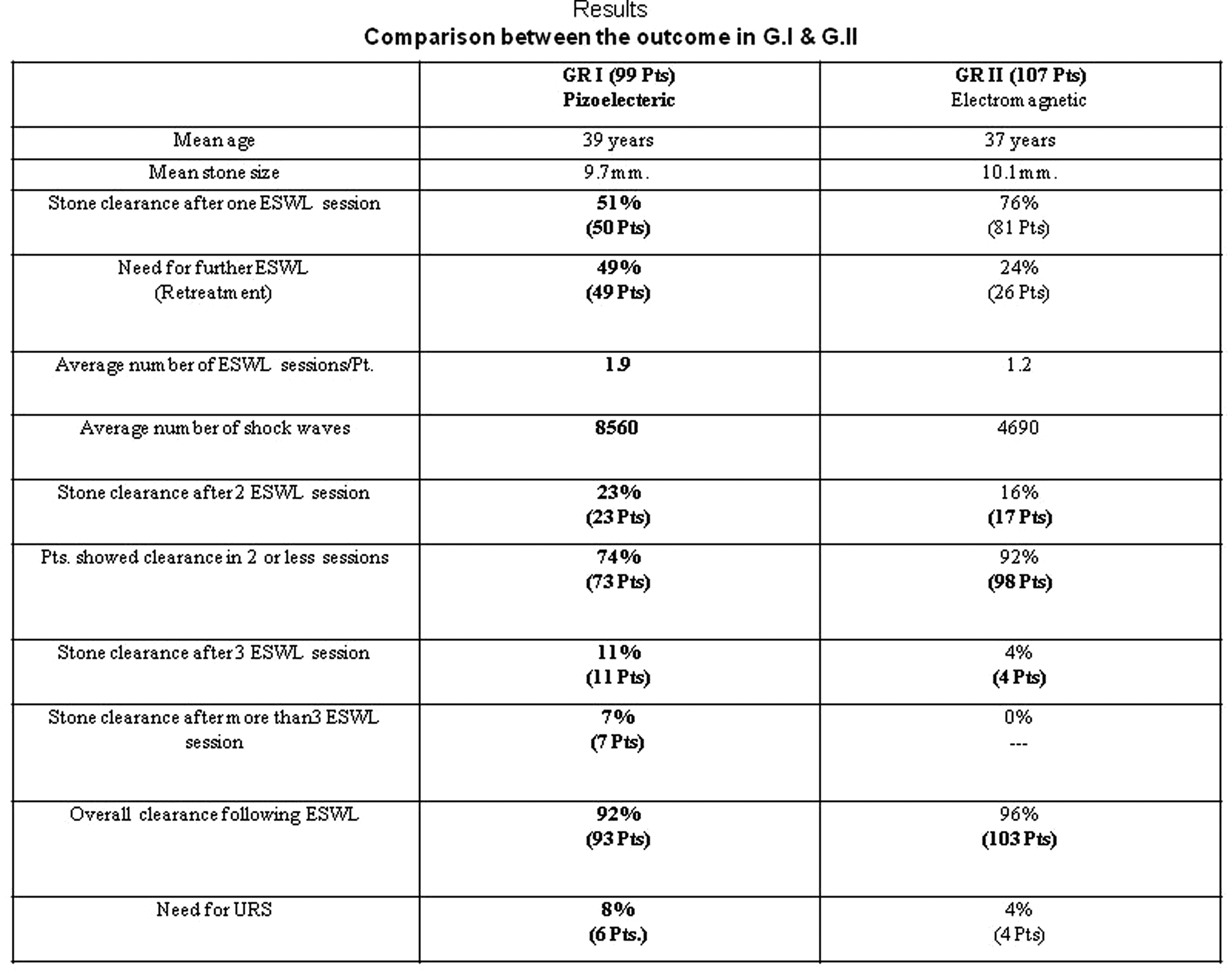
Urology Department, Charing Cross Hospital, Imperial College Healthcare NHS
Introduction1-4% patients who have their kidney stone treated with ESWL develop steinstrasse. At the two hospitals the first line of treatment is ESWL.Purpose: to demonstrate the efficacy of our technique Method:We have devised three different protocols depending on the type of steinstrasse seen on imaging.Type I: steinstrasse with a large lead fragment.Type II: steinstrasse with multiple very small fragments (no lead fragment).Type III: steinstrasse with multiple different size fragments but the largest is not the lead fragmentFor each type a different protocol was applied. The protocols differed in number of Shocks given, energy level, frequency and which fragments to treat. All patient had a KUB x-ray prior to the treatment, usually after 3-4 weeks from the kidney stone treatment, or earlier if patient attended A&E with renal colic.ResultsOut of 65patients with steinstrasse treated with ESWL, 86% were stone free (no ureteric stone) after 1 or 2 sessions. The other patient required ureteroscopy or JJ. ConclusionOur self defined protocols are reproducible and effective in managing this complication in a minimally invasive fashion and avoiding endoscopic intervention. ESWL should be considered the the first line treatment t of stienstrasee
Comparison of Efficacy Between First- and Fourth-Generation Lithotripters in the Modern Era: A Washington University Update

Predictive Factors for Outcomes of ESWL with Treating Ureteral Stones
Introduction and Purpose: Extracorporeal Shock Wave Lithotripsy (ESWL) has shown successful outcomes for ureteral stones. So we investigated predictive factors for failure of ESWL with treating ureteral stones. Materials and Methods: Between July 2006 and July 2009, a total of 153 patients underwent ESWL for ureteral stones diagnosed on NESCT were divided into two groups (group A, stone size <=10mm; group B,>10mm). The failure of ESWL was defined as with remnant stones larger than 4mm. We assessed age, sex, body mass index (BMI), stone size, location, laterality, skin-to-stone distance (SSD), hounsfield unit (HU) and the presence of secondary signs (hydronephrosis, perinephric edema, perinephric fat stranding and tissue rim sign). And we investigated predictive factors for failure of ESWL using logistic regression in each group. Results: The success rates were 90.2% and 68.6% in group A and B. In univariate analysis of each group, stone size, SSD and all of secondary signs had statistically significant differences in outcomes of ESWL (p<0.05). In multivariate logistic regression, stone size (OR=25.980; p<0.001) was an independent predictive factor for failure of ESWL in group A. And presence of perinephric fat standing (OR=20.536; p<0.006) and stone size (OR=27.156; p<0.001) were independent predictive factors in group B. Conclusions: Stone size is an independent predictive factor influencing failure of ESWL with treating ureteral stones. In addition to stone size, the presence of perinephric fat stranding is also an independent predictive factor in larger ureteral stones (>10mm).
MP25: Female Urology/Pediatrics
Dept of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction: Laparoscopic procedures for children with urologicalproblems are common in the present scenario. Laparoscopicsurgery is associated with complications such as port site hernia,which are not associated with open surgery. Drain site hernia is onevariety of port site hernia. Materials and methods: We undertookretrospective analysis of the pediatric patients who underwentlaparoscopic procedures, for the development of drain site hernias.We also analysed the various methods of prevention. Results:Among the 148 children who underwent laparoscopic procedures, 5(3.4%) had a port site hernia in the early post operative period. Allof them were drain site hernias with early presentations and thecontent was omentum. 3 patients had reduction under sedation. 2patients needed laparoscopy, one for the reduction into preperitonel space and the other for the non reducible hernia due toomental edema. All the patients had uneventful recovery.Conclusion: Port site hernia is an uncommon complication inchildren undergoing laparoscopy. Sedation during drain removaland judicious use of drain may help to decrease the complications.
Department of Urology, Tokai university Oiso Hospital, Oiso, Japan
Objective: Vesicoureteral reflux (VUR) can be treated with antibiotic therapy, open surgery or endoscopic injection. A goal in children is to reduce the incidence of febrile urinary tract infections (UTIs) and renal injury. The aim of this study is to investigate the outcomes of endoscopic injection for VUR and the incidence of febrile UTIs.Patients and methods: Between 1994 and 2010, a total 68 children (100 ureters) 0.2 to 15 years old with grade 2 to grade 5 VUR confirmed by voiding cystourethrography underwent endoscopic treatment with Teflon paste, collagen and dextranomer/hyaluronic acid polymer (DHAP). 13 ureters had grade2. 57, 25 and 5 ureters had grade 3, 4 and 5 refluxes, respectively. Results: The success rates were 85.2%, 77% and 90% with Teflon paste, collagen and DHAP by single injection, respectively. After second injections, 92.5% with successfully treated with Teflon paste and 83.6% was success with collagen. After endoscopic treatment with variable follow-up, febrile UTIs developed in 3% of all patients.Conclusions: Endoscopic treatment provides a high rate of success in children with reflux, and this treatment was associated with a low number of febrile UTIs following this treatment.
Scott Department of Urology, Baylor College of Medicine, Houston, Texas, USA
INTRODUCTION: Laparoscopic inguinal herniorraphy has been associated with reduced pain and easier contralateral evaluation and repair compared to the open approach in children. PURPOSE: We compare surgical outcomes in patients who underwent laparoscopic and open inguinal hernia repairs at our institution over the past seven years. METHODS AND MATERIALS: We retrospectively reviewed medical records from children who underwent an inguinal hernia repair by a single surgeon from 2003-2010. Surgical outcomes were compared with age-matched controls who underwent an open repair. RESULTS: Of 292 patients reviewed, 162 children underwent laparoscopic inguinal hernia repair, and 130 children underwent open inguinal hernia repair. Mean age for the laparoscopic and open cohorts was 5.55 years and 5.26 years, respectively. Intraoperative findings resulted in a change from a proposed unilateral to a bilateral repair in 45.1% in the laparoscopic group, versus none in the open group. Mean OR time for the laparoscopic and open groups was 66.5 and 30.6 minutes for those undergoing unilateral repair (p<0.001), and 75.95 and 46.6 minutes, respectively, for those undergoing bilateral repair (p<0.001). EBL, hospital stay, post-operative complications, and recurrences were comparable. There were three subsequent contralateral inguinal hernia repairs in the open group, versus none in the open group. CONCLUSIONS: Our study demonstrates a potential advantage of the laparoscopic inguinal hernia repair in the evaluation and repair of a contralateral patent processus vaginalis when compared to the open approach. Operative times were greater in the laparoscopic group, although safety and efficacy were comparable between groups.
Scott Department of Urology, Baylor College of Medicine, Houston, Texas, USA
INTRODUCTION: Although rare, large prostatic utricles have a higher incidence in male patients with perineal or peno-scrotal hypospadias. They may present with recurrent urinary tract infections, epididymitis, stones, urinary incontinence, and urinary retention, prompting surgical management. PURPOSE: We describe our experience with the resection of prostatic utricles using the laparoscopic approach. MATERIALS AND METHODS: A retrospective review was performed using medical records of patients undergoing a laparoscopic prostatic utricle resection by a single surgeon from 2003-2011. RESULTS: Four patients underwent laparoscopic excision of the prostatic utricle from 2003-2011. Three patients (75%) had a history of XX SRY-negative sex reversal, but all patients had a history of penoscrotal hypospadias and ambiguous genitalia. Mean age was 5 years (range: 2-7 years). Indications for surgery included recurrent urinary tract infections (50%), urinary retention (25%), and post-void incontinence (25%). There were no intra-operative complications, and hospital length of stay was 0.5 days (0-2 days). Mean follow-up time was 1.67 years. There were no post-operative complications, and none of the patients required additional procedures. On follow-up, all patients denied recurrent urinary tract infections or significant problems with voiding. CONCLUSIONS: Laparoscopic prostatic utriclectomy is a safe and effective treatment with minimal morbidity in patients with ongoing urinary symptoms due to an enlarged prostatic utricle.
Resonance Metallic Stents Do Not Effectively Relieve Extrinsic Ureteral Compression in Pediatric Patients
Introduction: The effectiveness of metallic stents Resonance to treat extrinsic ureteral compression in children has not been reported. We present our experience with these stents in children.Methods:2 patients underwent placement of Resonance stents for extrinsic compression at the Childrens Hospital of the University of Pittsburgh.Patient 1, a 12 yo female with a solitary left kidney and pelvic rhabdomyosarcoma, treated with surgery and chemoradiation. She developed worsening renal function secondary to ureteral strictures. Patient 2, a 14 yo female with Gardner syndrome, with desmoid tumors in the pelvis and retroperitoneum leading to right ureteral obstruction. Results:Both patients underwent successful placement of Resonance stents. Time to failure for patient 1 was 3 months and for patient 2, 3 weeks.Patient 1 represented in renal failure necessitating nephrostomy tube placement. She required an ileal ureter to preserve renal function in her solitary kidney.Patient 2 developed recurrent episodes of pyelonephritis and worsening hydronephrosis. She underwent a right subtotal ureterectomy with a right to left ureteroureterostomy. Conclusion:Metallic stents are ineffective in children, with a short time to failure. Further research is needed to develop stents that relieve extrinsic compression in children.
Is ESWL Daily Treatment for Children?
To determine the safety, efficacy and daily usable of extracorporeal shock wave lithotripsy (ESWL) in the treatment of pediatric nephrolithiasis and to analyze the stone size and location on stone clearance.This was a retrospective case series of 128 pediatric patients (17 years or younger) undergoing lithotripsy using a Low energy lithotripsy with the Siemens Lithostar lithotriptor. Treatment failure was analyzed to find any correlation with stone size and site and even they came to emergency service after ESWL treatment in same day's night.The overall stone-free rate was 93%. In the overall, treatment failed in 8 patients, who subsequently required ancillary procedures. Nineteen patients (15%) went to emergency service at the same night of the day with ESWL after ESWL procedure and the mean stone size was 9,36mm.We think that urolithiasis remains a one of the serious problem in children in our country. ESWL is highly effective for pediatric renal stones, with minimal morbidity. ESWL treatment should not be used as a daily treatment in children with kidney stone which has metabolic disorder.
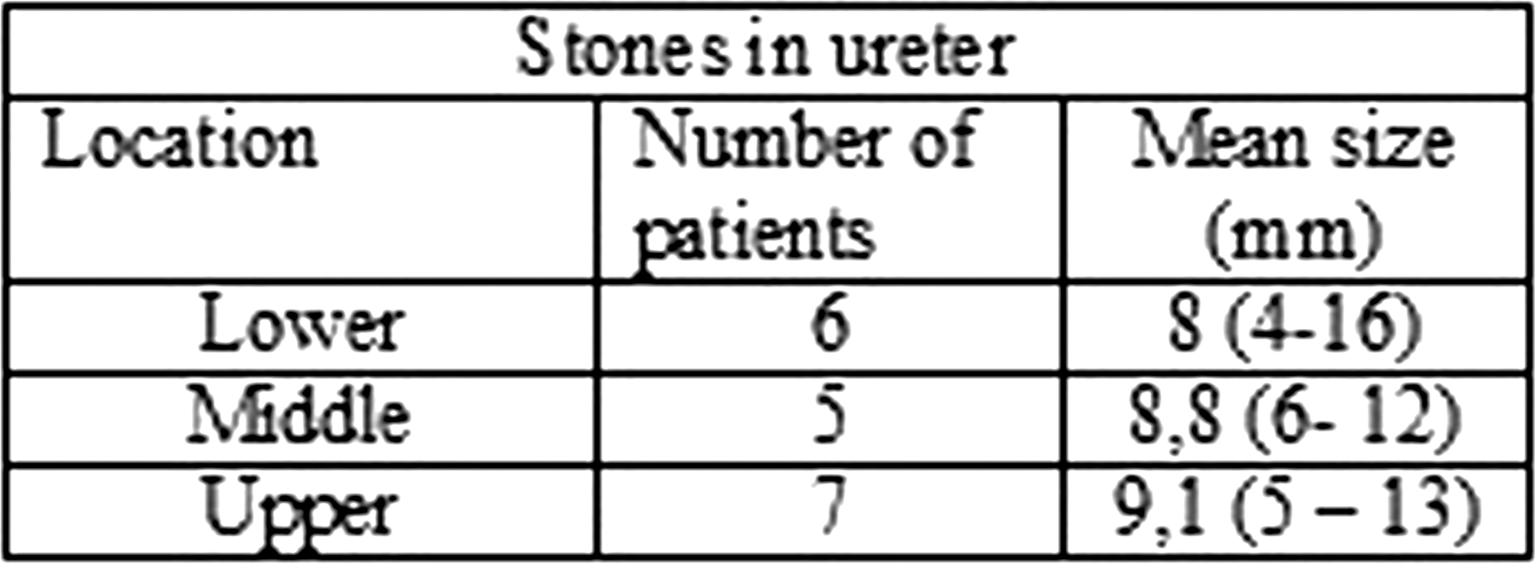
Department of Urology, Children's Hospital Boston, Harvard Medical School, Boston, USA
Introduction:Urolithiasis is associated with systemic medical conditions in adults, but associations have not been well studied in children. We investigated the association of urolithiasis with diabetes mellitus (DM), hypertension (HTN), and obesity among children with and without urolithiasis.
Methods:We performed a matched case-control study using the Pediatric Health Information System (PHIS) database. ICD-9 codes identified urolithiasis cases from 2004-2009. Four randomly selected controls were matched by age, hospital, type of hospital visit, and year of treatment. Diagnoses from all hospital encounters were ascertained for comorbid conditions. Univariate and multivariable conditional logistic regression were used to assess the associations of urolithiasis with DM, HTN, and obesity.
Results:We identified 9,843 urolithiasis cases and 39,047 controls. On univariate analysis, stone patients had significantly higher odds of obesity (OR 1.4, 95% CI 1.3-1.6) and HTN (OR 2.1, 95% CI 1.9-2.4) compared to controls. The odds of Type I DM was lower among cases compared to controls (OR 0.4, 95% CI 0.3-0.5). After adjusting for gender, race, insurance type, and number of visits using logistic regression, children with urolithiasis still had higher odds of obesity (AOR 1.3, 95% CI 1.1-1.3) and HTN (AOR 1.6, 95% CI 1.4-1.9) and lower odds of Type I DM (AOR 0.3, 95% CI 0.3-0.4) as compared to controls.
Conclusions:Among pediatric patients at freestanding childrens hospitals, urolithiasis is associated with higher odds of obesity and hypertension and a lower odds of Type I DM. These findings may be helpful in further elucidating the etiology of pediatric urolithiasis.

North Khorasan University of Medical Sciences and Health Services, Bojnurd,iran
ABSTRACTBackground & purpose:To evaluate and report our experience in performing tubeless percutaneouse nephrolithotomy (PCNL) in children. Patients & methods:Between 2007 and 2010, 22child underwent PCNL for complex renal calculi . The dilatation was performed with amplatz dilatator and 24 F nephroscope and 30 Fr sheet were used . lithotripsy was done using pnoumatic with or without ultrasound. In large and branched stones two tracts were obtained as needed .We reviewed stone size and clearance, complication rates and hospital stay of the children.the parents were informed preoperatively.Results:Patients were 14 boys and 8 girls with the mean age of 6.7 years ( ranges 1−10).The average operative time was 65.11 minutes. The mean stone size was 17.6 ( range 10−30 )mm and the mean percent of stone free rate was 89.09%. The mean level of hemoglobin was 13.09mg/dl and 11.96(SD=0.85) mg/dl before and after PCNL, respectively. The mean drop of Hb was 1.14mg/dl.The mean number of tract was 1.27and the mean duration of hospitalization was 2.91day ranges between 2 to 4 days.Transient postoperative fever was the commonest complication (27.3%) .There were not any sepsis or blood transfusion.Conclusion:Using 24 F nephroscope in pediatric ,PNL is safe and effective and in the absence of arterial bleeding, bleeding that abundant continuing procedure, and integrity disrupted of pyelocalyceyl system, we do not need to left nephrostomy tube at the end of procedure.KEYWORDSTubeless PCNL, pediatric, urolithiasis,
Comparison of Adults and Children in Laparoscopic Pyeloplasty for Ureteropelvic Junction Obstruction
Purpose: We compared the technical details and surgical outcomes of adult and pediatric laparoscopic pyeloplasty and discussed the lessons learned from these comparisons.Materials and Methods: Forty-nine patients underwent laparoscopic pyeloplasty for the management of ureteropelvic junction obstruction (UPJO) between August 2006 and Novemver 2010. The patients were divided into two groups; adults (over 16 years old; n=22) and children (under 15 years old; n=27). Medical records and surgical videos were reviewed with particular attention paid to patient characteristics, procedures, and surgical outcomes.Results: Crossing vessels were more common in adults (P<0.05). After June 2009, we tried to perform a transmesenteric approach for left UPJO, and actually performed this for 4 of 6 (67%) adults and 9 of 13 (69%) children. There was no significant difference in median operative time between adults and children; however, the mean time required for exposure of the UPJ in children (50 minutes) was less than that in adults (78 minutes; P<0.005). The mean time required for ureteropelvic anastomosis tended to be longer in children. Postoperative complications were found in 3 adults and 2 child. The percentage reduction in anterior-posterior diameter of the renal pelvis in children was significantly greater than that of adults (P<0.05). Successful resolution of UPJO was observed in 90.9% of adult and in 92.6% of children.Conclusions: Understanding of the key surgical steps by experience of both adult and pediatric laparoscopic pyeloplasty can provide for the improvement of laparoscopic skills and facilitate procedures in both adult and pediatric populations.
Department of Urology, University Hospital Basel, Basel, Switzerland
ABSTRACT WITHDRAWN
Texas Children's Hospital, Houston, Texas, USA
INTRODUCTION: The laparoscopic dismembered pyeloplasty has evolved as a major treatment option of ureteropelvic junction obstruction in children, with several technique modifications to facilitate the laparoscopic approach. PURPOSE: We attempt to mimic the open technique by placing interrupted anastomotic sutures and avoiding ureteral stenting. We report our experience with 100 consecutive cases. MATERIALS AND METHODS: An IRB-approved retrospective analysis was performed based on medical records of all patients undergoing laparoscopic pyeloplasty at our institution from 2002 to 2009. RESULTS: 98 patients and 100 renal units were reviewed. Average patient age was 10.2 years (0.1-19.7). Six of the cases were re-do procedures. Kidneys were approached through a mesenteric window in 49 and by reflecting the colon in 51. An interrupted anastomosis was performed in all. No intraoperative injuries were encountered. Twenty-eight patients were stented; the remainder had JP drains placed as alternative drainage. Three patients had self-limited anastomotic leaks requiring prolonged JP drainage, while ten patients required a post-op stent or nephrostomy. Six patients required drainage within 16 days of pyeloplasty and the other four were placed later for workup of chronic pain. Two patients experienced post-op UTIs and two presented later with retained stents. Six patients ultimately required an endopyelotomy or repeat pyeloplasty, three of which were re-do procedures. Mean follow up was 9.2 months. CONCLUSIONS: Laparoscopic pyeloplasty can closely emulate the open dismembered pyeloplasty, the gold standard. A high success rate can be expected when performing an interrupted anastomosis with minimal ureteral stenting.
Pediatric Urology, Washington University School of Medicine, Saint Louis, Missouri, USA
Department of Urology, University of California, Irvine School of Medicine, Orange, USA
OBJECTIVE: Botulinum-A toxin is a well established medikation for neurogenic detrusor overactivity. Recent studies showed good short term results for therapy of ideopathic detrusor overactivity in adults. This prospective study included therapy resistant children with overactive bladder. METHODS: 17 children (6 boys and 11 girls) with resistant non neurogenic detrusor overactivity, decreased bladder capacity for age, urge incontinence as well as enuresis were enrolled. Main treatment duration before botox injection was 39 month. A dose of 100 U of Botulinum-A toxin was injected in the detrusor muscle. RESULTS:12 patients showed full reponse after 1st injection (dry over the day and complete loss of urge) with a mean increase in bladder capacity from 147cc to 233cc (p<0.02). 4 children showed partial response with 60% decrease in incontinence episodes over the day and urge, increase of bladder capacity from 162cc to 251cc (p < 0.001). One boy remained unchanged. 11 of the 12 full responders were still cured after 12 month, while 1 boy showed relapse after 7 month. 3 girls and 1 boy underwent 2nd injection with full response in 3 of the 4 children. Side effects were reported in 3 children mit temporaryly increased residual bladder volume up to 2 weeks after injection, 1 girl experienced 1 episode of symptomatic lower urinary tract infection. CONCLUSIONS:Botulinum-A toxin injection in children with non-neurogenic overactive detrusor is an excellent treatment adjunct with marginal side effects and good long time results after 1 injection of 71%, after 2nd injection of 88%.
Vesicouterine Fistula Presenting with Cyclic Heamaturia : A Case Report
AbstractBACKGROUND: Vesicouterine fistula is a rare complication most commonly associated with cesarean section. Presentation and position of fistulas make their diagnoses difficult. CASE: A 32-year-old woman presented with cyclic hematuria following a cesarean section for a dead 28 week fetus .She presented two week following cesarean section. it was initially thought to be a simple cystitis. Careful evaluation and a high index of suspicion resulted in the correct diagnosis of a vesicouterine fistula. The definitive diagnosis was made with cystoscopy. The patient was successfully treated with uterus-sparing laparoscopic surgery.CONCLUSION: Vesicouterine fisula rarely is thought of in the differential diagnosis because of its rarity and negative results on radiologic and endoscopic tests .This case illustrates the importance of a comprehensive evaluation of all patients suspected of having a urogenital fistula or those with unusuall sign and symptoms following cesarean section. Although surgical repair of vesico-uterine fistulas are performed by different open approaches , it seems laparoscopy has the same results with its unique benefits. Key words: Vesicouterine fistula, Caesarean section.
Recurrence Bacterial Cystitis: Bladder Instillation with a Combinated Solution of Sodium Halurate and Chondroitin Sulphate (IALURIL)
The chronic cystitis in women is a problem. The pathogenesis is not very clear, but the bladder epithelium defect has a fundamental role. In the genesis of bladder flogosis the defect of glycosaminoglycans (GAGs) plays, probably, a role of the primo movens. In this study we evaluated the role ofbladder instillation with a combinated solution of sodium halurate and chondroitin sulphate (IALURIL) in patients with recurrent bacterial cystitis.MATERIALS AND METHODS:From march 2010 to march 2011 55 patients is presented, mean age of 54 years, with diagnosis of recurrent bacterial cystitis, no responder to conventional teraphy. We treated, weekly, with intravesical solution of sodium halurate and chondroitin sulphate (IALURIL), in sterile solution, over a period of four weeks. Then, after steril urine, one instillation monthly for eight months. We evaluated, monthly, the urinocolture. The patients with positive urinocolture no underwent bladder instillation. RESULTS: There was no toxicity arising from the treatment, given that no adverse effects were recorded in relation to it. 27 pts (49.09%), after the complete cycle of instillation, had urinoculture negative in each exam evaluated. 14 pts (25.4%) had sterile urinoculture after the first four instillation, but they recurred after subsequent two months (11 pts) or three months (2 pts) or four months (1 pts). 11 pts presented in the first instillation positive urinocolture (20%).CONCLUSION: the clinical use of IALURIL in patients with chronic cystitis has a good tollerance. This combinated sterile solution is effective in pts with a possible GAG layer deficit, reducing recurrence and bladder sintoms.
Narrow-Band Imaging System as a New Diagnostic and Therapeutic Tool for Ulcer Type Interstitial Cystitis/Painful Bladder Syndrome
The current diagnostic standard for interstitial cystitis/painful bladder syndrome (IC/PBS) is cystoscopic examination with hydrodistention and endoscopic fulguration (TUF) is applicable for Hunner lesions. We evaluated the diagnostic efficacy of NBI for the detection of Hunner ulcers and therapeutic efficacy of narrow band imaging (NBI)-assisted TUF for ulcer type IC/PBS. Nineteen patients suspected of having IC/PBS were enrolled. Patients were first evaluated by white light imaging (WLI) and second by NBI. Presence and number of the ulcers were estimated by each cystoscopy. Then, ulcers were endoscopically fulgurated. Treatment outcomes of TUF were evaluated by OLeary and Sant Symptom and Problem score and VAS. Seventeen patients were diagnosed as IC/PBS. Whereas WLI detected ulcers in 12 cases, NBI detected in 13. The mean number of ulcers detected by WLI and NBI were 2.4 and 3.5 per patient, respectively. TUF was performed in twelve cases and Symptom score, Problem score and VAS were significantly decreased postoperatively (Table). Perioperative complications were noted in two and aggravation of symptoms was found in four and re-TUF was done in one during follow-up. Our results demonstrate that NBI could be a new diagnostic and therapeutic tool for ulcer type IC/PBS.
Department of Pelvic Reconstructive Surgery, Tokyo Women's Medical University Medical Center East, Tokyo, Japan
Aims of Study: Interstitial cystitis (IC) commonly affects females, whose symptoms include pain from bladder filling and urinary frequency. Hydrodistension (HD) is a common therapy, but the effects of HD are short-lived, because transurethral coagulation (TUC) is necessary for classic IC, which is characterized by Hunner ulcer. In this retrospective study, we evaluated the patients with classic IC, treated by HD with TUC.
Materials and Methods: Sixty-nine classic IC cases in women were treated by HD (n=19) or HD with TUC (n=50). They were followed with the frequency volume chart, O'Leary Sant questionnaire (ICSI / ICPI), and a VAS of pain before the surgery, and at 2months and 6 months after the surgery.
Results: The mean ages of the patients were 66±10 years. 24-hour frequency was 20±17. The mean voided volume and maximum voided volume were 102±46ml and 179±74ml respectively. ICSI and ICPI were 15±4 and 12±3 respectively, and VAS was 7±2. All data improved significantly at 2 and 6 months after the surgery, but the data at 6 months became worse compared to that at 2 months after the surgery. In HD with TUC group, all data at 2 months after the surgery and voided volume at 6 months after the surgery improved compared to the HD group. In the group of HD with TUC, the patients whose ulcers were coagulated completely improved, compared to the patients with incomplete coagulations.
Conclusions: HD with TUC is useful rather than HD and the complete coagulation of ulcer in TUC is more effective.
MP26: Robotic/Lap Upper urinary Tract 5
Laparoscopic Ureterolysis for Retroperitoneal Fibrosis.
INTRODUCTIONRetro-peritoneal fibrosis is caused by the entrapment of one or more commonly both ureters in thick fibro-collagenous material, due to variable aetiologies. This presents by bilateral hydronephrosis, and is treated by freeing the ureter, intraperitonealisation of the ureter and or omental wrapping.PURPOSETo outline our experience with uretrolysis for cases with reteoperitoneal fibrosis.PATIENTS AND METHODSWe performed laparoscopic ureterolysis, and intraperitonealization of the ureter in 6 renal units in 3 patients. Two females and one male, ages were 36, 48 and 49 respectively. The aetiologies were idiopathic in all patients.. We started by insertion of bilateral Double J stents, before the procedure.The technique was done in the left lateral position, and the patients position was changed during the procedure.RESULTS Operative time was 6, 4 and 5 hours respectively. No intra operativeor post operative complications or bleeding were encountered . Hospital stay was 48 hours. CONCLUSIONLaparoscopic ureterolysis, is a safe and effective substitution to open ureterolysis, and saves the patient the morbidity of the large abdominal incision.
R.E.N.A.L Nephrometry Score: Impact of Robotic Programme on Utilization Rates of Partial Nephrectomy in T1 Tumors.
Background: R.E.N.A.L Nephrometry score (RNS) have been proven to be effective for decision-making and comparison between renal masses. It has been shown to provide accurate description of the complexity of renal mass. Objective: To do a retrospective analysis of RNS of clinical T1 renal tumors of patients with normal renal function to determine the utilization rates of various MIS treatment modalities in a single centre.Material and Methods: The patients underwent either radical (multiport [LRN]/LESS [LESS RN]) or partial (open [OPN]/lap [LPN]/ robotic [RAPN] nephrectomy for T1 tumors. 3D CT scan was retrospectively studied for RNS calculation. RPN was utilized only during last 6 months. Any association between the RNS score and various procedures were then studied using students t test using SPSS software 15.Results: A total of 32 patients radical 10(LRN-6, LESS RN-4) and partial (OPN-5, LPN-5, RAPN-12) were operated between July 2010 and 2011. The RNS were 8.75±1.70, 8.5±1.37, 9.2±1.41, 7.2±0.89 and 8.75±1.21, respectively. In the partial nephrectomy group, there was significantly higher RNS for OPN (p=0.027) and RPN (p=0.021) vs. LPN. In the radical nephrectomy group, there was no difference between LRN and LESS RN group. When radical and partial nephrectomy were compared, there was no difference between LRN and OPN (p=0.89) and LRN and RAPN (p=0.42) while significantly more between LRN and LPN group (p=0.032).Conclusion: LPN had significantly lesser RNS. RAPN could be performed on patients with higher RNS, thereby decreasing the utilization rates of OPN and LRN.
Laparoscopic Radical Versus Laparoscopic Partial Nephrectomy for Kidney Cancer Resection: Long-Term Oncologic Outcomes.
INTRODUCTION:We compared oncologic outcomes of laparoscopic radical nephrectomy (LRN) and laparoscopic partial nephrectomy (LPN) for localized renal cell carcinoma.METHODS:This retrospective analysis compared patients undergoing LRN (n=197) or LPN (n=243) at a tertiary referral center from December 2002 to July 2011 for renal cell carcinoma. Exclusion criteria were: distant metastasis at diagnosis ,bilateral tumors and venous system involvement.The endpoints included radiologically verified systemic and local recurrence, cancer-specific survival and overall survival.RESULTS:No significant differences in 5 years, metastasis free survival (MFS), disease free survival(DFS), cancer specific survival (CSS) and overall survival (OS), between LRN and LPN for the resection of kidney cancer were observed.The 5 years MFS and DFS for patients treated with LRN and LPN were 89.1% vs 90.4% (p=0.331) and 86.4% vs 90.3% (p=0.737), respectively. CSS and OS for patients who underwent LRN and LPN were 98% vs 96.6 % (p=0.661) and 96.8% vs 94.1% (p=0.79), respectively. Local recurrence free survival was similar between the two groups 90.2%. CONCLUSIONS:The current retrospective data comparing long-term oncologic outcomes between LRN and LPN demonstrate that in patients with localized kidney cancer, LPN provides equivalent oncologic efficacy of LRN during a follow-up period of 5 years.
Department of Urology, Tohoku University School of Medicine, Miyagi, Japan
Purpose:Despite clear trends toward minimally invasive surgery, information about laparoscopic partial nephrectomy (LPN) in Japan is sparse. We conducted a retrospective survey to clarify time trends for LPN and analyze surgical and oncological outcomes. Material and Methods:A nationwide survey was performed. Between 1998 and 2008, 1,375 patients underwent LPN at 54 institutions. Complications, patterns of tumor recurrence and recurrence-free survival were analyzed. Results:Renal pedicle clamping was used in 1,031 cases (75%) and renal cooling was performed in 64%. Median warm/cold ischemic time was 37/53 min. Median tumor size was 2.3 cm (IQR 1.6 to 2.7). Multivariate analysis identified total operative time, operative blood loss and surgical margin status as independently associated with high grade (grade 3-5) urological and non-urological complications. Despite increases in central tumor, a trend was seen toward shorter warm/cold ischemic time in recent cases and the overall complication rate did not change throughout the study period. With a median follow-up of 26 months for 1,193 malignancies, 22 patients (1.7%) developed recurrence, including local recurrence in 7 (0.5%), lung in 8 (0.7%), lymph nodes in 2 (0.1%) and bone in 4 (0.3%). Of the 26 cases with positive surgical margins, only one developed local tumor recurrence. Conclusions:We performed the nationwide survey of LPN in Japan. LPN could be performed with acceptable positive margins and complication rates. Most tumor recurrences occur as metastases, and surgical margin status appears to have little impact on oncological outcomes.
Comparable Long-Term Oncologic Outcomes for Radiofrequency Ablation Versus Partial Nephrectomy in Patients with Solitary Clinical T1a Renal Cell Carcinoma
We compared long-term oncologic outcomes for radiofrequency ablation (RFA) versus partial nephrectomy (PN) for treatment of clinical T1a renal cell carcinoma (RCC).
We retrospectively reviewed outcomes for RFA vs. PN performed for solitary cT1a RCC among patients with a minimum post-treatment follow-up of 5 years. Those with hereditary RCC syndromes, multiple and/or bilateral tumors, metastatic disease and/or metachronous tumors at presentation were excluded. The Kaplan-Meier method and long-rank test were used to compare 5-year overall survival (OS), cancer-specific survival (CSS), local recurrence-free survival (local RFS), overall disease-free survival (DFS) and metastasis-free survival (MFS) for RFA vs. PN.
35 RFA and 34 PN patients met selection criteria. For RFA vs. PN respectively: mean age was 62.6 vs. 52.7 years (p=0.0001). All other demographic and clinical variables were similar. Median follow-up was 6.5 vs. 6.0 years. OS, CSS, local RFS, DFS and MFS were 100% vs. 100%, 100% vs. 100%, 91.4% vs. 94.1% (p=0.99), 91.4% vs. 91.2% (p=0.70), and 100% vs. 97.1% (p=0.33).
In appropriately selected patients with cT1a RCC, long-term oncologic outcomes for RFA are favorable and comparable to those for PN. Prospective larger series with extended follow-up are needed to better define its clinical role in this context.
Laparoscopic and Robotic Partial Nephrectomy with Controlled Hypotensive Anesthesia to Avoid Hilar Clamping: Feasibility,Safety and Perioperative Functional Outcomes
IntroductionAim of the study was to evaluate feasibility and safety of Laparoscopic and Robotic Assisted Partial Nephrectomy (RAPN) with controlled hypotensive anesthesia to avoid hilar clamping and eliminate renal ischemia.Matherials and MethodsSixty patients with renal tumors eligible for NSS and without any contraindications to hypotensive anesthesia underwent partial nephrectomy (PN) without hilar clamping and in controlled hypotension (CH) during tumor excision. Forty Laparoscopic Partial Nephrectomy (LPN) and 20 (RAPN) were performed. All patients eligible for LPN or RPN regardless of tumor site, size or growth pattern (endophytic-esophytic) were included in this study.PADUA and RENAL score were recorded for all renal masses.Closure of the renal defect was performed while restoring normotension. Results All cases were successfully completed. Median tumor size was 3,6 cm (range: 1.8-10); operative time was 2 h (range 1-3.5), blood loss was 200 ml (range 30-700), and hospital stay was 3 d (range 3-8). Median duration of CH with a median MAP of 65 mmHg (raange 55-70) was 14 minutes (range 7- 16).During surgery blood transfusion was not necessary in any patient. Four patients (6%) required one packed red blood transfusion postoperatively.Postoperative complications occurred in 3 patients: port site bleeding, hemorrhage and hematoma. Median pre and postoperative serum creatinine levels were 0.9mg/dl and 1.02mg/dl, while eGFR was 91,11 and 70,06, respectively.Conclusions: in our experience CH allowed to perform LPN and RAPN without the need of renal hilum clamping. All procedures were safely completed and perioperative outcomes are encouraging.
Robotic Partial Nephrectomy Using Robotic Bulldog Clamps: Initial Series
Introduction
The need for a skilled assistant to perform hilar clamping during robotic partial nephrectomy is a potential limitation of the technique.
Purpose
We describe our experience using robotic bulldog clamps applied by the console surgeon for hilar clamping.
Materials and Methods
A total of 60 consecutive patients underwent robotic partial nephrectomy, 30 using laparoscopic bulldog clamps applied by the assistant and 30 using robotic bulldog clamps applied with the robotic Prograsp instrument. Perioperative outcomes were compared between groups.
Results
All 30 patients underwent successful hilar clamping during robotic partial nephrectomy using robotic bulldog clamps with no intraoperative complications and without the need for readjustment/reclamping. Robotic bulldog clamps provided adequate ischemia even for tumors greater than 4cm, hilar, endophytic, multiple tumors and multiple renal arteries. Both groups had similar baseline characteristics. The group with robotic bulldogs had perioperative outcomes at least comparable to the laparoscopic bulldog group for median console time (174 min vs. 189.5 min, p=0.09), mean warm ischemia time (19.4 min; range: 8-30; vs. 22.1 min; range: 10-32; p=0.08), and median EBL (75 vs. 125 ml, p=0.06). There was a trend to lower console time, warm ischemia time, and estimated blood loss.
Conclusions
Robotically applied bulldog clamps are a safe and feasible method of hilar occlusion during robotic partial nephrectomy, performing at least as well as laparoscopic bulldog clamps while allowing the console surgeon greater autonomy and precision for hilar clamping.
Robot-Assisted Laparoscopic Partial Nephrectomy for T1a Renal Tumor. Initial Series at Fujita Health University.
INTRODUCTION: The challenge of Laparoscopic partial nephrectomy (LPN) is to resect a tumor in a bloodless field within a limited warm ischemia time (WIT), followed by hemostatic renorrhaphy under restricted movement of laparoscopic instruments. Therefore, LPN still remains challenging to even experienced laparoscopic surgeon. daVinci device improved the movability of forceps and provided 3D visualization. We evaluated outcome and safety of our initial series of robot-assisted laparoscopic partial nephrectomy (RALPN) for kidney tumor. METHODS: Since July 2010, RALPN were carried out in six cases. Tumor size ranged from 15 to 36 mm, and RENAL score consisted of 4 pts in one, 5 pts in 3, 6 pts and 9 pts in one case each. RALPN was undertaken by single surgeon through transperitoneal or retroperitoneal approach in three cases each.RESULTS: RALPN was completed in all cases without conversion to open or hand-assisted surgery. The median operative time and WIT were 212 and 18 minutes and 40 ml, respectively. Postoperatively, urine leakage from the resected surface was noted in one case, which was manageable by urinary tract drainage alone. Pathological examination showed renal cell carcinoma with negative surgical margin in all cases. CONCLUSIONS: Introduction of daVinci device to LPN made this procedure, RALPN, a secured and promising one, which leading to shorten the WIT and to achieve satisfied renorrhaphy. Even for the complex and technically challenging renal tumors, robotic assistance is expected to provide patients the benefit of minimally invasive surgery with safety and satisfactory renal function.
Laparoscopic Versus Robotic-Assisted Partial Nephrectomy: Comparison of Perioperative Outcomes in 100 Consecutive Cases by a Single Surgeon.
INTRODUCTION: Laparoscopic (LPN) and robotic-assisted (RPN) partial nephrectomy have emerged as minimally-invasive alternatives for the surgical management of renal malignancies. Few studies have directly compared these two approaches in a large single-surgeon series. PURPOSE: We report our experience with 100 consecutive patients undergoing laparoscopic or robotic-assisted partial nephrectomy. METHODS AND MATERIALS: A retrospective chart review was performed on 100 consecutive patients with suspicious renal lesions undergoing either LPN or RPN from 2005-2010 by a single surgeon. RESULTS: 23 patients (23.7%) underwent LPN and 74 patients (76.3%) underwent RPN. Age, gender, BMI, and pre-operative creatinine were similar across groups. Median pre-operative tumor size was 3.4 cm in the LPN group and 3.0 cm in the RPN group (p>0.05). 20% of lesions in the LPN group were>50% intraparenchymal versus 49.1% the RPN group, and 27% of the lesions in the LPN group were<7 mm from the collecting system, versus 69% in the RPN group. Mean operative time and warm ischemia time were 243.7 minutes and 30.4 minutes in the LPN group and 207.4 minutes and 25.4 minutes in the RPN group, respectively. The positive margin rate was 4.3% for LPN and 2.7% for RPN (p>0.05). No patient developed local recurrence or metastatic disease. CONCLUSIONS: Patients undergoing RPN had more challenging tumors compared to patients undergoing LPN in this series. Despite this, RPN offered equivalent oncologic outcomes to LPN but with less blood loss, shorter operating time, and shorter warm ischemia times.
Enucleation of Renal Masses Versus Standard Wedge Resection During Robotic-Assisted Laparoscopic Partial Nephrectomy
INTRODUCTION: Recent studies have demonstrated the efficacy of simple enucleation for selected T1 renal tumors during open partial nephrectomy. Less is known about the efficacy of enucleation during robotic-assisted laparoscopic surgery. PURPOSE: We compare our experience with enucleation and standard resection of renal masses in patients undergoing robotic-assisted (RPN) partial nephrectomy. METHODS: A retrospective chart review was performed on 74 patients undergoing RPN from 2005-2010 by a single surgeon. RESULTS: Of the 74 patients who underwent RPN, 44 underwent the standard resection, and 30 underwent simple enucleation. Groups were similar in age, sex, BMI, and pre-operative creatinine. Median pre-operative tumor size was identical in both groups (3.1cm). Although average nephrometry score in the enucleation group was higher (7.36 vs 6.40; p=0.033), warm ischemia time (WIT) was shorter (21.9 vs. 28.1 minutes, p=0.003), compared to the standard resection group. Mean operative time, estimated blood loss, and length of hospital stay was similar. There were 2 positive margins in the standard resection group, and none in the enucleation group. Intra-operative complications (including open conversions and conversion to radical nephrectomy) were 13.6% and 3.3% for the standard resection and wedge resection groups, respectively. There were no local recurrences or progression to metastatic disease in either group. CONCLUSIONS: Enucleation appears to be a safe and efficacious technique in the robotic-assisted laparoscopic resection of renal masses, allowing for extirpation of more challenging tumors with shorter operative times and WIT, as well as fewer positive margins, complications, and conversion rates, than traditional wedge resection.
Open Versus Robot-Assisted Partial Nephrectomy: Effect on Clinical Outcome by a Single Surgeon
Introduction and Purpose Robot-assisted partial nephrectomy (RPN) has emerged as a viable alternative to open partial nephrectomy (OPN) for small renal masses (SRMs). Comparative outcomes of RPN and OPN by a single surgeon were analyzed. Materials and MethodsA retrospective review was performed to compare 50 RPNs with 50 OPNs between May 2003 and May 2011. Clinicopathologic variables, operative parameters, and renal functional outcomes were analyzed.ResultsThere were no significant differences between the two cohorts with respect to patient age, sex, preoperative estimated glomerular filtration rate (eGFR), estimated blood loss and tumor size. The mean operative time was longer in the RPN group (192 vs 142 min, P<0.001). The mean warm ischemia time was longer in the RPN cohort (22.99 vs 18.87 min, P<0.001), but there were no significant differences in the postoperative eGFR (P=0.162) and change in the eGFR (P=0.520). The length of hospitalization (6.2 vs 8.9 d, P<0.001) and use of postoperative analgesics (ketoprofen, 0.26 vs 0.88 ampules, P<0.001) were more favorable in the RPN cohort. The intraoperative complication rates were 2.0% and 6.0% in the RPN and OPN groups, respectively (P=0.999). The overall postoperative complication rates were 8.0% and 14.0% in the RPN and OPN groups, respectively (P=0.158). ConclusionsRPN is a viable option as a nephron-sparing surgical procedure for SRMs considering the perioperative parameters and postoperative renal function changes, in addition to the traditional benefits of the laparoscopic procedure.
The Learning Curve for Reducing Warm Ischemic Time of Robot-Assisted Partial Nephrectomy by a Single Surgeon
Introduction and Purpose We investigated the learning curve for performing robot-assisted partial nephrectomy (RPN) based on warm ischemic time (WIT).Materials and MethodsWe reviewed data for 54 consecutive patients who underwent RPN performed by a single experienced surgeon between September 2008 and May 2011. WIT, total operation time, complications, and length of hospitalization according to the surgeon experience were evaluated by linear regression analysis. Associations between learning curve and other operative factors were analyzed by multivariate analyses. ResultsMean size of the resected specimens was 3.82 cm, mean WIT was 21.8 minutes, mean total operation time was 182.9 minutes, and the complication rate was 18.5%. After 20 cases, WIT and the overall complication rate stabilized, and total operation time was reduced after 50 cases. WIT significantly correlated with the resected mass size (p<0.001). In the multivariate analysis, the surgeon experience after 20 cases of RPN significantly lower the probability of WIT>20 minutes (HR=0.129, p=0.010). Tumor size also was a significant factor for predicting WIT but not the tumor location. ConclusionsRPN is safe procedure associated with a short learning curve, and is a viable option for partial nephrectomy in patients with small renal masses.
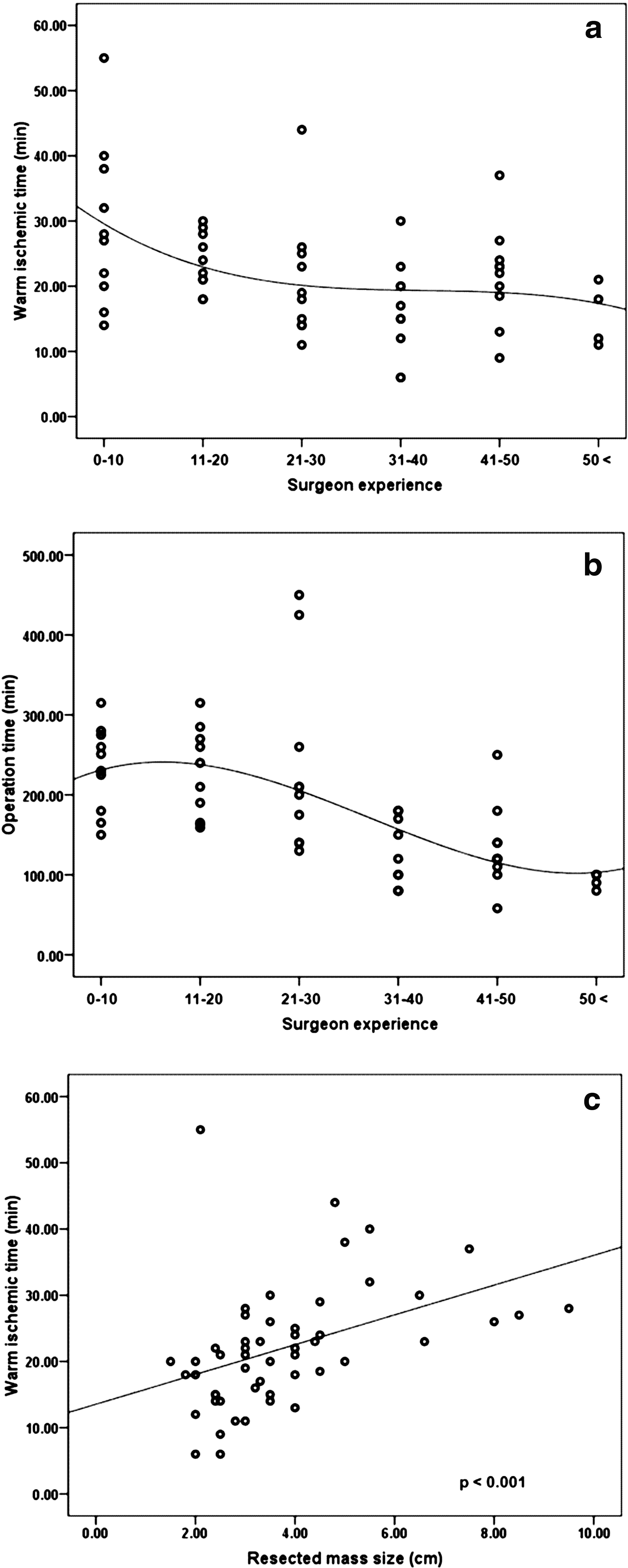
Laparoscopic Partial Nephrectomy for Hilar Tumors
Objective To verify the safety and feasibility of applying laparoscopic partial nephrectomy for hilar tumors. Methods Between January 2007 and January 2011, 5 of 93 patients(5.38%) undergoing LPN for renal tumors had a hilar tumor. We defined hilar tumor as a tumor located in the renal hilum that was demonstrated to be adjacent to renal artery and/or renal vein within 5mm on computerized tomography. Renal artery clamping with cold excision of the tumor, including its delicate mobilization from the renal vessels, followed by sutured renal reconstruction was performed routinely. Results Laparoscopic surgery was successful in all cases without any open conversions or operative re-interventions. Mean tumor size was 29.4(SD8.29)mm. a indication for LPN was imperative in 3 patients because of low GFR of the contralateral kidney. Pelvicaliceal repair was performed in 3(60%) patients, mean warm ischemia time was 26.2(SD7.60) minutes, mean blood loss was 142(SD202.16)ml, mean total operative time was 205.4(SD50.66) minutes and mean hospital stay was 16.2(SD6.76) days. Histopathology confirmed renal cell carcinoma in 3(60%) patients, of whom all had negative margins. One patient suffer from pneumonia after operation. No hemorrhagic complications occurred. No kidney was lost for technical reasons. Conclusion LPN for hilar tumors is feasible and safety for proper selected cases. However, the surgical approach should be handled by experienced laparoscopic surgeons because of difficulties associated with the procedure.
Off Clamp vs. Clamp Robotic Assisted Partial Nephrectomy
Introduction: The benefit of minimizing or eliminating warm ischemia during partial nephrectomy is well established. We report our experience with off-clamp robotic assisted partial nephrectomy (OC-RAPN) to demonstrate the safety of this technique.Materials & Methods: From November.2008 to March.2011, we reviewed all patients that underwent RAPN by a single surgeon(DE). We compared our OC-RAPN peri-operative data with patients that underwent hilar clamping.Results: Of 87 patients undergoing RAPN, 10 had multiple site combined procedures and were excluded. Of the remaining 77 patients, 15 patients underwent OC-RAPN.There was no difference among those that underwent hilar clamping vs. OC-RAPN in mean estimated blood loss (164.7 cc vs. 137.7 cc, p=0.47), length of stay (1.6 d vs. 2.3 d, p=0.43), and margin status (0=negative margin, 1=positive margin) (0.07 vs. 0.11, p=0.76), respectively. There was a difference in mean operative console time (144.3 min [clamp] vs. 99.1 min [off-clamp], p=0.001). OC-RAPN compared to clamped RPN, were performed on smaller tumors (mean 2.4 cm [range: 1.3-3.9cm] vs. mean 3.3 cm [range: 1-11cm]; p=0.02) and more often in exophytic tumors (77% vs. 31%). Pre and post-operative MDRD GFR decreased significantly for clamped RAPNs (77 vs. 67; p=0.04) but was not significant in OC-RAPNs (86 vs 82; p=0.78). 1 patient in the clamped group required a postoperative blood transfusion and no one had a post-operative urinoma.ConclusionsIn our experience, OC-RAPN is a safe technique in smaller and exophytic tumors.
Comparison of Robotic Partial Nephrectomy Experience in Obese and Non-Obese Patients
Introduction: Obesity has been increasing in the US in the last 2 decades at an alarming rate. With the increasing popularity of robot assisted partial nephrectomy (RAPN), we report our experience in non-obese (BMI<30), obese (BMI 30-35) and morbidly obese patients (BMI>35). Materials & Methods: From November 2008 to March 2011, we reviewed all patients that underwent RAPN by a single surgeon(DE), stratifying operative and peri-operative data by BMI. Results: Of 87 patients undergoing RPN, 10 had multiple site combined procedures and were excluded. Of the remaining 77 patients, BMI ranged from 20-63. Distribution of BMI was 52% non-obese, 26% obese and 22% morbidly obese. There was no statistically significant difference in console operative time for non-obese vs. obese patients (119.4 min vs. 143.8 min, p=0.12), but there was a difference among morbidly obese patients compared to non-obese patients. (119.4 min vs. 163.5 min, p=0.03). Median warm ischemia time approached statistically significant difference in non-obese vs. morbidly obese patients (19.3 min. vs. 23.6 min, p=0.06), and was not statistically significant different in non-obese vs. obese patients (19.3 min. vs. 23.6 min, p=0.10). There were no differences in estimated blood loss, length of stay, renal mass size on preoperative imaging, margin status, and pathologic tumor size. Conclusions: As stratified by BMI, morbid obesity is associated with increased console operative times. Other operative parameters were similar in non-obese, obese, and morbidly obese patients.
The Impact of Body Mass Index on Surgical Outcomes of Robotic Partial Nephrectomy
Objectives: Obesity is a major healthcare issue in industrialized countries. Robotic partial nephrectomy (RPN) is gaining ground as a minimally invasive treatment for localized renal tumors. Purpose: To assess the impact of body mass index (BMI) on the surgical outcomes of RPN.Methods: Medical charts of 250 consecutive patients who underwent RPN at our institution from 2006 to 2010 were reviewed. Patients were categorized based on their BMI into 4 groups: normal (BMI<25 kg/m2), overweight (25-29.9), obese (30-39.9) and morbidly obese (40 and above). Preoperative characteristics as well as perioperative and postoperative outcomes were analyzed. Results: Forty three patients (17.2 %) were non obese, 104 (41.6%) overweight, 75 (30%) obese, and 28 (11.2%) morbidly obese. Groups were comparable in terms of age, gender, history of previous surgery, nephrometry score (p=0.5). Patients with higher BMI had a higher ASA score (median 3 for obese and morbidly obese groups versus 2 for non obese groups; p=0.002), tumor size (median 3.6, 2.9, 2.5 and 2.3 cm in morbidly obese, obese, overweight and normal BMI, respectively; p=0.005). Patients with morbidly obese groups had more estimated blood loss (median 250 mls) as compared to other groups (median: 200, 200, 150 mls respectively) (p=0.03). No significant difference was detected between the groups in terms of operative time, warm ischemia time, transfusion rate and postoperative complications.Conclusion: RPN represents an effective treatment modality for renal tumors providing equivalent surgical outcomes even for patients with BMI more than 40.
MP27: Adrenal
Right Laparoscopic Adrenalectomy: Optimized Technique with a Modified Trocar Arrangement and Dynamic Liver Retraction
Objectives: Right Laparoscopic adrenalectomy (LA) is technically more challenging than left LA, because of the anatomical position of the right adrenal gland and vein. We modified the technique for right LA to optimize the procedure, and report the outcomes of 15 transperitoneal LA procedures. Patients and Methods: A total of 14 cases of adrenal mass treated with 15 LA were reviewed retrospectively. For modified right LA, we used a 4-port transperitoneal laparoscopic approach that omitted the subxiphoid trocar (classically used for liver retraction), and instead, an assistant applied continuous, dynamic upward liver retraction in a plane perpendicular to the inferior vena cava (IVC). Left LA was done with conventional technique. Results: 14 patients (4 men, 28.6%) with adrenal mass were included in this study. Mean operative time was 122.5 min (range 60 to 195 min), with no significant difference between left (117.5 min) versus right (126.3 min) LA (p=0.79). Mean operative time was 118.6 min for tumors<5 cm and 126.4 min for tumors>5 cm (p=0.60). Right side LA (n=9) was done without difficulty and with excellent direct exposure of the upper and medial aspect of the adrenal gland and adrenal vein using our modification. Conclusion: Modified right LA with a 4-port approach and dynamic upward liver retraction in a plane perpendicular to IVC resulted in direct exposure of the upper and medial aspect of the adrenal gland and adrenal vein. This approach can be effective in challenging cases when the infrahepatic fossa is poorly exposed.
Recurrence Pattern of Varicoceles After Laparoscopic Varicocelectomy
Introduction: Laparoscopic varicocelectomy (LPV) has been proven effective for treatment of varicoceles, however, the recurrence rate is higher after LPV (5-20%) than after microsurgical inguinal or subinguinal approach (1-2%).Purpose: To identify the recurrence mechanism after laparoscopic LPV by comparing the clinical parameters and operative findings of recurrent varicoceles after LPV and Palomo high ligation.Materials and Methods: Ten infertile men with persistent left varicoceles participated in this study: four recurrences after LPV performed at other institutions (within recent 2 years) and 6 occurred after Palomo (within 15 years). The internal spermatic artery was preserved in 3 LPV cases. Varicocele grade, color Doppler findings and intraoperative varicocele findings (number and diameter of veins) were compared among the patients. Microscopic high inguinal approach was used for redo varicocelectomy.Results: All the recurrences were left sided. All the patients who underwent Palomo had grade 2 varicoceles, whereas 2 patients who underwent LPV had grade 3 varicoceles. Peak retrograde flows were 11.2 and 28.8 cm/s after Palomo and LPV, respectively (p<0.05). Although there were several veins in the spermatic cord after Palomo, the maximum vein diameter (2.4 mm) was smaller than that observed after LPV (4.3 mm) (p<0.05).Conclusions: Our study did not show the incidence of recurrence after LPV; nonetheless, residual spermatic veins are considered to be involved in the recurrence because of the incidence during the short period, massive reflux and large spermatic veins adjacent to the internal spermatic artery. LPV, especially artery-sparing, should be performed to avoid the residual veins.
Extraperitoneal Laparoscopic Retroperitoneal Lymph Node Dissection for Early Stage Testicular Nonseminomatous Germ Cell Tumors
Introduction: Laparoscopic retroperitoneal lymph node dissection(LRLND) for clinical early stage testicular nonseminomatous germ cell tumor(NSGCT) is an accurate pathological staging method. Conventional approach is transperitoneal.
Purpose: To investigate a modified laparoscopic retroperitoneal lymph node dissection technique using an extraperitoneal approach and evaluate its feasibility.
Materials and methods: A cohort of consecutive patients from a single institution who received extraperitoneal RLND weeks after orchiectomy for primary testicular NSGCT.Patients were placed in supine position with 15 degree tilted up in affected side. Four trocars were introduced. The boundaries of dissection included renal vein (proximal), bifurcation of common iliac vessel (distal), ureter (lateral) and para-abdominal aorta/inferior vena cava area (medial).
Results: EL-RLND was successfully performed in 10 patients (Left 3 cases, Right 7 cases). Mean operative time was 165 min. Mean blood loss was 295 ml and without blood transfusion. The complication rate was 20%. An intraoperative complication was injury of the vena cava in one case. Mean postoperative intestinal function recovery time was 2 days. Mean postoperative hospitalization was 5.3days. Normal antegrade ejaculation was preserved in all patients. Pathologic studies revealed positive lymph nodes in 2 cases (20%). No recurrence or distantmetastasis occurred during 4-37 months of follow-up.
Conclusions: EL-RLND is a feasible procedure through improved extroperitoneal approach, which provides minimal invasion and rapid recovery of patients.
Endoscopic Inguinofemoral Lymphadenectomy for Genitourinary Malignancies
Purpose: Inguinofemoral lymphadenectomy is a standard procedure for genitourinary malignancies. Open lymphadenectomy is associated with complication rates exceeding 50%. We present our experience with modified endoscopic inguinofemoral lymphadenectomy (EL).Methods: Patients with palpable and non non-palpable nodes who underwent inguinofemoral lymphadenectomy were identified. OL consisted of classical superficial and deep inguinofemoral lymph node dissection. EL was done using a 3-trocar approach respecting the same boundaries. We apply a reduced CO2-pressure of 5 mmHg. A suction drain was always placed. Operative data and postoperative outcomes were assessed and statistically compared.Results: We performed 54 inguinofemoral lymph node dissections in 38 patients. 22 procedures were completed endoscopically. Follow-up was 55.3 months (1-75). Mean OR-time for OL was 102.5 minutes (38-195) being significantly shorter than for EL (146.3 minutes, 90-186), p<0.001. Both groups are comparable with respect to the number of nodes (OL 7.1, 2-16 vs EL 6.9, 4-13) as well as to the number of affected nodes (OL 1.8 vs EL 1.6). The edema, secondary wound healing occurred extremely rare (1/22) after EL leaving an overall complication rate of 9.1%. Complications appeared in more than half of the OL-cases (56.2%). There were no problems due to CO2-insufflation.Conclusions: OL and EL are reliable for inguinofemoral lymphadenectomy regarding oncological efficacy. EL may be more technically challenging. EL can avoid secondary wound healing and lymphatic stasis. EL is safe with a low complication rate. A reduction of CO2-pressures attributes to the safety profile. Oncological and functional endurance could be documented in an extended follow-up.
Laparoendoscopic Single Site Surgery: Initial Experience with the A Novel Reusable Platform
Purpose:Single-port surgery (S-portal) is increasingly used in urology. Several disposable platforms have been introduced to date. Cost is limiting the widespread use of such devices. We present our experience with the first reusable S-portal -platform.Methods:Between January 2010 and June 2011, we performed S-portal procedures in 42 patients including nephrectomy (n=12), adrenalectomy (n=2), partial nephrectomy (n=2), pyeloplasty (n=2), renal cyst ablation (n=3), pelvic lymphadenectomy (n=15) and others (n=6). Data were prospectively collected in a database. All procedures were performed using a novel reusable single-port device (X-Cone R, Karl-StorzR) with a combination of standard and pre-bent laparoscopic instruments. We obtained peri-operative data as well as analgesia requirements and time to convalescence. Complications were recorded using Clavien grading.Results:Mean age was 54.6 years and BMI was 28.7. Conversion to standard multiport laparoscopy was necessary in 3 and addition of a single 3mm instrument was necessary in 7 cases. There was no conversion to open surgery. Intra- and postoperative complications occurred in 3 and 0 cases, respectively. Mean operative time was 115, 71, and 153 minutes and hospital stay was 4.2, 3.6 and 4.1 days for nephrectomy, pelvic lymphadenectomy, and pyeloplasty.Conclusions:S-portal surgery with a rigid reusable device is feasible for various indications in urology yielding favourable cosmetic and functional results. Meticulous patient selection is pivotal to reduce complications rates. The combination of straight instruments with one pre-bent grasper facilitates handling and shortens the learning curve. Reusable materials help to reduce cost leading to a wider acceptance of S-portal surgery.
Anatomical Retroperitoneal Laparoscopic Adrenalectomy: A Report of 142 Cases
Purpose: Anatomical retroperitoneal laparoscopic adrenalectomy was developed after further study in the anatomy of the abdominal cavity. The main technological characteristic was the utilization of the 3 latent anatomic spaces of pneumoretroperitoneum to free adrenal. This technique has advantages such as clear operation field, less bleeding,less complications. This study retrospectively analyzed 142 cases who received anatomical retroperitoneal laparoscopic adrenalectomy for adrenal disease in the past three years in our hospital. Method :142 patients with adrenal diseases received anatomical retroperitoneal laparoscopic adrenalectomy, including 52 cases with aldosterone-producing adenoma , 22 cases of adrenal nodular hyperplasia, 25 cases of adrenal pheochromocytoma ,10 cases of nonfunctional adenoma and 7 cases of localized adrenal carcinoma, 81 lesions were on the left side and 61 on the right side. All the cases received preoperative imaging and functional examination. Operations were performed under general anesthesia. The patients were lay on the lateral position. The typical 3-ports approach was adopted. Signs of retroperitoneal anatomy should be very clear in mind and the surgery should be performed following anatomical layer.Result:All of 142 cases were operated successfully,the mean operation time was 41 min, the mean food recover time was 1.2 d,the mean movement recover time was 0.8d, and the mean hospital stay was 4.9 d .No severe complications occur and no cases conversed to open surgery.Conclusion: Anatomical retroperitoneal laparoscopic adrenalectomy has several advantages including less bleeding, less complications and rapid recovery. This technique may provide better exposure for the removal of the lesions.
Laparoscopic Simultaneous Bilateral Adrenalectomy: Assessment of Feasibility and Potential Indication
<Introduction> We undertook laparoscopic simultaneous bilateral adrenalectomy (LSBA) for patients with bilateral adrenal disease. <Purpose> The purpose of this study is to review our experience of LSBA and evaluate its safety, surgical outcome, and potential indication of this challenging procedure. <Methods> A total of 21 patients underwent LSBA between 2000 and 2010. We had 4 patients with pure bilateral Cushing's syndrome (CS), 2 with bilateral pheochromocytoma, and one with bilateral metastatic tumor. Eleven patients had unilateral or bilateral aldosterone producing adenoma (APA) in whom CS or subclinical CS were also associated. Three patients had unilateral APA with contralateral non-functioning adenoma. We initiated partial adrenalectomy first with 4 ports. After one gland was excised, the patient was repositioned for removal of the contralateral side. <Results> LSBA was completed for all 21 patients without major comorbidities. The mean operative time was 329.7 min. with estimated blood loss of 94.1 ml. The mean tumor size was 21.8 mm. Among 16 patients receiving adrenal-sparing procedure, nine patients out of 11 discontinued glucocorticoid replacement after 2 years. We experienced no open conversion, no deaths or no adrenal insufficiency in our series. <Conclusions> Since LSBA is less morbid and well tolerated in perioperative/postoperative period, it is a safe and acceptable treatment option for selected patients with bilateral adrenal disease including combined PA and (subclinical) CS.
Adrenal Cysts Our Laparoscopic Experience
Introduction: Cystic lesions of the adrenals are rare with an incidence of 0.06% in autopsies, and the most frequently found are either the endothelial cysts or the pseudocysts. We report our series of patients presenting with adrenal cysts. Materials and Methods: Case records of patients presenting with adrenal cysts were reviewed and analyzed. Age, gender, presenting symptoms, physical examination findings, laboratory investigations, imaging records were all noted and analysed.Results: During the 10 year study period, 14 patients, with a mean age of 41.36±5.57 years were diagnosed to have adrenal cysts. Laparoscopic excision of cyst was done in three and laparoscopic adrenalectomy in the remaining eleven.Conclusions: Adrenal cysts are rare and intervention is indicated whenever they are large (>5 cms), symptomatic, functional and potentially malignant. Laparoscopic management of these cysts in the form of either decortication/excision is safe, effective, minimally invasive, with minimal blood loss and shorter duration of hospitalization.
Brady Urological Institute, Johns Hopkins Hospital
Introduction:Primary laparoscopic RPLND (LRPLND) at our institution is performed with therapeutic intent and technically duplicates the open approach. Controversies associated with LRPLND have included the thoroughness of dissection, high rate of chemotherapy exposure, and potential deleterious effects of pneumoperitoneum. Herein we present our experience with LRPLND for the management of clinical stage I non-seminomatous germ cell tumor.Methods:The Johns Hopkins Minimally Invasive Surgery Database (1995-2010) was queried for stage I NSGCT patients undergoing LRPLND. Demographic, perioperative, pathological, and follow-up information were collected and analyzed. Results:Ninety-one patients underwent extended template LRPLND during the study period. Sixty patients (66%) had lymphovascular invasion and 55 (60%) had>40% embryonal carcinoma. Median EBL was 200cc and mean length of stay was 2.1 days (1-4). Four patients (4.3%) experienced intra-operative complications, and there were 4 open conversions (4.3%). Nine patients (9.8%) experienced postoperative complications. Mean lymph node count was 26.1 (7-72), and 28 patients (31%) had retroperitoneal metastasis. Follow-up was available in 55 patients for mean 43.1 months (12-168). No patient with pN0 disease recurred in the retroperitoneum, and there were 5 systemic relapses in pN0 patients. Of patients with pN1 disease (21), 14 opted for chemotherapy while the remainder (7) opted for surveillance. There were no relapses in either group. Conclusion:LRPLND appears to be a safe, viable, and effective procedure for patients with stage I NSGCT. Lack of retroperitoneal recurrences in pN0-N1 patients supports the oncologic efficacy of this approach. Low morbidity and rapid convalescence compare favorably with open series.
Laparoscopic Adrenalectomy for Large Adrenal Masses: a Safe Surgical Procedure
Introduction: Since the description of Gagner in 1992, laparoscopic adrenalectomy (LA) has become the gold standard for surgical management of adrenal masses, due to its adventages over the traditional open approach, like diminished post operative pain and faster convalescence. However, the role of laparoscopy for large volume masses is still controversial considering technical and oncological factors. The state of the art has established 6 cms. as the dimension related with a malignant condition. Nevertheless, a lot of patients present adrenal tumours over that limit at diagnosis. Purpose: The aim of this study is to compare the technical feasibility, surgical results, and morbidity of LA for adrenal masses of less and over 8 cm. Materials & Methods:Between June 1993 and March 2011, a total of 330 patients underwent a LA at our institution. We prospectively recorded demographic, surgical and post operative data, which were reviewed retrospectively, dividing the population in two groups according to tumor size: Group A : mass<8 cms. Group B: mass equal or over 8 cms. Categorical variables were compared using Chi-square test. Numerical variables were compared using t test.ResultsGroup A is composed by 273 patients. Group B is composed by 55 patients. The mean surgical time, surgical bleeding, hospital stay and tumor size were greater in group B (p<0,05). However, the number of complications (9 and 3 respectively) was not showed statistic significance. ConclusionsLA is a safe and feasible surgical approach for management of large adrenal masses.
Laparoscopic Resection of Large Pheochromocytomas: A Safe, Feasible and Curative Surgical Approach.
Introduction: Despite the reports about that laparoscopic resection for adrenal tumours >6cm is a safe minimally invasive approach, the use of laparoscopy for large pheocromocytomas (PHE) is still controversial and not recommended in tumor size >7cm. Objective: The aim of this study is to compare the technical feasibility, operative results, morbidity, and followup of laparoscopic resection (LR) of PHE of less and over 7 cm. Materials & Methods: Between June 1993 and March 2011, a total of 46 patients underwent a LR for PHE at our institution. We prospectively recorded demographic, surgical and post operative data, dividing the population in two groups according to tumor size: Group A : mass<7 cms. Group B: mass equal or over 7 cms. Statistical analysis was performed by Chi-square test and the t test.Results: Group A is composed by 33 patients. Group B is composed by 13 patients. In group A, the mean surgical time was 77,5 min; the mean tumor size was 4,6 cms; the median of surgical bleeding was 20 cc; the mean hospital stay was 3,1 days; we did not experience complications. In group B, the mean surgical time, surgical bleeding, and tumor size were greater than group A (p<0,05). However, hospital stay and number of complications (1) was not showed statistic significance. No recurrences have been recorded after a mean of 36 months followup.Conclusions: LR is a safe, feasible, cost effective and curative surgical approach for management of large PHE adrenal masses.
Department of Urology, Graduate School of Medicine, Chiba University, Chiba, Japan
Introduction: Primary aldosteronism (PA) is the most common curable cause of secondary hypertension, but, despite resection, many patients continue to require antihypertensive drugs to control their blood pressure even postoperatively. Purpose: The aim of this study was to identify the predictors for complete resolution of hypertension after laparoscopic adrenalectomy. Materials and Methods: Records of 102 Japanese patients who underwent unilateral laparoscopic adrenalectomy for PA between November 1995 and January 2011 were reviewed. Patients were divided into two groups according to whether blood pressure (BP) was normal (<140/90 mmHg) without antihypertensive drugs at 6 months postoperatively. Clinical and biochemical data were evaluated at baseline and after the follow-up of 6 months. Results: BP normalized in 43.1% of the patients. Multivariate logistic regression analysis showed that the patients who had complete resolution of hypertension without need for antihypertensive drugs were significantly more likely to have a higher ratio of a mineralocorticoid receptor antagonist (MRA) to all preoperative antihypertensive drugs (odds ratio [OR], 10.604; P=0.0001), a shorter duration of hypertension (OR, 5.018; P=0.0017), and be female (OR, 4.014; P=0.0081). Additional factors associated with complete resolution of hypertension based on univariate analysis included younger age, lesser body mass index, lesser fasting blood sugar, lesser serum triglyceride, lesser uricemia, greater estimated glomerular filtration rate, and no history of smoking (P<0.05). Conclusions: Complete resolution of hypertension after surgery for PA is independently associated with three major predictors: 0.5 or higher ratio of MRA to all antihypertensive drugs, under 6 years of hypertension and female sex.
Open Conversion of Laparoscopic Adrenalectomy in Shinshu University Hospital
[Introduction]From September 1994 to May 2011, a total of 136 laparoscopic adrenalectomies were performed at Shinshu university hospital. We examined open conversion cases in laparoscopic adrenalectomies.
[Result]8 cases (5.8%) laparoscopic adrenalectomies required open conversion. 3 cases were on the right and 5 were left. 7 cases were transperitoneal approach, 1 was retroperitoneal. 3 cases were Cushing syndrome, 2 were pheochromocytoma, 1 is primary aldosteronism, 2 were the others. The reasons of conversion were high adhesion : 3, bleeding : 3, high intraabdominal fat: 2. In laparoscopic cases, the average age were 51±12, the average Body Mass Index (BMI) was 23.2±3.5, the average operation time was 195±65 minutes, the average resected mass volume was 26±31g and the average blood loss was 45±60g. In conversion cases, age were 59±9, BMI was 25.7±4.4, operation time was 247±87 minutes, mass volume was 34±20g, blood loss was 610±506g.
[Conclusion]We performed safe laparoscopic adrenalectomy in Shinshu university hospital. In conversion cases, average age and blood loss were significantly higher. Average BMI, operation time and resected mass volume showed no significant differences.
Laparoendoscopic Adrenalectomy – Clinical Evaluation of 160 Cases in a Single Institution.
PURPOSE :The purpose of this study was to describe our clinical experience and assess the feasibility and safety of laparoendoscopic surgery in the treatment of benign adrenal tumors.PATIENTS AND METHODS : We retrospectively reviewed the records of patients who underwent laparoendoscopic transperitoneal adrenalectomy (LA) for benign adrenal tumors at our institution from 2001 to 2011. All operations were performed by 2 experienced laparoscopic surgeons. Demographic, perioperative, and pathologic data were collected and clinically verified. We evaluated the effects of perioperative variables on operative time.RESULTS:Mean patient age was 50 years. Pre-operative evaluation revealed 129 functional adrenal tumors (71 primary aldosteronism, 29 pheochromocytomas, 29 Cushing syndrome). Previous operations were performed in 45 (28%) patients. Mean tumor size was 2.6 cm (0.5-9.0 cm), mean operative time was 131 minutes (46-335 minutes), and mean pneumoperitoneal time was 94 minutes (32-230 minutes). No patient required conversion to open surgery or transfusion. Mortality was zero and the two major complications were cardiac infarction and renal infarction in one patient each. Multivariate analysis demonstrated that tumor size>4 cm (p=0.020, HR=2.61) and pheochromocytoma (p=0.034, HR=2.88) were independent risk factors for operative time.CONCLUSIONS: LA for benign adrenal tumor was safely performed. Statistical analysis of perioperative variables revealed that tumor size and pheochromocytoma were factors that significantly prolonged operative time.
Retroperitoneal Laparoscopic Adrenalectomy for Large Adrenal Tumor (8-12cm)
OBJECTIVES: To evaluate the feasibility of retroperitoneal laparoscopic adrenalectomy for large adrenal tumor. METHODS: A total of 16 cases of retroperitoneal laparoscopic adrenalectomy for large adrenal tumor (8-12cm) was performed from Oct 2006 to Apr 2009. In one of the cases the ipsilateral nephrectomy was performed meanwhile as the right renal artery stretched across the adrenal tumor. The entire group studied was comprised of 7 males and 9 females with a mean age 48 years (range 22-65years). The mean tumor size was 10.8cm (range 8-12cm). 6 cases of the tumors were located on the right and 10 cases on the left. We favored the three-port lateral approach and an additional port was required in 5 cases. In the procedure, the dorsal side and ventral side of tumor were first dissected, posteriorly the upper side and lower side, finally the medial side, because blood supply was affluent medially and the lower and medial side of tumor was adjacent to renal artery. Specimen was entrapped with a sac and extracted. RESULTS: All the operations were performed successfully. The mean operative time and estimated blood loss were 95min (range 60-170min) and 118ml (range 50-220ml). The pathology of tumors included 7 cases of adrenocortical adenoma (2 of primary aldosteronism, and 5 of nonfunctional adenoma), 4 cases of pheochromocytoma, 2 cases of ganglioneuroma, 2 cases of adrenal myelolipoma, 1 case of adrenocortical nodular hyperplasia. CONCLUSIONS: Retroperitoneal laparoscopic adrenalectomy for large adrenal tumor (8-12cm) is a minimally invasive and safe procedure for skillful surgeon.
Analysis of 146 Cases of Laparoscopic Adrenalectomies
[Introduction] We report the analysis of 146 cases of laparoscopic adrenalectomies in Shinshu University Hospital. [Results] The average age was 52 years old (male 41, female 105). The average Body Mass Index (BMI) was 23.3. The average operation time was 200 minutes, the average resected mass volume was 26g and the average blood loss was 102g. In 49 Cushing syndrome, BMI was 24.4, operation time was 209 minutes, resected mass volume was 25g and the blood loss was 131g. In 66 primary aldosteronism, that was 22.8, 197 minutes, 19.1g, 48g. In 22 pheochromocytoma, that was 22.3, 176 minutes, 49.1g, 114.5g. In 97 left side tumors, that was 23.1, 202 minutes, 18g, 112g. In 49 right side tumors, that was 23.5, 190 minutes, 32g, 96g. The open conversion from laparoscopic surgeries was 8 cases (high liver adhesion: 2 cases, high obesity: 2 cases, previous operation adhesion: 1 case, high bleeding: 3 cases). [Summary] In Cushing syndrome, because of the high BMI, we took longer operation time and higher bleeding volume. In pheochromocytoma, even if the larger resected mass volume, the operation time and blood loss were small. We might select the suitable cases for laparoscopic surgeries.
MP28: Robotic/Lap Prostate 4
Prostate-Specific Antigen Screening in Patients with End-Stage Renal Disease
Introduction: Patients who are being evaluated for renal transplant (RT) must have non-cutaneous malignancy excluded in order to be eligible for RT. There is no agreed upon PSA cut point to prompt prostate biopsy (PB) in this patient population.
Purpose: To evaluate PSA cut points and prostate cancer (PC) detection in patients with end-stage renal disease (ESRD) awaiting RT.
Materials and Methods: A retrospective review was conducted of 820 patients at a single institution who are or have been on the RT waiting list who also had a serum PSA measurement. PSA levels were stratified by age to determine a 95th percentile reference range for each age decade.
Results: The serum PSA 95th percentile reference ranges for patients with ESRD were 0.0-2.1 ng/mL for 40-49 years, 0-3.5 ng/mL for 50-59 years, and 0-4.7 ng/mL at 60-69 years. In patients with PSA >=4 ng/mL (n=53), PB detected PC in 41.5% of the patients, with an additional 5.8% of patients having pre-malignant changes. For patients with PSA between 2.5 and 4 ng/mL (n=26), the PC detection rate was 42.3%, with an additional 12% of patients having pre-malignant changes. Overall, PB for PSA>2.5 showed PC in 41.8% of patients and pre-malignant lesions in 7.7%.
Conclusions: ESRD patients had higher age-specific PSA levels than those with normal renal function. A PSA cutoff of 2.5 resulted in an elevated PC detection rate in patients with ESRD, compared to historical controls. These findings should be considered when implementing biopsy protocols for patients with ESRD.
Impact of Total and Free Testosterone on Physiological Characteristics of Men and Aggressiveness of Prostate Cancer in Men Undergoing RARP
Objective: Recovery from RARP varies widely among men and has been linked to age, BMI and other health related factors. We present longitudinal data of Total Testosterone (TT) and calculated Free Testosterone (FT) in men undergoing RARP for correlation with physiological characteristics and cancer aggressiveness. Methods: Prospective preoperative TT and FT data was entered into a data base for men undergoing RARP (N=149). Parameters included age, AUAss, IIEF-5, BMI, prostate weight, GS, stage, SM.Results: TT and FT decrease with age, however more so for FT. Table 1 presents pertinent findings based on FT levels. Low FT/TT correlates with a variety of physiologic characteristics including: higher body weight, BMI, higher prostate weight and lower Hgb. Separately, low FT and TT are associated with oncological factors including primary Gleason>4 (p=0.002), an increased risk of high grade cancer Gl. 4+3, 8-10 vs Gl. 3+4, 0-6 (p<0.003) and also a higher risk of + SM 23.5% vs 8.6% (p<0.11).Conclusions: As serum levels of TT/FT stepwise decline so do a variety of general physiologic/health characteristics which impact RARP clinical outcomes. With TT<350 we found a significant association with primary Gleason score 4, high grade cancer, higher volume cancer and + SMs.
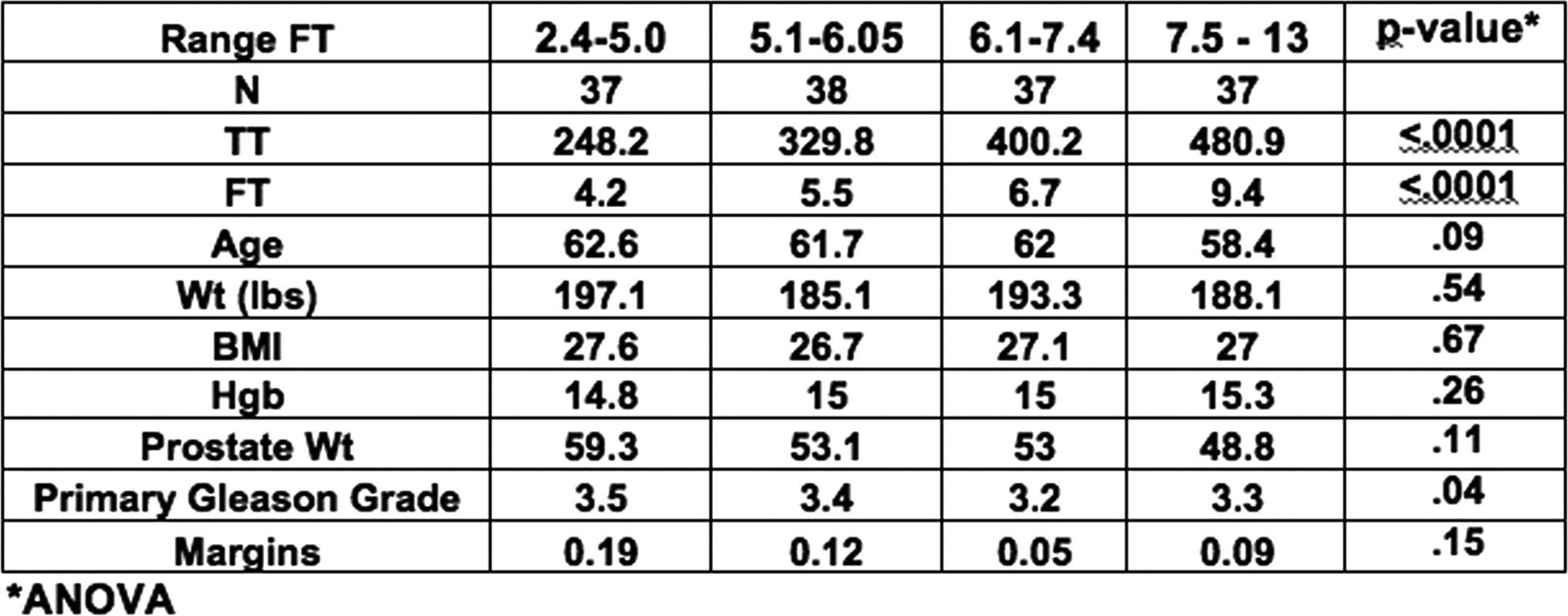
Results of Carbon Dioxide Laser Used for Bladder Neck-Sparing Robotic Assisted Radical Prostatectomy
OBJECTIVE:Robot Assisted Radical Prostatectomy (RARP) has become the preferred method to treat surgically patients with prostate cancer. Carbon dioxide (CO2) lasers have been proposed as a method to deliver energy with minimal thermal spread. The use of the CO2 laser during neurovascular bundle dissection (NVD) has been proposed to improve functional outcomes with regard to sexual potency after RARP. We utilized a CO2 laser during dissection of bladder neck to assess continence outcomes.MATERIALS:The CO2 laser fiber (OmniGuide BeamPath URO-LG CO(2) laser) was used for the bladder neck dissection on 14 selected patients with low (8 Pts) and intermediate risk (6Pts) prostate cancer during RARP. 28 patients with a standard bladder neck dissection with electrocautery were used as a comparative group on terms of functional outcomes. Bilateral interfascial nerve sparing was performed on all patients. Follow-up was done at 12 months to evaluate erectile dysfunction and incontinence. RESULTS:Estimated blood loss (EBL) was similar between the CO2 Laser and standard groups (125 ml vs. 100 ml respectively). At 1 year follow up no biochemical recurrence was reported (PSA<0.1). Total continence at the 3 month and 1 year was 42.8% and 78.5% (CO2 Laser) vs. 50% and 86% (Standard group). Additionally, 71.4% vs. 82.1% (CO2 laser vs. Standard respectively) were able to have intercourse at one year.CONCLUSIONS:The CO2 laser,s ability to deliver lower thermal spread does not appear to translate to improved continence outcomes.
Nerve Sparing is a Graded Rather than an All-or-None Phenomenon: Demonstration by Assessment of Nerve Tissue on Surgery Specimens
Objective: To demonstrate the existence of different degrees of nerve sparing (NS) (graded NS) by comparing our NS grading system with residual nerve tissue on prostatectomy specimens. Methods: 133 consecutive patients who underwent RALP between January and February 2011 included. NS was classified by the surgeon independently for either side in a score from 1 to 5 as follows: 1=non NS, 2=<50% preservation, 3=50%, 4=75% preservation and 5=complete nerve sparing. A pathologist then measured the area of residual nerve tissue in the posterolateral surface of the apex, mid prostate and base at either side. Mean age±SD was 60±8 years, median(IQR) BMI, SHIM score, AUA symptom score, PSA and prostate volume were 28(5), 20(13), 7(11), 5.2(2.8) ng/ml and 48(22) ml, respectively. There was a significant difference in the area of residual nerve tissue as function of the NS score (p<0.001) (Table 1). Conclusions: Higher intent of NS resulted in significantly less area of residual neural tissue present in the final specimen. Small changes in NS scores were associated with significant difference in the area of residual neural tissue especially for the higher levels of nerve preservation, reflecting that nerve sparing is a graded rather than an all-or-none phenomenon.
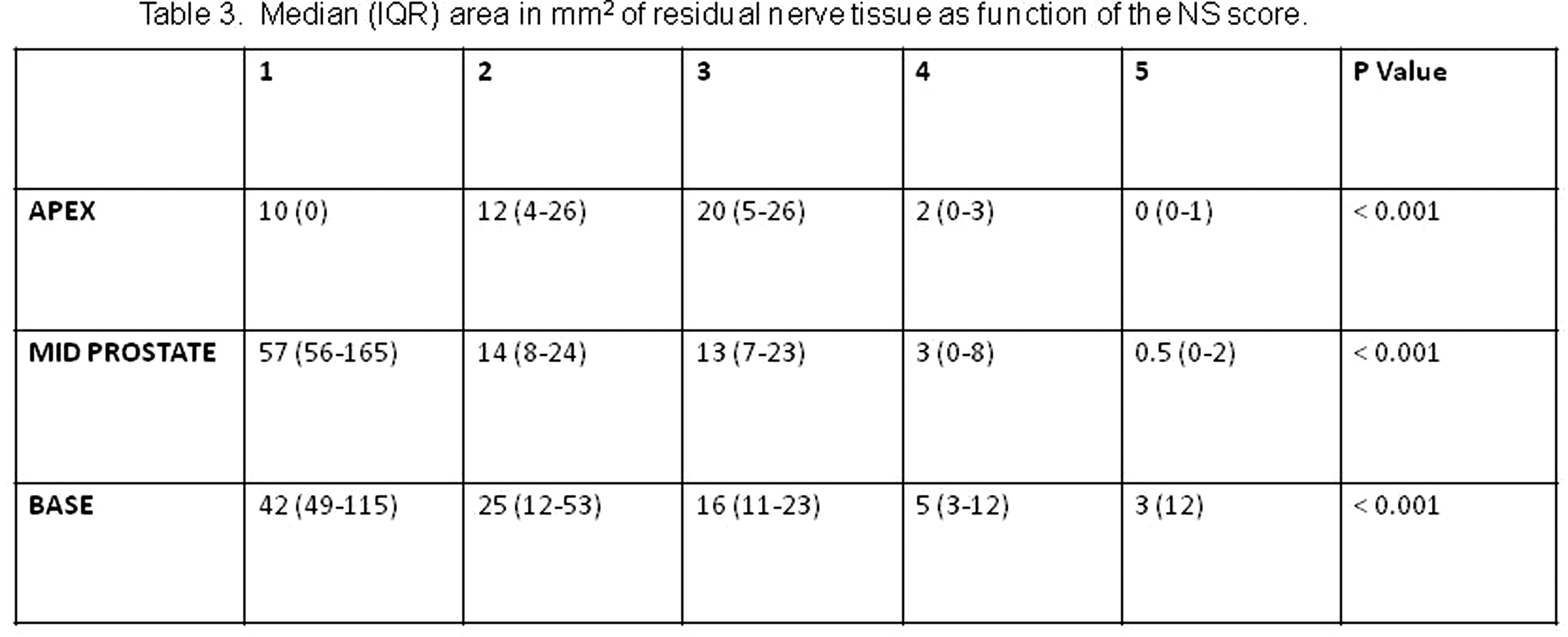
Predictors of Complete Nerve Sparing During Robot Assisted Radical Prostatectomy
Objective: To identify the variables involved in complete nerve preservation at the time of radical prostatectomy. Methods: The area of neural tissue at the posterolateral aspect of the prostate was measured in pathology slides of 124 consecutive patients who underwent RALP. Complete nerve sparing (NS) was defined as the absence of neural tissue on the specimen. Univariate and multivariate logistic regression analysis was performed to assess for potential predictive factors associated with achievement of complete NS. Area and predictors were independently assessed and analyzed for each side. Statistical significance was set at p<0.05.Results: Mean age±SD was 60±8 years, median (IQR) BMI, SHIM score, PSA and prostate volume were 28(5), 20(13), 5.2(2.8) ng/ml and 48(22) cc, respectively. See Table 1.Conclusion: Decreasing percentage of tumor and performance of a retrograde nerve sparing were independent predictors for achievement of complete nerve sparing. Interestingly, increased difficulty during the NS was not a predictive factor in our series, probably reflecting the maturity of our surgical technique.

