
Abstract
Purpose:
We report our experience and present our technique with the robot-assisted laparoscopic ipsilateral ureteroureterostomy (IUU) in the management of ureteral duplication with ectopia in children.
Patients and Methods:
We reviewed our institutional experience for all patients who underwent a robot-assisted laparoscopic IUU at the University of Minnesota Amplatz Children's Hospital between December 2010 and October 2011. An intraoperative, three-port technique was used after a ureteral stent was placed into the ipsilateral lower pole. Demographic information, diagnosis, operative time, hospital course, complications, and follow-up were all evaluated.
Results:
Our series included four female patients and one male patient with a mean age of 61 months (6 to 182 mos). All five had a diagnosis of upper pole ectopic ureters, one of which was associated with an ureterocele. Mean total operative time was 225 minutes (181 to 253 min), and mean hospital stay was 1.2 days (1–2 days). There were no intraoperative complications. In follow-up, at the time of ureteral stent removal, pyelonephritis developed in one patient, but all patients had resolution of their presenting symptoms including urinary tract infections and incontinence. A significant reduction in upper pole hydronephrosis was seen in all patients.
Conclusions:
Our experience indicates that robot-assisted laparoscopic IUU is safe and effective in the management of ureteral duplication anomalies in children.
Introduction
There are a paucity of pediatric reports on robot-assisted laparoscopic management of ureteral duplication with IUU. We illustrate and evaluate our technique. 7
Patients and Methods
We performed an Institutional Review Board approved, retrospective chart review of all patients who underwent robot-assisted laparoscopic IUU by one surgeon (AS) between December 2010 and October 2011 at the University of Minnesota Amplatz Children's Hospital. In total, five patients, four female and one male, were identified. Patient 1, the oldest patient of the series, had already had a CT scan of her abdomen and pelvis at the time she was referred to our institution. The other four patients underwent preoperative investigation with renal ultrasonography and voiding cystourethrography. Upper pole renal function was evaluated with technetium-99m mercaptoacetyltriglycine diuretic renography or magnetic resonance urography. No patient had evidence of vesicoureteral reflux into the duplicated upper pole moiety. Patient 3 had a diagnosis of ectopic ureterocele that was not separately incised before the operation.
All patients were placed in the low lithotomy position. We began by performing cystoscopy, retrograde pyelography of the lower pole system, and placement of an appropriately sized indwelling Double-J ureteral stent into the lower pole ureter. The stent aids in the identification and mobilization of the ureter, while also serving as a scaffold during creation of the anastomosis. Postoperatively, the stent was intended to protect the anastomosis during initial recovery and reduce the chance of anastomotic leak.
A urethral Foley catheter was placed, followed by insertion of the robotic camera and arm trocars (Fig. 1). Initial placement of the camera port was midline infraumbilical by a modified Hasson technique with placement of a Veress needle through a small fascial incision. Once pneumoperitoneum to 12 mm Hg was achieved, a blunt tip 8-mm or 12-mm camera trocar was placed infraumbilically. Two 5-mm robot arm ports were then placed under direct vision. The arm port ipsilateral to the site of repair was positioned just lateral to the rectus belly approximately 1 cm inferior to the midline camera port. The arm port contralateral to the site of repair was positioned just lateral to the rectus belly at the level of the anterior superior iliac spine. The patient was then placed in the Trendelenburg position, and the robot was docked between the legs.
