
Abstract
Background and Purpose:
The existence of upper urinary tract calculus may cause complete loss of renal function, which eventually results in nephrectomy. Our purpose was to describe the prevalence and clinical characteristics of upper urinary tract calculus cases among a series of patients undergoing nephrectomy during a 10-year period.
Patients and Methods:
The data of 1059 patients undergoing nephrectomy between January 2001 and December 2010 in our center were reviewed. The prevalence and clinical characteristics of upper urinary tract calculi-derived nonfunctioning kidney were analyzed.
Results:
Among 1059 patients, 177 (16.7%) had nonfunctioning kidneys, which were second in number to renal tumor cases (801, 75.6%). Upper urinary tract calculi accounted for the greatest cause (101, 57.1%) in these nonfunctioning kidney cases. These patients were mainly screened by ultrasonography and the diagnosis confirmed by CT, intravenous urography, and nuclear renography. There were 44 (43.6%) patients with a single renal stone in the ureteropelvic junction, 36 (35.6%) with a single ureteral stone, and 21 (20.8%) with multiple unilateral renal and ureteral stones. The average size of the renal stones and ureteral stones were 15.6±8.8 mm (4–50 mm) and 13.4±4.0 mm (4–21mm) in diameter, respectively. Prevalence of urolithiasis derived nonfunctioning kidney had not changed significantly over 10 years and even showed a slight increase. Most of the stones were more than 10 mm in diameter. A nonfunctioning kidney was more likely to develop in females or patients with a low living standard.
Conclusions:
Upper urinary tract calculus (>10 mm) and loss to follow-up are the greatest risk factors for a nonfunctioning kidney. A nonfunctioning kidney develops more easily in females or patients with a low living standard. A regular urinary system health examination is recommended. Routine follow-up of urolithiasis is also recommended for patients with a stone history to prevent renal dysfunction.
Introduction
Upper urinary tract urolithiasis may lead to hydronephrosis, a peculiar type of atrophy of the kidney that may terminate in renal insufficiency or unilateral, complete destruction of the organ. 4 Urolithiasis-derived nonfunctioning kidney (NFK) may eventually lead to nephrectomy. It is an evolutionary process, however, and if we can detect it early before deterioration, nephrectomy can be avoided.
We reviewed the data of 1059 patients who underwent nephrectomies in our center and analyzed the clinical characteristics of urolithiasis-derived NFK.
Patients and Methods
From January 2001 to December 2010, a total of 1059 patients underwent nephrectomies (simple and radical) via open or laparoscopic procedures in our center. There were 633 (59.8%) males and 426 (40.2%) females. The mean age was 53.7±14.0 years (range 11–86 years) including 54.0±14.1 in males and 53.4±13.9 in females (P>0.05). Among 1059 patients undergoing nephrectomy, the primary diseases were: Renal tumor in 801 (75.6%), upper urinary tract lithiasis in 101 (9.5%), tuberculosis in 28 (2.6%), iatrogenic causes (mostly missed ligation of ureter during gynecologic operations) in 14 (1.3%), and other causes in 115 (10.9%), including duplex kidney in 8 (0.8%), polycystic kidney-derived chronic kidney disease in 9 (0.9%), rejection of transplanted kidney in 12 (1.1%), donors of renal transplantation in 15 (1.4%) (Table 1). There were no patients with both calculus and renal tumor.
UPJ=ureteropelvic junction; NFK=nonfunctioning kidney.
These urolithiasis patients were screened by ultrasonography or by incidental CT scan for other purposes. All these patients needed to have intravenous urography (IVU), noncontrast CT, and nuclear renography.
The criteria of NFK were as follows: (1) Glomerular filtration rate (GFR)<10 mL/min/1.73 m2 in the affected kidney by nuclear renography 5 and (2) nonvisualization of unilateral kidney by IVU. Thin renal cortex (≤5 mm) by noncontrast CT highly indicated NFK.