Proposal of a Method to Assess and Report the Extent of Residual Nerve Tissue Present on Radical Prostatectomy Specimens.
Introduction:Radical prostatectomy specimens harbor a variable amount of extraprostatic neural tissue, however this is usually not mentioned during pathology reports. The amount of extracapsular neural tissue is an objective assessment of the amount of nerve sparing performed during surgery and could have an impact in recovery of erectile function. We propose a method to report the amount of nerve tissue present on radical prostatectomy.Materials and Methods: The data of 133 consecutive patients who underwent robot assisted radical prostatectomy by a single surgeon (VRP) were prospectively collected. Degree of nerve sparing was intraoperatively graded by the surgeon independently at either side as complete, partial or none. A pathologist who was blinded to the surgeon's classification measured the following parameters at the posteroaleteral aspect of the apex, base and mid prostate at either side of the specimen: length, width and area of neural tissue, number of nerves per high power field and number of total slides containing neural tissue. Measurements were correlated to the surgeon's intraoperative perception.Results: see tableConclusion: Area of nerve tissue showed the highest correlation with surgeon's intent of nerve sparing. We propose that this parameter should be included into the standard reporting of radical prostatectomy specimens.
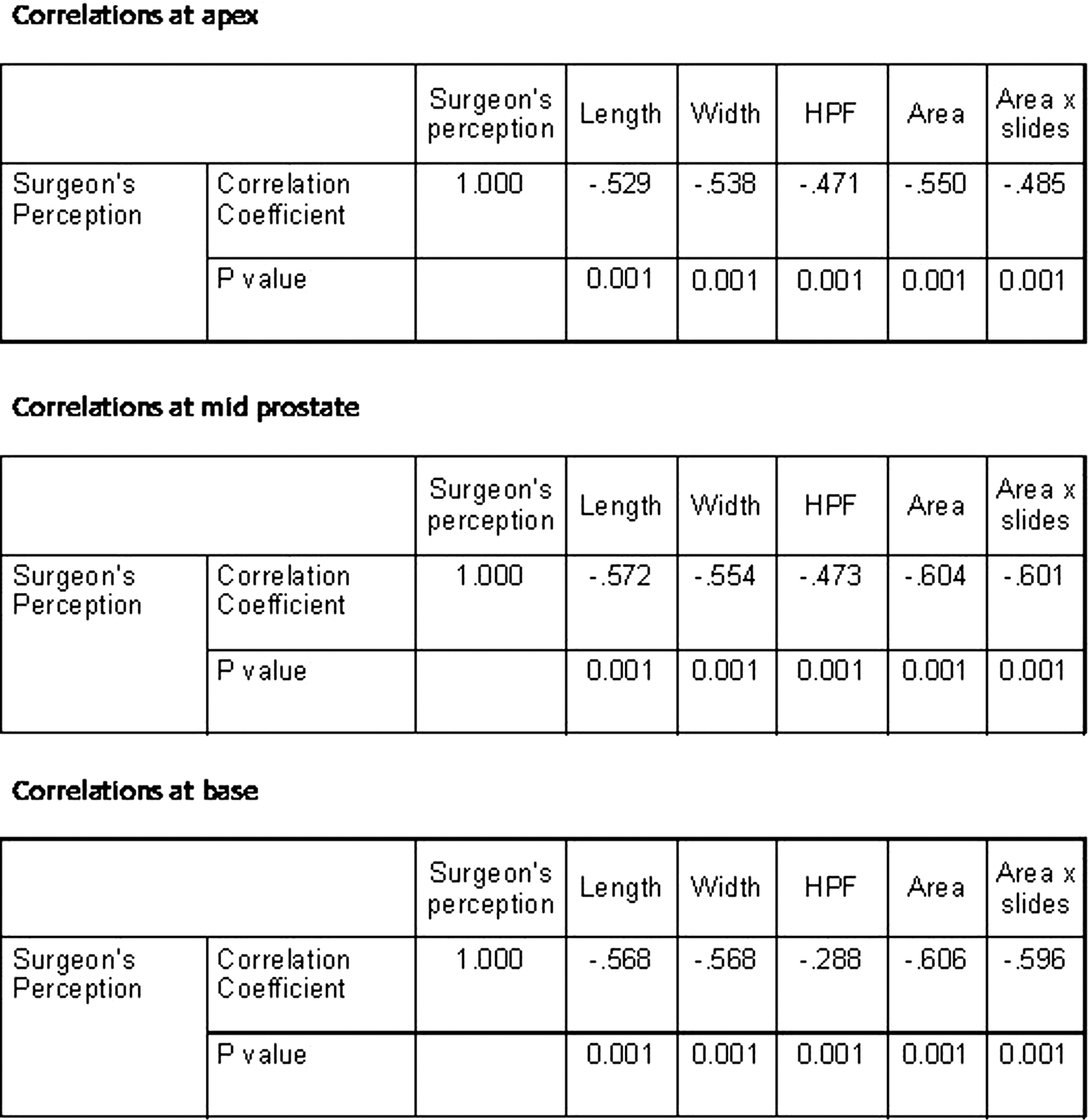
Dean and Betty Gallo Prostate Cancer Center and Section of Urologic Oncology, The Cancer Institute of New Jersey, Robert Wood Johnson Medical School, New Brunswick, NJ, USA
Introduction: The precise incidence of erectile dysfunction (ED) following radical prostatectomy (RP) is difficult to determine.Purpose: In the present study, we have attempted to determine the rate of erectile dysfunction following RP by comparing the pre- and post-operative sexual health inventory for men (SHIM).Materials and Methods: We retrospectively reviewed the charts of 503 patients who underwent Robot-Assisted RP over a 5-year period. Of these men, there were 206 who had bilateral nerves spared and SHIM scores recorded pre-operatively and at 12 month after surgery. Postoperative potency was defined as both Q2 and Q3 of SHIM score of 4 or 5. Results: There was 36.9% (76/206) who has continued PDE5 inhibitor 12 month after RP. Based on the pre-operative SHIM score, patients were divided into 4 categories; normal (SHIM>21), mild (SHIM 17-21), moderate (SHIM 12-16), and sever (SHIM<12). Overall, the average pre-operative SHIM score was 20.7 and 18.0 post-operatively (p<0.001). Conclusions: As a result, we find out potent does not mean no ED on SHIM and total SHIM score is significantly affected by the score (4 or 5) of Q2/Q3 of SHIM and Q18 of EPIC. We suggest that the discrepancy of total SHIM is caused by the difference of total scoreaccording to each question score of SHIM and EPIC as well as score 5 (always or whenever) of brief questionscould be more proper as a cut-off point for the accordance with total SHIM score than score 4 (more than half).
Department of Urology, Hackensack University Medical Center, Hackensack, NJ, USA
Introduction:Patients with larger prostates may pose increased technical challenges during robotic surgery despite having better visualization and magnification. Since very few studies have assessed the effects of prostate size on robotic surgery, we evaluated the impact of prostate weight on robot-assisted laparoscopic radical prostatectomy (RALP) functional outcomes. Purpose:To evaluate the influence of prostate gland size on perioperative, pathologic and erectile function outcomes after RALP. Methods:A retrospective review of 158 patients, who underwent RALP from June 2008 to June 2010 was performed. Data was collected on patient and tumor characteristics, oncological and erectile function outcomes. Postoperative potency was assessed by asking questions based on the Erection Hardness Score. Patients with prostates of<68 g or>68 g were compared. Results:Patients with larger prostates were significantly older (62 vs. 59 y, p<0.03), had higher preoperative PSA levels (5.4 vs. 4.9 ng/ml, p<0.04), had longer overall operative times (195 vs. 165 min, p<0.01) and lower pathological Gleason score (6 vs. 7, p<0.05) than patients with smaller glands. No significant differences were observed in intraoperative blood loss, laparoscopic operative time, preoperative Sexual Health Inventory for Men score, neurovascular bundle preservation, margin status, clinical stage and pathological stage. There was a trend for more patients with smaller glands to have "erections sufficient for penetration" compared to patients with larger glands (p=0.079). Conclusions:Outcomes for RALP in patients with larger prostates are favorable in terms of cancer control despite higher preoperative PSA levels. However, recovery of postoperative erectile function can be delayed in men with larger prostates.
Department of Urology, Heartlands Hospital, Heart of England NHS Foundation Trust, Birmingham, West Midlands, UK.
Introduction: The main concern of conducting Laparoscopic Radical Prostatectomy(LRP) includes achieving the trifecta of oncological control,continence preservation and maintenance of potency. With respect to potency preservation, athermia and tension free dissection with minimal disruption of the neurovascular bundle is cited by many as a main facet. In a previous study in the cadaver, the concept of planar dissection of periprostatic tissue by instillation of fluid with the potential for preservation of the neurovascular bundles (NVB) was demonstrated (Kommu et al. Journal of Endourology.WCE 2009). Purpose: To test the technique of Transrectal Ultrasound (TRUS) Doppler aided perabdomial interfascial instillation of planar fluid for nerve sparing laparoscopic radical prostatectomy. Method: The technique involved real-time TRUS Doppler imaging of the periprostatic tissue with focus on the neurovasular bundles. The surgeon used conventional laparoscopic ports. Real-time dissection was achieved by serial pneumatic dilation of tissue planes with simultaneous instillation of water via a specially devised needle inserted via one of the ports. Five patients were tested. Result: All five men had a demonstrable lift (wheal of separation) of the NVB (mean=6mm;range 3.5 to 7.2) of the 10 sites done. Histopathological analysis of specimens revealed no evidence of NVB or tumour at margins at micro or macroscopic level. All five men remained potent with negative margins . At a mean of 18 months follow up, there was no evidence of biochemical recurrence. Conclusion: TRUS Doppler aided interfascial instillation of planar fluid allows tension free dissection and preservation of the neurovascular bundles during LRP.
Relationship Between Recovery of Urinary Continence After Laparoscopic Radical Prostatectomy and Preoperative Membranous Urethral Length
Objective To assess whether recovery of urinary continence after laparoscopic radical prostatectomy is associated with membranous urethral length on preoperative magnetic resonance imaging. Methods 86 cases with pathologic confirmed prostate carcinoma were performed laparoscopic by a signal surgeon. Patients were categorized into two groups according to membranous urethral length(MUL) on preoperative magnetic resonance imaging(Group A and B), and MUL was measured on coronal images as the distance from the prostatic apex to the entry of the urethra into the penile bulb. After surgery we recorded and analyzed recovery of urinary continence of patients at least one year. Results In the 86 patients who underwent MRI preoperatively mean membranous urethral length was 14.8(10.2∼24.3)mm. Three months after surgery, group A had 79.2% and group B had 47.4% were completely continent (p=0.016). Six months after surgery continence rate was 87.5% and 71.1%, one year was 93.8% and 89.5% for group A and B separately. There was a significant difference between group A and group B in the urinary continence curve (p=0.039). Conclusion Shorter membranous urethra lengths is associated with significantly more slow return of urinary continence, especially for early recovery (3 months) of continence after laparoscopic radical prostatectomy.
Urinary Continence After Laparoscopic Radical Prostatectomy : Association with Urethral Length Measured by Real-Time Intraoperative Transrectal Ultrasonography
Background : Urinary incontinence after radical prostatectomy is one of the major complications. The authors assessed the relationship between urinary continence after laparoscopic radical prostatectomy and various factors including membranous urethral length examined by real-time intraoperative ultrasonography.Patients and Methods : Between 2009 and 2011, 120 patients with localized prostate cancer underwent laparoscopic radical prostatectomy with real-time intraoperative ultrasonography. Membranous urethral length just before and after operation, prostate size and postoperative urethra-bladder angle were measured by real-time intraoperative ultrasonography.Results : Fifty-three patients were evaluated for urinary continence for more than 6 months. Four, 15 and 27 patients regained continence 1, 3 and 6 months after laparoscopic radical prostatectomy, respectively. Longer postoperative urethral length was associated with recovery of urinary continence 1, 3 and 6 months after radical prostatectomy. In addition, the more difference between preoperative and postoperative urethral length was also correlated with superior continence. Shorter operation time and less blood loss resulted in postoperative urinary continence 1 month after surgery. Larger prostate volume was related to postoperative continence 6 months after surgery. Age, urethra-bladder angle and preoperative urethral length had no correlation with urinary continence.Conclusions : Postoperative membranous urethral length was an important factor for recovery of urinary continence after laparoscopic radical prostatectomy. Therefore, preservation of urethra during surgery may be recommended.
Urinary Status After Laparoscopic Radical Prostatectomy
INTRODUCTION AND OBJECTIVES: Post-prostatectomy urinary incontinence is a major cause of morbidity from radical prostatectomy. We evaluate urinary continence after laparoscopic radical prostatectomy(LRP) at our institution.
METHODS: 279 patients underwent LRP at our institution from Jan 2007 to June 2011 at our institution and were followed up in terms of regular PSA checks.
RESULTS: Continence is defined as use of 0-1 urinary pads. 207 patients had achieved continence. At one month after prostatectomy, the continence rate was 9.8%. After three months, the ratio was 42.8 and one year was 83%.
CONCLUSIONS: A lot of factors of achieving urnary continence after prostatectomy are proposed. We propose our technical efforts of laparoscopic prostatectomy and compared other techniches.
Comparative Study of Quality of Life in Patients Who Underwent Minimum Incision Endoscopic or Laparoscopic Radical Prostatectomy
(Purpose) To investigate quality of life in patients with prostate cancer following minimum incision endoscopic (MIES-RRP) or laparoscopic radical prostatectomy (LRP) for more than one year.(Patients and Methods) This study included a consecutive series of 68 patient. General health-related and disease-specific quality of life (HRQOL) was assessed by SF-8 and EPIC, respectively. Pre- and post-operative QOL scores were compared according to surgical procedures, respectively.(Results)MIES-RRP and LRP were performed for 37 and 31 patients, respectively. There were no statistically different clinicopathological and peri-operative factors among MIES-RRP and LRP groups except intra-operative blood loss. HRQOL of all 8 components did not significantly differed between pre- and post-operative status as well as MIES-RRP and LRP groups. Among all components of disease-specific QOL assessed by EPIC, post-operative scores in sexual function, voiding function and urinary incontinence were significantly lower than those of pre-operative scores. However, there was no statistically difference in all components between MIES-RRP and LRP groups. Post-operative urinary incontinence and sexual bother were significantly associated with less satisfaction rating for definitive operation, although satisfaction rating did not significantly differed between MIES-RRP and LRP groups.(Conclusions)Post-operative HRQOL and disease-specific QOL in patients who underwent LRP was equivalent when compared with those in patients underwent MIES-RRP. It appears that post-operative urinary incontinence and sexual bother were important factors which may affect satisfaction rating for definitive operation.
Reporting Complications in Over 1500 Extraperitoneal Robot Assisted Radical Prostatectomy (E-RARP) Cases Using the Standardized Martin Criteria.
Introduction: In 2002, 10 Martin criteria were proposed that should be met when reporting complications following surgery. To date, few studies have evaluated complication rates after robot assisted radical prostatectomy using these criteria. Therefore, we assessed complications in a single surgeon series of E-RARP using this standardized reporting methodology.Materials and methods: Complications in 1503 consecutive patients who underwent E-RARP by a single surgeon between July 2003 and April 2010 were identified retrospectively. All 10 Martin criteria for a high quality report of complications were fulfilled. Results: 152 complications in 127 patients (10.11 %) were detected at a mean follow-up of 47.4 days. The majority of complications were of Clavien grade 2 (41.45%). The incidence of lymphocele formation was 1.46% occurring in 22 (14.47%) cases. Mean hospital stay was 1.12 days. Predictors of any complications in bivariable analysis were operative time (p=0.002) and previous appendectomy (p=0.007). Predictors of major complications were operative time (p=0.001) and case order (p=0.005). These associations remained statistically significant in multivariable analysis. Relevant data is summarized in table 1.Conclusions: Our data confirms that E-RARP is a safe and equal alternative to the classical approach whilst eliminating the potential complications associated with accessing the abdominal cavity.
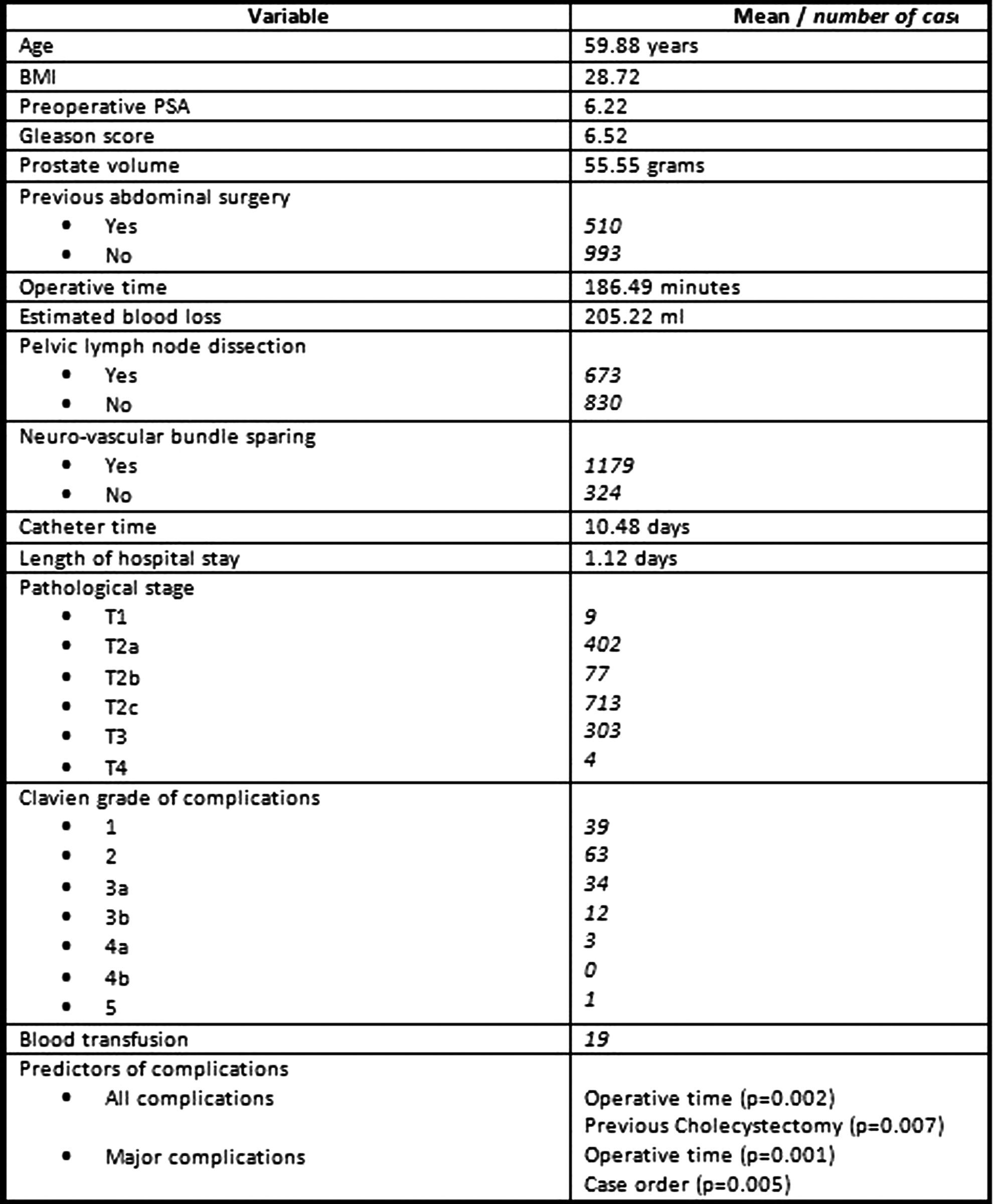
Urology Department, University Hospital of Tours, Tours, France
Introduction: Urinary incontinence remains a major concern for patients after robotic-assisted laparoscopic prostatectomy (RALP). Several technical modifications have been described to improve continence, with inconsistent results. Most widely spread techniques are anterior suspension (AS) of puboprostatic ligaments and posterior reconstruction (PR) of the rhabdomyosphincter.Purpose: To assess the impact on urinary continence of AS combined with PR during RALP.Materials and Methods: Between July 2009 and July 2010, 72 patients were prospectively randomized into two groups: Group A had AS associated with PR during RALP, and Group B underwent standard RALP procedure.AS consisted of a suture passed between the urethra and the dorsal veinous complex, then through the periostium of the pubic bone, twice. PR consisted of a three-point running suture between Denonvilliers fascia at the posterior face of the bladder and the rhabdosphincter tissue beneath the urethra.Continence was assessed using the UCLA-PCI questionnaire at 15 days, one, three and six months postoperatively. Other outcome measures were operative time, blood loss, length of hospital stay, complications and positive margin rate.Results: Continence rates at 15 days, one, three and six months postoperatively were 5.9%, 26.5%, 45.2% and 65.4%, respectively in group A, and 3.6%, 7.1%, 15.4% and 57.9% in group B, with a statistical difference at one and three months (p=0.047 and p=0.016 respectively). No difference was found regarding complications (p=0.8) or positive margin rate (p=0.46).Conclusion: Anterior suspension combined with posterior reconstruction during RALP improved early return of continence, without increasing complications.
Department of Urology, Okayama University Graduate School of Medicine, Okayama, Japan
Introduction and Purpose: Urinary incontinence is one of the major prostate cancer treatment-related morbidities. We review our initial RALP experience, focusing on post surgery continence rates.
Materials and Methods: A bladder neck sparing dissection was preferentially performed during transperitoneal RALP. The urethrovesical anastomosis was completed using a running double-armed 3-0 Monocryl suture±bladder neck tailoring when appropriate. On POD 5 or 6 (clinic logistics), the urethral catheter was removed following normal cystography.
Results: 233 consecutive patients were identified, having a mean age of 61.9±8.4 years and PSA of 6.0±4.5 ng/mL. Mean operating room time was 202.6±56.4 minutes and estimated blood loss was 101.0±147.5 mL. 4 (1.7%) patients had bladder neck reconstruction, while 195 (83.7%) had bilateral, 20 (8.6%) had unilateral and 18 (7.7%) did not undergo nerve sparing prostatectomy. 2 (0.8%) pTx, 34 (14.6%) pT2a, 13 (5.6%) pT2b, 144 (61.8%) pT2c and 40 (17.2%) pT3 cancers were reported, having a mean prostate volume of 44.8±12.7 mL. Mean hospitalization was 1.2±0.9 days and median urethral catheter duration was 5.0±3.5 days. At 6 weeks, a mean 1.3±1.4 per day pad usage was reported. Of the 146 patients having a minimum 12 month follow-up, 136/146 (93.2%) achieved urinary continence without pads within 12 months, with a mean time to continence of 10.8±8.7 weeks.
Conclusions: Our results suggest that a bladder neck sparing dissection in combination with a running 3-0 monocryl vesicourethral anastomosis allows for early return of urinary continence following RALP.
Real-Time Pelvic Sphincterial Electromyographic Monitoring During Laparoscopic Radical Prostatectomy: Initial Experience of 30 cases.
Real-time Pelvic Sphincterial Electromyographic Monitoring during Laparoscopic Radical Prostatectomy: Initial experience of 30 cases.Gao Xin, Si-tu Jie, Pang Jun, Hu Cheng, Huang Wentao, Wen Xinqiao, Zheng Junming Department of Urology, 3rd Hospital of Sun Yat-Sen University, Guangzhou, China,510630[ABSTRACT]Introduction The protection of neurovascular bundle during laparoscopic radical prostatectomy plays an important role on the maintance of urinary continence and erectile function postoperatively.OBJECTIVE To assess the significance and clinic value of monitoring the peri-prostatic nerve during laparoscopic radical prostatectomy by real-time pelvic sphincterial electromyographic monitoring.METHODS 30 patients diagnosed as prostate cancer(T1b-T2c) received laparoscopic radical prostatectomy under general anesthesia. Two active probes were inserted in the anal sphincter and femoral internus respectively, the negative probe was inserted in the upper arm. NIM-ResponseTM electromyographic (EMG) monitor system was used for assistant of dissection, explosion and protection of the peri-prostatic nerve during the surgical procedure. The existence of nerve was proved and protected on the bladder neck, periprostate and periurethra. urinary continence was assessed on the 30th, 60th and 90th day postoperatively.RESULTS The operation completed successfully, the urinary continence rate reached 80%(24/30), 90%(27/30) and 96%(29/30) on the 30th, 60th and 90th day after the surgery respectively contribute to the real-time pelvic sphincterial electromyographic monitoring.CONCLUSION The anatomy and functional distribution of peri-prostatic nerve is observed by the combination of laparoscopic radical prostatectomy and real-time pelvic sphincterial electromyographic monitor, which would improve urinary continence postoperatively.
Preliminary Clinical Experience of Photodynamic Diagnosis for the Detection of Positive Surgical Margins During Radical Prostatectomy
IntroductionPositive surgical margins in prostate cancer lead to a unfavable outcome to life prognosis. 5-aminolevulinic acid (ALA)-mediated photodynamic diagnosis (PDD) is widespread use in bladder cancer. Therefore we investigated the feasibility of intraoperative photodynamic diagnosis using 5-ALA in prostate cancer.MethodAll patients were diagnosed as prostate cancer by biopsy. They had the positive core in apex or highly suspicious positive margin estimated by Japan PC table. Radical prostatectomy was performed to those patients(Open:18 cases, Laparoscopic:2cases). Three hour prior to observation, 1g 5-ALA dissolve in 50ml of 5% glucose solution was given orally though levin tube. Intraoperative PDD was performed using the laparoscope and PDD system(KARL STORZ Endoscopy Japan K.K., Tokyo). The laparoscope was positioned in front of the margins(urethral side, bladder side and rectal side). Red fluorescent area was resected in surgical margins. Harvested prostate was sectioned and also examined by PDD. Red fluorescent-positive and fluorescent-negative areas were biopsied and compared with pathological result.ResultIn all 20 cases, we had no red fluorescent-positive margins and no pathological-positive margins. But one patient had red fluorescent-positive margin of harvested prostate in capsule and histologically comfirmed extraprostatic extention. In the section of harvested prostate, we obtained 75 biopsied samples. The fluorescent positives were 19 samples and pathological positives were 13 samples. The sensitivity and specificity were 76.9% and 85.5%. One case had transient nausea as adverse events and all procedures were tolerated by all patients.ConclusionIntraoperative photodynamic diagnosis is feasible for the detection of surgical margins in prostate cancer.
MP29: Ureter/Urothelial Cancer
Vancouver General Hospital, University of British Columbia, Vancouver, Canada
Introduction and ObjectiveConventional ureteral stents are prone to irritation, encrustation and infection. A novel stent, engineered from absorbable suture material degrades in a retrograde fashion and may reduce morbidity while maintaining urinary drainage. This study evaluated the degradation time, physiologic and histologic responses elicited by a third generation ureteral stent in a porcine model.MethodsIn 16 female Yorkshire pigs, 10 biodegradable (Poly-Med Inc, Anderson, SC) and 6 biostable (Polaris, Boston Scientific) stents were inserted unilaterally cystsoscopically. Intravenous pyleograms (IVPs), blood and urine tests were performed on Days 0, 7, 10, 14, 17, 24 and 28. Biostable stents were removed on Day 21. On Day 28, all animals were necropsied for microscopic and histologic evaluation.Results9/10 Uriprene stents degraded completely by 4 weeks; one animal had three small (<1.5cm) fragments in the bladder. IVPs showed equivalent drainage and significantly less hydronephrosis in degradable-stented kidneys. Blood and urine parameters were equal between biostable and degradable stented animals; however, a transient increase in serum creatinine on day 7 in 40% of the degradable stented animals resolved by day 10. There was significantly less bullous edema and bladder mucosal irritation in the degradable stent group. ConclusionsThis study demonstrates the safety and effectiveness of this degradable stent in a porcine model. The stent degraded in retrograde fashion without distal ureteral obstruction and provided equivalent drainage to the biostable-stented group.
Comparison of Unimodal and Multimodal Approaches for Entombed Stents
Introduction: Entombed stents represent a complex management problem in endourologic patients. Based on stone and patient characteristics, surgeons may select either a unimodal or multimodal approach.
Purpose: To compare unimodal and multimodal approaches in a large cohort of patients with entombed stents.
Materials and Methods: A retrospective chart review was performed of 127 patients who presented with entombed stents at 3 institutions between February 1993 and May 2011. Patient demographics, surgical approach, and clinical outcomes were analyzed using a Student's t-test and chi-square (α=0.05).
Results: Of the 127 patients, 60 were treated with a unimodal procedure and 67 received multimodal treatment. In the unimodal approach, procedures included cystolithopaxy (n=17), ureteroscopy (n=25), SWL (n=13), and PCNL (n=5). The most common multimodal approach was SWL + ureteroscopy + cystoscopy (n=22). Median indwelling stent time was similar (11.8 vs. 13.5 months) in the unimodal and multimodal treatment groups, respectively (p=0.49). In a single setting, multimodal treatment had a higher success rate for stent removal (82.1% vs. 61.7%; p=0.01) with no difference in complication rates (31.3% vs. 22.4%; p=0.27) compared to unimodal therapy.
Conclusion: Multimodal approach should be considered for patients with entombed stents due to its higher success rate.
Palliative Treatment of Malignant Ureteral Obstruction with Covered Self-Expandable Metal Stent: Initial Experience
IntroductionUreteral patency in malignant ureteral obstruction cases is a therapeutic challenge. Self-expandable metal stents have been used for malignant ureteral obstruction with acceptable results but obstruction by urothelial hyperplasia or tumor ingrowth occur. Polytetrafluoroethylene membrane covered mesh stent can maintain its patency by preventing ingrowth.PurposeTo report initial experience with retrograde placement of covered self-expandable metal mesh stents (CEMS) for palliative treatment of extrinsic malignant ureteral obstruction.Materials and MethodsFrom October 2010 to June 2011, 10 ureters of 9 patients (3 males and 6 females, mean age: 61) with unilateral or bilateral extrinsic malignant ureteral obstruction underwent CEMS (Niti-S, TaeWoong Medical, Korea) placement. CEMS was deployed retrogradely under cystoscopy and fluoroscopy. The indication was non-function of double pigtail stent or excessive bladder irritation symptoms.ResultsThe primary cancer sites were uterine cervix in 4, rectum in 3, stomach in 1, and other in 1. The mean length of obstruction was 8.8cm (range: 2cm∼17cm). The level of obstruction was upper ureter in 1 ureter, lower in 4 ureters, and mixed in 5 ureters. Simultaneous balloon dilation was performed in 5 patients. CEMS was successfully placed in all ureters. There was no CEMS obstruction during follow-up period but de-novo obstruction distal to CEMS by tumor growth was found in 2 patients at 3 months after procedure. No significant complication developed except for transient and self limiting hematuria and pain.ConclusionsCEMS could relieve malignant ureteral obstruction safely and easily. Long term follow up is necessary to confirm its efficacy.
Defining the Factors Influencing the Decision on Post-Ureteroscopic Stenting: A Multivariate Analysis
Aim: To identify factors influencing the drainage option after ureteroscopic procedures. Patients and methods: The study comprises a consecutive series of 160 patients referred for retrograde endoscopic treatment of stone disease. Internal stents were left postoperatively in 96 (60%) patients (stented group), and no drainage were chosen in 64 (40%) patients (non-stented group). Demographic, clinical and intraoperative data were statistically assessed. Results: Ureteroscopy (URS), retrograde nephroscopy (RN) and combined URS and RNs were performed in 95(59%), 48 (30%) and 17 (11%) patients, respectively. Bilateral procedures were performed in 8 (5%) patients. Univariate analysis demonstrated that significant prognosticators for non-stenting decision are: stone size<9 mm (p=0.01); previous endoscopic treatment (OR 5.8, p=0.04); preoperative internal stent (OR 13.4, p<0.001); operative time<25 min (p<0.001); surgeon experience (p=0.004); basket stone removal (OR 3.4, p=0.0003), no stone (OR 8.1, p=0.04). Significant prognosticators for stenting were stone size>9 mm (OR 3.2, p=0.0008), previous SWL (OR 5, p=0.04), holmium laser fragmentation (OR 5, p<0.0001) and operative time>25 min (OR 10.9, p<0.0001). Age, gender, operation type, stone location and bilateralism did not significantly influence the decision for postoperative stenting. Multivariate analysis demonstrated that previous treatment, preoperative internal stent, operative time and surgeon experience are independent prognosticators of the choice of postoperative drainage.Conclusions: The choice of drainage after ureteroscopic procedures is independently influenced by previous treatment, preoperative internal stent, operative time and surgeon experience. These findings may help in the decision-making process about the type of postoperative drainage, contributing in decreasing secondary morbidity.
Management Ofrecurrent Ureteropelvic Junction Obstruction With Self-Expandable Metallic Stents
Introduction. Metallic ureteral stents are widely used in cases of malignant ureteral obstruction and in patients with ureteroileal anactomotic strictures. Metallic stents for treatment of ureteropelvic junction obstruction (UPJO) are used rarely.Purpose. We report our experience with self-expandable metallic stents for treating UPJO.Materials and methods. We have operated 6 patients of mean age 45 y.o. (range 32 - 58 y.o.) with recurrent UPJO and inserted self-expandable metallic nitinol stents. The 6 patients with recurrent UPJO were assessed 6,8,12,18 20 and 24 months after surgery: 4 after open pyeloplasty, 1 - after laparoscopic pyeloplasty, 1 - after open pyelolithotomy.Dismembered Anderson-Hynes pyeloplasty was performed in 5 cases. Excretory urography and diurethic renography were performed 6 and 12 months after metallic stent unsertion.Results. Mean follow up was 20 months (range 8 to 38). A self-expandable stent placement was successful and immediate patency was achieved in all cases. During follow up 5 patients required no further intervention since the stented UPJO remained patient and without stent dislocation. In 1 patient 12 months after initial surgery we revealed stone in proximal end of endoprostesis. The stone was successfully treated with percutaneous nephrolithotripsy and the patient remained asymptomatic thereafter.Coclusion. In recurrent UPJO after unsuccessful pyelolasty and endopyelotomy the use of self-expandable metallic stents is optimum method for treatment of UPJO.
Outcomes of Metallic Resonance Stents in Malignant Ureteral Obstruction
INTRODUCTION: Malignant ureteral obstruction (MUO) often necessitates chronic indwelling ureteral stents or nephrostomy tubes. A metallic stent (Resonance) by Cook Medical has a reported 12-month dwell time. Its clinical outcomes in MUO have yet to be completely defined.
PURPOSE: To evaluate outcomes of Resonance stents placed for MUO.
METHODS: Patients undergoing placement of Resonance stents at Duke University were identified retrospectively. Indications for stent, and stent failure rates (defined as flank pain or increased hydronephrosis, radiographic evidence of stent migration, or need for repeat instrumentation in<12 months) were compiled.
RESULTS: Twenty-four patients were identified, with a total of 35 stents since September 2010. Mean age was 65 years. Mean follow-up was 3 months. Sixteen (45%) were placed as conversion from traditional types of stents, while 7 (20%) were placed as the initial modality. Seven (20%) were placed for salvage in patients who had failed traditional stents. Nine (26%) stents were identified to fail. Mean time to failure was 15.5 weeks. Increased hydronephrosis was the most common marker of stent failure (55%), followed by decreased GFR (44%), and flank pain (22%). Three failed stents (33%) had migrated distally. Stent failure was managed by replacement of the Resonance stent (44%), placing an alternative ureteral stent (22%), nephrostomy (11%), or observation (22%).
CONCLUSIONS: Consideration should be given to monitoring patients with creatinine and imaging within three months following Resonance& placement. With a 26% failure rate at 3 months, long term follow-up is needed to determine if failure rates continue to rise.
A Novel Method to Maintain Access to the Renal Pelvis During a Rendezvous JJ Stenting-a Point of Technique.
Introduction: Insertion of JJ stent across a tight ureteric obstruction is difficult. A rendezvous technique is employed to obtain a through and through guide wire to facilitate stent insertion. Retention of the nephrostomy tube at the end of the procedure is felt necessary as a safety mechanism. We describe a technique which prevents accidental slippage of the guide wire during this procedure.Material and Methods: A total of 22 rendezvous procedures were undertaken from 2009 to 2011 for complex ureteric obstruction. After a successful insertion of a JJ stent over a through and through guide wire, stent pusher is inserted over the guide wire from its proximal end with metallic end first. The tip of the pusher kept kissing the upper end of stent. The guide wire is then withdrawn while maintaining contact between stent and pusher. As soon as the wire leaves the stent lumen, it curls away from the tip of the pusher. The guide wire is now advanced through the pusher which is in the renal pelvis. Nephrostomy tube is inserted over the guide wire. We undertook this technique during 5 procedures under fluoroscopic control.Results: This technique was successful in all cases. No difficulty was encountered. Conclusion: This a simple but effective technique which prevents loss of access to the upper tract during difficult JJ stenting. No additional equipment is necessary
The Rendezvous Procedure for Ureteric Stenting: Results with Our Selection Criteria and Modified Technique
Introduction: Nephrostomy tube decompression is necessary in selected patients with ureteric obstruction. Unsuccessful JJ stenting by antegrade route needs a rendezvous technique. We chose to undertake the latter as a primary procedure in pre-selected group of patients. Success was improved with modifications technique.Material and Methods: 22 patients with ureteric obstruction underwent JJ stent insertion with Rendezvous technique between 2009 and 2011. The underlying pathology of ureteric obstruction was malignancy. Patients were selected for this technique by pre-selected criteria. These included complete stenosis, strictures longer than 2 cm, multiple strictures, and involvement of ureteric orifice. Modified technique included hydrophilic, small guide wires, biliary manipulating catheter, semi-rigid ureteroscopes to get the guide wire across the obstruction. A JJ stent was inserted over guide wire and nephrostomy tube removed. All procedures were undertaken under general anaesthesia. Results: Guide wire placement was successful in 21 patients (95.4%). Retrieval of guide wire from below was possible in 18 patients and in ureter in 3 patients. This was facilitated by a semi-rigid ureteroscope. Resection of tumour overlying the ureteric orifice to retrieve the guide wire was necessary in 18 patients. There were one failures due to a very tight obstruction. Conclusions: We feel patients with criteria mentioned should be selected for a primary rendezvous stenting. It is likely to achieve a greater degree of success with minimal discomfort to the patient and avoids the need for repeated attempts of stenting thus reducing the length of stay. Our modifications ensure a higher degree of success.
Long Term Follow up of Retrograde Ureteroscopic Holmium LASER Endopyelotomy in Ureteropelvic junction obstruction
Purpose: To review our long term experience with retrograde ureteroscopic Holmium LASER endopyelotomy for correction of ureteropelvic junction obstruction (UPJ-O). Patients and methods: From 2001 to 2010, 15 men and 34 women (mean age 49 years) underwent 58 ureteroscopic endopyelotomy procedures for treatment of primary (N=41) or secondary (N=17) UPJ-O. Renal function was estimated on renal diuretic scan before and after surgery with a mean renographic follow-up of 1 year. Subjective results were based on questionnaires which were returned from 45 patients (mean follow-up 5.4 years). Endopyelotomy was performed under direct vision using a flexible ureteroscope with a laser setting of 1 J at 10 Hz. Success was defined as symptomatic relief combined with either stable or improved renography. Results: Of all patients that underwent primary endopyelotomy, 34% had recurring symptoms or decreased renal function in the long term. For this reason, nine patients had a second endopyelotomy, two patients an open pyeloplasty and one patient a nephrectomy. Mean time to reintervention was 2.2 years. After a second endopyelotomy, 78% of the patients had a significant decrease of symptoms. Two patients had further deterioration in renal function, one requiring a nephrectomy. Secondary UPJ-O after an alternative primary procedure was treated by endopyelotomy in 7 patients. Forty-two percent of these patients had a significant reduction in symptoms. Conclusions: After one or two endopyelotomy procedures eventually 82% of the patients were successfully treated with this minimally invasive surgery. Long term follow up is recommended to identify late recurrences.
He Successful Factors of Retrograde Holmium-Laser Endopyelotomy for Ureteropelvic Junction Obstruction (UPJO) Patients
Introduction: The retrograde holmium-laser endopyelotomy for UPJO has adventage of minimal invasion. But this procedure maybe has low success rate. Purpose: To define the successful factors of retrograde holmium-laser endopyelotomy for UPJO patients. Materials and Methods: We retrospectively collected the data of all 21 UPJO patients who had accepted retrograde holmium-laser endopyelotomy from April 2006 to May 2011. All UPJO patients were selected for this research excepted patients who had high inserting ureter or aberrant polar crossing vessels. Nephrogram, IVP and/or ureter CT scan were used before and after procedures to estimate the effect of this procedure. The successful criteria defined as renal function was improved or hydronephrosis was reduced. Average follow-up were 19 months. We analysis these factors as follow with multivariate analysis: Degree of hydronephrosis, function of UPJO kidney, inflammation or stones in UPJO renal pelvic, length of stenosis. Results: Success rate of retrograde holmium-laser endopyelotomy for UPJO was 71.4% (15/21 cases). Univariate analysis show that length of stenosis(p=0.031), function of UPJO kidney(p=0.042), degree of hydronephrosis(p=0.049) were predictive factors for the success of this procedure. In multivariate analysis, length of stenosis (OR=1.446, 95%CI: 0.624-2.185) was the only predictive factors of this procedure. Conclusions: Retrograde holmium-laser endopyelotomy for UPJO patients, the length of stenosis is the only factor related to the success of this procedure.
The Predictive Factors for the Success of Holmium-Laser Retrograde Endoureterotomy for Ureteral Stenosis
Introduction: Holmium-laser retrograde endoureterotomy is minimal invasive procedure for the treatment of ureteral stenosis. Purpose: To define the predictive factors for the success of holmium-laser retrograde endoureterotomy for ureteral stenosis. Materials and Methods: We retrospectively reviewed 34 patients with ureteral stenosis who had undergone holmium-laser retrograde endoureterotomy from April 2006 to may 2011. The causes of ureteral stenosis included: primary stricture, secondary to stone or inflammation, UPJO. The patients with complete ureteral obstruction or external compression on ureter were excluded. Nephrogram, IVP and/or ureter CT scan were used before and after operations to estimate the success of endoureterotomy. Success was defined as no obvious ureteral stenosis in imaging examination, and renal function was improved or preserved. Average follow-up were 13 months. The factors: age, time from diagnosis to treatment, degree of stenosis, length of stenosis, degree of nephrosis, function of ipsilateral renal, urinary tract infection in ipsilateral upper urinary tract and stones at ipsilateral upper urinary tract were analyzed in logistic regression. Results: holmium-laser retrograde endoureterotomy were achieved in 24 patients (70.6%). In logistic regression analysis: age(OR=1.618, 95%CI:0.724-3.611), time from diagnosis to treatment(OR=1.899, 95%CI=1.146-3.353), degree of stenosis(OR=0.622, 95%CI=0.363-1.087), degree of nephrosis(OR=1.244, 95%CI=0.621-2.345), function of ipsilateral renal(OR=0.587, 95%CI=0.333-1.089), urinary tract infection in ipsilateral upper urinary tract(OR=0.812, 95%CI=0.454-1.433) and stones at ipsilateral upper urinary tract(OR=0.186,95%CI=0.072-0.567) had no correlation with successful endoureterotomy, only length of stenosis(OR=3.422,95%CI=2.011-6.343) was significant predictive factor.
Ureteroscopic Management for Upper Tract Urothelial Carcinoma: Long-Term Single inStitution Experience
Introduction and Objective: We evaluate the outcome of ureteroscopic management for upper tract urothelical carcinoma (UT-UC).Methods:Between July 1991 and February 2011, 14 patients (12 male, 2 female) underwent ureteroscopic management of UT-UC (renal pelvis: 8, ureter: 6) at Okayama University Hospital. The indication criteria for the ureteroscopic management were the following: 1) tumor size less than 20mm, 2) superficial tumor. Results: There were 8 (57%) solitary kidney, 1 (7%) bilateral disease and 5 (36%) elective cases. The median follow-up was 71 month (5-182 months). Initial pathological T-stage was pTa in 11 (79%), pT1 in 2 (14%) and pTa + pTis in 1 (7%, bilateral disease). Tumor grade was G1 in 1 (7%), G2 in 11 (79%), G3 in 1 (7%) and G2 + G3 in 1 (7%, bilateral disease). Ten (71%) patients had recurrent disease during follow-up. Adjuvant upper tract BCG irrigation was offered to those with frequent recurrent disease. Five patients agreed with adjuvant upper tract BCG irrigation and 3 of those (3/5, 60%) have become recurrent-free after adjuvant upper tract BCG irrigation. One underwent neoadjuvant chemotherapy (gemcitabine, cisplatin, paclitaxel) for tumor shrinkage and underwent successful ureteroscopic surgery.Nephron sparing rate was 12/13 (93%). Cancer-specific survival rate was 12/13 (93%). Conclusions: Our results suggest that ureteroscopic management for UT-UC in selected patients provides high nephron sparing rate (93%) and cancer-specific survival rate (93%) during a long follow-up. Adjuvant upper tract BCG irrigation may be useful for the patients with frequent recurrent disease.
Endoscopic Management of Upper Tract Urothelial Carcinoma as Primary and Salvage Treatment Following Systemic Chemotherapy
Background: Endoscopic management of upper tract urothelial carcinoma is becoming acceptance as renal preserving procedure for selected patients. However the procedure has limitation for tumor size and potential invasiveness of the disease. Here we reported our results of endoscopic ablation for both types of disease.Materials and Methods: From 1999 to 2008, five patients with urothelial carcinoma (size 0.2 to 0.7 cm)of ureter and renal pelvis were successfully ablated with self made electrode through ureteroscope.Of three patients with tumors larger than one cm and arising from bilateral renal pelvis, two patients were respond to initial systemic chemotherapy. Both residual lesions were then ablated by cauterization through ureteroscope. Another patient without response to chemotherapy was then was resected through nephroscopy for one side and nephroureterectomy for other side.Results: Patients age ranged from 40 to 83 with a mean age of 59. Two patients had grade I, 4 grade II and 2 grade III tumor. Follow up ranged from 3 to 12 years. Five had recurrent free survival for 3 to 8 years. Three patients had upper tract recurrence, one died of unrelated disease and the other two patients still survived following repeated ureteroscopic management. Conclusion: Endoscopic management of small low grade urothelial carcinoma of ureter and renal pelvis is encouraging. For larger tumors or high grade without board base tumor, initial systemic chemotherapy then followed by endoscopic ablation is potentially feasible.
Recurrent Upper Urinary Tract Transitional Cell Carcinoma After Opposite Side Nephroureterectomy:the Feasibility of Endoscopic Treatment with Laser Device
Introduction: It is difficult for urologist to choose an effective method to treat the patients with recurrent upper urinary tract transitional cell carcinoma (UUT-TCC), who have received nephroureterectomy on opposite side previously.Purpose: To appraisal the feasibility of endoscopic treatment with laser for recurrent UUT-TCC after opposite side nephroureterectomy. Materials and Methods: We retrospectively reviewed all 12 patients who had undergone opposite side nephroureterectomy received endoscopic treatment with laser for recurrent UUT-TCC from January 2006 to May 2011. Clinical characteristics, operation results and functional outcomes were investigated. Mean follow-up were 15 months. End points of follow-up included: complete ureteral obstruction, or tumor locally advanced, or distant metastasis.Results: Clinical characteristics: All patients had superficial lesions of UUT-TCC. five patients had mild gross hematuria and others had no severe symptoms. Eight patients were multifocus and ten patients had mild hydronephrosis. Operative results: mean operation time was 32±11.5 mins, and mean times of procedures per patient were 2.1±0.9 times. Mean recurrent time was 4.4±1.6 months. Ureteral perforation happened in four patients (33.3%) and no other complications. Functional outcomes: during follow-up, renal function (58.3%) were preserved in 7 patients, five patients (41.7%) convert to open surgery or nephrostomy because of complete ureteral obstruction, or tumor locally advanced, or distant metastasis. Conclusions: endoscopic treatment with laser for patients in this situation is effective. This procedure could minimize invasion and be duplicable in spite of less efficient for cure and function preservation.
Department of Urology, Addenbrooke's Hospital, Cambridge, UK
IntroductionTo determine the accuracy of ureteroscopy, biopsy and upper-tract cytology in predicting the histopathology of patients undergoing nephroureterectomy for suspected upper-tract transitional cell carcinoma (UTTCC) at two tertiary centres.Materials and MethodsFrom 2004-2010, 56 UTTCCs were diagnosed ureteroscopically and underwent nephroureterectomy at two tertiary centres. Indications for diagnostic ureteroscopy were noted. In 46 patients ureteroscopic biopsy was performed and upper-tract urine cytology sent in 30 patients. Ureteroscopic findings, upper-tract cytology and biopsy data were compared with final surgical specimen histopathology. ResultA filling defect on imaging was the commonest indication for diagnostic ureteroscopy (64%). Upper-tract urine cytology was positive in19 out of 30 cases (63%), but did not predict grade accurately. Ureteroscopic biopsy grading was not possible in 7 out of 46 cases (15%). The biopsy grade proved to be identical in 25 of the remaining 39 cases (64%). Grade 1 or 2 ureteroscopic biopsy subsequently had low stage tumour (Ta or T1) in 13 of 16 (81%) cases. Grade 3 ureteroscopic biopsy had high stage tumour (T2 or worse) in14 of 20 (70%) cases. One patient with ureteroscopic biopsy suspicious of UTTCC had no tumour identified on nephroureterectomy specimen. When UTTCC was visually diagnosed at ureteroscopy (53/56 cases (95%)), final histopathology confirmed UTTCC in all cases. ConclusionIn experienced hands, UTTCC can be accurately diagnosed by ureteroscopy. However, a combination of ureteroscopic appearance, upper-tract urine cytology and biopsy are necessary to identify high grade UTTCC which is predictive of higher stage disease, not suitable for conservative therapy.
The Application of Percutaneous Nephroscopy in Treatment of Upper Urinary Tract Carcinoma ( Report of 8 Cases)
Objectives To evaluate the application of technique of percutaneous nephroscopy in the upper urinary transitional cell carcinoma,especiallly the renal pelvic carcinoma.Material and Methods From June 2006 to June 2010, 8 cases (10 sides) of renal pelvic carcinoma received percutaneous tumor resection, of which 6 males ( 7 sides) and 2 females(3 sides). 6 cases of patients with solitary kidney, two side of the renal pelvic tumor in 2 cases. 4 cases of high-grade tumors, low-grade tumors in 6 cases. Age ranged from 52 to 72 years old (average 61.2 years).Tumor diameter ranged from 0.5 to 3.5cm( average 2.6 cm). Patients were treated with percutaneous nephroscopy laser or electrocautery. Ureteral stent was retended intraoperatively. Chemotherapy drugs was irrigated postoperative through the nephrostomy tube. Results Operations were successful, the operation time of 45-95min (average 73 mins), blood loss 20-300ml (average 50ml), No remarkeble difference were found in serum creatinine level between postoperative and preoperative. After 10 to 36 months following up using CT and MRI and ureteroscopy and so on, One patient died of tumor metastasis, two patients with local tumor recurrence. The remaining patients have a good prognosis.Conclusions The technique of percutaneous nephroscopy in treating renal pelvic tumor is safe and feasible , with a satisfactory result. This is a better choice for the renal pelvic carcinoma patients unsuitable for ureteronephrectomy.
MP30: Ureteroscopy 2
Active Stone Removal for Patients with 5 mm or Smaller Ureteral Calculi
Introduction and Purpose: For patients with 5 mm or smaller ureteral calculi, conservative therapy is performed as first-line therapy. If pain relief and spontaneous passage cannot be achieved, stone removal is carried out. We retrospectively evaluated whether active stone removal for these patients was reasonable based on endoscopic ureteral findings.Material and Methods: Between April 2009 and June 2011, 76 patients with 5 mm or smaller upper ureteral calculi were treated with an ureterorenoscope (URS). URS was performed for 43 patients (56.6%) because of the lack of pain relief and for 33 patients (43.4%) because of the absence of spontaneous stone passage. The course of the procedure and clinical course were evaluated. Results: The study involved in 76 patients with a mean age of 53.0±14.8 years. The mean stone diameter was 4.1±0.9 mm. The mean interval until stone treatment was 12.5±14.8 days. The mean operative time was 23.5±9.5 min. A stone-free state after single URS was achieved in 70 patients (92.1%). However, in 6 patients (7.9%), additional URS were needed due to lower ureteral stricture. Endoscopic ureteral findings revealed ureteral edema in 50 patients (65.8%) and stricture in 38 patients (48.7%). Also, lower ureteral stricture was detected in 43 patients (56.6%).Conclusions: Endoscopic findings revealed lower ureteral stricture and ureteral edema in many patients. These situations could make it difficult to achieve spontaneous stone passage. Considering these ureteral findings, active stone removal with URS is reasonable for patients showing no pain relief or spontaneous stone passage.
Impacted Proximal Ureteral Stones Treated by Retrograde Ureteroscopic Approach
Introduction: The AUA/EAU Ureteral Stones Guideline Panel reports similar results for SWL or ureteroscopy in proximal ureteral stones. However, impacted ureteral calculi are more difficult to treat by SWL. Purpose: To assess the efficacy, safety, and complications of retrograde ureteroscopy for impacted upper ureteral stones. Materials and Methods: Between June 1994 and December 2010, 5895 patients underwent retrograde ureteroscopy (6282 ureteroscopic procedures). This type of procedure was performed in 208 cases with impacted proximal ureteral stones ranging between 8 and 24 mm. The follow-up protocol included ultrasonography, KUB and, in selected cases, CT.Results: The procedure was successfully completed in 192 cases (92.3%). In the other cases, stone fragments migrated in the pyelocaliceal system imposed their retrieval with the flexible ureteroscope in 8 cases, SWL in 7 cases and percutaneous nephrolithotomy in 1 case. The complication rate was 4.3%: persistent hematuria (4 cases), fever (3 cases) and ureteral perforation (2 cases). Two patients developed ureteral strictures at the impaction site. Conclusions: In experienced hands, the use of semirigid ureteroscopy in impacted upper ureteral stones has very satisfactory results with minimal complications. Various intraoperative incidents may require complex endoscopic approach.
Accordion - Music to the Endourologist.
Introduction: Management of upper ureteric stones with ureteroscopy and laser fragmentation can be tricky, especially if there is migration of fragments to the kidney, needing flexible ureteroscopic management. Stone immobilisation devices are cumbersome and are not satisfactory. We present our initial experiences with the novel PercSys Accordion® [PA] stone management device.Methods: The PA consists of its own introducer, an advanced microcatheter that features a proprietary film occlusion device with radio opaque markers. The device is introduced into the ureter through a cystoscope. There is a locking handle mechanism to manipulate the position of the occluding film. PA is placed beyond the stone under radiological guidance and deployed by pulling the inner guide wire. The occluding film takes a concertina configuration like an accordion, hence the name. Once deployed the PA prevents migration of stone which can be fragmented with laser or other devices. Once fragmentation is complete the device is trawled down removing residual fragments.Results: The device was used in 20 radio opaque upper ureteric stone patients. Seven of these were non-stented. Mean stone size was 9 mm [range 8mm - 14mm]. Two were impacted. Placement and deployment was successful in all cases. Stone fragmentation was performed using the holmium-YAG laser. Irrigation was kept at high flow and the vision was excellent. The mean laser time was 391 sec (139-672). Conclusion: The PA is satisfactory and avoids the need for additional procedures or baskets. We believe that this device will be an essential part of endourological armamentarium.
Effective Research Of Ureteroscopic Lithotripsy Combined with Stone Basket for the Treatment of Upper Ureteral Stone
Objectives: Discuss the safe and effective treatment for the upper urteral stones. Material and Methods: From January 2009 to July 2010, 35 patients of upper ureteral stones received ureteroscopic lithotripsy combined with stone basket therapy. The equipment of lithotripsy was Holmium laser or ballistic. Negative stones were 5 cases( male 3, female 2). 12 stones located in the left side with 23 cases right. Stone size ranging from 3mm*5mm to 11mm*215m.Ureteral stones could be found by the ultrasound or plain film of abdominal obviously. Negative stones were also confirmed by computed tomography. Equipment including ureterscopy (F8/9.8, WOLF, Germany),stone basket ( COOK, America), ballistic lithotripsy machine and 30W Holmium laser.Operative time varies from 7 minutes to 48 minutes. Ureteral stent were indwelled routinely in the end of surgery.Results: The successful rate of lithotripsy was 97% (34/35), One case of stone was washed into the calyx because of the high location. Other patients received satisfied effects. Postoperative abdominal plain film showed no residual stones. Patients discharged between 1 to 3 days after operation. Conclusions: Ureteroscopic lithotripsy combined with stone basket therapy is effective to the upper ureteral stone. For it can not only avoid the risk of blind use of stone basket ,but also improve the efficency of lithotripsy. We consider it a safe and effective method to be wide for promotion.
Urology Department, Acibadem University, Istanbul, Turkey
Introduction: Flexible ureterorenoscopy (f-URS) is increasingly used for treatment of large and/or multiple upper urinary tract (UUT) stones. However, multiple sessions may be necessary for complete stone clearance.Purpose: To assess the efficiency of single session f-URS for treatment of large and/or multiple UUT stones.Material and Methods: A retrospective database analysis was carried out to identify patients with large and/or multiple UUT stones. Storz Flex II or Wolf Cobra scopes were used. Holmium laser was used for fragmentation. Patients were considered stone-free if no residual fragments or fragments smaller than 2 mm (CIRF) were seen radiographically after the procedure. Efficiency and safety of the procedures were analyzed.Results: Between 2001 and 2011, 126 procedures were performed. Twenty-three patients had large (equal/or greater than 2 cm) and/or multiple UUT stones in 25 renal units. Twelve patients had renal (2 bilateral), 8 had renal + ureteral and 3 had ureteral stones. Mean stone size was 29.2 mm. In 19 patients (76%), single session f-URS achieved the goal of complete stone clearance. In 4 patients second session was necessary. In 1 patient, the stone could not be reached because of narrow ureter and PCNL was performed. In another patient SWL was necessary for complete stone clearance. One patient who had undergone bilateral intervention had urosepsis treated uneventfully.Conclusions: Flexible ureteroscopy combined with Holmium laser is an efficient method for treatment of large and/or multiple UUT stones. However, additional treatment such as second session f-URS, SWL or PCNL may be needed in some patients.
Assesment of Ureteral Access Sheath-Related Ureteral Injury During Flexible Ureteroscopic Lithotripsy: Is Inserting of Access Sheath Safe?
INTRODUCTION AND OBJECTIVE: To evaluate ureteral damage caused by ureteral access sheath (UAS) insertion and whether inserting of UAS is safe to avoid ureteral stricture.METHODS: We reviewed total 1014 cases flexible ureteroscopy with holmium YAG (f-URS) from April 2007 to June 2011 in single center. Amongst them, 24 cases of UAS-related injuries when inserted were encountered. Those were intraoperatively stratified by URS to 3 grades of injuries in terms of depth (Grade1: only mucosal, Grade2: muscle layer and Grade3: peri-ureteral fat). Then 2nd f-URS was subsequently scheduled for some cases whose stone burden still remained due to early event of the injury. On the other hand for stone-free cases by first session, intravenous urography was alternatively performed after removal of the stent to exclude long term stricture formation.RESULTS: UAS-related complication rate was 2.4%. There were 11 cases of 2nd f-URS performed for residual fragments. There were 16 cases of Grade1 injury, 5 of Grade2 and 3 of Grade3. Complete ureteral healings were confirmed by URS for all cases without 2 cases (only mucosal healings: Grade2 and Grade3, respectively) which showed enough durability for 2nd sheath insertion. All injured cases achieved stone free. No long-term ureteral strictures were identified at present. CONCLUSIONS: It appeared that 3 weeks ureteral stent placement can facilitate surgeons to perform 2nd f-URS to achieve safer stone retrieval as well as final stone free status without prolonged ureteral complications. It is also resulted that insertion of UAS for f-URS is safe maneuver.
The Efficacy of Flexible Ureteroscopy in Patients with Single Renal Stone Less than 2cm
Purpose: To assess efficacy of flexible ureteroscopy in patients with single renal stone less than 2cm. Patients and Methods: The clinical date on 35 patients with single renal stone less than 2cm who performed flexible ureteroscopic lithotripsy was retrospectively analyzed. The flexible ureteroscope was 8.8F . Patients were considered stone free if no residual stones were seen endoscopically and radiographically during or after the procedure. Results: Between 2008 and 2010, 35 flexible ureteroscopic procedures were performed in our department. The mean age was 46.2y(19-56), 19 of whom were male and 17 were female.Holmium laser lithotripsy was used in all of the patients. The mean stone size was 1.8cm, the mean operative time was 45 min. The overall stone-free rate after a single procedure of flexible ureteroscopy was 78.2%. Complications have been recorded in 3 patients, including urinary tract infection in two and hematuria in one patient. No major complications occurred. All patients who had a resident stone were treated conservatively.Conclusions: flexible ureteroscopy is an effective treatment option in patients with single renal stone less than 2cm. The procedure have a high stone-free rates and a low rate of complications.
Efficacy of Tamsulosin 0.2mg/day in Relieving Double-J Stent-Related Symptoms: a Randomized Controlled Study
PURPOSE: To evaluate the efficacy of tamsulosin (0.2mg/day) in improving stent-related symptoms and quality of life in patients with in-dwelling double-J ureteral stents. PATIENTS AND METHODS: A total of 64 patients with ureteral stent placement following ureteroscopy were prospectively randomized into two groups of 32 patients. Mean patient age was 44±18 years (48% male, range 14-76 y) and 46±17 years (54% male, range 16-83 y) in groups 1 and 2, respectively. Group 1 received 0.2 mg tamsulosin once daily for 4 weeks and group 2 was a non-placebo, non-treatment control. All patients completed the International Prostate Symptom Score (IPSS) and SF-36 questionnaires at 2 and 4 weeks post-operatively. RESULTS: The IPSS scores were significantly lower in group 1 than group 2 at both 2 and 4 weeks. Among the eight domains of SF-36, role limitation due to physical health and bodily pain was significantly better in group 1 at 2 and 4 weeks. General health was also significantly better in group 1 at 2 weeks. CONCLUSIONS: Tamsulosin improved both urinary symptoms and quality of life without causing serious side-effects.
Early Ureterolithotripsy for Obstructive Stones in Single Kidney Patients
INTRODUCTION Aim of this study was to evaluate safety and efficacy of an immediate disobstructive ureteroscopic treatment in patients with obstructed single functional kidney due to ureteral stone.MATERIALS & METHODS We analyzed medical records of 368 patients underwent retrograde semirigid or flexible ureteroscopy between March 2005 and December 2010. Average age was 42+11 years, 59,7% male and 40,3% female. 28 (7,6%) patients with single functional obstructed kidney were treated by urgent ureteroscopy, Holmiun laser lithotripsy and ureteral stent placement. Out of 28 patients, 8 (28,5%) showed anuria, flank pain and serum creatinina above 7 mg/ml, 3 (10,7%) had urosepsis secondary to pyonephrosis (so percutaneous nephrostomy was applied immediately), and one patient (3,57%) had a neglected stent placed for obstructing stone one year before. 16 (57,1%) patients showed flank pain, oliguria, and moderate elevation of urea and serum creatinine. Most of these patients knew to have a single functional kidney and all of them suffers for obstruction diagnosed by ultrasound and spiral CT scan. RESULTS Normalization of renal function occurred in 23 (82,1%) patients few days after the procedure. Three (10,7%) patients were discharged with acceptable renal function and 2 (7,1%) remained stable with serum creatinine of 3,2 after 6 weeks follow up. CONCLUSION In cases of obstructed single functional kidney immediate ureterolithotripsy looks to be an effective and definitive procedure. It prevents others long term treatments and their possible complications. In some critical cases restabilization of better clinical conditions and sespis treatment is mandatory.
Dpartment of Urology, Aberdeen Royal Infirmary, Aberdeen, Scotland, UK
Introduction: Urolithiasis in pregnancy has been reported in up to 1:200 women and can be the cause of maternal and foetal distress. We conducted a systematic review of the literature to look at the role of ureteroscopy in stone management during pregnancy. Material & Methods: We searched MEDLINE, PubMed and the Cochrane Library from January 1990 to June 2010 for results of ureteroscopy and stone treatment in pregnancy. Inclusion criteria were all English language articles with at least 3 patients. Data was extracted on the outcomes and complications reported in the literature. Results: A total of fifteen studies were indentified reporting on 126 procedures. Of these, the treatment was done in the third trimester (3 studies), second or third trimester (6 studies) and anytime during pregnancy (2 studies). The surgical method of stone management was stone extraction with basket only (n=60), laser fragmentation (n=17, holmium; n=7, pulse dye), impact lithotripsy (n=22) and ultrasonic lithotripsy (n=6). Ten of these procedures were done utilising flexible ureteroscopy. Post-operative stents were inserted in 73/118 (40%). A successful outcome was seen in 107/120 (89%). There were 2 major (one ureteral perforation and one premature uterine contraction) and 7 minor complications (5 UTI and 2 post-op pain).Conclusion: Retrograde stone treatment using URS is a relatively safe option in pregnancy with a high success rate
Vancouver General Hospital, University of British Columbia, Vancouver, Canada
Introduction and Objective: Shockwave lithotripsy may not be an option in obese patients. We determined the effectiveness of ureteroscopic laser lithotripsy in obese patients compared to controls. Methods: Patients who underwent ureteroscopic procedures for urolithiasis at four centres with fellowship-trained endourologists were retrospectively analyzed.Results: The 292 patients included 163 obese (BMI>30 kg/m2), 76 overweight (BMI=25-30), and 53 normal weight controls (BMI<25). There were significantly more patients in ASA categories 2, 3, and 4 in the overweight and obese groups. The rate of diabetes was significantly higher in the obese and overweight groups (P=0.0240). The percentage of obese patients requiring flexible ureteroscopy (79%) was higher than in the other groups (P<0.0001). Stone free rate (SFR) did not differ among groups. Flexible ureteroscopy was associated with a lower stone free rate on multivariate analysis (p=0.034). There was no difference in SFRs of patients who required a ureteral access sheath, basket extraction, or received a post-operative stent. The complication rate did not differ between groups, although patients with an elevated BMI were less likely to have day surgery. Conclusion: SFRs are similar in obese and overweight populations to normal weight patients. The decreased SFR seen with flexible ureteroscopy was likely due to more proximal stone locations. Higher BMI was associated with a longer hospital stay. Ureteroscopic laser lithotripsy is an effective and safe technique to treat urolithiasis in the overweight/obese patient. The use of stents, baskets, or access sheaths did not affect the SFR in any group.
Department of Urology, Aberdeen Royal Infirmary, Aberdeen, UK.
Introduction: The management of urolithiasis in morbidly obese patients is difficult. Modalities such as shock wave lithotripsy and PCNL can be difficult or impossible in these patients due to problems with patient positioning, anatomical landmarks and increased skin to stone distance. URSL may be the only/best treatment option. Purpose: To conduct a systematic review of literature to look at the role of ureteroscopy for stone management in morbidly obese patients. Material & Methods: We searched MEDLINE, PubMed and the Cochrane Library from January 1990 to June 2010 for results of ureteroscopy and stone treatment in morbidly obese patients. Inclusion criteria were all English language articles reporting on ureteroscopy in patients with morbid obesity. Data was extracted on the outcomes and complications. Results: A total of 5 studies were identified during this period. One hundred and twenty patients (125 procedures) with morbid obesity underwent flexible ureteroscopy and stone treatment. The mode of fragmentation was pulse dye laser (n=49), holmium laser (n=52) and a combined modality including electrohydraulic lithotripsy and basket retrieval in others. The stone free rate was 81% (n=98) after the first treatment and increased to 93% (n=116) after the second treatment. Six patients (5%) had complications including post operative sepsis in 4 patients, pyelonephritis and ureteral perforation in one patient each. Conclusion: Retrograde stone treatment using ureteroscopy and lasertripsy in morbidly obese patients can be safely performed with good stone clearance rates and a low complication rate.
Managing Anesthetic Risk in the Super Morbidly Obese: Use of Flexible Uretersocopy Under Minimal Sedation
Introduction: Super-morbidly obese patients present challenges to surgeons and anesthesiologists. Standard surgical approaches are often impossible and airway management is difficult. Heavy sedation without intubation is ill-advised, as emergent airway management is tenuous. These patients are prone to post-operative respiratory complications. Purpose: Describe our experience with super-morbidly obese patients treated with flexible ureteroscopy (URS) under anesthesiologist-monitored minimal sedation.Methods: Between September 2009 and September 2010 we performed flexible URS procedures under minimal sedation on 3 super-morbidly obese patients. All were males with a mean age of 45.3 years, mean BMI of 74.6 and mean ASA class of 3.67. All procedures were performed on beds supportive of 800 pounds. All were positioned split-leg, in reverse Trendelenberg position to maximize ventillatory capacity and airway access. Sedative administration was initiated just prior to the procedure start, with the intent of keeping the patient comfortable, but conversant. Results: All required flexible cystoscopy for bladder entry and wire access to the ureter. For the 2 patients undergoing stone treatment, access sheaths were utilized. For diagnostic URS, the ureteroscope was advanced over a wire. Mean operative time was 96 minutes. All patients were conversant throughout the procedures. Patient 1 (diagnostic) received 5mg midazolam and 380mg propofol, Patient 2 (stones) received 4mg midazolam and 550mcg fentanyl and Patient 3 (stones) received 10mg midazolam and 150mg ketamine. No patient experienced complications intra- or post-operatively. Mean recovery time before discharge was 87.3 minutes.Conclusions: Outpatient flexible URS procedures can be performed in the super-morbidly obese under anesthesiologist-monitored minimal sedation.
Department of Urology, the first affiliated hospital of Guangzhou Medical College, Guangzhou, China, 2Guangdong Key Laboratory of Urology, Guangdong, China
Introduction and objective: Advances in the design of ureteroscope and ancillary instruments have resulted in miniaturization and increased durability of the smaller scopes required for pediatric patients, increased the ability of the urologist to evaluate and treat endoscopically the urinary tract in even the smallest patients with a relative stricture ureter. We investigated the safety and feasibility of ureteroscopy in treating mid and distal ureteric calculi of preschool children. Material and methods:19preschool children (12 boys and 6 girls, 8 months to 6 years) were enrolled. 4 cases in mid ureter and 15 cases in distal ureter including 3 case in bilateralis. Stone burden ranged from 0.30X0.52cm to 0.62×1.28cm,mean 0.59×0.87cm. Results: 1 case with a mid ureteric calculi received open surgery because of failure of ureteroscopy and also ESWL.5 cases received successful ureteroscopy with 6.5/8.5Fr semi-rigid ureteroscope and Ho:YAG laser lithotripsy in the first session, 3 cases had a successful ureteroscopy with a 8/9.8Fr rigid ureteroscope after a dilation of the ureteric orifice by rigid dilators and/or balloon dilator, 10 cases received passive dilation by indwelling of ureteric stents for 1 to 3 weeks and underwent successful ureteroscopy with 8/9.8Fr rigid ureteroscope. 19 cases received 28 ureteroscopic procedures in all, and all the cases were rendered stone free without any severe complication. Conclusion: Our experience shows that ureteroscopy in treating mid and distal ureteric calculi in preschool children was a straightforward, successful and feasible technique.
Guangdong Key Laboratory of Urology, Guangdong, China
Introduction and objective:To investigate the safety and feasibility of minimally invasive PCNL via 14-18Fr percutaneous working channel in treating renal calculi in children. Material and methods:28 preschool children (12 boys and 16 girls, ranged from 1.5 to 10 years, mean age 4.2 years) were enrolled, with a mean stone burden of 252mm2, ranged from 167 to 428 mm2. After retrograde ureter catheterization with ureteroscope, fluoroscopy-guided percutaneous punctures were made by urologists into the designed calyx after retrograde injection of constrast medium. A flexible 0.035 inch guide wire was then inserted, percutaneous tract was dilated to 14-18Fr by fascial dilators along the guide wire stepwisely. A matched peel-away sheath was inserted. The stones were fragmented with a pneumatic lithotripter through 8/9.8Fr rigid ureteroscope. Results: Mean operating time was 65 minutes (43-95 minutes). Complete stone clearance was achieved in 23 cases (23/28, 82.1%) in a single session, 2 patients received a second-look operation and were rendered stone free, 3 patients had residual stone less than 4mm. Therefore, a total clearance rate of 89.3% was achieved. Mean blood loss was 0.75g/L (0.42-1.31 g/L), no case need blood transfusion. 3 patients had a postoperative fever of 38.5 centi-degree or greater. No other severe complications were noted. The stone composition was that, calcium oxalate (10.71%), calcium Phosphate (7.14%), struvite (14.29%), uric acid (3.35%), cystine (3.57%) and admixture with the main bulk of calcium oxalate and calcium phosphate (60.71%).Conclusion: Our experience shows that MPCNL via 14-18Fr percutaneous tract was safety and feasible for children.
Pediatric Urinary Stone Composition in the United States
Introduction: There has been an increase in pediatric urolithiasis in recent years. While stone composition in adults has been well reported, studies in the pediatric population are scarce. The aim of our study was to analyze urinary stone composition in the pediatric population to determine trends in age groupings, gender, and geographic location within the United States. Methods: Stone analyses from pediatric patients in all 50 states were obtained from a reference laboratory over a 10-year period. Patients were excluded if they were older than 18 years or younger than 1 year, or if there was no crystalline component identified in the submitted specimen. The frequency of stone composition was analyzed along with age, gender, and geographic differences. Logistic regression analyses were performed to check for age, gender, age and gender, and regional differences in incidence of individual stone components. Results: A total of 5,245 stones were included in our analysis. Calcium was found in 89.2% of stones. Both age and gender had significant effects on stone composition. The percentage of stones containing calcium oxalate increased with age while magnesium ammonium phosphate and ammonium acid urate stones decreased. Calcium oxalate and magnesium ammonium phosphate stones were more common in females. Uric acid stones were more common in males. Geographic distribution was not significantly associated with stone composition.Conclusion: Our series is the largest pediatric stone composition analysis from the United States to date. Our analysis demonstrates age and gender differences in stone composition, but no differences based on geographical distribution.
MP31: Robotic/Lap Upper urinary Tract 6
Nephrometry Plus: Adding Upper Pole and Posterior Locations to the Nephrometry Score Increases Correlation with Minimally Invasive Partial Nephrectomy Outcomes.
Introduction: The nephrometry score was orignially developed from open and laparoscopic partial and radical nephrectomies.Purpose: To determine whether upper pole and posterior location added to Nephrometry score was more strongly associated with perioperative outcomes for laparoscopic and robotic partial nephrectomy. Methods: Nephrometry scores were calculated from mass size, proportion exophytic, proximity to collecting system, and position relative to the hilum. Complexity was graded low (4-5), medium (6-7), or high (8 or higher). The adjusted nephrometry score added upper pole (3pts) versus other locations (1pt) and posterior (3pts) versus anterior (1pt), which were graded low (6-8), medium (9-11), and highly (12-14) complex. Results: 77 partial nephrectomies (18 laparoscopic, 59 robotic) were reviewed. Complexity was similar in 61.3%, increased in 17.3%, and decreased in 21.3% following adjustment. Correlation between operative time and nephrometry score was 0.229 (p=0.05), improving to 0.374 after adjustment (p=0.001). Correlation between ischemia time and nephrometry score was 0.330 (p=0.006),and 0.378 after adjustment (p=0.001). Using nephrometry score, decline in postoperative GFR>10% occurred in 13/23 scored 8 or higher, and 20/50 scored<8, (p=0.188). After adjustment, 12/18 scored 12 or higher and 21/55 scored<12 declined in GFR>10% postoperatively (p=0.035). Two converted to radical nephrectomy (highly complex on both scales), 1 open (low versus intermediate on original versus adjusted scales), and one had a urine leak (highly complex on both). Conclusion: Adjustment of nephrometry score to include upper and posterior locations improved correlation with operative time and GFR decline, but not ischemia time and complications.
Comparison Between Laparoscopic and Open Partial Nephrectomy for Renal Tumors
INTRODUCTION: Controversies still remain regarding the best approach for partial nephrectomy.PURPOSE:to compare the outcomes of laparoscopic partial nephrectomy (LPN) and open partial nephrectomy (OPN).MATERIAL AND METHODS: Retrospective analyses of prospective database of 271 patients who underwent LPN and OPN for single tumors; solitary kidneys were excluded. RESULTS: 161 patients underwent LPN approach and 111 OPN approach. The OPN group was older, with poorer renal function and a higher ASA score than LPN group. The tumor size was clinically and statistic larger in the OPN group. The transoperative results were similar for operative time, warm ischemia time, estimated blood lost and positive margins. The hospitalization length and complication rate were higher in the OPN group. The OPN group did not have conversion to radical nephrectomy and the LPN performed one conversion to open partial nephrectomy and one to laparoscopic radical nephrectomy. CONCLUSIONs: Despite of the select biases, at our experience, patients underwent OPN have a longer hospitalization length of stay and had 4.5 times more complications.
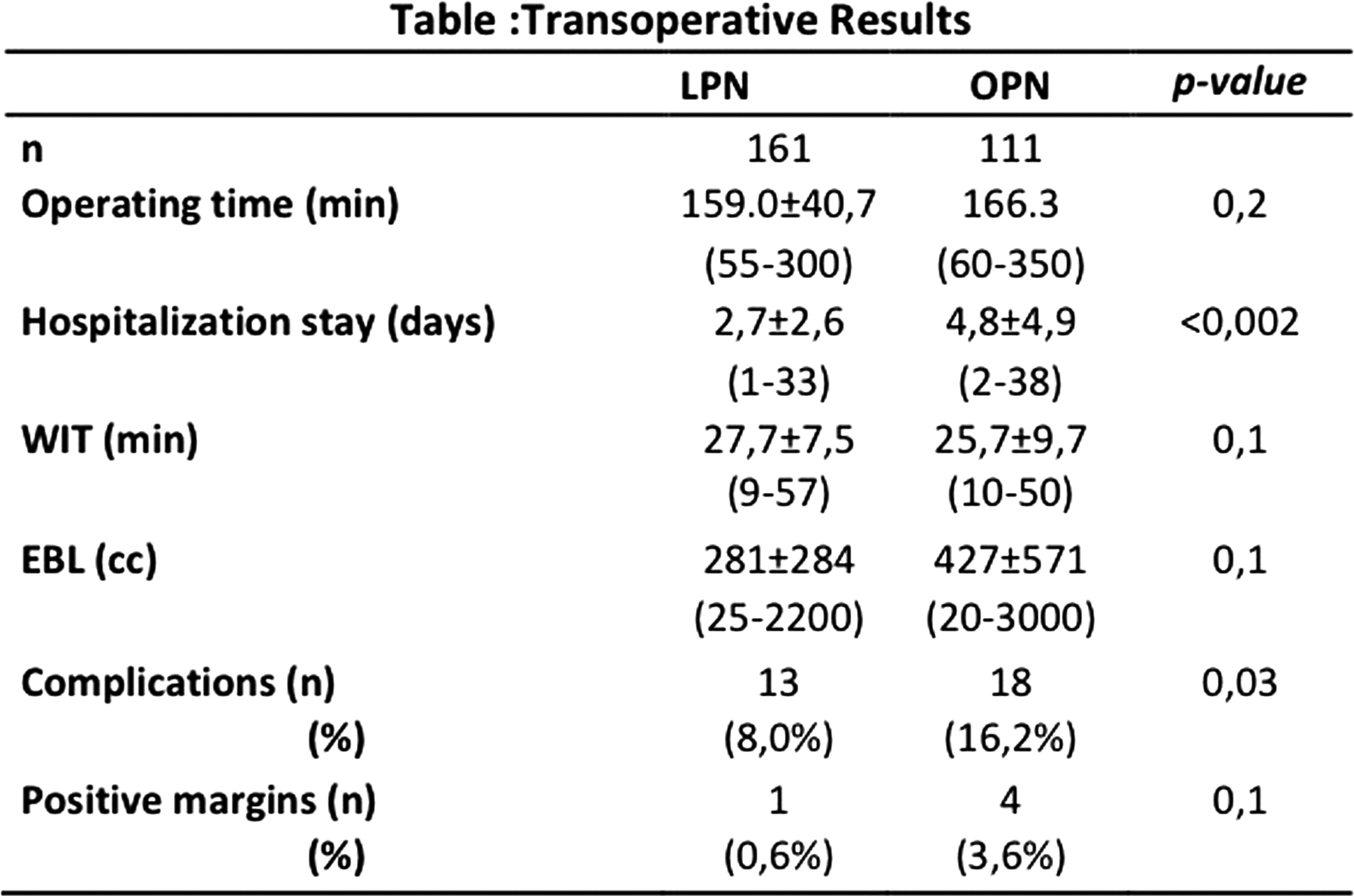
Influence of Nephrometry Score on the Incidence of Complication of Laparoscopic Partial Nephrectomy
<Introduction> Nephrometry scoring system has been introduced to quantitate the anatomical characteristics of renal tumors. High Nephrometry sum can be considered as the high complex tumors for partial nephrectomy. We examined the influence of Nephrometry score on the incidence of complication in laparoscopic partial nephrectomy.<Patients and Methods>From January 2005 until June 2011, 78 patients underwent laparoscopic partial nephrectomy with hilar clamping in our department. Of these, 44 patients had surface cooling with ice slush. <Results> The complication occurred in 7 patients (8.9%) during and after surgery, including urinary fistula in 3, psuedoaneurysm in 1, urinary retention in 1, intraoperative injury to tumor capsule in 1, intraoperative hemorrhage requiring transfusion in 1. Nephrometry score sum was 4 at 9% of the patients, 5 at 23%, 6 at 24%, 7 at 24%, 8 at 17%, and 9 at 3%. The incidence of complication according to Nephrometry sum was 20% in 4 points, 0% in 5, 14% in 6, 14% in 7, 10% in 8, and 0% in 9. There was no significant association between incidence of complication and Nephrometry sum (p=0.11). We also examined the influence of Nephrometry sum and each components on the incidence of complication with Clavien grade 3 or more, but could not find any significant relationship among them.<Conclusions>Nephrometry score was not significantly associated with the incidence of complication during laparoscopic partial nephrectomy in our experience.
Oncological Outcomes for Partial and Radical Nephrectomy for Renal Tumors from 4 to 7 cm.
Introduction: Partial nephrectomy for T1b is uncommon and most surgeons perform radical nephrectomy in this population. Purpose: to compare the early and intermediary oncological results of radical (RN) and partial nephrectomy (PN) for T1b.METHODS: From 2000 to 2010, a prospective database with116 patients with tumors from 4 to 7 cm (RN=75, PN=41) was evaluated. Both open and laparoscopic approaches were used. Clinical, laboratory and imaging evaluation was performed. RESULTS: No difference was observed among clinical variables evaluated (age, sex, ASA score, comorbidities, BMI and preoperative serum creatinine). Patients underwent RN had larger tumors (5,4 cm vs 4,8cm, p=0,006). The tumors on RN group were more frequently malignant (76% vs 61%, p=0,004), upstaged to pt3 (21,3% vs 0%, p=0,005) and had higher Fuhrman grade (17,2% Fuhrman 3 or 4 vs 0%, p=0,04). The 1-year overall survival (OS) in the RN group was 95,7%, recurrence free survival (RFS) 97,8% and no death related to disease (DRD) was observed. The 3-year OS in the RN group was 89,7%, RFS 96,6% and DRD 3,4%. No death or recurrence were observed in the PN group in the first 3 years of observation. Medium follow-up was 30,7 months. CONCLUSION: Partial nephrectomy is a feasible approach for managing renal tumors from 4 to 7cm and provide early and intermediary oncological results similar to radical nephrectomy
Influence of Nephrometry Scoring System on the Incidence of Complication of Laparoscopic Partial Nephrectomy
Objectives
Nephrometry scoring system has been introduced to quantitate the anatomical characteristics of renal tumors. High Nephrometry sum can be considered as the high complex tumors for partial nephrectomy. We examined the influence of Nephrometry score on the incidence of complication in laparoscopic partial nephrectomy.
Patients and Methods
From January 2005 until June 2011, 78 patients underwent laparoscopic partial nephrectomy with hilar clamping in our department. Of these, 44 patients had surface cooling with ice slush.
Results
The complication occurred in 7 patients (8.9%) during and after surgery, including urinary fistula in 3, psuedoaneurysm in 1, urinary retention in 1, intraoperative injury to tumor capsule in 1, intraoperative hemorrhage requiring transfusion in 1. Nephrometry score sum was 4 at 9% of the patients, 5 at 23%, 6 at 24%, 7 at 24%, 8 at 17%, and 9 at 3%. The incidence of complication according to Nephrometry sum was 20% in 4 points, 0% in 5, 14% in 6, 14% in 7, 10% in 8, and 0% in 9. There was no significant association between incidence of complication and Nephrometry sum (p=0.11). We also examined the influence of Nephrometry sum and each components on the incidence of complication with Clavien grade 3 or more, but could not find any significant relationship among them.
Conclusions
Nephrometry score was not significantly associated with the incidence of complication during laparoscopic partial nephrectomy in our experience.
Outcomes of Laparoscopic Partial Nephrectomy for Renal Tumors in the Past 10 Years
INTRODUCTION: Nephron sparing surgery has been used in the treatment of malignant and benign symptomatic kidney tumor. PURPOSE: Describe outcomes of laparoscopic partial pephrectomy (LPN) in the past ten years. MATERIAL AND METHODS: Retrospective analysis of a prospective database and descriptive statistical analysis of 166 tumors in 162 patients whom underwent LPN. RESULTS: Enhanced solid lesions comprised 75.8% of the operated tumors, the complex renal cysts 17.4% and the angiomyolipomas greater than 5cm comprised 6.6% of all tumors operated. The type of resection performed most of times was wedge resection (55.9%). The solid lesions less than 4 cm were found to be malignant in 83.4%, with renal cell carcinoma being the most prevalent tumor (69% of the malignant lesions). The average time of the surgery was 160 minutes, longer in the subgroup of lesions of greater than 4 cm and Bosniak IV complex cysts. The mean warm ischemia time (WIT) was 28 minutes. Most patients stayed in hospital for 2 days. One conversion to open partial nephrectomy and one to laparoscopic radical nephrectomy occurred in the time. The mean estimated blood loss was 300cc, 13 patients (8%) experimented complications and only 1 case of focally positive surgical margins. CONCLUSION: After 10 years of LPN in our institution, this technique is safe, feasible, with tolerable rate of complications.
Laparoscopic Partial Nephrectomy for Renal Cell Carcinoma: Analysis of Complication
Purpose: We compare intra and post-operative complication of laparoscopic partial nephrectomy(LPN) with open partial nephrectomy(OPN) and laparoscopic radical nephrectomy(LRN). Method: From February 2003 to June 2011, 68 patients underwent LPN, 27 patients underwent OPN and 77 patients underwent LRN for pre-operative diagnosis of clinical stage T1aN0M0 renal cell carcinoma. They were retrospectively evaluated. Result: Intra and post-operative complication rate of LPN, OPN and LRN were 10.3% (7 cases), 11.1%(3 cases) and 5.1%(4 cases), respectively. In comparison with other procedures, the complication rate of LPN was equivalent(OPN: p=0.85, LRN: p=0.61). Complications of LPN we experienced is shown below. Intraoperative bleeding occurred in 3 patients, resulting in OPN in 2 patients and LRN in 1 patient. 1 patient presented with hematuria due to arteriovenous fistula(AVF) 3weeks after LPN. Transcatheter arterial embolization of AVF was performed for the hemostasis. Other 3 cases underwent Grade1 complications. There is no case of urine leak. The decrease ratio of eGFR after LPN, OPN and LRN were 10%, 8% and 35% at 1 year after surgery, respectively. The decrease ratio of eGFR after LPN is significantly lower than that of LRN(p<0.001). All patients who underwent LPN are recurrence free within follow-up period. Conclusion: LPN is regarded as a procedure which is susceptible to complications. In our experience, LPN could be performed safely in appropriate methods and indications.
STILUS Academic Research Group (SARG). London. UK.
Introduction: The operating theatre (OT) is a complex platform. Its utility, especially when dedicated to laparoscopic and robotic urological surgery, poses special efficiency challenges. Purpose: To develop, apply and test the impact of a modified Lean and Six Sigma method on laparoscopic and robotic surgical theatre efficiency. Materials and Methods: We developed a linear pathway that traced patient journey from preoperative assessment till departure from OT and identified 6 zones of focus. Zone 1(preoperative check listing a week prior to the list such that chances of day-of-surgery cancellation were kept to a minimal),Zone 2(modified WHO Checklist done a day prior to day of surgery),Zone 3(minimizing net non-operating time [NNOT]),Zone 4(performance domains split into surgeon and nurse directed during the actual operation itself),Zone 5(communication platforms and recovery transfer domains to minimize exit from the OT) and Zone 6(represented a transition phase leading to optimal streamlining of process such that the net time of next case entry would be minimal). Data was collected over a 4-week period in a high volume tertiary referral military teaching hospital with a dedicated surgical platform for advanced upper tract laparoscopic and robotic urological surgery. Changes were structured and implemented in the six zones and impact tallied over a further 4-week period. Results:Following 6 zone process restructuring, a significant improvement in theatre efficiency was noted. There were no cancellations and theatre utility was 100% with a significant reduction of NNOT. Conclusions:Utilization of the modified Lean and Six Sigma approach led to increased efficiency in our dedicated OT.
Impact of Transition to Early Unclamping in Robotic Partial Nephrectomy
Introduction: Minimizing warm ischemia time (WIT) during robotic partial nephrectomy (RPN) reduces renal injury, but adequate renorrhaphy prevents complications. Early unclamping (EU) of the renal artery before completing renorrhaphy reduces WIT in laparoscopic partial nephrectomy. Robotics may also reduce WIT, but the impact of adding EU to RPN is unknown. Objective: We evaluated the impact of transitioning to routine EU by comparison with traditional renorrhaphy completion under ischemia. Methods: We reviewed 122 RPNs by a single surgeon (RA) excluding 29 off-clamp resections and one with renal arterial cold perfusion, leaving 54 EU and 38 non-EU procedures. Of the initial 40 procedures with clamping, EU was used only 2 times after which it became routine when clamping. Procedures with and without EU were compared. Results: There was no difference between groups in mean age, BMI, ASA score, or preoperative creatinine. Mean tumor size was higher for EU at 4.4cm (1.6-10cm) vs. 3.2cm (1.3-9.4cm) as was R.E.N.A.L. nephrometry score at 8.7 (5-12) vs. 7.2 (4-10) and frequency of collecting system entry (74% vs. 42%). Nevertheless, mean WIT trended toward shorter times with EU (p=0.09) at 15.2min (5.5-27.3min) vs. 17.0min (9.5-30.0min). There was no difference in mean blood loss, operative time, or postoperative creatinine (1.21 vs. 1.18). No EU patient had a positive margin, and only one required transfusion with 2 minor urine leaks. Conclusions: While WIT was not significantly reduced by EU, EU allowed larger and more complex RPN with uniformly<30min of WIT and a comparable average of only 15min.
Increasing Experience Leads to Decreased Warm Ischemia Times During Robotic Partial Nephrectomy
Introduction: Prolonged warm ischemia time (WIT) during partial nephrectomy has been associated with poor clinical outcomes. As robotic-assisted partial nephrectomy (RPN) grows in usage and popularity for the treatment of small renal masses, we must assess what roll experience plays in obtaining short ischemia times. Purpose: To evaluate WIT relative to case volume and surgeon experience.Methods: Retrospective chart review was performed on all patients undergoing RPN by a single surgeon from August 2008 until September 2010 using the daVinci Surgical System (intuitive Surgical, Sunnyvale, CA). Warm ischemia was accomplished with the use of laparoscopic bulldog clamps on the renal arteries and veins. A sliding hem-o-lok renorrhaphy was used on all patients.Results: 72 patients underwent RPN from August 2008-September 2010. Mean patient age, tumor size, BMI, and length of stay were 58 years, 2.8 cm, 30.1 and 2.4 days. 52 (70.1%) of tumors were renal cell carcinomas. Average WIT in the entire cohort was 17 minutes. From first to last, mean WIT per quartile of patients was 20, 18, 17, and 14 minutes (p=0.003). There was no significant difference in tumor size or rate of collecting system repair across the groups.Conclusions: WIT during RPN is dependent on a multitude of factors. Increased experience allows more efficiency and leads to decreased average WIT. As our average WIT continues to decrease, and has not yet reached a plateau, the exact number of cases needed to overcome the learning curve remains unknown.
Department of Urology, Hokkaido University Graduate School of Medicine, Sapporo, Japan
OBJECTIVE: Aiming to reduce warm ischemia damage, we introduced 15-minutes ice slush cooling in retroperitoneal laparoscopic partial nephrectomy (LPN). We evaluated the perioperative outcome and the midterm renal function after surgery.
METHODS: Seventy-one patients (pts) undergoing retroperitoneal LPN with ice slush cooling between 2003 and 2010 were included (median age 60 years, male/female=42/29). Perioperative outcomes were reviewed retrospectively. Total renal function was evaluated by the estimated glomerular filtration rate preoperatively and at the latest visit in 69 pts with more than 6 months follow-up. Split renal function was also evaluated by MAG3 scintigraphy preoperatively and 6 months postoperatively in 61 pts.
RESULTS: The median operative time was 246 minutes (range, 155-424). The median ischemic time, including the initial 15minutes hypothermia, was 57 minutes (range, 34-112). Complication occurred in 9 pts, including postoperative hemorrhage in 5 pts. Median baseline eGFR and last followup eGFR was 77.2 (range, 36.1-121.3) and 67.6 (range, 16.1-127.1) ml/min/1.73m2. In addition, median baseline split renal function (SRF) of affected kidney and 6 months postoperative SRF was 49.3% (range, 40.3-57.6) and 40.7% (range, 13.8-54.5).
CONCLUSIONS: The decrease of eGFR was consistent with the previous report from a high volume center (Gill et al, J Urol 2010), although the ischemic time was longer in our series. In addition, the decrease of split renal function of the affected kidney was small. These observations would support the effectiveness of hypothermia in LPN.
Department of Urology, Graduate School of Medical Sciences Kyusyu University
Introduction: To determine the cause of decreased renal function after partial nephrectomy, we analyzed the relation between the operative data and the postoperative recovery in affected renal function.
Materials and Methods: From May 2005 to December 2010, the pre- and postoperative(one week and three month after the procedure) renal function was evaluated by 99mTc-mercaptoacetyltriglycine(MAG3) clearance in 51 patients treated with OPN(n=24) and LPN(n=27). LPN were achieved via retroperitoneal(RPLPN;n=14) or transperitoneal(TPLPN;n=13) routes. Renal cooling was performed after renal hilar clamping in OPN and RPLPN, but not TPLPN.
Results: Ten patients(2 in OPN, 6 in TPLPN, 2 in RPLPN) had continuous decrease of renal function from 1 week to 3 month after partial nephrectomy. The laparoscopic procedure(vs. open,P<0.05) and warm ischemia(vs. cold ischemia,p<0.01) during renal hilar clamping resulted in the decreased renal function. In multivariate analysis, the renal cooling influenced the postoperative decreasing of renal function(p<0.01).
Conclusions: Successful preservation of renal function after PN depends on cold ischemia during tumor extraction. Cold ischemia during renal hilar clamping is recommended to avoiding deterioration.
Acute Kidney Injury and Long Term Renal Function in Patients Undergoing Surgeon Controlled Robotic Partial Nephrectomy
Introduction: The association between short term changes in renal function immediately following surgeon controlled robotic partial nephrectomy (RPN) have not been linked to long term functional outcomes. Purpose:To evaluate what perioperative parameters, including acute kidney injury (AKI), following RPN predict changes in long term renal function. Materials and Methods:Analyzing a prospectively maintained institutional review board approved database of 151 patients who underwent RPN by a single surgeon between March 2008 and June 2011 we identified 77 who had serum creatinine measurements greater than 3 months following discharge. AKI was defined as 25% decrease in MDRD calculated GFR at the time of discharge from the RIFLE definition. Median follow up was months (Range 3-36) Results:21 of 77 patients (27%) had AKI based on greater than 25% decrease in calculated GFR at the time of discharge (Median 31%, range 25-44%). Patient with AKI had a median 14% decrease (range 13% increase to 46% decrease) in estimated GFR as compared to those patient without AKI (median 4% decrease, range 50% increase to 64% decrease, p=0.01). On multivariate analysis including warm ischemia time, EBL, tumor size, and clamping technique, preoperative GFR and % change in GFR at discharge had the strongest association with change in GFR (p=0.0096 and 0.0207 respectively). Conclusions:Change in GFR at the time of discharge predicts worse renal function at three months. Patients who have AKI may require more frequent monitoring of renal function postoperatively to ensure maintenance of GFR.
The Comparative Study of Different Suture Techniques in Laparoscopic Partial Nephrectomy
Objects:We accumulate the experience on the laparoscopic partial nephrectomy of the earlier stage, and make some technical improvements to shorten warm ischemia time as possible as we can.We present the clinical data to compare the outcome of different suture techniques in laparoscopic partial nephrectomy.Methods:Between Nov. 2010 and May 2011, the same surgeon performed retroperitoneal laparoscopic partial nephrectomy for 38 patients with renal masses. They were divided into two groups due to the suture methods, one adopted interrupted suture for renal collecting system and renal parenchyma and the other adopted consecutive suture technique without knotting. Results:In the two groups, no obvious differences in renal arterial branches, intraoperative blood loss, postoperative time of lying in bed and drainage volume were observed. However, warm ischemia time of both groups had statistic difference: the group with interrupted suture (21-36 min), the group with suture technique without knotting (15-28 min) (p<0.05), and pathological margins of both groups were negative. No complications such as conversion to open surgery, secondary surgery and leakage of urine, etc. Conclusions:Consecutive suture technique without knotting is comparatively simple and can shorten the learning curve, which has a high value of clinical application. For suturing the collecting system, it is recommended to adopt interrupted suture technique.
Istanbul American Hospital, Istanbul, Turkey
OBJECTIVE: Robotic technique with its unique advantages allows safe tumor removal and reconstruction without renal hilar occlusion. Herein we evaluate operative outcomes among patients undergoing robotic nephron-sparing surgery (RNSS) without renal hilar clamping during the initial phase of our learning curve.PATIENTS AND METHODS: Between June 2010 and May 2011, 31 patients with upper urinary tract pathologies (24 kidney tumors) were managed with daVinci robot by a single surgeon (TE) highly experienced in open procedures. Out of 15 RNSS's, 11 were managed without renal hilar clamping under perfused conditions. The decision of not to clamp renal hilus was given during operation. Demographic data, and preoperative tumor size and location (assessed by R.E.N.A.L. nephrometry score) were retrospectively analyzed. Operative data, including mean operative time, estimated blood loss (EBL), and the presence of any complications, were reviewed.RESULTS: Mean age of patients managed under perfused conditions was 52.3 years, mean operative time 138 min, mean EBL 364 mL and mean hospitalization was 3.8 days. The median RENAL nephrometry score was 4. Pathology showed renal cell carcinoma in all patients; mean tumor size was 3.2 cm. Final pathological margins were negative in all patients. Adverse events included blood transfusion in 1 patient. Serum creatinine level slightly increased in 2 patients but returned to baseline during follow-up. CONCLUSIONS: Our preliminary data suggest that open surgical skills can be transferred to robotic technique and RNSS can be safe in selected patients without renal hilar clamping even in the learning curve with daVinci robot.
Zero Ishcemia Robotic Partial Nephrectomy
Exposing the kidney to worm ischemia is the main disadvantage of robotic and laparoscopic nephron sparing surgery. We describe our clampless robotic partial nephrectomy (CRPN). Material and Methods:We elected to avoid hillar clamping in 23 small exophytic renal masses out of 68 at our institute. We placed multiple 1- Vicryl sutures under the tumor bed using ultrasound guidance before resecting the tumors. A Hem-O-Loc clip was placed on the stitches on each side of the renal parenchyma under tenssion The renal function was assessed before and 6 weeks after surgery.Results:The mean OR time was 180 min, mean tumor size was 1.4 cm (range 0.8-2.7). The mean blood loss was 140 cc. The difference between the mean GFR before surgery (82 ml/min) and after surgery (74 ml/min) was not statistically significant (P<0.64). 20 patient had clear cell renal cell carcinoma on the final pathology. Two oncocytoma and one benign renal were diagnosed in the rest patients. All the surgical margins were negative in the surgical specimens.Conclusion:Utilizing clampless technique eliminate warm ischemia, spares the GFR, without significant blood loss. CRPN does not jeopardize the oncologic outcome of nephron sparing surgery in well selected patients.
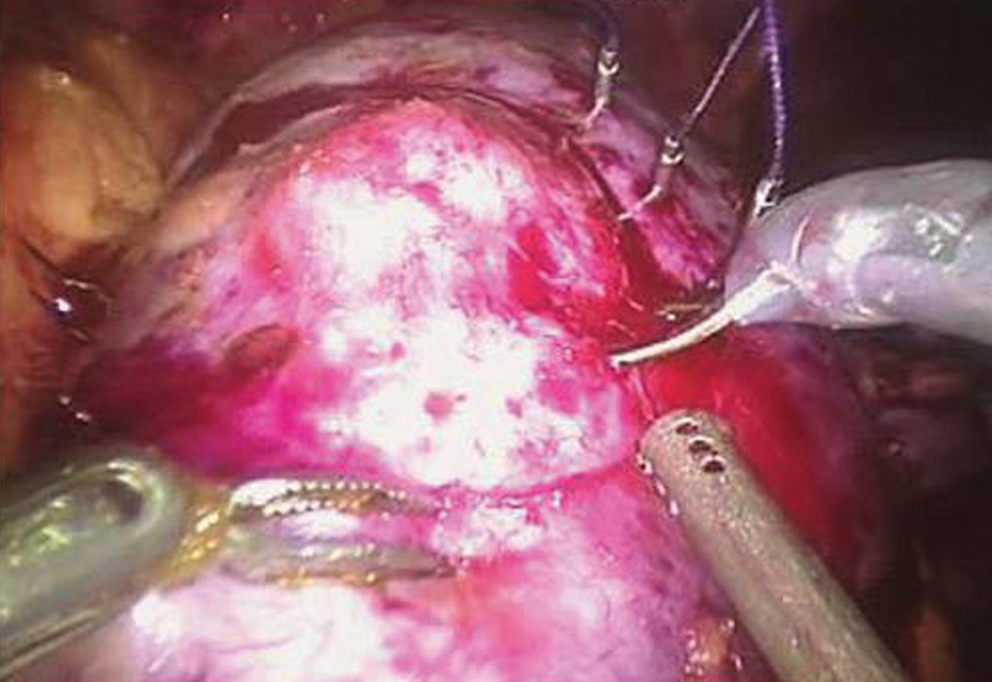
Selective Arterial Clamping with the Assistance of Near Infrared Fluorescence Imaging for Robotic Assisted Laparoscopic Partial Nephrectomy (RALPN)
ABSTRACT WITHDRAWN
MP32: Prostate, Minimally Invasive Therapy/New Technology/Imaging 2
Department of Urology, Graduate School of Medicine, Chiba University, Chiba, Japan
Purpose: alpha1-Adrenoceptor (alpha1-AR) antagonists are the main treatment for Benign prostatic hyperplasia (BPH), but there is no study the effect of alpha1-ARs on dilatation of the prostatic urethra as visual image in patients. To evaluate the effect of the alpha1-AR antagonist tamsulosin hydrochloride on the prostatic urethra in patients using a new software program that processes an opened, three-dimensional image of the urethra from a cystourethroscopic video image.
Materials and Methods: 25 BPH patients enrolled in this study. The opening image of the prostatic urethra was generated in all patients before and 1 month after the tamsulosin treatment (0.2 mg/day). The prostatic urethra was divided into five points from the verumontanum (Veru) to the bladder neck (BN), including the points (Veru), (A), (B), (C), and (BN). Urethral diameters were measured at each location before and after tamusulosin treatment, together with IPSS storage and voiding subscale scores.
Results: There was significant dilation at all 5 points after treatment (P<0.001). The greatest dilation was observed at verumontanum (119.6%), while the least was observed at bladder neck (107.9%). Patients with large urethral distension (n=14) showed significantly greater improvement of IPSS (P=0.0033) than those with small urethral distension (n=11).
Conclusions: To the best of our knowledge, this is the first study to demonstrate that tamusulosin mediates prostatic urethral opening in BPH patients, which was significantly correlated with improvements in voiding and storage symptoms. Thus, physiological opening of the prostatic urethra may be the key mediator of improvement of LUTS in BPH patients.
Length of Stricture: The Most Important Factor of Successful Holmium:YAG Laser Splitting Procedure for Urethral Strictures
Introduction: Holmium:YAG laser splitting procedure is popular for the treatment of urethral stricture for its mini-invasive feature. Purpose: To define the successful factors of urethral stricture Holmium:YAG laser splitting procedure. Materials and Methods: We retrospectively reviewed all 19 male cases with urethral stricture who had undergone holmium:YAG laser splitting procedures. The causes of stricture included: pelvic trauma, urethral trauma, post transurethral operations. The locations of strictures included: anterior and posterior urethra. Pre-, post-operation urethrography, urine flow rate were used to estimate the effect of splitting procedures. Success was defined as no obvious urethral stricture in urethrography and maximum urine flow rate more than 10ml/s. Average follow-up were 3.6 months. Research factors included: age, location of stricture, degree of stricture, length of stricture, cause of stricture, urine flow rate before operation.Results: successful holmium:YAG laser splitting procedure were achieved in 11 cases (57.9%). In univariate analysis, degree of stricture(p=0.021), length of stricture(p=0.001), urine flow rate before operation(p=0.045) were significant predictive factors. In multivariate analysis, only length of stricture (OR=2.378, 95%CI: 1.238-4.565) was significant predictive factors of successful holmium:YAG laser splitting procedure.Conclusions: Holmium:YAG laser splitting procedure has more than moderate success rate for urethral stricture. The length of ureteral stricture is the only predictive factor for the success of this procedure.
Prostatic Dynamic Contrast Enhanced Mr: Comparation Before and after HIFU Treatment for Prostate Cancer
To evaluate the diagnostic performance of the D-CE-MR in adenocarcinoma of the prostate before and after trans-rectal HIFU. Materials and methods:In 2009we analysed 25patients affected by prostate cancer (T1-T2). The average age was 70years (PSA value of 9.0-5.3 ng/ml Prostate volume of 28- 13 cm3 . All patients, , underwent transurethral resection of the prostate (TURP). PSA was evaluated at 1, 4 and 6 months after robotic HIFU. Results :Evaluation of the MR images: before, the intraglandular lesions, hypointense in T2-w sequences and hyperintense in the post-contrast adm.T1-w sequences, were sites of neoplasiain all 25 patients (p0.001). Evaluation of the MR images (1 mo. post rHIFU): in the CE-MRI, the region that underwent treatment showed in all 25 patients, a central portion without contrast uptake surrounded by a thin portion with an important contrast agent uptake (inflammatory condition). Evaluation of the MR images (4-6 mo. post rHIFU): the prostate presented a significantly reduced total volume (average61%), a signal hypointensity in the T2-w sequences and homogeneous contrast uptake of the glandular parenchima. Conclusions: Our results show that CE-MR can be ua non-invasive method, for the visualization of adenocarcinoma of the prostate. after HIFU treatment: regular trend with no rapid rise nor peaks of enhancement in the 1, 4 and 6 month MR evaluation. Correlation among MRI, PSA and TRUS to value the reduction of prostate volume. MRI as non invasive methodic for evaluating remaining illness. No positive biopsies at 6 mo.
USC Institute of Urology, Keck School of Medicine, University of Southern California Los Angeles, California, USA.
PURPOSE: Critical issue for focal therapy is patient selection. The aim was to define the role of TRUS-visibility of prostate cancer in candidates for focal therapy. METHODS: 93 potential candidates for focal cryotherapy underwent gray-scale and Doppler TRUS-guided biopsy by an expert. All real-time TRUS images were recorded and spatial mapping of TRUS-visible lesions and targeted sampling areas were individually documented. Data from the baseline imaging-targeted biopsies were compared to systematic (non-targeted) biopsies performed at outside institutions. Of the 93 patients, 75 patients with low- to intermediate-risk disease were eventually selected for focal cryosurgery. RESULTS: Among 93 patients, a total of 681 biopsy cores were available for analysis, including imaging-targeted (n=256, 37.5%) and systematic (n=425, 62.5%) cores. 65% (167/256) of targeted biopsy cores were positive for cancer, compared to 6.2% (26/425) in systematic (non-targeted) cores (p<0.001). 88% (82/93) of biopsy-proven cancer index lesions were TRUS-visible. Comparing TRUS-visible versus image-invisible index lesions, cancer-involved core length was 6.1 vs. 1.5 mm (p=0.0005), respectively. Furthermore, percent of core with involved cancer was 48% vs. 16 % (p=0.0008), and average Gleason score was 7.0 vs. 6.2 (p=0.0001). With increasing size of the TRUS-visible lesion (<10, 11-15, 16-20,>20 mm), cancer-involved core length and percent of core with cancer also significantly increased (p=0.009 and p=0.008, respectively). CONCLUSION: TRUS-guided targeted biopsies significantly improved detection and staging of higher grade and larger volume cancer, compared to image-blind (non-targeted systematic) biopsies. Image-visibility allows for more accurate cancer spatial mapping and likely more precisely targeted therapy and follow-up monitoring.
The Adequate Indication for Focal HIFU
Introduction: New concept of focal therapy as opposed to traditional radical treatment appeared in clinical practice. However, the ideal candidate for focal therapy remains unclear. Purpose: We evaluated the oncological results to establish the adequate eligible indication for focal HIFU. Materials and Methods: We included a total of 42 patients received focal HIFU using the Sonoblate device at our institution. Our inclusion criteria is as follows: men with unilateral prostate cancer on DRE and TRUS guided 12-core biopsy, PSA less or equal 20 ng/ml, Gleason scores less or equal 8. Follow-up criteria is DRE and PSA every 3 months and MRS and routine biopsy at 6 and 12 months after focal HIFU. Cox proportional hazards model was used to determine independent predictors of biochemical disease-free survival (DFS). Results: Median age was 71 years (range; 53-82). The median pre-HIFU PSA was 5.8 ng/ml (range, 1.768-20.0). The 5-year biochemical and pathological DFS rate in all patients was 53.3% and 70.0%, respectively. Results from univariable Cox proportional hazards models showed that Gleason score>7, PSA>10ng/ml, PSA velocity>2, and the meeting with Task Force criteria (cT1 or cT2a, PSA<10 ng/ml, PSA density<0.15 ng/ml/cc, Gleason grade<4 were independent prognostic factors for the 5-year biochemical DFS after focal HIFU. Results from multivariable Cox proportional hazards models showed that Gleason score>7 and PSA>10ng/ml were independent prognostic factors for the 5-year biochemical DFS after focal HIFU. Conclusions: The patients with Gleason score>7 and PSA>10ng/ml were good candidates for focal HIFU.
Prostate Cancer Detection Rates Using a MR/TRUS Fusion System: In Patients with a Previous Negative Prostate Biopsy
Objective We sought to determine the cancer detection rates using our MR/US fusion prostate biopsy platform in patients who have had at least one prior negative biopsy.MethodsRadiologists reviewed MR images from patients with suspicion or diagnosis of prostate cancer (CaP). Imaging consisted of T2, DCE, DWI, and spectroscopy images. All lesions were then identified and graded by number of modalities positive: low (<= 2), moderate (3) and high (4) suspicion. The protocol biopsy included a standard 12 core biopsy followed by a MRI/US fusion biopsy of the suspicious MR targeted lesions.Results 53 patients entered the study with at least one previous negative biopsy. The mean age was 61.6 years with a mean of PSA 14.0 ng/ml and median PSA 9.6 ng/ml. The detection rate for cancer in patients with one, two or three or more previous negative biopsy was 42.1%, 50.0%, and 55.6%, respectively. The overall cancer detection rate in patient with at least one previously negative biopsy was 49.1%. The standard biopsy missed 4/9 patients with high grade lesions. ConclusionPatients with a prior negative prostate biopsy, applying the imaging protocol, patients with at least one high suspicion lesion had an 84.6% incidence of CaP being detected on a protocol biopsy. This novel platform may be useful in patients with previous negative biopsies and a rising PSA. It is evident from this data that imaging does have an impact on cancer detection rates and even further identifying patients with high risk disease which had previously gone undiagnosed.
Fragmentation of Trans-Rectal Ultrasound Guided Biopsy Cores is Influenced by the Method of Specimen Retrieval
Introduction: Fragmentation of tissue at transrectal ultrasound guided biopsy can affect tissue quality and potentially also the assessment of cancer volume. This has implications for active surveillance protocols which have inclusion criteria stipulating the number of positive cores and/or percentage core involvement with cancerMaterials: Ninety patients undergoing tranrectal ultrasound guided biopsy were randomly assigned to having biopsy cores retrieved by either "swishing" into saline or being "swiped" onto paper before being placed into formalin solution.Results: 44 patients were assigned to the "swish" and 46 to the "swipe" group. There was no difference in mean prebiopsy PSA or in the rate of cancer detection between groups. The cancer patients in the swish group had both fewer and longer core fragments than the swipe group. The swish group cancer patients had fewer cores on final pathology (p=0.005). These cores had a mean length of 14.1mm, compared with 12.3mm in the swipe group (p=0.01). The fragmentation rate was significantly greater in the benign sextant locations (p=0.017). No significant difference in core fragmentation was noted between benign and malignant sextant locations when the 21 cancer patients were analysed on their own and there was no significant difference between groups when analysed according to Gleason score.Conclusion: Fragmentation of tissue obtained at TRUS biopsy can be affected by the method of tissue retrieval, with consequent implications for the choice of treatment offered to patients with low volume disease.
The Relationship of Prostate Volume, Prostate Biopsy Cores and Prostate Cancer (Pca) Detection Rate
Introduction: The cores of prostate biopsy have being increased. However, prostate cancer detection rate do not increase.Purpose: To investigate the relationship of prostate volume, prostate biopsy cores and Pca detection rate.Materials and Methods: A total of 292 patients underwent 12-core prostate biopsy from January 2007 to December 2009. Transrectal ultrasound was used to determine prostate volume. 12-core biopsy protocol originated from classic 6-core protocol. patients were divided into 4(less than30ml, 30 to 60ml,60 to 90ml,more than 90ml) groups according prostate volume, And then we compared the Pca detection rates of 6-, 8-, 10- and 12-core protocols. Results: The total Pca detection rate was 25.0% (73/292). In less than 30ml group, Pca detection rates were same between each protocols (39.13%, 21/54). In 30 to 60ml group, Pca detection rates of 6-core (21.3%, 23/108), 8-core (23.1%, 25/108), 10-core (23.1%, 25/108) and 12-core(24.1%, 26/108) protocols were not significantly different (p>0.05). In 60 to 90ml group, 6-core (12.9%, 12/93) protocol had significantly lower Pca detection rate (p<0.05) than 8-core (19.4%, 18/93), 10-core (20.4%, 19/93), 12-core (20.4%, 19/93) protocols. In more than 90ml groups, Pca detection rates of 6-core (8.1%, 3/37), 8-core (8.1%, 3/37) protocols were significantly lower (p<0.05) than 10-core (18.9%, 7/37), 12-core (18.9%, 7/37) protocols.Conclusions: Prostate volume could be an important factor for how many cores which we choice for prostate biopsy. Increasing cores would not improve Pca detection rate without considering prostate volume.
Department of Urology, Edogawa hospital, Tokyo, Japan
Introduction and methodThe current standard for diagnosing prostate cancer is based on random biopsies utilizing gray scale ultrasound. Although about 5% of cancers were confined to the TZ on random biopsies, 50% of all prostate cancer patients had TZ involvement. To detect TZ cancer, we made phantom of prostate cancer model and we developed new transurethral biopsy system with a tiny ultrasound transducer, a rigid Ultrasonic Probe. The probe enables to perform trans-urethral ultrasound-guided biopsy with a needle. To explore the medical benefits of the probe, a prostate model was also newly developed. MRI volumetric image was acquired from a normal case, the border of its prostate, rectum and urethra were traced. The model was produced using the trace dataset. 3 targets were embedded at anterior apex. The 3 targets, the prostate and the region around it, were separately colored to distinguish their specimens respectively by their colors after the biopsy. ResultsThe specimens were acquired under the trans-rectal biopsy. The specimens were easily sampled from the targets under the trans-urethral biopsy. The differences between trans-rectal biopsy and trans-urethral biopsy are distance and angle.The followings seem to cause the trans-rectal biopsy to be often performed unsuccessfully. Long distance of transrectal techinique causes the needle not the target. Small angle of transurethral technique causes the needle to sheer easily away from the target.
Does Prostate Biopsy Pose Problems in the Staging of Prostate Cancer by Magnetic Resonance Imaging (MRI) Scan?
Introduction: We conducted a prospective study to see if there is any difficulty in the interpretation of MRI scan following (TRUS) guided prostate biopsy.Methods: This study includes 101 patients from May 2008 to June 2010. MRI scan was performed 25 to 35 days following prostate biopsies. TRUS biopsy procedure was carried out using B & K medical ultrasound scanner no.2002 (Panther unit) using Biplanor rectal probe (8551). The usual number of cores of biopsies taken varied from 14 to 22 depending on the size of the gland.Results: The average time between biopsy and MRI scan was 30.63 days. (Median 30 days, range 25-35). Post biopsy haemorrhage was not seen in the scan in 79 (79%) patients and minimal haemorrhage in 19 (19%) patients and it did not interfere in the staging. of MRI scan. Significant residual haemorrhage was seen only in 3 (3%) patients and it did not correlate with the age or size of the prostate.Statistical analysis with t-test showed no significant difference between age, days of post- biopsy, Gleason grade and PSA of patients with and without haemorrhage. Patients with haemorrhage on MRI were statistically more likely to have low stage disease (T1, T2 VS T3, T4, p=0.02) on chi square test as patients with low stage disease required more cores (maximum 22) for the diagnosis.Conclusion: This study suggests that MRI scan done within 25 to 35 days of TRUS biopsy did not lead to any significant difficulty in interpretation of the scan.
18F-Choline PET/CT for Early Detection of Prostate Cancer Recurrence after Radical Prostatectomy
Introduction: The role of 18F-Choline PET-CT for detection of recurrence after radical prostatectomy is controversial. Methods: Between March 2007 and December 2010, 445 patients with biochemical recurrence underwent 18F-Choline PET-CT. Exclusion criteria were previous radiotherapy or systemic therapy after PET-CT. Two hundred-eightyfour patients with median PSA value of 1.4ng/mL (IQR 0.6-3.7) were selected for analysis. Positive PET-CT results were confirmed with histology (biopsy, lymphnode dissection) or with PSA levels following targeted treatment of lesions identified with PET-CT (when site was not suitable for biopsy) and negative PET-CT findings was confirmed with PSA-velocity. Results: Sensitivity, specificity, PPV and NPV were 85.7%, 82.3%, 98.7% and 26.9%, respectively, while in a subgroup of patients with PSA level<1ng/mL not receiving hormonal treatment were 73.4%, 78.5%, 94% and 39.2%, respectively.All findings, stratified on PSA levels, and separately evaluated in patients receiving androgen deprivation treatment, were summarized in table 1. Conclusions: 18F-Choline PET/CT in patients with PSA<1 ng/mL showed a PPV of 94.9% and a NPV of 40.6%. A 73.4% sensitivity rate in patients not receiving hormonal treatment with PSA<1 ng/mL allows to early detect and selectively treat recurrences with surgery or radiotherapy, avoiding or delaying systemic treatment.

Department of Urology, Teikyo University, School of Medicine, Tokyo, Japan
Introduction: The objective of this study was to evaluate the diagnosis capabilities of 1H-MRS for the accurate detection of the results with histopathologic examination results. Materials and Methods: This study included 42 patients with localized prostate cancer who underwent radical prostatectomy as primary therapy. Preoperative analysis of 1H-MRS was compared with the histologic Gleason score findings to determine the accuracy of 1H-MRS for the distribution of prostate cancer. 1H-MRS was conducted prior to the biopsy procedure, and any region in which the [choline + creatine]/citrate (Ccr) ratio was greater than 1.07 was considered positive for cancer. Results: The median age of the patients was 64 years (range, 52-72 years). The median period from 1H-MRS to radical prostatectomy was 5 days (range, 1-137 days). The median PSA level was 9.3 ng/ml (range, 3.2-46.0 ng/ml). According to the microscopic examination, 109 discrete prostate cancer lesions (mean; 2.6 lesions/prostate) were diagnosed by the pathologist. Gleason scores of each lesions were as follows; <=3+3 57lesions (52.3%), 3+4 30lesions (27.5%), 4+3 9lesions (8.3%), >=4+4 13lesions (11.9%). There are significant correlations between Gleason score and Ccr ratio (mean: <=3+3; 1.07, 3+4; 1.86, 4+3; 1.96, >=4+4; 2.12, P=0.0000). Conclusions: Our data suggest that 1H-MRS is a useful noninvasive diagnostic modality to predict Gleason score of small daughter lesion in patients with localized prostate cancer.
Multiphoton Microscopy for Identification of Prostatic and Periprostatic Structures in Human Radical Prostatectomy Specimens
INTRODUCTION AND OBJECTIVES: The aim of this study was to assess the potential of Multiphoton Microscopy (MPM) to provide virtual histology as a proof of principle for real-time imaging during nerve sparing radical prostatectomy and for MPM guidedbiopsy.METHODS: We used two types of specimens for imaging: (1) intraoperative margins and biopsies; (2) tissue sectionsobtained from the excised prostate. The imaging was carried out using intrinsic fluorescence and scattering properties of the tissueswithout any exogenous dye or contrast agent. A custom-built MPM, consisting of an Olympus BX61WI upright frame and a modifiedBio-Rad MRC 1024 scanhead was used. The corresponding tissues were subjected to hematoxylin and eosin staining for histologicconfirmation of the structures.RESULTS: High-resolution images of the periprostatic tissue, nerves, prostate capsule and individual acinar cells were obtained at varying magnifications. Histologic confirmation of the periprostatic tissue, prostate gland, fat, blood vessels, and nerves validated the findings of MPM.CONCLUSIONS: We have utilized a novel approach for tissue imaging which appears to provide microscopy levelresolution in fresh tissue. This may allow more accurate surgical decisions during nerve sparing radical prostatectomy and also improve the accuracy of prostate biopsy, once the technology is clinically translated.
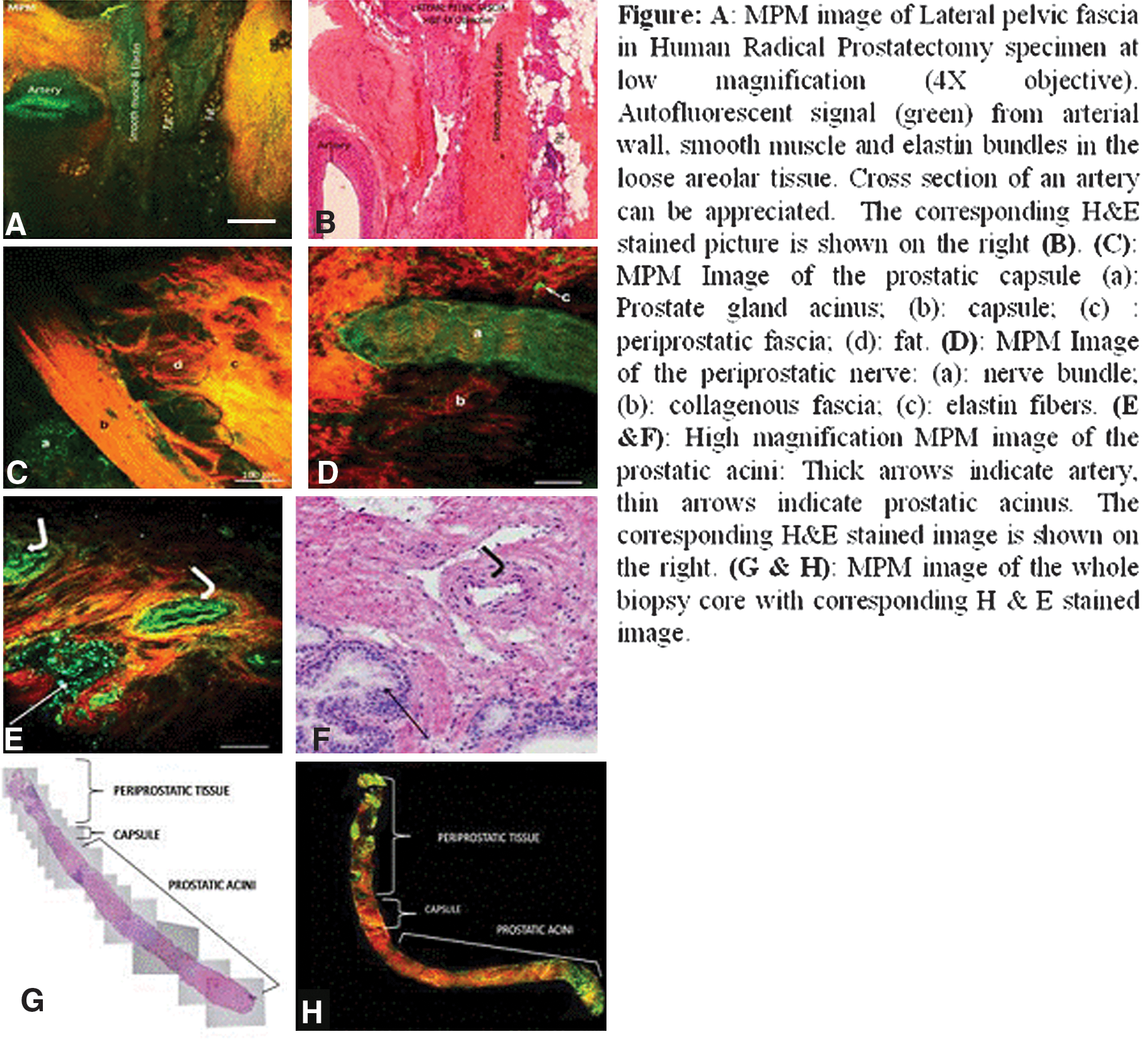
Dept of Urology, Akdeniz University, Antalya, Turkey
Introduction: The most common treatment of Prostat cancer (Pca) is radical prostatectomy (RP). Low recurrence rate depends on detecting positive surgical margins (PSM) in RP. Currently, intraoperative frozen pathology are used to detect PSM. However, it has low sensitivity and specificity. Propose: Elastic light single-scattering spectroscopy (ELSSS) system has been evaluated in differentiation between cancerous (CPT) and noncancerous prostate tissues (NCPT) at surgical margins. In the study, it has been shown that this system can differentiate CPT from NCPT.Materials and Methods: ELSSS with a single optical fiber probe was employed to differentiate CPT from NCPT ex-vivo just after RP. First, ELSSS spectra were acquired from CPT to define its spectral features. Then, spectra were acquired from surgical margins of excised prostate tissue to detect PSM based on the spectral features of the spectra taken from CPT. Of the total 128 tissue samples were evaluated from 18 patients by ELSSS system.Results: Comparing of histopathology results and ELSSS measurements revealed that sign of the spectral slopes of CPT is negative and NCPT is positive in the wavelength range from 450 to 750 nm. Sign of the spectral slopes were used as a discrimination parameter between CPT and NCPT. Based on the correlation between histopathology results and sign of the spectral slopes, ELSSS system differentiates CPT from NCPT with a sensitivity of 0.97 and a specificity of 0.87. Conclusions: Developed spectroscopic system has a potential to be used detection of PSM in real time with a high sensitivity and specificity.
Novel Robotic Real-Time Targeted Near Infrared Fluorescence Detection in a Mouse Model of Prostate Cancer
IntroductionReal-time intraoperative fluorescence-imaging of prostate tissue could potentially enhance preservation of structures surrounding the gland and decrease positive margins of radical prostatectomies.Purpose To evaluate real-time NIR-fluorescence detection from prostate tumors stained with a PSMA-targeted tracer developed at our Institution with the novel Intuitive Surgical da Vinci® Fluorescence Imaging Vision System.Materials and Methods PC3-pip(PSMA-positive) and PC3-flu(PSMA-negative) prostate cancer cell-lines were implanted subcutaneously into 6 immunodeficient mice. When tumors reached 5mm, a PSMA-targeted fluorescent conjugate was injected through the tail vein. The first 3 mice were imaged immediately and at 1-hour intervals after IV-injection for up to 4h to determine the time to obtain optimal signal intensity and were euthanized. The last 3 mice were imaged once preoperatively, immediately after IV-injection and were euthanized 120min later. Dissection and excision of the implanted tumors in the carcasses of the last 3 mice were performed by using a new robotic imaging system to detect NIR fluorescence in real time. Specimens were submitted for pathologic analysis.Results We were able to detect fluorescence from the PSMA-positive tumors in 2 of 3 mice. In the PSMA-negative tumors, no fluorescence was identified. Pathology confirmed prostate cancer and negative margins in all PSMA-positive tumors. One of the PSMA-negative tumors had positive margins.ConclusionsReal-time NIR-fluorescence imaging of prostate cancer was feasible with a novel robotic system. Further research is needed to optimize the signal intensity detectable from prostate cancer with our fluorescent PSMA-targeted agent. Toxicological studies are needed prior to clinical use of this tracer.
The da Vinci Robot Overcomes Innate Hand Dominance Among Surgeons
Background:The robotic surgical platform has allowed for improved ergonomics, tremor filtration, motion scaling, and increased precision during minimally invasive surgery. Through a synergism of these effects, additional beneficial aspects of the robotic platform may be realized. Purpose:We examined the impact of the da Vinci Surgical System (dVSS) on the lateralization of manual dexterity (or handedness), innate to most surgeons.Methods:All subjects enrolled in the study (19 robotic novices) initially completed a 30-minute robotic basic skills training session. After completing this standardized introduction to the functionality and capabilities of the dVSS, subjects underwent manual dexterity testing using the Purdue Pegboard test and a Needle targeting test; conducted both in the open and robotic platforms. Manual dexterity test scores were then compared among all subjects.Results:The majority of subjects (84%) were right handed and all subjects described their dominant hand as significantly or moderately more dexterous than their non-dominant hand. The participants had significant differences between the dominant and non-dominant hand in open skills testing using the Purdue Pegboard test (15.5 vs 14.6 pegs, p=0.023) and needle targeting test (4.5 vs 3.7 targets, p=0.015). When performing the same tasks using the robot, differences between hands were no longer observed. (1.8 vs 2.1 pegs, p=0.203; 3.2 vs 3.1 targets, p=0.764)Conclusions:The dVSS is capable of compensating for innate dexterity or handedness among novice surgical trainees. This provides evidence of another beneficial aspect of robotic surgery over traditional open surgery and may facilitate operative performance of complex tasks.
Urology Department, Lukas Hospital Neuss, Neuss, Germany
Purpose: In this study we investigated the sphincteric/perisphincteric lesions and alterations in patients with iatrogenic damage to the external urethral sphincter and consecutive urinary incontinence after radical prostatectomy.Patients and Methods: A total of 169 patients with postprostatectomy urinary incontinence, referred from different 28 German hospitals have been evaluated from December 2004 to March 2009. Patients were elegible when presenting with refractory grade III stress urinary incontinence and duration of incontinence of at least 12 months. Patients underwent clinical, ultrasonographic examination, urethrocystoscopy, and if technically possible, urethrocystomanometry.We classified and evaluated sphincteric defects with regard to type and localization.Results: Mean duration of incontinence before evalulation was 44.8 months. Prostatectomy technique were as follows: 66.9% retropubic RP, 27.8% laparoscopic RP, 3.5% perineal RP, and 1.8% robot-assisted RP. A sphincter transection was seen in 65.1% (110/169) of cases, a sphincter penetration in 46.2% (78/169) of cases. A combination of both sphincter injuries was seen in 37% (63/169) of patients. In 87% (147/169) of the cases, the sphincter defect was localized to the lower circumference, and in 13% (22/169) of cases, to the upper circumference. A stricture of the vesicourethral anastomosis was found in 45% (76/169) of cases.Conclusions: Direct iatrogenic damages to the urethral sphincter may cause postprostatectomy urinary incontinence. They seem to follow a particular local distribution pattern. Cystoscopic evaluation of the sphincteric region in incontinent patients after surgery may be a valuable tool for examination.
Urology Department, Lukas Hospital Neuss, Neuss, Germany
Purpose: Postprostatectomy urinary incontinence may be caused by iatrogenic sphincter lesions. We investigated the effect of early endoscopic suture removal in patients with sphincter penetration with suture material during previous radical prostatectomy.Materials and Methods: Among 374 patients who had undergone radical prostatectomy from 2005 to 2009 at our institution we identified 19 cases with the symptomatic trias of urinary incontinence, reduced uroflow and residual bladder volumen after catheter removal, assumed indicative for sphincter penetration. Patients presenting this trias underwent endoscopic evaluation of the sphincter region. At presence of the suspected sphincter penetration, the transsection and removal of the sutures were performed on the subsequent day.Results: In 79% (15/19) of the patients exclusive sphincter penetration by suture material was detected whereas 21 % (4/19) showed additional sphincter transection. The suture penetration was observed predominantly in 3"(7/19) and 6"(8/19) position, in two cases each we could see the penetration in 12/6" position, respectively. The 4 concomitant sphincter transections were seen in the lower circumference. All treated patients with sphincter penetration only, were continent after the procedure. At a follow-up of 6 months the respectively treated patients remained continent. Two of 4 patients with combined sphincter damage not benefitting from the endoscopic suture removal were successfully treated by autologous transplantation of muscle derived cells whereas 2 patients received an artificial sphincter system.Conclusion: Reduced uroflow, residual volumen plus incontinence may indicate sphincter penetration by anastomosis sutures. Early transurethral removal of the sutures decreased the incontinence rate to 1% (4/374).
MP33: BPH laser 2
Division of Artificial System Science, Graduate School of Engineering, Chiba University, Chiba, Japan
Background: Reconstruction of 3D structure of the intraluminal cavity of the prostatic urethra would be one of potent approaches for estimating voiding dysfunction in BPH patients. We had developed a method for process virtual urethroscopy from actual cystourethroscopic video. Further we developed another method to simulate urine flow on the processed virtual urethroscopy, and tested the validity of the method using video files of the BPH patients before and after administration of alpha1-blocker in comparison to voiding parameters.Materials and Methods: Virtual urethroscopic images were processed in five patients with BPH from cystourethroscopic video files under approval of local ethic committee. The 3D structure of intraluminal cavity was reconstructed using CAD software, then fluid flow simulation was carried out in each patients.Results: Overt vortex of the urine stream was observed at the distal part of the prostatic urethra and was reduced after administration of alpha1-blocker in every five patients. Reduction of IPSS score was clearly corresponded with that of vortex.Conclusions: Hydraulic simulation of urine in the prostatic urethra using cystourethroscopic image processing would be a promising method for estimating voiding dysfunction and pharmaceutical effects in patients with BPH.
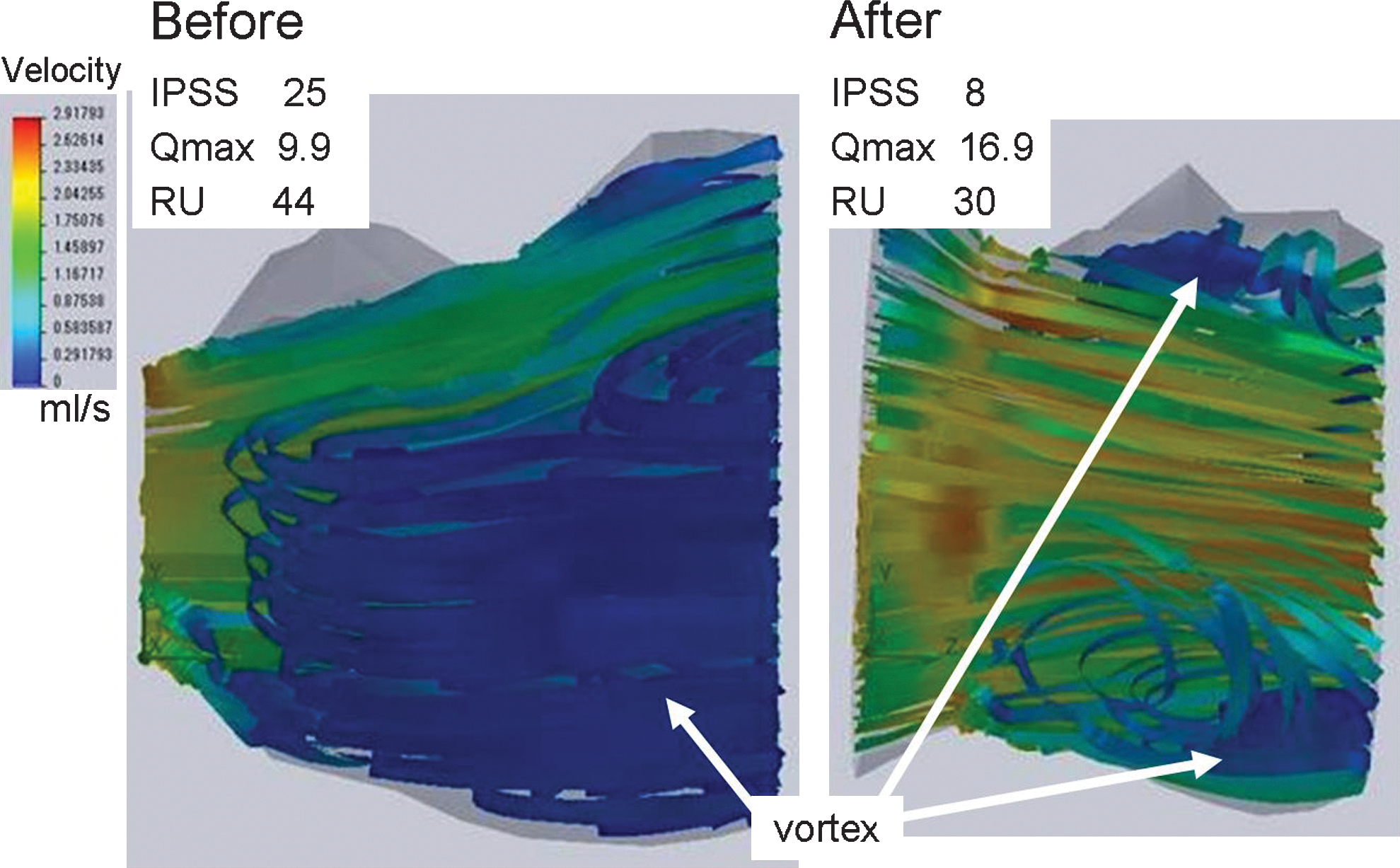
Holmium Laser Enucleation of the Prostate (HoLEP): A Surgeon's Initial Experience
HoLEP is an excellent surgical treatment for patients with lower urinary tract symptoms due to benign prostatic hyperplasia(BPH), but it has not become widespread because of the prolonged learning curve.
After observing 2 performances of experts, HoLEP was introduced at our institution. Our aim is to evaluate the safety and efficacy of HoLEP performed by a single surgeon (Omori).
From January 2010 to April 2011, HoLEP was performed in 70 consecutive patients. Pre and post operative international prostate symptoms score (IPSS), Quality of life (Qol), maximum flow rate (Qmax) and post-voiding residual urine volume (PVR) were recorded. Intra and post operative complications were assessed.
The mean age of patients was 72.6 years. Mean prostate volume was 62.3ml and mean enucleated tissue weight was 27.9mg. Pre and post operative mean IPSS was 18.7 and 6.4, mean Qol was 4.4 and 1.8, mean Qmax was 8.6 and 19.1 mL/sec, mean PVR was 127.4 and 20.7ml respectively. The mean hemoglobin change was 1.0 g/dl. Intraoperative complications were bladder injury (3), morcellator dysfunction (4). Postoperative complications were urinary retention (4), urinary tract infection (4), sepsis (1), urethral stricture (2). Stress urinary incontinence at the time of hospital discharge and post operative 3 months were 27 and 3 cases respectively.
Until reaching the learning curve, we have experienced some complications. By observing experts' operations and videos and continuing surgical procedures carefully, HoLEP has become a safe and effective technique for surgical treatment of BPH.
HoLEP/Antiageing/Testosterone
In Teikyo University urology, we do HoLEP from October, 2006.We paid attention to that we caused increase of voided volume as well as a discharge symptom.We supposed that there was connection with vesical chronic ischemia, and the collection of urine disorder measured bladder blood flow after HoLEP . We reviewed it for 118 cases during a HoLEP operation case by the bladder blood flow measurement.Furthermore, HoLEP was preoperative, and a change of serum testosterone value measured a change of IIEF5 again by after an operation.We recognized serum testosterone value, a rise of free testosterone value more significantly from after an operation.In addition, it increased about IIEF5 more postoperative three months later, and maintenance of a reproductive function, potency of amelioration were suggested.As for the HOLEP operation, the potency that it could be it was suggested for a male anti-ageing operation as well as an urination symptom, improvement of a lower urinary tract symptom such as a collection of urine symptom by amelioration of bladder blood volume, amelioration of serum testosterone value, amelioration of IIEF 5.

Assessment of Learning Effect in Holmium Laser Enucleation of the Prostate (HoLEP) by a Single Endourologist
Objective: To assess the learning effect in HoLEP performed by a single endourologist.Methods: Urination parameters in 580 patients with benign prostatic hypertrophy who underwent HoLEP at Hiratsuka City Hospital were assessed based on the number of patients operated on. Their mean age at the time of surgery was 71.2 years, the mean preoperative PSA level was 6.0 ng/mL, the mean estimated prostate volume was 60.7 mL, the mean weight of enucleated tissue was 33.4 g, and the mean operating time was 75.7 minutes. The 580 consecutive patients were divided into groups of 100 patients; then, enucleation and morcellation efficiency, as well as preoperative and postoperative IPSS, QOL, Qmax, and Hb decrease, etc., were determined.Results: Regarding the learning effect of surgery, enucleation and morcellation efficiency improved as more patients were operated on (P<0.05). The correlation coefficient was 0.272 and 0.315, respectively. Although no significant difference in postoperative IPSS, QOL or Qmax was noted among the groups, there was a trend toward improvement. There was no significant difference in Hb decrease either.Discussion: The results suggest that as the number of patients operated on increases, an endourologist can perform HoLEP more efficiently, as indicated by enucleation and morcellation time decrease. Postoperative IPSS, QOL and Qmax also tended to improve as more experience was gained. Since no significant difference in Hb decrease was observed from the early stage of experience with the procedure, we believe that an endourologist can soon perform HoLEP safely.
Holmium Laser Enucleation of the Prostate (HoLEP) for Glands Larger than 200 Grams
Introduction: Holmium laser technology has allowed for enucleation of large glands with outcomes equivalent or superior to those of open prostatectomy.Purpose: Describe our experience with HoLEP for glands>/=200 grams.Methods: Between January 1999 and February 2011, 58 patients with glands >/=; 200 grams underwent HoLEP. Mean age was 72.6 years. Mean pre-operative values include transrectal ultrasound (TRUS) volume of 218 cc, AUA symptom score (AUASS) of 18.9, Qmax of 7.5 ml/sec, post-void residual (PVR) of 237.6 cc and PSA of 19.9 ng/mL. 29% (17/58) patients required catheterization pre-operatively. Results: Mean enucleation and morcellation times were 86.7 min and 49.3 min. Mean enucleation and morcellation efficiency were 2.8 g/min and 6.3 g/min. Mean tissue removed was 213.4 grams. Two patients (3.4%) required perineal urethrostomy. Eight patients (13.8%) had concomitant procedures (bladder neck incision (2), cystolithopaxy (5), bladder biopsy (1)). One patient (1.7%) each required cystotomy for tissue retrieval, same-day take back for clot evacuation and take back 48 hours post-operatively to complete morcellation. Mean pre- and post-operative hemoglobin were 14.1 g/dL and 11.5 g/dL. Two patients (3.4%) required transfusion (mean 4 units). Mean catheterization time was 19.9 hours and all patients voided spontaneously post-operatively. Mean AUASS at 12 months was 3.86 and mean PVR at 12 months was 34.9 cc. Mean PSA at 6 months was 0.85 ng/ml (mean reduction 87.4%). One patient (1.7%) developed a urethral stricture and 0 patients required secondary procedures.Conclusion: HoLEP can be safely performed in patients for glands>/=200 grams.
The Department of Urology, King's College Hospital, London, UK
Introduction:We present the preliminary results of the first multicentre prospective study of prostate vaporisation and enucleation using the Evolve 150W diode laser at two wavelengths (1470nm and 980nm) in men with benign prostatic hyperplasia (BPH).
Methods: 49 patients in four international centres were treated for lower urinary tract symptoms suggestive of BPH. Prostate volume, IPPS, IIEF, flow rate and PSA values were measured preoperatively and at 3months. Mean age was 67 years (50-86). 16 (33%) were in retention at the time of the surgery, and 22.4% (n=11) were taking antiplatetet medication. Contact vaporisation technique was used to give a TURP-like cavity. Postoperative irrigation was not used routinely.
Results: All patients voided successfully post-surgery. Median catheterisation and hospitalization times were 14hours. At 3month follow-up, significant improvements were observed in IPSS, QOL, RV and Peak flow. Mean prostate volume reduced significantly from 63cc to 33cc. Only one patient (2%) needed bladder irrigation for more than two hours. No patients underwent transfusion, return to theatre, or experienced TURP syndrome. We have not observed stress incontinence or new erectile dysfunction.
Conclusions: Evolve dual 150W laser prostatectomy provides safe and effective treatment of patients with lower urinary tract symptoms and urinary retention. It can be safely carried out as a day surgery procedure, often without a catheter. In this multicentre study we have shown results similar to those expected with TURP, with excellent safety characteristics. We found the learning curve short and the procedure intuitive for both senior urologists and trainees.
Safety and Efficacy of Eraser Laser Enucleation of the Prostate (ELEP), Preliminary Report
PurposeTo ascertain the safety and efficacy of a 1,318-nm diode laser for transurethral enucleation of the prostate. The Eraser laser has been successfully used to resect lung metastasis. It has been recognized to cut and coagulate vascular rich tissue safely and effectively. We describe a prospective randomized trial of Eraser enucleation (ELEP) of the prostate versus bipolar transurethral resection of the prostate (TURP). Materials and MethodsA total of 60 patients with lower urinary tract symptoms suggestive of bladder outlet obstruction and a mean prostate size of 59.5 ml on transrectal ultrasound were randomized to ELEP or bipolar TURP. Patients were assessed preoperatively and at 1 and 6 months postoperatively.ResultsELEP was equivalent to bipolar TURP in terms of improvement in IPSS, maximal flow rates and quality of life. ELEP was significantly superior to bipolar TURP for measured blood loss (116.83±97.02 vs 409.83±148.61ml, p<0.05), catheter time (32.80±8.74 vs 65.73±13.72 hours, p<0.05) and hospital time (45.13±14.77 vs 91.20±11.76 hours, p<0.05). Using the validated Clavien-Dindo system there were 3 grade Id complications and 1 grade II complication. ConclusionsELEP and bipolar TURP were equally safe and effective. ELEP has the advantage of less blood loss, shorter catheter time and hospital stay.
Laser Enucleation of the Prostate with New 120W Thulium Laser Device: First Clinical Results
Introduction: We report our initial experience with laser enucleation of the prostate using a novel 1.9μm thulium laser.Methods: We report our initial experience with the first 30 patients undergoing thulium laser enucleation of the prostate in our department using the Vela XL at a wavelength of 1.9microm. Results: 30 consecutive patients (mean age 74±8 years) with a prostate volume of 98±70 cc undergoing thulium laser enucleation of the prostate between 5/2010 and 3/2011 in our department by a single surgeon were prospectively evaluated. In a mean operation time of 149±54 min 51±42 g tissue were enucleated. 13 of 30 patients (43%) presented in urinary retention, the others displayed a max. flow rate of 6.7±3.2 ml/s and a post void residual volume (PVR) of 110±109 ml preoperatively. Max. flow rate and PVR were improved to 16.9±5.1 ml/s and 27±26 ml, respectively. 2 patients (6.7%) displayed high PVRs and were discharged with a suprapubic catheter. Complications included bleeding requiring coagulation and transfusion in 2 (6.7%), fever in 2, temporary re-catheterization in 2, grade I-II stress incontinence in 1, postoperative hydronephrosis in 1 and myocardial infarction in 1 patient. Morcellation was postponed because of device malfunction (2 patients), prolonged OR-time (2 patients) and bleeding impairing visibility (1 patient). Mean catheter time was 3.0±1.0 days and hospital stay was 5.3±1.1 days.Conclusion: Thulium laser enucleation of the prostate with the Vela XL is a safe and efficient treatment modality for laser enucleation of the prostate in large prostates.
Bipolar TURP vs HoLEP: Selective Improvement after 1yr Follow-Up. Comparative Analysis of Two Learning Curves
INTRODUCTION:Traditional monopolar TURP has evolved to other minimally invasive surgical techniques for treatment of benign prostate obstruction, expanding their indications with promising results.Complications in the learning curves should be critically analysed.PURPOSE: Analyse and compare the impact of the learning curves of Bipolar TURP(B-TURP) and HoLEP by two self-taught urologists: functional outcomes and complications at 1yr follow-up. MATERIAL AND METHODS:HoLEP(Lumenis VersaPulse 100W) was performed from 2006 to 2008 by one surgeon. Since then, another surgeon began with B-TURP(TURis SurgMaster UES-40).We analyse the 65 firsts procedures of each one.RESULTS:Preoperative variables (age, prostate volume,Qmax,PVR,IPSS) in both groups were similar, with no statistical differences.Operative time was 64min in B-TURP Vs 124min in HoLEP (p<0,05).Tissue weight ressected was 24gr(B-TURP) Vs 32gr(HoLEP) (p:ns), hospital stay was 27h(B-TURP) Vs 35,5(HoLEP (p:ns). At 1yr follow-up, major complications requiring surgery were 0 in B-TURP and 9 in HoLEP (urethral stricture(2), bladder neck contracture(4), artificial sphincther(1),persistent prostate obstruction(2), plus 7 more cases waiting for surgery at 1yr follow-up cut-off. Incontinence rates at 1yr were 0%(B-TURP) and 17% for HoLEP (5 SUI and 6 UUI). Functional outcomes at 1 yr were similar:Qmax was 25ml/s(B-TRUP) Vs 23,2ml/s(HoLEP)(p:ns), PVR 6,7ml(B-TURP) Vs 25,5ml(HoLEP)(p:ns), residual prostate volume was 24cc(B-TRUP) Vs 15,2cc(HoLEP)(p:ns), PSA 2,1(B-TRUP) Vs 1,2(HoLEP)(p:ns),and IPSS 4,7(B-TURP) Vs 5,6(HoLEP) (p:ns). CONCLUSIONS:Bipolar TURP is faster and safer than HoLEP in the learning curve period with equivalent functional outcomes. The complication rates of HoLEP should be taken in mind before considering the introduction of this technique.
Comparative Evaluation of Safety, Cost Effectiveness and Resource Implications of Holmium Laser Enucleation of Prostate (HoLEP)as a Day Case Procedure.
Department of Urology, Hoshi General Hospital, Koriyama, Japan
Transurethral enucleation with bipolar (TUEB) is regarded as effective treatment, independent of size, for patients of benign prostatic enlargement. But detailed surgical techniques are not well described. We show our technical modification to protect the urethral sphincter. TUEB is the removal of prostatic adenoma from the capsule using blunt dissection. The prostatic capsule is identified easily at the 6 oclock position adjacent to the verumontanum and the 12 oclock position near the vesical neck. Dissection of the median lobe is started at the 6 oclock position adjacent to the verumontanum and continued proximally. For the left lobe, the dissection is started from the 5 oclock position near the vermontanum, where were dissected by the median lobe procedure, and continued proximally. The apical portion of the left lobe is not dissected at this time which has not been distinguished from sphincter yet. Dissection of the left lobe is then started at 12 oclock position and carried down to the 3 oclock position of the vesical neck, and continued distally. At this stage, the left lobe is shifted proximally and can be gently lifted anteriorly. This allows entire prostatic apex to be visualized and distinguished from the sphincter.
Comparison Between Efficacies of Transurethral Enucleation with Bipolar (TUEB) and TURP for BPH with Volume of Greater than 50ml.
PURPOSE: To retrospectively compare the efficacies of TUEB with TURP for BPH.
MATERIALS AND METHODS: From July 2005 to February 2011, 49 patients were diagnosed as BPH with volume of greater than 50 ml (75.6±26.2 and 63.2±21.8 ml, respectively), and subsequently underwent TUEB (n=33) or TURP (n=16). The mean age was 69.6 and 72.2 years (range; 54-85 and 56-84). All the patients were assessed using IPSS&QOL, Qmax, postvoid residual (PVR) before and 3 months after surgery. Perioperative parameters evaluated included operating time, removed prostate weight, changes of hemoglobin level. Intra- and post-operative complications were also investigated.
RESULTS: Preoperative IPSS&QOL were comparable between both groups (19.4±6.7 vs. 19.6±7.2/5.0±0.8 vs. 4.3±1.5). TUEB group showed larger removed prostate weight and longer operating times, compared with TURP group (40.9±23.0 vs. 25.1±26.7g, p=0.003, and 145.5±44.0 vs. 105.8±46.1min, p=0.012, respectively). However, no significant difference was found in losses of Hb (1.55±0.93 vs. 1.79±1.73 g/dl, p=0.67). Postoperatively, all symptoms in IPSS, except urgency, significantly improved (p<0.05), and were qualified as insignificant (mild) in all cases of both groups. TUEB group showed significantly greater improvement of Qmax (16.6±7.0 vs. 8.6±4.0 ml/s, p=0.002), and PVR (35.6±47.2 vs. 162.1±131.0 ml, p=0.01) at 3 month after surgery. Two episodes of acute prostatitis were identified in TUEB group, and 2 urethral strictures occurred in TURP group. No case with postoperative Incontinence was noted.
CONCLUSIONS: TUEB showed favorable efficacies and comparable incidence of perioperative complications, compared with TURP. TUEB may be alternative in treatment of BPH with volume of greater than 50ml.
Management of Benign Prostatic Hyperplasia (BPH) with Holmium Laser Enucleation of the Prostate (HoLEP) and Transurethral Enucleation with Bipolar (TUEB)
Purpose: Techniques of transurethral enucleation of the prostate by HoLEP or TUEB for treatment of BPH have attracted attention due to the minimally invasive character of these surgeries. We report a retrospective study comparing both procedures, HoLEP and TUEB. Materials and methods: 129 HoLEP patients were followed postoperatively, and 36 TUEB patients were followed postoperatively. The effects of treatment using the IPSS, QoL score and maximum flow rate (Qmax) were recorded just before surgery and at the third postoperative month. Results: The preoperative prostatic volume did not show significant difference between HoLEP (101.1ml) and TUEB (106.2ml) (p=0.62). There were no statistically significant differences between HoLEP and TUEB for preoperative IPSS, QoL, and Qmax. The average operating time was 154 minutes and resected tissue weight was 55.1g in HoLEP patients and 137 minutes and 55.6g in TUEB patients (p=0.67, p=0.95). No occurrence of hyponatremia was reported in either group. Postoperative IPSS, QoL, and Qmax for both urinary flow dynamics were significantly improved, and no statistically substantial differences were found between the groups. Postoperative transient urinary stress incontinence was present in 10.3% of the HoLEP patients and 8.8% of the TUEB patients at the third month of the study (p=0.846). Five cases of urethral stricture (13.9%) occurred in the TUEB patients as compared with four cases (3.1%) in the HoLEP patients (p<0.05). Conclusions: Our study demonstrates that the HoLEP and TUEB are equally effective in managing large BPH with symptom improvement and urodynamic results.
MP34: Urolithiasis/PNL/Ureteroscopy
Per Cutaneus Nephro-Lithotomy with a New Modified Amplatz Sheath for Complex Stones: Initial Experience.
Introduction: We present our experience of a novel modification of the Amplatz sheath for PCNLs. This modified sheath has a side hole in its proximal end, which permits the passage of flexible cystoscope to gain access to stones located in deep calyces without resorting to additional tracts. Material and Methods: A side hole (6mm wide, 10 mm long) is created in Amplatz sheath 5 mm from proximal end. Access to the renal pelvis and dilatation is performed. After clearance of the stone/s in the renal pelvis, a flexible cystoscope is passed through the side hole to access to remove deep-seated calyceal stones. Laser fragmentation and dormia basket extraction is used. 20 patients with stone sizes from 17 to 30 mm underwent PCNL procedures. Stones were located deep in 10 patients. Dormia extraction was achieved in 8 while laser fragmentation was needed in two. Results: 20 PCNLs were performed with this modified Amplatz sheath. Access to cayces was successfully obtained in all patients. Stone clearance rates were 90%. Clearance rates for stones located in calyces away from the main tract was 100%. Minimal bleeding from tract into side hole obscured vision in 2 patients. This was controlled by rotating the sheath. No patient required insertion of additional tract for stone clearance.Conclusions: This is a relatively simple modification which permits access to deep seated calculi without resorting to additional tract thus reducing the morbidity of PCNL. It is particularly helpful in patients with a small renal pelvis and deep seated calculi.
A New Access Catheter to Prevent Stone Migration During PCNL
Introduction: We present our feasibility study of a new access catheter Accordian CoAxR Stone Control device - during PCNL. This has a reversible roll-up tip which occludes the PUJ preventing migration of stone fragments.Material and Methods: The Accordian CoAXR access catheter is 4.3 F wide at its narrow end and 6.5 F at working end. It is introduced over a 0.038 guide-wire. Position of tip is confirmed by radio-opaque markers. The device can be folded on itself to create a reversible occlusion of the PUJ. This is reversed at the end of the procedure and the device withdrawn. The roll-up and unfurling of the device is achieved by a ratchet mechanism at the end of device. Contrast can be injected into the pevi-calyceal system. We have used this device in 4 pcnl procedures. Stone size was 20 mm (mean) with the range of 17 to 35 mm. Access was obtained from the lower calyx in 3 and the middle calyx in 1. Stone clearance was 100%. No complications were observed.Results: There were no difficulties during the insertion of catheter, puncture or the procedure. The roll-up mechanism diminished the view of lower calyx in one case but this did not have an impact on stone clearance. No stone fragments escaped down the ureter in any of the cases. Conclusion: We feel this is an interesting modification of the access catheter. It is easy to insert, and prevents the downward migration of fragments and can be easily removed.
Renal Pelvic Pressure During PNL
Renal pelvic pressure during percutaneous nephrolithotomy (PNL) relates to postoperative urinary tract infection.However, there were few reports about renal pelvic pressure during PNL. We measured renal pelvic pressure during PNL to evaluate the correlation with postoperative urinary tract infection. Between september 2010 and july 2011, 6 pressure flow study was performed using the occulusion-balloon catheter. Percutaneous puncture of the lower calyx was performed with fluoroscopic guidance. The tract was dilated to 18Fr, 24Fr or 30Fr with balloon dilator. Calculus fragmentation was undertaken using LithoClast® or Ho-YAG laser through a rigid nephroscope (16.5Fr or 24Fr). Mean age was 67.5 years. 4 males and 2 females, 3 right kidneys and 3 left was undergone. Mean calculus length was 37.6mm, and mean operative time was 193 minutes. Mean pressure before puncture was 35cmH2O, and rised to 70cmH2O during tract making. The pressure during calculus fragmentation through 18Fr tract was approximately equal to the pressure before puncture. Through 24Fr and 30Fr, the pressure during calculus fragmentation was low about 10cmH2O and about 20cm H2O to the pressure before puncture,respectively. Our results suggest that smaller tract may result in higher pressure and therefore in infection calculus, larger tract may be suitable. Accumulation of further cases will be needed from now on.
How High is the Intraluminal Pelvic Pressure During Flexible Ureterorenoscopy?
ObjectiveIrrigation and instrumentation during ureterorenoscopic procedures causes increased pelvic pressure (PP), which may be followed by intrarenal backflow with potential harmful adverse effects. In order to assess the pressure increases during ureterorenoscopy, we measured the intraluminal pelvic pressure during retrograde intrarenal stone surgery (RIRS).Material and methodsTwelve patients admitted for RIRS were included. Irrigation rate was standardized to 8 ml/min. A ureteral catheter was retrogradely placed in the renal pelvis for PP measurements. PP was measured two times per second during introduction and use of the Storz Flex-X ureteroscope, during introduction of stone-basket, during forced irrigation with contrast and when using a Holmium-laser fibre to disintegrate the stone.ResultsBaseline PP was mean 10(±4.0) mm Hg. During simple ureterorenoscopy, PP was mean 35(±10) mm Hg. During the use of stone basket and Holmium-laser, the average PP was 54(±18) mm Hg and pelvic pressure peaks up to 328 mm Hg occurred. In a five-minute standardized period of simple ureterorenoscopy, 83 pressure peaks above 50 mm Hg were measured in average per patient (range 2-238). Forced irrigation with contrast in a 20 ml syringe yielded pressure peaks up to 288 mm Hg.ConclusionVery high pelvic pressures (PPs) are obtained during ureterorenoscopy. Taking into consideration that the limit for intrarenal backflow is 30-35 mm Hg, it is concerning that PPs above 300 mm Hg are not uncommon during these procedures. Procedures to lower the PP during ureterorenoscopy, therefore, are considered of importance.
Shielding Using Automated Settings Increases Radiation Exposure to Surrounding Unshielded Tissues
Introduction: Automatic brightness control (ABC) is a function of modern fluoroscopy machines that adjusts X-ray intensity in real-time to obtain better image quality. While shielding reduces radiation exposure to protected areas in patients, it is unknown how much radiation unshielded areas receive using automated settings.
Purpose: To assess radiation dosage to surrounding unshielded tissue when using fluoroscopic ABC mode compared to fixed exposure settings.
Materials and Methods: Simulating ureteroscopy, thermoluminescent dosimeters (TLDs) were placed at 3 sites in a female human cadaver (BMI 21.9), including the right kidney, right distal ureter near the uterus, and the uterus. The cadaver received 60 seconds of radiation exposure using a C-arm fluoroscopy system under ABC and fixed settings (1.38mAs, 66kVp) with and without shielding of the uterus. Radiation dosage absorbed by the TLDs was compared using two-way ANOVA and least-squares confidence intervals.
Results: Shielding significantly reduced radiation to the uterus by 2.5 and 5.5 times (p<0.05) in ABC and fixed settings, respectively. However, when the uterus was shielded in automatic settings, there was an approximate 2-fold increase in radiation dosage to the ureter and ipsilateral kidney (p<0.05) compared to non-shielding. Under fixed settings, there was no significant difference (p>0.05) in radiation levels at these locations regardless of shielding status.
Conclusion: There was approximately a 2-fold increase in radiation exposure to surrounding unshielded tissue in ABC mode when the uterus was protected. Radiation can be reduced and image quality improved using fixed settings when shielding is indicated.
Comparing Fluoroscopy Time in Shockwave Lithotripsy and Ureteroscopy
Introduction: The harmful effects of radiation are well known. Subsequently, physicians employ ALARA (as low as reasonably achievable) to reduce radiation exposure. Therefore, it is important for physicians to understand the amount of fluoroscopy required to perform common urologic procedures.
Purpose: To compare fluoroscopy time and success rates between ureteroscopic lithotripsy and shockwave lithotripsy (SWL).
Materials and Methods: A retrospective review of patients treated with SWL or ureteroscopic lithotripsy was conducted between January 2007 and June 2011 at a single center (n=426). Fluoroscopy time, operative time, perioperative complications, stone size, stone location, and postoperative outcomes were compared using a Student's t-test and chi-square (α=0.05).
Results: Mean fluoroscopy time for SWL was nearly three times that of ureteroscopic lithotripsy (157.8 vs. 55.7 s, respectively; p<0.001). The mean operative time was longer for ureteroscopic lithotripsy (69.6 vs. 46.2 min.; p<0.001). Additionally, ureteroscopic lithotripsy had a higher overall stone free rate (84.6% vs. 72.5%; p=0.005). Furthermore, ureteroscopic lithotripsy had a higher stone free rate for renal stones than for SWL (86.9% vs. 69.8%; p=0.001), but a similar stone free rate for ureteral stones, (86.7% vs. 82.6%; p=0.372). However, patients undergoing ureteroscopic lithotripsy had longer hospitalization times (0.32 vs. 0.042 days; p<0.001).
Conclusion: Compared to SWL, ureteroscopic lithotripsy was associated with longer hospitalization time, higher stone-free rate, but significantly reduced fluoroscopy time.
Development of a Pre-Fluoroscopy Checklist to Reduce Radiation Exposure During Pediatric Ureteroscopy
Introduction. The ALARA principle requires efforts to minimize radiation exposure to the patient (As Low As Reasonably Achievable), but our research has shown that that radiation exposure during pediatric ureteroscopy (URS) is substantial. We sought to develop an intervention to reduce exposure during these procedures.Methods: We observed 48 consecutive URS procedures as part of a quality improvement initiative, and collected data on patient and surgical factors, fluoroscopy settings, and radiation exposure (total fluoroscopy time and skin entrance dose (SED, in mGy)). Modifiable factors were identified, including machine settings, positioning factors (e.g. skin-to-source distance), and minimization of fluoroscopy time. Based on these observations, a pre-fluoroscopy checklist was developed and pilot tested.Results: The median SED was 42.7mGy (range 2.23-223.4). (Chest x-ray SED is 0.16 mGy.) Median fluoroscopy time of 2.85 min (range 0.4-6.7), and was highly associated with exposure (p<0.0001). The other primary modifiable variable associated with SED was source-to-skin distance (shorter SSD associated with higher exposure, p=0.02). Other factors including image rate and field of view demonstrated opportunities for dose reduction. An initial 20-item checklist was reduced to 13 items after expert review. Pilot testing during 5 live pediatric URS procedures demonstrated that the checklist could be used in<60 seconds in all cases. Conclusions: Pilot testing of a pre-fluoroscopy checklist for pediatric ureteroscopy indicated that it is a practical and easily-implemented tool for radiation exposure reduction. After implementation into routine usage, we will measure the effect of the checklist on radiation exposure during pediatric URS procedures.
Radiation Exposure to the Resident, Fellow and Attending During Endourology Cases
INTRODUCTIONThe purpose of our study was to measure the radiation scatter exposure to residents, fellows and attendings during endourology cases at an academic institution.MATERIALS AND METHODSRadiation dosimeter badges were worn by the urology resident, fellow and attending for all endourology cases for 1 month at our institution. Badges worn included: eye(E),thyroid(T),chest(C) and waist(W) dosimeters for the residents and fellow, the attending wore a chest dosimeter. Separate dosimeters were worn for 1.) cystoscopy(Cysto) and ureteroscopy(URS) cases and 2.) percutaneous nephrolithotomy(PCNL) cases. RESULTSA total of 3 PCNLs and 24 Cysto/URS cases (2 Cysto with stent change, 22 URS) were performed during the study. Total fluoroscopy time for the PCNL and Cysto/URS cases was 668 and 1049 seconds respectively. Total radiation dosage as measured from the C-arm was 5892 and 6448 radcm2 respectively. The dose equivalents as measured by the radiation dosimeters for residents during PCNL were : E<1,T=2,C=5,W=21 mRem; for the fellow: E<1,T=9,C=16,W=46 mRem. The dose equivalents as measured by the dosimeters for residents during Cysto/URS were: E<1,T=4,C=5,W=20 mRem. The dose equivalent for the attending chest dosimeter was<1 mRem for the PCNL and Cysto/URS cases.CONCLUSIONThe radiation exposure to the eye during PCNL and Cysto/URS cases was minimal (<1 mRem). Higher radiation exposure to the resident and fellow are noted for waist dosimeters compared to chest dosimeters due to the c-arm source. Because the fellow was responsible for helping obtain access with interventional radiology during PCNL, he was exposed to the highest amount of radiation.
Comparison of Radiation Exposure with Continuous and Pulsed Fluoroscopy
Introduction: While pulsed fluoroscopy has reduced fluoroscopy times, studies have shown no difference in effective dose compared to continuous fluoroscopy due to the ramp-and-trail effect in older systems. Modern systems deliver more uniform current by minimizing this effect.
Purpose: To compare radiation dosage and image quality of pulsed fluoroscopy against continuous fluoroscopy in a modern C-arm system.
Materials and Methods: Thermoluminescent dosimeters (TLDs) were implanted at the left kidney, posterior skin, and anterior skin of a female cadaver. Thirty pedal activations at 69 kVp and 1.51 mAs were administered either in pulsed mode at 1 pulse/second or in continuous mode to visualize an implanted guide wire and radio-opaque stone. Radiation dosage was recorded and analyzed, and fluoroscopic images were ranked by 21 blinded urologists.
Results: Pulsed fluoroscopy delivered lower doses of radiation compared to continuous fluoroscopy at all sites: left kidney (0.15 vs 0.40 mGy, p<0.001), posterior skin (0.92 vs 2.62 mGy, p<0.001), and anterior skin (0.10 vs 0.26 mGy, p<0.001). Mean fluoroscopy time was significantly lower in pulsed mode (3.0 s) than continuous (12.5 s; p<0.001). However, continuous mode delivered less radiation per second compared to pulsed mode (0.009 vs 0.013 cGy/sec; p<0.001). Although pulsed fluoroscopy created grainier images, both were adequate for routine tasks during ureteroscopy (p=0.06).
Conclusion: While continuous fluoroscopy delivers a lower radiation dose per second, pulsed fluoroscopy significantly reduces radiation due to reduced fluoroscopy times while providing adequate image quality. Pulsed fluoroscopy should be used to minimize radiation exposure to patients whenever appropriate.
Totally Tubeless Percutaneous Nephrostolithotomy (PCNL). Is it Feasible? a Prospective Study
Purpose: comparing results of totally tubeless PCNL versus other modalities of PCNL.Material and Methods: 80 patients (53 men and 27 women) were rolled in the study in four groups: 1. conventional PCNL (with nephrostomy tube and ureteral catethery)2. Tubeless PCNL (ureteral catether without nephrostomy tube 3. placement DJ after PCNL without any other catether 4. Totally tubeless PCNL.IVP and routine laboratory tests were performed in all patients. We evaluate early and late complication and also, pain in these groups.Results: There were not differences in mean patients age (P=0.7) and duration of surgery (P=0.6) and also in early and late complication (P=0.2) in four groups. Hospital staying was longest in group 1(3.3±0.6) and was shortest in group 4 (1.7±0.5) (P Value<0.05).Mean scores of pain were significantly different in four groups (the first day:P Value=0.4 and in the seventh day: P=0.02).Conclusion: Totally tubeless PCNL is a suitable approach in selected patients.Keywords: percutaneous, tubeless, totally, nephrolithotomy
City Hospitals Sunderland NHS Foundation Trust, Department of Urology, Sunderland, UK
Background:Percutaneous Nephrolithotomy (PCNL) has undergone numerous changes,notably the use of 'The Tubeless PCNL' has improved the patient experience of the procedure simultaneously reducing morbidity and hospital stay. Traditionally required hospital admission for 2-4 days in most experienced centres. We studied the feasibility of PCNL with a 23-hour maximum hospital stay.Methods:We present a single surgeon experience in a unit with 4 stone surgeons.N=56 . Calculi of sizes ranging from 9mm to 35mm were operated on. 13 patients had a previous PCNL. A tubeless PCNL procedure was performed in all patients. Ureteric stents were removed 2 weeks later in an outpatient setting. Patient satisfaction was assessed using a validated modified stent symptom questionnaire [Bristol USSQ]Results:Complete stone in all 56 patients. All patients were discharged home within 23 hours of admission. 97.2% of patients were very satisfied.In 70% of patients urgency was only symptom. The 13 patients who had PCNL procedure in the past found the short stay option better than the longer stay option, with a quicker return to work. Cost saving benefits to the department in the region of £800 per patient per night hospital stay considering a minimum reduction in stay per patient by atleast a day.Conclusion:With this prospective study, we have demonstrated that short stay PCNL is a safe, feasible and cost effective option with complete stone clearance and a high patient satisfaction. We strongly recommend this as a future primary option for PCNL procedures in high throughput centres.
Tube or Tubeless During Percutaneous Nephrolithotomy?
Objective To investigate the safety and efficacy of tubeless technique during percutaneous nephrolithotomy. Methods 15 consecutive cases underwent single access tubeless PCNL were enrolled. All the percutaneous tracts were 24 Fr and holmium laser was used to fragment the stone. The operative time, duration of hospitalization, clearance, blood loss and other complications was noted, and these data were analyzed retrospectively.Results The mean operation time was 55 minutes, ranged from 40 minutes to 72 minutes. The duration of hospitalization was 4.5 days. Postoperative imaging studies showed all cases were stone free. No cases required blood transfusion. Postoperative fever occurred in 2 cases. And the temperature reached 38.5 centigrade or greater. Conclusions Tubeless PCNL appears to be safe and well tolerated without associated morbidity.
Percutaneous Nephrolithotomy: A Single Institute Experience of 1003 Cases
Introduction: Percutaneous nephrolithotomy (PCNL) is still the first-line treatment option for removal of larger or multiple stones, however, the incidence of complications should be considered.Purpose: The outcomes and complications of PCNL were evaluated at a single institute with a large series.Materials and Methods: A total of 1003 PCNL procedures between Jan 2000 and Dec 2010 for 186 staghorn stone (18.5%), 515 renal stone (51.3%), 203 proximal ureteral stone (20.2%), and 99 combined renal and proximal ureteral stone (9.9%) were included. Stone-free status was defined as no visible residual calcification or remnant calcification smaller than 5 mm in diameter on a plain KUB image. Stone characteristics, operation time, stone-free rate and complications were evaluated.Results: Initial mean stone burden was 1150.6 mm2. Average operation time was 88 minutes. The mean hospital stay was 4 days. The initial stone free rate was 77.7% (staghorn stone 41.4%, renal stone 82.3%, proximal ureteral stone 98.0%, combined renal and proximal ureteral stone 79.8%). Ancillary procedures were required in only 9.4% patients, including 7.6% ESWL, 1.0% secondary PCNL, 0.4% ureteroscopic procedure and 0.4% combined methods of above. Postoperative urinary tract infection and the blood transfusion rate was 9.6 and 3.1%, respectively. Complications were found in 48 procedures (4.8%), including 1.1% sepsis, 1.5% pleural complications, 0.7% JJ malposition, 0.4% urine leakage, 0.2% major bleeding, 0.9% other complications.Conclusions: PCNL is an effective and safe method for the treatment of staghorn, renal stone, and upper ureteral stones with low complication rates and short hospital stay.
Natural Course of Clinically Insignificant Residual Fragments after Percutaneous Nephrolithotomy
IntroductionThere remain unanswered questions with regard to long-term stone recurrence after percutaneous nephrolithotomy (PCNL). PurposeWe retrospectively evaluated the natural course of clinically insignificant residual fragments (CIRF) after PCNL as well as the factors affecting the clinical course using non-enhanced thin sectioned computerized tomography (CT).Materials & MethodsAfter PCNL for calcium renal stones between January 2004 and December 2010, we compared two groups-48 patients with CIRF (CIRF group) and 73 patients with no residual fragments (NRF group) with regard to recurrence and spontaneous passage. New stone formation, an increase in the size of residual fragments, symptomatic episodes or any clinical situation requiring additional intervention were regarded as recurrence. ResultsThe recurrence free survival at 24 months were 77.8% in the NRF group, and 61.9% in the CIRF group (p=0.29). In the CIRF group, stones passed spontaneously in 10 (20.8%) patients, treatment interventions were required in 6 (12.5%) patients, and stone size increased to a significant level without intervention in 9 (18.7%) patients. In the NRF group, 9 (12.3%) patients needed treatment interventions and new stone formation was detected without further treatments in 9 (12.3%) patients. In the CIRF group, smaller size of each residual fragments was the only significant factor affecting spontaneous passage (p=0.012). ConclusionsThere was no difference in recurrence rate between two groups. In patients with small size residual fragments, spontaneous passage of residual fragments can be expected. Patients without residual stones should also continue to be followed because of the risk of recurrence.
Department of Urology, the first affiliated hospital of Guangzhou Medical College, Guangzhou, China, 2Guangdong Key Laboratory of Urology, Guangdong, China
Introduction: To describe the technique of combination of standard PCNL and mini PCNL for the management of staghorn calculi, which combines the main advantages of the two techniques by using standard PCNL to rapidly remove large volumes of stone and by using mini PCNL to fragment stones that are difficult to access with PCNL without much more injury.Patients and Methods: 26 patients with staghorn calculi were treated by PCNL. Mean age was 42.4 years(23-55).12 cases had a partial staghorn calculi, 10 cases had complete staghorn calculi, 4 cases had multiple stone, with mean burden of 1789.4mm2(11007.2-3210.3). After ureter catheteration, fluoroscopy-guided punctures were made and tract was dilated to 26Fr by Amplatz dilators. The stones were fragmented with a pneumatic lithotripter through nephroscope. The latter punctures were created to the target calyx for residual calculi, while the tract was dilated to 16Fr, and 8/9.8Fr rigid ureteroscope was used.Results: Mean operating time was 102 minutes(78-115),60 tracts were established in 26 renal units. 4 cases with 3 tracts and 2 cases with 4 tracts, and 20 cases with 2 tracts. Complete stone clearance was achieved in 22 cases(84.6%) in a single session, 4 cases with 3-11mm calculi remained. Blood loss was 180ml (100-620), 1 patient required transfusion. 1 patient had hydropneumothorax.Conclusion: Judiciously made multiple percutaneous tracts in a single session combination of standard PCNL and mini PCNL for treating staghorn calculi was safe, feasible and efficient with an acceptable morbidity.
Does Morbidity of PCNL Increases in the Treatment of Staghorn Stones?

