
Abstract
Background and Purpose:
Because of the impact warm ischemia time may have on renal function, various surgical techniques have been proposed to minimize or eliminate warm ischemia. The purpose of this study is to evaluate our initial renal functional outcomes of off-clamp robot-assisted partial nephrectomy (RAPN), while assessing the safety profile of this unconventional surgical approach.
Patients and Methods:
We performed a retrospective review of our off-clamp RAPN experience between August 2007 and January 2012. All patients with baseline and postoperative serum creatinine determinations were included. Patient demographics, operative information, perioperative outcomes, and renal functional outcomes were evaluated for this cohort.
Results:
Forty-two patients with a mean age of 59.9 years (standard deviation [SD]=12) had a median follow-up of 100 days (range 1–1007 days). In all cases, warm ischemia time was 0 minutes. Mean operative time was 143 minutes (SD=59), and median estimated blood loss was 138 mL (range 50–1500 mL). No intraoperative complications were encountered, and all surgical margins were negative. Our postoperative complication rate was 14.3%. At the most recent follow-up, the mean estimated glomerular filtration rate (eGFR) was 76.2 mL/min/1.73 m2 (SD=27.6), compared with 78.5 mL/min/1.73 m2 (SD=28.9) preoperatively (P=0.11). Therefore, the mean eGFR decline of 2.3 mL/min/1.73 m2 (SD=9.1) was not significant.
Conclusions:
Off-clamp RAPN is associated with minimal morbidity and minimal decline in renal function on short-term follow-up. Further studies and continued monitoring of renal function are needed to determine if off-clamp RAPN provides any advantage in renal function preservation relative to the traditional RAPN with vascular clamping.
Introduction
More recently, both laparoscopic partial nephrectomy (LPN) and robot-assisted partial nephrectomy (RAPN) have been shown to be viable alternatives to open surgery. 7,8 In spite of the increased use of these techniques, methods for achieving renal hypothermia during renal hilar clamping have yet to achieve widespread use. Thus, renal tumor excision during LPN and RAPN is typically performed under warm ischemia conditions.
Even limited warm ischemia time (WIT) may potentially damage renal parenchyma and have an adverse effect on long-term renal function. As a result, variations in surgical technique have been attempted to reduce or eliminate WIT. The purpose of our study is to evaluate renal functional outcomes of off-clamp RAPN based on the initial Washington University experience. We also assess the safety profile of this alternative surgical technique.
Patients and Methods
With Institutional Review Board approval, a retrospective chart review identified 42 patients who underwent off-clamp RAPN for suspected renal-cell carcinoma (RCC) at our institution between August 2007 and January 2012. Of these 42 off-clamp RAPN cases, 2 were performed in 2007, 5 in 2008, 5 in 2009, 5 in 2010, 20 in 2011, and 5 in January of 2012, reflecting a progressive increase in the use of the off-clamp technique in later years. All cases were performed by two minimally invasive renal surgeons with significant experience in the off-clamp technique.
Preoperative CT or MRI demonstrated contrast-enhancing renal masses suspicious for RCC in all patients. All treatment options, including surveillance, were discussed with the patients. Indications for RAPN and selection of the off-clamp technique were based on tumor size and location, patient comorbidities, and patient and surgeon preference. Of note, with increasing experience using the off-clamp technique, off-clamp PN was attempted for tumors of progressively greater complexity. Figure 1 presents preoperative images of actual cases of off-clamp RAPN performed for tumors of variable size, location, and overall degree of complexity.
