
Abstract
Purpose:
To report our operative experience and short-term outcomes for the laparoendoscopic single-site (LESS) management of large renal tumors and tumors of advanced stage.
Patients and Methods:
Ten consecutive patients underwent LESS-radical nephrectomy (RN) for large (≥7 cm) and/or locally advanced tumors (>T2). Intraoperative, postoperative, and short-term follow-up data were analyzed.
Results:
Median surgical time was 146 minutes (range 73–164 min), and median estimated blood loss was 100 mL (range 25–400 mL). No procedure needed conversion to open RN or hand-assisted laparoscopic RN. The median hospital stay was 47 hours (range 42 hours–12 days). One (10%) patient had a minor complication (postoperative fever treated with antibiotics) and one (10%) patient had a major complication (small bowel obstruction necessitating reoperation). Of the 10 tumors, 2 were pathologic stage T1b, 4 were pathologic stage T2, and 4 were stage T3a. At a median follow-up of 12.3 months (range 1–16 mos), six (60%) patients were alive without evidence of recurrence, and 4 (40%) patients were alive with disease. Of those four patients, all four had known metastatic disease before surgery.
Conclusion:
LESS-RN for large or advanced stage renal masses is a technically challenging operation. In experienced hands, however, it is a safe and feasible therapeutic option for the management of these tumors.
Introduction
The advantages of laparoscopy over open surgical approaches are well known. Intraoperative blood loss, length of hospital stay, analgesic requirements, and time of convalescence have all been shown to be decreased for laparoscopic surgery without sacrificing oncologic efficacy. 8 For these reasons, many surgeons prefer LRN over open radical nephrectomy (RN) for renal masses ≤7 cm. In a published series from our institution, we demonstrated that in the hands of experienced laparoscopic surgeons, these benefits can be extended to the management of larger, locally advanced tumors, T2 and greater. 9
Laparoendoscopic single-site (LESS) surgery represents a potential improvement on traditional laparoscopic surgery. It is performed through a single small skin incision, which is partially concealed at the umbilicus. In addition to cosmetic advantages, patients may experience less postoperative pain, shorter convalescence, and fewer port-site related complications. Since the first single port transumbilical nephrectomy was described in 2008, there have been many published series of LESS nephrectomy for benign conditions as well as malignant disease. In the current series, we present our experience with large and/or advanced stage tumors that were managed with a LESS approach.
The goal of this study is to apply the potential benefits of the LESS approach to large renal masses. We have demonstrated in the past that laparoscopic nephrectomy for large renal masses is feasible and that increased size is not a contraindication to using a minimally invasive technique. Here we intend to examine the applicability of LESS-RN in a case series of larger and/or higher stage renal masses. Defining the limits for which this new technique is appropriate or practical is important for establishing its role within the scope of surgical management of renal tumors. If the procedure can be shown to be safe and effective, then we propose to extend the benefits of the LESS approach to this patient population.
Patients and Methods
Patients
Ten consecutive patients underwent LESS-RN by one surgeon (JD) between October 2010 and July 2011 for larger and/or higher stage renal masses. All tumors were ≥7 cm in greatest dimension or stage >pT2 and had a pathologic diagnosis of RCC. Axial and coronal CT images of a 7 cm left renal mass are shown (Figs. 1 and 2). There were seven men and three women, six with left-sided tumors and four with right-sided tumors. The median age of the patients was 53.7 years with a median American Society of Anesthesiologists score of 2 and a mean body mass index (BMI) of 25.0 kg/m2. Four patients had known metastatic disease before surgery and underwent cytoreductive nephrectomy. There were no traditional LRNs performed at our institution during this time. Other than undergoing surgery during this period, there were no identifiable selection criteria for LESS-RN vs LRN.

Axial CT image: 7 cm left renal mass.

Coronal CT image: 7 cm left renal mass.
LESS technique
All patients undergo bowel preparation with a clear liquid diet and a bottle of magnesium citrate 1 day before surgery. Perioperative antibiotics are infused in the operating room, and general anesthesia with endotracheal intubation is used in all cases. The single access GelPOINT device (Applied Medical, Rancho Santa Margarita, CA) is used for all cases. Left LESS nephrectomy is performed with three trocars inserted through the GelPOINT device. Right LESS nephrectomy uses a fourth trocar to allow placement of a liver retractor.