UP01: Unmoderated Poster Session 1
Case of Spermatic Cord and Testicle Angiomyolipoma
Introduction: In this case report, we describe a rare case of testicular AML. Clinic Case A 53 year old male with a history of congenital motor defects, mental retardation, presented a left testicular pain. His physical exam was significant for an indurated and painful left testicle and epididymis. His blood tests were non-contributory.A scrotal sonogram was performed which showed bilateral testicular micorcalcifications as well as an enlarged and hypoechoic left epididymal head. He had normal arterial and venous flow bilaterally. After no successed therapy the patient underwent a trans-inguinal exploration and left inguinal orchiectomy. Gross examination of the testicle revealed a soft brown mass replacing most of the testicular parenchyma. Pathologic examination revealed medium to large calibre thick-walled blood vessels with ectatic lumina, surround by sclerotic, fibrous smooth muscle bundles in a fatty milieu. The thin rim of testicular tissue remaining around the tumor displayed diffuse hemorrhage and necrosis within the seminiferous tubules and interstitial xanthogranulomatous flogistic infiltrate with blood cell extravasation and siderophages. The tunica albuginea was irregularly thickened. DiscussionTo our knowledge there is only one other case of testicular AML reported in the literature, though there is also a case involving the spermatic cord and spleen. Given the rarity of these tumors, despite the histopathologic nomenclature, until further studies are done to establish reliable methods of diagnosis and treatment, we feel that it is most prudent to perform a transinguinal orchiectomy on these tumors.
The Divisions of Urology, Department of Surgery, Chi Mei Medical Center, Tainan, Taiwan
Purpose:
We reported our experience in series of retroperitoneal laparoscopic resection for pheochromocytoma and evaluated the safety and efficacy of this surgical procedure.
Materials and Methods:
In total 9 cases undergoing retroperitoneoscopic adrenalectomy in the ChiMei Medical Center were reviewed retrospectively. The general date, preoperative condition, intraoperative blood pressure fluctuation, operating time, blood loss, size of lesion, postoperative condition and prognosis were summarized and analyzed.
Results:
The series comprised 5 males and 4 females. The mean age was 45.7 year-old. Right-sided tumors were more common (5 cases). The mean operation time was 263 minutes. The mean diameter of the excised masses was 3.3 cm (range 1.5 to 6 cm). The mean hospital stay was 4 days (range 2 to 6 days). No patients had major complication and none died.
Conclusions:
Retroperitoneal laparoscopic adrenalectomy without previous control of the adrenal vein is effective and safe for ablation of pheochromocytoma.
Is larger Tumor Size a Contraindication to Retroperitoneal Laparoscopic Adrenalectomy?
Introduction: Adrenal tumor size larger than 5cm is known to be relative contraindication of retroperitoneal laparoscopic adrenelectomy.
Purpose: We analyzed the surgical outcome of retroperitoneal laparoscopic adrenalectomy, according to tumor size.
Materials and Methods: One-hundred twelve patients underwent retroperitoneal laparoscopic adrenalectomy were enrolled. They were divided into two groups according to tumor size: group 1 (<5cm, n=42) and group 2 (>= 5cm, n=70). Operative outcomes of all patients were compared: the operation time, change of hemoglobin level, estimated blood loss, necessity of blood transfusion, time to ambulation, hospitalization durations, complications and conversion to open surgery.
Results: The estimated blood loss (241.9±230.3 vs. 354.4±266.5 p=0.025), time to ambulation (1.45±0.50 vs. 1.89±0.32, p=0.001), hospitalization durations (7.26±3.32 vs. 9.04±2.96, p=0.004) were significantly larger and longer in group 2. Operation time(192.1±71.6 vs. 207.5±71.1, p=0.270), change of hemoglobin (1.15±1.14 vs. 1.21±0.94, p=0.756) did not show statistically significant difference between two groups. Blood transfusion were done in 2 cases (group1) and 6 cases (group 2), respectively(4.8% vs. 8.6%, p=0.449). Neither of groups had complication or conversion to open surgery.
Conclusions: Patients with larger size of tumor (>= 5cm) had larger estimated blood loss than patients with smaller size of tumor but change of hemoglobin was not differing. Patient with larger tumor showed delayed ambulation and longer hospitalization duration than patients with smaller size of tumor. However, complication and conversion to open surgery did not occur in those patients. Retroperitoneal laparoscopic adrenalectomy can be applied to patients with tumor size larger than 5 cm.
A Comparison Between Open Surgery and Laparoscopy for Adrenal Pheochromocytoma Less than 10 cms.
Introduction: Management of Pheochromocytoma is a challenge for surgeons whether operation is done by open surgery or laparoscopy. This paper compares the results of open surgery and laparoscopy for adrenal pheochromocytoma.Materials and Methods: Retrospective Analysis was performed on 40 consecutive patients who underwent adrenalectomy for adrenal Pheochromocytoma between 1996 to 2011. 21 patients who underwent transperitoneal laparoscopy were compared with 19 patients who underwent open surgery.Results: Both groups were matched in age, tumor size , preoperative blood pressure, heart rate and plasma catecholamines. We found significant differences between laparoscopic and open groups in the operative time, blood loss, postoperative hospital stay, pain and scar size. No significant differences were found in intraoperative blood pressures and heart rates. No patient needed a blood transfusion. There were no complications in either group. Conclusions: For adrenal Pheochromocytoma, the laparoscopic procedure decreased operative time, blood loss, postoperative hospital stay, pain and scar size compared to traditional open surgery. Intraoperative hemodynamic values during laparoscopic adrenalectomy are comparable to those of traditional open surgery. Laparoscopy seems to be a safe and preferred alternative to open surgery for adrenal Pheochromocytoma less than 10 cms.
Department of Urology, Hamamatsu University School of Medicine, Hamamatsu, Japan
<Methods> We analyzed clinical outcome of 4 patients with extra-adrenal paraganglioma (PGL) removed by laparoscopic surgery. <Results> Median age of the patients was 41 years old. Distribution of gender and tumor location showed male/female 2/2 and right/left 1/3, respectively. Preoperative diagnosis was PGL in 1 located in left side and adrenal pheochromocytoma in 3. Median value of preoperative laboratory studies were as follows: serum (s) epinephrine: 29 pg/mL, s-norepinephrine: 1741 pg/mL, s-dopamine: 16 pg/mL, 24-hour urine collection for (u) metanephrine: 0.28 mg/24h and u-normetanephrine: 0.97 mg/24h, respectively. MIBG scintigraphy revealed abnormal accumulation in 3. Two patients preoperatively suffered from hypertension and one of them often presented paroxysmal attacks of blood pressure. Laparoscopic transperitoneal excision was performed in all cases. Median of the operation time and estimated blood loss were 167 min and 65 mL, respectively. Median values were 12 g in weight of the specimen and 27 mm in diameter of the tumor, respectively. Maximal blood pressure was elevated to 280 mmHg in 1, and less than 160 mmHg was observed in the other 3 cases during the operation. Intraoperative and postoperative course was uneventful in all cases. Median period of the postoperative course was 37 months. One patient with VHL disease underwent pancreatoduodenectomy for the PGL of pancreas head 3 months after the operation. There was no evidence of recurrence in the other 3 cases. <Conclusion> Laparoscopic surgery for extra-adrenal PGL could be safely performed by paying careful attention to intraoperative hypertention.
Clinical Outcome of Laparoscopic Adrenalectomy
Objectives: The objective of this study was to present the clinical outcomes of 139 patients who underwent laparoscopic adrenalectomy at our institution.Patients and methods: A total of 139 patients with adrenal tumor underwent laparoscopic adrenalectomy in our institute between 1994 and 2011. A laparoscopic transperitoneal approach was used in 137 cases and retroperitoneal approach in 2 cases. Underlying pathologies comprised Cushing syndrome (n=27), pheochromocytoma (n=15), primary aldosteronism (n=49), non-functioning adenoma (n=41) and others (n=7).Results: 130 laparoscopic adrenalectomies were finished successfully, and open surgery was necessary in 9 cases. There was no operative mortality. Mean operative duration was 233 min, and mean estimated blood loss was 137 mL. Tumor diameter was significantly larger for pheochromocytoma than for primary aldosteronism and non-functioning adenoma. No significant differences in operative time and estimated blood loss were noted between benign tumors. Conclusions: Laparoscopic adrenalectomy for adrenal tumor offers excellent surgical outcomes and convalescence.
Post Chemotherapy Extraperitoneal Laparoscopic Retroperitoneal Lymph Node Dissection for Testicular Cancer
Objectives: To assess the surgical and oncological outcome of extraperitoneal laparoscopic retroperitoneal lymph node dissection (L-RPLND) for testicular cancer after chemotherapy. Methods: A total of 33 patients (15 of stage IIA, 11 of IIB, 1 of IIC, 6 of stage III) underwent extraperitoneal L-RPLND after chemotherapy in the supine position from April 2002 to May 2010. The morbidity and oncological outcome were reviewed retrospectively. Results: The mean operating time was 209 minutes (range 89 to 399 min.). Mean blood loss was 57ml (range scarce to 520 ml). Pathological assessment of lymph nodes showed no viable cells in 29 patients, residual carcinoma in 2 patients and mature teratoma in 2 patients. The mean lymph node size of pre-chemotherapy and post–chemotherapy was 2.0(0.8-5.0cm) and 1.0 (0.5-4.2cm).There were no conversions to open procedure. 10 patients had prolonged lymphorrhea treated with conservative therapy. 16 patients had chylous lymphorrhea. No disease recurrence was observed during a median follow-up of 48 months (range 14 to 112 months). Conclusions: Extraperitoneal L-RPLND after chemotherapy is a feasible and oncological safe procedure.
Division of Nephro-Urologic Surgery, Mie University Graduate School of Medicine, Tsu, Japan
Objectives: We could perform percutaneous radiofrequency ablation (RFA) for 7 functioning adrenocortical adenomas under local anesthesia. We evaluated our experience at a 55-month mean follow-up concerning the feasibility, safety, and therapeutic effects. Methods: From February 2003 to September 2010, 6 patients having adrenocortical adenoma with Cushing syndrome and one patient with primary aldosteronism underwent CT- guided percutaneous RFA. All patients chose RFA treatment but laparoscopic adrenalectomy. This sutudy was approved by our Institutional Review Board and written informed consent was obtained from each patient. RFA was performed using Cool-tip RF generator of Radionics. Dynamic contrast-enhanced computed tomography and magnetic resonance imaging performed to evaluate of treatment completion.Results: RFA was technically successful in all patients and tumor enhancement was eliminated in all tumors but one. The hormonal levels were normalized after RFA in all patients. Adosterol scintigraphy demonstrated no uptake in adrenal tumor after RFA in all patients. One patient having the residual enhancing area of tumor continuously was performed second RFA three years later when morning cortisol value elevated, resulting in the elimination of residual enhancement. There were no major complications related to the procedures except that one patient had a pneumothorax.Conclusions: Percutaneous RFA under local anesthesia is a feasible, safe, and effective alternative treatment of the functioning adrenocortical adenoma for the patients having refused the surgery due to high surgical risk, high age and the cosmetic viewpoint.This procedure could be repeated again and again when the hormonal value of the patient would increase in the future.
Clinical Evaluation of Laparoscopic Adrenalectomy at Our Institute
Background: To evaluate safety and efficacy of laparoscopic adrenarectomy. Patients and Methods: From April 2001 to December 2010, thirty seven cases underwent laparoscopic adrenalectomy at Kinki University Medical Hospital. Mean age was 54 years old (25 to 78 years old, 19 males and 18 females). Preoperative diagnosis consisted of 19 aldosteronomas, non-functioning adenoma in 10, preclinical Cushing syndrome in 3, Cushing syndrome in 2, adrenal cyst in one, and one metastatic adrenal tumor from RCC. Laparoscopic adrenalectomy was performed either via transperitoneal (36 cases) or via retroperitoneal (one case) approach under general anesthesia. These cases were reviewed retrospectively. Results: Average tumor size was 24.62 mm (10 to 56 mm), and mean operative time was 164 minutes (95 to 300 min.). There was no case who required transfusion during operation or postoperatively. In one case, despite preoperative diagnosis of non-functioning adenoma, pheochromocytoma was found because of intraoperative hypertension and pathological findings. Conclusions: Laparoscopic adrenalectomy is safe and standard procedure for adrenal tumors.
Clinical Statistics of Laparoscopic Adrenalectomy
Recently, the laparoscopic adrenalectomy is a standard surgery for adrenal tumor. Between January 2006 and May 2011, 18 patients underwent laparoscopic adrenalectmy for their adrenal tumor (primary aldsteronism:8 cases, Cushnig syndrome: 4cases, Pheochromocytoma:2cases, subclinical Cushing 1case, non-functional adenoma 1case, adrenal hematoma: 1case, and adrenal neuroganglioma:1case) in our institution. The Mean operation time was 152min (101-252 min). The blood loss volume was little in all cases except 2 pheochromocytoma (120 and 735ml). There was none of conversion to open surgery. A case of neuroganglioma had a large tumor (9cm). Laparoscopic adrenalectomy is considered safe and standard operation for adrenal tumor.
Laparoscopic Adrenalectomy on a Patient with Cushing's Syndrome During Pregnancy
The present case involved a 33-year-old female primipara patient. Two years prior to the admission, the patient had noted face and leg edema and throat thickness. She was hospitalized in June of 2011 because of suspected Cushing's syndrome at 8 weeks of gestation. In addition to the signs of Cushing's syndrome, she had high blood cortisol, and low levels of ACTH, and abdominal US showed CT 37mm in the left adrenal, so she was diagnosed with Cushing's syndrome associated with pregnancy. Cushing's syndrome is considered to increase the rate of fetal death and maternal miscarriage, premature delivery, IUGR due to hyperglycemia and hypertension. We performed a laparoscopic adrenalectomy (transperitoneal approach) at 16 weeks gestation. The length of the operation was 140 min, the laparoscopic time was 110 min, and she lost 10 ml of blood. The pressure pneumoperitoneum during surgery minimized the effect on the fetus to 6 mmHg, and did not use monopolar . Seven days postoperatively, the mother and fetus were discharged with no problems.Conclusion: We herein report a case of Cushing's syndrome who underwent laparoscopic resection of the left adrenal gland during pregnancy and also discuss the pertinent literature. However, only a small number of published studies was found on this topic in the literature.
Laparoscopic Retroperitoneal Lymph Node Dissection after Chemotherapy for Testicular Cancer
We have experienced three cases of laparoscopic lymph node dissection after chemotherapy for testicular cancer. Case1, A 33 year-old male with right testicular non-seminoma staged pT2N0M0, stage1 developed retroperitoneal lymph node metastasis after surveillance and received four courses of combination chemotherapy composed of bleomycin, etoposide and cisplatin (BEP). Laparoscopic lymph node dissection was performed through transperitoneal approach. Pneumoperitoneum time was 358 min and estimated blood loss was less than 50 ml. Case 2, A 23 year-old male with left testicular non-seminoma staged pT2N1M0, stage2A received three courses of BEP therapy. Laparoscopic lymph node dissection was performed through retroperitoneal approach. Pneumoperitoneum time was 430 min and estimated blood loss was less than 150 ml. He developed lymphorrhea and recovered conservatively. Case3, A 47 year-old male with left testicular non-seminoma staged pT2N0M0, stage1 developed retroperitoneal lymph node metastasis after surveillance and received three courses BEP therapy. Laparoscopic lymph node dissection was performed through retroperitoneal approach. Pneumoperitoneum time was 400 min and estimated blood loss was 50 ml. All cases had no serious adverse events. Although dissection of adhesive tissues was problematic and careful attention to surrounded organs such as the major vessels, the intestine and the ureter was required, this procedure resulted in minimal bleeding and could be less invasive.
Laparoscopic Adrenalectomy for Adrenal Metastasis
The indications for laparoscopic adrenalectomy in cases of adrenal metastatis remain controversial. To clarify outcomes of adrenalectomy for adrenal metastasis, we performed a retrospective review of all 5 patients who underwent adrenalectomy for adrenal metastasis between 2007 and 2011 in Kagawa University Hospital. The median age was 70 (50–78) years. The Primary tumor was lung cancer in 3 cases, and rectal cancer, thyroid cancer in 1 case each. Three patients had other metastasis, and were performed removal of all metastases. Laparoscopic adrenalectomy was performed in all cases, and 1 case converted to open surgery. All patients alive for average sixteen months postoperatively, include 3 were considered tumor-free. We conclude that patients with adrenal metastasis may benefit from laparoscopic adrenalectomy and that resection could be considered as a therapy for adrenal metastasis.
A Case of Laparoscopic Right Adrenalectomy with Left Sided Inferior Vena Cava
Left sided inferior vena cava (IVC) is an extremely rare anomaly. We report a case of laparoscopic right adrenalectomy with left sided IVC in a 43-year-old male. An abdominal computer tomography showed a right adrenal adenoma with a diameter of 10 mm and left sided IVC. Left sided IVC joined the left renal vein and crossed anterior to the aorta. After joining right renal vein at right side of aorta, IVC drained into the right atrium normally. Right adrenal vein were directly connected to the posterior side of IVC. The diagnosis of the adrenal adenoma was primary aldosteronism and laparoscopic right adrenalectomy was performed with transperitoneal approach. We first identified IVC crossing the aorta and then right renal vein draining into the IVC. Because right renal vein ran along the medial side of right adrenal gland and drained into IVC at more rostral site than usual, separation of medial side of the adrenal grand was more difficult than that in the surgery without anomalies. Operation time was 3 hour and 10 min. Amount of bleeding was 40 ml. It is estimated that transperitoneal approach is appropriate in the current case for anatomical orientation. A thorough evaluation before the surgery and a meticulous procedure were important especially in laparoscopic surgery with venous anomalies such as left sided IVC.
Laparoscopic Adrenalectomy for Isolated Metastasis of Adrenal Glands
Objectives: The treatment of adrenal metastases using laparoscopic surgery is considered controversial. The aim of this study is to present our experience in laparoscopic adrenalectomy for isolated adrenal metastasis.Methods: From June 2004 to June 2011, 6 adults (5 males/ 1 female) with adrenal metastases underwent laparoscopic adrenalectomy. The primary tumors diagnosed were 3 cases of lung carcinoma, 2 cases of hepatocellular carcinoma, a case of renal cell carcinoma. The median patient age was 66 (range 61 to 72), and the median tumor size was 3.5cm (range 2.5 to 7.0).Results: Laparoscopic adrenalectomies were performed by 4 transperitoneal approach, 2 retroperitoneal without any complications. The median operative time was 139.5 minutes (range 126 to 174), and the estimated blood loss was 47ml (range 25 to 220). One procedure was converted to open surgery due to severe liver adhesion to the abdominal wall.After these surgeries, one lung cancer patient has been treated with adjuvant chemotherapy, other 5 patients with no adjuvant therapy. Regarding the oncological outcome, 4 of 6 patients were alive without any recurrence at a median follow-up of 27 months. One case was alive with lung metastasis occurred at 15 months later, another was dead of primary cancer, 14 months after surgery. Conclusions: Laparoscopic adrenalectomy for isolated adrenal metastasis is thought to be feasible. However, the indication of surgery must be determined after due consideration about tumor size, cancer characteristics, risk factors and so on, additionally,the operative procedure must be discussed sufficiently.
Strategies to Reduce Perioperative Costs of Robotic Partial Nephrectomy
Introduction: Robotic partial nephrectomy (RPN) has become the preferred technique for minimally invasive nephron-sparing surgery based on improved dexterity, magnification, and ergonomics compared with laparoscopy. A deterrent to adoption of this technology has been the high costs associated with robotics. While the purchase and maintenance costs of robotics may be fixed, perioperative supplies may be strategically chosen to substantially decrease overall costs of this procedure.Methods: We reviewed data from our hospitals financial office regarding the costs of supplies that are commonly utilized during RPN. We identified specific supplies that might be omitted, or for which less expensive items might be substituted. Cost savings that would result from these strategies were assessed.Results: We found that $1870 can be eliminated from RPN based on limiting of specific resources. These include eliminating use of the fourth arm with its associated instrument cost ($270), using only one needle driver ($220), not performing frozen section analysis ($422), eliminating use of LapraTys for securing bolster stitches ($131) (and rather using Weck clips), eliminating use of argon beam ($239), and forgoing hemostatic products including Surgicel ($114), Floseal ($100), fibrin sealant ($374). Conclusions: There are specific modifications of RPN resource utilization that might substantially decrease perioperative costs. These strategies may be valuable in settings of limited health care resources, both in established and nascent robotics programs.
Laparoscopic Repair of Urinary Leak after Pyeloplast Using a Novel Peritoneal Patch
Introduction: Urinary leak after pyeloplasty can prolong morbidity and hospital stay. For persistent urinary leak, conservative measures are usually used however, small group of patients may require surgical correction which is often challenging. Purpose:We aim to describe a laparoscopic repair of persistent urinary leak after pyeloplast, using a novel peritoneal patch. Material and Methods:A young female with solitary functioning left kidney underwent laparoscpic left pyeloplasty for ureteropelvic junction (UPJ) obstruction. The procedure proved technically demanding due to extensive peri-ureteric fibrosis. Post operatively, she developed persistent urine discharge from the surgical drain. A trans-peritoneal laparoscopic repair of the leak was attempted. A wide defect was observed at the anastmosis. The defect was sutured however the gap was difficult to close. A 5 x 4 cm peritoneal patch was excised from the parietal peritoneum and the defect was bridged by this peritoneal patch. Retrograde pyelography was performed after 6 weeks of the surgery and renal function were monitored on monthly basis.Results:Patient recovered well and the drain was removed on third post op day. After 6 weeks the JJ stent was removed and retrograde pyelography showed good drainage from the left kidney. At six months follow up, patient remained asymptomatic with stable renal profile.Conclusions: Laparoscopic repair of persistent urinary leak after pyeloplast is feasible and a peritoneal patch can be used where repair of the defect is difficult.
Department of Urology, School of Medicine, Kyungpook National University Hospital, Daegu, Korea
Introduction: Robot assisted partial nephrectomy is rapidly emerging as an alternative to laparoscopic partial nephrectomy for the treatment of renal malignancy. We report comparison of the 2 approaches, describing outcomes from single experienced surgeon.Purpose: To compare perioperative outcomes of robot assisted partial nephrectomy (RPN) with laparoscopic partial nephrectomy (LPN) by a single surgeon at a single institution.Metrial and Methods: Between January 2006 and December 2010, retrospective review of 66 patients who underwent RPN (n=26) or LPN (n=40) by a single surgeon was done. Perioperative and short-term oncological outcomes of RPN were compared with LPN.Results: There was no significant difference between two groups with respect to age, sex, body mass index, preoperative mass size, laterality and tumor location. Mean operative time for RPN was 225.5±31.3min versus for LPN was 223±52.8min (p=0.882). Mean estimated blood loss was higher in LPN than RPN (381.6±134.2ml versus 507.8±323.4ml, p=0.032). Mean warm ischemic time was shorter in RPN (27.9±5.8min versus 35.6±7.3min, p<0.001). Mean change in estimated glomerular filtration rate was lower in RPN but not statistically significant (8.9±8.2% versus 10.1±8.4%, p=0.605). The complication rate (p=0.557) and conversion to open surgery rate (p=0.660) were similar in both groups. There was no positive surgical margin case in both groups. No recurrence or metastasis was found during mean follow up of 22 months (3-55).Conclusions: The results of our study have shown that RPN was safe and effective alternative option to LPN. Further prospective comparative studies with long term follow up will confirm this encouraging result.
Department of Urology, Keio Unversity School of Medicine, Tokyo, Japan
Introduction and Objective: In general, obesity is thought to be a major factor influencing the degree of technical difficulity, and often body mass index (BMI) is substituted for the parameter of obesity. Meanwhile, metabolic syndrome is the focus of so much attention. In this study, we focused on visceral fat which diagnoses metabolic syndrome, and examined the impacts on operative complexity in laparoscopic nephrectomy as measured by operative time. Methods: We reviewed 121 patients treated with laparoscopic nephrectomy from 2006 to 2010 at our institution. The total fat area (TFA), visceral fat area (VFA), and subcutaneous fat area (SFA) were measured at the level of the umbilicus by computed tomography. To demonstrate the type of obesity, the VFA/TFA ratio was calculated based on the measured data. Results: Statistically significant correlations were observed between operating time and BMI (p=0.033). The VFA/TFA ratio also had a significant correlation with operating time (p=0.008). Univariate analysis revealed that high BMI>25 and a high VFA/TFA ratio>0.455 (median), which was defined as the visceral adiposity, resulted in a prolonged operative time. Sex, age, tumor size, location, and stage were not related to operative time. Multivariate analysis demonstrated that visceral adiposity was an independent risk factor for prolonged operating time (p=0.001, odds ratio; 11.30). On the other hand, BMI did not become the risk factor. Conclusions: The visceral adiposity influenced operating time more as compared with BMI in laparoscopic nephrectomy. This preoperative information may potentially be used to help predict technical difficulty.
Department of Urology and Endoscopic Surgery, NTT-East Corporation Sapporo Medical Center, Sapporo, Japan
Objectives: It has been expected that laparoscopic surgery has significant benefits over open surgery. Minimum invasive procedures will be increasingly required in elderly patents, because life expectancy continues to increase. The aim of this study was to assess whether elderly patients over 80 years old revealed comparable perioperative outcomes to those achieved in younger patients. Methods: A total of 126 laparoscopic procedures has been performed in our hospital since April 2006. We retrospectively reviewed the records of 15 patients over 80 years old who had undergone laparoscopic surgery. The clinical and pathologic features and complication rates were analyzed. Results: The median age of our 15 patients was 85.3 years (range 80-94). Seven patients had undergone laparoscopic radical nephrectmomy (Nx), and eight patients had undergone radical nephroureterectomy (NUx). The median operating time (165 min in Nx, 250 min in NUx) and the median estimated blood loss (10ml in Nx, 250ml in NUx) were comparable to those of younger patients (under 79 years old). Nobody needed transfusion during and after the operations. The median length of hospital stay (9 days in Nx, 11days in NUx) and overall complication rate were also comparable to those of younger patients. Conclusions: Our data revealed the safety and feasibility of laparoscopic procedures in elderly patients. The overall complication rates and other perioperative parameters appear to be comparable to those of younger patients under 79 years old. These data may be helpful in preoperative decision making and informed consent in elderly patients.
Retroperitoneoscopic Nephrectomy Using a GelPort as the Main Access Platform: Standardization of Surgical Approach Beyond the Purpose of Nephrectomy
Introduction: Previously, we performed laparoscopic nephrectomy with various surgical approaches depending on the purpose of nephrectomy: radical nephrectomy with transperitoneal access, nephroureterectomy with retroperitoneal access followed by bladder-cuff excision through an additional lower pararectal incision with open procedures, and gasless laparoscopy-assisted living donor nephrectomy with retroperitoneal access. Since 2008, we have been performing these nephrectomies with a standardized approach, where retroperitoneal access using a GelPort as the main platform is applied. This device has several advantages including no need to extend the primary incision for extraction, flexible readjustment of port positioning, and flexible shift to not only hand-assisted but also open procedures.Purpose: To report our experience with laparoscopic nephrectomy with the standardized approach.Materials and Methods: Between September 2008 and May 2011, we performed laparoscopic nephrectomy in 107 patients for various indications. These included radical nephrectomy (N=35), nephroureterectomy (N=16), and donor nephrectomy (N=56). In all cases, the standardized approach was applied.Results: Conversion to open surgery was necessary in 2 cases. Two intraoperative complications occurred in nephroureterectomy although laparoscopic isolation of the kidney was accomplished uneventfully. Surgical site infection occurred in 1 case. Median operative time and blood loss until the kidney was completely freed were 170, 163 and 251 minutes and, 20, 30 and 120 mL for radical nephrectomy, nephroureterectomy, and donor nephrectomy, respectively.Conclusions : Retroperitoneoscopic nephrectomy utilizing a GelPort is technically feasible with acceptable safety for a variety of indications. Moreover, standardization of surgical approach may lead to shorter learning curve.
Division of Urology, Department of Surgery, Chi-Mei Medical Center, Tainan, Taiwan
INTRODUCTION: We reviewed peri-operative outcomes with retroperitoneal laparoscopic partial nephrectomy (RLPN) for renal cortical neoplasms (RCN) in our hospital.METHODS: We reviewed a prospectively established database from September 2005 to February 2011 and identified 72 patients who underwent RLPN for RCN. Data were evaluated for oncological, functional, and recovery outcomes. And tumors were stratified by size. There were 31 male and 41 female. The mean tumor size was 4.1 cm (range 1.2-10 cm).RESULTS: The mean operative time was 237 minutes (range 135-375 minutes) and the mean blood loss was 315 ml (range 100-1750 ml). There were 14 (19.4%) complications. The mean warm ischemia time was 26.9 minutes. Overall, 40% of the tumors were malignant renal cell carcinoma variants with a positive margin rate of 0%. With a median follow-up of 35.7 months, there was 1 local recurrence. The median change between preoperative and 3 months' follow-up glomerular filtration rates of the affected kidney were 50.7 ml per minute and 40.6 ml per minute, respectively. Reduction of the affected kidney was 14.5%. CONCLUSIONS: RLPN is a safe and effective treatment option for RCN. With extensive experience and a well-developed surgical technique, patient outcomes are improved and postoperative complications are reduced. RLPN might be applied to more complex cases including larger and hilar tumors.
Thurlium Laser Partial Nephrectomy for a Benign Renal Mass with Obvious Contrast Enhancement and Central Necrosis
We reported the 39 year-old female presented with incidentally found left renal mass. Abdominal computed Tomography showed one left renal mass about 2.2x2.4x2.5 cm with obvious contrast enhancement and central necrosis at middile pole cortex. Laparoscopic partial nephrectomy via thurlium laser was done using five-trocar method. Total operation 155 minutes, warm ischemic time 9 minutes and blood loss about 50 cc The pathology showed angiomyolipoma with leiomyomatous component predominant. Concvalence was uneventful and the patient was discharged under stable condition.Laparoscopic partial nephrectomy is a technically challenging procedure. It have advantages of lower cost, decreased postoperative pain and early recovery. In previous animal model we use pig and thurlium laser partial neprectomy was performed. We successfully performed thurlium laser partial nephrectomy in our hospital. We were agreeted by IRB. Therefore in this case we performed laparoscopic partial nephrectomy with thurlium laser. This method seem been a safe and feasible way to treat superficial cortex renal mass.
Department of Urology, Singapore General Hospital, Singapore.
IntroductionThe R.E.N.A.L. Nephrometry score is a relatively new tool to quantify renal tumour size, location and depth. A higher score is associated with a more complex tumour and can be more technically demanding during nephron sparing surgery.PurposeWe seek to validate the nephrometry score with perioperative outcomes and complication rate during laparoscopic partial nephrectomy (LPN).Materials and MethodsAll patients undergoing LPN from 2006 and 2010 in Westmead Hospital, Sydney, Australia were enrolled. Preoperative and perioperative data were retrospectively collected. The Clavien-Dindo classification system is used to stratify severity of complications.ResultsSee table.A higher nephrometry score correlates with longer operative and warm ischaemia times, greater estimated blood loss and higher conversion and complication rates.ConclusionA higher nephrometry score is associated with adverse perioperative outcomes and greater complication rates. This information is helpful in the preoperative planning and counseling process for patients undergoing nephron sparing surgery for renal tumours.

Laparoscope-Assisted Minimally Invasive Surgery for Complex Renal Vascular Disease
Purpose: We report our experience of four cases with complex renal vascular diseases underwent laparoscope-assisted minimally invasive surgery. Endovascular approaches were impossible in these cases because of the risk of branch occlusion and stent migration.Material and Methods:Three patients have complex renal artery aneurysms involving bifurcatin and one patient has Nutcracker syndrome with symptoms. Three cases with complex renal artery aneurysms were underwent retroperitoneoscopic nephrectomy, ex-vivo repair using autologous internal iliac artery and ipsilateral iliac fossa autotransplant . The patient with nutcracker syndrome was treated with laparoscopic dissection from the surrounding tissue and in situ re-anastomosis to inferior vena cava .Results:Patients were three women and one man. Mean age was 61.3 years (range, 51-72).The mean operative time, the estimated operative blood loss, the average warm ischemic time and the total ischemic time were respectively 729 minutes (range,628-910), 789 ml(range,100-1405), 31 minutes (range,3-78) and 383 minutes (range,308-516) in the patients with complex renal artery aneurysms. No perioperative complication was noted. Renal scinti graph showed good patency in all autotransplanted kidneys.Conclusions:These procedures are safe and effective. These technical advantages are a minimally invasive approach even in complex cases and early postoperative recovery.
Urology, Changwon Samsung Hospital, Sungkyunkwan University, Changwon, Korea
INTRODUCTION AND OBJECTIVES: To compare the feasibility of laparoendoscopic single site surgery (LESS) via the retroperitonealapproach and conventional retroperitoneal laparoscopic radical nephrectomy for renal cell carcinoma (RCC). METHODS: This study was designed as a match case-controlled study from a RCC database of our hospital. 10 consecutivepatients undergoing LESS radical nephrectomy were compared with 20 patients undergoing conventional retroperitoneal laparoscopic radical nephrectomy. Controls were matched for age, gender, side of operation, and mass size, body mass index via a statistically generated selection of all laparoscopic radical nephrectomies. RESULTS: Mean operative time in the LESS group was 174.0(130-210) min compared with 170.3 (115-240) min in the conventionallaparoscopic group (p=0.763). There were no significant differences in mean blood loss (176.0 cc versus 161.1, p=0.752), andcomplication rate (20.0 versus 5.0%, p=0.014) between the LESS and conventional laparoscopic group. Postoperative pain, as measured by visual analogue scale at postoperative day 1 (4.4 versus 5.3 points,p=0.011), 3 (3.0 versus 4.3 points, p=0.001), and discharge (1.9 versus 2.8 point, p=0.018 ) was significantly lower in the LESS group. CONCLUSIONS: Retroperitoneal LESS radical nephrectomy is technically feasible and offers a safe surgical option for RCC, whichhave additional benefits of decreased postoperative pain and cosmetics.
Outcomes of Retroperitoneoscopic Live Donor Nephrectomy (RPLDN): Experience of 500 Cases at a Single Center
Outcomes of Retroperitoneoscopic Live Donor Nephrectomy in Patients with Renal Artery Aneurysm

Outcome of Retroperitoneoscopic Living Donor Nephrectomy in Obese Donors
Outcome of Kidney Transplantation with Right Single Versus Left Multiple Renal Arteries after Retroperitoneoscopic Donor Nephrectomy.
Hand-Assisted Laparoscopic Partial Nephrectomy; Finger Tip Dissection Technique and Early Outcomes
Purpose: We report our experience about hand-assisted laparoscopic partial nephrectomy (HALPN) with finger tip dissection technique. Materials and Methods: Between February 2007 and June 2011, 11 patients underwent HALPN in a transperitoneal approach. After entire hilum was thoroughly mobilized, only renal artery was hanged with a Nelaton catheter in case for hilar occlusion if bleeding occurs. Surgeon finger tip was used for the mass dissection that the resection plane is gradually deepened directing centrally along the renal pyramids with finger tip. During the procedure, if we felt the vessels, calyx on the finger-tip, we used hem-o-lok to secure. Results: The HALPN was successfully performed without any major complications and open conversion in all patients. Meantumor size was 2.1cm (range 1.0-3.0cm), operation time was 163mins (range 120-310mins). All patients had negative resection margin and 6 patients do not clamped renal artery. Mean warm ischemic time was 23.3min (range 15-30mins). Mean EBL was 305ml (range 63-980ml) and two patients got transfusion after operation. Conclusions: HALPN with finger tip dissection technique for small renal mass is safe and effective treatment method. Due to the tactile sense of finger, operator can do the mass dissection and bleeding control easier and safer.
Department of Urology, Cheil General Hospital, Kwandong University, Seoul, Korea
OBJECTIVE: The use of the daVinci robotic surgical system has allowed surgeons to perform partial nephrectomy through an umbilical incision. Our objective is to compare the outcomes between modified robot-assisted laparoendoscopic single site partial nephrectomy (modified RLESSPN) and standard robot-assisted laparoscopic partial nephrectomy (RALPN).METHODS: From May 2009 to February 2010, 35 modified RLESSPN were done by a single surgeon in our institution. A cohort of 35 patients who underwent RALPN from September 2006 to July 2009 was selected for retrospective comparison, and matched for tumor size, depth, and location. All patients underwent PN using the daVinci surgical robotic platform. Modified RLESSPN used a home-made umbilical port and an assistant port at the infraumbilical area while RALPN utilized standard laparoscopic port placement. RESULTS: There was a non-statistically significant longer operative time (187.5 vs. 172.1 minutes, p=0.149), longer warm ischemia time (29.5 vs. 29.4 minutes, p=0.210), higher estimated blood loss (257 vs. 253.4ml, p=0.884), higher blood transfusion (8.6% vs 2.9%, p=0.303) and complication (17.1% vs. 14.3%, p=0.743) rates, higher pain scores on the 1st post-operative day (4.5 vs. 4, p=0.275) and in-hospital morphine requirements (130.5 vs. 119.2mg, p=0.415) in the modified RLESSPN group. CONCLUSION: This comparison of modified RLESSPN to standard RALPN shows that the outcomes of both techniques are comparable with a trend toward better outcomes in the RALPN group. Until a more advanced robotic platform specifically designed for LESS is developed, robot-assisted single port surgery cannot be widely recommended.
Bilateral Purely Laparoscopic Radical Nephrectomy for Renal Cell Carcinoma: A Case Report
IntroductionBilateral nephrectomy is an infrequently performed procedure. The indications include bilateral masses too large for nephron-sparing surgery, uncontrolled hypertension and pain, infection,or large symptomatic polycystic kidney disease in patients on dialysis and kidney transplant recipients. Only a few case reports exist today describing synchronous purely laparoscopic treatment of bilateral solid renal masses. PurposeTo report the clinical experience with bilateral purely laparoscopic radical nephrectomy for renal cell carcinoma (RCC).Materials and MethodsA 70-year-old man was reffered for the management of bilateral renal masses. On abdominal CT, he had bilateral enhancing renal masses suspicious for RCC (rt side: 10.3x9.2x8.1cm, lt side: 8.5x7.1x6.6cm). He underwent bilateral transperitoneal purely laparoscopic radical nephrectomy. He was placed in a semiflank position for both sides. On the left side, 4 trocars were placed and the specimen was extracted through a 7-cm lower midline incision. Afterwards, the trocar sites and incision were closed and the patient was repositioned. On the right side, 5 trocars were placed and the specimen was extracted through the same incision.ResultsThe procedure was completed in 481min (endoscopic time: rt side was 186min and lt side was 170min). There were no intraoperative or postoperative complications, and the blood loss was 30ml. Final pathology revealed a right clear cell RCC stage pT2bN0 and a left clear cell RCC stage pT2aN0.ConclusionsBilateral purely laparoscopic radical nephrectomy can be performed safely and efficiently. This technique assures the patient the benefits of minimal invasive surgery in terms of postoperative pain and recovery.
Retroperitoneoscopic Laparoscopic Pyeloplasty for Primary Uretero-Pelvic Junction Obstruction in Horse-Shoe Kidney.
Aim: To present our experience of retroperitoneoscopic laparoscopic pyeloplasty for primary uretero-pelvic junction obstruction (right moiety) in a patient with horse-shoe kidney (HSK). Material and Methods: A male aged 20 years, presented with recurrent right flank pain. His renal ultrasound revealed the presence of horse-shoe kidney with moderately dilated pelvicaliceal system of right moiety. The intravenous urogram showed the presence of HSK of right sided hydronephrosis. DTPA scan confirmed the right sided subrenal obstruction with split renal function of 40%. The patient was managed by right retroperitoneoscopic laparoscopic pyeloplasty. Cystoscopy and right double J stent insertion was performed prior to the surgery. One 10 mm port was placed for the camera, below and in front of 12th rib. Retroperitoneal space was created and indigenous balloon dilatation for space creation was performed. One 12 mm port in anterior axillary line and another 5 mm port in posterior axillary line were placed. The redundant pelvic wall and stenotic segment of the right upper ureter were excised. The ureteric lumen was spatulated and ureteropelvic anastomosis was performed using 4-0 polyglactin over a double J stent.Result: IVU was performed following stent removal and showed dependent and patent ureteropelvic anastomotic region. DTPA scan done 6 months later and did not reveal any obstruction.Conclusion: Retroperitoneoscopic laparoscopic pyeloplasty in primary UPJ obstruction in a horse-shoe kidney is an effective minimally invasive treatment.
Departments of Urology, Chi Mei Medical Center, Tainan, Taiwan
Introduction: Living-donor nephrectomy is performed via a standard flank approach during open surgery in contrast to laparoscopy where kidneys are procured transperitoneally.Purpose: Being more familiar with retroperitoneal laparoscopic for the surgery of the upper urinary tract, we investigated the feasibility of living donor nephrectomy by this approach. Materials and Methods: We perform laparoscopic retroperitoneal nephrectomy in 8 living donors. The patients were placed in flank position. The retroperitoneal space was developed with blunt finger dissection, through a 2-cm mini-lumbotomy above anterior superior ileal crest in the posterior axillary line. After primary access to the renal artery and vein, these were dissected to their junctions with the aorta and inferior vena cava, respectively, before freeing the kidney of its perinephric attachments. The kidney was delivered manually, through Gibson " s incision or Pfannenstiel incision. Results: The average duration of surgery was 193±48 (120∼240) min; warm ischemia time less than 5 min (4.9±2.0). Average blood loss was 153 ml. Most of donors present grade 2 postoperative morbidity accorded to modified Clavien grading system and were discharged after an average of 3.8±1.1 days(2∼6). All 8 kidneys harvested laparoscopically had immediate function with urine production after revascularization; most patients " serum creatinine levels returned to normal within 1 week. Conclusion: Our data suggest that retroperitoneal laparoscopic donor nephrectomy may represent a reasonable option in centers in which more extensive experience has been accumulated with retroperitoneal than with transperitoneal laparoscopy for the surgery of the upper urinary tract.
Retroperitoneoscopic Partial Nephrectomy versus Open Partial Nephrectomy for Small Renal Tumors: Results of a Retrospective Trial of Chinese Patients
Objective We evaluated the efficiency and safety of Retroperitoneoscopic Partial Nephrectomy(RPN) for Small Renal Tumors. Materials and Methods Clinical data on 28 patients who underwent retroperitoneoscopic partial nephrectomy were retrospectively compared with those 24 who received Open Partial Nephrectomy(OPN),including patient demographic date, perioperative indexes and clinical outcomes. Results There were no significant difference in age, sex and tumor size in the two groups. Except one patient in the RPN group was transferred into open surgery because of serious bleeding from renal artery,all procedures were successful performed. In the comparison of intraoperative parameters,the operative time in RPN group was higher than OPN group(118.4±16.2min vs 102.3±22.4min ), but the difference had no statistical significance. The intraoperative estimated blood loss was comparable between the two groups(102.6±12.8mlvs298.1±19.5ml, P>0.05) .The warm ischemia time in the RPN group was 26.6±4.2min,and 16.5±1.8min in the OPN group. The difference was significant. Comparison of postoperative parameters showed that the use of analgesic, resumption of oral intake and postoperative hospital stay were better in the RPN group(P<0.05).The serum creatinine of all patients in the two groups were normal postoperatively. No serious complications occurred, the complication rate was 26.2% in the RPN group,and 25.4% in the OPN group,no difference was observed. During the follow-up of 1 to 30 months,no tumor reoccurence or metastasis developed. Conclusion Although retroperitoneoscopic partial nephrectomy is a technically challenging procedure, it can be performed in a safe manner with perioperative outcomes comparable to those reported for open approach.
Laparoscopic Radical versus Laparoscopic Partial Nephrectomy for Clinical pT1 Renal Cell Carcinoma: Comparison of Perioperative, Pathological and Functional Outcomes
Objective: To compare outcomes in patients undergoing laparoscopic radical nephrectomy (LRN) and laparoscopic partial nephrectomy (LPN) for small renal masses.Patients and Methods: This study included 177 and 51 patients who were treated with LPN and LRN, respectively, and subsequently diagnosed as having pT1 renal cell carcinoma (RCC) between 2004 and 2010. Perioperative, pathological, and postoperative outcomes were compared between these two groups.Results: There were no significant differences in age, gender and preoperative eGFR between the LRN and LPN groups. Despite the lack of significant difference in estimated blood loss, operative time in the LPN group was significantly longer than that in the LRN group. There were no significant differences in the incidences of intra- and post-operative complications between these two groups. All patients in the LPN groups were diagnosed as having pT1a disease, while there were 67 patients with pT1b disease in the LRN group. During the observation period of this study, disease recurrence developed in 9 patients in the LRN group, of whom 4 died of disease progression, however, no recurrence occurred in the LPN group. A 32.4% and 11.3% decline in eGFR was observed in the LRN and LPN groups, respectively.Conclusion: Surgical treatment for pT1 RCC could provide comparatively favorable outcomes irrespective of surgical approaches; however, preservation of postoperative renal function in the LPN groups was evidently superior to that in the LPN group.
Clinical Experience of Laparoscopic Nephroureterectomy in National Defense Medical College
Introduction. We evaluated clinical results in patients undergoing retroperitoneal endoscopic nephroureterectomy (LNUx). Methods. We performed 54 LNUxs after 2001. In the operation the affected kidneys were transected endoscopically, and the bladder-cuff resection was performed using Gibson's incision.Results. The 54 patients undergoing LNUx included 40 male and 14 female. The average age was 67.7 years. The tumors included 29 renal pelvic tumors, 21 ureteral tumors and 4 other pathology. The average operation time of LNUx was 220 minutes and the average of total operation time was 315minutes. The average amount of blood loss in laparoscopic procedure was 71 ml (median; 26cc). In one patient the operation was converted to open procedure due to a hemorrhage from IVC.Two severe complications including intraoperative hemorrhage from IVC and a perforation of duodenum in postoperative day1 occurred in the first half of the patients undergoing LNUx, and no severe complication was encountered in the last half. The median start of food intake was postoperative day 2. The median postoperative hospitalization was 11 days. The 3-year and 5-year cause specific survival rates were 85.4 and 80.9%, respectively. Intravesical recurrence was found 15 of 50 patients (30%). In eight patients,24h vesical irrigation using adriamycin (ADM) was performed just after the operation, and the occurrence of vesical recurrence was not significantly different between patients with ADM irrigation and those without ADM irrigation.Conclusion. Although the complication rate and the quality of operative procedures gradually improved, efforts to improve surgical outcomes of LNUx must continue.
Department of Urology, Kinki university faculty of medecine
Laparoscopy is a standard surgical option for live donor nephrectomy. The aim of this study was a retrospective assessment of the safety of laparoscopic live donor nephrectomy.From July 2009 to January 2011, we performed 21 laparoscopic live donor nephrectomy(4 right nephrectomies, 17 left nephrectomies) . Hand assisted laparoscopy was performed in all cases. All donors are alive and 20 recipients are alive (only one recipient died with functional graft). Donor's mean BMI were 22.8. The mean operative time was 243.57 + -46.0min(range 145-352). The mean blood loss were 46.1 + -10.1ml(10-152),and there were no case of blood transfusion.Surgical complication in the donors was one surgical site infection.The donor's mean hospital stay was 11.09 + -2.71 days. Laparoscopic live donor nephrectomy was confirmed to be safe and effective.
Laparoscopic Live Donor Nephrectomy at a Single Center Experience.
Introduction: Laparoscopic donor nephrectomy (LDN) is now widely accepted as a minimal invasive procedure for donor of living renal transplantation. Since September 2001, LDN has been performed as a standard procedure for donor of living donor nephrectomy at our institution. We compared our experience with laparoscopic and open donor nephrectomy in our institution.Patients and Methods: Between 1992 and 20010 we preformed open donor nephrectomy and 63 pure laparoscopic donor nephrectomy. In LDN, there were 19 males and 46 females with median age of 57 (range, 33-73) years old. RESULS: Mean BMI of donors was 23.4 (range 18-26). 51/63 (80.9%) patients were left LDN. Mean operative time was 256 (145-350), warm ischemic time was 343 seconds (120-710). Mean length of hospital stay was 7.3 (4-13) days. Only one patient was led to open conversion. There have been no cases of donor renal failure or procedure-related death. Donor nephrectomy was associated with less blood loss (p<0.01), a shorter hospital stay (p<0.01), less analgesic usage (p<0.01) compared to open donor nephrectomies.Conclusion: Laparoscopic donor nephrectomy resulted in less blood loss and shorter hospital stay than open nephrectomy. LDN appears to provide advantages for the donor in comparison to open donor nephrectomy.
Laparoscopic Surgery for Retroperitoneal Schwannoma
We report three cases of retroperitoneal schwannoma treated by laparoscopic surgery. They included one male and two female patients, and their age ranged from 54 to 65 years. All of them were diagnosed incidentally. With a diagnosis of non-functioning adrenal tumor in two patients and retroperitoneal neurogenic tumor in one, all three patients underwent laparoscopic surgery with transperitoneal approach. Operative time ranged from 152 to 177 min, bleeding minimun to 100ml, and tumor weight 25 to 160 g. There were no adverse events in postoperative course. The treatment of retroperitoneal schwannoma is en-bloc resection. There were 16 reported cases of laparoscopically treated retroperitoneal schwanoma in Japan. Both transperitoneal and retroperotoneal approach are eligible, but we prefer transperitoneal aproach especially in case of large tumor.
Clinical Significance of the Laparoscopic Retroperitoneal Lymph Nodes Dissection for Urothelial Carcinoma of the Upper Urinary Tract
<Object>Lymph nodes dissection (LND) for urothelial carcinoma of the upper urinary tract (UCUUT) is getting common in ordinary clinical settings. We try to clear the role and feasibility of laparoscopic retroperitoneal LND for UCUUT.<Patients and Methods>We collected the data of the number of lymph nodes removed, complications and recurrence of 37 patients with laparoscopic retroperitoneal LND for UCUUT from April 2008 to March 2011. <Results>Laparoscopic retroperitoneal LND needed about one hour. We did not found any major complications. Sealing apparatus were useful to prevent lymphorrhea. The average number of lymph nodes removed was 7.6 (1-33), among which only two cases were positive. No clear correlations were observed between the number of lymph nodes and recurrence. <Conclusion> Laparoscopic retroperitoneal LND were feasible in ordinary clinical settings. Randomized clinical study is essential to elucidate the role of LND of UCUUT.
Comparison of Surgical and Functional Outcomes Between Laparoscopic and Open Partial Nephrectomy
Purpose
To compare surgical and functional outcomes of laparoscopic partial nephrectomy (LPN) and open partial nephrectomy (OPN).
Patients and Methods
From September 2005 to May 2011, 60 patients underwent LPN or OPN in our institution. After excluding imperative cases (10 patients) and cases of intraoperative conversion to radical nephrectomy (1 of LPN, 5 of OPN), a total of 44 patients were evaluated retrospectively. LPN (11 cases) and OPN (33 cases) were performed via retroperitoneal approach with cold ischemia except 1 case.
Results
In LPN versus OPN group, median age was 66 vs 69 years, operation time 220 vs 286 min, ischemic time 62 vs 47 min, blood loss 13 vs 294 ml, and maximum tumor diameter 1.6 vs 2.5cm, respectively. Blood transfusion was required only in one case of OPN. Histology was clear cell renal cell carcinoma in 82% of LPN and 88% of OPN. Positive surgical margin was identified in one case of each group, including angiomyolipoma in LPN and chromophobe renal cell carcinoma in OPN. Median ratio of postoperative eGFR to preoperative eGFR was 87.6% in LPN and 87.3% in OPN. There was only 1 case of major complication in OPN that required coil embolization because of postoperative pseudoaneurysm.
Conclusions
Although cold ischemic time tended to be longer in LPN because of learning curve, preservation of renal function was similar between LPN and OPN. We conclude that LPN is a safe procedure for small renal tumor with surgical and functional outcomes equal or superior to OPN.
Surgical and Oncological Outcome of Retroperitoneoscopic Nephroureterectomy for Upper Urinary Tract Tumor
Purpose: To evaluate surgical and oncological outcome of retroperitoneoscopic nephroureterectomy for upper urinary tract tumor.Materials and methods: Between Feb. 2005 and Mar. 2011, we performed consecutive 34 retroperitoneoscopic nephroureterectomies for upper urinary tract tumor. The patients consisted of 20 males and 14 females. After the kidney was freed by retroperitoneal approach, a 6 cm para-rectal incision was made for the dissection of lower ureter. The ureter was dissected free into bladder wall for cuff-resection. Result: Mean operation time was 202 min. including 112 min. with pneumoretroperitoneal time. Mean estimated blood loss was 154 g. We experienced 1 retroperitoneal hematoma, 1 wound infection, and 1 open conversion due to intraoperative blood gas deterioration. There were 15 renal pelvic tumors and 19 ureter tumors. Histopathologic diagnosis was urothelial carcinoma except for 1 MALT lymphoma. There were 2 pTis, 3 pTa, 14 pT1, 4 pT2, and 10 pT3 disease. Intra-vesical recurrence occurred in 9 cases during the mean follow-up of 17 months. Distant metastasis occurred in 5 cases after the operation. Cancer-specific survival was 100% during the follow-up periode.Conclusion: Retroperitoneoscopic nephroureterectomy for upper urinary tract tumor is safe and feasible. However, comparative study with open surgery is necessary for evaluation of cancer control of the present procedure.
Impact of the Number of Renal Vessels on the Laparoscopic Nephrectomy
Objective: In the present study, we sought to evaluate the exact number of the renal arteries and veins which should be transected during laparoscopic nephrectomy and its impact on the surgical parameters.Methods: From January 2003 to October 2010, 90 laparoscopic nephrectomies were performed at our institution, including 60 radical nephrecotomy for renal cell cancer and 30 nephroureterectomy for upper urinary tract urothelial cancer. The number of renal arteries and veins which divided during surgery, operative time, estimated intraoperative blood loss, post operative hospital day, as well as complication rate were recorded and studied retrospectively.Results: Multiple renal arteries and veins were found in 37(41.1%) and 24(26.7%) of the 90 kidneys, respectively. 45 (50.0%) kidneys had multiple arteries and/or multiple veins. Multiple renal arteries were presented in 37 kidneys and this significantly more often occurred on the right side than the left side: 23 of 45(48.9%) right kidneys vs. 14 of 45 kidneys(31.1%) left kidneys. No significant difference was found in a comparison of veins of the right and left kidneys. Significant difference was found between the single and multiple vessels groups for operating time in transperitoneal laparoscopic radical nephrectomy (p<0.05).Conclusion: Our results have shown that multiple renal vessels significantly increase operation time of transperitoneal laparoscopic radical nephrectomy. In half the cases, more than 3 vessels should be divided during laparoscopic nephrectomy. Anatomical knowledge of the variations in the renal vascular supply is important for laparoscopic renal surgeries.
Staged Management with Endovascular Abdominal Aortic Aneurysm Repair and Retroperitoneal Laparoscopic Radical Nephrectomy in an Elderly and High Risk Case
An 82-year-old male patient with hypertension and some comorbidities was referred to the department of urology and vascular surgery in our hospital because of a finding regarding his left double renal tumors and abdominal aortic aneurysm (AAA) with a diameter of 6cm on ultrasonography. He was deemed to be an appropriate candidate for endovascular AAA repair (EVAR) by his vascular surgeon team and retroperitoneal laparoscopic radical nephrectomy by us based on preoperative imaging. Because of high age and his comorbidities, a staged management was planned: EVAR followed by nephrectomy. The patient underwent successful EVAR for AAA. 3months later, the patient underwent retroperitoneal laparoscopic radical nephrectomy. Post nephrectomy, retroperitoneal abscess was occurred, but it was cured by drainage. The patient recovered well from both EVAR and drainage. For the patient with AAA and renal tumors, especially in an elderly and high risk case, we recommend a combination of minimally invasive treatment of EVAR and retroperitoneal laparoscopic surgery in a staged management.
Oncological Outcomes after Nephroureterectomy for Upper Urinary Tract Urothelial Cancer: Laparoscopic versus Hand-Assisted Laparoscopic versus Open Approaches
Department of Urology, Nagoya Tokushukai General Hospital, Nagoya, Japan
(case report) 35-years old woman. The chief complaint was microscopic hematuria. A cystic tumor as big as 9cm was detected just anterior side of the right kidney. A cystic tumor was water density on CT and MRI. Malignant potential was not suspected. After half a year, the cystic tumor increased to an excess large 12cm. An abdomen dull pain and a right hydronephrosis came to be taken as an symptom. The cystic tumor was removed with en bloc laparoscopically. The content liquid is chyle. Immunohistochemically, ndothelium-like cells had D2-40 positivity, the CD34 positivity, and calretinin negativity, cystic tumor was diagnosed as the retroperitoneal lymphangioma. The relapse is not admitted though two years after the operation. The lymphangioma is a benign tumor with both peaks in infant period and in one's forties, and it accounts for 0.25% of the retroperitoneal tumor. The spontaneous involution is few and the complete surgical resection is basic of treatment.
Knotless uninterrupted running suture using V-Lock180™ stitch in laparoscopic partial nephrectomy
Objective: To assess the surgical outcome of knotless uninterrupted running suture using V-Lock180™ stitch in laparoscopic partial nephrectomy. Patients and Methods: In May and June 2011, 7 patients underwent laparoscopic partial nephrectomy using knotless uninterrupted running suture using V-Lock180™ stitch. The median age, BMI, and maximum tumor diameter were 61 years old (40-82 years), 23.3 (17.3-31.8), and 17mm (14-22mm), respectively. Four of the tumors were protruded and 3 were buried. Transretroperitoneal and transperitoneal approaches were used in 3 and 4 patients, respectively. Partial nephrectomy with hypothermia using ice-cold saline was performed during temporary renal artery clamping. In a case of exposure of the urinary tract, running suture repair was performed with an absorbable stitch. The renal parenchyma was stitched with 2-0 V-Lock180™ thread of approximately 30cm in length. After application of thrombin sealant to the defect, the thread was tightened and locked with a Hem-o-lok clip at the tip and end. Renal reperfusion was resumed after completing the parenchymal suture. Results: The median renal ischemic time, insufflation time, estimated blood loss, and tumor weight were 22min (15-31min), 180min (132-232 min), 10ml (5-350ml) and 8g (4-27g), respectively. No patients required open conversion or had operative complications. All specimens were tumor-free at the surgical margin. The median time from the operation to discharge was 7 days. Conclusion: Knotless running suture using V-Lock180™ stitch in laparoscopic partial nephrectomy was simple and safe. Further studies are needed to confirm the utility of this wound closure device.
DEpartment of Urology, Teiko Univesity Chima Medical Center
Objective) We tracked various proficiency indicators for the learning curve as a single Japanese surgeon became familiar with laparoscopic pyeloplasty by performing 51 initial procedures.Methods) Between April 2005 and June 2011, 51 consecutive patients were classified into Group 1 (Cases 1-17) or Group 2 (Cases 18-34) or Group3(cases35-51). Pre-operative clinical characteristics, operative parameters, and postoperative parameters were assessed.Results) The success rate was100%. The mean follow-up was 26.8 months (range 2-62). Intraoperative complications occurred in 1 (2.0%) of 51 patients and postoperative complications in 3 (6%) of 51 patients. No statistically significant differences were seen between the incidence of intra- and postoperative complications among the compared groups. Pre-operative stent were significantly higher in Group 2 than in Group 1 (7.03 vs. 6.13, P<0.01). The duration of surgery showed a statistically significant reduction from200.3 minutes in Group 1 to154.3 minutes in Group 2 (p<0.01 )and 147minutes in group3. There was no other difference among 3 groups.Conclusion) After gaining experience by performing an initial 51 laparoscopic pyeloplasty. the subsequent 17 surgeries established proficiency as determined by duration of surgery.
Laparoscopic Pyeloplasty for Ureteral Obstruction Associated with Horseshoe Kidney
BMI as a Predictor of Intraoperative Blood Loss in Laparoscopic Radical Nephrectomy
Purpose: We evaluated the effect of BMI on perioperative data in laparoscopic radical nephrectomy for patients with kidney tumors. Methods: We reviewed the medical records of patients treated with laparoscopic radical nephrectomy at our hospital and assessed the association between BMI and clinical results.Hand-assisted laparoscopic surgery, laparoscopic partial nephrectomy and nephroureterectomy for urothelial malignancy were excluded. Results: Twnety-seven patients were identified. Sixteen were male and 14 had the disease in the left side. Retroperitoneal approach was employed for 20 patients (74%) and transperitoneal for 7 (26%). Histological subtype were clear cell (20 patients, 74%), papillary (2, 7.4%), chromophobe (1, 3.7%), angiomyolipoma (1, 3.7%), and metastasis from other malignancy to the kidney (3, 11.1%). Mean age, height, weight, BMI, and tumor diameter were 65.6 years, 161.2 cm, 61.1 kg, 23.5, and 33mm, respectively. Seven patients had BMI 25.0 and over (mean, 27.4) and the rest had BMI less than 25.0 (mean, 22.1). No difference was observed in age, height, tumor diameter, and operative duration between high and low BMI groups. Intraoperative blood loss was significantly greater in high BMI group (mean, 189.9 ml) than low BMI (mean, 62.2 ml). Conclusion: High BMI may be a risk factor for intraoperative bleeding in laparoscopic radical nephrectomy.
Evaluation of the Effect of Mannitol on Postoperative Renal Function in Patients Who Underwent Laparoscopic Partial Nephrectomy
(Objective) We administered Mannitol to patients during laparoscopic partial nephrectomy in order to protect their renal function. But the effect of Mannitol on postoperative renal function was not evident. We compared their postoperative renal function with that of the patients who underwent laparoscopic partial nephrectomy without Mannitol.(Material and Methods) We retrospectively reviewed the records of 66 patients who underwent laparoscopic partial nephrectomy from March 1986 to March 2011 with normal contralateral renal function and who were followed-up postoperatively for at least 3 months. Of the 66 patients, Mannitol was administered to 12 patients(Group A) and not to 54 patients(Group B). We compared the postoperative serum creatinine between the two groups.(Results) In Group A, the mean age was 61.4 years, mean operative time was 197 minutes, mean resected tumor size was 17.5 mm, and mean preoperative serum creatinine was 0.815. In Group B, the mean age was 58.4 years, mean operative time was 260 minutes, mean resected tumor size was 18.9 mm, and mean preoperative serum creatinine was 0.803. There were no significant differences in clinical features other than the operative time between the two groups. Mean postoperative serum creatinine was 0.905 and 0.901 at 1 month after surgery, and 0.891 and 0.869 at 3 months after surgery respectively in Group A and Group B. There were no significant differences in postoperative creatinine between the two groups.(Conclusion) In this study, we cannot find any advantage of administering Mannitol during laparoscopic partial nephrectomy for patients with normal contralateral renal function.
Clinical Outcome of Retroperitonal Laparoscopic Nephroureterectomy Performed by an Inexperienced Surgeon for Renal Pelvis and Ureter Cancer
Objective: To evaluate the safety and cancer control of retroperitoneal laparoscopic nephroureterectomy (RLNU) performed by an inexperienced surgeon, we compared clinical outcomes between RLNU and open nephroureterectomy (ONU). Materials and methods: From 2005 to 2010, thirty five patients underwent RLNU (n=16) or ONU (n=19) for pelvic or ureter cancer at our hospital. RLNU was performed by an inexperienced surgeon without instruction of certificated surgeon during operation. Perioperative parameters (operative time, blood loss, and complications), and oncologic outocomes (intravesical recurrence and overall survival: OS) were analyzed retrospectively. Results: The median operative time of RLNU and ONU was 345 and 284 minutes (p<0.005), and the median blood loss was 123ml and 218ml (p<0.028) respectively. Severe adverse event was not observed in RLNU group. Time to start of eating, walking, and hospital stay was significantly shorter in RLNU group. There was no significant difference in patient characteristics and pathological results between two groups. Regarding oncologic outcomes, no significant difference was found in both OS rate and intravesical recurrence rate between two groups.Conclusions: RLNU could be performed safely and less invasively, in addition it might provide equivalent oncologic outcome compared with ONU, even if RLNU is performed in the hospital without certificated surgeon.
Laparoscopic Radical Nephrectomy is Less Invasive Compared with Open Radical Nephrectomy Regarding the Post Operative Atrophy of Abdominal Rectus Muscle
Objective: To compare the invasiveness of laparoscopic surgery with that of conventional open surgery, we retrospectively determined the postoperative atrophy of the abdominal rectus muscle (ARM) in patients who underwent radical nephrectomy (RN). Material and Methods:From January 2005 to May 2011 we conducted RN for 87 patients with renal cell carcinoma. Of those patients preoperative and postoperative image data of abdominal CT scan were available in 39 patients. Laparoscopic RN with reteroperitoneal approach and transperitoneal open RN were conducted in 12 patients and 27 patients, respectively. Open RN were carried out with midline incision (9 cases), subcostal incision (15 cases) or L-shape incision (3 cases). Preoperative and post operative rectus muscle volume on the operative side at the umbilical level were determined based on the CT scan image and compared in each case. Results: Postoperative muscle volume 6 months after surgery in laparoscopic RN group and open RN group were respectively 94.8+9.3% and 77.2+18.6% of preoperative volume. In open RN group, postoperative muscle volume of midline incision cases, subcostal incision cases, and L-shape incision cases were respectively 96.9+9.3%, 68.6+12.5%, and 60.6+18.4% of preoperative volume. Muscle atrophy in subcostal incision cases, and L-shape incision cases were significantly (P<0.01) greater than that of laparoscopic group. Conclusion: Laparoscopic RN was less invasive compared with open RN using subcostal incision or L-shape incision with regard to the post operative atrophy of abdominal rectus muscle.
Retroperitoneoscopic Live Donor Nephrectomy: Current Our Procedure and Outcome
IntroductionLiving donor kidney transplantation has been carried out in 60 patients since March 2003 until June 2010 at our institution. After 10 successful open donor nephrectomy, hand-assisted retroperitoneoscopic nephrectomy was started. We will show our current operative procedure and clinical outcome.Materials & MethodsChanges in operative techniques over time were separately analyzed according to the early 25 patients and the latter 25 patients. Operation time, warm ischemic time, time to urine production after revascularization and complications were investigated. ResultsDifferences in operative techniques between the two periods were 1) timing of hand-assistance 2) frequency of vessel sealing device usage 3) way of kidney removal. Mean operative time of the earlier group was 327 minutes and that of the latter group was 258 minutes (P=0.34). Mean warm ischemic time of the earlier group was 306 seconds and that of the latter group was 243 seconds (P=0.88). Mean Time to urine production after revascularization was 24 minutes in the early group and 15 minutes in the latter group (P=0.34). There was no graft function delay. Open conversion was required in 1 case in the earlier group. ConclusionsThe intraoperative and perioperative parameters as to our laparoscopic donor nephrectomy in the current half cases have improved as compared to the earlier cases although they did not reach statistical significance. The hand-assisted retroperitoneal approach of laparoscopic donor nephrectomy is certainly safe and less invasive without compromising the harvested kidney function.
Three Cases of Local Recurrence of Renal Cell Carcinoma in Hemodialysis Patients after Retroperitoneoscopic Radical Nephrectomy
IntroductionAlthough laparoscopic radical nephrectomy for hemodialysis patients became a common type of surgery, narrow surgical space sometimes results in rapture of a renal cyst, which leads to accidental comorbidity and local recurrence of cancer. PurposeTo review characteristics of patients with local recurrence of renal cell carcinoma (RCC) after laparoscopic radical nephrectomy.Materials and MethodsBetween January 2000 and June 2011, 162 hemodialysis patients with RCC who underwent laparoscopic radical nephrectomy were the subjects of this study.ResultsThree patients (1.8%) appeared with local recurrence in retroperitoneal space (table). All cases underwent retroperitoneal approach radical nephrectomy. ConclusionsThe transperitoneal approach has the possibility to reduce local recurrence after radical nephrectomy in hemodialysis patients with acquired cystic kidney rather than the retroperitoneal approach because of large surgical space.
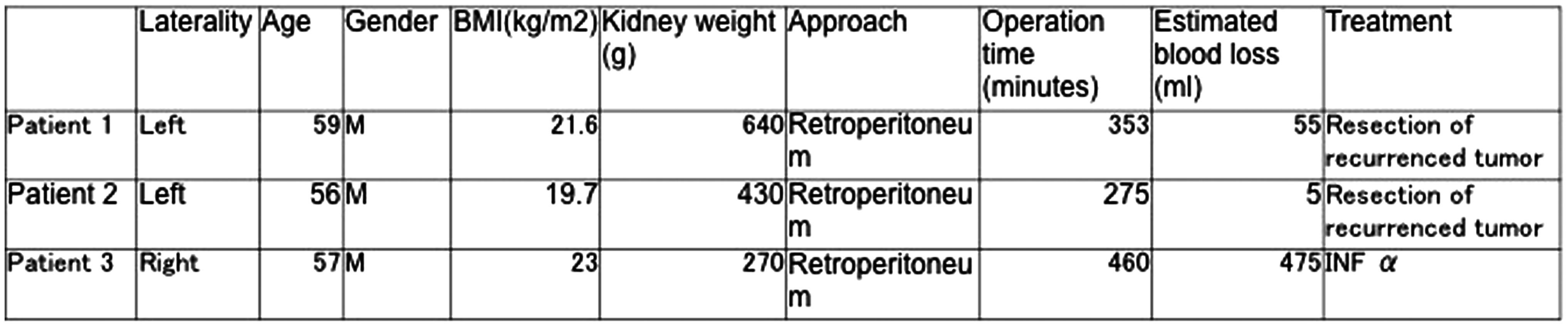
Clinical Outcome of Hand-Assisted Living Donor Nephrectomy
We commenced hand-assisted living donor nephrectomy in 2003. In this report, we compared the results of 60 cases of laparoscopic surgery and those of 38 cases of open one to assess the feasibility of the laparoscopic donor nephrectomy. We made comparative study on the operation time, the amount of blood, the duration of hospital stays, and the analgesic use frequency. The operation time for laparoscopic surgery was significantly longer, while the amount of blood and the duration of hospital stays for laparoscopic surgery were significantly shorter. The safety and the less invasiveness of laparoscopic donor nephrectomy are in the process of being established and our study has provided evidences to support this notion.
Department of Urology, chukyo Hospital
It is difficult to identify the narrow lumen of the ureter from the outside while performing laparoscopic pyeloplasty. We developed a new method to identify the narrow lumen of the ureter using a Fogarty catheter. A 4 to 5 French-sized Fogarty catheter was inserted from a small incision of the pelvis to the proximal ureter. It was inflated with air of 0.7ml and was withdrawn gently feeling the resistance. The narrow lumen of the ureter was identified and spatulated. The Fogarty catheter was inserted again. If the inflated balloon wasn't withdrawn easily, additional spatulation was done. Since 2007, we applied this technique for 11 children (median age 7.8 years) and 7 adults (median age 33.8 years) performed laparoscopic pyeloplasty. Symptoms were back or flank pain in 14, macrohematuria in 2 and renal dysfunction in 2. The operative methods were dismembered pyeloplasty in 17 and Fenger non-dismembered pyeloplasty in 1. In 17 patients (94%), followup studies revealed hydronephrosis was improved and symptoms were disappeared. One patient who underwent Fenger method was failed and reoperation by dismembered method was done. This technique is useful to perform successful laparoscopic pyeloplasty especially to patients whose ureters have more than two narrow sites.
Clinical Evaluation in Dialysis Patients who Underwent Laparoscopic Nephrectomy Without a Drainage Tube
IntroductionDialysis patients have to be ambulatory immediately after surgery to prevent postoperative complications, particularly pulmonary embolism, because most of them have a coagulation disorder. Laparoscopic surgery for renal tumors is suitable for dialysis patients with respect to minimally invasive therapy. Moreover, we do not place a drainage tube at the surgical site for early postoperative ambulation. Purpose To examine the postoperative clinical course after laparoscopic nephrectomy without a drainage tube in dialysis patients.Materials and Methods One hundred and one patients who underwent laparoscopic nephrectomy from April 2011 to March 2007 were the subjects of this study. Of these, no drainage tube was used for 66 patients.Results Patients without a drainage tube comprised 45 men and 21 women of median age 59 years (range: 12-75). Fifty eight and 8 patients underwent surgery by the transperitoneal and retroperitoneal approaches, respectively. Perioperative clinical courses were as follows: median operative duration (median: 232 minutes, range: 119-482), estimated blood loss (median: 15ml, range: 3-275) and postoperative hospital stay (median: 4.5day, range 2-15). One patient suffered phlebitis after surgery. Pathological findings showed malignancy in 52 and benign findings in 12 including a renal cyst in 10 and oncocytoma in 2. ConclusionsThere were no postoperative fatalities in the patients in whom no drainage tube was used. No placement of a drainage tube was thought to be the standard method of avoiding infection via a drainage tube, in a procedure coupled with early ambulation.
A Comparison of Early Complications Between Open and Robot-Assisted Radical Cystectomy
IntroductionRobotic cystectomy (RC) has been emerged as an alternative treatment of muscle-invasive bladder cancer. However, there has been a little data to compare the complication rate between open cystectomy (OC) and RC.PurposeThe aim of our study was to compare early complication rates between RC and OC using Clavien system. Patients and MethodsFrom September 2008 to March 2011, 35 and 104 patients underwent OC and RC, respectively. Data on all patients were reviewed retrospectively. All complications were categorized using a modified Clavien system. We also sought to identify independent predictive factors of grade II or greater complications.ResultsThere were no significant differences between OC and RC with regard to age, BMI, american society of anesthesiologists score, clinical stage, previous surgery history or sex. The RC group had more cases of ileal neobladder (p<0.001). We did not find any differences regarding pathologic stage or hopital stay. The OC had more grade II or greater complications (p=0.001), wound problems (p=0.043), multiple complications (p=0.014), greater estimated blood loss (p<0.001), and needed more transfusions (p<0.001). However, a longer operation time was required in RC group. Logistic analysis demonstrated that the OC (p=0.045, OR=2.44), EBL (>500 mL, p=0.013, 2.75) and female sex (p=0.028, 4.06) were independent predictors of grade II or greater complications. ConclusionsThe RC group was comparable to the OC group regarding complications using Clavien system. However, further long-term and randomized trials are needed because RARC is still not considered the standard therapy for bladder cancer.
Laparoscopic Radical Cystectomy with Ileal Conduit Urinary Diversion: A Single Surgeon Experience of 30 Cases with an Oncologic Follow-Up
Introduction: We present a single surgeon's experience and short-term oncologic outcomes of laparoscopic radical cystectomy (LRC) with ileal conduit in 30 patients. Purpose: To report a feasibility of LRC in the current era of robot-assisted surgery.Materials and Methods: Between November 2007 and May 2011, 30 patients (5 women and 25 men; median age 63 years, range 45 to 81) with bladder cancer underwent LRC and ileal conduit by a single surgeon. Urinary diversion was performed extracorporeally.Results: The median operating time was 527.5 minutes, and the median estimated blood loss was 275 ml. No patients required conversion to open surgery. The median time to oral intake was 5 days and the median postoperative hospital stay was 12 days. The immediate, early postoperative, and late postoperative complication rates were 6.7%, 20%, and 20%, respectively. Histopathologic analysis showed 40% of patients had organ-confined disease (stage pT2 or less), 30% locally advanced extravesical disease (stage pT3), 23.3% prostatic invasions (stage pT4), and 26.7% had node-positive disease. At a median follow-up of 16 (range 0.8 to 42.6) months, the overall survival rate and recurrence-free survival rate were 70% and 56.7%, respectively. Conclusions: LRC is a feasible procedure for the management of muscle-invasive bladder cancer and also can be a reasonable alternative to open radical cystectomy (ORC) or robot-assisted laparoscopic radical cystectomy (RALRC) in the current era of robot-assisted surgery. However, studies on the long-term oncologic outcomes after LRC and comparative studies with ORC and RALRC are needed.
The Department of Urology, University of Soonchunhyang, Cheonan, Korea
Introduction In laparoscopic partial cystectomy (LPC), exact lesion location and extent are essential for oncologically correct surgery and adequate tumor resection margins. Endoscopic India ink tattooing techniques are often used for the intraoperative location of polyps and early stage neoplasms in part of laparoscopic gastroenterological surgery. Purpose We applied this technique for planning the resection margin before laparoscopic partial cystectomy. Materials and Methods LPC was performed in 10 cases between October 2005 and December 2010 at our institute. Before surgery, the cystoscopy assisted India ink injection with fine needle was performed at intervals of 1 to 2cm approximately 1cm away from the outer margin of lesion. All patients were operated by transperitoneal approach with 3 or 4 trocars. Results All operations proceeded smoothly. Mean age of patients was 39.1 years old. Mean operative time was 130.5 minutes and mean estimated blood loss was 93 mL. Mean duration of Foley catheterization was 10.7 days and mean hospital stay was 13.1 days. No open conversion was required and no patient had significant peri-operative complications, but 1 case with delayed leak and 1 with delayed wound healing were found. The bladder pathologies included four urachal cysts, two pheochromocytomas, two inflammatory masses, one urachal cancer, one urachal remnant. Surgical margins were free of lesions in all patients. Conclusions The cystoscopy assisted fine needle tattooing technique with India ink is simple and effective technique for intraoperative location of pathological bladder lesion. This technique can help to determine the correct surgical margin during LPC.
First Experience of Robot-Assisted Laparoscopic Anterior Pelvic Exenteration for the Female Case of Muscle-Invasive Urinary Tract Carcinoma
INTRODUCTION: We have performed 70 cases of robot-assisted laparoscopic surgery including prostate and partial nephrectomy since August 2009. Here we report a case of robot-assisted laparoscopic anterior pelvic exenteration (RALAE) for recurrence of muscle-invasive bladder and right lower ureteral cancer. CASE: A 60-year-old female patient had undergone nephroureterectomy for left ureteral carcinoma at different hospital about 2.5 years ago. She was introduced to our institute for the treatment of recurrent UCs in bladder and right lower ureter. After 3 courses of preoperative chemotherapy, RALAE with resection of right-lower ureter was performed following rt-ureteral cutaneostomy. METHODS: Transperitoneal approach was applied with 6 port placement, which was almost same position with prostatectomy procedure (RALP) except about 3 cm higher than RALP. Under 8 mmHg of carbon dioxide pneumoperitneum, anterior pelvic exenteration was performed using the 30 degree down lens. Bladder, lower segment of right ureter, bilateral adnexal tissues and the uterus were dissected and removed en bloc through the vagina. Extended pelvic lymphnode dissection was also performed. Whole operational and console time were 231, and 181 minutes, respectively. Estimated blood loss was 400ml and no blood transfusion was needed. Pathological examination revealed T1 UC in bladder without ureteral or lymphnode involvement. Intra and post operative course was uneventful. CONCLUSIONS: Robot-assisted laparoscopic anterior pelvic exenteration was considered a safe and viable option for the female case of invasive bladder and ureteral cancer.
Complications and Surgical Outcomes Associated with Extended Pelvic Lymphadenectomy in Laparoscopic Radical Cystectomy
Introduction & Objectives: Extended pelvic lymphadenectomy (EPLND) belongs to the essential steps of radical cystectomy. In addition to staging, adequate EPLND has been found to alter both the prognosis for and the course of the disease after radical cystectomy.Material & Methods: From December 2009 to April 2011, we performed 18 laparoscopic cystectomies with an EPLND. Patient and tumor characteristics, the number of lymph nodes examined, and the postoperative complications encountered were evaluated.Surgical procedure: The approach is transperitoneal. five trocars are inserted and used a 30degree telescope during EPLND. Lymph node dissection is performed at obturator, deep obturator ,external iliac, hypogastric, presacral and common iliac nodes. The superior limit of this dissection is at least the aortic bifurcation.Results: Mean total operative time was 307 min (range 280-520), with a mean operative time of 104 min (range 77-127) for the EPLND. The average number of lymph nodes examined was 21.7 (range 10-36), with 8 nodes positive for metastasis. 0nly one patient had pelvic lymph node recurrence at 8 month after the surgery. A total of 2 complications occurred, including 1 lymphedema and 1 lymphocele.Conclusions: Our data indicate that, laparoscopic approach is an appropriate technique of extended pelvic lymphadenectomy fulfilling oncologic controls and present standards of radical cystectomy.
Depratment of Urology, Yokohama City Medical Center, Yokohama, Japan
Department of Urology, Osaka Medical College, Osaka, Japan
63-years-old man referred to our hospital as a bladder diverticulum. Cystoscopy and echography eventually revealed a solid tumor in the diverticulum of the bladder. Cold cup biopsy result was grade 1 urothelial carcinoma of the bladder. The tumor, along with the diverticulum were located close to ureteral orifice and the inlet of the diverticulum was small in size - made the transurethral resection not amenable. Therefore, retroperitoneoscopic bladder diverticulectomy were picked. Fat tissue of Retzius' surrounding the diverticulum made it difficult to detect the resection margin of the diverticulum. Hence, we utilized simultaneous cystoscopic light guidance, so that we were able to go through with the diverticulotomy with an adequate margin around the tumor. The bladder was sutured in two layers. Leak test filled with saline solution identified areas of leakage, which were subsequently reinforced with additional sutures. En-block histopathological diagnosis was grade 2 urothelial carcinoma accompanied with carcinoma in situ. Intravesical BCG immunotherapy for 6 weeks was postoperatively followed as an adjuvant therapy.
Department of Urology, NewYork-Presbyterian Hospital, Weill Cornell Medical College, New York, NY
INTRODUCTION AND OBJECTIVES: Prostate cancer patients are routinely diagnosed through biopsies. Many patients who have low Gleason biopsy score in their first biopsy are put on active surveillance, which typically leads to multiple biopsies. We hypothesize that multiple biopsies cause tissue scarring and dissection difficulties during surgery, which results in poorer functional outcomes.
METHODS: We retrospectively analyzed the data of 366 consecutive patients who underwent RALP between May 2009 and December 2009 at a single institution by a single surgeon. They were grouped into those who had single biopsy (n=316) and multiple biopsy (n=50) before the operation. Using DAmico risk criteria, patients were stratified into low, intermediate and high-risk groups. We excluded intermediate and high-risk cases, those with a pre-operative SHIM<22, and those that underwent non-nerve sparing surgery. We then matched the control group with the study group, yielding a total of 69 matched patients: 22 in the multiple biopsy group and 47 in single biopsy group.
RESULTS: At 3 months, 55.0% and 44.1% patients were potent in single biopsy and multiple biopsy groups respectively (p<0.05); at 6 months 84% and 75% patients were potent in single biopsy and multiple biopsy groups respectively (p<0.05). In terms of continence function, the two groups did not differ significantly.
CONCLUSIONS: Patients subject to multiple biopsies have worse potency outcomes after radical surgery than those who have gone straight for surgery after single biopsy. This needs to be taken into account when counseling patients regarding active surveillance.
Comparative Outcome Analysis of Open Versus Laparoscopic Versus Robotic-Assisted Radical Prostatectomy Matched by DAmico Risk in a Multinational, Multi-Institutional Database
INTRODUCTION AND OBJECTIVES: We report a comparison of the biochemical recurrence rates (BCR) of ORP, LRP, and RARP in a large multinational, multi-institutional series.
METHODS: 22,403 patients with prostate cancer underwent RP from January 2000 onwards by 40 surgeons at 15 institutions. 10,092 patients underwent ORP with a median follow up of 32.2 months; 7873 patients underwent LRP with a median follow up of 32.3 months; 4438 patients underwent RARP with a median follow up of 22.3 months. BCR was stratified by DAmico risk. Cox regression was used to identify independent predictors of BCR.
RESULTS: 7543 patients were DAmico low risk, 7387 patients were intermediate risk, and 2969 patients were high risk. The percentage of patients that remained free of BCR was 95.4% ORP, 93.0% LRP, and 97.8% RARP for low risk; 80.1% ORP, 82.1% LRP, and 94.2% RARP for intermediate risk; and 57.3% ORP, 68.0% LRP, and 86.4% RARP for high risk. Cox regression analysis identified preop PSA, RP Gleason 7, RP Gleason ≥ 8, positive margins, ECE, and SVI as independent predictors of BCR for all risk categories. LRP was also identified as an independent predictor of BCR for DAmico low risk, and RARP was identified as a negative predictor for DAmico intermediate (OR=0.64) and high (OR=0.68) risk groups.
CONCLUSIONS: RARP appears to be at least non-inferior to ORP and LRP in terms of short to medium term BCR rate, regardless of DAmico risk categorization.
Impact of Technical Modifications and Surgeon's Experience in Laparoscopic radical Prostatectomy on Early Continence Recovery
OBJECTIVE:We report the effect of surgeon's experience and simple method during LRP on continence recovery.
PATIENTS AND METHODS:Between July 2001 to June 2011, 292 consecutive patients underwent LRP in our center by a single surgeon. After gaining experience by performing an initial 130 LRPs, the subsequent surgeries were classified into three Groups according to 3 periods whether the experienced surgeon mainly performed the procedures or not, and whether there was surgical technique for improving urinary continence or not: Group 1 (2007 to 2008): experienced surgeon as the first surgeon and no additional methods to improve early return of continence (N=64), Group 2 (2009 to 20010): The assistant partially performed the procedures and anterior suspension (N=76), Group 3 ( 2011 to June 2011): the experienced surgeon as the first surgeon performed the entire procedures and anterior suspension and posterior reconstruction (N=22).
RESULTS:The groups were comparable with respect to patient demographics. The groups had similar operative time, estimated blood loss, and length of stay.Continence rate at 3 months was statistically higher in Groups 3 (90.0%) than in Group 2 (51.4%) and Group 1 (50.0%). positive surgical margin of pT2 and pT3 was 12.2 and 40.9% for group 1, 15.9 and 45.2% for group 2 and 7.7 and 2.2% for group 3.
CONCLUSIONS:Posterior reconstruction and anterior suspension procedure resulted in a statistically significantly higher continence rates at 3 mo after the procedure. Also, as a surgeon's experience increases, urinary function after radical prostatectomy improves.
Department of urology, College of medicine, The Catholic University of Korea, Seoul, Korea
INTRODUCTIONRobot-assisted laparoscopic radical prostatectomy (RALP) is gaining popularity in recent days. Despite of increasing case, just few data is available on the impact of previous surgical background on the learning of the RALP. We investigated that the different background of surgeon(laparoscopy-experienced versus laparoscopy-naive surgeon) may affect the surgical outcome after RALP.MATERIALS AND METHODSA total of 89 patients were enrolled who were treated with RALP by two surgeons from March, 2009 to March, 2011 at a single center.Patients were divided into two groups (laparoscopy-experienced (over 200 cases of LRP), laparoscopy-naive; n=53, n=36).We investigated factors including age, preoperative PSA, biopsy Gleason sum, operation time, pathology Gleason sum and surgical margin (SM) status. Then we compared these factors in these two groups. RESULTSThe study groups did not show the significant difference in age at surgery and preoperative PSA (p=0.10, 0.75). Mean operation time and blood loss were higher in laparoscopy-naive surgeon group (290.5 vs. 302.2 minutes and 392cc vs. 465cc for laparoscopy-experienced vs. laparoscopy-naive group, p=0.49, 0.22), but, did not show the significant difference. In aspect of SM, we could not find the significant difference between two groups (p=0.39).CONCLUSIONSAlthough mean of operation time and blood loss was higher in laparoscopy-naive surgeon group, there was no significant difference between two groups and, in addition, SM status in prostate cancer patient treated with RALP. But limit of study size, this study may need to be evaluated in larger size of patient group with longer period of follow-up.
Deparment of Urology, NewYork-Presbyterian Hospital, Weill Cornell Medical College, New York, NY
OBJECTIVES: We evaluated the impact of BMI on oncologic outcomes in patients treated with robotic-assisted radical prostatectomy (RALP).
METHODS: The study comprised of 2344 consecutive patients treated with RALP for clinically localized prostate cancer by a single surgeon at a single institution. BMI was defined as a categorical variable: normal weight (<25 kg/m2), overweight (25-29.9 kg/m2), or obese (>30 kg/m2).
RESULTS: The median patient BMI was 26 kg/m2 (IQR: 24-29); 589 patients had a normal weight, 1267 patients were overweight, and 488 patients were obese. There was no significant difference in clinical (PSA, total number of biopsy cores taken, total number of positive cores, maximum percent biopsy, Gleason score, perineural invasion, high grade prostatic intraepithelial neoplasia, and clinical stage) or pathologic (extracapsular extension, seminal vesicle invasion, and lymphovascular invasion) features across BMI categories. There was no significant difference in biochemical recurrence-free survival rates, overall positive surgical margin rates, and apical positive surgical margin rates across BMI categories. Actuarial biochemical recurrence-free survival rates at 70 months were>85% for all BMI groups.
CONCLUSIONS: BMI was not associated with oncologic outcomes in a contemporary cohort of patients treated with RALP for clinically localized prostate cancer. This could be due to good general health in this select cohort of patients or to surgeon experience/surgical technique. Longer follow up is needed to ascertain the impact of BMI on oncologic outcomes after RALP. Moreover, the effects of BMI on complications, erectile function, and continence after RALP remain to be investigated.
Impact of Repeated Prostate Biopsy on Laparoscopic Radical Prostatectomy
IntroductionLaparoscopic radical prostatectomy (LRP) has been widely used for prostate cancer. Several papers have reported a correlation between prostate weight, body mass index (BMI) and operative time. However, the effects of repeated transrectal needle biopsy (TRNB), which may cause severe adhesion to the rectum, has not been fully evaluated.Materials and MethodsWe retrospectively evaluated the records of 92 patients who underwent extraperitoneal LRP. The data were analyzed to determine whether repeated TRNB affects operative outcome. ResultsFourteen (15.2%) of the 92 cases underwent repeated TRNB. No significant differences in BMI, prostate weight, and with or without previous lower abdominal surgery and neoadjuvant hormone therapy were observed between one time and repeated TRNB group. Mean pneumoperitoneum time was 167.3min. Univariate analysis demonstrated that BMI, repeated TRNB, and prostate weight are significant predictors of prolonged time (p=0.001, p=0.020, p=0.027, respectively). Multivariate analysis demonstrated that BMI and repeated TRNB are significant indicators of prolonged time (p=0.001, odds ratio=1.432 and p=0.012, odds ratio=6.437). In the analysis of the step time of the dissection seminal vesicle, vas deference and prostate from rectum (mean 47.1min), BMI and repeated TRNB were independent factors for a longer time (p=0.002, odds ratio=1.435 and p=0.023, odds ratio=5.505). Although repeated TRNB caused a slight increase in estimated blood loss, it was not an independent factor. No significant difference in positive margin rates was observed between the two groups (p=0.326).ConclusionsAlthough LRP is technically established, it should be performed with caution in high BMI and/or repeated TRNB cases.
Are Men with Lower Urinary Tract Symptoms at an Increased Risk for Aggressive Prostate Cancer?
ABSTRACT WITHDRAWN
Assessment of Health-Related Quality of Life in Patients with Prostate Cancer after Laparoscopic Radical Prostatectomy
Objective:This study was undertaken to evaluate the health-related quality of life (HPQOL) after laparoscopic radical prostatectomy (LRP) at a single institution.Method:A total of 115 patients who underwent LRP were prospectively enrolled in this study. We measured the disease specific HRQOL with expanded prostate cancer index composite (EPIC) and International Prostate Symptom Score (IPSS). The participants were asked to complete the questionnaires before and 1, 3, 6, and 12 months after surgery.Results:The urinary and sexual scores in the 1 month were worse from baseline and urinary irritative/obstructive domain ahead of urinary incontinence score recovered to baseline within 6 month. Although urinary incontinence score and sexual score gradually recovered, they had not recovered to baseline level after 12 months. The bowel and hormonal score temporarily deteriorated at 1month, but they recovered to baseline level within 3 month postoperatively. Patients with moderate and severe lower urinary tract symptoms (LUTS) at baseline (IPSS ≥ 8, N=55) significantly improved IPSS and QOL index after 6months postoperatively. For these patients, urinary bother after 6month postoperatively was equivalent to the baseline level. On the other hands, in patients with mild LUTS at baseline (IPSS<8, N=60), the deteriorated urinary function and bother at 1 month after surgery gradually improved, but this did not recovered to baseline at 12 months.Conclusions:The deteriorated urinary irritative and obstructive score recovered to baseline within 6 month after LRP, but urinary incontinence domain did not recover to baseline at 12 months.
Robotic Radical Prostatectomy : Intial Experience at MPUH
Objectives : RARP is a known minimally invasive procedure for treating localized Carcinoma prostate. We present our initial experience of RARP in study period between September 2010 to May 2011. Materials and methods:A step by step approach of RARP is presented in this paper. We also analysed record of 31 patients who underwent of RARP during study period of September 2010 to May 2011. The patients were analysed for multiple variables including age, clinical stage, intraoperative complications, postoperative continence at 1 month and 3 month , mean PSA at 1 and 3 month.Results:Average age of the patients was 63±6.5 years & clinical stage was<T2N0M0. RARP was successful in all cases. The average operative time was 189±32 minutes. Posterior vesical dissection was difficult in 6 cases and urethrovesical anastomosis was difficult in 4 cases. Final Hisology report showed T3 disease in 10 ( 32%) patients . Continence rate at 1 month was 21/31 (74 %). During follow up maximum period of 6 month mean PSA in margin positive cases was 0.36±0.20 ng/ml and in margin negative cases was 0.25±0.22 ng/mlConclusion:RARP is good alternative as a minimally invasive, safe, effective procedure. Initial results of RARP are encouraging.
Department of Urology, New York-Presbyterian Hospital, Weill Cornell Medical College, New York, NY
INTRODUCTION AND OBJECTIVES: In this study, we evaluate BCR rates stratified by DAmico risk in a large cohort of robotic-assisted radical prostatectomy patients (RARP).
METHODS: 2309 patients underwent RARP at our institution and were followed up in terms of regular PSA checks. BCR was defined as a PSA≥0.2 at any post-operative time point, and patients were censored if and when this happened. Kaplan-Meier survival analysis was used to investigate BCR rates in low, intermediate, and high risk patients, defined by standard DAmico criteria.
RESULTS: 18/1370 (1.3%) low risk, 52/973 (5.3%) intermediate risk, and 44/229 (19.2%) high-risk patients suffered BCR at a median follow up of 16 months (range 2-70 months). The overall BCR rate for the three groups combined was 114/2572 (4.4%). Mean time to recurrence was 71.6 months (95%CI 69.4-73.8 months) for low-risk patients, 62.7 months (95%CI 60.6-64.8 months) for intermediate risk patients, and 50.1 months (95%CI 45.3-54.9 months) for high risk patients. The overall mean time to recurrence for the three groups combined was 68.1 months (95%CI 66.3-70.0 months). Actuarial recurrence-free survival rates at 70 months were>90% for low and intermediate risk patients and<70% for high risk patients. Log rank analyses revealed highly statistically different BCR survival rates when DAmico groups were compared to each other (p<0.001 for all pair wise comparisons).
CONCLUSIONS: RARP has at least equivalent short- and medium- term oncologic outcomes to other established treatments for early prostate cancer for all DAmico risk groups.
Feasibility of Laparoscopic Radical Prostatectomy in Complex Surgical Cases
Creation of a Nomogram for Predicting Gleason Sum Upgrading in Potential Candidates for Activesurveillance of Presumed Low-Risk Prostate Cancer
INTRODUCTION AND OBJECTIVES: We evaluated the pathologic outcomes in our cohort treated by robotic prostatectomy and who fit active surveillance criteria. A nomogram was devised to predict which patients in this group were at risk of Gleason upgrading which would exclude them from active surveillance.
METHODS: 750 radical prostatectomy patients from Jan 2005-present formed the study cohort. The radical prostatectomy specimens were graded, and any upgrading (Gleason sum>6) was considered an exclusion criterion for active surveillance. Univariate analyses were performed to determine the upgrading from the list of preoperative variables. A multivariate logistic regression model was used to develop a predictive nomogram for this purpose.
RESULTS: 297/750 (39.6%) patients were upgraded to>Gleason 7 at final pathology. Multivariate analysis found that preoperative PSA, number of positive cores and prostate volume were significantly predictive of Gleason upgrading. The nomogram was reasonably discriminatory between patients who would and would not have been eligible for surveillance.
CONCLUSIONS: Almost 40% of patients that were eligible for surveillance had worse prognostic factors when subjected to robotic prostatectomy. We suggest the use of this nomogram to adequately counsel primary prostate cancer patients deemed clinically eligible for active surveillance.

