
Abstract
Background and Purpose:
During the past decade, the incidence of severe infections after transrectal ultrasonography-guided prostate biopsy has increased. Antibacterial sustained-release varnish has been shown to reduce bacterial infections. This varnish has yet to be tested in the field of urology. We undertook an in vitro study to assess the possibility of reducing infection rates after prostate biopsy by coating the needle with a novel sustained, yet rapid release chlorhexidine varnish (SRV-CHX) specifically modified for prostate biopsy.
Materials and Methods:
A model simulating the microbiologic environment of a prostate biopsy was developed. The model consisted of two layers of agar, of which the first represented the rectum and was preinfected with Escherichia coli. The second layer was sterile and represented tissue interposed between the rectum and prostate. SRV-CHX–coated biopsy needles were inserted 12 times through the two layers, into the third agar layer representing the prostate. Infection transmission was determined by assessing bacterial growth at inoculation sites within the agar plate representing the prostate. Bacterial growth inhibition was measured as an inhibition zone on the contaminated agar.
Results:
Testing the antibacterial effect of the SRV-CHX–coated needle, we found a substantial reduction of infection transmission as well as sustained inhibition of bacterial growth compared with control needles.
Conclusions:
Needles coated with SRV-CHX offer a new strategy in infection control after prostate biopsy. A new strategy of SRV-coated prostate biopsy needles supplemented with various antibacterial agents, combined with prophylactic oral antibiotics should result in decreased infection rates after prostate biopsies. Further in vitro studies are needed to formulate the SRV with an optimal antibacterial agent.
Introduction
Attempts to reduce the increasing infection rate after TRPB have focused on many aspects of the procedure, including: Identification of patients at risk; 9,10 broadening the antibiotic prophylaxis regime; 11,12 reducing bowel bacterial load; 13 preventing equipment-associated contamination; 14 –16 and shifting the biopsy approach from a transrectal to a transperineal (cutaneous) approach. 5,17
Of note is an interesting approach investigated by Koc and colleagues 18 who claimed that washing the biopsy needle with povodine-iodine does not have an additional benefit. One can speculate that no benefit was observed in their study because the liquid antiseptic solution is easily removed from the needle, resulting in a nondurable disinfective property. In theory, to achieve a sustained response, the needle should be coated with a formulation that would adhere to the needle yet still be able to release its disinfective agent in a controlled mode. This type of formulation has been investigated in the field of dentistry in which teeth, dentures, dental implants, and prosthetic devices were coated with a sustained release varnish (SRV) supplemented with either antibacterial agents, fluoride, or antibiotics. 19 –22 Studies have shown a predictable release rate combined with an antibacterial effect.
In this in vitro study, biopsy needles were coated with a novel sustained-release varnish of chlorhexidine (SRV-CHX). We investigated the effect of the SRV-CHX on infection transmission and bacterial growth inhibition during a simulated prostate biopsy.
Materials and Methods
Sustained release varnish preparation
The SRV-CHX was formulated by a similar method to that described by Friedman and associates, 23 yet modified to achieve a rapid-release kinetic property. Briefly, ethylcellulose and polyethylene glycol 400 (PEG 400) were used as the polymeric matrix, and CHX was used as the active antibacterial agent. Ethanol was used as the solvent. The resulting varnish contained 1% (W/W) CHX. The placebo varnish was prepared identically to the experimental SRV, omitting the CHX from the formulation.
Biopsy needle coating
Standard prostate biopsy needles (18 gauge, 20 cm, Pro Mag™ Angiotech, Medical Device Technologies, Inc; Bard Limited, UK) were coated with the above SRV-CHX as follows: The proximal 3 cm of the needles were immersed in a vial containing the varnish preparation for approximately 5 seconds and allowed to dry at room temperature for 10 minutes, thus forming a coating.
Preliminary study
A preliminary study was designed to ensure that the antibacterial efficacy of the CHX was not diminished because of its incorporation into the SRV and that it was properly released from the coated biopsy needles.
