
Abstract
Background and Purpose:
Fruits and vegetables are natural suppliers of potassium, bicarbonate, or bicarbonate precursors such as citrate, malate and others—hence, possessing potential effects on citraturia. We aimed to compare the acute effects of a noncitrus (melon) fruit vs citric ones (orange and lime) on citraturia and other lithogenic parameters.
Patients and Methods:
Two-hour urine samples were collected from 30 hypocitraturic stone-forming patients after an overnight fast and 2, 4, and 6 hours after the consumption of 385 mL (13 oz) of either freshly squeezed orange juice (n=10), freshly blended melon juice (n=10), or freshly squeezed lime juice (n=10). Urinary citrate, potassium, pH, and other lithogenic parameters were determined and net gastrointestinal alkali absorption (NGIA) was calculated. Potential renal acid load (PRAL) and pH from juices were determined.
Results:
Significant and comparable increases of mean urinary citrate were observed in all groups, whereas mean urinary potassium, pH, and NGIA were significantly increased only after consumption of melon and orange juices. The pH of melon juice was higher and the PRAL value was more negative compared with orange juice, indicating a higher alkalinity.
Conclusions:
These findings suggested that melon, a noncitrus source of potassium, citrate, and malate, yielded an increase in urinary citrate excretion equivalent to that provided by orange, and hence represents another dietary alternative for the treatment of hypocitraturic stone-formers. Despite its low potassium content, lime also produced comparable increases in citraturia possibly because of its high citric acid content.
Introduction
Citrus fruits, such as oranges, lemons, limes, and some tangerines, are a natural source of dietary citrate and may be a nonpharmacologic dietary alternative therapy to potassium citrate. Numerous short-term studies of urinary chemistry measures have demonstrated that urinary citrate levels increased after consumption of either grapefruit juice 3,4 or orange juice 4 –6 or lemonade, 7 –10 whereas a few yielded no improvements in citraturia with lemonade. 5,11
Whenever citrate is in the form of a potassium salt, virtually all citrate absorbed from the gastrointestinal tract is oxidized in the liver to form bicarbonate, with no serum bicarbonate titration, leading to systemic alkalinization. Subsequently, alkalosis decreases renal tubule reabsorption of citrate, increasing urinary citrate excretion. 1 This is the case for citrate in orange and grapefruit, complexed mainly by potassium. 5 In contrast, if citrate is ingested as citric acid, as in lemon, in which the accompanying cations are protons, neutralization of the bicarbonate formed in the liver is ensured so that there is no net effect on acid-base status. 12 Nevertheless, citraturic effects of oral citric acid may be attributed to some of the absorbed citrate escaping liver oxidation and degradation. 12
The extent of systemic alkalinization seems to be more important than direct delivery of unmetabolized citrate to the kidney to determine citrate excretion. Therefore, any compound that causes a systemic alkalosis increases citrate excretion. Malate is a polycarboxylic anion, like citrate, that is present in many fruits and fruit juices. If delivered as an alkali salt, malate should also increase urinary citrate as described by Eisner and associates. 13
In two large observational studies, Curhan and colleagues 14,15 have shown that the incidence of stone disease dropped in proportion to the increase of potassium in the diet. A significant direct correlation between urinary potassium and citrate excretion has previously been reported by our group. 16 A study conducted by Meschi and coworkers 17 has shown that the addition of fruits and vegetables to the diet of 26 hypocitraturic stone formers not used to eating them led to a markedly significant increase in urinary citrate, potassium, volume, and pH and a decrease in ammonium excretion. Fruit and vegetable supplementation for these stone formers contained freshly squeezed orange juice, a choice of fresh mixed fruits (citrus and noncitrus, such as oranges, melons, etc) rich in potassium and/or malate or citrate, consumed along with fresh mixed vegetables, providing an additional intake of potassium of almost 50 mmoL/d. Although the association between potassium and citrate excretion from induced changes in intracellular pH is well defined, the separate contribution of dietary citrus vs noncitrus sources of citrate and potassium could not be distinguished. 17
In the present study, we aimed to investigate the acute effects of a noncitrus fruit (melon) vs citric ones (orange and lime) on citraturia and other lithogenic parameters in hypocitraturic stone formers.
