
Abstract
Background and Purpose:
Whether the retroperitoneal approach (RA) or the transperitoneal approach (TA) for performing laparoscopic donor nephrectomy (LDN) in kidney transplant donors is less invasive is unclear. In this study, we compared the clinical outcome and systemic inflammatory marker levels between RA and TA to assess surgical invasiveness.
Patients and Methods:
We enrolled 105 donors (RA: 41, TA: 64) who underwent LDN in our hospital. Evaluation of both approaches included comparison of conventional clinical parameters and preoperative, immediate postoperative, and 1-day postoperative levels of the following circulating inflammatory cytokines: Tumor necrosis factor-α, interleukin (IL)-1β, IL-6, IL-8, IL-10, and IL-12p70.
Results:
The frequency of right nephrectomy being performed was significantly lower in the TA than in the RA group (3/64 vs 12/41, P<0.001). Other clinical parameters in the TA group, including the frequency of surgical complications and incidence of delayed graft function, were comparable to those in the RA group. Immediate and 1-day postoperative mean serum IL-6 levels were significantly higher in the RA than in the TA group (P=0.023 and 0.044, respectively). The 1-day postoperative mean serum IL-10 level was also significantly higher in the RA than in the TA group (P=0.041). Meanwhile, the mean serum IL-6 and IL-10 levels were not associated with surgical duration or estimated intraoperative blood loss.
Conclusions:
Conventional clinical parameters related to surgical invasiveness were comparable in both approaches, thus indicating that both LDN approaches were similar and equally effective as minimally invasive procedures. The clinical significance of the higher postoperative mean serum IL-6 and IL-10 levels in the RA group remains to be clarified in a future study.
Introduction
The transperitoneal approach (TA) for LDN may be favored by a greater number of surgeons than the retroperitoneal approach (RA) because of the wider working space and the greater number of anatomic landmarks with TA. Some surgeons, however, prefer RA 4,5 because TA may increase the risk of intra-abdominal organ injuries and gastrointestinal complications. 6 In addition, the surgeons who select RA for LDN expect that the limited dissection and visceral manipulation in RA may decrease postoperative recovery time and pain compared with TA. 4 There is no proven scientific basis for this speculation, however. Which approach is less invasive for living kidney transplant donors has not yet been established.
Surgical invasiveness is usually evaluated not only on the basis of clinical parameters, including surgical duration, estimated intraoperative blood loss, analgesic dose, and time needed to return to work, but also by the quantification of systemic biologic responses to surgery, including metabolic, hormonal, and cytokine responses. 7 –9 To the best of our knowledge, however, there have been no reports that compare the surgical invasiveness of RA and TA in terms of systemic inflammatory marker levels, including circulating cytokine levels, to date.
LDN is an optimal model for evaluating surgical invasiveness by measuring circulating cytokine levels because renal transplant donors are not affected by disease status. In this study, the clinical outcome and systemic inflammatory marker levels of RA and TA for LDN were compared to assess the surgical invasiveness of these two approaches.
Patients and Methods
In total, 105 donors who underwent LDN in our hospital between October 2003 and March 2010 were enrolled in this study along with the recipients who received kidneys from these donors. Of these, 41 donors underwent LDN via RA and 64 via TA. We changed the standard approach from RA to TA in June 2005 in our hospital; TA for LDN is technically easier than RA because of the wider working space and the greater number of anatomic landmarks. We selected RA only when donors had a history of upper intra-abdominal surgery.
Donor nephrectomies were performed by multiple surgeons (RA group: n=9, TA group: n=12) with various degrees of experience. All procedures were performed or mentored/guided by two senior surgeons (NT and TH). Donors in both groups were compared with regard to background, perioperative clinical data, incidence
To evaluate the glomerular filtration rate (GFR) of the donors, an intravenous bolus injection of technetium-99m diethylenetriamine pentaacetic acid was administered with the donor positioned under the gamma camera. The estimated GFR of the donors was evaluated using the formula for calculating GFR in Japanese patients. 10
Preoperative, immediate postoperative, and 1-day postoperative blood samples from all donors in the TA group and 15 recent donors in the RA group were obtained. Serum samples were stored at −80°C until measurement. Preoperative, immediate postoperative, and 1-day postoperative white blood cell (WBC) count, C-reactive protein (CRP), and the six kinds of inflammatory cytokines: Tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1β, IL-6, IL-8, IL-10, and IL-12p70 were also measured. Cytokine levels were measured using a BD FACS-Calibur™ flow cytometer (BD, Franklin Lakes, NJ) and the Cytometric Bead Array Human Inflammatory Cytokines Kit (BD Biosciences, San Jose, CA).