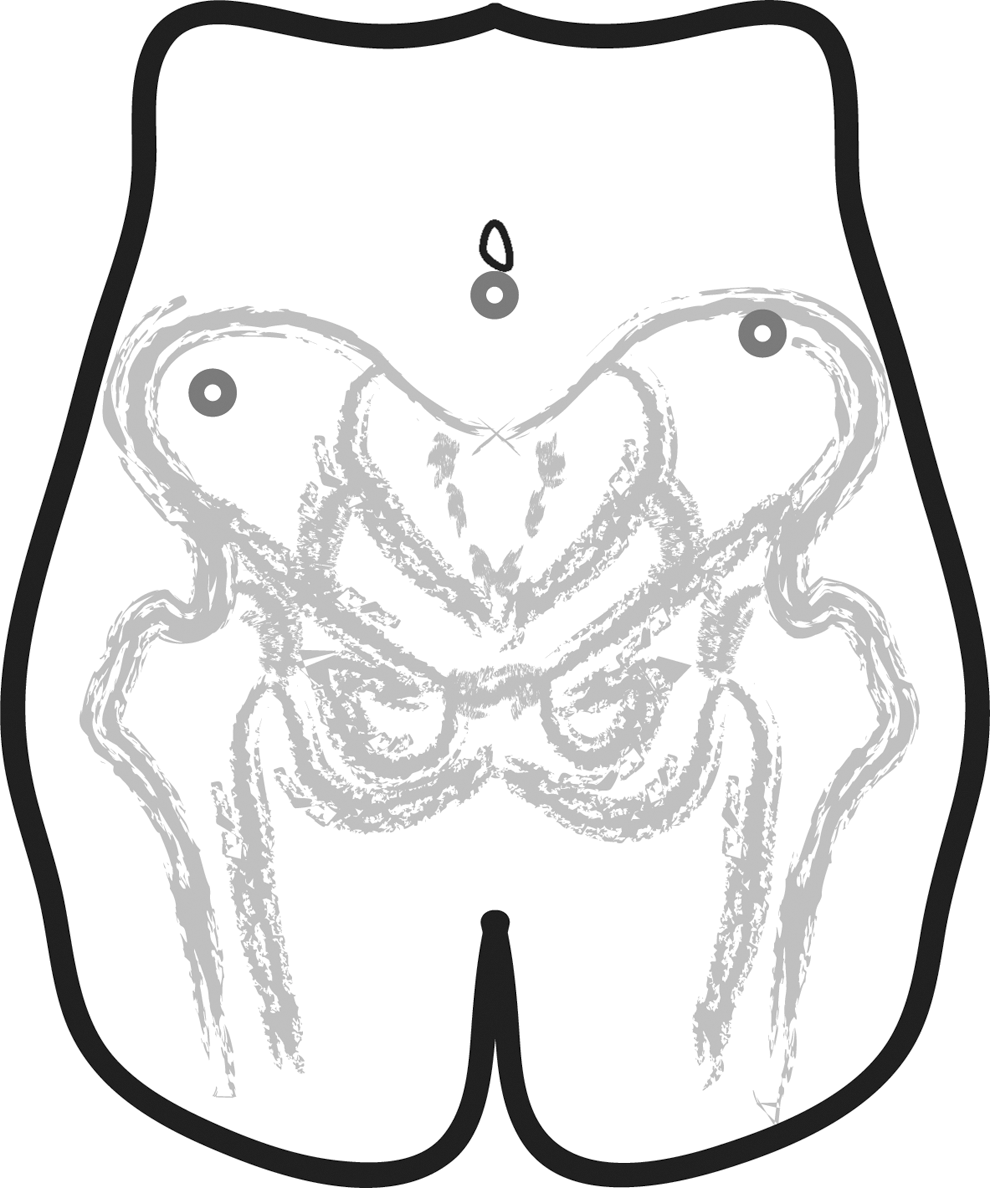
Schematic of robot camera (infraumbilical) and arm port placement for left ipsilateral ureteroureterostomy (IUU).
We chose to perform our mobilization and anastomosis at the level of the distal ureter, where it crosses the iliac vessels. At this location, using blunt dissection and electrocautery, the duplicated right or left ureters were identified without mobilization of the colon. Careful dissection with the aid of the previously placed stent was performed with a curved Maryland dissector and either cold scissors or a monopolar hook. Currently, there are no 5-mm monopolar scissors available with the daVinci system.
The dilated ectopic ureter was mobilized as distal as possible and divided using scissors (Fig. 2). An extracorporeal hitch stitch was used to improve exposure during creation of the anastomosis by gently distracting the lower pole ureter anteriorly (Fig. 2). For small patients, a 3-0 polypropylene suture with a straightened SH needle was used. For larger patients, a 2-0 polypropylene on a Keith needle was used. Tension was adjusted by clamping the suture outside the body. Proximally, the ectopic ureter was divided and spatulated as necessary to allow for an adequately sized anastomosis (Fig. 2).
