
Abstract
Background and Purpose:
Automatic brightness control (ABC), a function of modern fluoroscopy machines, adjusts radiation intensity in real time to enhance image quality. While shielding reduces radiation exposure to protected areas, it is unknown how much radiation adjacent unshielded areas receive when using ABC settings. Our purpose was to assess radiation dosage to shielded and unshielded tissue when using fluoroscopic ABC mode compared with fixed exposure settings.
Materials and Methods:
In a simulated ureteroscopy, thermoluminescent dosimeters (TLDs) were placed at three sites in a female human cadaver, including the right renal hilum, right distal ureter adjacent to the uterus, and directly over the uterus. The cadaver received 60 seconds of radiation exposure using a C-arm fluoroscopy system under ABC and fixed settings (1.38 mAs, 66 kVp) with and without uterine shielding. Radiation dosage absorbed by the TLDs was compared using two-way analysis of variance and least-squares confidence intervals.
Results:
Shielding significantly reduced radiation dose to the uterus by 62% and 82% (P<0.05 for both) in ABC and fixed settings, respectively. Shielding of the uterus in ABC, however, resulted in an approximately twofold increase in radiation dosage to the ureter and ipsilateral kidney (P<0.05 for both) and a decrease in image quality. Using fixed settings, shielding of the uterus did not increase radiation dose to the ipsilateral ureter and kidney.
Conclusion:
There is a significant increase in radiation dosage to surrounding tissues when shielding is used with ABC mode during fluoroscopy. Radiation can be reduced and image quality improved by using fixed settings when shielding is indicated.
Introduction
One way to reduce fluoroscopy time is to ensure that all images are taken at the optimal settings to obtain a high-quality fluoroscopic image.
Modern fluoroscopy machines allow for operation in either a manual fixed or automatically adjusted exposure settings. 6 Automatic brightness control (ABC), automatically adjusts radiation intensity (milliamperes/second [mAs] and kilovoltage peak [kVp]) in response to tissue density to achieve optimal image quality. 1 Used in fluoroscopy, ABC mode allows X-ray machines to automatically and instantaneously adjust settings to provide better picture quality and enhance procedural efficiency. ABC mode may also decrease overall radiation exposure by reducing the number of unnecessary poor quality images. 6, 7
While useful in some settings, the effects of ABC in conjunction with shielding have not been fully characterized. In ABC mode, the fluoroscopy machine could automatically increase the mAs and kVp in an attempt to penetrate the dense shield. This increased radiation intensity may subsequently expose surrounding tissue to an increased level of radiation because of a false overestimation of tissue density.
The purpose of this study is to determine the effect of shielding during ABC and fixed settings in both shielded and surrounding unshielded tissues during simulated ureteroscopy.
Materials and Methods
After approval of the protocol by the department of anatomic pathology, and in accordance with the institutional policies for use of anatomic specimens, a single female cadaver (body mass index [BMI] 22) was used for the study. The cadaver was exposed to fluoroscopic imaging with and without uterine shielding during a simulated right ureteroscopy.
The procedure was performed in the operating room, and fluoroscopic imaging was taken using a GE OEC 9900 portable C-arm system in a manner identical to that used for clinical patients. The exposure modalities tested in this study included: (1) ABC without shielding, (2) fixed settings without shielding, (3) ABC with shielding of the uterus, and (4) fixed settings with shielding of the uterus. Five trials were performed for each modality using a fluoroscopy time of 60 seconds per trial. Radiation parameters for fixed exposure mode were 1.38 mAs and 66 kVp as determined by satisfactory scout images. Shielding was performed using a 0.5 mm portable lead plate with dimensions of 15 cm by 25 cm. Several scout images were taken to ensure satisfactory shield placement, and the beam and shield position were maintained constant throughout the study.
