
Abstract
Purpose:
To investigate changes in renal function after retroperitoneal laparoscopic partial nephrectomy (LPN) with renal hypothermia induced by ice-slush cooling.
Patients and Methods:
Seventy-one patients undergoing retroperitoneal LPN with renal hypothermia were included. Perioperative outcomes were reviewed retrospectively. The total renal function was evaluated by an estimated glomerular filtration rate (eGFR) preoperatively and 6 months postoperatively in 69 patients. Split renal function (SRF) was also evaluated by 99mTc-mercaptoacetyltriglycine scintigraphy preoperatively and 6 months postoperatively in 61 patients.
Results:
The median operative time was 246 minutes (range, 155–424). The median cold ischemic time, including the initial 15 minutes of hypothermia, was 57 minutes (range, 34–112). In the 21 patients whose renal temperature was monitored, median lowest renal temperature was 20.7°C (range, 12.1–27.6). The median baseline eGFR and 6-month postoperative eGFR were 77.2 mL/min/1.73 m2 (range, 36.1–121.3) and 68.3 mL/min/1.73 m2 (range, 33.2–103.4), and the median baseline SRF and 6-month postoperative SRF of the affected kidney were 49.3% (range, 40.3–57.6) and 40.7% (range, 13.8–54.5). Using multivariate analysis, the baseline eGFR (p<0.0001) and the ischemic time (p=0.0073) were associated with the 6-month postoperative eGFR, and the 6-month postoperative SRF was only associated with a baseline SRF (p=0.0185).
Conclusions:
Ice-slush cooling could provide renal hypothermia also under LPN. The decrease in renal function was small, whereas our ischemic time was longer than experts' warm ischemic series. These observations suggested the protective effect of our cooling methods against ischemic injury.
Introduction
Patients and Methods
The Institutional Review Board approved the retrospective collection of data and reporting of results. Between August 2003 and December 2010, LPN with renal vascular clamp was performed in 84 patients. Excluding 2 patients whose operation was converted to open surgery, 2 patients requiring radical nephrectomy, 3 patients with bilateral renal tumors, and 6 patients undergoing LPN without renal hypothermia, 71 patients were included in the present study. Patient characteristics, perioperative outcomes, and data regarding renal function were collected retrospectively from medical charts. Renal nephrometry scores were also calculated based on the criteria proposed by Kutikov and Uzzo. 4 Postoperative complications were graded according to an established five-grade modification of the Clavien system. 5 Regarding the indication for LPN, we actively selected a laparoscopic approach in elective cases with bilateral functioning kidneys. Generally, we selected a retroperitoneal approach for renal hypothermia, while we performed transperitoneal LPN without renal hypothermia in anterior hilar tumors. An open approach is currently selected for imperative cases such as tumor in a solitary kidney or a case with significant renal impairment.
Surgical technique
Surgery was performed by five different surgeons. At the start of surgery, 5F open-ended ureteral catheter was placed cystoscopically in the renal pelvis of the affected kidney for retrograde injection of saline with indigo carmine dye. The patient was then placed in the flank position. A retroperitoneal laparoscopic approach was performed using four trocars. The renal artery was mobilized and secured. The kidney was mobilized within Gerota's fascia, if possible, maintaining perirenal fat over tumor. Laparoscopic ultrasonography was performed to delineate tumor and circumferentially score the line of resection around it. After intravenous administration of 30 g mannitol, the renal artery was clamped by laparoscopic bulldog clamp. Thereafter, ice-cold saline was injected using an irrigation device, and ice slush was also injected through a 12-mm trocar using a metallic funnel (Fig. 1a, b) until the kidney completely sank in. After immersing the kidney in ice-cold water and ice slush for 15 minutes, ice-cold water was aspirated to create the operative field, and the tumor was resected using laparoscopic shears (Fig. 1c). During the cutting procedure, ice-cold water was used for irrigation. The surgical specimen was extracted with an endoscopy bag through the primary port site, and a negative surgical margin was confirmed macroscopically. The opened caliceal system and vessels were repaired by suturing with 3–0 polyglactin, and hemorrhage was controlled with bipolar forceps. Renal parenchymal defect was repaired with 2–0 polyglactin sutures and hemolock (Fig. 1d). Fibrin glue was applied to the cut surface, and a laparoscopic bulldog clamp was then removed. In the early cases (n=21), the renal parenchymal temperature was measured by a needle sensor inserted about 15-mm deep in the nondiseased portion of the kidney.