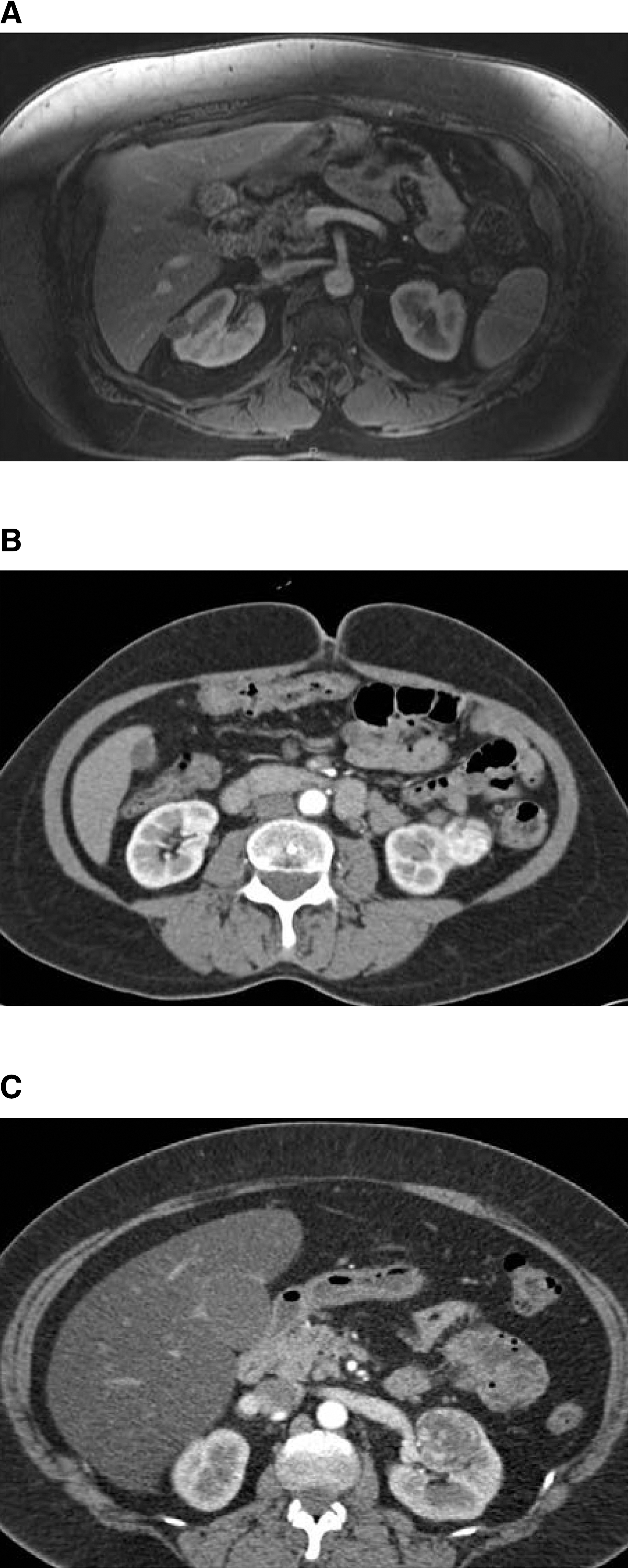
The images represent actual cases of robot-assisted partial nephrectomy performed using the off-clamp technique.
Surgical technique
A transperitoneal or retroperitoneal robotic approach was chosen based on tumor location, patient surgical history, and surgeon preference. Generally, we used a transperitoneal approach for anterior tumors and a retroperitoneal approach for posterior tumors. After dissecting out the kidney and sweeping the perinephric fat away from the tumor, the depth of the tumor was assessed, and the resection site was marked with the aid of intraoperative ultrasonography. As a precautionary measure, the renal hilum was dissected out and fully exposed to enable prompt hilar control in case of excessive bleeding during tumor excision. No hilar occlusion was performed, however.
Tumor excision was generally performed with electrocautery at 50 watts, although the Habib-4X bipolar resection device (Angio Dynamics, Queensbury, NY) was used for tumor resection in several of the initial cases. During tumor excision, bleeding vessels were controlled with monopolar or bipolar electrocautery. Meticulous electrocautery during tumor resection usually ensured adequate hemostasis. Large blood vessels that remained patent despite electrocautery were temporarily occluded with the Prograsp forceps and either clipped using Weck Hem-o-lok clips (Teleflex, Research Triangle Park, NC) or clamped with robotic bulldog clamps until tumor resection was completed. Once the tumor was excised, the resection base was inspected and judiciously cauterized to ensure hemostasis.
Then 2.0 polyglactin sutures were used for closure of the collecting system and/or large blood vessels at the resection base when indicated, with simultaneous release of any robotic bulldog clamps used during tumor resection. Reapproximation of the renal parenchyma was performed with 0 polyglactin simple mattress sutures, secured with sliding Weck Hem-o-lok clips and reinforced with Lapra-Ty clips (Ethicon, Cincinnati, OH). After renal reconstruction, hemostasis was again ensured with careful inspection of the surgical bed under low insufflation pressure. The specimen was extracted, the gross margins of the tumor were inspected, and the specimen was sent to the pathology laboratory for permanent section.