Agar plates were embedded with green fluorescence protein (GFP) labeled Escherichia coli (E coli, ATCC 25922) and then punctured or grooved by a SRV-CHX coated needle. After 24 hours of incubation at 37°C, the plates were examined under a confocal laser scanning microscope (Olympus IX70) and assessed for fluorescence indicating bacterial growth. Nonfluorescent zones around puncture sites and grooves represented growth inhibition zones.
Testing model
A model simulating the environment of a transrectal prostate biopsy was designed (Fig. 1). The principle guiding the construction of the model was to imitate the individual bacteriologic media to which the biopsy needle is exposed to during a TRPB procedure. The first anatomic layer encountered by the needle is the rectal lumen, which is an infected environment colonized by gut flora, of which E coli is of special clinical significance. The second layer transversed by the needle is sterile and consists of tissue interposed between the rectum and the prostate gland, mainly the Denonvilliers fascia. The last structure entered by the needle is the prostate tissue itself, which, in healthy individuals, is considered to be sterile as well. In accordance with these principles, the model consisted of two agar layers (brain heart infusion agar), of which the first, representing the rectal lumen, was preinfected with E coli and the second remained sterile. The third medium, representing the prostate, consisted of a sterile agar plate.
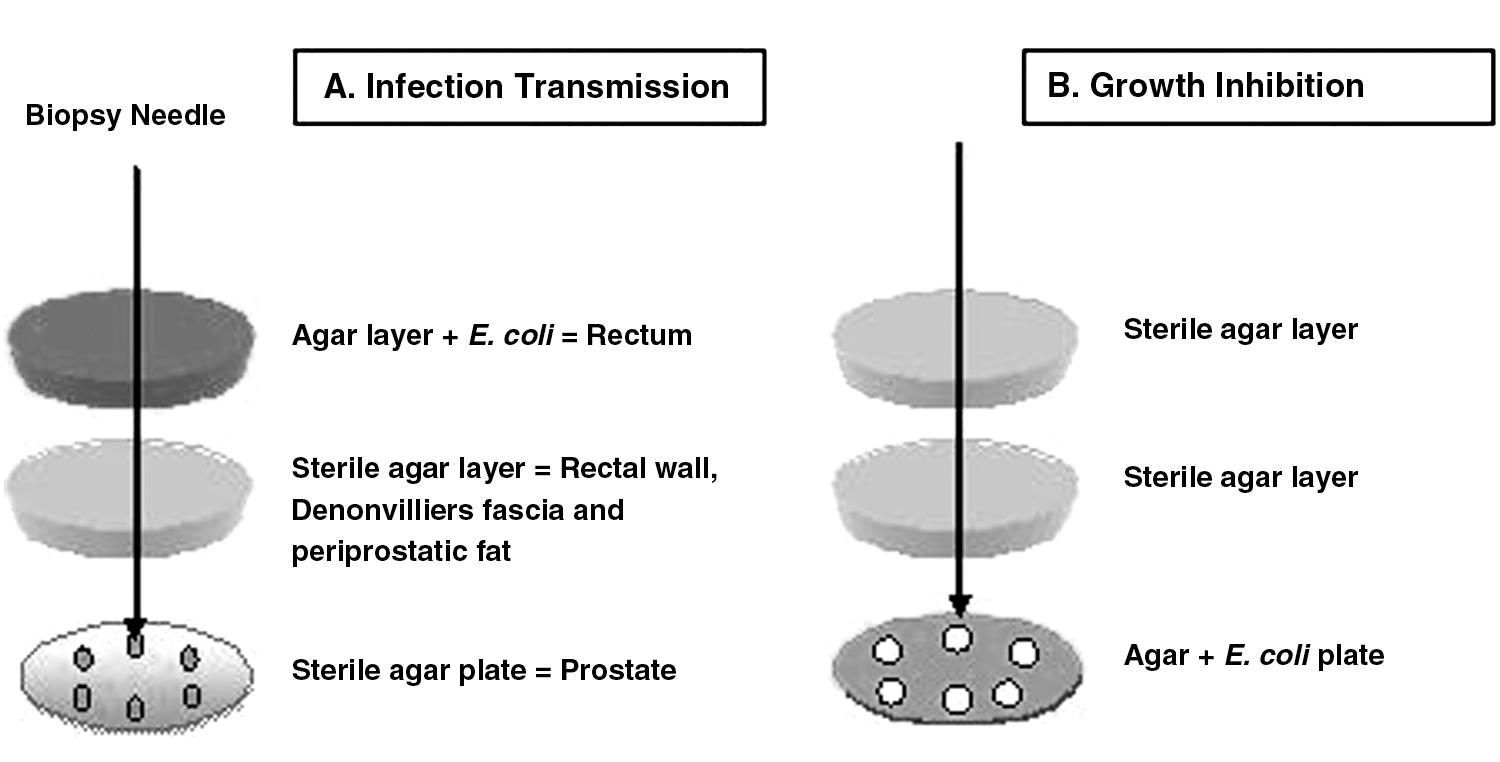
Prostate biopsy models.
Study protocol
The ability to reduce transmission of infection was assessed by inserting the SRV-CHX coated needles into the model (Fig. 1A). Each needle traveled through the first two agar layers before puncturing the sterile agar plate (prostate). This process was repeated 12 consecutive times with each needle (6 times per plate to allow better analysis), simulating current 12-core biopsy templates.
The agar plates representing the prostate were incubated for 24 hours at 37°C and assessed for bacterial growth at the puncture sites. This evaluation was conducted using a magnified viewer and repeated after 48 hours of incubation.
Negative controls included uncoated and placebo varnish-coated needles. Positive controls included needles immersed in a standard CHX 1% (W/W) solution. Single immersion (only before the first insertion into the model) as well as sequential immersions (before each of the 12 consecutive insertions into the model) were evaluated. The experiment was repeated three times.