Radiation dosage was recorded directly using thermoluminescent dosimeters (TLDs) (Harshaw TLD-100 chips; Thermo Fisher Scientific, Waltham, MA). TLDs were placed in the hilum of the right kidney, on the right distal ureter (adjacent to the shield), and on the uterus. A single person was responsible for TLD placement at each site to ensure positional consistency between trials. To minimize absorption of stray radiation, TLDs were maintained outside of the operating room in a dark environment until utilization. Each TLD underwent a four-part calibration process. TLDs were first annealed in a PTW annealing oven (PTW-New York Corporation, New York, NY) for 6 hours at high temperature to remove any previous radiation exposure. They were then exposed to a known dose (.052 centigray [cGy]) with ∼35 kiloelectron volt [KeV] X-rays and stored for 24 hours. The TLDs were then read using the Harshaw 3500 TLD reader (Thermo Fisher Scientific, Waltham, MA) and assigned a calibration factor (average calibration factor of 26.9 nC/cGy). Before the procedure, the TLDs were reannealed, packaged individually into labeled plastic bags, and were carefully inventoried throughout the simulation.
Radiation dose obtained from the TLDs was compared by location alone, exposure mode alone, and location and exposure mode together. In addition, fluoroscopic picture quality was graded using a blinded survey of 15 urology attending physicians. Radiation dosages were first log-transformed to normalize the data and compared using two-way analysis of variance with location and exposure mode as factors. Results were presented as least square (LS) means and 95% confidence intervals after back-transformation. Tukey's honestly significant difference tests were used for any posthoc pairwise comparisons while image quality was compared using chi-square analysis. Significance was considered to be α≤0.05.
