
Abstract
Purpose:
To present a critical overview of the current literature on the role of laparoscopy for the surgical treatment of patients with large prostatic adenomas.
Materials and methods:
A MedLine search for peer-reviewed studies on laparoscopic simple prostatectomy (LSP) was performed. The clinical studies that reported most of the following information were included: number of patients, prostate volume, operative time, blood loss, hospital stay, and the duration of catheterization, as well as functional outcomes and complications. Articles reporting a mean total prostate volume of <80 mL or a mean prostatic adenoma of <60 mL were excluded. The review was performed according to the PRISMA statement.
Results:
Fourteen articles on LSP were included in this systematic review with a total of 626 patients treated. Both transperitoneal and extraperitoneal approaches, as well as transvesical and transcapsular routes, have been described. Eleven articles were case-series and three were comparative retrospective nonrandomized studies. When compared with open simple prostatectomy (OP), LSP is associated with a less blood loss and a reduced irrigation requirement, a shorter postoperative catheterization period, and a shorter hospital stay, at the expense of an extended operative time. The limited number of patients treated, the selection biases due to the retrospective nature of several published articles on LSP, and the short follow-up periods are evident limits of the literature. I-square test demonstrated a high heterogeneity (93%) and consequently a high variability in the intervention effects in terms of maximum urinary flow rate (Qmax).
Conclusions:
Even if LSP seems feasible and safe, there is still limited evidence regarding its long-term outcomes compared with OP.
Introduction
The laparoscopic approach for the treatment of large prostatic adenoma was first proposed by Mariano in 2002. 8 Since then, several series on laparoscopic simple prostatectomy (LSP), with or without robotic assistance, have been published. These investigations have sought to combine the durable outcomes of OP with the limited invasiveness and the magnified view of the laparoscopic approach.
Aims
To present a critical overview of the current literature on the role of laparoscopy for the surgical treatment of patients with large prostatic adenomas.
Patients and Methods
We performed a MedLine search for peer-reviewed studies, published from 2002–2011, on the surgical treatment of benign prostatic obstruction (BPO) due to benign prostatic hyperplasia (BPH) with pure LSP. The keywords used were “BPH,” “laparoscopy,” “adenomectomy,” “Millin,” “simple prostatectomy,” and “large prostate” (alone or in combination).
Two individuals (A.D.A. and R.M.) independently screened the titles and abstracts of each citation. The reference lists of the eligible articles were reviewed, and the “Related citations” PubMed feature was utilized. Publications in languages other than English were not considered.
The clinical studies that reported most of the following information were included: number of patients, prostate volume, operative time, blood loss, hospital stay, and the duration of catheterization, as well as functional outcomes in terms of Qmax and the International Prostate Symptom Score (IPSS), and complications. Articles reporting a mean total prostate volume of <80 mL or a mean prostatic adenoma of <60 mL were excluded.
LSP studies reporting outcomes for <10 patients were also excluded. Abstracts were not considered for this review nor were articles referring to robotic and laparoendoscopic single-site simple prostatectomy.
Statistical heterogeneity was tested using the I-square test (I2). I-square test describes the rate of variation across studies because of heterogeneity rather than chance and ranges from 0 (no heterogeneity) to 100 (maximum heterogeneity).