The patient is placed in the flank position with adequate padding for the brachial plexus and the dependent hip, knees, and ankles. The lower leg is flexed while the upper leg is gently extended and a pillow placed between them. The operating table is gently flexed to optimize exposure of the flank. A 5-cm vertical periumbilical incision is made with the abdominal skin on stretch. After creating a vertical midline anterior rectus fasciotomy, the abdomen is entered. The GelPOINT device is inserted into the abdomen and pneumoperitoneum established at 15 mm Hg. For left LESS nephrectomy, two 10-mm trocars and one 15-mm trocar are inserted into the device before skin incision. The distance between the two 10-mm trocars is approximately 7.5 cm. The 15-mm trocar is inserted equidistant between (and 2.5 cm below) the two 10-mm trocars. A bariatric 10-mm rigid laparoscope is used through the 15-mm port with a right angle attachment for the light cord to maximize space for triangulation (Fig. 3). Standard nonarticulating laparoscopic instruments are used for the procedure, including the Harmonic ultrasonic scalpel (Ethicon, Somerville, NJ).
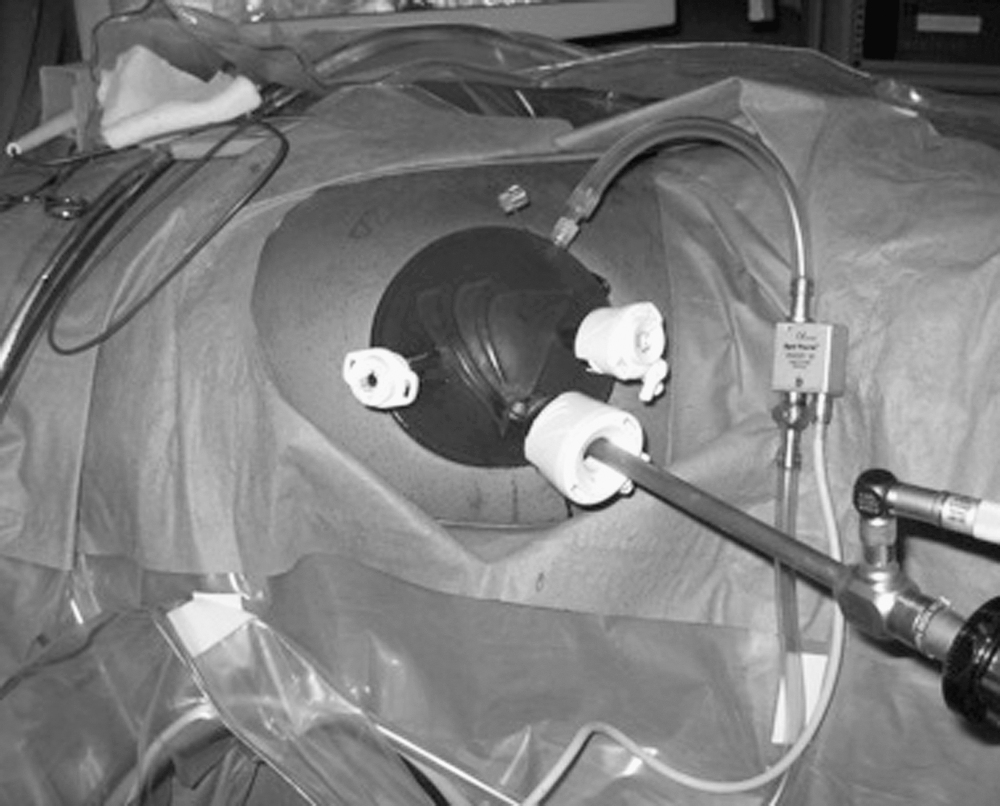
Port placement for left-sided laparoendoscopic single-site radical nephrectomy.
The LESS-RN surgical technique essentially duplicates standard LRN. In left-sided LESS nephrectomy, the descending colon, pancreas, and spleen are mobilized generously without the need for continuous retraction. The ureter and gonadal vein are identified and lifted off the psoas muscle together, maintaining periureteral attachments. This packet is mobilized distally and then dissected toward the renal hilum. The renal vein is skeletonized and the adrenal vein is identified. In certain cases, the adrenal gland is preserved. In these instances, the adrenal vein is divided between clips, and the adrenal gland is released from the upper pole of the kidney. Otherwise, the adrenal gland is removed en bloc with the kidney.