Unilateral nephrectomy was performed in these NFK patients to eliminate the existing or to avoid the imminent harm such as recurrent urinary tract infection (UTI), hematuria, flank pain, or hypertension.
The parameters of patients with urolithiasis, including demographic information, patient history, clinical manifestations, stone location and size, and laboratory examinations, were collected and analyzed. Stone location and size were confirmed and calculated on the kidney specimens after removal.
The t test and chi-square test were used to compare groups for categorical variables, and a P value<0.05 was considered a significant difference.
Results
There were 101 patients who underwent nephrectomy who had primary disease of upper urinary tract stones compared with a contemporary series of 1059 cases of nephrectomy. There were 48 (47.5%) males and 53 (52.5%) females in this group. The mean age was 52.2±12.7 years (15–74) including 50.7±12.0 in males and 53.4±13.3 in females (P>0.05). Prevalence of urolithiasis-derived NFK had not changed significantly during the 10 years. Five-year incidence per 1000 nephrectomies increased slightly from 87.82 (2001–2005) to 99.15 (2006–2010) (Figs. 1 –3).
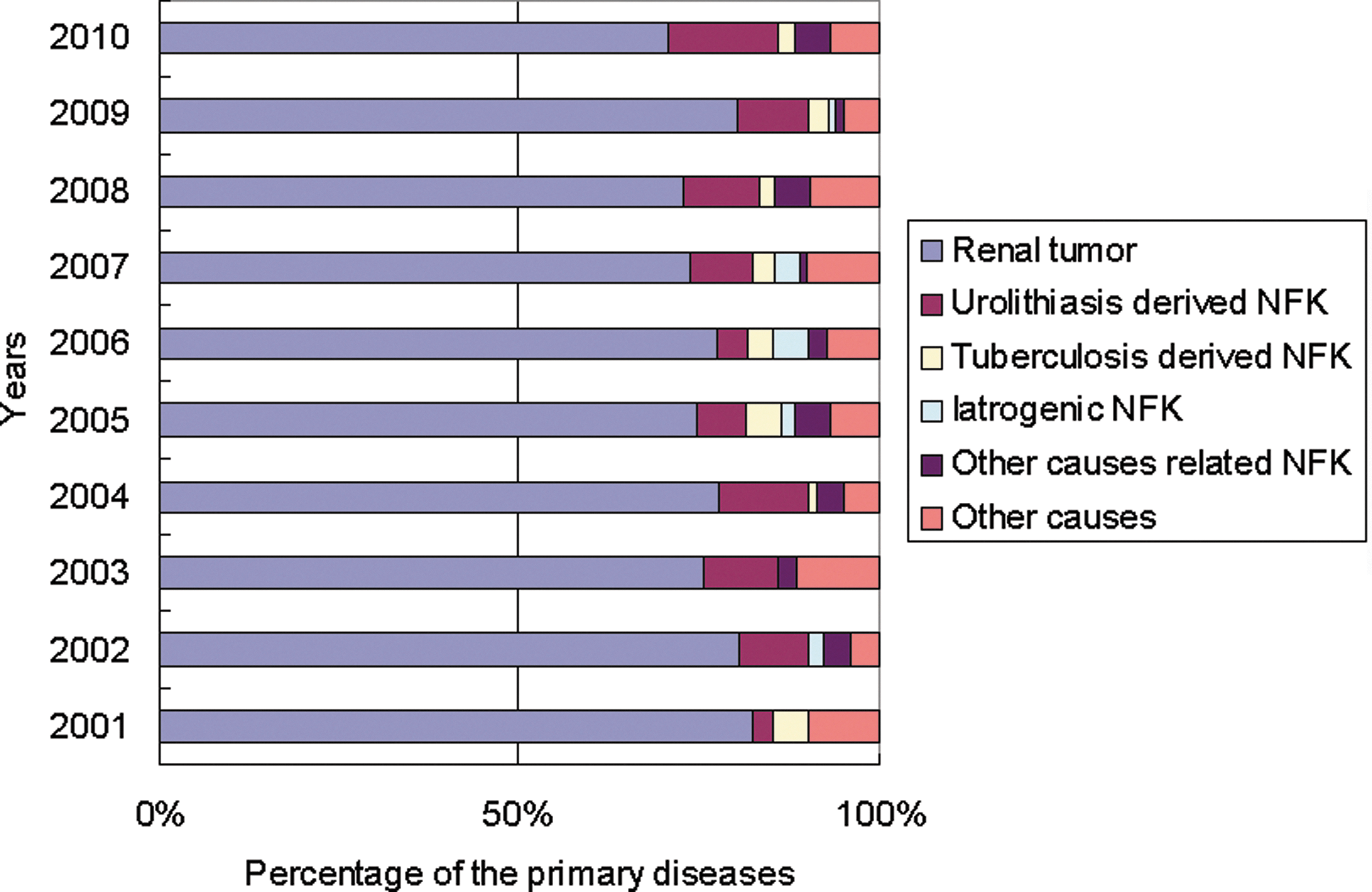
Annual prevalence of urolithiasis-derived nonfunctioning kidney (NFK) during 2001 to 2010. The prevalence had not changed obviously during these 10 years.