The biopsy needles were weighed before and after being coated to determine the amount of applied SRV.
The ability of the coated needle to inhibit bacterial growth was assessed by modifying the model, as illustrated in Fig. 1B. Each biopsy needle was inserted 12 consecutive times through the first two layers of sterile agar and then entered the third E coli contaminated agar. These E coli plates were incubated for 24 hours at 37°C after which the presence of an inhibition zone around each puncture site was assessed and measured as described above. The experiment was repeated three times.
Scanning electron microscopy (SEM)
Needles were inspected under a scanning electron microscope (Environmental SEM Quanta 200) for both topographic evidence of mechanical defects in the varnish coat as well as for the presence of bacteria and organic material on the needles.
Results
Preliminary study
When examining the GFP-labeled E coli plates, a strong fluorescence signal was clearly visible representing bacterial growth. This signal was completely undetectable around the puncture site (Fig. 2A) as well as along the groove created by the SRV-CHX coated needle (Fig. 2B). A continuous inhibition zone along the full length of the groove indicated a rapid and sustained release of CHX from the SRV.

Confocal laser microscopy images. Green fluorescence indicates green fluorescence protein Escherichia coli growth whereas an inhibition zone is blacked out.
Transmission of infection
Examination of the agar plates punctured by the SRV-CHX–coated needles showed no signs of growth at any of the first 9 of 12 puncture sites (Fig. 3A). In contrast, bacterial growth was clearly identified at every puncture site in agar plates inoculated by the negative control needles (Figs. 3B, 3C). The agar punctured by positive control needles, disinfected once with CHX solution, showed no bacterial growth at the first punctured site followed by bacterial growth at each of the next consecutive sites. Control needles disinfected with CHX before every puncture (ie, 12 times) showed an unpredictable fluctuating antibacterial effect, with no bacterial growth noted at the first puncture site followed by occasional positive or negative growth at the next consecutive puncture sites (Fig. 3D). The results of all tested samples were maintained after an additional 24 hours of incubation. The average amount of SRV applied was 10 mg. Similar results were obtained in the three repetitions of the experiment.