Results
Using fluoroscopy in the ABC mode with shielding resulted in average exposure settings of 2.25 mAs and 81 kVp. As mentioned, the fixed settings were 1.38 mAs and 66 kVp. In contrast, ABC mode without shielding resulted in average exposure settings of 1.61 mAs and 70.8 kVp. LS mean radiation dosages to the uterus were 0.16 cGy and 0.10 cGy for ABC and fixed settings without shielding, respectively, and 0.06 cGy and 0.02 cGy for ABC and fixed settings with shielding, respectively (Table 1). LS mean radiation dosages to the ureter were 0.11 cGy and 0.08 cGy for ABC and fixed settings without shielding of the uterus, respectively, and 0.22 cGy and 0.06 cGy for ABC and fixed settings with shielding of the uterus, respectively. Similarly, LS mean radiation dosages to the kidney were 0.03 cGy and 0.02 cGy for ABC and fixed settings without shielding of the uterus, respectively, and 0.05 cGy and 0.02 cGy with shielding of the uterus, respectively.
LS=least square; CI=confidence interval; ABC=automatic brightness control.
Overall fixed radiation doses were significantly lower than those delivered in ABC settings (with or without shielding; P for all <0.05). When analyzed by individual modalities, fixed settings with shielding received the lowest dose. ABC with shielding received the highest dose (3.4-fold increase compared with fixed settings with shielding) (Fig. 1). Total exposure (summation of dosage at all three sites) was not significantly different based on shielding status in the ABC mode. In comparison, shielding lowered the total exposure in the fixed mode (Fig. 1).