Patients and Methods
Patients and study design
Thirty adult hypocitraturic calcium–stone-forming patients followed up at the renal lithiasis unit of the nephrology division from Universidade Federal de São Paulo participated in the study, which was approved by the local ethics committee. A written consent was obtained from all subjects. Stone disease was diagnosed on the basis of renal colic with confirmed hematuria and voiding of a calculus and/or previous surgical or endoscopic removal of stone(s), and/or radiographic evidence of stone(s). Patients were classified as hypocitraturic based on the results of 24-hour urine samples indicating values of urinary citrate <320 mg/24 h (mean of two nonconsecutive samples), available from their medical records. Data concerning the presence of other metabolic abnormalities related to stone formation were also obtained from these records with normal ranges adopted as previously described. 18
Exclusion criteria were abnormal renal function (defined as estimated glomerular filtration rate <60 mL/min/1.73 m2), urinary tract infection, diabetes, cystinuria, renal tubular acidosis, inflammatory bowel disease, diarrhea, primary hyperparathyroidism, and pregnancy. To avoid any influence of diet on citrate excretion other than juice consumption, during 72 hours preceding the test, patients were placed on a diet totally devoid of fruits, vegetables, and alcohol, containing 2000 Kcal, with 60% of the energy from carbohydrates (300 g/d), 16% from protein (80 g/d) and 24% from fat (53 g/d), and up to 100 mEq of sodium and 40 mEq of potassium per day.
Patients were instructed to discontinue the use of potassium citrate, vitamin C, or thiazides during this period. Each patient was randomly assigned to an experimental group who received either freshly squeezed orange juice (orange, n=10), freshly blended cantaloupe juice plus water (melon, n=10), or a limeade preparation containing pure lime juice (freshly squeezed) plus water and sucralose as artificial sweetener (lime, n=10). The total administered volume of melon and lime juices was standardized through adding water in sufficient amounts to achieve the 385 mL (13 oz) of plain orange juice, as shown in Table 1. The composition of juices given in the table was based on the United States Department of Agriculture Nutrient Database, 19 and the citrate and malate contents were measured by ion chromatography using an ICS 2000 system equipped with an AG-11 guard column and an AS-11 analytical column in series (Dionex, Sunnyvale, CA). 20
Numbers in parentheses indicate amounts expressed as mEq/serving size.
After an overnight fast of 12 hours, the patients arrived at the laboratory on the test day at 6:00 AM, discarded the first urine specimen, and drank 300 mL of water. The first period of 2-hour urine collection (baseline), initiated on arrival at the outpatient unit, ended at 8:00 AM when the respective juice was then administered. Three 2-hour urine samples were obtained at 2 hours (08:00–10:00 AM), 4 hours (10:00–12:00 AM), and 6 hours (12:00– 02:00 PM) after the juice intake. Each urine sample was collected for analysis of creatinine, calcium, magnesium, uric acid, sodium, potassium, chloride, phosphate, citrate, ammonium, and pH.
Creatinine level was determined according to a modified Jaffe reaction by an isotope dilution mass spectrometry traceable method. Levels of calcium and magnesium were determined by a colorimetric method; uric acid by an uricase method; sodium, potassium, and chloride by ion-selective electrodes; phosphorus by a modified microcolorimetric method of Fiske and Subbarrow; and citrate by an enzymatic assay using citrate lyase, as described previously. 21 All the above parameters were measured on an Olympus Clinical Chemistry Analyzer (AU400-America Inc, Center Valley, PA). Ammonium was measured by a direct nesslerization method and potentiometric pH by a pH meter.
Net gastrointestinal alkali absorption (NGIA) was calculated from the results of urinary mineral cations (Na, K, Ca, and Mg) and anions (Cl and P) using the method described by Oh. 22 Because potential renal acid load (PRAL) provides an estimate of the production of endogenous acid that exceeds the level of alkali produced for a given amount of food ingested, its value was determined according to Remer and colleagues 23 : Positive values are indicative of acid foods while negative values represent alkaline-forming ones.
