
Abstract
Purpose:
We describe surgical techniques and experience with retroperitoneal laparoscopic pyeloureterostomy in five cases of retrocaval ureter (RU). We also report the laparoscopic approach reconstruction for RU from peer-reviewed publications.
Patients and Methods:
Five patients with RU underwent retroperitoneal laparoscopic pyeloureterostomy. Nuclear renography, intravenous urography (IVU), and ultrasonography follow-up was performed postoperatively. Science Citation Index searches were conducted to identify laparoscopic reconstruction for RU outcomes. Studies published after 1994 were included in the analysis.
Results:
Operations were completed successfully and without complications in five patients. The mean operative time was 90.2±34.4 minutes. The mean time needed to insert the Double-J stent and reanastomosis was 51.2±11.4 minutes. Blood loss was minimal. Over a follow-up of 12 to 37 months, hydronephrosis was found to decrease substantially. There were 24 peer-reviewed studies covering a total of 62 patients suitable for inclusion in our final analysis. The most common method for reconstruction of the ureter was ureteroureterostomy, followed by pyeloureterostomy and pyelopyelotomy.
Conclusion:
Retroperitoneal laparoscopy for RU is a safe and effective procedure that should be considered as a first-line treatment for patients with this anatomic anomaly.
Introduction
In 1994, Baba and colleagues 3 first treated RU with transperitoneal laparoscopic pyeloureterostomy. In 1999, Salomon and associates 4 performed the first retroperitoneal laparoscopic ureteroureterostomy for RU. Since then, minimally invasive approaches have been found to produce results equivalent to those of open surgery, with shorter convalescence and lower amounts of analgesic agents. 5,6 The performance of laparoscopic operations in the setting of a RU added challenges of extensive dissection both lateral and medial to the vena cava.
Between 2003 and 2010, we performed retroperitoneal laparoscopic reconstruction for five patients with RU. We present our surgical techniques and experience and review the reported cases of laparoscopic correction of RU in the English-language literature included in the Science Citation Index journal from 1994 to 2011.
Patients and Methods
The medical records of five patients (four male and one female), with a mean age of 29.4±12.6 years (range 16–47 years), with RU received laparoscopic operations between 2003 and 2010 in the department of urology at the Affiliated Zhongda Hospital of Southeast University. These cases are reviewed in the present study. All patients complained of recurrent mild to moderate right flank pain or hematuria, and diagnoses were made based on retrograde pyelography (RP) (Fig. 1A) or/and CT urography (CTU) (Fig. 1B) preoperatively. These demonstrated a typical S-shaped deformity of the right ureter and moderate hydronephrosis and a dilated proximal ureter in all patients. The type of RU was determined according to the classification system described by Bateson and Atkinson. 7

General anesthesia was administered to all patients. The patients were placed in the left lateral decubitus position with overextension. A standard four-port retroperitoneal approach was used. First a 2.0-cm incision was made below the right 12th rib in the posterior axillary line (point A), the muscular layer, and lumbodorsal fascia were bluntly divided by vascular forceps, and an index finger was inserted to separate the retroperitoneal space bluntly. A domestic balloon dissector was placed into the retroperitoneal space. About 600 to 700 mL of air was infused to maintain the balloon dilatation for 2 minutes. The air was then evacuated and the balloon dissector removed.
A 1.0-cm skin incision was made above the superior border of the right iliac crest in the midaxillary line (point B) for the laparoscope; under the guidance of the index finger extending into the retroperitoneal space through point A, a puncture cannula (10 mm) was inserted in point B. A 0.5-cm skin incision was made below the right costal margin in the anterior axillary line (point C). Another 0.5-cm skin incision was made in the posterior and above of point B (point D). Then 5-mm puncture cannulas were inserted at points C and D, respectively. Finally, a 12-mm puncture cannula was inserted at point A, and then the skin incision of point A around the puncture cannula was sutured. The cannula at point A was connected to the carbon dioxide insufflator to achieve the pneumoretroperitoneum (pressure 14 mm Hg).
The Gerota fascia was incised longitudinally after the retroperitoneal fat was freed (Fig. 2A). The perirenal fat was dissected to reveal the posterior surface of the mid and lower poles of the right kidney. The dilated renal pelvis, upper ureter, and vena cava were identified and fully isolated. The ureter in the interaortocaval region was dissected to facilitate tension-free pyeloureterostomy anastomosis. The retrocaval segment of the ureter was eventually completely released (Fig. 2B). The ureter was spatulated laterally at the ureteropelvic junction (Fig. 2C). The retrocaval segment of the ureter was mobilized and transposed anterior to the vena cava.