Results
Ultimately, 14 articles on LSP 9 –22 were eligible for inclusion in this systematic review. Figure 1 provides a four-phase diagram on the flow of information through the different phases of this systematic review, which followed the PRISMA guidelines. 23
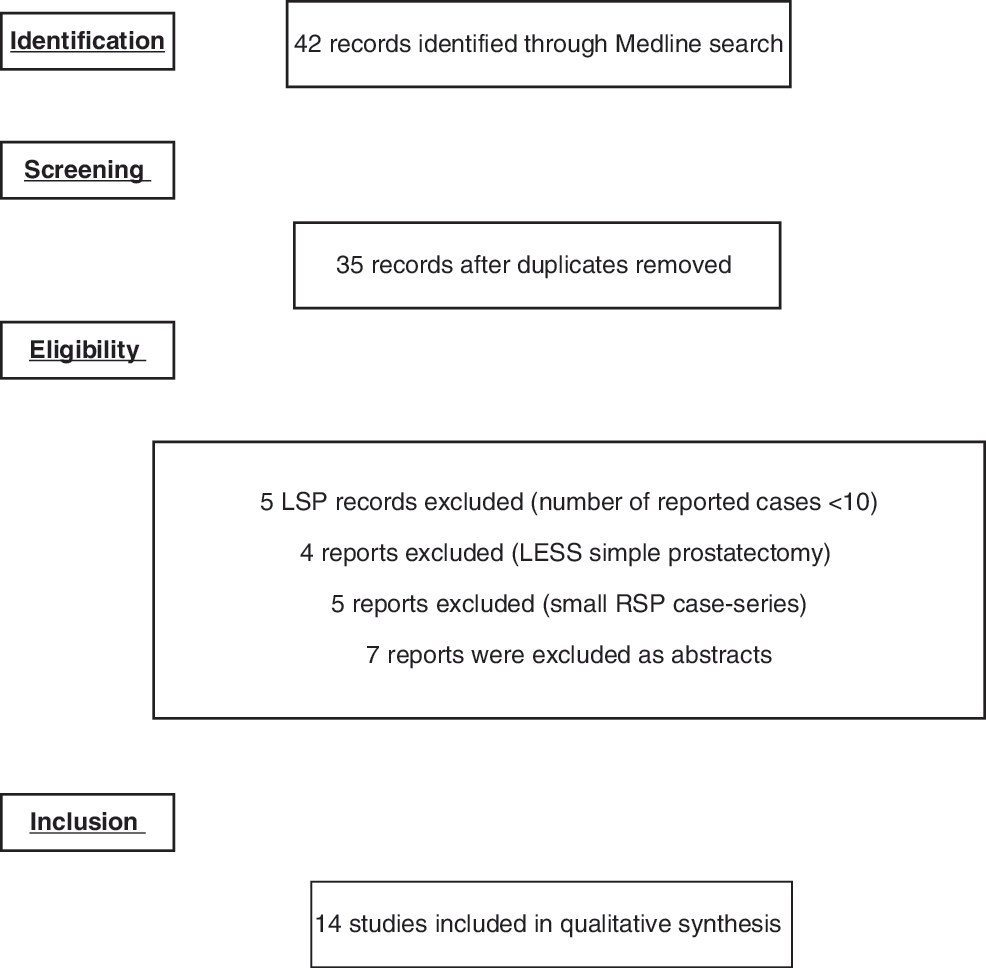
Flow of information through the different phases of this systematic review. LSP=laparoscopic simple prostatectomy; LESS=laparoendoscopic single site; RSP=robotic simple prostatectomy.
Eleven studies were case-series, 9 –14,17 –19,21–22 and three were comparative retrospective nonrandomized studies. 15,16,20 Both transperitoneal and extraperitoneal approaches, as well as transvesical (Freyer) and transcapsular (Millin) routes, with or without finger assistance, have been described. The perioperative data, functional outcomes, and complications of the reviewed LSP studies are shown in Tables 1, 2, and 3, respectively. Table 4 focuses on the outcomes of the three studies comparing LSP and OP, while Figure 2 plots the changes in the mean Qmax values after LSP. The eligible articles included a total of 626 patients who underwent LSP. Twelve articles described the extraperitoneal approach, 9,10,12,14 –22 one described the transperitoneal approach, 11 and one author used both the extra- and transperitoneal approaches. 13 Transverse capsulotomy (Millin) and a pure transvesical (Freyer) approach were performed in nine 10 –12,16,17,19 –22 and two studies, 9,13 respectively; two other articles 14,18 described a mixed transvesical-prostatic approach (longitudinal capsulotomy extending from the anterior aspect of the prostate to the anterior part of the bladder wall), while a single study described both the transcapsular and the transvesical-prostatic approaches. 15 Finger assistance was routinely used by McCullough, 16 Chlosta, 19 and Hoepffner, 21 as well as when separation of the hyperplastic tissue was difficult. Zhou 12 described the use of the finger-assistance technique only in his first case. Enucleation was typically performed with a harmonic scalpel but monopolar scissors, bipolar diathermy, a J-hook, an aspiration cannula, Maryland dissection forceps, a disposable Endo-dissect® (Tyco®) 5 mm, a prostatotome, and claw graspers were also used in various cases. In some cases, two lateral stay sutures between the cut prostatic capsule and the Cooper ligament were used to provide a clear visualization of the fossa and of the cleavage plane. The average weight of enucleated tissue was 106.6 g. The mean operative time was 117.64 minutes, while an average of 314.33 mL of blood loss was observed. The average catheterization time was 5.07 days, and the average hospital stay was 5 days. No deaths or conversions to OP were described. The comparative studies 15,16,20 demonstrated that LSP is associated with less blood loss 15,20 and a reduced irrigation requirement, 15 a shorter postoperative catheterization period, 15,16 and a shorter hospital stay, 15,16 at the expense of an extended operative time. 15,16 Significant differences between LSP and OP were observed in terms of urinary tract infections and urosepsis (with superior results in the LSP group) 16 as well as recatheterization fistula (with superior results in the OP group). 16 No significant differences between IPSS and Qmax were observed between the surgical approaches, even when follow-up was extended >12 months. 20 The only study comparing Millin with transvesical LSP 15 found no significant difference in terms of IPSS or Qmax improvement, operative time, blood loss, irrigation time, catheterization, or hospital stay. Eight studies described a technique for preventive vascular control that involved ligation of the dorsal vein complex and/or of the lateral prostatic pedicles, while six studies did not report the use of any technique for vascular control (Table 5). No significant differences were observed in terms of blood loss between studies that did or did not involve vascular control.