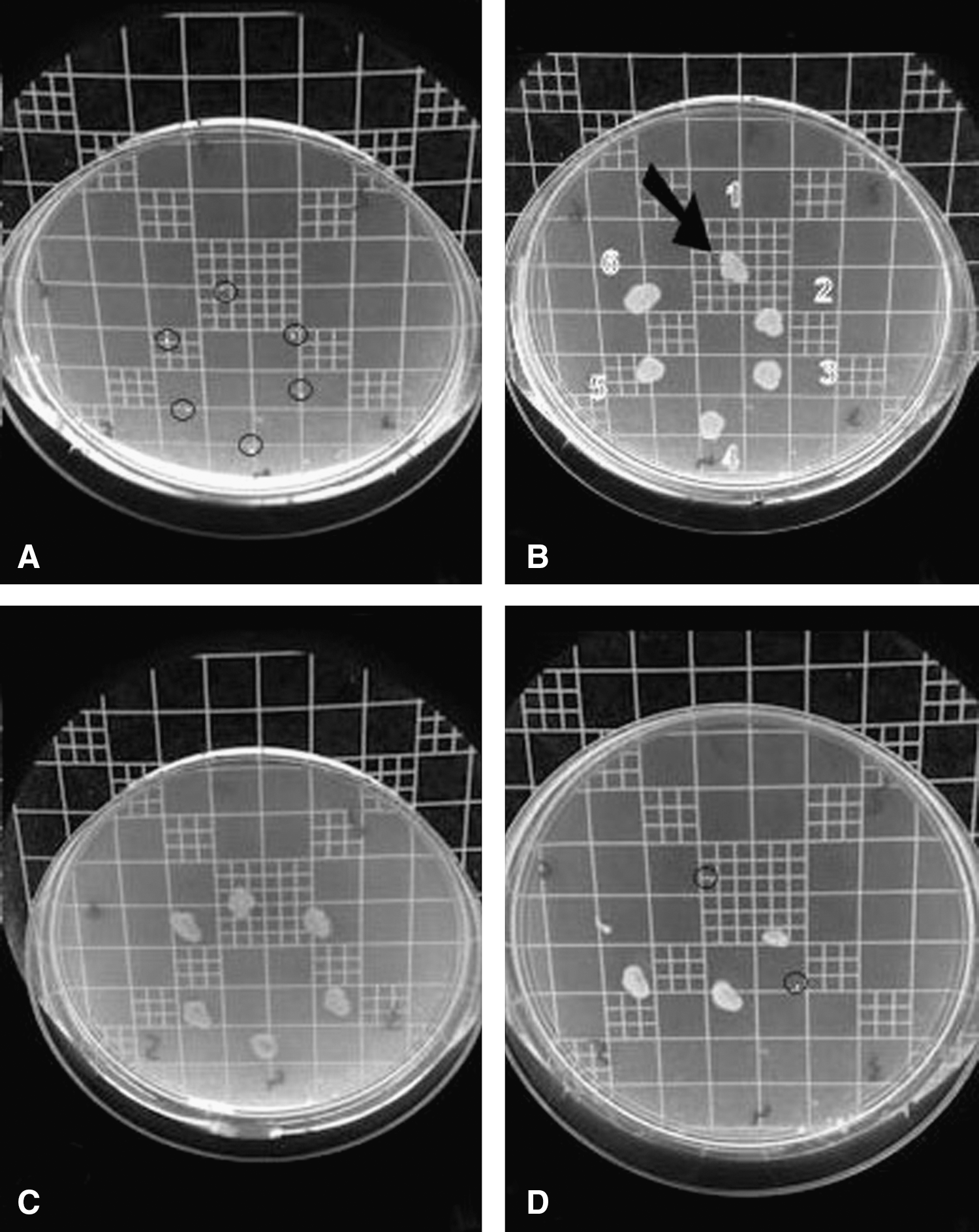
Results of infection transmission assessment after inoculation with
Bacterial growth inhibition
Contaminated agar plates punctured by the SRV-CHX–coated needles demonstrated a clear inhibition zone around each of the puncture sites (Fig. 4A). A dose-dependent response was noted because the inhibition zone diameter of the first inoculation site measured 8 mm and that of the 12th site measured 4 mm.

