
Abstract
Background and Purpose:
Ureteral stents are indispensable tools in endourology, although they often are associated with bothersome lower urinary tract symptoms. This study was conducted to evaluate the effect of alfuzosin on urinary symptoms, quality of life, and pain in patients after Double-J ureteral stent placement in a randomized, placebo-controlled trial.
Patients and Methods:
This study was conducted from July 2008 to May 2009. A total of 130 patients underwent placement of a Double-J stent after retrograde semirigid ureteroscopy for ureteral stones. They were randomized in two groups. Group 1 (n=65) received alfuzosin 10 mg once daily and group 2 (n=65) received placebo for 1 week. Both groups also received standardized analgesia. The stent symptoms were measured and recorded 1 week after the procedure. Statistical analyses were performed using the chi-square test and Student t test with P<0.05 considered significant.
Results:
The demographic profile including patient and stone-related parameters were comparable. Group 1 had significantly less urinary symptoms (P<0.05). The quality-of-life assessment was better in the alfuzosin arm than in the placebo arm (P<0.001). The mean pain score was 1.15 in group 1 and 3.89 in the placebo group (P<0.001). None of the patients in either of the arms withdrew from treatment; there were minimal adverse effects in the treatment arm. The limitation of the current work includes relatively smaller sample size and use of single type of stent.
Conclusions:
Alfuzosin 10 mg once daily in patients with a Double-J stent significantly decreases the bothersome urinary symptoms, besides decreasing significantly the pain associated with the stent.
Introduction
The exact pathophysiology of stent symptoms remains unknown. It could be related to lower ureteral spasms and local trigonal sensitivity to the ureteral stent, however. 5 This problem is persistent despite several modifications in stent materials and composition, designs, shapes, and diameters. 6 Most of these symptoms are self-limiting and do not last beyond the first few weeks. In fact, after the initial few months, the Double-J stent becomes so asymptomatic that it is often forgotten; it is recommended that there be a system of reminding patients for their timely removal. 7
Deliveliotis and colleagues 8 in 2006 proposed for the first time that the selective alpha-1 blocker (such as alfuzosin) improves stent-related pain and urinary symptoms. They hypothesized that it can influence these symptoms, because stent-related symptoms mimic the lower urinary tract symptoms (LUTS) from benign prostatic hyperplasia (BPH). Alfuzosin, being a competitive antagonist of the alpha-1 adrenoreceptor, thus inhibits the contraction of prostatic, bladder, distal ureteral, and proximal urethral smooth muscles and, therefore, ureteral pressure and resistance, bladder outlet resistance, bladder irritability, and relevant symptoms are reduced. 9
Other studies have shown the beneficial effects of alpha-blockers in the treatment of voiding symptoms in women. Alpha-blockers have a modulating effect on bladder smooth muscle that decreases the frequency, urgency, and urge incontinence in women as proven by urodynamic studies. 10,11
In view of these evidences, we performed a double-blind, randomized, placebo-controlled trial to determine the possible role of the alpha-blocker alfuzosin in improving stent-related urinary symptoms, pain, and quality of life after its placement.
Patients and Methods
Study design and inclusion criteria
It was a double-blind, randomized, placebo-controlled trial conducted over the duration of 10 months from July 2008 to May 2009. The study protocol, consent form, and questionnaire were approved by the Institutional Review Board. All male and female patients who underwent unilateral retrograde placement of a Double-J stent (after semirigid ureteroscopy with pneumatic lithotripsy with the Swiss LithoClast™ for stone disease) that was retained for at least 1 week were included in the study. No adjustments were made for stent length in relation to the patient's body height, because all patients had a multilength stent.
The indication for stent placement after ureteroscopy was at the clinical judgment of the admitting urologist. The indications were large stone burden, mucosal trauma, and need for ureteral dilation to access tight ureters. Double-J stents were not routinely placed after uncomplicated ureteroscopy in the absence of the above indications.