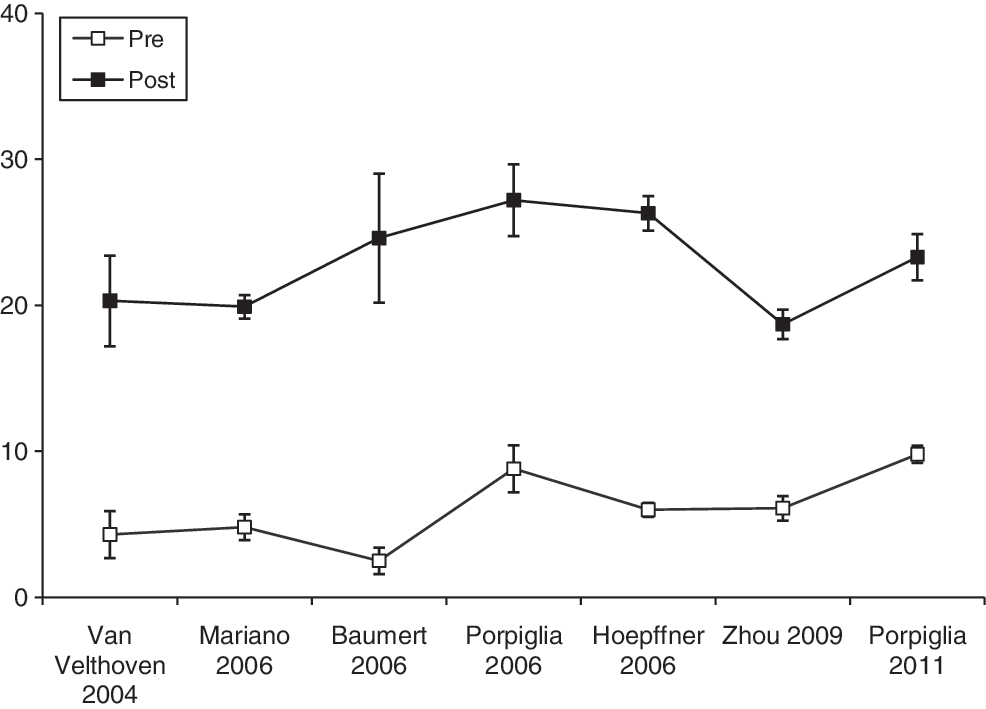
Plot on the change in Qmax after LSP.
LSP=laparoscopic simple prostatectomy; SD=standard deviation.
IPSS=International Prostate Symptom Score; Qmax=maximum urinary flow rate; AUASS=American Urological Association Symptom Score.
SD=standard deviation; OSP=open simple prostatectomy.
Seven studies were excluded from the statistical analysis of heterogeneity; in five of them only the mean (or median) value of Qmax (with range) was reported without any data on standard deviation 9,13,14,17,19 while in two studies no data on Qmax 16,18 were reported at all. Among the evaluated studies, I-square test demonstrated a high heterogeneity (93%) and consequently a high variability in the intervention effects.
Discussion
Surgical treatment of large prostatic adenomas remains a controversial issue.
What does “large prostate” mean? The definition is given indirectly by the maximum tissue volume that can be resected through monopolar TURP while avoiding excessive fluid reabsorption and TUR syndrome. EAU guidelines consider TURP as the current surgical standard procedure for men with prostate sizes <80 mL, BPO, and moderate-to-severe lower urinary tract symptoms (LUTSs). 24 Consequently, we can assume that a large prostate should be defined as a gland >80 mL, even if the upper TURP limit is strongly influenced by the experience/skills of the operator.