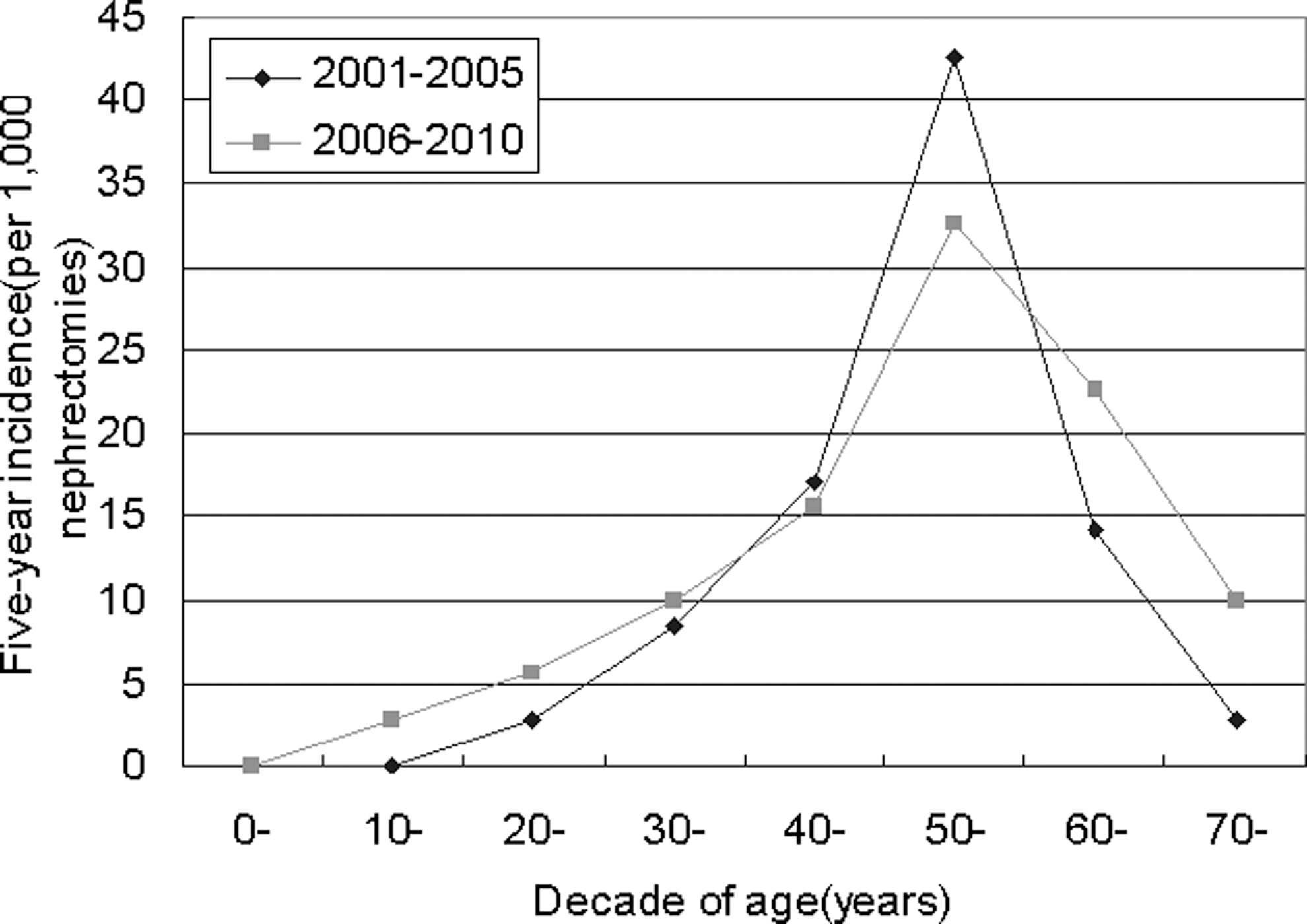
Five-year incidence of urolithiasis-derived nonfunctioning kidney (NFK) per 1000 nephrectomies by decade of age during 2001 to 2005 and 2006 to 2010. Five-year incidence had not changed during 10 years, and distribution pattern in the age group was uniform.
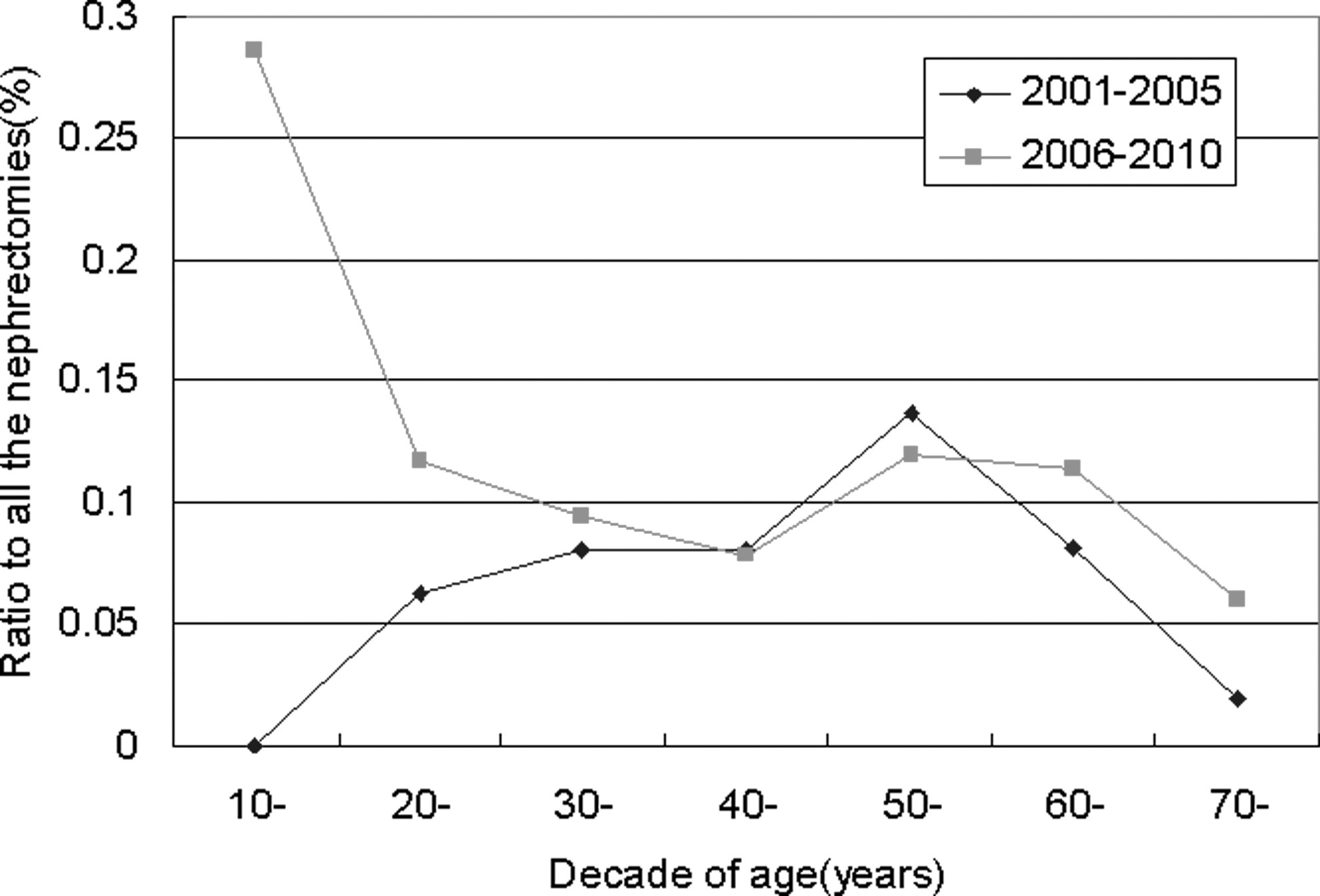
Ratio to all the nephrectomies shown by decade of age during 2001 to 2005 and 2006 to 2010. Extremely high rate in 10s in 2006 to 2010 was observed, possibly because of the small basic number of 10s patients. Decrease of population in 30s and increase in 50s were observed as well. Possibly because of the counterbalance of these young and old generations, incidence was not changed by age adjustment.
There were 24.8% (25 in 101) patients who had no symptoms, such as renal and ureteral pain or gross hematuria, and were accidentally detected by ultrasonography or CT scan for health