
Abstract
Purpose:
To narrate our experience with laparoscopic reconstruction of obstructive megaureter (MGU) and assess the intermediate-term outcome achieved.
Patients and Methods:
Patients were evaluated in detail including presenting complaints, biochemical profile, and imaging (ultrasonography [USG], diuretic renography [DR], magnetic resonance urography [MRU], and voiding cystourethrography [VCUG]). All patients with a diagnosis of obstructive MGU and salvageable renal unit were offered laparoscopic reconstruction. The standard laparoscopic exercise included ureteral adhesiolysis until the pathologic segment, dismemberment, straightening of the lower ureter, excisional tapering, and a nonrefluxing ureteroneocystostomy. Operative and postoperative parameters were recorded. Patients were evaluated postprocedure on a 3-month schedule. Follow-up imaging included USG and VCUG at 6 months and 1 year postprocedure and then at yearly intervals. MRU and DR were repeated at 1 year postprocedure.
Results:
Twelve patients (13 units—11 unilateral, and 1 bilateral) underwent laparoscopic tailoring and reimplantation for obstructive MGU. Mean age was 98.6 months. All patients were male. Mean body mass index was 17.69 kg/m2. Presenting complaints were flank pain (n=8) and recurrent urinary infection (n=12). All procedures were completed via a laparoscopic approach. Mean operation duration was 183 minutes, and mean blood loss was 75 mL. Mean duration of hospital stay was 2.1 days. No major intraoperative or postoperative happenings were recorded. All patients were asymptomatic at follow-up with stable renal profile. Follow-up MRU revealed a decrease in ureteral and upper tract dilatation with satisfactory drainage in all. Follow-up VCUG demonstrated grade I vesicoureteral reflux in one patient. Eight patients completed 3-year follow-up with a satisfactory outcome.
Conclusion:
Laparoscopic reconstruction of obstructive MGU offers satisfactory immediate- and intermediate-term outcome without undue prolonged morbidity.
Introduction
An armamentarium of approaches has been in vogue for definitive management of obstructive MGU. 2 –6 Conventionally, these approaches have been performed through incisional access; the patient is subjected to additional access-related morbidity, and the recovery is prolonged. Although laparoscopic access has been appraised for superior cosmesis and morbidity profile and has been increasingly performed for reconstruction of various urologic pathologies, 7 only limited citations to date report successful reconstruction of obstructive MGU by a purely laparoscopic approach. 8 This may be attributed to the complexity of these exercises.
We report our experience with pure laparoscopic reconstruction of obstructive MGU and assess the short- and long-term outcome. To our knowledge, this is the largest series of laparoscopic reconstruction of obstructive MGU reported to date.
Patients and Methods
Patient cohort
Patients undergoing laparoscopic reconstruction for obstructive MGU in our institute between April 2005 and October 2010 were included in the study cohort. Patients were evaluated in detail with assessment of presenting complaints, previous similar complaints and treatment summary, prenatal history, and any other relevant history. Laboratory evaluation included urine microscopy and blood profile. Imaging protocol included voiding cystourethrography (VCUG), ultrasonography (USG), and retrograde urethrography. Hydronephrosis was graded according to the Society of Fetal Urology guidelines. 9 Intravenous urography or magnetic resonance urography (MRU) and diuretic renography (DR) were conducted for assessment of the upper tract drainage status.
Operative exercise
Cystoscopy was performed first, followed by insertion of a perurethral catheter. The patients were then placed in a steep Trendelenberg decubitus position. Four ports were used (Fig. 1). The first exercise was adhesiolysis and straightening the tortuous ureter. Ureteral dissection was commenced from the level of the ipsilateral sacroiliac joint. Adhesiolysis was performed, and the ureter was dissected free until the level of the pathologic segment. Cold scissors was used for ureteral adhesiolysis, and the periureteral adventitia was meticulously preserved. The use of thermal energy was restricted during this step. The pathologic ureter was dismembered immediately proximal to the pathologic segment using cold scissors (Fig. 2A). The adynamic segment was excised. Any additional tortuosity was then lysed and the dismembered ureter was straightened. The distance between the dismembered ureter and bladder was assessed and if necessary additional adhesiolysis was performed above the level of the sacroiliac joint.