Written informed consent was obtained from all donors for possible use of the materials for research. This study was approved by the Ethics Review Board of Akita University Hospital.
Surgical techniques
During LDN via TA, a hand port device, the LapDisc® (Hakko Co. Ltd., Nagano, Japan), was placed for kidney removal through a vertical midline or pararectal incision approximately 7 cm in length at the level of the umbilicus (Fig. 1a). A working 12-mm port was placed in the LapDisc and used as a medium to transfer instruments until kidney removal. The third and fourth ports were placed at the positions indicated in Figure 1a. Most surgical procedures were purely laparoscopic; hand assistance was necessary at the time of kidney removal. The renal artery was secured with a Multifire Endo TA™ 30 stapler (Covidien Japan Inc, Tokyo, Japan) and then transected. The renal vein was also stapled using the same device and then divided. The isolated kidney was retrieved through the hand port manually or using a retrieval bag.
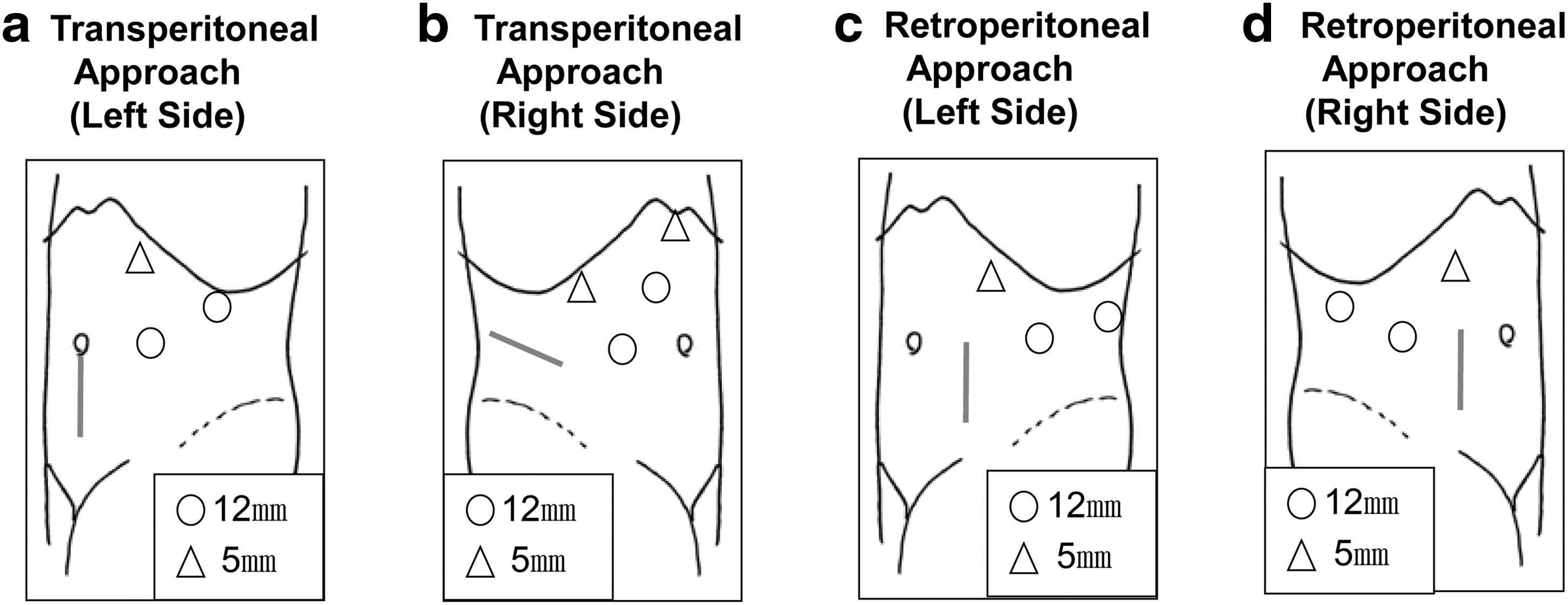
Schema of kidney removal and port sites.
LDN via TA for the right kidney is almost identical to left LDN. The two differences are as follows: In right TA, a subcostal flank incision is made using the muscle-splitting method to place the hand port device (Fig. 1b). In addition, a fourth 5-mm trocar is inserted below the xiphoid process to retract the liver.
