
Abstract
Background and Purpose:
Seminal vesicle cyst (SVC) is a rare disease and its treatment is still controversial. This article contains the largest series of transperitoneal laparoscopic excision of SVC to date, summarizing our surgical techniques and clinical experience with this disease.
Patients and Methods:
From December 2003 to May 2010, seven patients received transperitoneal laparoscopic excision of SVC using a five-port transperitoneal approach. Nearly the total cyst was removed by only leaving a narrow strip of the cyst wall with the bilateral vas deferens and SV preserved completely. Pelvic CT or MRI was performed 3 and 6 months after surgery, and thereafter annually for at least 3 years.
Results:
Transperitoneal laparoscopic excision of SVC was completed successfully in all seven patients without conversion to open surgery. The mean operative time was 73 minutes (range 60–100 min) with negligible blood loss (less than 20 mL). The mean postoperative hospital stay was 4.3 days (range 3–5 days). No intraoperative or postoperative complication occurred. The patients were followed up for a mean of 45 months (range 18–84 mos), during which they all remained symptom free with normal erectile and ejaculatory function without evidence of recurrence.
Conclusion:
Our study has demonstrated that transperitoneal laparoscopic excision of SVC is a safe, feasible, and efficacious procedure, and offers an excellent option for minimally invasive treatment of patients with SVC.
Introduction
The present study is a summary of our surgical techniques and experience with transperitoneal laparoscopic excision of SVC in seven patients. To the best of our knowledge, our report contains the largest series of transperitoneal laparoscopic excision of SVC to date.
Patients and Methods
Patients
Between December 2003 and May 2010, seven male patients with a mean age of 44 years (range 21–58 years) underwent transperitoneal laparoscopic excision for SVC. The preoperative data of these patients are shown in Table 1. All patients were evaluated preoperatively with digital rectal examination, urinary tract ultrasonography, and pelvic CT or MRI, which confirmed the presence of pelvic masses consistent with SVC (Fig. 1). No patient had received urinary tract or pelvic surgery previously. Pelvic CT or MRI was performed 3 and 6 months after surgery, and thereafter annually for at least 3 years.
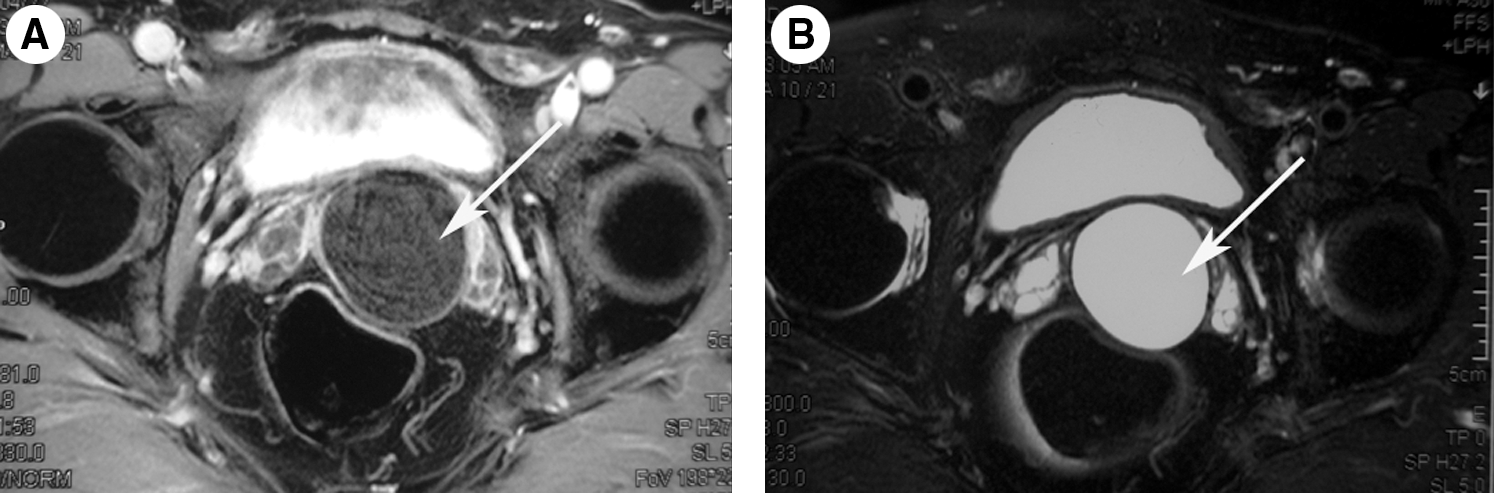
Preoperative contrast-enhanced T1 weighted image
DRE=digital rectal examination; NVB=neurovascular bundle.