Postoperative follow-up
Serum creatinine was routinely measured 1 day, 1 month, 3 months, 6 months, and yearly after surgery.
Data collection
Patient demographics and baseline clinical characteristics, tumor characteristics, perioperative parameters, and postoperative serum creatinine levels were recorded. Determination of renal functional outcomes was based on postoperative changes in estimated glomerular filtration rate (eGFR), relative to preoperative eGFR. The Chronic Kidney Disease Epidemiology Collaboration formula was used for eGFR calculation. 9
Statistical analysis was performed using MedCalc-11.6. Preoperative eGFR was compared with the most recent eGFR using the paired t test, with P<0.05 (two-tailed) defining statistical significance.
Results
Patient demographics and comorbidities are outlined in Table 1. Forty-two patients, 26 males (61.9%) and 16 females (38.1%), with a mean age of 59.9 years (standard deviation [SD]=12) underwent off-clamp RAPN. The cohort's mean American Society of Anesthesiologists (ASA) score was 2.4 (SD=0.7); mean age-adjusted Charlson Comorbidity Index (CCI) was 2.5 (SD=1.3).
SD=standard deviation; ASA=American Society of Anesthesiologists; CCI=Charlson Comorbidity Index.
Tumor characteristics are depicted in Table 2. Forty-one patients underwent RAPN for a single renal mass, while the remaining patient had eight masses excised. The mean tumor size was 2.7 cm (SD=1.4), and mean nephrometry score 10 was 6.1 (SD=1.9). Twenty-seven (55%) of the 49 tumors resected were of lower tumor complexity (nephrometry score 4–6); 17/49 (35%) were of intermediate tumor complexity (nephrometry score 7–9); 5/49 (10%) were of higher tumor complexity (nephrometry score 10–12). Of the 49 renal tumors, 37 (75.5%) were malignant on final pathologic determination.
SD=standard deviation; RCC=renal-cell carcinoma.
Perioperative data are provided in Table 3. WIT was 0 minutes in all cases. Mean operative time was 143 minutes (SD=59). Median estimated blood loss (EBL) was 138 mL (range 50–1500), while mean EBL was 210 mL (SD=245). All surgical margins were negative. One patient had a non-ST-elevation myocardial infarction on postoperative day 3, necessitating cardiac catheterization and coronary artery stent placement (Clavien IV). Blood transfusion (Clavien II) was needed in only one patient, who underwent off-clamp RAPN for eight renal masses. Two patients experienced significant chest pain leading to a workup to rule out myocardial infarction with negative results (Clavien I). A new resting oxygen requirement developed in one patient, necessitating discharge on home oxygen after an unremarkable pulmonary evaluation (Clavien I). Another patient experienced postoperative ileus and nausea, resulting in a relatively prolonged hospital course (Clavien I).
SD=standard deviation; WIT=warm ischemia time; EBL=estimated blood loss.
Table 4 summarizes renal functional outcomes after off-clamp RAPN. Median follow-up duration was 100 days (range 1–1007 days), while mean follow-up was 235 days (SD=310). Mean preoperative eGFR was 78.5 mL/min/1.73 m2 (SD=28.9), and mean eGFR at most recent follow-up was 76.2 mL/min/1.73 m2 (SD=27.6; P=0.11). On average, this change represents a 2.9% decline in eGFR at most recent follow-up (SD=9.1).
SD=standard deviation; eGFR=estimated glomerular filtration rate; CI=confidence interval.