examination or other purposes. There were 16.8% (17 in 101) patients who had such symptoms, but received a diagnosis of NFK the first time. The rest of the patients (58.4%, 59 in 101) had such symptoms and were not well-treated because of loss to follow-up and in whom NFK developed afterward. There were 34.7% (35 in 101) patients who had a history of urolithiasis. Thirty-one of them had been treated with medication, extracorporeal shockwave lithotripsy (SWL), ureteroscopy (URS), percutaneous nephrolithotripsy (PCNL), open or laparoscopic ureterolithotomy before, and then NFK developed within 7.20±6.94 years on average (1 month to 30 years). Of these patients, all NFK were caused by recurrent stone disease and patients in whom stricture disease developed secondary to surgical intervention were grouped to “Other causes related NFK.”
There were 44 (43.6%) patients with renal stones obstructed in the ureteropelvic junction, 36 (35.6%) patients with ureteral stones, and 21 (20.8%) patients with multiple unilateral renal and ureteral stones. The average size of the renal stones and ureteral stones was 15.6±8.8 mm (4–50 mm) and 13.4±4.0 mm (4–21 mm) in diameter, respectively (Table 2). The blood creatinine level of patients with urolithiasis (88.60±31.61 μmol/L) was significantly higher than that of other patients undergoing nephrectomy (80.52±36.99μmol/L) (P<0.05). In addition, the urine white cell count of patients with urolithiasis before surgery (235.82±585.59/μL) was also significantly higher than that of others (62.50±179.92/μL) (P<0.01). There also existed sex difference (359.54±753.04/μL in female and 92.85±227.8/μL in male, P<0.05) in urolithiasis cases (normal range 0–16.9/μL). The patients with urolithiasis who had UTI (70 in 101, 69.3%) was much higher than in nonstone patients (379 in 958, 39.6%).
UPJ=ureteropelvic junction.