Indications for the surgeries of SVC included patients with symptoms such as frequency, urgency, dysuria, hematuria, perineal and suprapubic pain, urinary retention, constipation, etc; the dilated cyst oppressed the ureter and caused hydronephrosis; the cyst is larger than 5 cm regardless of the existence of symptoms or hydronephrosis or renal agenesis.
Laparoscopic techniques
The patients were placed in a Trendelenburg position. Transperitoneal access was achieved through five laparoscopic ports, including a 10-mm port at the umbilicus through which the peritoneal cavity was insufflated with CO2 to 12 to 15 mm Hg. The other four trocars were inserted in the lateral border of the rectus abdominis between the umbilicus and the pubic symphysis in a fan-shaped fashion. The pelvic intestine was pulled up with intestinal forceps to expose the rectovesical pouch.
Two (upper and lower) arcuate bulges were formed by retrovesical peritoneal reflection so that the dilated cyst was easily identified transversely in the upper bulge (Fig. 2A). The bladder was pushed anteriorly, and the vas deferens was identified and dissected medially, which was used as a guide to the SV (Fig. 2B, 2C). The dilated cyst was dissected as far as possible along the direction to its base (junction of the vas deferens or SV neck ampulla or ejaculatory duct or prostate) (Fig. 2D, 2E); Hem-o-lok clips or titanium clips were applied close to the cyst wall (CW) to control the vascular supply; then the cyst was punctured close to the normal SV and drained by aspiration (Fig. 2F and Fig. 3G). To further facilitate dissection from the surrounding structures, the cyst cavity (CC) was opened and the CW was raised (Fig. 3H, 3I). If the cyst volume was giant or near the lateral vascular pedicles of the prostate, a blunt dissection was used to release the neurovascular bundle from the CW. Finally, the dilated cyst was clipped and excised at the level of its base by nearly total cyst removal, only leaving a narrow strip of the CW along its base with the bilateral vas deferens and SV completely retained (Fig. 3J).
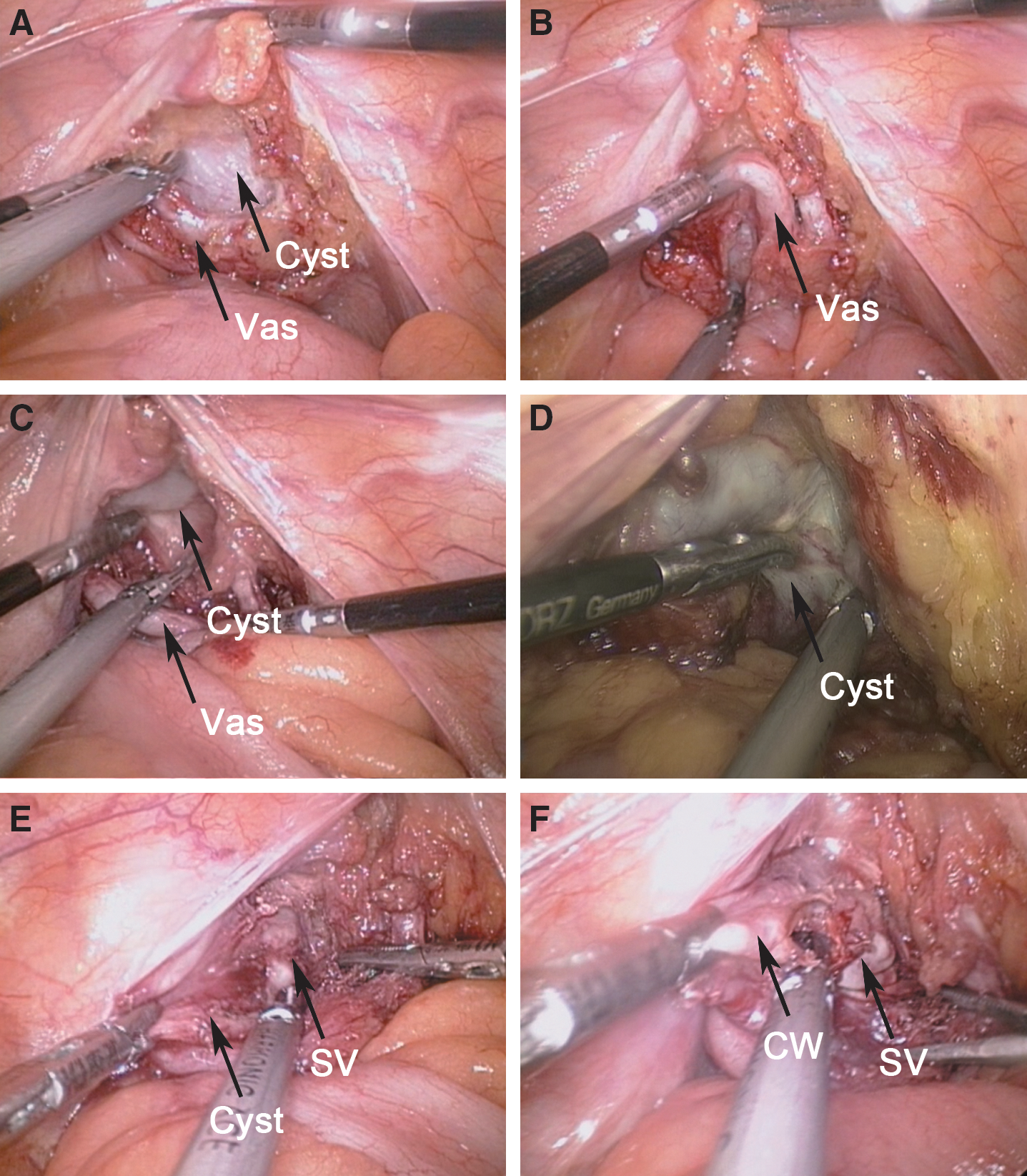
Operative steps in transperitoneal laparoscopic excision of SVC.
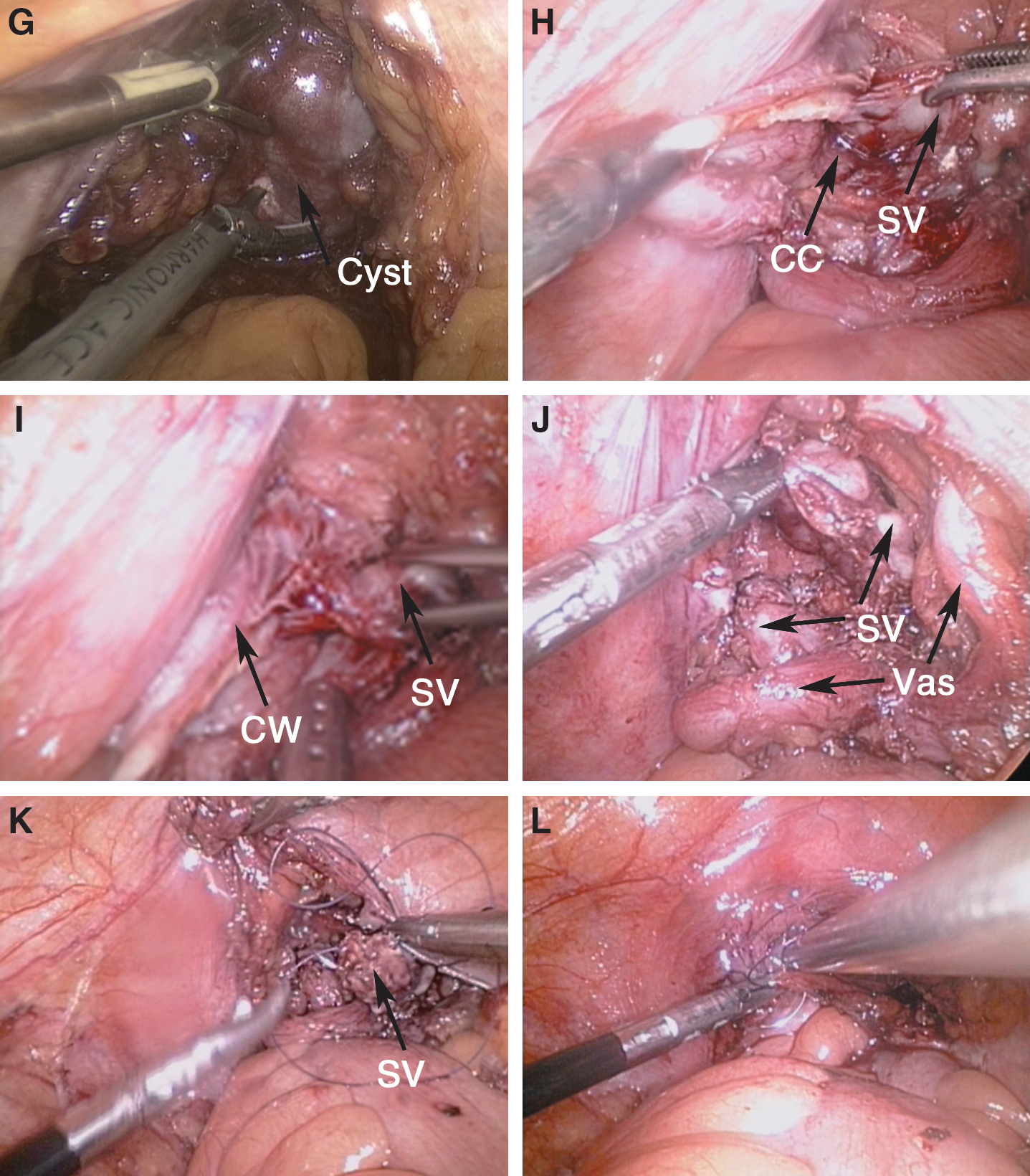
Hemostasis was checked carefully after lowering the pressure of the pneumoperitoneum. The entire SV cystic specimen was removed through the 10-mm port. The peritoneum was reapproximated by using intracorporeal interrupted suturing technique (Fig. 3L).
The nasogastric tube was removed when the patient regained full consciousness after the procedure. Prophylactic antibiotics (second-generation cephalosporin) were administered routinely. The Foley catheter was removed 1 day after surgery. The closed suction drain was subsequently removed if the drainage output remained stable and was less than 20 mL within 24 hours.
Results
All procedures were completed laparoscopically without conversion to open surgery. In one case (No. 3), the normal SV was broken because of failure to distinguish the boundary of the normal SV and the dilated cyst, and it was repaired using laparoscopic intracorporeal continuous suture technique with 3/0 polyglycolic acid absorbable suture (Fig. 3K). The mean operative time was 73 minutes (range 60–100 min) with negligible blood loss (less than 20 mL), and no blood transfusion was needed in any patient. No intraoperative and postoperative complications occurred. Intraoperative and postoperative data of the patients are indicated in Table 2.
EBL=estimated blood loss.
