
Abstract
Purpose:
The purpose of the study was to prospectively compare operative and postoperative characteristics and outcomes in elderly patients undergoing percutaneous nephrolithotomy (PCNL) compared with younger patients.
Patients and Methods:
Prospectively collected data from the Clinical Research Office of the Endourological Society (CROES) Global PCNL Study database were used. Elderly patients were defined as those aged 70 years and above, while younger patients were those between 18 and 70 years of age. Matched and unmatched group comparisons were performed based on imaging modality used for assessing stone-free status. Patient characteristics, operative data, and postoperative outcomes were compared.
Results:
The median age of the elderly group vs the young group was 74 years (range 70–93 years) vs 49 years. In the unmatched analysis, staghorn stones were seen at higher rates in the elderly group (27.8% vs 21.8%, P=0.014); however, the mean stone size was not significantly different (465.0 vs 422.8, P=0.063). The length of hospitalization was significantly longer in the elderly group compared with the young group in the unmatched analysis (5 days vs 4.1 days, P<0.001). The same difference was not apparent in the matched analysis (5.0 days vs 4.4 days, P=0.288). Overall complication rates were not significantly different in the unmatched analysis. In the matched analysis, however, a statistically significant higher rate of overall complications was seen. Stone-free rates were similar among all groups.
Conclusion:
PCNL in elderly patients over the age of 70 years produces results comparable to those seen in younger patients. With only a slightly higher—be it statistically significant—complication rate, the stone-free rate in older patients was the same as in the younger group.
Introduction
Kidney stone disease is associated with a very high recurrence rate after an initial episode. The recurrence rate varies from 30% to 50% after 5 years. Data on the management of stones in the elderly are lacking, with very few published results. Also, the definition of “elderly” continues to be revised upward as life expectancy increases and medical advances result in less morbidity associated with treatment of the elderly.
The purpose of the Clinical Research Office of the Endourological Society (CROES) Global Percutaneous Nephrolithotomy (PCNL) Study was to establish a prospective global database for the current indications and outcomes of PCNL. The objectives of the present study were to compare the patient characteristics, operative characteristics, and outcomes in elderly patients with younger patients undergoing PCNL. It was anticipated that the endourologist would not be as compulsive about rendering an elderly frail patient totally stone free.
Patients and Methods
The CROES Global PCNL Study was a prospective observational study during which data were collected for consecutive patients who were treated at each participating center over a 1-year period. The study organization and methods have been published previously. 9 The patient was considered stone free after all stones had been cleared and remained clear for 30 days after treatment. Inclusion criteria were patients above 18 years of age. Patients with previous PCNL, solitary kidney, renal congenital anomalies were excluded from the current analysis. The patients were grouped according to age as follows:
Elderly: Defined as 70 years and above.
Younger: Defined as 18 to 70 years.
A matched sample of an equal number of elderly and younger patients was created. Stone-free status assessment methods included CT scan, Ultrasonography, and plain abdominal radiography of the kidneys, ureters, and bladder (KUB). In creating the matched sample, equal numbers of elderly and younger patients assessed for stone-free status with the same imaging modality (CT, ultrasonography, KUB) were chosen, and the sample was balanced according to presence of staghorn stones and location and number of stones (Fig. 1). Stone-free status was defined by the contributing center based on the criteria set by the individual contributing centers. Direct comparison of the demographic characteristics, preoperative and postoperative data, and outcomes between the two groups was performed with both unmatched and matched samples. Data were compared descriptively in the two patient groups.
