
Abstract
We present a technique of transurethral transvesical endoscopic management of an intraperitoneal retrovesical hydatid cyst. Cystoscopy is performed using a 20.8F nephroscope. The cyst is punctured using an 18-gauge, 36-cm needle through the nephroscope operating channel. Saline (20%) is used as scolicidal agent. After balloon tract dilation, the nephroscope is introduced into the cyst, and the hydatid material is evacuated.
Introduction
Technique
Under spinal anesthesia, the patient is placed in the lithotomy position. Cystoscopy is performed using a 20.8F nephroscope (Richard Wolf Medical Instruments Corp, Knittlingen, Germany). The cyst is found protruding behind the bladder-trigone. An 18-gauge, 36-cm needle is passed through the nephroscope operating channel, and the cyst is punctured (Fig. 1). A clear hydatid fluid is aspirated. Contrast media is injected to ensure that the needle is within the cyst (Fig. 2). Then, 20% saline is used as a scolicidal agent during 10 minutes. A guidewire is coiled into the cyst under fluoroscopic guidance, and the tract is dilated using an 18F dilation balloon. Then the nephroscope is introduced into the cyst (Fig. 3). The suction tube is adapted to the nephroscope operating channel. The hydatid material is progressively evacuated using the vacuum technique 5 by aspiration through the working channel of the nephroscope. After total evacuation and meticulous exploration, the cystic cavity is once again filled, this time with a 3% hydrogen peroxide scolicidal solution during 5 minutes. A 14F Foley catheter is advanced into the cystic cavity over the guidewire, and an 18F three-way Foley catheter is inserted into the bladder.
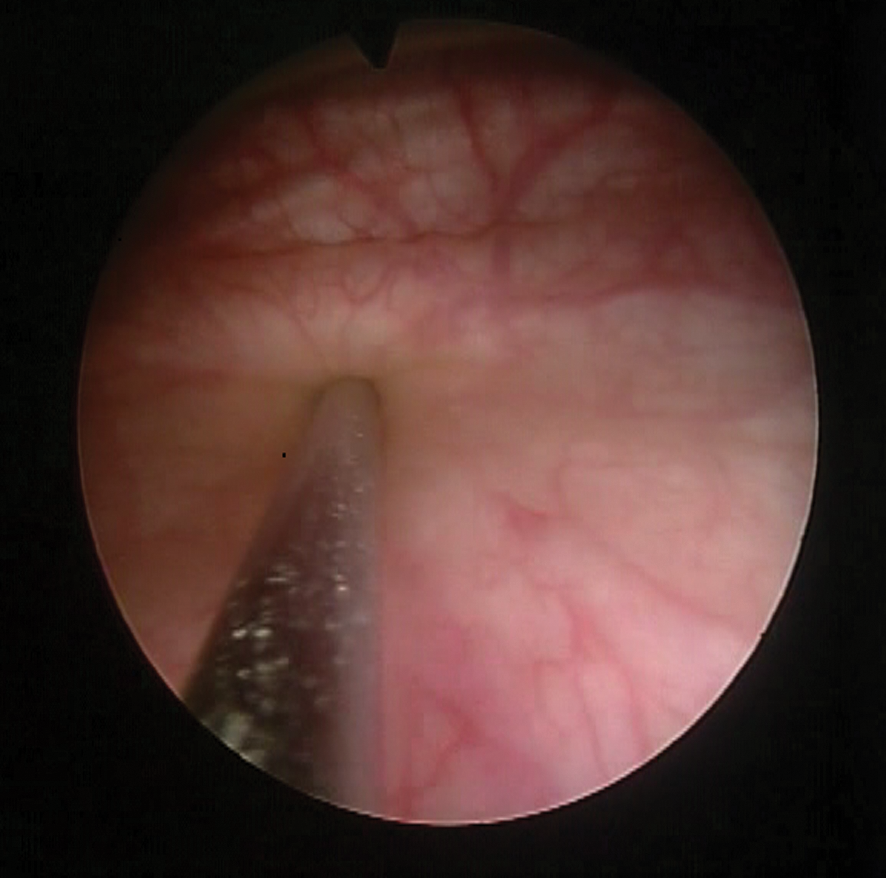
The cyst was punctured with an 18-gauge 36-cm needle passed through the nephroscope operating channel.
