
Abstract
Background and Purpose:
Laparoscopic repair of ureteropelvic junction obstruction is now the standard of care at many institutions. The objective of this study is to compare costs associated with robot-assisted pyeloplasty (RP) vs laparoscopic pyeloplasty (LP).
Materials and Methods:
A decision analysis model was developed to compare costs of each procedure based on hospital-related cost centers. A literature search was performed to identify nonoverlapping studies with outcomes for RP and LP. Weighted means were calculated for operative time and length of stay. Cost data were obtained from our institution. One- and two-way sensitivity analyses were performed to evaluate the effect of changing variables on the cost-effectiveness of RP.
Results:
Eight studies were identified with 181 and 145 patients undergoing RP or LP, respectively. Operative times were 211 minutes for RP and 224 minutes for LP. Hospital stays were shorter for RP at 1.54 days compared with 1.98 days for LP. Mean direct costs were higher for RP at $10,635 vs $9,065 for LP. The largest difference was in fixed surgical supply costs per case at $1357 for RP and $406 for LP. One-way sensitivity analysis showed that RP would be cost effective if performed in less than 96 minutes. Even if RP was performed on an outpatient basis or more than 1000 cases/year, however, LP would still be cost superior. Two-way analyses showed areas where RP could be more cost-effective than LP.
Conclusions:
RP is associated with higher cost compared with LP, predominately because of the cost of the robot and surgical supply costs. Decreasing operative time and equipment costs may result in RP being more cost-effective than LP. Shorter hospital stay alone, however, is insufficient to allow RP to be cost-effective. One would need to demonstrate tangible advantages to the robot to justify the added costs.
Introduction
The proliferation of robot-assisted surgery programs using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) has reduced some of the technical difficulties of pure laparoscopic surgery. Robot-assisted surgery allows for improved three-dimensional viewing with increased magnification and increased degrees of freedom with surgical instruments making complex intracorporeal suturing far easier compared with traditional laparoscopic instruments. Although limited data exist on the number of pyeloplasties performed yearly, it is likely that robot-assisted pyeloplasty (RP) is now more common than LP. Outcomes with LP or RP appear to be equivalent, although conflicting evidence exists in regard to differences in operative times and length of stay. 4
The rapid adoption of robot-assisted surgery in urology has often not considered the cost vs the benefit of the new technology. 5 Cost analyses performed for other urologic procedures have shown that robot-assisted procedures are more expensive without a commensurate improvement in outcomes. 6,7 There are little data on the cost-effectiveness of RP. In this study, we performed a cost comparison of RP and LP using direct costs from our institution and outcomes data from the literature.
Materials and Methods
Literature review
A literature search was performed using PubMed and MEDLINE to identify nonoverlapping studies for LP and RP that included data on operative times and length of stay. A meta-analysis of RP vs LP was identified and data on operating room (OR) time and length of stay (LOS) was extracted and used for all cost analyses. 4
Cost analysis
Hospital cost data were obtained from our institution. Hospital charge data were not used in our analysis because such data incorporate profit margins, which do not directly correlate to resources allocated. Financial analyses were based on cost rather than charges. Hospital costs comprised OR time costs, supplies, anesthesia services, room and board, laboratory, and medication costs. Operative time and hospital stay data used in the analysis were derived from the literature.
For robotic procedures, the purchase and maintenance costs must also be taken into account. The purchase price for the da Vinci robot is estimated at $1.5 million, with maintenance fees at about $150,000 per year. In our cost model, it was assumed the robot would be used across specialties for a total of 300 cases/year over a 7-year period. This case volume was used because it is a reasonable estimate for total cases per year for a busy robotic surgical program using one system and also reduces the bias with respect to low utilization of the robot. The cost was also amortized over a 7-year period given that this is the typical accounting method for capital equipment at our institution as well as others. Not including surgical supplies, the robot adds an additional $364,285 per year to hospital costs, or $1214 per case.
OR costs were calculated based on institution rates of $12.90 per minute or $774 per hour. 6 Some surgical supplies are identical for both procedures, such as drapes and suture. Primary equipment costs for RP and LP include disposable items such as trocars, Visiport™ device, suction irrigator, and clip appliers. Robotic instruments have a fixed number of uses and include hot shears, two needle drivers, and two graspers. Averaged over 10 cases, the cost of each instrument is $220 per use. The recovery room fee was estimated at $270 based on similar patients undergoing laparoscopic or robot-assisted procedures. 6,7
Room and board costs are $508 per night at our institution. Medication and pharmacy costs were estimated at $200 per day, assuming similar needs between patients undergoing RP or LP and patients undergoing laparoscopic radical prostatectomy. 6
Decision analysis model
Cost models were created with TreeAge Pro 2009 (TreeAge Software, Williamstown, MA) using hospital cost data obtained from University of Texas Southwestern OR administration and billing office. Based on existing data, we assumed minimal differences in complication rates between procedures. 4 One- and two-way sensitivity analyses were performed to evaluate the effect of varying OR time, LOS, and equipment costs on the cost-effectiveness of RP and LP.