The surgical technique of LDN via RA in our hospital has been described previously (Figs. 1c, 1d). 11,12 Briefly, a 12-mm camera port was placed at the tip of the 12th rib along the anterior axillary line after dilating the retroperitoneal space. Under the pneumoretroperitoneum created by carbon dioxide insufflation at 10 mm Hg, second (12 mm) and third (5 mm) ports were placed at the positions indicated in Figures 1c and 1d. A hand port device, LapDisc or Gelport® (Applied Medical, Rancho Santa Margarita, CA), was placed through a 7-cm pararectal abdominal skin incision (Figs. 1c, 1d) to facilitate instrument and hand-assisted manipulation during surgery. Hand-assisted manipulation was temporally used to dissect the upper kidney pole and dorsal plane of the renal pedicles.
The renal artery was secured with triple proximal clips and divided. The renal vein was transected with an EndoGIA® Universal stapler (US Surgical, Norwalk, CT), while the kidney was held with the hand. The kidney was then removed manually using the hand port device. Carbon dioxide insufflation at a constant pressure of 8 to 10 mm Hg was used in the intra- and retroperitoneal spaces in all laparoscopic procedures examined in this study.
Statistical analysis
Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) ver. 16.0J (IBM Japan, Tokyo, Japan). Student t test was used for parametric continuous variables, and the Mann–Whitney U test was used for nonparametric continuous valuables. The chi-square test was used for categorical variables. Correlations between various parameters were analyzed using the Spearman rank correlation test. The data were expressed as mean±standard deviation, and differences at P<0.05 were considered statistically significant.
Results
Preoperative characteristics of the donors
Table 1 shows the preoperative characteristics of the donors in both groups. The donors were not significantly different in terms of age, sex, body mass index, and preoperative renal function in the RA and TA groups. Similarly, no significant difference was found in terms of parameters mentioned above between the TA group and the 15 recent donors of the RA group (data not shown). The frequency of right nephrectomy was significantly lower in the TA than in the RA group (3/64 vs 12/41, P<0.001).
SD=standard deviation; RA=retroperitoneal approach; TA=transperitoneal approach; M/F=male/female; BMI=body mass index; e-GFR=estimated glomerular filtration rate; S-Cr=serum creatinine level; L/R=left kidney/right kidney.
Intra- and postoperative clinical outcomes of the donors and recipients
Table 2 shows the intra- and postoperative clinical outcomes of donors and recipients in both groups. There were no significant differences between the groups in terms of surgical duration, estimated intraoperative blood loss, warm ischemia time, and postoperative donor renal function. Similarly, no significant difference was found in terms of parameters mentioned above between the TA group and the 15 recent donors of the RA group (data not shown).
SD=standard deviation; RA=retroperitoneal approach; TA=transperitoneal approach; WIT=warm ischemia time; TIT=total ischemia time; e-GFR=estimated glomerular filtration rate; POD=postoperative day(s); S-Cr=serum creatinine level.
The incidences of DGF (1 [6.7%] in the 15 recent donors of the RA group) and SGF were comparable between the groups. With regard to early graft function, no significant difference was noted between the groups. Only one recipient lost the graft within 3 months after transplantation. This patient received a kidney from a donor who underwent LDN via RA. Severe acute antibody-mediated rejection developed in this patient after ABO blood group-incompatible transplantation, and he lost the graft 2 months after surgery.
Perioperative systemic inflammatory markers of the donors
Table 3 shows the results of the perioperative systemic inflammatory marker (WBC, CRP, and the six kinds of circulating inflammatory cytokine levels) measurements of the donors of both groups. Immediate and 1-day postoperative mean serum IL-6 levels were significantly higher in the RA than in the TA group (148.9±136.8 pg/mL vs 78.1±97.1 pg/mL, P=0.023 and 136.0±256.4 pg/mL vs 41.6±66.5 pg/mL, P=0.044, respectively). The 1-day postoperative mean serum IL-10 level was also significantly higher in the RA than in the TA group (P=0.041). When the results of the left side were analyzed independently, both the immediate postoperative mean serum IL-6 and IL-10 levels were significantly higher in the RA than in the TA group (RA group: n=10, TA group: n=61; IL-6 levels: 176.6±151.7 pg/mL vs 79.8±99.2 pg/mL, respectively, P=0.024; IL-10 levels: 113.3±125.8 pg/mL vs 44.7±50.1 pg/mL, respectively, P=0.037). No significant differences in other cytokine levels were found between the two groups even when the results of the right and left sides were compared independently.