Statistical analysis
Data are presented as mean±standard deviation or area under the curve (AUC) when appropriate. Changes in urinary parameters during each period after the juice intake were compared using repeated measures analysis of variance and the Tukey test. The difference between the AUC among the three groups was compared by Kruskal-Wallis one-way analysis of variance on ranks complemented by the Dunn test. Statistical analyses were conducted using SAS System for Windows (Statistical Analysis System 8.02, SAS Institute Inc, Cary, NC). A P value less than 0.05 was regarded as statistically significant.
Results
The dietary composition of juices is given in Table 1. Melon juice contained more citrate and malate in the alkali form, resulting in higher total alkali content, and possessed a higher pH than the orange juice. On the other hand, the content of citric acid in lime juice was much higher than in the other two. The value of calculated PRAL was – 4.45 mEq/100 g in melon, −3.66 mEq/100 g in orange, and −2.44 mEq/100 g in lime.
Participants in the melon (n=10, 3M/7F), orange (n=10, 1M/9F), and lime juice (n=10, 4M/6F) groups were not statistically different regarding mean age, 47±13, 48±11, and 49±12 years and body mass index, 27.1±2.5, 26.6±4.3, and 29.2±5.8 Kg/m2, respectively (data not shown in tables). In addition to hypocitraturia, other associated baseline metabolic abnormalities were observed in melon, orange, and lime groups. Hypercalciuria was evidenced, respectively, in three, one, and two patients from each group. Hyperuricosuria was observed in only one patient from the lime group (data not shown).