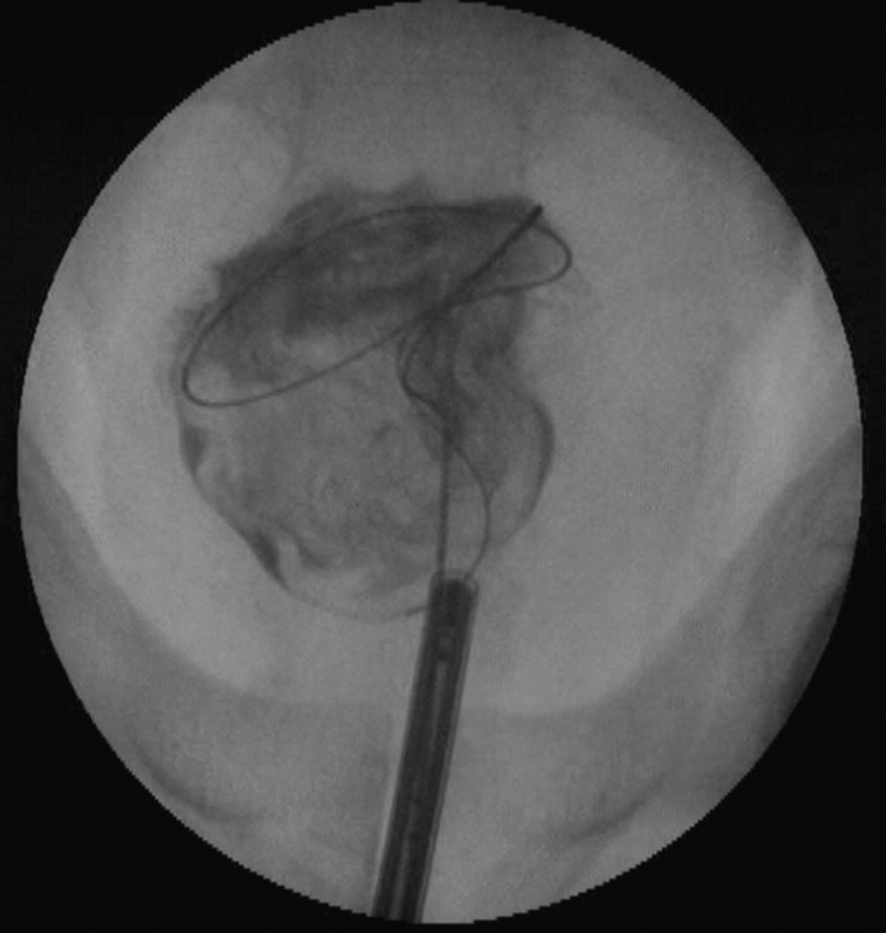
The cyst was filled with contrast media and a scolicidal agent; then a guidewire was inserted.