Department of Urology, NewYork-Presbyterian Hospital, Weill Cornell Medical College, New York, NY
OBJECTIVES: We investigated the risk of BCR in DAmico low risk patients with differing extents of upgrading as well as other clinicopathologic factors that might be independent predictors.
METHODS: 7080 out of 22,403 men who underwent radical prostatectomy at more than 15 institutions were categorized as DAmico low risk patients. Kaplan-Meier survival analysis was performed to compare BCR rates in patients with different extents of upgrading. Cox proportional hazard analysis was done to identify independent predictors of BCR. The median follow-up period for the selected patients was 30.6 months (IQR: 14.5-51.5).
RESULTS: GS upgrading to 3+4, 4+3, and >=8 was present in 35.6%, 8.5%, and 1.6% of patients on final histopathology, respectively. 96.8% of men with no GS upgrading remained free of BCR, while the percentages of patients who remained free of BCR with GS upgrading to 3+4, 4+3, and >=8 were 95.8%, 90.1%, and 84.4%, respectively. Cox proportional hazard regression modeling identified preoperative PSA (OR=1.18; p<0.001), upgrading to Gleason 4+3 (OR=2.21; p<0.001), upgrading to GS >=8 (OR=3.60; p<0.001), positive margins (OR=3.29; p<0.001), EPE (OR=1.61; p=0.004), and SVI (OR=3.17; p<0.001) as significant independent predictors of BCR.
CONCLUSIONS: Patients classified as DAmico low-risk upgraded to GS >=8 and 4+3 are at increased risk of BCR. Patients upgraded to 3+4 are not at higher risk of BCR. Preop PSA, positive margins, ECE, and SVI are also important independent predictors of BCR in this cohort
Outcomes of ORP vs. LRP vs. RALP for High Risk Prostate Cancer in a Large, Multi-National Institutional Database
INTRODUCTION AND OBJECTIVES: We report a comparison of the biochemical recurrence rates (BCR) of ORP versus LRP versus RALP prostate cancer patients defined as high-risk according to different criteria.
METHODS: 22,403 patients underwent ORP (n=10,092), LRP (n=7873), or RALP (n=4438) from January 2000 onwards. Four definitions of high-risk disease were used: (i) PSA≥20, (ii) Biopsy Gleason≥8, (iii)≥cT3, and (iv) DAmico high risk. Kaplan-Meier (KM) survival analysis was used to compare BCR rates and Cox regression analysis was used to identify independent predictors of BCR.
RESULTS: The percentages of patients that remained free of BCR were 46.4% ORP, 59.5% LRP, and 81.3% RALP with PSA≥20; 54.7% ORP, 63.5% LRP, and 83.3% RALP with Gleason≥8; 41.1% ORP, 67.4% LRP, and 81.8% RALP with≥cT3; and 57.3% ORP, 68.0% LRP, and 86.4% RALP with DAmico high risk. Cox regression analysis identified Preoperative PSA, RP Gleason 7, RP Gleason≥8, positive margins, ECE, and SVI as independent predictors of BCR in the Biopsy Gleason≥8 and DAmico High Risk groups. RP Gleason 7, RP Gleason≥8, ECE, SVI were independent predictors for the≥20 group, while RP Gleason≥8 and SVI were for the≥cT3 cohort. RALP was an independent predictor in the Biopsy Gleason≥8 (OR=0.60) and DAmico High Risk (OR=0.68) groups.
CONCLUSIONS: RALP appears to be at least non-inferior to ORP and LRP in terms of short to medium term BCR rates for all our high-risk cohorts.
kaomei Urologic Clinic, kaohsiung
Extraperitoneal laparoscopic radical prostatectomy (ELRP) was a minimally invasive and viable alternative to the open procedure. Here, we share our initial experience for ELRP in 20 patients Material and methods:Between February 2006 to June 2009, total of 20 patients underwent extraperitoneal laparoscopic radical prostatectomy. Demographic data, including age, preoperastive PSA, prostate volume , Gleason score, and ASA score were collected. Besides, Surgical parameters, pathological staging, postoperative complication, hospital stay, continence state, and oncological outcome were retrospectively reviewed.Results: The mean age was 67.5 (54∼81) years. Mean preoperative PSA was 24.6±15.8 ng/ml and prostate volume was 47.8±22.5 (17∼92) cc. Mean operative time was 325±58 (220∼465)minutes. Mean blood loss was 450±300 (250∼3000) ml. The mean post-OP hospitalization was 10.4±4.9 (5∼25) days. One major complication was deep venous thrombosis and venous filter implantation was applied. One anastomosis disruption and three had bladder neck contracture. All patients had transient stress urinary incontinence but almost 80% are continence 9 months later. Biochemical failure was noted in 5 patients, and they received adjuvant hormone or radiation therapy. All patients are alive except one had pelvic lymph node involvement (N1) with bony metastasis and was finally died in postoperative 34 months.Conclusion : A major benefit of ELRP is to avoid intraperitoneal injury compared with transperitoneal approach. Besides, it can also isolate the urine leakage. From our 5 year short-term follow up, it provides equality in tumor control as radical prostatectomy. We think as experience accumulated, better postoperative oncological and functional outcome could be expected.
Georgetown University, Department of Urology
Purpose: Open suprapubic simple prostatectomy is the treatment of choice for symptomatic, large volume BPH. While series of robotic-assisted simple prostatectomies have been reported, they are limited to medium-size prostates that may be amenable to transurethral treatments. We report our multi-institutional experience and outcomes with robotic-assisted simple prostatectomy for glands (>100gm).Materials/Methods: From August 2009 to May 2011, 13 robotic simple suprapubic prostatectomies were performed in patients with symptomatic large volume BPH (mean volume on transrectal ultrasonography 163cc). An essential aspect of our technique included use of use of a laparoscopic/robotic tinaculum grasper to aid in retraction of adenoma during dissection.Results: Mean operative time was 179 minutes (range 900 to 270), blood loss was 219 ml (range 50 to 500), hospital stay was 2.7 days (range 1 to 8), and foley catheter duration was 8.8 days (range 5 to 14). Mean specimen weight on pathological examination was 127 gm (range 100 to 165). Intraoperative complications included an introaperative leak in one patient and failure to progress with abortion of case in another. No patients required blood transfusions. All patients were followed for at least 4 months and significant improvement from baseline was noted in the international prostate symptom score (preoperative vs postoperative 18.1 vs 5.3, p<0.001) and the maximum urine flow rate (preoperative vs postoperative 4.3 vs 19.0 cc per minute, p<0.001).Conclusions: Minimally-invasive robotic simple prostatectomy is techincally feasible in patients with large volume (>100gm) BPH and is associated with significant improvement in obstructive urinary symptoms.
What Prevents Lymphocele Development after Laparoscopic Radical Prostatectomy?
<Purpose> We evaluated the efficacy of a vessel sealing device (VSD) and fibrin glue for the prevention of lymphocele development after laparoscopic radical prostatectomy (LRP). <Methods> A total of 120 patients who underwent LRP with pelvic lymphadenectomy were prospectively enrolled. The patients were randomly assigned to one of four groups; lymphadenectomy using a conventional technique (group 1), lymphadenectomy with the spraying of fibrin glue during lymph node dissection (group 2), lymphadenectomy with VSD (group 3), and the use of fibrin glue and VSD (group 4). All patients underwent CT scanning one month postoperatively to evaluate the lymphocele size. <Results> Lymphoceles over 1500 cm2 were observed in 23 cases (19.2%). Mean major axis of 23 cases was 78 mm. One (0.8%) was symptomatic with infection, and drainage tube placement was required. In the other 22 patients the lymphoceles developed asymptomatically and were detected by CT scanning. Lymphoceles were present in 9 of 30 patients in group 1, 9 of 30 patients in group 2, 3 of 30 patients in group 3, and in 2 of 30 patients in group 4. The groups with VSD had significantly lower lymphocele rates than those without. Multivariate analysis demonstrated that the VSD significantly prevented the occurrence of lymphoceles (p=0.017, HR=5.13). <Conclusion> The efficacy of VSD for preventing lymphocele development after LRP was confirmed, however, fibrin glue did not contribute to a reduction in lymphocele development.
Department of urology, Anjo Kosei Hospital, Aichi, Japan
Objective: Laparoscopic or extraperitoneal laparoendoscopic radical prostatectomy (RP) is generally performed using a five-port technique. We report a unique technique of two-port extraperitoneal laparoendoscopic RP with a multichannel trocar.Methods: Starting November, 2010, when we introduced two-port extraperitoneal laparoendoscopic RP, we have performed the procedure for 9 patients diagnosed with early-stage prostate cancer (cT1c,T2N0). In each case a multichannel port was inserted extraperitoneally through a 2.5-cm lower umbilical incision and one additional port was inserted in the left fossa to allow an adequate working angle during the most critical steps of the procedure.Results: The operation could be successfully completed in all 9 cases, without any necessity for conversion to a standard laparoscopic approach. Median operation time was 253 minutes (range 207-388), median blood loss, including urine was 808 ml (range 257-1454), and no patient required blood transfusion. Median Foley catheter indwelling period was 6 days (range 3-6) after the surgery. No intraoperative complications occurred.Conclusions: Judging from this initial trial, our original two-port extraperitoneal laparoendoscopic RP procedure can be readily performed safely if the surgeon is familiar with conventional 5 port laparoscopic radical prostatectomy. Additional investigations are now needed to further evaluate the safety and oncologic adequacy of this new approach.
Initial Experience of Laparoscopic Radical Prostatectomy in Tonami General Hospital, Japan
Introduction: Robot-assisted laparoscopic radical prostatectomy (LRP) is becoming popular as a minimally invasive surgery. However, in Japan, conventional open prostatectomy is still the mainstay due to limited availability of surgical robots. Under these circumstances, LRP without a robot may still play an essential role in Japan. Methods: Between November 2009 and May 2011, 41 LRPs were performed by a single surgeon. The evaluated parameters included age, preoperative PSA, clinical stage, pathological stage, biopsy Gleason score (GS), positive surgical margin (PSM) rate, estimated blood loss (EBL), operative time (OT), urinary continent status (defined as 0 to 1 pad use per day) and adverse events (AE) at surgery. Results: Mean age and preoperative PSA were 65.3 years and 13.7 ng/ml. Clinical stages were cT1c in 19 patients, cT2 in 19 and cT3 in 3. Biopsy GSs were 6 or less in 6 patients, 7 in 13 and 8 or greater in 12. Surgeries were successfully completed in all patients without any AE. Mean OT and EBL were 286 min and 288 g respectively. Overall PSM rate was 26.8% (13.8% for pT2 and 58.3% for pT3). Continence rate was 25% at 1 m, 71.8% at 3 m, 85.7% at 6 m and 95.8% at 1 y. Comparing the first half (n=21) with the second (n=20), mean OT and EBL were significantly decreased (347 vs 223 minutes, 340 vs 233 g). Conclusion: Although LRP is technically demanding, it can be performed safely even in a low volume center like Tonami General Hospital.
Analysis of the Factors that Influence the early Continence after Laparoscopic Radical Prostatectomy
Objectives: This study was aimed to analyze the factors that influence the early continence after laparoscopic radical prostatectomy (LRP). Materials and Methods: A total of 145 patients with clinically organ confined prostate cancer underwent LRP and were performed longitudinal surveys about quality of life. Of the 145 patients, 53 patients need one or less diaper a day at three months after LRP (group A) and 48 patients needed to wear 3 or more diapers a day (group B). All clinico-pathological parameters were compared between the two groups.Results: There were no significant differences in patient age, body mass index, operating time, estimated blood loss and prostate volume between the two groups, respectivel. Furthermore, whether nerve sparing surgery was performed or not was not correlated to the early continence at three months after LRP. However, significant high incidence of urinary incontinence was observed in the patients with the positive leakage at the urethrogram which performed routinely at seventh day after LRP (table). Conclusion: It was very difficult to predict the early urinary conditions by the pre and perioperative parameters. The finding of the postoperative urethrogram was significantly correlated to the early urinary continence.
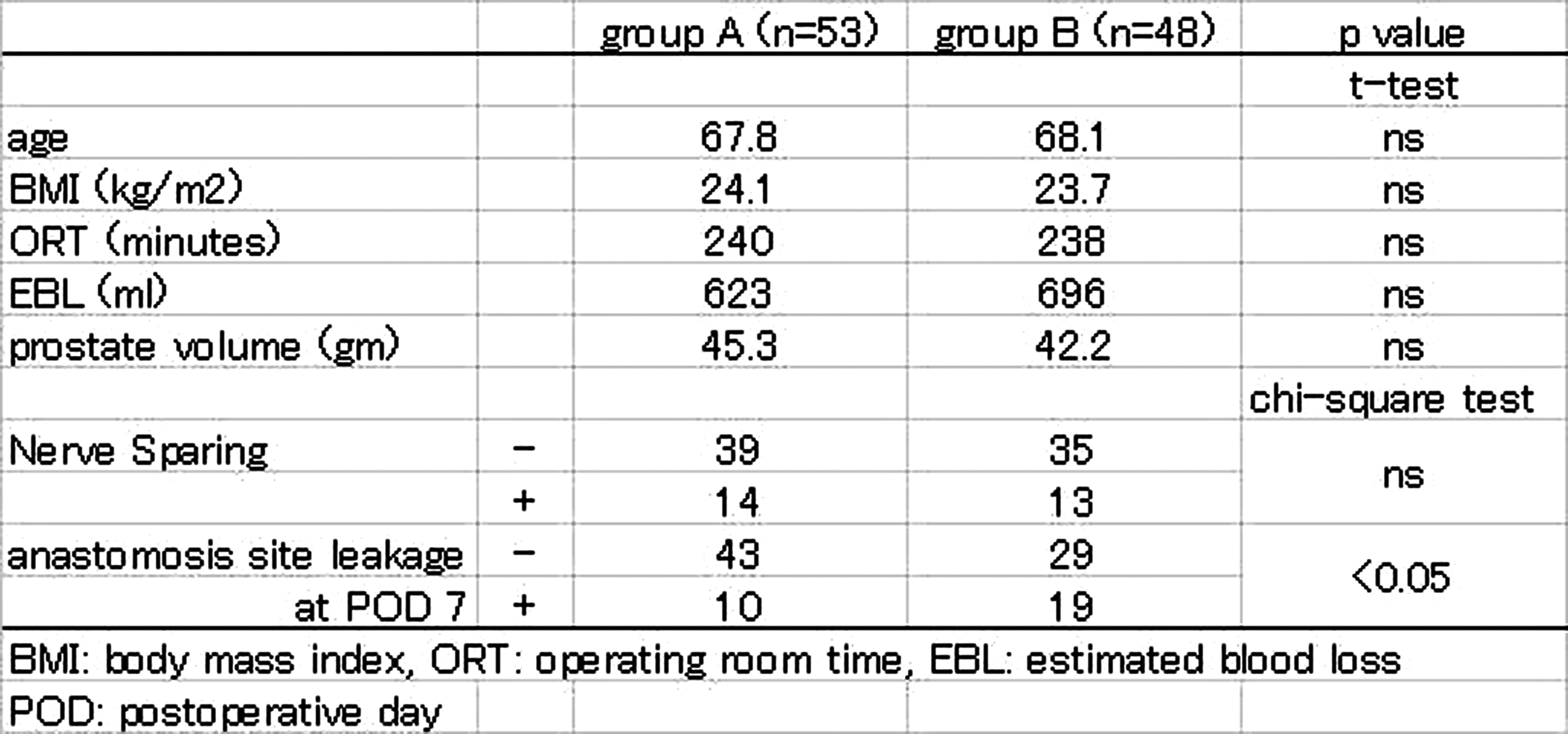
Does Obese have any Influences on Treatment success of Laparoscopic Radical Prostatectomy for Localized Prostate Cancer?
PURPOSE; To evaluate the impact of obese on the operation outcome and post-operative followup of the patients who underwent laparoscopic prostatectomy. METHODS AND PATIENTS; From July 2007 to April 2010, 150 consecutive localized prostate cancer patients with complete data set were included in the current study. BMI 25 were used for the cut-off value as being obese. Mann Whitney test was used to evaluate biochemical recurrence free survival, and statistical difference between the groups was estimated by means of Logrank method. RESULTS; Among 150 patients, 94 patients were found to have BMI greater than 22 – a desirable cut-off for Japanese population. 56 patients had BMI=22 or smaller. 33 patients were found to be obese. There was no statistically significant difference in biochemical recurrence rate compared between obese and non-obese ( mean 9.091% v.s. 9.402%, respectively, p=0.9605). Among other operative and clinicopathological factors, including bleeding (p=0.9855), positive surgical margin (p=0.9945), capsular invasion(p=0.2226), seminal vesicle invasion (p=0.3625), and pads number at 6 months after surgery (p=0.6621), only operation time was found to significantly differ among two groups ( mean 268.3min v.s. 247.1min, respectively, p=0.0475). There was no statistically significant difference in biochemical recurrence free survival (p=0.6320, HR 1.426, CI 0.3337 - 6.09). Also, there was no statistically significant difference in biochemical recurrence free survival in patients with BMI>22 and in patients with BMI=22 or smaller ( p=0.4231, HR 1.562, CI 0.5244 - 4.654). CONCLUSION; Laparoscopic prostatectomy can be safely conducted even in obese patients. Post-operative followup results were competitive to non-obese patients.
Oncologic Outcome and Urinary Continence Following Laparoscopic Radical Prostatectomy as Several Modifications of Surgical Procedure
(Purpose) Positive surgical margin (PSM) rate and urinary continence following laparoscopic radical prostatectomy (LRP) were evaluated in several different surgical procedures. (Material and Methods) Eighty patients with clinically localized prostate cancer were treated with LRP between Feb 2006 and May 2011. Several surgical procedures have been modified during the period. In the early period, LRP were performed with intraperitoneal approach, and the endopelvic fascia and puboprostatic ligaments were dissected. After that, the approach was altered to extra-peritoneal. The dissection layer was then modified from the extra-fascial to the inter-fascial, and the fascia and ligaments were attempted to be preserved. The PSM rates and the urinary continence in each procedure were evaluated. (Results) Pathological stages of 68 patients were pT2, and 10 were pT3. In pT2 cases, PSM was observed in 12 out of 30 (40%) with intraperitoneal approach, and 11 out of 38 (29%) with extraperitoneal approach. According to the dissection layer, PSM was recognized in 38.7% with extra-fascial, 36.8% with inter-fascial, and 25% with combined methods dissecting extra-fascial layer on only the cancer-positive side. Urinary continence was achieved in 96.7% with the dissection of fascia and ligaments, and in 82.1% with the preservation of these.(Conclusions) Clear relation between each surgical procedure and the outcomes were not recognized. However, PSM rates were tended to decrease in later duration of the observation, and this is supposed possibly related to a learning curve. The extra-fascial dissection of the cancer-positive side might be useful for avoiding PSM.
Impact of Running Suture Between the Rhabdosphincter and Denonvilliers' Fascia on Recovery of Continence after Laparoscopic Radical Prostatectomy (LRP)
Purpose. In the present study we evaluated the efficacy of our posterior reconstruction procedure.Methods. Before 2010 we performed 5 operative procedures to achieve early recovery of continence in LRP. These procedures were to keep the levator fascia undamaged, to preserve the bladder neck, to keep the functional urethra long, to push needles thinly though the anterior urethra in vesicourethral anastomosis, and to suspend the anterior bladder neck. Since 2010 we added a running suture between the rhabdospinctor and Denonvilliers' fascia. During this procedure the running suture was secured by LapraTy. In vesicourethral anastomosis a 2-0 absorbable ligature was tied and used for the anastomosis. At the 5 and 7 o' clock positions of the urethra we took enough urethral epithelium and the rhabdosphincter simultaneously. Cystography was performed postoperatively evaluate shape of the bladder and vesicourethral anastomosis. Clinical results were compared between patients with this procedure and those without.Results. Cystograms showed that our posterior reconstruction procedure appeared to shorten the vertical length of the bladder and to increase the posterior and the anterior angles between the urethra and bladder neck. More than 90% of patients treated with this procedure were continent within 3 months. At 3 months UCLA-PCI scores of patients treated with this procedure were significantly better than those of patients who were not. Conclusion. By using our posterior reconstruction procedure resulted in early recovery of urinary continence. The changes of bladder figure resulting this procedure may in part contribute to the improvement of continence.
Advanced Technique of Mini-Laparotomy Radical Prostatectomy for Improved Functional Outcome Based on the Knowledge of Periprostatic Anatomy
Background: Along the pelvic sidewall at the lateral aspect of the prostate, the parietal and the visceral components of the endopelvic fascia are fused. As a fascial condensation, this fusion is often recognizable as a whitish line and named the fascial tendinous arch of the pelvis. During surgery, access to the lateral prostate may be gained by incision of the endopelvic fascia either medial or lateral to this fusion. Some authors have suggested that avoiding incision of the endopelvic fascia during radical prostatectomy, often combined with an inter-fascial procedure, might improve early recovery of urinary continence.Methods: Peri-operative outcomes as well as continence rate after surgery were evaluated comparing inter-fascial and extra-fascial approaches through mini-laparotomy radical prostatectomy.Results: There were no statistical differences in age, PSA value, biopsy Gleason score and clinical stage between 10 each cases of inter- and extra-fascial radical prostatectomies. Average OR time, EBL, pathological T stage and positive margin rate were similar in both surgeries. Urinary continence recovered by 80% vs. 30% in 3 months and 100% vs. 70% in 6 months by inter- and extra-fascial prostatectomies, respectively.Conclusion: Precise knowledge of anatomic structures facilitates improved functional outcomes after radical prostatecomy.
Department of Urology, Kitasato University, Kanagawa, Japan
PURPOSE: Quality of life (QOL) issues associated with defferent treatments are important. The studies evaluating the effect on QOL of localized prostate cancer patients receiving the laparoscopic radical prostatectomy (LRP) and I125 low-dose-rate brachytherapy (LRP), the Ir192 high-dose-rate brachytherapy (HDR), which could have affected their outcomes. In this study, we investigate QOL outcome for men treated with these treatment.PATIENTS AND METHODS: From November 2003, 172 patients with prostate cancer who were underwent LRP (52 patients) and LDR (99 patients) and HDR (89 patients) were evaluated QOL score with SF-36 ver. 2.0 and UCLA-PCI.RESULT: LRP and HDR were temporary decrease in several domains of SF-36 at 1 month after treatment. But these domains recovered to baseline within 3 months. LRP and HDR reported a lower Urinary function score at 1 month after treatment, whereas LDR was 3 months later.CONCLUSION: The results of this study have indicated that LRP and LDR and HDR have meaningfully different profiles in the recovery of general QOL.
Laparoscopic Radical Prostatectomy: Initial Experience at Hiroshima City Asa Hospital
Objective: To assess the initial surgical outcome of laparoscopic radical prostatectomy at Hiroshima City Asa Hospital. Patients and Methods: Between September 2010 and June 2011, 31 patients underwent laparoscopic radical prostatectomy at our hospital. The median age, BMI and serum PSA were 66 years old (53-75 years old), 24.3 (20.7-29.3), and 7.0 ng/ml (3.5-18.6ng/ml), respectively. In preoperative prostate biopsy, the Gleason scores were 6, 7, 8, 9 and 10 in 7, 12, 9, 1 and 2 patients, respectively. In the D'Amico risk classification, the numbers of patients at low, intermediate and high risk were 7, 12 and 12, respectively. All patients underwent surgery through a transretroperitoneal approach.Results: The median insufflation time, estimated blood loss including urine volume, and tumor weight were 208 min. (140-295min.), 600 ml (80-1500ml), and 44 g (28-66g), respectively. No patients required open conversion or blood transfusion. The intra- and postoperative course was uneventful in all cases. The pathological stage was pT2 in 23 patients, pT3a in 5, and pT3b in 3. A positive surgical margin was found in 10 patients, including 4 in pT2 and 6 in pT3 cases. The median periods from the operation until urethral catheter removal and discharge were 4 days (4-15 days) and 7 days (6-18 days), respectively. Conclusion: Our initial experience with laparoscopic radical prostatectomy suggests that problems associated with patient selection, shortening of the operation time, and reduction of the positive margin rate still need to be resolved.
Department of Urology, Nagoya City East Medical Center, Nagoya, Japsn
PurposeTo compare perioperative parameters and clinical outcomes of laparoscopic radical prostatectomy between operative time within 120 minutes and over.MethodsWe performed 111 LRPs. This study included a total of 57 patients whom underwent by same operation stuff. In this study, these patients were divided into the following two groups according to operative time within 120 minutes (n=11) and over (n=47). We evaluated the perioperative parameters and clinical outcomes (BMI, PSA, neoadjuvant therapy, gleason score, prostate volume, estimated blood loss, catheterization time, surgical margin, surgeon). Also we divided operation methods into 6 steps, analyzed operative time of any steps.ResultThere were significant differences in estimated blood loss (104.5ml vs 648.5ml) and surgeon. Operative time related to the anterior dissection (endo-pelvic fascia incision, dorsal venous complex ligation) and bladder neck dissection, urethro-vesical anastomosis.
Sexual Function Following Laparoscopic Radical Prostatectomy
Purpose: Laparoscopic radical prostatectomy(LRP) is one of the most frequently selected therapeutic modalities for patients with localized prostate cancer; however, LRP has been shown to accompany significant morbidities, including erectile dysfunction(ED). In this study, therefore, we assessed the sexual function in patients treated for prostate cancer with LRP.Material and methods: This study included 102 patients with potency undergoing LRP between January 2001 and April 2010. Of the 102 patients, 15 (15%) had undergone a bilateral nerve-sparing (NS) procedure, 43 (42%) had undergone a unilateral NS procedure, and 44 (43%) had undergone a non-NS procedure. Sexual function was evaluated using International Index of Erectile Function (IIEF) before and 12months after LRP. Several factors associated with erectile dysfunction after LRP were identified by univariate analysis.Results: After surgery, the rates of sufficient for intercourse in the bilateral NS group, unilateral NS group, and non-NS group were 56%(8/15), 23%(10/43) and 16%(7/44) respectively. and the difference between bilateral NS group and other groups were significant. In a multivariate analysis, risk factor affected ED was only neurovascular bundle status. Improvement of sexual function was greater in the NS group than non-NS group by use of PDE5i.Conclusions: Compared to the unilateral nerve-sparing procedure, the bilateral nerve sparing technique revealed much better results in recovery of intercourse without use of sexual aids
The Learning Curve for Laparoscopic Radical Prostatectomy: 200 Cases of a Single Surgeon
OBJECTIVEThe objective of this study is to analyze the learning curve of laparoscopic radical prostatectomy (LRP) by a single surgeon.PATIENTS AND METHODSIn 403 consecutive patients underwent LRP at our institution between February 2000 and March 2011, 200 cases of LRP which is performed by a single surgeon (M.I.) was included in this retrospective study. The patients were classified into four groups: 1-50 cases (Group 1), 51-100 (Group 2), 101-150 (Group 3), and 151-200 (Group 4). The mean age was 66 years, and the mean preoperative prostate-specific antigen level was 7.2ng/ml. RESULTS Median operating time was gradually shortened from Group 1 to Group 4 (310 min, 255min, 210min, and 198min in Groups 1, 2, 3 and 4, respectively; P<0.001). Significantly less positive margin rates (PMR) occurred after 100 cases (PMR; 44%, 40%, 21%, and 24% in Groups 1, 2, 3 and 4, respectively; P<0.001). Complication rates were 18%, 20%, 20%, and 10% in Groups 1, 2, 3 and 4, respectively. Blood transfusion was performed for only one patient in Group 3. CONCLUSIONSThe learning curve for positive margin rates after LRP plateaus at approximately 100 cases in this study. However, the learning curve for operating time continued to improve during Group1-4, suggesting that the learning curve for LRP may be longer than 200 cases.
Department of Urology, Nakatsu Saiseikai Hospital, Osaka, Japan
We report the utility of transrectal ultrasonography guidance for laparoscopic radical prostatectomy (LRP), and the effect of a novel surgical approach of seven key elements of operative skill for the early recovery of urinary continence. Among 170 patients who underwent laparoscopic prostatectomy, 72 were treated on the basis of these 7 key elements (group 1), which included the preservation of 1) endopelvic fascia, 2) bladder neck, 3) pelvic nerve, 4) membranous urethra, 5) urethral sphincter and fixation of the organ positioning with 6) bladder neck sling suspension, and 7) restoration of the Denonvilliers' fascia, while the remaining 98 were not (group 2). We compared these two groups with regards to the time taken for recovery of continence, and post-operative course. Application of the 7 key elements led to significantly earlier recovery of continence. In group 1, the number of urinary pads used after surgery was significantly reduced at all of the examined time-points after surgery (1, 3, 6 and 12 months) (p<0.0001). In group 1, more than half of the patients (54%) achieved urinary continence within 3 months, 93% achieved it within 6 months, and all patients had achieved it within 12 months after surgery. However, in group 2,<10% of the patients (8.5%, p<0.0001) achieved continence within 3 months, and 23% (P<0.0001) achieved it within 6 months. Therefore, the results show that the 7 key elements of operative skill with transrectal ultrasonography guidance significantly improve the outcome of LRP, reducing the time required for the recovery of continence.
Laparoscopic Radical Prostatectomy–Initial 100 cases by a Single Surgeon At Kumamoto University Hospital
PURPOSE: We report on our initial experience with 100 extraperitoneal laparoscopic radical prostatectomy(LRP) by a single surgeon.METHODS: From Sep 2009 to Jun 2011, LRP was performed on 100 men, aged 46 to 79 years. Patient characteristics, surgical statistics, and pathologic results were retrospectively collected.RESULTS: The median BMI was 23.4 (range 17.8-35.1). The median operative time was 255 minutes (range 165-570 minutes).The median blood loss (with urine) was 505 ml (range 50-2900 ml).The blood transfusion rate was 1.0% . No open conversion case was observed. One major complication, DVT(with IVC filter insertion) and one laparoscopic repair of a rectal injury were observed. The pathologic stage was pT2a in 10 patients (10%), pT2b in 22 (22%), pT2c in 41 (41%), pT3a in 17 (17%), pT3b in 7 (7%), and pT4 in 2 (2%) uncertain in 1 (1%). Positive surgical margins were found in 2.7% of patients (2/73) with pT2 tumors and 26.9% of patients (7/26) with pT3 or pT4 tumors. The median catheterization time was 5 days(range 4-12 days). The continence rates (no pads or pad for safety) at 1, 3, 6 and 12 months were 19.8% (19/96), 44.0% (33/75), 75.4% (46/61), and 92.0% (23/25), respectively. After a nerve-sparing procedure, the total potency rates at 3 and 6 months were 37.5% (21/56) and 48.8% (21/43), respectively.CONCLUSION: The LRP shows significant promise for reducing surgical morbidity and improving the anatomic radical prostatectomy.
Department of Urology, Nishinomiya Municipal Central Hospital, Nishinomiya, Japan
Purpose:Laparoscopic radical prostatectomy (LRP) may be relatively difficult compared with other urological laparoscopic procedures. Two dimensional image is potential impediment, so we currently use a 3-dimensional (3-D) endoscope display system to confirm its availability on LRP.Methods:We compared 26 LRP cases using a 3-D display system with 8 LRP cases using a 2-dimensional (2-D) endoscope system in terms of clinical outcomes.Results:The average OR time and estimated blood loss in 2-D and 3-D group were 367 minutes and 1102ml, and 305 minutes and 868ml, respectively. Average OR time was significantly shorter in 3-D group (p=0.011). Especially, the time for the dissection of bladder neck from prostate and the division of DVC and urethra was shorter in 3-D group. The continence ratio at 1 month and 3 months after surgery in 2-D and 3-D group were 25 % and 41 %, respectively, while and 57 % and 78 %, respectively. Using a 3-D display system, the number of cases and positive margin ratio of pT2 and pT3 cases were 13 and 33 %, and 13 and 25 %, respectively.Conclusion:These results shows that 3-D endoscope display system could contribute to shorter OR time, satisfactory positive margin ratio in pT3 group and continence ratio after surgery.
Robot-Assisted Laparoscopic Prostatectomy: Kobe University Experience
Purpose: We performed a prospective analysis of clinical outcomes following robot-assisted laparoscopic prostatectomy (RALP) at Kobe University Hospital. Materials and Methods: A total of 28 men with a median age of 67.5 years underwent RALP between October 2010 and June 2011. Preoperative clinical stage was T1c in 3 patients, T2a in 15, T2c in 8 and T3a in 2. Median preoperative PSA was 6.56 ng/ml. Operating time, complication rate, transfusion rate, catheterization time, pathological results, continence rate and erectile function were reviewed. Results: Median operative time and console time was 336 min and 268 min including lymphadenectomy with no conversion to pure laparoscopic or open surgery. No intraoperative complication occurred except one autologous blood transfusion. Pathological stage was pT2a in 8 patients, pT2b in 2, pT2c in 12, pT3a in 3 and pT3b in 1. The positive margin rate was 23.1% for all patients. The one-month follow-up indicated continence rate of 54.2% and potency rate of 41.7%. Conclusions: On the basis of short-term follow-up data, our prospective evaluation confirmed that RALP provides satisfactory results. We believe that RALP can be the technique of choice also in Japan.
A Comparison of Laparoscopic and Robotic-Assisted Laparoscopic Radical Prostatectomy:a Single Surgeon Experience
Purpose: We have performed over 400 cases of laparoscopic radical prostatectomy (LRP) by the trans-abdominal posterior approach during the recent 10 years. We began robotic-assisted laparoscopic radical prostatectomy (RALP) using the same approach as LRP in May 2011. In this study, we compared the surgical outcomes of LRP and RALP performed by a single surgeon.Methods: Twenty patients underwent LRP and RALP for localized prostate cancer between September 2010 and July 2011. This study compared surgical duration, suturing time, blood loss and complications between the two procedures. Medical records and videos were reviewed with particular attention paid to patient characteristics and procedures.Results: All procedures were successfully completed in 20 cases without any necessity for conversion to other approaches. There was no significant difference in surgical duration between LRP and RALP (181.6 min vs. 217.3 min). Regarding blood loss, there was no significant difference between LRP and RALP (436.4 ml vs. 333.0 ml). There were no intra-operative complications in any of the cases.Conclusion: The transition from LRP to RALP was extremely smooth in our institute. For laparoscopists with extensive experience in LRP, robotics are useful for improving motion, which may have implications for highly complex procedures in limited workspaces.
Department of Urology, Shintoshi hospital, Iwata, Japan
OBJECTIVE: We study the value and feasibility of LAPARO-ANGLE needle holder on urethrovesical anastomosis during radical laparoscopic prostatectomy. METHODS: We underwent radical laparoscopic prostatectomy through the placement of two separate needles for running urethrovesical anastomosis. When the first stitch was placed in the posterior urethral wall of anastomosis (at 6 o'clock), LAPARO-ANGLE needle holder was mainly used. Then, clockwise and anti-clockwise running suture was made from 7 to 12 o'clock and 5 to 12 o'clock position. RESULTS: The needle hung as 6 o'clock of urethral wall had an enough thickness squarely, fixing the needle holder tip after the needle had been held, and turning the rotation knob. Moreover, it has been understood the posterior wall of the urethra is drawn out forward, and the suture of the direction can be steady at 4 from 8 o'clock of urethra. CONCLUTIONS: As for LAPARO-ANGLE needle holder, a completely right-angled needling is possible though the grip force of the needle is weak, and the experience is necessary for the operation. Especially, there is a possibility of contributing to a decrease in the urinary incontinence at the early postoperative period because it can firmly anastomose the posterior wall of the urethra and bladder neck during LRP.
Adaptation of the Neurovascular Bundle Preservation in the Laparoscopic Radical Prostatectomy
Objectives : To examine the adaptation of the neurovascular bundle (NVB) preservation in the laparoscopic radical prostatectomy. Methods : 82 patients who underwent prostate biopsy (12 cores) were performed laparoscopic radical prostatectomy from 2009 to 2011. Adaptation of the NVB preservation (veil technique, intrafacial) was determined using cancer map made by the whole mounted step sections. Using the possible case of NVB preservation, the following aspects were investigated whether they are useful on determining adaptation of preservation; PSA before biopsy, digital rectal examination (DRE) findings, MRI, biopsy findings (Gleason score, number of positive core on one side, maximal cancer occupancy rate of core (%), presence of positive rectal margins)Result : 68 patients were determined to be possible for NVB preservation. Within that, 25 cases were possible on the both side and 43 cases were only unilateral side. The number of positive core (possible case : 1(median), impossible : 3) and cancer occupancy rate (possible : 10%, impossible : 60%) had significant differences (p<0.0001). PSA was tended to be lower in possible cases (possible : 6.64ng/ml, impossible : 8.11) (p=0.0822) and Gleason pattern 5 was the indicator of impossible cases. MRI was useful as showing 78.4% of sensitivity and 64.8% of specificity. However, DRE and positive rectal margins had low specificity (43.8% and 28.8%, each). Conclusions : Less than 1 positive core within 6 unilateral cores and cancer occupancy rate of core below 20% were useful indicator of the NVB preservation.
Laparo-Endoscopic Single-Site (LESS) Surgery for Upper Urinary Tract Cancer: Our Initial Experience
Introduction and Objectives: Laparoendoscopic single-site surgery (LESS) has been reported as technically feasible in some urologic diseases. We herein describe our initial experience with LESS surgery for upper urinary tract cancer. Methods: We retrospectively reviewed our experience with 6 patients who have undergone LESS nephroureterectomy (LESS-NU) for upper urinary tract cancer. Results: We employed multiport umbilical approach in the first one case, but in the remaining 5 patients, 4-6 cm pararectal incision was made and the GelPort was inserted. Three or four trocars were used. The mean age, mean operative time, estimated blood loss and length of stay were 76 years (range 60-82), 392.5 min (range 301-428), 640 ml (range 100-890), and 16.5 days (range 8-25), respectively. Only one patient needed vessel repair for the injury of an external iliac artery. The postoperative courses were uneventful without major complications, with the exception of one patient who had a wound infection. Conclusions: Although the operative time of the LESS-NU is still longer compared with conventional laparoscopic-NU in our preliminary experience, LESS-NU is technically feasible procedure and improves cosmesis. Furthermore, through the pararectal incision, the pelvic lymphadenectomy and the bladder cuff incision can be performed using minilaparotomy technique. The development of LESS surgery for upper urinary tract cancer is underway, thus the further studies are necessary to define the advantages and limitations of this technique.
Three cases of Laparoscopic single-site Surgery Unclamp- Nephron-Sparing Surgery
(Objectives)Nephron-sparing surgery (NSS) is a surgery operative method of the first choice for the small renal tumor. Laparoscopic single-site surgery: LESS) is one of the development types of the minimally invasive surgery. And we will report LESS unclamp NSS and consider usehulness of this procedure. (Patients and methods) We performed LESS unclamp NSS for three cases of exophoric isolated renal tumor less than a diameter of 4 centimeters by March, 2011 from December, 2010. Using a multichannel port, two cases were transperitoneal approach and the other was retroperitoneal approach. LESS unclamp NSS performed with a microwave tissue coagulater. (Results) Because the applicator of microwave tissue coagulator did not have flexibility, additional 5mm port was necessary in all three cases. In the case with retroperitoneal approach, LESS unclamp NSS converted to conventional laparoscopic PN with four ports due to control of bleeding. Operation time and blood loss of two transabdominal approach was 3.3 hrs and 40ml and those of one retroperitoneal approach was 6.1hrs and 300ml, respectively. (Discussion)It seemed that enough operating space could be got even if retroperitoneal approach. In these cases, we coagulated tumor circumstance with rigid applicator and additional 5mm port was necessary to avoid calyx injurty. If flexible applicator of microwave tissue coagulator and forceps would be ready and appropriate choice would be performed, LESS-PN without ischemia would become one of the surgical procedure for small renal tumor.
Division of Urology, Department of Surgery, Far Eastern Memorial Hospital, Ban Ciao, Taipei, Taiwan
Objective: To present the initial experience of LESS nephroureterectomy via the transperitoneal approach using the Alexis wound retractor and bladder cuff resection by Endo-loop. Methods: Two patients received LESS nephroureterectomies and bladder cuffs resection with homemade single ports, which were created by using an Alexis wound retractor as an access platform through a 4cm incision. Distal ureters were resected through the same incision with Endo-loop. No additional ports were used and both procedures were completed successfully. Results: Both LESS procedures were completed successfully without traditional laparoscopic conversion or complication. LESS nephreoureterectomy with bladder cuff excision was performed in 325 and 165 minutes with estimated blood loss of 30 and 65 mL, respectively. Patients were discharged on postoperative days 3 and 7, respectively.Conclusions: Our initial results demonstrated that our LESS technique of nephroureterectomy and bladder cuff resection with Endo-loop is a safe and feasible procedure for urothelial carcinoma of upper urinary tract.
Simultaneous LESS Radical Nephrectomy and Open Non-ischemic Partial Nephrectomy to Treat Concomitant RCCs in Native and Transplant Kidneys
OBJECTIVE: To report a technique of minimally invasive radical nephrectomy for a native renal cell carcinoma (RCC), and non-ischemic open partial nephrectomy for a transplant kidney RCC just via a laparoendoscopic single site (LESS) incision. Concomitant RCCs in a native and transplant kidneys are very rare. Conventional surgical approach requires a long incision.METHODS: A 50 year-old man 14 years after renal transplant was found incidentally with concomitant RCCs in his native right kidney and transplant kidney. A right lower abdomen Gibson incision, along his transplant wound, was used initially for LESS right radical nephrectomy and lymphadenectomy, and that same wound was employed for a non-ischemic open partial nephrectomy in the transplant kidney. RESULTS: The LESS right radical nephrectomy took 3.25 hours with estimated blood loss (EBL) of 80 mL and the partial nephrectomy for the transplant kidney took 3 hours with the EBL of 220 mL. No transfusion was required. Pathologic examination revealed both tumors are RCC, clear cell type; 6.5 and 2.8 cm in diameter, respectively. The final wound measured 9 cm. Post-operative recovery was uneventful with and in-patient narcotic requirement of 37 mg morphine sulfate equivalent, and oral intake in 2.5 days. His allograft function was well preserved with a serum creatinine unchanged (1.4 mg/dL) at discharge.CONCLUSIONS: In a patient with concomitant tumors in a native kidney and a transplant kidney, this unique approach provides exceptional benefits of minimally invasive tumor excision for both tumors, and good preservation of the renal function.
Evaluation of Neoadjuvant Hormonal Therapy on treatment outcome of High-Intensity Focused Ultrasound for Prostate Cancer
INTRODUCTION AND OBJECTIVE: HIFU is a new minimally invasive therapeutic method for prostate cancer in nonsurgical patients. The purpose of the present study is to report the short to mid-term outcome in patients with low-, intermediate-, and high-risk prostate cancer treated by HIFU with or without concomitant hormonal therapy in one center during the initial experience with the procedure. METHODS: Between June 2004 and February 2008, 134 men with clinically localized prostate cancer were treated using the Sonablate-500®. We stratified the patients into three risk categories according to the classification of D,Amico et al. : low risk intermediate risk (clinical stage T2b or PSA 10-20 ng/ml or GS 7),and high risk (clinical stage T2c or PSA ≥ 20 ng/ml or GS 8-10). On post-operative follow-up, the PSA level was obtained 2 days after treatment and every 1, 3, 6, 12, 18, 24, and 33 months. Of the 134 patients, 49 (36.6 %), 46 (34.3 %) and 39 (29.1 %) were respectively stratified in low, intermediate, and high risk groups.There was, however, no significant difference between the groups in the PSA value over the period of follow-up with mean PSA levels at 1, 3, 6, 12, and 18 months. Also, There was no statistical association between the use of neoadjuvant hormonal therapy and the risk of biochemical failure. CONCLUSIONS: In patients with localized prostate cancer, HIFU therapy resulted in comparable immediate cancer control. The present results indicate that combined treatment using hormonal therapy and HIFU does not have a synergistic effect on PSA nadir.
Laparoendoscopic Single-Site Adrenalectomy with Needlescopic Instrument
(Purpose) The objective of the modern surgery is not only perform surgical procedures aiming to improve the health condition of the patient, but whenever possible to use minimally invasive approach and to ensure the satisfying cosmetic result. Therefore laparoendoscopic single-site(LESS) surgery is practicable in many fields of surgery, including surgery of the adrenal glands at present. We report the initial sereies of LESS adrenalectomy with needlescopic instrument.(Patients and Methods) Between October 2010 and January 2011, 2 patients underwent LESS adrenalectomy with needlescopic instrument. The first patient is a 44-year-old woman who was diagnosed with primary aldosteronism due to left adrenal tumor with small multiple nodules. The second patient is a 54-year-old man who was diagnosed with cushing syndrome due to left adrenal tumor, 33x25mm in size. SILS port (Covidien, Norwalk, CT) was used through a 2.5cm subcostal incision with 5mm flexible laparoscope (Olympus, Japan) and two 5mm instruments. One additional 2.1mm trocar was added using needlescopic instrument (NITI-ON, Japan). The procedure was performed in a standard manner of conventional laparoscopic adrenalectomy.(Result) Patient 1: The operative time was 218 minutes, and the estimated blood loss was a little. The hospital stay was 9 days. Patient 2: The operative time was 178 minutes, and the estimated blood loss was a little. The hospital stay was 12 days. There were no morbidity and mortality.(Conclusion) LESS adrenalectomy with needlescopic instrument is easier and safer than that with LESS alone. LESS with needlescopic procedure is as cosmetically effective as LESS alone.
Laparoendoscopic Single-Site Surgery FOR RENAL CANCER
IntroductionDespite better cosmesis and potentially less surgical trauma, concerns have arisen about oncological efficacy of laparoendoscopic single-site surgery(LESS). PurposeTo evaluate surgical, functional, and early oncological outcomes of LESS for renal tumors. Materials and MethodsSince 2007, 34 patients have undergone LESS procedures for renal tumor at our center, including partial nephrectomy(PN)(11), radical nephrectomy(17), cryoablation(5), and metastectomy(1). Articulating and straight laparoscopic instruments were used for standard LESS procedures(22) and the da Vinci system for robotic LESS procedures(12). Surgical, functional, and oncological outcomes were evaluated.ResultsMean operative time was 189±51.8min and mean blood loss was 252±305mL. Tumors for PN procedures had median PADUA and RENAL nephrometry scores of 7 and 6, respectively; with a mean warm ischemia time of 20.2±7.1min. Overall, mean visual analog pain scale at discharge was 1.5(1-10). Mean length of stay was 3.4 days. One focally positive margin was noted after a PN, with negative intraoperative frozen section. Mean decrease of glomerular filtration rate was 15.9%. Postoperative complications included retroperitoneal abscess(Clavien IIIa) in 1 patient, and bleeding(Clavien II) in 6 patients, treated conservatively. Most of the transfusions occurred in the PN subgroup. There were 2 conversions to standard laparoscopy and 2 to open surgery. Overall, recurrence-free, and cancer specific survival were 98%, 100%, and 100%, respectively, with a mean follow-up of 26 months.ConclusionsLESS is a feasible approach for treatment of renal cancer in carefully selected patients. Initial results of oncological adequacy are similar to published standard laparoscopy series; however, longer follow up is awaited.
Transumbilical Approach for Laparo-Endoscopic Single-Site Adrenalectomy: Initial Experience and Short-Term Outcome
Objectives: We here report our initial experience with transumbilical LESS for adrenal tumors by using a single port with a multichannel cannula (SILS port) and bent laparoscopic instrumentation.
Methods: Between December 2009 and December 2010, 30 patients underwent transumbilical laparo-endoscopic single-site adrenalectomy (LESS-A) at our hospital. A multichannel port (SILS port), bent laparoscopic instruments, and Opti4 laparoscopic electrodes were used in all cases. The intraperitoneal space was approached through the umbilicus. The SILS port was placed through a 2 cm incision at the inner edge of the umbilicus. A 5 mm flexible laparoscope was introduced to maintain an adequate laparoscopic view, and surgical specimens were extracted using an Endocatch bag.
Results: Transumbilical LESS-A was performed for adrenal cortical adenoma in 17 cases, adrenal pheochromocytoma in 7 cases, and other types of tumors in 6 cases. All procedures were successfully completed, with only one incision through the umbilicus, and without conversion to a standard laparoscopic approach. Mean operative time for LESS-A was 120.1±34.7 min. Tumor laterality and patient BMI did not affect surgical morbidity in these procedures. The initial 15 cases had a significantly longer mean pneumoperitoneum time (95.8±37.5 min) than the last 15 cases (70.5±18.7 min). A postoperative complication (postoperative hematoma) was observed in only 1 patient.
Conclusions: The transumbilical approach in LESS for adrenalectomy is safe and feasible and also results in superior cosmesis. Improvements in surgical devices may aid the further development of this approach.
Laparoendoscopic Single-Site Surgery for Partial Nephrectomy by Using the Microwave Tissue Coagulator
Introduction: Recently, laparoendoscopic single-site surgery (LESS) has been developed for many urological surgeries. However, few studies have demonstrated the feasibility of LESS for partial nephrectomy.Purpose: We report our initial experience with LESS partial nephrectomy (LESSPN) by using the microwave tissue coagulator (MTC).Materials and Methods: Two patients with small and exophytic renal tumors underwent LESSPN. In imaging technique, those tumors showed at least 5 mm of normal renal tissue between the tumor margin and the collecting system. The multichannel port was inserted into the peritoneal or retroperitoneal space through the 3 cm skin incision. After the tumor exposure, surgeon introduced a laparoscopic MTC instrument through the 5 mm port and the tumor margin was coagulated circumferentially. After coagulation, the tumor was resected without renal pedicle clamping.Results: These procedures were successfully performed without any open conversions and the operative time was 183 and 160 minutes, respectively. The estimated blood loss was<150 mL in both cases. There was no postoperative complication, including urine leakage or loss of renal function. Conclusions: To the best of our knowledge, this is the first report of LESSPN by using the MTC. This novel surgical technique is feasible and provides bloodless resection of the renal tumor without renal pedicle clamping. However, it should be attempted in selected patients with favorable tumor anatomic features. Further clinical experience and longer follow-up are needed to define the benefits of this new technique.
Department of Urology, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
UP02: Unmoderated Poster Session 2
Comparison of TUERP Versus TURP in the Treatment of Prostates : 2 Years follow up
Introduction: Transurethral enucleation and resection of prostate (TUERP) is a method that match the results achieve by transurethral resection of the prostate (TURP) and open prostatectomy. It can be performed by routine instruments, using the resectoscope beak like surgeon's finger to enucleate the prostate lobes from the surgery capsule, without use of the extra and expensive devices, such as laser.Purpose:To compare the efficacy of TUERP versus TURP during a 2-year follow-up.Materials and Methods:50 elderly men with lower urinary tract symptoms due to benign prostatic hyperplasia (BPH) were randomized into two groups of 25 each. Preoperative workup included the International Prostate Symptom Score (IPSS), Quality of Life (QoL) scores, uroflowmetry, post-void residual volume (PVR), prostate volume(PV)determined by transrectal ultrasonography. Postoperative follow-up at 6, 12, 18 and 24 months included assessment of IPSS,QOL,PVR, uroflowmetry and pressure flow studies.Results :There were no significant difference between two groups pre-operatively. mean preoperative prostate volumesd was 65.5±17.3ml in TUEPR group and 63.4±18.2ml in TURP group. Compared TUERP and TURP groups, the postoperative PV were significantly different, more prostate tissue has been resected in the TUERP group. There were no significant differences in IPSS, QOL, and Qmax between two groups during follow up. However, TUERP has superior urodynamic outcomes than TURP in releaving bladder outlet obstruction.Conclusion:TUERP is safe and effective in the surgical management of BPH, with the advantage of resected more prostate tissue and urodynamic outcome.
Bipolar Turp(TURis): Selective Symptomatic Improvement After 1yr Follow-Up.
INTRODUCTION:Bipolar TURP(B-TURP) has emerged as an alternative to conventional monopolar TURP. An interesting key point is a selective analysis of symptomatic outcomes, in order to compare it with other surgical techniques. PURPOSE:Analyse the results of B-TURP, focusing on functional outcomes by selective improvement of each IPSS value at 1yr follow-up. MATERIAL AND METHODS:From 2008, 120 B-TURP (TURis Olympus SurgMaster UES-40) were performed by single surgeon. Patients with <12 months of follow-up were excluded.RESULTS:Preoperative variables (mean (range)): age 69,7yr (50-89), prostate volume 61cc (24-134), PSA 5,5ng/ml (0,25-11,2) Qmax 8,2ml/s (2-15), PVR 198cc (0-1000), IPSS 23,2 (8-34), IPSS QoL:4,9 (1-6). Peroperative variables (mean(range)): surgical time 64min (13-120), tissue weight ressected 24g (4-66), hospital stay 27h (11-95). No major complications occured.According to IPSS, selective improvement observed was (basal- 3mo-12mo-%decrease): IPSS(1)-Incomplete voiding: (3,4-0,5-0,5-85,3%)IPSS(2)-Urinary frequency: (3,7-1,3-1,2-67,5%)IPSS(3)-Interrupted micturition: (3,4-0,6-0,4-88,2%)IPSS(4)-Urgency: (3,8-1,3-0,6-84,2%)IPSS(5)-Low flow: (3,9-0,5-0,4-89,7%)IPSS(6)-Abdominal press: (2,3-0,2-0,2-91,3%)IPSS(7)-Nicturia: (3,3-1,5-1,3-60,6%)IPSS Quality of Life: (4,9-1,3-1,0-79,6%)Incontinence rates at 1yr was 0% Qmax was 25ml/s, PVR 6,7ml, residual prostate volume 24cc, PSA 2,1 and global IPSS 4,7.CONCLUSIONS:B-TURP is a safe technique with excellent results in storage and voiding syptoms at least at 1yr. Symptomatic outcome is optimal at 3 months, only urgency tends to a slower recovery. This data can be useful when comparing with other surgical techniques.
The Clinical Analysis of Urodynamic Test in Treating BPH Complicated with Neurogenic Disease
Operative Impacts on LUTS of BPH and Prostatitis Patients ; Comparison of Post Transurethral Resection State
Objectives : Combination of benign prostatic hyperplasia (BPH) with prostatitis aggravates clinical symptoms of BPH and complicated its treatment. Pronounced dysuria, persistent pain are highly resistant to conventional medicational management. Unsatisfactory results of transurethral resection of prostate (TUR-P) in BPH with prostatitis are attributed to poor improvement of LUTS after catheter removal. Methods : From 2005 ∼ 2010 , 116 male patients are investigated who had treated by transurethral resection of prostate (TUR-P). international prostate symptom score (IPSS) was checked before and after of TUR-P within 1yrs. Prostate cancer patients are excluded. Group A was BPH patients without prostatitis, and group B was BPH patients without prostatitisResults : Average preoperative IPSS was 21.56±0.26, prostate volume was 41.56±0.44g and PSA was 3.52ng/dl. pathologic confirmation showed only prostatic hyperplasia on 58 patients and hyperplasia with prostatitis on 58 patients. Preoperative IPSS of group B was higher (22.95±5.65) than group A(group B vs group A, 20.14±5.61, p=0.001), Especially preoperative irritative symptom score was notably high. (group A: 6.63±3.57, group B: 9.29±4.06, p=0.015) The gap of preoperative IPSS and postoperative IPSS was 5.51 on group A, 8.83 on group B. (p<0.001). There was no statistical difference between groups. (group B vs group A; p=0.634 vs p=0.637)Conclusion : Prostate hyperplasia was independent aggravating factor on LUTS. Prostatitis also was one of the risk factors on LUTS after operation. When the prostate hyperplasia was combined to inflammation, LUTS was more aggravated than hyperplasia only patients. And the efficacy of TUR-P on prostatitic BPH was better than naïve BPH patients.
The RevoLix 2 Micron Wave Laser Vaporesection for the Treatment of Patients with Benign Prostatic Hyperplasia
[Purpose] Classical transurethal resection of prostate( TUPR) was so-called gold stantard for the treatment of prostate. To evaluate the safety and efficacy of the RevoLix 120W 2 micron continuous wave laser vaporesection in the treatment of patients with benign prostatic hyperplasia (BPH).[Materials and methods] A retrospective chart review of 59 BPH patients who underwent RevoLix 120W 2 micron continuous wave laser vaporesection from May 2010 to May 2011 in the first hospital of Jilin university was performed. The average age of patients is 74 years (68 years to 95 years). The operative time, drop in hemoglobin, indwelling catheterization time, operative complications, international prostatic symptom scores (IPSS), quality of life (QoL), urinary flow rate (Qmax), and post voiding residual urine volume (PVR) were observed.[Results] All 59 patients recovered without any incident. The mean operative time was 58±23.2 min. Occasional venous hemorrhage occurred during the operation, but no arterial hemorrhage was observed. Hemoglobin decreased from preoperative 14.6 g/dL to postoperative 13.8 g/d(P>0.05). IPSS decreased from preoperative 20±5.8 to postoperative 8±4.2(P<0.05), QoL scores decreased from 4.8±0.8 to 2.2±0.9(P<0.05), Qmax increased from 7.9±4.8 to 20.6±10.3 mL/sec(P<0.05), PVR decreased from 90.6±52.7 to 20.2±3.8 mL(P<0.05). [Conclusions] The RevoLix 120W 2-&mum continuous wave laser vaporesection is safe and effective in the treatment of patients with BPH.
5 Years Reports of the Outcomes of Radical Retropubic Prostatectomy
Introduction: Radical prostatectomy (RP) is still the gold standard treatment of localized prostate because providing the best outcomes in terms of cancer control and quality of life.This study presents the 5 years reports of the outcomes of radical retropubic prostatectomy of 108 patients.Patients and Methods: A total of 108 patients with localized prostate cancer (Gleason score or less ) with life expectancy more than 10 years, underwent radical retropubic prostatectomy (RRP) during 2003 to 2008.Results: In 84(77.7%) cases, localized cancer was reported with gleason score 7 or less. Extra capsular involvement was reported in 20 cases (18.5%).The most early complication was bleeding which was measured 800cc as mean. 45 cases (41.6%) were potent after one year .92.5% had urinary continence at the end to one year after RP. No mortality during the hospitalization time was reported.Conclusion: Retropubic radical prostatectomy with bilateral nerve sparing method is a selective treatment method of local prostate cancer. Its results are very good based on the surgeon's experience and the technique of performing this method; it is followed by few and acceptable complications. Key words: Radical Retropubic Prostatectomy, localized prostate cancer, treatment
Efficacy of Desmopressin and Celecoxib in Treatment of Nocturia Caused by Benign Prostatic Hyperplasia
Introduction:BPH treatment has relative response to alpha1 blockers and 5alpha reductase inhibitors (25-39%)in spite of these treatment many of patients complain of nocturia. Desmopressin & celecoxibe has been used in BPH for treatment of nocturia but these isnt any study that compare to effectiveness of these two drugs for nocturia.Method:First group(a)and second group(b)received 0.2 mg desmopressin and 100mg celecoxib at 9pm every night along with previous treatment for 1 month. Reevaluation of patients after treatment was performed. According to response to treatment patients were divided 3 groups: Excellent(nocturia disappeared or decreased by 2 or more void/night), Improve (nocturia decreased by 1 void/night) and no change .Results: 65 patients with mean age 63.86 years old were studied, initial means were IPSS=19.41,prostate volume=42.52 ,PSA=2.82 ,PVR=49.23 ,MFR=12.48, frequency of nocturia=5.09 respectively. After treatment these values were changed to IPSS=16.76 , prostate volume=42.52, PSA=2.72, PVR=49.23 , MFR=13.27 , frequency of nocturia=2.84 respectively.Excellent , Improve, Not change responces obtained in 54.2%, 22.6%,23.2% respectively in desmoperessin group and 74.6% , 5.9% , 19.5% in celecoxib group.Conclusion: improved or disappeared nocturia were 76.8% and 80.5% in two groups of patients. We advice to use desmopressin or celecoxib in combination with standard medical therapy for BPH as a useful treatment, so there is no different between two drugs statistically(p=0.077)
Fuchinobe General Hospital
Purpose: Holmiumu laser enucleation of prostate (HoLEP) has been recognized as minimum invasive surgery for the patients with symptomatic benign prostatic hyperplasia (BPH) of any size.Encounterment to patients with urinary retention increased recently. We reviewed HoLEP for the patient with urinary retention.Materials and Methods: We retrospectively reviewed 88 consecutive patients who underwent HoLEP by single practice hand, between January 2010 and December 2010. 30 cases were noted to have urinary retention and we selected them as A group,other 58 cases are selected as B group.Results: Preoperative estimated prostatic volume (ml) was large with a significant difference in Group A; likewise total operation time(min), enucleation time(min), morcellation time (min), encleation volume(g) and total energy for used(kJ) recognized significant difference.However, for postoperative Hb decrease, a postoperative catheterization time (days), enucleation efficiency(g/min), encleated volume per energy for used (g/kJ), IPSS-QOL score in postoperative the first month, the maximum flow rate in post operative first month did not show any significant differences in both groups.Conclusions: HoLEP is a safe and effective treatment for patients with urinary retention.
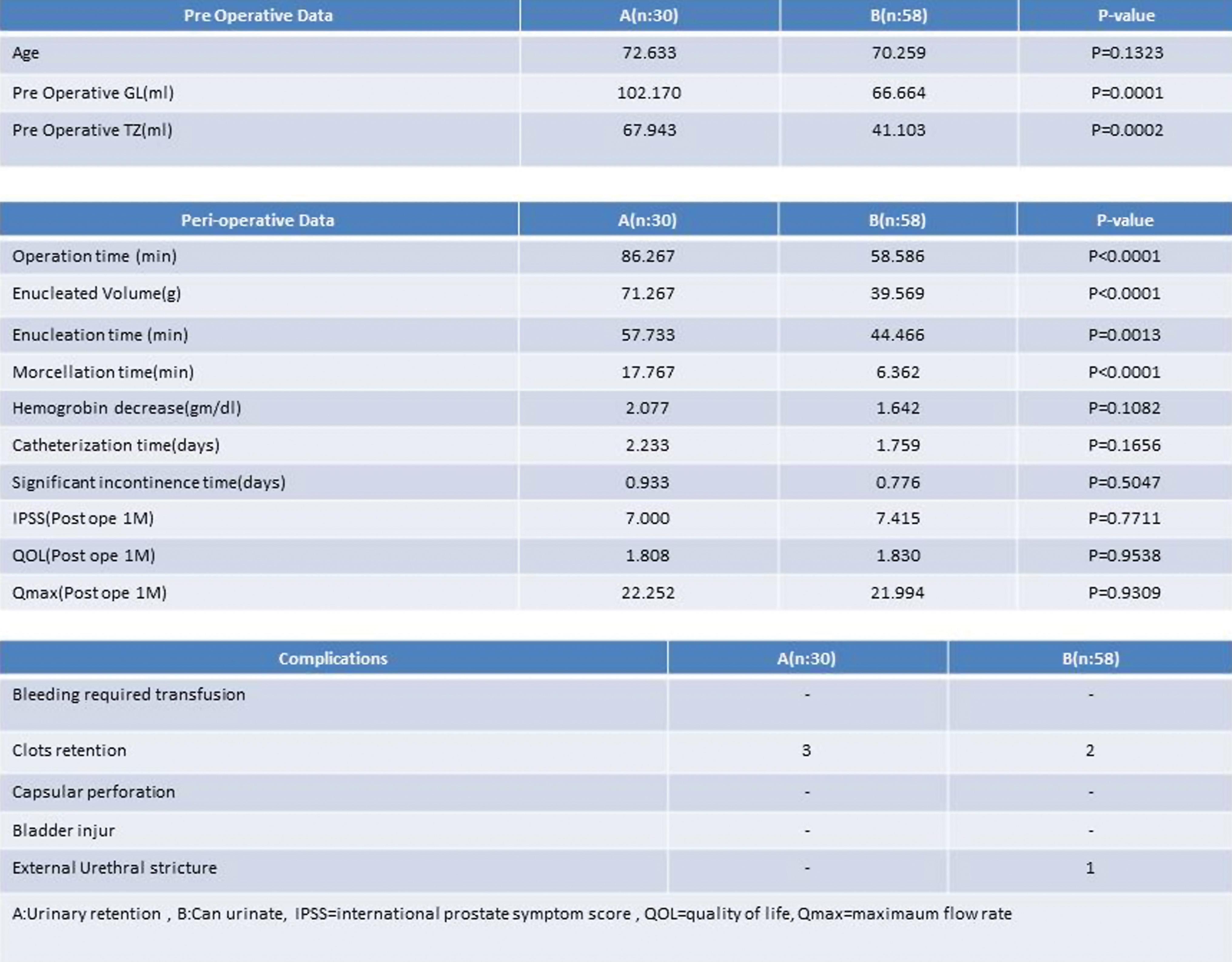
Holmium Laser Enucleation of the Prostate in Patients on Anticoagulant Therapy
ObjectiveWe assessed the safety and efficacy of holmium laser enucleation of the prostate (HoLEP) in patients on anticoagulant therapy.MethodsWe retrospectively reviewed the records of 137 consecutive patients who underwent HoLEP at our institution between October 2004 and June 2011. Thirty-two patients were on chronic oral anticoagulant therapy (group 1) and 105 without anticoagulant therapy were regarded as control (group 2). Two patients underwent HoLEP without oral anticoagulant withdrawal, 8 underwent with heparin substitution and 22 stopped anticoagulants before surgery. Postoperatively, anticoagulants were resumed after the patients could receive medication. Perioperative and postoperative data were compared between the two groups.ResultsThe mean total operating time was 138 and 170 minutes in group1 and group 2, respectively (P=0.038). The weight of tissue retrieved was 46.1 g and 59.4 g, respectively (P=0.039). The decrease in hemoglobin level was 1.2 g/dl and 2.1 g/dl (P=0.003). There were no significant differences in the duration of postoperative catheterization (group 1, 2.3 days; group 2, 2.0 days; P=0.48) and that of hospital stay (group 1, 7.7 days; group 2 6.9 days; P=0.29) between these two groups. One patient in group 1 undergoing heparin substitution and 2 patients in gruop2 required blood transfusion. No patients required termination of the procedure because of intraoperative bleeding.ConclusionsHoLEP may be the ideal treatment for patients on anticoagulant therapy with symptomatic benign prostatic hyperplasia.
Transurethral Enucleation with Bipolar for Prostatic Hyperplasia beyond 100 cc.
Transurethral resection of the prostate (TURP) is the standard treatment for men with benign prostatic hyperplasia, but because of the risks of bleeding and TUR syndrome, patients with large prostates are usually offered open removal of prostate tissue. We assessed 14 patients with prostates of>100cc who underwent transurethral enucleation with bipolar (TUEB) between January 2008 and March 2010. In TUEB, incomplete enucleation is performed with a TUEB detaching blade, and this is followed by removal of the prostatic tissue by TURP.The mean duration of surgery was 109 min. The mean weight of removed prostate tissue was 58.7 g. The mean decrease in the level of hemoglobin was 0.5g/dl. There were no major complications, and no patients developed transurethral resection syndrome or required blood transfusion. At preoperative baseline the mean symptom score was 23.0, mean peak urinary flow rate 7.0 cc/s, and mean post-void residual urine volume 152 cc. At 3 months postoperatively the mean symptom score was 7.8, mean peak urinary flow rate 11.4 cc/s, and mean post-void residual urine volume 14 cc. Significant improvements in all parameters were observed after surgery. The short-term outcomes showed that this technique was a suitable alternative to open prostatectomy and TURP.
Rapid Restoration of Voiding Function after Transurethral Enucleation of Prostate With Bipolar (TUEB)
[PURPOSE]To evaluate voiding function after TUEB(transurethral enucleation with bipolar) for the patients with BPH. [OBJECT AND METHOD] Objects are 24 BPH patients who underwent TUEB from February, 2008 to October, 2010. Average age was 68 years old. Average estimated prostate volume was 61.1ml. Urethral catheter was removed on the fifth day after TUEB. Voiding function was evaluated on that day. [RESULT] The average operation time was 102 min. The average resected volume was 27g. Blood hemoglobin (Hb) and serum Na concentration were significantly decreased after TUEB as follows; Hb 14.5g/dl to 12.8g/dl(p=0.00), Na 143.7mEq/l to 141.6mEq/l (p=0.001). There was no patient who required transfusion. IPSS, QOL score, mean flow rate, and residual urine volume were remarkably improved after TUEB as follows; IPSS 24.3 point to 13.5 point (p=0.01), QOL score 5.3 point to 3.0 point (p=0.004), MFR 7.5ml/sec. to 14.1ml/sec.(p=0.001), residual urine volume 112ml to 28ml(p=0.001). [CONCLUSION]Although the present study is small and retrospective, voiding function rapidly improved 5 days after TUEB. Electric coagulation procedures can be reduced in TUEB comparing with TURP. This may be, at least in part, a possible reason for the rapid restoration of voiding function after TUEB. A larger study with longer follow-up is warranted.
Department of surgery related division of urology, Kobe university graduate school of medicine
Introduction and objectivesHolmium laser enucleation of the prostate (HoLEP) is being increasingly performed for the surgical management of bladder outlet obstruction. It is a safe and effective therapeutic procedure, independent of prostate size, with low morbidity and a short hospital stay. There were very few reports regarding the method for adverse events including infectious complication. MethodsOne hundred and twenty-six patients had HoLEP at our institution from February 2005 to March 2011. We assessed the post-operative complications including infectious complications and their prevention. ResultsCefazolin was used in 54 cases, sulbactam/ampicillin in 29, cefotiam in 9 were used as prophylactic antibiotic administration. The mean duration of dosing was 2 days (range: 1-5). There were 8 infectious complications (6.3%) after HoLEP, including acute prostatitis in 7 cases and epididymitis in 1. In them, 6 cases had a history of retention, and 5 with catheterization. Additionally, the prostate size of 4 cases were more than 100 ml. Serratia marcescens in 2 cases and Proteus mirabilis in 1 were detected from urine culture. The febrile infection occurred median 3 days after HoLEP. All patients with febrile infection were cured by dosing oral levofloxacin in 5 cases and carvapenem in 3. Other major complications included transient urinary incontinence (37.6%), gross hematuria (10.4%), miction pain (3.2%), perineal pain (4.8%), dysuria (2.4%), and did not become severe. ConclusionsWe plan to continue this study for the establishment of guideline for prevention of especially infectious complication.associated with HoLEP.
Turis Botton Prostate Resection: Our Preliminare Experience
Objective: Aim of this study was to evaluate efficacy and safety of Botton TURis technique. Methods: From June 2010 to March 2011, a single surgeon treated with Botton TURis vaporesection 15 pts with a minimum followup of 3 months. A database was elaborated with the preoperatory parameters, surgical data, peri and postoperative complications, postoperative informations and follow up data after 1, 3 and 6 months (PSA, prostate ultrasound, uroflowmetry index including postvoiding residual, IPSS, IqoL, IIEF5, Hgb and Hct, urine exams and urinocolture).Results: The average of the patients was 66 years (range 47-90) and medium follow up was 6 mo (9-3 mo). We observed, in all the patients, a statistically significant increment in respect of the Qmax and Qave (p<0,001) baseline, the IPSS (p<0,01) and the QOL (p <0,01). Mean post-surgical hospitalization and catheterization periods were, respectively, 36 and 12 hours; besides mean post-surgical Hb value was 14,45 g/dl. These results (Qmax, Qave, RPM, IPSS, IEFF-5, TRUS) significantly improved as functional outcome from the third month onward remaining stable in the follow-up. No patient underwent neither post-surgical hemotransfusion nor short term complications. No patients discontinued antiplatelet therapy in progress.Conclusions: TURis is a potential new alternative way to standard TURP and allows virtually bloodness resections, good tissue removal and a prostatic TURP-like cavity. It seems to be a safe procedure, also for patients at high risk of bleeding. In our opinion TURis is an easy to learn technique, much more cost-efficient than laser.
Assessment of Botulinum A Toxin (BTX-A) effect in Treatment of Spastic Neurogenic Bladder
Introduction:Overactive bladder (OAB) is a common cause of LUTS. The main symptoms included urgency with or without urge incontinence, frequency and nucturia. Treatment of incontinence due to detrusor overactivity is a problem. Nowadays, this syndrome treats with Anticholinergics (conventional therapy), neurostimulation, and biofeedback but none of them are so effective in relieving symptoms. In this study we analyzed intravesical injection of BTX-A in treatment of OAB. Materials & Methods:This study included 25 patients all of them refractory to anticholinergic therapy or could not continue their treatment due to side effects. The patients were followed 3-5 weeks clinically and by urodynamic study and success rates was defined as a decrease in symptoms (specially for incontinence) and improvement of bladder capacity and maximal detrusor pressure.Also, we evaluated their clinical status 6 months after the initial follow-up. Results:25 patients were studied in the BTX-A group. The mean age was 17.64±14.25 years. In BTX-A group bladder sensation improved from 4.4±0.65 to 1.5±0.65 while, cystometric capacity and postvoid residual urine volume increased and maximal flow rate and detrusor pressure at maximal flow rate decreased. The treatment was effective 4 to 6 months. Conclusion:We concluded that intravesical injection of BTX-A has significant therapeutic effects on overactive bladder. Keywords:Overactive bladder(OAB),botulinum-a toxin(BTX-A),detrusor overactivity.
Clinical Analysis of the Failure in the Treatment of Posterior Urethral Stricture with Holmium Laser Endourethrotomy
The Causes Analysis of Urethral Stricture after Transurethral Resection of Prostate
Clinical outcome from 2nd TUR-Bt:single center experience.
Purpose: We assessed clinical outcome from 2nd TUR-Bt for high risk superficial bladder cancer in our institution.Material and Methods: We investigated patients who undergone 2nd TUR-Bt for superficial bladder cancer from September 2007 to June 2011. All patients had T1G2 or T1G3 urothelial carcinoma(UC) at 1st TUR-Bt. Results: A total of 17 patients (male 15, female 2) performed 2nd TUR-Bt 18 times in all. Mean age was 71.7 (53-80) years old. In 1st TUR-Bt, the number of T1G2 and T1G3 patients were 4 and 14 respectively, and with the exception of urothelial carcinoma, adenocarcinom and squamous cell carcinoma were detected in a patient respectively. In 2nd TUR-Bt, a total of five patients(28%) had UC. Three of them had T1G2, and the other two had T1G3. Of twelve patients with no malignant findings, six had recurrence after that. But all patients still alive without one patient who died of prostatic cancer and have no serious complications.Conclusion: Because we can performed 2nd TUR-Bt for high risk superficial bladder cancer in safety and are sometimes able to resect residual tumor in 2nd TUR-Bt, we may conduct 2nd TUR-Bt more aggressively.
Comparison of Prostatic Abscess Treatment: Is Transurethral Resection of Prostatic Abscess more effective than Needle Aspiration
Abstract Withdrawn
Department of Urology, Chungnam National University School of Medicine
Purpose: Our aim was to evaluate the efficacy of photoselective vaporization of the prostate (PVP) in the patients with weak bladder contractility who were unresponsive to medical treatment.Materials and Methods: From May 2008 to March 2011, we evaluated consecutive 61 cases who had preoperative urodynamic evaluations among the patients who underwent PVP for lower urinary tract symptoms. According to bladder contractility index, the patients were assigned to 2 groups: Group I consisted of patients who had weak bladder contractility (n=28), and Group II consisted of patients who had normal bladder contractility. The efficacy of the PVP was assessed at 1, 3, 6, and 12 months postoperatively using the International Prostate Symptom Score (IPSS), uroflowmetry, postvoid residual urine volume (PVR), and 3-day frequency-volume charts (FVC). Results: The IPSS, PVR and FVC were significantly improved in Group I and all parameters in Group II. Patients in Group II showed a more significant improvement with regard to the IPSS and QoL than Group I.Conclusions: PVP is considered an optional procedure for the treatment of men with weak bladder contractility who are unresponsive to medical treatment.
Bipolar TURP versus Greenlight Laser PVP for High-Risk Patients- Experience from a single UK Institution
Introduction:It has been suggested that both bipolar-TURP and KTP (Greenlight) laser vaporisation of the prostate (PVP) are safe surgical options for high-risk patients with symptomatic BPH. With the number of high-risk patients requiring surgery increasing, it is important to identify the safest treatment modality for this group. Purpose:This is the first study to compare bipolar-TURP to KTP PVP in high-risk patients from a single UK centre. Methods:Case-notes of all high-risk patients (ASA >3) who underwent bipolar-TURP or KTP PVP over a 1-year period were retrospectively analysed. Results:126 case-matched patients were included. 60 underwent bipolar-TURP and 66 underwent laser PVP. Operative time was significantly shorter for bipolar-TURP (38 min v. 62 min), although the laser group experienced a reduced length of stay (P=0.01). There were no cases of TUR-syndrome and no differences in intra-operative bleeding rates. Symptomatic outcomes at 3-month follow-up were similar, with a mean±SD improvement in IPSS of 7.7±7.4 (bipolar-TURP) and 10±6.2 (KTP PVP), a mean (range) improvement in Qmax of 6.2 (3.5-13.9) for bipolar-TURP and 6.6 (0.8- 11.1) for KTP PVP, and a mean fall in post-void residual volume of 75% for bipolar TURP and 66% for KTP PVP. Furthermore, there was no significant difference in re-intervention rates (13% for bipolar-TURP vs. 10% for KTP PVP). Conclusion:Both bipolar and laser technologies are valid treatment options with minimal morbidity in carefully selected ASA >3 patients with symptomatic BPH. Long-term randomised studies are required to confirm our preliminary findings.
Comparative Study about the Efficacy and Complications of Photoselective Vaporization for Benign Prostatic Hyperplasia Classified by the Volumn of Prostate
Introduction: We evaluated the efficacy and stability of photoselective vaporization of prostate.
Purpose: This study was planned to compare the efficacy and complications of photoselective vaporization for benign prostatic hyperplasia, classified by the volumn of prostate.
Materials and Methods: We performed comparative analysis of 158 patients suffering with symptomatic bladder outlet obstruction due to BPH, who had undergone photoselective vaporization for prostate using potassium-titanyl-phosphate laser, between June 2008 and December 2010. Each patients were classified into three groups by the volumn of prostate :<40cc; group I, 40-60cc; group II,>60cc; group III. The clinical efficacy of each group was compared in terms of the International Prostate Symptom Score, quality of life index, changes in the maximum urinary flow rate, postvoid residual urine and complications. The mean follow-up period was 5.2 months. Student t-test and ANOVA were performed for statistical analysis.
Results: All efficacy parameters were significantly improved in all patients p<0.05. With respect to each of the three classified groups, the efficacy parameters of each group were also significantly improved p<0.05. However, in group III, the postoperative IPSS and QoL index were lower than the average value. Especially, the items for frequency, nocturia and urgency of the IPSS resulted in bad grades. The rate of complications in group III were higher than those in groups I and II, such as urinary retention, delayed hematuria and bladder neck contracture.
Conclusions: Despite the excellence of KTP laser, careful consideration must be given when the operation is performed on patients with a large prostate size.
Endoscopic Urology Department, Russian Medical Academy of Postgraduate Education, Moscow, Russia
The Initial 100 caces of Anteroposterior HoLEP
OBJECTIVES: HoLEP surgical procedure still has no unified view, tend to become complex procedures, often difficult to learn. Stress urinary incontinence (SUI) is an probrem that often caused by damage to the sphincter. The problem was resolved by a new surgical technic, anteroposterior dissection.METHODS: A total of 100 cases of anteroposterior HoLEP were performed between March 2010 and june 2011. We retrospectively reviewed the database. Mean age of patients was 70.1 years (range: 52-87), preoperative mean prostate size was 64.5ml (range: 20-245). All patients were assessed at least 1 months postopelativery for peak flow rate (Qmax), and residual urine, international prostate symptom score (IPSS), quality of life (QOL), and clinical SUI.RESULTS: Of five surgeons, three was beginners and two was experts. The mean weight of the resected tissue was 39.7g (8-175). The mean total operation time was 100.1 mean enuclation time was 67.6min, and mean morcellation time was 10.5min. Preoperative mean IPSS, QOL Q(max) and residual urine were 18.6, 4.8 6.2 ml/sec and 89.1ml, respectively. At 1 mouths after surgery, mean IPSS, QOL, Q(max) and residual urine were improved to 6.9 , 1.9, 17.0 ml/sec and 17.0ml, respectively. Urethral stricture was noted in 2 patients (2.0%). Postoperative mean hemoglobin decrease was 0.6 g/dl, and there were no cases of transfusion. Clinical SUI at 1 month after surgery was noted in 7 patients.CONCLUSIONS: These results indicate that our anteroposterior dissection HoLEP is safe and low complications rate because of the clear procedure.
Department of Urology, Kitakyushu General Hospital, Fukuoka, Japan
Objectives; Transurethral resection of bladder tumor in one piece (TURBO) was reported in the Journal of Urology in 2000 by Ukai. We analyzed treatment results of TURBO in our hospital and examined the value of this procedure, especially for the pathological findings, recurrence and indication of second TUR for TURBO. Methods; A total of 18 patients with bladder tumors carried out TURBO under spinal anesthesia, in some cases blocking the obtulater nerve, from April 2006 to July 2010 in our hospital. All cases were followed for over 1 year. The procedure has 4 steps in accordance with the Ukai's method. We investigated pathological findings (margin situation) and recurrence. Results; It is possible to diagnose the precise pathological findings by TURBO. We judged the width and depth ew in sequential section. Operation time of TURBO 92.2min (36-170 min) was longer than TUR-BT. 5 cases (27.8%) had a recurrence in 18 cases. 2 cases (11.1%) had a recurrence in under 1 year, but the locations were other places. One case had a same place recurrence after 13 months. There were no cases of same place recurrence in under 1 year among margin-negative cases. Therefore we judged that ew-negative cases had no residual cancers. Conclusions; TURBO is a safe and useful procedure that provides precise pathological findings with minimal complications. It seems that the indication of Second TUR for TURBO is ew-positive cases. TURBO has a possibility to be gold standard of the treatment for non-muscle invasive bladder cancer.
Partial Cystectomy for Metastatic Bladder Tumor using Transurethral Incision
Introduction: In open partial cystectomy, the margin of the bladder tumor is usually detected by manual perception. However, in laparoscopic surgery, it is hard to find the margin of the tumor. The usefulness of a simultaneous transurethral cystoscopy with illumination has been reported to identify the margin of the bladder tumor. Perivesical fat is too thick to define the tumor margin with guidance of transvesicular illumination in obese patients. Purpose: We report a case of metastatic bladder tumor that had underwent partial cystectomy using transurethral incision. Materials and Methods: A 67 years old male patient with gross hematuria has detected a single 2cm solid tumor on posterior wall of the bladder. Transurethral resection of the bladder tumor was performed and pathologically diagnosed as metastatic colon carcinoma (He had a sigmoid carcinoma and sigmoid colon resection was done 2 years ago). There was no other metastasis. Partial cystectomy was performed using a transurethral resectoscope. The edge of the tumor was cleanly identified by the resectoscope and the mucosa was circumferentially incised with 10mm margin to penetrate the perivesical fat, and the bladder wall containing the tumor had been resected. Results: Transurethral incision was a useful method for partial cystectomy of the bladder tumor. The tumor was pathologically reported adenocarcinoma, pT1N0M0 with negative surgical margin. It was compatible with metastatic colon carcinoma. Conclusions: Transurethral incision using a resectoscope is a safe and useful method for partial cystectomy of metastatic bladder tumor.
Transurethral En Bloc Resection of Bladder Tumors using TURis System
Objective: Conventional bladder tumor transurethral resection entails problems as the resected specimens are unsuitable for pathological evaluation and there is the possibility of implantation because cancer cells scatter as the tumor is fragmented. Transurethral en bloc resection of bladder tumors is desirable for the evaluation of the pathological depth of bladder tumors in resected specimens and for decreasing recurrence without cancer cell scattering. Transurethral resection in saline (TURis) system for bladder cancer en bloc resection is evaluated. Materials & Methods: Thirty men and 5 women (50 tumors), 42 to 88 years old underwent transurethral en bloc resection with the muscle layer using TURis system. The circular incision connected marks made about 10 mm. away from the tumor edge and continued until the superficial muscle layer was visualized using knife electrode. The level incision beneath it with subsequent tumor retrieval using flat electrode. Finally, the resected specimen was grasped with a loop electrode and retrieved. Results: Tissue slides crossing the center of the tumor correctly determined the depth of cancer invasion as stages pTa to pT2. No uncontrollable bleeding, perforation or other serious complications occurred. However, air bubbles are frequent and bothered with TURis. Conclusions: Transurethral en bloc resection is a safe and useful technique that also provides sufficient material for pathological evaluation. Additional prospective studies are needed to determine the independent prognostic role. Also company is urged to develop new technology against air bubbles.
Department of Urology, Fuchinobe General Hospital, Kanagawa, Japan
Purpose: Holmium laser enucleation of the prostate (HoLEP), first reported by Gilling et al. in 1998, has recognized as safe and effective transurethral treatment option in patients with symptomatic BPH of any size, and recently it has been proposed as a new gold standard for treatment of BPH. It is known that a steep learning curve and longer operation time has been main limitation of HoLEP. Usually expertise to this procedure could be quantified by the enucleated tissue weight / operation time (g/min). In addition to this index, we had analyzed the total energy used for HoLEP.Materials and Methods: We retrospectively reviewed the 55 patients who underwent HoLEP by equivalence maneuver by single practiced hand for the enucleated time, enucleated tissue volume and total energy used between January 2010 and May 2010 at our hospital.Results: Total energy increased with an increase of enucleated volume. Energy per enucleation time was approximately constant regardless of enucleated volume. Energy per enucleated tissue volume was approximately constant regardless of weight, but higher energy was required for when enucleated tissue weight was 30g or less.Conclusions:It has been understood that energy per minutes and energy per gram are constant in this analysis. Moreover, it was noted that enucleation of smaller prostate size is inefficient from the energy dissipation stand point.
Department of Urology, Kitasato University School of Medicine, Sagamihara, Japan
INTRODUCTION: High grade non-muscle invasive bladder urothelial carcinoma is potentially aggressive cancer diatheses of the bladder with heterogeneous clinical behaviors. PURPOSE: We sought to determine whether the molecular markers E-cadherin, coxsackie-adenovirus receptor (CAR), S100A4 and uroplakin III are associated with clinicopathological outcomes and prognosis in high grade (grade 3) non-muscle invasive bladder cancer treated with transurethral resection of bladder tumors (TURBT). METHODS: Immunohistochemical staining was carried out on serial sections from archival specimens of 81 patients who underwent TURBT. Altered expression of these proteins was stratified further into simple (one or fewer) and multiple altered (two or more) for the purpose of analyses. Mean and median follow-up time was 53.5 and 34.4 months, respectively. RESULTS: E-cadherin, CAR, S100A4 and uroplakin III expression were altered in 16, 16, 28, and 59% tumors, respectively. Multiple altered molecular markers had a significantly increased risk of bladder cancer-specific mortality (p=0.020, log-rank test). Multivariate models that included clinicopathologic outcomes and categorized molecular markers found multiple altered molecular markers and lack of BCG instillation to be predictors of cancer-specific death (p=0.049 and 0.020, respectively). However, no individual altered protein was associated with prognosis. CONCLUSIONS: Multiple alteration of molecular markers is a strong predictor of mortality in bladder cancer patients undergoing TURBT, suggesting that high-grade non-muscle invasive cancer is heterogeneous and has a variety of biologically aggressive behaviors. A combination of molecular markers plays a more pivotal role in bladder cancer progression, and may aid a minimally invasive modality for determining their prognosis.
Epidemiology of Stone disease in Australia
Introduction: Renal colic is a common presentation to emergency departments worldwide. However, despite the significant morbidity and the considerable financial cost associated with this condition, there is surprisingly little epidemiological data published on stone disease in Australia. Objective: To determine the incidence and treatment rate of stone disease in Australia, and examine published data on associated metabolic disorders. Materials and methods: The Medicare Australia and Australian Institute of Health and Welfare (AIHW) databases were used to determine the incidence rates of stone disease in Australia. Literature review was conducted to evaluate available local epidemiological data pertaining to risk factors for stone disease. Results: The incidence of upper urinary tract calculi in Australia is around 129 cases per 100,000, which has remained relatively constant over the past decade. This contrasts the annual stone treatment rate, which has increased significantly from 80 to 96 per 100,000 during the same period. In regards to metabolic factors of stone disease, historical data from a metropolitan stone clinic reported abnormalities in calcium metabolism to affect almost one-third of stone formers. This contrasts a study conducted in a rural desert town of central Australia, which found a disproportionate number of uric acid stone formers, highlighting the influence of environmental factors in stone formation. Conclusion: The incidence of stone disease in Australia would appear similar to other Western countries and has been stable over the past decade. More contemporary data is required to determine any changes to stone type and metabolic factors affecting stone disease in Australia.
Clinical Analysis of Septic shock after Holmium Laser Lithotripsy for Ureteral Calculus
Clinical Analysis of Failed Ureteroscopic Holmium Laser Lithotripsy in the Treatment of Ureteral Calculus
Department of Urology,Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
Introduction: Nonenhanced helical computed tomography (NHCT) has evolved into a well-accepted diagnostic method in patients with suspected ureterolithiasis. NHCT not only shows stones within the lumen of the ureter, it also permits evaluation of the secondary signs associated with ureteral obstruction from stones.Purpose: To compare the degree of secondary signs in NHCT between calcium and uric acid stone formers.Materials and Methods: 117 patients of ureteral stone who underwent NHCT examination and FTIR analysis of stone sample were enrolled for study. Clinical data of age, sex, estimated GFR, urine pH, and radiological data of secondary signs on NHCT were collected.Results: The uric acid stone formers have significantly lower urine pH and GFR in compare to calcium stone formers. They also have a higher percentage of the secondary signs on NHCT compared to calcium stone formers, including rim sign (78.9% to 60.2%), hydroureter (94.7% to 89.8%), perirenal stranding (84.2% to 59.2%) and kidney density difference (73.7% to 50.0%). The radiological difference is statistically significant in perirenal stranding. (p=0.041).Conclusions: Uric acid stone formers have more severe degree of secondary signs on NHCT compared with calcium stone formers, a tendency which may result from acidic urine environment .
Robotic and Laparoscopic Ureterolithotomy: Indications and Technique
Introduction: We share our experience with laparoscopic/robotic ureterolithotomy and present indications for this technique in the treatment of large, impacted ureteral stones.Methods: We have compiled a series of 9 laparoscopic ureterolithomies (4 robotic-assisted) between January 2008 and June 2011. Our criteria for inclusion were large stones (greater than 1cm) and had evidence of ureteral impaction on CT scan imaging (hydronephrosis with ureteral thinning). Results: The stones were located in the proximal ureter in four patients, mid-ureter in three patients and in the distal ureter in one patient. Stone sizes ranged from 1.3 cm to 3.1 cm. Composition revealed predominantly calcium oxalate monohydrate in five patients, uric acid in two patients, brushite in one, and calcium oxalate dehydrate in one. Seven of the stone retrievals were performed via anterior ureterolithotomy and primary closure, and in two patients, ureteral resection with end-to-end spatulated ureteral anastomosis was required.Mean operative time was 195 minutes. Average blood loss was 45cc. There were no intraoperative/postoperative complications and no conversions to open surgery. Patients were discharged on postoperative day one. All of the patients were rendered stone free, and urography performed 4-6 weeks after surgery reveal no extravasation, ureteral strictures or hydronephrosis.Conclusions: In our series, post-operative imaging has rendered our patients 100% stone-free. The greatest advantage of laparoscopic or robotic ureterolithotomy is the high probability of rendering a patient stone-free in one session. Longer follow-up of our patients will determine the long-term stricture rate with this method.
Columbia University Medical Center, New York, NY, USA
Introduction: Many clinicians are reluctant to treat vitamin D deficiency in kidney stone formers because of the theoretical risk of increasing urinary calcium (UCa) excretion and the risk of calcium stone recurrence. Purpose: We report on the effect of vitamin D repletion on UCa among stone-formers.Methods: Patients were recruited from three metabolic stone clinics. Enrollment criteria included: 1)history of nephrolithiasis; 2)UCa between 150 and 400 mg/day; 3)serum 25-hydroxyvitamin D (25(OH)D) level less than 30 ng/ml. Patients were given oral ergocalciferol 50,000 IU weekly for 8 weeks. Serum and 24-hour urine tests were repeated after 8 weeks.Results: 30 patients were enrolled and 29 completed the study. Vitamin D repletion resulted in no significant change in UCa excretion [table 1]. Other urinary parameters were similarly unchanged. Subgroup analysis on the basis of initial 25OHD and parathyroid hormone levels revealed no change in UCa excretion in any subgroup. No patient experienced any side effects, including kidney stone recurrence, while taking vitamin D.Conclusions: Among stone-formers with vitamin D deficiency and moderate levels of hypercalciuria, vitamin D repletion does not appear to increase UCa excretion. Vitamin D therapy, if indicated, should not be withheld on the basis of prior stone disease.
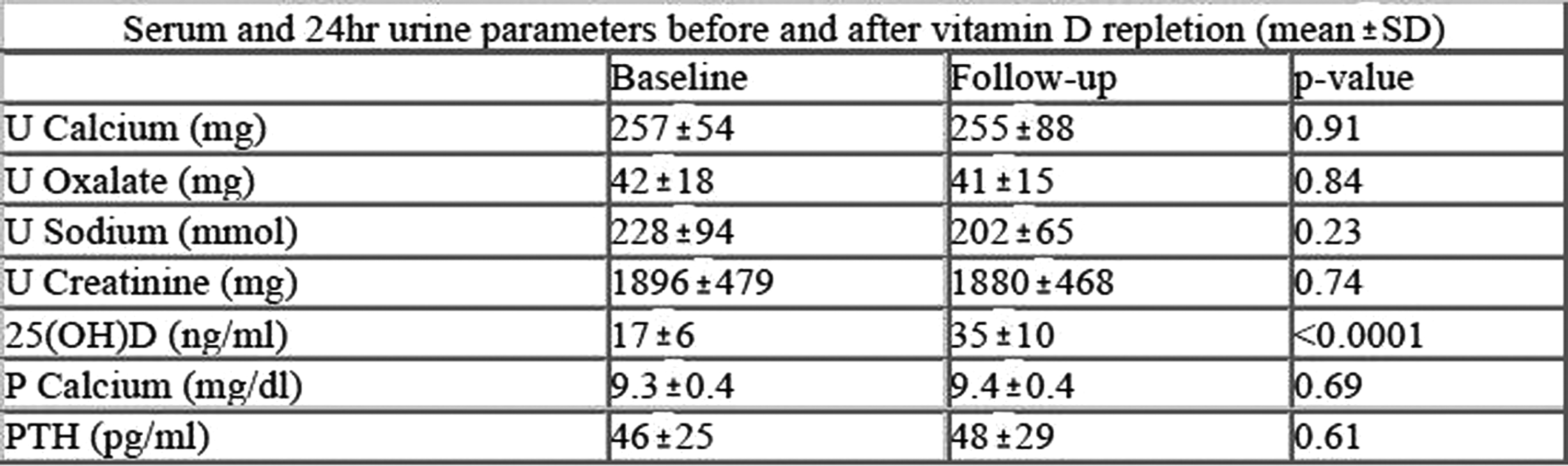
A Case Report of Successful Transurethral Ureteroscopic Lithotripsy for right Ureteral Stone in a Retrocaval Ureter without Surgical Correction
Introduction:Several reports of urolithiasis in a retrocaval ureter were observed but transurethral ureteroscopic lithotripsy (TUL) for right upper ureteral stone in a retrocaval ureter was not reported. Purpose:We report on a successful TUL treatment of right upper ureteral stone in a retrocaval ureter without surgical correction.Materials and Methods:A 48-year-old woman consulted to us for right back pain. CT revealed right ureter run behind the inferior vena cava (IVC) at the level of L2 and right ureteral stone 8 mm in size existed between the IVC and the aorta as far as L3 level. Excretory urography demonstrated right hydronephrosis at the level of L3. Right ureteral stone was not shown by KUB because stone was duplicated with vertebral bone. Right double J ureteral stent was inserted. This retrocaval ureter was classified as type 2 : the upper ureter is not kinked but passes behind the IVC at a higher level, with the renal pelvis and upper ureter lying almost horizontal before encircling the IVC. Results:TUL using flexible fiber and ureteral access sheath was performed. Stone was pushed up into the middle renal calyx and crushed by the holmium:YAG laser. Conclusions: Although TUL for stone in type 1 (S shaped ureter) retrocaval ureter without surgical correction might be difficult, TUL for stone in type 2 might be possible. To our knowledge, this could be a first report of TUL for urolithiasis in a retrocaval ureter.
Department of Urology, Chiayi Christian Hospital, Chiayi, Taiwan
IntroductionStone matrix protein (SMP) plays an important role in kidney stone formation. Several proteomic studies applied to calcium-containing stones have been reported and more then 100 SMPs have been discovered. However, proteomic study on kidney uric acid stone (KUAS) has never been reported before. PurposeIn this study we analyzed kidney KUAS SMPs with mass spectrometry (MS) and immunoblot methodologies.Materials and MethodsPurified KUAS from 5 individuals were de-mineralized and SMPs were isolated. The obtained proteins were analyzed with reverse phase liquid chromatography (LC)-tandem MS. The acquired data were searched against a Swiss Prot human protein database using Matrix Science Mascot. The sequences of the identified proteins were submitted to the Amigo website for gene ontology analysis. They were also submitted to Metacore software and Kyoto Encyclopedia of Genes and Genomes website (KEGG) for pathway analysis. Expression of the MS-determined proteins was verified by immunoblot assays.ResultsLC MS analysis identified 242 (52-156) proteins. Metacore software analysis suggests that inflammation may play an important role for KUAS formation. Endogenous metabolic pathways were also analyzed and submitted to KEGG website which revealed that these proteins may participate in fat metabolism. Five identified proteins were selected for immunoblot validation and four proteins were confirmed.ConclusionsOur results suggest that inflammatory process may play a role in KUAS formation. Our endogenous metabolic pathway analysis data revealed that these proteins may also participate in lipid metabolism. Whether our findings establish a relationship between lipotoxicity and KUAS formation requires further efforts of research.
Effectiveness of Same Session Bilateral Ureteroscopy for Bilateral Upper Urinary Tract Caliculi
Objective: We sought to determine the safety and efficacy of ureteroscopy and laser lithotripsy for the treatment of bilateral upper urinary tract caliculi.Patients and methods: From January 2010 to June 2011, we performed ureteroscopic treatment in 82 patients with upper urinary tract caliculi, of which 10 patients (12.2%) were done as same session bilateral ureteroscopy. Patients were considered stone free if no residual stones were seen endoscopically and radiographically after the procedures. Success was defined as stone free with no hydronephrosis after the last treatment. In all cases we used 6.4 Fr semirigid and 8.5 Fr flexible ureteroscope. Holmium: yttrium-aluminum garnet laser was used as a lithotripter. Results: The mean stone size was 8.1±2.5 mm (range: 3-14). The mean operative time was 85.7±25.5 min (range: 50-132). The overall stone-free rate was 90.5%. The success rate was 100%. Complications have been recorded in no patients. This is a retrospective review and our results are based on a relatively small sample size.Conclusions: For select patients with bilateral upper urinary tract caliculi, ureteroscopy with laser lithotripsy is efficacious and safe.
Female Bladder Caculi. Risk Factors and Natural History
INTRODUCTION: Urolithiasis is increasingly becoming prevalent in women. Bladder stones are rare in women, but appear to be rising in incidence, and this diagnosis should be entertained in some patients with medical comorbidities, pelvic organ prolapse or neurological conditions.METHODS: We retrospectively reviewed 1439 consecutive stone clinic patients at our medical center from Jan 2008 until Dec 2010. Female patients with bladder stones were identified, and patient demographics, associated medical comorbidities (gout, diabetes, neurologic conditions, pelvic organ prolapse, etc.), stone size, stone composition and type of intervention (medical versus surgical) were evaluated.RESULTS: 12 female patients presented to urology for bladder stones. The average age on presentation was 57.3 years (range 27-89), and mean stone burden was 1.2cm (range 2-40mm). 33% were composed of struvite + calcium phosphate, 17% were calcium phosphate, 8% uric acid and remainder calcium oxalate. 50% of patients had previous bladder or renal stone history, and 33% of patientsm with bladder stones had neurogenic bladder from Parkinson's, multiple sclerosis, sacral agenesis and pelvic radiation. In patients without neurogenic bladder, underlying conditions of urethral stricture, mesh extrusion into urinary bladder, grade 3 pelvic organ prolapse, hyperthyroidism were diagnosed.CONCLUSIONS: Women with neurogenic bladder and pelvic organ prolapse with LUTS should be evaluated for possible bladder stones. Interestingly, only 50% of patients with an average age of 57 ad no previous bladder or renal stone history.
In-Hospital Stays for Urolithiasis: Analysis of Trends in French National Data
Introduction & Objectives: Urolithiasis is of health economics concern since it is very frequent. However, there is few data upon its issue in France.Material & Methods: We have analyzed the data issued from the national coding system for in-hospital stays and interventions, using urolithiasis codes and compared between public and private sectors. We have observed evolution of procedures and stays until 2009.Results: Public and private sectors were quite similar in terms of stays numbers (144,324 in 2009, and an evaluated total cost of more than 168 millions of euros). Since 2000, there has been an increase of more than 20% in the number of stays in the public sector and a stagnation in the private one. Public and private sectors appeared different in terms of: (1) stays without intervention (53 vs 26%; p <0.0001); (2) stays without associated diagnosis (5.78 vs 8.41%; p <0.0001). Since 2006, there has been a stagnation for percutaneous and surgical interventions (less than 5% of the number of interventions) whereas there has been a clear increase in endoscopic (+29% in private sector and + 16% in public one) and lithotriptic (+19 and + 5%) interventions.Conclusions: There were strong disparities between public and private sectors. Endoscopic interventions and lithotrity sessions have shown a sustained increase. Surgical and percutaneous interventions have shown a stagnation.
Comparative Study about Patients Satisfaction for Treatment Outcomes between Shock Wave Lithotripsy and Ureteroscopy for Upper Ureter Stones
Introduction: Both of shock wave lithotripsy and ureteroscopic removal of stone are widely used for treating proximal ureter stone.
Purpose: We evaluated patients satisfaction for treatment outcomes after shock wave lithotripsy and ureteroscopic removal of stone for proximal ureter stones.
Materials and Methods: We evaluated 183 patients who underwent SWL<n=113>or URS<n=70>for proximal ureter stone. Stone-free rates defined as no visible fragment on plain X-ray, complications and patient satisfaction were compared. Patient satisfaction was examined through specifically tailored questionnaire that included overall satisfaction and 4 domains; pain, voiding symptoms, cost and stone-free status.
Results: The stone-free rates after first, second and third sessions of SWL were 39.4%, 68.5%, and 87.6%. Overall stone-free rate of URS was 85.7%, which was comparable to that of third session of SWL. Complications were similar between two groups. Overall satisfaction and voiding symptoms, cost and stone-free status showed no significant difference between groups. In the pain domain, the SWL group had relatively lower satisfaction rate than URS group; p=0.05. Subanalysis showed that satisfaction rate of URS group with stone-free status was significantly lower than that of SWL group in patients with>10mm stones; p=0.035.
Conclusions: Overall treatment outcomes and patient satisfaction were not significantly different between SWL and URS. However, patients undergoing URS for>10mm proximal ureteral stones had lesser satisfaction with stone-free status, because of relatively lower stone-free rates due to upward migration. We suggest that factors regarding the subjective satisfaction of patients be included in counseling about treatment options for proximal ureteral stones.
Can an Efficient Emergency Stone Service be also Cost-Effective?
Despite existence of established guidelines on ureteric colic management, many patients are faced with delays and often receive suboptimal treatment. This wastes resources, and contributes to lower patient satisfaction. We evaluated our local practice of ureteric colic management to find avenues for providing efficient and cost-effective emergency stone service.This retrospective audit includes all 91 radiologically-confirmed ureteric colic cases admitted at our unit in one year period from 1/10/2009 to 30/09/2010. 20% of patients had complete basic metabolic screen during admission and definitive imaging was performed within recommended 24 hours in 70% of cases. Following admission, 45 cases (50%) were managed conservatively with a 4.4% readmission rate, (median length of stay 46 hours). Median follow up time in this group was 56 days with a 33% non-attendance rate. Intervention was required in 46 cases (50%). Ureteric stenting was performed in 26 cases. Better alternatives to stenting were available in 17 (65%) cases. Ureteroscopy was performed in 12 cases, whilst 9 patients had lithotripsy.Standards of investigation fall short of BAUS recommendations. Timely imaging has a potential for reduction of unnecessary admissions. If conservative treatment was delivered on outpatient basis this could provide potential savings on ward costs of £27,360, whilst further £14,620 could have been saved if 17 patients received definitive treatment instead of a stent. Patients receiving prompt definitive treatment and a trust running a cost effective service are not mutually exclusive.
Endoscopic Urology Department, Russian Medical Academy of Postgraduate Education, Moscow, Russia
Complications, as fornicalis bleeding, collecting system perforation, did not occur.
Connection to Amplats tube a tube of vacuum aspirator allowed to reduce average operation time on 20 min.
Urolithiasis as an Initial Presentation of Primary Hyperparathyroidism in the Normocalcemic Patient - Implications for Screening
IntroductionUrologists currently screen calcium stone formers for primary hyperparathyroidism, a known cause of urolithiasis in 1-2% of cases, by performing serum biochemical evaluations. PurposeEvaluate the relationship between urolithiasis and primary hyperparathyroidism in the normocalcemic, normoparathyroid hormone patient and provide implications for screening stone formers. Materials and MethodsPatient charts between 2005-2010 were retrospectively reviewed for evidence of urolithiasis upon initial evaluation for primary hyperparathyroidism in the surgical endocrine clinic. Of 400 patients who underwent parathyroidectomy, 78 were stone formers. All 78 patients had pathologically confirmed primary hyperparathyroidism.These 78 patients represented the study cohort. Data entered included basic demographic data, laboratory data (total calcium, ionized calcium, intact parathyroid hormone (iPTH), serum creatinine, and 24 hour urine studies when available). ResultsOf 78 stone formers, 6 (8%) had the combination of normal calcium (either ionized or total) and normal iPTH. Of the remaining 72 patients, 18 (23%) had normal serum ionized calcium, 10 (13%) had normal total calcium, and 22 (28%) had normal iPTH. Of 40 patients with 24 hour urine studies, 21 had normal calcium levels.ConclusionsWhile the ultimate relationship between primary hyperparathyroidism and urolithiasis remains to be elucidated, our data suggest urologists should look beyond serum chemistry studies when screening for primary hyperparathyroidism. Our data proposes we could double the detection rate of primary hyperparathyroidism among stone formers. Detailed screening would specifically include primary hyperparathyroidism symptomatology inquiries. This would likely lead to more expeditious referrals to specialists for workup.
Department of Urology,The University of Kyorin School of Medicine, Tokyo, Japan
Purpose: We evaluated the efficacy of the alpha1a-blocker silodosin and alpha1d-blocker naftopidil on stone clearance in shock wave lithotripsy (SWL) for solitary ureteral stones.Material and Methods: Fifty-one male patients with ureteral stones who underwent SWL were randomly divided into three groups. Group S (16 patients) was given silodosin (0.8mg/day); group N (19 patients) was given naftopidil (75mg/day); and group C (16 patients) received no medication (or only the pain relieving therapy). Stone clearance was assessed at 7, 14,21, and 28 days after SWL using plain abdominal radiography. Results: The stone-free rate was 31%, 42% and 19% for group S, N and C, respectively (NS). Among the patients with upper ureteral stones, the stone-free rate was 39%( 5/13 ), 47%( 7/15 ) and 0%( 0/13 ) for group S, N and C, respectively(P<0.05).Conclusion: When compared with no treatment, silodosin and naftopidil can significantly facilitate expulsion of upper ureteral stone fragments following SWL.
Impact of Stone Burden at Ureteroscopy on its Results
[purpose]The definition of stone burden at ureteroscopy was uncertain. Sum of maximum diameter, surface area and volume often were reported as stone burden. We investigated that what style of stone burden were the most reliable predictor of success rate in the ureteroscopy.[materials and method]The subjects of this study were 88 patients with urolithiasis who underwent ureteroscopy in Ooguchihigashi general hospital between August 2010 and June 2011. The primary endpoint was strict stone-free status. That was assessed by KUB on postoperative day 1. We retrospectively evaluated the relationship between surgical outcome and clinical features of calculi.[Results]Overall stone-free rate was 71%. Mean sum of maximum diameter of stone, surface area and volume were 30.5mm, 1042.6mm2 and 1720.1mm3, respectively. In multivariate analysis, stone surface (p=0.001), volume (p=0.013) and number of stone (p<0.001) were an independent significant factor for stone-free status. [Conclusions]This study demonstrated that stone surface, volume and number can be the predictors of ureteroscopy outcome.
Risk Factors for Uroseptic Shock in Patients with Calculous Pyelonephritis
To analyze the risk factors of uroseptic shock induced by acute calculous pyelonephritis, clinical characteristics of the patients were retrospectively evaluated. During January 2005 to December 2010, 54 patients including 30 female and 24 male were admitted to our hospital for the treatment of pyelonephritis associated with obstructive urolithiasis. Median age was 69 years old. Of 54 patients 37 had Karnofsky performance status 80% or more and 17 had 70% or less before the onset of pyelonephritis. Central nervous system disorder and diabetes mellitus were respectively detected in 15 and 8 patients as comobidity. Twenty-three patients had a past history of urolithiasis. Urine culture was positive in 43 of 53 examined and blood culture was positive in 16 of 36 examined. Escherichia coli was recognized as the most frequent pathogen. Laboratory findings revealed DIC in 14 patients. Urinary drainage with ureteral stent or nephrostomy were conducted in 47 cases. Septic shock which required vasopressor infusion against circulatory collapse was observed in 20 patients. These patients showed significantly lower thrombocyte counts and higher CRP values compared with the patients who did not require vasopressing agent. Three patients died of multi organ failure from septic shock. Our present data analysis revealed that thrombocytopenia, high CRP at hospitalization were the significant risk factors for the development of uroseptic shock from calculous pyelonephritis., but gender, age, performance status, comobidity had not significant correlation with the development of septic shock.
TUL for Ureteral Stone with Obstructive Pyelonephritis
Although an obstructed, infected kidney caused by upper urinary tract calculi can be lethal and therefore requires urgent drainage followed by complete stone removal, optimal method of drainage and stone removal remains to be established. In particular, the safety and feasibility of transurethral lithotripsy (TUL) is still unknown, because it is thought that TUL may cause postoperative sepsis by increasing intrarenal pressure. In this study, we aimed at examining the safety of TUL following ureteral stenting for septic patients with obstructing stones. From January 2008 to December 2010, 31 patients (male 17, female 14) with obstructed, infected kidney caused by ureteral stone were treated with retrograde drainage followed by TUL. The mean stone size was 6.7mm, and stone was located on proximal ureter: 20(65%), mid ureter: 6 (19%), and distal ureter 5 (16%). Intensive management such as the use of anticoagulants was performed in 4 patients (13%). Stones in the ureter were successfully removed by TUL in all cases. In one cases (3%), postoperative sepsis occurred. These results indicate that TUL following ureteral stenting is safe and feasible with no increased complication rate and excellent stone free rate. Therefore, we recommend that TUL following ureteral stenting can be a standard choice for the treatment of septic patients with obstructing stones.
Intentional Preoperative Stenting (IPS) for Ureteroscopy for Large Renal Stone.
Introduction
A large stone burden can be treated ureteroscopically, but the treatment often requires more than one procedure. Although the use of prestenting before ureteroscopy has been reported recently, the reasons for prestenting were passive, such as for urosepsis, to avoid pain, and to protect renal functions. This study investigated the effectiveness of intentional preoperative stenting (IPS) before ureteroscopy for large renal stones.
Materials and Methods
From April of 2010 to June of 2011, a total of 265 patients underwent ureteroscopic surgery. In these patients, we intended to insert 25 ureteral stents (IPS) before ureteroscopy for a large renal stone (stone burden>15mm). The 36 non-prestented matched controls (NPS) were used for comparison.
Results
The median stone burden was 29.4mm in the IPS group and 26.9mm in the NPS group. The median maximum stone size was 21mm in both groups. IPS significantly improves the stone free rate, defined as stones<2mm and<4mm, and not significant stone free rate. defined as 0mm. The median length of the operation was not significantly different, at 103 min (IPS) and 110 min (NPS).
Conclusions
The results show that IPS for ureteroscopy facilitates the stone free rate for large renal stones.