Patients who were excluded from the study included those with bladder outflow obstruction secondary to BPH, chronic prostatitis, or prostatic carcinoma; patients receiving chronic medication (alpha-blocker or analgesia) or those with hypersensitivity/adverse reaction to these agents; pregnant women; patients with bilateral ureteral obstruction or obstruction from malignant pathology; patients who had additional open, percutaneous, or transurethral procedures except ureterorenoscopy; patients with a history of recurrent/untreated urinary tract infections and various forms of cystitis such as tuberculous, interstitial, or drug-induced; and patients who had a history of Double-J stent placement in the last 6 months.
Statistical analysis
A sample size of 65 patients in each group was calculated at a significance level of 0.05 and a power of 80%, considering the proportion of patients in the placebo group with pain as 66% and the experimental group as 44 % (adapted from the previous study by Deliveliotis and coworkers 8 ). An informed consent was obtained, and patients received an explanation of the surgical procedure, indication of placement of the Double-J stent after ureteroscopy (if needed), and use of a drug for alleviation of stent symptoms. All patients were fully informed about the potential side effects of alfuzosin; however, they were not aware that they were receiving placebo or alfuzosin. Patients were prospectively randomized at the end of placement of the Double-J stent by lots drawn by a third person not related to the study from a box containing 130 paper slips with 65 labeled as group A and 65 as group B with and equal chance of being selected in each group. Group A received 10 mg alfuzosin once a day for 1 week and group B received placebo for 1 week.
An attempt was made to ensure that all the medications were taken by counting the leftover pills and asking the family and the patient direct questions regarding medication and dosage. The statistical analyses were performed on Statistical Package for Social Sciences (SPSS) version 16 software. The student t test and chi-square test were applied as appropriate to test for significance of difference. A P value <0.05 was considered to be significant.
Use of pain medication
To eliminate the confounding effect of additional analgesia, during the first week of stent placement, all patients received standardized analgesia (5 days of oral paracetamol 1 g four times a day and oral diclofenac 50 mg, when needed, up to three times a day). All patients received perioperative antibiotic prophylaxis for 3 days.
Procedure details
After ureteroscopy with an 8F semirigid ureteroscope (Wolf, Knittlingen, Germany) and stone fragmentation using the pneumatic Swiss LithoClast, all stents were placed under combined fluoroscopic and cystoscopic (19F or 22F sheath) guidance, and the same material Double-J stent (polyurethane, double-pigtail, multilength by Cook Medical, Bloomington, IN) was used. The urinary symptoms and quality of life were evaluated by the urinary symptom index of the Ureteral Stent Symptom Questionnaire (USSQ), and a visual analogue scale (VAS) was used for evaluating body pain on which 0 represents no pain and 10 represents severe pain.
The degree of hematuria in the two group were assessed by asking the patient for the presence of hematuria (gross) after 72 hours of the procedure and by determining the number of red blood cells in urine microscopy at the first week of the procedure. The primary outcome measure was assessment of difference in ureteral stent symptoms, pain, and quality of life in the treatment and placebo groups. Patients were also asked direct questions concerning the known side effects of the medications during the follow-up clinic visits. The USSQ and VAS were administered 1 week after the procedure.
Results
During the study period, the total number of ureteroscopies performed for ureteral calculi were 328, of which 159 necessitated placement of a Double-J stent (48.5%). Twenty-nine patients were excluded from the study, and the final study population was 130—65 in each group (Fig. 1). No patient in either arm discontinued treatment. All patients completed the study. There was no statistically significant difference between the two groups with respect to age, sex, stone location within the ureter, side of the ureter on which ureteroscopy was performed, and size of the Double-J stent placed (Table 1).
