
Abstract
Background and Purpose:
Surgical intervention is warranted for symptomatic congenital bladder diverticula (CBD) in children. We hypothesized that a robot-assisted approach to bladder diverticulectomy could be performed with safety and with good efficacy. Descriptions of our approach and results with robot-assisted laparoscopic bladder diverticulectomy (RALBD) are presented.
Patients and Methods:
We retrospectively reviewed a prospective database with Institutional Review Board approval. Eligible patients were those who underwent excision of a bladder diverticulum via a robotic approach. Data were collected on presenting symptoms, and intraoperative and postoperative courses. Voiding cystourethrography (VCUG) was performed at 3-month follow-up. Renal and bladder ultrasonography was performed at 3- and 12-month follow-up.
Results:
Fourteen patients were identified. Of the 14 patients, 6 also had a history of diurnal enuresis. Mean patient age was 7.9 years (range 4–13 years). The operation was performed via a transperitoneal approach with robot assistance. The mean operative time (including cystoscopy) was 132.7 minutes (range 113–192 min). The average length of stay was 24.4 hours (range 18–31 hours). There were no intraoperative or postoperative complications in this group. Each patient was followed for at least 1 year. All patients had a normal results of VCUG on follow-up without evidence of a diverticulum. Within 3 months, diurnal enuresis resolved in 6/6 patients.
Conclusions:
RALBD appears to be a safe and effective modality for treatment of patients with CBD. It can serve as an alternative to the open surgical approach.
Introduction
Various surgical approaches to excise CBD have been used, including transvesical, extravesical, and laparoscopic. To our knowledge, a single case report of robot-assisted laparoscopic bladder diverticulectomy (RALBD) in children exists in the literature. 3 We hypothesize that a robot-assisted approach to bladder diverticulectomy can be performed with safety and with good efficacy in the pediatric population. Descriptions of our approach and results of our series of RALBD are presented.
Patients and Methods
We retrospectively reviewed an Institutional Review Board approved prospective database of patients undergoing a minimally invasive surgical procedure at our pediatric institution from 2005 to 2011. Parents consented to inclusion in the database for the patients before the minimally invasive intervention. Eligible patients were those who underwent excision of a congenital (primary) bladder diverticulum via a robotic approach. Diagnosis of the lesion was based on findings from preoperative voiding cystourethrography (VCUG) (Fig. 1). Those with vesicoureteral reflux into a ureter associated with a paraureteral diverticulum were excluded from this review.
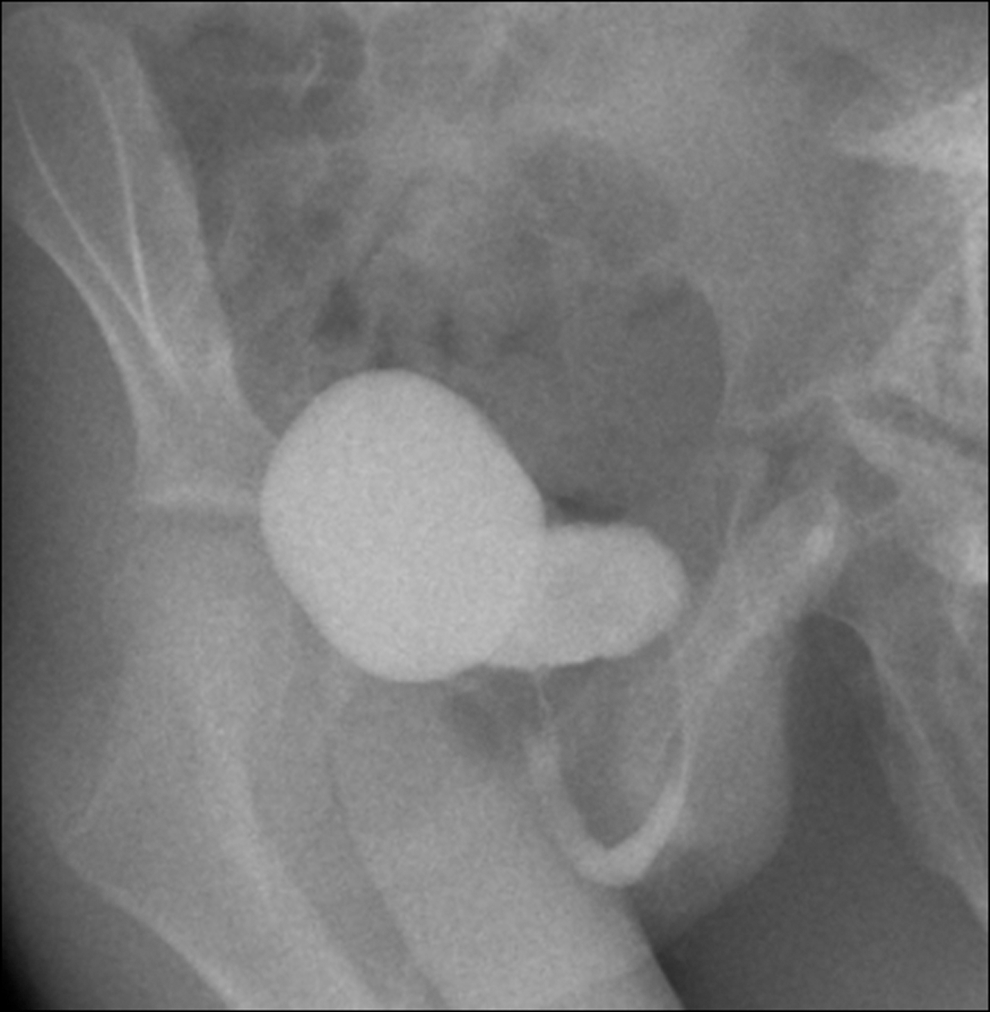
Large congenital bladder diverticulum demonstrated on a voiding cystourethrogram.
