
Abstract
Ureteral stents are commonly used in urologic practice and have a number of well recognized complications. A rare complication is knotting with associated difficult removal having been reported in only 15 previous cases. Various methods of removal have been described. We report an additional case in which a ureteroscopic holmium laser was successfully used to remove a knotted ureteral stent. A literature review of all previous cases of this rare complication is also presented.
Introduction
We present an additional case describing our eventual choice of holmium laser ablation to remove a proximal knotted Double-J stent and a literature review of other methods previously used.
Case
A 43-year-old man with Crohn's disease underwent a combined plastics and colorectal surgery for recurrent perineal abscess and parastomal hernia. Colorectal surgeons performed a laparotomy with division of adhesions and resiting of the ileostomy in addition to a wide local excision of the perineal abscess. Plastic surgeons fashioned a gracilis flap reconstruction. Before the abdominal procedure, urologic surgeons placed bilateral 6F Double-J stents via rigid cystoscopy as an aid to intraoperative identification. Bilateral retrograde pyelography showed normal upper tract anatomy and correct stent placement. The patient had originally undergone a total colectomy via abdominoperineal resection with ileostomy for medically unresponsive Crohn's disease 5 months previously.
Eleven days postprocedure, the patient's stents were planned for removal via flexible cystoscopy. The left Double-J stent was removed easily. On attempting to remove the right Double-J stent, firm resistance was encountered, and the attempt abandoned. Plain radiography (Fig. 1) demonstrated the proximal part of the stent had knotted and lodged in the proximal ureter at the level of L4. Retrograde pyelography showed the knot was partially obstructing the ureter with little contrast flowing proximal to the knot.

Plain radiograph demonstrating knotted ureteric stent at L4 level.
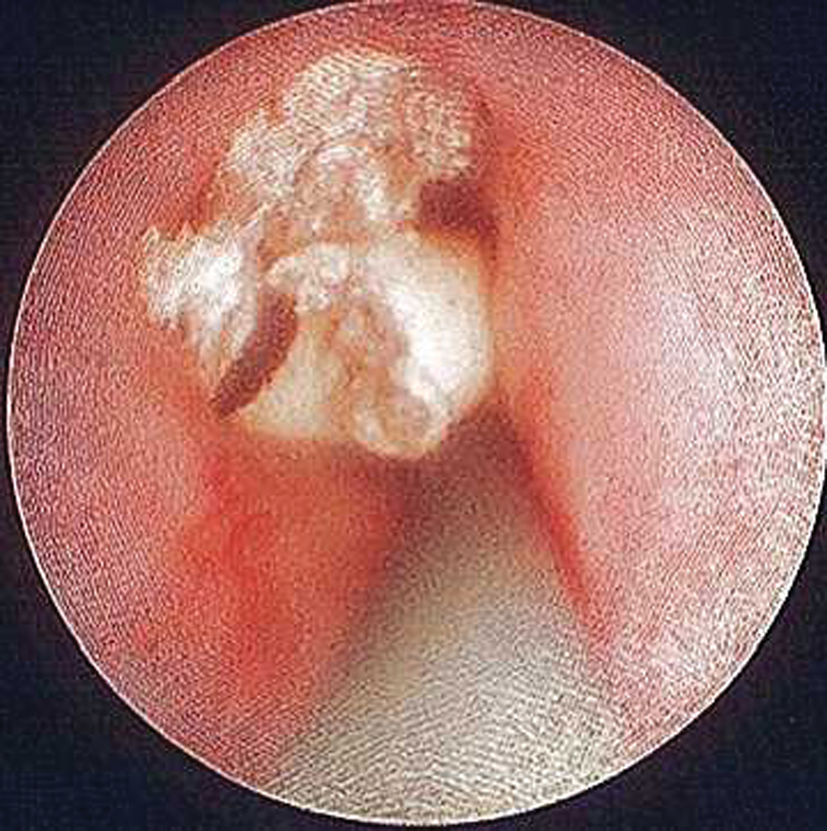
Initially, removal with gentle traction with rigid cystoscopy with the patient under general anesthetic was attempted but without success. Secondly, a rigid guidewire was used to cannulate the distal end of the Double-J stent, to try to straighten out the proximal knot, again unsuccessfully. Next, a flexible guidewire was negotiated past the knot into the renal pelvis with some difficulty. A rigid ureteroscope was inserted to the level of the knot (Fig. 2).