Clinical Study of Transurethral Lithotripsy with Holmium:Yag Laser and Extracorporeal Shock-Wave Lithotripsy for Upper Urinary Tract Stone
We analyzed the clinical outcome of transurethral lithotripsy (TUL) with the holmium:YAG laser and extracorporeal shock wave lithotripsy (ESWL) for upper urinary tract stone. Between July 2007 and April 2011, surgical treatment was undertaken for 844 patients with 1047 stones. TUL was performed in 367 patients (TUL group) and ESWL in 477 patients (ESWL group). In the TUL group, the number of stones according to location was 312 stones in the renal pelvis and/or calyx (R2), 40 in the ureteropelvic junction (R3), 101 in the proximal ureter (U1), 45 in the middle ureter (U2), and 63 in the distal ureter (U3). In the ESWL group, the number was 142 in the R2, 46 in the R3, 200 in the U1, 23 in the U2, and 75 in the U3. Success was defined as stone-free on plain radiograph and renal sonograph etc., with no hydronephrosis at 3 months after surgery. When an additional procedure was needed, the former procedure was defined as having failed. The success rates in the TUL group and the ESWL group were 78.8 % and 38.0 % in the R2, 92.5 % and 58.7 % in the R3, 95.0 % and 82.0 % in the U1, 97.8% and 82.6 % in the U2, and 95.2% and 82.7 % in the U3, respectively. TUL showed significantly excellent success rates for all upper urinary tract stones compared with ESWL. In conclusion, all upper urinary tract stones can be treated efficiently with TUL better than ESWL.
Changing Trends in the Indications for Ureteroscopic Lithotropsy at Wakayama Medical University
[Introduction] The 2002 Japanese Clinical Practice Guidelines (CPG) on Urolithiasis recommend ureteroscopy (URS) for stones in the middle and distal ureter. However, recent advances in flexible URS allow the treatment of stones located anywhere in the upper urinary tract. [Purpose] We evaluated changing trends in the indications for URS and clinical outcomes in the last 5 years. [Materials and Methods] A total of 105 patients underwent URS from 2007 to 2011. We compared the indications for URS and stone-free rate (SFR) before and after the increased application of flexible URS in 2009. SFR was defined as less than 4mm of residual stone burden assessed within 3 months after treatment. [Results] (1) Of the 33 patients before 2009, 11 (33.3%) were non-CPG-recommended cases (renal and proximal ureter), of which 54% and 27% were those with SWL-failure and impacted stone, respectively. SFR was 100% for CPG-recommended cases (middle and distal ureter) and 91% for non-CPG-recommended cases. (2) Non-CPG-recommended cases were increased up to 65.3% (47 of 72 patients) after 2009. Of these, cases with SWL-failure decreased to 21%, while those with large stone burden (≥ 2cm/multiple) increased up to 28%. SFR was 100% for CPG-recommended cases and 74% for non-CPG-recommended cases. All of the non-CPG-recommended cases with residual stones had lower pole calculi.[Conclusions] Increasing application of URS for non-CPG-recommended cases resulted in unfavorable SFR, especially in patients with lower pole calculi. Technical improvements and more appropriate indication criteria are required.
Clinical Outcome of Urinary Stone Disease in Children
INTRODUCTION AND OBJECTIVES: Urinary stone disease in children is rare and its rate is only about 1% in the total urinary stone disease. Metabolic disorders and anatomical alterations are frequently observed in pediatric patients. We retrospectively reviewed pediatric patients and analyzed about underlying disease, chemical analysis of stones.
METHOD: From January 1998 to June 2011, we retrospectively reviewed 27 cases of urinary stone disease in children. 19 were male and 8 were female, with a mean age of 6.9 years (range 0-15years).
RESULT: 25 patients were upper urinary tract stones and 2 patients were lower urinary tract stones. 11 patients (41%) were treated conservatively, and 16 patients (59%) underwent surgical treatment. Of these patients, 6 patients were treated with ESWL, 5 patients with PNL, 4 patients with TUL, and 2 patients with others. 20 patients were made an investigation into underlying disease. A cause for stone was identified in 12 patients. Metabolic disorders were found in 4 patients and anatomical alterations were found in 2 patients. Chemical analysis of stones was performed in 14 patients and it showed calcium oxalate in 64% of the cases.
CONCLISION: This present study reveal that urinary stone disease in children has underlying disease in many cases.
Clinical Evaluation of the Calculous Pyelonephritis
Objetive:Calculous pyelonephritis often occur serious state including sepsis and disseminated intravascular coagulopathy(DIC). We compared calculous pyelonephritis with non-calculous pyelonephritis, and evaluated risk factor for necessity of vasopressor and development of DIC.Patients and methods:The subjects were the patients with pyelonephritis who admitted in our department between 2006 and 2011. Pyelonephritis associated with operation and/or indwelling catheter was excluded. 66 patients had calculous pyelonephritis (Stone group), and 100 patients had non-calculous pyelonephritis (Non-stone group). Results:Mean age of patients with Stone group were significantly higher than those with Non-stone group (64 years vs. 55 years; p<0.01). Normalization of leukocytosis in peripheral blood after treatment in Stone group was significantly longer than those in Non-stone group (4.7 days vs. 3.5 days; p<0.01). In Stone group, 21 patients (32%) had the condition of vasopressor use and 9 patients (14%) had the development of DIC. In contrast, Only one patient (1%) had the condition of vasopressor use and none of patient (0%) had the development of DIC in Non-stone group. On multivariate analysis, calculosis, poor performance status and diabetes mellitus prevalence were significant predictive factor for necessity of vasopressor after the onset of pyelonephritis (p<0.01). In patients with calculous pyelonephritis, diabetes mellitus prevalence and need of drainage, including double-J ureteral stent or percutaneous nephrostomy, were significant risk factor for necessity of vasopressor (p<0.05).Conclusion:This study suggested that calculous pyelonephritis with diabetes mellitus and need of drainage might be high risk for hypotensive status.
Size Matters: EelectroConductive Technology (Sonolith Vision-Technomed) in Extracorporeal Shockwave Lithotripsy (EC-ESWL) of large renal stones
Introduction: The first line treatment for large renal stones>2cm is PCNL. We present our experience in Electroconductive technology ESWL(EC-ESWL) in a specific group of patients who is either unfit, with solitary kidney, had previous unsuccessful PCNL, or preferred ESWL. Materials and Methods: Our database of>700 treatments using the Sonolith Vision Lithotriptoridentified 32 patients with renal stones>2cm. Location, stone- free rate, ESWL sessions, and auxillary treatments are presented . We identified the reasons, and outcomes with ESWL as first line treatment.Results: 17 female:15 male, mean age 48.8. 24 preferred ESWL, 3 were considered unfit for PCNL, 3 previous unsuccessful PCNL and 2 with solitary kidney. Before treatment, 29 patients had JJ stent, 1 had nephrostomy, 2 had neither. All were free from significant complications.Average stone size: 23 mm (20-35 mm). 15 localised in renal pelvis, 6 lower calyx, 5 upper calyx, 4 PUJ, 2 partial staghorn. Complete fragmentation and clearance in 12 patients (37.5%). 9 were completely stone-free, 3 had clinically insignificant fragments. Median ESWL sessions: 3. Complete stone fragmentation but partial clearance of fragments>4mm in 20 patients (62.5%). Median ESWL sessions:3. 8 underwent PCNL for fragments>7mm, 7 ureteroscopic lithotripsy, 1 had combined PCNL/ureteroscopy, 3 asymptomatic stone fragment>4mm are observed conservatively, 1 patient moved away.Conclusions: EC-ESWL remains a safe initial option for large renal stones in this specific group of patients. Auxillary treatments for residual fragments must be planned and counselling provided before commencing ESWL treatment.
Does The Rate of Extracorporeal Shock Wave Delivery Affect Stone Fragmentation?
Introduction; There are a number of variables that can affect the shock efficiency of SWL, the objective is to eliminate the stones in the patients.Purpose; Slower shock wave delivery rate was believed to have better stone fragmentation success rate. So, we would like to compare the effect of previous fast shock wave delivery rate(120 shocks/min) and slow shock wave rate(60 shocks/min) on SWL success rate and patient's pain tolerance.Materials and Methods; Patients with previous untreated radiopaque renal stone sized from 5 mm to 20 mm were randomized to SWL at 60 or 120 shocks/min using Sonolith Praktis lithotripter(EDAP, France). Success rate was defined as stone free status or asymptomatic fragments less than 4 mm at 3 months after treatment. Pain tolerance was assessed by numeric rating scale score(0-10).Results; Of the patients 66 were randomized to 60 shocks/min and 68 were randomized to 120 shocks/min. The 2 groups were similar. The success rate was higher for 60 shockes/min compared to 120 shocks/min(66% vs 52%, p=0.036). For stone length<10mm, the success rate were 74% and 65%, respectively (p=0.292). For stone length>10 mm, the success rate were 54% and 39%, respectively(p=0.042). Median pain score were 3.8(2-5) at 60 shocks/min and 4.9(3-6) at 120 shocks/min, respectively(p=0.018).Conclusion; SWL treatment at 60 shocks/min yields better outcomes than at 120 shocks/min, particularly for renal stone length 10 mm or greater. Slower shock wave delivery rate may result less pain to the patient.
Results and Prospective Re-Audit of Mobile Shock Wave Lithotripsy: Where do we stand
Introduction:Our aim was to re-audit the results of our mobile lithotripsy service and compare our results with our previous results.Methods: Between March and September 2010, 126 patients were treated using Storz modulith SLX (elcctromagnetic) lithotripter. The prospective record of age, stone size and site, fragmentation, number of shock waves, outcome, complications, and, auxiliary procedure was made. Matched pair results of 50 patients were compared to the prospective results of 50 patients treated 8 years ago using the same machine(Ref).Results:The mean stone size was 7.5mm (3-16mm) and 45 patients (36%) had multiple stones. The stone position was in the upper calyx (n=16;13%), middle calyx (n=21;17%), lower calyx (n=63;50%), renal pelvis (n=9;7%), PUJ (n=8;6%) and upper ureter (n=9;7%). After a follow-up of 3 months, fifty-four (43%) were stone free although successful fragmentation was achieved in 64 (50%). Auxiliary procedure was required in 8 (6%) patients. In all, ten patients (8%) had minor complications with no major complications seen. When we compared the matched pair results of 50 patients for a mean stone size of 10.1 mm, the successful fragmentation and complications were similar to that of our previous results (42%, 10%)1.Conclusions: The treatment of urinary stones using mobile lithotripters is a feasible option. We are now treating more multiple and lower pole calyceal stones. Our results are comparable to our previous results from 8 years ago, although they are poorer than fixed site lithotripter. Reference:Ong E,et al.Prospective Non-Randomised comparison of efficacy using mobile lithotripters:Does energy source matter?J Endourol 2004;18(S1):A153.
The Feasibility of Shockwave Lithotripsy for the Treatment of over 1cm sized, Lower Calyceal Stones
There have been some controversies to choose the optimal treatment of over 1cm sized, lower pole renal calculi. Recently, percutaneous nephrolithotomy (PNL) has been introduced as a feasible option to manage over 1cm sized, lower calyceal stones instead of SWL.
The aim of this study was to compare the results of treatment of lower pole calculi between SWL and PNL group and to assess the feasibility of SWL for the management of over 1cm sized, lower calyceal stones.
We retrospectively reviewed the data who were undergone PNL or SWL due to over 1cm sized, lower calyceal stones. PNL group consisted of patients who underwent PNL to manage lower pole renal calculi under general anesthesia during the period 2008-2009. SWL group consisted of patients who were performed SWL to treat lower pole renal calculi from 2010 to 2011. We compared age, sex, stone size, co-morbidities, postoperative complications and additional interventions between two groups.
A total of 55 patients were enrolled in this study (PNL group 22, SWL group 33). Between PNL and SWL group, mean age (±SD) were 50.0 (±10.6) and 55.1 (±13.0) years, respectively (p=0.377). Mean stone size were 1.95 (±0.84) and 1.63 (±0.67) cm (p=0.298). There were no significant difference in the results of co-morbidities between two groups. However, three cases (3/22) of postoperative complications were reported in PNL group.
In our study, SWL was a safe, feasible treatment for over 1cm sized, lower calyceal stones.
Additive Expulsion Effect of Tamsulosin after Shock Wave Lithotripsy for Upper Ureteral Stones
Introductions : We evaluates if the administration of tamsulosin increases the efficacy of extracorporeal shock wave lithotripsy (ESWL) in the patients with upper ureteral stones and if this decreased the use of analgesic drugs after the procedure.Materials and Methods : A total of 45 patients with stones 6-12mm in size that were located in the upper ureter were enrolled. The patients were randomly divided into two groups. Group 1 (n=23) received 3 times a day oral 20mg caroverine (spasmolytic drug). Group 2 (n=22) received one time a day oral 0.2mg tamsulosin. All the patients received oral treatment for 14 days. Both groups were allowed to use 30mg ketorolac trimethamine intramuscular injections on demand. The endpoint of the study was the stone expulsion rate, the use of analgesics and the drug adverse effects during treatment.Results : The average stone size was 7.9±2.79mm for group 1 and 8.2±3.14mm for group 2. No statistical difference between the two groups was found for the stone size, age and gender distribution. The expulsion rate was significantly higher in group 2 (90.9%) compared with group 1 (65.2%) (p=0.038). The average number of pain control injections was 0.78 for group 1 and 0.23 for group 2, and there was a statistically significant difference between the two groups (p=0.042).Conclusions : The use of tamsulosin proved to be effective and safe, as demonstrated by the increased stone expulsion rate and the lesser need for pain control than that when using just a spasmolytic drug for ESWL of upper ureter stones.
More Efficient and Safer Extracorporeal Shock Wave Lithotripsy (ESWL) using Dornier Lithotripter S II. -Comparison with our Conventional Equipments-
<Introduction and Objective>In 1984, Sanjukai hospital started the very first case of shock wave lithotripsy (SWL) in Japan as a minimal invasive treatment. We retrospectively reviewed the treatment outcomes of SWL using Dornier HM3 (HM3), Philips Litho Diagnost M (LDM), and Dornier Lithotripter S II (S II), and analyzed recent efficiencies and adverse effects of SWL using the new S II compared with our historical controls using LDM and HM3.<Methods>Among the 17,529 SWL procedures treated since 1984, we analyzed the 7,198 procedures performed after 2000. In these patients, the former 5,997 (LDM period) were treated with LDM (76.9%), HM3 (7.8%), and a combination of both (15.3%), and in the latter 1,201 (S II period), 99.6 % were completed SWL using only SII. For further analysis, the treatment efficiencies and adverse effects were assessed. Comparing these periods (LDM: 2007-2008 and S II: 2009-2010), they had similar backgrounds; mean age, position and number of stones. However, stone discharge rates within 1 month were 16%:40% (p<0.05). Pain and fever-free rates were 78%:96% (p<0.05). Moreover, as we assessed the necessities of repeated treatments for these stone disintegrations, more patients in LDM period needed repeated SWL procedures than in S II period (24%:19%). LDM and HM3 needed to compensate with second procedure. Recently, we are using only S II for SWL procedure because it was shown to have superior stone disintegration and fewer complications. Since the introduction of S II, SWL became safer and more efficient treatment.
Department of Urology, Faculty of Medicine, Yamagata University, Yamagata, Japan
Comparison of the Clinical Outcomes According to Slowing the rate of Shock Wave,for Urinary Tract Stone
PURPOSE: To determine the efficiency of slow delivery rate of shockwaves(SW) on stone fragmentation and treatment outcomes in patients with urinary tract stone.PATIENTS AND METHOD: Using the Dornier Lithotripter D, we treated 232 sessions at a fast delivery rate (80 SW/min, between October 2007 and September 2009), 101 sessions at a slow delivery rate (60 SW/min, between October 2009 and August 2010).Clinical success was defined as stone-free status or asymptomatic insignificant residual fragments of<4 mm, judged from next day's KUB. RESULT: The two groups (fast group vs. slow group) were comparable in terms of sex, average age(54years vs. 55years), mean stone size(8.4mm vs. 9.9mm) and stone location(U1:172 vs. 74,U2: 17 vs.7 ,U3 :43vs.20).Clinical success rate of slow rate group was higher than fast rate group(20.2% vs. 29.7%).CONCLUSION: Slowing the SW delivery rate to 60SW/min may improve treatment efficiency.
A case of the Purulent Spondylitis that Occurred after ESWL for Renal Calculus.
Extracorporeal shock wave lithotripsy (ESWL) is a safe and effective therapy, but sometimes causes serious complications. We report our experience with the case of purulent spondylitis that occurred after ESWL. The case was a 65 years old man. He had left renal calculus with MRSA infection. We started ESWL after insertion of left ureteral stent. The patient showed fever after ESWL, but the fever was improved by antimicrobial therapy. However, the patient was re-hospitalized because of recurrent high fever after three weeks of the initial ESWL. We diagnosed as pyelonephritis caused by MRSA and treated him by the antibiotics treatment. The fever was settled smoothly once, but high fever and the right lumbago were recurred after six weeks of the initial ESWL. At first, we regarded the right lumbago and the fever as a symptom with right pyelonephritis. But the right lumbago and the fever were resistant to treatment, and MRSA was detected from blood cultures. By CT and MR imaging, the cause of symptoms was diagnosed as his right iliopsoas muscle abscess and purulent spondylitis. The symptoms were gradually relieved after having started the dosage of Linezolid, but needed 7-month hospitalizing by healing in total. Purulent spondylitis is a serious infection to need a long term for treatment. The purulent spondylitis seems to be rare complications of the ESWL. But it is serious complications to require a long term for treatment when it occurs once, so it is necessary to pay attention.
Retrograde Nephrostomy Access and Tubeless Percutaneous Nephrolithotomy: is this the way to go?
Abstract Withdrawn
Radiofrequency Ablation of Renal Tumor : Our Experience
Department of Urology, the first affiliated hospital of Guangzhou Medical College, Guangzhou, China, 2Guangdong Key Laboratory of Urology, Guangdong, China
Introsuction and objectives: Subcostal puncture was preferred in order to avoid complications such as hydropneumothorax or laceration of lung. However, under unfavorable conditions, such as unusual body build, high position of a kidney, stone in the upper ureter, the optimal access was a supra 11th rib approach. The purpose of this study was to investigate the treatment of hydropneumothorax following percutaneous nephrolithotomy. Material and methods: 7 cases who received supracostal puncture PCNL had a postoperative hydropneumothorax. All the patients had a definite diagnosis of hydrothorax or pneumothorax by a X-ray chest examination and/or ultrasonography, a prompt treatment was received. Results: Of 7 cases, 2 cases had a closed thoracic drainage,2 case had a suction under B-ultrasonography guidacnce, 1 case for hydrothorax combinated with a ureteric steinstrasse received a ureteroscopic lithotripsy, 2 case with a mild pneumothorax had a conserve observation, respectively. All cases cured successfully, in a follow up of 6-12 months, the X ray chest examination showed no special sign.Conclusion: Hydropneumothorax following MPCNL could be cured after a prompt treatment, and this complication could be avoided under well preparation and careful manipulation.
Prevention of Major Complications Following Percutaneous Nephrolithotomy in 1000 Patient with Renal Calculi
Introduction: The frequency of major complications after pcnl is rare but when happen, most of them are disasters. In this study we discuss our schemes to reduce these disasters.Methods and materials: Proper patient selection, preoperative imaging for planning the operation, hospitalization of patient a day before operation, mechanical bowl preparation, adequate antibiotic prophylaxis and therapy, ultrasonogrphic evaluation of flank area preoperatively, manipulation of the collecting system only under fluoroscopic or endoscopic control, use of a continuous flow system, and use of normal saline as irrigant fluid, are necessary to prevent percutaneous nephrolithotomy complications. Results: we retrospectively analyzed the data of 1000 patients who had under gone PCNL for removal of renal calculi at our hospital between 2001and 2010. Mean age of patients was 46(6-78), mean stone size was 34+_8.6 cm. Stone free rate was 76.95. Transfusion rate was 4.5%, post operative diarrhea which suspect colon perforation was seen in 2 patient but we cannot showed colon injury with radiological contrast study.2 patient had delayed hemorrhage due to arteriovenous fistula which controlled by selective angioiembolization. One patient had intraperitoneal extravasations. One of our patient expired due to pulmonary embolism. We had not any main vascular, liver or splenic injury. We never need change to open surgery in our patients. Conclusion: with some simple and planed schemes the endourologist can reduce severe complication of PCNL and when it occurs because of preoperative preparations he can control them easer than unplanned situations.
Feasibility and Safety of Total Extraperitoneal Inguinal Hernia Repair after Previous Lower Abdominal Surgery: A Case-Control Study
Objective: To evaluate the feasibility and safety of totally extraperitoneal (TEP) endoscopic hernia surgery after previous lower abdominal surgery, which may preclude preperitoneal dissection. Methods: Between January 2008 and December 2010 all 331 consecutive patients undergoing TEP surgery were included in a prospective cohort study. This case-control study includes a study group and a comparison group. The study group consisted of 23 patients with a history of previous lower abdominal surgery before undergoing TEP endoscopic hernia repair. We randomly selected 46 patients (two for every patient in study group) matched with the study cohort in terms of age, gender and laterality of inguinal hernia. Peri-operative data were obtained for all patients including demographic data, operation time, length of hospital stay, narcotic dose, conversions and complications.Results: A total of 69 patients with inguinal hernias underwent TEP surgery: 23 patients with previous abdominal surgery (study group) and 46 patients without (control group). No conversions were necessary in the control group, but 1 cases (4.4%) were converted to transabdominal preperitoneal hernia repair (TAPP) in the study group (P=0.33). Peritoneal injury requiring intracorporeal repair were encountered in six and eight patients in study and control groups respectively (p=0.53). No differences were observed between groups regarding operative times, analgesic use, hospital stay, return to daily activities and postoperative complications. Conclusions: TEP hernia repair for patients with previous lower abdominal surgery can be safely performed by experienced hands, with operative outcomes comparable to those who do not have previous history of lower abdominal surgery.
Clinical Analysis of the Treatment of Solitary Kidney Calculi with Minimally Invasive Percutaneous Holmium Laser Lithotripsy
Clinical Study of Spontaneous Rupture of the Upper Urinary Tract
Purpose:To clarify the clinical characteristics of patients with spontaneous rupture of the urinary tract.
Methods:We retrospectively analyzed a series of such patients and reviewed documented cases. Between January 2005 and December 2010, cases of 5 patients with spontaneous rupture of the upper urinary tract were reviewed.
Results:These patients comprised 3 men and 2 women (age range, 54 - 85 years). The chief complaint was flank pain in all patients. Of the 5 patients, 3 had ureteral stones, 1 had bladder tumor and 1 had cancerous peritonitis. Spontaneous rupture was diagnosed by abdominal computed tomography in 4 patients and by intravenous pyelography in 1. Because extravasation was observed around the kidney and/or upper ureter in the 5 patients of this study, prompt drainage was required. This included ureteral stent placement in 4 patients and percutaneous nephrostomy in 1. In all patients, pain disappeared without any complications, such as subsequent high fever. And the catheter was removed in the patients without malignancy. Spontaneous rupture of the upper urinary tract was mostly caused by renal pelvic or ureteral stones. Documented reports describe that approximately 10% of spontaneous ruptures are caused by urological malignancy, mostly involving the renal pelvis or ureter, bladder tumors are rare.
Conclusions:Eemergency treatment by ureteral stenting or percutaneous nephrostomy would be preferred with a few exceptions. These treatments relieve pain promptly and prevent the development of urinary tract infection in patients with spontaneous rupture of the upper urinary tract.
Endoscopic Urology Department, Russian Medical Academy of Postgraduate Education, Moscow, Russia
Percutaneous Management of Renal Pelvis of a Solitary Kidney Transitional Cell Carcinoma with Instillation of Medicine into the Renal Pelvis
Objective To study endourological management of transitional cell carcinoma of the upper urinary tract and the solution of the instillation of medicine into the renal pelvis. Methods A 69-year-old female with renal pelvis of a solitary kidney transitional cell carcinoma was reported. The patient had a left nephroureterectomy with removal of a cuff of bladder surrounding the ipsilateral ureteral orifice 1 year ago and 3-day's interval anodynia gross hematuria before her admission. The RP(Fig1) and CT(Fig2) showed that there was a 1.0*1.0cm tumor in the right renal pelvis. The PubMed and CBM databases were searched for related articles, and their clinical data were reviewed. Results Resection the tumor with percutaneous management. Postoperative pathology found transitional cell carcinoma grade 2. Instillation of hydroxycamptothecin into the renal pelvis was performed following the surgery. Follow-up of 14 months showed no recurrence(Fig3-4). Conclusions In the situations of low grade and low stage lesions, regional treatment options using an endoscopic approach with instillation of medicine into the renal pelvis have a good therapeutic effect, especially in the situations of tumor in the solitary unit bilateral synchronous tumors, renal insufficiency, this method could be the best way.
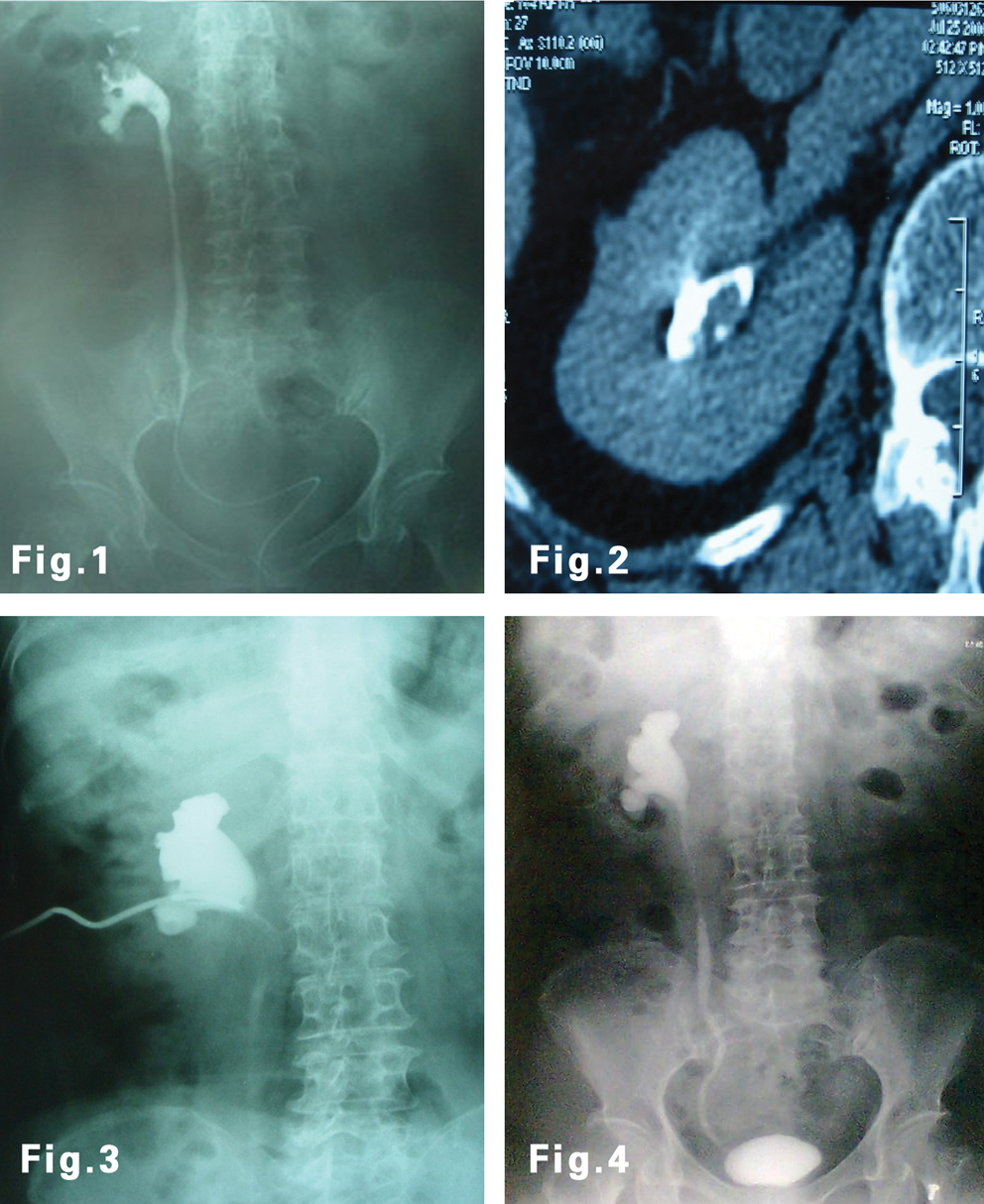
Urological Cancer Outcomes Centre
Objective: Prostate cancer is the most common male urological malignancy in the developed countries. With our ageing population, prostate cancer will continue to be one of the major healthcare concerns because of the increasing incidence of prostate cancer with advancing age. We studied whether local treatments of the primary prostate cancer give palliative benefit to men who later develop castrate resistant prostate cancer (CRPC). Local treatments of primary prostate cancer are defined as radical retro-pubic prostatectomy (RRP) or external beam radiation (XRT). Methods: We reviewed the patient records in 5 different hospitals in Sydney, Australia and identified 263 men who have CRPC. Eligible patients were men who had progressive disease during androgen deprivation therapy with castrate levels of testosterone. Clinical and pathological data were reviewed and evaluated in Chi-square and relative risk to determine the relationship between previous local prostate treatment and complications secondary to local disease. The end point was complications and morbidity attributed to cancer progression locally (from the prostate). Results: Primary prostatic treatment by either RRP or XRT significantly reduces the incidence of local complications compared to no primary treatment (31.5% v 54.6% p<0.001). In addition, RRP demonstrated a significantly lower level of local complications compared to XRT ( 17.8% vs 46.7% p=0.003). The most common local complications were bladder outlet obstruction (34.2%) and ureteric obstruction (15.2%).Conclusion: This retrospective analysis supports the hypothesis that primary local prostatic treatment gives palliative benefit to men who later develop CRPC. RRP gives the greatest reduction in local complications.
Department of Urology, Osaka City University Graduate School of Medicine, Osaka, Japan
51-year old female visited our hospital complaining of microhematuria and proteinuria in February 2010. She had past history of SWL for bilateral renal stone 15 years ago, but many residual stones existed in renal parenchyma. In September 2010, she got a fever of 39 degrees centigrade. Because CT revealed 5.8-cm abscess in right kidney, she was diagnosed sepsis by renal abscess. She was successfully treated by drainage of renal abscess and antibiotics. However, renal abscess was recurred 4 times for 4 months and we considered right nephrectomy to control renal abscess. Her split renal function examination showed right renal function was better than left renal function (R: 34 ml/min, L: 22 ml/min) and she desired treatment other than nephrectomy.Under approval of Institutional Review Board, we applied radiofrequency ablation (RFA) to treat renal abscess. In February 2011, we performed RFA for renal abscess without any complications under local anesthesia. Five months after RFA, renal abscess was remained but shrank with no clinical symptoms and her renal function was maintained. Japanese guideline for renal tumor shows as RFA can be alternative therapy indicated for small tumor and its complication rate is low, but renal abscess after RFA has been reported. However RFA as a treatment for renal abscess has not reported yet. This is first report of intractable renal abscess successfully treated by RFA.
Removal of Asymptomatic Ipsilateral Renal Stones Following Rigid Ureteroscopy for Ureteral Stones
Objective: To evaluate the feasibility and outcome of rigid ureteroscopic removal of asymptomatic reachable renal stone(s) following rigid ureteroscopy for ureteral stones. Methods and Materials: 110 patients underwent rigid ureteroscopy for removal of ureteral stones. All had asymptomatic renal stone(s) on the same side, which were then removed using rigid ureteroscopy. The renal stones were either removed intact with a grasp or fragmented with the pneumatic lithotripsy to small pieces, with grasp removal of larger fragments. The size of stones, added time for renal ureteroscopy and intraoperative and postoperative complications were recorded. Follow-up at 1 month included a plain abdominal film and renal ultrasonography.Results: 110 renal stones with a mean size of 8 mm were treated. 60 patients had stone on the right side, and 50 had stones on the left. The mean added operative time 7minutes. Stones were removed intact in 70 patients and fragmented in 40 patients. One-month follow-up confirmed none of patients had new onset stones or hydronephrosis. Conclusions: Removal of asymptomatic reachable renal stones at the time of rigid ureteroscopy for ureteral stones appears safe and effective and requires little additional operative time.
Extra-Corporeal Shock Wave Lithotripsy (ESWL) Versus Ureteroscopic Management for Ureteric Calculi
Background Urinary stones frequently cause renal colic and if left untreated can cause obstructive uropathy. Shock Wave Lithotripsy (SWL) and ureteroscopy are the two most commonly offered for the management of calculi. However, there is no evidence to suggest which treatment option is more successful. Therefor a systematic review was aimed to compare the two modalities.Search methods We searched the Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, CINAHL, Clinicaltrials.gov, Google Scholar, reference lists of articles and abstracts from conference proceedings without language restriction.Selection criteria RCTs comparing ESWL with ureteroscopic retrieval of ureteric stones were included. Participants were adults with ureteric stones requiring intervention. Published and unpublished sources were considered.Results Seven RCTs (1205 patients) were included. The stone-free rates were lower in the ESWL group (P=0.01; RR 0.84 95% CI 0.73 to 0.96). The retreatment rates were lower in the ureteroscopy group (P<0.00001; RR 6.18 95% CI 3.68 to 10.38) however the need for auxiliary treatment were lower in the ESWL group (P=0.003; RR 0.43 95% CI 0.25 to 0.74). The rate of complications was lower in the ESWL group (P=0.01; RR 0.54 95% CI 0.33 to 0.88). Length of hospital stay was less for ESWL treatment (P<0.00001; MD −2.55 95% CI −3.24 to −1.86). Conclusions Ureteroscopic removal of ureteral stones achieves a higher stone-free state in addition to a lower retreatment rate, but with a higher complication rate and a longer hospital stay.
The Selection of Surgical Approach in the Treatment of Restenosis after Ureteropelvic Junction Stricture Surgery
Department of Urology, Graduate School of Medical Sciences, Kyushu University
Introduction A new concept for insertion of a ureteral access sheath (UAS) has recently been presented allowing transforming the working guide wire into a safety guidewire. The first evaluation in Europe, which was presented at 28th WCE Chicago, demonstrated interest for endoscopic procedures.Purpose The current multicentre evaluation in Japan aimed to present ureteral insertion rates with this new technique and compare with the result in Europe. Material and Methods The UAS, Re-Trace (12/14Fr, Coloplast), is designed to allow the disengagement in one step of the working guidewire which then lies besides the UAS in the ureter and becomes automatically a safety guidewire. Three institutions in Japan have participated in a prospective evaluation of this UAS. The outcome was the placement of this UAS. Gender and pre-stenting were recorded. Insertion rates were compared with that in Europe.Results 45 UASs were used in 25 male and 20 female patients. 26.7% of ureters were pre-stented. The Re-Trace insertion rates were 88.0% in male and 80.0% in female. The overall insertion rates in Japan and Europe were 84.4% and 84.3%, respectively. A tendency of easier insertion was found in pre-stented (100%) versus non pre-stented ureters (78.8%). The guidewire disengagement was possible in 100% of cases. These results showed similar trend to Europe data.Conclusions Re-Trace UAS showed good overall insertion rates. Variations related to pre-stenting corresponded to the general expectations. This evaluation confirm the interest of this concept of guidewire disengagement: a single wire automatically switches from working to safety role.
Clinical Analysis of Treatment of Distal Ureteral Stricture by Ureteroscope Holmium Laser Endouretertomy
Application of Ureteroscopy in the Treatment of Iatrogenic Ureteral Injury
Correlation between Pre-Operative Ureteral Stents, Intra-Operative Renal Pelvic Pressures, and Post-Operative pain in Patients Undergoing Flexible Ureteroscopy and Laser Lithotripsy
Introduction:Ureteric stenting has been advocated prior to ureteroscopy in order to facilitate stone-free rates and reduce complications. However, its effect on post-operative pain is unknown. Increased renal-pelvic pressure is considered to be a significant cause of post-operative pain in patients undergoing flexible ureteroscopy and laser lithotripsy. However, clinical data on the topic are few. Purpose:This study aims to analyse the correlation between presence of pre-operative ureteral stents, renal pelvic pressures, and post-operative pain-scores in patients undergoing flexible ureteroscopy for renal calculi. Methods:We prospectively collected data on 27 patients undergoing flexible ureteroscopy and Holmium:YAG laser lithotripsy for renal stones. Intra-renal pressure was measured with transducers at the beginning and end of the procedure. Post-operative pain was assessed using a visual-analogue scale (0-10). Correlation coefficients were calculated between the presence of pre-operative ureteric stent, intra-renal pressure, energy used and post-operative pain. Results:21 patients had a pre-operative stent with a mean initial pelvic pressure of 16.4cmH2O (4- 44). Six patients did not have a ureteric stent pre-operatively, although the mean initial pelvic pressure was similar at 17.3cmH2O (4- 40). There was no correlation between the presence of a pre-operative ureteric stent (r=− 0.08), intra-operative initial (r=− 0.03) or final pelvic pressure (r=0.004) and post-operative pain score. Conclusion:While it may reduce other complications, routine placement of ureteric stents prior to ureteroscopy does not seem to affect post-operative pain. The explanation may be the absence of correlation between presence of stent and intra-operative renal pelvic pressure.
Does Endoscopic Management of Upper Urinary Tract Transitional Cell Carcinoma Increase the Incidence of Metachronus Bladder Transitional Cell Carcinoma?
Objective:To evaluate and compare the incidence of metachronous TCC of bladder following ablative and nephron sparing (ureteroscopic) treatment of upper unitary tract TCC . Patients and methods:We evaluated the data of all patients diagnosed and managed with upper tract TCC over 5 years (2004 to 2009) at our institution. We analyzed demographic, clinical and pathological data to determine incidence of bladder tumours following treatment of UTCC in the two groups. Results:There were 56 patients who underwent curative treatment for UTCC during this period [M=38 (68%) F=18 (32%)]. Two thirds (n=37) had primary lesion in the kidney with the rest 19 (n=19) had it in ureter. Forty two patients underwent nephro-ureterectomy while 14 were initially managed by ureteroscopic ablation. Of these, 12 patients with superficial disease who continued with ureteroscopic treatment were (Tumour Gr 1=2 & Gr 2=10) compared with neproureterectomy group (N=15) having similar histological disease (Gr1=2 & Gr2=13). Mean tumor size was 3.75 cm (SD±1.45) in nephro-ureterectomy group and 2.2cm (SD±0.91) in endoscopic group. Mean follow-up period was 38 months (SD±25.0) in nephro-ureterectomy group and 29 months (SD±14.86) in endoscopic group. Five (41%) patients in endoscopic group (17 recurrences), had metachronous bladder TCC recurrences as compared to six patients (40%) in nephro-ureterectomy group (17 recurrences) which was not statistically significant (p value>0.5). Conclusion:In our experience, nephron sparing management of UTCC in select group (superficial disease) of patients is not associated with increased incidence of recurrent bladder TCC. Study with larger numbers would help to substantiate our findings.
Tenon Hospital, Paris
Introduction & Objectives: Retrograde intra-renal surgery is now a standard approach for the treatment of renal stones. Although its morbidity seems very low, there is few specifical data upon hemorragic complications. The aim of this study is to collect data on hemorragic complications after retrograde intra renal surgery.Material & Methods: We reviewed files from patients with hemorragic complication after retrograde intra-renal surgery and collected data such as operative indication and duration, consequences, and existence of a blood coagulation disorder.Results: From 2001 to 2009, more than 2000 RIRS were performed in our 5 centers. We found 13 cases (frequency lower than 0.65%) of hemorragic complication listed as follows : 1 subcapsular hematoma, 5 retroperitoneal hematomas and 7 upper urinary tract clotting. Diagnosis was made before the third post-operative day in 6 patients and within the month for the rest. As a consequence, nephrectomy was performed in 4 patients and one patient was temporary contra-indicated for hepatic transplantation. Mean opeartive time was 81 minutes (25-120). Among patients, there were one with haemophilia, one with acquired blood coagulation disorder, two treated with anti-agregants, and one with coumadin.Conclusions: Hemorragic complication after RIRS are rare but can be severe.
Prediction of Patients Suitable for day case Ureteroscopy: Position of Stone is Important
Introduction:Stone disease makes up a large proportion of elective urological work. We offer a 23 hour stay facility, but are moving to a split site inpatient and fully day-case stone facility. We wish to predict who would be suitable for the day-case unit. Patients and Methods:We collected prospectively, via a database, data on all ureteroscopies (flexible and semi-rigid) performed by a single surgeon between March 2010-April 2011. We collected admission data, patient demographics, ASA grade, stone burden, location and operative outcome. Results:Complete data was available for 108 operations from 89 individual patients. Average age and ASA grade were 54 years and 2.0 respectively. 82% were performed for stone disease whilst 18% were diagnostic. Average stone burden was 9.2 mm, 53%, being renal, 19% proximal ureter, 4% mid-ureter and 24% distal ureter (including vesico-ureteric junction (VUJ)). 32% of patients were discharged the same day, 51% the next day and 17% stayed for 2 nights or more. Subgroup analysis revealed no statistical difference in age, ASA, stone size, pre or post-operative stenting. A significant difference (p-value 0.05) was seen when comparing discharge times of patients with renal stones (average 1.3 nights) versus proximal stones (0.7 nights). This was not seen when comparing renal to distal ureteric/VUJ stones. Conclusion:It appears that proximal stones have a shorter length of stay when compared to either renal or VUJ stones and a preference should be made towards these patients when selecting for a day-case procedure. VUJ stones should not be underestimated.
Clinical outcome of Flexible Transurethral Lithotripsy for Renal Calculi
-INTRODUCTION AND OBJECTIVES: Gold standard of treatment for renal calculi is ESWL or PNL. However, since new flexible ureterorenoscope and Ho:YAG laser have been invented, flexible transurethral lithotripsy (fTUL) can be performed safely and effectively.
Successful Management using Antegrade Ureteroscopy of a Ureteral Stone Patient after Urinary Diversion with Sigmoid Colon (Reddy method).
A 63-year-old man who received total cystectomy with sigmoid colon neobladder due to bladder and prostate cancer visited our hospital presening high fever and right CVA pain. We diagnosed an obstructive pyelonephritis due to ureteral stones. First of all we tried to drainage of the right kidney by retrograde catheterization, but failed because we could not find out the right ureteral orifice. Next we successfully performed a percutaneous nephrostomy and chemotherapy with antibiotics for several days. After he recovered we performed percutaneous nephro-ureterolithotripsy as follows.1; inserted a guide wire from the PNS catheter to ureter. 2; removed the PNS catheter and inserted a balloon dilator and a sheath. 3; performed nephrolithotripsy by a rigid nephroscope. 4; inserted a ureteral access sheath and fiber ureteroscopic lithotripsy by a basket catheter. 5; after ureteroscopy throughout a right ureter to ensure stone free, we inserted a double J catheter by antegrade.Discussion: It is difficult to find out ureteral orifices in the neobladder, especially in the case of obstructive disease because unable to use an indigocarmin intra venous injection. On the other hand, it is easy to make percutaneous nephrostomy in the case of hydronephrosis and reach to the obstructive portion because of upper urinary hydroureter. We easily performed fiber ureteroscopy by antegrade and smoothly removed a ureteral stone by a basket catheter using the ureteral access sheath. We recommend using the ureteral access sheath not only retrograde fiber ureteroscopy but also antegrade approach.
Transurethral Lithotripsy using Flexible Ureterorenoscope for Renal Staghorn Calculi
A total of 11 patient with renal staghorn calculi underwent transurethral lithotripsy using flexible ureterorenoscope (f-TUL). A flexible ureterorenoscope was successfully introduced up to the stone in all patients. All of the case received 1 to 6 sessions of f-TUL for complete fragmentation using Holmium:YAG laser device without severe complication:2 cases received a single session,4 cases received two sessions,3 cases received three sessions,the remaining 2 cases received over four sesseions. After the stones were removed as much as possible,a double J ureteral stent was inserted and the patients was discharged. In conclusion,f-TUL is safe and suitable endoscopic surgery for renal staghorn calculi not only for small renal and ureteral stone.
Use of a Ureteroscopic Stone Entrapment device(Accordion) to prevent retrograde stone migraton during ureteral laser lithotripsy
IntroductionRetrograde stone migration during ureteroscopic lithotripsy occurs in 5% to 40% of ureteral stone cases. This migration increases morbidity and the need for auxiliary procedures. The Accordion stone management device is a hydrophilic microcatheter-based tool that blocks stone migration. To determine the incidence of calculus retropulsion and additional procedures after ureteroscopy with intracorporeal laser lithotripsy while using the Accordion.Materials and Methods We used this device during ureteroscopic laser lithotripsy in 8 patients to prevent retrograde migration of stone fragments. Post-operative imaging was abdominal plain radiography or computed tomography next day of the surgery.ResultsThe Accordion was successfully placed in all 8 cases via ureteroscopy. The device is easily inserted and deployed, preventing retrograde stone fragment migration in all patients. Retrograde fluoroscopy revealed complete prevention of reflux in 4 patients and a little reflux in 2 patients. Postoperatively one patient had a urinary infection. No patient required auxiliary procedures.ConclusionsThe Accordion minimized stone retropulsion during ureteroscopic laser lithotripsy. The Accordion has the potential to increase the success rate, decrease secondary procedures for migrated stones, and shorten operative times.
Investigation into Indications for Ureteroscopy in Detection of Upper Urinary Tract Carcinoma
<Background> Recently, ureteroscopy has become a essential step for diagnosis in patients with upper urinary tract carcinoma. However, the certain consensus for indications of ureteroscopy has not been fixed yet. We investigated into the indication for ureteroscopy based on urine cytology and radiographic findings in detection of upper urinary tract carcinoma.<Patients and Methods>In a retrospective, 56 patients (34 men and 22 women) with a mean age of 65.4 years (range, 15-87 years) undergoing diagnostic ureteroscopy were evaluated, in the past 10 years in our institution. All patients were divided into three subgroups based on voided urine cytology and preoperative radiographic findings, group A (n=15); positive cytology and positive image, group B (n=7) ; positive cytology and negative image, group C (n=34) ; negative cytology and positive or negative image. Ureteroscopic findings including histology were compared with urine cytology and radiographic findings. <Results> All patients of group A had been revealed to be carcinoma. In group B, two revealed carcinoma, however, the remaining five had not been detected to be carcinoma. Four of the five people had history of bladder tumor, one had no history. In group C, nine patients (26.5%) had been detected to be carcinoma. <Conclusions> Ureteroscopy is essential for detecting upper urinary tract carcinoma with negative voiding cytology, however, ureteroscopy is redundant for patients with positive cytology and radiographic findings.
Ureteroscopic Surveillance for Urothelial Carcinoma of the Upper Urinary Tract Using Flexible Uretero-Reno Videoscope With NBI
We previously reported that endoscopic treatment of small, localized, low-grade tumors of the upper urinary tract (UUT) was a safe and feasible alternative to nephroureterectomy in selected patients (Int J Urol 13: 1-6, 2006). The endoscopic treatment of UUT tumors needs a high quality of endoscopic exploration in order to visualize all the existing tumors. The conventional flexible uretero-renoscope relays the image of an object to a CCD camera via fiber-optics and cannot provide a clear image. A new digital flexible video uretero-renoscope (URF-V: Olympus, Japan) has a CCD image sensor at the distal end. It is compatible with the Narrow Band Imaging (NBI) technology which enables enhanced visualization of the capillary network of mucosal surface. We report a benefit used URF-V for the surveillance after endoscopic treatment of UUT tumors. Patient was followed by ureteroscopic surveillance at 3- to 6-month intervals during 125 months after initial treatment. He received 16 ureteroscopic surveillance procedures, and 4 recurrences were successfully treated. Now, he remained alive with no signs indicative of disease.The image of URF-V is about three times larger than that of conventional fiberscope (URF-P5), making higher resolution image quality and enhancing observation. Regarding tumor observation with NBI technology, we could clearly recognize fine capillary patterns of the tumor. NBI was also useful for determination whether there was residual tumor after vaporization by laser.In conclusion, flexible uretero-renoscopy in UUT tumor was highly improved by digital technology providing high resolution image. NBI was useful for the surveillance after endoscopic treatment.
Flexible Ureteroscopic Treatment for Renal and Upper Ureteral Stones
Purpose: Despite new designs with increased deflection and smaller calibers, durability of new flexible ureteroscopes has not been compromised. The advantages of improved imaging system by videoscopes are high resolution and quality of images. We report our experience with flexible ureteroscopy in the management of renal and upper ureteral stones. Patients and Methods: We retrospectively analyzed the hospital records of 158 patients who underwent flexible ureteroscopy for renal and upper ureteral stones from January 1995 to December 2010. Lithotripsy was performed with five different flexible ureteroscopes (Storz 11274AA, Olympus URF-P2, URF-P3, URF-P5 and URF-V). The success rate was defined as the absence of any stones in the kidney and ureter or residual stone fragments less than 2mm. All patients underwent IVU or CT within 3 months after the last treatment. Results: The treatment for intrarenal stones was performed 21% for the 11274AA, 26% for the URF-P2, 27% for the P3, 53% for the P5 and 56% for the V (P=0.0008), respectively. Overall success rate at 3 months after treatment was 93% for the 11274AA, P2 and P3, 92% for the P5 and 88% for the V (P=0.8386), respectively. Conclusion: We challenge to treat the lower pole calculi aggressively after induction of URF-P5. Instead of increasing to treatment of lower pole calculi, success rate remains over 88%. Both technological advances of ureteroscope design with increased deflection and smaller calibers and technical advances of the operators make this satisfactory result.
Experience of Flexible Ureteroscopy with Holminium Laser for Upper Urinary Tract Calculus
Purpose: We investigated the effect of treatments with using flexible ureteroscopy(F-URS) with Holminium Laser for upper urinary tract calculus in our hospital.Materials : F-URS was performed on 70 patients, male 51 and female 19 with upper urinary tract calculus from February 2008 to April 2011. Median age is 63 years old. The median stone size was 17mm.The location was R2 in 30 cases, R3 in 19 cases and U1 in 21 cases. Results: The median operation time was 92 minutes. In operations, stones of 17 cases were completely crushed, 50 cases were partially crushed, and 3 cases were failed. There were no complications during these operations. However acute pyelonephritis in 5 cases (include sepsis in 3 cases), the stone street in 5 cases , and ureteral stricture in 3 cases, those symptoms were not serious. SWL was performed on 46 cases after F-URS. The median stone size was 20mm and the location was R2 in 24 cases, R3 in 12 cases and U1 in 10 cases. The median SWL frequency was 3 times. One month after treatment, The stone-free rate was 57% (38/67patients). 23 patients had residual fragment of sand state. 5 patients had residual fragment of less than 4 mm and One was more.Conclusions:We thought that even on comparatively large calculus, the use of F-URS and supplemental SWL , can get minimally invasive treatment and good outcome. We will add more cases and report at the congress.
Flexible Ureteroscopy for Renal Stone Larger than 2 cm
Holmium YAG Laser Ureteroscopic Nephrolithotripsy of large (greater than 4 cm) Renal Calculi
Purpose:The gold standard for treatment of large and complex renal stones is percutaneous nephrolithotomy (PCNL). However, in patients with significant comorbididties, this option may be suboptimal. We reviewed our experiences with ureterorenoscopy and Holmium laser lithotripsy (UL) for the primary management of large and complex intrarenal calculi.material and method:A total of 12 patients with 13 branched renal calculi ranging from 40 to 90 mm (mean 56) underwent staged ureteroscopic nephrolithotripsy monotherapyresult:Mobile stone-free status was achieved in 3 of 13 renal units with a mean of 2.6 stages and efficacy status (stone volume<5mm) was achieved in 3of 13 renal units. There were 4 patients admitted for fever and no patient required a blood transfusion.conclusion:Staged ureteroscopic nephrolithotripsy of large renal calculi (smaller than 6cm) is feasible.
Salvage Genitourinary Fistula Repair: Our Experience
Objectives: The objectives are to present the results of salvage genitourinary fistula repaires operations using vaginal flap in Mashad university of medical sciences , Ghaem Hospital.Patients and methods : Nine women ,20-60 years old, suffering from fistula who failed primary repair( Some of them had up to 4 times failed repair) underwent salvage vaginal reconstruction for damaged urethra or bladder . Defects were closed with vaginal wall pedicle flap which was interposed to secure a watertight separation. Results: The repair was successful in all nine patients even in one with rectovesicovaginal fistula and one with large vesicovaginal fistula and sphincter dysfunction .Conclusion:Pedicle vaginal wall flap is an easy prepared ,well- vascularized tissue that can be most helpful in achieving a long-time favorable out-comes in vaginal reconstructive surgery and genitourinary fistula.Keywords : Vaginal wall pedicle flap.vaginal surgery .vesicovaginal fistula, vaginal reconstrution.
Department of Urology, Graduate School of Biochmical Sciences, Hiroshima University, Hiroshima, Japan
Aim of study:Interstitial cystitis (IC) in children may be not as rare as the literatures suggest. We investigated whether glomerulations could be observed in children with refractory overactive bladder (OAB) after bladder hydrodistention .Materials and methods:Fifteen children who underwent bladder hydrodistention were enrolled. Ten children had refractory OAB (OAB group) and other five without OAB were included as controls. The efficacy of hydrodistention in OAB group was assessed by a questionnaire about urinary symptoms and frequency/volume charts. The data were assessed statistically using the non-parametric Mann-Whitney U test.Results:Mea age of each group was 7.2 and 7.6 years, respectively. Whereas glomerulations after bladder hydrodistention were detected in eight children (80%) and hemorrhage in two in OAB group, glomerulations were found in one in controls. Relief of refractory OAB symptoms were obtained in six, and relief of chronic bladder pain were gained in two (20%) with a mean follow-up of 12.2 months in OAB group. Conclusion:In our study, the most important findings were that 80% of children with refractory OAB developed glomerulations after hydrodistention and that glomerulations were significantly more frequent in children with refractory OAB than in controls. There must be some overlapping of symptoms and pathology between refractory OAB and IC in children.
Department of Urology, Graduate School of Biochmical Sciences, Hiroshima University, Hiroshima, Japan
Abstract Withdrawn
Surgical Outcomes of Laparoscopic Dismembered Pyeloplasty in Children with Giant Hydronephrosis Secondary to Ureteropelvic Junction Obstruction
Introduction: Giant hydronephrosis (GH) is defined as massive hydronephrosis in which the renal pelvis crosses the midline. Studies of surgical outcomes after reconstructive surgery for these GH-UPJ obstruction are limited . Over the past two decades laparoscopic pyeloplasty has gradually replaced open repair in children in several centres. The objective of this study was to assess surgical outcomes of laparoscopic pyeloplasty in children with GH .Materials and Methods: Children with unilateral primary UPJ obstruction with huge/giant hydronephrosis were prospectively included and planned for laparoscopic pyeloplasty. Post-operative Ultrasonography was repeated post-operatively at 3 and 12 months to assess the Renal parenchymal thickness , and similarly renogram was repeated to assess improvement in Differential renal function . Results: During the study period Jan 2005 to Dec 2009 , 53 children underwent laparoscopic dismembered pyeloplasty for UPJ obstruction . Of these , eight children had a giant hydronephrosis (GH) caused by UPJ obstruction . The postoperative DRF (Differential renal function) improved in all these eight children . The improvement of RPT at the end of 12 months post-operation in these 8 children with giant hydronephrosis was comparable to that of the non-GH group . Conclusions: At 12 months, surgical outcomes after laparoscopic pyeloplasty for GH were satisfactory. Relief of obstruction allows adequate and comparable nephron sparing.
Laparoscopic Percutaneous Extraperitoneal Closure (LPEC) method for Pediatric Communicating Hydrocele Testis.
We report the experience of laparoscopic percutaneous extraperitoneal closure (LPEC) method for 6 pediatric patients with communicating hydrocele testis. The mean age was 5 years 1month. The left side was affected in 2 boys and the right in 4. Of 6 patients, 2 underwent contralateral prophylactic synchronous closure for pinhole patency of internal inguinal ring to prevent postoperative contralateral hydrocele occurrence. Mean operating time were 44.8 and 67 min. on unilateral and bilateral, respectively. There were no perioperative complications and no recurrences. LPEC method was developed by Takahara in 1997 as a new technique to repair inguinal hernia. There are some reports that apply LPEC method to communicating hydrocele testis because those pathologies are essentially the same. Comparing with conventional Potts repair, the advantages of LPEC are (1) safety because of magnified monitoring, (2) prevention of postoperative contralateral occurrence and (3) cosmetic. However, the patent processus vaginalis is only ligated totally but left undismembered in LPEC method. We should care inadequate ligation, especially the needle skip over peritoneum to prevent recurrent hydrocele.
The efficacy of Endoscopic Surgery for the Pediatric Patients with voiding Disturbance
Objective: Children with voiding disturbance represent various symptoms, such as daytime incontinence, enuresis, and dysuria. For accurate diagnosis, urethrocystoscopy is often performed. In the present study, we reviewed our experiences and evaluated the efficacy of endoscopic surgery for the pediatric patients. Patients: We reviewed the medical records of 13 patients (11 boys and 2 girls) which have performed endoscopic procedures from December 2000 to June 2011. Mean age of their first visit was 6 years and 4 months old. Their chief complaints were daytime incontinence (n=7), pain on urination (n=2), dysuria (n=2), urinary tract infection (n=1), and others (n=1). Postoperatively we evaluated the treatment effects. Results: Three cases of urethral stricture, 2 posterior urethral valve, and 1 urethral ring were recognized, and we performed urethrotomy for these 6 cases. In another 7 cases, we could not detect abnormal findings of urethra. Because specific findings of bladder mucosa were observed, hydrodistenstion of the bladder was performed in the 4 cases. Of the 5 cases in which bladder biopsy was also performed, 2 cases have specific histopathological findings of interstitial cystitis.Discussion: In all cases received urethrotomy, voiding disturbance was disappeared, suggesting that various symptoms were caused by obstruction of lower urinary tract. Of 5 cases received the hydrodistenstion of the bladder, in 4 cases the symptoms were improved. Voiding disturbance in the pediatric patients was involved in not only anatomical abnormalities, but also functional disorders of bladder. It is likely that the endoscopic procedures are one of the effective treatments.
Department of Renal and Genitourinary Surgery, Hokkaido University Graduate School of Medicine, Sapporo, Japan
Diagnostic Accuracy of Transrectal Elastosonography Imaging for the Diagnosis of Prostate Cancer: a Systematic Review
BackgroundTransrectal elastosonography (TRES) is a newly emerging investigative tool that maps out the tissue stiffness of the prostate gland. Recent studies have shown that using TRES can detect up to 90% of prostate cancers. Furthermore, whether the enhanced visual imaging of the prostate cancer by TRES could allow a more targeted biopsy of the cancer and thereby reducing the number of biopsies taken is uncertain. To this end, a review was conducted to assess the diagnostic performance of TRES.Methods Systematic review and quantitative meta-analysis was performed using studies identified by systematic electronic literature search. Articles were included if they reported data on elastosonography and compared this with either standard systematic biopsies or histopathology of radical prostatectomy. Quality was assessed with a validated quality assessment tool for diagnostic accuracy. A random effects model was used to obtain sensitivity, specificity and diagnostic odd ratio. Results Sixteen studies were included in the review. Using histopathology of radical prostatectomy as reference standard, the pooled data of 4 studies showed that the sensitivity of TRES ranged from 0.71 to 0.82 and the specificity ranged between 0.60-0.95, DOR:19.6 ( 95% CI:7.7-50.03). The sensitivity varied from 0.26-0.87 and specificity varied from 0.17- 0.76 using at least 10 TRUS biopsies as a reference standard. Conclusions Elastosonography techniques reported for the detection of prostate cancer seems to have better prostate cancer detection rates. This limits generalizability of the findings. Further refinements in the technology, preferably aimed at reducing the compressional component are needed.
Department of Urology, Ninewells Hospital and Medical School, University of Dundee, United Kingdom
Introduction:Accurate cystoscopic diagnosis of bladder cancer, in particular, post adjuvant intravesical treatment remains a challenge. Raman spectroscopy, with high chemical specificity has potential to provide fingerprint of the tissues. Purpose:We describe development of a novel probe and its application in the diagnosis of bladder cancer in a feasibility study. Material and methods:A prototype clinical Raman instrument including a compact diode laser, spectrograph, CCD detector and a computer mounted on a portable cart suitable for clinical use within an operating room was designed. A novel optical fibre based portable near infrared (785 nm excitation) Raman spectroscopy was used to acquire data from TURBT tissue specimen (freshly resected bladder tumour and normal tissue of size about 2-3 mm).The acquisition time for each spectrum was 5 s. The Raman spectra were correlated with histopathology. Results:20 (10 normal and 10 cancer) fresh urinary fresh bladder specimen (at TURBT) were scanned ex-vivo prior to histopathology analyses. Raman spectra clearly showed the biochemical difference between tumour and normal tissue with significantly high sensitivity and specificity and were distinctive for normal and cancer tissue in all the patients. Conclusions:The feasibility study showed successful translation of Raman spectroscopy technology in the diagnosis of bladder cancer. Raman spectra obtained using novel probe are distinctive for between bladder cancer and normal mucosa.
Harlachinger Krebshilfe e.V. am Klinikum Harlaching, Muenchen-Germany
INTRODUCTION: Earlier onset of androgen deprivation therapy (ADT) and longer overall patient survival lead to an increase of patients with biochemical PSA relaps under ADT. In this prospective monocentric study, the effect of early local tumor ablation with rHIFU of castration refractory prostate cancer (CRPCa) was analyzed. METHODS: 56 patients with locally, non-metastasized, biopsy proven PCa with triple PSA increase under permanent (&ht; 2 years) ADT were included in the study: median(*) age 74 (55-88). Staging: T2: 29%, T3-4: 71%; *Gleason: 7.5 (4-9); N0/M0; Permanent ADT before: 5.1 years; *PSA at HIFU 13.8 (7%&HT;50) ng/ml. Robotic HIFU after TUR was performed under spinal anaesthesia in one session using Ablatherm (EDAP-TMS, Lyon) at 3 MHz. Efficacy and side effects have been analyzed with a follow-up of max. 9.5 years. RESULTS: Efficacy: *PSA Nadir: 0.9 (0-69) ng/ml: of those 71%<4ng/ml and 10% &ht;20mg/ml. Time to *Nadir (months): 1.7(0.3-8.6). *PSA reduction by 84%. Mean follow up time 26 months; *Last PSA: 4.9 ng/ml. Survival rate was 66% at a mean time of 27 months. 34% of the patients died during follow-up: 11% were PCa related, 18% not PCa related, 5% unknown. CONCLUSIONS: TURP & rHIFU in CrPCa reduced PSA by 84% and resulted in a *PSA velocity of 2.95 ng/ml/year. 1/3 did not received further ADT. 2/3 rd of the patients were still alive after a follow up of 2 years and had a PSA below entry PSA at treatment inclusion ! Source of Funding: Harlachinger Krebshilfe e.V. and Lingen foundation.
StoneBreaker: Initial experience of a portable pneumatic lithotripter in 20 patients with bladder stones
Introduction: Bladder stones are not uncommon in patients with lower urnary tract symptoms. Minimally invasive endoscopic approach with various energy delivering systems to achieve stone clearance has been the first line option. We report our initial experience using a portable pneumatic lithotripter, StoneBreaker, that does not require external power or access to compressed air supply , in the treatment of bladder stones.Method & Material: 20 patients with 31 bladder stones were treated with the StoneBreaker, which is a portable intracorporeal lithotripter using an independent compressed air canister. A nephroscope was used for the introduction of the lithotripter probe and fragment clearance. The bladder was examined with cystoscope for intraoperative probe-related injury, and residual fragments.Results: 17 male and 3 female patients were treated. 4 patients had multiple stone (median 4, Range 2-5). All 31 stones with maximum diameter of 2.5cm (median 2.5cm, average 2cm) are completely fragmented and cleared. Average number of shocks to each stone: 8 (Range 6-24). Typically, one air canister was used in each patient. Probe related bladder mucosal injury, perforation or urosepsis was not detected. All patients were discharged within 48 hours (median 23 hours, average 32 hours) without a urethral catheter.Conclusion: The new portable pneumatic StoneBreaker is safe, effective and efficient for bladder lithotripsy. With the independent compress air canister supply, operator fatigue caused by cables and tubings during long lithotripsy sessions can be eliminated.
Department of Urology, University of California Irvine, Irvine, USA
Introduction
Prediction and risk estimation are important for patient counseling and treatment in prostate cancer. Although many nomograms exist, they are limited by reliance on subjective Gleason scoring. Advanced imaging analysis of specimens has been used by Aureon to develop a novel predictive model.
Purpose
Our objective was to compare the Kattan nomogram (pre- and post-operative) and the D'Amico risk classification with the Aureon preoperative Px±and Post-Op Px models.
Materials and Methods
In a retrospective study of 124 patients, Kattan pre- and post-operative progression-free probabilities were compared to Px±and Post-Op Px disease progression likelihoods using linear regression. D'Amico risk of biochemical recurrence after surgery was compared to Aureon disease progression likelihood, favorable pathology classification and PSA recurrence risk.
Results:
Correlation coefficients describing the relationship between Px±and five- and ten-year Kattan models were 0.6489 and 0.6607. Post-operative data was less well correlated with correlation coefficients 0.1367, 0.1843, 0.2037 and 0.2288 describing the relationship between Post-Op Px and Kattan two-, five-, seven- and ten-year models. Risk of biochemical recurrence comparison analysis found the likelihood that a patient who is D'Amico high risk will also be classified as Post-Op Px high risk is 82%, while the likelihoods for intermediate and low risk patients are 31% and 4%.
Conclusions:
Preoperative Px±disease progression probability was well correlated with Kattan progression-free probability, while post-operative Px data was well correlated with D'Amico risk criteria. These models may be valuable predictive tools to add to the physician's tool box.
Urology Department Saint Savas Hospital Athens Greece
Introduction Argus male sling is a re-adjustable male sling used for the treatment of stress urinary incontinence in men. Several complications are reported in the literature. Purpose We report our results after the first 20 implantations as well as the complications that were encountered in our clinical practice and discuss on how to manage them.Materials and Methods Between 03/2009 and 08/2010 we have implanted the Argus sling in 20 patients. Eighteen had stress urinary incontinence after radical prostatectomy and two after TURP following brachytherapy. Mild, moderate and severe incontinence was found in 5, 7 and 8 of them respectively. Eleven patients had a negative prognostic factor (adjuvant radiotherapy, urethral stricture, previous failed attempt of surgical treatment of incontinence).Results Primary complications include perforation of bladder from the needles, small perineal hematoma,wound disruption of the suprapubic incision due to subcutaneous reactive fluid collection and temporary retention of urine due to overtreatment. Late complications include persistent perineal discomfort for more than 2 months, dislocation of the sling, urethral erosion, infection and abscess formation. In 5 patients the sling was removed because of late complications. After a median follow up time of 15.8 months, 12 out of the 15 remaining patients are dry and 3 report improvement of symptoms. Conclusions Pain can be managed with analgesic and will improve in most cases. Special care should be taken during the operation to avoid bladder perforation. A loose sling is preferable than overtreatment because the re-adjustement procedure is much easier in the first case.
KTP Laser PVP at 5-year follow-up- Identification of an Unusual Complication
Introduction:The use of the 80-W potassium-titanyl-phosphate (KTP) laser for the treatment of symptomatic benign prostatic hyperplasia (BPH) has increased recently. Both prospective and comparative studies have confirmed its efficacy, and single-centre long-term studies have demonstrated its durability. However, the paucity of long-term data has limited the analysis of long-term complications. Bladder-neck stenoses, urethral strictures, and re-operation are well-described. We aimed to identify the complication rates at long-term follow-up from a single UK centre. Specifically, we report 5 cases of bladder and prostatic urethral calculi presenting up to 4 years following the initial procedure. Patients and Methods:We retrospectively analysed data from all patients who underwent 80-W GreenLight laser PVP from 2004-2006. Evaluation occurred pre-operatively, and then at 3, 6, 9, 12 and 60 months post-operatively. This included IPSS, peak urinary flow rate (Qmax), and post void residual volume (PVR), as well as analysis of any complications. Results:A total of 90 patients were eligible for analysis, with a mean age of 71 and mean prostate volume of 55.8 grams. At 5-year follow-up there were no cases of urethral strictures, but a 3.3% (3) rate of bladder neck stenosis and a re-treatment rate of 21% (19). Interestingly, 5 (4.3%) patients developed calculi in the prostatic urethra and bladder requiring litholopaxy.Conclusion:The formation of bladder and prostatic urethral stones as a long-term complication of KTP laser PVP has not been widely described. This is a complication which may require re-treatment many years later, and patients should be advised of this.
Department of Urology, Osaka Medical College
Purpose; To assess the association between development of urethral stricture and disease-free survival for patients with localized prostate cancer treated with high-intensity focused ultrasound (HIFU).Materials and Methods; The inclusion criteria for treatment were clinical stage T1-T2N0M0 prostate cancer. Treatment failure was defined according to the Phoenix criteria, and the disease-free survival rate (DFSR) was evaluated using this definition. Patients were divided into two subgroups according to whether or not they developed a urethral stricture or a subclinical urethral stricture (SCUS) during follow-up. Results; A total of 144 patients were included in the present study. The median follow-up time was 47 months (range 2 - 70). Grade 1-4 urethral stricture occurred during follow-up in 28 (19.5%) patients. Clinically insignificant bladder outlet obstruction requiring transient catheterization, which was defined as SCUS was found in 30 (20.8%). The 5-year DFSR by Kaplan-Meier estimation was 61.2% for the entire cohort, 78.2% for patients who developed urethral stricture and/or SCUS (US/SCUS) and 47.8% for those without US/SCUS (p<0.001). On Cox regression analysis development of US/SCUS proved to be an independent predictor of DFSR.Conclusions; Development of US/SCUS was identified as a predictor of favorable HIFU treatment outcome.
Salvage high-dose-rate Brachytherapy for Local Prostate Cancer Recurrence after Initial Treatment
Objectives: We assessed the preliminary clinical results of salvage high-dose-rate brachytherapy (HDR-BT) applied in cases of suspected local recurrence or of residual tumor after initial treatment.Patients and methods: The subjects were 20 patients who met the above conditions and underwent salvage HDR-BT between December 2006 and July 2010. The T stage at the initial treatment was T1c in 3 patients, T2 in 13 patients, and T3 in 4 patients. Seventeen patients received HDR-BT + -external beam radiation therapy (EBRT), two patient received proton-beam irradiation and one patient received HIFU. Follow-up after the completion of salvage HDR-BT lasted 12-51 months (median: 24 months). A dose of 11.0 Gy radiation was delivered twice (22.0 Gy in total), separated by a 6-hour interval, on the day the applicators were inserted. Results: Fourteen of the 20 cases (70%) remained in a biochemical non-evidence of disease (bNED) state. Three year PSA failure free survival rate was 52.6%. Hormone administration was initiated in the six cases of recurrence. No G3 or more severe events occurred, and the incidence of G2 was low during this study period. Conclusion: Twenty cases treated with salvage HDR-BT, PSA levels remained low in fourteen cases, and the incidence of complications was also low. This suggests that salvage HDR-BT is effective as an option for treatment of local prostate cancer recurrence after radiotherapy.
Comparison of Tissue Temperature and Damage between Enseal and Bipolar Vessel Sealing Devices in an Animal Model
Purpose: EnsealTM (Ethicon Endosurgery, Cincinnati, Ohio) performs effective safe cutting and hemostasis. In this study we examine tip temperature and histological changes after cutting tissue with 3 devises : Enseal, LigaSureTM (Valley Lab, Boulder, CO, USA), and BiClamp TM (ERBE, Tuebringen, Germany) .Material and methods: Chicken muscle, pig greater omentum and intestine were used in this study. 1) Tissue temperatures of Enseal were recorded at 5s, 15s, 30s and 45s activation. 2) In the 3 devises tip temperatures were recorded after dividing tissue both extracorporeally and intracorporeally (laparoscopic), and 3) histological changes in pig intestine touched to the tip were compared after 5s, 15s, 30s and 45s activation.Results: 1) Enseal: Tissue temperature rose during activation from 53 to 68 degrees C. 2.) Enseal and Ligasure: tip temperature remained below 60 degrees C in both intracorporeal and extracorporeal conditions. 3) Histological tissue damage was observed in proportion to the activation time. Severe damage was observed after 15 seconds in all devices, especially BiClamp.Conclusion: A longer sustained period of Enseal and Ligasure activation causes greater tissue thermal damage while short activation (within 5 seconds) does not. Surgeons should pay close attention to neighboring tissue and organs around the tip during activation.
Safety Evaluation of Orally Administered 5-Aminolevulinic Acid for Photodynamic Diagnosis
Introduction: Photodynamic diagnosis (PDD) using orally administered 5-aminolevulinic acid (5-ALA) has been applied for various malignant neoplasms. 5-ALA is a naturally occurring amino acid and present in virtually all human cells. Purpose: Oral administration of 5-ALA is regarded safe for PDD. However, there are few reports which demonstrated safety for orally administered 5-ALA. We investigated on safety evaluation of orally administered 5-ALA.Material and Methods: 231 patients were performed PDD after oral administration of 5-ALA. 1.0 g of 5-ALA was given orally four hours before surgical resection of tumors. We did not isolate patients from direct sunlight exposure. Blood was collected for biochemical tests on pre- and postoperative day one. We assessed whether adverse events were associated with patient's age, sex, height, weight, body surface area(BSA), or body mass index(BMI).Results: Thirty-two, two and two patients had liver dysfunction, vomiting and photodermatosis. No treatment was needed for liver dysfunction and vomiting. Photodermatosis was cured as soon as 1-2 days postoperatively by avoidance of direct sunlight, closing the curtains. There was no significant difference in patient's age, sex, height, weight, BSA and BMI between the group with adverse events and that without adverse events.Conclusions: Patients were administered not only 5-ALA but also many kinds of drugs such as anesthetics or antibiotics perioperatively. Therefore, it is unclear that 5-ALA can cause adverse events of liver dysfunction. No treatment to all of liver dysfunctions was needed. We thus conclude that the oral administration of 1.0g of 5-ALA would be safe for PDD.
Aichi Cancer Center Hospital and Research Institute, Aichi, Japan
(Introduction) Biopsies of renal masses still has a limited role, due to low diagnostic accuracy and complications including bleeding and needle tract disseminations associated with biopsies. To address these issues, we performed renal biopsies after ablation therapy or arterial embolization to evaluate the sufficiency of the pathological diagnoses. (Materials and methods) Between July 2002 and February 2011, a total of 49 cases who had undergone biopsies of renal masses were enrolled in this study. The patients were divided into two groups that included 38 cases with biopsies carried out immediately after radiofrequency ablation (RFA) and 11 cases with transcatheter arterial embolization (TAE) followed by immediate biopsy. The needle core biopsies of the renal masses were performed under real time CT guided .(Results) There was not significantly difference of background, including age, gender and tumor side, between two groups. The final pathological results of the diagnosed malignant tumors in the RFA group were 36 clear cell and 2 chromophobe tumors. The TAE group included 11 cases with clear cell malignant tumors. The incidence of deconstruction in cancer clusters induced by pre-treatment therapy was significantly higher in the RFA group (36/38, 94.7%) than in the TAE group (5/11, 45.6%) (P<0.001). The accuracy of classification using the Fuhrman nuclear grade was significantly lower in the RFA group (12/38, 31.5%) than in the TAE group (11/11, 100%) (P<0.001). (Conclusion) A high incidence of deconstruction in cancer clusters and the Fuhrman nuclear grade having relatively low diagnostic accuracy in RFA cases.
Georgetown University Hospital, Department of Urology, Washington DC USA
Introduction: Transrectal ultrasound plays a central role in the diagnosis of prostate cancer, however, false negative rates have been reported as high as 30%. Mapping of radical prostatectomy specimens have shown undersampling of the peripheral zone with standard TRUS biopsy techniques, including the apical lateral horns. With development of a 3D-image fusion model which tracks biopsy location in real-time, we report our apical prostate sampling rate during standard twelve core TRUS biopsy.Materials & Methods: Twenty patients underwent 3T endorectal coil multiparametric prostate MRI prior to biopsy and 3D TRUS images were obtained. An electromagnetic positioning device was attached to the TRUS probe in order to track the position of each needle pass. The 3D-TRUS image documenting the location of each biopsy was recorded and compared to its intended site.Results: Twenty patients (median age 66) with a median PSA of 5.63 ng/ml and median prostatic volume of 43 cc underwent MRI fusion biopsy with electromagnetic tracking. Out of eighty total intended apical biopsies, the prostatic apex was succesfully biopsied only 71% of the time with 29% of biopsies incorrectly targeting the prostatic mid-gland.Conclusions: In our series, standard TRUS biopsy led to a significant undersampling of the apical prostate. Approximately 30% of the identified biopsies of the prostatic apex on transrectal ultrasound incorrectly sampled the prostate mid gland. The large false negative rate of TRUS should be considered as alternative imaging and diagnostic modalities, such as MRI, are being developed and may provide more reliable sampling of the prostate.
Georgetown University Hospital
Introduction: Transrectal high-intensity focused ultrasound (HIFU) is becoming increasingly utilized despite its lack of availability in the USA. As treatment guidelines are not established, we report our experience with multiparametric MRI (mpMRI) and image guided fusion biopsy technology in the perioperative detection of occult malignancy in patients undergoing HIFU.Materials & Methods: Eleven patients were referred to the NIH for 3T-endorectal coil mpMRI, with areas suspicious for malignancy sampled via a MRI/TRUS fusion biopsy platform. Three patients were being considered for primary HIFU treatment (median PSA 4.97, Gleason 6) and eight patients were post HIFU ablation (median time 41 months) with a rising serum PSA (median 4.3) and prior negative TRUS biopsies.Results: Of the three patients undergoing preablative evaluation, our standard TRUS biopsy revealed similar patterns of prostate cancer as their outside institution. However, in two of these patients (67%), MRI targeted fusion-biopsy of suspicious lesions identified new areas of Gleason 6 disease. Of the eight patients who presented with biochemical recurrence post-HIFU, four patients (50%) had residual malignancy detected on the MRI targeted biopsy and not on the standard TRUS.Conclusions: In this series, our mpMRI and image-fusion biopsy platform was able to identify occult malignancy in patients who have had biochemical recurrence after HIFU. New areas of malignancy were also identified in pre-HIFU planning when compared to standard-TRUS. MR imaging may be useful in delineating the burden of disease in patients being selected for HIFU as primary therapy or in managing patients with post HIFU ablation failure.
Virtual Cavernoscopy: The Evaluation of Arteries Inside the Corpus Cavernosum
Introduction and Objective: Due to recent advances in digital technology, virtual endoscopic images have become available in clinical practice. This technology can be applied to the corpus cavernosum. We observed the arteries inside the corpus cavernosum using virtual cavernoscopy. Materials and Methods: The study subjects were 40 patients who visited our out-patient clinic for examination of erectile dysfunction and who underwent 3D-CT cavernosography. Retrospectively, virtual cavernoscopic images were reconstructed from 3D-CT cavernosographic image data. We visualized and evaluated the main artery, and the existence of the penetrating artery of penile dorsal artery, inside the corpus cavernosum. Results: The cavernous artery was visualized as the main artery in 51 corpus cavernosal lumen out of the 80. The penetrating artery of the dorsal artery was visualized as the main artery in 22 lumen, and the branch of the cavernous artery to the other side of the corpus cavernosum was visualized in 4. The penetrating artery of the dorsal artery was detected in 41 lumen. Conclusions: Use of virtual cavernoscopy to understand the arteries inside the corpus cavernosum as in each cases before arterial revascularization surgery, may be valuable in selecting the appropriate reconstruction method.
Koc University School of Medicine, Istanbul, Turkey, 2Istanbul American Hospital
OBJECTIVE: There is still an ongoing debate about the transferability of open surgical skills to daVinci robot techniques. Herein we present initial results of a single surgeon, highly experienced in open surgery, incorporating robot-assisted radical prostatectomy (RARP) into his practice. PATIENTS AND METHODS: Between June 2010 and June 2011, 30 patients with prostate managed with RARP by a single surgeon (TE) highly experienced in open procedures (over 1000 open radiacal prostatectomies). Demographic data, including age, body mass index (BMI), preoperative PSA and clinical stage as well as erectile functions (IEFF score) were prospectively documented. Operative data, including mean operative time, presence of any complications and final pathological findings were collected. RESULTS: Mean age was 53.7 (range:43-70) years and mean operation time 153.3 (range:120-185) minutes. There was rectal injury and open conversion in one case, who also underwent blood transfusion. Mean hospitalization was 4.1 days. Median urethral catheter removal time was 7 days. Final pathologic assessment revealed pT2 tumors in 23 (surgical margins (+) in 8%) and pT3 in 7 (surgical margins (+) in 28%) cases. After a median follow-up of 6 months, 20 (66%) can achieve erections w/wo PDE-5 inhibitors, and 25 (83%) are fully (zero pad) continent. CONCLUSIONS: Our initial results suggest that open surgical skills can be transferred to RARP by experienced surgeons not only by reasonable functional outcome but more importantly by the low margin positivity rate in organ confined disease.
User Satisfaction on Multi-purpose Linin Bag for Laparoscopic Surgery
At the present, the trends in the operative management of urologic disease at a university hospital are minimally invasive surgery. There is a possibility of the development of laparoscopic surgery move from conventional laparoscopy to be laparo-endoscopic single site surgery (LESS) such as single port surgery. Nevertheless, all procedure requires a longer instrument than a standard instrument. During laparoscopic surgery, a damaged instrument arises from falling down to the ground. This specific danger arises from many slop areas in a position of a patient in a urologic procedure; such as a lateral or lithotomy position. The surgeons usually drop the surgical instruments on the operative floor. These expensive instruments can be broken or lost. Moreover, if there is no reserved instrument in the operative theatre, the operation has been prolonged or stopped. The multi-purpose linin bag can be used to prevent the drop of the surgical instruments. This could be confirmed by the incidence of surgical instrument drop rate was zero after the use of this bag. The users were satisfied with this invention. The satisfied score was between 4.53-4.77 (S.D.=0.466-0.629). Therefore we have developed a multi-purpose linen bag that uses local material, practical and economic. Our new inventional bag is not only flexible and sustainable development, but also lean and seamless.
Hospital Punta Pacifica, Panama City, Panama
Introduction: Flexible ureteroscopy with Holmium:YAG laser lithotripsy has a known learning curve; although this laser is the safest flexible intracorporeal lithotrite, complications occur with greater frequency early in its adoption. Herein, we review the implementation of a didactic and practical curriculum to introduce the Holmium:YAG laser for flexible URS. Following the initial tutorial period, we assessed procedure outcomes and complications. Methods: A 15watt Holmium:YAG laser was introduced to Hospital Punta Pacifica, a newly developed hospital affiliated with Johns Hopkins Medicine International. We created a three-day curriculum including classroom-based lectures and live surgical experience. Lectures were designed to review laser properties and surgical applications; technical points emphasized included the "dusting" technique of laser lithotripsy rather than active fragment extraction. Live surgeries were performed as demonstrations and then as mentored procedures. The medical records of all patients undergoing Flex URS/Laser in the 12 months following this program were reviewed. Results: A total of 32 Flex URS/Laser procedures were performed. Mean age was 43.0 years; there were 19 males and 13 females. Twenty-nine procedures were for the treatment of stone, and three were for incision of ureteral stricture. Five stones were located in the ureter, with the remainder in the kidney. All stones were accessed and fragmented with the laser, and no peri-operative or post-operative complications were encountered. Conclusions: A focused curriculum can simplify the introduction of Flex URS/Laser and permit the rapid achievement of acceptable results. An emphasis on limiting active fragment extraction may reduce the likelihood of ureteral injuries.
Department of Urology, Kurashiki Medical Center, Kurashiki, Japan
<Introduction>The combination therapy of PNL and ESWL is recommended for most patients with staghorn calculus. There is still no nation-wide PNL training program in Japan. TAP (TUL-assisted PNL) is minimally invasive surgery for refractory urinary stone, and TAP live demonstration by experts would induce the motivation to learn PNL for staghorn calculus.<Material and method>A 70-year-old woman was follow-up with right renal stone and left contracted kidney after cystectomy and ileal conduit formation. In February 2011, renal stone grew up to complete staghorn calculus (60*30mm) without hydronephrosis. Renal insufficiency (Cr: 1.8mg/dl) was found in further examination. Isolated organism from urine was P. aeruginosa. Staffs in admitting hospital are unfamiliar with PNL.2-staged TAP following right ureteral stenting was planned by informed consent under supervisors from affiliated facility. Stage-1: Calyceal needle puncture was made in the Valdivia position. Nephrostomy balloon catheter and ureteral stent were indwelled in the space after stone clearance with simultaneous TUL and PNL. Stage-2: Lithotripsy and litholapaxy were performed in flank position one week later.<Results> Operating time was 155 min. (stage-1) and 245 min. (stage-2) respectively. Estimated bleeding volume was 129 ml. Stone free was accomplished before discharge without infection shock and significant aggravation of renal function (Cr: 1.9mg/dl). Stone analysis revealed struvite.<Conclusion> TAP was safe and useful for the complete staghorn calculus patient with ileal conduit, renal insufficiency and infection risk. TAP live demonstration by experts served endourological fellow with real-life hands-on training of TUL in addition to PNL.
Which Factors will affect the Laparoscopic Suturing skill in Beginners?
PurposeWe tried to analyze the factors which influence laparoscopic suture skill in beginners.Material and MethodFrom April 2008 to March 2011, 124 medical students who were in twenties received medical training in our institution. They were instructed laparoscopic suturing and ligation techniques with use of dry-box by expert of laparoscopic surgery. After one week self-training, a total time of Suture to Ligation Time (SLT) which composed suturing, twice ligation, cutting, and needle retrieving was measured. We asked them several questions i.e. a: “Do you know laparoscopic surgery was done by urologist?”, b: “Do you play the video games routinely?” c: “Are you interested in laparoscopic surgery?”, d: “Do you wish to be a surgeon in future?”. We investigate the relationship between SLT and answers. ResultA mean SLT of men and women were 106.2 and 89.7 second (not significant). SLT of group “yes” in question were 97.6, 81.4, 90.4, and 110.9 seconds, and “no” in question were 100.4, 106.8, 141, and 92 seconds respectively. SLT of students who are interested in laparoscopic surgery was significant shorter than that of “no interested” students (p=0.002). The difference of SLT between students who play video games routinely and who don't play was marginally significant (p=0.051).DiscussionIt is assumed that students who are interested in laparoscopic surgery practiced enthusiastically, and their SLT was shorter than others. For effective training of laparoscopic technique in beginners, the interest and motivation to laparoscopic surgery are important issues.
Preoperative Simulation of Partial Nephrectomy with Stereoscopic Reconstruction of Multi-Slice Computed Tomography
Impact of a Systematic Educational Program to Shorten the Learning Curve for Holmium Laser Enucleation of the Prostate
Introduction and Objectives: Holmium laser enucleation of the prostate (HoLEP), a new possible Gold Standard for benign prostatic hyperplasia, has been thought a long learning curve for beginner. We succeeded in shortening the learning curve by introducing a new method named anteroposterior dissection HoLEP, and training the surgery to step by step. Method: Seventy-four consecutive patients with benign prostatic hyperplasia underwent HoLEP from March 2010 to February 2011. All surgeries were performed based on the same procedures, anteroposterior dissection HoLEP described elsewhere (Urology, 2010:76.1451-1455). Out of 74, 58 HoLEPs (group 1) were performed by supervisors, and 7 cases (group 2) by a HoLEP beginner, who has experienced more than 20 TURPs. Nine cases (group 3) were performed by another, who has experienced a few TURPs. The first phase of training is a setting machines and a preparation for studying with tutorial video. The trainee experiences more than five examples as an assistant. The second phase is a surgical skills of incision, hemostasis and morcellation using an inverse (downward) technique. The third phase is a middle lobe removal and subsequently cutting at 12 o'clock to appropriate layer. The fourth phase is a removal of either right or left adenoma. The fifth phase is an independently completion of HoLEP. Results: Two beginners were able to independently complete HoLEP according to our training system by less than ten cases. Conclusions: Our techniques and the educational system step by step can enable the beginner to complete HoLEP in a shorter learning curve.
Department of Urology, Hanyang University College of Medicine, Seoul, Korea
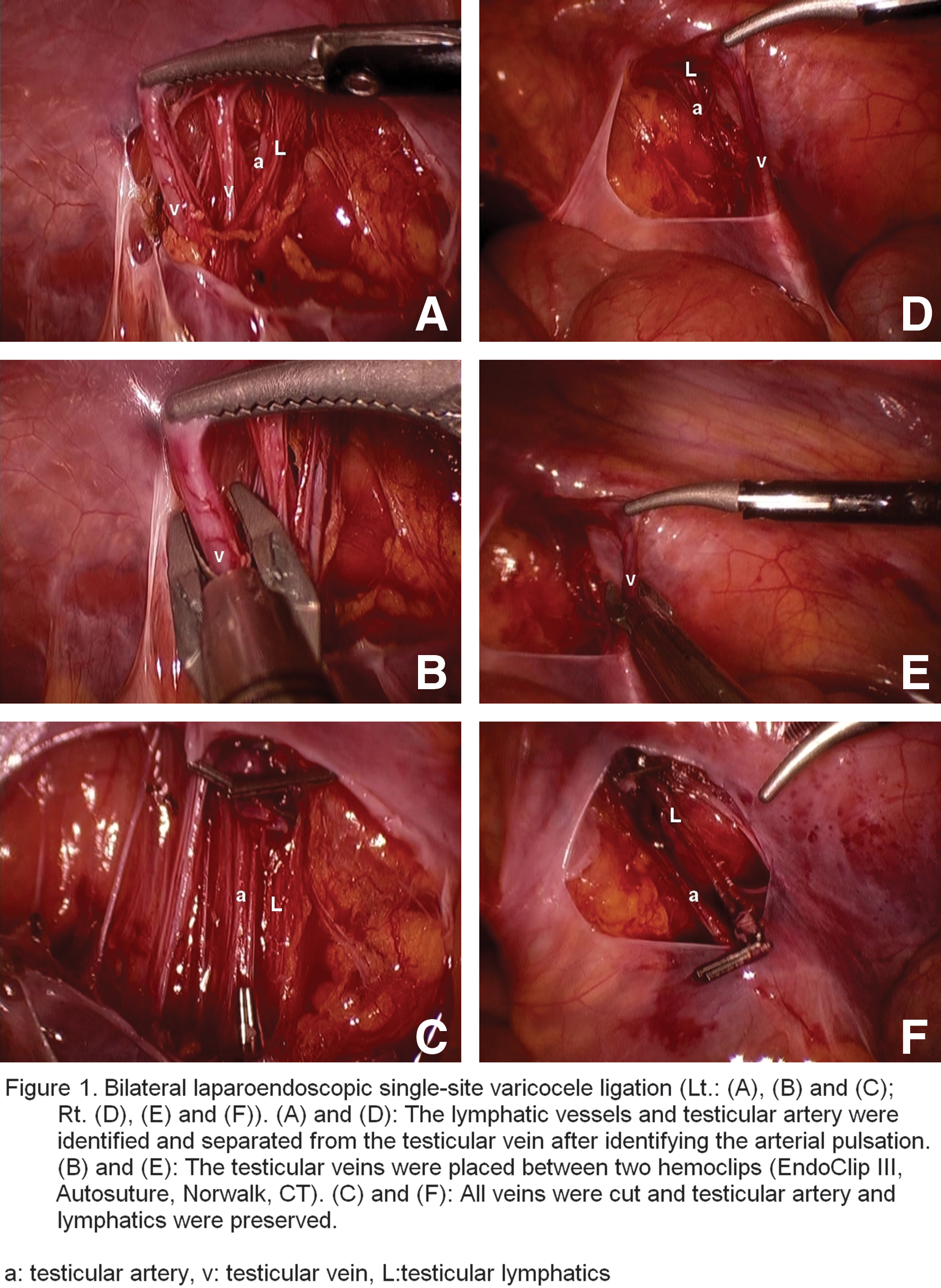
Department of Urology, Hanyang University College of Medicine, Seoul, Korea

NorthShore University HealthSystem, Evanston, IL, USA
INTRODUCTION:The widespread use of computed tomography (CT) may lead to overtreatment of uric acid stones with surgery, as opposed to oral alkalinization. Our study aims to determine the natural history and contemporary treatment of uric acid stones, including how often patients undergo surgery as opposed to medical dissolution therapy; bilateraityl, recurrence rate, and associated comorbidities.METHODS:We retrospectively reviewed 1439 urinary stone analyses obtained at our institution from Jan/2008 until Dec/2010. 149 uric acid stones were identified, and patient demographics, associated comorbidities (gout, diabetes, etc.), location, size, multifocality, Hounsfield units, and intervention (medical versus surgical) were evaluated. RESULTS:The average age of uric acid stone formers was 58, and 68% were male. The average ureteral stone was 3.9x2.9mm whereas renal stones were 6x5.3mm. 65% of patients underwent ureteroscopy with laser/basketing, either primarily or after initial ureteral stenting for infection or acute renal failure. 12% underwent shockwave lithotripsy, 12% underwent alkalinization therapy alone and 7% underwent percutaneous nephrolithomy. 50% of patients had hypertension, 29% had Diabetes and 21% had hypercholesterolemia. The average Hounsfield units was 413.CONCLUSIONS: Uric acid stones represented 11% of our stone forming cohort. Common comorbid conditions include diabetes, hypertension and lipid disorders. Although Hounsfield units and urinary pH can lead to a correct diagnosis and alkalinization curative, over 50% patients in our cohort underwent a surgical procedure because they are older, and presented with evidence of infection and acute renal failure.
Urolithiasis in Octogenarians and Nonagenarians
Introduction: Urolithiasis is occurring more frequently in patients over 80. Early recognition/management may be more critical in this physiologically compromised group.Materials and Methods: We retrospectively reviewed 1439 patients presenting to our stone center from Jan-2008 until Dec-2010. N=44 patients over 80 were identified, and their demographics, medical comorbidities, stone composition, size, and intervention type (medical/surgical) were evaluated. Results: The mean age at presentation was 84.3 years (range 80-99), and 32% were female. 18 patients (41%) had no previous stones, and 86% presented with acute ureteral colic. Mean BMI was 27 (range 19.6-44), mean stone size was 7.0mmx5.3mm. 16% presented with urosepsis and 9% with acute renal failure. Only 14% of patients passed their stone spontaneously, and all the remaining underwent surgery, including 5% PCNL, 21% SWL and 74% delayed ureteroscopy after primary stenting. There were no deaths or ICU stays in this elderly cohort. Stone analysis demonstrated calcium oxalate in 68% , 20% uric acid, 9% mixed CaOx/uric acid and 3% Calcium phosphate. 55% had hyperlipidemia, 68% hypertension, 23% thyroid disorders and 32% underlying malignancy. Conclusions: Over 40% of patients over 80 years present with their first stone, and 86% with acute colic. Early recognition and ureteral stenting are critical in avoiding ICU stays and mortality. Ureteroscopy, SWL and PCNL are well tolerated in this group.
There is Increased Incidence of Pneumomediastinum, Pneumothorax and Subcutaneous Emphysema After Less Surgery
INTRODUCTION: Laparoendoscopic Single Site Surgery (LESS) requires use of specialized ports, instruments and unusual surgeon movements. This project shows that unusual complications such as pneumomediastinum and pnuemothorax increase after LESS.MATERIALS: We identified two patients with significant pneumomediastinum and subcutaneous emphysema in our LESS database. RESULTS: Case 1: 76-year-old man underwent LESS nephrectomy for 6.3cm RCC using Applied-Medical-Gelpoint. OR-time 168 minutes, BMI 28.7 and EBL 200cc without complications. CT scan on postoperative day 2 for worsening abdominal pain demonstrated severe subcutaneous emphysema around port site. He was discharged on POD 3 after ileus resolved. Case 2: 25-year-old woman underwent LESS dismembered pyeloplasty using Applied-Medical-Gelpoint. OR-time 225 minutes, BMI 20.6 and EBL 50cc without complications. CT scan on postoperative day 1 for persistent chest pain demonstrated subcutaneous emphysema, pneumomediastinum, pneumoretroperitoneum. Discharged home on POD 2 after pain resolved.CONCLUSIONS: Unlike multi-port laparoscopy, LESS requires more aggressive instrument movement and torquing. Vigorous torquing causes insufflation gas to escape between the port and the peritonotomy, tracking along the subcutaneous space. We conclude that due to longer operative times and more vigorous torquing, high volumes of subcutaneous gas can track under Scarpa's fascia all the way into the mediastinum and pleura in LESS patients.
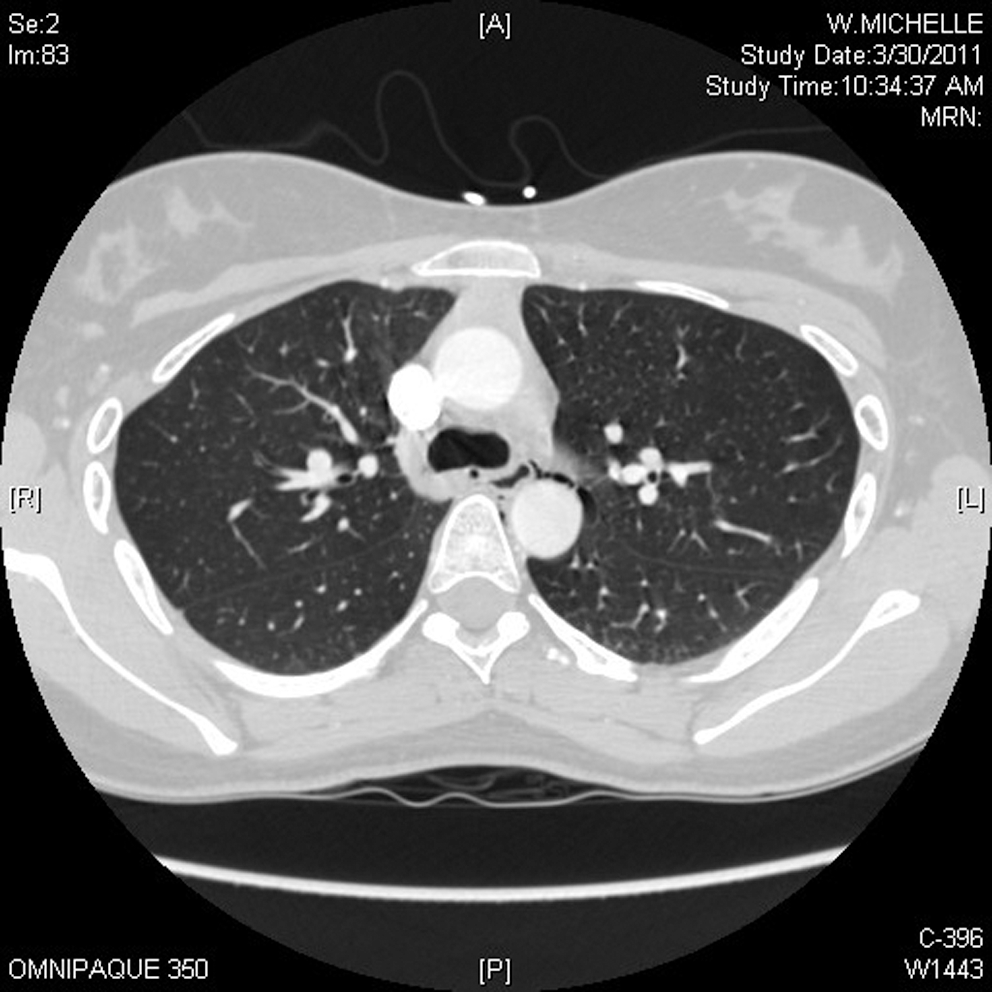
Correlation of the R.E.N.A.L. Nephrometry Score with Warm Ischemia Time After Robotic Partial Nephrectomy
IntroductionProlonged warm ischemia time(WIT) is associated with renal damage during partial nephrectomy. The R.E.N.A.L. nephrometry score(RNS) was developed to standardize the description of renal tumor anatomy in a quantifiable manner. We analyzed preoperative factors and individual categories of the RNS to identify those predicting a longer WIT and affecting postoperative renal function.PurposeTo determine whether individual categories of the RNS have different impact on the WIT of patients undergoing robotic partial nephrectomy(RPN).Materials and MethodsOf 251 patients who underwent RPN between January 2007 and June 2010, RNS was determined in 187 with available imaging. Multivariable linear regression analysis was performed to identify which factors were more significantly associated with WIT.ResultsMean patient age, BMI, and tumor size were 59 years, 30Kg/m2, and 3.15cm, respectively. Overall RNS was of low(4-6), moderate(7-9), and high complexity(10-12) in 84(45%), 80(43%), and 23(12%) patients, respectively. Longer WIT was associated with size>4cm(p<0.0001), entirely endophytic properties(p=0.005), tumor<4mm from the collecting system/sinus(p<0.0001), and location>50% across the polar line, or crossing the axial renal midline, or entirely between the polar lines(p=0.004). Total RNS and WIT were highly correlated(Spearman correlation coefficient=0.54, p<0.0001). There was a significant trend of higher WIT with increased tumor complexity(p for trend<0.0001).ConclusionsThe anterior/posterior subcategory has no significant impact on the WIT of patients undergoing RPN. WIT is similarly and significantly affected by the other subcategories, as well as by the overall RNS. This study further validates the role of the RNS as a predictor of surgical outcomes.
Renal Nephrometry Score and Complication Rate after Robotic Partial Nephrectomy
IntroductionThe R.E.N.A.L. nephrometry score(RNS) was developed to standardize the description of renal tumors anatomy in a quantifiable manner.PurposeTo evaluate the RNS as a predictor of postoperative complications related to robotic partial nephrectomy(RPN). Materials and MethodsOf 251 patients who underwent RPN between January 2007 and June 2010, RNS was determined in 187 with available imaging. We evaluated the relation between the complication rate and each component of the RNS using logistic regression analysis.ResultsMean patient age, BMI, and tumor size were 59.6 years, 30.6Kg/m2, and 3.15cm, respectively. Tumor was located in the upper pole in 22%, interpolar or hilar region in 46%, and lower pole in 32% of the patients. The mean warm ischemia time was 18.3min. The overall RNS was categorized as low complexity(4-6) in 84 patients(45%), moderate complexity(7-9) in 80(43%), and high complexity(10-12) in 23(12%). Larger tumors were associated with a higher frequency of complications(Chi-square test p=0.005). Forty-six percent of the patients with tumors > 4cm had complications, against 21.3% of the patients with tumors < 4cm(Fisher exact test, p=0.0021). There was no relation between E(p=0.8), N(p=0.2), A(p=0.8), L(p=0.3) components and complications. Complications were significantly associated with more complex tumors, according to the total RNS(Chi-square test p=0.003). There was no correlation between grade of complications and complexity of the tumor, according to RNS(Chi-square test p=0.252).ConclusionsHigher RNS is associated with increased risk of perioperative complications. Of all RNS categories, larger tumor size has the highest correlation with complication incidence.
VP01: Robotic/Lap Bladder/LESS/NOTES
Department of Urology, Policlinico di Modena, Univerista' di Modena e Reggio Emilia
IntroductionRecently NOTES (Natuaral Orifice Trans Endoscopic Surgery) and has been evaluated for urologic procedures.This technique combine laparoscopy and endourology, providing new and interesting solutions.PurposePresent the initial ex vivo development of NOTES radical prostatectomy (NOTES-RP).Materials and MethodsFrom June 2010 to April 2011 fifteen cadaveric NOTES-RP were performed. Laser dissection was started at the prostate apex laterally at veru montanum and then continued clockwise ( right lobe) and anticlockwise ( left lobe); holmium:yttrium-aluminum-garnet laser was used in first eight cases, for the last seven cases 100 W thulium laser was used. Nine NOTES-RP were performed using an intrafascial plane, after developing the plane between the prostate capsule and lateral prostatic fascia, the other six were performed extrafascially. NOTES-RP was completed with endoscopic resection of seminal vesicles from the posterior wall of the bladder. Urethrovescical anastomosis was performed using a suturing device developed for this purpose (SR-5LS suture device, LSI solutions, Victor, NY).ResultsProcedures were successfully completed in except for the three cases due to lenghty operative time .Conclusions Lack of reliable anatomical landmarks makes the procedure quite lengthy to be performed repeatedly in a step-by-step fashion. The presence of anatomical planes seen from the inside rather than from outside as in all other prostatectomies is another element to consider in order to perform a totally nerve sparing procedure while leaving positive surgical margins. Our aim is to codify this procedure in order to offer such revolutionary treatment to petients with low risk prostate cancer
Laparoendoscopic single-site Radical Prostatectomy: the Establishment of feasible Techniques in Japanese Initial Experiences.
Objective: Laproendoscopic single-site radical prostatectomy (LESSRP) is a challenging operation. We evaluate our establishing techniques with suitable appliances.Patients and methods: Between July 2010 and June 2011 we performed five LESSRP for the patients with localized prostate cancer. Quad Port™ or SILS Port™ was used as the multichannel trocar at an umbilical incision. And Miniloop Retractor™ or 2.1mm forceps was inserted at the left iliac fossa in the later cases. As the single port devices, Diamond-Flex Forceps™ or SILS Dissector™ was used for the left hand manipulation and Opti4™ or LigaSure Blunt Tip™ for the right hand. Also, Autonomy needleholder was employed for a part of the vesico-urethral anstomosis. The procedures were followed our usual manner of the laparoscopic radical prostatectomy with the extraperitoneal approach.Results: All cases were completed without any severe complications. The pneumoperitoneum time was reduced to 214 min from 320 min. The mean blood loss was 150ml. Only a patient needed once analgesic after the surgery. The catheter was always removed for three days and all patients were discharged at five days after the operation. The last four patients were fully continent within one month after the surgery and all recovered their continence. Their PSA levels were undetectable in the short-term follow up.Conclusion: Our procedure of LESSRP is feasible and the learning curve is rapidly improved. Additional investigation is needed for the final optimization and to evaluate the oncologic adequacy.
Quality of Lymphadenectomy is Equivalent in robotic and Open Cystectomy Using an Extended Template
Introduction: Extended lymph node dissection (eLND) more accurately assigns nodal stage, removes more positive nodes, and may have survival benefit. Minimally-invasive cystectomy techniques have been criticized over ability to perform eLND. Objective: We determined whether the quality of eLND in robotic and open cystectomy is comparable by assessing node yield and positivity. Methods: eLND was performed in 120 open and 35 robotic cystectomy patients by a dedicated open or dedicated robotic surgeon. eLND was strictly defined as thorough skeletonization of anatomical structures in each nodal group below the aortic bifurcation, including common iliac, external iliac, obturator, hypogastric, and presacral node chains. The hypogastric nodes included skeletonization of the triangle of Marcille (presciatic space). Nodes from robotic cases were extracted and submitted as a maximum of two specimens while nodes from open cases were submitted as 10 packets. Results: Mean node count from open cases was 36.9±14.8 (range, 11-87). Only 12 of 120 patients (10%) had<20 nodes. In robotic cases, mean node yield was 37.5±13.2 (range, 18-64) with only 2 of 35 patients (6%) having<20 nodes. In the open group, 36 patients (30%) were LN + , and in the robotic group, 11 patients (31%) were LN + with comparable stage distribution. Among open surgical patients, 36% of patients received neoadjuvant chemotherapy as compared with 31% in the robotic surgery group. Conclusions: No difference was identified in the nodal yield and number of LN + patients when comparing open and robotic cystectomy with eLND. High-quality eLND is possible robotically.
Initial Experience with Robotic-assisted Radical Cystectomy: A Comparison of Major Outcome Parameters
Introduction: Robotic-assisted cystectomy is rapidly becoming an acceptable alternative to the open approach at high volume surgical centers. As more centers with robotic surgical capabilities begin to perform this procedure, concerns remain regarding initial outcomes.
Purpose: This study reports a comparison of major outcomes from our first 10 robotic-assisted cystectomies in comparison to 28 consecutive open radical cystectomies performed between 2009 and 2011.
Materials and Methods: A retrospective chart review of consecutive cystectomies at our institution between January 2009 and March 2011 revealed 10 robotic-assisted and 28 open cystectomies. Of the open procedures, half occurred prior to the first robotic case. Outcome measures included operative time, operative blood loss, hospital stay, major postoperative complications (>3Clavien-Dindo) and lymph node yield. Statistical analyses were performed (Mann-Whitney-U and Fischers exact test) to compare outcomes.
Results: There were no statistically significant differences between open and robotic-assisted laparoscopic cystectomies for patient age (64.6 robotic vs 62.6 open, p=0.759), mean operative time (408 min robotic vs 360 min open, p=0.259) or mean hospital stay (7.7 days robotic vs 11.1 days open, p=0.097). Median lymph node yield in procedures performed for cancer (10 robotic vs 8.5 open, p=0.249) and major complication rates (20% robotic vs 21% open, p=0.652) were also similar. Only mean operative blood loss showed a statistically significant difference (177 ml robotic vs 943 ml open, p>0.001).
Conclusions: Transition from open cystectomies to robotic-assisted laparoscopic cystectomies with trained robotic surgeons can be accomplished with similar intraoperative, postoperative and oncologic outcomes.
Laparoscopic Partial Cystectomy for Symptomatic Paraganglioma of the Urinary Bladder
Paragangliomas of the bladder are uncommon neuroendocrine neoplasms. As a result of its rarity, a standard operative method has not been established. An open partial cystectomy is usually performed because all layers of the bladder are involved. We report an initial case of laparoscopic partial cystectomy to minimize the surgical morbidity of the transabdominal approach and review the management of this condition. A 43-year-old female presented with symptomatic paraganglioma of the bladder. The patient was pretreated with alpha and beta-adrenergic blockers before laparoscopic partial cystectomy was carried out. A 4-port technique was performed with the patient in the Trendelenburg lithotomy position. The bladder mass was excised with a rim of normal mucosa under both cystoscopic and laparoscopic vision. The bladder was closed intracorporeally and the specimen removed through the 12mm right iliac fossa port. The operation was uncomplicated. Total operative time was 170 minutes and blood loss was less than 100 ml. The patients blood pressure remained stable throughout the operation. Normal diet was resumed 2 days after the operation and the patient was discharged with an indwelling catheter. A cystogram performed after the operation showed no leakage. The final histology showed a 6 cm paraganglioma with clear resection margins. Laparoscopic partial cystectomy is a feasible method of excising a symptomatic paraganglioma with adequate pre-operative adrenergic blockage to prevent a hypertensive crisis during resection.
Pelvic Lymph node Dissection in Laparoscopic Radical Cystectomy
Objective: We report our results of pelvic lymph node dissection in laparoscopoic radical cystectomy in our centre. Materials and methods: Laparoscopic pelvic lymph node dissection was performed according to the template proposed by Roth et al (2010) in patients with bladder cancer undergoing laparoscopic radical cystectomy in our centre since May 2010. Patient demographic data, operative data, pathology finding and post-op complications were recorded in a prospective database. Results: Eleven patients (7 male and 4 female; mean age 66years, range 51 to 84 years) received laparoscopic pelvic lymph node dissection from May 2010 to Jun 2011. On average an additional 2 hours required for the procedure. Mean total number of lymph nodes retrieved was 27.4 (9 to 50). 3 out of 11 patients turned out to have N2 disease and the rest of the patients have N0 disease. One patient was readmitted for serous discharge from drain wound which resolved with conservative treatment. Conclusion: Laparoscopic pelvic lymph node dissection using the proposed template yielded an adequate number of lymph node for N-staging in patients undergone laparoscopic radical cystectomy.
Laparoscopic Re-Implantation of right Ureter and Psoas Hitch
Introduction: The traditional treatment of ureteric stricture following injury and failed endoscopic management has been open urteric re-implantation. Few investigators have described laparoscopic ureteral re-implantation with varying techniques and short term success rates. Purpose:We describe our experience on a lady who had a total laparoscopic guided right ureteric re-implant with a psoas hitch for a failed endoscopic management of 3 cm ischaemic distal ureteric stricture.Materials and Methods:40 years female with past history of laparoscopic appendicectomy in March 2010 was diagnosed with a right distal ureteric stricture and hydronephrosis on intravenous urogram for right loin pain. She failed an attempt at endosopic balloon dilatation and stenting and underwent a successful laparoscopic right ureteric reimplant with a psoas hitch.3 port technique, laparoscopic adhesiolysis , mobilisation of the right ureter and bladder done, ureter divided and spatulated and psoas hitch done to the right psoas tendon. Uretero-neocystostomy performed .DJ stent then passed retrogradely from bladder into right kidney. Anastomosis was tested. No leak noted. Results: Minimal intra-operative blood loss. Patient was discharged on the second post-operative day. At 3 month out patient follow-up, she was asymptomatic with stable renal function and post-op IVU showed complete drainage of the right ureter with good renal function. Conclusions:Laparoscopic ureteric re-implant for this lady was successfully done replicating the open re-implantation principles with excellent outcome and nil morbidity.
Laparoendoscopic Single-site Surgery Varicocoele Repair (LESS-VR) - Initial Single Centre UK Experience
Laparoendoscopic Single-Site Surgery for Urachal Remnants
<Introduction> Urachal remnants are relatively rare but may potentially cause various symptoms and an increased risk for developing adenocarcinoma. Open or laparoscopic surgery is usually used for their resection.<Purpose> To fulfill the requirement for less invasiveness, laparoendoscopic single-site surgery (LESS) or single-incision laparoscopic surgery (SILS) has been developed, although there are not many reports that a urachal remnant was treated using the LESS or SILS procedure. We describe here our LESS procedure and discuss several useful ideas for excision of urachal remnants. <Materials and methods>Laparoendoscopic single-site surgery was performed transperitoneally via one port at sub-umbilical semi-circular incision using traditional non-flexible laparoscopic instruments except for a flexible camera. Two cases of vesicourachal diverticulum with a bladder cuff were completely excised under the supporting view of cystoscopy. <Result> The total operative duration was 140 minutes and 148 minutes respectivery. The intraoperative bleeding was minimal in both cases. The urethral catheters were removed after cystography on postoperative sixth and eighth day in each. There were no complications postoperatively. The small scar was almost invisible. <Conclusions> Our experience in two cases showed that our technique is safe, minimally invasive and has a good cosmetic outcome. Our LESS approach is an excellent option for the radical resection of urachal remnants.
Ergonomic tricks of Laparos-Endoscopic Single-Site Surgery by using Conventional Laparoscopic Instruments
Introduction: The laparoendoscopic single site surgery (LESS) procedure usually required extremely proximity of instruments through a fixed skin incision with limited range of movement, thus improving ergonomic of LESS is a critical issue.Objective: We reported our ergonomic principles when performing LESS with conventional straight laparoscopic instruments. Materials and Methods: LESS procedures were performed with a homemade single port, 30 degree laparoscope and conventional instruments. In order to minimize the chances of instrument clashing and enhance procedure efficiency, we have to keep one instrument static for tissue traction to provide enough space of movement for the other dynamic instrument for dissection. Then alternate the status of dynamic and static instrument flexibly to decrease the chances of instrument fighting. A video clip demonstrating the ergonomic tricks was included.Results: Between 2008 and 2011, 175 patients underwent LESS with the same ergonomic principles. All procedures were completed successfully without ancillary ports or articulating instruments except two cases that required laparoscopic conversion. The mean operative time was 99.7 minutes and mean hospital stay was 2.1 days. No intra-operative complication occurred.Conclusions: According to our ergonomic principles, conventional laparoscopic instruments is feasible and safe by following good ergonomic priniples.
Laparoendoscopic and Robotic Laparoendoscopic Single-Site Nephrectomy: Initial Series Outcomes
Introduction: Laparoendoscopic single-site surgery (LESS) has potential benefits over traditional minimally invasive techniques that include less pain, shorter recovery times and improved cosmesis.
Purpose: The purpose of this study is to report our initial experience with robotic and traditional laparoendoscopic single-site nephrectomies.
Materials and Methods: A retrospective review identified all patients who underwent a single-site nephrectomy at our institution. Two different multichannel ports were used for single-port access. Preoperative patient data included age, BMI, and indications for surgery. Intraoperative data included estimated blood loss (EBL), operative time, port used, and intraoperative complications. Postoperative data included pathology, postoperative complications, and length of hospital stay (LOS).
Results: Four laparoendoscopic and three robotic laparoendoscopic single-site nephrectomies were performed between November 2010 and June 2011. The median patient age was 39 years and median BMI was 25. Four cases were performed for enhancing renal masses and the remaining three were completed for chronic ureteropelvic obstruction with associated non-functioning kidney. Average EBL and operative time were 97 ml and 203 minutes respectively. One patient required an additional 5mm port for failure to progress. The same patient had a postoperative fever that delayed discharge. No additional complications occurred. Mean LOS was 3.1 days. All four patients with renal masses had a diagnosis of renal cell carcinoma with negative margins.
Conclusions: Transition from traditional laparoscopic and robotic nephrectomies to single-site surgery can be done with minimal complications and excellent initial oncologic outcomes.
Laparoendoscopic Single-Site Retroperitoneal Lymph Node Dissection:Initial Experience
Feasibility of Transrectal Hybrid Natural Orifice Transluminal Endoscopic Surgery (NOTES) Nephrectomy in a Cadaveric Model
INTRODUCTION: Natural orifice translumenal endoscopic surgery (NOTES) uses ports of entry to the abdominal cavity instead of abdominal wall incisions, thereby eliminating visible scar and potentially reducing postoperative pain. PURPOSE: We examined feasibility of transrectal hybrid NOTES nephrectomy in the cadaveric model.METHODS: 3 Hybrid transrectal NOTES nephrectomies were performed on 3 cadavers (2 female/1male, 2 right/1 left; median weight 78 Kg). Pneumoperitoneum was created by periumbilically-inserted 12-mm trocar, through which a laparoscope was advanced to obtain intra-abdominal visualization. 4-cm horizontal incision was made 2-cm above the dentate line and a submucosal tunnel was created in the posterior rectal wall/presacral space. A dual-channel gastroscope was advanced through the submucosal tunnel and retroperitoneum to the level of the kidney using air insufflation. A peritoneal window was created and renal mobilization was completed. Transumbilically applied mechanical clips and laparoscopic 45-mm stapler were used to transect the ureter and renal hilum, respectively. A specimen extraction bag was deployed transrectally with intact specimen extraction, followed by transrectal incision closure.RESULTS Transrectal hybrid NOTES nephrectomy was successfully performed in all cases. Mean operative time was 180 minutes (30 minutes rectal access). Median dimensions of removed kidneys were length 11 cm, width 5.5 cm, thickness 3.5 cm.CONCLUSIONS In this initial report on feasibility of transrectal hybrid NOTES nephrectomy in a human cadaveric model, we were able to perform the procedures with intact specimen extraction. Animal survival studies are prerequisite to assess sterility and complications. This approach may be useful as an alternative to transvaginal access.
Transrectal Hybrid Natural Orifice Transluminal Endoscopic Surgery (NOTES) Partial Nephrectomy in a Porcine Model
INTRODUCTION: Natural orifice translumenal endoscopic surgery (NOTES) uses ports of entry to the abdomen instead of abdominal wall incisions, eliminating visible scar and potentially reducing postoperative pain. OBJECTIVE: We examined feasibility of transrectal hybrid NOTES partial nephrectomy in the porcine model.METHODS: 3 female pigs (45 kg) underwent transrectal hybrid NOTES partial nephrectomy [TR-NOTES-PN; 2 right/1 left]. Pneumoperitoneum was created by periumbilically-inserted 12-mm trocar, through which a laparoscope was advanced to obtain intra-abdominal visualization. A horizontal incision was made 2-cm above the dentate line and a submucosal tunnel was created in the posterior rectal wall/presacral space. Dual-channel gastroscope was advanced through the submucosal tunnel and retroperitoneum to the level of the kidney using air insufflation. A peritoneal window was created followed by renal mobilization. Transumbilically-deployed Habib(TM) Bipolar Radiofrequency Coagulator (Angiodynamics) was used to perform lower pole heminephrectomy without ischemic vessel occlusion; parenchymal defect was sealed by Evicel fibrin sealant (Ethicon). Transrectally-deployed specimen extraction bag was used to extract intact specimen, followed by transrectal incision closure. Necropsy was performed to evaluate for intra-abdominal injuries and to harvest and assess renal remnants.RESULTS: TR-NOTES-PN was successfully performed in all 3 pigs. Mean operative time was 133 minutes. Mean TR access time was 38 minutes. Mean Estimated Blood loss was 43 mL. Mean volume of resected specimen was 10.12 cm3. Post necropsy renal remnants did not demonstrate resection site extravasation by ureterally-injected methylene blue; no intraabdominal injuries were noted.CONCLUSIONS: We demonstrate proof-of-principle for TR-NOTES-PN in swine. Further preclinical survival are requisite.
Transvaginal Natural Orifice Transluminal Endoscopic Nephrectomy in a Porcine Survival Model: Comparison with Conventional Laparoscopic Nephrectomy
Introduction: The clinical application of natural orifice transluminal endoscopic surgery (NOTES) is associated with several problems that need to be overcome.Purpose: We aimed to evaluate the technical feasibility, safety and physiologic impacts of transvaginal NOTES nephrectomy compared with conventional laparoscopic nephrectomy in a porcine model.Materials and methods: A total of 10 female pigs weighing 30 to 35 kg were randomized to receive transvaginal NOTES nephrectomy (n=5) or conventional laparoscopic nephrectomy (n=5). Postoperatively, all pigs were recovered and monitored for well-being during convalescence. Several laboratory and immunologic parameters were compared between two groups during the observation period. Re-exploration was performed 1 week after surgery for evaluation of intraperitoneal complications and cultures for microorganism.Results: All procedures were performed successfully without additional trocar insertion or any kind of conversion. Although total operation times were longer for transvaginal NOTES nephrectomy than for conventional laparoscopic nephrectomy (51 vs. 12 min, p<0.001), there were no evidence of peritonitis, intraperitoneal abscess, bleeding, or organ injury on re-exploration. All laboratory and immunologic parameters including white blood cell count, TNF-α, IL-1, and IL-6 did not differ between two groups during the whole observational period.Conclusions: Transvaginal NOTES nephrectomy could be performed successfully with well preserved immune function similar to those of conventional laparoscopic surgery as evaluated in a porcine model.
VP02: Robotic/Lap Adrenal and Kidney
Robot-Assisted Laparoscopic Ileal Ureteral Reconstruction for Bilateral Ureteral Strictures: Report of A Complex Case
OBJECTIVE: Description of a complex case of bilateral ureteral strictures managed with robot-assisted ileal ureteral reconstruction.METHODS:A 47-year-old female was referred to our center for management of bilateral ureteral obstruction, sepsis, acute renal failure and subsequent bilateral nephrostomy tube placement. This resulted from treatment for endometrial carcinoma with radical hysterectomy and extended pelvic lymphadenectomy followed by external beam radiation and intravaginal brachytherapy which resulted in bilateral iliac occlusion and subsequent aortobifemoral bypass. A robotic approach for repair was performed utilizing a 6 ports were placed in a fan distribution in the patients upper abdomen and an additional port in the left lower quadrant area for extensive lysis of adhesions. Bilateral ureteral lysis was performed. A 17-cm ileal segment was harvested for reconstruction with laparoscopic staplers (Endo GIA Universal Roticulator, Covidien, Autosuture, Norwalk, CT, USA). A side-to-side ileoileal anastomosis was performed to re-establish the continuity of the small bowel. Ureteroileal and ileovesical anatomosis were performed to connect the ureters to the ileal segment and then the ileal segment to the bladder dome. RESULTS:Operative time was approximately 5 hours. Estimated blood loss was 50 ml. Postoperative course was uneventful and the patient was discharged on postoperative day 4 and the catheter removed on postoperative day 14. At the 22-month followup, the patient had no hydronephrosis bilaterally with normal kidney function and without any complications. CONCLUSIONS:Robot-assisted laparoscopic ileal ureteral reconstruction for bilateral ureteral strictures is a feasible alternative to open surgery with potential for decreased morbidity in the postoperative period.
Robot-Assisted Laparoscopic Nephroureterectomy: Strategies and Outcomes
Background: A variety of techniques have been described in minimally invasive nephroureterectomy for radical surgical treatment of upper tract urothelial carcinoma. However, it involved 2 procedures (radical nephrectomy & distal ureterectomy) at opposite ends of the retroperitoneum, with no consensus on port configuration or patient positioning. We present surgical strategies and short-term outcomes of our initial 34 cases of robotic nephroureterectomy (RNU).Materials & Methods: From December 2007 to November 2010 a total of 34 cases of RNU were performed for upper urinary tract urothelial cancer. Three different robotic set-ups and patient positioning strategies depending on patients BMI and height, past surgical history, and location of the tumor were utilized. Patient demographics, perioperative parameters, operative strategies, pathologic data, and followup outcomes are summarized in table 1. Results: Surgical strategies included; redocking with patient repositioning, redocking without repositioning and neither repositioning nor redocking, in which 16, 13 and 4 patients were included respectively. Open bladder cuff excision was performed in a single patient.Conclusions: RNU offers the ability to perform minimally invasive nephroureterctomy effectively, even in complicated conditions. To date it is difficult for a single strategy to be applied for all RNU cases with equal operative and oncological efficiency.

Section of Laparoscopic and Robotic Surgery, Department of Urology, Frimley Park Hospitals NHS Foudation Trust, Surrey, UK.
Introduction: There has recently been an increase in detection of small (<or=4 cm) renal neoplasms. This has followed by the exploration of novel forms of minimally invasive therapies including Laparoscopic Guided Cryoablation (LGC) and Robot Assisted Laparoscopic Partial Nephrectomy (RALPN) in the treatment of these lesions. Purpose: We aim to report the early experience of LGC and RALPN in the management of small renal tumours in our centre.Patients and methods: Since 2008, 44 patients had LGC and 21 patients had RALPN using the da Vinci® Robotic platform. Intra-operative, post-operative and oncological outcomes were prospectively collected.Results: Patient mean age was 70 years (range:42-90) & 60 years (range:47-77) for LGC & RALPN respectively (P<0.05). No significant difference was identified in tumour size (LGC=26.72±1.219; RALPN=29.94±2.481, P=0.1970). Mean operative time was 146 mins (range:75-240) & 165 mins (90-240) for LGC & RALPN (P=0.0941). Mean blood loss was minimal in both with no patient requiring blood transfusion. For RALPN the mean warm ischemia time was 25 mins (range:11-40). Median hospital stay was similar being 1 night for both modalities. At a mean follow-up of 19 months for LGC, tumour recurrence was 3.1% (n=1) & RALPN=0. Conclusions: Both LGC and RALPN appear to be equally safe and effective in the management of small renal masses in selected patients.
Department of Urology, Faculty of Medicine, University of Miyazaki
Introduction: During transperitoneal laparoscopic radical nephrectomy, it can be difficult to ligate the renal artery because of the tumor size and location. Therefore, other optional methods for avoiding open conversion in this situation are required.Purpose: To investigate the effectiveness of scheduled hand assistance in transperitoneal laparoscopic radical nephrectomy using video imagery.Materials and Methods: A 43-year-old man had a left renal tumor and a 76-year-old woman had a right renal tumor. These tumors were approximately 10 cm in size, located in the lower half of the kidneys.Results: We first inserted the laparoscopic port lower than usual because we planned to change the port for hand assistance in the latter half of the operation. After having difficulty in finding the renal artery, we made an incision in the peritoneum at the lateral part of the kidney. The kidney fell forward. We were then able to ligate the renal artery from the rear of the kidney. We then began hand-assisted laparoscopic surgery while holding the kidney back because it was difficult to ligate the renal vein from the rear of the kidney. We successfully continued the operation while holding the kidney back by hand. Operating times were 5 hours, 18 minutes and 4 hours, 13 minutes. Estimated blood loss was 50 ml and 20 ml. There were no complications after these surgeries.Conclusion: We confirmed the usefulness of scheduled hand-assisted transperitoneal laparoscopic radical nephrectomy.
Laparoscopic Management in Ectopic Ureter
Introduction: Ectopic ureter presents different symptoms in infant, young child, and in adult. The management depends on precise diagnosis and the presentations of the patients.Purpose: To report the laparoscopic (LPS) management in ectopic ureter.Materials and Methods: The hospital records of patients with ectopic ureter undergoing LPS management between August 2005 and September 2010 were retrospectively reviewed. Surgical indications include prenatal hydronephrosis, continuous urine incontinence, and recurrent acute pyelonephritis. The operation methods include ureterectomy plus end-to-side ureteroureterostomy for a functioning kidney, and nephrectomy for an atrophic kidney.Results: 4 patients were included. 2 have double ureter with upper moiety hydronephrosis underwent LPS and laparoendoscopic single site (LESS) ureteroureterostomy, respectively. 2 have continuous urine incontinence: one underwent LPS ureterectomy plus ureteroureterostomy, and the other received LPS nephrectomy. The operation time are 265 minutes for LESS ureteroureterostomy in a young women with recurrent APN, 400 minutes for LPS ureteroureterostomy in a baby with prenatal hydronephrosis, 300 minutes for LPS ureteroureterostomy in a girl with continuous urine incontinence, and 180 minutes for the LPS nephrectomy. No post-operative complication happened. At a follow up from 4 to 27 months, the patients with urinary incontinence present no more wet pants. The 2 patients with hydronephrosis demonstrated improvement of symptoms and decrease in the grade of hydronephrosis on sonography.Conclusion: With this novel technique, the success rate of ureteroureterostomy is high, and the wounds are very small so that the patients recovered fast. LPS management for ectopic ureter is an effective and safe procedure.
Department of Urology, Saitama Medical University, Saitama, Japan
Background: Symptomatic ureterocele is usually diagnosed in childhood. But, ureterocele found in adulthoot with the episode of retention is very rare, even though 7.4% of urinary retention of children are complicated with ureterocele. We report a case of bulky ureterocele with dilated urinary tract diagnosed in adulthood treated by laparoscopic surgery.Method: A 43 years-old woman patient visited our department with the complaint of urinary retention.Left complete ureteral duplication with bulky ureterocele was diagnosed. Dilated ureter was also found through entire region up to bladder. The ureter from normal parenchyma was fused with dilated ureter at ureterocele.Results: Laparoscopic resection of duplicated tract and the ureterocele was performed. The dilated ureter and the atrophic upper pole of the left renal parenchyma were removed. Branches of the renal vessels into the superior pole of kidney were carefully incised. Following laparoscopic procedure, incision was added on lower abdominal wall. The isolated urinary tract fused with normal ureter in the bladder wall. Ureterocele was removed from bladder wall with dilated ureter. Ureteroneocystostomy was made. Discussion: As for the treatment of the ureterocele itself, TUR or incision of ureterocele is recommended, but VUR is known as a common complication, which would be a problem in this presented case because of dilated atrophic duplicated tract. Laparoscopic surgery could be chosen in this situation.
A case of Retroperitoneoscopic Nephroureterectomy in Urothelial Carcinoma with situs Inversus Totalis: Effect of pre-operative planning using Patient-Specific Simulator
(Introduction) Situs inverses totalis(SIT) is a rare, congenital anomaly associated both with vascular and visceral abnormalities and intestinal malformations. The majority of reports of laparoscopic procedures in patients with SIT cite technical difficulties and longer operative times due to disorientation from the reversed abdominal organs and the modification of the surgeon's movements and techniques.(Purpose) We are developing patient-specific simulator for laparoscopic renal surgeryand using it for the pre-operative planning. We present a case of retroperitoneoscopic nephroureterectomy in renal pelvis urothelial carcinoma with situs inversus totalis . Our patient specific simulator was used for the pre-operative planning. (Materials and Methods) We simulated 2 days before operation, using computed tomography scanning which we had 20 days before operation. We compared the actual anatomy of the operation with the imaging of our simulator.(Result) The insufflate time was 182 minutes and the estimate blood loss was 50 mL. We approached retroperitoneally and the lymphadenectomy was also performed. The operator could performed retroperitoneoscopic nephroureterectomy safely without feeling lost. Our simulator demonstrated situs inversus totalis with a left-sided inferior vena cava and an aorta right of the midline. There were two renal arteries to the right kidney and a right renal vein ramifying an adrenal vein, a lumber vein and a gonadal vein. The actual vascular anatomy of the renal hilum was same as the imaging of our simulator. (Conclusion) Pre-operative planning using patient-specific simulator was useful for a case of retroperitoneoscopic nephroureterectomy in renal pelvic urothelial carcinoma with situs inversus totalis
Department of Urologic Surgery, Sapporo Medical University, Sapporo, Japan
Purpose: To develop a new technique for closure of the renal parenchyma in laparoscopic partial nephrectomy shortening the suturing time.Patients and Methods: Between 2008 and 2011, 58 patients with renal masses 4 cm or smaller in diameter underwent transabdominal laparoscopic partial nephrectomy by a single surgeon in a single institute. The suturing technique of the renal parenchyma was changed from interrupted sutures without ligation for the initial 9 patients (group A), running sutures for the next 9 patients (group B) and interrupted sutures with ligation using felt, a Hem-o-lok and a Lapra-Ty for the last 39 patients (group C). For group C, the sutures were done using 2-0 vicryl CT-1 with a 1.2 x 1.2 cm piece of felt and both sutures were temporarily held using a Hem-o-lok. After all sutures (2 to 5, median 3) were completed, they were sequentially fixed by sliding the Hem-o-lok, and then locked using the Lapra-Ty. Results: The median times for suturing the renal parenchyma were 36, 30 and 13 min. for groups A, B and C, respectively. Corresponding to the suturing time, the median ischemic time in group C (28 min.) was shorter than in groups A (69 min.) and B (54 min.). The arrangement of the wound and hemostasis were excellent in group C. No patients developed urinoma or postoperative bleeding.Conclusions: The method of interrupted sutures using felt, a Hem-o-lok and a Lapra-Ty is an easy, time-saving and safe procedure even for surgeons who are not experts in intra-abdominal suturing.
Department of Urology, National University Health System, Singapore
Introduction:Robotic assistance may augment partial nephrectomy by aiding in dissection and renal reconstruction, especially if difficulty is anticipated due to unfavourable location, larger or complex tumours. Purpose: We aim to review the surgical techniques of robotic assisted laparoscopic partial nephrectomy (RALPN) performed for complex renal masses. Materials & Methods: Patient records were reviewed for 3 patients who underwent RALPN for complex renal masses in a single institution.Results: Case1: 44 year old female with a 6 cm angiomyolipoma in the lower pole of her left kidney. Only the lower pole segmental renal artery was clamped prior to tumour excision. Case2: 59 year old female with a 4.7x4.2 cm (T1b) renal cell carcinoma at the interpolar part of the right kidney. The tumour was deep and in close proximity to the renal vein. Case3: 59 year old female with a 1.6 cm renal cell carcinoma which was mostly (95%) endophytic, in the lower pole of her left kidney. Excision was performed using intra-operative ultrasound guidance. The average operative time was 97 minutes, average warm ischaemia time was 20 minutes and blood losses were minimal. There were no intra- or post-operative complications and the mean hospital stay was 4.3 days. Compete excision of renal tumours with resection margins negative for malignancy, were achieved in all cases. No recurrence is seen on CT imaging after a mean of 10 months follow-up.Conclusion:Robotic assistance with modified technique can produce reasonable results for patients undergoing laparoscopic partial nephrectomy for complex renal tumours.
Tokyo Women's Medical University Medical Center East, Tokyo, Japan
Retroperitoneal neural tumors are rarely excised laparoscopically. We report a case of retroperitoneal tumor treated by laparoscopic surgery using the four-trocar technique. A 64-year old woman presented with a mass in the retroperitoneal space that was incidentally revealed by abdominal echography. Computed tomography showed a mass 60mm in diameter in the retroperitoneal cavity which had a cystic component. With a diagnosis of retroperitoneal tumor, laparoscopic resection was performed. Pathological diagnosis was Neurilemmoma. Although difficult to diagnose preoperatively, neural tumors in the retroperitoneal space are most often benign, with a good prognosis. Retroperitonel tumors are commonly localized and hypovascular,and they can easily be dissected from the adjacent tissues. Laparoscopic surgical techniques for retroperitoneal tumors are safe, less invasive and useful.
Robot-Assisted Partial Nephrectomy using Barbed Suture for Renorhraphy
IntroductionBarbed suture allows for knotless wound closure and improves suturing efficacy. We present our results of barbed suture for renorrhaphy robot-assisted partial nephrectomy (RAPN). Patients and MethodsTwo male patients were referred to our hospital for right renal mass. CT scan showed right renal mass in both patients. The diameters were 2.5 cm and 1.6 cm, respectively. Robot-assisted partial nephrectomy was planned. The usual robot-assisted transperitoneal approach was utilized. Tumor excision was begun with scissors through the full-thickness renal cortex to reach renal medulla and sinus fat with renal artery clamping, using bulldog clamps. Renorrhaphy was performed in two layers. We used 15-cm 3-0 V-Loc sutures on V-20 needles for the inner renorrhaphy layer and 30-cm 2-0 V-Loc sutures on GS-21 needles. These sutures were run continuously. ResultsMean operative time, console time and warm ischemia time were 270 min, 315 min and 20 min, respectively. No complication was occurred during operation. The decrease ratios of eGFR a week after operation were 17.2 % and 1.9 %, respectivelyConclusionsUse of barbed suture during RAPN improves suturing efficiency, allowing for short warm ischemia time.
University of Modena & Reggio Emilia, Policlinico di Modena, Modena, Italy
Purpose: The Boari flap is appropriate when long strictures of the ureter must be bridged. We report our preliminary experience and surgical technique of creating a "mega Boari flap" to bridge renal pelvic and long proximal ureteral strictures.Methods: From March 2010 to May 2011, four patients underwent laparoscopic mega Boari flap ureteroneocystotomies. The bladder was fully mobilized by incising the peritoneum lateral to the obliterated umbilical arteries, the urachus, and the vascular pedicle on the contralateral side. A modified Boari flap was created, transversely along the anterior bladder wall. Following several releasing incisions into the bladder flap, it was transposed cranially. Finally, the mega Boari flap was rolled and anastomosed to the renal pelvis and closed longitudinally over a 7Fr x 28cm double-J ureteral stent. Results: All procedures were successfully performed laparoscopically without any intraoperative complications or need for open conversion. Perioperative data is presented in Table #1. Postoperative cystography revealed patency in all cases demonstrated by vesicoureteral reflux.Conclusion: Laparoscopic mega Boari flap is feasible. The most important technical considerations are extensive bladder mobilization, formation of a large transverse bladder flap, and releasing incisions providing a longer tubularized segment than in the classic Boari technique.
Selective Arterial Clamping with the Assistance of near Infrared Fluorescence Imaging for Robotic Assisted Laparoscopic Partial Nephrectomy
Introduction: Isolating the area of ischemia to only the tumor and surrounding tissue may lead to improved renal preservation during partial nephrectomy.Purpose: To assess if selective arterial clamping using near infrared fluorescence (NIRF) is a safe and feasible method of improving renal preservation during robotic assisted laparoscopic partial nephrectomy (RALPN).Methods: Between March 2011 and June 2011, 13 patients underwent RALPN and NIRF. NIRF was achieved using the daVinci video fluorescence system with real-time indocyanine green (ICG) angiography. Secondary and tertiary vessels leading to the tumor were clamped and NIRF was utilized to assess for adequate ischemia to tumor.Results: Selective arterial clamping was achieved in 6/13 patients (46%). The remaining 7 were limited by technical factors (bleeding 2, multifocality 2, hilar location 3). In these cases NIRF was used to assist in dissection and to confirm ischemia. Outcomes of selectively clamped cases were comparable to our prior experiences, see Table 1. There were no intraoperative complications and all surgical margins were negative.Conclusions: Selective arterial clamping during RALPN is feasible and safe.

Factors that Influence the Surgical Outcomes of Retroperitoneal and Transperitoneal Approach for Laparoscopic Surgery of the Renal Tumors
Objective of this paper is to investigate several technical and morphological factors that might influence the outcomes of the laparoscopic surgery for renal tumors.Material and method. From a total of 94 patients that underwent surgery for renal tumors in the last 3 years at our institution in 20 patients laparoscopic surgery was performed. 14 patients underwent laparoscopic radical nephrectomy (LRN) and 6 patients laparoscopic partial nephrectomy (LPN). The aproach was retroperitoneal and transperitoneal. The parameters followed were: mean operative time, mean tumor size, warm ischemia time, position of the renal tumor, the percentage of exophitic part, clinical and pathological stage.Results. Mean operative time for LRN was 116 min (115 vs 119 min TP vs RP) and 212,6 min for LPN ( 212,6 vs 212,5 TP vs RP). The mean tumor size and warm ischemia time did not differ between the transperitoneal and retroperitoneal aproaches. The clinical and pathological stage was not correlated to the duration of the operation. The percentage of exophitic part of the tumor was correlated with the duration of warm ischemia time for laparoscopic partial nephrectomy, but did not influence the outcomes of the radical nephrectomy.Conclusions. The percetage of exophitic part of the tumor seems to influence the duration of the warm ischemia time in laparoscopic partial nephrectomy. There were no significant differences between the transperitoneal and retroperitoneal aproaches with regard to the operative time, clinical and pathological stage, tumor size and position of the tumor.
Section of Laparoscopic and Robotic Surgery, Department of Urology, Frimley Park Hospitals NHS Foundation Trust. Surrey. UK
Division of Urology, Department of Surgery, Shin Kong WHS Memorial Hospital, Taipei, Taiwan
Purpose: We report our series in retroperitoneoscopic adrenalectomy with a modified approach.Materials and Methods:From April, 2005 to February, 2011, 93 retroperitoneoscopic adrenalectomies were performed by a single surgeon with modified approach. The surgical technique started with posterior dissection along the psoas muscle and then to the peritoneum anteriorly. The dissection carried on to the plane between kidney upper pole and the adrenal gland. The main adrenal vein was controlled after all the steps were completed. The demographic, pre-operative parameters, operative and post-operative details were collected retrospectively and analyzed. Results:Among the 93 patients, 52 were females with a mean age of 50.9±12.5 years old. Forty-nine lesions were located at left side. Mean OP time was 125±40 minutes and mean blood loss was 99±109 ml. Complication rate was 4.3% (4/93) and complications were fever in 2, 1 wound infection and 1 pancreatic injury. Conversion rate was 1% (1/93) in the patient of pancreatic injury. The patients were divided into 3 groups according to the timeline, OP time was significantly shorter while the experience increased (148 vs. 127 vs. 101 minutes, p<0.001). However, no difference can be observed in the blood loss and length of stay. Complication rate was 0% in the recent 40 patients. No difference in intra-OP parameters between left side and right side. Conclusion:Retroperitoneoscopic adrenalectomy with this technique is a feasible and safe. Learning curve improves while experience increases. Complication rate is low and post-operative outcome is good.
VP03: Prostate Diagnosis/Urotherial Cancer/Education
STILUS Academic Research Group (SARG). London. U.K.
Introduction: There is increasing demand for optimisation of skill acquisition of robotic upper tract urological skills. We developed a training model with the incorporation of the novel concept of Predictive Video Training also called the Next Step Approach. Purpose: To test the concept of Predictive Video Training using the Next Step Approach in urological trainees using the robotic platform. Materials and Methods: The study involved the tutoring of trainees interested in robotic renal surgery by means of one to one scrutiny of video footage on a desktop computer. Each of two mentors sat next to each of four trainees (with intermediate level laparoscopic skills) and scrutinised video recordings of previously documented/recorded cases of Robot Assisted Pyeloplasty(RAP), Robot Assisted Partial Nephrectomy(RAPN) and Robot Assisted Nephroureterectomy(RANU). Each training session was such that as the case progressed in a linear fashion on the video, the mentor paused the session and queried the candidate in a structured format regarding his/her Next Step that the candidate would take. Two trainees were taken through the next step approach and two were not. At the end of the sessions, the candidates were mentored through the live human cases of RAP, RAPN and RAPN. Performance was objectively scored. Results: Candidates who were primed with Predictive Video Training using the Next Step Approach were noted to perform better overall with higher scores compared with the non primed group. Conclusion: Predictive Video Training using the Next Step Approach is a useful supplementary tool for skill acquisition in robotic renal surgery.
STILUS Academic Research Group (SARG). London. U.K.
Introduction: We previously built and tested the concept of advanced skill acquisition in the conventional laparoscopic surgery model using a Hostile Environment Platform (HEP) [WCE 2010 Chicago]. Herein, we applied the same to the ex vivo utility of the da Vinci Robot. Purpose: To build and test the impact of the HEP using the robot model. Materials and Methods: The Learning Platform consisted of a box kit and da Vinci robot such that a trainee would practice advanced target tasks including ex vivo vesicourethral anastomosis(VUA), dorsal vein complex(DVC) ligation, Pyeloplasty and Partial Nephrectomy using the concept of Levels of Models (J Endourol.2007,21(s1):A1-A292). The HEP consisted of application of tandem stressors such as noise, smoke at target site, distraction via excess camera shake and other parameters. The impact on the learning curve was studied in 4 trainees. Two were made to practice without the HEP and two with HEP. Following 10 hrs. of practice on each target task, each trainee was required to undertake standard Non-HEP VUA, DVC ligation, Pyeloplasty and Partial Nephrectomy. The times for task completion and individual metrics were tallied. Results: Trainees from the HEP group performed the individual target tasks of VUA, DVC ligation, Pyeloplasty and Partial Nephrectomy in the ex vivo setting 2.8, 3.7, 3.5 and 3.6 times quicker respectively with better metrics in the test than those who initially practiced on the Non-HEP group. Conclusions: Candidates who trained on the Hostile Environment Robotic Platform had shortened times and better overall target task performance.
Construct and Concurrent Validation Study of a Virtual Reality Robotic Simulator
Background:Virtual reality simulators are often utilized for surgical skills training. In order to be considered useful for assessment purposes, rigorous criterion validity testing is required.Purpose:We conduct concurrent validity testing of a commercially available robotic surgical simulator; dV-Trainer™; (dVT).Methods:Urology residents, fellows, and attending surgeons were enrolled in this IRB-approved study. Subjects first completed 3 repetitions of 4 different tasks (PB, MB, NT, RR) on the dVT. One week later, subjects completed 4 similar tasks using the da Vinci(R); robot (dVR). For each exercise, participants were assessed on total task time as well as total errors using the built-in scoring algorithm or manual scoring for the dVT and dVR, respectively. Results:13 novice (NRS) and 7 experienced robotic surgeons (ERS) were included in the study; ERS defined by>50hours of robotic console time. ERS outperformed NRS in many of the dVT and dVR exercises, particularly with respect to number of errors (see table). On pooled data analysis, both dVT total task time and total errors correlated with dVR total task time (p=0.026) and total errors (p=0.011), respectively.Conclusions:This study demonstrates that in addition to face, content, and construct validity, the dV-Trainer™; also has concurrent validity.

Development of an Intraoperative Navigation System using A Magnetic Tracking System for Laparoscopic Nephrectomy
<Introduction> Recent developments in technology related to three-dimensional (3D) CT provide a wealth of information about renal shape, hilar anatomy and tumor location. Real-time navigation systems, in which 3D CT images are synchronized with the laparoscopic view, would be helpful in increasing safety in surgical procedures as well as increasing knowledge in teaching situations. With this in mind, we have developed a novel intraoperative real-time navigation system for laparoscopic nephrectomy. <Methods> The free DICOM viewer OsiriX was used to generate volume rendering images from preoperative CT data. This required positioning and angle information from a laparoscopic camera to synchronize the 3D CT image with the laparoscopic image in real-time. A magnetic tracking system was used to detect the position, direction and angle of the sensor cord tip. The sensor cord was attached to the grip of the laparoscopic camera, which allowed information from the tip of the camera to be calibrated. The laparoscopic virtual view and camera image were displayed on a secondary monitor positioned next to the main monitor. <Results> 3D imaging of the hilar anatomy, inferior vena cava and aorta matched the direction of the camera view. Our system can successfully synchronize the virtual laparoscopic image with the intraoperative laparoscopic view. <Conclusions> We conclude that our navigation system could be a useful tool in increasing safety in surgical procedures. In future, we would like to use this system to increase our understanding of renal hilar anatomy and to examine the usefulness of our system in other applications.
The GreenlightSim Trainer Demonstrates Acceptability, Face, Content and Construct Validity
Reliabilty, Face, Content and Construct Validation of the Computer Assisted Laparoscopic Surgical Simulator UROBOX
Introduction: UROBOX laparoscopic surgical simulator was developed as an objective computer assisted training tool for the trainees at the beginning of the learning curve in laparoscopy.Objective: The objective of this paper is to present the reliability testing and face, content and construct validation of the UROBOX computer assisted surgical simulator.Material and methodThere were three groups of participants; the first one consisted of 20 medical students without any experience in laparoscopy, 10 residents in training with basic laparoscopic skills and 5 experts in laparoscopy. The participants were asked to perform 4 tasks on the UROBOX simulator: touching a fixed point, following of the 2D track, following of a 3D track and intracorporeal suturing. The computer automatically calculated the score for each task and decided when to advance to the next level of training. Standardized questionnaires were used for face and content validity. ResultsFace and content validity was confirmed by answering a standardized questionnaire by the participans in the study. Reliability (r>0.85) was confirmed by interobserver, intraobserver, and test-retest method. There was a statistically significant difference (p<0.001) in the UROBOX scores between the three groups, and also there was a significant improvement over time in the scores in the first two groups (p<0.002), evidence of construct validity. ConclusionsThe UROBOX simulator is a reliable objective tool for teaching laparoscopy and assessing the progress on the learning curve. The validity of the UROBOX simulator was demonstrated for face, content and construct criteria.
STILUS Academic Research Group (SARG). London. U.K.
Introduction: Preliminary consensus is resounding in that Laroendoscopic Single-Site Surgery (LESS) requires technical expertise with an even narrower margin for error than conventional laparoscopic urological surgery (LUS). We previously found that dexterity and skill with cross hand instrument manipulation is a valuable tool for target task completion in LESS (ASIT 2010). Purpose: We developed and tested a model for training in LESS by means of a Stepped or graduated Skill Acquisition Platform for Cross Hand Flexible Instrument Manipulation. Materials and Methods: Articulating needle holders and scissors were used to perform preset tasks with hands crossed such that triangulation was achieved for task completion. The instruments were deployed in a purpose built LESS platform consisting of a box model (DIY-LTK) which was fitted with an R-Port. The training model required each of 4 novices to undergo a Three-Point Stepped regime i.e. Step 1-basic exercises using the nondominant hand only for 20 hrs; Step 2-basic exercises using both hands without crossing for 20 hrs; Step 3-cross hand exercises including glove pattern cutting, loop stacking and suturing for 20 hrs each. The test index task was to perform a vesicourethral anastomosis in a wet format. The Stepped regime candidates were compared to four other novices who were asked to perform the index task from the outset following matched time for practice. Results: Trainees who were taught on the Stepped regime were able to perform the index task 4.3 times quicker compared to the control group. Conclusions: Stepped Skill Acquisition for Cross Hand Flexible Instrument Manipulation in LESS permits target task completion at a much quicker rate compared to the conventional approach and could be a useful tool in training programmes.
Human versus Robot: Who can perform more accurate prostate biopsy?
Introduction: Prostate biopsy is typically performed freehand with a transrectal ultrasound (TRUS) guidance. However, the spatial distribution of TRUS-guided sextant biopsy cores is unknown. Using a biopsy simulation system, we compared the accuracy of the biopsy core distribution by urologists and a novel robot that holds and manipulates TRUS probe (TRUS Robot). Methods: A simulation model was built to accurately measure in-vitro biopsy locations using a custom-built gelatin-based pelvic mockup and an optical tracking system. The gold standard was defined using 12-core biopsy plan. We determined how accurately 5 experienced urologists and the TRUS Robot can perform a biopsy compared to the gold standard. Results: The simulated biopsy cores by urologists were generally clustered and a large portion of the prostate gland was often undersampled. The average error was approximately 9 mm. The simulated biopsy cores by the TRUS Robot were consistently accurate compared to the gold standard and uniformly distributed. Conclusion: Freehand TRUS-guided prostate biopsies may not closely follow sextant biopsy scheme. TRUS Robot can provide uniform sampling during TRUS-guided prostate biopsy.
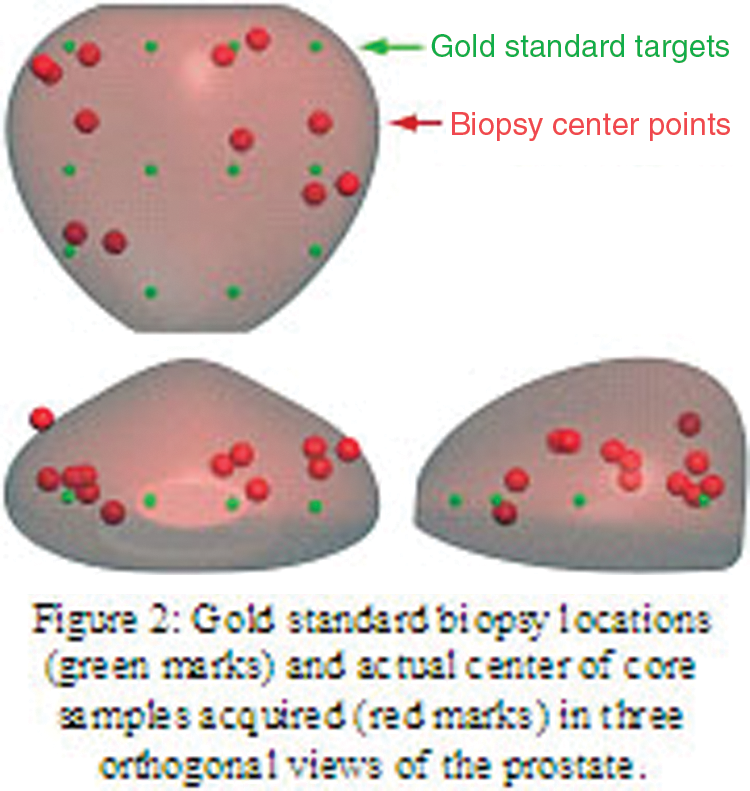
Histopathologic Correlation Using MRI-Based Specimen Molds to Determine the Positive/Negative Predictive Value of Multiparametric 3T MRI of Prostate Cancer
We report the correlation of whole mount histopathology (WMH) with multiparametric (MP) MR imaging in patients with a prostate cancer.METHODS: 45 patients, mean age 60.2 years, with a mean PSA level of 6.37 ng/mL, who had been diagnosed with prostate cancer. All patients underwent MP MRI (T2, DWI, MRS, DCE)of the prostate on a 3 Tesla scanner using cardiac and endorectal coils. Using imaging, patient specific MRI based specimen molds were created. The specimen was sliced in 6mm sections in the customized 3D mold. Tumors were mapped prospectively on MP MRI and WMH separately and independently blinded to all results. The customized mold provided tissues blocks that have one to one correspondence to the in vivo MR images. PPV and NPV of the MRI were calculated in peripheral zone and central gland. RESULTS: PPV and NPV values of MRI sequences in different prostate zones are presented in Table 1. CONCLUSION: The use of the custom mold enables more exact correlation between each MR parameter and the histopathological specimens. The mold is the key in supporting the validation of MP MRI in the screening and diagnosis of patients with prostate cancer due to its ability to perform a stringent correlation.