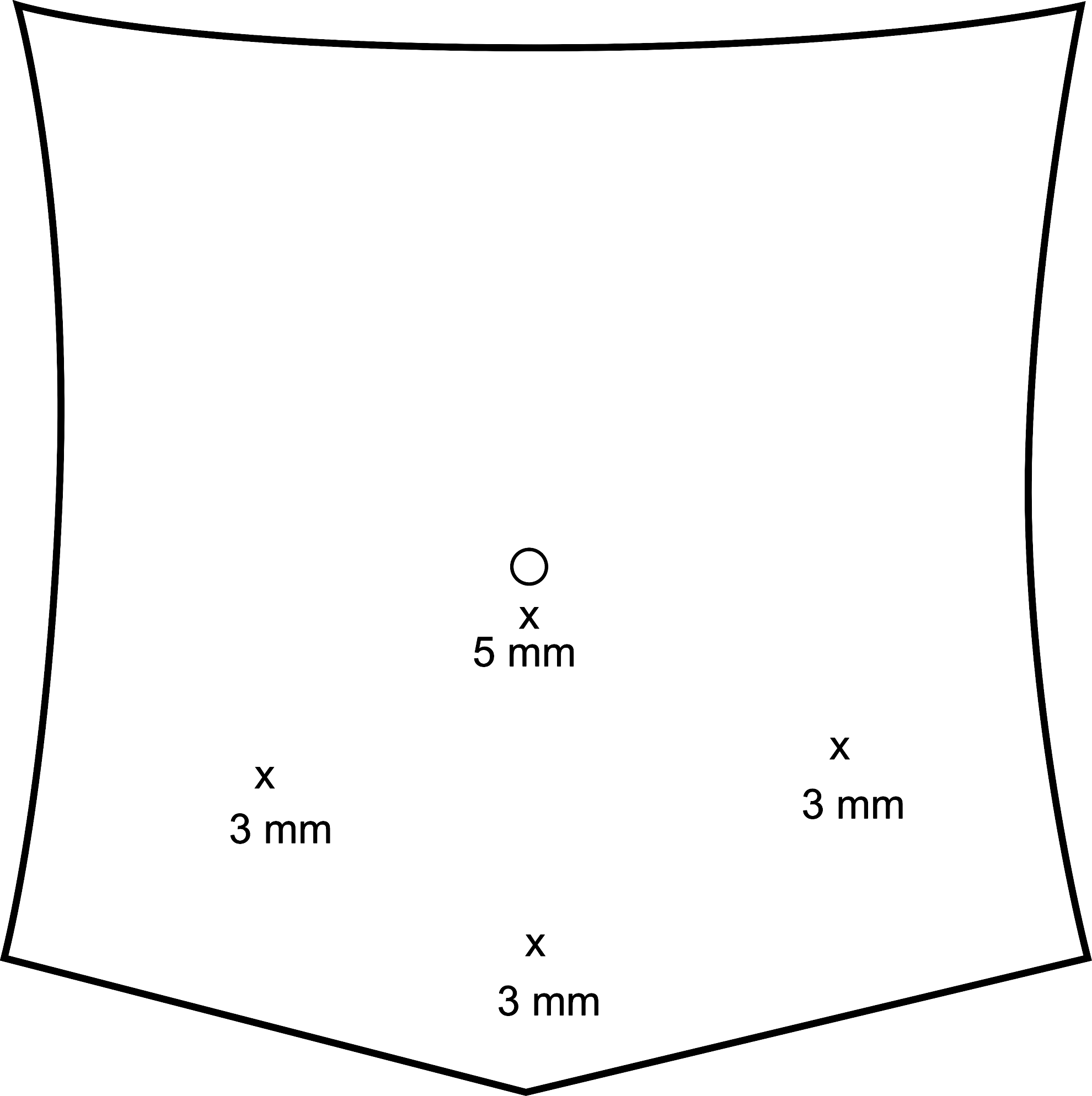
Ports used for the procedure.