Results
A meta-analysis of eight studies with LP vs RP data series was used for this study, comprising 181 patients who underwent RP and 145 patients who underwent LP. 4,8 –13 Weighted mean operative times were 211 and 224 minutes for RP and LP, respectively. Hospital stays for RP at 1.54 days compared with 1.98 days for LP. Our data show that RP was more costly at $10,634.51 per case compared with $9065.44 per case for LP (Table 1).
LP=laparoscopic pyeloplasty; RP=robot-assisted pyeloplasty; OR=operating room; LOS=length of stay.
Sensitivity analyses were performed to identify potential variables to improve cost-effectiveness of the robotic procedure. One-way sensitivity analyses evaluate one variable at a time to measure its effect on cost while the remaining variables are fixed (Table 2). These analyses found that RP would be cost-equivalent to LP if laparoscopic equipment costs were increased to $1975, or if LP hospital stay increased to 4.2 days, robotic OR times were decreased to 139 minutes, or laparoscopic OR time increased to 296 minutes per case (Table 2). On the other hand, no decrease in robotic cost, robotic equipment, or robotic LOS or increase in robotic cases alone would result in RP reaching cost-equivalence with LP.
Lap=laparoscopic; OR=operating room; LOS=length of stay.
no threshold reached.
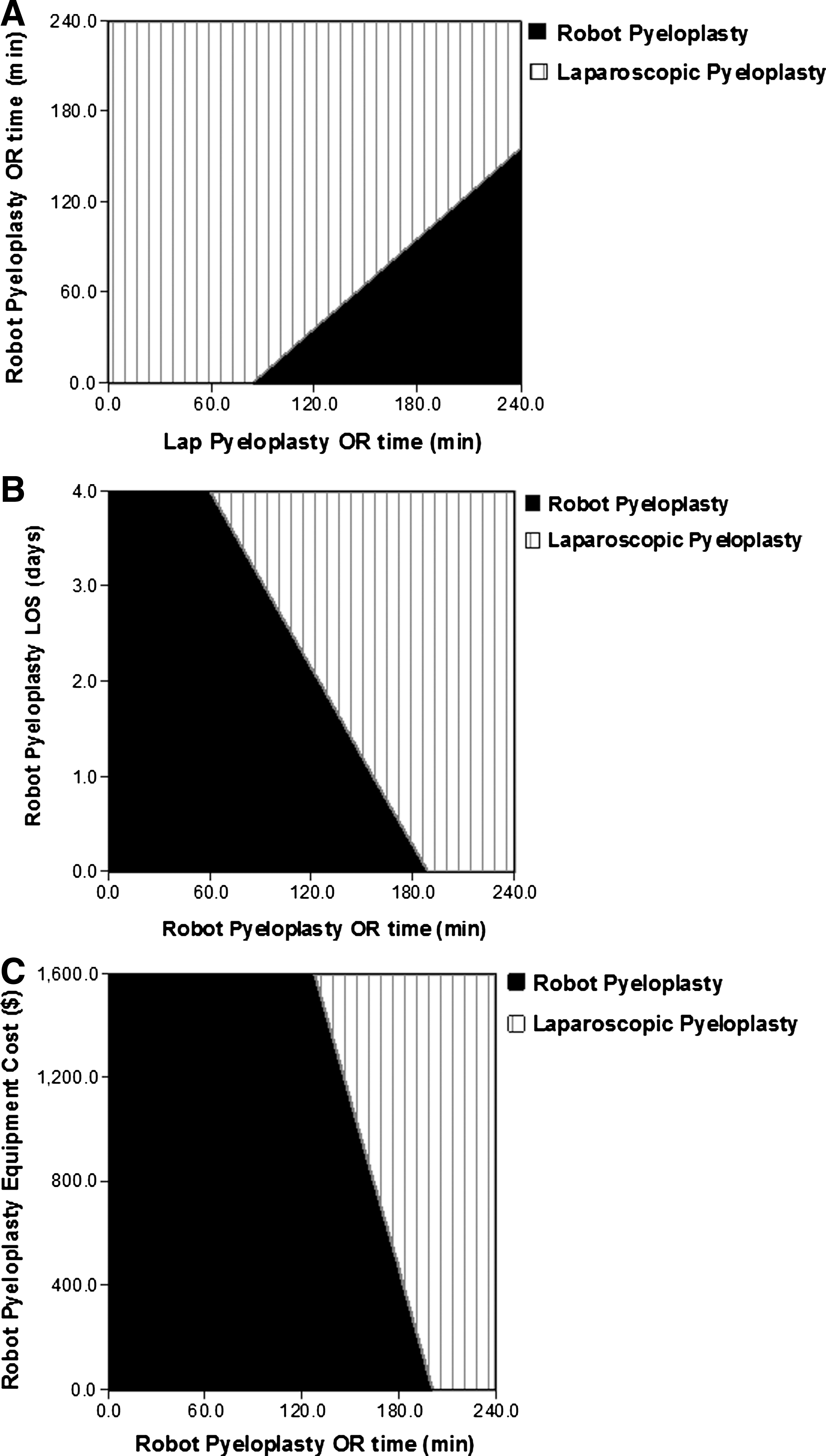
Two-way sensitivity analyses modify two variables simultaneously to evaluate the effect on cost. In the first analysis (Fig. 1A), we varied RP and LP OR times. One can see that if you are able to perform RP in 2 hours, LP is still more cost-effective as long as it takes no more than 3.5 hours. In figure 1B, we varied RP LOS and OR time. For RP to be more cost-effective than LP, there either needs to be a short LOS along with reduced OR time—for example, LOS 1 day and OR time of 2 hours would result in RP being cost-effective. Similarly, if you can do LP in 2 hours, then there is no OR time for which RP is cost-effective. In Figure 1C, we varied RP equipment costs and OR time. Again, there needs to be a decrease in equipment cost and OR time for RP to be cost superior. At an equipment cost of $1000/case, RP needs to be close to 2 hours to be cost-superior.
