
Abstract
Purpose:
To compare blind and nerve stimulation guided transurethral obturator nerve block (ONB) in transurethral resection of bladder tumor (TURBT) to prevent obturator reflex.
Patients and Methods:
One hundred and twelve patients with lateral bladder wall tumors and at high risk for general anesthesia were categorized randomly in three groups. In the first group (34 patients), after spinal analgesia was administered, the exact site of the obturator nerve was determined by nerve stimulation and 15 mL of lidocaine HCl 2% was injected around the nerve. In the second group (31 patients), we determined the obturator nerve using nerve stimulation (like the first group), then 20 mL of saline was injected. In the third group (47 patients), the obturator nerve was determined based on anatomic landmarks and blocked subsequently. Leg jerking was reported and compared in the three groups.
Results:
The median ages in the three groups were 55.4, 59.4, 57.8 years in the first, second, and third groups, respectively. Male/female ratios were 79.5% in the first, 80.7% in the second, and 80.9% in the third group (P=0.986). Leg jerking was reported in 5.8%, 34%, and 6.3% of patients in the first, second, and third groups, respectively (P=0.0001). ONB took 6.7 minutes in the first, 6.1 minutes in the second, and 5.2 minutes in the third group, on average. There was no report of adverse effects of lidocaine HCl in this study.
Conclusion:
Transvesical ONB is a safe and effective method of ONB before TURBT. This method is feasible by urologists and promising even without nerve stimulation and only by anatomic landmarks.
Introduction
Bladder perforation is a disastrous event in this scenario. As a matter of fact, general anesthesia (GA) and injection of muscle relaxant agents is the preferred method of anesthesia in these patients. 1,2 When GA is high risk because of cardiopulmonary diseases, spinal analgesia (SA) plus local blockade of the obturator nerve is an alternative. 3,4
Recently, a new technique of obturator nerve block (ONB) has been introduced. In this technique, the obturator nerve is detected by nerve stimulation during cystoscopy. Then, 15 mL of lidocaine HCl 2% is injected around the nerve by a needle through the working channel of the cystoscope (Fig. 1).
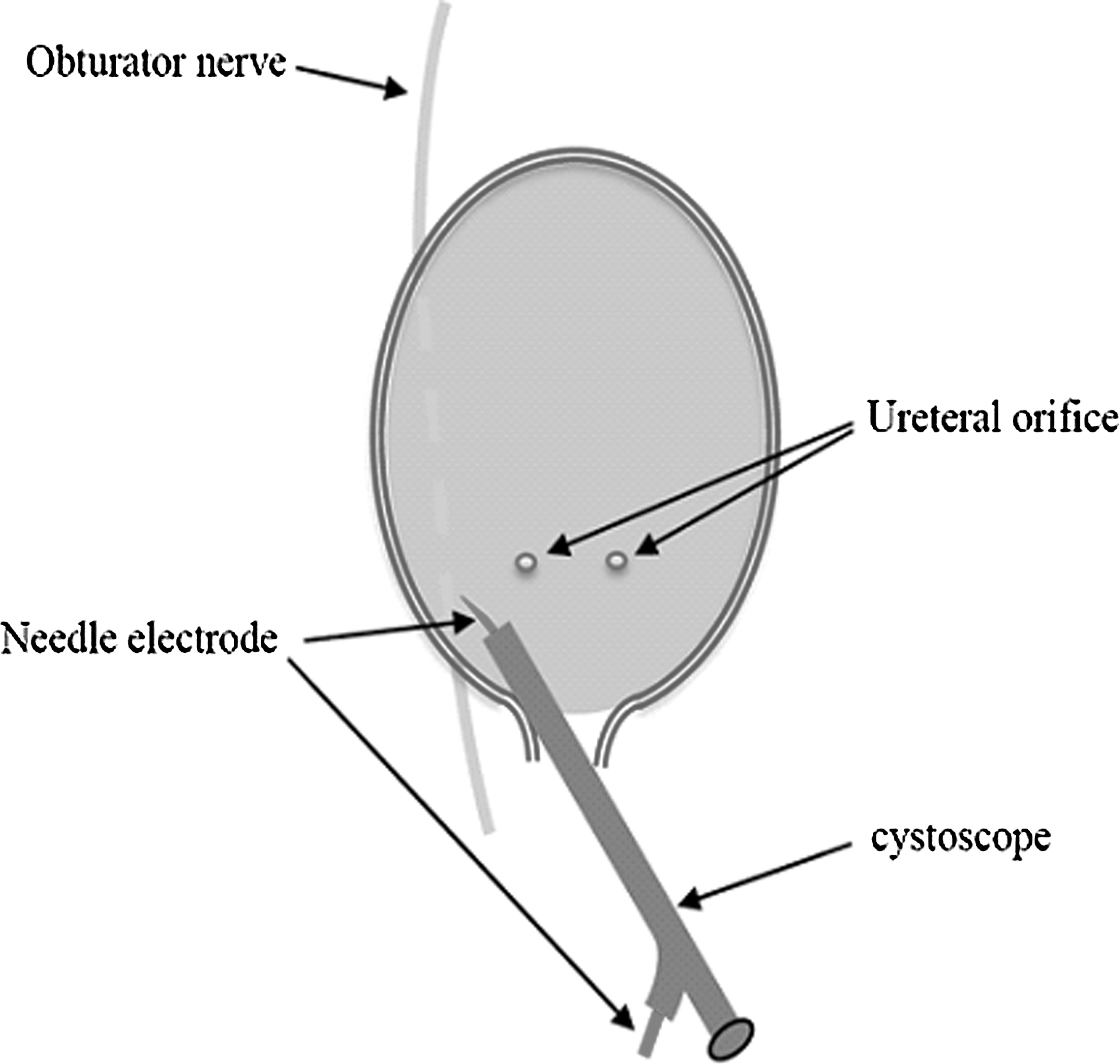
Nerve stimulation and lidocaine injection using a needle electrode through the working channel of the cystoscope.