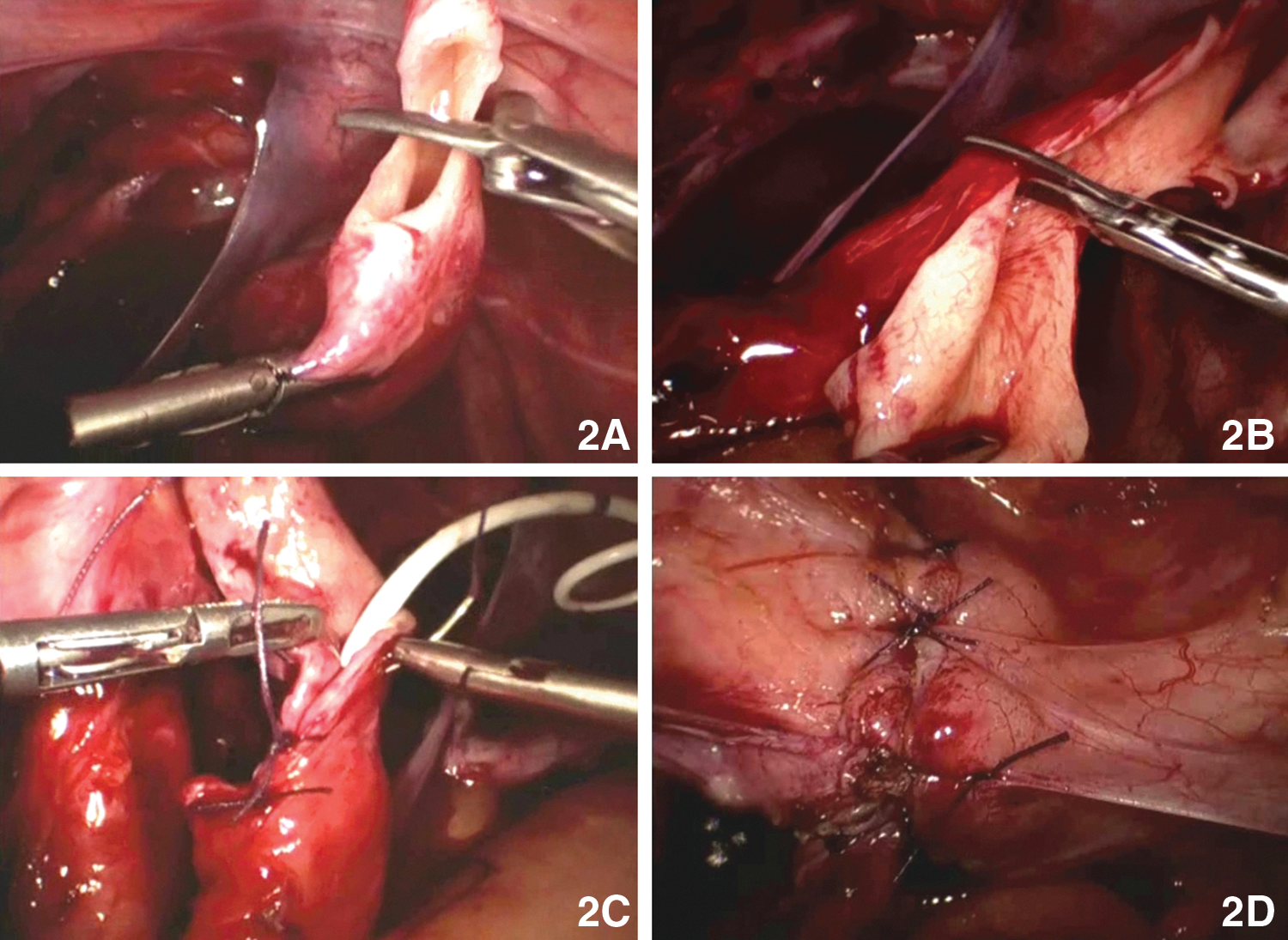
Tapering the circumference of the ureter remains the next exercise, and we conduct excisional tailoring. The lower five centimeters of the dismembered ureter are tapered. An atraumatic grasper is introduced through the midline suprapubic port and the dismembered ureter held with gentle traction, maintaining the alignment. A laparoscopic Babcock forceps was introduced through the right hand working port and the circumference of the ureter just adequate to allow insertion of a 6F ureteral stent was delineated. Excess ureter was excised using cold scissors (Fig. 2B). A 6F ureteral stent was then inserted in a retrograde fashion. The tapered ureter was then tubularized over the ureteral stent approximating mucosa on either side. A 3-0 polyglactin suture (4-0 polyglactin in children <5 years old) was used for this purpose. Intracorporeal suturing was performed in an interrupted fashion (Fig. 2C).