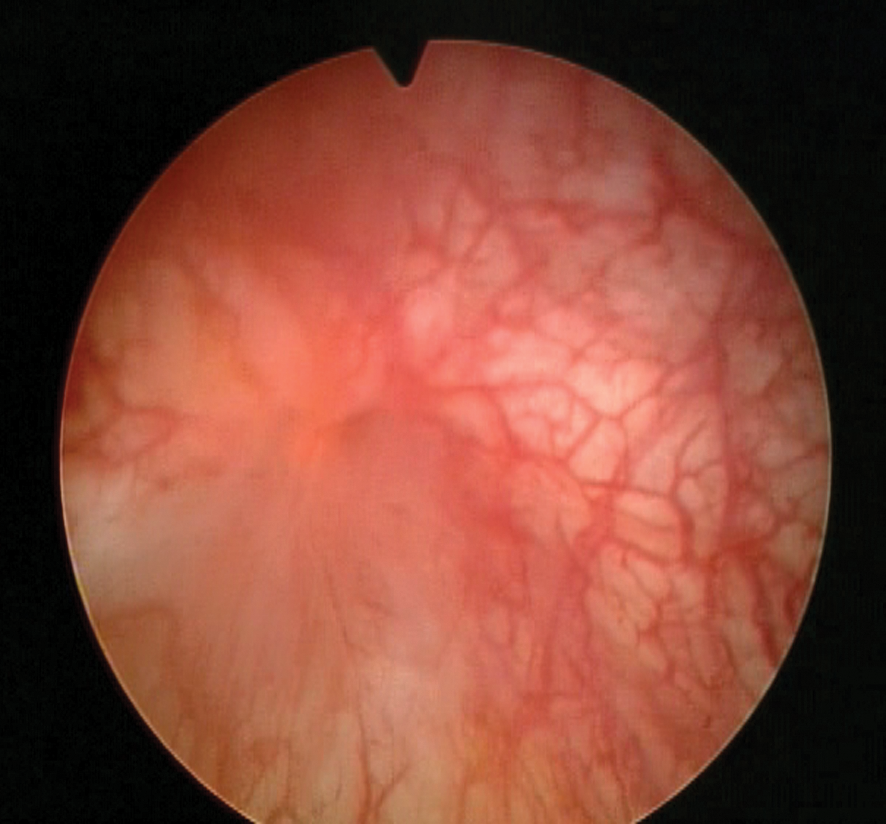
Exploration of the cyst. The germinal layer of the hydatid cyst and the daughter cysts had a yellow translucent texture, not the usual white-nacreous texture, which might be a sign of albendazole therapy efficacy.
Role in Urologic Practice
This technique was performed in a 57-year-old man with a history of a hepatic hydatid cyst who was treated 7 years ago by open surgery. He was referred to our department for an intraperitoneal retrovesical hydatid cyst that was diagnosed by ultrasonography; he had mild irritative voiding symptoms. Pelvic ultrasonography had shown a 7-cm multilocular retrovesical cystic mass, confirmed by CT scan (Fig. 4). The hydatid serology test had positive results. The patient had signed a consent form after the procedure was thoroughly explained. He had received 400 mg twice daily of albendazole chemotherapy during the 3 months before the operation.
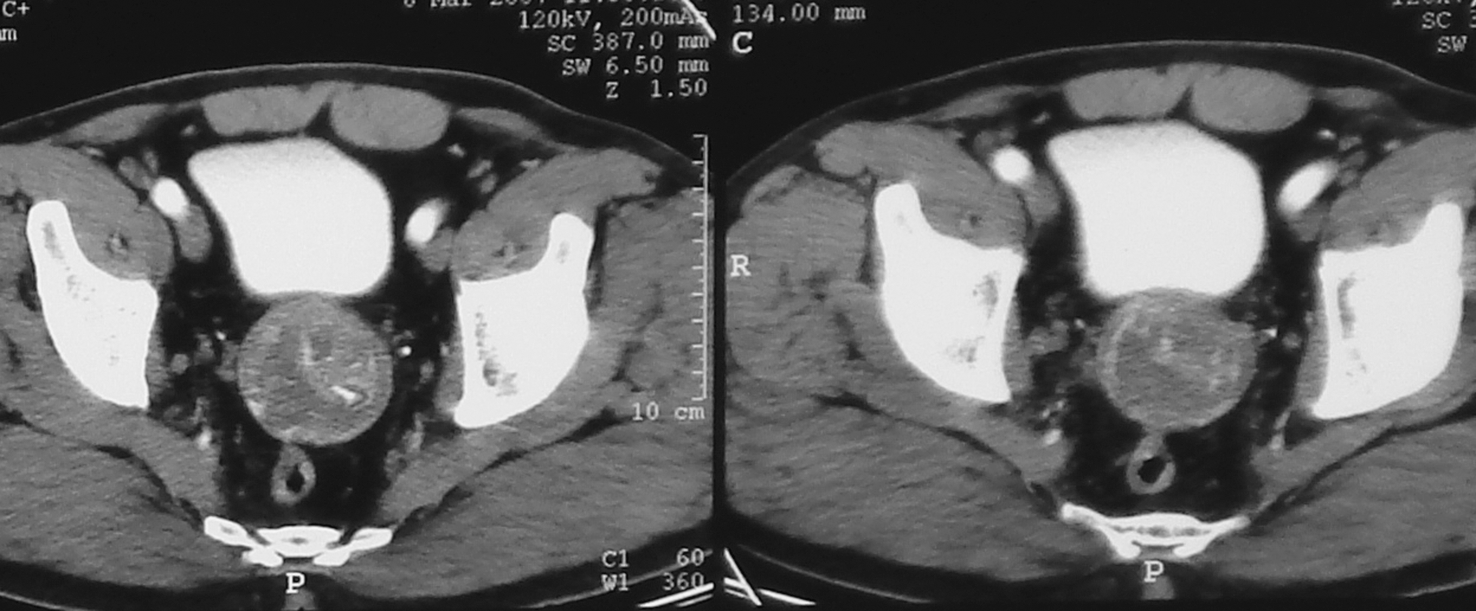
Preoperative CT scan showing a 7-cm intraperitoneal multilocular retrovesical cystic mass with calcifications.