According to the average annual per capita disposable income of every city during 2001 to 2010 published in the website of National Bureau of Statistics of China, 6 both urolithiasis and other nephrectomized patients were estimated and divided into three groups: Low income (≤$1500), middle income ($1500–$2250), and high income (≥$2250). Low-income urolithiasis patients accounted for 19.8% (20 in 101), which was significantly higher than other nephrectomized low-income patients—6.8% (65 in 958), (P<0.05). High-income urolithiasis patients accounted for 67.3% (68 in 101), which was significantly lower than other nephrectomized high-income patients—77.5% (742 in 958), (P<0.05). There was no significant difference of middle-income patients between urolithiasis and other nephrectomized patients (Table 3).
In addition to urolithiasis-caused NFK, there were another 14 NFK patients with a diagnosis of iatrogenic stricture. Among them, 12 patients had a history of gynecologic surgery, such as total hysterectomy, and there were two patients with cervical cancer who had received radiotherapy and chemotherapy after surgery. There were another six patients with pyelolithotomy or ureterolithotomy surgery (one of them underwent laparoscopy) who were grouped as “Other causes related NFK.” The gynecologic patients averaged 2.81 years from the previous operation to the time when nephrectomy was necessary. For the cervical cancer patients, NFK developed in one after 5 years and in another, 6 months after radiotherapy and chemotherapy.
For lithotomy patients, the time interval between stone surgery and need for nephrectomy was quite different, with a range from 1 to 16 years and an average of 6.1 years. Thirteen (65.0%) patients complained of loin soreness and discomfort. Four (20.0%) patients complained of recurrent loin pain, and three (15.0%) patients were found by health examination with no symptoms. Two (10.0%) patients in this series also had hematuria.
Discussion
The annual incidence of upper urinary tract calculi has steadily increased in the Asian area, and this trend is predicted to continue in the near future. 7,8 The modern technologies, including SWL, URS, and PCNL, are widely used and have favorable outcomes for upper urinary tract stones. Our data, however, showed that there were still some urolithiasis patients (1.7%, 101 in 5781 urolithiasis patients treated with nephrectomy and other modalities in our center during these 10 years) who needed nephrectomy.
Total removal is the eventual choice for the kidney that completely loses its function. The actual occurrence of NFK had not changed during 10 years and even showed a trend toward a slight increase. Therefore, how to detect it and to prevent it from happening becomes important.
NFK is more likely to develop in females. In the general population, males are more likely to get urinary tract lithiasis. In this series, however, there were 47.5% of males and 52.5% of females with urolithiasis-derived NFK compared with the overall incidence of urolithiasis between men (70.77%) and women (29.23%) 7 (P<0.05). Estrogen may contribute to the protective effect on the progression of chronic renal disease. 9 –11 The female patients with NFK in this series had an average age of 53.4±13.3 years. The great decrease of estrogen might cause the loss of the protective effect. What is more, the urine white cell count of female urolithiasis patients was significantly higher than that of male patients. UTI might contribute to renal function loss. Whether UTI is the cause of renal function loss or the result of NFK, however, still needs further study.
The size of stones was the risk factor in this series of patients in whom NFK developed. The mean sizes of both renal stones and ureteral stones were >10 mm in diameter. It was reported that most stones were smaller than 5 mm in diameter at the time of diagnosis. 12 Coll and associates 13 also demonstrated the size of ureteral calculi at an average of 4.38 mm at the time of diagnosis. This series of patients had larger ureteral calculi (13.4±4.0 mm) compared with the calculi in a series of patients who were treated with URS and holmium laser lithotripsy (12.0 mm) in our center (P<0.05). 14 The kidney stones were bigger and were in the ureteropelvic junction, which tobstructed the urinary tract and caused the renal function loss. 4 Bigger stones were prone to cause severe obstruction that eventually led to NFK.
NFK was more likely to develop in patients with a low living standard. The prevalence of urolithiasi- derived NFK in the high-income area was comparatively low (P<0.05), while patients in the low-income area had high prevalence (P<0.05). The prevalence of urolithiasis-derived NFK had a negative relationship with the living standard. Low income, however, may be only a surface phenomenon. It will lead to lots of socioeconomic issues that will influence the patients' medical counseling behavior.
