
Abstract
Background and Purpose:
Partial nephrectomy (PN) can be technically challenging, especially if performed in a minimally invasive manner. Although ultrasound technology has been shown to have therapeutic capabilities, including tissue ablation and hemostasis, it has not gained clinical use in the PN setting. The purpose of this study is to evaluate the ability of a high-intensity ultrasound clamp to create an ablation plane in the kidney providing hemostasis that could potentially aid in laparoscopic PN.
Methods:
A new instrument was created using a laparoscopic Padron endoscopic exposing retractor. Ultrasound elements were engineered on both sides of the retractor to administer high-intensity ultrasound energy between the two sides of the clamp. This high-intensity focused ultrasound (HIFU) clamp was placed 2 to 2.5 cm from the upper and lower poles of 10 porcine kidneys to evaluate its effectiveness at different levels and duration of energy delivery. PN transection was performed through the distal portion of the clamped margin. Kidneys postintervention and after PN were evaluated and blood loss estimated by weighing gauze placed at the defect. Histologic analysis was performed with hematoxylin and eosin and nicotinamide adenine dinucleotide staining to evaluate for tissue viability and thermal spread.
Results:
Gross parenchymal changes were seen with obvious demarcation between treated and untreated tissue. Increased ultrasound exposure time (10 vs 5 and 2 min), even at lower power settings, was more effective in causing destruction and necrosis of tissue. Transmural ablation was achieved in three of four renal units after 10 minutes of exposure with significantly less blood loss (<2 g vs 30–100 g). Nonviable tissue was confirmed histologically. There was minimal thermal spread outside the clamped margin (1.2–3.2 mm).
Conclusion:
In this preliminary porcine evaluation, a novel HIFU clamp induced hemostasis and created an ablation plane in the kidney. This technology could serve as a useful adjunct to laparoscopic PN in the future and potentially obviate the need for renal hilar clamping.
Introduction
PN can be technically challenging, especially if performed in a minimally invasive manner, and complication rates are not insignificant. 6 –8 Techniques to facilitate minimally invasive PN have been reported to try to reduce renal ischemia time by facilitating the excision and reconstruction. 9 –12 Prolonged renal ischemia during PN is known to affect postoperative renal function. 13,14 “Off-clamp” PN is an option, but decreased visualization from blood loss while excising the mass may compromise oncologic results, although this was not seen in an expert series in terms of margin status. 15 More recently, other methods to induce selective renal ischemia have been described, such as segmental renal artery clamping and the use of a parenchymal clamp, which avoid global renal ischemia. 16 –19
It is believed that not all patients with an incidentally found small renal mass need surgical excision. Active surveillance has emerged as an option for small renal masses in select patient populations. 20 Other patients who may not be ideal candidates for excisional therapy may consider an “intermediate” option, such as renal ablative treatment with cryoablation or radiofrequency ablation (RFA). In addition, ultrasound technology has moved beyond being just a diagnostic tool to having therapeutic capabilities and has been used for tissue ablation, treatment of solid tumors, and hemostasis. 21
High-intensity focused ultrasound (HIFU) has theoretical benefits over cryoablation and RFA because it is administered without the need to place a probe into the tumor directly. Unfortunately, the initial HIFU reports have shown suboptimal results for the treatment of renal tumors. 22 Potentially, while not serving as the treatment for renal tumors, HIFU may help facilitate the excision of the renal tumor through its hemostatic properties. 23
The purpose of this article is to introduce a high-intensity ultrasound parenchymal clamp that does not ablate the tumor but achieves hemostasis by developing a plane of cauterization. This effect could potentially aid nephron-sparing surgery, most notably laparoscopic PN.
Methods
A novel HIFU instrument was created by mounting custom ultrasound transducers on the opposing arms of a laparoscopic PEER retractor (Fig. 1). The transducer array was mounted on both arms of the retractor to administer high-intensity ultrasound energy between the two sides of the clamp, thus creating a plane of cauterization. The transducers were made from eight rectangular 2 MHz piezoceramic crystals (APC International Ltd, Mackeyville, PA) with a plastic housing and a 0.45 mm thick graphite matching layer. Each individual crystal is 10 mm×5 mm×1 mm. A 0.005 mm thick brass shim is sandwiched between the crystals and the graphite layer with epoxy for bonding purposes. Electrical matching networks made of LC-circuits were constructed to perform the impedance match for both the main circuit and each individual branch circuit of the transducers at 50 ohms.