Ureteroneocystostomy remains the next exercise, and the bladder was inflated with 150 mL saline (physiologic saline, 0.9% weight/volume). Bladder mobilization was conducted anteriorly, and he tbladder was displaced posteriorly to ensure a tension-free approximation. This was performed using Harmonic shears. A buttonhole cystostomy was created. Ureteroneocystostomy was then performed using interrupted 3-0 polyglactin sutures in a tension-free manner. Antireflux was then constructed following the Lich Gregoir principle. From the point of ureterovesical anastomosis, a seromuscular detrusor tunnel was fashioned for a length about five times the diameter of the tapered lower ureter. The ureter was guided into the detrusor tunnel; and detrusorrhaphy completed using interrupted sutures of 3-0 polyglactin (Fig. 2D).
Procedure completion/postprocedure
All patients were allowed oral intake once comfortable. The drain was removed as indicated. The catheter was removed at a revisit after 1 week. Any significant intraoperative or postoperative happenings were recorded.
Follow-up
Ureteral stents were removed by 6 weeks postprocedure. All patients were followed on a 3-month schedule with assessment of clinical profile and renal parameters. USG and VCUG were repeated at 6 months and 1 year postprocedure and then at yearly intervals. MRU and DR were repeated at 1 year postprocedure.
Statistics
Analysis was performed by using mean, standard deviation, range statistics, and applying equal variance t test, Aspin-Welch unequal variance t test, and analysis of variance tests. A P value<0.05 was considered statistically significant.
Results
Twelve patients (13 units—11 unilateral and 1 bilateral) underwent laparoscopic tailoring and reimplantation for obstructive MGU. The patient profile is projected in Table 1. All patients were males. Presenting complaints were flank pain (n=8) and recurrent urinary infection (n=12). One patient with ipsilateral lower caliceal renal calculi and lower ureteral calculi underwent percutaneous nephrolithotomy and laparoscopic ureterolithotomy along with laparoscopic tailoring. One patient presented with obstructive MGU that affected a predominantly solitary functioning unit with contralateral dysplastic unit and preoperative deranged renal profile (serum creatinine 3.2 mg/dL).
SD=standard deviation; BMI=body mass index; GFR=glomerular filtration rate.
All procedures were completed via a laparoscopic approach. Operative, immediate postoperative, and follow-up parameters are listed in Table 2. No major intraoperative or postoperative happenings were recorded. No patients experienced any voiding dysfunction in the postoperative period. All patients were asymptomatic at follow-up. VCUG at 6 months revealed grade I reflux in one patient that resolved with conservative management.
SD=standard deviation; GFR=glomerular filtration rate.
One year follow-up imaging revealed a decrease in ureteral diameter with satisfactory drainage in all patients. There was no incidence of ureteral stricture. In all cases, there was improvement in the grade of hydronephrosis. Although the change in creatinine (last follow-up vs preprocedure) did not reach a level of statistical significance (P=0.70), the improvement in the glomerular filtration rate was statistically significant (P=0.00). A statistically significant reduction was also achieved in the follow-up ureteral diameter in comparison with the preoperative ureteral diameter (P=0.00). Eight patients in our cohort completed a 3-year follow-up and are clinically stable with no hydronephrosis, good drainage pattern, and no vesicoureteral reflux.
Discussion
The principal pathology in obstructive MGU is an adynamic ureteral segment in the vicinity of the ureterovesical confluence that hinders urine drainage through this segment. Cumulation of large volumes of urine proximal to the dysfunctional segment leads to loss of ureteral tone and an increase in the ureteral circumference. In long-standing pathologies, the ureter may be grossly dilated and tortuous. Consequently, ureteral rehabilitation in obstructive MGU demands bypass of the pathologic segment to allow unobstructed urine efflux to the bladder. In addition, the ureteral tortuosities need to be straightened and the ureteral circumference tailored to allow satisfactory coaptation of the ureteral walls. This facilitates satisfactory tunneling of the ureter for reimplantation and may also promote restoration of ureteral peristalsis.