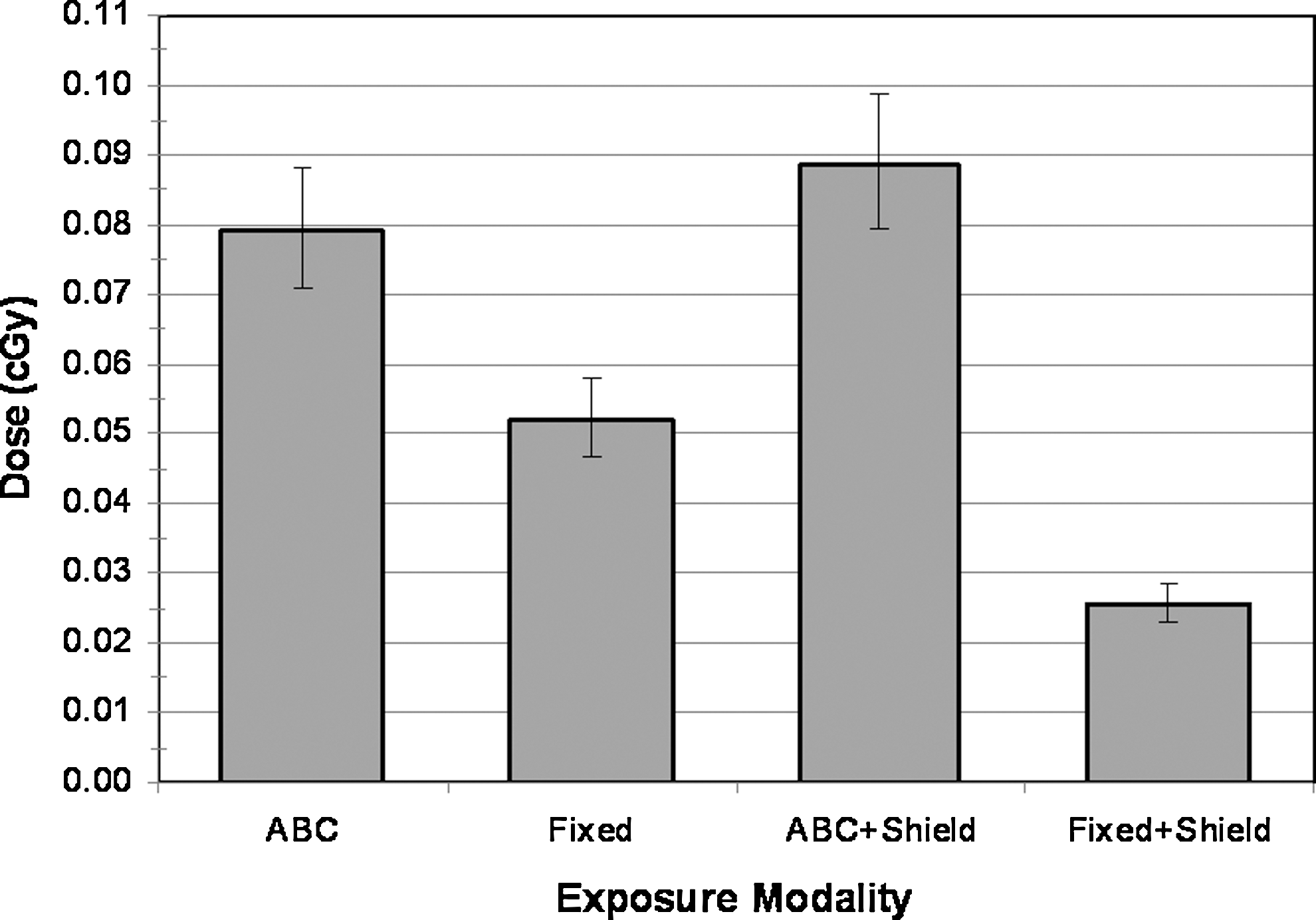
Average overall radiation exposure by modality (three sites combined).
Figure 2 depicts radiation dose analyzed by location and exposure modality. When shielding was performed under fixed exposure, radiation dosage at the uterus was significantly reduced by 82% (P<0.05). When performed in ABC mode, shielding also significantly reduced radiation to the uterus by 62%. When the uterus was shielded, however, radiation dose at the ureter and kidney was significantly increased by 95%, and 88%, respectively, using ABC. Increased radiation to surrounding structures did not occur with shielding in fixed settings.
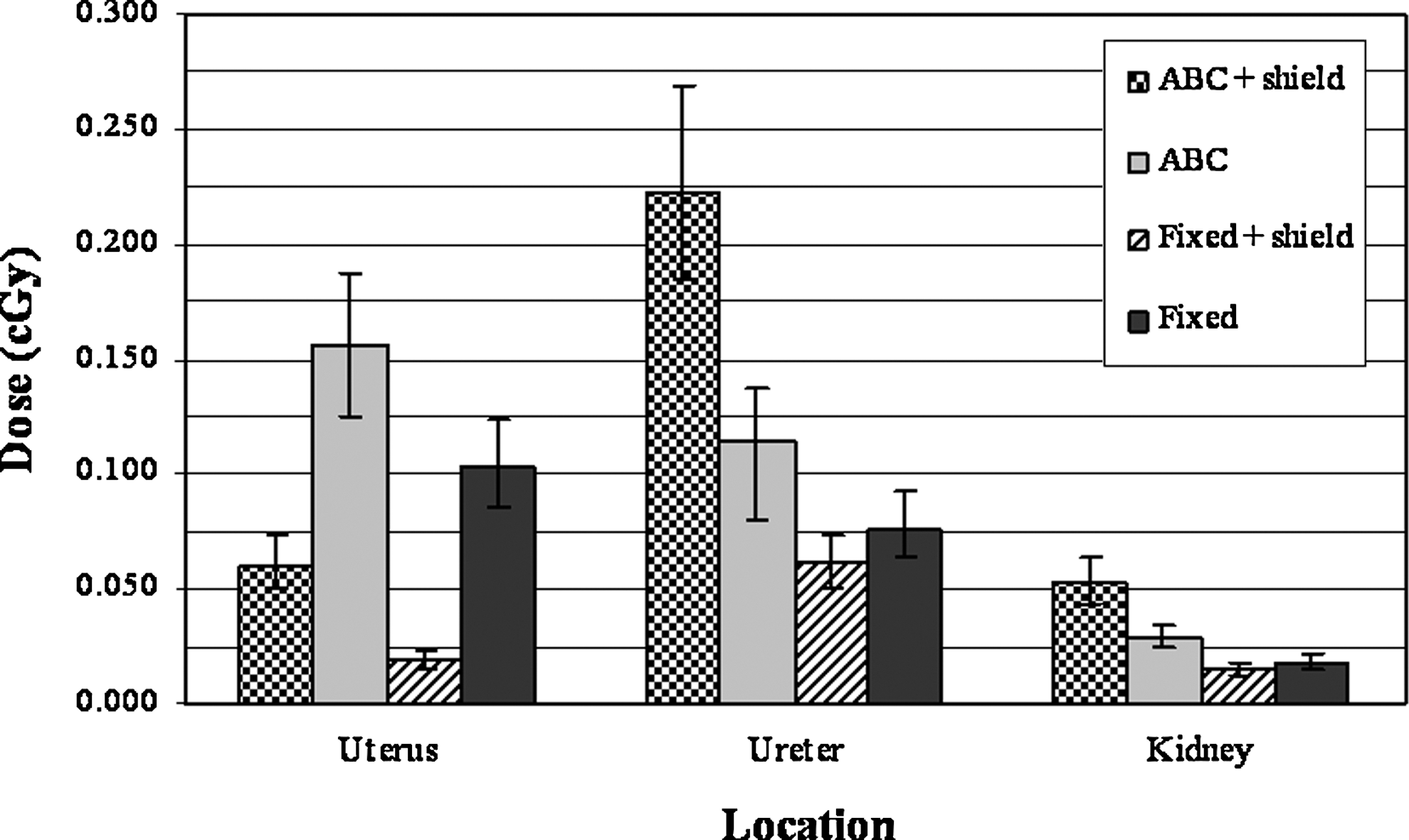
Radiation dose received by location and exposure modality expressed as least square mean with 95% confidence interval.
Comparing nonshielded ABC with nonshielded fixed settings, differences in radiation dose at all locations were statistically significant (P for all <0.05). Exposure at the uterus, ureter, and kidney was reduced by 34%, 33%, and 36% in fixed settings compared with the nonshielded ABC mode, respectively. Similarly, in the presence of shielding, radiation dose at all locations was significantly decreased by 69% at the uterus, 73% at the ureter, and 71% at the kidney in fixed settings when compared with ABC (P for all <0.05) (Fig. 2).
A review of the images recorded during our procedure shows that ABC mode also provided worse image quality than when fixed settings were used in the presence of a shield (Fig. 3). Fifteen of fifteen attending urologists rated fixed images as superior to ABC images when shielding was used.