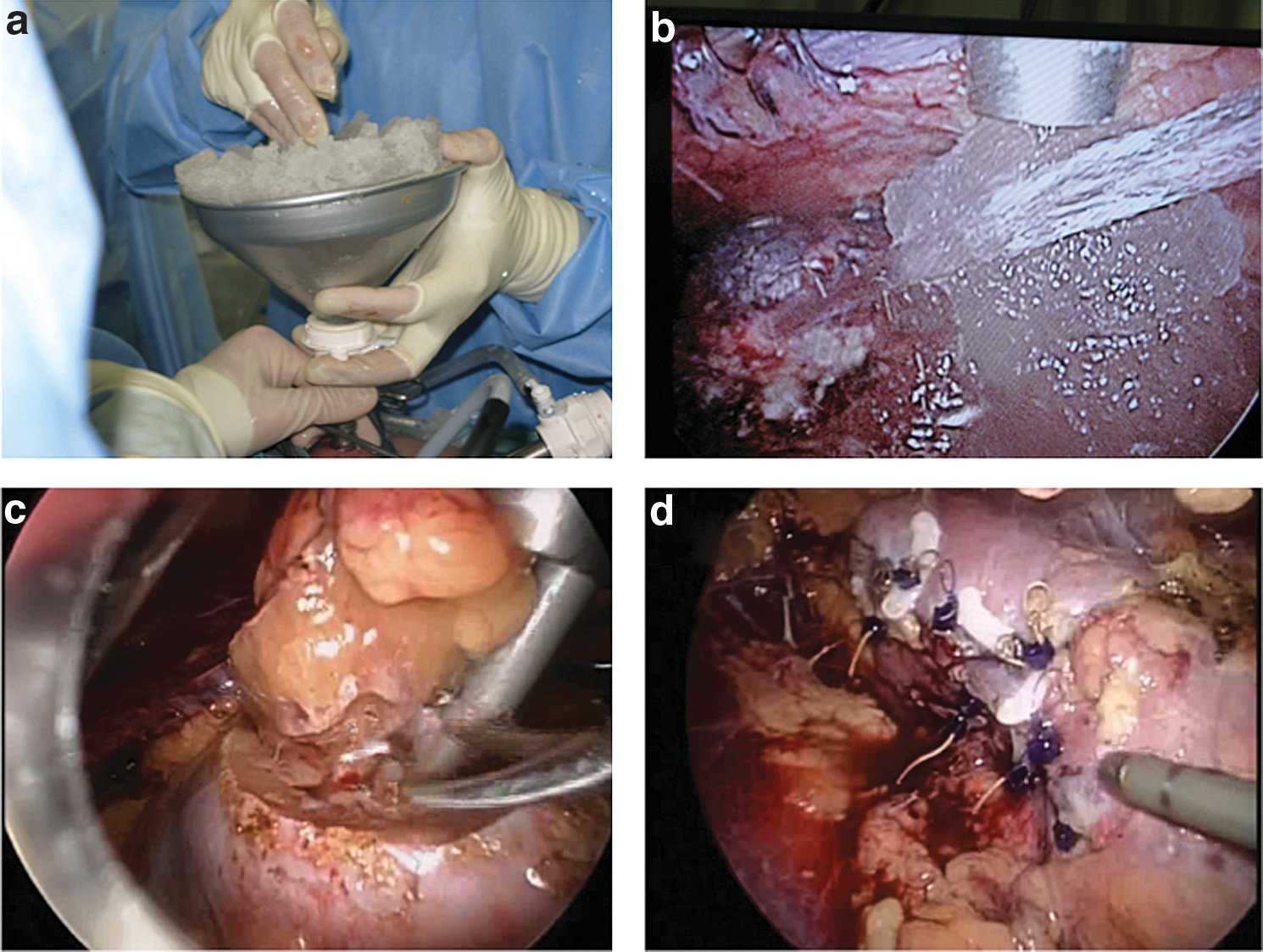
Intraoperative photograph.