The role of monopolar TURP in treating large prostates is limited, mainly due to intraoperative and postoperative morbidities, such as bleeding (with need for transfusion), TUR syndrome, urethral strictures, and a frequent need for reoperation. 25 Further, the morbidity of the procedure increases with operative time. 26 Bipolar TURP offers an attractive alternative to monopolar TURP for the treatment of a large adenoma with similar efficacy but lower morbidity. 5 The risk of TUR syndrome is minimized because bipolar systems use saline irrigation for electrosurgical tissue cutting, which prolongs surgical times. However, considering the lack of high-quality scientific evidence on the role of bipolar TURP for the treatment of large prostates, definitive conclusions cannot be drawn.
Holmium laser appears as the new size-independent gold-standard surgical treatment for large prostates. 3 The long learning curve and the costs are the main factors that have limited widespread diffusion of the technique. 4
Recently, GreenLight® laser technology also showed promising results in treating large prostate adenomas. 6,7 The approach provided good functional outcomes, reduced catheterization and hospital stay, and showed excellent hemostatic properties. However, it does not offer the possibility for definitive histology and it has yet to be judged on a long-term basis to determine whether this promising procedure can withstand the test of time. 25
Simple OP for large prostates is undoubtedly the most common and widely used technique (14%–32% of all invasive procedures performed for BPH in Europe). 25 The EAU guidelines 24 suggest that OP is the most effective and durable procedure for the treatment of BPH-LUTS among men with prostates >80–100 mL who cannot be treated with the Holmium laser. The former technique offers the highest probability of symptomatic improvement and the lowest failure rate. However, OP is also considered the most invasive surgical treatment of BPH and is associated with high morbidity and complication rates. 24
The ideal treatment for large BPH should combine a low degree of invasiveness, reduced complication rates, durable long-term outcomes, quick catheter removal, and a brief hospital stay. In an effort to combine the durable outcomes of OP with the limited invasiveness and the magnified view provided by laparoscopy, LSP and then robotic simple prostatectomy (RSP) were investigated. The surgeon's confidence in his knowledge of prostate anatomy as obtained through previous experience with laparoscopic radical prostatectomy favored the application of laparoscopy to the treatment of large prostatic adenomas.
LSP utilizes the same surgical steps previously described in OP (Millin or Freyer techniques) and a magnified laparoscopic view, which allow for improved hemostasis. A detailed description of the laparoscopic technique has been provided by our group in a previous report. 27
Our review shows that LSP is feasible and safe with acceptable rates of complications, although the scientific literature is still inadequate with respect to definitive conclusions, due to the absence of controlled randomized trials. Even if larger series and long-term follow-up are needed, the functional outcomes of the procedure seem promising and comparable to those obtained with OP. Moreover, the studies comparing LSP and OP demonstrated a global advantage of LSP in terms of blood loss, 15,20 hospital stay, 15,16 and catheterization time. 15,16 However, the majority of studies agree that the procedure is more time consuming. 15,16 Nevertheless, Porpiglia et al 20 showed that the increase in experience leads to a significant reduction in surgical time. The same author stated that the learning curve of LSP is ∼10 cases for an experienced laparoscopist, 20 although no adequately designed studies on learning curve have been conducted. Operative time can also be significantly reduced with the finger-assistance technique for enucleation of the adenoma, as described for the transcapsular approach. For this technique, the finger enters the preperitoneal space through a midline sovrapubic incision or the sovrapubic port; in cases where the surgeon's finger cannot reach the prostate, the index of the contralateral hand can be placed in the rectum to elevate the prostate and assist in enucleation. Considering only the transcapsular procedures, the mean operative time when finger assistance was utilized was 72.1 minutes versus 131.8 minutes with pure laparoscopic enucleation. These results indicate a 1-hour reduction in surgical time. However, body mass index (BMI) may represent a potential limit of this technique. 21 Finally, maneuvers of vascular control, such as ligation of the lateral prostatic pedicles and/or dorsal vein complex, do not seem to significantly influence the mean reported blood loss.
The first description of the feasibility of the RSP was reported by John (in the form of an abstract) for use in the preperitoneal setting 28 ; Sotelo reported his results in the transperitoneal setting. 29 The introduction of the Da-Vinci surgical system in the field of simple prostatectomy seems to allow for improved dexterity, increased visualization, tremor filtration, and an ergonomic setting that enhances the surgeon's comfort. The robotic system also offers the possibility of a complete vesico-urethral anastomosis and facilitates plication of the posterior prostatic capsule. The use of this technique guarantees reduced blood loss, lower blood transfusion rates, and a shorter length of hospital stay, which eliminates the need for postoperative continuous bladder irrigation. 30 Our experience with the same technique in the context of pure LSP (unpublished data) confirms that a complete, running urethrovesicar anastomosis after adenomectomy abolishes the need for postoperative irrigation and minimizes the duration of catheterization. Long-term follow-up is required to evaluate whether this technique is associated with an increased risk of anastomotic strictures.