Results of growth inhibition assessment after inoculation with:
In the contaminated agar plates punctured by the negative control needles, no inhibition zone was noted (Figs. 4B, 4C). The agar punctured by the positive control needles disinfected once with a CHX solution had a short-term transient effect showing an inhibition zone, measuring up to 3 mm, only around the first three puncture sites (Fig. 5). The plates punctured by control needles disinfected with CHX before every puncture had an inhibition zone around every puncture site of up to 4 mm, and this effect fluctuated unpredictably (Fig. 4D, Fig. 5). The results of all plates remained unchanged after 48 hours of incubation. The average amount of SRV applied was 12 mg. Similar results were obtained in the three repetitions of the experiment.
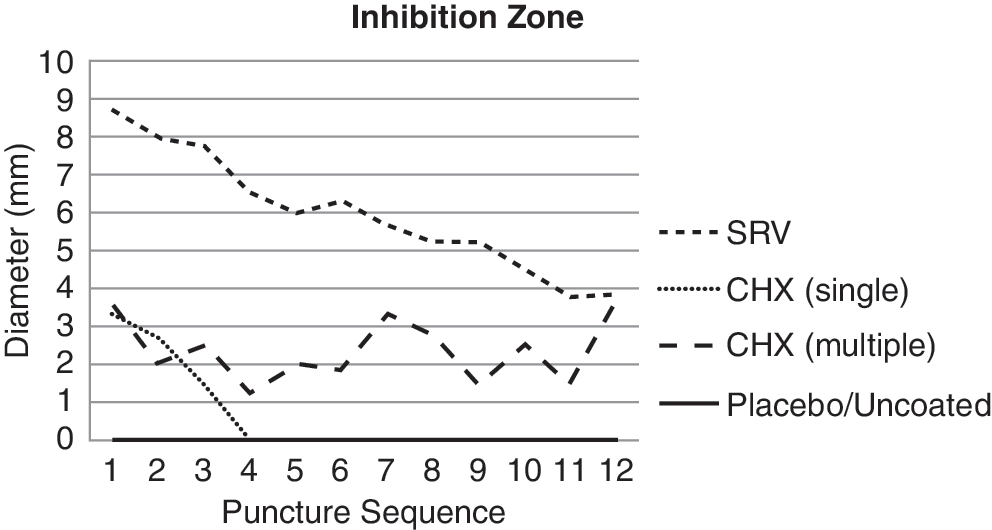
Inhibition zone size. The sustained-release varnish of chlorhexidine (CHX) resulted in sustained large inhibition zones followed by a gradual diminishing effect. Single time immersion in CHX resulted in a small and rapidly diminishing inhibition zone, whereas multiple immersions in CHX resulted in small fluctuating inhibition zones.
SEM
Inspection of the unused SRV-CHX coated needles revealed a circumferential homogeneous coating, measuring approximately 3 to 5 mm (Fig. 6A). Coated needles did not show any mechanical defects in the varnish coat after being inserted 12 times into the model; however, the needles were partially covered by organic material (Fig. 6B).