All patients achieved uneventful postoperative recovery, and no significant postoperative complication occurred. No patient needed painkillers for postoperative pain control in the recovery room and ward. The Foley catheter was removed 1 day after surgery. The closed suction drain placed in the rectovesical pouch was removed 3.1 (range 2–4) days after surgery. The mean postoperative hospital stay was 4.3 days (range 3–5 days). Pelvic CT or MRI was performed at 3 and 6 months after surgery, and annually thereafter for at least 3 years. During the18 to 84 month follow-up period (mean 45 mos), all patients remained symptom free with normal erectile and ejaculatory function without evidence of recurrence.
Discussion
The male reproductive and urinary systems are embryologically derived from the mesonephric duct. Anomalies of the reproductive systems are commonly associated with abnormalities of other structures derived from the mesonephric duct, such as the vas deferens, kidney, and ureter. 4 About two-thirds of congenital SVCs are associated with ipsilateral renal agenesis, and most SVCs were found and diagnosed in the third to fifth decades of life. 5,6
Abdominopelvic and transrectal ultrasonography is the initial and conventional diagnostic tool for long-standing pelvic pain and suspicious physical findings. 7 CT and MRI can both accurately show renal and SV anomalies. Additional studies include intravenous urography, cystoscopic evaluation, and seminovesiculography. 7,8 Dilated SVs could be diagnosed as other forms of cysts or fluid-filled structures originating from surrounding organs. These include prostate gland cysts, prostatic utricle cysts, ejaculatory duct cysts, müllerian duct cysts, bladder diverticula, and ureteroceles, among others. 9 We consider that MRI is a better tool for accurately defining anatomic relationships when surgeons plan to excise SVC laparoscopically. In addition, we think that physical examinations, especially digital rectal examination, are important for detecting dilated SVC and understanding the condition of the prostate and rectum as well.
Patients with SVC are usually asymptomatic, although some patients may present with inconsistent symptoms arising from an endopelvic mass that occupies space of the surrounding structures. The endopelvic cystic mass may cause obstruction of the spermatic tract and irritation or obstruction of the urinary bladder, leading to various clinical manifestations including frequency, urgency, dysuria, hematuria, perineal and suprapubic pain, urinary retention, and constipation. 7,10,11 The most frequent symptoms, however, are epididymitis and postcoital pain. 12 In our seven patients, five had symptoms before surgery, including hematospermia in two patients, perineal pain in two patients, and lumbosacral soreness and tenesmus in one patient.
Surgical treatment is usually needed for large and symptomatic SVC, including open surgery, laparoscopic cyst excision, and endoscopic cyst resection or unroofing or aspiration. Although an open operation offers excellent outcomes, it is likely to be associated with a high rate of morbidities, including rectal and bladder wall laceration, erectile neurovascular bundles, ureteral injury, and pelvic urinoma. 4 Transurethral resection or unroofing or aspiration of SVC usually provides temporary relief, and high rates of infection and recurrence have been reported. 8 The success rate of endoscopic technique is reported to be about 75%. 13 We consider that transurethral resection and aspiration may be used as an initial management for small and caudally situated SVC. When an SVC is large and protrudes into the bladder, the larger cyst tends to be relatively cephalic; it may be more difficult for the surgeon to access and drain adequately using an endoscopic technique.
Although SVC is usually located deep in the pelvic cavity, the transperitoneal laparoscopic approach can still provide straightforward access and excellent visualization. Recently, some medical centers have issued several case reports of successful laparoscopic excision of SVC. 4,6,8,14 –18 To the best of our knowledge, our report contains the largest series of transperitoneal laparoscopic excision for SVC to date because of the huge population in China. In our seven cases, the dilated cysts were clipped and excised at the level of their bases with nearly total removal, only leaving a narrow strip of the CW along the base. In addition, the vas deferens and SV were completely retained, which otherwise might lead to infertility.
