
Abstract
Background and Purpose:
Considering the anatomic proximity of the internal iliac lymph nodes and the pelvic plexus, it may be expected that more extensive pelvic nodal dissection is associated with an increased risk of damage to the small pelvis neural and vascular structures. We evaluate whether nodal dissection is associated with functional outcome after robot-assisted radical prostatectomy (RARP).
Patients and Methods:
In a series of 798 RARP procedures, 325 (40.7%) patients underwent a lymph node dissection. Continence, sexual function, and lower urinary tract symptoms (LUTS) were assessed using the International Consultation of Incontinence Questionnaire short form (ICIQ)-SF), International Index of Erectile Function-15, and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ)-PR25 questionnaires before and at 6 months intervals after RARP.
Results:
Preoperative ICIQ-SF, IIEF-15, and PR25-LUTS scores were similar for men with and without nodal dissection. Normal postoperative erectile function (IIEF-EF >24) at 6 months was reported by 1.7%, 9.1%, and 50.4% of men with no, unilateral, and bilateral nerve preservation and normal preoperative erectile function. All domains of the IIEF-15 score showed a negative correlation with the number of removed lymph nodes. In 70 of 325 (21%) cases with nodal dissection, more than 10 nodes were removed. Men with more than 10 nodes removed had lower IIEF-15 domain scores compared with men with 1 to 10 removed lymph nodes. The postoperative ICIQ-SF and PR25-LUTS scores were not associated with extent of nodal dissection. Nodal metastases were found in 5.9% and 15.7% of men with ≤10 nodes and >10 nodes removed (P=0.005). In a multivariate analysis, extent of fascia preservation (FP-score), preoperative IIEF-EF, and number of removed nodes were the strongest independent predictors of postoperative erectile function recovery.
Conclusion:
More extensive nodal dissection was associated with impaired postoperative sexual function recovery but not continence and voiding function after RARP, independent of preoperative function and nerve preservation.
Introduction
Nodal dissection is recommended for the obturator, external iliac, internal iliac, and common iliac region up to the ureter vessel crossing. Data on prostate lymph node landing sites showed that 25% of nodes were found in the internal iliac region. 8 Including the internal iliac lymph node in the dissection, Menon and associates 9 showed increased detection in nodal metastases. When nodal metastases are present, these are to be found in the internal iliac region in 20% of cases. 10 Nodes at the level of the internal iliac vessels lay in close proximity to the hypogastric plexus that contains both sympathetic and parasympathetic innervation to the small pelvis. 11 –14 Dissection of the nodes at the level of the internal iliac vessels, therefore, may damage the pelvic plexus, which may result in impaired functional recovery after prostatectomy.
Although many factors associated with postprostatectomy erectile function have been studied, the role of more extended nodal dissection on sexual function and voiding recovery received little attention. Many series on prostatectomy and erectile function (EF) do not address the role of nodal dissection. 15 –18 Patel and colleagues 19 did not find lymph node dissection to be associated with pentafecta (among which erectile function) outcome after RARP with limited nodal dissection. Bianchi and coworkers 20 found no difference in EF after bilateral nerve-sparing open prostatectomy in men with and without extended nodal dissection. The influence of extent of nodal dissection in cases with less nerve preservation is unknown, however. Interestingly, combining mesorectal excision with extended pelvic lymph node dissection for rectal cancer reduced the patients' ability to maintain erections sufficient for intercourse postoperatively. 14,21,22
Voiding problems are frequently reported after prostatectomy, 23 and men with preoperative complaints may benefit from prostatectomy. 24,25 No data on the effects of nodal dissection on postprostatectomy voiding complaints were presented. In extensive small pelvis surgery for rectal diseases, voiding problems do occur in up to half the patients. 26 These findings suggest that (para)sympathetic innervation may be damaged during more extensive pelvic node dissection, in particular in the internal iliac region.
We studied the effects of pelvic node dissection on voiding and sexual function after prostatectomy for prostate cancer using standardized questionnaires with special attention to the extent of nerve preservation and nodal dissection.
Patients and Methods
Robot-assisted radical prostatectomy (RARP) was performed in 798 consecutive men between January 4, 2006 and January 2, 2011 using the da Vinci S Surgical System (Intuitive Surgical, Sunnyvale, CA). Two surgeons with experience of at least 50 robot-assisted procedures were included in this series. Nodal dissection was performed when the risk of nodal metastases was more than 10%, as estimated by the Briganti 27 nomogram. The extent of nodal dissection comprised the obturator and external iliac region during the first 3 years, with the growing insight into the role of more extensive nodal dissection since 2009 patients underwent a more extensive dissection. Besides dissection of the obturator and external iliac nodes, the nodes in the internal iliac and common iliac region up to the ureter also were removed.