University of Cincinnati College of Medicine
Introduction: Improved MR accuracy for detection of ECE is desirable given the therapeutic decision making process changes radically when an organ-confined versus extracapsular disease is faced.To the best of our knowledge, our study is the first to describe PT-NVB by DTI and to show its relevance in ECE detection. Methods: A total of 15 patients with biopsy-proven prostate cancer who underwent endorectal prostate MRI at 3T (Signa GE Medical Systems, Milwaukee, Wis) followed by robot-assisted radical prostatectomy between 2009 and 2011 were included in this study. Transverse DTI covering the entire prostate and seminal vesicles were obtained by using a single-shot echo-planar imaging sequence with the same slice location as the T2 sequences. One body-imaging fellow (HM) post-processed DTI in a dedicated workstation using BrainLab Software (iPlan v2.6, Feldkirchen, Germany). Accuracy of T2-WI and DTI findings was validated by final pathology assessment of cross-section prostatectomy slides by a single uropathologist. Logistic regression with SPSS software was used for statistical analysis.Results: Mean patient's age was 60.4±8 years (range: 48-75). The comparative efficacy T2-WI and DTI alone and in combination to detect ECE presented in table. T2-WI (%) DTI (%) T2-W1 + DTI (%)Sensitivity 100 57.1 57.1Specificity 37.5 87.5 100Positive predictive value 58.3 80 100Negative predictive value 100 70 72.7Accuracy 66.7 73.3 80Conclusion: The addition of DTI findings to T2WI can improve the accuracy of MR imaging in ECE detection.
Conservative Management of Upper Urinary Tract Transitional Cell Carcinoma (Retrograde Endoscopic Treatment with mean follow up of 4 years)
Objective: To evaluate the clinical outcome after a conservative treatment of upper urinary tract transitional cell carcinoma (UUT-UCC) using retrograde endoscopic surgery with holmium laser.Patients and methods: records of 64 patients treated between 2004 and 2010 were retrospectively reviewed. All patients underwent retrograde flexible ureterorenoscopy treatment. Sex, age, ASA score, anatomical variation, single or multiple tumor, concomitant bladder cancer, tumour localisation, tumour size, stage and grade, recurrence, and progression were evaluated. Results: The mean age was 65 + /-14.6 years (range: 37-88). The tumour involved the renal pelvis and the caliceal system in 37 cases (57.8), the ureter in 12 cases (18.7%), and both in 15 cases (23.5%). 21 patients (32.8%) had a history of bladder carcinoma. Tumor stage was superficial in 63% (57% were pTa and 6% were pT1) and not available in 37%. Tumor grade was low, high, and unavailable in 49, 14, and 37%, respectively. The median follow-up was 47 months (range: 12-66), and 38 patients had a recurrence (59%). The median survival rate without recurrence was 10 months. Four patients underwent nephroureterectomy during follow-up. One patient died of disease progression. The main limitation was the limited length of follow-up. Conclusions: Conservative treatment is preferred in patients with bilateral disease, a solitary kidney, or co morbidities that contraindicate major surgery. Because of a high recurrence rate, long-term surveillance is recommended.
Ureteral Stent Complications: Evaluation on 3.501 Procedures
Introduction: Ureteral JJ stenting has well-known indications, value and advantages but may also determine a specific pathology. Purpose: To evaluate the complications related to this procedure.Material and Methods: Between January 2000 - January 2011, in our department were performed 3.501 JJ stent insertions (3282 unilateral and 219 bilateral). This procedure was indicated either for renal drainage or as complementary maneuver following endoscopic, laparoscopic or open surgery. The stent insertion had been done by endoscopic approach (3293 procedures) and during laparoscopic or open surgery (208 procedures). 546 of the procedures (15.6%) were performed in emergency. Results: Complications rate associated to ureteral stenting was 14.4%: stent ascension (0.3%), descendant migration (2.6%), spontaneous elimination (0.3%), calcification of the inferior loop (1.1%), calcification of the superior loop (0.4%), calcifications of both the inferior and superior loop (0.3%), calcification of the inferior loop and the ureteral segment of the stent (0.2%), calcification of the superior loop and the ureteral segment of the stent (0.1%), calcification of the entire length of the stent (0.2%), persistent hematuria (0.9%), stent fracture (0.2%), symptomatic vesico-ureteral reflux (7%), fever (0.8%), perirenal haematoma due to superior calyx perforation (0.04%). Endoscopic surgical treatment was necessary in 87 cases (2.5%). Conclusions: Ureteral JJ stenting is a minimally invasive procedure but associated with specific morbidity. Most of these complications may be endoscopically solved. In order to reduce complications rate, stented patients must be monitored after the procedure.
Treatment Changes and Long-Term Recurrence Rates after HAL Fluorescence Cystoscopy: A Prospective, Randomized, Long Term Comparison to the Standard Approach
Introduction: A prospective, randomized, long term comparison between hexaminolevulinate blue light cystoscopy (HAL-BLC) and standard white light cystoscopy (WLC) was performed. Purpose: The study aimed to evaluate the impact of this method concerning the diagnostic accuracy, treatment changes and recurrence rates in cases of non-muscle invasive bladder cancer (NMIBC).Materials and Methods: A total of 362 NMIBC suspected patients were included in the trial based on positive urinary cytology and/or ultrasonographic suspicion of bladder tumors. The 181 patients of the BL series underwent both WLC and BLC. The follow-up protocol consisting of urinary cytology and WLC was performed for a period of two years. Results: HAL-BLC emphasized significantly improved CIS, pTa, pT1 and overall cases and tumors detection rates. Additional tumors were found HAL-BLC in a significantly higher proportion of cases (35.2% versus 14.1%). Consequently, the recurrence and progression risk categories of patients changed significantly due to HAL-BLC results (16.2% and 21.1% versus 4.9% and 7%, respectively). The postoperative treatment was modified due to HAL-BLC for a significantly larger proportion of patients by comparison to WLC (19% versus 6.3%). The overall 3 months, one and two years recurrence rates were significantly reduced in the BL group (7.2% versus 15.8%, 21.6% versus 32.5% and 31.2% versus 45.6%, respectively). Conclusions: HAL-BLC emphasized superior patients and tumors detection rates in NMIBC cases, as well as a significant impact in terms of postoperative treatment modifications. The 3 months, one and two years recurrence rates were significantly improved in the BL arm.
Prospective Evaluation of Routine Fluorescence Cystoscopy Demonstrates Significantly Increased CIS Detection
The Staging Role of 18FDG PET-CT in Patients with Muscle-Invasive Bladder Cancer Selected for Radical Cystectomy.
Introduction: Preoperative staging of patients with muscle invasive bladder cancer includes either CT scan or MR imaging. Few reports addressed the staging role of 18FDG PET-CT and its role has not been defined. Methods: Between November 2010 and May 2011, 35 consecutive patients with muscle-invasive bladder cancer and conventional imaging negative for nodal or distant metastasis, underwent 18FDG PET-CT before radical cystectomy. Four patients, excluded from the analysis due to the evidence of bone metastases at PET-CT, underwent palliative cystectomy, all other patients underwent radical cystectomy and extended lymph-node dissection 2cm over the aortic bifurcation. Nodes were sent to pathologist into separate packages (obturator, internal iliac, external iliac and common iliac, presacral, paraaortic, paracaval). We tested sensitivity, specificity, PPV and NPV after matching 18FDG PET-CT results with pathological examinations of nodal packages removed. Results: Nodal packages removed were 284. At pathological staging, according to 2009 TNM staging system, 19 patients were pN0, 2 patients were pN1, 5 patients were pN2 and 5 patients were pN3.Positive sites detected by 18FDG PET-CT were confirmed by histology in 38 cases and were not in 6 cases, while 226 sites were true negative versus 14 one false negative (8 cases of nodal micrometastasis).Sensitivity, specificity, PPV and NPV were 73%, 97.4%, 86.3% and 94.1%, respectively. Conclusions: In our experience 18FDG PET-CT provided an excellent preoperative staging, allowing us to exclude 4 patients due to the presence of clinical metastasis and had a 97.4% specificity rate on detection of nodal involvement.
VP04: Urolithiasis
Dornier MedTech Systems, Wessling, Germany
Division of Urology, Duke University, Durham, North Carolina, USA
Introduction: Various methods have been employed to obtain improved stone comminution during shock wave lithotripsy (SWL). We evaluated the effects of respiratory motion in an in vitro model with an electromagnetic lithotripter, incorporating both an original acoustic focusing lens and a newer lens modified to have a focal size that better resembles that of the Dornier HM3.
Methods: Spherical BegoStone phantoms (44 trials with each lens) were placed in a flat-based cylindrical tube and set into translational motion with various excursion distances (15 or 30mm), respiratory rates (12, 18, and 24 bpm), and various drift factors. Drift simulated variability in kidney excursion or small patient movements. Stone comminution tests were performed with both lenses at equivalent acoustic energies.
Results: In 5 of 6 configurations tested, the new lens statistically improved stone comminution (p<0.01) compared to the original lens design. With low drift (<5mm) conditions, the new lens produced higher stone comminution. For both lenses, lower respiration rates and lower excursion distances were associated with better stone comminution (except for high drift patterns with the new lens). Notably, motion patterns producing a maximum drift >5mm in the direction of simulated inhalation (inferior direction) resulted in worse stone comminution efficiency (p<0.02), compared with all other drift conditions.
Conclusions: Comminution efficiency has a strong dependence on excursion distance, respiratory rate, and stone drift. Despite these differences, the new lens produced better stone comminution. Combined with more studies of patient movement during SWL, better stone comminution can be achieved in the future.
Day Surgery Laparoscopic Ureterolithotomy: The First Experience in Vietnam After 100 Cases
To define the feasibility of day surgery laparoscopic ureterolithotomy in the treatment of impacted upper ureteral calculi.
From June 2009 to June 2011, retroperitoneoscopic ureterolithotomy was performed as a primary procedure in 100 patients with large impacted upper ureteral calculi. The mean (range) age was 63 years old (25 to 88 years old) and the mean (range) stone size was 18mm (13 to 28mm). The ureter was closed with intracorporeal laparoscopic suture after antegrade insertion of a DJ stent. There was no retroperitoneal drainage after operation. Patients were discharge whenever they are met by the discharge criteria of IAAS.
Stone removal was successful in 100% of cases. The mean (range) operative time was 51 minutes (40 to 70 minutes). No intraoperative complications were recorded. Sixty patients can discharge from hospital after a mean (range) post-operation time of 6.2 hours (6.5 to 10.2 hours). The rest of the patients had a mean (range) post-operation time of 22.4 hours (15 to 23.5 hours). Postoperative complications included prolonged urinary leakage in 2 patients and macroscopic haematuria in 10 patients.
Day-surgery retroperitoneoscopic ureterolithotomy is safe and feasible. This minimally invasive treatment is now considered as first-line management for large impacted upper ureteral calculi in Vietnam
PCNL and Nephroscopic Decortication of Parapelvic Cyst
This is a novel description of percutaneous renal cyst decortication during PCNL in a suitably selected patient, without significant complications and with excellent outcome. The patient with an upper pole calcyceal calculus caused by an obstructing parapelvic cyst is prepared for PCNL in the standard fashion. Via an upper pole access, the stone is fragmented and removed completely via a 30F amplatz sheath. Nephroscopic resectoscope with a Colin's knife (bipolar in saline, and later monopolar in glycine) then incises the parapelvic cyst such that it communicates fully with the pelvicalyceal system. No hemorrhage encountered. Intraoperative placement of redrubber nephrostomy catheter and ureteric DJ stent (with proximal stent coil curled within the decorticated cyst). Nephrostomy removed on POD 2, and DJ stent removed at 4 weeks. Postoperative IVU at 3 months is stone free and shows disappearance of the parapelvic cyst. Opportunistic percutaneous decortication of parapelvic cysts can be performed safely in selected patients.
The Department of Urology, Nozakihigashi Hospotal, Miyazaki, Japan
Objectives PNL is usually abundant to enforce at the prone position. This study, to reduce the patient's burden, it carried out retrograde renal calyx puncture under ureteroscope in Modified Valdivia position, then considered the clinical investigation as PNL was enforced.Patients 15(3 men, 12 women) patients were enforced PNL by retrograde renal calyx puncture From May 2010 to May 2011, the average age were 63.5 years and the maximum average of ureteral stones were 29.5mm.Results Average operation time was 193 minutes; the availability was 100% in case of remaining stone of 4mm or less were clinical effective. The result can stand comparison with previous PNL in prone position without any major complications during and after operations.ConclusionsPNL by Retrograde renal calyx puncture seemed that the operative method was useful for reduce the patient's burden during operation.
Modified Technique for Tract Closure in Tubeless PCNL
Introduction: Various techniques have been described in the literature for closure of the PCNL tract. We describe here an antegrade techinique which can be easily be reproduced. Purpose: The technique involves using Floseal with a retrograde balloon occlusion catheter to seal the tract after completion of the PCNL. A double J stent is used for internal drainage.Materials & Methods: Video files demonstrating the technique have been attached. A Fogarty balloon occlusion catheter is passed antegrade over the guidewire within the amplatz sheath. Next, under endoscopic guidance, with a rigid nephroscope, the Amplatz sheath is pulled back to the torn edge of the calyx through which the nephrostomy tract enters the kidney. Under endoscopic guidance, the balloon is inflated at the torn edge. Next, the FloSeal applicator is passed through the amplatz sheath until it encounters resistance from the occlusion balloon catheter. FloSeal is injected down the sheath as the sheath is slowly withdrawn simultaneously with the FloSeal applicator until both have cleared the nephrostomy incision. After about 2 minutes, the balloon is deflated and withdrawn followed by removal of the guidewire. Results: Thirty four patients underwent this technique of tract closure after tubeless PCNL in our institute. Data showed that the amount of pain relief required was comparatively less that standard PCNLs.Conclusions: The above described technique is a procedure associated with fewer complications and can be safely performed for tubeless or nephrostomy free PCNL.
“Staghorn Morphometry”: A New Tool for Clinicalclassification and Prediction Model for PCNL Monotherapy.
Background: Staghorn stone volume and its distribution within thecollecting system “staghorn morphomerty” predicts the requirementof tracts and stages of percutaneous nephrolithotomy (PCNL)monotherapy.Objective: To develop a CTU staghorn morphomerty basedprediction algorithm to predict tract(s) and stage(s) for PCNLmonotherapy and classify staghorn accordingly.Material and methods: A retrospective study of 94units was used. CT software calculated the total stone volume(TSV) with absolute volume and percentile volume in the pelvis,planned entry calyx, favorable and unfavorable calyx. Entry calyxwas the optimum calyx chosen, keeping the relations of the ribsand adjoining viscera that could clear maximum stone volume. Unfavorable calyx was defined as having acute angle from the entrycalyx and infundibular width of less than 8 mm. A prediction model with OR(95 % CI) was constructed on multivariateregression factors.Results: Multivariate analysis showed that unfavorable calyx stone percentile volumepredicted tract (AUC - 0.91) while TSV and unfavorable calyx stonepercentile volume (AUC-0.846) predicted stage. OR basedprediction model suggested need for single tract and stage PCNLvs. multiple tract and stage PCNL for TSV and unfavorable calyxpercentile stone volume of (<5,000 mm3 and 5%) and (>20,000mm3 and 10%), respectively.Conclusion: The model predicts the tract and stage for PCNLmonotherapy. Staghorn morphometry differentiates staghorn intotype 1(single tract and stage); type 2 (single tract-single/multiplestage or multiple tract-single stage), and type 3 (multiple tract andstage).
Tubeless Percutaneous Renal Surgery in Patients with Solitary Kidneys: Initial Experience
IntroductionA tubeless percutaneous approach to renal surgery offers a shorter hospital stay and lower analgesia requirements. It has been suggested that a tubeless approach is contraindicated in patients with a solitary kidney. We present our experience with tubeless percutaneous renal surgery in patients with a solitary kidney to determine patient outcome and renal functional results. MethodsBetween July 2009 and August 2011, 4 patients with a solitary kidney were treated with planned tubeless percutaneous renal surgery. The solitary kidney was anatomic in 3 patients and a transplant allograft in another. Demographic data, hemoglobin values, serum creatinine and complications were studied. RESULTS: The average patient age was 54 years. Percutaneous surgery was performed for stone disease in 3 patients and for urothelial carcinoma of in 1. Of the patients with renal stones, the mean stone burden was 924 mm2. A planned tubeless percutaneous procedure was successfully performed in 3 of the 4 patients. The mean operative time was 116 minutes and overall estimated blood loss was 150cc. There were no major complications noted. The mean hemoglobin decrease was 1.2mg/dL, and mean length of stay was 2 days. At a mean follow-up of 18 (6-60) months all patients were stone free. In the entire cohort the MDRD estimated glomerular filtration rate was 44.7, 42.5, and 49.9 ml per minute per 1.73 m2 at baseline, immediately postoperatively and at 1 month respectively. CONCLUSIONS: Tubeless percutaneous surgery in the solitary kidney is safe in select patients and results in renal function preservation.
The Role of the Learning Curve in Supine Percutaneous Nephrolithotomy
Objective: To compare the efficacy and safety of percutaneous nephrolithotomy (PNL) in supine position, during the introduction of the method and after a certain experience was gained.Material and methods: Supine PNL was performed for the first time in the Department of Urology of the Victor Babes University of Medicine and Pharmacy Timisoara, Romania, in March 2009. Since then, 149 procedures were performed (until 31 December 2010). We have analyzed the first 40 performed cases and compared them with the last 40 cases. We have studied the following parameters: procedure duration, duration of postoperative hospitalization, stone free rate, and complications.Results: During the initial period, the average procedure duration was 28.7 minutes, the average postoperative hospitalization 4.4 days, the average stone free rate 81.5%, and the average overall complication rate 35.0%. Most complications (11 cases) were represented by moderate intraoperative/postoperative bleeding; we had 2 cases of pelvic perforation and one case of colon perforation, which all have closed spontaneously, without the need for re-intervention. In the final 40 cases of the evaluated period, the average procedure duration was 13.7 minutes, the average hospitalization time 3.4 days, the average stone free rate 92.3%, and the average overall complication rate 20.0%. From the 8 complications observed in this group, 7 were represented by moderate intraoperative/postoperative bleeding and 1 was intraoperative pelvic perforation. Conclusion: After an initial learning period of at least 40 cases, supine PNL is a safe and effective method, which may prove to be superior to the classical prone approach.
Safe Percutaneous Renal Access in Intermediate Supine Decubitus (ISD)
Introduction: Percutaneous nephrolithotomy (PCNL) is the technique of choice for treating complex renal stones.There are different possible decubitus to perform PCNL. We use the Intermediate Supine Decubitus (ISD). The aim of this study is to demonstrate that lumbar puncture performed from behind and below the free end of the twelfth rib, on patients whose kidneys are in normal position and are positioned in ISD never incurs colonic injury, and in a high percentage of cases, enables access to the kidney through its posterior valve. Materials and Methods: a prospective study was carried out on 200 patients with renal lithiasis, who underwent a PCNL in ISD between July, 2008 and July, 2010. The position of the nephrostomy placement in the kidney was determined by computed tomography.Out of the 200 patients, 186 fulfilled the criteria of kidney in normal anatomical localization and puncture was performed below the 12 th rib. Results: the mean age was 48 years old (r: 17-73). The mean body mass index (BMI) was 25 (r: 19.3-38). Staghorn lithiasis was present in 35% (n: 70) and the mean lithiasis surface area treated was 3.5cc (r: 1.5-5.8). Lithiasis was on the right side in 45% (n:90). None of the 186 patients sustained lesions to neighbouring organs, and in 183 (98.3%), renal access was gained through the posterior valve.Conclusion: In patients whose kidneys are in normal position, ISD allows to perform a safe renal punture using the free end of the 12th rib as excellent anatomical reference.
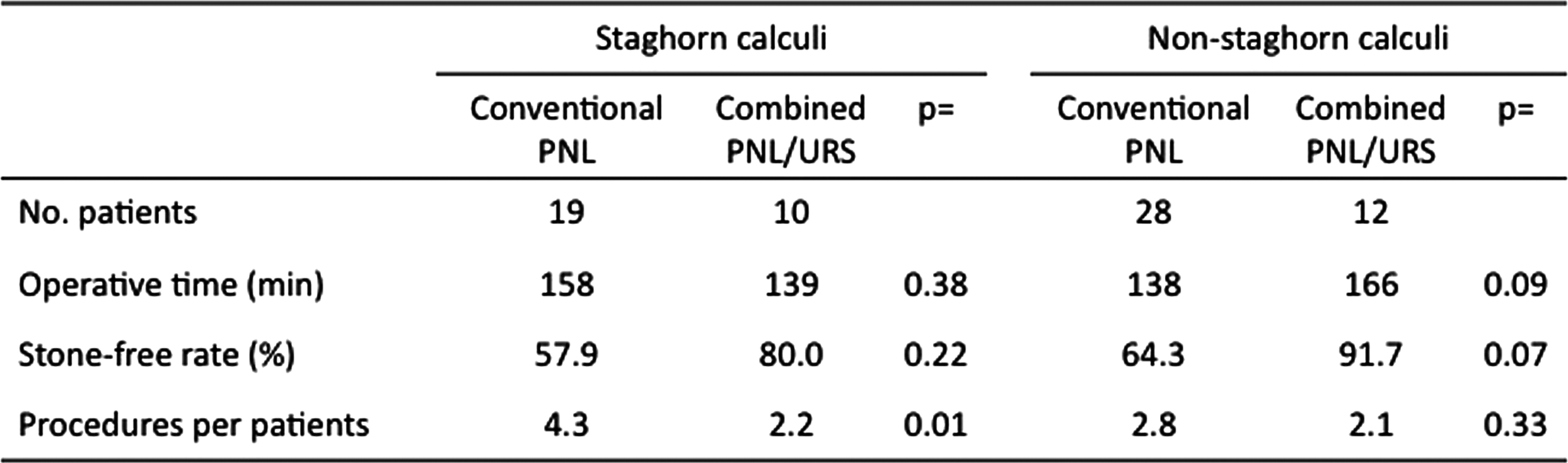
Simultaneous Combined Percutaneous and Retrograde Approach Versus Percutaneous Approach for Complex Renal Calculi
INTRODUCTION: A recently developed technique with simultaneous combined application of percutaneous nephrolithotomy (PNL) and flexible ureteroscopy (URS) has the potential to reduce the number of procedures, complications and residual stones in patients with complex renal stones.PURPOSE: We compared clinical outcomes of conventional PNL vs. combined PNL/URS.MATERIALS AND METHODS: We retrospectively evaluated patients who underwent conventional PNL from 2001 to 2007 and those did combined PNL/URS from 2008 to 2011 at our institution. RESULTS: A total of 47 patients underwent conventional PNL for staghorn (n=19) and non-staghorn calculi (n=28), and 22 patients underwent combined PNL/URS for staghorn (n=10) and non-staghorn calculi (n=12). (1) In staghorn calculi, operative time (OT) and stone-free rate (SFR) (57.9% vs. 80.0%, p=0.22) were similar in both procedures. Procedures per patient (PPP) in combined PNL/URS were less than those in conventional PNL (2.2 vs. 4.3, p=0.01). (2) In non-staghorn calculi, combined approach showed higher SFR (91.7% vs. 64.3%, p=0.07), but longer OT (166 min vs. 138 min, p=0.09) compared to conventional PNL. PPP were similar in both procedures. CONCLUSIONS: The results indicate that combined PNL/URS can effectively reduce the number of procedures and improves SFR in complex renal calculi.
Medicana International Hospital Department of Urology, Ankara, Turkey
We designed a novel robot which enables to use the commercially available ureterorenoscopes functions remotely. In this video we showed the effectivity and advantages of robotic flexible ureterorenoscopic treatment of the larger kidney stones with increased number of the patients.Material and MethodWe evaluated 21 patients with intra renal single stone, without ureteral obstruction.We used 7,5F Storz Flex- X2 Flexible Uretero Reno Scope (FURS). After initial rigid ureteroscopy and insertion of 35 cm access sheath, we introduced the FURS into the sheath manually and connected the FURS to the robot. We controlled the FURSs forward and backward movement, rotation and deflection of the tip and the movement of the laser fiber by a joystic remotely from a radiation free area. With the help of reset function the device is capable to reset all the movements and can take the neutral position easily. We dusted and fragmented the stones precisely, while seated, outside of the radiation zone. Results Mean stone size was 19mm (9-38mm). We successfully controlled all functions of the FURS remotely with robot and we could dusted/fragmented all of the stones. VAS was 9 for the movement,rotation and deflection of the FURS and it was 8 for the remote laser fiber movementConclusion:We confirmed that remote robotic control of the commercial flexible ureterenoscopes provides the treatment for even larger kidney stones in a shorter time, with the advantages of recent development of the flexible ureterorenoscopes, while seated, outside of the radiation zone.
Is There a Difference in the outcome of upper urinary tract stone treatment between Digital and Conventional Flexible Ureterorenoscopy Procedures
Purpose: We aimed to compare the outcomes of patients who were treated using digital and fiberoptic flexible ureterorenoscopy (URS) for kidney stones. Patients and Methods: Between September 2009 and April 2011, a total of 118 patients who were treated with either a conventional flexible ureterorenoscope (CFU) (59 patients) or digital flexible ureterorenoscope (DFU) (59 patients) were compared. The same surgeon performed all procedures. Preoperative, operative, and postoperative data were retrospectively analyzed.Results: The mean stone size was 1.2 + /- 6 cm in the CFU group while it was 1.1 + /- 5.3 cm in DFU group (P=0.15). The initial assessment of the entire pyelocaliceal system was possible in 58 of 59 cases (98%) in the CFU group and in 56 of 59 cases (94%) in the DFU group (P=0.09). The mean operative time was significantly longer in the CFU group (53.4 + /- 16.8 minutes VS 41.5 + /-14.9 minutes, P=0.001). The overall stone free rate one month after the procedure was 91.2% in the FFU group and 88.7% in the DFU group (P=0.11). The average number of uses for FFU and DFU before repair necessity was 52 and 44, respectively.Conclusion: Although the DFU have more limited maneuverability, comparable success rates can be achieved with both conventional and digital instruments. Nevertheless, the DFU significantly reduced the operative time compared with the conventional one.
Urology Department, Pierre and Marie Curie University, Paris, France
Objective: Renal stone management in obese patients may represent a challenge. We sought to evaluate the efficacy of flexible ureterorenoscopy with holmium laser lithotripsy in this category of patients.Patients and Materials: We retrospectively reviewed records of 923 patients who underwent flexible ureteroscopy (F-URS) with holmium laser lithotripsy for renal stones from 2005 to 2010. We identified 136 patients (141 renal units) who met the inclusion criteria set by this study (BMI more than 30 m/Kg2). Stone-free status, operative findings and post-operative complications were evaluated. Re-treatment was carried out if incomplete stone fragmentation, otherwise, renal ultrasound or non-enhanced CT scan was performed 4 weeks post operatively.Results: Stone free rate was obtained in 122 renal units (86.5%) after first session of F-URS. This could be improved to 93.6% and 98.5% after second and third session respectively. Stone free status was defined as the absence of renal stone or residual fragments less than 2 mm. stone burden was 11.4 mm (range 4 to 42). The mean number of procedures was 1.4. Urinary tract infection was reported in 3.5% as well as hematuria post-operatoire that resolved within 48 hrs. There were no major complications. Conclusion: For obese patients with renal stone, F-URS with homium laser fragmentation represents a safe efficient technique with acceptable results and low morbidity.
Modular Polyscope for Ureterorenoscopy: Initial Experience at MPUH
Background :The modular design of polyscope makes it a more cost effective option. Relatively cheap and disposable multilumen catheters preclude the need for sterilization of optic cable, thus decreasing the chances of handling-related damages and chance of instrument related infection.Objective :The aim of our study was to highlight our initial experience with cheaper flexible ureteroscopy using polyscope, a new advancement in the era of flexible ureterorenoscopy.Material and Method : We used a 7.5 Fr modular flexible, retrograde steerable, torsion resistant polyscope for diagnostic biopsy and therapeutic purposes for removal of small renal stones from December 2010 to June 2011. Polyscope was passed through 12 Fr access sheath after dilating the ureter with 12 Fr Nottingham dilator over guidewire. Standard flexible ureterorenoscopy with a limited angle of deflection was done. Postoperatively DJ stent was placed for drainage.Result : Mean age of the patient was 47.25±19.26 years. The Polyscope was used for treating seven cases of renal stones and for biopsy of one case with hematuria. The average stone size was 12.58±8.6 mm and average Houncefield Unit(HU) was 1135±496 . Mean hospital stay was 5.62±3.62 days. Vision rating was 6.2±2 mm on a VAS score scale of 1to 10 mm. Stones were successfully treated in all cases. The initial 2 cases required additional scope for successful stone removal.Conclusion : Polyscope is successful as a cheaper flexible ureterorenoscopy option.
Urology Department, Pierre and Marie Curie University, Paris, France
Introduction: The incidence of stone disease after urinary deviation is frequently reported and causes significant morbidity in patients. Multiple factors increase stone formation and these can be a significant cause of renal failure. We present our experience in the minimal invasive management of post renal complications in urinary diversions.Patients and Methods: From 2005 to 2011, 15 antegrade URS procedures with the use of a flexible ureteroscope were performed in 11 patients with a urinary diversion and with a median age of 45 years (ranging from 32 to 79). The urinary diversions in the population consisted of ileal conduits, orthotopic neobladders, catherisable pouches and an ureterosigmoidostomy in respectively 4,4,2 and 1 patient. The most important reason for treatment was recurrent upper urinary tract infection. The indication for intervention was stone disease in 12 procedures and strictures in 3 cases. Average time to stone development after urinary diversion until the first procedure was 13.5 years. In two patients multiple treatments were performed. Results: A nephrostomy tube was already in place in 63.6% of procedures which was the access route used. Successful puncture was performed in all other patients. 75% of patients were rendered stone free after the first antegrade session. Moreover, all strictures were successfully treated by dilatation. In two sequential procedures in a patient there was an inability to stone treatment due to abnormal position of the ureter (Siphoned), which did not allow the ureterenoscope to pass. All other procedures were uneventful. Postoperative complications were reported in 4 procedures. Significant urinary tract infection in 2 patients as well as an obstructed nephrostomy tube in 2 patients. Conclusion: Antegrade endoscopic procedure in patients presenting with urinary diversion associated complications is feasible, safe and well tolerated technique especially which the increasing use of smaller access sheaths.
VP05: Robotic/Lap/TUR Prostate
Department of Urology, Seoul National University Bundang Hospital, Seongnam, Korea
The posterior detrusor apron (PDA) is a strong and thick functional tissue more appropriate for pulling and fixing the median dorsal fibrous raphe (MDFR) during posterior reconstruction (PR) of radical prostatectomy. Thus we hypothesized that PDA is more important structure for PR than the Denonvilliers' fascia (DF).
We investigated whether our new PR technique which opposes MDFR not to DF but solely to PDA during robot-assisted laparoscopic prostatectomy (RALP), could improve continence recovery.
Consecutive patients who underwent RALP by a single surgeon were included. One hundred and sixteen patients who received PR with this new technique between March 2010 and January 2011 (case group) were compared to a cohort of 126 patients who did not receive PR between January and October in 2009 (control group). The primary end point was continence recovery rate (no pad use) after surgery.
The case group showed higher continence rates at all points of evaluation, which were 2 weeks (30.1% vs. 19.8%), 1 month (58.4% vs. 45.7%), 3 months (82.7% vs. 70.5%) and 6 months (95.3% vs. 86.4%)(log-rank test, p=0.007). Application of the new PR, age, and membranous urethra length were significant variables to complete recovery of continence, not only in univariate but also in multivariate analysis.
This study demonstrates that application of this new PR technique during RALP significantly improves recovery of continence compared with standard technique not incorporating PR. In addition, PDA is assumed to be the more appropriate key structure at the proximal side for PR than DF.
Prospective,Randomized Use Of The VLOC Suture to Facilitate Vesicourethral Anastamosis During Robot Assisted Radical Prostatectomy: Time Reduction and Cost Benefit
Introduction:Robotic vesicourethral anastomosis(VUA) using the Van Velthoven technique has significantly improved urinary reconstruction during RARP. Recent case series have suggested that the use of barbed polyglyconate suture may facilitate VUA. Compared to standard monofilament posterior reconstruction(PR) and VUA technique, we sought to evaluate the effectiveness of VLOC-180suture for urinary reconstruction.Methods: A prospective,randomized study was conducted in 70 consecutive RARP cases by a single-surgeon.Assurance of watertight closure was ensured with 300mLintraoperatively. Time to complete the suture setup, anastomosis time and need to adjust suture tension were recorded. Suture related complications, validated-questionnaire continence and a cost analysis were also analyzed. Results: Compared to our conventional reconstruction technique, there was a significant reduction in mean nurse setup time of suture material (31 vs 294sec;p<0.01) and reconstruction time(13.1vs20.8min;p<0.01).Need to readjust suture tension or place additional LapraTy clips to establish a watertight closure was observed in 8(24%) vs 2(6%) of cases(p=0.03).A cost reduction was also seen at our institution 48.05$vs70.25$CAN) with the use of the interlocked VLOC technique. Time to foley removal was comparable between groups(4.1vs4.2 days,p=0.87). With a mean followup of 6.2months, no delayed clinical anastomotic leaks or bladder neck contractures were observed in either group. Padfree continence outcomes at 1 (64%vs69%,p=0.60),3 (76%vs81%,p=0.54) and 6 months (88%vs92%,p=0.67) were also comparable.Conclusions:Compared to standard monofilament suture, the unidirectional barbed VLOC suture appears to provide a safe, more efficient and cost effective PR and VUA during RARP. Use of the interlocked-VLOC suture technique prevents slippage,precluding the need for assistance,knot tying,and constant reassessing of anastomosis integrity.
Ligation Free Versus Suture Ligation of Dorsal Venous Complex During Laparoscopical Radical Prostatectomy
A Simple and Novel Method of Preventing Postoperative Inguinal Hernia after Laparoscopic Prostatectomy
Introduction: Inguinal hernia is a late complication of radical retropubic prostatectomy (RRP) and laparoscopic radical prostatectomy (LRP). Here, we compared the incidence of postoperative inguinal hernia between RRP and LRP. We also report a novel and simple method of preventing post-LRP inguinal hernia.Subjects and methods: Between April 2004 and December 2010, we examined 272 and 340 patients after RRP and LRP, respectively. As prophylaxis for preventing inguinal hernia after RRP, we released the bilateral spermatic cord from the peritoneum. We applied prophylaxis to 101 patients (RRP prophylaxis [+] group) and compared the results to those in 171 patients without prophylaxis (RRP prophylaxis [-] group). We also applied the same prophylaxis in the transperitoneal approach LRP. For prophylaxis in LRP, we released the bilateral spermatic cord from the peritoneum in the prevesical space (LRP prophylaxis [ + ] group). Results: Inguinal hernia developed in 20 (11.7%) and 26 (7.6%) of the RRP and LRP prophylaxis (-) patients, respectively. BMI of LRP patients with inguinal hernia was significantly lower than that of those without hernia (22.0±2.5 vs. 23.2±2.7; p<0.05). The prophylactic procedure against inguinal hernia in LRP was accomplished within 5 minutes (234±26 seconds) without any side effects. Inguinal hernia did not develop in any patients in the RRP and LRP prophylaxis (+) groups.Conclusions: A low BMI affects the incidence of inguinal hernia after LRP. We developed a novel and simple method of preventing inguinal hernia after LRP.
Can we Predict Urine Leakage at the Urethro-Vesical Anastomosis Post- Robot-Assisted Radical Prostatectomy? (Surgeon Experience: Does It Matter?)
OBJECTIVE: Our aim is to determine if low-risk patients can be identified in whom cystography is unnecessary to assess the integrity of the vesico-urethral anastomosis after robot-assisted radical prostatectomy.PATIENTS AND METHODS:A total of 133 consecutive patients who underwent robot-assisted radical prostatectomy with an intraperitoneal approach were evaluated. Patient demographics, intraoperative data, postoperative data, and complications were recorded prospectively. Surgical technique, blood loss and comorbidity were recorded. Cystograms were taken 6 to 7 days after RARP to assess vesico-urethral integrity before catheter removal.RESULTS:Of the 133 patients, 83.3% of patients had no leak on cystography and were catheter-free at 7 days. 11 patients with leaks were identified, of which 1 (9.0%) was moderate. The 2 groups were similar in age, Gleason score, and history of previous urethral/bladder neck surgery. Univariate analysis showed no statistical difference among case duration, estimated blood loss, need for bladder neck reconstruction, presence of visible anastomotic leak, use of pelvic drains, Previous prostatic surgeries or ischaemic heart disease. No patient in either group had urinary retention, urinary tract infection, renal failure, or bladder neck contracture develop. The degree of postoperative urinary incontinence was similar between groups.CONCLUSIONS:Leakage cannot be reliably predicted at the vesico-urethral anastomosis. Foley catheter removal on postoperative days 6-8 after robot-assisted radical prostatectomy without routine cystography appears safe.
Three-Dimensional Vision using a Flat High-Definition 3D Screen: Does it improve the Quality of Assistance During Robotic Surgery?
ObjectivesThree-Dimensional (3D) visualization for the surgeon is considered to be one of the major advantages of robotic prostatectomy. However, the assistants working on the patients side have to depend on 2-dimensional (2D) images projected onto a flat screen monitor. This study was designed to evaluate the impact of 3D vision on the performance of assistants using a new 3D system. MethodsWe developed a control box that can translate the da Vinci 3D signals to the 3D signals for a flat screen. They are projected onto a same screen through different polarizing filters. The assistants wear polarized glasses to have optimal 3D vision. Method 1: Six surgeons varying experience performed 3 tasks (7 small holes, elastic bands and suturing) with laparoscopic devices as laparoscopic training. Performance times were recorded using both 2D and 3D vision for each task. Method 2: The assistant wore polarized glasses for a flat screen 3D monitor throughout the robotic prostatectomy. The efficiency of the 3D system for assistance was evaluated on a scale of 0-100 subjectively.ResultsThe polarized glasses were comfortable to wear, and direct vision was seldom influenced. Performance time in task 1, 2 and 3 was reduced by 84%, 56% and 10% using 3D imaging, respectively. Performance time for all 3 skills confirm an advantage of 3D vision. During robotic prostatectomy, overall satisfaction was scored + 85.ConclusionThe use of 3D visualization seems to improve the efficiency of assistance during robotic surgery.
Department of urology, National University Hospital, Singapore
Introduction:Robotic assisted laparoscopic radical prostatectomy requires experience and technical expertise. It is even more challenging in a patient with a previous renal transplant and requires unique modifications with an attention to detail during the procedure.Purpose:We report the feasibility , technical issues and outcome in a 56 year old man with a previously successful kidney transplant and newly diagnosed prostate cancer who underwent a robotic radical prostatectomy at our institution.Materials and Methods:56 male, previous renal transplant in 2009. Newly diagnosed prostate cancer in June 2010 , Gleason score 3+3 , PSA 3.33, underwent subsequent robotic radical prostatectomy.Ports were positioned in a standard manner but under careful direct visualisation cognizant of the transplanted kidney in the right iliac fossa. An anterior transperitoneal approach was undertaken with the video illustrating care to avoid the renal graft and the dome of the bladder both during passage of instruments and dissection. The video also illustrates steps to ensure tension free urethro-vesical anastomosis , application of Rocco stitch and the use of V-LOC suture.Results:Total operative time was 240 minutes, minimal blood loss, no intra-operative or post-operative surgical or anaesthetic complications. Immunosuppression was resumed from day 1 post-op. renal function and urine output was good during post-op recovery. Patient was discharged on 3rd post-op day. Histology showed all margins were clear. Post-op MCU showed no urinary leak .Conclusions:With attention to detail and unique modifications robotic assisted radical prostatectomy is feasible with good surgical outcomes in a kidney transplant patient.
Prospective Randomised Study Comparing Monopolar Transurethral Resection Versus Photo-Selective 80-W Potassium-Titanyl-Phosphate Laser Vaporisation.
Introduction : Endoscopic management is the most frequent treatment for LUTS. Photo-selective 80-W potassium-titanyl-phosphate laser vaporisation is becoming more popular but single center randomised studies are rare.Purpose : Present our results of a prospective randomised single center study comparing monopolar transurethral resection (TURP) versus photo-selective 80-W potassium-titanyl-phosphate laser vaporization (KTP).Material and Method :All patients requiring endoscopic managment for benign prostatic hyperplasia since 2007 were randomised for TURP or KTP. Preoperative workup included prostate volume, flow, post void residual (PVR), IPSS and Qol. Length of procedure, hospital stay and complication were recorded. Flow, PVR, IPSS and Qol were assesed at 1,3,6,12 and 24 month.Results: A total of 182 patients were included. Both arms were comparable in terms of preoperative parameters. Statistical significance was found for higher blood loss in the TURP Group (17g/l versus 8g/l ; p<0,05). Hospital stay was shorter for KTP group (1,6 days versus 3.1 days ; p<0,05). Long terms results showed only a significant difference in IPSS at one month (7,8 for TURP versus 11.8 for KTP; P=0.006) and in prostate volume reduction (7 ml for KTP et 16 for TURP p<0.05).Conclusion : This study confirms the efficacy of both techinques, KTP laser has the advantage of a shorter length of stay and less blood loss. However symptom relief is faster with traditionnal resection.
Sydney Adventist Hospital Clinical School, University of Sydney, New South Wales, Australia
Histological changes in human prostates following PVP have not been documented.
To examine and document histological changes in the human prostate after PVP versus TURP.
The prostates of 3 men who underwent 532nm PVP followed by RRP (mean age 61.5 years) were compared to the prostates of 5 contemporaneous men who underwent bipolar diathermy TURP followed by RRP (mean age 58.7 years). All operations were performed by a single surgeon. Time from PVP or TURP to RRP (for prostate cancer) was greater than 6 months. All specimens were examined by a single uropathologist who was blinded to the initial treatment modality. The prostates were fixed in formalin, examined macroscopically, and sliced in step sections. Paraffin sections were taken and stained with H&E, MT, and MSB.
Amongst the PVP group, H&E staining showed patchy foci of residual coagulative necrosis in the submucosa of the prostatic urethra. MT and MSB staining demonstrated submucosal fibrosis in both PVP and TURP groups, but with differing patterns of distribution. In the PVP group, fibrosis was discontinuous, as discrete foci, extending as tongues into adjacent fibromuscular stroma. In the TURP group, a continuous band of submucosal fibrosis formed a "tight cuff" around the prostatic urethra which demonstrated more prominent squamous metaplasia.
This histopathological study is the first to document the medium-term effects of PVP on human prostates. The absence of a continuous submucosal fibrosis "cuff", leads to the hypothesis that PVP may be associated with less risk of complication with bladder neck contracture, compared with TURP.
Clinical Significance of Hyponatremia After Monopolar Transurethral Prostatectomy Using Distilled Water Irrigation
Introduction: Water is absorbed during monopolar transurethral prostatectomy (TURP) and may cause hyponatremia. Distilled Water (DW) irrigation during TURP is cheaper and widely used in developing countries. Purpose: To determine if DW irrigation during monopolar TURP results in clinically significant hyponatremia.Methods: Seventy male patients underwent monopolar TURP using DW irrigation for obstructing benign prostatic enlargement. Serum sodium was taken immediately after TURP. Hyponatremia was defined as decrease in serum sodium of 5 nmol/l or more. Signs and symptoms of hyponatremia were recorded after TURP.Results: Pre-TURP mean serum sodium was 140.64 nmol/l (Range: 135-148). Post-TURP mean serum sodium was 138.35 nmol/l (Range: 127-147). Hyponatremia after TURP developed in 14 patients (20%). Mean resection time was 57.55 minutes (Range: 15-130). Of these, only 24 patients (34%) went over one hour of TURP. Mean specimen weight was 49.73 grams (Range: 15-149). Mean blood loss was 262.78 ml (Range: 50-1000). The 14 post-TURP hyponatremic patients had mean resection times of 63.69 minutes, mean specimen weights of 50.33 grams and mean blood loss of 209.09 ml. Only one patient (1.4%) showed signs of TUR syndrome without further consequence. The other 69 patients (98.6%) did not show any clinical signs or symptoms of hyponatremia like vomiting, restlessness, seizures or changes in sensorium. Conclusion: Patients who developed hyponatremia after monopolar TURP using Distilled Water irrigation showed no clinically significant signs and symptoms of hyponatremia. These hyponatremic patients were noted to have longer resection times, similar specimen weights and lower blood loss compared with normonatremic patients.
Transurethral Prostatectomy with Bipolar Plasmakinetic: the First Experience in Vietnam
To evaluate the early functional outcomes of transurethral prostatectomy with bipolar plasmakinetic
In all, 67 patients with benign prostatic hyperplasia (BPH) with a maximum urinary flow rate (Qmax) of below 10mL/s, an International Prostate Symptom Score (IPSS) of above 19 and prostate volume of 30 to 100 mL were enrolled in this prospective study. Patients were divided into 3 groups of intervention: (1) pure vaporization was performed in patients with high ASA risk score or in patients with anticoagulant therapy; (2) resection combined with vaporzation was applied for patients withI prostate volume of 50 to 70 mL and (3) transurethral enucleation of the prostate was performed in patients with prostate volume above 70mL. All patients were evaluated preoperatively and at 1, 3 months after operation by IPSS, Qmax and postvoid residual urine volume (PVR).
There were 14 patients in group 1; 33 patients in group 2 and 20 patients in group 3. Mean prostate volume in group 1, group 2 and group 3 was 44.5 ml, 53.8ml and 71.2 ml respectively. Mean operative duration was 35.1 minutes in group 1, 50.4 minutes in group 2 and 80.2 minutes in group 3. Catheterization time was 23.6 hours, 72.2 hours and 74.3 hours in group 1, group 2 and group 3, respectively. At the 1, 3 months follow-ups, improvements in the variables measured were significantly better than the pre-op values.
Transurethral prostatectomy with bipolar plasmakinetic represents a new valuable endoscopic treatment for patients with BPH
Department of Urology, Fuchinobe General Hospital, Kanagawa, Japan
Purpose:Holmium YAG laser allows precise removal of obstructing prostatic tissue with a hemostatic effect that limits bleeding during enucleation. However some arterial bleedings are remaining and a pinpoint hemostasis must be carried out for these bleeding. Holmium laser is highly absorbed by water, resulting, laser effects changes in proportion to distance from the tissue. Appropriate power of hemostasis can be adjusted by an operator by decreasing the energy pulse or increasing the distance from the tip of the laser to the target tissue. A highly experienced expert can easily control the appropriate distance for hemostsis. However urologist in learning periods cannot control and keep the distance well for required hemostasis. We report the lowest energy pulse setting of hemostasis for its safety and efficacy.Materials and Methods:We retrospectively reviewed the patients who underwent HoLEP uisng low energy pulse setting (0.2kJx40Hz)for hemostasis in our hospital from January 18th 2011. Results:Bleedings were well controlled for all of them and had no complications. With the low energy pulse setting, a tip of laser fiber almost come into contact with the target bleeding site and energy could be applied in very pin pointed fashion. Then every bleeding was able to control well. Another advantage of this method is that, this hemostasis effect is very limited and has very little influence on surrounding tissue.Conclusions: Low energy pulse for hemostasis can be safer for urologists in learning periods and can make more delicate hemostasis for even experts.
Department of Urology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan
Introduction: There are limited evidences available to support the use of photoselective vaporization of the prostate (PVP).Purpose: To compare the improvement in clinical outcomes between GreenLight HPS laser PVP and conventional transurethral resection of the prostate (TURP) in men with symptomatic benign prostatic enlargement (BPE). Materials and Methods: All men with symptomatic BPE without exclusion criteria who had undergone PVP (n=327) and TURP (n=777) were reviewed retrospectively. Baseline characteristics of patients including pre-operative urodynamic parameters were evaluated. The improvement of total International Prostate Symptom Score (IPSS), quality of life (QOL) index, peak urinary flow rate (Qmax), and post-void residual (PVR) as parameters of clinical outcomes were evaluated after 3 and 12 months following surgery and were compared between PVP and TURP.Results: All baseline urodynamic parameters were comparable except for bladder contractility index (BCI) and detrusor pressure at Qmax. Despite older age with lower BCI, patients in PVP group demonstrated significantly higher improvement of total IPSS, QOL index, Qmax and PVR after 3 months and 12 months following surgery (Table. 1).Conclusions: The results of this study suggest the superiority of PVP for the improvement in clinical outcomes following surgery in men with symptomatic BPE.
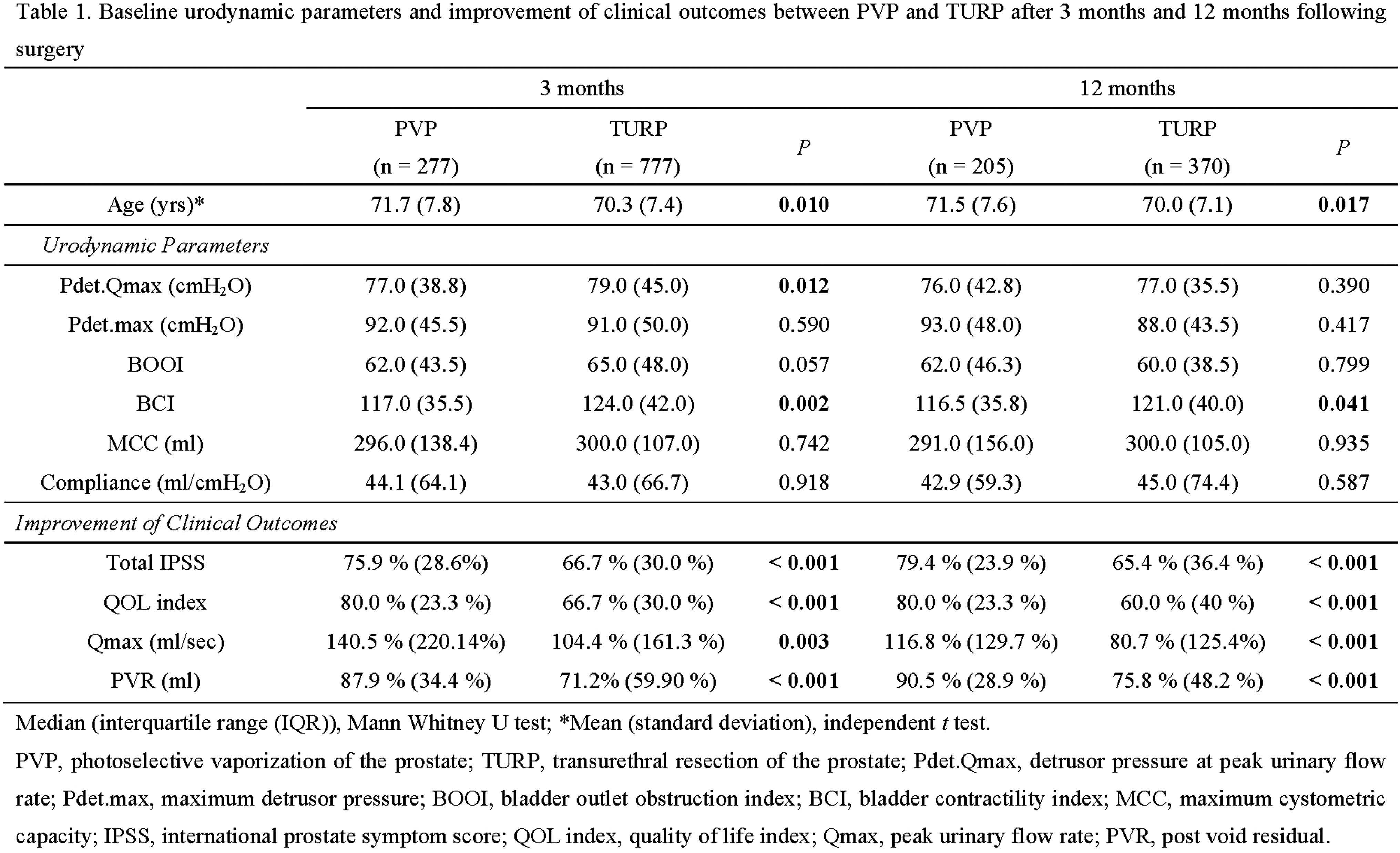
Antegrade HoLEP A Useful Salvage Procedure in more than 200 gm BEP
Introduction: Holmium laser enucleation of prostate (HoLEP) for benign prostatic enlargement (BEP) more than 200 gms is technically challenging. We report the use of additional antegrade access to successfully complete HoLEP in such a case. Material & Method: A-78-year obese gentleman presented with refractory retention. Comorbidity included hypertension with ventricular ectopics, controlled on medication. Transrectal ultrasound revealed a 212 gm BEP. PSA was 10.1 ng/ml. Digital rectal examination revealed a smooth, grade IV prostatic enlargement. Hematological and biochemical profile was normal. At cystoscopy, large bilobar BEP was seen with the cystoscope length barely reaching the bladder neck. HoLEP was initiated using 26Fr resectoscope with modified laser fibre carrier, in a retrograde fashion. After initial trench formation at 6 and 12 o clock, plane of enucleation could reach only 4/5th of the gland. A 28Fr percutaneous suprapubicvesical access was created and 1/5th adenoma was enucleated intravesically, using laser. Postoperatively, 18Fr SPC and 22Fr transurethral foleys was inserted. Morcellation was performed as a second stage, 48hours later.Result: Procedure was successfully completed in 3 hours 30 min. lasing time was 2hours 30 min. SPC was removed on day 2, after morcellation. Successful voiding trial was done on day 4. Conclusion: Antegrade access for completing HoLEP in large glands is technically feasible. It is useful where instrument length falls short. It also reduces urethral manipulation.
Peculiarities of HoLEP for large more than 150 gm Prostates.
Introduction:- Holmium Laser Enucleation of Prostate (HoLEP) is an endoscopic equivalent of open prostatectomy with a steep learning curve. We are doing HoLEP since July 2000 and have analysed intraoperative peculiarities in large glands more than 150 gms.Material and Methods:-Since July 2000 till June 2011, 3284 HoLEP have been done at RG Stone Urology & Laproscopy Hospital, New Delhi, India. Glands more than 150 gms (n=227) were evaluated. All patients had complete workup & intra-operative issues were analaysed.Results:- Mean Prostate size was 212 gms (150 to 424 gm). 71 % cases had catheter. 67 % had significant comorbidities including 12 % on anticoagulants. Intra-operative problems noted were poor vision, poor coagulation of large bleeders & rigors.Placement of a suprapubic cannula significantly improved vision and reduced incidence of rigors. 8.2 % needed diathermy coagulation. In 5.6 % cases morcellation was done as second stage after 48 hours.In one case the endoscope could not reach full length of prostate and needed ante-grade enucleation through Supra pubic tract. 2.3 % cases needed transfusion. Fall in hematrocrit was 1.2 gm (0.4-3.8). All patients voided well. Transient stress incontinence was noted in 7.8% which reduced to 1.6% at 3 weeks.Conclusion:- Bleeding causing poor vision and rigors can occur during HoLEP for large more than 150 gm prostates. Supra-pubic cannula improves vision, and permits safe completion of procedure. Antegrade HoLEP is feasible if instrument falls short. Staged morcellation after 48 hrs is a safe adjunct.
University of Montreal Hospital Center, Cancer Prognostics and Health Outcomes Unit, Montreal, Canada
INTRODUCTION: To perform a comparative-analysis of the efficacy of GreenLight120W-HPS laser vaporization in men with obstructiveBPH with prostates volumes(PV)<60,60-100 and>100cc.METHODS:Clinical data of men with symptomatic BPH who underwent PVP(2007-2009) were retrospectively analyzed. Functional followup included IPSS,SHIM, serum-PSA, Qmax, post-void residual(PVR) determinations and TRUS sizing.Functional-evaluations were performed at 3,6 and 12 months with PSA obtained at 6months.Change in baseline outcomes, complications and retreatment rates were compared.RESULTS:Among 250 consecutive PVPs, 134,76 and 40 men had prostate volumes<60, 60-100 and>100cc, respectively. Mean laser time,energy and fibre usage were 31,44 and59 minutes;163,309 and 473kJ, and 1.4,2.2 and 3.2 fibers,respectively (p<0.01 for all). At 1 year, mean IPSS improved 69%,63% and 50%,Qmax increased by 194%,175% and 162% and PVR decreased by 88%,81% and 1%,respectively (p<0.01 for all). Mean decrease in pre-operative PSA at 6 months was 63%,52% and41%(p<0.01), respectively. Hospital stay, catheterization time and complication rates were comparable between groups, however retreatment rates were significantly higher for prostates>100cc (1.5%vs2.6%vs9%;p=0.02).CONCLUSIONS:At 1 year, significant and durable improvements in the subjective and objective voiding parameters were observed in all prostate volume groups. Although larger prostates require more time and energy delivery, HPS-PVP is safe and efficacious as an outpatient procedure for me with LUTS regardless of prostate size. However, laser vaporization for glands>100cc appears to have a reduced reduction in PSA and a higher rate of retreatment. Such findings are valuable in counseling patients undergoing PVP. Further research is required to address the optimal surgical management for men with prostate volumes>100cc.
VP06: Imaging/New Technology/Pediatrics
Department of Urology, Nagoya University, Nagoya, Japan
Laparoscopic retroperitoneal lymph node dissection is still a technically difficult procedure retrieving all lymph node diseases within a template field for patients with large and wide-spread retroperitoneal masses receiving prior chemotherapy. We report on the procedure of L-RPLND in bilateral template with right-sided unilateral port-setting in the supine position. Four patients underwent simultaneous bilateral extraperitoneal L-RPLND. Patients were placed in the supine position and the first trocar was inserted between the right anterior iliac spine and the navel. Three more ports were inserted into the retroperitoneal space after distention; each was close to the right-lateral end of the peritoneum. All residual tumors included in the bilateral templates including paracaval, postcaval, intraaortocaval, preaortic, paraaortic, and ipsilateral common iliac nodes were dissected completely through right-sided laparoscopic ports without changing patient position or additional ports. Maximum diameter of the dissected lymph node was 3.5 cm and the average number of the dissected node was 7. The mean operative time was 3.6 hours and the estimated blood loss was less than 50 mL. No intraoperative or postoperative complications occurred. No viable cancers were revealed histopathologically in all patients. Teratomas were identified in bilateral residual tumors which could not be retrieved by L-RPLND with unilateral modified template. Extraperitoneal L-RPLND with right sided-port setting in the supine position is technically feasible and useful for testicular cancer with bilateral residual retroperitoneal tumors after chemotherapy. More medially-centralized port setting in right flank in the extraperitoneal approach helps entire dissection in bilateral templates.
Scott Department of Urology, Baylor College of Medicine, Houston, Texas, USA, 2Texas Children's Hospital
INTRODUCTION: Laparoscopic management of vesicoureteral reflux (VUR) offers the advantages of minimally invasive procedures with the ability to manage complex anatomy and achieve higher success rates than endoscopic therapy. PURPOSE: We evaluated a single pediatric tertiary center experience with the laparoscopic extravesical reimplantation (LED) in patients with simple and complex ureteral and bladder anatomy. MATERIALS AND METHODS: We retrospectively evaluated medical charts of children undergoing laparoscopic extravesical detrusorraphy at our institution over the past nine years. RESULTS: A total of 144 ureters in 98 patients were treated with LED over the study period. Mean patient age was 6.7 years, and 84.7% were female. 24.5% had known pre-operative dysfunctional elimination syndrome. Mean pre-operative reflux grade was 3.2, with VUR on the right in 22.4% and bilateral VUR in 46.9%. 27.6% had complex urologic anatomies. Reflux resolved in 93.5% of patients. Average length of stay was 1.7 days for children 5 + years and 1.0 days for children<5 years. New-onset post-operative hydronephrosis occurred in 30.1%, with 92.3% returning to baseline at their second renal ultrasound. Two patients had intraoperative inadvertent ureterotomies during the detrusor tunnel dissection, and three required temporary ureteral stents in the post-operative setting. 16.7% of patients had post-operative culture-proven UTI with 11.2% having febrile UTI. Urinary retention occurred in 6.5% of children with bilateral reimplantations and in 0% undergoing unilateral reimplantation, all of which resolved. CONCLUSIONS: LED is a safe and effective procedure for the management of VUR in both simple and complex ureteral anatomy.
The Laparoscopic Alternative in the Treatment of Genito-Urinary Tract Malformations
Objective of this study was to present the technical aspects regarding the laparoscopic treatment of genito-urinary tract malformations.Material and method. We included in this study 31 patients for which 23 patients underwent laparoscopic pyeloplasty, 6 patients laparoscopic cyst excision, 1 patient excision of an ectopic ureterocele, 1 patient with partial heminephrectomy for upper pole nonfunctioning parenchyma in a patient with complete ureteral duplication and ureterocele on the upper pole ureter. The pyeloplasties were performed by using the Hynes Anderson technique in 12 patients, Fenger technique in 8 patients, and "rain drop " technique, previously published by our team, in 3 patients. Results The mean operative time was 146 min for Hynes Anderson pyeloplasty, 107,5 min for Fenger pyeloplasty, 82,33 min for "rain drop " pyeloplasty, 58 min for laparoscopic cyst excision, 195 min excision of the ectopic ureterocele and 127 min for the heminephrectomy. The approach was retroperitoneal in all cases. The ICU and hospital stay were minimum. The use of intraoperative ultrasonography significantly reduced the operative time for the cyst excision, and helped in identification of the ectopic ureterocele. Conclusions Laparoscopic surgery is a feasible and valid alternative in treatment of genito-urinary tract malformations. Lparoscopic cyst excision is a simple procedure and can be recommended for beginners teams. Laparoscopic pyeloplasty is a technically chalenging procedure that requires a trained laproscopic team.
A Novel Diagnostic and Therapeutic Technique for Persistent and Recurrent Hemospermia: Transurethral Seminal Vesiculoscopy with a Ureteroscope
Introduction: Hemospermia can be a relatively distressing symptom. It is often slight, self-limited and requires only simple management. Nevertheless, in a few patients, it may be recur or persist and it is alarming for the patient and his partner. The diagnosis and treatment of persistent and recurrent hemospermia presents significant difficulty. This study was to characterize a novel diagnostic and therapeutic technique for it.Aims: To investigate a novel technique of transurethral seminal vesiculoscopy with a ureteroscope for evaluation and management of persistent hematospermia. Methods: The clinical data of 8 patients with persistent hematospermia underwent transurethral seminal vesiculoscopy from 2008 Sep in our clinic were analyzed retrospectively. The age ranged from 26 to 55 years (mean 42). Eight patients with a course of 6 to 48 months (mean 12 months) were not cured by pharmacologic therapy. The definite etiologies of it were excluded by physical examination including BP measurement and DRE, PSA and bleeding time, and further imaging investigation such as TRUS, CT or MRI. The ejaculatory duct and seminal vesicle were observed under direct vision using a 7F rigid ureteroscope. Results: Eight patients were successfully performed by transurethral seminal vesiculoscopy (five seminal vesiculitis, two seminal stone and one vas deferens obstruction). The mean follow-up period was 10 months (range 6-24). Hematospermia in 7 cases disappeared and 1 patient recurred in 9 month after receiving seminal vesiculoscopy. Conclusions: Transurethral seminal vesiculoscopy could be performed easily using slender rigid ureteroscopy and was an effective therapeutic approach to persistent hematospermia.
Department of Urology, Ludwig-Maximilians-University Munich, Germany
ABSTRACT WITHDRAWN
Evaluation of a New 3D-laparoendoscopic Vision System - Ex-vivo Results
Introduction: 3D imaging for laparoendoscopic procedures was recently introduced for robot-assisted procedures. A new 3D-system (Einstein Vision) is now available for conventional laparoscopy. However, benefits of 3D vs. 2D imaging for key hole surgery is not known. We evaluated a new 3D-system in an ex-vivo model. Material and methods: The Einstein Vision system (Schoelly Fiberoptic, Germany) consists of stereoscopic endoscope and a digital HD system (camera and 32inch monitor). The endoscope was fixed on a robotic arm system. The tasks included manipulation of rings, needle handling and suturing. Time, loss of tools, failed picks and need for assistance were assessed and the whole session was video recorded. 10 untrained individuals and 10 experts performed all tasks. Results: The handling of the tasks did well differentiate between experts and non-trained novices. All tasks were complete significantly faster by the expert group. The following parameters were superior for 3D vs. 2D-imaging in novices: Overall time (596 vs. 938 sec., p=0.01), losses of tools (2.0 vs 4.8, p=0.007) and failed picks (4.4 vs. 15.4 sec., p=0.005). For the expert group, 3D was superior in terms of failed picks (0.8 vs. 9.0, p=0.003), while other parameters did not differ significantly. Analysis of the video recordings demonstrated straighter instrument movements with the 3D system for both novices and experts. Conclusions: We could demonstrate a significant improvement of laparoscopic tasks handling with 3D-imaging. This advantage was more evident for the non-trained group. Further studies have to demonstrate the impact of 3D visualisation in clinical practise.
STILUS Academic Research Group (SARG). London. UK
Introduction: Current laparoscopic surgery is restricted by 2 and/or 3 Dimensional image(s) rendered by a laparoscope and inherently restricted by not being able to visualize behind the target organ. We developed a holographic interface for real-time movement such that a real-time avatar of the target organ could be projected and movement translated by using laparoscopic instruments. Purpose: We tested the potential impact of a real-time hologram in laparoscopic surgery. Materials and Methods: We placed 8 small cameras in a semi-circle on a frame embedded in a laparoscopic training box. The cameras surrounded a styrofoam model in the shape of a kidney with a defect (representing a tumour on the surface). A special wired fabric canvas was developed with capability of converting light energy into electrical pulses. The canvas covered the kidney model. Electrical pulses generated were streamed such that they could create an image. The laparoscope camera was equipped with a laser such that a composite could be made to the site of focus and fused with images from the 8 cameras. Results: The model permitted a hologram to be projected outside of the box in a real time fashion with appearance (refresh time) every 6 seconds. Movement of the kidney model in the box kit with laparoscopic instruments led to movement in the projected avatar. The focal defect in the model kidney was excised entirely by viewing the holographic avatar. Conclusions: Holographic real-time movement translation is feasible in the laparoscopic urological surgery ex vivo platform.
Randomized Prospective Trial to Assess Impact of TUR in Narrow Band Imaging Modality on Non Muscle Invasive Bladder Cancer Recurrence
Narrow band imaging (NBI) is an optical enhancement technology for endoscopy which consists of filtering the standard white light into 2 bandwidths of illumination centered on 415 nm (blue) and 540 nm (green). NBI cystocopy increases the bladder cancer detection rate and therefore it may influence positively recurrence rate. To assess impact of NBI on bladder cancer recurrence rate consecutive patients with overt or suspected bladder cancer were included in a prospective study (registration code NCT0100421) and randomized to 2 treatment arms, respectively TUR performed entirely in standard or NBI modality. Excluding patients with muscle invasive bladder cancer, negative pathological examination or without follow up, the study population was composed by 148 subjects randomized from August 2009 to September 2010 to NBI TUR, 76, or standard TUR, 72. Clinical and pathological characteristics and incidence of secondary treatments (intravesical instillations) of the 2 groups were similar. The median follow up of the whole group is 10 months, range 1 to 19. Overall 24 patients (32%) recurred in the NBI group and 36 (50%) in the standard group (Yates-corrected chi-square Chi square test, p 0.034). Median time to relapse was 7 months in both groups. In multivariate Cox regression analysis confirmed that NBI was a protective factor against recurrence in our series (hazard ratio 0.53, p 0.0224) as well adjuvant topic therapy (hazard ratio 0.43, p 0.0094). TUR performed in NBI modality was able to reduce significantly the recurrence rate of non muscle invasive bladder cancer in our series.
Two Phase Angiography (2F AG) of Renal Vessels in 3T MRI Before Kidney Tumour Surgery
Introduction: Advantages of imaging of MRI vs. MDCT are well known to urologists (e.g. cystic lesions etc.). But 1,5T MRI 2F AG hasnot been used by urologist for planning of renal surgery due to no perfect resolution. New generation 3T MRI has higher resolution than 1,5. We want to present to urologists our first opinion with 3T MRI 2F AG in pilot group.Methods: It is prospective study approved by ethical committee. Since 4/2011 to 6/2011, 15 patients with kidney tumour underwent 3T MRI 2F AG (machine Magnetom SKYRA 3T, Siemens). Fourteen had MDCT, only one of them 2F CT AG. Twelve had assessed renal vessels in details by operation (open or laparoscopic, radical or partial nephrectomy).Results: In ten, there was consensus of MRI AG and preoperative finding. In two, aberrant renal artery 1,5 mm and vein 3,5 mm were found by surgeon. Sensitivity of 3TMRI2FAG in accessing of renal vessels was 83%, specificity 100%.Conclusion: 3T MRI 2F AG gives urologists detailed information about renal vessels including topographic anatomy. Results are similar to 2F CT AG. MRI AG It can be used for planning of operation, mainly in laparoscopic surgery, especially in resection. Only small aberrant vessels can be missed. Quality of 3D reconstruction is highly depending on skills of radiologist. The work was supported by grant MSM 0021620819.
James Buchanan Brady Urological Institute, Johns Hopkins University
Introduction: Benign pathology is disclosed by surgery in 20-30% of small renal cortical masses (SRM)<4cm. Purpose: To analyze the enhancement patterns of SRM during 4-phase CT imaging to predict histology. Methods: One-hundred consecutive patients with SRM and 4-phase preoperative CT-imaging who underwent extirpative surgery with a pathologic diagnosis of RCC, AML or oncocytoma were identified from a single institution. An expert radiologist blinded to histological results retrospectively recorded tumor size, RENAL nephrometry score and tumor attenuation as well as renal cortex on all 4 acquisitions (precontrast, corticomedullary [CM], nephrogenic [NG] and delayed density). Tumor enhancement was calculated by subtracting the mean Houndsfield Units (HU) from the precontrast phase from each subsequent phase. Results: Forty-eight patients had clear-cell RCC (ccRCC), 22 papillary RCC (pRCC), 10 chromophobe RCC (chRCC), 13 oncocytoma and 7 AML. There was no significant difference in median tumor size (p=0.8), nephrometry score (p=0.98) or anatomic location (p>0.2) among histologies. Significant differences were noted in peak enhancement (p<0.001) and phase-specific enhancement (p<0.007) by histology. pRCC demonstrated a distinct enhancement pattern with a peak HU of 56, and greatest enhancement during the NG and delayed phases. Both ccRCC and oncocytoma demonstrated the highest peak HU (117 and 125 respectively); ccRCC more often peaked in the CM phase while oncocytoma peaked in the NG phase. Conclusions: In a series of patients with small renal masses undergoing 4-phase CT, differing tumor histology demonstrated distinct enhancement patterns. Preoperative 4-phase CT imaging can provide information regarding pathological diagnosis in patients undergoing extirpative surgery.
Experience of Retroperitoneal Laparoscopic Partial Nephrectomy using the VIO Soft Coagulation System for Renal Cell Carcinoma. -The Preliminary Report-
Purpose: The VIO soft-coagulation system (SC) is a new device for tissue coagulation. We hypothesized that SC would be more effective device for hemostasis in the retroperitoneal laparoscopic partial nephrectomy for renal cell carcinoma (RLPN) compared with the conventional electrosurgical coagulation systems. We report the preliminary cases of using SC in RLPN.
Material and Method: A 72-year-old man with 18x19 mm of renal cell carcinoma and a 50-year-old woman with 11x13 mm of renal cell carcinoma were underwent RLPN. After the wedge resections for tumor were carried out using laparoscopic scissors, SC was used for the hemostasis of renal parenchyma. A ball-type electrode was employed for SC. Cooling was not performed for RLPN. The fibrin glue was applied for the aid of hemostasis after SC. The sutures of renal parenchyma for closing the renal defects were not performed in both cases.
Results: The SC achieved relative hemostasis during the resection of the tumor. The bleeding of bigger vessels occurred in the former case that was an initial trial of RLPN without renal artery occlusion. Few hemostatic sutures were needed in both cases. Although the renal defects were remained unclosed, rebleeding did not occur. The warm renal ischemia times were 27 and 17 minutes. The amounts of bleeding were 200ml and a little. The deduction rates of hemoglobin were 20.9 % and 4.9%. The increase rates of creatinine were 32.9% and 3.0%.
Conclusions: The SC is an effective tool for hemostasis in RLPN in preliminary cases.
Fixed Platform Target Organ Fixation and Sealant Tool During Laparoscopic Partial Nephrectomy: One Step Closer to Zero Ischaemia
Introduction: The current recommended modality for the treatment of small renal tumours i.e. less than 4.0cms includes partial nephrectomy(PN). Laparoscopic partial nephrectomy(LPN) is a recognised but challenging mode for surgical extirpation. Ischaemia time has been shown to be critical for nephron sparing surgery. Herein, we developed a fixed platform tool that permits the application of apposition, pressure, sealant and suture to the post extirpation renal parenchyma in one single step. Purpose: To test the preliminary role of a fixed platform target organ fixation and sealant tool in the ex vivo model. Materials and Methods: A fresh bovine kidney was procured from the local abattoir(following sacrifice for the supermarket). The main vessel stumps were intact. The kidney was placed in a plastic box model attached to conventional laparoscopic instruments. The kidney was fashioned on a bench such that water tight system whereby red dye was pumped under pressure. A scored section mimicking tumour was then resected with the inflow clamped. The fixation sealant tool was embedded with floseal and loaded with 5 sutures such that these could be mechanically deployed with the kidney fixed in position. The clamp was then released. Results: The total ischaemic time was 2 minutes. Loss of fluid was less than 5mls. The resection base was fully sealed macroscopically. Conclusion: The fixed platform target organ sealant tool, in the ex vivo model, is effective and can be deployed with minimal time. This could have potential use for LPN.
Robotic Partial Nephrectomy Using A Robotic Ultrasound Probe For Tumor Identification: Initial Series And Outcomes
Introduction
Accurate tumor identification during robotic partial nephrectomy (RPN) is essential for successful cancer control. Intraoperative laparoscopic ultrasonography is useful for tumor localization during RPN, but the ultrasound probe is controlled by the assistant.
Purpose
We evaluate a novel robotic ultrasound probe (RUP) that is controlled by the surgeon and compare results to RPN using a laparoscopic ultrasound probe (LUP).
Materials and Methods
RPN was performed in 22 consecutive patients between 2010-2011, using a novel RUP under surgeon control using the robotic Prograsp. In eight patients, both LUP and RUP were used sequentially for tumor identification. Intraoperative images were analyzed for percentage of circumferential tumor margin identified, frequency of need to grasp probe and probe slippage during margin demarcation, and frequency of adjustment of scored margin from the LUP when using the RUP.
Results
22 patients underwent RPN using the RUP; mean age: 59 years, mean tumor size: 2.7 cm, and mean warm ischemia time :17.9 min. All patients had negative margins. Compared to the LUP, the RUP identified a greater mean percentage of tumor circumference (90.0% vs. 63.1%, p<0.001), resulted in adjustment of the scored margin in 63% of cases, avoided the need to grab the probe to adjust placement (average 3.5 times/case with LUP) and eliminated probe slippage (average 2.5 times/case with LUP).
Conclusion
Use of a novel RUP during RPN allows the surgeon to control tumor identification and utilize the precision and articulation of the Prograsp, resulting in improved identification of tumor margins over a LUP.
Ex Vivo Continuum Based Level 3 Kidney Model: Early Hilar Control Using Sonoscopic Aided Laparoscopic Instrument Manipulation
Introduction: One of the key steps to laparoscopic nephrectomy and partial nephrectomy is hilar control especially with the transperitoneal approach. Purpose: To describe and test the concept of using audio cues by means of sonoscopic aided instrument manipulation. To describe its use in an ex vivo platform for gaining early hilar control. Materials and Methods: A box model was fitted with conventional laparoscopic instruments. The Level 3 Model comprised of a bovine kidney procured from the butcher shop and augmented with projection optics. The vascular stump/hilum was specially fashioned in a watertight fashion and attached to a purpose built high-pressure bag such that if the pedicle/hilum were to be breeched, a torrential ejection of red dye would occur. The fashioned hilum was then encased with supermarket chicken fat and sprayed with a resin that caused it to stick to the hilum. The model was placed in a box model was fitted with conventional laparoscopic instruments. Three intermediate level trainees were required to dissected out the vessels and apply Hemolok Clips to achieve hilar control (CT group). Three other similar level trainees had the benefit of a laparoscopic Doppler tool and used audio cues coupled to the laparoscopic instruments (SGT group). Times to hilar control were tallied. Result: SGT group achieved hilar control 3.2 times quicker than CT group. Conclusion: This is the first report of sonoscopy to supplement visual feedback. We propose that the coupling of visual and audio feedback could aid in shortened time for hilar control.
Department of Urology, Dokkyo Medical University Koshigaya Hospital, Saitama, Japan
Division of Urology, Duke University, Durham, North Carolina, USA
Introduction: For imaging nephrolithiasis, digital tomosynthesis (DT) has been developed to improve upon traditional KUB/tomograms while minimizing radiation exposure. However, both DT and KUB are less sensitive than non-contrast CT (NCCT) for detection of nephrolithiasis. We measured effective radiation doses for NCCT, digital tomosynthesis with tomograms, and standard KUB with tomograms, using a validated model.
Materials and Methods: An anthropomorphic male phantom was placed prone on a 64-slice GE Healthcare VCT scanner. High sensitivity metal oxide semiconductor field effect transistors (MOSFET) dosimeters were placed at 20 organ locations and used to measure organ radiation doses. KUB/tomogram and digital tomogram doses were estimated using PCXMC 2.0 (STUK, Finland), a Monte Carlo simulation-based software designed for estimation of patient dose from medical x-ray exposures. Simulations were performed using a 2D stationary field onto the corresponding body area of the built-in digital phantom, with actual kVp, mAs, and geometrical parameters of the protocols.
Results: With a NCCT for renal stones, the effective dose is 3.04 mSv. With a KUB (0.63 mSv) and three tomograms performed at 20 degree sweeps (each 1.1 mSv), the total dose is 3.93 mSv. With a digital KUB and tomogram, only one tomographic sweep is required, for a dose of 1.73 mSv.
Conclusions: With modern NCCT protocols, the effective dose of radiation is comparable to standard KUB and tomograms. This information is causing us to modify how we follow patients with recurrent nephrolithiasis. Digital tomosynthesis may potentially substitute for standard KUB and tomograms, while providing a lower radiation dose.
VS01: Laparoscopic Partial Nephrectomy
department of urology, CES clinic, Medellín, Colombia
OBJECTIVE: In recent years, the indication of partial laparoscopic nephrectomy has increased and this has allowed the realization of minimally invasive procedures. However, it is a complex procedure that requires extensive surgeon experience. Our goal is to describe the surgical technique performed by introducing some steps that are not usually used to facilitate the surgical approach and optimize the results.MATERIALS AND METHODS: We describe a case of a patient who underwent laparoscopic partial nephrectomy, A 22 years old female patient with intermittent abdominal pain, ultrasound found right renal mass, the CT scan shows a 3 cm intraparenchymatous mass, centered in the lower pole of right kidney.SURGICAL TECHNIQUE: patient preparation with antibiotic prophylaxis.Lateral modified decubitus, transperitoneal laparoscopic approach,pneumoperitoneum with an intraabdominal pressure of 15 mm Hgretroperitoneal tissue release to identify the ureter.Renal lower pole and renal pedicle Identification.1. We make a proper dissection of the renal vessels, allowing a more precise clamping.2. Vessel loops are located, individualizing renal artery and vein for later clamping. We use a segment of foley catheter and a hem o lock to make a safe clamp.3. The laparoscopic ultrasound allows precise visualization and real-time tumor localization. Resection of the tumor, using laparoscopic Scissors leaving an adequate margin of safety.4. Closure of the collecting system with microbarbed suture Roll of haemostatic agent is placed and the same suture is used to close the renal parenchyma. Hemostasis is reviewed and a drain is leaved in the surgical bedRESULTS: The mean ischemia time was 15 minutes, we conducted individual clamping of renal artery and vein with use of vessel loops, intraoperative ultrasound was used to define appropriate safety margins, the renal parenchyma was closed with microbarbed sutures, no intraoperative complicationsRESULTS INTERPRETATIONIn this video we see that there are 4 basic steps that will facilitate and optimize surgical outcomes of laparoscopic partial nephrectomy.1. The meticulous dissection of the renal vessels 2. There are different methods of vascular occlusion, bulldogs, Rumel tourniquet and the Satinsky clamp. In this video, we observed that the use of the vessel loop make easier the induction of ischemia.3. The suture of the renal parenchyma is made with microbarbed suture (V-Loc) that does not lose the tension and make a perfect closure of the renal opening4. The use of intraoperative ultrasound allows adequate safety margins to ensure oncological outcome.CONCLUSIONS: this video shows that during the course of laparoscopic partial nephrectomy is possible to use some resources to facilitate the procedure and improves postoperative outcomesKEYWORDS: Laparoscopic partial nephrectomy, surgical technique, intraoperative ultrasound, vessel loop, self-locking suture.BIBLIOGRAPHY1. Cáceres F, et al. Nefrectomía parcial laparoscópica. Actas Urol Esp. 2011. doi:10.1016/j.acuro.2011.03.0152. Gill IS, Desai MM, Kaouk JH, Meraney AM, Murhpy DP, Sung GT, et al. Laparoscopic partial nephrectomy for renal tumor: duplicating open surgical techniques. J Urol. 2002;167 (2 Pt 1):467& 8212;9.3. Haber GP, Gill IS. Laparoscopic partial nephrectomy: comtemporary technique and automes. Eur Urol. 2006;49:660& 8212;5.Uzzo R, Novick AC. Nephron Sparing Surgery for renal tumors: indications, techniques and outcomes. J Urol. 2001;166:6& 8212;9.4. Gill IS, Kamoi K, Aron M, Desai MM. 800 Laparoscopic partial nepfrectomies: a single surgeon series. J Urol. 2010;183:34& 8212;41. 10. 5. Colombo JR, Gill IS. Nefrectomía parcial laparoscópica: técnica y resultados. Actas Urol Esp. 2006;30:501& 8212;5. 11. Brawn JA, Hubosky SG, Gomella LG, Strup SE.
Zero Ischemia Robot Assisted Laparoscopic Partial Nephrectomy
IntroductionWe present a case of zero ischemia robot-assisted laparoscopic partial nephrectomy for a 4cm left lower pole renal tumor.MethodsBetween January 2011 and 2011, data from 60 consecutive patients who underwent zero ischemia laparoscopic or robotic partial nephrectomy were collected in a prospectively-maintained database. Forty Laparoscopic Partial Nephrectomy (LPN) and 20 (RAPN) were performed. A transperitoneal approach was performed and hilar vessels were not isolated. When performing the deeper tumor dissection controlled hypotension was performed and intra-operative pneumoperitoneum pressure was raised to 20 mmHg. Selective hilar microdissection was performed and vessels supplying the tumor were identified, selectively clip-ligated and transected with cold scissors. Hemostasis was completed performing a parenchymal suture.ResultsThe zero ischemia procedures with CH was successfully completed all cases. Median tumor size was 3,6 cm (range: 1.8-10); operative time was 2 h (range 1-3.5), blood loss was 200 ml (range 30-700), and hospital stay was 3 d (range 3-8). Median duration of CH with a median MAP of 65 mmHg (raange 55-70) was 14 minutes (range 7-16). During surgery blood transfusion was not necessary in any patient. Four patients required one packed red blood transfusion postoperatively. Postoperative complications occurred in 3 patients: port site bleeding, hemorrhage and hematoma. Median pre and postoperative serum creatinine levels were 0.9mg/dl and 1.02mg/dl, while eGFR was 91,11 and 70,06, respectively.Conclusions All procedures were successfully completed, with acceptable complications rate and encouraging preliminary functional outcomes. In our experience CH allowed to perform LPN and RAPN without the need of renal hilum clamping.
Zero Ischemia Sutureless Laparoscopic Partial Nephrectomy with 10mm Ligasure
IntroductionWe present two cases of zero ischemia sutureless laparoscopic partial nephrectomy for renal tumors with low nephrometry score.MethodsBetween August 2003 and January 2010, data from 101 consecutive patients who underwent this technique were collected in a prospectively-maintained database. Inclusion criteria were tumor size <=4cm, predominant exophytic growth and intraparenchymal depth <=1.5cm with a minimum distance of 5mm from the urinary collecting system. Hilar vessels were not isolated, tumor dissection was performed with 10-mm LigaSure, and hemostasis was performed with coagulation and biologic hemostatic agents without reconstructing renal parenchyma.ResultsMedian tumor size was 2.4cm (range:1.5-4 cm), and median intraparenchymal depth was0.7cm(range:0.4-1.4 cm). Hilar clamping was not necessary in any case, and suture was performedin four cases to ensure a complete hemostasis. Median operative time was 60min (range:45-160min), and median intraoperative blood loss was 100 ml (range:20-240 ml). Postoperativecomplications included fever(n=4), low urinary output(n=3), and hematoma treatedconservatively(n=2). Median hospital stay was 3d (range:2-5d). The pathologist reported 30benign tumors and renal cell carcinoma in 71 cases (69 pT1a, 2 pT1b). At a median follow-up of 57mo, one patient underwent radical nephrectomy for ipsilateral recurrence. One-year mediandecrease of split renal function at renal scintigraphy was 1% (range:0-5%).Conclusion Zero ischemia LPN is a reasonable approach to small and peripheral tumors, and asutureless procedure is feasible in most cases. This technique has a low complication rate andprovides excellent functional outcome without impairing oncologic results.
Laparoscopic Partial Nephrectomy with Controlled Hypotensive Anesthesia to Avoid Hilar Clamping.
Introduction Unclamping techniques are emerging as a desirable approach for nephron-sparing surgery (NSS).Matherials and MethodsSixty patients with renal tumors eligible for NSS and without any contraindications to hypotensive anesthesia underwent partial nephrectomy (PN) without hilar clamping and with controlled hypotension (CH) during tumor excision. Forty Laparoscopic Partial Nephrectomy (LPN) and 20 (RAPN) were performed. A transperitoneal approach was performed used. Intra-operative pressure using to create the pneumoperitoneum was 14 mmHg. Selective hilar microdissection was performed and vessels supplying the tumor were identified, selectively clip-ligated and transected with cold scissors. Hemostasis was completed performing a parenchymal suture.ResultsThe zero ischemia procedures with CH was successfully completed all cases. Median tumor size was 3,6 cm (range: 1.8-10); operative time was 2 h (range 1-3.5), blood loss was 200 ml (range 30-700), and hospital stay was 3 d (range 3-8). Median duration of CH with a median MAP of 65 mmHg (raange 55-70) was 14 minutes (range 7- 16). During surgery blood transfusion was not necessary in any patient. Four patients required one packed red blood transfusion postoperatively.Postoperative complications occurred in 3 patients: port site bleeding, hemorrhage and hematoma. Median pre and postoperative serum creatinine levels were 0.9mg/dl and 1.02mg/dl, while eGFR was 91,11 and 70,06, respectively.Conclusions In our experience CH allowed to perform LPN and RAPN without the need of renal hilum clamping. All procedures were safely completed and perioperative outcomes are encouraging.
Partial Nephrectomy by Retroperitoneoscopy without Hilar Clamping
ABSTRACT WITHDRAWN
Dept. Urology, Univeristy Hospital MIguel Servet, Zaragoza, Spain
ObjectivesWe analyzed KTP laser laparoscopic partial nephrectomy feasibility and compare it with conventional laparoscopic partial nephrectomy. Material and Methods30 pigs were randomized to either laparoscopic KTP partial nephrectomy or conventional partial nephrectomy.Previously, right laparoscopic partial nephrectomy was done in all animals, in order to make a mono-kidney model, and to analyze the impact of surgery in renal function. Tumor model was placed in the left kidney All partial nephrectomy were done until collecting system in all kidneys. Follow up has done for 6 weeks, with blood and urine test. Doppler color ultrasound and retrograde pyelography at presurgery, postsurgery, at 3 weeks and at the end of the study, to study renal function and healing of urinary systemAt the end of the study, pathological exam of both kidney and surgical specimen was done. Results:We present the feasibility of KTP laser laparoscopic partial nephrectomy. We show in this video kidney parenchymal resection until collecting system, through a laparoscopic approach, in a viable and safe manner. Conventional laparoscopic technique is explained as a gold standard and its comparison with laser technique.There were 2 urinary fistulas in the laser group versus none in the conventional group. All KTP laser partial were performed without ischemia.No differences were seen in surgical marginConclusions:Laser KTP Partial Laparoscopic Partial Nephrectomy is feasibility and safe in the animal model. It may result in an easier and simpler alternative to conventional laparoscopic partial nephrectomy.
Department of Urology, Kosin University, Busan, Korea
OBJECTIVES: We evaluated the feasibility, safety, and effect of transperitoneal laparoscopic heminephrectomy in the adult duplex kidney.METHODS: We retrospectively reviewed the records of patients with urinary tract duplex abnormalities who underwent transperitoneal laparoscopic heminephrectomy between 2010 to 2011. We placed ureteral stent preoperatively in normal ipsilateral ureter for identification and for preventing injury. Carefully, we exposed and ligated polar renal arteries, and then, excised affected renal moiety. After complete resection, parenchymal suture was done for hemostasis. RESULTS: Three patients were underwent heminephrectomy and they were all female. The sites of surgery consisted of 2 left lower, and 1 left upper heminephrectomy. The presenting symptoms were recurrent urinary tract infection and flank pain. All patients underwent laparoscopic surgery successfully without open conversion. The mean operative time was 170 minutes (range 160-190). The mean estimated blood loss was 250 mL (range 150-400). There were no major complications such as urinary leakage, fistula, and open conversion. The radiologic assessment showed normal ipsilateral renal growth without atrophy or hydronephrosis at follow-up of 6-12 months.CONCLUSIONS: Our initial clinical experience suggests that laparoscopic heminephrectomy using a transperitoneal approach for the duplex kidney is feasible, safe, and effective.
Managing Parahilar Tumors during Laparoscopic Partial Nephrectomy: Use of Hilar Dissection and Sinus Fat Plane
Partial nephrectomy(PN) has been accepted as a reference standard for SRMs. Although laparoscopic approach (LPN) may provide rapid convalescence, its open counterpart is often preferred in complex situations like solitary kidneys or parahilar location. WeperformLPN for such renal masses using the sinus fat plane. A small mass encroaching renal sinus lip will expand renal capsule and is unlikely to encroach the sinus fat. The sinus fat also provides the dissection plane at depth, the plane most likely to be transgressed during surgery, thus providing safe margins.We present two such complex situations dealt with LPN. The first case is a 4 cm mass at left renal hilum encroaching the lower pole. The mass at the hilum was displacing the vessels as well as the renal pelvis anteriorly. In the second case, a 7.5 cm left parahilar renal mass in a solitary kidney was managed with LPN. The mass involved lower pole and the anterior cortical lip, pushing the pelvicalyceaal system posteriorly. Hilar dissection of the vessels and their branches and the renal pelvicalyceal system provide important guides for dissection.32 of 35 parahilar masses could be managed with LPN with average warm ischemia time of 23.5 minutes. Average operating time was 140 minutes and estimated blood loss was 350 ml. Major complications included prolonged urinary leak (>2 weeks) in 6 cases, laparoscopic re-explorarion in 1 and angioembolization in 2 cases .There were no positive margins. LPN via sinus fat plane can thus be accomplished in complex hilar and parahilar masses.
Simultaneous Double Partial Nephrectomy For A Double Ipsilateral Tumor
ABSTRACT WITHDRAWN
Laparoscopic Partial Nephrectomy in Polycystic Kidney
ABSTRACT WITHDRAWN
VS02: Robotic Partial Nephrectomy
Robot-Assisted Partial Nephrectomy of Eight Renal Masses with No Ischemia Time
IntroductionRobot-assisted partial nephrectomy (RAPN) has emerged as a viable alternative to open nephron-sparing surgery (NSS) for small renal tumors in select patients [1]. However, the role of RAPN in the treatment of multiple, ipsilateral tumors is not well established. Warm ischemia time (WIT) has typically limited the utilization of RAPN in these patients. Recently, successful laparoscopic NSS and RAPN with no WIT have been described [2]. Minimally invasive approaches and minimization of WIT are beneficial to most patients, but are especially important to those with hereditary renal cancer syndromes who frequently require repeat interventions for recurrent as well as de novo disease. PurposeTo demonstrate a technique of RAPN with no WIT as a viable approach to the treatment of multiple renal masses.Materials and MethodsOperative, radiologic, laboratory, and pathology data were obtained from chart review. Functional outcome was assessed using estimated GFR (eGFR) before and after surgery, calculated by the MDRD equation. All video was recorded intraoperatively. Results and ConclusionsOur patient was 37 years-old at the time of intervention and suffered from known von-Hippel-Lindau. His preoperative eGFR was 161mL/min/1.73m2. Total operative time was 304 minutes with estimated blood loss of 1500mL. A total of eight masses were removed. Final pathology found one atypical cyst and seven Fuhrman grade III clear cell RCC masses, measuring between 1.0 and 3.9cm. All margins were negative. He was discharged on postoperative day five. His eGFR on discharge was 174mL/min/1.73m2.
Renovascular and Tumor 3-D Reconstruction to Facilitate Zero-Ischemia Partial Nephrectomy
Cold Ischemia via Retrograde Cooling for Robotic Partial Nephrectomy in Patients with Solitary Kidney
PURPOSE: Renal hypothermia is commonly utilized during nephron sparing surgery to minimize ischemic tissue damage. We propose a method to induce renal hypothermia using continuous retrograde irrigation of iced saline via dual-lumen ureteral catheter and report results first in an ex-vivo porcine model and then clinical outcomes in a series of patients with solitary kidney undergoing robotic assisted laparoscopic partial nephrectomy (RALPN).MATERIALS AND METHODS: We performed temperature measurements during retrograde renal cooling first in a porcine model before investigating the technique in humans. In porcine experiments, renal cortical temperature measurements (n=270) were recorded during retrograde infusion of ice cold saline via a 10Fr dual lumen ureteral catheter placed in ureter. Subsequently, a series of patients (n=7) undergoing (RALPN) with a solitary kidney had concomitant intra-operative retrograde renal cooling. A 10 Fr dual-lumen ureteral catheter was placed at initiation of anesthesia and cold saline initiated prior to renal artery clamping. RESULTS: Porcine cortical temperature reached the target temperature (greater than or equal to 20 degrees Celsius) within an average of 203 seconds of retrograde irrigation. In the clinical series, patients' mean preoperative creatinine was 1.24mg/dL (GFR=61). At a median followup of 7months (range 2-12 months), post-operative creatinine was 1.87mg/dL (GFR=47). Average clamp time was 19 minutes. All patients had negative surgical margins. CONCLUSIONS: Retrograde irrigation is a technically feasible method to induce cold ischemia which may provide an additional protective effect of renal function in patients who have a solitary kidney undergoing surgery via a minimally invasive approach.
Robotic Zero-ischemia Partial Nephrectomy for Hilar Tumors.
Introduction Significant concern with robotic partial nephrectomy (RPN) is the warm ischemia time (WIT). Recently we reported our initial experience with a novel Zero-ischemia laparoscopic/robotic partial nephrectomy (PN) technique.Purpose Detail our Zero-ischemia RPN for hilar tumors technique and present peri-operative outcomes.Patients and MethodsFrom 05/2010 to 05/2011, over 100 patients underwent minimally invasive zero-ischemia PN (21 RPN). Of these, 7 RPN for hilar tumors. Briefly, Zero-ischemia technique consists in excise renal tumor performing renovascular microdissection and applying superselective neurosurgical micro-bulldogs in specific arterial feeding tumor, avoiding global renal ischemia. The procedure was offered to all comers irrespective of tumor complexity, vascular anatomy or renal function. Data were prospectively collected and analyzed. Results Zero-ischemia RPN was successful in all seven cases without hilar clamping, conversion to open surgery or radical nephrectomy. Mean Age (years), tumor size (cm), C-index, R.E.N.A.L. score were 59, 3.8, 1.5, 9.4, respectively. Mean operative time (min), WIT (min), estimated blood loss (cc), percent kidney spared, hospital stay (days) were 237, zero, 228, 74, 4.1, respectively. Transfusion was required in one patient. There were two complications (Clavien grade I and II). Pathology showed malignancy in 6 cases with all tumors margins negative. Mean pre-operative and discharge serum creatinine (mg/dl) and eGRF were 1.1, 1.3 (p=0.38) and 66, 67 (p=0.83), respectively. Conclusion Zero-ischemia RPN for hilar tumors is safe and feasible. To our knowledge, the initial report is presented. Global renal ischemia may not be necessary. Absence of warm ischemia seems to optimally preserve renal function.
Advances in Robot-Assisted Partial Nephrectomy
Introduction
Robot assisted partial nephrectomy (RAPN) is a minimally invasive approach for nephron sparing surgery. We demonstrate recent advances in RAPN and discuss related outcomes.
Methods
Three novel developments have modified our operative technique. A flexible Doppler probe (Vascular Technology Inc.) is now used in select cases for the identification of hilar vessels. Robotically applied bulldog clamps (Klein Surgical Inc) allow for hilar clamping to be performed by the console surgeon without dependence on a skilled bedside assistant. The V-Loc 180 (Covidien) is a unidirectional barbed suture used for knotless renorrhaphy.
Results
The flexible Doppler probe is used to identify renal vessels and does not need a dedicated port. It also helps in the confirmation of renal parenchymal ischemia when there is suspicion of unrecognized aberrant vessels. Robotic bulldog clamps were recently compared to a consecutive series of patients with the standard bulldog clamps. There were no intraoperative complications in the former group and there was a trend towards shorter operative and shorter console time.In a recent series we compared RAPN with the V-loc and vicryl sutures and found the V-loc group had a warm ischemia time (WIT) that was shorter by 6.2 min (18.5 vs. 24.7 min, p=0.008) even though the baseline characteristics were equivalent between the two groups. This represented a 25% reduction in WIT.
Conclusion
The flexible Doppler probe and robotic bulldog clamps help with the critical steps of hilar dissection and clamping, while Vloc-renorrhaphy brings about a significant reduction in the WIT during RAPN.
Robotic Partial Nephrectomy for Renal Cell Carcinomas with Venous Tumor Thrombus
Introduction: Renal cell carcinoma (RCC) has a predilection for extension into veins, which can prevent the ability to perform partial nephrectomy when otherwise possible. Objective: Partial nephrectomy with venous tumor thrombus is feasible when venous drainage of the remaining kidney is preserved and negative surgical margins can be achieved. We present two first such reports of robotic partial nephrectomy (RPN) in the setting of venous extension of RCC, including one with extension into a vein branch within the parenchyma and a second case extending into the main renal vein. Methods: One 4.3cm tumor was found to have extension into a branch of the renal vein on intraoperative ultrasound. The mass was excised with the vein and tumor thrombus as one unit, following the vein into the parenchyma until the end of the tumor thrombus was found. Another patient undergoing heminephrectomy for a 9.3cm RCC had extension from one of two major branches into the main renal vein. The tumor and associated branch were excised as one unit, extracting the tumor thrombus from the main renal vein with suture reconstruction for drainage of the remaining half of the kidney. Results: Both were performed with less than 30min of warm ischemia time. Both patients were discharged on the first postoperative day without complications and with negative surgical margins. Conclusion: RPN can be successfully performed for selected tumors with venous tumor thrombus. While local control can likely be achieved as well as nephrectomy, systemic recurrence remains the greater threat in such T3a patients.
Section of Laparoscopic and Robotic Surgery, Department of Urology, Frimley Park Hospitals NHS Foundation Trust. Surrey. UK
Robotic Assisted Laparoscopic Partial Nephrectomy in a Jehovahs Witness Patient - Hemostatic Techniques
Introduction and Purpose: Partial nephrectomy can be associated a significant blood loss. This can be a serious problem in Jehovahs Witness patients because of religious beliefs prohibiting transfusion of blood products. We demonstrate techniques to minimize blood loss during robotic partial nephrectomy.Methods: A 52-year-old Afro-american patient (BMI of 37) presented with a 4 cm right lower pole enhancing renal mass. He has history of MI, hypertension and diabetes with a preoperative serum creatinine of 1.1mg/dl. His Hb was 14g/dl. A lower pole partial nephrectomy was performed using a standard daVinci robot with 3 arms. The mass was excised under laparoscopic ultrasound guidance. The renal bed including the collecting system suture closure was performed in 2 layers. Parenchymal renorrhaphy was performed using sliding clip technique. Argon beam coagulator and Floseal; hemostatic agent was also used. We have incorporated the above hemostatic techniques in 40 patients during robot-assisted partial nephrectomy.Results: The warm ischemic time was 27 minutes. The estimated blood loss was 100mls. His hematocrit on post operative day 1 was 39%. The patient was discharged on post-operative day 3. The hemoglobin remained stable at a month follow up visit. His serum was 1.45mg/dl. Pathology confirmed clear cell renal carcinoma (T1a), Furhman grade II with negative margins. With the above hemostatic techniques in 40 patients, there were no blood transfusions, conversion to open procedure or radical nephrectomy. Conclusions: Robotic lower pole partial nephrectomy for a renal mass in a Jehovahs Witness with methods for hemostasis is reviewed.
VS03: Robotic/Laparoscopic Prostate Surgery 1
Anatomical Considerations in Nerve-Sparing Robotic Radical Prostatectomy-Tottori experience-
We describe a technique of anatomical robotic radical prostatectomy, which considers pelvic anatomy in regard to autonomic nerves and pelvic fascias in order to achieve trifecta of radical prostatectomy
Incision of the endopelvic fascia
Levator fascia is bluntly dissected off from the prostatic fascia. When a nerve-sparing is performed, this incision is not extended to the apex of the prostate for the prostatic color preservation.
Transection of the posterior bladder neck
There is no histological boundary or surgical plane in this area. The landmark which denotes the end of this muscle layer incision is the longuituidal muscle fiber which continues from the longuituidal bladder detrusor.When the longuituidal muscle fiber is incised, fibroadipose tissue in continuation with the bladder adventitia is exposed.
Exposure of the posterior prostate
A firm membrane of the Denonvilliers fascia should be incised.
Hemostasis of the vascular pedicle
To avoid thermal injury and traction injury, the sliding clip technique is used. To simplify this technique, 3-0 barbed suture is employed.
Preservation of the prostatic fascia
We classify the nerve sparing grade into four grades.
Posterior reconstruction
To simplify this continuous suture, the 3-0 barbed suture is employed. The reconstruction is done double-layered. Distal suture should not contain rhabdosphincter for fear of the cavernous nerve injury.
Anterior reconstruction
This step involves using a 3-0 barbed suture to approximate remaining arcus tendineus and puboprostatic ligament to the bladder neck.
Instituto Medico la Floresta, Caracas Venezuela
INTRODUCTION AND OBJECTIVES: Minimally invasive approaches for treatment of localized prostate cancer are replacing the gold standard open surgical approach, duplicating its results with lower morbidity. Concerns have been raised regarding possible traction injury for an anterograde robotic or laparoscopic approach., we describe our experience with retrograde robotic radical prostatectomy.METHODS: Technique: transperitoneal port placement, posterior peritoneotomy,. The bladder is released from the anterior abdominal wall, endopelvic fascia and lateral prostatic fascia are incised, beginning the neurovascular bundle (NVB) release starting at the mid gland to the apex. A back-bleeding suture is placed, the dorsal venous complex is ligated. The urethra is transected, apical dissection is completed, vas and seminal vesicle dissection, and rectum release. The bladder neck is dissected. The pedicle, now better defined in relation to the distal NVB and prostate contour, is divided and completed. The urethro-vesical anastomosis performed.RESULTS: This is a feasible procedure. Challenges in visualizing the apex can be overcome with a 30 degree down lens, and retraction on the back-bleeding stitch. Potentially, a precise apical NVB dissection is accomplished. The retrograde approach potentially avoids over dissection of the bundle beyond the urethra-prostate junction.CONCLUSIONS: Open retrograde technique can be duplicated robotically To overcome challenges in visualizing this plane, the 30 degree down lens and retraction on the backbleeding suture are helpful.Advantages include more precise apical bundle dissection, avoiding overdissecting of the bundle beyond the urethra- prostate junction, and facilitating dissection of the distal 1/3 of the neurovascular bundle Further studies are needed.
instituto Medico la Floresta, Caracas Venezuela
INTRODUCTION AND OBJECTIVES: Robot-assisted laparoscopic radical prostatectomy is used for the management of organ confinated prostate cancer. Although complications are uncommon, incisional hernias at extraction site have been reported and their impact on the morbidity can be serious. For development of incisional hernia there are personal and physical risk factors and those related with the surgical technique. The overall incidente of hernias in the trocar site is around 0.65 to 2.8%. Usually, the camera port placed 1-2 cm above the umbilicus is enlarged to accommodate the size of the prostate to be removed which increases the risk. we report our experience in the diagnosis and management of incisional hernias after robot-assisted laparoscopic radical prostatectomy.METHODS: We recorded data on 275 patients who underwent to robot-assisted laparoscopic radical prostatectomy at our institution since 2007 to 2010, who presented incisional hernias by the site of extraction of the surgical specimen or in the trocars placed in different locations from the midline.RESULTS: to date, we found 2 patients with incisional hernia, one at the site of specimen extraction which noted than increase the periumbilical wound volumen after 3 months, and in a second patient, hernia was identified at the site of the right lower quadrant trocar.CONCLUSIONS: Incisional hernia at the site of port placement is a rare condition, but is a potentially serious complication after robot-assisted laparoscopic radical prostatectomy. Further studies are needed to estimate the incidente, the risk factor, how to prevent and suggest the best approach to repair
Management of Difficult Anatomy During Robot Assisted Radical Prostatectomy: The Median Lobe
INTRODUCTION AND OBJECTIVES: To report the effect of median lobe on perioperative outcomes, positive surgicalmargin (PSM) rates and short-term urinary continence outcomes after RARP.METHODS: We analyzed 1693 consecutive patients who underwent RARP by a single surgeon for treatment of clinicallylocalized prostate cancer. Patients were categorized in two groups based on the presence or absence of a median lobe identifiedduring RARP. RESULTS: Median lobe was intra-operatively identified in 323 (19%) patients. Patients with median lobes were slightlyolder (median 63 vs. 60 years, p<0.001), had higher PSA levels (median 5.7 vs. 4.7ng/ml, P<0.001) and higher AUA-SS beforeRARP (10 vs. 6, p<0.001). The number of bladder neck reconstruction procedures (93.5% vs. 65.7%, p<0.001) and the medianprostate weight (64 vs. 46g, p<0.001) were also higher. The median OR time was slightly greater in patients with median lobe(80 vs. 75minutes, p<0.001). Continence rates were also equivalent between patients with and without median lobe at 1week (27.8% vs. 27%,p=0.870), 4 weeks (42.3% vs. 48%, p=0.136), 6 weeks (64.1% vs. 69.5%, p=0.126), 12 weeks (82.5% vs. 86.8%, p=0.107) and24weeks (91.5% vs. 94.1%, p=0.183. Finally, the median time to recovery of continence was similar between the groups in theKaplan-Meier curves (median: 5wks, 95% CI: 4.41-5.59 vs. median: 5 wks, CI 4.66-5.34; log rank test, p=0.113)CONCLUSIONS: The presence of a median lobe does not affect perioperative outcomes, PSM rates and early continenceoutcomes in patients undergoing RARP.
The role of the Prostatic Vasculature as an Intraoperative Landmark for Nerve Sparing During Robot Assisted Radical Prostatectomy
Introduction and Objective: Preservation of the cavernosal nerves is one of the most challenging steps during radical prostatectomy, in part due to the lack of consistent macroscopic landmarks that can aid in the intraoperative identification of these microscopic structures. The prostatic artery runs along the lateral border of the prostate and could aid in identifying the location of the cavernosal nerves during robot assisted radical prostatectomy. The aim of this study is to assess the role of the prostatic vasculature as a landmark for nerve sparing during robot assisted radical prostatectomy. Materials and methods: The data of 133 consecutive patients operated between January and February 2011 were prospectively collected. Intraoperative assessment was performed in order to identify the relation of the NS technique to the prostatic arterial supply. The area of residual nerve tissue on prostatectomy specimens was measured as a proof of the degree of NS.Results: The prostatic artery running along the lateral border of the prostate was identified in 73.3% (195/266) of the operated sides. The area of residual nerve tissue was significantly different whether the NS was performed medial (between the prostatic artery and the prostate) or lateral to the prostatic artery (median (IQR) of 0 (0-3) mm2 vs 14 (9-25) mm2, p<0.001). Conclusion: The prostatic artery is an identifiable landmark during NS. Fine tailoring on its medial border can consistently result in a complete or almost complete NS, while performing the NS on its lateral border results in several degrees of incomplete NS.
Direct Comparison of Three Different Methods for Performing the Urethro-Vesical Anastomosis During Extraperitoneal Laparoscopic Radical Prostatectomy.
Objective of this paper was to compare three methods for performing urethro-vesical anastomosis during extraperitoneal laparoscopic radical prostatectomyMaterial and method We included in this study 25 patients in which extraperitoneal laparoscopic radical prostatectomy was performed at the Ion Chiricuta Oncological Institute Cluj Napoca. The urethro-vesical anastomosis was performed using three different techniques: VanVelthoven technique, Single knot running suture and no knot running suture using V-lock;. The compared parameters were: time to perform the anastomosis, number of points of suture, leakage days and incidence of anastomotic strictures.Results The VanVelthoven technique was performed in 16 patients, Single knot running suture in 6 patients and no knot running suture using V-lock; in 3 patients. The time to perform the anastomosis was significantly higher for the VanVelthoven technique 39 vs 16.6 vs 18 min respectively. The VanVelthoven technique was used at the beginning of the learning curve. There were no differences between the number of points of suture 6,812 vs 6,83 vs 6,67 and leakage days 0,85 vs 0,66 vs 1. 3 patients presented anastomotic strictures in the VanVelthoven technique group, but the follow-up in this group is significantly longer than in the other two groups 7 vs 2 vs 1.Conclusions There are no differences between these methods with regard to number of points of suture and leakage days. The VanVelthoven technique seems to take a longer time to perform compared to the other two. The incidence of anastomotic strictures is higher for the VanVelthoven technique but longer follow-up is needed.
Department of Urology, Anjo Kosei Hospital
[OBJECTIVE] We evaluated the potential advantage of our original procedure of an Extraperitoneal two-port endoscopic radical prostatectomy(2-ERP). [METHODS] Since November, 2010, we have performed 2-ERP for early-stage prostate cancer (cT1c,T2). Througha lower umbilical U incision, a multi-channel trocar (EZ ACCESS, EZ trocar 5mm, Lap protector, Hakko, Japan) was placed just beneath the rectus muscle and anterior to the peritoneum. A 5 mm laparoscope with a flexible tip used by an assistant. We used standard laparoscopic instruments and a harmonic scalpel (Harmonic ACE , Ethicon EndSurgery). An additional 12 mm port was inserted in the left fossa. [RESULTS] The operation could be successfully completed without any necessity for open conversion. Our technical points were as followed. 1. The dorsal vein complex ligation and an urethrovesical anastomos were performed using left hand. 2. A metal angle-bougie was inserted to draw the prostate in an anterior direction after the bladder neck incision. 3. Careful camera work was needed in the left side prostatic fibrovascular pedicles incision. [CONCLUSIONS] The potentialadvantage of this new approach is similar surgical method to conventional five port Laparoscopic RP, using standard laparoscopicinstruments, less crashing with laparoscope and instruments, adequate working angle, advantageous hemostasis(Hemolock in left side 12mm port independent of laparoscope) and unnecessary Trendelenburg position. This minimal invasive technique appears to be good compromise between a pure LESS-RP and standard Laparoscopic-RP.
Modifications to facilitate extraperitoneal robot assisted radical prostatectomy post kidney transplant
Introduction:Advances in immunosuppression have significantly improved the long-term outcome of renal transplant recipients. Subsequently, urologists are encountering more transplant recipients with genitourinary malignancies and therefore urologists are becoming increasingly compelled to offer curative treatment options. Materials and methods:We present modifications to facilitate extraperitoneal robot assisted radical prostatectomy (E-RARP) in these patients that include; modified trocar arrangement, late division of the bladder neck, utilizing the robotic Hem-o-loc applier, posterior reconstruction of the anastomosis using a barbed suture and introduction of the specimen bag via the midline trocar. A 68 years old male with end-stage renal failure and an allograft renal transplantation in the right iliac fossa, presented with T1c, Gleason 3+3 prostate cancer. Patient characteristics included; preoperative PSA of 6.93ng/ml, ASA score 3, BMI of 26 kg/m2 and a negative work-up for metastasis (MRI and Bone scan). A 5-port 3-arm approach at an insufflation pressure of 10mmHg was utilized. Results:E-RARP was successful at a total console time and estimated blood loss of 130 minutes and 125 ml. A unilateral interfascial nerve sparing procedure was performed. Final pathology was T2bNx, gleason 3+4 with negative surgical margins. The catheter was removed at POD 10 with no intraoperative or immediate postoperative complications and stable serum creatinine. At 6 months follow-up, PSA remained undetected (0.04) with satisfactory functional outcomes (1 security pad / day).Conclusion:E-RARP in the carefully selected renal allograft recipient is feasible and accomplished safely with technical modifications to avoid injuring the renal allograft, transplanted ureter, and ureteroneocystostomy.
VS04: Notes/Less 1
Experience Sharing on Laparo-Endoscopic Single Site Surgery LESS Nephrectomy with Glove Port
Introduction:LESS surgery is one of the fastest developing fronts in modern day surgery. There are a lot of hurdles for surgeons to overcome in the development of this technique. High cost and fighting for space are the two mostly encountered difficulies.
PurposeThis study described the difficulties encountered in LESS nephrectomy. Possible solutions to these difficulties were suggested.
Materials and Methods:We described our LESS nephrectomy approach using home made glove and wound retractor. The set up and the operative procedures were described in surgical video. The results of LESS nephrectomy in our center were retrospectively reviewed.
Results:To avoid clashing of instruments inside the body, using a 5cm wound and both curved and straight instruments would be used. Staggered trocars, extra-long instruments and reversing the handle could avoid clashing instruments outside the body. Intussception of trocar into the glove port avoided trapping intruments and the sutures would facilitates tissue retraction. From March 2010 to January 2011, 7 patients had LESS nephrectomy done. Glove ports were used in the 5 cases. The mean age of the patients was 68 years old. The mean operative time was 198min including two cases of nephroureterectomy and the mean blood loss was 190ml. All the patients had uneventful recovery.
Conclusions:Glove port can be used to facilitate LESS nephrectomy to cut done on cost with satisfactory results.
Less Simple Nephrectomy
INTRODUCTIONWhile laparoscopic nephrectomy has become the gold standard for many years, single port nephrectomy is still in the early phase and the acual benefits of this technique is still being studied.PURPOSETo report our initial experience with LESS nephrectomy.PATIENTS AND METHODS8 patients underwent single port simple nephrectomy. SILS port was used in 6 and Triport was used in 2. All the procedures were left nephrectomies, with specimen extraction through the port site. Patients age range was 18 to 41, BMI was less than 25 kg/m2. Indication for nephrectomy was for atrophic non functioning kidneys. 4 patients had chronic renal failure and were scheduled for transplantation.RESULTS Mean operative time was 110 minutes. Blood loss was less than 50 cc. pain score was between 1 to 2 in all patients. Hospital stay was 1 day. No inta o rpost operative complications were encountered. No analgesics were required. CONCLUSIONWith the superior cosmetic outcome single port nephrectomy is an attractive alternative to laparoscopic nephrectomy, in selected patients. Larger number of procedures are required with sufficient follow-up data, are required to point out the actual role of single port nephrectomy.
Single Incision Laparoscopic Left Nephrectomy Using the GelPoint Device
Introduction: Single incision laparoscopic surgery has potential benefits over traditional minimally invasive techniques including fewer scars, less pain and shorter recovery times. The GelPoint device is an available access port to help accomplish these procedures.Purpose: This video demonstrates the current technique for a single port laparoscopic nephrectomy using the GelPoint device at our institution.Materials and Methods: The patient shown in this video is an 18 year-old man with a history of left abdominal pain and a renal scan showing 10% function of the left kidney. Computed tomography was consistent with a chronic left ureteropelvic junction obstruction with severe hydronephroisis. For this operation, a 5mm, 30 degree down camera was used with a GelPoint device and non-articulating laparoscopic instruments. No additional ports were needed throughout the procedure.Results: The operation was completed with minimal blood loss and without complication. Total operative time was 125 minutes. The patient was discharged home less than 24 hours after surgery. Conclusions: As shown in this video, using the GelPoint device to complete a single incision laparoscopic nephrectomy is a quick, safe and effective treatment for select patients with excellent cosmetic and surgical outcomes.
Less Pyeloplasty
INTRODUCTION Laparoscopic pyeloplasty has become the standard of care in treatment of primary ureteropelvic junction obstruction(UPJO).PURPOPSEto report our initial experience with LESS pyeloplasty.PATIENTS AND METHODS 4 patients underwent LESS-pyeloplasty (LESS-P) by the same surgeon. We used SILS port that was inserted through a 20-30-mm umbilical incision.Anderson-Hynes technique was used in all patients. I.V.U and diuretic renogram were done to all patients preoperatively. Ultrasonography 3 months , and diuretic renogram 6 months postoperative. RESULTS Patients age range 18 to 22 years old. Mean operative time 193 min.Mean blood loss was negligable.Hospital stay was 2 days. Visual analogue pain score was ranging from 1 to 2 for all patients. No need for analgesic use in the early post operative period. All the procedures was completed successfully without need for additional ports our instruments. We developed our own technique in suturing to overcome the difficulties with the use of the single port surgery.A percutaneous antegrade stenting technique was used in all patients.uretheral catheter were removed after 7 days while ureteral stents were removed after 6 weeks. Mean follow up period was 4.6 months. Success rate was 100%, with no back pressure on ultrasonography, and no residual obstruction to drainage on diuretic renogram. CONCLUSION LESS pyeloplasty is a promising technique, although its technically demanding, and needs a high level of laparoscoplic skill. We need a larger number of cases with longer follow up, and radomised controlled trials to establish the success of this technique.
Less Ureterolithotomy
INTRODUCTION AS the laparoendoscopic single site surgery(LESS) using a transumbilical access represents the closest surgical technique to scarless surgery we assess the feasibility of LESS in management of ureteral stones .PURPOSEto report our initial experience in LESS ureterolithotomy.PATIENTS AND METHODS Four cases of LESS ureterolithotomy were performed by a single laparoscopic surgeon. The indications for LESS ureterolithotomy were a stone size of larger than 20 mm, an impacted stone or failure of endourological management. All procedures were done using SILS port that was inserted through a 20-30-mm umbilical incision. Patients age range was 36 to 44, BMI was less than 25 kg/m2.Articulating instruments were used.RESULTS Mean operative time was 87 minutes. Blood loss was less than 50 cc. The mean stone size was 22.4 mm. The stones were located in the upper ureter in two patients and in the middle ureter in the other 2 patients.Ureteral stent were fixed in all patients after stone remval.Pain score was between 1 to 2 in all patients. Mean hospital stay was 2 days. Uretheral catheter were removed after 5 days. No intra or post operative complications were encountered. No analgesics were required. Ureteral stent were removed after 4 weeks.CONCLUSION LESS ureterolithotomy is technically feasible procedure however a large number of cases is needed to establish its efficiency as a line of management.
Instituto Medico la Floresta, Caracas Venezuela
INTRODUCTION AND OBJECTIVES: Present a technique for the management of the bladder cuff during distal ureterectomy under pneumovesicum using a single port device inserted transvesically.METHODS: Two cases, the first case a patient with malignant disease an 80 year old man with a 5cm left renal pelvic tumor. Second case in a 25 year old woman with history of recurrent urinary tract infections in whom with upper pole hydroureteronephrosis.RESULTS: The first patient underwent left laparoendoscopic single site (LESS)radical nephroureterectomy with retroperitoneal lymph node dissection and bladder cuff excision under pneumovesicum for a left renal pelvic transitional cell carcinoma; final histopathology revealed pathologic G3 T3 N0 with 7 negative nodes. and estimated blood loss 250cc. No postoperative complications or recurrence were noted after one year of follow up. The second patient underwent LESS upper pole heminephroureterectomy for treatment of a duplicated left collecting system and upper pole hydronephrosis. Final pathology revealed chronic pyelonephritis. The operative time 210 minutes including 30 minutes for bladder cuff excision and estimated blood loss was 400cc, length of stay was three days. Postoperatively the patient presented lower pole renal vein thrombosis.CONCLUSIONS: LESS transvesical bladder cuff excision may offer many advantages including the ability to allow precise marking of the bladder cuff, avoiding potential injury to the contralateral ureteral orifice, and allowing water-tight closure of the bladder. It can be performed trough a small suprapubic skin incision with a small cystotomy pubic incision it can be also then used to assist the laparoscopic dissection.
Less Radical Cystectomy