A subset analysis of perioperative and renal functional outcomes was performed for tumors >2 cm (31 tumors in 28 patients), tumors that were >50% endophytic (11 tumors in 10 patients), and hilar tumors (5 tumors in 4 patients) to assess the impact of increased tumor complexity on surgical outcomes. For tumors >2 cm in size, mean operative time was 160 minutes (SD=62). Median EBL was 150 mL (range 50–1500 mL), and mean EBL was 225 mL (SD=282). Mean preoperative eGFR in this subset of patients was 76.9 mL/min/1.73 m2 (SD=32.1), compared with 76.3 mL/min/1.73 m2 (SD=31.2; P=0.58) at a mean follow-up of 162 days (SD=276). For endophytic tumors, mean operative time was 168 minutes (SD=62). Median EBL was 125 mL (range 50–1500), while mean EBL was 315 mL (SD=438). Mean preoperative eGFR was 96.7 mL/min/1.73 m2 (SD=20.7) vs 95.9 mL/min/1.73 m2 (SD=15.5; P=0.75) at a mean follow-up of 197 days (SD=256). For hilar tumors, mean operative time was 204 minutes (SD=74). Median EBL was 175 mL (range 50–1500); mean EBL was 475 mL (SD=686). Mean preoperative eGFR in this group was 89.9 mL/min/1.73 m2 (SD=31.1), compared with 92.1mL/min/1.73 m2 (SD=28.5; P=0.59) at a mean follow-up of 56 days (SD=110).
Discussion
Increasing evidence highlighting the importance of renal preservation, 1 –4 in conjunction with data documenting the oncologic efficacy of PN, 11 have established PN as the standard of care for treatment of patients with small renal masses. 5 The impact of WIT on renal functional preservation after PN is still debated, however. The historical “safe” duration of WIT, after which complete recovery of renal function could be expected, was commonly considered to be 30 minutes. 12,13 Lately, however, this notion has been challenged. In view of studies demonstrating negligible effects on renal function after renal pedicle clamping for 90 minutes in porcine models 14 –16 as well as retrospective clinical observations suggesting that WIT of 40 to 55 minutes may be tolerated, 16,17 some have asserted that the kidney can tolerate longer periods of WIT. Conversely, others have contended that the cutoff defining safe WIT be drawn at 20 minutes, 18 –20 a view supported by a recent international collaborative review. 21
While efforts to define an appropriate cutoff for WIT abound, a compelling joint Cleveland Clinic/Mayo Clinic study examined the impact of WIT as a continuous variable on renal functional outcomes. In this study of 362 patients with a solitary kidney undergoing open or laparoscopic PN, longer WIT was associated with increased odds of acute renal failure as well as development of new-onset stage IV chronic kidney disease during follow-up. Thus, the authors concluded that, “every minute counts when the renal hilum is clamped without hypothermic techniques.” 22
In recognition of the potential impact that even limited WIT may have on long-term renal function, multiple variations in surgical technique aimed at minimizing or eliminating WIT have been described. Among such techniques is the “early unclamping technique,” whereby the hilar vessels are clamped only during sharp dissection of the tumor, closure of exposed vessels, and repair of collecting system defects at the resection base. 23 –25 Gill and associates 23 reported decreasing their WIT for LPN from 31.6 to 14.4 minutes using this technique. Another variation of renal hilar clamping aimed at minimizing WIT during PN is “selective renal parenchymal clamping”; with this technique, the renal parenchyma is regionally clamped only in the area of planned excision. Viprakasit and colleagues 26 described successful use of this technique in three patients undergoing RAPN. 26 We previously reported improved renal functional outcomes with segmental rather than complete hilar clamping in a porcine model 27 and demonstrated the safety and feasibility of this technique in humans. 28 More recently, some surgeons have performed PN without any clamping of the renal hilum and have suggested that off-clamp PN can be safely performed in carefully selected patients. 29,30 Gill and coworkers 30 described their technique of “zero-ischemia” PN, whereby tumor excision is performed without hilar clamping in the setting of medically induced and carefully monitored hypotension. The authors report successful use of this technique in 12 cases of LPN and three cases of RAPN. 30
In the current study, RAPN was performed without renal hilar clamping and without blood pressure manipulation. We evaluated the renal functional outcomes and safety profile of off-clamp RAPN based on our preliminary experience at Washington University. Of note, this technique represents an evolution in our efforts to minimize WIT, building on our previous experience with segmental arterial clamping. 27,28 In the short-term, a minimal and statistically insignificant decline in renal function was seen after off-clamp RAPN. The mean EBL (210 mL) and operative time (143 min) were clinically appropriate, and all surgical margins were negative for tumor. Our complication rate of 14.3% falls well within the standard of care for PN. In reference to the single patient who experienced a myocardial infarction on postoperative day 3 and needed coronary artery stent placement, we note that there were no intraoperative complications during her case; EBL was 400 mL and operative time was 199 minutes for this patient. Although possible, it seems unlikely that a traditional clamped approach would have prevented this perioperative complication.