A prophylactic dose of antibiotics was administered intravenously within 30 minutes of the start of the case. Cefazolin was typically used in a dose of 25 mg/kg unless allergies dictated choice of another antibiotic. The procedure began with a cystoscopy to assess the precise location of the diverticulum as well as its proximity to a ureteral orifice. Cystoscopy was most often performed with a Wolf 10F pediatric cystoscope with a 5F working channel and a 25-degree lens. A 3F or 4F whistle-tipped ureteral catheter was used to intubate the ipsilateral ureter to aid with identification during transperitoneal dissection of the diverticulum. In cases of very large CBD, both ureters may need to be intubated.
The patients were then repositioned into a supine Trendelenburg position with the legs separated. An 8.5-mm camera port was then placed at the umbilicus, and an 8-mm working port was placed along the midclavicular line at a level approximately one fingerbreadth caudal to the umbilicus (one working port on each side). The robot (da Vinci Surgical System,® Intuitive Surgical, Sunnyvale, CA) was docked after pneumoperitoneum was established. Transperitoneal dissection of the diverticulum then proceeded. The peritoneal lining over the posterior bladder was opened and dissection continued down to the stalk of the diverticulum (Fig. 2). The diverticulum was then sharply excised (Fig. 3), and the bladder was closed in two running layers with 4-0 polyglactin suture (Fig. 4).
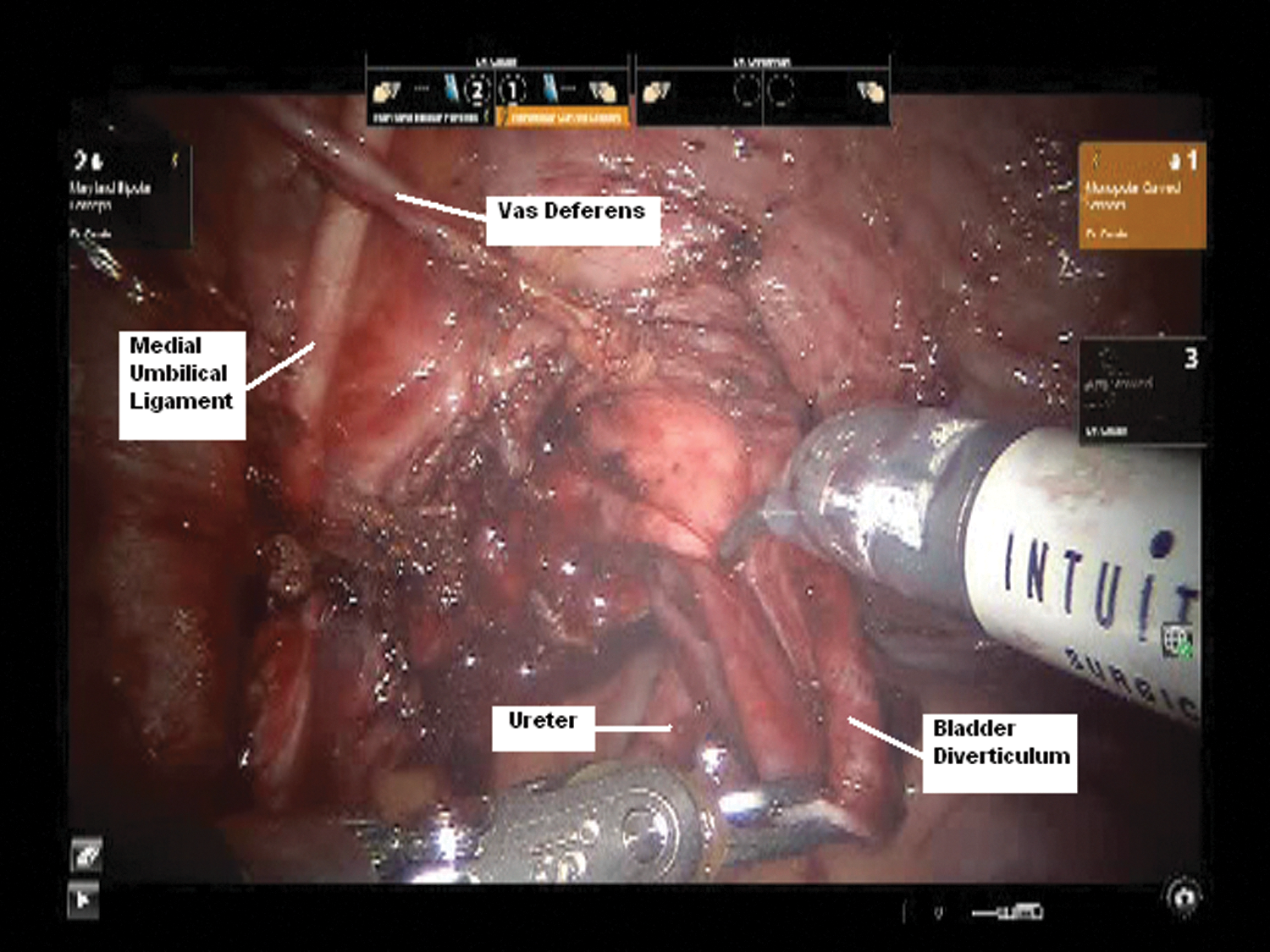
Transperitoneal view of a bladder diverticulum demonstrating dissection of the diverticulum down to its connection with the bladder.