Prostatectomy was performed in an antegrade fashion. In case of fascia preservation (FP), the pedicle vessels were clipped. The extent of FP was dependent on the patients' wish to preserve erectile function and the extent of tumor as assessed by biopsy location and preoperative imaging (transrectal MRI and/or transrectal ultrasonography). The Santorini plexus was suture ligated, and the urethra was transsected with cold scissors. The extent of FP was scored using the FP-score as described earlier. 28 We preferred the FP score over the distinction of interfascial or intrafascial preservation based on earlier observed superiority of this score.
All men filled out the International Consultation on Incontinence Short Form (ICIQ-SF) (urinary continence), International Index of Erectile Function (IIEF-15) (sexual function), 29 and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ)-PR25 (prostate specific complaints) questionnaires before prostatectomy and at 6 months intervals after the procedure.
One week postoperatively, cystography was performed, and the transurethral catheter was removed when the bladder-urethra anastomosis was leak free. Patients were counseled for pelvic floor exercises and were offered phosphodiesterase type-5 inhibitors for penile rehabilitation.
Definitions
Normal EF was defined as an IIEF score (questions 1, 2, 3, 4, 5, and 15 of the IIEF-15 questionnaire) of more than 24. Urinary continence was defined as no involuntary urine loss and no pad use and an ICIQ-SF score of 0. The median preoperative EORTC-QLQ-PR25 lower urinary tract symptoms (LUTS) domain score (12) was taken as normal value for LUTS.
Statistical analysis
EF and urinary continence were evaluated at 6 months and 1 year postoperatively. The Mann-Whitney U nonparametric test was used for comparison of questionnaire results at the different time intervals. Multivariate binary logistic regression analysis was performed to study the clinical characteristics to predict postoperative outcome for urinary continence, LUTS, and sexual function. PASW-SPSS version 18.0 was used for statistical analysis.
Results
Patients
Men who underwent a nodal dissection were significantly older, had a higher preoperative prostate-specific antigen level, higher biopsy Gleason score, higher clinical T stage, and a lower FP-score (Table 1). The mean number of removed lymph nodes in 325 men was 9 (1–28). Nodal metastases were found in 27/325 (8.3%) cases. One, 2 to 5, and >5 positive nodes were found in 16, 10, and 1 patients. Men who had more than 10 nodes resected had a higher percentage of nodal metastases when compared with men with fewer than 10 nodes resected (15.7% vs 5.9%, P=0.005).
LND=lymph node dissection; preop=preoperative; PSA=prostate-specific antigen; FP=fascia préservation; IIEF=International Index of Erectile Function; ICIQ-SF=International Consultation of Incontinence Questionnaire-short form; LUTS=lower urinary tract symptoms.
Preoperative functions
The preoperative scores for IIEF-15, ICIQ-SF, and PR25-LUTS domain were similar for both groups (Table 1). In 81% of men, a preoperative ICIQ-SF score of 0 was reported. The most frequently reported preoperative condition of urine loss (ICIQ-SF question 4) was: “It leaks when you have finished urinating and are dressed” (6.1 %). In 310 (38.8%) men, normal preoperative EF (IIEF-EF score >24) was reported. Age at surgery was significantly associated with preoperative IIEF-EF (r=−0.382, P=0.0001) and PR25-LUTS domain score (r=0.104, P=0.007). The number of removed lymph nodes was not correlated with the preoperative IIEF-EF or PR25-LUTS score.
Functional outcome
Postoperative questionnaire results were obtained from 78% and 74% of men at 6 and 12 months. Response rate was similar for men with and without nodal dissection. The postoperative ICIQ-SF score was not significantly different for men with and without node dissection at 6 and 12 months postoperatively. The most frequently reported circumstance of involuntary urine loss was: “Leaks when you cough or sneeze,” in 62.2% and 6.7% of men at 6 and 12 months.
At 6 and 12 months, 82% and 69% of responding men reported erectile dysfunction (IIEF-EF<25). Of men with normal preoperative EF (IIEF-EF >24), this was 73% and 48%, respectively. Voiding problems (PR25-LUTS score >12) were observed in 30% and 27% of men at 6 and 12 months.
Since from 2009 onward, a more extensive nodal template was used, we compared the patients from before and after 2009 and observed a significantly lower IIEF-15 overall score (P=0.030), lower intercourse (P=0.012), and overall satisfaction (P=0.014) in the group of men who underwent a nodal dissection after 2008 while age and FP score were similar for both groups.
