
Abstract
Purpose:
To compare the dynamics of systemic inflammatory indices during laparoscopic nephrectomy (LN) and standard open donor nephrectomy.
Patients and Methods:
Participants in this cohort study were 54 adults without a history of renal surgery and no evidence of urinary tract infection who underwent transperitoneal LN (n=29) and open donor nephrectomy (n=25, control group). We recorded demographic characteristics, intraoperative parameters, and changes 24 hours postoperatively in systemic inflammatory and immunologic values (body temperature, concentrations of white blood cell count [WBC], C-reactive protein [CRP], interleukin [IL]-6, and tumor necrosis factor [TNF]-α), and compared the mean changes between groups.
Results:
Mean age was older in the LN group (45.6 vs 30.9 years; P<0.0001), and mean operative time was significantly shorter (83.1 min vs 101.6 min; P=0.004). Mean postoperative increase in IL-6 and body temperature in LN was significantly less than in control: For IL-6, 15.87 vs 29.09 pg/mL, P=0.03; for body temperature, +0.22°C vs +0.71°C, P=0.001). Mean postoperative increases in levels of other inflammatory markers (CRP, TNF-α, WBC) did not differ significantly. No statistical correlation was found between operative time and changes in IL-6, CRP, TNF-α, WBC, or body temperature.
Conclusion:
Based on the smaller increase in serum IL-6 as the most important indicator of surgical stress, the surgical trauma-induced immune dysfunction may be less intense after LN than open surgery. This may explain the smooth convalescence after LN.
Introduction
Despite the enthusiasm for LN, little is known about the exact pathophysiologic mechanisms of these observations, and the end points of almost all previous clinical comparative studies have been based on subjective parameters. Surgical trauma and its associated tissue injury induce various immunologic alternations in the patient. Both humoral and cell-mediated immunity are believed to be evoked during the perioperative period and are proportional to the extent of surgical injury. The greater the immune response to surgical injury, the greater the expected postoperative immunosuppression and its resultant postoperative morbidity and mortality. 3 This may especially have a great impact on the recurrence rate and survival in cancer patients.
Laparoscopic surgery, because of its minimally invasive nature, is thought to induce weaker systemic immune responses. The likely mechanisms are the minimal manipulation of organs as well as smaller surgical incisions. Furthermore, CO2 pneumoperitoneum, in contrast to exposing the viscera to air, directly reduces the systemic stress response by suppressing the activation of peritoneal macrophages, polymorphonuclear migration, chemotaxis, and free radical production. 3 –6 Despite previous extensive experimental and clinical studies on the immunologic effect of laparoscopy in the general surgery and gynecology literature, to our knowledge, few clinical studies have been designed to address the immunologic responses to LN.
Traditionally, ON has been performed retroperitoneally. LN at many centers, such as ours, is performed transperitoneally, however. 1,7,8 Although the morbidity and outcome of transperitoneal laparoscopy vs retroperitoneoscopic nephrectomy have been shown to be similar, 1,7,8 concerns remain that peritoneal manipulation during transperitoneal LN (TP-LN) may affect postoperative morbidity.
In this prospective study, we compared the systemic stress response in patients who underwent TP-LN and in candidates for standard open donor nephrectomy as a control group to objectively measure postoperative morbidity. No subjective postoperative parameter was assessed in this trial, and we specifically focused on immunologic markers of interleukin (IL)-6, as the main determining indicator of surgical trauma, 9,10 tumor necrosis factor (TNF)-α, which is involved in both humoral and cell mediated immunity, 3,10 and C-reactive protein (CRP) as an important acute phase reactant produced by liver.
Patients and Methods
Ethics
Approval from our Institutional Review Board was obtained, as was written informed consent from all patients. The advantages and risks of the laparoscopic approach with the possible need for open conversion were explained before the operation.
Patients
Between May 2009 and December 2010, we enrolled 29 patients who needed LN and 25 candidates for ON in the study.