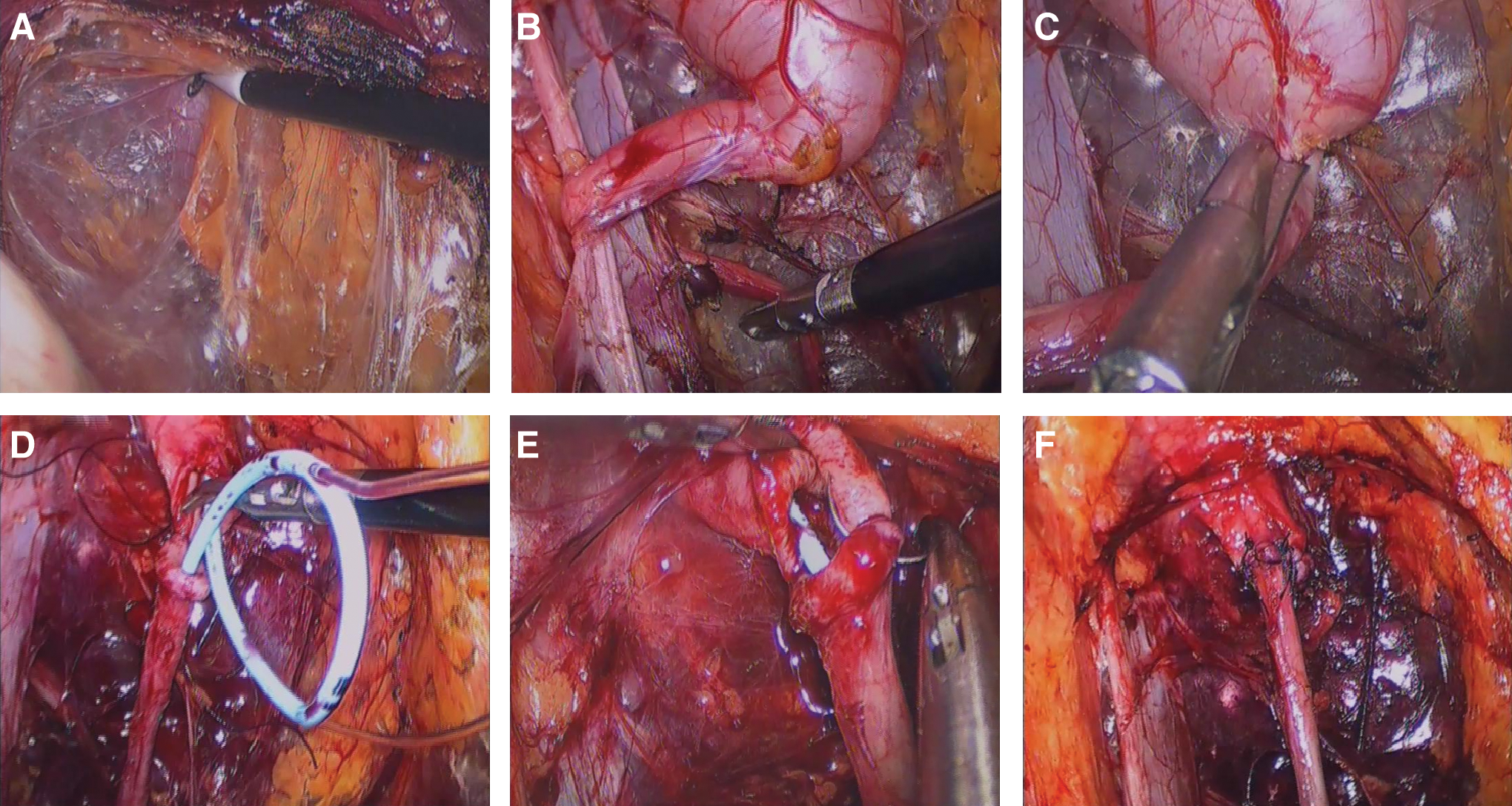
Operative steps of retroperitoneal laparoscopic pyelouretrostomy.