SD=standard deviation; RA=retroperitoneal approach; TA=transperitoneal approach; WBC=white blood cells; POD=postoperative day(s); CRP=C-reactive protein; TNF-α=tumor necrotic factor-α; IL=interleukin.
In addition, no significant associations were observed between mean serum IL-6 or IL-10 levels and surgical duration or estimated intraoperative blood loss and between the two cytokine levels (data not shown).
Complications
No donor procedures needed conversion to open surgery, and no donors needed blood transfusion or reoperation in this series. According to the Clavien classification system, all complications in this series were classified as Grade I. 13 In the TA group, one diaphragmatic injury (1.6%) occurred and was repaired laparoscopically without installation of a chest drainage tube. Atelectasis developed in two (4.9%) donors in the RA and three (4.7%) donors in the TA group, which spontaneously improved. The frequency of wound site infection did not differ statistically between the groups (2 [4.9%] in the RA group and 6 [9.4%] in the TA group). Sensory paralysis in the left thigh developed in one female donor in the RA group without obvious cause, but the symptom spontaneously disappeared 1 week after surgery. No serious complications, such as death, intraoperative organ injuries, or graft malfunction, occurred.
Discussion
LDN has been widely recognized as a minimally invasive procedure for living kidney transplant donors compared with ODN. 1 Whether the RA or TA is less invasive, however, has still not been clearly defined. Several clinical studies comparing TA procedures with hand-assisted RA procedures revealed that the mean surgical duration in the latter was shorter than that in the former; in addition, TA has certain other drawbacks. 14,15 Most of the TA procedures in these reports, however, were purely laparoscopic. Also, these reports were based on nonrandomized studies using small study samples. 14,15 The surgical duration of hand-assisted procedures tends to be shorter than that of purely laparoscopic procedures. 16 Other clinical studies involving a relatively large number of cases, however, demonstrated no differences between approaches in terms of clinical outcome and safety. 5,17
In this study, intra-abdominal organ injuries or gastrointestinal complications did not develop in any donors. One recent report documented a relatively low incidence of these complications with TA procedures. 18 These intra-abdominal complications, however, reportedly occur even during retroperitoneal nephrectomy procedures. 19
According to previous reports 5,17 and the results of the present study, no obvious differences can be identified between patients undergoing LDN via RA and TA in terms of clinical outcome, surgical invasiveness, donor recovery, and donor safety. 5,17 Similarly, in a prospective randomized clinical trial of RA vs TA for laparoscopic radical nephrectomy in renal cancer patients, the safety, recovery time, and clinical outcome were comparable for both approaches, although surgical duration in the RA group was shorter than that in the TA group. 20 The authors stated that the choice of laparoscopic approach for nephrectomy should depend on the skill and preference of individual laparoscopic surgeons. 20
Finally, we compared the surgical invasiveness of RA and TA by measuring intraoperative systemic biologic responses to LDN. Surgical intervention induces systemic inflammatory metabolic and endocrine responses. Postoperative systemic homeostasis and the recovery process are both influenced by various secreted hormones and cytokines. The strength of these systemic biologic responses is reportedly proportional to the severity of surgical stress. 7,21 Therefore, measurement of circulating inflammatory cytokine levels has often been used as an objective evaluation of surgical invasiveness. 7 –9,22,23 When comparing open vs laparoscopic surgery with regard to the inflammatory cytokine levels, many studies reported significantly lower levels in patients who underwent laparoscopic surgery compared with those who underwent open surgery, suggesting that laparoscopic surgery is less invasive than open surgery. 7 –9,22,23 To the best of our knowledge, only two reports have assessed cytokine responses in laparoscopic and open nephrectomy procedures using a porcine model, 22,23 but there have been no such reports in humans.
In this study, immediate and 1-day postoperative mean serum IL-6 levels were significantly higher in the RA than in the TA group. The 1-day postoperative mean serum IL-10 level was also significantly higher in the RA than in the TA group. In addition, when limited to the left side, the immediate postoperative mean serum levels of both IL-6 and IL-10 were significantly higher in the RA than in the TA group. IL-6 promotes inflammatory reactions more strongly and quickly than does CRP and is considered a very useful indicator of surgical invasiveness because of its stability in serum. IL-10 is known as a suppressor of inflammatory reactions. Serum IL-10 level reportedly correlates with estimated intraoperative blood loss and IL-6, 24 and serum IL-68 and IL-1024 levels are reportedly proportional to the severity of surgical stress. No significant associations were found, however, between the mean serum IL-6 or IL-10 levels and surgical duration or estimated intraoperative blood loss and between the two cytokine levels in this study.