Operative time was 40 minutes. The postoperative period was uneventful; the patient did not need any pain medication. From postoperative day 1 to 5, the cystic cavity was filled with a 30-mL povidone-iodine solution through the 14F Foley catheter; the solution was left indwelling for 30 minutes. Simultaneously, the bladder was irrigated with physiologic saline, through the 18F three-way Foley catheter. Thus, the urothelium of the bladder would be protected from the eventual backflow of the povidone-iodine solution in the bladder. The catheter in the cystic cavity was removed on postoperative day 5. On postoperative day 10, cystography documented the sealing of the bladder breach; then, the bladder catheter was removed. The patient continued albendazole chemotherapy for 3 months. Cystoscopy confirmed a complete healing of the communication between the bladder and the cystic cavity (Fig. 5). After 56 months of follow-up with ultrasonography and/or CT scan, the patient is free of symptoms with no evidence of residual or recurrent disease (Fig. 6).
At 3 months, cystoscopy has confirmed the closure of the communication between the bladder and the cystic cavity—endoscopic view showing the bladder scar.
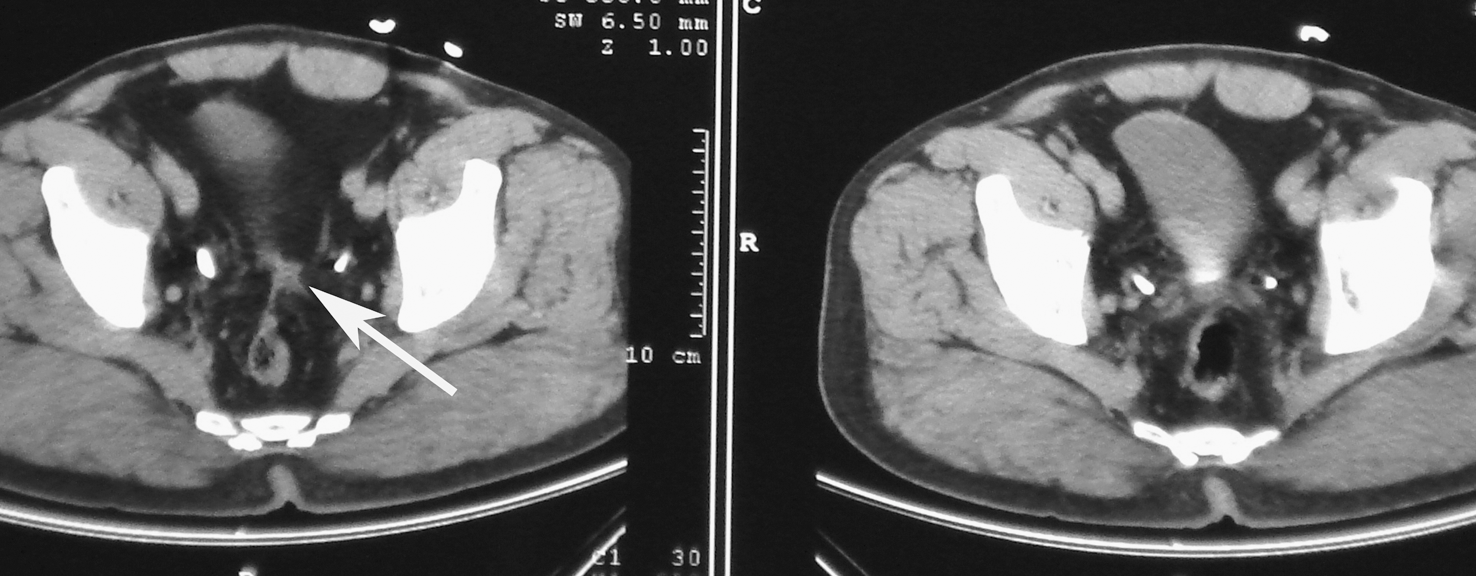
The cystic cavity had almost disappeared (white arrow) at CT scan 22 months postoperatively.