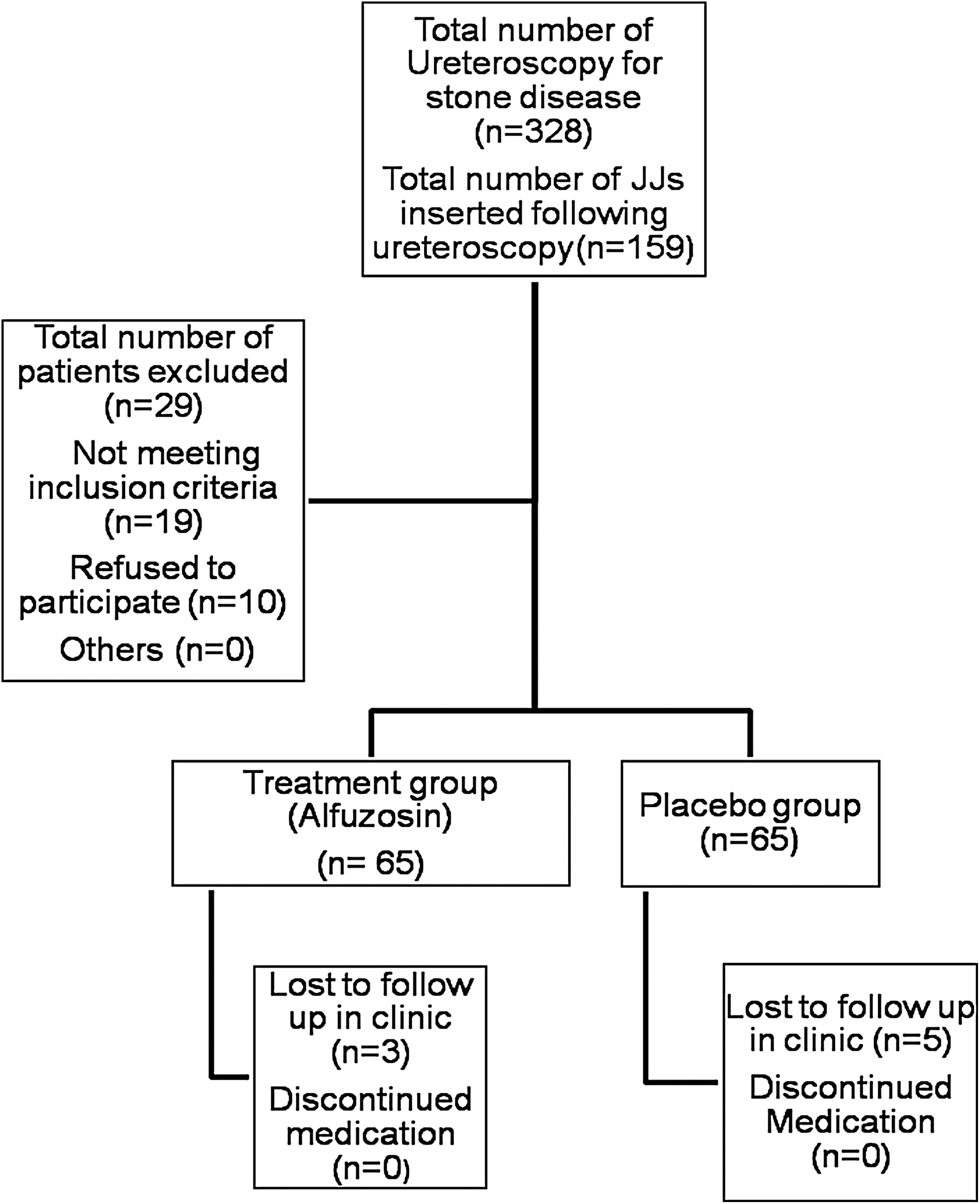
Consort flow diagram explaining patient accrual and exclusion. JJ=Double-J.
Analysis of stent symptoms between the two groups (Table 2) revealed a statistically significant difference between the two groups with respect to daytime frequency of micturition. More than half of the patients who received alfuzosin did not experience urinary frequency (score of 1) as opposed to 94% of patients who received placebo. Similarly, statistically significant differences were observed with respect to other irritative urinary symptoms such as nocturia, urgency, and urge incontinence. The symptoms of sense of incomplete voiding, dysuria, and quantity of blood in urine, and frequency of hematuria did not show any statistical significance.