Next, the renal artery is dissected down to its origin and the interaortocaval region is skeletonized. Lastly, the kidney is dissected from its posterior attachments. The right 10-mm trocar is exchanged for a 12-mm trocar in anticipation of using the vascular staplers. Next, the ureter and gonadal vein are divided at the level of the pelvic brim using an Endo-GIA vascular stapler (Covidien, Norwalk, CT). The renal artery is then divided using the vascular stapling device. Next, the renal vein is dissected free of surrounding tissues and divided, again using the vascular stapling device.
A large Endo Catch bag (Covidien, Norwalk, CT) is introduced through the 15mm port. The kidney and adrenal gland along with Gerota's fascia are placed inside the laparoscopic specimen bag and delivered via the umbilical incision by removing the gel cap. If needed, the fascial incision is extended 1 to 2 cm to facilitate specimen removal. Extension of the skin incision was generally not necessary (in a single case, the skin incision was extended by 1.5 cm to allow removal of the specimen). The gel cap is then replaced, and pneumoperitoneum is reestablished at 10 mm Hg and the operative field inspected. The operative field is then again inspected at a pressure of 5mm Hg. After ensuring adequate hemostasis, the GelPOINT device is removed and the fascia and skin closed in standard fashion.
For right-sided LESS nephrectomy, a fourth trocar (5 mm) is placed through the GelPOINT device (Fig. 4). The right colon and hepatic flexure are medially mobilized, and the right lobe of the liver is released from the body wall. A liver retractor is placed through the fourth port to provide adequate exposure. The coronary ligament is incised to expose the upper pole of the kidney, the upper border of the adrenal gland, and the inferior vena cava. The inferior phrenic vessels are divided with a Harmonic scalpel, and the adrenal vein is controlled with clips and divided. The duodenum is mobilized medially with the Kocher maneuver for exposure of the renal hilum. The renal hilum is then dissected for identification of the renal artery and vein. Once the renal artery and vein are sufficiently dissected, the ureter is divided. Then, the renal artery and the renal vein are divided using the Endo-GIA vascular stapler, leaving the gonadal vein intact, when possible. The adrenal gland is also preserved when possible and clinically indicated. Otherwise, the remaining attachments of the kidney and adrenal are then dissected from surrounding tissues with the Harmonic scalpel. The specimen is then placed in a large Endo Catch bag and removed.

Port placement for right-sided laparoendoscopic single-site radical nephrectomy.
Results
Intraoperative data
The median total operating room time was 207 minutes (range 128–295 min), and the median surgical time was 145 minutes (range 73–164 min). The median surgical time for left-sided nephrectomy was 142 minutes (range 102–163 min) and 149 minutes (range 73–164 min) for right-sided nephrectomy. The median estimated blood loss (EBL) was 100 mL (range 25–400 mL). The median EBL for left-sided nephrectomy was 75 mL (range 50–400 mL) and 125 mL (range 25–400 mL) for right-sided nephrectomy. There were no intraoperative complications. There were no conversions to open nephrectomy or hand-assisted laparoscopic nephrectomy. No extraumbilical ports were needed in any of the cases (Table 1).
EBL=estimated blood loss.
Postoperative data
In the postoperative period, there was one major complication (bowel obstruction necessitating reoperation) and one minor complication (fever treated with antibiotics). These were classified according to the modified Clavien system 10 and are described further below. The median hospital stay was 47 hours (range 42 hours–12 days). Aside from the 12-day hospitalization for the patient who needed reoperation, the length of stay ranged from 42 to 74 hours. The median intravenous narcotic requirement (morphine sulfate or calculated equivalent) was 4.7 mg (range 0–37.3 mg). The median oral narcotic requirement (oxycodone or calculated equivalent) was 25 mg (range 0–130 mg). The median time to initiation of regular diet, as determined by passage of flatus, was 33 hours (range 24–67 hours, excluding the patient with bowel obstruction).