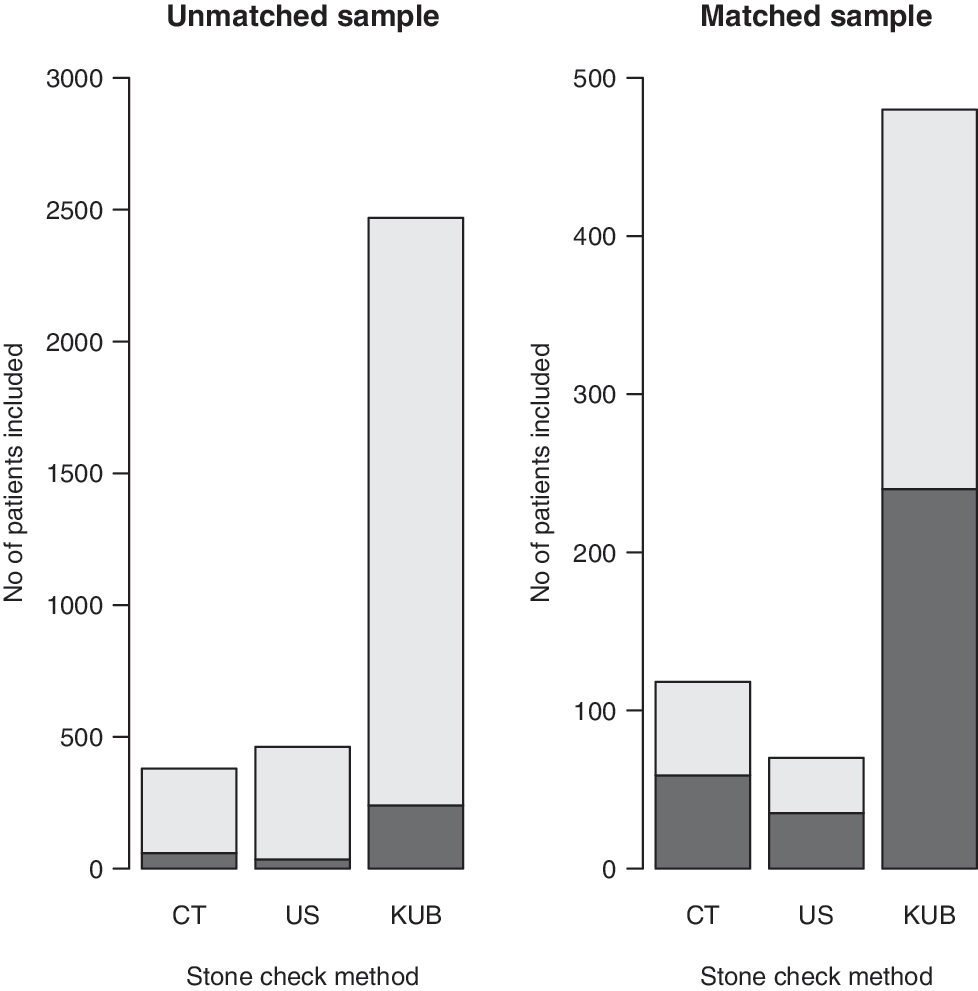
Stone check methods used in matched and unmatched samples. Dark shade represents elderly patients, light shade represents younger patients. CT=computed tomography; US=ultrasonography; KUB=kidneys, ureters, and bladder.
The level of significance for differences between groups was estimated using chi-square tests and Mann-Whitney U tests for categorical and continuous variables, respectively. Perioperative complications were assessed and graded according to the modified Clavien system applied to PCNL. 10 Statistical significance was defined as P<0.05.
Results
A total of 334 patients meeting the elderly definition was compared with 2976 younger patients in an unmatched sample analysis. The median age of the elderly group vs the younger group was 74 years (range 70–93 years) vs 49 years (range 18–69 years). Similar age difference was seen for the matched sample analysis (Tables 1A, 1B). Statistically significantly higher rates of comorbid diseases, higher American Society of Anesthesiologists scores, anticoagulant use, were seen in the elderly patients across both the matched and unmatched samples. Elderly patients had lower mean preoperative estimated glomerular filtration rates (EGFR) compared with the younger patients across both matched and unmatched samples.
SD=standard deviation; ASA=American Society of Anesthesiologists; EGFR=estimated glomerular filtration rate.
SD=standard deviation; ASA=American Society of Anesthesiologists; EGFR=estimated glomerular filtration rate.
Operative characteristics were similar across both groups in both the matched and unmatched samples with the exception of the supine approach being used more frequently in the young group in the matched sample analysis (Tables 2A, 2B). Collecting system perforation was also seen more commonly in the elderly group in the matched sample analysis. The mean drop in hemoglobin and transfusion rates was not statistically significant across both groups in both matched and unmatched analyses (Tables 2A, 2B). In the unmatched analysis, staghorn stones were seen at higher rates in the elderly group (27.8% vs 21.8%, P=0.014); however, the mean stone size was not significantly different (465.0 vs 422.8, P=0.063). In the matched analysis, however, staghorn stones rates were similar (27.8% vs 27.8%, P=0.931), but a significantly larger stone burden was seen in the elderly (465.0 mm2 vs 357.2 mm2, P<0.001) (Tables 3A, 3B).
SD=standard deviation.
SD=standard deviation.
SD=standard deviation.
Matching variables
SD=standard deviation.
Postoperative outcomes were mostly similar with some notable exceptions. As expected, length of hospitalization was significantly longer in the elderly group compared with the younger group in the unmatched analysis (5 days vs 4.1 days, P<0.001). The same difference was not apparent in the matched analysis (5.0 days vs 4.4 days, P=0.288). There was a slight reduction in EGFR estimated from creatinine collected in the immediate postoperative period in both groups after PCNL. Elderly patients had a postoperative fever rate of 7.5% vs 9.2% in the unmatched sample and 7.5% vs 5.2% in the matched sample. These rates were not statistically significant. Subgroup analysis, however, showed significantly higher Clavien classifications in the elderly, with Clavien IVA complications accounting for the majority of the difference. In the matched analysis, a statistically significantly higher rate of overall complications was seen. This difference persisted across higher Clavien classifications. The re-treatment rates, stone-free rates, and modality of re-treatment were not significantly different (Tables 4A, 4B). Complication rates and length of stay were greater among the elderly patients when analysis was limited to high volume (>100 cases) centers (Tables 5).