Hence, the most popular exercise for reconstruction of obstructive MGU is dismemberment, tapering, and reimplantation. Despite the entire ureter being dilated, tapering of the lower 4 to 5 cm of ureter may suffice. 10 Restoration of lower ureteral tone facilitates return of upper ureteral tone and reestablishment of satisfactory peristalsis. Although both plication and excisional tapering have been practiced to achieve reduction of the ureteral caliber, excisional tailoring outscores in the presence of grossly dilated (>1.75 cm) and thick ureters. 11 In our series, all pathologic units were grossly dilated, and hence we followed this exercise universally.
The key issues in satisfactory reconstruction of obstructive MGU by a pure laparoscopic approach are achieving satisfactory lower ureteral adhesiolysis, preservation of orientation during ureteral tailoring, satisfactory downsizing of the ureteral circumference by intracorporeal suturing, and durable antireflux creation. This multitude of tasks increases the complexity of these reconstructions. We have been regularly performing various ureteral reconstructions through a laparoscopic approach, 12 –16 and the familiarity from these exercises motivated us to embark on this approach in all these cases. Even bilateral pathologies could be successfully addressed simultaneously by a pure laparoscopic approach.
Preservation of ureteral vascularity during adhesiolysis is crucial. Diligent handling of the ureter, preservation of generous periureteral adventitia, and limited use of thermal energy are the key steps that need to be followed. In grossly dilated ureters, optimum straightening of the lower ureter may be possible only after dismemberment and release of residual tortuosities. Straightening increases the available ureteral length for a tension-free ureteral reimplantation. Thereby unnecessary mobilization of the mid or upper ureter may be avoided, and upper ureteral vascularity remains uninterfered.
Maintainance of ureteral orientation during tapering has remained a key concern with this exercise, and several technical modifications have been proposed to resolve this issue. Ansari and associates 17 advocated extracorporeal tailoring after ureteral dismemberment, whereas Agarwal and colleagues 8 resorted to tailoring before dismemberment. We refrained from following these doctrines, however. Extracorporeal tailoring may be difficult to achieve in obese persons and risks jeopardizing the tenuous blood supply to the adhesiolysed lower ureter. Tailoring without dismemberment limits the adhesiolysis achieved, especially in grossly dilated ureters. This may lead to suboptimal straightening and loss of utilizable length of the ureter.
In our series, ureteral orientation during tailoring is preserved under direct supervision by grasping the ureter with an atraumatic grasper under slight tension, and tapering could be completed successfully in all cases. All of our patients had satisfactory reduction of ureteral caliber during follow-up, and no patients experienced any ureteral stricture.
Construction of a satisfactory antireflux also remains an important goal of these reconstructions to avoid any further deterioration of the renal profile secondary to reflux. Although both intravesical and extravesical antireflux constructions have been successfully achieved laparoscopically, 18 –20 we favored extravesical reimplantation because it is an easier exercise and the morbidity consequent to breach of the bladder mucosa could be avoided. No patients in our cohort reported any voiding dysfunction postprocedure. Satisfactory antireflux construction was appraised in most scenarios in follow-up VCUG. The patient with grade I reflux did not need any additional interventions for reflux rectification.
Reported incidences of postoperative obstruction and reflux after various corrective procedures for MGU through incisional access range from 0% to15% and 0% to 17%, respectively. 21 The outcome achieved after laparoscopic reconstruction in our cohort is comparable to that in the published literature. Recently, reports of tailoring by a robotic approach have also been published in literature. 22 There is no availability of this modality in our institute, however, and hence we did not embark on this access.
In our patient cohort, the time needed for laparoscopic tailoring was significantly more than other laparoscopic ureteral reimplantations. This may be explained by the multitude of tasks performed during laparoscopic tailoring and reimplantation in comparison with other exercises (Fig. 3, author's own experience, unpublished data). Although long-term outcome after tailoring through incisional access has been derived, 23 no citations to date have reflected on the long-term outcome after laparoscopic tailoring. In our cohort, the 3-year follow-up outcome was also appreciable.