Renal function assessment
Total renal function was evaluated preoperatively and 6 months postoperatively using the estimated glomerular filtration rate (eGFR), calculated by the Modification of Diet in Renal Disease Study equation modified for Japanese patients: GFR (mL/min/1.73 m2)=194×0.739 if female/Serum creatinine1.094×Age0.287. 6 Split renal function (SRF) was also evaluated using 99mTc-mercaptoacetyltriglycine (MAG3) scintigraphy preoperatively and 6 months postoperatively.
Statistical methods
The groups were directly compared using appropriate parametric (Chi-square) and nonparametric (Kruskal–Wallis) methods. A multivariate linear regression model was used for the determination of independent factors of postoperative renal function. JMP® version 6.03. was used for all calculations. p-values<0.05 were considered significant.
Results
Table 1 shows the summary of patient characteristics. The median patient age was 60 years (range, 20–81). The median cold ischemic time (CIT), including the initial 15 minutes of hypothermia, was 57 minutes (range, 34–112). In the present series, no patient required blood transfusion intraoperatively. Complications occurred in 10 patients, including postoperative hemorrhages in 5 patients. In these 5 patients, angioembolization and blood transfusion were required in one patient, angioembolization in one, blood transfusion in one, and the remaining two patients resolved under bed rest (Grade 3a; n=2, Grade 1; n=3). Pathologic examinations revealed renal cell carcinoma in 62 patients, angiomyolipoma in 7, oncocytoma in 1, and other benign tumor in 1. Resection margins were negative in all patients. Figure 2 shows individual renal temperature graphs during renal hypothermia in 21 patients. The median lowest renal temperature was 20.7°C (range, 12.1–27.6), and the median time to reach the lowest temperature was 19 minutes (range, 9–39). In nine patients, renal temperature decreased to below 20°C.

Individual renal temperature graphs during renal hypothermia in the early 21 patients. In nine patients (blue line), renal temperature decreased to below 20°C.
RCC=renal cell carcinoma.
Table 2 shows the summary of the outcome of renal function. Excluding two patients who were lost to follow-up, changes in eGFR were evaluated in 69 patients. In addition, changes in SRF were also evaluated in 61 patients. Median baseline eGFR and 6-month postoperative eGFR were 77.2 mL/min/1.73 m2 (range, 36.1–121.3) and 68.3 mL/min/1.73 m2 (range, 33.2–103.4). Median SRF of the affected kidney and 6-month postoperative SRF were 49.3% (range, 40.3–57.6) and 40.7% (range, 13.8–54.5). When patients were divided into three groups according to their ischemic times (≤45 minutes, 46–59 minutes, and ≥60 minutes) and the outcome of renal function was compared, the results of median 6-month postoperative eGFR were 76.1 mL/min/1.73 m2 with ≤45-minute CIT, 72.6 mL/min/1.73 m2 with 46–59-minute CIT, and 62.1 mL/min/1.73 m2 with ≥60 minute-CIT (Kruskal–Wallis test, p=0.0436). Regarding changes in SRF, the decrease in SRF was larger in the ≥60-minute CIT group (median 10.9%) than those in the other two groups (≤45-minute CIT group; median 8.5%, 46–59 minute-CIT group; median 8.5%), although there were no significant differences among the three groups. Using multivariate analysis, baseline eGFR (p<0.0001) and ischemic time (p=0.0073) were associated with 6-month postoperative eGFR, whereas only baseline SRF (p=0.0185) was associated with 6-month postoperative SRF (Table 3).
preop=preoperative; postop=postoperative; eGFR=estimated glomerular filtration rate; SRF=split renal function.
CI=confidence interval.
Discussion
Historically, the impact of temporary renal ischemia with the normothermic kidney was extensively studied in the late 1970s and early 1980s when complex nephrolithotomies were the only therapeutic solution for many staghorn stones. 7 –10 Based on animal experiments and morphologic studies of human kidneys, 30 minutes is generally considered the limit of normothermic ischemia duration. 7,8,10 In terms of renal hypothermia, it could protect renal ischemic damage and allow longer ischemic duration. Based on histologic examinations of human kidneys, Rocca Rosetti reported that cold ischemia was tolerated within 60–70 minutes. 10 In open partial nephrectomy, surface cooling of the kidney with ice slush has been traditionally used to minimize renal ischemic damage. From these standpoints, we have been duplicating ice-slush cooling in LPN to minimize renal ischemic damage as well as permit a longer ischemic duration. When a novice surgeon performs this type of surgery, or when an expert surgeon performs surgery on a difficult case, cold ischemia could offer the surgeon extra time.