CT=computed tomography; US=ultrasonography; KUB=kidneys, ureters, and bladder; URS=ureteroscopy; PCNL=percutaneous nephrolithotomy; SWL=shockwave lithotripsy; SD=standard deviation; EGFR=estimated glomerular filtration rate.
CT=computed tomography; US=ultrasonography; KUB=kidneys, ureters, and bladder; URS=ureteroscopy; PCNL=percutaneous nephrolithotomy; SWL=shockwave lithotripsy; SD=standard deviation; EGFR=estimated glomerular filtration rate.
SD=standard deviation; EGFR=estimated glomerular filtration rate.
Discussion
Untreated large burden urolithiasis is associated with a risk of chronic deterioration of renal function. 11 –13 Also, the risk of urinary tract infection and sepsis is present when obstruction results from an untreated stone. As a result, treatment is often recommended in patients who are able to tolerate the associated morbidity. For most small, asymptomatic stones in the elderly with significant comorbidities, observation is preferred. As reported by Burgher and associates, 14 progression of disease is seen more often than not in observed stones. In that study, 77% of 300 male patients with an average age of almost 63 years with a diagnosis of asymptomatic renal stones, observed for a mean duration of nearly 3.3 years, experienced progression. The study authors noted a positive correlation between stone size of 4 mm or larger and progression of disease during the period of observation. 14 The safety and effectiveness of extracorporeal shockwave lithotripsy (SWL) has been well established in elderly patients and is often the most commonly used modality in elderly patients. 15 Some reports, however, have suggested that SWL might be less efficacious in elderly patients. 16 In some cases, PCNL thus becomes the optimal and most efficient surgical option, particularly in cases where multiple anesthetic sessions may be risky.
Comorbid disease is known to be more prevalent in the elderly. In a comparison of datasets from Kidney Early Evaluation Program, National Health and Nutrition Examination Survey 1999 to 2006 and data on chronic kidney disease as determined from billing codes in a Medicare 5% sample, Stevens and colleagues 17 noted a higher prevalence of diabetes, hypertension, high cholesterol level, coronary artery disease, congestive heart failure, cerebral-vascular disease, peripheral vascular disease, and cancer in patients 75 years and older. The authors also observed a higher prevalence of chronic kidney disease and its associated complications of anemia, hypocalcemia, hyperphosphatemia, and hyperparathyroidism. This observation was true across all three data samples.
In our study, in both the matched and unmatched samples, comorbid diseases were seen more commonly in the elderly (Tables 1A & 1B). Also, there was a greater rate of anticoagulant use in the elderly group when compared with the younger cohort (Tables 1A & 1B). Anticoagulant use has been associated with the presence of cardiovascular disease and other chronic illnesses. 18 Hence, the elderly patients in this group can be assumed to have a higher prevalence of cardiovascular disease. Despite these higher rates of associated comorbidities, the elderly patients in our unmatched cohort had postoperative complication rates similarto the younger patients (19.9% vs 17.4%, P=0.286) (Table 4A). In the matched sample, however, the complications rates seen in the elderly cohort were higher (19.9% vs 6.6%, P<0.001) (Table 4B). These complication rates are low and acceptable when compared with other studies. 15,19
Optimizing medical management of chronic comorbid diseases is important in controlling the anesthetic risks associated with surgery. The surgeon's experience with the procedure is also important so that an experienced surgeon would not find PCNL technically more challenging in an elderly patient. As shown in our study, the total operative time was not significantly different among the groups in both the matched and unmatched samples. Despite a higher rate of anticoagulant use, the mean drop in hemoglobin as well as transfusion rates did not differ significantly in our elderly group compared with the younger group (Tables 4A & 4B).
Length of hospitalization was predictably longer for the elderly group when compared with the younger group in our study (Tables 4A & 4B). Stone-free rates were similar for both the elderly and the younger groups of patients. This is in keeping with the results from other studies showing excellent stone free-rates for elderly patients comparable to that of younger patients. 15,19
One potential weakness of this study is that the definition of stone-free status was not uniform at all centers. Stone-free status was defined by the contributing center based on the criteria set by that institution. This ranged from no residual fragments, fragments less than 2 mm, and less than 4 mm. Imaging modalities used for assessment of stone-free status were helical CT, ultrasonography, and in some cases, nephrostography and KUB. We accounted for these differences in our matching protocol to ensure that appropriate comparisons of stone-free status were made across the elderly and younger groups. It is understood that the gold standard imaging modality for stone-free status determination is helical CT. 20,21 This has not become the standard practice at centers across the globe, however, for several reasons, including cost and availability.
Conclusions
This current study supports the efficacy and safety of PCNL in elderly patients. Stone-free status in the elderly was the same as in the younger group. In spite of a well-established increase in comorbidity in the elderly, the outcome is the same with only a mild increase in complications.
Footnotes
Acknowledgment
The Global PCNL Study was supported by an unrestricted educational grant from Olympus.
Disclosure Statement
No competing financial interests exist.