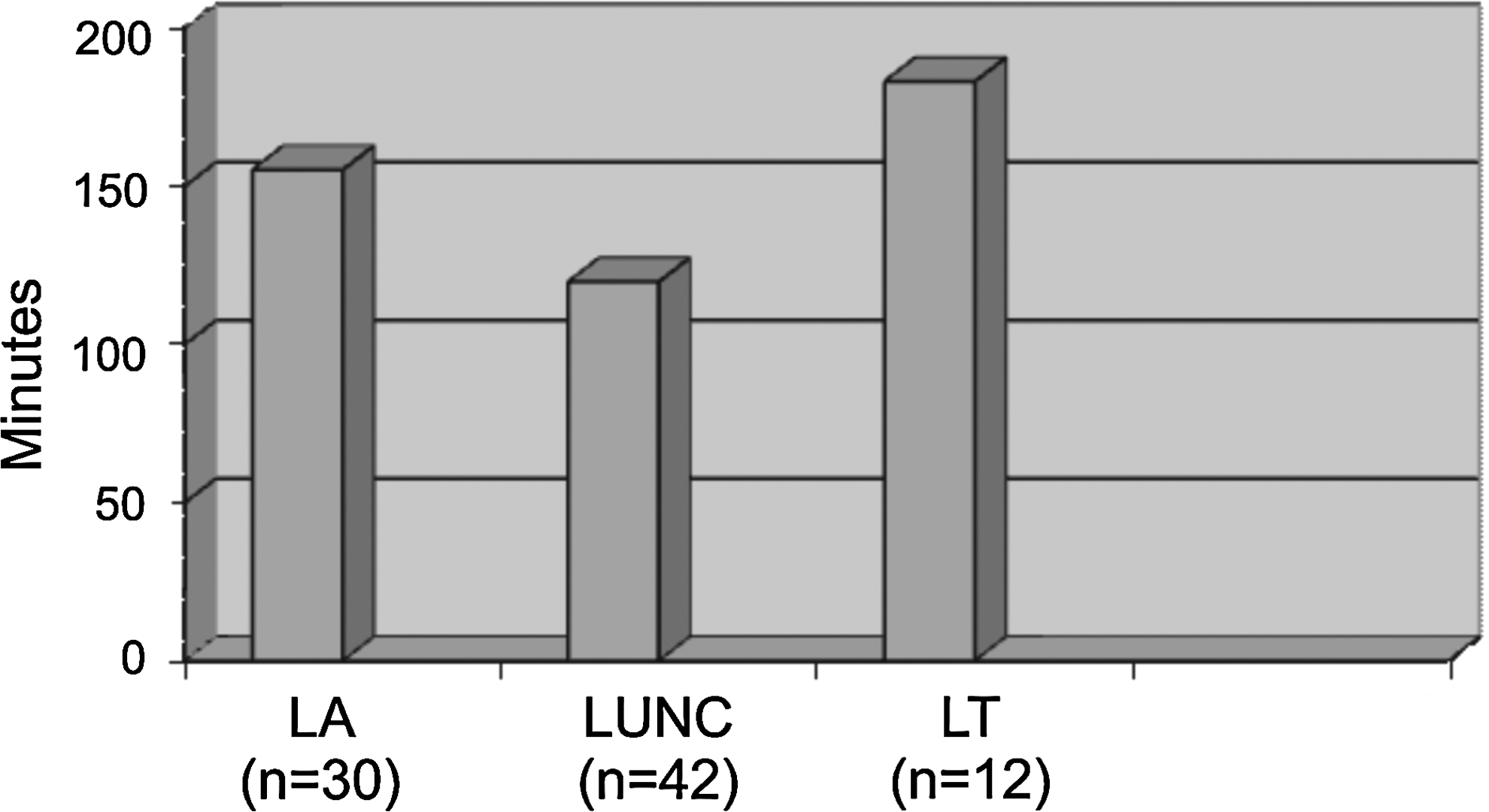
Comparison of operation duration of different laparoscopic ureteric reimplantations by the same operator. P=0.00, analysis of variance, operator's own series, unpublished data. LA=laparoscopic antireflux; LUNC=laparoscopic ureteroneo cystostomy; LT=laparoscopic tailoring.
Conclusion
Laparoscopic reconstruction for obstructive MGU is a feasible option with appreciable morbidity profile and durable results. Dismemberment, straightening the lower ureter, tailoring the lower segment, and tension-free nonrefluxing ureteroneocystostomy are key steps for this exercise. The intermediate-term outcome is also satisfactory.
Footnotes
Acknowledgments
Sooraj Rajasekharan Kartha contributed the statistics in this article.
Disclosure Statement
No competing financial interests exist.