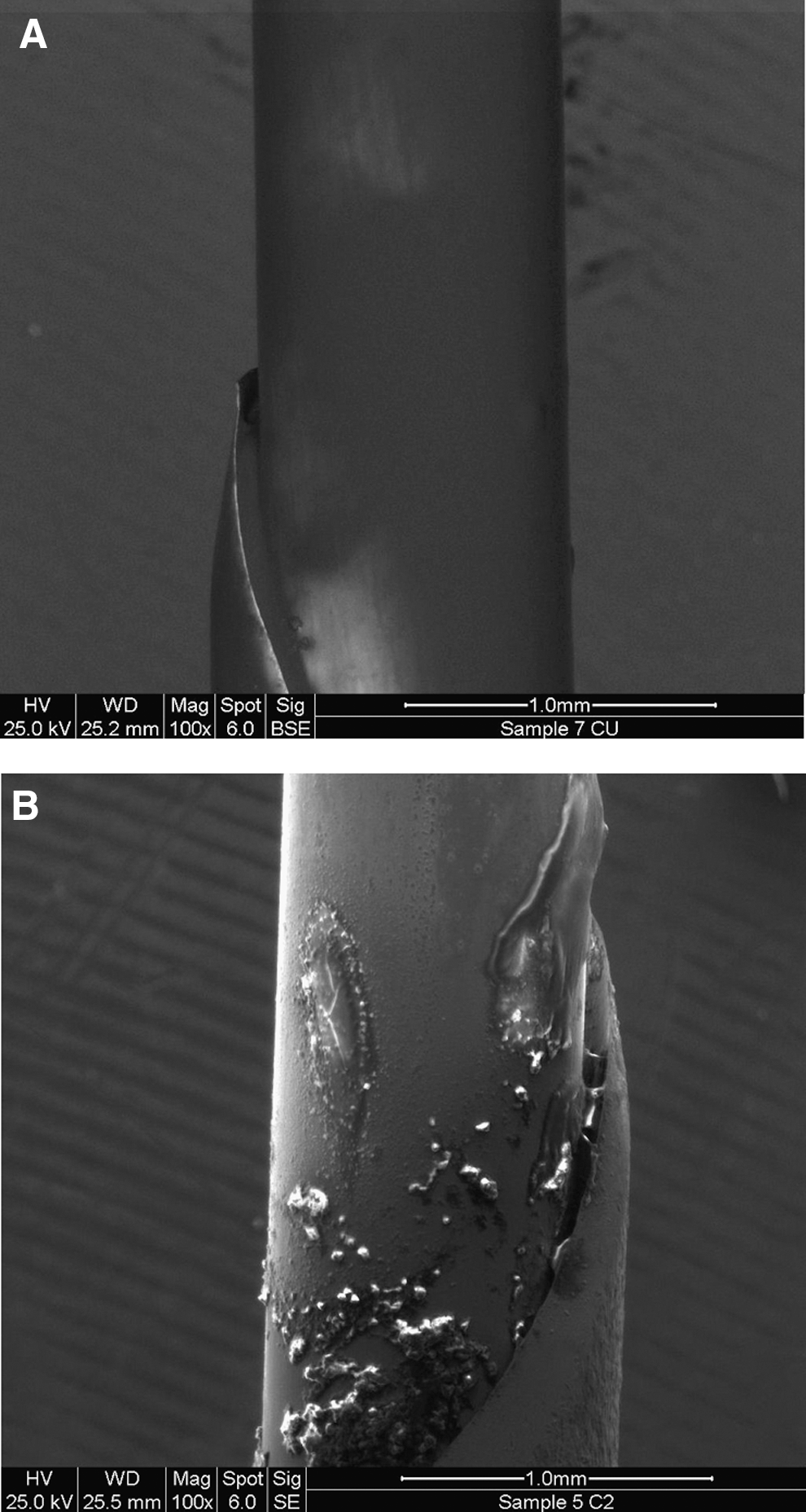
Scanning electron microscopy images.