To investigate the potential association, we did a telephone follow-up of 41 patients in this series with 15 low income ones; we found 93.3% of those 15 low income ones had an educational level lower than undergraduate and 40.0% of those 15 low income ones had no health insurance or only a low welfare one. In addition, lots of those 15 low income ones lived far away from big hospitals in a rural area. Approximately three quarters of is low income ones regarded flank discomfort as normal and did not need further medical counseling. All those socioeconomic factors will influence patients not to go for medical consultation.
Loss to follow-up was the greatest risk factor for urolithiasis-derived NFK. Routine follow-up is important for patients with a history of urolithiasis, and regular health examination is also recommended. More than half of the NFK patients received a diagnosis of urolithiasis but had no consultation with urologists and were not well-treated because of loss to follow-up. Also, through the telephone follow-up we did, we found that nearly two-thirds of them regarded flank discomfort as normal and only needed a rest to relieve the discomfort. Among those who had received a diagnosis of urolithiasis before NFK, most of them thought it did not matter and would not affect their health, so they did not go to the doctor for medical consulation.
Therefore, the publicity of scientific knowledge of urolithiasis will be critical at this time. As for us physicians, especially general practioners, we should emphasize its importance and harm and ask patients to go to a specialty physician for medical assistance. In addition, lots of socioeconomic factors influence the patients as well. For example, the low-income–related issue will influence the patients, as stated.
Meanwhile, although some urolithiasis patients (around one-third) had been treated with medication or surgical modalities, the recurrent stone can lead to urinary obstruction again. What is more, nearly one-fourth of patients in this series were incidentally detected by ultrasonography during a health examination. Nearly one-fifth patients received a diagnosis of NFK right after the presentation of symptoms. Furthermore, renal function loss caused by urinary tract obstruction is an evolutionary process and if we can detect it early before deterioration, nephrectomy can be avoided. Therefore, no matter whether treated or not, routine follow-up for patients with a urolithiasis history and regular health examination of the urinary system becomes quite necessary. Ultrasonography is often a first-line option, because it remains relatively inexpensive and widely available. 5
For iatrogenic stricture patients, both gynecologic and lithotomy surgery were the leading cause. Although the incidence rate was low, we should strive to reduce its occurrence. NFK is a gradual process; in most patients, it took years for NFK to develop with slight symptoms. The majority feel flank soreness or discomfort. Thus, we cannot neglect such unspecific symptoms and should prescribe ultrasonography or renography (GFR) to know the renal function, etc.
For stone surgery, lithotomy may lead to cicatricial constriction in the original incision because of scar formation. For gynecologic surgeries the ureter is located quite close to female reproductive organ and postoperative peritoneal/pelvic adhesions are the most frequent complication of surgery. Therefore, such pelvic adhesions may lead to ureteral stricture. What is more, it is quite easy for the ureter to be injured because of its close anatomic relationship. We just found one postgynecologic case, in which the patient received a diagnosis of hydronephrosis by health examination. During nephrectomy, we found a titanium clip on the ureter. Therefore, the urologist should improve the ureteral suture method to prevent cicatricial constriction-caused NFK. Gynecologists should have a better grasp of ureteral anatomy and should carefully preserve the ureter during the operation.
As for limitations, selection bias of the patients may be one of them. We include all the nephrectomy cases in these 10 years in our center, however, and what we consider is the changing tendency of the constituent ratio of all the etiologic factors. Therefore, it should not be a major concern.
Conclusions
Upper urinary tract calculus is the main primary cause of NFK and is the major disease with nephrectomy for nontumor patients. The prevalence of NFK remains constant regardless of the widely used endoscopic technique and screening. Loss to follow-up is the major reason for NFK; in addition, the size of stones (>10 mm) is also a risk factor. NFK is more likely to develop in females. Regular health examination of the urinary system is recommended. Routine follow-up of urolithiasis is recommended for patients with stone history, especially for those in low-income areas.
Footnotes
Disclosure Statement
No competing financial interests exist.