Discussion
Laparoscopic pyeloplasty has now been performed for more than 10 years, with demonstration of comparable outcomes to the open approach and is now considered by many to be the gold standard treatment for patients with UPJ obstruction. The technical demand associated with laparoscopic intracorporeal suturing may limit the utilization of this approach. Introduction of robotic technology has decreased many of the limitations associated with laparoscopic surgery, offering increased range of motion, mimicking the surgeon's natural hand movements. These factors mitigate the difficulty associated with intracorporeal suturing, making the robotic platform a desirable alternative to laparoscopic pyeloplasty. Series report the outcomes of RP to be technically feasible, with similar short-term outcomes. Because robotic surgery may reduce the technical challenges associated with LP, however, we sought to further evaluate the impact on cost and economic considerations.
Previously, Bhayani and associates 8 reported their cost analysis of RP compared with laparoscopy. This series compared 8 robotic procedures with 13 case-matched LPs. Analyzing the cost of robot maintenance and operative times, they similarly concluded that robotic procedures are more costly, even when adjusting OR times. We corroborate these data with a much larger cohort of patients, including a more comprehensive evaluation of cost variables.
Our study demonstrates that LP is the most cost-effective pyeloplasty approach, with a direct cost advantage of $1569.07. For the robotic approach to become cost-equivalent, a variety of factors must be changed, as are outlined in our sensitivities analyses. If there are no changes to the cost of the robot or of robotic equipment, then the only factor that can be impacted by a surgeon is operative time. If robotic OR time can be decreased to 139 minutes, then it would be superior, assuming the time for LP for the same surgeon was 224 minutes (ie, similar to the literature average). On the other hand, less dramatic decreases in operative time for RP can result in RP being cost-superior if they are accompanied by decreases in LOS. Obviously, a decrease in the cost of the robot and robotic equipment improves the cost-effectiveness of RP without necessitating changes in OR time or LOS.
The fixed costs of robotic equipment, instruments, and maintenance represent the bulk of the cost difference between RP and LP. This finding has been corroborated in other studies examining the cost-effectiveness of robotic surgery for multiple surgical procedures, including prostatectomy, cystectomy, and in other surgical fields. 14 –16 The additional cost of a robot-assisted prostatectomy, however, is potentially mitigated by its decreased risk of complications and shorter hospital stay. Compared with open prostatectomy, robotic surgery offers benefits with regard to LOS and blood loss. 17 Earlier work, illustrating a decision tree analysis for UPJ obstruction treatments, looked at laparoscopic and open pyeloplasty, as well as antegrade and retrograde endopyelotomy. 18 While retrograde pyelotomy was the most cost-effective modality, this study highlights that success rate and other variables are important in the decision process. In regard to outcomes for pyeloplasty, however, there appears to be no difference in postoperative outcomes and complication rates between robotic and laparoscopic cohorts. 4
There is a potential bias that most publications involve endourologists who can perform the procedure using both laparoscopic and robot-assisted approaches. If one is unable to perform a procedure laparoscopically and the alternative is an open approach, then the benefits for using the robot would include those inherent to laparoscopy, including reduced pain, short LOS, earlier return to work. These benefits would likely justify the added cost of a robot.
There are inherent limitations to this study, which is based on a meta-analysis of other reported series comparing robotic and laparoscopic pyeloplasty. 4 All of the series analyzed were retrospective, with no randomized controlled trials available for comparison. In addition, the amortization of the robot purchase is divided by number of cases per year, which likely differ per institution. Furthermore, costs can vary between institutions, but this limitation is mitigated by the sensitivity analyses performed.
Conclusions
Despite shorter operative times and LOS, the robotic approach is more costly than LP. The main differences in costs arise from the fixed cost of the robot and surgical supplies. Shorter operative times and decreasing equipment costs may lead to RP becoming more cost-effective than LP.
Footnotes
Disclosure Statement
No competing financial interests exist.