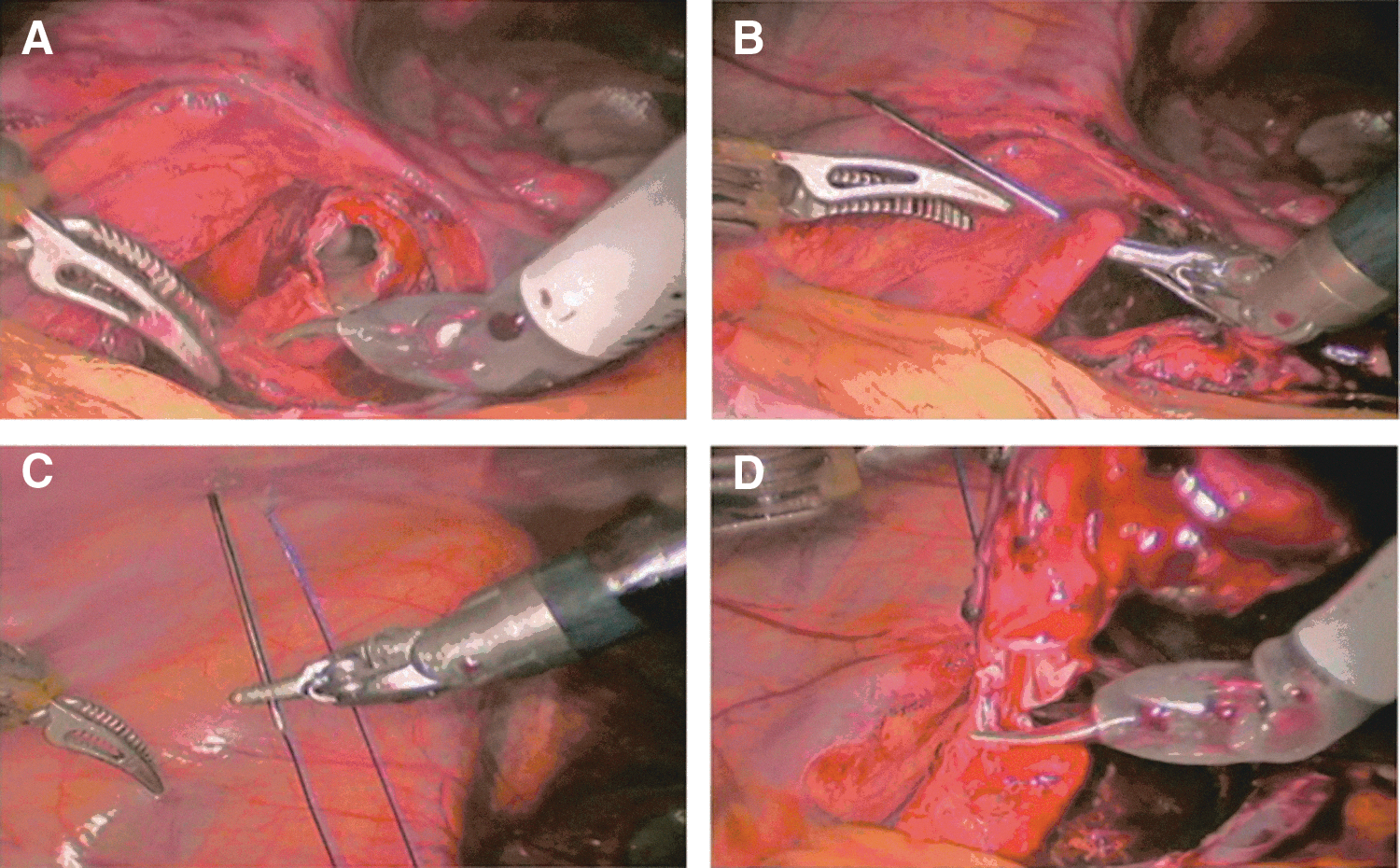
A left-sided robotic IUU.