The retrocaval segment of the ureter was reserved in four patients because they had a grossly normal appearance without obvious stenosis. One patient was excised for an obvious stenosis in the retrocaval segment ureter. Two segments of semirigid silica gel catheter of appropriate length were used as indwelling guides. They were passed into a 7F 28-cm Double-J stent from the side holes of the stent. After the first posterior layer suture, the Double-J stent was pushed into the ureter, with its distal curl in the bladder and the proximal curl in the pelvis; then the silica gel catheter was removed (Fig. 2D).
The pyelo-ureter reanastomosis was formed with interrupted sutures in a tension-free fashion, using 4-0 polyglactin sutures (Fig. 2E), and the anastomosis was completed (Fig. 2F). Hemostasis was checked carefully. A closed 14F silica gel drain was placed through point C. Carbon dioxide was evacuated, and the port sites were closed. Nuclear renography and intravenous urography (IVU) were performed at 3 and 6 months postoperatively. Then ultrasonography was performed as a routine follow-up method at 6-month intervals.
We used Science Citation Index to search all publications in English with the keywords “retrocaval ureter” or “circumcaval ureter” and “laparoscopic.” We mainly concentrated on the type of operation, approach, manner of reconstruction and suture, the excision or preservation of the retrocaval segment ureter, operative time, blood loss, and complications.
Results
All operations were successful without conversion to open surgery. The mean operative time was 90.2±34.4 minutes (range 81–126 min). The mean time needed for insertion of the Double-J stent and reanastomosis was 51.2±11.4 minutes. The mean blood loss was 38.3±9.4 mL (range 21–50 mL). No intraoperative or postoperative complications were observed. Recovery was uneventful. The return of bowel function and discharge commenced on postoperative days 1.6 and 6.5, respectively. The Foley catheter and drain were removed after 5 days; the Double-J stents were removed 8 weeks postoperatively. At the follow-up visits, the nuclear renography and IVU that were performed at 3 and 6 months postoperatively revealed no evidence of obstruction (Figs. 3A and 3B). The patients remained symptom-free. Renal ultrasonography demonstrated substantial decrease in hydronephrosis.
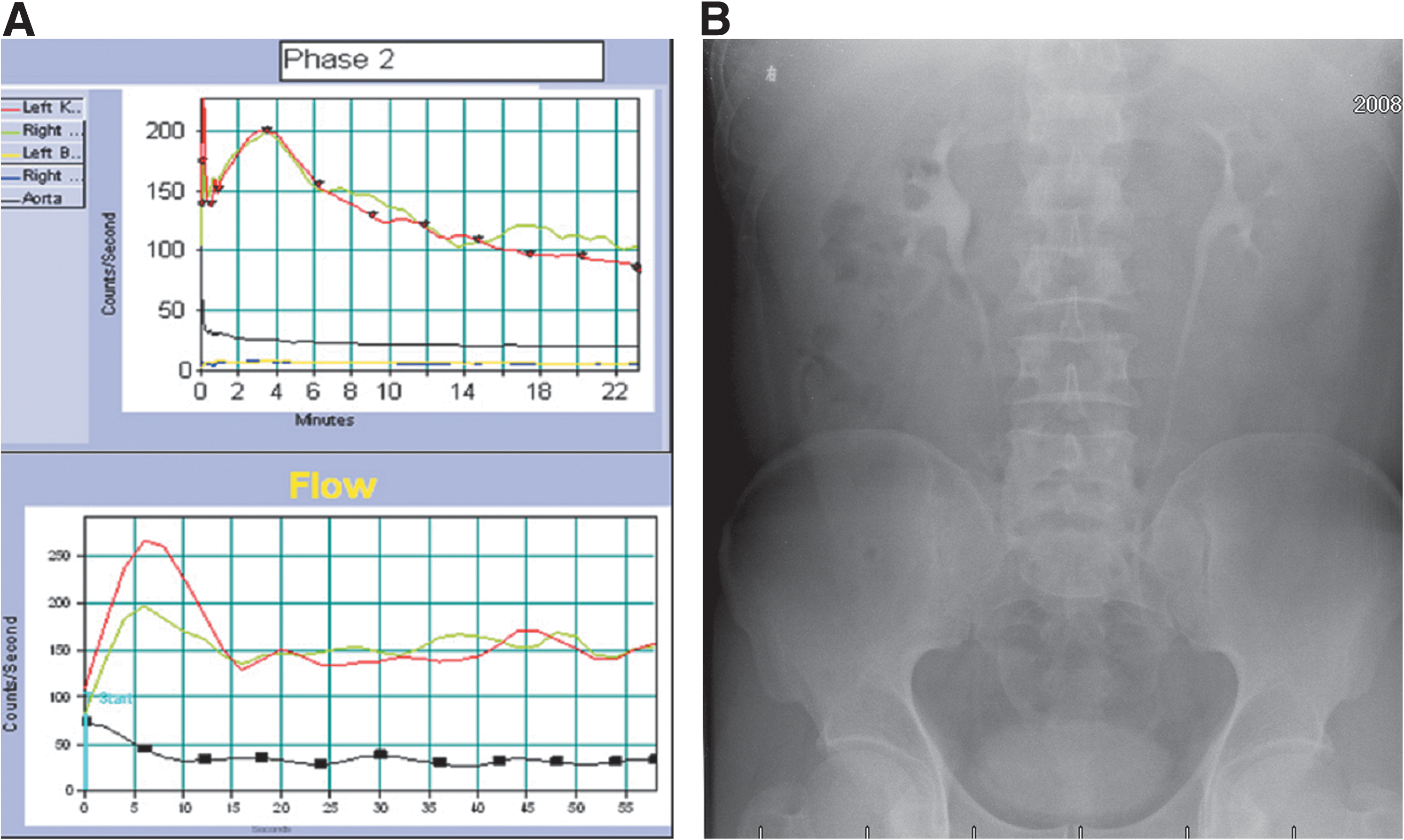
Three-month follow-up:
We found 24 articles covering 62 patients who had undergone laparoscopic reconstruction of the RU. The age at surgery ranged from 4 to 56 years; there were 44 men and 18 women (male:female ratio=2.4:1), including 3 children. The first laparoscopic reconstruction for RU was performed in 1994 by Baba and coworkers. 3 Seven articles (7/24, 29.2%) described the retroperitoneal approach in 33 patients (33/62, 53.2%). 4,8 –13 Seventeen articles (17/24, 70.8%) described a transperitoneal approach, which was used in 29 patients (29/62, 46.8%). 3,14 –29 This included 2 cases of robot-assisted laparoscopy, 1 case of single-port laparoscopy, and 59 cases of pure laparoscopy. 14,25,26 The mean operative time was 170.1 minutes (range, 42–560 min), not including one case in which the operative time was not reported. The mean operative time of pure laparoscopy was 169.3 minutes, while those of the retroperitoneal and transperitoneal approaches were 120.4 and 228.6 minutes, respectively. Blood loss was minimal (less than 50 mL) in all patients. No intraoperative complication occurred, and no procedures were converted to open surgery (Table 1).
Not reported in the literature.
RAL=robot-assisted laparoscopic; SPL=single-port laparoscopic; PL=pure laparoscopic; RP=retroperitoneal laparoscopic; TP=transperitoneal laparoscopic.
Laparoscopic ureteroureterostomy was described in 17 articles covering 47 patients (17/24, 70.8%; 47/62, 75.8%). 4,8 –14,18 –24,26,28 Pyeloureterostomy was described in four articles covering four patients (4/24, 13.7%; 4/62, 6.5%). 3,15,16,27 Pyelopyelostomy was described in three articles covering 11 patients (3/24, 12.5%; 11/62, 17.7%). 17,25,29 The procedure was used to reconstruct the ureter. The retrocaval segment of the ureter was preserved in 16 articles covering 41 patients (16/24, 66.7%; 41/62, 66.1%). 4,8,9,11 –14,16 –19,24 –27,29 It was excised in 11 articles covering 24 patients (11/24, 45.8%; 24/62, 38.7%). 3,9 –11,15,18,20 –23,28 The anastomosis was performed with running sutures in eight articles covering 25 patients (8/24, 33.3%; 25/62, 40.3%). 9,12 –17,29 It was performed with interrupted sutures in 14 articles covering 35 patients (14/24, 58.3%; 35/62, 56.5%). 3,4, 8,10,11,18 –20,22 –27 Another two patients were not reported (Table 2). 20,28
In three literature reports, the surgeons excised the stenotic retrocaval segment of ureter and preserved the ureter if there was no stenosis.
U-U=ureteroureterostomy; P-U=pyeloureterostomy; P-P=pyelopyelostomy.