Pathology
There was a pathologic diagnosis of clear-cell RCC for all 10 patients. One patient had clear-cell RCC with sarcomatoid features. The median Fuhrman nuclear grade of the tumors was 3 (range 2–4). In terms of staging, two were pathologic stage T1b. Of note, both of these tumors were 7.0 cm in greatest dimension. Four tumors were pathologic stage T2, ranging in size from 8.0 to 8.5 cm. Four tumors were pathologic stage T3a. Of the four T3a tumors, two had perinephric fat invasion, one had tumor extension into the renal vein, and one tumor demonstrated both perinephric fat invasion and renal vein invasion. One tumor demonstrated lymphatic invasion. All surgical margins were negative. Four patients had removal of suspicious lymphatic tissue (one node in three patients, two nodes in one patient). These had all negative results for metastasis (Table 1).
Complications
One patient (10%) had a minor complication. He developed a fever postoperatively that was treated at an outside hospital with antibiotics (Clavien grade II). Blood cultures and urine cultures had negative results. Another patient (10%) had a major complication. He had a small bowel obstruction, which was thought to be from an internal hernia. This necessitated an exploratory laparotomy and closure of the hernia defect (Clavien grade IIIb).
Follow-up
At a median follow-up of 12.3 months (range 1–16 mos), six patients (60%) showed no evidence of disease recurrence. Four patients (40%), who had known metastases before cytoreductive nephrectomy, were alive with disease.
Discussion
Since the first laparoscopic nephrectomy was described in 1991 by Clayman and associates, 11 the prevalence of this procedure has expanded considerably. The operative time for the initial procedure was 7 hours. The patient needed a blood transfusion and a 6-day hospital stay. Nine years later, the same group published their experience on 61 patients who underwent LRN for tumors up to 10 cm, demonstrating decreased intraoperative blood loss, diminished pain medication requirement postoperatively, shorter hospital stay, and more rapid return to normal activity. 12 Subsequently, numerous studies have demonstrated the benefit of laparoscopy over open nephrectomy for lesions not amenable to partial nephrectomy. These have compared the postoperative and short-term outcomes of laparoscopic nephrectomy with the traditional open approach, as well as longer term equivalence in cancer control. 1,4,5,8,13 –15
Several publications have also addressed the feasibility of the laparoscopic approach for large renal tumors, when compared with the open approach. 9,16,17 Most recently, the single-site approach has been gaining acceptance as a viable alternative to traditional laparoscopy both for donor nephrectomy as well as for RN. 4,18,19 Here, we suggest that the LESS approach is a reasonable surgical option for management of larger or higher stage renal tumors, as well as for cytoreductive purposes, as has been proposed by others. 20 –23
Steinberg and coworkers 13 compared surgical outcomes for RN among four groups: Laparoscopic nephrectomy for T1 lesions, laparoscopic nephrectomy for T2 lesions, open nephrectomy for T1 lesions, and open nephrectomy for T2 lesions. In comparing the two laparoscopic groups, their data showed no significant difference in number of operative complications, number of postoperative complications, rate of conversion to open surgery, narcotic requirements, length of hospital stay, or time to return to normal activity. The only statistically significant difference between the two laparoscopic groups was blood loss (200 mL for the T2 group vs 100 mL for the T1 group), which the authors describe as clinically negligible. This study also demonstrated the benefits of laparoscopic nephrectomy over open nephrectomy for larger tumors. The laparoscopic T2 group had significantly shorter operative time, less blood loss, decreased analgesic requirements, shorter hospital stay, and a more rapid convalescence in comparison with the open T2 group.
In a series of 41 open, 18 hand-assisted, and 15 pure laparoscopic nephrectomies, Shuford and colleagues 17 demonstrated that LRN has an acceptably low complication rate and compares favorably with open RN in this regard. The low rate of complications combined with the advantages of decreased pain and length of hospital stay favor a laparoscopic approach for the majority of patients with stage T1 and T2 tumors.