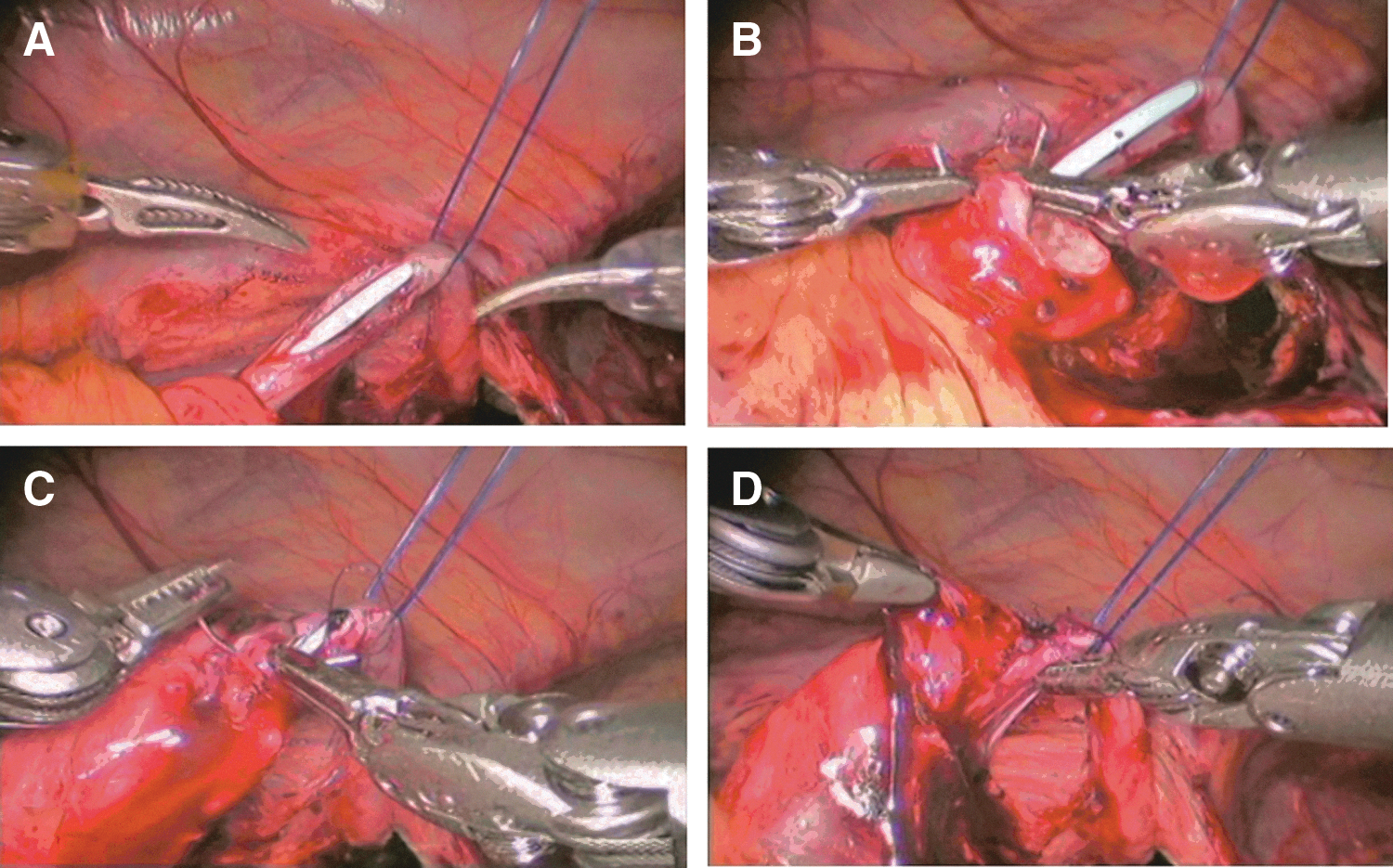
Scissors were used to open an anteromedial ureterotomy on the normally inserting lower pole ureter (Fig. 3). An end to side anastomosis was created using a combination of interrupted and running 5-0 or 6-0 polydioxanone sutures (Fig. 3). The lateral edge was first closed using a running stitch after which the posterior edge was closed under direct vision. The hitch stitch was then released, and if a surgical drain was placed, it was inserted through one of the 5-mm arm ports before port removal. The abdomen was deflated and ports were removed and examined for bleeding. The skin and port sites were closed using either 4-0 or 5-0 poliglicaprone subcutaneous sutures. The urethral Foley catheter, and drain if placed, were removed the following morning.