Discussion
RU is a rare anatomic anomaly. It occurs predominantly on the right side of the body and usually becomes symptomatic in the third or fourth decade of life. 1 Bateson and Atkinson 7 described two types of RU. 7 Type 1, the more common form, is a characteristic S or fishhook deformity of the ureter (Fig. 1A). It is usually associated with moderate to severe hydronephrosis. Type 2, the rarer form, is a sickle-shaped ureteral curve. It is usually associated with mild hydronephrosis. In patients with minimal calicectasis and no symptoms, surgical correction is not mandatory, but observation should be maintained. Surgical treatment is usually needed when the patient is symptomatic or an obstruction develops. 30 The performance of dismembered pyeloplasty is the accepted treatment modality. The treatment of this clinical situation is well suited to minimally invasive approaches.
IVU and RP were commonly used to diagnose RU. MRI has been suggested as a method of choice because it does not involve radiation. 30 Recently, however, CTU has become more common. 17,26 In our opinion, CTU should be a first-choice diagnostic approach because it accurately determines the anatomic relationship between the vena cava and ureter and because it is noninvasive.
Open surgery remained the gold standard approach to treat patients with RU for many years. Over the past 10 years, however, minimally invasive laparoscopic procedures have almost entirely replaced open surgery. 30,31 Pure laparoscopy has become the predominantly means of managing RU, as indicated by most articles (Table 1). Robotic technology has been incorporated into certain areas of urology, as in robotic prostatectomy, and has become well accepted. The main advantage of robotic technology is the ease of dissection and intracorporeal suturing. Expert laparoscopic surgeons, however, do not require robots for these procedures.
Anastomosis and insertion of Double-J stents can be performed by laparoscopy alone without increasing blood loss or the rate of intraoperative complication. 9,10 The downside of the robotic approach is the cost. Single-port laparoscopy has been used for nephrectomy, prostatectomy, and so on. The cosmetic advantage is also an appealing aspect of single-port laparoscopy, especially for younger patients. Further refinement in instrumentation is needed, however, before the technique may achieve any level of standardization. 14 It has no advantage over conventional laparoscopy with respect to operative time. We recommend that pure laparoscopy rather than robot-assisted or single-port laparoscopy should be the method of choice for reconstruction of RU.
For laparoscopic reconstruction of RU, the transperitoneal approach was the method of choice in most published articles (17/24, 70.8%), and the retroperitoneal approach was used less frequently (7/24, 29.2%) (Table 1). Studies have shown both different results and conclusions regarding transperitoneal and retroperitoneal approaches to RU. 19,4,8,12 Bagheri and associates 18 reported in a literature review that 27 patients underwent laparoscopic surgery and found no significant differences between the two approaches. 18 The choice of either transperitoneal or retroperitoneal approach was found to depend on the preferences of the surgeon performing the procedure.
We evaluated five cases of retroperitoneal laparoscopic surgery for RU. They had a mean operative time of 90.2 minutes, showed no intraoperative complications, and involved minimal blood loss. We selected the retroperitoneal approach because of our extensive experience with many retroperitoneal laparoscopic procedures. In our literature review, the operative time of the retroperitoneal laparoscopic procedure was found to be less than that of transperitoneal procedures (120.4 vs 228.6 min) but did not involve increased bleeding or complications. In our opinion, which is shared by Gupta and colleagues 8 and Mugiya and coworkers, 12 this is an effective and safe technique when performed by an experienced surgeon.
Retroperitoneal laparoscopy for RU is convenient and reduces operative time. It provides direct access to the ureter and vena cava while avoiding spillage into the peritoneal cavity. It also prevents the need for dissection of the retrocaval segment ureter, because dissection of the retroperitoneal space was not hindered by intra-abdominal organs.