Prediction of functional outcome
At 6 months, the number of removed lymph nodes was inversely correlated with IIEF-EF score, IIEF-OF (orgastic function), IIEF-IS (intercourse satisfaction), IIEF-SD (sexual desire), and IIEF-OS (overall satisfaction) but not with the ICIQ-SF score for incontinence, or the PR25 LUTS domain score (Fig. 1). Besides the number of removed lymph nodes, several clinical characteristics were associated with postoperative functions (Table 2). A higher FP score was associated with a higher postoperative IIEF-EF and lower PR25-LUTS score. In a multivariate analysis to predict EF recovery at 6 months, the preoperative IIEF-EF score, FP score, and number of removed lymph nodes showed independent correlation (Table 2). In men with normal preoperative EF (IIEF-EF >24), those men who underwent a more extensive node dissection (>10 nodes removed) were twice more likely to experience erectile dysfunction at 6 months after the procedure (4.3% vs 17.8%). Age was the only characteristic that was associated with continence outcome (Table 2).
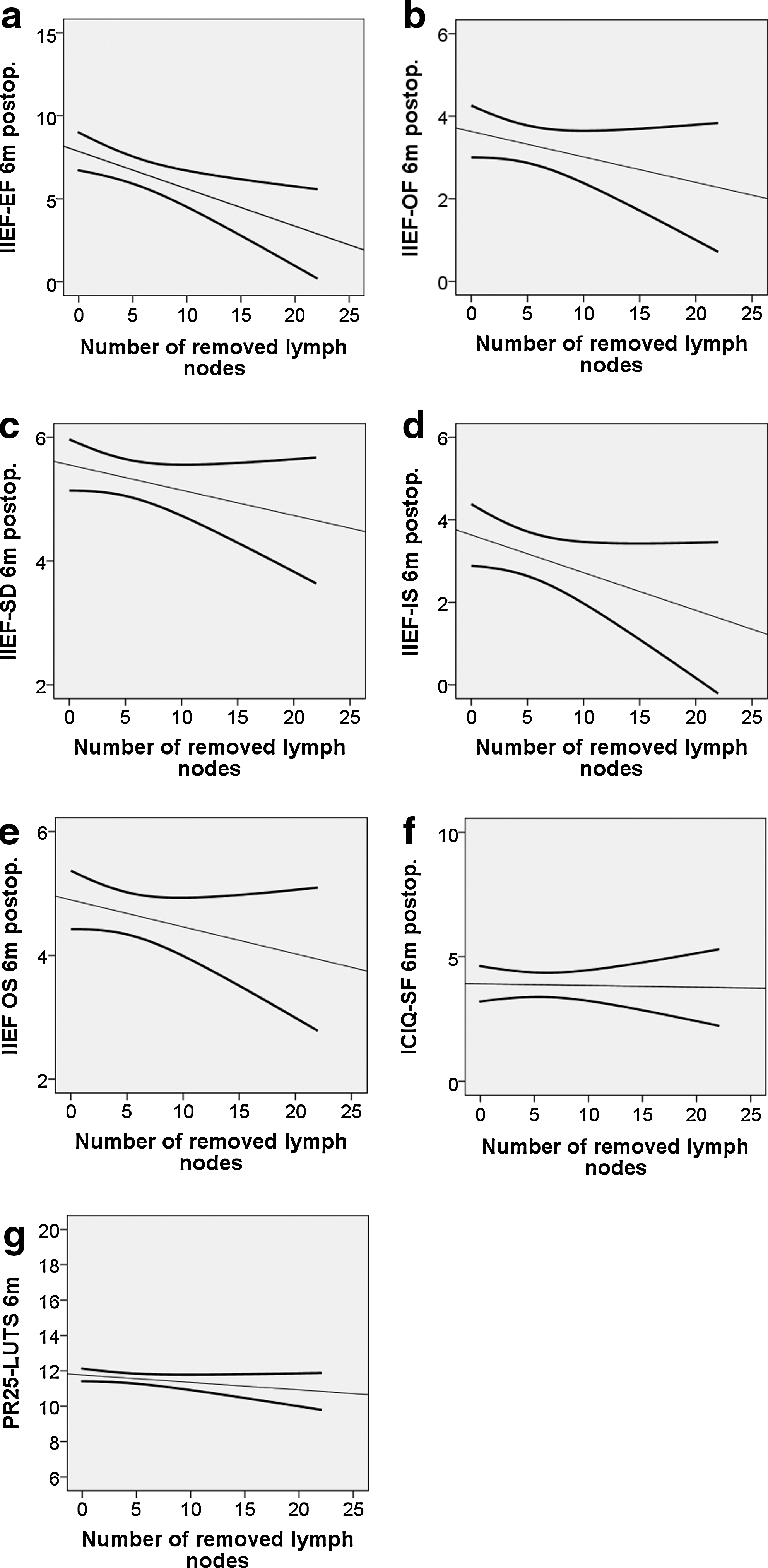
Relation of mean International Index of Erectile Function (IIEF-15) domain scores:
CI=confidence interval; ICIQ-SF=International Consultation of Incontinence Questionnaire-short form; FP=fascia preservation; L=limited; E=extended.