Inclusion criteria in the laparoscopy group were symptomatic nonfunctioning small or hydronephrotic kidneys because of ischemic nephropathy, renovascular hypertension, or chronic obstructive uropathy. The exclusion criteria were any type of malignancy, evidence of pyelonephritis, positive results of urinalysis or urine culture, renal insufficiency, diabetes, autoimmune disorder, liver disease, any systemic inflammatory or rheumatologic disorder, and recent use of nonsteroidal anti-inflammatory drugs or corticosteroids. Patients who needed intraoperative or postoperative blood transfusion and those whose procedure should be converted to open nephrectomy were also excluded.
All procedures were performed under general anesthesia using a similar protocol. All LN procedures were performed by the same surgeon (AA) using a transperitoneal approach. A 10-mm camera port was placed in the umbilicus, and two 5-mm ports together with a 10-mm port were used as working ports. The specimen was retrieved via the site of the 10-mm port. All ON procedures were performed by the same surgeon (MS) with a classic flank retroperitoneal approach through a 12- to 15-cm incision.
Outcome measures
From all patients, we obtained a 5-mL peripheral venous blood sample before anesthesia was induced and a second sample 24 hours after surgery. The samples were analyzed with quantitative enzyme linked immunoassays (Bender Med Systems, GmbH, Austria) for IL-6, TNF-α, and CRP. The kits were read by Elisys Uno (HUMAN Diagnostics Worldwide, GmbH, Wiesbaden, Germany) device. In addition, the white blood cell count (WBC) and hemoglobin (Hb) concentration were recorded with an automated hematology analyzer. Body temperature was recorded preoperatively and 24 hours postoperatively.
Statistical analysis
The Student t test was used to compare quantitative demographic data between the two groups. Postoperative–preoperative differences in inflammatory and immunologic values were recorded for each patient, and the mean values of these changes in each group were compared and analyzed with the Mann-Whitney test. Correlations between parameters were tested by calculating the Spearman correlation coefficient. SPSS® version 15.0 software was used for all data analyses.
Results
A total of 54 patients were enrolled in the study: 29 (53.7%) of them (15 men, 51.7%) underwent LN for nonfunctioning kidneys, and as a control group, 25 (46.3%) persons (14 men, 56%) underwent ON.
Each group was sex-matched, but mean age was older in the laparoscopy group (45.6 vs 30.9 years, P<0.0001). There were no open conversions in the laparoscopy group, and no intraoperative and postoperative complications (including the need for blood transfusion) in any of the patients in either group. Mean operative time calculated from the insertion of the first trocar (or skin incision in ON) was significantly shorter in the LN group (83.1 min vs 101.6 min, P=0.004). Mean Hb decreases after the operation were similar in the laparoscopic vs open group (−1.15 vs −1.52 g/dL, P=0.7).
Table 1 and Figure 1 summarize the changes with time in the inflammatory and immunologic markers in the two groups. Briefly, mean preoperative inflammatory and immunologic markers (IL-6, CRP, TNF-α, WBC, and body temperature) were similar in both groups (Table 1, Fig. 1). There was a trend toward an increase in all inflammatory and immunologic markers 24 hours after the operation. The mean postoperative increase in IL-6 and body temperature in the LN group was significantly less than in the ON group: For IL-6, 15.87 vs 29.09 pg/mL, P=0.03; for body temperature, +0.22°C vs +0.71°C, P=0.001. The mean postoperative increases in other inflammatory markers (CRP, TNF-α, and WBC) did not differ significantly between the groups (Table 1, Fig. 1). No statistical correlation was found between operative time and changes in IL-6, CRP, TNF-α, WBC, or body temperature.