Till now, only small case-series (with about 40 cases described worldwide) have been published on the efficacy, safety, and functional outcomes of RSP, 29,31 –33 with no comparative study between this technique and either OP or LSP; thus, no definitive conclusions can be drawn on the role of RSP in the surgical treatment of large prostates.
What is the current role of LSP in the surgical treatment of large prostates? Considering the limits of the published literature, it may be hypothesized that selected patients who are not suitable for transurethral procedures (i.e., serious urethral stricture, previous urethroplasty, hip ankylosis, etc.) or suffering from a large bladder diverticulum or large bladder stones may benefit from laparoscopic approaches instead of OP. Moreover, in centers where the Holmium laser is not available, LSP/RSP could be proposed if the surgeons present have laparoscopic or robotic expertise.
Is the trans- or extraperitoneal approach to the prostate preferable? Which one between the transcapsular and the transvesical approach to the adenoma is easier to perform and safer for the patient? No direct comparisons between trans- and extraperitoneal LSP regarding the rates of complications have been reported. For LSP, the transperitoneal approach was only described by Mariano 11 and Sotelo 13 with prolonged ileum reported in three patients; most of the authors preferred the extraperitoneal approach to avoid communication between the peritoneal cavity and urine—that could result in infection, such as in cases of bladder stones, high-postvoiding residual volume, and indwelling bladder catheters. Moreover, a less dramatic Trendelenburg position is necessary to reduce the anesthesiological risks. There is only one study 15 reporting a single surgeon's experience with transcapsular and transvesical LSP. The results did not demonstrate any significant difference in terms of functional outcomes (IPSS and Qmax improvement) or operative time, blood loss, irrigation time, catheterization time, or hospital stay. However, the authors found it more difficult to enucleate the adenoma through the transcapsular incision, mainly in cases with large glands or when a large median prostatic lobe was present. The concomitant removal of bladder stones was also easier with a transvesical-prostatic approach. Because there is a lack of definitive evidence in this field, it can be assumed that the practical habits and preferences of the surgeon are the main factors leading to the selection of a particular technique.
To our knowledge, there are no published studies comparing costs among RSP, LSP, and OP. Cost comparison between procedures is rarely performed due to differences among national healthcare systems, surgical team management strategies, surgical traditions, hospital strategies, as well as reimbursement policies. Laparoscopic operations are generally considered more expensive when compared with the open counterpart. In the case of LSP, this is only partially true because the cost of the laparoscopic armamentarium could be amortized by its multiple uses, mainly in a department dedicated to this type of surgery. Nondisposable instruments compared with disposable instruments can further reduce the cost. Finally, the literature demonstrates a shorter hospital stay for patients treated laparoscopically with respect to OP, 15,16 a fact that guarantees a potentially quicker patient turnover and consequently a further reduction in cost.
Initial case-series on single-port transvesical enucleation of the prostate in patients with large-volume BPH have also been published recently. The procedure—performed with placement of the R-port intraperitoneally 34 or into the bladder, under cystoscopic guidance, with the establishment of pneumovesicum 35 —seems to increase support for the combination of the magnified view obtained by laparoscopy with the promise of improved cosmesis. However, the first case-series demonstrated that this advantage is obtained at the expense of instrument triangulation, clashing, operative time, and comfort of the surgeon.
Considering the high variability in the intervention effects, our findings should be interpreted with caution. The limitations of the studies published include the limited number of patients, selection biases due to the retrospective nature of several published articles on LSP, and the short follow-up periods. Most of the published series on LSP are case series or feasibility studies; consequently, the reported results are influenced by the initial learning curve. A standardized classification of complications such as that proposed by Clavien-Dindo, 36 which incorporates the criteria proposed by Martin 37 and Donat, 38 should be used to adequately collect and report rates of surgical complications of LSP, avoiding the heterogeneity that renders any comparison among different surgical approaches or institutional series problematic.
Conclusions
Even if LSP seems feasible and safe, there is still only limited evidence regarding its long-term outcomes compared with OP. Prospective, randomized, single-surgeon comparisons following the CONSORT statement 39 with associated cost-analysis evaluations among OP, LSP, RSP, and lasers for the surgical treatment of large prostates are required. Considering the trend to transform the surgical management of BPH to an outpatient basis and to abandon transabdominal approaches, it seems difficult, if not impossible, for both LSP and RSP to be widely adopted as standards of care in this field.
Footnotes
Acknowledgments
The first author is scholar of Alexander S. Onassis Public Benefit Foundation.
Disclosure Statement
No competing financial interests exist.