Our only other postoperative complication with a Clavien grade >I—the need for blood transfusion for decreased hematocrit—occurred in a patient who underwent off-clamp RAPN for eight ipsilateral tumors. Minimization of WIT was especially important in his case, because the patient has von-Hippel-Lindau disease and has had multiple interventions for contralateral kidney lesions in the past. The patient's tumors ranged from 1.0 to 3.9 cm, with nephrometry scores ranging from 4 to 10. His operative time (304 minutes) and EBL (1500 mL) represent the upper bounds of our range for these parameters; he was the only patient to need blood transfusion. Seven masses were found to be Fuhrman grade III clear-cell RCC, and one mass was found to be an atypical cyst; all surgical margins were negative. The patient's postoperative course was unremarkable, and he was discharged on postoperative day 3. Notably, he has experienced a decline in eGFR of only 0.8 mL/min/1.73 m2 at 220 days of follow-up. Although an outlier, this patient demonstrates the feasibility of performing off-clamp RAPN even in complex cases involving multiple ipsilateral tumors.
Our study is limited by its retrospective design and limited follow-up duration. To capture as much data as possible, even those patients who underwent off-clamp RAPN very recently were included. Median follow-up (with range) as well as mean follow-up (with SD) are included to delineate the distribution of our follow-up data. Also noteworthy is that our study reflects surgical outcomes of two surgeons with considerable experience and training in minimally invasive renal surgery. Given the advanced level of technical expertise needed to safely and effectively perform off-clamp RAPN, the surgical outcomes of this technique may certainly differ in lower volume settings.
Another criticism of this study is the lack of strictly defined indications for off-clamp RAPN. Tumor size and location, patient comorbidities, and surgeon preference all contributed to the decision to forgo hilar occlusion. It is important to recognize that our mean tumor size of 2.7 cm and our mean nephrometry score of 6.1 reflect generally smaller and less complex tumors. As a consequence, our outcomes—especially those pertaining to intraoperative parameters—may not necessarily be applicable to larger and less accessible tumors. Indeed, the 42 cases of off-clamp RAPN performed in the time frame of this study (August 2007 to January 2012) represent carefully selected patients from a pool of more than 450 cases of RAPN performed by the same two surgeons over the same time frame.
Furthermore, our study may not have been adequately powered to detect very subtle changes in eGFR after off-clamp RAPN. Although the slight postoperative decrease in eGFR of 2.3 mL/min/1.73 m2 did not achieve statistical significance (P=0.11) based on the current sample size, a statistical trend was noted. Our relatively small sample size also limits the interpretation of complication rates and other reported perioperative data.
To better delineate the impact of the off-clamp technique on renal function as well as perioperative outcomes, a comparison of off-clamp PN with traditional clamped PN is necessary. While a randomized prospective study comparing these techniques is ideal, off-clamp PN should be performed only in carefully selected patients, especially during the initial experience with this technique. A matched cohort study comparing the outcomes of off-clamp PN and clamped PN would, therefore, be the most appropriate next step in evaluating the off-clamp technique and will certainly be the subject of future reports.
Our preliminary data on a matched cohort study comparing 29 patients who underwent off-clamp RAPN between 2008 and 2011 and 29 control patients with identical nephrometry scores and comparable baseline renal function who underwent clamped RAPN during the same period demonstrates favorable renal functional outcomes in the off-clamp group, albeit with a slightly increased (although clinically acceptable) EBL. Because we have gained more experience in performing off-clamp PN, we are currently making an effort to use this technique in almost every case. As we continue to progress further along our learning curve for this technique, a randomized prospective study comparing off-clamp and clamped RAPN may become feasible in the future.
Conclusions
Off-clamp RAPN is associated with a favorable morbidity profile and minimal loss in renal function in the short term. Further studies are needed to compare the renal functional outcomes of off-clamp RAPN with those of the traditional clamped RAPN to assess the relative efficacy of the off-clamp technique in preserving renal function.
Footnotes
Disclosure Statement
No competing financial interests exist.