Ureteroscopic view of knotted ureteric stent.
A 2100 nm holmium laser was used to transect the proximal knot in the stent. Settings were 8 Hz and 0.6 J. This resulted in the knot breaking into three parts and being detached from the proximal end, which was easily removed (Fig. 3). The ureteroscope could then push the remaining parts of the stent into the renal pelvis where they unfolded and were removed via grasper. A 6F Double-J stent was placed afterward under radiographic guidance, and the patient was discharged home the following day.
Ureteroscopic view of knotted ureteric stent post application of holmium laser.
Discussion
Knotting of ureteral stents is an uncommon but serious complication encountered in urological practice. Of the 15 cases reported, 14 involved the proximal end of the stent with only one involving the distal end, which had been lost through the ureteral orifice. 8 Associated pathology reported resulting in stent use was renal calculi in nine cases, ureteral surgery in two cases, patients with an ileal conduit in two cases, and ureteral stent placement as a precaution in one of the cases. Pathology was not recorded in one case. 9 These numbers may simply reflect the prevalence of pathology in daily practice as opposed to any predilection to stent knotting.
Stent type was almost universally Double-J multilength with 4.8F, 6F, and 7F used. Previous discussion regarding stent knotting has suggested that excessive length of insertion may increase the risk, 10 but this did not prove to be universal in all cases. After review of existing cases and our own experience, we postulate that the use of double coiled stents is likely to increase the risk of knot formation.
Of the methods used to remove knotted stents, graduated traction was the most common, being successful in 8 of the 15 reported cases. 9,10 –16 This, however, can pose the risk of ureteral avulsion. Various adjuncts to traction were used, such as shockwave lithotripsy in a patient with an encrusted proximal end 8 and the insertion of lubricant combined with rotation of the stent in a patient with an ileal conduit. 11 In one case where the knot was nonobstructing, traction was applied for successful removal over 3 days. 14
Other methods used included insertion of a stiff Amplatz wire to untie the knot in one case 17 and ureteroscopic manipulation in another. 8
Notably, in 4 of the reported 15 cases, the aforementioned methods failed or were unsuitable, and percutaneous access to aid removal was needed. 18 –21 Percutaneous nephrostomy is not without its own risks and adds an additional treatment to a patient who was originally scheduled for a simple stent removal.
Holmium laser is well established in urological practice for urolithiasis. 22 It is can also be used for treatment of patients with urethral and ureteral strictures, 23,24 bladder outlet obstruction, 25 and treatment of the caliceal diverticula neck. 26 Notably, holmium laser has been reported as useful in other urologic cases for urinary tract foreign body removal, such as urethral catheters and stone baskets. 27 –29 In our case, as was reported by Richards and associates, the use of holmium laser delivered via rigid ureteroscopy offers an endoscopic option for the difficult knotted stent removal and that may allow avoidance of percutaneous intervention.
Conclusion
Knotting is an uncommon but serious complication that must be considered when firm resistance is encountered on removal of ureteral stents. It is possible that the use of double coiled stents increases the risk of knot formation. The first treatment is to avoid excessive traction, which may risk ureteral avulsion. Failing simple maneuvers removing the stent, a variety of methods both endoscopic and percutaneous exist for their removal. Holmium laser application via flexible or rigid ureteroscopy is a useful alternative that may be used when other noninvasive methods have failed, before proceeding to more morbid options.
Footnotes
Disclosure Statement
No competing financial interests exist.