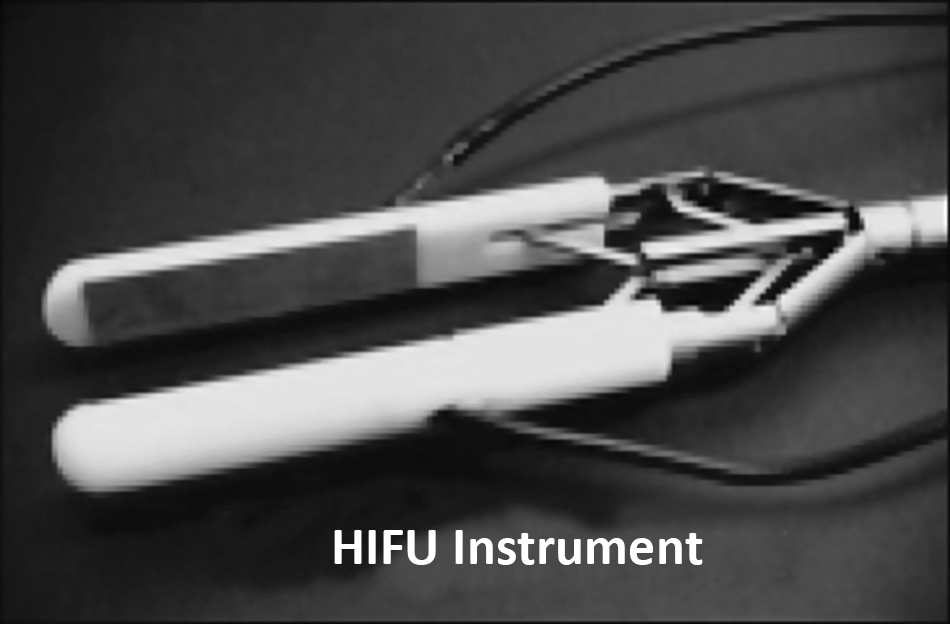
High-intensity focused ultrasound (HIFU) instrument.
All procedures were conducted in accordance with the guidelines of the National Institutes of Health for use of laboratory animals. The experimental protocol was approved by the University of Washington Institute of Animal Care and Use Committee. Kidneys from common domestic swine were used in nonsurvival studies to assess effectiveness of the device for achieving a plane of cauterization in a perfused kidney. The kidneys were exposed with an open surgical technique. The renal Gerota's fascia was entered and the abdominal cavity was filled with degassed phosphate buffered saline (PBS) at physiologic temperature. Degassed PBS was primarily used to provide coupling for the ultrasound and secondarily to provide cooling for the ultrasound transducers.
The transducers were used in a pulsed wave regime such that various acoustic protocols could be systematically evaluated without overheating the passively cooled transducers. The passive cooling limited the acoustic protocols to high power, short burst lengths and short treatment times or low power, moderate burst lengths, and longer treatment times. As such, the burst lengths ranged between 20 and 100 ms, duty factors ranging from 10% to 50%, and acoustic powers ranging from 20 W to 50 W per transducer. Treatment times ranged between 1 and 10 minutes, resulting in acoustic energies delivered between 2000 and 9000 joules.
The HIFU clamp was placed 2 to 2.5 cm from the upper and lower poles of 10 live porcine kidneys. In this feasibility study, various levels and duration of energy delivery, mentioned above, were used to evaluate the clamp's effectiveness. There was also a control or sham arm in which the clamp was applied to the kidney without administration of HIFU. After all treatments (HIFU or sham), the clamp was removed and tissue grossly inspected.
Cold knife transection of renal tissue (PN) was performed. The line of excision was made through the distal aspect of the gross lesion on the polar side. Hemostasis was evaluated and observed. Gauze was placed at the transection defect to collect blood for 1 minute and later weighed to estimate blood loss. In this feasibility study, when bleeding was significant and there was obvious incomplete ablation, compression and hemostatic renorrhaphy was initiated before 1 minute to avoid significantly higher unnecessary bleeding. All kidneys were procured and immediately sectioned for gross and histologic analysis. Histology was performed with hematoxylin and eosin and nicotinamide adenine dinucleotide NADH staining to evaluate for tissue viability and thermal spread.
Results
Ten porcine kidneys underwent either HIFU treatment or were used as a sham control. There was unilateral device malfunction in four attempts of ultrasound administration. This was the result of transducer failure secondary to elements decoupling from the housing and water getting into the electronics. Renal units with device malfunction were excluded from PN.