There was a female preponderance in all groups. A significant increase in mean citrate excretion, as seen in Figure 1, was observed in the melon group after 4 hours vs baseline (0.35±0.15 vs 0.22±0.10 mg/mg creatinine), in the orange group after 2 hours (0.32±0.17 mg/mg creatinine), 4 hours (0.28±0.17 mg/mg creatinine), and 6 hours (0.21±0.14 mg/mg creatinine) vs baseline (0.14±0.09 mg/mg creatinine), and in the lime group after 2 hours (0.39±0.30 mg/mg creatinine) and 4 hours (0.29±0.21 mg/mg creatinine) vs baseline (0.15±0.12 mg/mg creatinine).
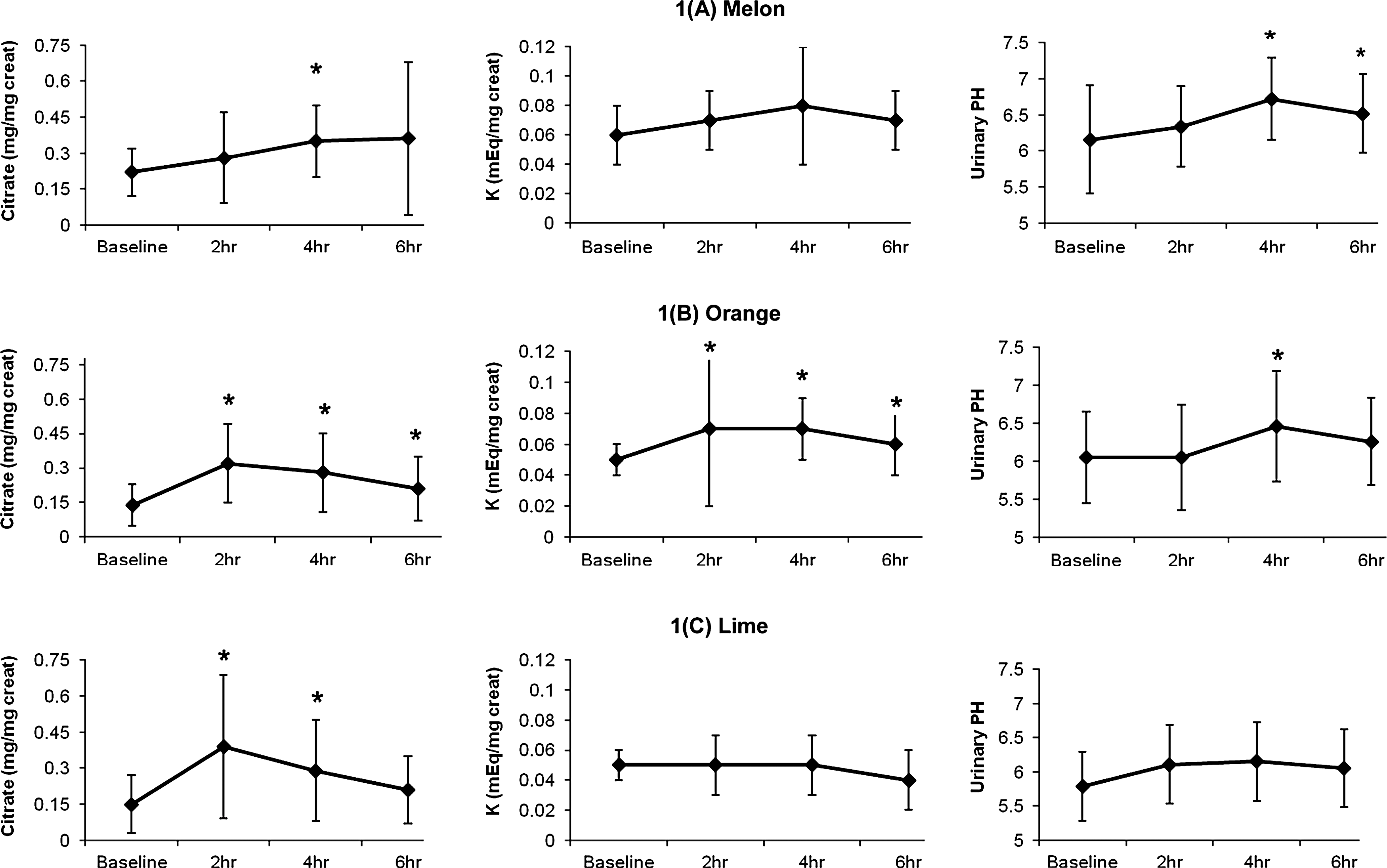
Effect of melon, orange, and lime on urinary citrate, potassium (K), and pH levels. Data are presented as mean±standard deviation. * Significant difference vs baseline. Creat=creatinine.
No significant difference in the mean AUC for urinary citrate was observed between melon, orange and lime groups (Fig. 2). In the melon group, mean urinary potassium increased after 2 hours (0.07±0.02 mEq/mg creatinine) and 4 hours (0.08±0.04 mEq/mg creatinine) vs baseline (0.06±0.02 mEq/mg creatinine), although not reaching statistical significance. Mean urinary potassium increased significantly in the orange group after 2 hours (0.07±0.04 mEq/mg creatinine), 4 hours (0.07±0.02 mEq/mg creatinine), and 6 hours (0.06±0.02 mEq/mg creatinine) vs baseline (0.05±0.01 mEq/mg creatinine). Mean potassium excretion did not differ between periods in the lime group (Fig. 1). As demonstrated in Figure 2, however, the mean AUC for urinary potassium in the melon group (0.43±0.15 mEq/mg creatinine) was not statistically different compared with the orange group (0.38±0.13 mEq/mg creatinine) whereas both were significantly higher compared with the lime group (0.29±0.01 mEq/mg creatinine).