No significant differences in TNF-α, IL-1β, IL-8, and IL-12p70 were found between the groups. TNF-α and IL-1β are induced by cytoclasis immediately after surgery, before IL-6. Because serum levels of both cytokines peak several hours postoperatively, 7,8 differences in cytokine levels may not have been detected at any of the sampling points set in this study. IL-8, which is known as a neutrophil chemotactic factor, has been reported to be higher in open procedures than in laparoscopic surgery. 9 Many investigators, however, have reported no difference in IL-8 levels between open and laparoscopic surgical procedures. 7,25 Although one study reports that IL-12 secretion from monocytes was inhibited by surgical stress, 26 assessment of surgical invasiveness by measuring IL-8 or IL-12 levels may not be common.
The results of this study indicated that TA was less invasive than RA from the viewpoint of inflammatory cytokine responses. “Creating the retroperitoneal space” by stripping the peritoneum can potentially give rise to traumatic peritonitis and hence promote local cytokine production. 17 Subsequently, inflammatory cytokines enter the peripheral blood and induce cytokinemia after secretion in the surgical field. 8 Differences in systemic inflammatory responses, however, such as differences in IL-6 and IL-10 levels, between the two groups in this study were not reflected in the conventional clinical outcome and parameters. Thus, our results indicated that both the RA and TA approaches for LDN were similar and equally effective as minimally invasive procedures. Future studies will determine whether certain IL-6 or IL-10 levels have any significant unseen clinical impact on postoperative recipient kidney function or donor recovery.
The incidence of DGF in this series was relatively high compared with that in previous reports (0%–11%). 1,2,5,27 The DGF incidence, however, is affected not only by procedural issues, but also by other variables such as female donor–male recipient relationship, recipients' general conditions, unrelated highly mismatched donors, and prolonged cold and total preservation times. 27
This clinical study has some limitations, including the retrospective nature and the relatively small sample size (only the 15 recent RA donors were evaluated for comparing systemic inflammatory marker levels). In addition, this study is not a randomized, controlled trial. The possibility of selection bias cannot be denied, because 12 donors of the RA group (since June 2005) had a history of upper intra-abdominal surgery. Differences in the number of surgeons (RA group, n=9; TA group, n=12) and hormonal responses were also not evaluated. Finally, frequency of right nephrectomy was significantly lower in the TA than in the RA group (Table 1). Frequencies of right nephrectomy in LDN ranging from 3.5% to 56% have been reported. 11,27 –29 Because early experiences with right LDN via TA were reportedly associated with high incidences of renal vein thrombosis and graft loss, 30 many centers have refrained from performing right LDN via TA. Careful donor selection during the induction period of TA may have influenced the decreased proportion of right LDN via TA, although our donor selection criteria remained unchanged over the course of the entire study period. Therefore, a randomized, prospective, large-scale clinical study is needed to confirm our results.
Conclusions
In this study, conventional clinical parameters related to surgical invasiveness were not significantly different between TA and RA for LDN, while the inflammatory cytokine response suggest that TA was less invasive than RA. While the results indicate that both approaches for LDN were similar and equally effective as minimally invasive procedures, the clinical significance of the higher postoperative mean serum IL-6 and IL-10 levels in the RA group remains to be clarified in a future study.
Footnotes
Acknowledgments
The authors thank Ms. Y. Mitobe, Ms. Y. Izumida, and Ms. T. Kakizaki for their technical assistance and for their help in sample preparation. The authors would like to thank Enago (
Each author's specific contributions to the work:
Mitsuru Saito is a main investigator and participated in the surgeries. M. Saito designed the study, collected and analyzed data from patients, and wrote the article.
Norihiko Tsuchiya participated in the surgeries and contributed to research designing, data analysis, and writing the article.
Shintaro Narita, Teruaki Kumazawa, Shinya Maita, Kazuyuki Numakura, Takashi Obara, Hiroshi Tsuruta, Takamitsu Inoue, Yohei Horikawa, and Shigeru Satoh participated in the surgeries and collected data from patients.
Tomonori Habuchi designed and organized the study, and wrote the article. T. Habuchi participated and was a main mentor in the surgeries.
Disclosure Statement
No competing financial interests exist.