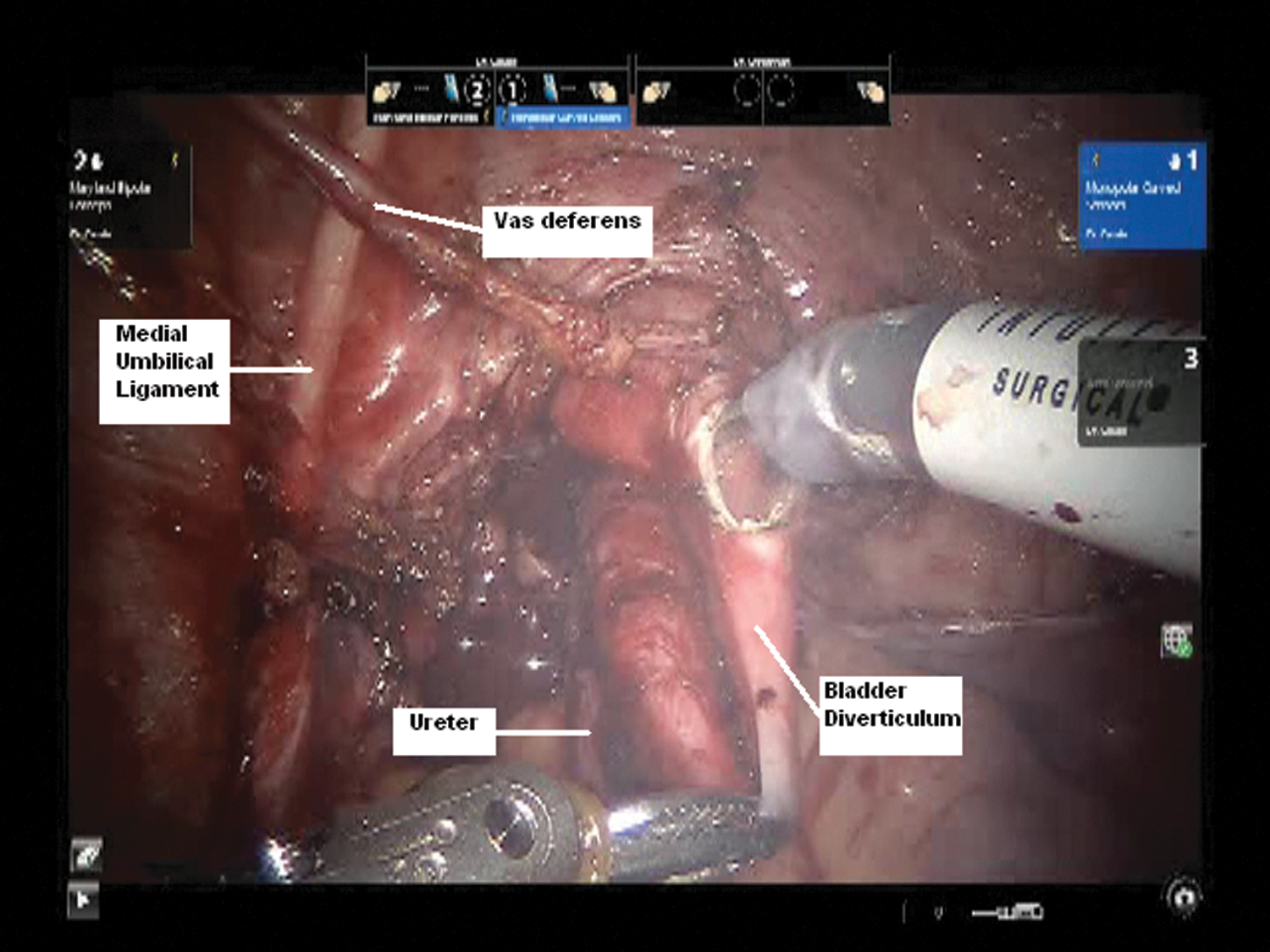
Preparing to excise the diverticulum by cystotomy near its neck.
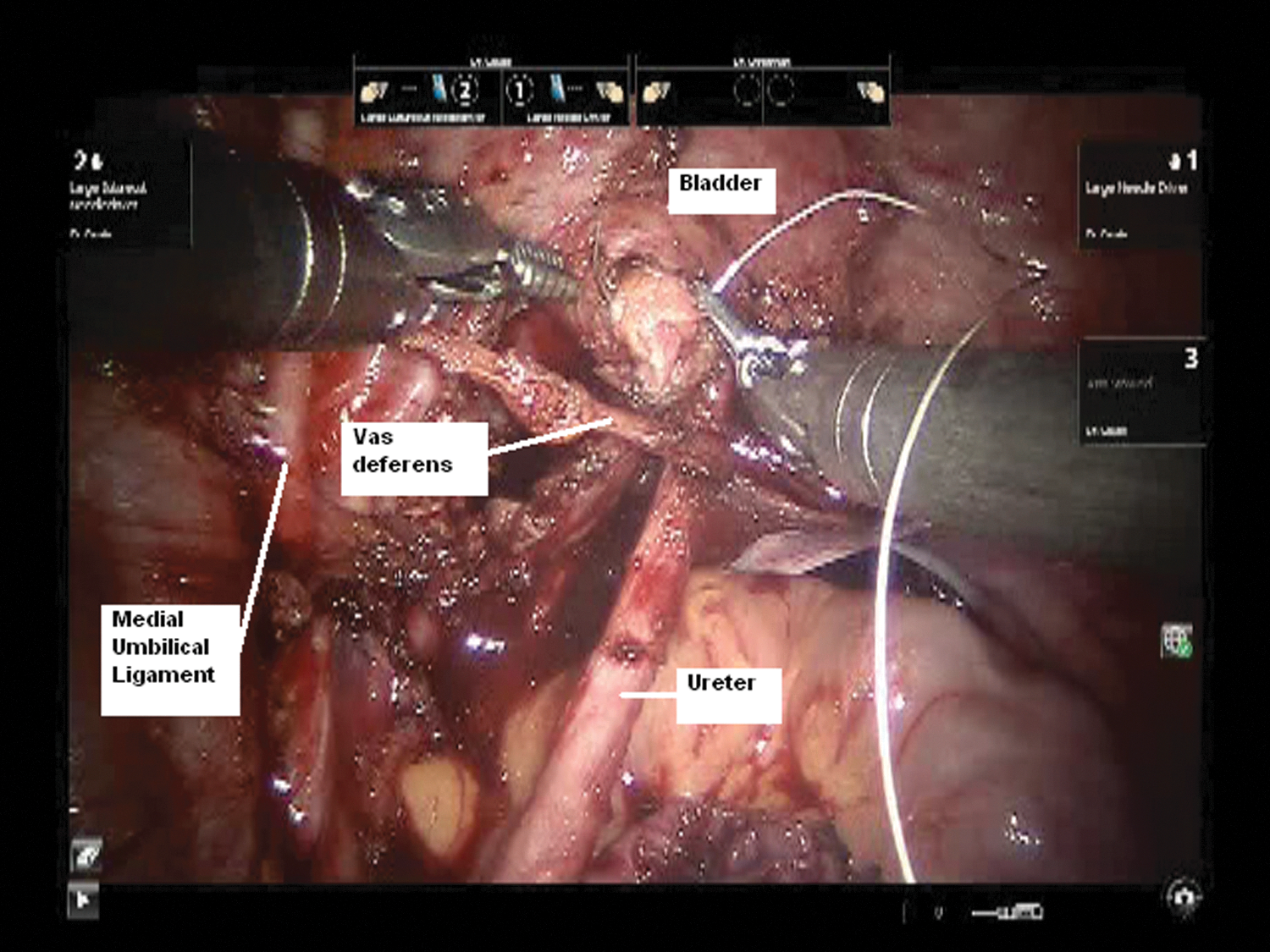
Closure of the cystotomy in watertight fashion.
The ureteral catheter and a Foley catheter were left in place at the conclusion of the procedure and were subsequently removed in the morning of the first postoperative day. Patients were later discharged after demonstrating an appropriate void.
Data were collected on presenting symptoms, operative time, length of stay, complications, uroflow with postvoid residual measurement, and resolution of presenting symptoms. VCUG was performed at the 3-month follow-up. Renal and bladder ultrasonography (RBUS) was performed at the 3- and 12-month follow-up.
Results
Bladder diverticula were found in 23 patients during the study period. Nine had a small paraureteral diverticulum associated with ipsilateral reflux and were therefore excluded from this series; these patients underwent ureteral reimplantation. The remaining 14 patients underwent excision of an isolated large CBD. Of the study group, 13 were boys and 1 was a girl. Mean patient age was 7.9 years (range 4–13 years).
All patients presented with recurrent cystitis and had completed toilet training at the time of diagnosis. Recurrent cystitis was defined as more than one episode per year of a symptomatic and documented culture-positive urinary tract infection. Four patients (29%, 4/14) had a history of febrile urinary