Using a nerve stimulation device is sophisticated. In this study, we performed transurethral ONB considering anatomic landmarks without nerve stimulation and compared it with the previous methods.
Patients and Methods
After consensus, 112 patients with lateral bladder wall tumors who were at high risk for GA were included in the study. Patients were categorized randomly in three groups. All the patients underwent SA before TURBT. After SA, ONB was performed by injection of 15 mL lidocaine HCl 2% using a needle through the working channel of the cystoscope in the first and third groups. In the first group, the obturator nerve was detected by nerve stimulation, but in the third group, we only used anatomic landmarks to determine the position of the obturator nerve. In the second group, we used physiologic saline instead of lidocaine as a placebo. All injections were performed at a tumor-free area of the lateral bladder wall. In cases of bladder tumor compromising the integrity of the bladder, the patients were excluded from study. One minute after ONB, TURBT was started, and leg jerking and the duration of the procedure were reported.
ONB using nerve stimulation to detect the nerve
In this group, after SA, with the patient in the lithotomy position and before draping, one electrode was attached to the adductor muscles and the other one was attached to a 22-gauge needle compatible with the working channel of the cystoscope.
The obturator nerve is next to the posterolateral wall of the bladder, trigone, and posterior urethra. 4 Considering this location, we inserted the needle between the bladder neck and ureteral orifice through the working channel of the cystoscope (Fig. 1). The bladder was filled, and then the needle was inserted approximately 1.5 cm in the bladder wall to pass its thickness. It is assumed that the obturator nerve is in these vicinities in the extraperitoneal space. We used a currency of up to 3 mA to stimulate the obturator nerve. To find the exact site of the obturator nerve, sometimes the needle tip was relocated several times. When obturator stimulation induced adductor contraction, the lidocaine was injected in the determined site.
Injection of physiologic saline instead of lidocaine
Exactly like the first group but instead of lidocaine, 15 mL of physiologic saline was used to evaluate the placebo effect.