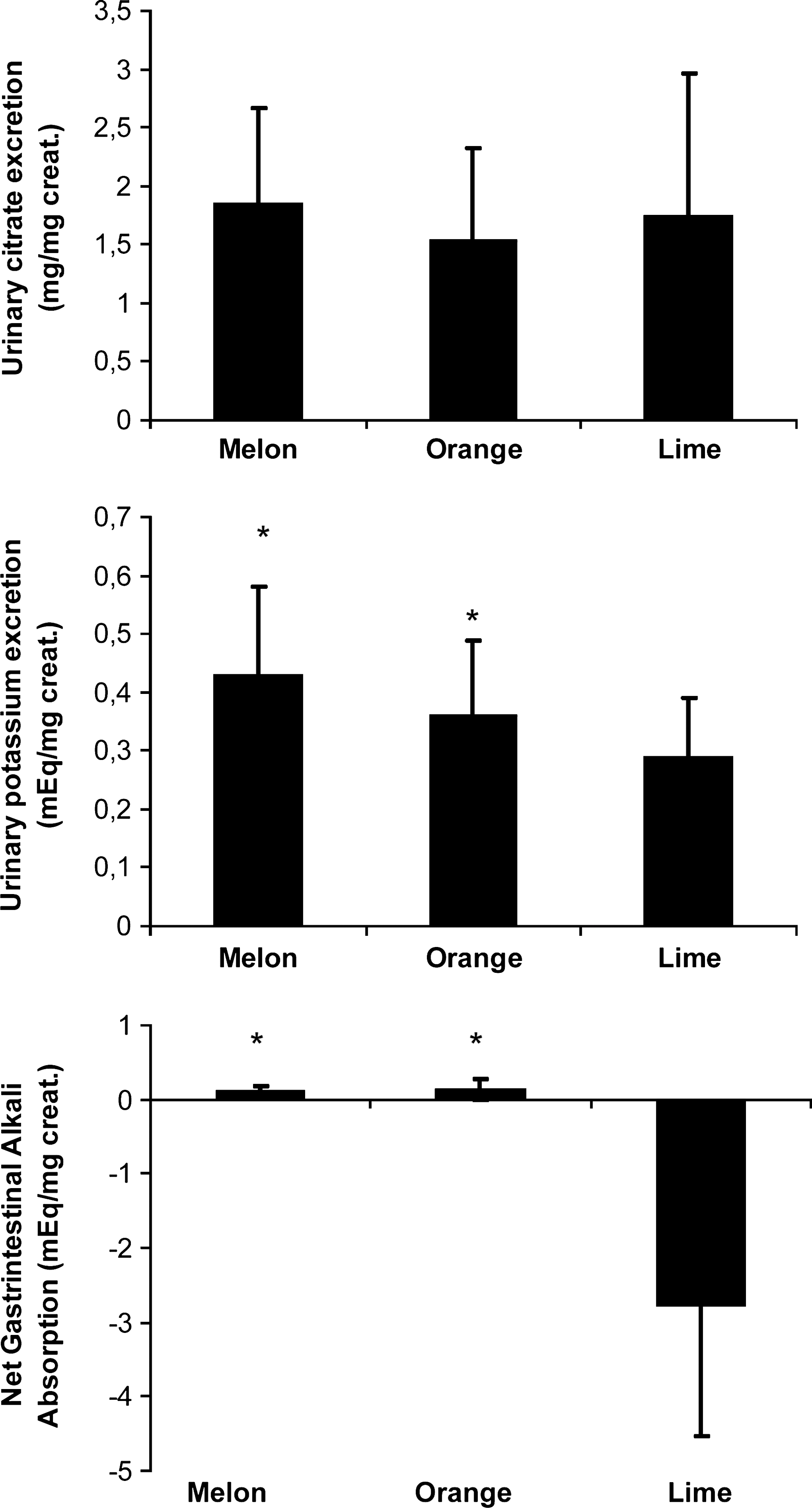
Mean area under the curve for urinary citrate, potassium, and net gastrointestinal alkali absorption in all groups. *Significant difference vs lime. Creat=creatinine.