Results
Between December 2010 and October 2011, five robot-assisted laparoscopic IUUs were performed. Table 1 shows patient demographics and perioperative characteristics. Four patients were female and one was a male with a mean age of 61 months (6 to 182 mos). The 6-month-old female and 7-month-old male each presented with antenatal hydronephrosis. The 3-year-old female presented with a febrile urinary tract infection (UTI), and the 6-year-old female presented with voiding dysfunction, incontinence, and a febrile UTI. The 15-year-old female presented with continuous incontinence that had unsuccessfully been treated with a sacral neuromodulator device previously at another institution. All five patients had upper pole ectopic ureters, and patient 3 also had an associated ureterocele. The duplication anomalies were isolated to the left in three patients, isolated to the right in one patient, and bilateral in one patient with only the left side showing evidence for obstruction.
There were no intraoperative complications. Mean estimated blood loss was 4 mL (2–10 mL). Drains and urethral Foley catheters were removed on postoperative day 1. Mean total operative time was 225 minutes (181–253 min). This time represents the total procedure time and includes cystoscopy, retrograde pyelography, stent placement, patient positioning, robot-assisted procedure, and wound closure. The mean hospital stay was 1.2 days (1–2 days).
Ureteral stents were removed between 1 and 2 weeks in children older than 1 year. The 6-month-old girl had her stent removed at 4 weeks. The 7-month-old boy had his stent removed at 7 weeks rather than the anticipated 4 weeks because of familial scheduling preferences. Patients received an initial renal ultrasonography during a follow-up clinic visit a mean of 3 months after surgery. Patient follow-up has continued to present for a mean and median of 10 months (3–14 months).
One postoperative complication with pyelonephritis occurring 9 days after stent removal in the 6-year-old was observed. Her voiding dysfunction subsequently resolved, and she has not had any recurrent UTIs. On follow-up ultrasonography, resolved or significantly improved hydronephrosis was noted for all children. Complete sonographic resolution of the ureterocele in patient 3 was also noted. The 15-year-old experienced full resolution of her incontinence and complete resolution of her hydronephrosis. The previously placed neuromodulator was removed at the time of ureteral reconstruction.
Discussion
Minimally invasive surgical techniques are increasingly used in all aspects of reconstructive pediatric urology. 8 Robot-assisted laparoscopic ureteroureterostomy has been used in treating patients with single-system ureteral obstruction. 5 Our group has reported its experience with the robot-assisted single-system ureteroureterostomy and pediatric pyeloplasty. 6,9 Here we report our initial experience with robotic ipsilateral distal ureteroureterostomy for duplicated anomalies of the upper urinary tract, and we suggest that our results indicate that a robotic approach is feasible, safe, and provides another treatment option in children as young as 6 months old with complex duplication anomalies.
Our surgical technique includes the initial placement of the ureteral stent, a distal ureteroureterostomy, leaving in-situ a minimal distal ureteral stump of the transected upper pole ureter, and use of a “hitch-stitch” to aid with ureteral exposure. The ureteral stent aids with identification of the lower pole ureter, provides support during anastomosis, helps minimize potential back-walling of the recipient ureter, and theoretically should minimize urine leakage at the fresh anastomosis.