Gross renal parenchymal changes were seen with obvious demarcation between treated and untreated tissue (Fig. 2). Increased ultrasound exposure time (10 vs 5 and 2 min) was more effective in creating ablative lesions and necrosis of tissue. Complete ablation planes were created in three of four renal units after 10 minutes of HIFU-clamp treatment. Blood loss in these three with complete ablation was minimal without any need for hemostatic maneuvers, and weighted gauze estimated blood loss was less than 2 g. Kidneys that underwent 1, 2, or 5 minutes of ultrasound exposure all had incomplete ablation. The blood loss within the first minute after transection in these kidneys as well as the sham controls was significantly higher, estimated at 30 to 100 g. In some with incomplete ablation or sham controls, however, 1 minute blood loss is underestimated, because manual compression took place after initial evaluation, to oversew arterial bleeding, as mentioned in the Methods section.

Kidney in-situ immediately following removal of HIFU clamp.
Histologic findings corresponded to hemostatic properties seen after transection. Complete transmural lesions were seen in three of four kidneys after 10 minutes of treatment time (Fig. 3). In comparison, skip lesions were seen in renal units that were subjected to fewer than 10 minutes of ultrasound clamp exposure time. There was no difference in tissue thickness between those with complete or incomplete ablation. Renal parenchymal thickness before clamping was estimated between 30 and 40 mm. After clamping, there was compression of the tissue of approximately 10 to 15 mm, and tissue thickness ranged between 18 and 28 mm. Those with complete ablation had postclamping thickness ranging from 20 to 25 mm. Histochemical staining confirmed nonviability of treated tissue compared with adjacent viability tissue (Figs. 4 and 5). Mean tissue damage from thermal spread was 2.02 mm±0.93 (range 1.19–3.22 mm), seen histologically.
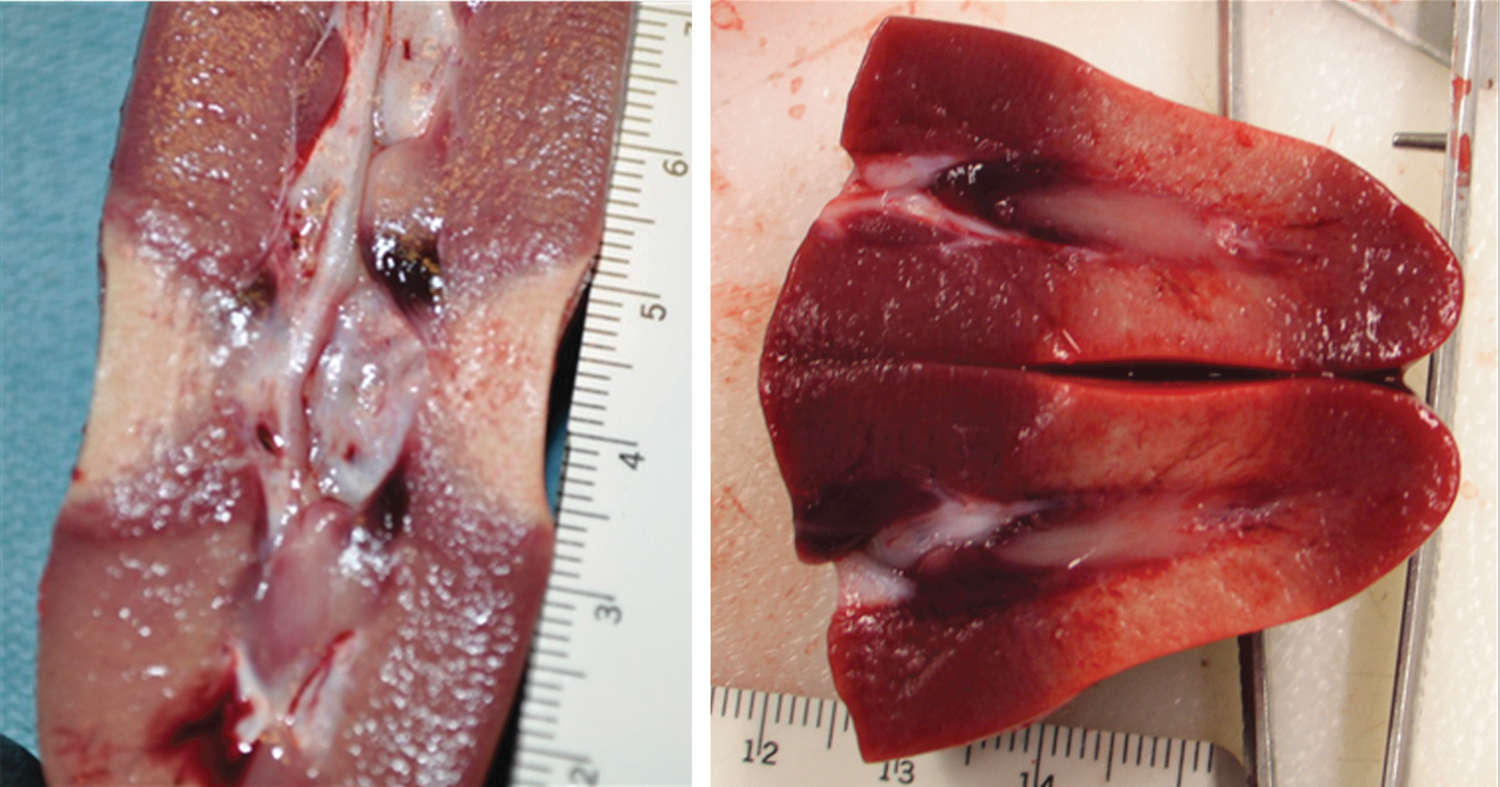
Sectioned kidney after high-intensity focused ultrasound clamp administration.