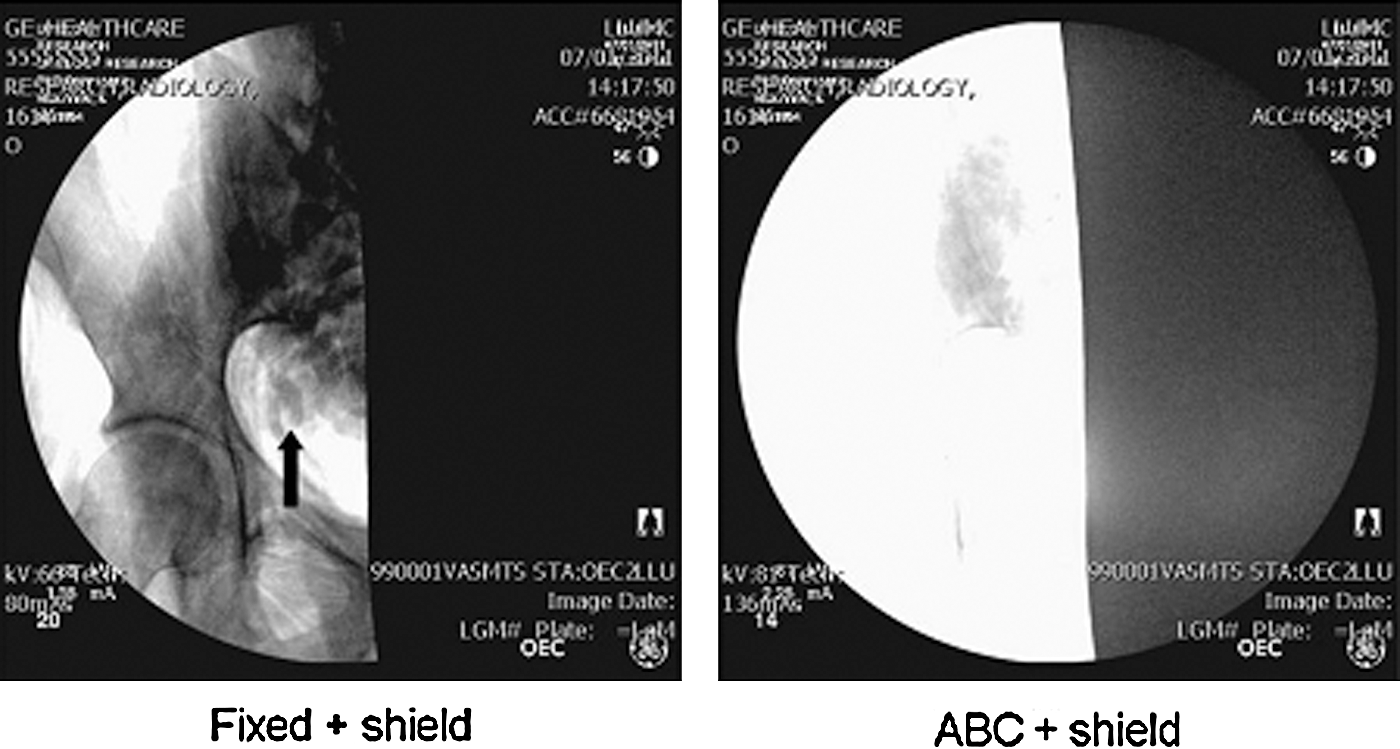
Representative scout images from each fluoroscopic setting and shielding combination. Arrow indicates distal ureteral stone.
Discussion
The discovery of X-rays by Roentgen in 1895 ushered in a new era of scientific achievement. 8 Subsequently, X-rays were used for a wide variety of medical and diagnostic purposes. Many of these early uses, such as using X-rays directed at the ovaries to treat infertility, were later found to be ineffective and resulted in deleterious side effects. In 1896, it was discovered that damage to the eye occurred with prolonged exposure to X-rays; in April of the same year, epilation and skin changes were first reported. 8 Awareness of these deleterious side effects led to the implementation of radiation protection measures. Dr. Rollins, a dentist and pioneer of radiation protection, developed several theories on radiation safety after a severe burn to his hand during early experimentation with X-rays. These principles included: Wearing radiopaque (leaded) glasses, enclosing X-ray tubes in a leaded housing, and irradiating only the area of interest. 8 This third principle of confining the radiation only to the area of interest is the premise behind both collimation and shielding. Unfortunately, at the time, his principles were mostly disregarded. For example, he first developed the rectangular collimator in 1903, but it was not widely adopted until the 1950s.
Because of the increased awareness of the risk of malignancy in patients receiving medical imaging, many centers have adopted measures to reduce unnecessary radiation to their patients. 3 Recently, this risk from radiation exposure during fluoroscopy was highlighted in a 2010 publication of the United States Food and Drug Administration that called for a reduction in radiation during fluoroscopy, CT, and nuclear medicine studies. 9 The United States is not alone in this action; the United Kingdom as well as Western Europe have initiated legislation to institute protective measures to reduce radiation exposure to patients undergoing medical imaging. 10
Fluoroscopy is an integral portion of most endoscopic cases, but the heavy reliance on this modality may result in significant radiation exposure for patients. Several methods have been reported to reduce radiation exposure during fluoroscopy. These include optimizing image intensifier positioning, use of last image hold, use of a laser guide, collimating the fluoroscopy beam, and shielding. 5 To optimize patient protection, it is important to use all possible measures.