tract infections. Of the 14 patients, 43% (6/14) also had a history of diurnal enuresis with a sense of urgency immediately after voiding. The remaining patients did not have enuresis but did have symptoms of frequency/urgency and sensations of incomplete emptying. RBUS was obtained in each given the history of recurrent cystitis in conjunction with symptoms of voiding dysfunction. The presence of the diverticulum on ultrasonography then prompted performance of VCUG. None had vesicoureteral reflux. All diverticula were noted to be large and did not empty completely on VCUG.
The mean operative time (including cystoscopy) was 132.7 minutes (range 113–192 min). The CBD were identified in the posterolateral wall of the bladder, in proximity to the ureter in all patients. Estimated blood loss was minimal (<10 mL) in all cases. Urethral catheters were removed the morning after surgery in each patient. The average length of stay was 24.4 hours (range 18–31 hours). There were no intraoperative complications in this group. Postoperative urinary retention or an urinoma did not develop in any patient.
Every patient was followed for a minimum of 1 year. All patients had a normal results of VCUG and RBUS at their 3-month follow-up, without evidence of a diverticulum. Similarly, the RBUS result at 12-month follow-up was also normal. No further episodes of cystitis developed postoperatively in any patient. Within 3 months, diurnal enuresis resolved in 6/6 patients. Symptoms of frequency and urgency improved in all.