INTRODUCTIONLaparoscopic radical cystectomy is not as popular as other laparoscopic procedures. However in our center it is most commonly performed. With the introduction of LESS, we are exploring the benefits and the feasibility of LESS in many procedures.PURPOSETo report our initial experience with LESS radical Cystectomy PATIENTS AND METHODS10 males underwent single port radical cystectomy, 9 using SILS port and one using single port access system from ethicon. Age range was 52- 74, all had BMI below 24 kg/m2, and all had no morbidities. Patients were selected with small size bladder masses. Diversion was performed through a separate pfennistiel incision all patients had orthotopic diversion with internal stents. RESULTS 9 of the 10 proceedures were completed successfully, and one was converted to open surgery due to local advanced disease.The mean operative time was 230 minutes for the cystectomy an lymphadenectomy. Blood loss was 600ml on the average.Time to oral feeding was 3 days, hospital stay was 5 days. Catheter time was 15 days, and stents were removed with the uretheral catheter, as they are fixed together. We encountered no intra or postoperative complications. CONCLUSIONWhile single port radical cystectomy is feasible, we concluded that it needs to be performed in highly selected patient. At this point we see no added benefit to laparoscopic radical cystectomy, however with the continuous development instrumentation and devices, we would expect it to become easier.
VS05: Adrenal/Upper Urinary Tract
Department of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction: Pheochromocytoma is one of the common tumours of the adrenal gland. 10% of adrenal tumours are bilateral. Laparoscopic adrenalectomy is the treatment of choice for pheochromocytoma. We present the video of laparoscopic excision of bilateral pheochromocytoma. Materials and Methods: A 34 year old male patient presented with uncontrolled hypertension. On evaluation he was found to have bilateral adrenal masses (8 cm on the right side and 4 cm on the left side) with elevated urinary catecholamines. Laparoscopic excision of the mass on left side (sparing normal adrenal gland) and laparoscopic adrenalectomy on right side was done. Patient was placed in the right lateral position initially. Using 4 ports, colon was mobilised and left adrenal mass was dissected. Pedicles were controlled and mass was excised. After completion on the left side, the position of the patient was changed to left lateral maintaining the previous epigastric port. Additional 3 ports were placed and right adrenalectomy was completed. The specimen were removed through a 6 cm muscle splitting incision in the right iliac fossa. Port sites were closed after placing a drain. Results: The operative time was 280 min. Blood loss was 150 ml(Approx). Post op stay was 3 days. Patient had adequate control of blood pressure with a single calcium channel blocker post operatively. He is on steroid and minerallocorticoid supplementation. Conclusion: Laparoscopic bilateral adrenalectomy is a feasible procedure with minimal morbidity in patients with bilateral adrenal tumour.
Departament of Urology, CES clinic, Medellín Colombia
INTRODUCTION: laparoscopic retroperitoneal lymphadenectomy are taking an important role in patients requiring salvage surgery for residual retroperitoneal mass after failed chemotherapy. This video shows the performance of salvage retroperitoneal lymphadenectomy in a patient with testicular seminoma and residual retroperitoneal mass after neoadjuvant chemotherapyMATERIALS AND METHODS: transperitoneal technique was used to perform laparoscopic salvage retroperitoneal lymphadenectomy, a 33 years old patient with a residual retroperitoneal mass of 6×6×9 cm after adjuvant chemotherapy; the final pathology of the mass was reported as embryonal carcinoma.RESULTS: the laparoscopic technique was useful to resect the retroperitoneal mass. in this case the laparoscopic technique was performed without complications, the entire mass, right paracaval, precaval and, interaortocaval lymphs was removed without complications, hospital stay of only two days and early postoperative recovery. CONCLUSIONS: laparoscopic retroperitoneal lymphadenectomy for patients with testicular cancer is an important treatment modality not only for patients with early stages of the disease but also for patients with residual masses after chemotherapy.Currently there is consensus to perform retroperitoneal lymphadenectomy in patients with seminoma and post-chemotherapy residual mass greater than 3 cm. The standard treatment has been the open technique; however the laparoscopic technique has evolved progressively to reach almost the same as those indications, which makes it an attractive option in this type of surgery to avoid the increased morbidity of the open technique.BIBLIOGRAPHY:1. jaetschek g, peschel r, hobisch a, bartsch g. laparoscopic retroperitoneal lymph node dissection. j endourol. 2001; 15:449-53.2. albqami n, janetschek g. laparoscopic retroperitoneal lymph-node dissection in the management of clinical stage i and ii testicular cancer. j endourol. 2005; 19:683-92.3. poulakis v, skriapas k, de vries r, dillenburg w, ferakis n, witzsch u, becht e. quality of life after laparoscopic and open retroperitoneal lymph node dissection in clinical stage i nonseminomatous germ cell tumor: a comparison study. urology. 2006; 68:154-60.4. donohue jp, thornhill ja, foster rs, rowland rg, bihrle r. primary retroperitoneal lymph node dissection in clinical stage a non-seminomatous germ cell testis cancer: review of the indiana university experience 1965-1989. br j urol. 1993; 71:326-35.5. yoon gh, stein jp, skinner dg. retroperitoneal lymph node dissection in the treatment of low-stage nonseminomatous germ cell tumors of the testicle: an update. urol oncol. 2005; 23:168-77.6. carver bs, sheinfeld j. the current status of laparoscopic retroperitoneal lymph node dissection for non-seminomatous germ-cell tumors. nat clin pract urol. 2005; 2:330-5.7. albqami n, janetschek g. laparoscopic retroperitoneal lymph-node dissection in the management of clinical stage i and ii testicular cancer. j endourol. 2005; 19:683-92.8. nelson jb, chen rn, bishoff jt, oh wk, kantoff pw, donehower rc, kavoussi lr. laparoscopic retroperitoneal lymph node dissection for clinical stage i nonseminomatous germ cell tumors. urology. 1999; 54:1064-7
Laparoscopic Diagnostic Retroperitoneal Lymph Node Biopsy
Introduction: In testicular malignancy, radiologic study is the standard method employed for clinical staging. The clinician often encounters equivocal imaging results that may not definitively dictate clinical stage. Purpose: We present a case which illustrates the utility of laparoscopic retroperitoneal lymph node biopsy in disease staging. Materials and Methods: The patient is a 23 year old male found to have a right testicular mass. A right radical orchiectomy revealed pure seminoma with lymphovascular invasion (pT2). CT scan showed two sub-centimeter inter-aortocaval lymph nodes, 7mm and 8mm. PET scan showed no increased uptake. Given the lymph nodes were sub-centimeter, the patient cannot be clearly classified as stage I or stage IIa. This difference was significant as clinical upstaging implied different recommended treatment. Thus, a laparoscopic retroperitoneal lymph node biopsy was performed for staging. Results: The pathology of the biopsy revealed pure seminoma nodal metastasis, measuring 1.5×1.0×0.8 cm and 1.6×1.0×0.7 cm in size. Subsequently, the patient was correctly counseled to undergo external beam radiation therapy for stage IIa disease instead of possible observation for Stage I seminoma. Conclusions: Laparoscopic retroperitoneal lymph node biopsies can be safely performed in a minimally invasive fashion to limit the morbidity, increase the staging accuracy, and ensure that the appropriate treatment plan is recommended.
Teikyo university chiba medical center, Chiba, Japan
Recently, the importance of lymph adenectomy for urotherial carcinoma of upper urinary tract has been discussed in order to attain the cancer control. Since 2008, laparoscopic lymph nodes dissection in renal pelvis and upper ureter cancer has been initiated at Chiba university hospital and at Teikyo university chiba medical center. We will discuss the result and detail about the procedure of operations. The range of lymph nodes dissection is between upper edge of the renal artery and the bifurcation point of the common iliac artery. If the cases are on the right side, dissection will be made at both para-caval and aorto-caval lymph nodes. If the cases are on the left side, dissection will be made at para-arotic lymph nodes. We have performed the 16 cases between May 2008 through March 2011. Among them, 13 cases are on the left side and 3 cases are on the right side. There were 13 renal pelvic cancer and 3 upper ureter cancer cases. The average length of the operation is around 1hr. The number of lymph nodes dissected are between 4 to 26; average 12.9. Positive lymph nodes are found in 2 cases. The outcome of this procedure will be more precisely determined after longer term of surveillances, however, we believe patients may be benefit in terms of cancer control by removing the lymph node. This procedure requires profound understanding in anatomy as well as skills in laparoscopic operation to precisely dissect the lymph nodes.
Department of Renal and Genitourinary surgery, Graduate School of Medicine, Hokkaido University, Sapporo, Japan
Introduction: Retroperitoneal paraganglioma is relatively uncommon tumor whose operative resection still remains technically challenging issue. Purpose: Feasibility of laparoscopic resection and its surgical outcomes were investigated in retroperitoneal paraganglioma. Materials and Methods: From January 2000 to December 2010, 10 patients underwent 11 laparoscopic resections. Tumors located in 2 of adrenal, 4 of renal hilum, and 5 of infra-hilar, inter-aorta-caval region. There were 5 females and 5 males with a median age of 59 years old (range, 17-78 years). Median tumor size was 3.3 cm (range, 1.5-7 cm) in maximum diameter. Median follow-up was 30 months (range 3-127 months). Results: 10 operations underwent by transperitoneal approach and 1 by retroperitoneal approach. 4 to 5 ports were placed and port position was changed according to tumor location. 2 patients needed taping of IVC. Median operative time and blood loss were 228 minutes (range, 79-513 minutes) and 50 ml (range, 79-1020 ml). Antihypertensive agents in 8 and vasopressor in 6 pts were needed at intraoperative changes of blood pressure. There was no conversion to open surgery. There were 2 perioperative morbidities (18.2%) and no mortality. No patient required a blood transfusion. Oral intake was started without delay. One patient encountered recurrent tumor twice in the other places. These tumors were excised again and all patients live free from tumor so far. Conclusion: Laparoscopic resection of paraganglioma can be accomplished safely although modification of port position and taping of IVC are mandatory according to the tumor location.
Laparoscopic Resection of a Large Functional Paraganglioma in the Organ of Zuckerkandl (PZ)
Laparoscopic Extracapsular Transplantectomy, Technical Considerarions.
INTRODUCTION: Primary kidney transplant neoplasms are uncommon, they usually appear lately after renal transplantation. Open extracapsular transplantectomy is the treatment of choice when partial nephrectomy is not feasible. The option of laparoscopic approach minimizes postopterative complications and patient pain.OBJECTIVES: To present technical details of laparoscopic approach for laparoscopic extracapsular transplantectomy in two cases of renal cell carcinoma involving the renal graft.METHODS: Patients are placed in supine, trendelenburg and left tilt position. A transperitoneal laparoscopy allows the control of the iliac vessels before graft disection. An extracapsular graft nephrectomy is performed and renal graft vessels are clamped separately. RESULTS: Mean operative time was 200 minutes and blood loss 300 ml. Graft was removed through a 5-cm length infraumbilical incision. Postoperative course was uneventful in both patients. Patients referred pain as minimum. Radical treatment was achieved with negative margins in both cases.CONCLUSIONS: Laparoscopic transplantectomy is safe, allows quick recovery and minimizes postoperative complications compared with classical open surgery
Department of Urology, Saitama Medical University, Saitama, Japan
<INTRODUCTION>Renal vein laceration is a major trouble during nephrectomy, especially with hard adhesion around renal pedicle. We demonstrate two cases of renal vein laceration in hard tissue surrounding renal pedicle.<SUBJECTS>The first case undertook removal of infected kidney with nephrostomy tube. The second case was diagnosed as renal cell carcinoma in hydronephrosis due to periaortitis which involved renal pedicle.<RESULT>In the first case, laceration occurred during blunt dissection. Bleeding point was clearly identified and immediately held by sealing device. Renal pedicle was incised only using sealing device. Bleeding point was not clearly seen at the time of injury in the second case. At first, bleeding point was compressed by device with the pressure of pneumoperitoneum, but vessel wall was molded in hard tissue. After completion of hemostasis, renal pedicle was roughly exposed, and then clips were used for ensuring hemostasis prior to incision.<DISCUSSION>Vessel laceration is one of the common reason for open conversion. However, even the bleeding with severe adhesion involving renal pedicle can be managed tactically. There are several steps to keep in mind when we encounter sudden bleeding. Control of bleeding must be the priority using compression by device and CO2 pressure. Once control could be achieved, then surgeon must notify the situation and give the appropriate order to staffs. The surgeon may step forward to complete hemostasis with complete understanding of situation.
Department of Urology,Ghaem Hospital,Mashhad University of Medical Sciences, Mashhad, Iran
IntroductionMany of the ureteral strictures are managed by endourologic techniques, including balloon dilatation and endoureterotomy.Some patients requires surgical excision and repair.Surgical considerations critical to successful repair include preservation of the vascular supply, adequate ureteral mobilization, and construction of a watertight and tension-free anastomosis.Although many ablative, laparoscopic techniques are established procedures, reconstructive laparoscopic procedures are still evolving.This is mainly due to the complexity and technical skill intensity inherent to such procedures.PurposeIn this report, we present our experience with laparoscopic ureteral reconstruction by primary end-to-end anastomosis for treatment of ureteral stricture.Materials & MethodsA 46 year-old man with right flank pain, hydroureteronephrosis and proximal ureteral stricture on IVP and history of laparoscopic ureterolithotomy, candidate for surgery.Laparoscopic ureteroureterostomy was performed transperitoneally with 4 ports.The right colon was mobilized and a large amount of fibrosis was found to be encasing the ureter.Laparoscopic ureteral exploration was done meticulously.After excision of the stricture, the ends of the ureter were spatulated and then reanastomosed using a 4-0 vicryl sutures that placed full thickness.A stent was placed.An abdominal drain and Foley catheter were left indwelling .Patient was discharged postoperative day 3 and the stent was removed 6 weeks postoperatively.ResultsOperative time was 180 min.No conversion to open surgery was necessary and there were no complications. Bleeding was minimal.The IVP showed excellent patency of the repair.ConclusionsLaparoscopic ureteroureterostomy is a potential treatment option for ureteral strictures in carefully selected patients.Laparoscopic ureteroureterostomy is technically feasible and efficacious in treating ureteral stricture.
VS06: Robotic/Laparoscopic Upper Urinary Tract Surgery 1
Laparoscopic Upper Pole Heminephrectomy for Duplicated Renal Collecting Systems
Introduction:Ureteral duplication is a relatively common congenital anomaly of the genitourinary tract. When symptomatic due to urinary tract infection, flank pain or urinary incontinence the standard surgical treatment is upper pole heminephrectomy. Until relatively recently surgery involved a flank incision with significant morbidity and prolonged recovery time. We report our experience with laparoscopic upper pole partial nephrectomy with a duplicated collecting system and an obstructed, poorly functioning upper pole renal moiety with ectopic ureter. Laparoscopic heminephrectomy is a well tolerated, minimally invasive, although technically demanding, procedure for children with a non-functioning moiety in a duplex kidney.Material & Methods:A 5 years girl with urinary incontinence underwent the transperitoneal approach.After reflecting the colon medially, both ipsilateral duplicated ureters are identified.The upper pole ureter is transected at the level of the iliac vessels, with the distal end left open.The upper pole ureter is then dissected cephalad toward the renal hilum and upper pole atrophic moiety. The vascular supply to the upper pole renal moiety is meticulously dissected and controlled using vascular clips. The renal upper pole moiety is then excised along the atrophic cleavage plane using electrocautery . Results: Operative time was150 min. No conversion to open surgery was necessary and there were no complications.Conclusion: The laparoscopic approach is feasible, safe, reduces hospital stay, does notincrease operating time and has better cosmetic results. We believe this should be the first option for heminephrectomy.
Knotless Laparoscopic Pyeloplasty using Barbed Suture
Intracorporeal suturing and knotting have remained the complex skill sets during pyeloplasty. Knotless urethrovesical anastomosis using barbed sutures during prostatectomy has lately become popular as a simpler and effective alternative. We have performed knotless pyeloplasty using such sutures.Two V-loc 3-0 suture length are joined together as in van Velthoven technique. Anastomosis is started posterior to the ureteric apex. The first suture is brought back into ureter and posterior wall of the ureteropelvic anastomosis completed. Suture is brought out of the pelvic flap at upper end, and left outside. The apical suture is now taken with the second suture length, which is continued to complete the anterior wall of ureteropelvic anastomosis. Ureteric strip is now transacted proximal to the anastomosis and the redundant pelvis excised in continuity. This segment is still left attached at the upper end of the pelvis to retract, bringing the pelvic walls together for later closure. Cut upper end of the ureter is now triangulated into pelvis using either or both sutures, completing the ureteropelvic anastomosis. One of the sutures is abandoned at this stage, while other is continued to complete the pelvic closure. Water-tightness of anastomosis can be checked before tightening the final pelvic bite. Sutures are run in surrounding facial layers to lockSixteen knotless PAD pyeloplaties have been done during last one year. This knotless procedure achieved a 11 minute reduction in procedure time without compromising the outcome.Knotless pyeloplasty is, thus, feasible, and saves precious OR time without compromising results.
Laparoscopic Culp Pyeloplasty: In a Case of Partial Intrarenal Pelvis with Ureteropelvic Junction Obstruction.
Introduction: A surgical technique for UPJ obstruction includes Open Pyeloplasty, Laparoscopic Pyeloplasty or Endopyelotomy. The indication for Laparoscopic Culp Pyeloplasty is partial Intrarenal Pelvis with UPJ obstruction were dismembered Pyeloplasty gives tension on anastomasis.Methods: Operative video: A case of UPJ obstruction having partial intrarenal pelvis in which Laparoscopic Culp Pyeloplasty was permored. 1.5cm spiral flap of renal pelvis was made with incision extended on UPJ to normal ureter up to 1.5cm. 5-0 Vicryl was used to take continuous stiches for flap placement over UPJ and ureter. JJ stent was kept; and pelvis was closed.Results: Out of 84 patients of UPJ obstruction 8 cases were treated with Culp Pyeloplasty and 76 were treated with laparoscopic dismembered Pyeloplasty. Post-operative recovery was uneventful. In 1 patient drain was kept for 6 days for leak. Follow-up at 3month after removal of JJ stent, USG was done showing decrese hydronephasis and at 12 month IVP shows smooth Passage and unobstructed flow.Conclusions: Laparoscopic Culp Pyeloplasty is feasible and safe in selected cases of partial intra renal pelvis with UPJ obstruction and gives better results over laparoscopic dismembered Pyeloplasty. This approach requires careful Patient selection as well as expertise in laparoscopic surgery.
Laparoscopic Robotic-Assisted Transmesocolic Left Pyeloplasty in a Horseshoe Kidney
Introduction: Horseshoe kidneys have an incidence of 1 in 400-1000 births, making it the most common renal anomaly. UPJOs are found in 15-33% of horseshoe kidneys and present particular challenges with difficult exposure, nondependent ureteral-pelvic junctions, longer stricture length, and anomalous vasculature. The standard approach to a left-sided laparoscopic pyeloplasty requires mobilization of the colon although a transmesocolic approach is gaining popularity. Purpose: To our knowledge, a case of laparoscopic robotic-assisted transmesocolic left pyeloplasty in a horseshoe kidney has not been reported in the literature. We present this video to share our experience.Materials and Methods: The patient was a 36 year-old male with multiple stones within a horseshoe kidney and a left UPJO. Five laparoscopic ports were placed and the da Vinci SI robotic system docked. We attempted to mobilize the colon, however the dissection was difficult and a transmesocolic approach was undertaken. After making a pyelotomy, a cystoscope was advanced through one of the laparoscopic ports and all stones basketed out. The anastomosis was completed and a 6F 24cm double-J ureteral stent was placed as well as a foley catheter and JP drain. Results: Total procedural time was 126 minutes, estimated blood loss was 10cc, and there were no intraoperative or postoperative complications. Length of hospital stay was three days. Four weeks the stent was removed and antegrade nephrostogram demonstrated good drainage; the patient was pain free.Conclusions: This video demonstrates that a transmesocolic approach to a left pyeloplasty in a horseshoe kidney is a technically feasible.
Department of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction:Pelvic lipomatosis is a benign proliferative disorder of the pelvic adipose tissue affecting middle aged individuals. The proliferative mass and the associated inflammation may cause compression or infiltration of the luminal structures such as ureter, bowel or the blood vessels. We report a case of pelvic lipomatosis with bilateral ureteric obstruction managed by bilateral laparoscopy assisted ileal ureter. Materials and method: A 45 years old male patient presented with lower urinary tract symptoms. He was evaluated and found to have pelvic lipomatosis with bilateral lower ureteric obstruction and small capacity, poorly compliant bladder, with minimal impairment in renal function.Under general anesthesia, using 5 ports both ureters and bladder was dissected. Using a 5cm sub umbilical incision, 30 cm ileal segment was harvested and a U shaped ileal ureter was constructed with both the ends anastamosed to the pelvis and the dependent part of the loop anastamosed with the dome of the bladder.Results: The The duration of the surgery was 360 minutes and the blood loss was about 350 ml. Patient discharged on 10th post operative day. Renal function stabilized at S.Creatinine of 1.2 mg/dl. Postoperative urodynamic study revealed improved compliance of bladder. Patient is on self intermittent catheterization twice a day for the obstruction and incomplete emptying. He however voids varied quantities (100-200 ml) in between self intermittent catheterization. 3 months after surgery patient remains asymptomatic.Conclusion: Laparoscopy assisted bilateral ileal ureter is a feasible and effective procedure in the management of pelvic lipomatosis with bilateral ureteric obstruction.
Department of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction: Upper ureteric stricture is one of the rare complications of ureteric injury during ureteroscopy. Ileal urete is one of the options for managing long ureteric stricture. We present the case report of a patient with long upper ureteric stricture managed by laparoscopy assisted ileal ureter. Materials and Method: 41yrs old male patient a recurrent stone former, who underwent PCNL 5 years ago and URS twicefor upper ureteric calculus 3 years ago, presented with loin pain for 3 months. He was evaluated and found to have upper ureteric stricture. Using 4 ports, laparoscopy was done and left ureter was dissected. Dense adhesions were present around the ureter. Using a 5 cm sub umbilical incision, 20 cm of ileum was isolated and bowel continuity restored. The ends of the ileal loop were anastamosed with the pelvis and bladder. Results: The operative time was 320 minutes. Blood loss was around 200ml. Post operative stay was for 5 days. Patient improved symptomatically and a CT urogram after 3 months showed a patent ileal ureter with reduced hydronephrosis. Conclusion: Laparoscopy assisted ileal ureter is a feasible and less morbid procedure for upper ureteric stricture compared to open ileal ureter.
Section of Laparoscopic and Robotic Surgery, Department of Urology, Frimley Park Hospitals NHS Foudation Trust, Surrey, UK
VS07: BPH,TUR,Female Urology
Holmium Laser Enucleation of the Prostate (Holep): Our Modified Technique
Introduction and Objectives: HoLEP is an effective surgical treatment for BPH, with low morbidity, good efficacy and short hospital stay. Recently we modified the enucleation method by starting from the anterior direction to more easily expose the adenoma capsule, and enucleate the lateral lobe more quickly. From June 2003 to July 2011, 700 consecutive patients with BPH underwent HoLEP.Today we will share our techniques to perhaps help others shorten the learning curve, and we will examine the utility of our current method.Methods: Enucleation was started from the median lobe, as is conventionally performed (Group A).Group B was treated using our modified method.Technical Considerations: There are four steps in our modified HoLEP technique : 1) First, enucleation begins with a transverse incision at the anterior lobe.2) Then the median lobe is enucleated.3) Then the lateral lobes are enucleated both downwards and upwards along the adenoma capsule.4) This is followed by transurethral morcellation.In most of our cases, postoperative irrigation was not needed and catheterization time was less than 24 hours.Results: In terms of procedure time and catheterization time, the modified method (group B) was significantly shorter than the conventional method (group A).Both groups presented pronounced and lasting postoperative improvements in Symptom Scores, Qmax, and PVR (p<0.001). No patients needed blood transfusions or experienced hyponatremia.Conclusions: Our modified method both simplifies the HoLEP procedure and shortens procedure time.This reduction in time was realized by the modification of the enucleation method.
HoLEP Retrograde One-Piece Enucleation Method
Introduction: Holmium laser enucleation of the prostate is a safe and effective treatment for prostatic hyperplasia. Despite the benefits of HoLEP the procedure has been slow to gain widespread acceptance. It seems that the complication of the current procedure and a higher prevalence of urinary incontinence are the drag of popularization. We perform retrograde one-piece enucleation method to simplify the procedure and reduce the prevalence of the urinary incontinence. Materials and methods: From July 2006 to June 2011 we performed 1,008 HoLEP by retrograde one-piece enucleation methods. Initially the apex of the prostate is dissected circumferentially, and then the adenoma is enucleated as a lump using the holmium laser, and pushed into the bladder. The enucleated prostatic tissue is evacuated from the bladder with a VersaCut morcellator. Results: Mean operative time was 62.9 minutes. Mean weight of resected tissue was 37.4 grams. One of them needed blood transfusion duo to massive blood loss during procedure. No critical complication was seen. No severe stress incontinence was observed. Conclusion: HoLEP by retrograde one-piece enucleation method is more intelligent treatment for prostatic hyperplasia.
In-Office Evolve(Tm) Laser Ablation of the Prostate for Symptomatic Benign Prostatic Hyperplasia (BPH)
Introduction and Objective: In this video we demonstrate patient preparation, technique and initial results using the Evolve(TM) laser system under local anesthesia as an in-office treatment for symptomatic BPH. Methods: Patient preparation including nerve block (transrectal and transurethral) and positioning, features of the Evolve(TM) laser system, and vaporization technique under local anesthesia are highlighted. Adverse events and both qualitative and quantitative measures of efficacy for BPH surgical intervention were recorded in a prospective fashion.Results:Under local prostatic nerve block, in-office laser ablation of the prostate is possible with few adverse events. Unique features of the Evolve(TM) laser system include an angled fiber (Twister SF (TM) fiber) that allows for enhanced fiber tip visualization during ablation. Initial evaluation in 40 patients demonstrated significant improvements in AUASS and Qmax values. The mean level of pain was 2 of 10 (max pain) during the procedure. 3 minor adverse events were noted intraoperatively that did not necessitate the abortion of the procedure. 30 (91%) of the 33 patients reported the procedure as a success, 2 reported it as mixed, and 1 patient reported it as a failure. Conclusions: Under local anesthesia in the urology office or clinic setting, Evolve(TM) laser ablation is feasible, safe and efficacious.
Department of Urology, China Medical University Beigang Hospital, Beigang, Taiwan
Introduction: We introduce a new vaporization incision technique (VIT) for BPH which is modified from standard photoselective vaporization of prostate (PVP). This technique is especially useful in big prostate larger.
Purpose: Because the standard PVP can hardly create an enough tunnel for big prostate and the lack of specimen which is required in some insurance issue, we introduce a way to perform VIT which can easily take the specimen off and directly approach to the surgical capsule.
Materials and Methods: Since Jan 2008 to April 2011, patients who received PVP or VIT in CMUHBG were retrospectively reviewed. The VIT of median lobe was done from 5 & 7 o'clock aspects while the lateral lobes started from 1& 5 and 8&11 o'clock aspects. The age, prostate size, IPSS, surgical time, pre-op and post-op maximum flow rate and residual urine amount were analyzed.
Results: The age is similar in both VIT and PVP groups. The post-op maximum flow rate and residual urine improved a lot in both group. The size of VIT group is larger than the PVP group (64.03 vs 41.12gm, p<0.05 ). The surgical time and laser time were longer in VIT group because of big prostate (p<0.05 ). However, the op time per gram of prostate is less in VIT group than PVP group (p<0.05 ) which implied the VIT is faster than PVP.
Conclusions: Both VIT and PVP are useful for BPH. However, the VIT may be more useful in big prostate according to our study.
Division of urology, Geneva University Hospital
Urethral diverticulum are rare events. Principally acquired (>70%), they can be congenital too. We report a case of a posterior bulbo-membranous urethral diverticulum with a probable congenital origin of 3×1 cm which was treated endoscopicaly in an eighteen year old man. An eighteen year old man came to our consultation for post-mictionnel dribbling which started several months ago without elements in favor of a post traumatic origin. Urine flowmeter showed a Qmax of 23ml/s for a 380 ml voided. Retrograde urethrography was performed and show a bulbo-membranous urethral diverticulum of 3 cm length. The cystoscopy identifies a diverticulum neck of 3-4 mm located between the proximal and mild bulbar urethra. Pelvic MRI showed a thin wall between the urethra and diverticulum and a thick corpus spongiosum. Therefore an endoscopic approach was preferred.After introduction of the cystoscope and identification of the neck, incision with a cold blade of the wall separating urethra from diverticulum was performed. Exploration showed a blind mucosa in its proximal end adjacent to the sphincter. Diverticulum ends distally is a zone where urethra is tighter. This zone was incised in a multiradial fashion with the urethrotome. Electrocoagultaion of diverticulum rim was performed. At the end of procedure, a 20 Fr transurethral catheter was left indwelling. No complications occurred post-operatively. Urinary catheter was removed at 10 post-operative. Post operative urine flowmeter was comparable to preoperative do and patient does no longer report post-mictionnel dribbling.Endoscopic treatment may be an option in some of urethral diverticulum.
Departamento de Urología clínica CES
MATERIALS AND METHODS This video illustrates the management of vaginal vault prolapse in a patient previously undergone hysterectomy, using laparoscopic sacrocolpopexy for the anchoring of a polypropylene mesh from the vaginal vault to the sacrum.DESCRIPTION OF SURGICAL TECHNIQUE: We performed a transperitoneal approach in supine, started with rejection of the bowel, Place a vaginal speculum valve to facilitate dissection. Dissect the peritoneum covering the vaginal vault, which is mobilized to identify the site where the pubocervical fascia fix the prolene mesh. The sacral promontory is identified and the peritoneum around is seperated. Using blunt dissection the anterior longitudinal ligament is exposed.Mesh segment, folded in half is extended from the vaginal apex to the sacral promontory.The proximal end of the mesh is fixed to the anterior longitudinal ligament of the sacral promontory using a polyester suture and the posterior part to the rectovaginal fascia using the same suture. The anterior margin of the mesh is fixed to the pubocervical fascia The mesh should create a tension-free suspension. Remaining pat of the mesh is cut.The peritoneum is closed to completely cover the mesh with absorbable suture.RESULTS: In managing a patient of 74 years with repeated urinary tract infections and vaginal sensation of mass associated with a grade III vaginal vault prolapse using laparoscopic sacrocolpopexy with polypropylene mesh fixed to the anterior longitudinal ligament of the sacrum with polyester non-absorbable suture is adequate we observed goog postoperative outcomes.INTRODUCTION Since the early 90's management of vaginal vault prolapse by laparoscopic sacrocolpopexy has been more frequent. Success rates are similar to open sacrocolpopexy and vaginal techniques (RR 0.34 CI: 0.1-0.8), but recovery, aesthetic result, and less hospital stay is favorable for laparoscopic surgery (1). The advantages of the technique is better visualization of the structures, better hemostasis provided, technical advantage or short vaginas recurrent prolapse after vaginal sacrocolpopexy. (2 technical advantage in short vaginas or recurrent prolapse after vaginal sacrocolpopexy. (2)The disadvantages mentioned higher learning curve for laparoscopic surgery.One of the difficulties mentioned is the approach to the presacral region which involves longer operating time. This video illustrates how access to the anterior longitudinal ligament of the sacrum can be more easily by lifting and fixing the colon to the abdominal wall facilitating the surgical approach.BIBLIOGRAPHY1. reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2010, Issue 8,2. FEMALE UROLOGY Copyright © 2008, 1996, 1983 by Saunders, an imprint of Elsevier Inc.
Departament of Urology, CES clinic, Medellín Colombia
OBJECTIVE: To show the laparoscopic management of complex urinary tract endometriosis, performing a laparoscopic hysterectomy, resection of bladder endometrioma and ureterovesical reimplantation.MATERIALS AND METHODS: We present the video of a 42 years old patient with 3 years of chronic pelvic pain, severe dysmenorrhea, dyspareunia and recurrent cystitis.Managed by gynecology with diagnosis of endometriosis. Obstructive involvement of right distal ureter, managed in other center with double J stent which was changed every 3 months. CT abdomen reported right distal ureteral stenosis of 3.5 cm and hydroureteronephrosis, DTPA renal scintigraphy showed global filtration of 84 ml/min, right kidney 20.5 ml/min with a T1/2 greater than 20 minutes and a normal left kidney.urethrocystoscopy found large endometrioma on the bladder floor 3 x 4 cm.Was programmed together with gynecology to anexo- hysterectomy, partial cystectomy and laparoscopic ureteral reimplantationSURGICAL TECHNIQUE Whit transperitoneal laparoscopic approach, the bladder is dissected and opened with harmonic scalpel; the double J catheters previously left are seen. The bladder endometriosis is identifiedComplete endometrioma resection was performed and right ureter is separated,Distal ureterectomy (endometriosis involvement) is made preserving healthy ureter.The ureter spatulatulation is performed to make the reimplatationthe anexo hysterectomy is finished and the uterus and endometrioma is removed through vaginal way. Vaginal vault suture is made with continuous Absorbable barbed suturecystorrhaphy is performed with the same type of sutureThe ureter was reimplanted with interrupted 2-0 vicryl suture.RESULTS: The patient has an adequate postoperative evolution, with short hospital stay and rapid recuperation. CONCLUSION: The urinary tract endometriosis can be treated through different ways, in this video we shows that severe obstructive endometriosis has a good operative outcome with the laparoscopic management.BIBLIOGRAPHY:1. ustilo-Ashby AM, Paraiso MF. Treatment of urinary tract endometriosis. J Minim Invasive Gynecol. 2006 Nov-Dec;13(6):559-65. Review.2. Perez-Utrilla Pérez M, Aguilera Bazán A, Alonso Dorrego JM, et al, J. Urinary tract endometriosis: clinical, diagnostic, and therapeutic aspects. Urology. 2009 Jan;73(1):47-51. Epub 2008 Oct 31.3. Bosev D, Nicoll LM, Bhagan L, Lemyre M, Et al, C.Laparoscopic management of ureteral endometriosis: the Stanford University hospital experience with 96 consecutive cases. J Urol. 2009 Dec;182(6):2748-52.Epub 2009 Oct 17.4. Scioscia M, Molon A, Grosso G, Minelli L. Laparoscopic management of ureteral endometriosis. Curr Opin Obstet Gynecol. 2009 Aug;21(4):325-8. Review
Laparoscopic Management of Vesicovaginal Fistula in Three Patients with Different History.
Purpose: To evaluate the safety and efficacy of laparoscopic repair in management of vesicovaginal fistula (VVF) in different clinical conditions.Material and method: Three patients underwent VVF repair in different postoperative fistula formation period (after one, four and six months postoperatively). Two patients had developed fistula following hysterectomy for uterine fibroma. The third patient underwent hysterectomy due to cervical carcinoma and received 25 sessions adjuvant radiotherapy. Laparoscopic repair was performed by opening the bladder from dome to the fistula. The vaginal edge of fistula was closed using 2-0 polyglycolic sutures. Bladder was closed using 2-0 polyglycolic sutures. Omentum was interposed between bladder and closed fistula in two cases. In the third case with previous history of radiation therapy with large fistula, no proper omentum was available to interpose between bladder and vaginal repair. Cystostomy tube was not placed in any of three cases. Results: There were no perioperative and postoperative complications. Patients were discharged at 3, 4 and 7 days postoperatively. Foley catheter was removed three weeks after operation. Incontinence was cured in all three patients following catheter removal. Conclusion: VVF can be managed successfully by laparoscopic approach in different postoperative period even in difficult cases with history of radiation therapy. Avoiding omental interposition in cases without proper omentum will not always have deleterious effect on final outcome.
VS08: Robotic/Laparoscopic Upper Urinary Tract Surgery 2
Robotic Radical Nephrectomy with Resection of Inferior Vena Cava Thrombus
Introduction: Treatment and management of Renal cell carcinoma with vascular invasion can be challenging. Extension of Renal Cell carcinoma to the level of the Inferior Vena Cava occurs between 4%-10% on initial presentation. We present our technique of resection of Renal Cell Carcinoma with Inferior vena caval thrombus resection.Materials and methods: After the renal artery was ligated, laparoscopic ultrasound was used to delineate the extent of the thrombus. It was noted that in the 2 weeks from imaging to surgery, the tumor had grown an additional 2 cm cephalad within the IVC, but still was infrahepatic. A vessel loop is passed circumferentially around the caudal extent of the thrombus in order to prepare the Rommel tourniquet. A Satinsky clamp is placed above the thrombus. Using the Potts scissors, the IVC is incised and the thrombus is shelled out. A 4-0 Prolene was used in running fashion to repair the IVC. Results: EBL was 200cc, final pathology was papillary renal cell carcinoma with sarcomatoid change, Fuhrman nuclear grade 3, Stage T3AN0M0. The patient was discharged on post day #2.Conclusion: Robotic radical nephrectomy with resection of IVC thrombus presents a challenging approach to vascular invasion of the IVC, however, repair and reconstruction of the IVC with thrombus extraction can be accomplished.
Robotic Radical Nephrectomy with Vena Caval Tumour Thrombectomy: Novice Robotic Surgeon Experience
Background:The introduction of robotic-assisted surgery has facilitated the application of minimally invasive surgical techniques to more complex procedures. With distinct advantages in precision and dexterity over standard laparoscopy, robotics has allowed even novice robotic surgeons to explore such applications.Purpose:We describe the management of a large renal mass with inferior vena caval (IVC) thrombus using a purely robotic approach.Methods:A 61-year-old male presenting with severe anemia, fatigue, and 100-lb weight-loss over a 4-month period was found to have a 12-cm right renal mass with IVC thrombus. The patient had a BMI of 43.5-kg/m2 and previous laparoscopic cholecystectomy. Staging revealed a 3.5-cm right adrenal mass but no other evidence of metastases. A robotic-assisted radical nephrectomy with caval thrombectomy, requiring complete cross-clamping of the IVC, was performed without major intra-operative complications.Results:Total operative time was 527-minutes with 15-minutes of cross-clamp time. Estimated blood loss (EBL) was 750-mL and a total of 4 units of pRBCs were transfused (2 pre-operatively, 2 post-operatively). Patient was discharged home on post-operative day #4. Final pathology revealed pT3b clear-cell renal cell carcinoma with rhabdoid differentiation, extra-capsular extension, and negative margins. Conclusions:In comparison to the only published series by an expert robotic surgeon (mean OR time 327-minutes, mean EBL 170-mL, no transfusions, no complications) we demonstrate the feasibility of novice robotic surgeons performing a purely robotic radical nephrectomy with caval thrombectomy, requiring IVC cross-clamping. Further validation is required.
Laparoscopic Nephrectomy in Acute Wünderlich Syndrome
ABSTRACT WITHDRAWN
Laparoscopic Left Nephrectomy in a Patient with Portal Hypertension and Spontaneous Splenorenal Shunt
Introduction: In patients with liver disease and renal masses surgical options are limited secondary to complications related to portal hypertension. Spontaneous splenorenal shunts present a particular concern because they are relatively uncommon (16%), however these patients remain suitable candidates for minimally invasive techniques. Specifically, retroperitoneal laparoscopic surgery can avoid the potential hazards associated with transperitoneal surgery in patients with portal hypertension allowing for similar visualization and tamponade of varices. Purpose: We present a video of a retroperitoneal laparoscopic left nephrectomy in a patient with a spontaneous splenorenal shunt to highlight technical difficulties that may be encountered.Materials and Methods: The patient was a 48 year-old male with a history of portal hypertension secondary to perisinusoidal fibrosis as a result of schistosomiasis and a large left splenorenal shunt who was found to have a 6-cm left renal mass. Three laparoscopic ports were placed in the standard fashion after the retroperitoneal space was developed using a retroperitoneal dissecting balloon. Careful dissection was carried out until the lumbar vein, renal artery, and renal vein were identified and stapled in turn, being careful to preserve the splenorenal shunt.Results: Total procedural time was 168 minutes, estimated blood loss was 10cc, and there were no intraoperative or postoperative complications. Length of hospital stay was four days.Conclusions: The literature has already demonstrated that retroperitoneal laparoscopic surgery is a safe option for patients with liver disease. The present case serves to further illustrate that knowledge of the retroperitoneal vascular anatomy can also facilitate the outcome.
Retroperitoneal Robot-Assisted Nephrolithotomy
IntroductionRobot-assisted lithotomy (RAL) has previously been shown to be effective with large stones, although its effectiveness has not been demonstrated in large staghorn calculi [1]. RAL can have advantages in cases where renal anatomic abnormalities make other stone extraction techniques difficult or risky. This approach can also be of benefit in instances where the patient is already undergoing a robotic surgical procedure, such as a partial nephrectomy. PurposeThis video demonstrates the efficacy and safety of retroperitoneal robot-assisted laparoscopic nephrolithotomy. Materials and MethodsVideo footage was filmed intraoperatively from a robot-assisted nephrolithotomy on a patient with a 4 cm lower pole partial staghorn renal calculus. We include our experience with three additional patients who underwent robot-assisted pyelolithotomy, two of whom had simultaneous robot-assisted partial nephrectomy. Results and ConclusionsThe results of this series show that robot-assisted lithotomy can be a viable treatment option in cases where laparoscopic intervention is advantageous to percutaneous stone extraction.References1) Badalto GM, Hemal AK, Menon M, Badani KK. Current role of robot-assisted pyelolithotomy for the management of large renal calculi: a contemporary analysis. J Endourol. 2009 Oct;23(10):1719-22.
Urology Department, Acibadem Maslak Hospital, Istanbul, Turkey
Introduction: Seven degree movement of the robotic arms is the major advantage of robotic surgery. Thus, it is very easy to perform intracorporeal suturing and knot tying in robotic surgery when compared to standard laparoscopy. However, running sutures may lose its tension and might become even untied during the robotic operations.Purpose: To describe a loop fixation knot for running sutures in robotic surgery.Material and Methods: This novel technique is demonstrated on chicken leg and in 2 patients (1 pyeloplasty, 1 bladder diverticulectomy). Once the needle is passed on each side, a loop is taken under the suture and passed to the other side. Then the needle is passed inside the loop. The knot is pushed towards to the skin with the right needle holder, while the suture is pulled back with the left hand. At the end, the running suture is fixed and strengthened.Conclusion: This novel loop knot technique provides precise and durable fixation of running sutures during robotic surgery.
VS09: Robotic/Laparoscopic Prostate Surgery 2
Correcting Surgical Planes During Robot-Assisted Radical Prostatectomy
Introduction. Optimal training of surgeons in robot-assisted radical prostatectomy (RARP) requires high case volumes, and may be enhanced by the video review of complications, difficult anatomy, and steps that required correction. Even in expert hands, the initial surgical plane selected may not be correct and have to be adjusted. We retrospectively searched our video catalog for representative examples of cases where a surgical plane had to be corrected.
Methods. From 12/2008-6/2011, a single surgeon catalogued the highlights of recorded cases. Comments were descriptive in nature and designed to highlight current techniques being attempted, difficult anatomy encountered, training comments, and difficulties with surgical access. During this time period, 559 cases were performed, and 92% had 1 or more highlights recorded.
Results. The most common highlighted features were neurovascular bundle dissection (34% positive, 2% critiqued), bladder neck (12% positive, 12% critiqued), and lymph node dissection (19% positive, 3% critiqued). For the video demonstration, we selected 5 critiqued cases where a surgical plane had to be corrected in one of these locations.
Conclusion. Prospective cataloguing of surgical videos can assist with locating examples of surgical steps where corrections were required, and may be a key component of an educational curriculum.
Urology Department, Acibadem Maslak Hospital, Istanbul, Turkey
Introduction: Suturing and stapling are commonly used techniques to control dorsal vein complex (DVC) during robot assisted radical prostatectomy (RARP) while some authors prefer not to control it.Purpose: To describe a novel technique to control DVC during RARP.Material and Methods: Once posterior and lateral dissection is completed, DVC is grabbed with a laparoscopic bulldog clamp prior to apical and urethral dissection. After division of the DVC and the urethra, the bulldog clamp is removed and DVC is controlled with 2/0 polyglactin suture material. This suture was used for periurethral suspension subsequently. In this video, the technique is described in 2 patients.Results: This technique was used in the last 35 patients in our series. Of these patients 19 undergone concomitant bilateral pelvic lymph node dissection (PLND). Mean age was 63 and EBL was 171 ml. Mean console time was 161 min and 119 min, in patients with or without PLND, respectively. There was no need to increase the intraabdominal pressure during the division of DVC in any patient. No transfusion was needed. No patient had positive surgical margin at the apex. Two patients had positive surgical margin at the posterolateral region (1 pT2, 1 pT3 disease).Conclusion: The use of laparoscopic bulldog clamp to control DVC enables a clear vision and precise dissection of the apex and the urethra during RARP. This may result with decrease in console time, blood loss and surgical margin positivity at the apex. The technique is easy to perform and feasible.
Departament of Urology, CES clinic, Medellín Colombia
INTRODUCTION: The vesicourethral anastomosis is a critical step in laparoscopic radical prostatectomy; this video shows the realization of this important part of the surgery using a Absorbable barbed suture that allows a uniform distribution of tension around the anastomosis to facilitate performing the procedure by not requiring continuous traction by the surgeon or assistantMATERIALS AND METHODS: An important step in the vesicourethral anastomosis is the reconstruction of rabdoesfinter with Rocco point which helps to reduce tension on the suture line and decreases the leakage around the anastomosis, in this case Rocco point was made with Vicryl 3 / 0 conventional manner and the vesicourethral anastomosis was performed using continuous Absorbable barbed suture that has a self Retaining System that facilitates the steps during the surgical procedure.RESULTS: Absorbable barbed suture is useful in vesicourethral reconstruction during laparoscopic radical prostatectomy; this allows a continuous and hermetic closure by reducing the technical complexity of the procedure. For over 6 months has been using this type of suture showing a marked decrease in the complexity of the procedure and decreased operative time with no cases of leakage around the anastomosis CONCLUSION: The use of Absorbable barbed suture with self Retaining System is a useful alternative for the vesicourethral anastomosis in laparoscopic radical prostatectomy as it helps simplify the steps for surgical reconstruction and keeps a uniform hermetic tension, simplifying the steps for surgical reconstruction.BIBLIOGRAPHY 1. Kaul S, Sammon J, Bhandari A, et al. A novel method of urethrovesical ansatmosis during robot-assisted radical prostatectomy using a unidirectional barbed wound closure device: Feasibilty study and early outcomes in 51 patients. J Endourol. 2010;24:1789& 8211;932. Tewari AK, Srivastava A, Sooriakumaran P, et al. Use of a novel absorbable barbed plastic surgical suture enables a self-cinching technique of vesicourethral anastomosis during robot-assisted prostatectomy and improves anastomotic times. J Endourol. 2010;24:1645& 8211;503. Williams SB, Alemozaffar M, Lei Y, et al. Randomized controlled trial of barbed polyglyconate versus polyglactin suture for robot-assisted laparoscopic prostatectomy anastomosis: technique and outcomes. Eur Urol. 2010 Aug 24. Moran ME, Marsh C, Perrotti M. Bidirectional-barbed sutured knotless running anastomosis v classic Van Velthoven suturing in a model system. J Endourol 2007;21:1175& 8211;1178.
Modified Periurethral Suspension Stitch during Laparoscopic Radical Prostatectomy
Introduction and purpose: The periurethral retropubic suspension stitch during robot-assisted laparoscopic radical prostatectomy was reported to contribute to facilitating the apical dissection and early recovery of continence (Patel et al. Eur Urol 2009). We modified this technique during laparoscopic radical prostatectomy (LRP), termed as modified periurethral suspension stitch (mPSS), and investigated its impact on the positive surgical margin rates at the apex (apical PSM rates) and early recovery of continence. Materials: Thirty-one consecutive patients underwent LRP between May 2010 and May 2011. Dorsal vein complex (DVC) ligation with and without mPSS was conducted to 16 and 15 patients, respectively. Surgical procedure: Before apical dissection and transection of urethra during LRP, a 40-cm 2-0 Vicryl™ (Ethicon Pty Ltd, Australia) on a CT-1 needle is doubly stitched around the distal DVC. The both ends of the suture are guided to the suprapubis using an Endo Close™ trocar site closure device (Tyco Healthcare, Australia) and tied with an adequate tension to acquire the anterior traction of DVC. Results: Apical PSM rates in the mPSS group and the control group were 0% and 20%, respectively. In our study, mPSS was not useful for early recovery of continence. Conclusions: We believe that mPSS contributes to low apical PSM rates by facilitating meticulous apical dissection.
Preservation of Pubovesical Fascia During Robotic Radical Prostatectomy
Introduction: One potential complication of radical prostatectomy is urinary incontinence. The acceptance of robotic surgery for prostate cancer has been accompanied by an evolution of robotic techniques. Recently, the importance of anatomic structures supporting the urethra and bladder neck in maintaining continence has been appreciated.
Purpose: To demonstrate a novel technique designed to improve continence by preserving the anterior support and the pubovesical fascia during robotic prostatectomy.
Materials and Methods: The pubovesical fascia sparing approach involves a more medial incision on the endopelvic fascia when compared to the traditional method. This spares the puboprostatic ligaments, pubovesical fascia, and the arcus tendineus support structures. An automatic stapling device used for dorsal vein transection also serves to secure the urethra anteriorly against the pubic symphysis.
Results: This video demonstrates a novel technique designed to preserve the support of the urethra and bladder neck. A stapling device is used to anchor the urethra to the puboprostatic ligaments which are in turn left with a broad attachment to the arcus tendineus levator ani and the pubovesical fascia. This maintains the natural support of the urethra and bladder neck. The patient demonstrated in this video had total continence with no leakage at 3 weeks follow-up.
Conclusions: Preservation of urethral and bladder neck support may contribute to post-prostatectomy continence. Though prospective, randomized trials will be required to validate this technique, it has the potential to improve patient quality of life following prostatectomy.
Steps and Challenges of Extraperitoneal Robotic Assisted Radical Prostatectomy
ABSTRACT WITHDRAWN
Robotic Excision of a Large Seminal Vesicle Cyst: Zinners Syndrome
Introduction: Zinners Syndrome is a rare disorder with a frequency of 214 per 100,000 patients. Associated seminal vesicle cysts are usually less than 5cm in size but may be greater than 12cm, causing bladder, ejaculator duct or rectal obstruction. Surgical excision may be indicated in certain patients including minimally invasive approaches.Purpose: This video demonstrates the robotic approach for excision of a large seminal vesicle cyst at our institution.Materials and Methods: The patient shown in this video is a 35 year-old man with a congenital solitary kidney and duplication of the right collecting system. Computed tomography showed a large seminal vesicle cyst after the patient presented with recurrent epididymo-orchitis symptoms, decreased ejaculatory volume and severe voiding symptoms. The cyst measured 6cm×7cm×9cm in size. The operation was completed with a 12mm camera, 3 robotic ports and two assistant ports. Port configuration and lithotomy position were identical to our set up for robotic prostatectomy.Results: The operation was completed with minimal blood loss and without complication. Total operative time was 120 minutes. The patient was discharged home less than 24 hours after surgery. Pathology confirmed a benign seminal vesicle cyst, 7.5cm in diameter. At six weeks follow-up, the patient had improvement in pain and voiding symptoms. Conclusions: As shown in this video, robotic excision of a large seminal vesicle cyst can be a safe and effective treatment option.
Department of Urology, Autonomous University of Barcelona, Hospital del Mar, Barcelona, Spain
VS10: Ureteroscopy/Endourology
Endopyelotomy in the Era of Laparoscopy and Robotic Pyeloplasty
Purpose: Endopyelotomy was the first minimally invasive technique used to manage congenital and acquired ureteropelvic junction obstruction. The subsequent introduction of laparoscopy allowed urologists to replicate the dismembered pyeloplasty, while sparing patients the morbidity of an open incision. As an ever-increasing number of urologists become facile with laparoscopy, the continued role of endopyelotomy in the management of ureteropelvic junction obstruction has been called into question by some clinicians. Materials and Methods: We demonstrate our antegrade and retrograde endopyelotomy techniques, highlighting their relative ease of adoption. The endopyelotomy and laparoscopic pyeloplasty literature is then reviewed with an emphasis on treatment efficacy for primary and secondary obstructions.Results: The largest antegrade endopyelotomy series included 401 patients. The subjective and objective success rate was 82% for primary ureteropelvic junction obstruction, which is less than Inagaki and colleagues' 95% success rate in 147 patients undergoing transperitoneal laparoscopic pyeloplasty. Gupta et al noted an 83.5% success rate in 41 patients with secondary obstruction treated with percutaneous endopyelotomy. This is in contrast to Sundaram and coworkers series of 36 patients undergoing secondary laparoscopic pyeloplasty. Their success rate was 83%. Conclusions: While less efficacious then laparoscopic pyeloplasty, endopyelotomy for primary ureteropelvic junction obstruction remains an attractive option given its shallower learning curve and cost effectiveness. Endopyelotomy should be considered a first-line option for secondary ureteropelvic junction obstruction given its equivalent success rates to the more technically complex salvage laparoscopic pyeloplasty.
Use of a Novel Anti-Retropulsion Device for Ureteroscopic Treatment of Ureteral Stones
Introduction Proximal migration of the stone during ureteroscopy can add time and cost to the procedure. The Backstop® is a novel anti-retropulsion device that can be used to prevent proximal migration of stones. Purpose:We report on our experience and demonstrate our technique utilizing the Backstop® during treatment of ureteral calculi.Materials and Methods:The stone is visualized within the ureter with a semi-rigid ureteroscope. The Backstop® is a liquid at room temperature and is deployed through a 3 Fr.catheter placed through the ureteroscope. It is injected proximal to the stone under vision and forms a solid plug at body temperature. Laser lithotripsy is performed. At the conclusion of laser lithotripsy, the Backstop® is converted back to a liquid with cold saline irrigation.Results:The Backstop® has been used in 15 cases. There has been no proximal migration of the stone or any fragments. There has been no need to convert to flexible ureteroscopy. There have been no intra-operative or post-operative complications. The stone-free rate as determined by post-operative intravenous pyelogram is 100% at a median follow up of 5 months.Conclusions:The Backstop® appears to be safe and effective at preventing proximal migration of ureteral stones and fragments during semi-rigid ureteroscopy. The advantages of the Backstop® include the ability to deploy under vision and the ability to dissolve the plug with cold saline irrigation. Routine use of the Backstop® avoids proximal stone migration, without the need for flexible ureteroscopy and therefore may lead to decreased operative times and costs.
Radiation Reduction Protocol for Ureteroscopic Lithotripsy
Introduction: Harmful effects resulting from patient exposure to radiation are well-known, including the risk of secondary malignancy. In February of 2010, the Food and Drug Administration (FDA) unveiled an initiative to reduce unnecessary radiation exposure from medical imaging. In response to the FDA released White Paper, we have developed and implemented a protocol designed to reduce radiation exposure during ureteroscopic lithotripsy.
Purpose: To demonstrate key aspects of this reduced fluoroscopy protocol.
Materials and Methods: Radiation reduction was achieved primarily through modification of C-arm utilization and surgeon technique. Using a laser-guide, minimizing radiation dose, and employing an experienced technician optimized the C-arm for fluoroscopy. The surgeon substituted tactile and visual cues in lieu of additional fluoroscopy time. Patients before protocol implementation were compared to those after.
Results: This video demonstrates several modifications of standard fluoroscopy during ureteroscopy designed to reduce radiation exposure. This video also demonstrates the implementation of these techniques in a patient undergoing stone removal via ureteroscopy. Utilizing this protocol, we achieved an 82% reduction in radiation in 30 patients with no difference in operative time, stone-free rate, or complication rate compared to 30 patients treated with a conventional technique.
Conclusions: Our protocol reduces radiation exposure by 82% in patients undergoing ureteroscopic lithotripsy when compared to the conventional method. Adoption of the techniques demonstrated in this video will allow urologic surgeons to significantly reduce radiation exposure to their patients and staff.
The Cleveland Clinic, Cleveland, OH
Objective:The XenX stone retention device (Xenolith Medical, Israel) has been developed to serve the dual purpose of preventing retrograde stone migration and serving as a guidewire over which a stent can be placed. Our objective was to evaluate its safety and efficacy in an ex vivo porcine model.
Methods:A 6 mm CaOx stone was inserted in the mid ureter of a porcine model (600lb hog). The XenX was advanced alongside a semi-rigid ureteroscope (Wolf 6/7.5F) past the stone until the tip was located in a major calyx of the kidney. The device was deployed past the stone, and a 200 μm Ho laser fiber was inserted into the working channel of the scope to begin lithotripsy. A stone basket (Sacred Heart Medical Halo, 1.5F) was used to remove large retained fragments. The ureter and kidney were separated, and migrated and retained stone fragments were collected by flushing irrigation toward the proximal end of the ureter. Fragments were later analyzed for size distribution. The ability to place stents was evaluated with the Inlay Optima (7F, Bard Urological), Percuflex (6F, Boston Scientific), and Silhouette (4.6F, Applied Medical).
Results: Retained stone fragments and those that migrated past the XenX during lithotripsy ranged from 1.0-3.0 mm, and 0.5-1.1 mm in their largest diameter, respectively. The XenX was easily maneuvered within the ex vivo model, and demonstrated the ability to place stents.
Conclusion: The XenX serves as an effective stone retention device with the potential to increase the efficiency of ureteroscopic stone extraction.
Polyscope TM , The First Disposable Flexible Ureteroscope:A Breakthrough in Flexible Endoscopy.
INTRODUCTION: Ureteroscopic treatment of renal stones is nowadays gaining quite large popularity among endourologists.Nevertheless, the major obstacle to dissemination of flexible ureteroscopy into everyday urological practice worldwide is endoscopes fragility and related maintenance costs rather than optical resolution. In this video we show a case of left renal stone of 1.7 cm in diameter treated ureteroscopically with Polyscope, the first disposable flexible ureteroscopeMM: This scope is only 8 french in diameter and delivers high quality images through a 10.000 pixels fiber optic. The catheter articulates up to 250 degrees only in one direction. It contains a 3.6 french working and irrigation channel. The Polyscope system adapts to all current video towers. RESULTS: Our initial series gathers 10 patients with a mean stone diameter of 1.2 cm (0.7-1.7) treated ureteroscopically with Polyscope . With a mean OR time of 62 min (41-84) we were able to achieve a stone free status in 80% of cases with an hospital stay ranging between 1 and 3 days (average 1.9). All these findings parallels what we usually obtain with the same procedure carried out with conventional reusable flexible ureteroscope.CONCLUSION: The Polyscope represents a breaktrough in flexible ureteroscopy providing a reliable, cost effective and disposable endoscope capable of delivering high quality images and eliminating the need for sterilization of instruments in between surgeries, the risk of tissue transfer and contamination from one patient to the next and the unexcusable procedures interruption due to unexpected scopes rupture.
Re-Trace: A New Concept of Ureteral Access Sheath
INTRODUCTION AND OBJECTIVES: Ureteral access sheaths (UAS) were developed to facilitate flexible ureteroscope movement. Several UASs were introduced into endourology field. We present in this work a new concept of a recently introduced UAS (Re-Trace) coloplast; that allows transforming working guide-wire into a safety guide-wire. Our aim is to evaluate and to demonstrate technical aspects of this instrument. METHODS AND MATERIALS: The new UAS, Re-Trace (12/14Fr) Coloplast, is designed to allow disengagement of working guide-wire in one step. This guide-wire lies in the ureter besides UAS and becomes automatically a safety guide-wire. In addition, this UAS works as double lumen catheter since contrast can be injected while guide-wire still in the renal cavities. Patient gender, pre-operative ureteral stenting and UAS placement outcome were prospectively evaluated. Indications for ureteroscopy were mainly stone treatment.RESULTS: 101 UASs were used in 101 ureters (61 in male patients and 40 in female patients.) 28 ureters (27.7%) were pre- stented: male/female ratio appeared to be higher in pre-stented (3.8) than in non pre-stented population (1.2). Overall Re-Trace insertion rate was 83%. Easier insertion was found in female (90%) versus male (77%) as well as (93%) in pre-stented ureters versus (78%) in non pre-stented ureters. This was confirmed when combining gender and pre-stenting parameters: 100% UAS insertion success in pre-stented women, 91% in pre-stented men, 88% in non-pre-stented women and 69% in non-pre-stented men. The guide-wire disengagement was obtained in 100% of cases. CONCLUSIONS: Re-Trace showed good overall insertion rates. Variations related to gender and pre-stenting corresponded to general expectations. This video is to show the prosperities and insertion technique of this instrument in order to present a new concept of guide-wire disengagement: a single guide-wire immediately turned from working to safety one.Pr Olivier Traxer is a consultant for coloplastDr Saeed Al-Qahtani has nothing to decalre.
Non-Specific Inflammatory Renal Changes Mimicking Upper Tract Urothelial Carcinoma
Introduction: upper urinary tact urothelial cancer is uncommon tumor presenting mainly with hematuria and renal filling defects in urographic studies and some inflammatory condition can present with same picture. Case and technic: 45-year-old male known diabetic and hypertensive, Presented with history of gross painless hematuria, with multiple filling defects on pyelography, Urine cytology showed atypical cell suspicious of urothelial carcinoma Ureteroscopy (video 1) showed multiple lesions mimicking carcinoma in situ involving the whole pelvicalyceal system, biopsy taken by BIGopsy forceps was negative for malignancy, The patient was offered laparoscopic Nephroureterectomy versus reevaluation and he chose the reevaluation witch was done 8 weeks later, the patient was asymptomatic, the repeated RGP showed resolution of the previously noted filling defects with negative selective cytology with improvement in renal function (from 16% to 26%), repeated ureteroscopy (video 2) shoed significant improvement and healing with most of the urothelium of the pelvicalyceal system being normal. Conclusion: some Non-specific inflammation involving the upper urinary tract epithelium could present clinically and radiologically like urothelial carcinoma.
Laser Management of Urothelial Carcinoma
Introduction: Lasers have assumed an integral role in the management of various urinary tract diseases, including urothelial carcinoma (UC). The holmium (Ho) and neodymium (Nd):YAG lasers are effective devices for the treatment of neoplasms throughout the urinary tract. Combining these two lasers gives maximal coagulative and ablative effects. Purpose: To demonstrate the application of the Ho and Nd:YAG lasers for the management of UC in the bladder, ureter, and intra-renal collecting system.Materials and Methods: Ho:YAG is a pulsed laser (λ2100 nm) which both coagulates and ablates tissue. In contrast, Nd:YAG is a continuous wave laser (λ1064 nm) which destroys tissues with coagulation. While Ho:YAG penetrates only 0.5 mm, Nd:YAG can penetrate 10 times deeper into tissue. Using a combined unit with dual foot switch, both lasers can be delivered through the same small quartz fiber and their unique properties may be exploited. These techniques can be demonstrated best in actual clinical applications. Results: The combined holmium and Nd:YAG laser can utilize the optimal effects of each laser to treat neoplasms throughout the urinary tract.Conclusions: Laser ablation and resection is an acceptable treatment option for bladder and upper tract urothelial carcinoma. Holmium and neodymium:YAG lasers are complimentary and effective devices for the endoscopic management of urinary tract tumors. Holmium:YAG laser may be used alone, preferentially with variable-pulse duration.
Cook Resonancetm Metallic Ureteric Stent Insertion Technique & Clinical Experience
Introduction and Objectives The Cook resonance metallic ureteric stent has been introduced as an alternative method for upper urinary tract obstruction. In this short video, we aim to demonstrate the insertion technique from a recent case, and then assess feasibility, safety and efficacy of the operative technique.Patients and Methods The technique of stent insertion is demonstrated in this video. Clinical experience at our institution was critically assessed, in terms of patient demographics, clinical indication, length of operative procedure, radiation exposure, as well as immediate and late complications.Results The enclosed video demonstrates the insertion technique. In the past 2 years, 6 patients have been treated, with 11 Cook Resonance metallic ureteric stent insertions (Median age 61 years;range 58-90). Indications for stent insertion was extrinsic malignant compression (n=7), retroperitoneal fibrosis (n=2) and benign stricture (n=2). Procedures were successful in all but one case, which required antegrade approach, due to migrated stent. Median duration of surgery was 45 mins (15-60). Median radiation exposure was 987CGycm2. Urosepsis occurred in 1 patient, and late complication occurred in only one case, being managed with nephrostomy insertion.Conclusions In this short video we have demonstrated Cook resonance metallic stent insertion technique for a case of upper urinary tract obstruction. In addition, we have demonstrated that this technique is feasible, safe and efficacious.
Use of the Accordion™ during Ureteroscopic and Percutaneous Lithotripsy to Prevent Stone Migration
Introduction: Endoscopic lithotripsy is often prolonged secondary to stone fragment migration. Several occlusion devices have been introduced to circumvent this problem, one of which is the Accordion™.Purpose: To demonstrate the utility of the Accordion™ in preventing retrograde and antegrade migration of calculi fragments during ureteroscopic lithotripsy (URS) and percutaneous nephrolithotomy (PCNL), respectively.Materials and Methods: The Accordion™ is inserted over a guidewire and readily followed under fluoroscopic visualization with its radiopaque markers or alternatively under direct endoscopic visualization. During PCNL, the Accordion™ is positioned at the ureteropelvic junction in either an antegrade fashion adjacent to the access sheath or in a retrograde fashion. After positioning, the device is deployed to form a multi-fold film occlusion. This telescoping design conforms to and fills the ureteral lumen, while simultaneously maintaining irrigant flow. Additionally, the Accordion™ may be used to "sweep" larger fragments following lithotripsy and to inject contrast for an ureteropyelogram. Results: The Accordion™ is a safe, easy-to-use occlusion device which decreases procedural time and improves efficiency of stone clearance during both URS and PCNL.Conclusions: The Accordion™ is a versatile device which effectively obstructs the ureter and prevents stone migration during endoscopic lithotripsy. This valuable tool is useful for both ureteroscopic and percutaneous procedures. Future prospective studies are warranted to compare the currently commercially available retropulsion devices.
VS11: Laparoscopic/Robotic Bladder Surgery
instituto Medico la Floresta, Caracas Venezuela
INTRODUCTION AND OBJECTIVES: Open Radical Cystectomy is the standard treatment for high grade and muscle invasive bladder cancer, with the potential early complications even in the most experienced. Over the last decade, we have witnessed the emergence and progression of minimally invasive surgery in urology including radical cystectomy. Any new technique applied to the treatment of invasive bladder cancer must be safe, maintain similar oncological principles as ORC, and provide similar options for lower urinary tract reconstruction. While many complications of radical cystectomy are shared between approaches, recognition and management in the robotic and laparoscopic surgery environment poses unique challenges. The goal of this video is to present graphic illustrations of complications during robotic or laparoscopic radical cystectomy.METHODS: A multi-institutional collection of surgical videos was compiled. These videos illustrate vascular injury, rectal injury, benign ureteral strictures and the presence of vesicovaginal fistula after surgery. RESULTS: We show possible complications and how often they are encountered, comparing the different approaches, open, laparoscopic and robotic. In addition, short and middle term complications in patient after Minimally invasive Radical Cystectomy are characterized.CONCLUSIONS: RARC and LRC must reproduce the robust oncological outcomes seen with ORC while attempting to minimize perioperative morbidity.RARC and LRC incurs acceptably low postoperative morbidity, with the vast majority of complications being low grade. High-grade complications are infrequent and similar to those encountered after ORC. Complications are similar in all approaches Early recognition and appropriate management is essential when these complications occur.
Open-Assisted Laparoscopic Radical Cystectomy with Ileal Neobladder with Intracorporeal Urethra-Neobladder Anastomosis
Introduction: The laparoscopic radical cystoprostatectomy for muscle invasive bladder cancer is now widely performed in many series. We present our experience in laparoscopic radical cystectomy with ileal neobladder that urethra- neobladder anastomosis was successfully performed intracorporeally.Materials and methods: We performed laparoscopic radical cystectomy with ileal neobladder with intracorporeal urethra-neobladder anastomosis in 5 patients. Four had muscle invasive bladder cancer and one had too large tumor. Laparoscopic radical cystectomy was performed as standard technique. The small low midline skin incision was created for specimen removal. Bilateral extended pelvic lymphadenectomy was performed. Studer neobladder was constructed extracorporeally. Ileal pouch was dropped back into abdomen. Urethra-neobladder anastomosis was performed by laparoscopic suturing technique, running with vicryl 2-0 until complete procedure.Results: Urethra-neobladder anastomosis was successfully done intracorporeally. The mean operative time was 6 hours and 30 minutes. Mean estimated blood loss was 560 ml. No intraoperative complications occured. Mean hospital stay was 19.6 days. Mean foley catheter indwelled time was 18 days. Time to return of bowel function was 4.8 days. Mean time to remove silastic drain was 14.2 days. After removal of foley catheter, all patients had spontaneous voiding without difficulty. Conclusion: Open assisted laparoscopic radical cystectomy with ileal neobladder with intracoporeal urethra-neobladder anastomosis could be done successfully. The advantage of this technique was more secured anastomosis from good visualization by laparoscopic view with minimal increase intraoperative time.
Laparoscopic Radical Cystectomy in a Patient with Bilateral Complete Ureteral Duplication
Objective. To present the technical aspects of laparoscopic radical cystectomy in a patient with bilateral complete ureteral duplication.Material and method From a group of 3 patients that underwent laparoscopic radical cystectomy in the last 6 month at the Ion Chiricuta Oncological Institute we selected a case of a 58 year old male, that presented with bilateral ureteral duplication. The laparoscopic aproach was transperitoneal with 5 trocars. Bilateral pelvic extended lymphadenectomy was performed. For urinary diversion bilateral cutaneous ureterostomy was performed.Results. The mean operative time was 270 minutes. The time for performing extedned lymphadenectomy was 75 minutes. The number of lymph nodes removed was 26. The ICU stay was 3 days, and the overall hospital stay was 5 days. The pathological stage was pT1G3No. Associated the patient was diagnosed with a prostate cancer Gleason 4 (2+2). All surgical margins were negative. At 8 month of follow-up the patient is without evidence of disease.Conclusions. Laparoscopic radical cystectomy in patients with bilateral ureteral duplication is a feasible and safe method. Bilateral ureteral duplication does not increase the technical difficulty of the laparoscopic surgery.
Department of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction: Ileal Conduit is one of the options in neurogenic bladder with compromised renal function. Once the renal function improves undiversion can be done. Laparoscopic undiversion is a technically challenging procedure. We present the video of a patient with an ileal conduit undiverted by laparoscopy. Materials and methods: A 10 year old boy, with neurogenic bladder with sacral agenesis, underwent laparoscopic ileal conduit diversion as he had deranged renal function. After 15 months his renal function improved and cystogram revealed a small capacity bladder(50 ml). Urodynamic study confirmed a small bladder capacity and low compliance (3ml/cm H2O). Laparoscopy was done with the patient in the supine position using 4 ports. Adhesiolysis was done. Bladder was mobilized and the dome of the bladder was dissected. Stoma of the conduit was released from the abdominal wall with a circumferential incision and stoma site was closed. The ileal loop was detubularised and sutured to the transverse cystotomy. Supra pubic catheter, urethral catheter and drain were placed and the port sites were closed. Results: The operative time was 250 minutes and blood loss was 180ml. The child required analgesics for 3 days. Drain was removed on the fifth day and he was discharged. Supra pubic catheter and urethral catheter were removed after cystogram. The patient was taught to do clean intermittent catheterization. At 2 years follow up, child has normal renal parameters with no intercurrent infection. Conclusion: Laparoscopic undiversion with augmentation is a feasible, effective and less morbid procedure in a child and possibly a better alternative to open undiversion.
Extraperitoneal Endoscopic Bladder Diverticulectomy for Multiple Large Infected Diverticuli
Introduction: Bladder diverticulum complicated by recurrent urinary tract infections and/or lower urinary tract dysfunction is not an uncommon entity. With significant advancement in the laparoscopic surgery and its proven advantages, minimally invasive surgery can be offered as an alternate option to open surgery. Purpose:To describe technical steps required for laparoscopic excision of multiple infected bladder diverticuli.Material & Methods: Video shows main steps of extraperitoneal endoscopic urinary bladder diverticulectomy. A 5-ports approach was used and complete excision of bladder diverticuli was achieved with the guidance of flexible cystoscopy. The video describes technical tips to avoid ureter in posterior-lateral location of the lesions and dissection in difficult perideverticular fibrosis complicated by previous infections. The diverticuli were successfully excised and removed. Urinary bladder defect was closed in three layers and checked for water tightness. Retzius space was drained and ports closed after checking haemostasis. Results: Operation lasted 230 minutes. Blood loss was 50 cc. Follow-up at 3 months- symptoms resolved.Conclusions: Extraperitoneal endoscopic diverticulectomy is an effective treatment for complicated bladder diverticuli and should be offered in centres with large experience in laparoscopic surgery.
Department of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction: Posterior urethral valve can cause various sequelae including low compliance bladder. Low compliance bladder may be associated with secondary diverticulum. Open diverticulocystoplasty for low compliance bladders has been reported. We present the video of laparoscopic diverticulocystoplasty in a child. Materials and methods: A 4 year old boy, presented with storage symptoms for 1 year. He had undergone posterior urethral valve ablation 15 months back. Imaging revealed thick walled (5mm) bladder and right posterolateral bladder diverticulum, left grade III reflux and right obstructive megaureter and normal posterior urethra. Urodynamic study showed poor compliance bladder (3 ml/cm H2O). Using 4 ports right ureter was mobilized upto the bladder. Diverticulum was dissected and the ureter was found entering the diverticular neck. Ureter was divided, exteriorized, and tailoring was done. Right ureteric reimplantation was done by Leadbetter-Politano technique. Cystoplasty was done by suturing the diverticulum to the bladder. Lich Gregoir antireflux procedure was done on the left side. Results: The operative time was 320 minutes, blood loss was 80ml and hospital stay was 4 days.At 12 months follow up, the child was asymptomatic. Compliance improved to 9ml/cmH2O on repeat urodynamic evaluation. Glomerular filtration rate improved on the right side (28.8 ml/min). Conclusion: Laparoscopic diverticulocystoplasty is a feasible option for paediatric patients with low compliance bladder with diverticulum.
Department of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction: Vesico ureteric reflux may present at any age. Urinary tract infection at any age needs investigation. Bilateral reflux with urinary tract infection in adults may need intervention. We present the video of laparoscopic bilateral detrusorraphy done in a patient with bilateral reflux and recurrent urinary tract infection. Materials and methods: A 28 year old lady presented with recurrent urinary tract infection. She was evaluated and found to have bilateral grade 3 vesico ureteric reflux. Under general anesthesia, using 5 ports, ureters were dissected bilaterally upto the bladder. Detrusorraphy was done bilaterally by wrapping the detrusor over the ureter near the uretero vesical junction. Port sites were closed after ensuring hemostasis. Results: the operative time was 200 minutes and the blood loss was around 100ml. Patient had a 3 days post operative stay in the hospital. Post operative voiding cysto urethrogram showed no reflux. Conclusion: Laparoscopic bilateral detrusorraphy is a feasible and effective treatment option for patients with bilateral vesico ureteric reflux.
First Experience with the Vesicoscopic Ureteral Reimplantation by Politano-Leadbetter technique
Purpose: We present a initial report with the vesicoscopic ureteral reimplantation by Politano-Leadbetter (P-L) technique under pneumovesicum. Methods: We attempted vesicoscopic ureteral reimplantation with the P-L technique for total 14 ureters, 8 girls with more than grade III vesicoureteral reflux (VUR) and 1 girl with vesico-ureteral stricture. To provide intravesical vision by 5 mm endoscope 5-mm Step port was placed on bladder dome under the cystoscopic guidance. Two 3 mm Step ports were placed on the lateral bladder wall subsequently. The bladder was drained and insufflated with CO2 to 8 mm Hg pressure. To assist intravesical surgical manipulation a 3-mm port was placed from the urethral meatus. All the endoscopic transvesical manipulations that was mobilization of ureter, was creation of 2.5 cm length new submucosal tunnel along with Politano-Leadbetter technique were performed under videoscopic guidance. Ureteral catheter was used for bilateral cases by next morrning. Urethral catheter was removed on day 2 postoperatively. After confirmed voiding, the patients were discharged same day afternoon. Results: There was no serioous complication after surgery. No patients required any narcotic analgesics postoperatively. After removal of the urethral catheter bladder spasm was minimal. At 8 weeks postoperatively, the patients had a repeat VCUG that showed no reflux in 12 uretes of 13 ureters. Of these patients VUR was persisted in a girl. In the first case, vesicoscopic ureteral reimplantation was converted to open surgery after finish the surgery of other ureter, because peumovesicum was unable to maintain.Conclusion: This technique is very useful for female patients with high grade VUR.
Cystoscopic Assisted Laparoscopic Excision of an Urachal Remnant
Introduction: Urachal defects are rare with urachal cysts being the most common anomaly. The treatment of choice for the urachal pathology is complete excision. Minimal invasive surgery is a potential alternate to open surgery. Purpose:To describe technical steps required for the complete laparoscopic excision of an urachal remnant.Material & Methods: Video shows main steps of cystoscopic assisted laparoscopic excision of an urachal cyst. A 5-ports transperitoneal approach was used and complete excision of the urachal cyst was achieved with the guidance of flexible cystoscopy. The video describes technical steps in identify exact location of the urachal remnant. With careful dissection and localization, the urachal cyst was completely excised and removed. Urinary bladder defect was closed and checked for water tightness. Retzius space was drained and ports closed after checking haemostasis. Results: Procedure was completed successfully via laparoscopy. No intra-operative or post operative complications were reported. Operative time was 120 minute and blood loss was 50 mls. Pathological evaluation revealed a benign urachal remnant.Conclusions: Cystoscopic assisted laparoscopic surgery assures accurate localization of the urachal remnant and the surgical results are comparable to conventional open surgery.
Instituto Medico la Floresta, Caracas Venezuela
INTRODUCTION AND OBJECTIVES: Vesicovaginal fistulas are among the most distressing complications of gynecologic and obstetric procedures. Complex fistulas as those with one or more of the following: greater than 2.5 cm, closely related or involving the ureters, multiple tracts, multiple organs involved, or post-radiotherapy. We present our experience with robotic repair of complex fistulas.METHODS: Two patients were diagnosed with complex post hysterectomy fistulas. The patient in Case 1 presented with both a vesicovaginal and a colovesical fistula. Case 2 had a 4 cm long vesicovaginal fistula with associated left ureteral obstruction. This patient had received pelvic irradiation. Technique: cystoscopy and stenting of the ureters and the fistulous tract, transperitoneal placement of ports for robotic repair, lysis of adhesions, colon dissection in case 1 and left ureteral dissection in case 2 cystotomy and vesicovaginal fistula identification, separation of the vaginal and bladder walls, closure of the vagina, omental flap interposition, bladder closure, transient loop ileostomy in case 1 and ureteral reimplantation in case 2.RESULTS: Fistula repair was initially successful in both cases, with a mean operative time of 150 minutes (180 and 120) and estimated blood loss of 250 mL. The length of hospital stay was of 3 days in both cases. The foley catheter was removed at day 30 and 15 respectively. The post-radiation fistula, recurred at 3 months.CONCLUSIONS: The daVinci Robot System allows successful identification of the correct tissue planes for appropriate dissection and help in suturing during the repair of fistula.
VS12: Notes/Less 2
Laparoendoscopic Single-Site Adrenalectomy Performed using Conventional Laparoscopic Instruments: The First 14 Cases
IntroductionMany bent and articulating instruments have been developed for laparoendoscopic single-site surgery (LESS); however definite evidence concerning their safety, feasibility, and necessity is not available. PurposeThis study aimed to examine the feasibility of performing LESS adrenalectomies using only conventional laparoscopic instruments.Materials and MethodsBetween June 2010 and April 2011, 2 surgeons treated 14 consecutive patients (mean age, 58.9 years; mean body mass index 23.1 kg/m2) by performing LESS adrenalectomy transperitoneally. A homemade single-port device was placed according to the method reported by Park (J Endourol 2009). All the operations were performed using conventional straight instruments and procedures similar to those used in conventional laparoscopic adrenalectomy. We evaluated the patients' characteristics and operative parameters. In this video, we have shown right LESS adrenalectomy performed for a 60 year-old male patient with primary aldosteronism caused by a 1.5-cm adrenal adenoma.ResultsWe made a 3.5-cm incision in the subcostal area for the first 11 patients and in the periumbilical area for the last 3 patients. The mean operation time was 191.2 minutes, and mean blood loss was 56.8 ml. All the operations were successfully completed without additional trocars, conversion to standard laparoscopic surgery, or major complications. ConclusionsReasonable outcomes can be obtained for LESS adrenalectomy performed using conventional laparoscopic instruments.
Transvaginal Notes Nephrectomy in a Series of 42 Cases: Stepwise Transition from Hybird to Pure Notes
Introduction The feasibility of hybrid transvaginal natural orifice transluminal endoscopic surgery (NOTES) nephrectomy (HTNN) has already been demonstrated. However, pure transvaginal NOTES nephrectomy (PTNN) has been limited to animal experiments with only one report of its use in humans.Purpose To describe our initial experience with the HTNN and stepwise transition toward PTNN. Materials and Methods Between May 2010 and January 2011, 40 HTNNs and 2 PTNNs were performed in our center. In our initial 33 procedures, HTNNs were performed using two umbilical trocars and one transvaginal trocar. In the subsequent 4 procedures, HTNNs were performed using one umbilical trocar and a transnaginal Triport. In the latter 3 procedures, all the laparoscopic instruments were introduced through the transvaginal Triport. However, the 3 procedures were aborted due to the limitation of the length of intruments. Transient umbilical assistance was necessary. In the last 2 procedures, two successful PTNNs were performed using the extra-long 5-mm flexible forceps and prebent laproscopic intruments.Results Thirty nine HTNNs and two PTNNs clinical cases were successfully accomplished. One patient was converted to open surgery because of injury of the inferior vena cava. The mean operative time was 143 min. The mean estimated blood loss was 180 ml. The mean postoperative hospitalization stay was 7.4 d. Conclusions HTNN is a feasible and safe in appropriate patients. Existing instruments are still needed improving. PTNN is technically challenging but may be feasibly and safely performed.
Pure Transvaginal Natural Orifice Transluminal Endoscopic Surgery (NOTES) for Unroofing of Renal Cyst: Report of 4 Cases
Introduction To date, there was no report about pure transvaginal natural orifice transluminal endoscopic surgery (NOTES) for unroofing of renal cyst in humans.Purpose To describe the initial clinical experience of pure transvaginal NOTES for unroofing of renal cyst, and evaluate its feasibility. Materials and Methods Between December 2010 and March 2011, four female patients with simple renal cysts (right 3, left 1), underwent pure transvaginal NOTES. After induction of general anesthesia, the patients were positioned in lithotomy with ipsilateral lumbar at 30 degree angle to the operating table. A 3-mm incision was made at the posterior vaginal fornix, and a 5-mm Trocar was introduced into the pelvic cavity guided by a 5-mm forceps. A 5-mm 0 degree flexible laparoscope was inserted into the pelvic cavity confirming no rectum injury. Then a Triport was introduced at the posterior vaginal fornix. The patients head end was uppered by 25 degree with right lumbar at 60 degree angle to the floor. The renal cyst was found after dissection. Then the partial renal cyst wall was cut by a harmonic scalpel and removed. The vaginal wound was closed under direct vision using a 2/0 absorbable suture. Results All the procedures were successfully completed. The median operative time was 85min (range 75 to 90). The median estimated blood loss was 30 ml (range 20 to 50). There were no intraoperative or postoperative complications. The patients were discharged on postoperative day 4. Conclusions Pure transvaginal NOTES for unroofing of renal cyst is feasible.
Laparoendoscopic Single Site Surgery (LESS) Radiofrequency Ablation Treatment for Renal Cell Carcinoma
Introduction radiofrequency ablation (RFA)has been increasingly applied in the management of small renal tumors. We reported our experience of laparoendoscopic single site surgery (LESS) RFA for the treatment of small renal tumors. Our objective was to assess the short-term oncologic efficacy of RFA. Material and MethodLESS of RFA with a temperature-based radiofrequency generator was performed on a exophytic renal tumor size range 2.7cm (c T1N0M0) in a female patient age 61 years. Initial contrast-enhanced computed tomography (CT) examination was performed 21 days after the procedure, with subsequent CT assessment at three months, six months, and every six months thereafter. We evaluated the technical success, technical effectiveness, ablation zone, benign periablation enhancement, irregular peripheral enhancement, and complications. ResultsThe tumor was biopsied before RFA, of which was diagnosed as renal cell carcinoma (RCC) Furhman nuclear grade II. The operative time was 210minutes, with an estimated blood loss of 100 mL and no patient required a blood transfusion and postoperative hospital stays of 3days . Technical success and effectiveness was achieved. There was complete ablation. No death or renal failure after the procedure has yet been found. Abdominal CT scans after 3weeks confirmed complete treatment of the lesion ConclusionOur results showed that the LESS RFA on small renal mass was safe as an alternative treatment for exophytic RCCs and represents a promising treatment for some patients with small RCCs. Further research and a longer follow-up period are needed to confirm our results.
Laparoendoscopic Single -Site Nephroureterectomy with an Endoscopic Distal Ureteral Approach for the Management of Upper Urinary Tract Transitional-Cell Carcinoma
IntroductionEndoscopic ureteral surgery has been proposed as a complementary step in nephroureterectomy, either open or laparoscopic, to obviate the low abdominal incision.Objective: To describe our technical details of laparoendoscopic single-site (LESS) nephroureterectomy with an endoscopic distal ureteral approach for the management of upper urinary tract transitional-cell carcinoma (TCC) based on oncologic principles.MethodA 61-year-old man with a TCC of the left renal pelvis underwent transperitoneal LESS nephroureterectomy with an endoscopic distal ureteral approach. The patient was placed in a left flank position. A 3-cm umbilical skin incision was made and extended down to the peritoneum. X-CONE port was inserted through the umbilicus. Using special curve or S-PORTAL and standard laparoscopic instruments, the LESS nephroureterectomy was performed in the same process as conventional laparoscopic nephrectomy. Then we changed the position of the patients to a supine position with a 30-degree Trendelenburg . Pluck transurethral detachment of intramural ureter by resection of ureteral meatus and surrounding tissue was performed with a resectoscope and subsequent cephalad extraction.ResultsThe procedure was completed successfully without conversional laparoscopic or open surgery and without additional extraumbilical trocars or incisions. LESS nephreoureterectomy with an endoscopic approach was performed in 380 minutes. There was no intraoperative complication. CONCLUSIONS: According to our experience, an endoscopic approach for upper urinary tract TCC is a minimally invasive technique that is safe and effective as a complementary technique for one-step LESS nephreoureterectomy and adheres to oncologic principles. Long terms of oncologic outcome are required.
Department of Urology, Seoul National University Bundang Hospital, Seongnam, Korea
The porcine uterine horn is similar to the human vermiform appendix. Therefore, its resection is an established animal model for the human appendectomy.
We evaluated the feasibility of a pure transvesical NOTES approach to uterine horn resection (UHR) in a porcine model.
We performed five operations on three female pigs (30-35kg) under general anesthesia in the Trendelenburg position. The laparoscope at the umbilicus was used only for the purpose of documentation. We used a rigid ureteroscope and a customized access system that prevented gas leakage and facilitated in-and-out passage of the instruments. A vesicostomy was created on the posterolateral bladder wall using a needle knife through the channel of the ureteroscope. The UHR was performed using an electric needle knife, hot forceps, and a polypectomy snare through the access system placed in vesicostomy. Bladder closure was performed with extracorporeal ties using metal clip tagged threads and a knot-pusher.
We successfully performed the pure transvesical NOTES UHR. The mean total operative time was 141.8 (±58.7) minutes, and blood loss was minimal in all cases. No leakage was observed at the bladder repair sites after filling with normal saline. The removed uterine horns were approximately 6-12cm long and 0.6-0.8cm in diameter. On final inspection, the urethras were not damaged.
This study demonstrates the feasibility of a pure transvesical NOTES UHR in a porcine model. To our knowledge, this is the world's first report on a pure transvesical NOTES with a therapeutic purpose.
Pure Transvesical Notes Uterine Horn Resection in Swine as an Appendectomy Model: Revised Technique
Previously we demonstrated the feasibility of a pure transvesical NOTES uterine horn resection (UHR) in swine as an appendectomy model. To our knowledge, it was the world's first report on a pure transvesical NOTES with a therapeutic purpose. However, the visualization of the ureteroscope was poor and there was room for improvement in this technique.
To improve visualization and operability, we modified the instruments and the technique of a pure transvesical NOTES UHR.
We performed eight operations on four female pigs (30-35kg) under general anesthesia with revised technique. The modified access system was customized with a Teflon tube having smaller outer and larger inner diameters than previous system. The rigid ureteroscope was substituted with the 5mm long laparoscope (500mm, 30 degree) as a main endoscope. In addition, metal clipped threads for bladder closure could be easily placed using long needle. The most surgical procedure was similar to the original technique.
The new set of instruments provided much better visualization and operability. The mean total operative time was shortened to 89.1±10.6 minutes compared to the original technique (141.8±58.7 minutes). Estimated blood loss was 11.3±9.2 ml. In addition, base of the uterine horn could be securely ligated using loop ligating snare. Metal clipped threads could be placed through the bladder with lesser traumatic method.
The revised technique of the pure transvesical NOTES UHR provided improved outcome and feasibility, making this approach more easily applicable to the human appendectomy in the future.
Department of Urology, Policlinico di Modena, Univerista' di Modena e Reggio Emilia
Introduction : Natural orifice translumenal endoscopic surgery (NOTES) has been evaluated for Urologic surgery. Purpose: Present our series of NOTES radical prostatectomy. Matherial and Methods :In April 2011 five NOTES radical prostatectomy were performed. Corpses were placed in lithotomic position. Equipment used consisted of: 22 ch cystoscopes (Karl Storz Endoskope) , 7 ch stabilizing catheter (Cook Medical Inc.), 100 W RevoLix Thulium laser (Dimed, LISA laser products). Urethrovescical anastomosis was performed using a 27 ch nephroscope with 5 mm working channel and SR5 suture device (LSI Solutions). Prostatic dissection started at 7 o'clock and carried out until the prostatic apex, the periprostatic fat was visualized, than dissection is continued from 7 to 11 o'clock. The left lobe of the prostate in dissected starting at 5 o'clock in an anticlockwise fashion. After seminal vesicles dissection from the posterior wall of the bladder, the remnants attachment between prostate and bladder neck were resected and the specimen was pushed into the bladder. Uretehrovescical anastomosis was performed using four interrupted sutures with extracorporeal knots that were seated using a knot pusher. Results: Mean operative time was 184 minutes; pathological examination showed a radical excision of the gland though assessment of the neurovascular bundles was not possible. Conclusion: NOTES radical prostatectomy is feasible in an ex vivo model. Clinical application of this technique is subject to careful patient selection . Acknowledgments: The authors wish to thank Let People Move Foundation for technical and organizational support and M.C.Nizzi for the video post production.
VS13: Robotic/Laparoscopic Upper Urinary Tract Surgery 3
Instituto Medico la Floresta, Caracas Venezuela
INTRODUCTION AND OBJECTIVES: Goals of partial nephrectomy are negative cancer margins, and renal functional preservation. At ischemia, each minute may compromise function of the renal remnant. Efforts to eliminate renal ischemia are imperative We present a novel "zero ischemia" technique of laparoscopic (LPN) partial nephrectomy in 16 patients with a small renal massMETHODS: : Sixteen patients underwent "zero ischemia" LPN with the following technique: micro-dissection of tumor- specific renal artery branches, plus controlled hypotension during excision. Controlled hypotension is designed to decrease intra-operative hemorrhage while providing excellent systemic perfusion. The goal is to lower the mean arterial pressure (MAP) to 50-65 mm Hg or a 30% reduction of baseline MAP. Pre- and intra-operative anesthesia-related hypotensive monitoring included continuous pulmonary artery pressure measurements, trans-esophageal echocardiography, and brain activity measurements. Timed, pharmacologically-induced hypotension was carefully calibrated by an expert anesthesiologist, corresponding with parenchymal resection. Hypotension was reversed after completing resection and initial renorrhaphy. Parenchymal reconstruction was completed under normotensive conditions to assure hemostasis was achieved.RESULTS: All cases were successfully completed without hilar clamping. Ischemia time was zero in all cases. Median tumor size was 2.7 cm (0.9-4), operative time 3 hrs (1-5), blood loss 100cc (20-200), and hospital stay 3 days (2-19). Nadir mean arterial pressure ranged from 49-65mmHg (median 60), No transfusions or complications were seen. Median preoperative and postoperative serum creatinine (0.9mg/dL and 0.95mg/dL) and estimated GFR (75.3 and 72.9) were comparable. CONCLUSIONS: "zero ischemia" technique represents a significant step itowards the goal of eliminating surgical ischemia.
Use of Laparoscopic Post-Anastomotic-Dismemberement (PAD) Pyeloplasty in Difficult Ureteropelvic Junction Obstruction (UPJO)
Laparoscopic pyeloplasty becomes technically challenging if the kidney is placed abnormally, or in patients with small intrarenal pelvis with or without a long atretic ureteric segment. Crossing vessels or associated anomalies may also add to difficulty. In our practiced method of pyeloplasty (Post-anastomotic-dismembered or PAD) we dismember ureteropelvic plate after the pelvic flap has been fixed to the spatulated ureter. The technique helps in difficult UPJO by keeping the flaps aligned and by providing handle for retraction. The young female in the first example has a small intrarenal pelvis and a long atretic UPJ segment. Pyeloplasty could be accomplished using the PAD technique. Patient In the second example has an ectopically placed left kidney with pelvis facing superolaterally. In addition, the latter patient also has a large cyst filling the whole ipsilateral renal fossa and a long narrow ureteropelvic segment. The cyst was excised in toto including its wall. Ureter was traced up from its pelvic location to the renal pelvis. A PAD pyeloplasty was successfully performed after creating the pelvic flap and the ureteric spatulation.211 laparoscopic PAD pyeloplasties have been performed till date. One or multiple difficult factors were present in 60 (28.4%) in form of abnormal location in 11 (horse shoe 6. Ectopic 5), long UPJ segment (>2.5 cm) in 14, small intrarenal pelvis in 3, crossing vessels in 41, and associated anomalies (cyst) in 1. A laparoscopic PAD pyeloplasty could be successfully performed in all.PAD pyeloplaty with its advantages is useful in difficult situations with UPJO.
LESS Pyeloplasty: A Combined Laparoscopic and Robotic Approach
Objective: Laparoendoscopic single-port (LESS) pyeloplasty has been introduced as another minimally invasive treatment option for ureteropelvic junction obstruction. We present a video demonstrating our combined laparoscopic and robotic approach. We theorize that laparoscopic dissection minimizes clashing of robotic arms in the tight working space. However, magnification and wristed instrumentation of the robotic instrumentation may better facilitate ureteral reconstruction.
Materials: A 29-year-old male presented with intermittent right sided abdominal pain. A crossing lower pole vessel was seen on a CT, and a MAG-3 renal scan demonstrated delayed clearance of radiotracer on the right side.
Results: Our 6-minute video demonstrates our technique for LESS pyeloplasty. The double-J ureteral stent is placed in a retrograde fashion with cystoscopy at the beginning of the procedure. A GelPoint port is then placed into a periumbilical incision. A flexible tip 5mm camera was used with straight laparoscopic instruments to reflect the colon and mobilize the redundant renal pelvis and ureter. Once the ureter was excised, we switched to robotic instruments and docked the DaVinci S robotic system to complete the ureteral reconstruction. There were no intraoperative complications. His post-operative renal scan demonstrated improvement in renal drainage.
Conclusions: Our LESS pyeloplasty technique combines elements of laparoscopy and robotic techniques in order to adapt to the single incision operative field. Our video demonstrates the safety and feasibility of this approach. We have successfully completed this operation on three patients, defined clinically and by renal scans. We continue to refine our technique and to decrease our operative times.
Section of Laparoscopic and Robotic Surgery, Department of Urology, Frimley Park Hospitals NHS Foundation Trust. Surrey. UK
Right Robot Assisted Ureteral Reimplantation with Psoas Hitch
Objective: We present the video of a 46yo female who underwent a robotic ureteral reimplantation after having sustained a ureteral injury during an abdominal hysterectomy.Methods: A transperitoneal approach was performed. Ports were place in the same configuration as robotic prostatectomy.Results: Operative time was 1 hour and 28 minutes. Blood loss was 100 ml. Postoperative renal scan showed complete resolution of obstruction. No perioperative complications occurred.Conclusion: Robot assisted ureteral reimplantation is a safe and feasible procedure for distal ureteric pathology.
Volgograd State Regional Center Of Urology and Nephrology, Volgograd, Russia
BACKGROUND AND PURPOSE: Laparoscopic retroperitoneal pyelolithotomy (LP) can be used for large single renal pelvic stones. We present our experience with this procedure in five patients. We compare laparoscopic pyelolithotomy and percutaneous nephrolithotomy in the management of solitary large renal pelvic stonesPATIENTS AND METHODS: Between May 2009 and May 2011, five patients underwent laparoscopic pyelolithotomy for a treatment a large renal-pelvic stones. All stones were solitary with a mean size>23 mm in diameter. All were approached retroperitoneally. They were compared with a group of 20 patients after PCNL.RESULTS:There was no difference between the two groups regarding the characteristics of patients and stones. Operative time duration was significantly longer in LP group (143 vs. 116 min).Mean hospital stay was respectively 8.5 and 6.2 days in groups LP and PCNL.mean estimated blood loss (145 mL vs 214mL), and stone-free rate (100 % vs 90 %).In LP-group all the procedures were completed laparoscopically with no conversions to open surgery. There was one (5%) case from the PCNL group converted to open surgery because of uncontrolled bleedingCONCLUSIONS: LP is effective and safe method of treatment pelvic stones. The results of LP and PCNL are comparable, but the operative time and hospital stay of LP is longer
Department of Urology, Hanyang Univesity College of Medicine, Seoul, Korea
Introduction: We report the initial experience of laparoscopic anatrophic nephrolithotomy (LAN) with ice-slush for staghorn stone.Materials and Methods: The patient was a 57-year-old man who presented to the urology department with abdominal pain and gross hematuria. Computed tomography revealed a large renal stone measuring 3.3x2.0x6.6cm and mild hydronephrosis in the left side. After the ureteral catheter was inserted, the patient underwent left LAN, which was performed transperitonealy via 4 ports in the left flank position. After superior retraction of the spleen and medial mobilization of the colon, the renal pedicle was exposed. After entrapment of kidney with entrapment bag, ice-slush was inserted through the Alexis port with 20cc syringe. 20 min before inducing kidney ischemia, 12.5 g of mannitol was infused. The renal artery and vein were clamped using a bulldog clamp. A nephrotomy incision was made on the Brodel line. The stone was extracted from the abdominal cavity using an endo-bag. The collecting system was irrigated with normal saline, and the collecting system was closed with 3-0 Monocryl running suture. The cortex was closed using 2-0 Monocryl by sliding knots technique.Results: During the LAN, blood loss was 650ml and cold ischemia time was 56 minutes. Total operative time was 280 minutes. Postoperative blood transfusion was required with 3 units of PRC. Hospital stay was 7 days. Postoperative ultrasonography showed no residual stone.Conclusions: Laparoscopic anatrophic nephrolithotomy is a feasible alternative for patients with staghorn stone who are candidates for open surgery.
VS14: Pediatric Surgery/New Technology
Texas Childrens Hospital, Houston, TX, USA, 2Baylor College of Medicine, Houston, TX USA
PURPOSEThe high intra-abdominal testicle is an operative challenge. In a small subset of patients, testicular autotransplantation is an alternative to the Fowler-Stevens approach. Autotransplantation allows for preservation of the spermatic artery and is suitable for patients with abnormal vasal anatomy. Epigastric vessel mobilization is traditionally done through a Gibson incision to assure adequate vascular length. We propose that laparoscopic mobilization of the epigastric artery and vein maximizes the length of the vessels and minimizes incisional co-morbidity.METHODSThree laparoscopic ports are placed in standard fashion. Testicular mobilization is performed as previously described. Mobilization of the epigastric vessels begins at the vessel bifurcation superiorly and extends down to the vessel origin. A small cosmetic groin incision is made. The testicular, and then epigastric vessels, are clipped and delivered through the groin incision. The testicle is secured in a dartos pouch and a microvascular anastomosis is performed to re-vascularize the testis. RESULTSSix patients (seven procedures) are included in this series. Mean estimated blood loss was less than 25cc and the mean operative time was 8 hours (6.1-11.5). A viable scrotal testis observed>6 months post-op was achieved in four of five patients. One testicle was lost due to necrosis/abscess. Two cases have recently been performed (<3 months) and are so far doing well.CONCLUSIONTesticular autotransplantation is a procedure reserved for rare cases of high intra-abdominal testicles. We propose that a laparoscopic mobilization of the epigastric vessels is technically straight-forward, provides excellent vessel length and surgical incision length is minimized.
Trus-Based Navigation of Prostate Intervention for Active Surveillance and Focal Therapy Using 3D Trus, GPS Tracking, Mr Fusion, and Robotics
USC Institute of Urology, University of Southern California, Los Angeles, USA
Introduction: To assist precise prostate targeting and accurate 3D mapping of the biopsy trajectory in the prostate model, computer-assisted guidance systems are developed. In previously reported systems, the devices for tracking the TRUS probe sometimes disturb or constrain the range of the free-hand manipulation, and thus those could affect against the smooth and precise biopsy operation. Purpose: The purpose of this study is to develop a novel tracking method of the TRUS probe to locate current scanning position in the prostate based on image registration accelerated by Graphics Processing Unit (GPU). Materials and Methods: The proposed method has two steps. First step is reconstruction of a 3D US image of the prostate from the series of simultaneous biplane US images by free-hand scanning. Second step is registration between the reconstructed 3D US image and live biplane US images to locate current scanning position. Reconstruction accuracy was evaluated by comparing the reconstructed 3D US image with the MR image of the prostate phantom. Tracking accuracy was evaluated by comparing the estimated position and orientation with those measured by the optical tracker. Results: Mean surface error was 0.71 mm and overlap ratio was 0.962 (1.0 means completely matched). Mean tracking error was 3.5 mm and 3.8 degrees in translation and rotation, respectively. The frame rate was 2.1 frames per second. Conclusions: We developed the new tracking method of the biplane TRUS image, which does not disturb the free-hand operation of the probe. The results suggest its feasibility and potential advantage.
Shahid Labbafinejad Medical Center, Tehran, Iran
Introduction:Benign urethral tumor as a cause of obstructive symptoms in children is rarePurpose:We present the technique of resection for a large prostatic urethral mass in a 3- year old boy.Materials and Methods:A 3- year old boy was referred to us because of obstructive outlet symptoms. On CT scan and MRU there was a large mass in prostatic urethra. We performed cystoscopy that showed a mass about 3*3 centimeters with a pedicle just close to verumontanum. Bladder was moderately trabeculated. Resection was done meticulously to prevent sphincteric damage. After resection and fulguration of pedicle, we were not able to remove the large mass through the urethra because of the size of the mass. A 2 centimeter incision was done on suprapubic area and the mass was removed.Result:Histologic examination was fibroelitheliuma and the symptoms were relieved.Conclusion:Benign tumors of urethra should be kept in mind in children that are easily manageable endoscopically.
The Surgical Outcomes of Mini-Laparoscopic Herniorrhaphy in Infants
Objective: To present the surgicqal technique of mini-laparoscopic herniorraphy and compare the surgical outcomes of mini-laparoscopic and open herniorraphy (MLH and OH) in infants.Materials and Methods: We enrolled 55 infants undergoing herniorrhaphy. Of them 24 had MLH and 31 had OH. Mean ages of the MLH and OH groups were 7.17±4.21 and 5.39±4.11 months, respectively (p=0.37). A contralateral PPV more than 2cm was repaired simultaneously in 13 (65%) of 20 infants who initially diagnosed as unilateral hernia. Finally, 17 and 7 infants had bilateral and unilateral MLH; 9 and 22 infants had bilateral and unilateral OH. Results: The mean follow-up periods in MLH and OH groups were 22.9±10.5, and 20.2±10.5 months, respectively (p=0.20). Contralateral metachronous inguinal hernia occurred in 4 (18%) of the 22 unilateral hernia in OH group, and in none of the 20 initially presented as unilateral hernia in MLH group (p<0.05). Recurrence occurred in 1 of the 40 open herniorrhaphy sites, and none of the 41 of mini-laparoscopic herniorraphy sites (p=0.49). For the unilateral herniorraphy, the mean operation time of MLH was longer than that of OH (80.00±18.97 vs. 51.15±23.27 minutes, p<0.05). For the bilateral repair, the mean operation time was comparable between these two groups (MLH vs. OH=82.52±14.74 vs. 95.62±20.62 minutes, p=0.35). Conclusions: Mini-laparoscopic herniorraphy in infants may prevent contralateral metachronous inguinal hernia, and was as effective as open herniorrhaphy in infants. The drawback of mini-laparoscopic repair was the longer operation time in the unilateral herniorraphy, which may be overcome by increasing experience.
Scott Department of Urology, Baylor College of Medicine, Houston, Texas, USA, 2Texas Children's Hospital
INTRODUCTION: The Mitrofanoff appendicovesicostomy has been a mainstay in pediatric urology as a treatment for urinary incontinence in patients with the inability to empty the bladder. PURPOSE: We present our experience with laparoscopic Mitrofanoff appendicovesicostomies and compare it with the open approach. MATERIALS AND METHODS: A retrospective analysis of medical records was performed comparing patients undergoing laparoscopic and open Mitrofanoff appendicovesicostomies from 2009-2011 at our institution. Patient demographics, hospital course, and surgical outcomes were analyzed. RESULTS: Twenty-five patients underwent a Mitrofanoff appendicovesicostomy at our institution over the past three years. Patients undergoing a major concomitant procedure, including augmentation cystoplasty and Malone antegrade continence enema procedure, were excluded. Four patients underwent a laparoscopic Mitrofanoff procedure, and five had an open Mitrofanoff appendicovesicostomy. There were no intraoperative complications nor any laparoscopic-to-open conversions. Post-operative hospital stay was a mean of 2.75 days for the laparoscopic group, and 6.6 days in the open group. In the laparoscopic approach, all three patients resumed a regular diet on post-operative day 1, compared to a mean of 4 days in the open group. There was no difference in time to initiation of catheterization between groups, and follow-up times were similar. There were no post-operative complications in the laparoscopic group, although one patient in the open group had a wound infection requiring bedside drainage. CONCLUSIONS: The laparoscopic approach to the Mitrofanoff procedure is a safe and technically feasible surgery with high efficacy and low complication rates.
Laparoscopic Treatment of an Ectopic Ureterocele in a Duplicated Left System
The Objective of this paper is to present a case of an ectopic ureterocele in a duplicated left system who was treated by extraperitoneal laparoscopic excision. Material and Method From a total of 31 patients with genito-urinary malformations that were treated by surgical approach we selected a case of a 17 year old girl, that presented with recurrent urinary tract infections and flank pain. Abdominal ultrasound and CT scan revealed an ectopic ureterocele in a duplicated left side system with intimate rapports with the left renal vessels. Results The mean operative time was 195 min. There were no postoperative complications. The patient was mobilized after 24 hours and the postoperative bowel movement resumed after 35 h. The patient was discharged after 5 days. At 15 month of follow-up the patient is free of symptoms with normal renal function and ultrasound.Conclusions. Laparoscopic approach for treatment of ectopic ureterocele in duplicated system is feasible even if the proximal end is at the level of renal hilum. Retroperitoneal approach is difficult due to the restricted working space, especially when dissecting the ureterocele from the anterior side of the renal vessels
The Roth-Net Device for Percutaneous Stone Retrieval
Objective: The Roth-Net retrieval device (US Endoscopy, Mentor OH) has been utilized for gastrointestinal endoscopy since 1993 for tissue retrieval and foreign body retrieval. Our objective was to evaluate its utility in stone retrieval for percutaneous nephrolithotomy. Methods: A 30F Amplatz sheath was placed into an ex vivo porcine kidney. Fifteen calculi ranging from 2 to 3 mm were placed percutaneously through the sheath and positioned in a dependent calyx. A Storz rigid nephroscope was utilized to observe the calculi. The 5.4F Pediatric Roth-Net retriever (US Endoscopy Model 00711057, Mentor OH) was deployed through the working channel. The device consists of a custom-woven nylon mesh with a 1 mm open spacing. The wire frame is a 0.018 in 3×3 stainless steel braided cable of medium stiffness. The net size is 2 cm wide×4 cm long. A total of five trials were performed with the Cook Perc-N-Circle stone basket and five trials were performed with the Roth-Net. Results: Multiple stone fragments were successfully retrieved with the Roth-Net device, whether free-floating, or lying dependent in a calyceal fornix. On the basis of the five trials performed on each device, the average number of stones retrieved with the Cook Perc-N-Circle was 1.5 per attempt, whereas the average number with the Roth-Net was 8. The calculi could be easily released by opening the Roth-Net device, and no endoscopic evidence of trauma to the urothelium was noted. Conclusion: The Roth-Net offers an effective alternative for percutaneous extraction of multiple small calculi.
Application of Sand Balloon Catheter™ for Laparoscopic Excision of a Giant Retroperitoneal Cystic Lymphangioma
Retroperitoneal cystic lymphangioma is rare benign tumor. Most patients eventually experience some symptoms that necessitate therapeutic intervention. Total excision should be chosen for the treatment to avoid tumor recurrence, since it is difficult to decide preoperatively whether the lesion is benign or not. Although laparoscopic resection would be preferable as minimum invasive surgery, complete resection is not easy when the tumor is extremely large. We have experienced laparoscopic resection of large cystic lesions with the use of the SAND balloon catheter™. We show video introducing technique of the laparoscopic excision of huge cystic lymphangioma with the SAND balloon catheter™. Puncture and aspiration of the cyst contention with this device made complete resection feasible. Laparoscopic surgical technique could be considered for treatment of such large cystic lesions with the application of SAND balloon catheter™.
Department of Urology, Fundació Puigvert, Barcelona, Spain.
ABSTRACT WITHDRAWN
VS15: Percutaneous Surgery
Micro / Minimicro PCNL with “all Seeing Needle”a New Way to do PCNL
Background: PCNL has undergone many developments; most recent advancement is micro and miniµ PCNL. Purpose: To study the safety and efficacy of micro and miniµ PCNL.Material & Method: A prospective nonrandomized study over one year period of micro and miniµ PCNL done in 34 cases. PCNL was done through either 4.85 Fr needle sheath (Micro) or 8Fr sheath (Mini-micro) after assess preformed by All seeing needle. 3way connector allowed irrigation, passage of flexible telescope and a 200 μm holmium: YAG laser fiber. All data was prospectively evaluated and analyzed.Results: A total of 34 case were done (14 Micro; 20 Mini-Micro). The preoperative demography included age 43.8±16 years, male-female ratio (26:8) and stone size (12.09 mm±3.9mm). 2 pediatric patient, 1 ectopic, 2 duplex, 22 calyceal and 9 pelvic stone were treated. Success was in all except 2. Intraoperative time was 82.20±32.43min, surgeon VAS score was 3.1±1.2 and hospital stay was 3.6±1.2 days. Stone free status at 1 month was 89.29%. Six patients had a self limiting post operative fever and 1 had persistent flank pain for which RIRS was done. Conclusion: Micro PCNL and Mini µ PCNL is technically feasible, safe and efficacious for small volume renal calculus disease.
The Locator: Novel PCNL device to Aid Collecting System Puncture.
IntroductionPrecise needle puncture of the renal collecting system is an essential step for successful percutaneous nephrolithotomy (PCNL). Puncture is technically challenging and has many pitfalls for the urological surgeon. PurposeWe describe the development of a novel navigation system, the Locator, to assist accurate percutaneous needle placement and compare this to conventional manual techniques. Materials and MethodsThe essence of the device is that it stabilizes the needle for PCNL puncture. It relies on an adjustable lockable multidirectional head that is securely fixed to the operating table. The radiolucent head holds a 10Fr metal guide that allows renal collecting system puncture. The system uses the traditional fluoroscopic bulls eye sign to achieve precise and fixed alignment. Objective assessment was obtained by in vitro testing using simulated PCNL puncture with and without using the Locator. Time to successful puncture and fluoroscopy screening time (FST) was assessed.Results Six urological trainees were recruited to test the Locator. Simulated PCNL puncture was quicker and with reduced fluoroscopy when the apparatus was used. The mean FST for traditional hand vs Locator puncture was 46 vs 16 seconds (p=0,03) and the mean time to puncture was 225 vs 118 seconds (p=0,26).ConclusionThe Locator is a simple, cheap and novel assistant to achieving successful PCNL puncture. Preliminary in vitro testing suggests that the device may reduce fluoroscopy exposure and be quicker. The device warrants further evaluation in the clinical setting.
Department of Urology, Keio University School of Medicine, Tokyo, Japan
We report a case of matrix stone in a 57-year-old man with sponge kidney. He had been followed-up due to sponge kidney since the age of 30. He had been hospitalized 7 times for acute pyelonephritis, and he had undergone 11 endourological treatments, such as TUL and ESWL. PNL was recommended because of the numerous and frequent admissions. The renal pelvis was filled with sludge having a dark brown-like matrix, and small calculi were scattered throughout the pelvis. All matrixes in the renal pelvis were removed using a suction tube under a nephroscope. The small calculi were removed with forceps. After left PNL, the formation and passage of stones disappeared and he no longer suffered from pyelonephritis. After a right PNL 10 months later, he became totally stone-free. Operation time of left PNL was 167 minutes, and right was 137 minutes.Matrix stones are an uncommon form of urinary calculi, and they are usually larger in volume and less likely to pass spontaneously. ESWL is usually ineffective due to the gelatinous nature- and lack of a disruptable mineral content of the stones. Ureteroscopic removal of matrix stones may be compromised by the large volume of stone material present, favoring the application of other techniques. Thus, percutaneous techniques afford the best chance of complete removal of matrix stones.