Regarding renal hypothermia using ice slush under LPN, Gill et al first reported placing a large endoscopic bag around the kidney and introducing ice slush to the bag during transperitoneal LPN. 11 Our method was a modification on the technique reported by Wakabayashi et al. 12 They developed a new cylindrical insertion device for ice slush, while we injected ice slush into the retroperitoneal space through a 12-mm laparoscopic port using a metallic funnel. In the present study, the median lowest renal temperature was 20.7°C (range, 12.1–27.6), and the median time to reach the lowest temperature was 19 minutes in the early 21 cases (Fig. 2). Because Novick described that it took 15–20 minutes to reach 20°C (range, 9–39) in their experiences of open surgery, 8 the efficiency of surface cooling seemed to be almost similar. Some disadvantages associated with ice-slush hypothermia in LPN may be variations in nadir temperature, which are probably influenced by the amount of ice slush injected around the kidney and perinephric fat removal before hypothermia, or the difficulty in adding ice slush during the cutting procedure. Other potential limitations may be a restriction where this technique can only be used in a retroperitoneal approach. Therefore, it cannot be used in anterior hilar tumors, which may be more suitable for a transperitoneal approach. The ice slush itself may obscure the operative field. However, we consider that our cooling method is more simple and effective than other cooling methods such as transarterial perfusion or transureteral perfusion of the renal pelvis. 12 –17
Regarding changes in total renal function, median baseline eGFR and 6-month postoperative eGFR were 77.2 mL/min/1.73 m2 (range, 36.1–121.3) and 68.3 mL/min/1.73 m2 (range, 33.2–103.4). Recently, Gill et al reported the functional outcome in the latest 235 LPN cases using an early unclamping technique (median ischemic time: 14 minutes) where the median baseline eGFR and latest eGFR were 77.8 mL/min/1.73 m2 and 67.7 mL/min/1.73 m2. 18 Shikanov et al also reported functional outcomes in 401 cases undergoing LPN (median ischemic time: 29 minutes), where the median baseline eGFR and latest eGFR after surgery were 78 mL/min/1.73 m2 and 71 mL/min/1.73 m2. 19 Although there was a big difference in ischemic times between their studies and ours, functional outcomes were similar, which suggested the protective effect of our cooling methods against ischemic injury. Regarding SRF of the affected kidney, the median baseline SRF and 6-month postoperative SRF of the affected kidney were 49.3% (range, 40.3–57.6) and 40.7% (range, 13.8–54.5), which was consistent with a previous study by Arai et al. They reported that in 32 patients undergoing LPN with hypothermia induced by cold saline, median SRF and 3-month postoperative SRF of the affected kidney were 48.7% and 42.9%. 20 We subsequently analyzed the impact of cold ischemic duration on renal function by dividing patients into three groups based on their ischemic times (≤45 minutes, 46–59 minutes, and ≥60 minutes). Median 6-month postoperative eGFR in the ≥60-minute CIT group was lower than those in the other two groups. The decrease in SRF was also larger in the ≥60-minute CIT group than those in the other two groups. Although a linear regression model revealed different results between eGFR and SRF, where baseline the eGFR and ischemic time were associated with 6-month postoperative eGFR; while only baseline SRF was associated with 6-month postoperative SRF, our observation is limited by the small number of patients. Taken together with aerobic metabolism in the kidney and previous histologic studies, 10 we consider that CIT should be kept within 60 minutes under our procedure.
The limitations of our study were the small sample size and its retrospective nature. In addition, there was no control group undergoing warm ischemic resection in the present cohort. Therefore, our study could not answer which is the better form of ischemia. Nevertheless, we consider that several important observations were demonstrated in the current study.
Conclusions
Ice-slush cooling could provide renal hypothermia also under LPN. The decrease in renal function was small, whereas our ischemic time was longer than experts' series of warm ischemia. These observations suggest the protective effect of our cooling methods against ischemic injury.
Footnotes
Disclosure Statement
No competing financial interests exist.