Transperitoneal laparoscopic excision of SVC is a technically challenging surgical procedure, with a proficiency requirement for dissection in the relatively confined pelvic cavity to completely retain the surrounding tissues, such as the vas deferens and SV. Besides, when the dilated cyst is near the lateral vascular pedicles of the prostate or compresses the ipsilateral ureter, special attention should be paid to the delicate blunt dissection technique to avoid complications. In our seven patients, the large dilated cysts were close to the surrounding structures, such as the ureter in two patients causing hydronephrosis; the lateral vascular pedicles of the prostate in two patients; the rectum; the vas deferens; the SV neck ampulla; the ejaculatory duct, and the prostate. All these organs and tissues remained intact after surgery.
More recently, several cases of robot-assisted laparoscopic excision of symptomatic retrovesical cysts have been reported. 10,19,20 With its inherent advantages, robot-assisted surgery increases dexterity and improves intracorporeal dissection. Robot-assisted surgery is comparatively expensive, however. There have only been three case reports describing pure robotic surgery for SVC, and more studies are warranted to assess the true utility of robotic surgery for this condition. During the last 3 years, a novel surgical style well coined as laparoendoscopic single-site surgery has been developed—which gives the surgical patients in the 21st century a novel surgical mentality of “minimally invasive, maximally effective and cosmetic” and has been applied also for the laparoscopic excision of SVC. 21
We consider that the dilated cyst and vas deferens are easily identified by a transverse approach in the upper bulge of retrovesical peritoneal reflection, where the vas deferens can be used as a guide to the SV. We also think that the cyst should be dissected along the base as completely as possible to understand the anatomic relationship nearby before it is punctured and drained by aspiration. To distinguish the boundaries of the dilated cyst and normal SV carefully, we recommend two key surgical procedures. First, the dilated cyst should be punctured near its base. Second, the CC should be opened. A larger SVC was more difficult compared with a smaller one, because it is usually adhered closely with the lateral vascular pedicles of the prostate or vas deferens or SV neck ampulla or ejaculatory duct. If the cyst is close to the lateral vascular pedicles of the prostate, we recommend using “cold” transaction or blunt dissection from the cyst base with minimal traction on the nearby neurovascular bundles for the sake of preserving normal erectile and ejaculatory function after surgery. In addition, special attention should be paid to the protection of the blood supply around the ureter during dissection between the cyst and the compressed ureter.
The dissection of the SVs in a similar technique has been described during transperitoneal laparoscopic radical prostatectomy with Montsouris technique in a large series. 22 Short-term postoperative follow-up outcomes in terms of spontaneous erections were reported in 85% of patients who underwent anatomic preservation of the two neurovascular bundles and no adjuvant treatment, among whom 66% of patients have experienced intercourse. 23
Our five-port transperitoneal approach can significantly shorten the operative time (mean 73 min; range 60–100 min) compared with previous reports, 6,15,17,18 because the first surgical assistant could easily help the surgeon with exposure during the operation. Besides, the five-port approach does not seem to affect the aesthetics compared with the total four-port transperitoneal approach reported in related literature. 4,6,8,14,16 The transperitoneal laparoscopic approach provides excellent visualization, and Hem-o-lok clips or titanium clips can be easily applied near the CW to control the blood supply. In our cases, the mean estimated blood loss was less than 20 mL, and no patient needed blood transfusion. No intraoperative or postoperative complications occurred.
Because SVC is a rare anomaly, studies related to laparoscopic techniques are limited, especially those concerning comparisons between laparoscopic surgery and open or endoscopic surgery. As this largest series demonstrated, however, with improvements in laparoscopic technology, transperitoneal laparoscopic excision of SVC can be completed safely and quickly with satisfactory results. In our surgical team, transperitoneal laparoscopic excision has been used as the treatment of choice for SVC.
Conclusions
Our study has demonstrated that transperitoneal laparoscopic excision of SVC is a safe, feasible, and efficacious procedure, and offers an excellent option for minimally invasive treatment of patients with SVC. All patients in our series remained symptom free with normal erectile and ejaculatory function, and no evidence of recurrence has been observed. Transperitoneal laparoscopic surgery may prove to be the treatment of choice for patients with SVC.
Footnotes
Disclosure Statement
No competing financial interests exist.