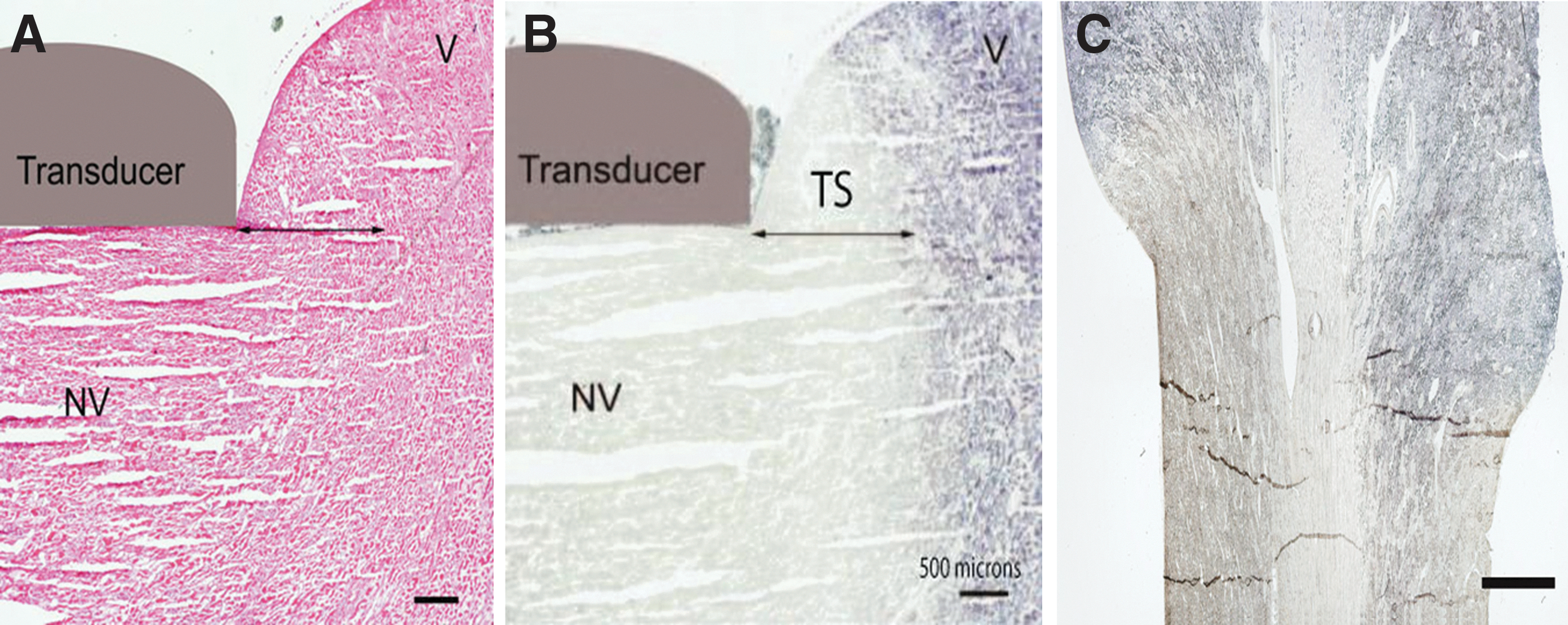
Histologic images after

Serial kidney sections taken from control (top) and ablated (bottom) tissue stained NADH nicotinamide adenine dinucleotide-d for viability (right) and hematoxylin and eosin (left). The images show magnified images of the renal cortex. Control tissue (top) displays normal histology and stains blue/purple with the viability stain, indicating viable tissue. Sections taken from the ablated regions (bottom), display subtle changes including vacuoles within the tissue and a generally more desiccated appearance. Although the renal lobules and corpuscles are relatively intact, they do not show completely normal structure and are more eosinophilic compared with the control sections. The lack of viability stain demonstrates that tissue in this area is not viable. Scale bar represents 200 μm.