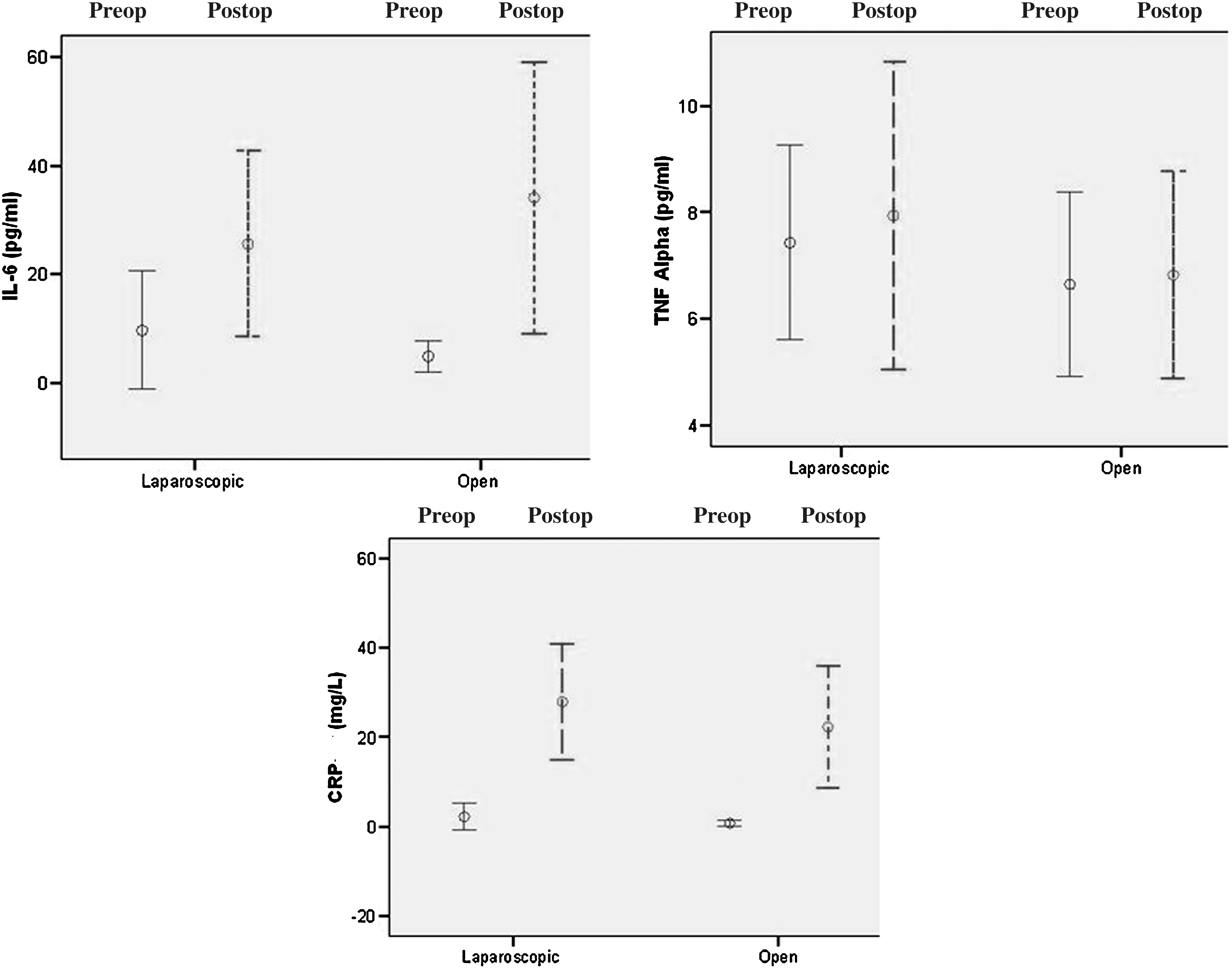
Postoperative (postop) changes in immunologic markers (interleukin [IL]-6, tumor necrosis factor [TNF]-α, and C-reactive protein [CRP]) in the laparoscopic vs open nephrectomy groups. Preop=preoperative.
The difference between postop and preop values (ΔPostop-Preop) for each marker was analyzed.
LN=laparoscopic nephrectomy; ON=Open nephrectomy; preop=preoperative; postop=postoperative; IL=interleukin; CRP=C-reactive protein; TNF=tumor necrosis factor; WBC=white blood cell count.