CI=confidence interval; FP=fascia preservation; International Index of Erectile Function; PSA=prostate-specific antigen; L=limited; E=extended.
Discussion
In this outcome assessment study, the extent of nodal dissection was associated with sexual function outcome as assessed by the patient-administered IIEF-15 questionnaire score at 6 and 12 months post-RARP, but not with post-RARP urinary continence or LUTS. In a multivariate analysis, the number of removed lymph nodes was of additional predictive value for postoperative EF recovery (IIEF-EF >24) to preoperative IIEF-EF score and extent of FP.
EF after prostatectomy is dependent on patient age and extent of nerve preservation. 18 Recent studies report improved EF preservation for robot-assisted procedures when compared with historical controls. 30,31 The option of more extensive periprostatic tissue preservation provided by improved intraoperative view by the surgical robotic system may contribute to this. A randomized comparison between laparoscopic and robot-assisted prostatectomy showed comparable oncologic and continence outcome, whereas the reported EF was superior for the robotic approach. 32
Limited nodal dissection (≤10 nodes removed) did not clearly impact on postoperative EF recovery. On the other hand, men who underwent a more extensive nodal dissection (>10 nodes) were less likely to recover sexual function. Until 2009, nodal dissection comprised mainly the obturator lymph region with, when present, removal of nodes on the external iliac vein. More extensive dissection included the internal iliac and common iliac region. We postulate that the resection of the internal iliac nodes may have contributed to damage of the nerves running lateral to the bladder in the hypogastric plexus (Fig. 2) 13 The hypogastric nerve plexus was shown to carry both sympathetic and cholinergic nerves and control erectile, ejaculatory, and bladder neck functions. 33 Data from our analysis, however, suggests that even within the group of men, the number of nodes removed was a stronger predictor of functional outcome than the presence or absence of internal node dissection. This finding may reflect the unclear and variable anatomic locations of the hypogastric plexus.
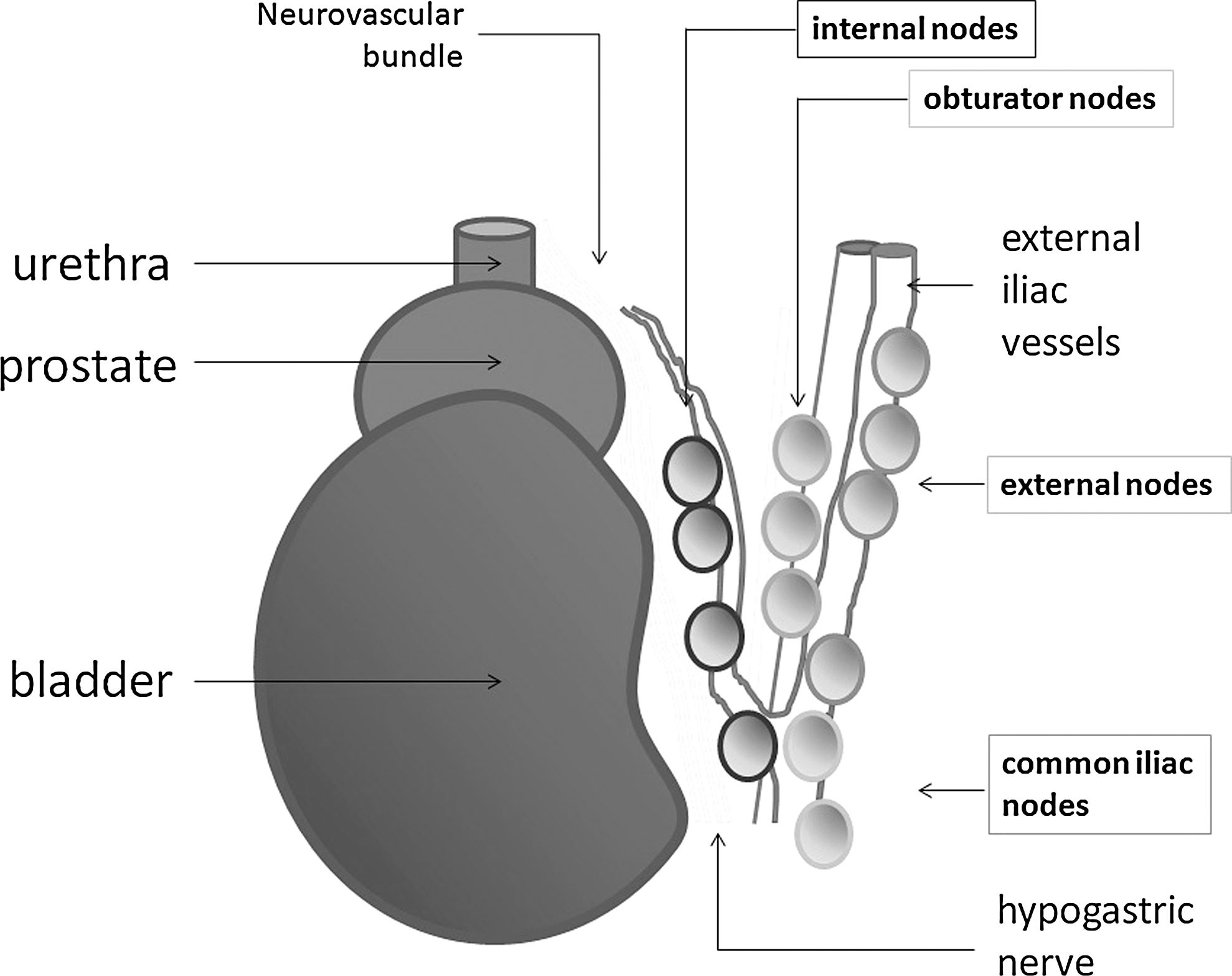
Anatomy of nodal regions.
Minimizing damage to the neural tissue in the internal iliac region seems of most importance for sexual function recovery as was suggested by the findings of Tewari and coworkers. 34 Nerve preservation improved the possibility of achieving orgasm postprostatectomy. These data are supported by our findings that show a decreased score for postoperative orgasmic function (IIEF-OF) in men with less nerve preservation and in those with more extensive nodal dissection.
The exact cause of neural damage to the hypogastric plexus remains to be established. Because recovery did occur with longer follow-up, full transection damage seems less likely. Although monopolar cauterization is avoided during the nodal dissection traction to the bundle when exposing the internal iliac region by traction to the bladder may have resulted in neuropraxia. Research is needed to confirm our findings and improve methods to preserve neurovascular function.