The quality of life was much better in those who were receiving alfuzosin compared with the placebo group. After completion of 1 week of medication, 26.1% were mostly dissatisfied and 8% were unhappy in the d placebo group as oppose to only 12% and 3% in the alfuzosin group.
The mean pain score, as measured by VAS on a scale of 0 to 10, was 1.15+1.3 in patients who received alfuzosin, and it was 3.89+1.77 in the placebo group (P<0.0001). Nearly 42% of patients in the alfuzosin group did not experience any flank pain vs only 9% of those in placebo group who were pain free.
In the alfuzosin group, no significant difference was found in pain score between male (1.23) and female (0.85) patients (P=0.435). Also, urinary symptoms between male and female patients in the alfuzosin group did not show any significant difference.
Only 12 patients (5 in the alfuzosin group and 7 in the placebo group) used additional analgesia after 5 days of Double-J stent placement. The difference in the two groups was not statistically significant (P=0.382), however. There were no major side effects experienced by patients in either group. Five and two patients experienced orthostatic dizziness, and two patients each experienced nasal stuffiness in the alfuzosin and placebo groups, respectively.
Discussion
Double-J stents were first introduced to clinical practice in 1978, and over the last 3 decades, the indications for its placement have broadened. Double-J stents have become an integral part of urology, especially in endourologic practice. Stents are regarded as a sort of insurance policy against postoperative complications, especially after intervention for ureteral stones. 12 Despite advancements in shapes, materials, and drug coatings of stents, no ideal stent has been designed to date that can significantly improve these complications. 13,14
Alpha-blockers are useful for management of symptoms associated with BPH and as medical expulsive therapy for ureteral calculi. 8 Alfuzosin reduces the ureteral pressure and resistance, bladder outlet resistance, and bladder irritability and, hence, the relevant symptoms. It competitively blocks the alpha-1 adrenoreceptor mediated contraction of distal ureteral, prostate, bladder, and proximal urethral smooth muscles. 9 This effect leads to reduced voiding pressures and therefore reduction in reflux of urine back to the kidney and the resulting pain.
Deliveliotis and colleagues 7 first proposed the role of alfuzosin 10 mg in relieving ureteral stent symptoms. A few studies have been published recently that have provided the early evidence of the role of alpha-blockers for decreasing the morbidity associated with ureteral stent placement. Beddingfield and coworkers 15 in their randomized controlled trial showed the beneficial effect of alfuzosin 10 mg once a day in relieving stent symptoms. They proposed that the ability of alfuzosin to decrease stent symptoms is also because of blockade of α1-D mediated effect on bladder and spinal cord. Wang and associates 5 evaluated the effect of tamsulosin 0.4 mg once a day to improve the symptoms in patients with ureteral stents.
There were also differences in the time interval after which stent symptoms were assessed following treatment with alpha-blockers. Deliveliotis and colleagues 8 evaluated patients' symptoms after 4 weeks of Double-J stent placement, and Wang and coworkers 5 did so after 2 weeks. We did evaluation after 1 week on follow-up in the clinic. Longer duration of time lapse after placement of the stent can result in more recall bias. It is also shown in the literature that overall tolerance to a stent improves with passage of time. 3 The assessment of symptoms after a longer time may not truly reflect the effect of alpha-blockers on stent symptoms for this reason.
Joshi and associates 4 collected data regarding the frequency and severity of stent-related symptoms and showed that 78% of patients with stents had bothersome urinary symptoms that included storage symptoms, incontinence, and hematuria. More than 80% had pain that affected daily activities, 32% reported sexual dysfunction, and 58% reported reduced work capacity and loss of income. These symptoms (especially urgency, increased daytime frequency, nocturia, and urge incontinence) were also present in 70% to 90% of our patients receiving placebo with various degrees of severity.