The urinary pH was significantly higher after both melon and orange juice consumption. This increase was observed after 2 hours (6.46±0.73) compared with baseline (6.05±0.60) in the orange group and after 4 hours (6.72±0.50) and 6 hours (6.52±0.50) in the melon group when compared with baseline (6.16±0.75). No significant changes were observed for urinary pH in any period in the lime group. The AUC for NGIA was significantly higher in the melon and orange groups vs lime (0.12±0.05 mEq/creatinine and 0.14±0.14 mEq/creatinine vs −2.78±1.76 mEq/creatinine, respectively) (Fig. 2). Table 2 shows the AUC of urinary calcium, magnesium, chloride, phosphate, ammonium, uric acid, and pH, which did not differ between melon, orange and lime groups. The AUC for urinary sodium was significantly higher for orange vs lime group (0.79±0.38 mEq/mg creatinine vs 0.47±0.18 mEq/mg creatinine).
Significant differences vs lime.
Discussion
Hypocitraturia can be managed through a combination of dietary modifications, oral alkali, and possibly lemonade or other citrus juice-based therapy, which can be particularly useful for patients who either cannot tolerate or afford potassium citrate medication. 1 In calcium stone formers, higher potassium excretion has been associated with higher citrate excretion as well. 16 The benefits of the alkali content of the Dietary Approach to Stop Hypertension (DASH)-style diet (rich in fruits and vegetables) have been confirmed by a recent cross-sectional study by Taylor and associates, 24 conducted in a large cohort of 3426 persons with or without nephrolithiasis, which showed that multivariate-adjusted 24-hour urinary citrate was up to 16% greater in those exhibiting the highest quintile of DASH scores. Higher urine potassium and pH were also significantly associated with higher DASH score in all cohorts.
Modulation of citrate excretion in the kidney is influenced by multiple factors of which tubular or intracellular pH has the strongest impact through several mechanisms. 1 Lowering tubular pH increases the concentration of citrate−2 available for transport by the sodium/dicarboxylate-1 (NaDC-1) transporter and reduces the concentration of citrate−3, thereby limiting its competitive inhibition. Even small decreases in tubular pH significantly increase citrate tubular reabsorption. 1 Alkali feeding, in turn, has no effect on NaDC-1 but decreases mitochondrial citrate transport and oxidation, partly through decreasing the activity and amount of the mitochondrial enzyme aconitase, responsible for the first step in citrate metabolism within the mitochondria. 1 According to some investigators, 25 urinary potassium and NGIA were independent factors that determined urinary citrate levels in recurrent stone-forming patients, with urinary potassium being the strongest predictor of urinary citrate.
Few investigators have evaluated the effect of noncitrus fruits, rich in potassium and alkali, as a means to improve dietary management of hypocitraturia, except for Hönow and coworkers. 4 The citrate content in fruits other than the citric ones is not available in the Nutritional Composition Tables, and the use of ion chromatography, a direct analytic technique to reliably determine the citrate and malate contents of melon, enabled us to conduct the present study. The results of the present study showed that equivalent amounts of potassium provided by high citrate preparations from either a dietary noncitrus source (melon) or a well known citrus source (orange), as well as from a dietary citrus source with low potassium content (lime), induced significant increases in urinary citrate through distinct mechanisms.
Melon juice consumption induced a progressive and significant increase in urinary citrate accompanied by parallel increases in urinary potassium and pH. The peak excretion of urinary potassium, albeit not significant, occurred at the same time as a marked and significant rise in urinary pH, suggesting that the sustained increase in urinary citrate after 6 hours of melon consumption and the increased NGIA (comparable to orange) might have resulted from the increased alkali load and/or to the high potassium content provided by this fruit. Although the mechanisms by which K+ repletion and/or increased alkali load induce elevations in citrate excretion are not completely elucidated, potassium repletion is expected to inhibit the activity of H+/K+- ATPase in the α-intercalated cells from the cortical collecting duct resulting in reduction of both K+ reabsorption and H+ secretion. 26 In addition, K+ repletion may favor K+ secretion in the principal cells with a concomitant increase in Na+ reabsorption as well. 26
Thus, it can be hypothesized that the resultant increase in volume expansion will, in its turn, ultimately lead to the inhibition of both Na+ and citrate reabsorption in proximal tubular cells. The more negative PRAL value of melon (−4.45 mEq/100 g) compared with both orange and lime (−3.66 mEq/100 g and −2.44 mEq/100 g, respectively) further supports its high alkalinity. In addition, as shown in Table 1, melon juice contained more citrate in the alkali form and malate than orange juice besides possessing a higher pH. As pointed by Goodman and associates, 27 urine citrate excretion and pH depend on the amount of potential base contained in the drink, which in turn is dependent on the beverage's pH and anion concentration.