Discussion
In the era of minimally invasive surgery, LN has become popular at many institutions as a standard procedure. Numerous studies based on subjective parameters, such as postoperative pain severity and duration, the need for postoperative analgesics, and the duration of hospital stay and convalescence, have concluded that LN is superior to ON. 1,2 Although TP-LN is considered a minimally invasive procedure, concerns about peritoneal invasion led us to use objective parameters to compare this technique with classic open retroperitoneal nephrectomy in terms of surgical trauma and the burden on the immune system. To our knowledge, this is the first prospective comparative clinical study to address this issue in candidates for simple nephrectomy.
During TP-LN, dissection of the retroperitoneal area is performed after entering the peritoneal space. This is a somewhat different approach from classic ON, in which dissection is confined to the retroperitoneal space. Therefore, although TP-LN appears to be a less morbid procedure than ON on the basis of subjective factors, it is important to use objective measures to investigate the immune response during and after TP-LN in comparison with open techniques.
The immune response to surgery is a complex cascade involving numerous mediators and immune cells. Among them, IL-6 is the most important indicator of surgical trauma. 9,10 Serum IL-6 levels rise in the early postoperative period, and these levels are a more sensitive indicator of tissue damage than procedural time. 9 –11 Furthermore, IL-6 stimulates the angiogenic pathways and vascular endothelial growth factor production, which plays a crucial role in tumor growth, recurrence, and metastasis. 12 Therefore, preservation of angiogenic mechanisms may confer more oncologic control in patients undergoing laparoscopic surgery for cancer. This potential advantage has been shown in colon cancer surgery. 12
TNF-α, another potent mediator of the host response, induces the production of IL-6, which in turn attenuates TNF-α activity through a feedback mechanisms. CRP is also a well-known acute phase reactant that is produced in the liver during tissue injury and peaks about 24 to 72 hours after injury (Fig. 2). 10

The immunologic pathways involving interleukin (IL)-6, tumor necrosis factor (TNF)-α, and C-reactive protein (CRP) after surgical trauma.
The beneficial immunomodulatory effects of CO2 pneumoperitoneum, as well as preservation of body heat during surgery and minimization of abdominal incisions in laparoscopic surgery, are well known. Ure and colleagues 6 reported a greater reduction in the peritoneal and systemic inflammatory responses after laparoscopy than after laparotomy, and after CO2 vs air pneumoperitoneum in an experimental model. Lee and associates, 13 in a similar experimental model, found that postoperative immune preservation was directly related to incision size. CO2 pneumoperitoneum suppresses peritoneal macrophages, the initiators of the inflammatory response in surgery, and this in turn suppresses the migration, chemotaxis, and free radical production of polymorphonuclear cells. 5 Despite conflicting results with different assays and surgical procedures, many studies in the previous two decades in the general surgery and gynecology literature have suggested that laparoscopy compares favorably with open techniques in reducing the systemic inflammatory response after surgery. Table 2 summarizes the results of some studies that analyzed the same cytokines as in our study. 14 –19
Only the results for IL-6, CRP, and TNF-α are shown.
↓A lesser increase in laparoscopy compared with laparotomy.
↔Similar increase in laparoscopy compared with laparotomy.
IL=interleukin; CRP=C-reactive protein; TNF=tumor necrosis factor; NE=not evaluated.
A few studies in the urology literature have addressed the immunologic aspects of laparoscopy. Miyake and coworkers 20 reported a lower increase in the levels of IL-6, IL-10, and granulocytic elastase after laparoscopic urology procedures compared with open techniques. Their study was limited by its retrospective nature, relatively small sample size, and the inclusion of different operative procedures that were analyzed together.
In contrast, Landman and associates 21 prospectively compared the systemic stress response after laparoscopic (n=14) vs open (n=10) radical nephrectomy in patients with localized renal-cell carcinoma. They recorded cortisol, norepinephrine, epinephrine, IL-2, 4, TNF-α, and markers of cell-mediated immunity, such as CD3, 4, 8, 9, and 14, and found no overall differences between laparoscopy vs open approaches. They concluded that the effect of the tumor tissue on host immunity or the longer mean operative time associated with LN may have masked any potential differences. Similarly, Greco and colleagues 22 compared the surgical stress after laparoendoscopic single-site surgery radical nephrectomy with conventional laparoscopic radical nephrectomy. Using IL-6, IL-10, CRP, and serum amyloid A antibody, they found no significant differences in terms of surgical trauma between the two procedures.