Malaeb and coworkers 8 showed similar advantages for hand-assisted laparoscopic nephrectomy over the open approach for T2 renal masses. In this series, 9 hand-assisted laparoscopic nephrectomies were compared with 10 open nephrectomies. The hand-assisted laparoscopy group had statistically significant advantages in terms of EBL, operative time, length of hospital stay, analgesic requirement, and time to regular diet. Hemal and associates 1 also demonstrated advantages for laparoscopic nephrectomy over open nephrectomy with similar findings to the above studies, although the laparoscopic group had significantly longer operative time. In addition, these patients were followed for more than 4 years, on average, and the long-term outcomes were compared. The 5-year overall, recurrence-free, and cancer-specific survival were similar for the two groups. 1
Most recently, Berger and colleagues 14 compared perioperative data for a series of LRNs. The large tumor group (≥7 cm, 40 patients) had significantly greater blood loss, longer operative time, and a trend toward a greater increase in postoperative creatinine than those patients in the small tumor group (<7 cm, 124 patients). All other perioperative measures were not significantly different. Furthermore, at a mean follow-up time of 22 months, only one recurrence developed in the large tumor group compared with no recurrences in the smaller tumor group.
Recently, the laparoscopic approach has evolved to incorporate a single-site access technique, either via a natural orifice or through a small single abdominal or flank incision. 24,25 Evaluation of the LESS approach for various renal procedures has been encouraging. With appropriate training, several authors have demonstrated equivalent results to those of conventional laparoscopy, with the added cosmetic benefits and possibly decreased time to convalescence. 18 –20,24 –26 We have previously published our results using LESS on kidney donors, supporting our confidence in this approach. 27,28 Furthermore, two groups have recently shown equivalent 29 or improved 30 perioperative outcomes for LESS-RN compared with LRN, albeit with smaller tumor sizes than in the current study.
In the current series, we report on our experience with 10 high stage and/or large renal masses managed by LESS-RN. The median surgical time was 145 minutes, and the mean EBL was 100 mL. The median hospital stay was 47 hours. No intraoperative complications occurred. One minor postoperative complication and one major postoperative complication occurred. It is difficult to interpret the complication rate in our series, however, because of the small number of patients. That being said, the occurrence of a single major postoperative complication is consistent with the incidence of major complications in LRN. In a large meta-analysis of laparoscopic renal surgery complications, Pareek and coworkers 31 report a rate of 10.7% for major complications in LRN. Although our particular major complication (intestinal herniation necessitating reoperation) is rare, it has been described after traditional laparoscopic nephrectomy. 32 Further, our practice was to close any recognized mesenteric defects with ligating clips. Taking into account the above factors, we do not think that this occurrence was related to the LESS technique itself.
Other studies have investigated the effect of tumor size on the oncologic efficacy of laparoscopic nephrectomy. 1 –3,7,33 The short-term oncologic outcome demonstrated in this article is consistent with previous findings, both for laparoscopic and open series. This supports the notion that recurrence of RCC is dependent on the stage of the disease at the time of resection, and not the surgical approach used to extirpate the lesion. 34 Still, many surgeons have reservations about the use of minimally invasive techniques for the removal of large renal masses. These include technical issues such as decreased visibility and limited working space as well as oncologic concerns such as the possibility of tumor seeding, increased blood loss from the vascularity of larger lesions, and the risk of an incomplete resection. Furthermore, the LESS approach demonstrates restricted mobility because of the proximity of instruments, diminished triangulation, and challenges with exposure.
We recognize those concerns as well as several limitations in this study. The most notable of these limitations is that our study is a retrospective, single-surgeon study with small patient numbers and a short median follow-up of 12.3 months. A larger, prospective, randomized study would enable us to draw more meaningful conclusions about the relative benefits of LESS surgery for management of larger renal masses. Longer follow-up would allow us to more accurately determine whether LESS-RN has the same long-term oncologic benefit as LRN or open RN. Furthermore, we do not provide a definition of “experience” with regard to LESS-RN. Although we have shown a decrease in operative time within the first 50 cases for LESS donor nephrectomy, 35 it is unclear if this can be extrapolated to LESS-RN. Despite these limitations, we have elected to report on these patients to emphasize the practicability of the LESS operative approach for advanced renal tumors. Our goal was to provide data on the safety and feasibility of this operation.
Conclusions
LESS-RN for large and/or locally advanced tumors is a technically challenging operation. For experienced surgeons who are familiar with the LESS approach, however, it is a reasonable therapeutic option for the management of these masses. Patients seem to experience similar perioperative benefits to those undergoing LRN. Nevertheless, further follow-up is necessary to determine if the surgical approach (or rather the biology of individual tumors) best determines the chances of cure.
Footnotes
Disclosure Statement
Dr. Del Pizzo is a lecturer for Applied Medical. For the remaining authors, no competing financial interests exist.