All forms of shielding have shown effectiveness in reducing direct as well as scatter radiation to various parts of the body, including the thyroid, breast, uterus, ovaries, and the testicular region in men. 11 –13 In addition to protection for patients, many studies have also evaluated methods to optimize work environments using lead curtains, tableside drapes, and lead vests to reduce radiation exposure to medical personnel. 14 –16 Because of such studies, shielding of the gonads and abdomen is recommended as an effective measure for reducing radiation exposure to patients. 17,18 Similarly, our results demonstrate the effectiveness of shielding to reduce exposure to the shielded organ.
The use of ABC with fluoroscopy is believed to help reduce overall radiation to patients by automatic calculation of the kVp and mAs needed for optimization of the fluoroscopic image based on the tissue density in the field of interest. This automatic control is based on a feedback mechanism from either the ionization chamber or the photodetector, which is then compared with a reference signal and automatically adjusted. This adjustment can occur in a number of ways, but typically when trying to reduce radiation, the kVp is first maximized to obtain the proper image quality, and beyond this maximal point the mAs is then increased. 6 An unfortunate side effect of this technology occurs when the tissue density is overestimated (as is observed with shielding), resulting in unnecessary increases in kVp and mAs. The sensor feedback then results in significantly higher exposure and decreased image quality as was demonstrated in our study. When shielding was used during ABC mode, we found a 95% and 88% increase in radiation exposure to the right adjacent ureter and ipsilateral kidney, respectively.
Fixed settings in fluoroscopy avoid the feedback mechanism of ABC, thus eliminating the possibility of falsely elevating exposure from shielding. The difference in exposure to surrounding tissue in fixed settings with or without shielding was not significant at either the kidney (P=0.30) or right ureter (P=0.24). This is in contrast to ABC mode where the surrounding tissue had significantly elevated radiation dosage at both the kidney and right ureter (P for all <0.01) with shielding in place. This benefit of reduced radiation outweighs the potential increased complexity of manual exposure adjustments. These manual settings can be easily created by a skilled fluoroscopy technician.
This is the first study to present the effects of radiation to the surrounding tissues when shielding is used during a simulated ureteroscopy. Similar ideas have been presented regarding other dense structures in the fluoroscopic field. A study performed in 2004 reported a 2.3-fold increase in skin dose when automated settings were used for imaging of the bladder in the presence of contrast. 19 A study by Leibovic and Caldicott 20 demonstrated that using ABC during a barium swallow resulted in a twofold increase in exposure. These studies in combination with the results of our study demonstrate that when a dense object is present within the fluoroscopic field, ABC settings should be avoided because it consistently results in higher radiation doses to patients.
There are some limitations of our study. One potential limitation may be the use of a thin cadaver with BMI of 22, which may not be representative of the general population of the United States. We intentionally selected this low BMI cadaver because it would most closely represent a child or young female of reproductive age, which represents the highest risk population for radiation exposure. Furthermore, it is likely that the increased radiation exposure with ABC would be consistently demonstrated regardless of BMI. Because the radiation shield is consistently more dense than surrounding human tissue, ABC mode will consistently overestimate density when shielding is used, resulting in an increased radiation exposure. The radiation exposure increase may have a smaller percent increase in a person with a high BMI, but the overall dose would presumably be higher because of the increased tissue density of the person.
Use of a cadaveric model with desiccated tissue may underestimate the tissue densities seen in living patients. Use of the cadaver model, however, allowed us to compare multiple exposure settings in the identical situation, something that would have been unethical in a living patient. Despite these limitations, our results demonstrate that physicians should use fixed settings in the presence of shielding to reduce radiation exposure and maximize picture quality.
Conclusion
Shielding is highly effective for reducing radiation exposure to the uterus using ABC and fixed settings. There is a drawback, however, to using automated settings in the form of increased radiation to surrounding unshielded tissue when there is a high-density region within the fluoroscopic field. For better image quality and overall reduction in radiation exposure, fixed fluoroscopic settings should be used when shielding is employed.
Footnotes
Disclosure Statement
No competing financial interests exist.