Discussion
Primary (aka congenital) bladder diverticula are classified as false diverticula in which the bladder mucosa herniates through a defect of the smooth muscle fibers of the bladder. The exact etiology for development of the primary lesions has not been defined; secondary bladder diverticula have been attributed to infravesical obstruction. The true incidence of CBD is unknown, although it has been estimated to occur in 1.7% of symptomatic children. 4 Persons with connective tissue disorders such as Williams elfin-facies, Menkes, and Ehlers-Danlos syndromes are thought to be at a higher risk for this anomaly. 5 –7 Furthermore, CBD occur almost exclusively in male patients. although some rare cases in girls have been described. 2,8
The pathophysiology of CBD has been well described. 8 It is thought that a large, posterior, inferiorly placed diverticulum passively fills during the filling phase of the bladder cycle. As the bladder contracts, urine is displaced into the diverticulum causing it to fill further. This displaces and compresses the proximal urethra, thereby causing outflow obstruction. The outflow obstruction leads to further filling of the diverticulum and therefore continuation of this cycle. In some cases, these large CBD can directly cause obstruction of the ureters, as well. 9
VCUG has been the mainstay of diagnostic evaluation of CBD. This study provides useful information related to concurrent vesicoureteral reflux as well as anatomic and functional imaging of the bladder neck and urethra. Intravenous pyelography or magnetic resonance urography can help to further define the relationship between the diverticulum and the ureter, especially in cases without reflux. Ultrasonography is also often used in theinitial workup of these patients. Identification of bladder diverticula on prenatal ultrasonography has also been described. 10
Reports of laparoscopic bladder diverticulectomy began to surface in the early 1990s. 11 This initial report described a transperitoneal approach; descriptions of extraperitoneal techniques soon followed. 12 With the introduction of the robot into the marketplace, its use for these procedures was not far behind. 13 A review of minimally invasive bladder diverticulectomy in 2010 identified 46 patients who underwent a laparoscopic procedure (from 17 articles), and 8 published reports of robot-assisted diverticulectomy with each of these robotic series having fewer than five patients. 14 These limited data were focused on an older, adult cohort of patients.
Experience with minimally invasive approaches to bladder diverticulectomy in pediatric patients is even less robust. Figenshau and associates 15 described a simultaneous laparoscopic nephroureterectomy and bladder diverticulectomy in a 6-year-old boy. Badawy and colleagues 16 described a pneumovesicoscopic approach that was derived from experience with laparoscopic ureteral reimplantation in the pediatric population. In the three patients (all boys), the mean operative time was 133 minutes. All patients in this series were discharged on the second postoperative day, and all had normal postoperative RBUS and VCUG results with a mean follow-up of 5 months.
Marte and coworkers 17 expanded on this series with their description of the procedure in six boys. Operative time in this series was slightly less, at 110 minutes. Postoperative ultrasonography and VCUG demonstrated resolution of the diverticulum. Two patients with voiding dysfunction had resolution of their symptoms of urgency, confirmed by urodynamics. Each author emphasized the value of the pneumovesicoscopic approach in avoiding entry into the peritoneum.
Overall, operative times and postoperative outcomes appear similar between these series of the pneumovesicoscopic approach when compared with this present series of the transperitoneal approach to minimally invasive bladder diverticulectomy. It should be noted, however, that bladder capacity can be a significant limiting factor for the pneumovesicoscopic approach in the pediatric population. The first, and to our knowledge only, previously published report of robot-assisted bladder diverticulectomy in children was published in 2009. 3 Advantages of the robot include three-dimensional visualization and articulating instruments that allow for dissecting and suturing work to be completed within the narrow pediatric pelvis and retrovesical space.
One of the limitations of the transperitoneal approach can be identification of the diverticulum. Several strategies have been described to help ease this difficulty. Placement of a Councill tip catheter over a stylet that has been placed directly into the diverticulum can then allow inflation of the catheter balloon within the diverticulum itself. 18 In similar fashion, others have described placement of an angiographic catheter into the diverticulum. 13 Another novel aid that has been described involves use of a flexible cystoscope to provide focused light into the diverticulum, enabling identification from within the peritoneum. 19
The retrospective nature of our study in this small cohort is a limitation of our study. The rarity of CBD precludes a comparison with a contemporary series of alternative approaches from our institution. Similarly, a comparative cost analysis cannot be performed, although the robotic approach is known to have equipment costs not needed for open surgery or even conventional laparoscopy. The rarity of this lesion could also potentially affect proficiency of the operation. It should be noted, however, that Hong and colleagues 20 recently showed that proficiency could be achieved with the robot for removal of retrovesical cysts—another rare anomaly.
Conclusions
RALBD appears to be a safe and effective modality for treatment of CBD in children. It should be considered as an alternative to the traditional open and laparoscopic surgical approaches.
Footnotes
Disclosure Statement
No competing financial interests exist. The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.