The consumption of orange juice also induced a significant increase in both urinary K+ and citrate excretion, reaching a peak after 2 hours, which was concomitant with the increase in potassium excretion. These increases were sustained and remained elevated until 6 hours compared with baseline. Its alkalinizing effect was also evidenced by a higher AUC for both urinary pH and NGIA. These findings are in agreement with data from several investigators who observed significant increases on citraturia after orange juice consumption in healthy subjects 4 –6 or in a few stone formers, 5 some of them with documented hypocitraturia. 4
Finally, we have shown that lime juice also induced an increase in urinary citrate not accompanied by significant changes in urinary pH, potassium, or NGIA. These findings agree well with many other studies that showed important increases in urinary citrate with lemonade 7 –10 without significant changes in urinary pH, but are in contrast with the data from Odvina, 5 who showed that orange juice, but not lemonade, promoted hypercitraturia because of the accompanying proton in lemon neutralizing the bicarbonate from the citrate present in lemon.
The discrepancies among the studies might have been ascribed to differences in the source of the lemon/lime used (straight lemon juice, homemade lemonade, lemonade beverage, frozen concentrate, bottled lemon juice, etc) and the resultant variable concentrations of citrate, depending on the method of preparation, when compared with the current study, where freshly squeezed lime juice has been used instead. Additional differences in outcomes among the studies can also be assigned to the different sample sizes, type of population (stone formers or not), duration of study, variability with regard to their retrospective or prospective nature. Whereas two studies were long-term, retrospective, and uncontrolled,9,10 three others were short-term metabolic studies 5,7,11 and one was an intermediate-term metabolic study. 8 In at least some of the studies, the citrate content was matched between one juice and another or with potassium citrate, which further compromises the comparisons between them. Only one study involved a controlled, metabolic diet, 5 and none of these trials has evaluated actual stone formation as a primary outcome parameter in a prospective or randomized fashion.
The present increase in citraturia after lime juice could have been a consequence of some citrate escaping in vivo metabolism, 12 because ol the large amount of citric acid present in lime. 7,28 The advantage of freshly squeezed lime juice, besides contributing to an increase in overall fluid consumption, is that it may also provide lower caloric load (19 calories) than orange (173 calories) if sweetened with artificial sweeteners, thereby minimizing increased calciuria associated with carbohydrate ingestion. In addition, we observed a significant lower sodium excretion after lime if compared with orange, as also disclosed by Odvina. 5 Finally, lime may represent a good dietary alternative for calcium phosphate formers, in whom increasing urinary pH is not warranted. 29,30 Despite the comparable and higher pH and AUC for NGIA indicating an alkali load provided by either melon or orange as opposed to lime juice, we did not detect statistical differences in AUC for urinary ammonium. It is possible that the short test period was not enough to show such changes.
Conclusion
The present study showed that melon, a noncitrus source of potassium, citrate, and malate, yielded equivalent increases in urinary citrate excretion as the ones provided by orange—hence, representing another dietary alternative for the treatment of hypocitraturic stone-formers. Despite its low potassium content, lime also produced comparable increases in citraturia from its high citric acid content. Because of the strong citraturic effects of melon, a longer term study of the beneficial effects of melon consumption (or other noncitrus alkaline fruits rich in citrate and/or malate as well) in increasing citrate excretion and decreasing stone risk in stone patients is warranted.
Footnotes
Acknowledgments
This research was supported by grants from Coordenação de Aperfeiçoamento Pessoal de Nível Superior (CAPES) and Fundação Oswaldo Ramos-Hospital do Rim e Hipertensão from Universidade Federal de São Paulo. We express our thanks to Milene Ormanji for technical assistance.
Disclosure Statement
No competing financial interests exist.