Endoscope-Guided Retrograde Renal Puncture for Percutaneous Nephrolithotomy in the Supine Position
Introduction: Percutaneous nephrolithotomy is an effective technique for minimally invasive removal of large stone burdens. Obtaining percutaneous access to the collecting system can be challenging, particularly for urologists who do not perform these procedures frequently. Endoscope-guided percutaneous renal access was previously proposed to facilitate accurate calyceal puncture. That technique requires prone positioning and leg spreader bars. In this video we demonstrate a new, simplified procedure to obtain retrograde percutaneous renal access in the supine position. Materials and Methods: 2 patients with 6 cm2 stone burden underwent the procedure. Patients were placed in Galdakao-modified supine Valdivia position. A safety wire and ureteral access sheath were placed from below. A ureteroscope was passed into the posterior calyx of choice and a Lawson set (Cook Medical, Spencer, IN) was used to puncture the kidney and flank in retrograde fashion. The puncture wire was exchanged for a guidewire and standard tract dilation was performed using a balloon under endoscopic and fluoroscopic guidance.Results: A single puncture attempt resulted in a straight tract in both cases. Mean operative time was 150 minutes. There were no intraoperative complications. Both patients were rendered stone free based on postoperative computed tomography. One patient had postoperative venous bleeding which resolved with conservative management. Conclusions: Endoscope-guided retrograde puncture in the supine position facilitates targeted percutaneous renal access by the urologist and obviates the need for prone positioning or spreader bars.
Comparative Study of Supine Versus Traditional Prone PCNL in Treatment of Urolithiasis
Introduction
Supine percutaneous nephrolithotomy (PCNL) has not gained wide acceptance among urologist since it was first described in 1998.
Purpose
To compare the outcome of PCNL in supine versus the standard prone position.
Materials and Methods
From January 2009 to March 2011, 81 patients (mean age 57.8 yr) who underwent PCNL in the North District Hospital, Hong Kong for large urolithiasis were analyzed. Technical choices about the position, percutaneous access, and use of concomitant ureteroscopy (URS) were at the surgeon's discretion.
Results
44 and 40 patients underwent supine and prone PCNL respectively. The two groups were comparable in age, gender and BMI. The maximum stone diameter was slightly larger in the prone group (27.4mm vs 21.7mm, p=0.02). Calyceal access was established by the urologist in 28 (63.6%) patients in the supine group and 38 (95%) in the prone group. Simultaneous URS was performed in 24 patients in the supine group, including 16 patients with ureteric stones. No significant difference was found in the operative time (supine, 108.7min vs. prone, 104.5min, p=0.62), haemoglobin drop (0.84g/dl vs. 0.91g/dl, p=0.799), stone clearance rate (86.4% vs. 82.5%, p=0.323), and the rate of auxiliary procedures (36.4% vs. 20%, p=0.097). Bleeding requiring transfusion occurred in one patient in each group. Pleural injury, colonic injury and renal pelvis perforation did not occur. One patient in each group developed pseudoaneurysm which required angioembolization.
Conclusions
Supine PCNL offers comparable outcome to prone PCNL. Simultaneous URSL is a feasible option for concurrent calyceal and ureteric stones.
Percutaneous Transitional Cell Carcinoma Resection with Temporary Renal Artery Occlusion
Introduction: The feasibility of intra-operative trans-arterial balloon occlusion of the renal artery as a novel technique to reduce blood loss was evaluated in a patient undergoing percutaneous resection of a large transitional cell tumor involving the renal collecting system. Methods: The patient was a 59 year old man who presented with gross hematuria and was found to have a large filling defect within the left renal collecting system. Prior to gaining renal access, interventional radiology performed intra-operative trans-femoral arteriography followed by left renal artery balloon occlusion. Access was then obtained by the urologist using fluoroscopic guidance. Rigid nephroscopy demonstrated a large papillary tumor, which was resected with loop electrocautery. Following resection, the arterial occlusion balloon was deflated and repeat renal angiography was performed. No active bleeding was noted. The angiographic catheter was removed thereby completing the case. Results: Marked subjective improvement in visualization was reported by the surgeon allowing thorough resection of the upper tract tumor. No intra-operative or peri-operative complications were noted. The estimated blood loss was 100 ml. Temporary renal artery occlusion was subsequently used in three patients. One underwent an antegrade endopyelotomy and two percutaneous nephrolithotomy for complex staghorn calculi. None of the patients experienced any intra-operative complications. Conclusions: Intra-operative balloon occlusion of the renal artery is feasible and safe in patients undergoing percutaneous renal surgery allowing for improved visualization during complex cases. The technique should be considered in patients with large staghorn calculi who will require multiple punctures and select high volume, low-grade upper tract tumors.
Percutaneous Resection of Renal Pelvis TCC in Solitary Kidney Following Neoadjuvant Chemotherapy
The patient is a 54 y.o. Caucasian female with history of Lynch Syndrome. She had undergone prior right laparoscopic nephroureterectomy for upper tract TCCa 4 years previously. She presented with a 2.8 cm x 2.8 cm calcified, enhancing renal pelvis mass in her solitary left kidney, and underwent neoadjuvant chemotherapy to attempt to downsize the lesion in preparation for renal-sparing endoscopic resection. After 3 cycles of chemotherapy, repeat CT scan demonstrated reduction in size to 1.1 cm=1.8 cm. She underwent percutaneous resection of her renal pelvis TCCa which was completed in “tubeless” fashion. She was discharged on POD #1. Pathology revealed low grade TCCa of the renal pelvis, stage pTa.
Urology and Nephrology Research Center, Tehran, Iran, 2Shahid Labbafinejad Medical Center, Tehran, Iran. 3Shahid Beheshti University, Tehran, Iran.
Introduction:Management of transitional cell carcinoma of renal pelvis, especially low grade tumors in challenging.Purpose: to avoid nephrectomy in a patient with single functioning kidney with large pelvic tumor we performed endoscopic resection plus intra pelvic BCG therapy.Materials and Methods:We present a 56- year male with complaint of hematuria and past history of renal pelvic tumor that was resected using open surgery. There was a large filling defect in UPJ region leading to mild pelvic dilatation. We were able to get access through percutaneous approach. At first, ureteral catheter was detected and used as a landmark to start resection. Resection and fulguration was performed completing in 360 degree around UPJ. The histologic examination showed low grade Ta, TCC and BCG instillation started 2 week then after.Result: 6 months post operation there is no complication and tumor recurrence. Conclusion:Percutaneous resection of even large tumor of renal pelvic is a viable part of treatment strategies for renal pelvic tumor, especially in single kidney patients.
VS16: Robotic/Laparoscopic Pelvic Surgery
Dept of Urology, PSG Institute of Medical Sciences and Research, Coimbatore, India
Introduction: Ileocystoplasty is one of the common augmentation procedures done for the management of low compliance and low capacity bladders. Mitrofanoff procedure is done to facililate self catheterization in patients who have urethral obstruction or apprehensive about self urethral catheterization,. We present the video of a patient who underwent laparoscopy assisted Ileocystoplasty with Mitrofanoff procedure with Yang-Monti tube. Materials and Method: A 46 year old diabetic patient presented with storage lower urinary tract symptoms for the previous 5 years. He was found to have low compliance, overactive bladder on urodynamic study. Under general anesthesia, using 5 ports, bladder was dissected and mobilised. Through a 5 cm sub umbilical incision, a 10 cm + 3.5 cm segment of ileum was isolated for Ileocystoplasty and Yang-Monti catheterisable channel respectively. Bowel continuity was restored. Ileo cystoplasty was completed by anastamosing detubularised bowel segment to the bladder. Mitrofanoff procedure was completed by a non refluxing anastomosis of catheterisable channel and a stoma was created in the right iliac fossa.. Results: The operative duration was 320 minutes and the approximate blood loss was 150 ml. Cystogram at 21 days showed no leak and catheters were removed. Patient is able to perform self catheterization through the mitrofanoff channel and is continent. Conlcusion: Laparoscopy assisted Ileocystoplasty with Yang Monti Mitrofanoff procedure is feasible and effective in patients who are unable to perform self urethral catheterization.
Departament of Urology, CES clinic, Medellín Colombia
OBJECTIVE: To show the laparoscopic surgical treatment of a giant bladder diverticulum and vesicoureteral reimplantation.MATERIALS AND METHODS: 75 years old male patient, with lower urinary tract symptoms. Cystoscopy shows endourethral prostate obstruction, middle lobe and a large bladder diverticulum in the left posterolateral wall with multiple stones, the left ureteral orifice is included into the bladder diverticulum.The patient underwent to transurethral resection of the prostate, with good results, then laparoscopic bladder diverticulectomy and vesicoureteral reimplantation was made.SURGICAL TECHNIQUE: Under general anesthesia and prophylactic antibiotics, transperitoneal laparoscopic approach is performedBladder dissection with harmonic scalpel. Exposition of the bladder mucosa and identification of the diverticulum neck, Gauzes are left inside the diverticulum to facilitate external identification.Separation of the bladder diverticulum, which includes the left ureteral orifice.The diverticulum is introduced into a bag and extracted. Cystorrhaphy with 2-0 polyglactin 910, continous suture.The ureter is exteriorized an a zebra guide is passes to the renal cavities, Double J catheter is leaved and the first stitch is made, the ureter is reintroducen into de abdominal cavity.The ureterovesical anastomosis is made with interrupted sutures of 2-0 VicrylAt the end of the procedure, a cistoscopy is made, confirming the absence of stones or diverticulum, Patients presents a proper evolution, without urinary symptoms and control cystography without fistulas or diverticula.RESULTS: The patient progressed satisfactorily, the cystoscopic control showing absence of the diverticulum, ureteral orifice and bladder healthy normal reiplanted.CONCLUSIONS: We believe that laparoscopic surgery of bladder diverticula is an option in the management of this patient, who requires surgical resolution, this paper show other procedures associated such as ureteral reimplantation, cystolithotomy at the same time of surgery with excellent postoperative results .KEYWORDS: Bladder diverticulum. Cystolithotomy, ureteral reimplantation, Laparoscopy.BIBLIOGRAPHY:1. Haber GP, Gill IS. Laparoscopic partial nephrectomy: comtemporary technique and automes. Eur Urol. 2006;49:660& 8212;5.2. Pablo Pizzi, Octavio Castillo, Diverticulectomia vesical laparoscópica transperitoneal, Arch. Esp. Urol. 59,8, 2006: 805-808.3. LINKE, C.; MONGIAT-ARTUS, P.: Management of vesical diverticula. Ann. Urol. (Paris), 38: 103, 2004.4. GEPI-ATTEE, S.; FENELEY, R.C.: Bladder diverticulectomy revisited: case reports of retention of urine caused by diverticula and discussion. J. Urol., 152: 954, 1994.
Robot Assisted Laparoscopic Management of Iatrogenic Lower Urinary Tract Injuries
Introduction: The reported incidence of ureteral injuries during laparoscopic hysterectomy ranges from 0.4% to 2.5%, owing to the anatomic proximity of the reproductive and lower urinary tracts. Most iatrogenic lower ureteral injuries are managed via an open approach, due to their late presentation, and the extent of scarring that is often encountered. We present our experience with robot assisted laparoscopic repair of gynecological iatrogenic ureteral injuries.Materials and methods Form December 2006 to April 2011, a total of 10 patients was diagnosed with a ureteral injury following gynecological surgery. All patients underwent underwent a robot assisted neocystotomy. Patient demographics are summarized in table 1.Results: All 10 cases were successfully completed using robot assistance without any conversion. Mean operative time and blood loss was 182 minutes and 60.6 ml respectively. Patients were discharged with no perioperative complications following an average hospital stay of 2.5 days. No patients experience ureteral obstruction, urine leakage, or fistula at a mean follow-up of 8.15 months.Conclusion: Robot assisted laparoscopic management of iatrogenic ureteral injury is an effective and safe option, consistent with the principles of open ureteral surgery, with the advantage of decreased morbidity.
Pure Laparoscopic Boari Flap for Pan Urethral Stricture Due to TB
INTRODUCTIONOne of the solutions to long segment ureteral strictures is Boari flap and Psoas Hitch. Patients presenting with long segment ureteric strictures are usually treated by open surgical Boari flap or ileal ureter substitutionPURPOSETo describe the technique for laparoscopic Boari flap uretero neocystotomy.PATIENTS AND METHODSA 26 year old female patient presented with long segmen ureteral stricture, on the right side. With ipsilateral hydronephrosis. Laparoscopic exploration, and removal of the strictured segment was done. Pathological examination of the specimen revealed isolated TB of the ureter. Laparoscopic Boari flap and psoas hitch were done. Double J stent was left for 3 months.RESULTS Operative time was 4 hours. Hospital stay was 3 days. Ureteral catheter was removed after 10 days, and stent was removed after 3 months. Follow up after Double J stent removal at 3, 6 and 12 months revealed completely normal upper urinary tract with no evidence of back pressure. And no intra or post operative complications nor long term complications were encountered.CONCLUSIONLaparoscopic Boari Flap is an effective and safe alternative for long segment uriteric strictures. With reduced morbidity and shorter hospital stay.
Robotic Assisted Uretero-Ureteral (Receiver-Donor) Anastomosis
Introduction : Kidney graft complex ureteral strictures and/or symptomatic vesico-ureteral reflux are significant challenges which may lead to anastomose the receivers ureter to the proximal ureter of the graft , or its pelvis. This is classically done through an open surgical access, which adds to the previously invasive process of kidney grafting. The da Vinci robot enables now to perform complex reconstructive laparoscopic procedures, and may hence be used for such reconstructions Purpose : This video illustrates the use of the da Vinci robot in uretero (receiver)-ureteral (donor) anastomotic reconstruction. Methods : Three consecutive patients of an average age of 59 years presented with recurrent ureteral strictures (n=2) or symptomatic uretero-vesical reflux (n=1). Two had received peritoneal dialysis before their kidney transplant. A 4-S or Si da Vinci robot was used, with 2 working trocars triangulating with the laparoscope in a disposition slightly oblique towards the iliac fossa. Results : The 2 first patients were discharged within post-operative day 5 without complications. After a 4 and 5 months follow-up, their kidney graft function has remained within preoperative values. A third patient required conversion to open surgery because of the difficulty to identify the graft ureter. In our institutution, length of hospital stay amounted to 9 days when such reconstructions were performed through an open access.Conclusion : Robot-assisted uretero-ureteral anastomosis is feasible in kidney graft patients, with a distinct minimally invasive advantage. To decrease the difficulty of graft ureter identification, pre-laparoscopic pigtail, per-operative ureteroscopy or laparoscopic ultrasound may prove useful.
Urology Department, Acibadem Maslak Hospital, Istanbul, Turkey
Introduction: Robotic assistance is very useful for excision of complicated and difficult tumors.Purpose: To describe robot assisted excision of a pelvic mass located at left obturator fossa.Material and Methods: A 61 years old patient presented with pain and numbness on the left leg. Computed tomography revealed a 12 cm lymph node located at the left obturator area compressing the iliac vessels. PSA was 3.2 ng/ml. CT guided biopsy of the mass was reported as low grade carcinoma of undefined origin. The result of the prostate biopsy was adenocarcinoma with Gleason score 6 (3+3). Bone scan was negative for metastasis. Robot assisted radical prostatectomy with simultaneous removal of the pelvic mass was planned. The enlarged lymph node was identified just lateral to the left ureter and medial umbilical ligament. The mass was completely freed from the obturator fossa. Remaining lymphatic tissue was also released. An extended lymph node dissection was performed on the right side. After completing the lymph node dissection, radical prostatectomy was performed. The pathology of the mass was reported as neuroendocrine tumor, probably originating from the prostate. The final pathology of the prostate was reported as adenocarcinoma Gleason score 6, with negative surgical margins. There was no lymphatic involvement from prostatic carcinoma. The patient received adjuvant chemotherapy. He is tumor free at 9 months follow-up with undetectable serum PSA.Conclusion: Robotic assistance eases excision of complicated and difficult masses. The technique is safe and feasible.
Urology Department, Acibadem Maslak Hospital, Istanbul, Turkey
Introduction: Cystadenoma is an extremely rare benign tumor of the seminal vesicle. To our knowledge, neither laparoscopic nor robot assisted excision of cystadenoma of seminal vesicle has been reported so far.Purpose: To demonstrate the technique of robot assisted excision of cystadenoma of vesicula seminalis by using 4 arm system.Material and Methods: A 48 years old man presented with diminished ejaculate volume. Transrectal ultrasonography revealed a right seminal vesicle mass 6 cm in diameter. Transrectal ultrasound guided biopsies revealed no malignancy. A double J stent was inserted into the right ureter. Four arm Si system was used for the procedure. Port configuration was similar to robot assisted radical prostatectomy. The peritoneum was incised; right vas deferens was identified, clipped and cut. Then right seminal vesicle was dissected out carefully without using any thermal energy around the lateral and medial aspect. The specimen was taken out via 12 mm assistant port on the right side. Frozen-section analysis revealed the presence of a benign lesion. A drain was placed into the cavity and the peritoneum was sutured.Results: Operative time was 240 min. EBL was 200 ml. Postoperative period was uneventful and the patient was discharged on postoperative day 3. Final histopathological examination revealed cystadenoma of the seminal vesicle.Conclusion: Cystadenoma of the seminal vesicle is very rare. Robot assisted excision is a safe and minimally invasive method compared to open surgery.
Robot-Assisted Laparoscopic Repair of a Vesicovaginal Fistula
We describe the use of robotic assistance to repair a VVF in a patient who sustained a bladder injury during transabdominal simple hysterectomy and review the literature for reports of robotic VVF repair.The patient is a 44 year old female who underwent transabdominal hysterectomy for a history of uterine fibroids. At the time of surgery, a supratrigonal bladder injury was identified, which was closed in two layers via the transabdominal incision. The patient subsequently developed a VVF which failed to close despite 3 months of foley catheter drainage. We present a video illustrating the technique of robot-assisted laparoscopic repair of the VVF.The patient first underwent cystoscopy and vaginoscopy to locate the fistulous tract. The da VinciTM robotic console was side-docked to allow cystoscopy to be performed during the procedure. The procedure was performed via a transperitoneal approach with 4 trocars. The plane between the vagina and bladder was developed, and the fistula was identified with the assistance of the 5-French catheter. The fistulous tract was excised, and the bladder and vagina were closed separately, with omental interposition. The foley catheter was left in place for 3 weeks. At one year follow-up, there is no evidence of recurrent fistula. A PubMed search yielded six cases of robotic VVF in the literature.The improved visualization and magnification provided by robotic assistance can assist in identifying often small fistulous tracts. A combined approach of simultaneous robotic dissection in the pelvis and cystoscopy or vaginoscopy can be useful to locate the fistula.
Nephroureterectomy with Primary Endoscopic Approach of the Intramural Ureter Using Bipolar Plasma Vaporization
Introduction: Nefroureterectomy with perimeatal cystectomy is still the gold standard in the treatment of urothelial upper urinary tract carcinoma (UUTC). Ureteral endoscopic surgery was proposed as a complementary first step in nephroureterectomy in order to obviate the low abdominal incision. Purpose: To establish the value of a novel method of endoscopic distal ureteral management in one-step nephroureterectomy for UUTC: pluck technique using bipolar plasma vaporization.Material and Methods: During the last two years, we performed nephroureterectomy with pluck transurethral detachment of the intramural ureter using the bipolar plasma vaporization in 42 cases of UUTC. The tumor was pyelocaliceal in 34 cases, ureteral in 7 cases and both ureteral and pyelocaliceal in 1 case. The follow-up protocol included cystoscopy with urinary cytology, ultrasonography, intravenous pyelography and CT. The mean follow-up period was 14 months (range 8 to 26 months).Results: All procedures were successfully completed. The complication rate was 4.8%: 2 cases of hematuria, one imposing endoscopic approach and another one treated conservatively. During follow-up, 6 patients presented bladder recurrences, 1 had renal fossa tumors and 1 had secondary lymph-node invasion. The disease-specific mortality rate was 4.8%.Conclusions: The endoscopic approach of the terminal ureter with bipolar plasma vaporization as part of one-step nephroureterectomy is a safe, facile and effective method, with good oncological results.
VS17: Notes/Less 3
Robot-Assisted Laparoendoscopic Single Site (LESS) Pyeloplasty
Introduction and Objectives: Single site surgery has been performed for various applications in urologic surgery and in other surgical fields. We report the use of robotic assistance to perform robot-assisted laparoendoscopic single site (LESS) pyeloplasty through a single periumbilical incision.Methods: The patient is a healthy 20 year old female who was found on computed tomography to have a symptomatic ureteropelvic junction obstruction (UPJO) in the setting of a crossing lower pole accessory artery. The patient elected for robot-assisted LESS pyeloplasty.Results: The patient underwent transperitoneal robot-assisted LESS pyeloplasty via a single periumbilical 2 cm incision utilizing a commercially available single-access device. The crossing artery was identified and dissected free from the renal pelvis. A dismembered pyeloplasty was performed, and a 1 cm segment of the ureteropelvic junction was excised. The anastomosis was performed using a barbed suture, with a running suture line on the posterior wall followed by the anterior wall. A ureteral stent was placed in a retrograde manner. She remains asymptomatic after stent removal and is being monitored with serial postoperative imaging studies.Conclusions: The use of the robotic platform for single-site pyeloplasty can be challenging, but in appropriately-selected patients can be successfully performed. Challenges to this procedure include limited lateral movement of the robotic arms. This challenge was less pronounced during this procedure as pyeloplasty does not require extensive robotic arm excursion. Deliberate, controlled movements of the robotic arms with communication between the console surgeon and bedside assistant can facilitate the success of the procedure.
Laparoendoscopic Single Site (LESS) Upper Urinary Tract Reconstruction with Conventional Straight Laparoscopic Instrument.
Introduction: Intracorporeal suturing under LESS usually required commercialized articulated instruments to maintain adequate instrument triangulation. However, these commercialized LESS devices were not globally available. Thus, developing LESS with existing facilities and conventional laparoscopic instruments is an important issue.Purpose: To present our initial experience of LESS upper urinary tract reconstruction with conventional straight laparoscopic instruments.Material and Methods: LESS upper urinary tract reconstruction was performed in three consecutive patients with upper urinary tract anomalies (1 duplex obstructed upper moiety and 2 UPJO). A home made single port, 30 degree 5-mm laparoscope, and conventional straight laparoscopic instruments were used for all procedures. No additional port was used.Results: All LESS upper urinary tract reconstruction were performed successfully without multiport laparoscopic or open conversion. The mean operative time was 215 minutes. There was no procedure related complication. The cosmetic results were excellent.Conclusions: LESS upper urinary tract reconstruction with conventional straight laparoscopic instruments was safe and effective for upper tract anomalies.
A Novel Approach for Embryonic Natural Orifice Transumbilical Endoscopic Surgery (E-NOTES) for Nephrectomy
Introduction The laparoscope and instruments continuously interfere with each other during embryonic natural orifice transumbilical endoscopic surgery (E-NOTES) nephrectomy. Purpose To report our initial experience with suprapubic-assisted E-NOTES nephrectomy using conventional laparoscopic instruments, and evaluate its feasibility, safety and efficacy.Patients and Methods Thirty three patients were subjected to suprapubic-assisted E-NOTES nephrectomy. The patient was secured on the operating table in lateral decubitus with affected side elevated 70 degree. One 5- and 10-mm (or two 5-mm) trocars were inserted at the umbilical edge. A 10-or 5-mm trocar was inserted into abdominal cavity below the pubic hairline. Our technique for the suprapubic-assisted E-NOTES nephrectomy is similar to that of the standard laparoscopy. Some bigger specimens were removed after the incisions below the pubic hairline were enlarged. Results The 33 procedures were all successfully performed. The median operative time was 106 and 91 minutes, and estimated blood loss was 213 and 115 mL for simple nephrectomy and radical nephrectomy, respectively. The mean follow-up of 5.2 (range 1 to 11) months showed hidden umbilicus scar. The scar below the pubic hairline was not detectable because of the covering of the pubic hairs. Conclusions Suprapubic-assisted E-NOTES nephrectomy appears to be feasible, safe and effective. It would not only lead to improved cosmetic results, but decrease the difficulty of operation.
Suprapubic-Assisted E-Notes Adrenalectomy
Introduction The laparoscope and instruments continuously interfere with each other during embryonic natural orifice transumbilical endoscopic surgery (E-NOTES) adrenalectomy. Purpose To report our initial experience with suprapubic-assisted E-NOTES adrenalectomy using conventional laparoscopic instruments, and evaluate its feasibility, safety and efficacy.Patients and Methods Six patients were subjected to suprapubic-assisted E-NOTES adrenalectomy. The patient was secured on the operating table in lateral decubitus with affected side elevated 70 degree. One 5- and 10-mm (or two 5-mm) trocars were inserted at the umbilical edge. A 10-or 5-mm trocar was inserted into abdominal cavity below the pubic hairline. Our technique for the suprapubic-assisted E-NOTES adrenalectomy is similar to that of the standard laparoscopy. Some bigger specimens were removed after the incisions below the pubic hairline were enlarged. Results The 6 procedures were all successfully performed. The median operative time was 81 minutes, and median estimated blood loss was 61 mL, respectively. The mean follow-up of 5.2 (range 1 to 11) months showed hidden umbilicus scar. The scar below the pubic hairline was not detectable because of the covering of the pubic hairs. Conclusions Suprapubic-assisted E-NOTES adrenalectomy appears to be feasible, safe and effective. It would not only lead to improved cosmetic results, but decrease the difficulty of operation.
Transvaginal Notes-Assisted Laparoscopic Adrenalectomy:First Clinical Experience
Introduction To our knowledge, transvaginal NOTES adrenalectomy was performed only on animals, not on human beings.Purpose To describe the initial clinical experience of transvaginal natural orifice transluminal endoscopic surgery (NOTES)-assisted laparoscopic adrenalectomy (TNLA) and to evaluate its feasibility and efficacy.Materials and Methods Between May and December 2010, 11 consecutive women were subjected to TNLA for adrenal tumors at the authors center. With the patient under general anesthesia, a 5-mm trocar and a 10-mm trocar were inserted in the umbilical edge for conventional operating apparatus, and a 10-mm trocar was inserted in the posterior vaginal fornix for a conventional 308 laparoscope. Dissection was performed according to the method of a standard laparoscopic adrenalectomy. The adrenal gland, its tumor, or both were put into a homemade bag and then removed via the incision of the posterior vaginal fornix after complete resection.Results A total of 11 TNLAs were performed in this series. Only one conversion to open surgery was performed for one patient with Cushing disease, who was subjected to a splenectomy synchronously for an injury of the spleen. Except for this patient, no patients required a blood transfusion. The median operative time was 102 min (range 80-310 min), and the median estimated blood loss was 80 ml (range 30-800 ml). All the patients except the one who had conversion to open surgery were very satisfied with the cosmetic result.Conclusions The findings show TNLA to be a feasible and effective surgical technique that results in excellent cosmesis.
Percutaneous Transvesical Laparoendoscopic Single-Site Surgery (LESS) for Bladder Diverticulum
IntroductionVarious single-incision techniques have been developed to decrease morbidity after laparoscopic port placement and to improve cosmetic results. One widespread single-port procedures is laparoendoscopic single-site surgery (LESS). We present our initial clinical experience of this approach for transvesical bladder diverticulectomy.Purpose To present a series of laparoendoscopic single-site surgeries for transvesical excision of symptomatic bladder diverticula. Materials and MethodsDuring March and April 2011, we operated on three men aged 62 to 76 yr (mean 67 yr) for symptomatic bladder diverticula using a standard lithotomy position and general anesthesia. The TriPort + trocar was inserted directly into the bladder under cystoscopic control through a 1,5-cm long suprapubic incision. The diverticula were dissected and removed from the bladder with a combination of standard laparoscopic and endoscopic instruments introduced through the TriPort + or the urethra. We closed the bladder wall opening with a running absorbable 3/0 V-Loc suture. An 18F Foley catheter was left in place for 4 to 7 days.ResultsThe average operative time was 105 min and the estimated blood loss was 20 ml. Patients were discharged on the third postoperative day with no intra- or post-operative complications. Three-month follow-up confirmed good operative results in all cases. ConclusionsWe consider this technique to be a feasible and safe procedure, and a valuable treatment option for bladder diverticulectomy.
Two-trocar Transumbilical Laparoscopic Surgery for High Ligation Of Spermatic Vein (Report of 32 Cases)
Introduction Laparoscopic varicocelectomy has been proposed as an alternative surgical procedure.Purpose To evaluate the clinical value of two-trocar transumbilical laparoscopic surgery for high ligation of spermatic vein. Materials and Methods Between May 2010 and May 2011, 32 cases with varicocele underwent two-trocar transumbilical laparoscopic high ligation of spermatic vein. Twenty cases were on the left side, 3 cases on the right side and 9 cases on both sides. Under general anesthesia, the patients were placed in the Tredelenburg position with head end lowered by 15 degree. Two 5-mm trocars were introduced into abdominal cavity at the right and left medial margin of umbilicus, respectively. A 5-mm 30 degree laparoscope was inserted from one of the two 5-mm trocars. The spermatic vein was dissociated at 2 to 3 cm above internal inguinal ring, and then ligated without dissection by two 7 silk sutures, which were knotted out of body and pushed into the abdomen cavity. Another side was managed using the same method if double-side varicoceles exist.Results All the procedures were successfully performed and there was no obvious complications occurred. The average operative time was 25 minutes for single side and 37 minutes for double. The average hospital stay was 4 days post-operatively. Follow-up was scheduled from 1 to 12 months; no scrotal swelling and testicular atrophy were observed postoperatively. Conclusions Two-trocar transumbilical laparoscopic high ligation of spermatic vein was not only safe and effective but also with less pain, shorter convalescence and good cosmesis.
Less Varicocelectomy-An Alternative Minimal Invasive Treatment Option
Introduction: Treatment options for varicoceles include open and laparoscopic varicocelectomy performed at various anatomical levels as well as sclerotherapy. Even robotic surgery has been introduced recently as an alternative surgical option for treatment of varicoceles. New techniques are emphasizing low morbidity and best surgical outcome.Purpose: To demonstrate the technique and feasibility of laparoendoscopic single site surgery (LESS) for the treatment of varicocele.Materials and Methods: A 28-year-old male patient complained about increasing pain and scrotal enlargement over the last six months. Clinical examination and color Doppler ultrasound confirmed a varicocele grade II on the left side. LESS varicocelectomy was performed with isolation of the gonadal vein, clipping with Hem-o-lok clips and dissection.Results: Operation time was 45 minutes with a minimal blood loss. The intra- and postoperative course was uneventful and the patient was discharged one day after surgery. He was completely asymptomatic six weeks later.Conclusions: In our experience the LESS procedure for the treatment of varicoceles is a safe and effective technique with comparable outcome to conventional surgery.
Late Breaking
The Correlation between Clinical Outcomes and some Parameters in Patients with Localized Prostate Cancer after High-Intensity Focused Ultrasound Treatment
We evaluated the correlation between clinical outcomes and some parameters in patients with localized prostate cancer after high-intensity focused ultrasound (HIFU) treatment. From 2003, 160 patients followed over 12 months after last HIFU were treated using the Sonablate 500. In follow-up, a prostate biopsy was conducted at 6 months or later, and serum prostate-specific antigen (PSA) was measured every 3 months. Recurrence was judged using ASTRO definition, histological findings, and metastasis. Disease-free survival (DFS) rate was calculated using Kaplan-Meier curves and a log-rank test was used to evaluate differences between these curves. A multivariate Cox proportional hazards regression model was used to estimate the prognostic relevance of age, clinical stage, Gleason score, prostate volume, pretreatment hormonal therapy, PSA at diagnosis, and nadir PSA during follow-up. The median follow-up period was 39 months (range 12–96). No patients received adjuvant therapy before recurrence. Of the 156 patients who underwent prostate biopsy or transurethral resection of the prostate at 6 months or later after HIFU, 11 were positive for cancer cells (7%). The 5-year DFS rate in total was 78% based on these criteria, and 93%, 81% and 64% in the low-, intermediate- and high-risk group, respectively, with a statistically significant difference. In Cox regression analysis, clinical stage (≥ T2), Gleason score (≥ 8) and PSA level at diagnosis (≥ 10) showed a significant association with prognosis, but prostate volume and pretreatment hormonal therapy were insignificant. HIFU is an effective treatment option for low- and intermediate-risk patients with localized prostate cancer.
Author Index
a, J., BR04-03
Abaza, R., MP08-09, MP13-11, MP13-12, MP13-13, MP16-13, MP17-09, MP31-09, VP01-03, VS02-06
Abbaraju, J., MP05-16, MP24-12
Abdalla, A.A., MP13-07, MP26-01, VS04-02, VS04-04, VS04-05, VS04-07, VS16-04
Abdel Hakim, A.M., MP13-07, MP26-01, VS04-02, VS04-04, VS04-05, VS04-07, VS16-04
Abdel Hakim, M.A., MP13-07, MP26-01, VS04-02, VS04-04, VS04-05, VS04-07, VS16-04
Abdulmajed, M., VS10-09
Abdulmajed, M.I., MP09-07, MP22-05
Abe, T., MP31-11, VS05-05
Abel, E.J., MP21-12
Aboumarzouk, O., UP01-017
Aboumarzouk, O.M., UP02-074, UP02-100
Abreu, A., VS02-02, VS14-02
Abreu, A.L., VS14-03
Abreu, A.L.C., MP15-11, MP16-16, MP32-04, VS02-04
Ackerman, A., MP08-14, MP21-09
Adibi, M., BR01-11
Adler, B., VP04-08
Afsar, F., MP27-01
Agarwal, G., MP07-01, MP07-02, MP14-07, MP14-10, MP21-14, MP28-01, MP34-09
Aggoun, A., MP09-03
Ahanian, A., VS15-08
Ahlawat, R.K., VS01-08, VS06-02, VS13-02
Ahlering, T., MP28-02
Ahmad, S., UP01-017, UP02-074, UP02-100, UP02-101, VS11-05, VS11-09
Ahmadnia, H., UP02-006, UP02-007, UP02-014, UP02-073, UP02-093
Ahmed, K., BR01-06, BR01-07, BR01-08
Aikawa, K., MP33-11
Akagashi, K., UP02-058
Akihiro, U., UP02-094, UP02-095
AKIN, Y., MP25-06
AKITA, H., UP01-087, VS03-07
Akpinar, H., MP08-13, MP16-11, MP30-05, VS08-06, VS16-06
ALANSARI, A., MP10-10, MP18-05
Alanzo, D., MP25-11
Albala, D., MP08-15, MP08-16
Albala, D.M., MP14-14
Albanesi, L., MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
albanesi, l.l., MP14-11, MP25-15
alenezi, H., VS10-07
Al-Essawi, T., UP02-062
Alexander, B., BR03-14
Alexandrov, I., VS13-06
Al-Hayek, S., MP18-14, MP18-15, MP18-16
Al Kadhi, O.S., MP05-17, MP19-06, MP29-15
ALKHAFAJI, H., MP18-05
Allaf, M., MP16-09, UP01-016
Allaf, M.E., MP03-03, MP03-12, MP03-16, MP09-05, MP09-06, MP14-01, MP17-02, MP17-08, MP27-09, VP06-10
Allan, R., MP14-04
Allender, C.J., BR01-01
Alloussi, S., MP27-04, MP27-05
Al-Naimi, A., MP10-10
ALNAIMI, A., MP18-05
Alnazari, M., VS10-07
ALOBAIDY, A., MP10-10, MP18-05
Alomar, M., VS10-07
Al-Qahtani, S.M., VP03-11, VP04-13, VP04-14, VP04-16, VP05-05, VS10-06
Altamar, H., MP30-11
Altunrende, F., UP01-019, UP01-112, UP02-127, UP02-128
Alturende, F., MP20-13
Aluru, P., MP34-11
Alvarado, A., UP02-117
Alvi, K., MP05-19
AMANO, T., UP01-111
Ambani, S., MP11-15
Aminsharifi, A., MP23-07, MP27-01
Amjadi, M., UP02-065
Amlani, J., BR02-02, BR02-04, BR02-07, BR02-08
Amón Sesmero, J., MP23-01
amooee, s., MP23-07
Anandaram, P.S., MP09-07, MP22-05, VS10-09
Anderson, D., BR01-06, BR01-07, BR01-08
Anderson, K.M., MP07-01, MP14-09, MP14-10, MP28-01, MP29-02, MP34-05, MP34-06, VS09-05, VS10-03
ANDO, R., UP01-087, VS03-07
Ando, T., MP12-12, UP01-106
Andonian, S., MP24-10
Andreassen, K., MP24-07
Andreassen, K.H., MP14-04
Andreeva, Y.Y., MP15-14
Andreoni, C., MP13-09, MP31-02, MP31-04, MP31-06
Andrikopoulos, O., BR01-02, BR03-01, BR04-06, MP06-13, MP12-08, MP12-09, MP12-11
Anidjar, M., MP24-10
Anjum, F., MP05-16, MP21-08, MP24-12, MP30-03
Antiporda, M., MP19-01
Anwar, M., MP01-15
Aoki, H., VP06-15, VS11-08
Aonuma, K., MP03-10, VP02-06, VS05-08
Aoyagi, T., MP31-11
Appu, S., MP04-16
ARADA, E.I.V., MP07-03, MP07-05, VP05-10
Arai, G., VP06-15, VS11-08
Arai, K., UP01-023
ARAI, Y., MP27-07, UP01-007, UP01-012, VS11-08
ARAKI, K., UP01-052, UP02-025, VS05-04
Araki, M., MP04-07, MP04-09, MP08-11, MP28-16
Arango, O., MP13-01, MP33-09, UP01-080, UP02-002, VS09-08
araño, p., MP22-04
Ardestanizadeh, A., MP06-02
Ardila, B., MP17-16, VS03-04
AREAL, J.J., VS05-07
Arif, F., UP02-080
ARIMA, K., UP01-008, UP02-111
Arnold, D.C., VS06-04, VS08-04
Arnold, II, D.C., MP07-01, MP07-02, MP14-09, MP21-14, MP28-01, MP29-02, MP34-05, MP34-06, VS09-05, VS10-03
Aron, M., MP16-16, VS02-02, VS02-04, VS14-02
Arriaga, J., VS03-02, VS03-03, VS04-06
Arsovska, O., MP05-06
Arvanitakis, T., UP02-105
Asadpour, A., VS06-01
Asakuma, J., UP01-040, UP01-092
Asakura, H., MP03-10, VP02-06, VS05-08
Asano, T., UP01-040, UP01-092
Asanuma, H., UP01-086, VP01-02, VS15-03
Ashizawa, Y., VP06-15
Aslzare, M., UP02-093, VS05-09, VS06-01
Asmad, I., MP01-15
Asplin, J.R., UP02-034
ASSADIQ, K., MP10-10, MP18-05
Assimos, D., MP05-02, MP05-09, MP05-14, MP05-15
Assimos, D.G., MP05-20
Astroza, G., BR04-10, BR04-12, BR04-13, BR04-14
Astroza, G.M., VP04-02, VP06-16
Athanasiadis, G., MP22-03
Atsuta, T., MP07-10
Attisani, F., MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
Atug, F., MP08-13, MP16-11, MP30-05, VS08-06, VS16-06
Au, W., VS04-01
Au, W.H., VP01-06
Aufderklamm, S., MP27-04, MP27-05
Austin, P.F., MP25-12
Autorino, R., MP20-13, MP26-16, MP32-15, UP01-019, UP01-112, UP02-127, UP02-128
Averch, T.D., MP18-14, MP18-15, MP18-16, MP19-11, MP19-13
Awadalla, W., BR01-01
Awsare, N., MP33-10
Azmi, M.D., MP10-10
Azuero, J., MP22-04, VS01-09, VS01-10
AZUMA, H., MP28-11, UP01-069, UP01-090, UP01-099, UP02-107, VP06-01
Azumi, M., MP20-10, UP01-067
B, K., VP06-09
BABA, S., MP03-18, MP06-10, UP01-042, UP01-053, UP01-094, UP01-098, UP02-008, UP02-027, UP02-028, VP05-12
Babbar, P., MP06-06, MP06-07
Baber, J., MP01-14
Bachmann, A., MP04-10, MP04-11, MP04-12, MP04-20, MP07-15, MP25-10, VS17-08
Badani, K., UP02-104
Badani, K.K., MP19-05
Bader, M., VP04-01
Bader, M.J., BR01-03
Bae, J.H., UP01-072, UP01-073
Bae, W.J., UP01-072
Bagley, D.H., MP19-04, VS10-08, VS10-10
Bahn, D., MP15-11, MP32-04
Bahnson, R., VP01-03
Baik, K.D., MP01-12, MP12-17, VP01-15
Bailey, K., VS02-03
Baker, L., MP09-08
Balarie, C., VP04-09
Baldwin, B.D., MP14-10
Baldwin, D.D., MP06-16, MP07-01, MP07-02, MP14-07, MP14-09, MP14-10, MP21-14, MP28-01, MP29-02, MP34-05, MP34-06, MP34-09, VS09-05, VS10-03
Baldwin, G., BR01-10
Baldwin, G.T., MP15-16, VP04-02
Balik, M., MP13-16
Ball, R., MP29-15
Ballesteros, C., MP07-03
Bandi, G., MP22-08, UP01-085
Barber, N.J., MP02-01, MP02-02, MP02-03, MP02-06, MP02-07, MP02-08, MP02-09, MP03-07, MP11-10, MP11-16, MP16-08, MP31-08, VP01-08, VP02-03, VP02-15, VP03-01, VP03-02, VP03-07, VS02-07, VS06-07, VS13-04
Bardan, R., VP04-09
Bariol, S.V., MP04-19, MP05-04, UP02-029
Barret, E., MP03-05, MP08-03, MP08-10, MP15-06, MP15-10
Barwari, K., BR01-12, MP03-02, MP03-04, MP16-05
Basiri, A., MP11-01, MP11-08, VS14-04, VS15-08
Bassorgun, I., MP32-14
Bates, C.S., MP30-16
Batiller, J., MP14-14
Bayer, T., MP04-18
BAYKARA, M., MP25-06, MP32-14
Bayne, A.P., VP06-02
Bazzi, W., MP01-03, MP01-10, MP01-16, VP01-13
Bazzi, W.M., VP01-14
Bdolah-Abram, T., MP10-01
Beardsley, H.E., BR01-04
Beck, C., MP04-04
Behar, M., BR02-12
Bellamy, E., MP14-05, MP29-07, MP29-08, MP34-01, MP34-02
Benamran, D.A., MP08-07
Ben-Chaim, J., MP29-04
Benetti, A., MP19-16, MP23-12, VS10-05
Benjamin, C.J., MP32-06, VP03-09
bensalah, K., UP02-081
Benson, A.D., BR01-15, BR03-02, BR03-08, BR04-11
Benway, B., MP03-09
Benway, B.M., MP03-15, MP24-04, MP24-15, VS02-01, VS08-05
Berendsen, C.L., MP29-09
Berger, A., VS02-02, VS02-04, VS14-02
Berger, A.k., MP16-16
Bergero, M.A., VP04-10
Beri, A., MP18-07, MP18-10
Berkovitz, N., MP10-01
Bernardo, M., VP03-09
Best, C.D., MP05-03
Best, S., MP21-16
Best, S.L., BR01-11, MP03-01, MP07-17, MP26-05
Bhattu, A., VP04-07
Bhayani, S., MP03-09
Bhayani, S.B., MP03-15, MP24-04, MP24-15, VS02-01, VS08-05
Bhojani, N., MP05-12
Bian, S.X., MP25-03, MP26-09, MP26-10
Bianchi, G., BR02-09, MP24-11, VP01-01, VS12-08
Bielsa, O., MP13-01, MP33-09, UP01-080, UP02-002, VS09-08
Bigley, J.D., MP18-15, MP19-13
Billières, J., MP17-04
Billordo Peres, N., VP04-10
Bird, V.G., MP06-16
Bishara, S., MP02-07, MP02-08
Bivalacqua, T.J., MP17-08
Black, P., UP02-107
Blumberg, J.M., VS05-03
Bo, X., MP29-16
Boctor, E., MP09-05, MP09-06
Boellaard, W., MP23-02
Bogoslavskiy, A.V., MP15-14
Bohin, D., VP05-05
Bohris, C., VP04-01
Bolgeri, M., UP02-079
Bolton, D., BR01-09, BR01-10, MP08-06, MP17-07, MP24-03, MP32-07
Bolton, D.M., MP17-05
Bonkat, G., BR03-14, MP04-20, MP04-12, VS17-08
Bonvissuto, G., VS10-05
Bonzo, J.R., UP02-043
Borgna, V., MP27-10, MP27-11
Borin, J., VS15-04
Boris, R.S., MP33-05
Borisenko, G.G., MP15-14, UP02-022, UP02-042, UP02-069
Borman, E.J., MP09-14
Borofsky, M.S., MP31-17, VP02-13
Botoca, M., MP23-02
Botto, H., VP05-05
Bourdoumis, A., MP22-03
Bowen, A., VS08-01
Bowen, J.L., BR01-01
Bratslavsky, G., UP02-112, UP02-113
Breda, A., MP23-02, VP04-14, VP04-16, VS01-05, VS08-03
Brehmer, M., VP04-14, VP04-16
Brinkman, W., MP02-04, MP02-05, MP02-16
Brodak, M., MP13-16
Brooks, A., MP04-19
Brooks, D., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-071, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Brown, T., UP02-101
Bruhn, A., MP30-11
Brunori, S., MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
Bruyere, F., MP28-15
Buchholz, N., MP05-05
Buckner, C., UP02-112
Bucuras, V., MP05-05, VP04-09
Bui, T., MP17-06
Burgess, N., MP29-15
Bylund, J., VS02-08
Byrne, D., VS11-05, VS11-09
Byrne, T.W., MP10-05, MP10-06
Byun, S.-S., MP07-04, VP05-01, VS12-06, VS12-07
Byun, S.S., MP26-11, MP26-12
Cadeddu, J.A., BR01-04, BR01-11, MP03-01, MP06-14, MP07-17, MP21-16, MP26-05
Cadillo, R., MP13-03, MP17-10
Cadillo-Chavez, R., MP13-04, MP26-14, MP26-15, MP28-03
Cahill, D., BR01-06, BR01-07, BR01-08
Cain, C.A., BR02-13
caire, a., UP02-033
Canales, C., MP02-11
Canes, D., VS03-02, VS03-03, VS11-01, VS11-10
Canpolat, M., MP32-14
Cantwell, C.P., MP21-15
Carbone, L., VS05-06
Carera, C.C., VS07-05
Carmona, L.M., MP33-06
Carmona, O., VS03-02, VS03-03, VS04-06, VS11-01, VS11-10, VS13-01
Cartlidge, D., MP02-01, MP02-02, MP02-03, MP02-06, MP02-09, VP03-01, VP03-02, VP03-07
Cashy, J., MP17-11
Castillo, O., VS11-01
Castillo, O.A., MP27-10, MP27-11
Castle, E., VS11-01
Cathala, N., MP08-10
Cathelineau, X., MP03-05, MP08-03, MP08-10, MP15-06, MP15-10
Caviezel, A., MP13-02, MP17-04, VP05-08
Caviezel, A.C., VS07-05
Centrella, D., VS10-05
Cespedes, C., VS01-01, VS05-02, VS07-06, VS07-07, VS09-03, VS16-02
Cezayirli, F., MP31-15, UP02-115
Chabannes, E., UP02-081
Chaimuengraj, S., MP13-14
Chakravarti, A., MP02-01, MP02-02, MP02-06, MP02-07, MP02-08, MP02-09, MP06-08, MP16-08, MP28-09, VP03-01, VP03-02, VP03-07, VP06-12, VP06-14
Chalasani, V., VP05-09
Challacombe, B., BR01-06, BR01-07, BR01-08
Chamberlain, M., MP24-03
Chamberlin, J.D., MP07-01, MP34-09
Chan, J., MP03-05
Chan, S., VS04-01
Chan, S.W.H., MP04-08, VP01-06
Chandrasekar, P., MP22-13, MP32-10
Chang, A., MP17-06, MP28-02, VS05-03
Chang, A.-W., UP02-032
Chang, D., VP03-08
Chang, G., MP01-16
Chang, J., UP02-056
Chang, J.S., MP04-02
Chang, S.-J., VS14-05
Chang, Y.S., MP04-02
Chanpasoppon, P., VS12-05
Chauhan, S., MP17-14, MP17-15, MP17-16, MP28-04, MP28-05, MP28-06, VS03-04, VS03-05, VS13-05
Chaussy, C.G., MP15-01, MP15-02, MP15-05, MP20-02, UP02-102
Chen, B., UP02-001
Chen, C.-C., MP08-02
Chen, C.-H., VS07-04
Chen, C.J., MP28-01, MP34-09
Chen, C.-S., MP08-02
Chen, F.-H., UP02-036
Chen, H.-E., VP02-16
Chen, K.-H., UP02-066
Chen, P.-C., MP34-13
Chen, Q., MP19-02, MP19-17, MP29-10, MP29-11, MP29-14, MP32-02, MP32-08, UP02-003, UP02-015, UP02-016, UP02-030, UP02-031, UP02-067, UP02-075, UP02-077, UP02-078
Chen, Q.H., MP14-03
Chen, S., MP27-06, MP34-12
Chen, S.-S., UP01-025
Chen, S.-Y., UP02-036
Chen, W., MP18-17, MP18-18, MP30-14, MP30-15, MP34-15, UP02-064
Chen, W.-M., MP08-02
Chen, Y.-W., VS14-03
Cheng, C., MP15-12
Cheng, C.-L., MP08-02, MP13-10
CHENG, H., MP20-05, MP28-17
Cheng, M.-C., MP34-13
Cheng, X., BR03-10
Cheng, Y.-H., VP02-16
Chew, B., MP05-06
Chew, B.H., BR04-02, MP29-01, MP30-11
Chia, P.H., BR01-09
Chia, S.-J., VP04-04
Chien, G., BR03-06, BR03-07, MP14-15, MP17-06
Chien, G.W., VS05-03
CHINA, T., MP15-04, MP32-05, MP32-12
Chinn, D., UP02-113
Chiong, E., VP02-09, VP05-07
Chitale, S., MP29-15
Chiu, A.-H., UP01-115
Chiu, A.W., MP06-01, MP12-02, MP16-06, UP01-002, UP01-024, UP01-025, UP01-037, UP01-084, VP02-16
Chiu, K.-Y., MP08-02
Chiu, Y., MP04-08, MP31-17, VP02-13
Chiu, Y.-C., MP12-02
Cho, H.J., UP01-072, UP01-073
Cho, K.S., UP02-123, MP12-07, MP20-08, VS13-07
Cho, S.Y., MP10-14
Choe, G., VP05-01
Choi, B., MP04-10, MP04-11, MP33-06
Choi, D., MP34-14
Choi, H., MP04-02
Choi, H.Y., MP10-15, UP01-063, UP01-064
Choi, H.Y.C., MP01-02
Choi, J.M., MP12-10, MP12-15, MP12-16, MP25-03, MP25-04, MP25-11, MP26-09, MP26-10, VP06-02, VS14-01, VS14-06
Choi, J.W., MP24-16
Choi, J.Y., UP01-020
Choi, W., UP02-106
Choi, Y.S., UP01-072
Chokshi, S., MP32-06
Chong, Y.-L., VP04-04
Choo, G.Y., UP01-033
Choo, M.S., MP03-17
Chou, W.-P., UP02-032
Chou, Y.-H., UP01-115, UP02-032
Chow, J., MP34-07
Chow, W.M., UP02-053, UP02-103
Choyke, P., UP02-112, UP02-113
Choyke, P.L., MP32-06, VP03-09
Chromecki, T.F., MP17-03, UP01-071, UP01-082, UP01-083
Chu, D., MP29-06
Chu, D.I., MP18-08, MP18-09
Chu, L., MP19-11
Chuech, L.S., UP01-108, UP02-066
Chueh, S.J., MP01-09, MP12-06, MP12-13, UP01-109
Chuen, C., MP09-08
Chung, A.S.J., MP04-14, MP04-15, VP05-09
Chung, B.H., MP12-07, UP01-076, UP02-018
Chung, J., VS13-07
Chung, J.H., MP20-01, UP02-123
Chung, K.J., MP14-06
Chung, M.S., UP01-076, UP02-018
Chung, P.H., MP32-06
Chung, S.-D., UP01-108, UP02-066
Chung, S.J., MP12-07
Chung, S.K., UP01-020
Chung, V.Y., VS04-01
ChunLei, X., MP21-01, MP30-04
chunxi, w., MP18-01, MP18-02, MP22-17, MP22-18, MP23-03, MP23-04, MP23-05, MP23-06, MP30-08, UP02-005
Chuo, K.-Y., VP02-16
Ciftcioglu, A., MP32-14
Cisek, L.J., MP25-03, MP25-04, MP25-11, VP06-02, VS14-01, VS14-06
Clayman, R., MP03-09
Clayman, R.V., MP05-07, MP05-08
Clinkscales, K., MP29-01
Cocks, Hadley F., MP15-16, VP04-02
Codreanu, C., VP02-14, VP03-06, VP06-03
Codreanu, C.C., VS03-06, VS11-03
Coelho, R., MP17-14, MP17-15
Coelho, R.F., MP17-16, MP28-04, VS03-04, VS03-05
Cohen, N., MP01-15, MP09-12, MP30-10, MP30-12, UP02-055
Cohen, S., MP01-03, MP01-10, VP01-14
Cohen, S.A., MP01-16, MP13-06
Colangelo, C., VP01-13, VP01-14
Colli, J., BR01-13, BR03-03, BR03-04, MP16-10, UP02-033, VS02-03, VS08-01
Colli, J.L., BR03-05
Collins, E., MP04-11
Conlin, M., BR02-05
Connolly, L., MP33-10
Consigliere, D., VP02-09
Consigliere, D.T., VP01-07
Cooper, A., BR02-12
Copel, l., MP10-01
Coplen, D.E., MP25-12
Corbeil, J., MP21-05
Corcoran, A.T., MP19-11
Cormier, L., MP28-15
Corner, G., UP02-100
Cosentino, M., VS01-09
Costantini, M., MP26-03, MP26-06, VS01-04
Cotter, K., BR03-05
Cozzupoli, P., VS05-06
Crenshaw, T.D., BR02-01
Crowe, A., BR04-02
Culkin, D.J., MP04-06, VS07-03
Cumpanas, A., VP04-09
Curhan, G.C., UP02-034
Daar, D., VP03-09
Daels, F.P., VP04-10
dahlstrand, c., MP04-01, MP04-03
Dalphin, M., MP14-18
Damia, O., VP04-10
Danial, T., MP14-15
Darabi Mahboub, M.R., BR02-03, BR02-11, BR03-09
Dasgupta, P., BR01-06, BR01-07, BR01-08
DasGupta, R., MP24-14
Davenport, D.L., UP02-043
David Nguyen, H.D., VP04-03
Davidson, P., MP14-18
Davila, H., VS11-10
Davis, J.W., VS09-01
Davisson, J.L., MP31-01
De, S., BR01-13
De Andrade, R., VS03-02, VS03-03, VS04-06, VS11-01, VS11-10
Deane, L.A., VS06-04, VS08-04
de Bruin, D.M., BR01-12
DEJIMA, T., UP02-024
Deklaj, T., VP05-16
de la Rosette, J., BR02-06, MP05-05, MP23-01, MP23-02
de la Rosette, J.J., BR01-12, MP03-02, MP03-04
de la Rosette, J.J.M.C.H., MP18-08, MP18-09
Delibeliotis, C., MP22-03
Delware, J., VP03-10
De Marco, F., MP04-18
Denis, R., VP05-02
Denkceken, T., MP32-14
Denstedt, J.D., BR02-06
Derweesh, I.H., MP01-03, MP01-10, MP01-16, VP01-13, VP01-14
Desai, A.C., MP24-04, MP24-15, VS08-05
Desai, M., MP10-13, MP19-12, MP20-15, MP26-02, UP01-078, VP04-07, VP04-15, VS02-02, VS04-06, VS13-01, VS14-02, VS15-01
Desai, M.M., MP16-16, VS02-04
De Sio, M., MP23-01
De Souza, P., BR04-09, UP02-071
De Stefani, S., BR02-09, MP24-11
Devarajan, R., MP18-11, VP04-06
Devaraju, S., MP22-12, MP27-08, UP02-096
Di, J.-M., VP06-04
Diaz Guemes Martin Portugues, I., VS01-06
Dickinson, I., MP24-12, MP30-03
Dickmann, M., VP04-01
Dietel, A., MP12-08, MP12-09
Do, M., MP12-08, MP12-09, MP12-11
DOBASHI, M., UP01-091, UP02-008, UP02-027, VP05-12
Dolat, M.T., MP20-14
Domen, T., UP02-068
Donderis, R., UP02-117
Donovan, J., MP21-04, VP03-10
Dorsey, Jr., P.J., VS02-03
Douaihy, N., MP08-07
Doumas, K., MP04-17
Dretler, S.P., MP05-13, MP05-19
Drummond, M., MP04-19
Dunn, M., MP05-03
Durand, M., MP08-04, MP08-08, MP32-13, UP01-070, UP01-079, UP01-081
Duryea, A.P., BR02-13
Duty, B., BR02-05, MP23-09, MP23-17, VP01-01, VS10-01, VS12-08, VS15-06
Duvdevani, M., MP09-17
Duvdevani, M., BR03-13
Dy, J., MP07-03
Eapen, R., MP04-16
Eaton, S.H., MP09-04, MP17-11
Ebara, S., MP29-12
Ebinger Mundorff, N., MP04-12
Ebinger-Mundorff, N., BR03-14
Eden, C.G., MP02-07, MP02-08
Edirisinghe, K., MP02-17
EGAWA, M., UP01-088
Eimer, C., MP32-17, MP32-18
Eisenberg, M., VS13-01
Eismma, R., MP02-13
El-Douaihy, Y., MP08-08
Elfar, M., MP02-17
El Feel., A.S., MP13-07, VS04-02, VS04-04, VS04-05, VS04-07
El-Hakim, A., VP05-02
Elhilali, M., MP24-10
El-Khalid, S., MP18-06
Elkoushy, M., MP24-10
El-Mokadem, I., MP02-13, MP09-08, VS11-09
Elspeth, M., MP11-04
Elwood, C.N., BR04-02
Emara, A.M., MP02-01, MP02-02, MP02-03, MP02-06, MP02-07, MP02-08, MP02-09, MP03-07, MP11-10, MP11-16, MP16-08, MP31-08, VP01-08, VP02-03, VP02-15, VP03-01, VP03-02, VP03-07, VP06-14, VS02-07, VS06-07, VS13-04
Emerson, D., MP21-05
Emtage, J.B., MP02-07, MP02-08
Ensannajad, A.H., UP02-065
Epishov, V., BR04-07
Ercolani, M., MP08-03
Erdeljan, P., MP06-16
ERDOGRU, T., MP25-06
Eret, V., MP11-13
Ergun, S., VP06-05
errando, c., MP22-04
Erturk, E., VP02-02, VS03-08
Escobar Jaramillo, F., VS01-01, VS05-02, VS07-06, VS07-07, VS09-03, VS16-02
Esen, T., MP31-15, UP02-115
Esquena, S., VS08-03
Estrade, V., UP02-081
Esuvarnathan, K., VP05-07
Eswara, J.R., MP05-11, MP21-15
Etafy, M., MP11-04, MP21-13, MP32-16, VP03-03
Etafy, M.H., MP05-07, MP05-08
etemadian, m., MP25-08
Eto, M., MP31-12, UP01-027, UP01-100
Eun (DE), D., MP13-04, MP26-14, MP26-15, MP28-03
Eun, D.D., MP13-03, MP17-10
Faber, D.J., BR01-12
Faddegon, S., BR01-04, MP03-01, MP06-14
Faerber, G.J., BR02-13, MP19-10
Fallah, M.A., VS14-04
Fan, Z., MP01-07, MP20-06, MP28-10
Fang, C.-Y., UP02-036
Fang, P., UP02-001
Fargusson, J.E., MP14-09, MP29-02, MP34-05, MP34-06, VS10-03
Fargusson, M.A., MP14-09, MP29-02, MP34-05, MP34-06
Farshi, A.R., UP02-065
Farzin, M., VS06-01
Fateri, F., VP05-08
Fatikhov, R., BR04-07
Favaretto, R., MP15-06
Fei, Y., MP23-11
Feizzadeh Kerigh, B., MP34-10
Feng, T., MP03-16, MP17-02
Feng, Z., MP14-12
fengming, j., MP18-01, MP23-03
Ferda, J., MP11-13
Fernandez, R., BR01-04
Fernando, H., MP18-11, VP04-06
Ferrandino, M., MP08-15, MP08-16
Ferrandino, M.N., BR04-10, BR04-12, BR04-13, BR04-14, MP15-16, MP18-08, MP18-09, MP29-06, VP04-02, VP06-16, VS10-02, VS13-03
Ferrari, N., BR02-09
Ferriero, M., MP15-09, MP26-03, MP26-06, MP32-11, VP03-15, VS01-02, VS01-03, VS01-04
Figenshau, R., MP03-09
Figenshau, R.S., MP03-15, MP06-16, MP24-04, MP24-15, MP25-12, VS02-01, VS08-05
Finch, W., MP09-11, MP19-03, MP29-15
Finch, W.J., MP19-06
Finch, W.J.G., MP05-17
Fischer, C., MP14-14
Fishman, E.K., VP06-10
Florencio, L., MP07-03
Foell, K., MP23-10, MP24-05, MP24-09
Forastiere, E., MP26-06, VS01-04
Forde, A.D., MP02-08, VP06-14
Forootan, M., MP23-07
Foster, C., MP11-04
Frances, A., MP13-01, UP01-080, UP02-002, VS09-08
Frank, E.L., MP30-16
Franke, M., MP14-04, MP24-07
frånlund, m., MP04-01, MP04-03
FU, K.K., MP23-13
Fuchs, E., BR02-05
Fuji, K., UP02-087
Fujii, T., UP02-108
Fujii, Y., VP05-04
Fujime, M., VP06-15
FUJISAWA, M., MP28-13, UP01-039, UP01-043, UP01-097, UP01-102, UP02-009, UP02-012, VP02-11, VP05-06
Fujisue, H., MP28-11
FUJISUE, Y., UP01-090, UP01-099, UP01-110, UP02-107
Fujita, M., UP02-108
FUJITA, T., MP03-18, MP06-10, UP01-042, UP02-008, UP02-027, UP02-028, UP02-109, VP05-12
Fukagai, T., UP02-087
FUKAMI, N., MP11-07, MP17-13, MP26-08, UP01-066
Fukata, T., MP28-18
FUKAYA, K., MP17-13, MP26-08, UP01-066
FUKUDA, M., UP01-088
Fukuda, N., VS14-03
Fukuhara, H., MP28-18
Fukuhara, T., VP06-11
FUKUI, H., MP16-07, UP01-105
FUKUI, K., UP01-101, VP03-04
Fukumoto, K., UP02-108
Fukuta, F., UP01-049
Fukuzawa, N., MP03-11
Fuller, A., BR02-06
Fumado, L., MP13-01, MP33-09, UP01-080, UP02-002
Furukawa, J., MP28-13, UP01-102, VP02-11, VP05-06
FURUSE, H., UP01-005
FUSE, H., UP01-114
Fussey, J., MP18-11, VP04-06
Gaber, A.O., MP12-16
Gabriel, J.C., MP15-16
Gabrielsen, J.S., MP30-16
Gafton, G.I., MP15-12
Gaitonde, K., MP21-04, VP03-10
Gakis, G., MP27-04, MP27-05
Galiano, M., MP03-05, MP08-10, MP15-06, MP15-10
Galli, E., BR02-09
Gallo Rios, J.F., VS01-01, VS05-02, VS07-06, VS07-07, VS09-03, VS16-02
Galloway, R.L., MP09-10
Gallucci, M., MP15-09, MP26-03, MP26-06, MP32-11, VP03-15, VS01-02, VS01-03, VS01-04
Ganpule, A., MP10-13, MP26-02, UP01-078, VP04-07, VS15-01
Gao, X., MP22-10, UP02-070, VP06-04
Garcia Marchiñena, P.A., VP04-10
Garston, H., MP18-11, VP04-06
Garza, R., VS03-03
Gasser, T., MP04-12, MP04-20, MP07-15
Gasser, T.C., BR03-14
Gates, S.P., MP32-06
Gauhar, V., VP01-07, VP02-09, VP05-07
Gautam, G., VP05-16
Gaviria, A., VS01-01, VS05-02, VS07-06, VS07-07, VS09-03, VS16-02
Gaya, J.M., VS08-03, VS09-06
Gayed, B., MP10-12
Gayed, B.A., MP25-05
Geavlete, B., MP18-13, MP22-09, MP22-11, MP22-15, MP30-02, VP03-12, VP03-13, VS16-09
Geavlete, P., MP18-13, MP22-09, MP22-11, MP22-15, MP23-01, MP30-02, VP03-12, VP03-13, VS16-09
gentile, b.c., MP14-11, MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
GENTILE, B.C.B.C., MP25-15
Georgas, E., MP32-18
Georgescu, D., MP18-13, MP22-09, MP22-11, MP22-15, VP03-12, VP03-13, VS16-09
Georgiadis, M., VP04-09
Georgiopoulos, I., BR01-14, BR04-06, MP06-13, MP12-09
Germinale, F., MP21-02, MP21-03, VP06-08
Geronatsiou, K., BR01-02
Gerullis, H., MP32-17, MP32-18
Gervais, D.A., MP21-15
Ghazi, A., MP21-07, MP28-14, VP02-01, VP02-02, VS03-08, VS16-03
Gherman, V., VP02-14, VP06-03
Gherman, V.G., VS03-06, VS11-03
Ghiculete, D., MP23-10, MP24-05, MP24-09
Gholipour, M., BR02-14
Ghulam, N., MP09-08, VS11-05
Giedelman, C., VS03-02, VS03-03, VS04-06, VS11-01, VS11-10, VS13-01
Gil Diez de Medina, S., VP03-11
Gilad, R., MP18-07
Gill, I., VS02-02, VS04-06, VS13-01, VS14-02
Gill, I.S., MP15-11, MP16-16, MP32-04, VS02-04, VS14-03
Gilling, P.J., MP14-17, MP14-18
Ginzburg, N., VS15-07
Giulianelli, R., MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
giulianelli, r.r., MP14-11, MP25-15
Giusti, G., MP19-16, MP23-12, VS10-05
Gkialas, I., MP04-17
Gleeson, J.W., MP18-12
Glisson, C.L., MP09-10
Gnade, B.E., BR01-04
Gnessin, E., MP05-12, MP30-13
Gofrit, O.N., BR03-13, MP09-17
Goh, A., MP26-10
Goh, A.C., MP26-09
Gohel, M.-D.I., BR04-01
Golan, R., MP13-04
Golash, A., MP02-07, MP06-08, MP28-09
Goldfarb, D.S., UP02-034
Goldsmith, Z.G., MP29-06, VP04-02, VP06-16
Golijanin, D., VP02-02
Gomella, L.G., MP17-12
Gomez-Sancha, F., MP04-10, MP04-11, MP33-06
Gonzalez, A., MP04-13, MP34-16
Gonzalez, M.S., VP04-10
GONZALEZ-SATUE, C., VS05-07
Goodman, C., UP02-101
Gooran, S., MP11-01
Goshtasebi, B., MP27-01
Goto, T., VP02-04, VP04-05
Gotoh, M., UP02-109, VP06-01
Gottlieb, P., MP10-01
Gowardhan, B., MP34-11
Goya, N., VP02-10
Gozen, A.S., MP16-05
Graham, D., MP25-07
Graham, J., MP09-12
Graham, S., UP02-082
Graham, S.J., UP02-041
Grange, P., MP09-03
Gratzke, C., BR01-03
Gravas, S., MP04-17
Graversen, J., MP05-08, UP02-104
Graversen, J.A., MP19-05
Graves, R.V., MP26-15
Graziotti, P., MP19-16, MP23-12, VS10-05
Greenstein, A., MP29-04
Grob, B.M., VP01-04, VS09-07
Grossman, L., BR01-13, BR03-04, MP16-10
Grover, S., MP08-04, MP08-08, MP32-13, UP01-070, UP01-074, UP01-079, UP01-081
Gu, X., MP04-07, MP04-09, MP08-11, MP28-16
Guaglianone, S., MP15-09, MP26-03, MP26-06, MP32-11, VP03-15, VS01-02, VS01-03, VS01-04
Guarella, V., VS10-05
Guilford, P., MP14-18
Guillotreau, J., MP20-13, MP32-15, UP01-112, UP02-127, UP02-128
Guliev, B.G., MP06-09, MP06-11, MP29-05
Guntaka, A., MP22-12, MP27-08, UP02-096
GUNTEKIN, E., MP25-06
Guo, K., UP02-001
Gupta, M., MP19-05, UP02-034
Gupta, N.P., MP18-08
Gurbuz, C., MP07-17
Gurney, H., BR04-09, UP02-071
Guruli, G., VP01-04
gutierrez, c., MP22-04
Gutierrez, J., MP04-13, MP23-01
Gutierrrez, J., MP34-16
Gyomber, D., MP08-06, MP17-05, MP17-07, MP24-03
H, M., VP06-09
Ha, U.-S., UP02-122, MP20-01
Haber, G.-P., MP20-13, MP32-15, UP01-112, UP02-127, UP02-128
Habuchi, T., MP12-14
Haefner, T., MP12-08, MP12-09
Haga, K., UP02-058
Haghighi, R., MP25-08, MP25-14
Haghpanah, R., MP27-01
Haghpanah, S., MP27-01
Hagiwara, M., UP01-021, VP01-02, VS15-03
HAGIWARA, N., UP01-010
Hagjpanah, A., MP23-07
Hailun, Z., MP23-11
Haitani, T., VS09-04, VS12-01
Haitov, Z., BR02-12
Hall, J., MP06-18
Hall, T.L., BR02-13, BR03-10, MP15-13, MP15-15, MP22-06
Haluk, S., BR04-04
Ham, W., UP01-034
Ham, W.S., MP12-07, MP20-08, UP02-123, VS13-07
HAMADA, S., UP01-040, UP01-092
HAMAKAWA, T., UP01-103, VP05-04
HAMANO, A., UP02-097
Hamilton, B., MP30-16
Hampton, L.J., MP20-14, VP01-04, VP01-11, VS04-03, VS09-07
Han, D.H., MP01-02, MP10-15, MP14-06, UP01-063, UP01-064
Han, D.S., MP14-10, UP02-019
Han, J.H., MP20-08
Han, M., MP17-08, VP03-08
Hanashima, F., MP03-10, VP02-06, VS05-08
Handa, S.E., MP05-12
Hanna, M.A., MP10-07, MP24-13, MP24-14
Hanzawa, T., UP02-058
HARA, H., MP01-05, MP33-13, UP01-006, UP02-044, UP02-089
HARA, I., UP01-089, UP02-050, VP04-11
HARA, K., MP16-07, UP01-105
Harabayashi, T., MP20-10, MP31-11, UP01-067, VS05-05
Harada, K., MP28-13
HARAGUCHI, T., UP01-097, UP01-102, UP02-009, UP02-012, VP05-06
HARIU, K., UP02-023, UP02-121
Harris, J.J., MP11-06
Hart, J., MP14-14
Haseebuddin, M., MP03-09
Hasegawa, M., UP01-021, UP01-075, UP01-077, UP01-086, UP01-113
HASEGAWA, Y., UP01-008
Haseke, N., BR01-03
Hashimoto, K., UP01-022
HASHIMOTO, Y., MP31-03, MP31-05, UP01-059
HASHIZUME, M., UP01-101
Hastings, R., MP28-03
HATAKEYAMA, S., UP01-046, UP02-011
Hatano, T., MP32-09
Hattori, M., MP02-12
Hattori, R., UP01-061, UP02-109, VP06-01
HATTORI, S., MP27-14, VS15-03
Hauser, J., MP13-02, VP05-08
Hauser, J.M., VS16-05
Hawaux, E.L., MP15-03
HAYAKAWA, K., MP11-07, UP01-094
HAYASHI, K., MP33-13, UP01-006, UP02-044, UP02-052, UP02-089
HAYASHI, M., MP15-08, UP02-024, UP02-090
HAYASHI, T., MP01-13, MP02-12, MP07-06, MP13-15, MP25-16, UP01-009, UP01-041, UP01-054
HAYASHI, Y., MP25-09, UP01-107, UP02-098, VP05-04
HAYASHIDA, Y., UP01-013, UP01-058, UP02-119
HAYASI, T., MP28-12
HAYATA, S., UP02-049
He, C., MP11-15
Healy, K.A., MP17-12, MP19-04, VS10-08, VS10-10
Hedican, S.P., MP09-15, MP21-12
Hejj, R., UP02-053, UP02-103
Heldt, J.P., MP07-01, MP07-02, MP14-07, MP14-09, MP14-10, MP21-14, MP28-01, MP29-02, MP34-05, MP34-06, MP34-09, VS10-03
Heller, L., VS14-01
Hemal, A., VP02-09, VP05-07
Hemal, A.K., MP05-20, MP06-03, MP06-06, MP06-07, MP11-09, MP16-14, MP16-15, MP31-13
Hendrikx, A., BR02-06
Hendrikx, A.J.M., MP02-04, MP02-05, MP02-16
Heng, C.T., VP01-05
Hengjun, X., MP23-11
Henry, N., VP03-11, VP04-13
Herrell, Duke S., MP09-10
Herrera, E., VS03-02
Herve, J.-M., VP05-05
Hes, O., MP11-13
Hess, B., MP05-05
Heston, W.D., MP32-15
Hew, M.N., MP03-04
HIEDA, K., MP01-13, MP02-12, MP07-06, MP13-15
HIGASHIHARA, E., MP01-05, MP33-13, UP01-006, UP02-044, UP02-052, UP02-089
HIKOSAKA, K., MP17-13, UP01-066
Hill, M.E., MP07-02
Hillyer, S., MP20-13, MP26-16, MP32-15, UP01-112, UP02-127, UP02-128
Hinata, N., MP06-15, VS03-01
Hindley, R., MP02-01, MP11-10, MP11-16, MP31-08, VP03-01
Hindley, R.G., VP02-03, VP02-15, VS02-07, VS06-07
Hinshaw, J.L., MP09-15
Hiradfar, M., UP02-014
HIRAMA, H., UP01-013, UP01-058, UP02-119
HIRANO, S., UP01-042, UP01-098
HIRANO, Y., MP24-06, MP26-08
HIRAYAMA, T., UP02-008, UP02-027, VP05-12
Hiremath, M., MP22-12, MP27-08, UP02-096
Hisasue, S., MP33-03
HISASUE, S.-I., MP15-04, MP32-12
HIURA, Y., MP28-12
Ho, H., MP15-12
Ho, H.-C., MP08-02
HO, K., MP23-13
Ho, L., VS04-01
Ho, L.Y., VP01-06
Ho, R., VS04-01
Ho Yee, T., VP05-07
Hocaoglu, Y., VP04-01
Hoenig, D., MP05-01, VS15-07
Hoenig, D.M., VP04-08
Hogea, M., VP02-14, VP06-03
Hogea, M.M., VS03-06, VS11-03
Hoh, C., MP21-05
Hollenbeck, B., MP11-15
Hollenbeck, B.K., MP06-05, MP19-10, MP22-01, MP22-02
Hollingsworth, J., MP11-15
Hollingsworth, J.M., BR02-13, MP06-05, MP19-10, MP22-01, MP22-02
Holmes, R., MP05-02, MP05-09, MP05-14, MP05-15
Holm-Nielsen, A., MP14-04
Holub, L., MP13-16
Homma, Y., MP24-06
Honda, J., UP01-027, UP01-100
Honda, M., MP06-15, VS03-01
HONDA, T., UP02-121
Honeck, P., MP23-14, MP23-18, MP33-08, VP03-14, VP06-06
Honey, John D'A R., MP23-10, MP24-09
Honey, R.J.D'A, MP24-05
Hong, S., MP08-12, MP28-07
Hong, S.H., UP01-072, UP01-073
Hong, S.K., MP07-04, MP26-11, MP26-12, VP05-01, VS12-06, VS12-07
HONGO, F., MP07-16, MP16-03, UP01-093
Hongoh, S., MP25-02
Honma, I., UP02-058
Hora, M., MP11-13
Horgan, S., VP01-13, VP01-14
HORI, J., UP01-045
HORI, Y., UP01-008
HORIE, S., MP15-04, MP32-12, MP33-03
Horiguchi, A., UP01-040, UP01-092
Horiguchi, H., MP24-06
Horikawa, Y., MP12-14
Horinaga, M., MP03-10, VP02-06, VS05-08
Horiuchi, K., MP33-01
Hoshina, A., UP01-056
HOSHINAGA, K., MP11-07, MP17-13, MP26-08, UP01-066
Hosking, D., UP02-062
Hoskins, J., VS02-08
Hosseini, M.M., MP23-07
Hossny, M.M., MP10-07, MP24-13, MP24-14
Hou, C.Y., MP14-02, MP14-03, MP18-03, MP18-04
Hou, Y., MP22-16, MP27-06, MP34-12
HoYee, T., VP01-07
Hoznek, A., MP23-01
Hruby, S., MP33-07
Hsieh, K.-L., UP01-002
Hsieh, Y.-C., UP02-036
Hsu, C.-W., VS07-04
Hsueh, T.Y., MP12-02, UP01-025
Hu, H.J., MP11-14, MP23-08
Hu, J., MP22-16, MP27-06
Huan, S.K., MP06-01, MP16-06, UP01-002, UP01-024, UP01-037, UP01-084
Huang, C.-H., UP01-115
Huang, C.-p., MP29-13
Huang, C.-Y., UP01-108
Huang, E., MP16-16
Huang, G.O., VS09-05, VS10-03
Huang, M., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-071, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Huang, S.S., MP32-15
Huang, W.-T., VP06-04
Hubert, K., MP25-07
Humphreys, M.R., MP30-11
Hung, A., VS02-02, VS14-02
Hung, A.J., MP15-11, MP32-04
Hung, E., VS02-04, VS14-02
Hung, S.-F., UP02-066
Hur, J., UP02-021, UP02-040
Hurtes, X., MP28-15
Huruse, H., UP02-088
Husek, P., MP13-16
Huyhn, V.B., VP03-03
Huynh, V.B., MP02-18
Hwang, E., UP02-019
Hwang, I., UP01-003
Hwang, I.S., MP05-10
Hwang, J., MP22-08, UP01-085
Hwang, T.I.S., VP02-16
Hwang, T.-K., UP01-073
Hwnag, I.S., MP24-02
Hyams, E.S., MP03-12, MP03-16, MP09-09, MP14-01, MP14-12, MP16-09, MP17-02, MP17-08, MP27-09, UP01-016, UP02-117, VP06-10
IBARZ, L., VS05-07
IBUKI, N., UP01-069, UP01-090
ICHIKAWA, T., MP27-12, MP32-01, UP02-049, VS05-04
ICHIMATSU, K., UP01-088
ICHIYANAGI, O., UP01-047, UP02-059
IDE, H., MP15-04, MP32-12
Igali, L., MP29-15
Igarashi, M., UP01-049
IGARASHI, T., BR01-05, MP32-01, MP33-01, VS05-04
Iguchi, R., UP01-044
Iguchi, T., UP01-060, UP02-072
Ihara, H., UP01-104
Ihara, T., UP01-015
Iida, T., VP01-09
IIZUKA, J., MP31-03, MP31-05, UP01-055, UP01-062
IKEDA, H., UP02-024
Ikeda, K., MP02-12
IKEDA, M., MP06-10
IKEZAWA, E., MP31-03, MP31-05, UP01-059, UP01-062
IKOMA, S., UP01-057, UP02-046
IMAI, Y., UP01-048
IMAMOTO, T., MP27-12, VS05-04
Imanee, M.M., UP02-014, UP02-073
IMAO, T., UP01-111
IMURA, M., UP02-098
INAGAKI, T., UP01-010, UP01-089, UP02-050, VP04-11
INAHARA, M., UP01-052, UP02-025, VS05-04
Inai, T., UP02-037
Inamoto, K., VP06-01
INAMOTO, T., MP28-11, UP01-069, UP01-090, UP01-099, UP02-107
Inman, B.A., MP29-06
Inokuchi, J., MP31-12, UP02-076
INOUE, H., MP27-13, MP27-16, UP01-014
INOUE, K., MP28-18, UP02-118
INOUE, M., MP32-05, MP32-12
Inoue, R., UP01-049
INOUE, S., MP01-13, MP02-12, MP06-15, MP07-06, MP13-15, MP25-16, UP01-061, UP02-017, UP02-051, UP02-083, UP02-094, UP02-095, VS03-01
INOUE, T., MP12-12, MP12-14, UP01-106
Introini, C., MP21-02, MP21-03, VP06-08
INUI, H., MP28-12
INUI, M., UP01-013, UP01-058, UP02-119
Inuzuka, H., UP01-015
Iqbal, M., MP18-08, MP18-09, VP04-02, VP06-16
IRIE, A., UP01-091
Irimie, A.A., VS03-06, VS11-03, VS14-07
Irving, S., MP29-15
Irwin, B., VS04-06
Isac, W., MP32-15, UP01-112, UP02-127, UP02-128, VS10-04
Isac, W.E., MP20-13, MP26-16
Ischia, J., BR01-10
Iselin, C., MP13-02, VP05-08
Iselin, C.E., MP08-07, MP17-04, VS16-05
Iselin, C.I., VS07-05
Isgro, G., BR02-09
Isgro', G., VP01-01, VS12-08
Ishida, H., MP11-02, UP01-029, UP01-030, UP01-031, UP01-032
ISHIDA, S., UP01-061, UP02-017, UP02-051, UP02-083
ISHIDOYA, S., MP27-07, UP01-007
ISHII, D., MP03-18, UP01-042
Ishii, J., UP01-091
Ishii, K., UP01-060
Ishii, T., BR01-05, MP33-01, UP01-009, UP01-041
ISHIKAWA, K., MP17-13, MP26-08, UP01-066, UP02-024
ISHIKAWA, R., UP02-027, VP05-12
ISHIMURA, H., UP01-046, UP02-011
ISHIMURA, T., UP01-039, UP01-043, UP01-097, UP01-102, VP02-11, VP05-06
ISHISE, H., MP17-13, MP26-08, UP01-066
ISHITO, N., UP02-118
Ishiura, Y., UP02-035
Ishiyama, H., UP01-094
ISHIZUKA, O., MP27-13, MP27-16, UP01-014
ISIKAWA, K., MP11-07
ISOTANI, S., MP15-04, MP32-12
Isoyama, T., MP06-15, VS03-01
Issa, W.M., MP15-03
Isuru, J., VS14-03
ITAMI, Y., UP01-054
ITAYA, N., MP01-05, MP33-13, UP01-006, UP02-044, UP02-052, UP02-089
ITO, A., MP26-04, MP27-07, UP01-007
ITO, F., MP25-17, VP02-10
Ito, H., UP02-045, UP02-048, UP02-092
ITO, K., UP01-040, UP01-092
Ito, N., UP01-044, UP02-084
Ito, T., UP01-005
Ito, Y., VS15-03
Itoh, N., UP01-022, VP02-08
ITOU, H., UP02-086
Itou, N., UP01-027
Ives, K., BR03-10
Iwabuchi, K., MP07-11
Iwami, D., MP03-11
Iwamoto, H., MP06-15, VP04-05, VS03-01
IWAMURA, M., MP03-18, MP06-10, MP26-04, UP01-042, UP01-053, UP01-094, UP01-098, UP02-008, UP02-027, UP02-028, VP05-12
IWATA, T., UP01-045, UP01-093
Iwicki, L., BR02-01
IZUKA, J., UP01-059
Izumi, K., MP14-13, UP02-114
IZUMI, T., UP02-059
J, F., VP06-09
J, K., VP06-09
Jack, G., MP08-06, MP17-05, MP32-07
Jack, G.S., MP17-07, MP24-03
Jackman, S.V., MP18-14, MP18-15, MP18-16, MP19-13
Jacobs, B.L., MP06-05, MP19-10, MP22-01, MP22-02
Jacobsohn, K.M., MP16-12, MP31-10
Jagtap, J., MP19-12
Jaime, L., MP11-04
Jain, S., MP08-14, MP16-01, MP16-02, MP16-17, MP28-08, VS16-08, VS17-01
James, P., MP02-01, MP02-02, MP02-03, MP02-06, MP02-09, VP03-01, VP03-02, VP03-07, VP06-14
Janetschek, G., MP05-05, MP33-07
Jang, S.H., UP02-054
Jansen, J.P., MP10-05, MP10-06
Januzis, N., BR04-12, VP06-16
Jayaratna, I., VS02-02, VS02-04
Jecu, M., MP22-09, MP22-11, MP22-15, VP03-13
Jellison, F.C., VS09-05
Jeon, S.S., MP01-02, MP10-15, MP14-06, UP01-063, UP01-064
Jeon, Y., UP01-065
Jeong, B.C., MP01-02, MP14-06, UP01-064
Jeong, C.W., MP07-04, MP26-11, MP26-12, VP05-01, VS12-06, VS12-07
Jeong, H., MP10-14
Jeong, I.G., BR03-11, BR03-12
Jeong, S.J., MP07-04, VP05-01, VS12-06, VS12-07
Jeschke, S., MP33-07
Jessen, J.P., MP23-14, MP23-18, MP33-08, VP03-14, VP06-06
Jiang, B., VS17-05
Jiang, M.-F., MP11-14, MP14-03, UP01-038, UP02-003, UP02-030, UP02-031, UP02-067, UP02-075, UP02-077, UP02-078
Jiang, M., MP14-02
Jiang, M.F., MP04-05, MP18-03, MP18-04, MP23-08, MP30-07
JIE, S., MP20-05, MP28-17
Jiefu, H., MP23-11
jin, b., MP01-04
Jinzaki, M., UP01-021
Jo, M.-K., MP29-03
Jo, S.S., VS01-07
JO, Y., UP02-108
Jochen, N., BR03-01
John, M., MP08-08
Johnsen, N., BR01-13, BR03-04
Johnson, P., MP34-11
Johnson, P.T., VP06-10
Johnston, R., MP09-11, MP19-03, MP19-06
Johnston, T., MP02-15
Jones, J.S., MP01-09, MP12-06, MP12-13
Jones, L., MP21-06
Jones, R., VS10-09
Jones, V.W., MP09-07, VS10-09
Joseph, J., MP21-07, MP28-14, VP02-02, VS03-08, VS16-03
Joshi, H., MP33-10, UP02-080
Joshi, H.B., BR01-01
Joshi, P., VP05-15
Joshi, V., BR02-02, BR02-04, BR02-07, BR02-08, BR04-03
Jou, Y.-C., MP34-13, UP02-036
Ju, Y.M., MP26-12
Juan, Y.-S., UP02-032
Juang, G.-D., VP02-16
JUN, P., MP20-05, MP28-17
Jung, B.C., MP10-15, UP01-063
Jung, H., MP17-06, UP02-056, VS05-03
Jung, H.U., MP34-04
Jung, J.H., MP19-08
Jung, J.Y., MP05-10
Jung, S.I., MP24-02
Jung, S.-I., UP01-003
JUNMING, Z., MP20-05, MP28-17
Jurado Vallejo, D., VP04-10
Kabakci, A.S., MP19-14
KABAKCI, S., VP04-12
KAGA, K., UP01-052, UP02-025, VS05-04
Kai, F., UP01-005
Kai, H., UP02-088
KAIHO, Y., MP27-07, UP01-007
Kajioka, S., VP05-13
Kajita, Y., VS09-04, VS12-01
KAJIWARA, M., MP01-13, MP02-12, MP07-06, MP13-15, MP25-16, UP02-094, UP02-095
KAKEHI, Y., UP01-013, UP01-058, UP02-119
KAKIMOTO, K., UP01-012
KAKINOKI, H., UP01-057, UP02-046
KAKIZAKI, H., UP01-045
Kalisvaart, J., MP05-07, MP05-08
Kallidonis, P., BR01-02, BR01-14, BR03-01, BR04-06, MP06-13, MP12-08, MP12-09, MP12-11
Kalogeropoulos, T., MP22-03
Kalogeropoulou, C., BR01-14
Kalsi, V., MP34-02
Kalyanaraman, B., MP21-04, VP03-10
Kamada, Y., UP02-072
Kamba, T., MP09-13, UP01-035, UP02-120
Kambara, Y., MP33-01
Kameh, D., MP28-04, MP28-05, MP28-06, VS03-05
KAMEOKA, H., MP33-11
KAMIGAITO, T., MP27-13
Kamiggaito, T., MP27-16
KAMIMURA, N., UP01-046, UP02-011
Kamimura, T., VP02-04
KAMIMURA, Y., UP01-088
KAMINAGA, T., MP15-04, MP32-12
KAMISAWA, H., UP02-098
KAMIYA, N., MP27-12
Kamiyama, M., UP01-015
Kamiyama, Y., UP01-044, UP02-084
KAMOI, K., MP07-16, MP16-03, UP01-093
Kamoto, T., VP02-04, VP04-05
Kan, C.F., VS04-01
Kanaev, S.V., MP15-12
Kanamaru, H., VS14-09
KANAMARU, S., UP01-044, UP02-084
KANDA, H., UP01-008
Kanda, K., UP02-037
Kane, C., MP13-06
Kane, C.J., MP01-03, MP01-16, VP01-13, VP01-14
Kaneko, G., UP01-075, VP01-02
Kang, D., MP08-12
Kang, D.H., MP12-04, MP20-08
Kang, D.I., MP28-07
Kang, K., UP02-124
Kang, T.W., MP24-02
Kang, T.-W., UP01-003
KANNO, T., MP10-04, MP34-03, UP02-047, UP02-060
Kao, S.L., VP01-05
Kaouk, J., MP20-13, MP26-16
Kaouk, J.H., MP32-15, UP01-112, UP02-127, UP02-128
Kapasi, F., MP22-13
Kapoor, R., MP18-09
Kapur, P., BR01-11
Karakewicz, P., VP05-02
Karakewicz, P.I., MP08-01, MP13-08
Karaolides, T., MP22-03
Karaolidis, T., UP02-105
KARASHIMA, T., UP02-118
Karet, F.E., MP05-17
Kargin, K., VS13-06
Karia, S., BR02-02, BR02-04, BR02-07, BR02-08, BR04-03
Karnabatidis, D., BR01-14
Kasahara, T., UP01-023
Kashi, A.H., MP11-08
Kastriotis, I., MP22-03
Kasuya, Y., MP22-07
Kaswick, J., MP17-06
Kaswick, J.A., VS05-03
Kata, G., UP01-017
Kata, S.G., UP02-074
KATO, M., UP01-008, UP01-051, UP01-095, UP02-109
KATO, S., MP33-04, VS07-01
KATO, T., UP01-013, UP01-047, UP01-058, UP02-059, UP02-088, UP02-119
Kato, Y., MP30-01, MP30-06
KATSUOKA, Y., UP01-069, UP02-107
KATSURO, T., UP01-111
Katz, M.H., VP05-16
Kaufman, S.R., MP06-05, MP19-10
Kaver, I., MP18-10
Kavoussi, L., MP27-09, VP02-12
Kavoussi, L.R., VP01-01, VS12-08
KAWA, G., MP13-05, MP28-12, VP01-09, VP03-04
Kawabata, G., VP06-11
Kawabata, T., VP01-09, VP03-04
Kawaguchi, T., MP07-11
KAWAHARA, T., UP02-045, UP02-048, UP02-086, UP02-092
KAWAI, N., MP25-09, UP01-087, UP01-103, UP01-107, VP05-04
KAWAMURA, H., UP02-097
KAWAMURA, K., MP27-12, UP02-010
Kawamura, M., UP01-042
KAWAMURA, Y., UP02-059
KAWANISHI, Y., MP14-13, UP02-114
Kawasaki, Y., MP27-07
Kawashima, H., UP01-060, UP02-072
KAWAUCHI, A., MP07-16, MP16-03, MP26-04, UP01-093
KAWAZOE, H., UP01-047, UP02-059
Kazemi Rashed, F., BR02-14
Keel, C., BR03-03, MP16-10
Keeley, F., MP03-06
Keil, M., MP09-06
Keller, E., BR03-10
Keller, J., BR03-10
Kerbl, D.C., MP02-18, MP32-16, VP03-03
Keren-Paz, G., MP18-07, MP18-10, MP29-04
Kern Laydner, H., MP32-15, UP01-112, UP02-127, UP02-128
Keshvari, M., BR03-09
Keskin, M.S., MP16-11, MP30-05, VS09-02, VS16-07
Keskin, S.M., MP08-13
Khadoury, S., UP02-112, UP02-113
Khan, F., BR01-07
Khan, M.S., BR01-06, BR01-07, BR01-08
Khan, N., BR01-06, BR01-07, BR01-08
Khanna, A., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Khanna, R., MP20-13, MP32-15, UP01-112, UP02-127, UP02-128, VS14-08
Khatri, N., MP26-02
Khazaeli, M., MP02-10
Khoje Daloee, M., UP02-014
Khongchareonsombat, W., VS11-02
Khoshdel, A., MP11-01
Kijvikai, K., MP18-08
Kikuchi, E., MP27-14, UP01-021, UP01-075, UP01-077, UP01-086, UP01-113, VP01-02, VS15-03
Kim, B.S., UP01-020
Kim, B.W., UP01-020
Kim, C., VP03-08
Kim, C.-S., BR03-11, BR03-12, MP14-08, MP34-14
Kim, D., UP01-065
Kim, D.K., MP19-08
Kim, E., MP03-15
Kim, E.H., MP25-12, VS02-01
Kim, E.T., MP19-08
Kim, H., MP15-07
Kim, H.G., UP01-033
Kim, H.H., MP01-12, MP03-17, MP12-17, VP01-15, VS12-06
Kim, H.J., MP01-02, MP04-02, UP01-063, UP01-064
Kim, H.T., MP07-04, MP24-16
Kim, I.Y., MP08-12, MP28-07
Kim, J.b., MP04-02
Kim, J.H., MP12-07
Kim, J.S., UP01-020
Kim, J.W., UP01-034
Kim, K.H., UP02-056
Kim, K.S., VS13-07
Kim, K.T., MP01-12, MP03-17, MP12-17, VP01-15
Kim, M., VS16-08
Kim, S., UP02-063
Kim, S.H., MP07-04
Kim, S.W., UP01-072, UP01-073
Kim, T.B., UP02-056
Kim, T.H., MP03-19, MP20-08
Kim, T.-H., UP01-020
Kim, T.S., VS01-07
Kim, W., MP34-14
Kimura, M., UP01-091
KIMURA, T., UP01-061, UP02-017, UP02-051, UP02-083
Kimura, Y., MP16-03, UP01-093
Kinebuchi, Y., MP27-16
King, N., MP08-14
King, T., MP18-11, VP04-06
KINOSHITA, H., MP02-19, MP13-05, MP28-12, VP01-09, VP03-04
KINUKAWA, T., UP01-061, UP02-017, UP02-051, UP02-083
KIRA, S., UP01-015, UP01-048
KITAHARA, K., UP01-045
Kitamoto, K., UP01-060
KITAMURA, H., UP01-049, VP02-08
Kitayama, S., UP02-091
Kitrou, P., BR01-14
Kitta, T., UP02-099
Kiyokawa, H., MP27-16
Kiyotaka, O., UP01-116
Klacz, J., VS17-06
Klausner, A.P., MP20-14
Klecka, J., MP11-13
Klein, T., BR01-13, BR03-04
Knight, J., MP05-09, MP05-14, MP05-15
Knight, R., MP12-16
Knoll, T., MP05-05, MP23-14, MP23-18, MP33-08, VP03-14, VP04-14, VP04-16, VP06-06
Knudsen, B., MP10-02, MP19-01
Ko, D.H., MP04-02
Ko, Y., MP17-14, MP17-15, MP17-16
Ko, Y.H., MP28-04, MP28-05, MP28-06, VS03-05, VS13-05
KOBATAKE, K., UP01-051, UP01-095
KOBAYASHI, H., MP31-03, MP31-05, UP01-015, UP01-059, UP01-062
KOBAYASHI, K., MP01-13, MP02-12, MP07-06, MP13-15, MP25-16
KOBAYASHI, T., UP01-087, VP04-05, VS03-07
KOBAYASHI, Y., MP29-12, UP01-009, UP01-054
Kobayasi, H., UP01-055
Kobori, Y., VP06-15, VS11-08
Kochakarn, W., MP13-14
Kochiev, D.G., MP15-14, UP02-022, UP02-042, UP02-069
KODAIRA, K., UP02-110
KODAMA, Y., UP01-089, UP02-050, VP04-11
Kodamala, S., VP06-07
Koga, S., MP32-09
KOHGUCHI, D., UP01-098
KOHJIMOTO, Y., UP01-089, UP02-050, VP04-11
KOHRI, K., MP25-09, UP01-050, UP01-087, UP01-096, UP01-103, UP01-107, UP02-098, VP05-04, VS03-07
Koichiro, M., UP01-090
KOIE, T., UP01-046, UP02-011
Koizumi, K., UP02-068
KOJIMA, S., UP01-052, UP02-025, VS05-04
KOJIMA, Y., MP25-09, UP01-103, UP02-098, VP05-04
Kokorowski, P., MP25-07, MP34-07
Komai, Y., VP01-09
KOMATSU, T., UP01-061, UP02-017, UP02-051, UP02-083
KOMIYA, A., UP01-114
Kommu, S.S., MP02-01, MP02-02, MP02-03, MP02-06, MP02-07, MP02-08, MP02-09, MP03-07, MP06-08, MP11-10, MP11-16, MP12-01, MP16-08, MP28-09, MP30-12, MP31-08, VP01-08, VP02-03, VP02-15, VP03-01, VP03-02, VP03-07, VP06-07, VP06-12, VP06-14, VS02-07, VS06-07, VS13-04
Komori, M., MP14-13, UP02-114
Komorowski, D.J., MP21-11
Komura, K., UP02-107
Komyakov, B.K., MP06-09, MP06-11, MP29-05
Konandreas, A., MP22-03
KONDO, K., UP01-068
KONDO, T., MP31-03, MP31-05, UP01-059, UP01-062
Kondou, T., UP01-055
Kongchareonsombat, W., MP13-14
Kono, H., UP01-086
Kono, J., UP01-090
Kopp, R., MP01-03, VP01-13
Kopp, R.P., MP01-10, VP01-14
Korets, R., MP19-05, UP02-034
Korley, F.K., MP09-09
KORUK, E., MP19-14, VP04-12
KOSEKI, T., MP32-05
Koshida, K., UP02-035
Kosina, J., MP13-16
Kouno, H., VS15-03
Koutsiaris, E., UP02-105
KOZIMA, Y., UP01-107
Krajka, K., VS17-06
Krambeck, A.E., MP05-12
Krane, L.S., MP06-06, MP06-07, MP16-14, MP16-15, MP31-13
Kreuker, J., UP02-112, UP02-113
Kreuzberg, B., MP11-13
Krishnan, R., UP02-079
Krueker, J., MP32-06
Krynauw, H., MP09-02
KUBO, S., UP02-008, UP02-027, VP05-12
KUBOTA, Y., MP31-07, VP02-07
Kucheria, R., MP24-14
Kudo, D., MP30-01, MP30-06
KUDO, S., UP01-015, UP01-046, UP02-011
KUDOU, S., UP01-048
Kugathasan, G., MP33-10
Kulkarni, M., MP34-01, MP34-02
Kulkarni, R., MP14-05, MP29-07, MP29-08, MP34-01, MP34-02
Kumagai, S., MP33-11
Kumar, s., VP01-07
Kume, H., MP24-06
Kumon, H., MP29-12
Kuo, S.S., MP19-11
Kural, A., VS11-10
KURAL, A.R., MP08-13, MP16-11, MP19-14, MP23-01, MP30-05, VP04-12, VS08-06, VS09-02, VS16-06, VS16-07
Kuratsukuri, K., UP01-060, UP02-072
Kurita, Y., UP01-005
Kurizaki, Y., MP27-16
Kuroda, K., UP01-040
Kuroda, Y., MP02-19
Kuroiwa, K., MP31-12
KUROKAWA, S., UP01-050, UP01-096
KUROSAKA, S., UP01-053, UP01-094, UP01-098
Kurumada, S., VS07-02
KUSAKA, M., MP11-07, MP17-13, MP26-08, UP01-066
Kusuda, Y., MP28-13
Kusuhara, Y., MP14-13, UP02-114
KUSUMOTO, H., UP01-089, UP02-050, VP04-11
Kuwabara, N., UP01-060
Kwak, K.W., UP01-028
Kwek, J.W., MP15-12
Kwon, D.D., MP24-02
Kwon, T.G., UP01-020
Kyriazis, I., BR01-02, BR01-14, BR03-01, BR04-06, MP06-13, MP12-08, MP12-09, MP12-11
L, K., MP30-10
Laciak, R.J., MP30-16
Laguna, M.P., VS01-06
Laguna, P., BR01-12, MP03-02, MP03-04, MP05-05
Lai, J.C., MP22-01, MP22-02
LAI, W.-H., UP01-024
Lai, Y.-w., UP01-025
Laing, K., MP09-12
Lake, B., MP03-15
Lake, B.M., VS02-01, VS08-05
Lallas, C.D., MP17-12
Lamb, A., MP09-11
Landau, E.H., BR03-13, MP09-17
Landerer, E.C., MP27-10, MP27-11
Landman, J., MP05-07, MP05-08, MP19-05, MP25-13, UP02-104
Lane, S., UP02-101
Lange, D., BR04-02, MP29-01, MP30-11
Lange, J., MP05-09, MP05-14, MP05-15
Langenstroer, P., MP16-12, MP31-10
Lanigan, P., MP09-03
Laporte, E., VS14-10
Laslo, I., VP03-06
Lasser, M., MP05-01, VS15-07
Latke, A., BR03-13, MP09-17
Lau, H., MP04-19
Lau, H.M.H., UP01-026
Lau, W., MP15-12
Lavery, H., MP08-09
Law, D.M.C., MP04-08
Lawrentschuk, N., MP17-05, MP32-07
Laxton, C., MP03-06
Laydner, H., MP20-13
Lazarus, J., MP09-01, MP09-02, VS15-02
Leaf, D.E., UP02-034
Lebret, T., VP05-05
Lechevallier, E., UP02-081
Lee, B., BR01-13, BR03-03, BR03-04, MP16-10, UP02-033, VS02-03
Lee, B.K., MP26-12
Lee, B.R., BR03-05, MP06-16, VS08-01
Lee, D., UP02-057
Lee, D.H., MP08-12, MP28-07, UP01-076, UP02-018
Lee, D.I., MP13-03, MP13-04, MP17-03, MP17-10, MP26-14, MP26-15, MP28-03, UP01-071, UP01-082
Lee, F.T., MP09-15
Lee, H., UP02-057
Lee, H.M., MP01-02, MP10-15, MP14-06, UP01-063, UP01-064
Lee, J., MP05-07, MP05-08, UP02-054
Lee, J.-R., MP08-02
Lee, J.Y., MP02-11, MP02-18, UP02-122, UP02-123, MP20-01, MP20-08, MP32-16, UP01-072, UP01-073, UP02-019, VP03-03, VS08-02
Lee, J.Z., UP01-028
Lee, K., UP01-065
Lee, K.S., MP20-08
Lee, L.-H., UP01-037
Lee, M.-C., MP04-19, MP05-04, UP02-029
Lee, M.-H., UP02-032
Lee, M.S., UP01-034
Lee, N., UP01-065
Lee, S., MP07-04, MP19-08, UP01-063, UP02-056, VP05-01, VS12-07
Lee, S.B., MP01-12, MP10-14, MP12-17, VP01-15, VS12-06
Lee, S.C., MP26-11, MP26-12
Lee, S.E., MP07-04, MP26-11, MP26-12, VP05-01, VS12-06, VS12-07
Lee, S.H., UP01-076, UP02-018
Lee, S.W., MP20-01, MP20-08, UP02-122, UP02-123, VS13-07
Lee, S.Y., MP01-02, UP01-064
Lee, T.Y., MP20-01, UP02-122, UP02-123, VS13-07
Lee, Y.-H., MP06-01, MP16-06, UP01-002, UP01-084
Leenanupund, C., MP13-14
Lehmann, K., MP04-20
Leichter, I., MP09-17
Letang, N., VP05-05
Leung, R., MP05-06, MP08-08, UP01-081
Leveillee, R.J., MP06-16
Leventis, A., MP04-17
Lewandowski, P., VS02-04
Lewandowski, P.-M., MP16-16, VS14-02
Lewis, I.E., MP02-08, VP06-14
Lho, Y.S., UP01-033
Li, C.-C., UP01-115, UP02-032
Li, H., UP02-001, VP05-03
Li, W.-M., UP02-032
Liao, L.W., UP02-036
Liao, Y., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Liastikos, E., VP04-14
Liatsikos, E., BR01-02, BR01-14, BR03-01, BR04-06, MP06-13, MP12-08, MP12-09, MP12-11, VP04-16
Liaw, A., MP11-05
Liberman, D., VP05-02, VP05-16
Lim, J.H., BR03-11, BR03-12, MP14-08, MP34-14
Lim, J.S., UP02-019
Lim, M.S., MP12-07
Limani, K.V., MP15-03
Lin, B., MP03-12
Lin, C.-D., MP06-12, VP02-05, VS14-05
Lin, C.-T., MP34-13
Lin, E.-S., MP12-02
Lin, S., MP02-11
Lin, Y.-C., VP02-16
Lindner, A., MP10-01
Linehan, W.M., MP32-06
Ling, A., MP04-19
Lingeman, J.E., MP05-12, MP10-05, MP10-06, MP30-13, MP33-05
Link, R.E., MP12-10, MP12-15, MP12-16, MP26-09, MP26-10
Linton, K.D., MP06-18
Liourdi, D., BR01-02, BR01-14, BR03-01, BR04-06
Lipkin, M.E., BR04-10, BR04-12, BR04-13, BR04-14, MP15-16, MP18-08, MP18-09, MP29-06, VP04-02, VP06-16, VS10-02, VS13-03
Liu, C., MP20-04, MP20-07, MP20-17, UP02-001, VP01-12, VP05-03, VS04-01
Liu, C.-C., UP02-032
Liu, C.-L., UP01-002
Liu, F., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-07
Liu, K., MP26-13
Liu, M.-E., UP02-032
Liu, P.-L., MP04-08
Liu, X., UP02-070
Liu, X.-P., MP22-10, VP06-04
Lloyd, G.L., MP20-16
Llukani, E., MP13-03, MP13-04, MP17-10, MP26-14, MP26-15, MP28-03
Locklin, J.K., MP32-06
Lojanapiwat, B., MP10-08
Londoño, D.C., MP14-15
Long, D., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
López, J.M., VS01-09
Lopez, V., VS11-10
Lorber, G., BR03-13
Lorente, J.A., MP13-01, MP33-09, UP01-080, UP02-002, VS09-08
Louie, M., MP11-04
Louie, M.K., MP05-07, MP05-08, VS08-02
Love, C., MP04-16
Lowery, C., BR04-12
Lowry, C., VP06-16
Lu, H.Z., MP11-14, MP30-07
Lu, J., UP02-003, UP02-015, UP02-016, UP02-030, UP02-031, UP02-067, UP02-075, UP02-077, UP02-078
Lu, Z., MP19-02, MP19-17, MP29-10, MP29-11, MP29-14, MP32-02, MP32-08, UP02-015, UP02-016
Lubner, M.G., MP09-15
Lucas, S.M., MP01-14, MP06-16, MP11-05, MP11-06, MP31-01
Lugangne, P.-M., VP05-05
Lugnani, F.M., MP15-09
Luke, M., BR02-06
Luke, P., MP06-16
Lulin, M., MP01-07, MP20-06, MP28-10
Lum, J., MP05-16
Lusch, A., MP25-13, MP28-02
Luscombe, C.J., MP02-07, MP06-08, MP28-09
Lusuardi, L., MP33-07
M, S., BR02-07
Ma, L., MP11-03, MP11-11, MP11-12, MP16-04
Mabjeesh, N.J., MP29-04
Macalalag, M., MP07-03, VP05-10
MACHIDA, J., MP16-07, UP01-105
Machida, T., MP33-02
Mackinnon, R., MP06-18
Maclean, F., VP05-09
Madaan, S., MP21-08, MP24-12
Maeda, T., MP27-14, UP01-077, UP01-086, UP01-113, UP02-087
Maeda, Y., UP01-100
Magrill, D., MP11-10, VP01-08, VP02-03, VP02-15
Maheshwari, P.N., BR04-05
Mahmud, M.S., MP18-06
Maini, C.L., MP32-11, VP03-15
Maita, S., MP12-14
Mak, S.K., VS15-05
Makanjuola, J.K., MP09-03
Makino, Y., UP01-044, UP02-084
MAKIYAMA, K., MP31-07, UP01-068, VP02-07
Malde, S., UP02-020, UP02-079, UP02-106
Malek, R., MP04-10
Malki, M.M., MP06-18
Mally, A., MP25-05
Mally, A.D., MP10-12
Mancini, J.G., BR04-14
Mandeville, J.A., MP05-12, MP30-13, MP33-05
Mani, H., VP03-09
Manny, T.B., MP05-20, MP06-03, MP06-06, MP06-07, MP11-09, MP16-14, MP16-15, MP31-13
Mansoriyan, e., UP02-006
Marien, T.P., MP10-03, MP31-17, VP02-13
Markuszewski, M., VS17-06
Marsh, H., MP05-16, MP21-08, MP24-12, MP30-03
Marsh, R., MP34-11
Martinez-Suarez, H., MP13-13
Maruyama, S., MP31-11, VS05-05
MARUYAMA, T., MP11-07, MP17-13, MP26-08, UP01-050, UP01-066, UP01-096
Marx, G., BR04-09, UP02-071
MASUDA, H., UP01-052, UP02-025, VS05-04
Masuda, T., MP22-07
Masumori, N., UP01-022, UP01-049, VP02-08
MASUMOTO, H., MP01-13, MP02-12, MP07-06, MP13-15, MP25-16
MASUNAGA, K., MP22-07
Matlaga, B., MP14-12, MP30-11, UP02-117
Matlaga, B.R., MP09-09, MP10-05, MP10-06
Matsoka, T., UP02-072
MATSUBARA, A., MP01-13, MP02-12, MP07-06, MP13-15, MP25-16, UP02-094, UP02-095
Matsubara, S., VP06-11
MATSUDA, A., MP10-04, MP34-03, UP02-047, UP02-060
Matsuda, K., MP03-10, VP02-06, VS05-08
Matsuda, S., MP24-06
Matsuda, T., MP02-19, MP13-05, VP01-09, VP03-04
Matsui, Y., MP09-13, UP02-120
Matsukawa, Y., UP02-109, VP06-01
MATSUMOTO, K., MP03-18, MP06-10, UP02-028
Matsumoto, M., MP06-15, UP02-012, VP05-06, VS03-01
Matsumoto, R., MP31-11
MATSUMOTO, S., UP01-045
MATSUMURA, N., UP01-089, UP02-050, VP04-11
MATSUO, M., UP01-011
MATSUO, R., UP02-085
MATSUOKA, K., UP01-011
Matsushima, M., VP01-02
Matsuta, Y., MP22-07
Matsuyama, H., MP27-02
MATSUZAKI, J., UP02-045, UP02-048, UP02-086
MATUDA, T., MP28-12
Matuzaki, j., UP02-092
Matzkin, H., MP18-07, MP18-10, MP29-04
MAugeri, O., VS10-05
mavila, l., MP19-07, MP19-15, MP32-03
Mavilla, L., MP22-14, MP24-01, MP30-09, UP01-001, UP02-013
Mayer, W.A., MP26-09, MP26-10
McAlister, G., MP15-16
McCahy, P., MP18-12
McClinton, S., MP01-15, MP09-12, MP30-10, MP30-12, UP02-055
McDougall, E.M., MP02-11, MP02-18, MP05-07, MP05-08, MP32-16, VP03-03
McFadden, M., MP30-16
McGovern, F.J., MP21-15
McKinney, Y.L., VP03-09
McLeroy, S., BR01-04
McLorie, G., MP05-02
Mcmillan, M., MP02-14
Meckel, K., UP02-104
Meckley, L.M., MP10-05, MP10-06
Medina, R., MP13-09
mehrzad, r., MP04-01, MP04-03
Mehrazin, R., MP01-10
Mehrotra, S., MP20-15, MP26-02, UP01-078, VP04-07, VS15-01
Mehta, S., MP32-10
Melekos, M.D., MP04-17, MP18-08
Mellon, M.J., MP31-01
Melzer, A., UP02-100
Mendiola, F., MP07-03, VP05-10
Menon, M., MP13-08, MP26-07, VP06-13
Merino, M.J., VP03-09
Merinov, D., BR04-07
Micali, S., BR02-09, MP24-11, VP01-01, VP02-12, VS12-08
Michal, M., MP11-13
Michel, M.S., MP25-13
MIKI, T., MP07-16, MP16-03, UP01-093
Milan, H., VP06-09
Millar, M., MP03-09
Miller, N., MP30-11
Miller, N.L., MP09-10
Mimata, H., MP12-12, MP20-12, UP01-106
Mimura, Y., UP02-068
MINAGAWA, S., UP02-023, UP02-121
MINAMI, K., MP20-10, UP01-067
Minami, T., UP01-009
MInamida, S., UP01-091
MInei, S., UP01-091
Minhua, L., MP23-11
Mir, C., MP24-03
Mir, S.A., MP03-01
Mirabile, G., MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
mirabile, g.g., MP14-11
Mirciulescu, V., MP18-13
Mishra, N., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-071, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Mishra, S., MP10-13, MP19-12, MP20-15, MP26-02, UP01-078, VP04-07, VP04-15, VS15-01
MITA, K., UP01-051, UP01-095
Mitchell, G., BR01-13, BR03-04, BR03-05
Mitchell, S.E., MP14-01
Mitsui, T., MP03-11, UP02-099
Mittal, S., MP22-08, UP01-085
Miura, H., MP30-01, MP30-06, UP02-076
MIURA, M., MP07-09
Miyahara, M., VS15-03
Miyaji, Y., UP02-108
Miyajima, A., MP27-14, UP01-021, UP01-075, UP01-077, UP01-086, UP01-113, VP01-02, VS15-03
Miyajima, N., MP03-11
MIYAKE, H., MP28-13, UP01-039, UP01-043, UP01-097, UP01-102, UP02-009, UP02-012, VP02-11, VP05-06
Miyakita, H., MP25-02
MIYAMOTO, K., MP01-13, MP02-12, MP07-06, MP13-15, MP25-16
Miyamoto, T., UP01-015
Miyaoka, R., BR04-02
Miyauchi, Y., MP11-02, UP01-029, UP01-030, UP01-031
Miyazaki, Y., VP01-02
Miyazato, M., MP27-07
MIYOSHI, Y., UP01-068
Mizoguchi, S., MP20-12
MIZOH, Y., UP01-101
MIZUNO, K., MP25-09, UP01-107, UP02-098
Mizuno, R., UP01-086, VS15-03
Mizuno, T., UP01-022
Mizusawa, H., UP02-068
Mizutani, K., UP02-109
MIZUTANI, Y., MP28-11, UP01-090, UP01-099
Moazzam, M., UP02-080
Mochida, J., MP33-12
Mochiduki, K., UP01-091
Mofferdin, A., BR02-09, MP24-11
mogharabiyan, n., UP02-093
Mohamadzadeh Rezaei, M.A., MP34-10
Mohammadian, R., MP27-01
Mohan, S., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-071, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Mohd Zam, N.A.B., UP01-026
Molaee, M., UP02-014
Moldoveanu, C., MP22-09, MP22-11, MP22-15, VP03-13
Mombet, A., MP08-10
Monahan, K., MP28-03
Monden, K., MP29-12
Monga, M., BR04-02, BR04-08, VS10-04, VS14-08
Monish, A., VS04-06, VS13-01
Monteferrante, E., MP09-12, UP02-055
Montgomery, J., MP11-15
Montgomery, J.S., MP19-10, MP22-01, MP22-02
Montorsi, F., MP17-03, UP01-071, UP01-082, UP01-083
Moon, H.S., MP20-01, UP02-122, UP02-123, VS13-07
MOORE, B.W., MP20-14, VP01-04, VP01-11, VS04-03, VS09-07
Morales, B., MP28-02
Morehouse, D., MP24-10
Morgenstern, H., MP06-05
Morhardt, D., VP01-04
Mori, K., MP12-12, UP01-106
MORI, M., UP01-010
MORI, S., MP33-04, VS07-01
MORIKAWA, H., UP02-023, UP02-121
MORITA, J., UP02-087
Morita, K., MP03-11
Morita, M., UP02-087
MORITOKI, Y., UP02-098
MORIYA, K., UP02-099
Morizane, S., MP06-15, VS03-01
Moss, M., MP18-11, VP04-06
Mostafavi, M., MP23-07
Moteria, S., BR02-02, BR02-04, BR02-08, BR04-03
MOTOO, A., MP29-12
Mottrie, A., UP01-083
Mouraviev, V., MP08-15, MP08-16, MP21-04, VP03-10
Mucksavage, P., MP02-11, MP02-18, MP05-07, MP05-08, MP11-04, MP32-16, VP03-03, VS08-02
Mueller, G., MP07-15
Mueller, P.R., MP21-15
Mues, A.C., MP19-05, UP02-104
Mufarrij, P., MP05-02, MP05-09, MP05-14, MP05-15, MP16-14, MP16-15, MP31-13
Mugiya, S., UP01-005, UP02-088
Muijtjens, A.M.M., MP02-04
Muir, G., MP04-10, MP04-11, MP33-06
Mukherjee, S., MP32-13
Müller, G., MP04-12
Mulligan, D., MP31-09
Mullins, J., MP14-12, MP16-09, MP27-09, UP01-016
Mullins, J.K., MP03-12, MP03-16, MP09-05, MP09-06, MP14-01, MP17-02, MP17-08, VP06-10
Multescu, R., MP18-13, MP22-09, MP22-11, MP22-15, MP30-02, VP03-12, VP03-13, VS16-09
Munshey, A., BR01-09
Munver, R., MP06-16, MP08-14, MP16-01, MP16-02, MP16-17, MP21-06, MP21-09, MP28-08, VS16-08, VS17-01
MURAKAMI, Y., UP01-053, UP01-091, UP01-098
MURAMAKI, M., MP28-13, UP01-039, UP01-097, UP01-102, VP05-06
Murat, A., BR04-04
Muresan, A., VP04-09
Murugesan, A., MP14-16, MP25-01, VS05-01, VS06-05, VS06-06, VS11-04, VS11-06, VS11-07, VS16-01
Musanejad, N., MP11-08
Musaoglu, A., MP31-15, UP02-115
Muschter, R., MP05-05
MUTO, S., MP15-04, MP32-05, MP32-12, MP33-03
Mutsuo, H., UP01-116
Myatt, A., MP33-07
Na, Y.G., UP02-019
Nabi, G., MP02-13, MP02-14, MP02-15, UP01-017, UP02-074, UP02-100, UP02-101, VS11-09
Nadler, R.B., MP06-16, MP09-04, MP17-11
NAGAE, M., MP32-05
Nagahama, K., VS14-09
Nagai, A., UP02-108
NAGAI, Y., UP01-054
Nagamori, S., MP20-10, UP01-067
NAGAOKA, A., UP01-047, UP02-059
NAGATA, D., UP01-050, UP01-096
Nagata, H., UP01-077, UP01-086, VS15-03
NAGATA, M., UP01-005, UP02-088
Nagata, Y., MP15-07
NAIKI, T., UP01-107, VS03-07
Nair, M., MP28-09
NAITO, S., MP26-04, MP31-12, UP01-047, UP02-059, UP02-076, VP05-13
NAITOH, Y., MP07-16, MP16-03, UP01-093
Najjaran, V., MP06-02
Nakada, S.Y., BR02-01, MP09-14, MP09-15, MP21-12, MP34-08
NAKADA, T., UP02-118
NAKAGAWA, G., UP01-011
Nakagawa, H., MP27-07
Nakagawa, K., MP26-04, MP27-14, UP01-021, UP01-075, UP01-077, UP01-086, UP01-113, VP01-02, VS15-03
NAKAGAWA, M., MP28-12, VP03-04
Nakahira, Y., MP03-10, VP02-06, VS05-08
Nakaigawa, A., VP02-07
NAKAIGAWA, N., MP31-07
Nakajima, H., UP02-058
Nakamoto, M., VS02-02, VS02-04, VS14-02, VS14-03
NAKAMURA, K., MP32-01, MP33-01, MP33-02, UP01-052, UP01-100
NAKAMURA, M., UP01-068
NAKAMURA, Y., MP33-13, UP01-006, UP02-052
NAKANE, A., UP01-087
Nakanishi, J., UP01-027
Nakanishi, R., UP02-037
Nakano, M., MP15-07, MP25-02
NAKANO, Y., UP01-039, UP01-043, UP01-097, UP01-102, UP02-009, UP02-012, VP02-11, VP05-06
NAKANOUCHI, T., UP01-010
NAKAO, T., UP01-057, UP02-046
NAKASHIMA, K., UP01-057, UP02-046
NAKATA, W., UP01-012
Nakatani, T., UP01-060, UP02-072
NAKATSUKA, H., UP02-061
NAKAYAMA, M., UP01-012
NAKAZAWA, H., MP25-17, VP02-10
Nakene, A., VS03-07
Nakhoda, Z., MP19-04
NAMPO, Y., UP01-089
NANPO, Y., UP02-050, VP04-11
Naoe, M., UP02-087
NARISAWA, T., UP01-047, UP02-059
Narita, S., MP12-14
Narra, V.R., VS02-01
Naryshkin, S.A., MP15-14, UP02-022, UP02-042, UP02-069
Naselli, A., MP21-02, MP21-03, VP06-08
Nasu, Y., MP29-12
Natalin, R., MP13-09
Navanimitkul, N., MP10-08
NAYA, K., MP32-01
NAYA, Y., BR01-05, MP27-12, MP33-01, UP01-010, UP01-052, UP02-025, VS05-04
Neal, D., UP01-071, UP01-083
Nechita, F., VP02-14, VP03-06, VP06-03
Nechita, F.V., VS03-06, VS11-03, VS14-07
Necmettin, P., BR04-04
Nedas, T., VS02-07, VS06-07, VS13-04
Neeman, V., MP09-17
Negro, C.L.A., MP04-10, MP33-06
Nelson, C., MP25-07, MP34-07
Nelson, E.D., MP25-03, MP25-11, VS14-01
Nerli, R., MP22-12, MP27-08, UP02-096
Neuzillet, Y., VP05-05
Neville, A., BR04-12
Neville, A.M., VP06-16
NG, A.T., MP23-13
Ng, C., MP16-16
NG, C.-f., BR04-01
Ng, E.H., MP23-10
Ng, L.G., UP01-026
Ngai, H.Y., VP01-06
NGUYEN DAVID, H.D., VP04-03, VP05-11
Nguyen, G., BR04-12, VP06-16
Nguyen, K.K., MP14-09, MP29-02, MP34-05, MP34-06
Nicolson, D.J., MP09-08
NIHEI, N., MP27-12, MP32-01, UP01-052, VS05-04
NIIMI, K., UP01-096
Niroomand, R., MP27-01
Nishi, K., UP01-027
NISHI, M., MP03-18, MP06-10, UP01-053
NISHIDA, H., UP01-047, UP02-059
Nishida, S., UP01-049, VP02-08
Nishida, T., MP28-11
NISHIKAWA, k., UP01-008
Nishikawa, N., UP02-072
Nishimatsu, H., MP24-06
NISHIMURA, K., UP01-012
NISHIO, H., UP02-098
Nishio, K., VP06-15, VS11-08
Nishiyama, T., UP01-023
NISHIYAMA, Y., UP02-049
NISHIZAWA, O., MP27-13, MP27-16, UP01-014
NISHIZAWA, S., MP27-16, UP01-089, UP02-050, VP04-11
Nitta, H., MP33-11
Nitta, T., UP02-058
Niwa, N., MP03-10, VP02-06, VS05-08
NOGUCHI, K., UP01-068
NOGUCHI, M., UP01-057, UP02-046
Noh, C.H., MP05-10
Nohales, G., MP33-09, UP01-080
NOJIRI, Y., MP22-07
NOMI, H., MP28-11, UP01-099
NOMURA, M., UP02-024
Nomura, T., MP12-12, MP20-12, UP01-106
Nonomura, K., MP03-11, MP31-11, UP02-099, VS05-05
Nose, K., UP01-041
Nosov, A.K., MP15-12
Nott, L., BR02-06
Nouralizadeh, A., MP02-10, MP06-02, MP11-08
Novak, R., MP08-09
NOZAKI, T., MP11-02, UP01-029, UP01-030, UP01-031, UP01-032, UP01-114
NOZAWA, M., UP01-009, UP01-041, UP01-054
Numakura, K., MP12-14
Nunez, R., MP30-11
NUTAHARA, K., MP01-05, MP33-13, UP01-006, UP02-044, UP02-052, UP02-089
Nyek Ntep, N., MP24-11
Nyirenda, T., MP28-08
O, H., VP06-09
Oae, M., VS14-09
Obara, T., MP12-14
Obatake, A., UP02-108
Obek, C., MP08-13, MP16-11, VS09-02, VS16-07
Obinata, D., MP33-12
Oda, T., VP02-11
OEGAWA, T., UP02-044
Ogasawara, M., MP07-11
Ogawa, O., MP07-10, MP09-13, UP01-035, UP02-120
OGAWA, T., UP02-109
OGAWA, Y., MP15-04, MP32-05, MP32-12, UP02-087
Oguchi, T., UP01-014
Oh, J.J., MP07-04, MP26-11, MP26-12, VP05-01, VS12-06, VS12-07
Oh, J.K., UP02-056
Oh, K.J., MP24-02
Oh, K.-J., UP01-003
Oh, T.H., UP01-028, UP02-019
Ohira, S., UP02-108
OHYAMA, C., UP01-046
Ohyama, T., UP01-091
Oishi, Y., MP20-10
Ojand, A., VS07-08
OKA, K., MP15-08, UP02-090
OKABE, T., UP02-110
Okada, H., VP06-15, VS11-08
Okada, S., MP30-01, MP30-06
Okada, Y., MP33-12
OKAMOTO, T., UP01-046, UP02-011
Okamura, K., MP22-07
OKAMURA, T., UP01-087, VS03-07
OKEGAWA, T., MP01-05, MP33-13, UP01-006, UP02-052, UP02-089
Okeke, Z., MP23-09, MP23-17, VS10-01, VS15-06
Okhunov, Z., MP23-09, MP23-17, VS10-01, VS15-06
Okihara, K., UP01-093
Okubo, K., MP09-13
OKUMURA, K., UP02-024
Okunbor, O., MP24-04, MP24-15
Okuno, M., VP06-11
Olamendi, S., MP05-07, MP05-08
Olbert, P.J., MP18-09
Olweny, E., MP21-16
Olweny, E.O., BR01-04, BR01-11, MP03-01, MP06-14, MP07-17, MP26-05
OMAE, K., UP01-055
Omori, Y., MP33-02
Omoto, K., MP11-02, UP01-029, UP01-030, UP01-031, UP01-032
Ong, E., UP02-055
Ong, R.E., MP09-10
ONISHI, T., UP01-056
Onizuka, C., VP02-04, VP04-05
OOGUTI, N., MP28-12
OOISHI, Y., UP01-067
OOSUGI, N., MP28-12
OOTA, T., UP02-044
Oottamasathien, S., MP30-16
Ordon, M., MP23-10, MP24-05, MP24-09
Ortiz, C., MP11-04, MP21-13
Ortiz, V., MP13-09, MP31-02, MP31-04, MP31-06
Orton, V.A., MP20-14, VP01-04, VP01-11, VS04-03, VS09-07
Orvieto, M.A., VS03-05
Oshinomi, K., UP02-087
Oshiro, O., MP02-19
Ost, M., MP10-12
Ost, M.C., MP25-05
Osther, P., MP05-05, VP04-14, VP04-16
Osther, P.J., MP24-07, MP34-04
Osther, P.J.Sloth, MP14-04
Osther, S., MP24-07
O'Sullivan, P., MP14-18
Otoshi, T., UP01-060
Otsubo, S., MP31-12
Otsuka, A., UP01-005, UP02-088
Otto, T., MP32-17, MP32-18
Ou, Y.-C., MP08-02, MP13-10
Owen, NP, D., MP13-11
Oya, M., MP27-14, UP01-021, UP01-075, UP01-077, UP01-086, UP01-113, VP01-02, VS15-03
Oyama, C., UP02-011
OYAMA, M., UP02-110
Ozono, S., UP01-005, UP02-088
P, S., VP06-09
Pace, K.T., MP23-10, MP24-05, MP24-09
Pacik, D., MP23-02
Pacovsky, J., MP13-16
Padilla, W., VS06-04, VS08-04
Paffen, M.L.J.E., MP29-09
Pai, M., VS05-01, VS06-05, VS06-06, VS11-04, VS11-06
Pai, M.G., MP14-16, MP25-01, VS11-07, VS16-01
Paick, S.H., UP01-033
Paiva, C., MP13-09
Pal, S.K., BR02-06
Palazzi-Churas, K., MP13-06
Palmer, J., MP21-08
Palmer, K., MP17-14, MP17-15
Palmer, K.J., MP17-16, MP28-04, MP28-05, MP28-06, VS03-04, VS03-05, VS13-05
Palmeri, M., BR04-13
Palou, J., VS01-05, VS01-09, VS01-10, VS08-03, VS09-06, VS14-10
Pan, S.-C., UP02-032
Pang, J., MP22-10
Pang, Y., VP03-09
Papadaki, H., BR01-02
Papalia, R., MP15-09, MP26-03, MP26-06, MP32-11, VP03-15, VS01-02, VS01-03, VS01-04
Pappas, A., MP22-03
Parekh, N., UP01-078
Parikh, N., VP04-15
Park, B., UP01-064
Park, B.H., MP04-02, MP10-15, MP14-06
Park, B.S., MP01-02, UP01-063
Park, H.K., MP14-08, UP01-033
Park, H.-K., MP34-14
Park, J., MP19-08, MP20-01, UP02-122
Park, J.M., UP02-019
Park, J.-W., MP29-03
Park, M., MP14-08
Park, S., MP21-16, UP02-038, UP02-124, UP02-125, UP02-126
Park, S.H., VS01-07
Park, S.K., BR01-11, MP03-01, MP06-14, MP07-17, MP26-05
Park, S.Y., MP20-01, UP02-122, UP02-123, VS13-07
Park, Y., UP02-057
Park, Y.H., MP01-12, MP03-17, MP12-17, VP01-15
Park, Y.K., UP01-020
Parker, F., MP17-05
Parra, E., VS03-03
Pascal, Z., VS04-06
Pasini, L., MP19-16, MP23-12
Patcharatrakul, S., MP13-14
Patel, H.D., MP03-16
patel, k., UP02-033
Patel, K.B., UP01-004, VS06-03
Patel, M., MP04-19
Patel, M.I., BR04-09, UP02-071
Patel, O., BR01-10
Patel, R., MP04-06, MP28-09, VS07-03
Patel, S.R., BR02-01, MP09-14, MP09-15, MP21-12, MP34-08
Patel, V., MP17-14, MP17-15, MP17-16, VS03-04
Patel, V.R., MP28-04, MP28-05, MP28-06, VS03-05, VS13-05
Paterson, R.F., MP05-06, MP29-01, MP30-11
Pathak, A., BR03-07
Patil, M., MP16-16, VS02-02
Patil, M.B., MP05-03
Patil, S., MP22-12, MP27-08, UP02-096
Pautler, S.E., MP06-16
Payne, D., MP03-06
Paz, A., BR04-08, VS10-04
Peabody, J., MP13-08
Pearle, M.S., BR01-04
Pedram Rad, B., BR02-11
Pelte, M.-F., MP08-07
Peltier, A.Y., MP15-03
Peña, J.A., VS01-05, VS01-09, VS01-10, VS08-03, VS09-06, VS14-10
Penkar, M., MP21-14
Pennison, M., MP34-07
Penniston, K.L., BR02-01
Pera, M., MP13-01, VS09-08
Perez Duarte, F., VS01-06
Perkin, H.B., MP05-03
Perlin, D., VS13-06
Permpongkosol, S., MP07-13, VS12-04, VS12-05
Perotte, P., MP08-01
Perry, K.T., MP09-04, MP17-11
Perscky, I., UP02-117
Persoon, M.C., MP02-04
Peschechera, R., MP19-16, MP23-12
Peters, E.M., MP14-10
Petrisor, D., VP03-08
Petros, F., MP26-07, VP06-13, VS02-05
Petrut, B., VP02-14, VP03-06, VP06-03
Petrut, B.B., VS03-06, VS11-03, VS14-07
Pham, J.C., MP09-09
Phillipou, P., MP03-06
PHO, M.T., VP04-03, VP05-11
Pick, D., MP05-07, MP05-08
Pickhardt, P.J., MP09-14
Piechaud, T., MP05-05
Pierorazio, P., MP16-09, MP27-09, UP01-016
Pierorazio, P.M., MP03-03, MP03-12, MP03-16, MP09-05, MP09-06, MP14-01, MP17-02, MP17-08, VP06-10
Pinheiro, T., MP13-09, MP31-02, MP31-04, MP31-06
Pino, L.A., MP33-09, UP02-002
Pinto, P., UP02-112, UP02-113
Pinto, P.A., MP32-06, VP03-09
Pisanti, F., MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
pisanti, f.f., MP14-11, MP25-15
Pittenger, N.T., MP14-10
piyasoontrawong, n., UP02-116
Plaza Mas, L., VS01-06
Png, K.S., MP01-14, MP11-05, MP11-06, MP31-01
Png, K.-S., VP04-04
Pode, D., BR03-13, MP09-17
Pohar, K., VP01-03
Pohida, T., VP03-09
Polland, A., UP02-104
Pompeo, V., MP26-03, VS01-03, VS01-04
Poniatowski, L., VP03-05
Porin, A., VP05-10
Potluri, B., MP32-10
Pozniak, M.A., MP09-14
Prabhu, A., MP32-10
Prapotnich, D., MP08-03, MP08-10, MP15-06
Preminger, G., VP04-02
Preminger, G.M., BR04-10, BR04-12, BR04-13, BR04-14, MP15-16, MP18-08, MP18-09, MP29-06, VP06-16, VS10-02
Prien, E.L., MP05-13
Proteek, O., MP27-09
Pucheril, D.T., MP13-03, MP17-10
Puppo, P., MP21-02, MP21-03, VP06-08
qihui, c., MP18-02, MP23-05, MP30-08
Qiu, J.-G., MP22-10, VP06-04
Quast, S., MP32-17
Quddus, B., MP18-06
Rabah, D.M., BR02-10
Rad, M., UP02-020
Raheem, O., MP01-03, MP01-10, MP01-16, VP01-13, VP01-14
Rahmani, J., MP02-10
Rai, B., MP02-13
Rais-Bahrami, S., VP02-12
Rajagopalan, A., UP02-106
Rajamahanty, S., MP11-09
Rajarubendra, N., BR01-09
Rajyaguru, K.B., UP01-004
Ramalingam, M., MP14-16, MP25-01, VS05-01, VS06-05, VS06-06, VS11-04, VS11-06, VS11-07, VS16-01
Ramirez, L.F., VS05-02
Ramirez, R., MP21-05
Ramjit, C., VP06-14
Ramos, E., VS01-05, VS01-10, VS09-06
Rane, A., MP02-07, MP02-08
Rangavajjula, A., MP17-12
Rankin, J., MP28-08
Rao, A., MP01-15
Rao, K., MP32-07
Rashid, H., MP20-16, MP21-07, VP02-01, VP02-02, VS16-03
Rashid, M., MP01-15
Rassweiler, J., MP05-05, MP23-02
Rassweiler, J.J., MP25-10
Rastinehad, A.R., MP32-06, VP03-09
Rawlings, L.D., MP33-05
Ray, A.A., MP23-10
RAYNAL, G., UP02-039, UP02-081, VP03-11
Razvi, H., BR02-06
Rebuck, D.A., MP09-04, MP17-11
Reddy, M., UP02-096
Reich, O., MP04-11, VP06-05
Reis-Santos, J., MP05-05
Remington, A., MP28-02
Rempelakos, A., UP02-105
Renard, J., MP08-07, MP13-02, MP17-04
renard, J.R., VS07-05
Rentsch, C.A., MP07-15, MP25-10, VS17-08
Reuther, R., MP14-17, MP14-18
Rha, K.H., MP12-07, UP01-034
Rheinwald, M., MP04-18
Rhew, H.Y., VS01-07
Richards, G.D., MP07-01, MP07-02, MP14-07, MP14-10, MP21-14, MP28-01, MP34-09, VS09-05
Richstone, L., VP01-01, VP02-12
Rieken, M., BR03-14, MP04-12, MP04-20, MP07-15, VS17-08
Rigopoulos, C., BR04-06
Rijo, E., MP13-01, MP33-09, UP01-080, UP02-002, VS09-08
Riley, J., MP18-14, MP18-16
Riley, J.M., MP19-11, MP19-13, MP25-05
Rioja, J., VS01-06
Rioja, L.A., VS01-06
Roberts, W.W., BR02-13, BR03-10, MP15-13, MP15-15, MP19-10, MP22-06
Robinson, C., MP05-17
Robinson, S.P., VP01-04, VP01-11
Rocco, B., MP17-14, MP17-15, MP17-16, VS03-05
Rodriguez, C., VS11-01
rodriguez, f., MP22-04
Rodríguez-Faba, O., VS08-03
Rogers, C.G., MP13-08, MP26-07, VP06-13, VS02-05
Roosen, A., VP04-01
Roslan, M., VS17-06
Rosol, T.J., BR03-10
Roupret, M., MP28-15
Rouse, P., MP09-03
Routh, J., MP25-07
Roytman, T., MP03-09
Rozet, F., MP03-05, MP08-03, MP08-10, MP15-06, MP15-10
Ruckle, H.C., MP28-01
Ruiz, L., UP02-117
Ruljancich, P., MP08-06, MP17-07
Ryazancev, A.A., MP15-14
Ryu, D.S., UP01-028
Rzetelski-West, K.F., MP18-12
Saavedra, J., VS03-02, VS03-03, VS04-06, VS11-01
Sabnis, R., MP10-13, MP19-12, MP20-15, UP01-078, VP04-07, VP04-15, VS15-01
Sabnis, R.B., MP26-02
Sacco, D., MP05-11, MP05-19
Sacco, D.E., MP05-13
Sadraee, A., MP34-10
Saeed, I., BR02-01
Saeedi, P., VS06-01
Saffarian, O., MP02-10
Saglam, R., MP19-14, VP04-12
Sahin, A., MP30-05, VS09-02, VS16-07
Saigal, C.S., MP22-01, MP22-02
Saisu, K., UP01-104
SAITO, H., MP26-04, MP27-07
SAITO, K., MP15-04, MP33-03, UP01-023
Saito, M., MP12-14
SAITO, S., UP02-026
Saito, t., UP01-014
Sakai, I., MP28-13, UP01-102, VP05-06
SAKAKIDA, H., MP16-07, UP01-105
SAKAMOTO, F., UP01-061, UP02-017, UP02-051, UP02-083
SAKAMOTO, H., MP03-10, MP10-04, MP34-03, UP02-047, UP02-060, VP02-06, VS05-08
SAKAMOTO, K., MP01-03, MP01-10, MP01-16, MP13-06, MP21-05, VP01-13, VP01-14
SAKAMOTO, S., MP32-01, UP01-052, VS05-04
Sakamoto, S.-i., MP33-01
SAKATA, R., MP31-07, VP02-07
Sakatani, T., UP01-035
SAKO, T., UP02-118
Sakuma, T., MP33-12
Sakurai, T., UP01-047
Sakuyama, G., MP33-01
Saleh, F., MP11-04, MP21-13
Salim, H., MP31-02, MP31-04, MP31-06
Salkini, M., MP31-16
Salkini, M.W., MP09-16
Samani, A., UP02-082
Sammon, J., MP13-08
Sammon, J.D., MP26-07, VP06-13
Samzadeh, M., MP02-10
Sancaktutar, A.A., BR04-04
Sanchez, E., MP12-15, MP12-16
Sanchez Hurtado, M., VS01-06
Sanchez Margallo, F.M., VS01-06
Sanchez-Salas, R., MP03-05, MP08-03, MP08-10, MP15-06, MP15-10
Sandner, S., VP04-01
SANEFUJI, H., UP02-024
Sangkum, P., VS11-02
Sankari, B., MP01-09, MP12-06, MP12-13, UP01-109
SANO, F., MP31-07, VP02-07
Sano, T., VS09-04, VS12-01
Santillana, J.M., VS01-05, VS14-10
Santos, R., MP05-07, MP05-08
Sarhangnejad, R., MP06-02, MP11-08
Sarica, K., MP05-05
Sarkissian, C., BR04-08, VS10-04
Sarkissian, C.L., VS14-08
SASAKI, H., MP11-07, MP17-13, MP26-08, UP01-066
SASAKI, S., UP01-107, UP02-098, VP05-04
Sasaki, T., UP01-056
SASAKI, Y., UP01-089, UP02-050, VP04-11
Sassa, N., UP02-109, VP06-01
Satasivam, P., BR01-09
Satisvatam, P., MP32-07
Sato, F., MP12-12, MP20-12, UP01-106
Sato, K., MP33-12
Sato, R., MP12-12, VP06-15, VS11-08
Sato, Y., UP02-058, VS14-03
Satoh, S., MP12-14
SATOH, T., MP06-10, UP01-094, UP01-098, UP02-028
SATOH, Y., UP01-057, UP02-028, UP02-046
SAWADA, K., UP01-101
SAWADA, N., UP01-048
SAWADA, Y., MP11-02, MP33-04, UP01-029, UP01-030, UP01-031, UP01-032, UP01-055, UP02-110, VS07-01
Sawaiker, M., MP20-15
Sawczuk, I., MP08-14, MP21-06
Sawczuk, I.S., MP28-08
Sawyer, M.D., MP09-10
Sazawa, A., MP03-11, MP31-11, VS05-05
Scales, C.D., VS10-02
Schade, G.R., BR03-10, MP15-13, MP22-06
Schaeffer, E.M., MP17-08
Schatloff, O., MP17-14, MP17-15, MP17-16, MP28-04, MP28-05, MP28-06, VS03-04, VS03-05, VS13-05
Scherpbier, A.J., MP02-04, MP02-16
Scherpbier, A.J.A., MP02-05
Schettini, M., MP19-07, MP19-15, MP22-14, MP24-01, MP30-09, MP32-03, UP01-001, UP02-013
schettini, m.m., MP14-11, MP25-15
Schilling, D., MP27-04
Schitcu, V., VP02-14, VP06-03
Schitcu, V.V., VS03-06, VS11-03
Schlaifer, A.E., MP07-01, MP14-09, MP28-01, MP29-02, MP34-05, MP34-06, VS09-05, VS10-03
Schmitges, J., MP08-01, MP13-08
Schout, B.M.A., MP02-05, MP02-16
Schroeder, G.T., MP14-10, MP21-14
Schulkes, A., BR01-10
Schulze, M., MP25-10
Schuricht, A.L., MP17-10
Schwartz, B.F., BR01-15, BR03-02, BR03-08, BR04-11
Schwartz, J., MP13-02, MP17-04, VP05-08, VS16-05
Schwentner, C., MP27-04, MP27-05
Sciuto, R., MP32-11, VP03-15
Scoffone, C., VP04-14, VP04-16
Scott, E., MP18-15
Secasan, C., VP04-09
Secin, F., MP08-03, MP08-10, MP15-06
See, W., MP16-12, MP31-10
Seguchi, K., UP01-040, UP01-092
Sehgal, S.S., MP26-14, MP26-15
Seibold, J., MP27-05
Seitz, M., VP06-05
Sejima, T., MP06-15, VS03-01
SEKI, M., MP15-08, UP01-111, UP01-116, UP02-090
Seki, N., MP31-12, VP05-13
Sellaturay, S., MP30-03
Sellaturay, S.V., MP05-16
Sengupta, S., BR01-09, UP02-020
Senthil, K., MP14-16, MP25-01, VS05-01, VS06-05, VS06-06, VS11-04, VS11-06, VS11-07, VS16-01
Seo, J., UP01-034, UP01-065
Seo, J.T., UP01-028, UP01-034
Seo, J.W., MP12-07
Seo, S.I., MP01-02, MP10-15, MP14-06, UP01-063, UP01-064
Seo, Y., UP02-021, UP02-040
Sepulveda, F., MP31-02, MP31-04, MP31-06
Serrano, M., VS08-03
Sethi, K., BR01-10
Sgrò, E., VS05-06
Shah, H., MP23-01
Shah, K., MP16-13, MP31-09
Shah, N., MP02-11, MP09-11, MP19-03, MP19-06, MP29-15
Shah, N.C., MP05-17
Shah, O., MP10-03, MP30-11
shah, T.T., UP02-082
Shah, V., VP03-09
Shahab, N., VP05-13
Shahrour, K., MP18-14, MP18-15, MP18-16, MP19-11
Shaida, N., MP09-11
Shaikh, N., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-071, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Shakhssalim, N., MP11-01
Shalaby, S., MP29-01
Shamsuddin, A., MP24-14
Shan, C., MP18-17, MP18-18, MP30-14, MP30-15, MP34-15, UP02-064
Shapiro, M., MP21-09
Shapur, N., BR03-13
Shariat, S., MP08-01, MP13-08, UP01-074
Shariat, S.F., MP17-03, UP01-071, UP01-082, UP01-083
Sharifi, S., VS15-08
Sharifiaghdas, F., MP11-08
Sharif-Tabrizi, A., MP05-11, MP05-19
Sharma, L., MP10-13
Sheikhi, Z., BR03-09
Shen, C.-H., MP34-13
Shen, J., MP14-14
Shen, K.-H., UP01-084
Shen, Y., VP03-05
Shergill, I., VS10-09
Shergill, I.S., MP09-07, MP22-05
Sherman, V., BR02-12
Shestani, T., MP22-14, MP24-01, MP30-09, UP01-001, UP02-013
Sheth, S., BR02-02, BR02-04, BR02-07, BR02-08, BR04-03
Shevchuk, M., MP32-13, UP01-070
Shibata, M., MP02-12
Shichiri, Y., VS09-04, VS12-01
SHIGA, Y., UP02-023, UP02-121
Shigemura, K., UP02-012, VP05-06
Shigeta, M., MP26-04
Shih, J., VP03-09
Shim, B., UP02-057
Shim, K., UP02-021, UP02-040
Shima, M., MP33-11
Shimizu, N., UP01-009
Shimizu, T., MP11-02, UP01-029, UP01-030, UP01-031, UP01-032
Shimizu, Y., MP07-10, UP01-035
Shin, D., MP28-08
Shin, J.H., UP02-019
Shin, T., MP12-12, UP01-106
Shinmei, S., MP13-15
Shinoda, K., UP01-086, VS15-03
Shinohara, N., MP31-11, VS05-05
Shintani, T., UP02-037
Shinya, U., MP29-12
Shiomi, K., VP02-10
SHIOTSUKA, Y., UP02-118
Shipilov, A.S., MP06-09, MP06-11, MP29-05
Shirai, S., MP16-07
Shiraishi, K., MP27-02
Shiraishi, T., UP02-111
Shirakawa, H., MP11-02, UP01-030, UP01-032
SHIROKI, R., MP17-13, MP26-08, UP01-066
SHISHIDO, T., MP01-05, MP33-13, UP01-006, UP02-052
shistani, t., MP19-07, MP19-15, MP32-03
SHITARA, T., UP02-008, UP02-027, VP05-12
Shitinohe, T., UP02-099
SHOJI, K., MP01-13, MP02-12, MP07-06
Shoji, S., MP15-07
SHOKEIR, A., MP18-05
Shokeir, A.A., MP10-10
shokohiyan, m., UP02-007
Shon, J., UP02-054
SHOO, T., UP02-024
Shore, D., MP19-01
Shoss, J.M., VP06-02
Shouji, K., MP25-16
Shrotri, N., UP02-020, UP02-079, UP02-106
ShuDong, Z., MP01-11, MP12-05, MP31-14
SHUIN, T., UP02-118, MP28-18
Shyam, S., MP13-08
Sicuro, O., VS05-06
Siddiqui, M., MP05-13
Siddiqui, M.M., MP05-19
Sieberer, M., MP33-07
Siegel, J., MP02-11
Siegel, Y., BR02-12
Siegel, Y.I., MP10-01
Siener, R., MP05-05
Sighinolfi, G., BR02-09
Sighinolfi, M.C., BR02-09, MP24-11
Silberstein, J., MP01-03, MP01-16
Silberstein, J.L., MP01-10
Silverman, P., MP15-11, MP32-04
Simforoosh, N.I., MP02-10, MP06-02, MP11-01, MP11-08, VS07-08
Simmons, W.N., BR04-13, BR04-14, MP15-16, VP04-02
Simoes, A., UP02-106
Simone, G., MP15-09, MP26-03, MP26-06, MP32-11, VP03-15, VS01-02, VS01-03, VS01-04
Sindhwani, P., MP04-06, VS07-03
Singh, G.P., UP02-101
Singh, V., MP06-04, MP06-17, MP20-11, UP01-036
Singla, M., VP05-15
Sinha, R.J., MP06-04, MP06-17, MP20-11, UP01-036
SIROKI, R., MP11-07
SISIDO, T., UP02-044
Sivalingam, S., UP02-062
Sivaraman, A., MP17-14, MP17-15, MP17-16, MP28-04, MP28-05, MP28-06, VS03-04, VS03-05, VS13-05
Skarecky, D., MP28-02
Skolarikos, A., MP22-03
Slezack, J., MP17-06
Sloan, D.A., UP02-043
Smith, A., MP23-01, MP23-09, MP23-17, VS10-01, VS15-06
Smith, D.L., MP07-01, MP07-02, MP14-07, MP14-09, MP14-10, MP21-14, MP28-01, MP29-02, MP34-05, MP34-06, MP34-09, VS09-05, VS10-03
Smith, I., MP06-08
Smith, J.C., MP14-09, MP14-10, MP21-14, MP34-05
Smith, N.B., VP04-02
Smith, P., MP02-01, MP02-02, MP02-03, MP02-06, MP02-07, MP02-08, MP02-09, MP03-07, MP28-09, MP31-08, VP03-01, VP03-02, VP03-07, VP06-07, VP06-14
Smith, P.G., BR03-16
Soames, R., MP02-13
Soar, J., MP03-06
Sobol, I., MP08-14
Soda, T., VS14-09
Soeda, A., UP02-084
SOEJIMA, H., MP16-07, UP01-105
SOEJIMA, K., MP16-07, UP01-105
Sofer, M., MP18-07, MP18-10, MP21-08, MP29-04
SOGA, N., UP02-111
SOH, J., MP07-16, MP16-03
SOH, S., MP06-10, VP06-15, VS11-08
Soleimanipour, P., VS05-09
Soltani, M.H., MP02-10, MP06-02, VS07-08
Somani, B., MP01-15, UP02-055
Somani, B.K., MP02-01, MP02-08, MP02-09, MP09-12, MP12-01, MP16-08, MP30-10, MP30-12, VP03-01, VP03-02, VP03-07, VP06-12, VP06-14
Song, H.-Y., BR03-11, BR03-12
Song, K., MP29-03
Song, K.H., UP02-019
Song, M., UP01-065
Song, P.H., MP24-16
Sooriakumaran, P., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-071, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Soria Galvez, F., VS01-06
Sotelo, R., VS03-02, VS03-03, VS04-06, VS11-01, VS11-10, VS13-01
Spaliviero, M., MP04-07, MP04-09, MP08-11, MP28-16
Spana, G., MP26-16, MP32-15, UP01-112, UP02-127, UP02-128
Spencer, D., MP05-17
Spernat, D., MP04-16
Spinelli, M., VS11-01
Sriprasad, S., MP05-16, MP21-08, MP24-12, MP30-03
Srivastava, A., MP08-04, MP08-08, MP17-03, MP32-13, UP01-070, UP01-071, UP01-074, UP01-079, UP01-081, UP01-082, UP01-083
Sroka, R., BR01-03
Stamatakis, L., MP12-15, MP12-16
Stanasel, I., MP05-02
Stanescu, F., MP22-09, MP22-11, MP22-15, VP03-13
Stanton, P., MP09-14
Starke, N.R., VP06-02
Stein, R., MP20-13, MP26-16
Stein, R.J., MP32-15, UP01-112, UP02-127, UP02-128
Steinberg, D., BR03-13
Steiner, R., VP03-14
Stenzl, S., MP27-05
Stenzl, A., MP27-04
Sterling, J., MP32-13
Stief, C.G., BR01-03, VP04-01, VP06-05
Stifelman, M., MP10-03
Stifelman, M.D., MP31-17, VP02-13
Stoffel, F.S., VS07-05
Stoianovici, D., VP03-08
Stolka, P.J., MP09-05, MP09-06
Stolzenburg, J.-U., BR03-01, MP06-13, MP12-08, MP12-09, MP12-11
Stransky, P., MP11-13
Strijbos, W.E.M., MP29-09
Strom, K.H., MP04-06, VS07-03
Stroup, S.P., MP01-03, MP01-10, MP01-16, VP01-13, VP01-14
Stuurman, R., VP04-13, VP04-16
Styn, N.R., MP15-15, MP22-06
Su, C.-C., UP01-084
Su, C.-K., MP08-02
Su, D., MP08-12, MP28-07
SUAREZ DE LIS, L., VS05-07
Subotic, S., MP07-15, MP25-10, VS17-08
SUGATA, A., UP01-006, UP02-044, UP02-052, UP02-089
SUGIHARA, T., MP24-06, UP01-104
SUGIMOTO, M., UP01-013, UP01-058, UP02-119
SUGIMURA, Y., UP01-008, UP02-111
Sugino, Y., MP07-10, UP01-035
SUGITA, A., UP01-042, UP01-053, UP01-098
SUGITANI, A., MP11-07
Sugiyama, T., UP01-005, UP02-088
Suh, L., UP02-104
Sukumar, S., MP26-07, VP06-13, VS02-05
Sul, C.K., UP02-019
Sumitomo, M., UP01-040, UP01-092
Sun, M., MP08-01, MP13-08, VP05-02
Sundaram, C.P., MP01-14, MP06-16, MP11-05, MP11-06, MP31-01
Sung, G.T., MP03-19
Sung, G.(M.), UP02-063
Sung, H.H., MP01-02, UP01-063, UP01-064
Sung, L.H., MP05-10, UP02-004
Suntharasivam, T., MP05-17
Sutton, R., MP05-06
SUYAMA, S., UP01-101
SUYAMA, T., MP32-01, UP01-052
SUZUKI, A., UP01-061, UP02-017, UP02-051, UP02-083
SUZUKI, H., MP27-12
Suzuki, K., UP01-104
Suzuki, T., UP02-088
SUZUKI, Y., UP01-046, UP02-011
Swash, M., MP09-03
Sweet, R.M., VP03-05
Sydnor, M.K., MP21-11
Syrkin, A.S., UP02-042
T, U., VP06-09
TABATA, K., UP01-098
Tabata, K.-i., UP01-094
Tabatabaei, S., MP04-10
Tabibi, A., MP11-01, MP11-08
Tada, Y., MP31-12
Tadashi, M., MP26-04
Tadtayev, S., UP02-041
Tadyadev, S., MP32-10
Tae-Kon, T.-K., UP01-072
Taghavi, R., BR02-03
Taghavi, s.R., UP02-007
Taguchi, I., VP06-11
Taguchi, K., VP05-04
Tailly, G.G., MP24-08
Tait, C., MP09-08
Takagi, S., MP28-11
TAKAGI, T., MP31-03, MP31-05, UP01-055, UP01-059, UP01-062
TAKAHARA, K., UP01-099
Takahashi, K., UP01-023
Takahashi, M., UP01-092
Takahashi, S., MP33-12, UP01-049, VP02-08
TAKAHASHI, W., UP01-100
Takahasi, W., UP01-027
Takaki, H., UP02-111
TAKAMOTO, H., UP02-118
Takashi, K., MP28-18
Takashi, S., MP29-12
Takayama, T., UP01-005, UP02-088
TAKAZAWA, R., UP02-091
TAKEDA, K., UP01-008, UP01-012
TAKEDA, M., UP01-015, UP01-043, UP01-048
Takeda, T., UP01-075, UP01-077, UP01-086, UP01-113
Takei, M., VP05-13
Takenaka, A., MP06-15, MP08-04, MP08-08, MP17-03, UP01-070, UP01-071, UP01-074, UP01-079, UP01-082, VS03-01
TAKESHI, N., UP01-069
Takeuchi, A., MP31-12
TAKEUCHI, I., UP01-010
Takimoto, K., VS09-04, VS12-01
TAKIUCHI, H., UP01-101
Takizawa, N., VP01-09
Talamini, M., VP01-13, VP01-14
Tam, H.M., VS15-05
TAMADA, S., UP01-060
Tamaddon, K., BR03-06, BR03-07
TAMAKI, G., UP01-045
TAMBO, M., UP02-052, UP02-089
Tamir, I., BR04-08, VS10-04
TAMUBO, M., UP02-044
TAMURA, K., MP28-18, MP33-02, UP02-118
Tan, G., UP01-081
Tan, Y.H., MP07-14
Tan, Y.K., BR01-04, BR01-11, MP03-01, MP06-14, MP07-17, MP21-16, MP26-05
TANABE, K., MP11-02, MP26-04, MP31-03, MP31-05, UP01-029, UP01-030, UP01-031, UP01-032, UP01-055, UP01-059, UP01-062
Tanagho, Y., MP03-09
Tanagho, Y.S., MP25-12
Tanaka, H., UP02-099
TANAKA, K., MP28-13, UP01-039, UP01-043, UP01-097, UP01-102, UP02-009, UP02-012, VP02-11, VP05-06
Tanaka, N., UP01-075
Tanaka, T., UP01-049, UP01-060
TANBO, M., MP33-13, UP01-006, UP02-089
Tanda, H., UP02-058
Tang, B., MP02-13, MP02-14, MP02-15
Tang, J., UP02-034
Tanigawa, F., UP01-100
TANIGUCHI, J., UP02-023, UP02-121
Taniguchi, N., MP03-11
Tannus, M., MP31-02, MP31-04, MP31-06
Tantirangsri, N., MP13-14
TAPIA, M., VS05-07
Tasaki, S., UP01-040
Tasi, Y.-C., VS14-05
TATENUMA, T., MP31-07, VP02-07
Tatsugami, K., MP31-12
Tatsugawa, A., MP02-12
Tau, A., MP25-11
Taue, R., UP02-037
Taverna, G., MP19-16, MP23-12, VS10-05
Tay, K.J., MP15-12
Tay, Y.K., MP18-12
Taylor, B., MP08-14, MP21-06
Taylor, E.N., UP02-034
Taylor, E.R., BR01-15, BR03-02, BR03-08, BR04-11
Tazaki, S., UP01-092
Teber, D., MP25-10
Tefekli, A., MP31-15, UP02-115
Teichman, J., MP19-01, MP30-11
Teijima, J., MP25-16
TEISHIMA, J., MP01-13, MP02-12, MP07-06, MP13-15, UP02-094, UP02-095
Teodorovich, O.V., MP15-14, UP02-022, UP02-042, UP02-069
Teplov, A.A., MP15-14
Terachi, T., MP15-07, MP25-02, MP26-04
TERANISHI, J.-I., UP01-068
TERAO, H., UP02-045, UP02-048, UP02-086, UP02-092
Tewari, A., MP08-04, MP32-13, UP01-070, UP01-074, UP01-079, UP01-081
Tewari, A.K., MP13-10
Thamboo, T., VP01-05
Thanos, A., MP22-03, UP02-105
Thng, C.H., MP15-12
Thomas, A., MP17-06, VP03-11, VP04-13, VS05-03
Thomas, A.A., MP14-15
Thomas, R., MP06-16, MP16-10, MP32-07
thomas, r., UP02-033
Thueroff, S.F.M., MP15-01, MP15-02, MP15-05, MP20-02, UP02-102
Thummar, H., BR02-02, BR02-04, BR02-07, BR02-08, BR04-03
Tian, Y.-F., UP01-037
Tian, Z., MP13-08
Tilki, D., VP06-05
Timoney, A., MP03-06
Tintila, B., VP03-06, VP06-03
Tintila, B.B., VS03-06, VS11-03, VS14-07
Tiong, H.Y., VP01-05, VP02-09
Tisnado, J., MP21-10, MP21-11
TIZAKI, R., MP28-12
Tjiam, I.M., MP02-04, MP02-05, MP02-16
Tligui, M., UP02-039, UP02-081
Tobe, M., UP02-058
Tobis, S., VP02-02
Todenhoefer, T., MP27-04
Todenhöfer, T., MP27-05
TOKATLI, Z., MP19-14, VP04-12
TOKIWA, S., MP32-05
TOKUDA, Y., UP01-057, UP02-046
Tomaszewski, J.J., MP19-11
TOMITA, Y., UP01-047, UP02-059
Tomiyama, N., VS14-03
TOMOE, H., MP25-17, VP02-10
Tomohiro, I., MP33-12
Toncheva, G., BR04-10, BR04-12, BR04-14, VP06-16
Toyohiko, W., MP29-12
TOZAWA, K., MP25-09, UP01-050, UP01-087, UP01-096, UP01-103, UP01-107, VP05-04
Trabulsi, E.J., MP17-12
Tran, S., MP13-02
Tran, S.N., VS16-05
Traxel, E.J., MP25-12
Traxer, O., MP30-10, UP02-039, UP02-076, UP02-081, VP03-11, VP04-13, VP04-14, VP04-16, VS10-06
Trimmer, C., MP26-05
Trinh, Q.-D., MP08-01, MP13-08, MP26-07, VP05-02, VP06-13, VS02-05
Trock, B., MP14-12
Tsai, S., VP06-10
Tsai, T.-F., VP02-16
Tsai, Y.-C., MP06-12, VP01-10, VP02-05
Tsai, Y.-S., UP02-036
Tsamandas, A., BR01-14
Tsang, W.C., VP01-05
Tsivian, M., MP08-15, MP08-16
Tsopanoglou, N., BR01-02
Tsounapi, P., MP06-15
Tsu, J.H.L., MP04-08
Tsu, J.-W., MP14-15
Tsuchida, T., UP01-015
Tsuchihashi, S., MP07-09
Tsuchiya, N., MP12-14
Tsugawa, M., MP29-12
TSUJI, Y., UP01-061, UP02-017, UP02-051, UP02-083
Tsujii, T., UP02-091
TSUJIMURA, K., MP25-17
TSUJITA, Y., UP02-110
Tsukamoto, T., UP01-049, VP02-08
Tsukimori, S., UP02-108
TSUMURA, H., UP02-028
TSUNEMORI, H., UP02-119
TSURU, N., UP01-104
Tuason, M.Z., MP07-03
Tufek, I., MP08-13, MP16-11, MP30-05, VS08-06, VS09-02, VS11-10, VS16-06, VS16-07
Tujimura, K., VP02-10
Turgeman, Y., MP09-17
Turkbey, B., MP32-06, UP02-112, UP02-113, VP03-09
Turkevich, V.G., MP15-12
Tushima, N., VP02-10
Tyler, P., MP02-01, MP02-02, MP02-06, MP02-07, VP03-01, VP03-02, VP03-07
Tytler, P., MP02-03, MP02-08, MP02-09, MP03-07, MP31-08, VP06-14
Tzortzis, V., MP04-17
UBAI, T., MP28-11, UP01-069, UP01-090, UP01-099
Ubre, A., MP13-01, UP01-080
Uchida, K., UP02-058, UP02-111
UCHIDA, T., MP15-07, UP01-013, UP01-058
UCHIMOTO, S., UP01-069
UDO, K., UP01-057, UP02-046
UEDA, N., UP01-012, UP01-013, UP01-058, UP02-119
UEHARA, H., MP28-11, UP01-090, UP01-099
UEMATSU, K., UP02-061
UEMURA, H., UP01-009, UP01-041, UP01-054
UENO, M., UP02-110
UETSUKI, H., UP02-119
Ukimura, O., MP15-11, MP16-16, MP32-04, VS02-02, VS02-04, VS14-02, VS14-03
UMEMOTO, Y., MP25-09, UP01-050, UP01-103, VP05-04
Umeoka, S., MP09-13
Ungbhakorn, P., VS12-04
UOZUMI, J., UP01-057, UP02-046
Uppot, R.N., MP21-15
URA, K., UP01-089, UP02-050, VP04-11
Urge, T., MP11-13
Uson Gargallo, J., VS01-06
Usui, Y., MP15-07
UTSUMI, T., MP27-12
V, E., VP06-09
Vaessen, C., MP28-15
Valero, R., MP17-14, MP17-15, MP17-16, MP28-04, MP28-05, MP28-06, VS03-04, VS03-05, VS11-10, VS13-05
VALVERDE, I., VS05-07
van Batavia, J., MP19-05
Van Cleynenbreugel, B., MP23-02
van der Vleuten, C.P., MP02-05
van Leeuwen, T.G., BR01-12
van Merrienboer, J.J., MP02-16
van Velthoven, R.F., MP15-03
Varga, B., MP24-12
Varghese, K., MP19-06
Varshney, A.K., VP05-14, VP05-15
Vaughn, N.P., VS02-01, VS08-05
Velasquez Ossa, D.A., VS01-01, VS05-02, VS07-07, VS09-03, VS16-02
Velásquez Ossa, D.A., VS07-06
Velásquez Ossa, J.E., VS01-01
Velásquez, J.G., VS07-07, VS09-03, VS16-02
Vemulapalli, P., VS02-06
Veneziano, D., VS05-06
Venkatesh, R., UP02-043, VS02-08
Vera, D., MP21-05
Verma, P., MP02-17
Verma, S., MP21-04, VP03-10
Vijverberg, P.L., MP18-09
Villamizar, J.M., VS01-05
Villavicencio, H., VS01-05, VS01-09, VS01-10, VS08-03, VS09-06, VS14-10, MP22-04
vincenti, g.g., MP14-11
Vint, R., MP09-12
Viprakasit, D.P., MP09-10
Virdi, J., MP22-13, MP32-10
Vora, A., MP22-08, UP01-085, UP02-112, UP02-113
Voth, K.D., MP17-02, MP17-08
Vrettos, T., BR01-14
Wada, Y., UP01-027, UP01-100
Wadhwa, P., VP05-14
Wagner, H.J., MP14-09, MP29-02, MP34-05, MP34-06
Wahjudi, I.N., MP14-09, MP29-02, MP34-05, MP34-06
Waingankar, N., MP23-09
WAKATABE, Y., UP01-091, UP02-008, UP02-027, VP05-12
Walicki, M., MP28-03
Wallace, A., MP21-05
Wallis, M.C., MP30-16
Walter, M., VS17-08
Walter, S., MP14-04
Walther, S., BR01-03, VP04-01
Wan, B., MP01-01, MP01-04, MP01-08, MP20-03
Wang, A.J., BR04-10, BR04-12, BR04-13, BR04-14, MP15-16, MP18-08, MP18-09, MP29-06, VP04-02, VP06-16, VS10-02, VS13-03
Wang, C., MP19-02, MP19-17,MP22-16, MP27-06, MP29-10, MP29-11, MP29-14, MP32-02, MP32-08, MP34-12, UP01-038, UP02-003, UP02-015, UP02-016, UP02-030, UP02-031, UP02-067, UP02-075, UP02-077, UP02-078, VP06-16
Wang, J., MP01-01, MP01-04, MP01-08, MP20-03
Wang, J.C., UP01-037
Wang, Q.X., MP04-05, MP11-14, MP14-02, MP14-03, MP18-03, MP18-04, MP23-08, MP30-07
Wang, S.-M., UP01-108
Wang, S.-S., MP08-02
Wang, X., MP01-06, MP07-07, MP07-08, MP34-12, UP01-038, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Wang, X.C., MP04-05, MP11-14, MP14-02, MP14-03, MP18-03, MP23-08
Wang, Y., MP04-05, MP19-02, MP19-17, MP22-16, MP29-10, MP29-11, MP29-14, MP32-02, MP32-08
Wang, Z., BR03-03, BR03-05
Waples, M., MP16-12, MP31-10
Ward, M., MP16-09, UP01-016
WATANABE, A., UP01-114
WATANABE, K., UP01-011
WATANABE, S., MP16-07, UP01-105
Watkiss, J., BR01-06, BR01-07, BR01-08
Watson, G., MP02-17
Watsuji, T., UP02-107
Webster, K., BR04-08, VS10-04
Wei, D., MP01-04, MP20-03
Weizer, A., MP11-15
Wen, S.-C., UP01-115
Wen, X.-Q., MP22-10, VP06-04
Wendt-Nordahl, G., MP23-14, MP23-18, MP33-08, VP03-14, VP06-06
WENTAO, H., MP20-05, MP28-17
Werntz, R.P., MP31-01
Wezel, F., MP25-13
Wheat, J.C., MP15-15
White, M., MP20-13, MP26-16
White, M.A., MP32-15, UP01-112, UP02-127, UP02-128
Wiesenthal, J.D., MP23-10, MP24-05, MP24-09
Wiklund, P., MP17-03, UP01-071, UP01-082, UP01-083
Williams, H., UP02-112, UP02-113
Williams, Jr., J.C., MP05-12
Williams, S., BR03-06, MP17-06
Williams, S.K., VP04-08
Wilson, J., MP17-09
Wirth, G., MP08-07
Wiseman, O., MP09-11, MP19-03, MP19-06, MP29-15
Wiseman, O.J., MP05-17
Witjes, J.A., MP02-04, MP02-05, MP02-16
Woldrich, J., MP01-03, MP01-10, MP01-16, VP01-13, VP01-14
Woldrich, J.M., MP13-06
Wolf, Jr., J.S., BR02-13, MP06-16, MP11-15, MP19-10
Wolf, J.S., MP06-05
Wolters, J.P., MP20-14, VP01-04
Won, A.C.H., BR04-09, UP02-071
Wong, C., MP04-07, MP04-09, MP08-11, MP28-16
Woo, H., MP04-10, MP04-11, MP04-19
Woo, H.H., BR03-16, MP04-14, MP04-15, VP05-09
Woo, S.H., MP08-12, MP19-08
Woo, S.H.Woo, MP28-07
Wood, B., UP02-112, UP02-113
Wood, B.J., MP32-06
Wood, C., MP14-14
Wood, K., MP05-02, MP05-09, MP05-14, MP05-15
Woodall, A., MP05-01
Woodward, T., MP03-06
Wootton, C.W., UP02-043
Wu, C., MP05-06
Wu, F., VP01-05
Wu, G., MP01-06, MP07-07, MP07-08, MP20-16, MP21-07, MP21-09, VP02-01, VP02-02, VS12-02, VS12-03, VS16-03, VS17-03, VS17-04, VS17-05, VS17-07
Wu, K., MP18-17, MP18-18, MP30-14, MP30-15, MP34-15, UP02-064
Wu, W.-J., UP01-115
Wu, Y., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Wuerstle, M., MP14-15, MP17-06
Wyler, S., BR03-14, MP04-12, MP04-20, MP07-15, MP25-10, VS17-08
Xiangfu, Z., MP23-11
Xiao, H., UP02-070
Xiao, H.-J., MP22-10, VP06-04
Xiao, L., BR01-10
Xiao, R., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
XIN, G., MP20-05, MP28-17
XINGQIAO, W., MP20-05, MP28-17
Xu, A., MP20-04, MP20-07, MP20-17, UP02-001, VP01-12, VP05-03
Xu, H., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Xu, K., UP02-001
Xu, S., MP32-06
Xu, Y., UP02-001
Xue, W., MP23-02
Xue, Y., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Yaegashi, H., UP02-035
Yagi, H., VP06-15, VS11-08
Yagihashi, Y., VS14-09
Yakoubi, R., MP20-13, MP32-15, UP01-112, UP02-127, UP02-128
YAMADA, D., UP02-061
YAMADA, H., MP10-04, MP34-03, UP02-047, UP02-060
YAMADA, S., MP27-07, UP01-007
YAMADA, Y., UP01-008
Yamagishi, A., UP01-047
Yamaguchi, A., UP02-076, VP05-13
Yamaguchi, K., MP33-12, UP01-102, VP05-06
YAMAGUCHI, R., MP15-04, MP32-12
YAMAGUCHI, T., MP33-13, UP02-089, UP02-052
Yamaguti, R., MP33-03
YAMAKADO, K., UP01-008, UP02-111
Yamamoto, A., MP14-13, UP02-072, UP02-114
Yamamoto, H., MP02-07, MP02-08, MP04-10, MP09-03, MP33-06
YAMAMOTO, R., UP02-023, UP02-121
YAMAMOTO, S., UP01-101
Yamamoto, T., UP02-109
YAMAMOTO, Y., UP01-009, UP01-012, UP02-118
Yamanaka, M., MP14-13, UP02-114
Yamanaka, Y., MP33-12
YAMANE, S., UP02-049
YAMANISHI, T., MP32-01, MP33-01
Yamao, Y., VP06-11
Yamasaki, K., VP02-04
Yamasaki, M., MP12-12
Yamashita, H., UP01-094
YAMASHITA, K., MP25-17, VP02-10
YAMASHITA, M., UP01-058, UP02-119
Yamauchi, T., MP30-01, MP30-06
Yamazaki, T., UP02-120
yan, w., MP22-18, MP23-04
Yanaihara, H., MP03-10, VP02-06, VS05-08
yanbo, w., MP18-01, MP18-02, MP22-17, MP22-18, MP23-03, MP23-04, MP23-05, MP23-06, MP30-08, UP02-005
Yang, B., UP01-112, UP02-127, UP02-128
Yang, C.-K., MP08-02, MP13-10
Yang, C.-r., MP29-13
Yang, C.-Y., MP34-13
Yang, H., UP01-065
Yang, J., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Yang, S.S., VS14-05
Yang, S.S.-D., MP06-12, VP02-05
Yao, A., MP06-15, VS03-01
YAO, M., MP31-07, VP02-07
Yao-Chou, T., VS17-02
Yarmohamadi, A., UP02-006, UP02-007, UP02-014, UP02-073, UP02-093
Yarmohammadi, A., VS05-09
Yasar, B., BR04-04
YASUI, T., MP25-09, UP01-103, VP05-04
Yasumizu, Y., UP01-086, VS15-03
Yasunaga, H., MP24-06
Yates, J., MP08-14, MP16-01, MP16-02, MP16-17, MP28-08, VS17-01
Yates, J.K., MP21-06, MP21-09, VS16-08
Ye, J., MP11-03, MP11-11, MP11-12, MP16-04
Yeh, C.-H., VP02-16
Yeh, H.-C., UP01-115
Yehiely, R., MP18-07
Yehyely, R., MP18-10
Yi, H., MP03-13, MP03-14
Yin, C., MP03-08, MP20-09, MP27-03
Yip, S.K.H., VS15-05
Yokomizo, A., MP31-12
Yokota, N., VP02-10
YOKOTA, S., MP25-17
YOKOYAMA, H., MP27-13, MP27-16, UP01-014, UP02-023, UP02-121
Yokoyama, T., UP02-108
Yonesi, M., UP02-014
YONEYAMA, T., UP01-046, UP02-011
Yong, D., MP08-15
Yoo, D.H., MP24-02
Yoon, J., MP10-09
Yoon, S.J., UP02-056
YOSHIDA, K., MP02-19, MP03-18, UP01-042, UP01-062, VP03-04
Yoshii, H., UP01-040, UP01-092
YOSHII, S., UP01-011
Yoshimizu, A., VS07-02
YOSHIMURA, K., MP07-10, MP09-13, UP01-009, UP01-035, UP01-041, UP01-054, UP02-120
Yoshino, Y., UP02-109, VP06-01
Yoshizumi, T.T., BR04-10, BR04-12, BR04-14, VP06-16
You, D., BR03-12, MP14-08
You, J.H., MP05-10
Younger, A., BR03-04
Yu, D.-H., UP01-003
Yu, H.S., MP12-07
Yu, M.-Y., VS07-04
Yuan, J., MP18-17, MP18-18, MP30-14, MP30-15, MP34-15, UP02-064
Yuan, Y., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
YUCEL, S., MP25-06, MP32-14
yuchuan, h., MP22-17, MP23-06, UP02-005
Yuen, J.W., BR04-01
YUKI, H., MP20-12, UP01-106
YUMURA, Y., UP01-068
YuQing, L., MP08-05, MP19-09, MP23-15, MP23-16, MP27-15
Zafar, H., MP02-03
Zagazechev, A.V., MP29-05
ZAKOJI, H., UP01-015
ZAKOUJI, H., UP01-048
Zakri, R., MP11-10
Zand, F., MP23-07
Zandegiacomo, S., MP19-16, MP23-12, VS10-05
Zappavigna, C., MP30-11
zare, z., MP23-07
Zavaglia, B., MP30-11
Zelichenko, G., MP09-17
Zelinski, N., MP09-14
Zenbutsu, S., BR01-05
Zeng, G., MP18-17, MP18-18, MP30-14, MP30-15, MP34-15, UP02-064
Zhai, Q.J., MP21-04, VP03-10
Zhan, H.-L., MP22-10
Zhang, G., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Zhang, H., MP22-10, UP02-070, VP06-04
Zhang, L., UP01-038
Zhang, Y., MP01-01, MP01-04, MP01-08, MP20-03, MP22-10, UP02-070, VP06-04
Zheng, S., MP20-04, MP20-07, MP20-17, UP02-001, VP01-12, VP05-03
Zhong, P., MP15-16, VP04-02
Zhong, W., MP18-17, MP18-18, MP30-14, MP30-15, MP34-15, UP02-064
Zhong, X., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07
Zhou, X.-F., MP22-10, VP06-04
Zhu, G., MP01-01, MP01-04, MP01-08, MP20-03
Zhu, J., VS15-04
Zhumkhawala, A.-A., VS05-03
Ziaee, A.M., MP11-01
Ziaee, M.S., VS05-09
Ziaee, S.A.M., MP06-02, MP11-08
Zigman, O., BR04-08, VS10-04
Zilberman, D., MP08-15, MP08-16
Zimmermann, R., MP33-07
Zipunnikov, V., VS13-06
Zolfaghari, A., BR02-14
Zondervan, P.J., MP03-02, MP16-05
Zorn, K.C., MP08-01, MP13-08, VP05-02, VP05-16
Zou, X., MP01-06, MP07-07, MP07-08, VS12-02, VS12-03, VS17-03, VS17-04, VS17-05, VS17-07