A distal anastomosis avoids manipulation and possible injury of the colon, gonadal vessels, and mesentery, which are necessary during more proximal anastomoses. Previous reports have shown low complication rates with incomplete removal of refluxing distal ureteral stumps in ectopic ureters and ureteroceles, which informs our own practice of mobilizing the upper pole, obstructed ureter to the deep pelvis and leaving a short stump. 10,11 The hitch-stitch around the recipient lower pole ureter helps to stabilize it and provides ample exposure during the ureteroureterostomy.
IUU is a well-established treatment modality in the surgical correction of duplex ureteral anomalies with a single obstructed ureter. 1,2,12,13 Our outcomes are comparable to open and pure laparoscopic approaches in terms of estimated blood loss, length of stay, improvement in upper pole hydronephrosis, and postoperative complications. 3,8,14 We experienced no intraoperative complications, and no case needed open conversion.
Operative time was similar to those in other small series of laparoscopic IUU 3,12,14 ; however, it was longer than that of a larger open series. 15 In the open series, the mean age of 10 months (2–56 mos) was significantly less than that of our series, which had a mean age of 61 months (6–182 mos). Compared with open surgery, the technique described here is longer because of a number of additional steps, such as cystoscopy, retrograde stent placement, and robot docking. We anticipate the operative times will diminish as the experience increases for the entire clinical staff. This learning-curve phenomenon is common and expected with the dispersion of new surgical procedures and technologies.
Robot assistance provides many benefits for the surgeon in comparison with standard laparoscopy. The use of wristed instrumentation, tremor abolition, and motion scaling in robotic surgery enhances dexterity by almost 50% compared with laparoscopic surgery. The use of three-dimensional visualization further enhances dexterity by 10% to 15% and decreases skills-based errors by 93%. 16 Furthermore, studies indicate that robot assistance helps reduce the learning curve for novices in suturing compared with standard laparoscopic procedures and enhances economy of motion for experts. 17 There is also emerging evidence that the use of the da Vinci robot may help to overcome innate handedness. 18 With specific regard to ureteroureterostomies, robot assistance allows for precise sharp dissection and spatulation of the ureter compared with standard laparoscopy. 19
In addition to the benefits over the standard laparoscopic procedure, previous studies indicate that robot assistance may offer certain advantages over open techniques. In a comparison of robot-assisted vs open pediatric pyleoplasties, the robot-assisted group had decreased hospital stay, decreased narcotic use and operative times at our institution. 20 We also found that pediatric robotic extravesical reimplantation similarly reduces length of hospitalization and narcotic requirement compared with the open cohort. 21 In addition, robot assistance may improve cosmesis with smaller incisions. 8
Pyelonephritis developed in a single patient. Her ureteral stent was removed at home and she developed pyelonephritis the following day. The suture dangle of the ureteral stent had been left intact transurethrally and secured to the patient's thigh, which we believe may have increased this patient's risk for UTI because of ascending colonization. We no longer leave the suture dangle and remove the ureteral stent cystoscopically if the stent is forecasted to be left in place for more than 7 days. One of the early laparoscopic ureteroureterostomy series noted two episodes of pyelonephritis in six patients (eight ureteroureterostomies), and these patients also had the transurethral string attached to the ureteral stent. 3
The robotic approach is applicable to males and females and to a wide range of pediatric ages, from the infant to the adolescent, with encouraging results in all patients. Four of the five patients in this study were female, and this is consistent with the known female predominance of duplex anomalies with ectopia. We anticipate patients with bilateral duplication anomalies could also be safely approached with robot assistance by placing each arm port lateral to the rectus bellies and 1 to 2 cm inferior to the umbilical camera port. Alternatively, the addition of a third robotic arm port would allow for independent and improved triangulation of the right and left side.
Conclusions
Our results indicate that the robot-assisted laparoscopic IUU is a safe and effective means to resolve ectopic, duplicated ureters in children. While many genitourinary reconstructive procedures are difficult to perform laparoscopically because of the inherent complexity of intracorporeal manipulation with extended learning curves, robot assistance may shift that curve and facilitate widespread adoption of complex minimally invasive techniques.
Footnotes
Acknowledgment
Dr. Paul Gleich assisted with image creation and formatting.
Disclosure Statement
No competing financial interests exist.