ONB considering anatomic landmarks
In this group, lidocaine was injected in three separate locations between the ureteral orifice and bladder neck in equal distances. Using this method, we can stain the outside of the posterolateral bladder wall in the extraperitoneal space by a rim of lidocaine; this is exactly where the obturator nerve passes. The bladder was half filled during the procedure and TURBT started 1 minute after lidocaine injection.
Results
The median ages in the three groups were not statistically different. These were 55.4, 57.8, and 58.4 years in the first, second, and third groups, respectively. Also the male/female ratios in the groups were similar. These were 79.5% male in the first, 80.9% in the second, and 80.7% in the third groups (P=0.986). Table 1 shows the final pathology results of tumors in each cohort of study.
Obturator reflexes and leg jerking were reported in 5.8% (2 patients), 34% (11 patients), and 6.3% (3 patients) in the first, second, and third groups, respectively. The occurrence of leg jerking was not different in the first and third groups.
The average tumor sizes seen in the preoperative ultrasonography were not significantly different. In the first group, it was 3.32±1.16 (1.5–5) cm; in the second group, it was 3.54±1.17 (1.7–5) cm; and in the third group, it was 3.64±1.32 (2–5) cm (P=0.544).
The procedure from the start to the end of ONB took on average 6.7, 6.1, and 5.2 minutes in the first, second, and third groups, respectively (P=0.0001). This was statistically equal in the first and third groups.
There was no case of bladder perforation or severe bleeding. Twenty-three cases of muscle invasion were detected after pathologic examination, and in 85 patients, the tumors were superficial.
Discussion
The obturator nerve is a motor neuron originating from T12–L2. The obturator nerve passes in close proximity to the prostatic urethra, bladder neck, and inferolateral wall of the bladder. 1
Obturator nerve stimulation during TURBT causes adductor muscle contraction and leg jerking. This can lead to bladder perforation, bleeding, and incomplete resection of tumor or hematoma and consequently may increase morbidity and mortality of the procedure. 3,5,6 Therefore, ONB should be considered in association with SA in patients who are at high risk for GA. 3
A few techniques have been introduced for ONB. Transcutaneous blockade using anatomic landmarks is performed by anesthesiologists, and it may be time consuming. The success rate of this technique in different studies is 60% to 91%.(2,6 –8)
There is a variety of modifications to increase the efficacy of ONB. 9 –13 Ultrasonography and nerve stimulation are modalities to determine the exact site of the obturator nerve and increase procedure efficacy. The method proposed by Winnie and associates 14 (injection of local anesthetic into the femoral nerve sheath) has been debatable because of its efficacy for obturator nerve block. Some anesthesiologists use ultrasonography to find the exact place of the anterior branch of the obturator nerve to block it selectively. 15
Introduction of the bipolar system and laser for TURBT has lowered adductor contraction and leg jerking.(16 –19) These modalities, however, are expensive and not available in many centers.
In this study, lidocaine injection in the extraperitoneal space around the obturator nerve even without applying nerve stimulation had sensible results. Lidocaine injection in this study was totally safe, and no prominent side effect related to lidocaine was reported in this study.
To show the distribution of injected material, in one of our patients, we added contrast agent to the lidocaine. In Figure 2, you can see the pelvic CT of that patient immediately after the procedure; the injected material has covered the posterolateral side of the bladder.

Distribution of lidocaine and contrast along the posterolateral wall of the bladder (arrow).
ONB without nerve stimulation has some pitfalls. First, there may be variations in the track of the obturator nerve. Second, the probability of tumor seeding is a scary flaw.
In spite of that, we believe that ONB based on anatomic landmarks and without nerve stimulation is effective and safe enough to be proposed in urologic centers. In contrast to transcutaneous techniques, this technique is performed by an urologist, not an anesthesiologist.
Conclusion
Transvesical ONB is a new technique in local blockade of the obturator nerve. This nerve blockade may be performed by the guide of nerve stimulation or anatomic landmarks. Relying on anatomic landmarks is effective and less sophisticated than applying nerve stimulation.
Footnotes
Disclosure Statement
No competing financial interests exist.