In the present prospective cohort study, we found that LN elicited a less robust immunologic response than ON in view of the lower increase in serum IL-6, the main determinant of surgical trauma and an important predictor of postoperative complications. 10,11 Because IL-6 is one of the most important contributing factors in fever, the lower increase in this cytokine may have resulted in a lower postoperative rise in body temperature in our LN patients. These findings are consistent with many earlier studies in the fields of general surgery and gynecology. 14 –19
We found no significant difference between LN and ON with regard to the surgery-associated rise in TNF-α, CRP, and WBC. Matsumoto and coworkers 23 compared the cytokine response of LN, hand-assisted nephrectomy, and ON in a model study in pigs. Smaller increases in the level of serum TNF-α and peritoneal IL-6 were found with the laparoscopic approach compared with hand-assisted and open techniques. The systemic increases in IL-6 and IL-1, however, were similar in all three groups.
Like others, Burgos and associates 24 reported a smaller increase in IL-levels in an experimental trial of LN in pigs. Sáenz and colleagues, 25 however, found that the increases in TNF-α, endothelin-1, and CRP were smaller, whereas serum IL levels were higher after LN in pigs. Because T-helper 1 cells play a major role in TNF-α production, 10,11,23 it seems that these cells are activated to a similar degree in both ON and LN.
As with previous series, 15,26 we found no significant correlation between leukocyte count and the increased synthesis of acute-phase reactant molecules. A finding that remains unexplained is the similar increase in CRP after LN and ON.
Our prospective trial has elucidated that the subjectively smooth convalescence after transperitoneal LN compared with retroperitoneal ON, established previously, 1,2 may be related to the lesser degree of immunologic activation in the former technique. As found with laparoscopic procedures involving other organs, not all of the immunologic parameters seem to be preserved after LN, but IL-6, the most important one, was significantly preserved.
Some limitations of our study, however, deserve mention. The patients enrolled in the laparoscopy arm were those who had a “diseased” kidney, whereas our control group consisted of candidates for donor nephrectomy (ie, “healthy” kidneys). The reason is that the first choice for nephrectomy in our urology department is the laparoscopic approach, but laparoscopic donor nephrectomy was not performed frequently in our transplantation unit during the study period. We think, however, that if we had enrolled persons who underwent laparoscopic donor nephrectomy instead of simple LN, the results would have been similar. Also, the two groups were not age-matched. We prospectively enrolled the otherwise healthy and with low surgical risk patients, but we found that those in the ON group were younger. This should be considered during data interpretations.
Furthermore, the measured markers throughout this trial are not enough to evaluate all the different types of immune responses such as cell-mediated immune response and delayed type hypersensivity reaction. These responses are particularly important in host defense mechanisms against perioperative infections with intracellular organisms, tumor implantation, and growth. 3,10
Conclusion
As found by earlier studies in general surgery and gynecology, laparoscopic transperitoneal nephrectomy leads to a less pronounced increase in the level of serum IL-6 compared with classic ON, which may explain the lesser interference of LN with the immune system. This relatively weaker immune system activation may translate as a more rapid functional recovery. The potential clinical applications of these findings, including for postoperative pharmacologic immunomodulation, have yet to be studied.
Footnotes
Acknowledgments
This research was supported by the Shiraz University of Medical Sciences and was extracted from the No. 2232 dissertation. We thank the Moadel Pathobiologic Laboratory for assisting in the analysis of specimens, Dr. W.A. Farhat for his valuable comments, and K. Shashok (AuthorAID in the Eastern Mediterranean) for improving the use of English in the manuscript.
Disclosure Statement
No competing financial interests exist.