Laparoscopic anastomosis is a technically challenging and lengthy surgical procedure. Great proficiency isneeded for intracorporeal suturing and knotting. In the published literature, summarized in Table 2, ureteroureterostomy was the most frequent choice (17/24 literature, 70.8%). Pyeloureterostomy and pyelopyelostomy were less frequently reported. The advantage of pyeloureterostomy and pyelopyelostomy was that the abundant vascular supplies of the pelvis and proximal ureter could be preserved, rendering postoperative stenosis at the anastomotic site less likely. 30
In our series, a transection was made at the level of the ureteropelvic junction. Then pyeloureterostomy with interrupted tying was performed. There was no stenosis at the anastomosis site, and no aggravation of hydronephrosis was observed. A severely dilated pelvis necessitates a reasonable transection at the level of the pelvis just above the ureteropelvic junction for pyelopyelostomy or at the level of the ureteropelvic junction for pyeloureterostomy. Pyelopyelostomy is indicated when RU is complicated by pelvic stones. Pyelolithotomy was performed before the anastomosis. The RU and pelvic stones were addressed during the same procedure. 15,17
In our opinion, the selection of the manner of reanastomosis depended on the level of ureteral transection. An approximately 1 cm spatulation of the distal or proximal ureteral end is recommended during a ureteroureterostomy or pyeloureterostomy. Pyeloureterostomy and pyelopyelostomy were both found to prevent stenosis at the site of anastomosis.
The decision of whether to excise or preserve the retrocaval segment ureter has been controversial. In the published literature, most surgeons were more likely to preserve the ureter (41/62, 66.1%), especially in patients receiving pyeloureterostomy and pyelopyelostomy (13/15, 86.7%). Excision of the retrocaval segment ureter was performed mainly in ureteroureterostomy (19/47, 40.4%). Zhang and coworkers 32 underlined that when an 8F catheter could not pass through the retrocaval segment easily, the stenotic section of the ureter must be excised. 32
We believe that the radiologic findings and intraoperative appearance of the ureter should be used to help determine whether to excise the retrocaval segment. The excision of the retrocaval segment ureter is an efficient means of avoiding stenosis at the anastomosis site, especially in patients undergoing ureteroureterostomy. If there is no stenosis in the retrocaval segment of the ureter, it can be preserved in patients undergoing pyeloureterostomy and pyelopyelostomy. In our series, the retrocaval segment was excised in one case because of obvious strictures at the retrocaval segment and preserved in another four cases. The deciding factors behind the excision or preservation of the retrocaval segment ureter were the manner of reanastomosis and the presence or absence of stenosis.
Most surgeons complete all reanastomosis using interrupted sutures (14/24, 58.3%). Fewer surgeons use running sutures (8/24, 33.3%). The manner of suturing is related to the manner of reanastomosis. Surgeons are more likely to use interrupted suturing with patients undergoing ureteroureterostomy (32/47, 68.1%) to avoid stenosis at the site of anastomosis. In patients undergoing pyeloureterostomy and pyelopyelostomy, however, the manner of running sutures is preferred by surgeons because it can reduce operative time without increasing the risk of stenosis. In our series, reanastomosis has been performed with interrupted sutures without lengthening the operative time. The decisive factor regarding the manner of suturing was found to be the manner of reanastomosis.
The placement of the Double-J stent was another challenge to laparoscopic surgery for RU. Some surgeons placed Double-J stents in a retrograde manner preoperatively using cystoscopy. 4,8,19 Previous ureteral stent or guidewire placement would hinder transection and anastomosis of the ureter. We inserted two semirigid indwelling guides into the Double-J stent from the side holes at reasonable sites, then placed the Double-J stent from the reanastomotic site into the bladder antegrade and into the pelvis retrograde intraoperatively (Fig. 2D). This technique can avoid complications of the retrograde procedure and cystoscopy and reduce operative time. We recommend this technique, which we found to be fast, safe, and easy to perform.
Conclusions
Retroperitoneal laparoscopic reconstruction of RU is safe, feasible, and effective. With the advantages of direct access to the ureter and vena cava, the dissection of the retrocaval segment ureter and reanastomosis was not hindered by intra-abdominal organs. Considering a review of published reports and our own experience, we have concluded that retroperitoneal laparoscopic access performed by experienced surgeons in well-equipped centers should be considered first-line treatment for patients with RU. The selection of reanastomosis and suture manner depends on the surgeons' experience and the pathology of the retrocaval segment ureters. Laparoscopic pyeloureterostomy using interrupted sutures without resection of the retrocaval segment and with intraoperative placement of a Double-J stent is a technically viable and reliable alternative.
Because the number of cases is small, further study of the safety and efficiency of the retroperitoneal laparoscopic pyeloureterostomy in an interrupted suture manner is also necessary.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (NO. 81070592), Natural Science Foundation of Jiangsu Province (BK2009275).
Disclosure Statement
No competing financial interests exist.