In earlier studies, age was found of predictive value for both EF and continence outcome. The fact that the preoperative IIEF-EF score was strongly correlated with age in our series may have caused age to drop out as an independent prognostic variable in the multivariate analysis.
Interestingly, in the current analysis, urinary continence as assessed by the ICIQ-SF was neither correlated to the number of resected lymph nodes nor with the extent of FP. This observation is in line with other reports that did not find nerve preservation of predictive value for continence recovery. 35,36
Based on our data, several recommendations can be made. We confirm earlier data that a more extensive nodal dissection is associated with an increased detection rate of nodal metastases. Until data from randomized studies become available, it will remain unclear if a more extensive nodal dissection can improve survival. Patients should be informed on the reduced sexual function recovery when extended nodal dissection is performed in combination with prostatectomy.
A limitation of the present analysis is the variation in nerve preservation. Men who underwent a lymph node dissection had less nerve preservation as assessed by the FP score. This is probably caused by the higher tumor stage in this group that influenced the decision making on nerve preservation. Although a multivariate analysis was performed that showed nodal dissection to be of additional predictive value of postoperative EF recovery, other factors interacting may be present. A prospective randomized setting would be needed to study the effects of nodal dissection independent of these unknown factors.
Second, in the presented population, the mean number of removed nodes increased over the study period. Because the exact learning curve for optimal nerve preservation is unknown, it may be that nerve preservation actually improved with experience. This and the increase in number of removed nodes over time would actually reduce the effect of nodal dissection on EF recovery. One may postulate, therefore, that the effect of nodal dissection on EF recovery is actually underestimated in the current series.
Finally, inherent with the use of mailed questionnaires, follow-up of some nonresponders is lacking. Because nonresponders were equally distributed among men who had a nodal dissection and those who did not, we think that this bias may be minimal.
Conclusion
In this Dutch single center RARP series, it was shown that more extensive nodal dissection reduced sexual function recovery. Other factors predictive of reduced EF recovery in the current population were reduced preoperative IIEF-EF score and a lower FP score. No effect of nodal dissection on continence recovery and LUTS was observed. A more extensive nodal dissection was associated with a higher node positive rate.
Footnotes
Disclosure Statement
No competing financial interests exist.