Discussion
Incidentally found small renal masses are being identified at a growing rate. 1 With this increased detection, a greater number of patients are confronted with the options for treatment vs surveillance. Although many of these masses are found in patients in whom symptoms may never develop or who may never have adverse sequelae, the thought of untreated cancer often provokes anxiety. PN is the gold standard when feasible in masses less than 4 cm, although ablative treatments and active surveillance are options for selected patients. There has been heightened awareness of the correlation of chronic kidney disease and increased cardiovascular events and death over the last several years. 2,3,24 As a result, nephron-sparing surgery is advocated whenever possible, including candidate masses greater than 4 cm. 7,24,25 With PN, renal artery clamping is frequently performed, resulting in global renal ischemia. It has been shown that longer warm renal ischemia times correlate with decreased postoperative renal function. 13,14 Therefore, PN techniques have been described that use selective renal ischemia or no ischemia. 26
Given the benefits of nephron-sparing surgery and complexity of PN, renal ablative options were developed to manage small renal masses. An alternative ablative modality to RFA and cryoablation is HIFU. HIFU has been described for ablation of many solid tumors including prostate, liver, pancreas, uterine, and kidney. 21 HIFU has been applied laparoscopically and extracorporeally for treatment of renal masses with a theroretical benefit of not having to puncture the tumor to achieve ablation. Initial evaluation of extracorporeal HIFU for renal ablation showed poor results. 27,28 A more contemporary report of extracorporeal HIFU demonstrated improved outcomes compared with early analyses, yet only two-thirds of patients had stable lesions after treatment. 29 Laparoscopic HIFU was shown to be feasible in a phase 1 study that potentially overcame the limitations of the extracorporeal approach. 30
We describe a novel HIFU clamp that harnesses the hemostatic properties of ultrasound energy. The current version incorporates ultrasound elements on both sides of the clamp. Our original design was based on linear acoustic modeling with the assumption that transducers on one side of the clamp and a reflector on the other would suffice. Several transducer versions were created with this configuration with suboptimal results. We then changed the design and placed transducers on both arms of the clamp with significant improvements in hemostatic properties. From there, we began systematically varying the parameters such that we could achieve complete ablation.
We believe that this device will facilitate PN by providing a bloodless field during excision while avoiding hilar clamping, and may avoid the need for reconstruction of the renal defect. Although optimal duration and magnitude of energy delivery have not yet been defined, this device was able to achieve complete transmural lesions with 10 minutes of exposure in the porcine model with minimal thermal spread.
It is recognized that when compared with other PN techniques, especially an enucleation, use of this clamp would result in excision of a wider margin of normal tissue. It has been reported, however, that there may be underutilization of PN nationwide for small renal masses. 31 Because the alternative for many patients may be a radical nephrectomy, PN with a wider margin would still offer benefits, in our opinion. The underutilization of PN is presumably secondary to the complexity of cutting into a well-vascularized organ during this operation. If our device could aid in hemostasis and lessen the stress of the excision and reconstructive aspects of PN, perhaps more patients would receive the beneficial outcomes of nephron-sparing surgery.
Our HIFU instrument is a prototype and therefore has many limitations that preclude it from being optimized for clinical use. The shape is not ideal: More force is applied at the “jaw,” and this required manual pressure distally for an even distribution of force. There are currently renal parenchymal clamps that have a more optimal design for this reason. Similar to currently available parenchymal clamps, the linear design is best suited for polar lesions, although selected lateral tumors can be treated as well. In the future, we anticipate a pliable clamp that would allow greater versatility. We also need to optimize the energy delivery parameters, although progress in this area was made during this study. There have been no survival studies to evaluate effects on the collecting system, because this was an initial feasibility study. It will be important in future studies to address this question. We envision having a control arm to evaluate changes after HIFU alone in addition to a PN arm to evaluate the risks of urine leak.
Additional research is under way to gain greater understanding of the capabilities afforded by this technology, as well as to develop a more optimal clamp design. We would like to develop this technology further before these next studies will be done and think that further research in this area is worth pursuing.
Conclusion
In this preliminary porcine evaluation, a novel HIFU clamp induced hemostasis and created an ablation plane in the kidney. This technology could serve as a useful adjunct to laparoscopic PN in the future and potentially obviate the need for renal hilar clamping.
Footnotes
Acknowledgment
This work was supported by NSBRI through NASA NCC 9-58 and NIH 1R01GM77318.
Disclosure Statement
No competing financial interests exist.