The flank pain has been described as one of the most painful stent-related symptoms by Joshi and colleagues. 4 Reflux of urine from the the urinary bladder to kidney especially during voiding causes stent-related flank pain. Alfuzosin resulted in significant reduction in both general and flank pain during voiding in our study. A large proportion of patients who received a,lfuzosin (41.5%) did not have any flank, loin or back pain. More than 90% of patients in the placebo arm complained of pain in our study. The intensity of pain measured on the VAS was much higher (3.89) in the placebo group than in the treatment group (1.15). By causing relaxation of the bladder neck and prostatic urethra, alfuzosin reduces the voiding pressure and therefore decreases both the frequency and intensity of pain. This finding was in contrast to what was reported by Deliveliotis and coworkers, 8 who did not show any significant differences in pain scores on the VAS between alfuzosin and placebo groups; however, stent-related pain was reported in a higher proportion of patients who received placebo. Beddingfield and colleagues, 15 however, showed a significantly less pain score in the treatment arm.
Our patients who received alfuzosin 10 mg for 1 week had significantly less pain (VAS 1.15+1.3) compare with those patients who received tamsulosin 0.4 mg for 2 weeks (VAS 3.91+0.95) in a study performed by Wang and colleagues. 5 This could represent the better effect of alfuzosin in relieving the flank pain associated with Double-J stents compared with other uroselective alpha-blockers such as tamsulosin.
Correct stent placement has been shown by some authors as a significant factor in decreasing stent-related symptoms. Work by Lee and coworkers 16 indicated that the correct stent placement is more important than medication. More recently. Giannarini and associates 17 showed that stent-related symptoms are worse when the stents are misplaced crossing the midline. In the current work, we used multilength stents and continuous fluoroscopic and cystoscopic guidance during stent placement. Although we did not specifically look postprocedure at the exact location of the stent, we believed that cystoscopic and fluoroscopic guidance and use of multilength with the redundant portion in the renal pelvis rather than the bladder are factors that significantly minimized the impact of misplaced stents. In our (unreported) experience, patients with significant LUTS have a bullous reaction indicating an allergic response to the stent material.
Recently, two other studies have also looked into the role of tamsulosin on stent-related morbidity. Both of them used the International Prostate Symptom Score (IPSS) as a tool to assess the storage and voiding symptoms associated with Double-J stents; however, this questionnaire has not been validated for stent symptoms per se. Navanimitkul and associates 18 reported the efficacy of tamsulosin in stent-related symptoms and quality of life using IPSS in a nonplacebo trial. Consistent with other studies, they showed that alpha-blockers result in decreased urinary symptoms. The authors, however, have not looked into its role in reducing stent-related pain.
The USSQ is a useful and sensitive tool that has been validated and shown to have good evaluative and discriminate properties. 19 It comprehensively assesses the urinary, pain, and sexual symptoms associated with ureteral stents.
Conclusions
The major limitation of our study was that we did not measure all symptoms (stent-related morbidity) according to this questionnaire (USSQ) because of its comprehensive nature and because it has not been validated in vernacular. Rather, we used a pro forma to quantify the most frequent urinary symptoms, quality of life, and pain. We did not evaluate the other domains included in USSQ—ie. general health, work performance, sexual matters, and additional problems. Another limitation is use of only a single stent design and material and only single indication for Double-J stent placement (postureteroscopy for ureteral stones). The other limitation is the relatively smaller sample size. Because there are limited studies in this aspect, the current study will add to the literature in this regard.
Future prospective randomized studies with larger sample size, using validated questionnaires, including other insertion indications for stent placement and various types of stents, are warranted to overcome these limitations.
Footnotes
Acknowledgments
The authors acknowledge Dr Tashfeen Ahmed and Dr. Ghulam Murtaza for their help in statistical analysis. The study was supported by the University research council grant from Aga Khan University.
Disclosure Statement
No competing financial interests exist.