Discussion
Open surgery is the standard therapy for hydatid cyst; the main goal is eradication of the parasite and treatment of the residual cavity. Consequently, the complete removal of the intact cyst is the best option, however, this is not often possible. Thus, frequently parasite evacuation and partial cystectomy is performed. 1,2 Recently, there have been a few reports of laparoscopically managed retrovesical hydatid cysts. 3 In addition, Shailesh and associates 4 reported the use of robot-assisted laparoscopic surgery for the management of a retrovesical hydatid cyst. They think that the enhanced magnification, three-dimensional vision, and robotic technology allow accurate dissection of the cyst. The laparoscopic approach, however, has to be performed by expert surgeons to minimize the risks of cyst rupture and dissemination during dissection, entrapment, and removal of the hydatid cyst.
Natural orifice translumenal endoscopic surgery (NOTES) 6 designates a surgical procedure that uses one or more patent natural orifices of the body with the intention to puncture hollow viscera in order to enter an otherwise inaccessible body cavity, with diagnostic or therapeutic intent. Our procedure seems to comply with the NOTES definition, because the hydatid cyst was outside the bladder, in the peritoneal cavity, and it was approached by puncturing the bladder wall. The advantages of our technique, which are similar to these of a NOTES procedure, come from avoiding an abdominal incision. Therefore, there is no abdominal scar, no postoperative abdominal-wall pain, and no risk of wound infection, hernia formation, or adhesions. In addition, the patient was operated on under spinal anesthesia, which might not be possible with open or laparoscopic surgery.
From the parasitologic view, the main advantage of this transvesical approach, over open or laparoscopic approach, is that there is no or less risk of peritoneal spillage or contamination, because there is adhesion between the bladder wall and the hydatid cyst and there is no passage through the peritoneal cavity. This adhesion has to be documented with ultrasonography or CT. Moreover, this adhesion is also crucial to ensure that there is no bowel interposition between the bladder wall and the cyst. Thus, there would be no risk of bowel injury. Consequently, this technique should not be performed if there is no adhesion between the bladder wall and the cyst. In this case, open or laparoscopic approaches are a better option.
Nevertheless, by creating a passage between the bladder and the cyst, there is risk of a permanent fistula. However, there are reports of conservative management of pelvic hydatid cyst spontaneous rupture into the bladder, however; cystoscopy confirmed the spontaneous sealing of the opening between the bladder and the cyst. 7,8 Moreover, transvesical NOTES reports in pigs demonstrated that the bladder wound closure is not necessary if bladder drainage is assured. 9 Furthermore, if a catheter can be placed in the cystic cavity using a direct percutaneous approach, then a primary bladder wound closure might be performed. In fact, techniques of endoscopic closure of the bladder perforation have been reported in transvesical NOTES, 10,11 to avoid or to decrease the bladder drainage time.
Albendazole therapy was performed to decrease viability of the hydatid cyst. 12,13 Studies have reported a significant decrease in echinococcal scoleces viability after 3 months of albendazole therapy compared with no therapy, 1 month, or 2 months of therapy. 12,13 In addition, adjuvant anthelminthic therapy was prescribed to prevent secondary hydatid disease. 14
The endoscopic transurethral transvesical treatment of hydatid cyst has fulfilled the same steps as open surgery. The parasite was killed before opening the cyst. The hydatid material was completely evacuated. The cystic cavity was treated, to avoid complications. 1,2 More technical experience and longer follow-up, in a larger group of patients are necessary, however, for further evaluation of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.