Discussion
The TRPB procedure may result in septic complications; therefore, antibiotic prophylaxis is recommended by both the American and European urologic associations. 2,4 Several antibiotic agents are known to be effective, of which fluoroquinolones are the ones most commonly used by urologists in North America, 24 Europe, 25 and Asia. 26 During the past decade, the incidence of TRPB-associated infections has increased despite the use of antibiotic prophylaxis 7,27 and is believed to be caused by fluoroquinolone-resistant bacteria in the gut of those undergoing the procedure. 9
In our study, we evaluated a new infection control approach by which coating the biopsy needle with a novel SRV-CHX can achieve a durable disinfective effect. The original varnish was first used in dentistry where it was tested in several human studies for duration of days, both in the oral cavity as well as inserted into periodontal pockets. 22 This varnish was designed to be slow-releasing 21 ; however, during a prostate biopsy, the duration of the interface between the needle and prostate tissue is very short, lasting less than 1 second. Accordingly, the original varnish formulation was modified to achieve rapid, yet sustained release kinetics.
Both antiseptic and antibiotic agents were considered as the active agent suitable to be incorporated into the SRV. We chose an antiseptic because it would not result in the emergence of antibiotic-resistant bacteria within the population. CHX was chosen because of its rapid killing action, broad spectrum of activity, persistent activity despite exposure to bodily fluids, residual effect, and superiority over povodine-iodine. 28,29 We do not exclude the possibility that in future studies, other antibacterial agents will be used, such as triclosan, nitrofurazone, and others. The PEG in the formulation was added as a control release factor. The amount of PEG 400 present in the varnish was about 100 times lower than that approved for oral use.
Preliminary tests performed with the novel SRV-CHX–coated needles demonstrated rapid and sustained release of the CHX from the varnish resulting in a durable inhibition zone.
Studies performed in a model simulating TRPB revealed inhibition of infection transmission achieved by the SRV-CHX–coated needles compared with the negative and positive control needles. This effect lasted during the first 9 of 12 punctures, probably because of the gradual release of the CHX from the SRV after each puncture. This is confirmed by the dose-response effect of the growth inhibition observed with the coated needles (Fig. 5). The inhibitory effect was manifested in each of the inoculation sites and did not vary after 48 hours of incubation, indicating a long-term antibacterial effect of the SRV-CHX.
The average amount of the SRV-CHX we applied onto the needle was 10 mg. SEM micrographs demonstrated that the SRV coating adhered well to the needle and did not shed during the puncture procedure. The SEM micrographs also indicated that nonvital organic material adhered to the coated needle. This is probably protein residues from the brain heart infusion agar.
Combining the findings of the above-mentioned tests, we believe the gradual diminishing effect of the SRV can be attributed to a gradual decline in the CHX concentration within the SRV, or to organic material adhering to the needle, thereby acting as a diffusion barrier to the CHX from the SRV.
Very limited information is available in the literature on prostate in vitro models. We have developed an in vitro model simulating TRPB. The primary aim of this present study was to evaluate the ability of a novel SRV drug delivery system, never before tested in the field of urology, to inhibit infection transmission during a simulated prostate biopsy. Now that feasibility tests have confirmed our scientific hypothesis, further studies using models more comparable to the in vivo conditions and other potential antibacterial drugs are justified. For example, the agar layer representing the rectum was infected solely with E coli and not with a polymicrobial population resembling that of the rectum. We chose this approach because the vast majority of TRPB-associated infections are caused by E coli, 7,11,12 making it the ideal target for our evaluation. In addition, this enabled us to differentiate bacterial growth from inoculation during the simulated biopsy procedure from that occurring because of external contamination. Further model assays would use multiple types of bacteria.
More so, we demonstrated inhibition of infection transmission in 9 of 12 punctures. Future modified SRVs that may incorporate other antibacterial agents should be formulated with a prolonged release effect lasting over 12 consecutive punctures.
Conclusions
In this in vitro study, we have shown for the first time that coating a prostate biopsy needle with a novel SRV-CHX can result in a substantial decrease in the transmission of infection associated with the procedure and inhibition of bacterial growth. This strategy represents a new approach in infection control after TRPB that can be widely implemented in all patients undergoing this procedure and will not contribute to the emergence of antibiotic-resistant bacteria. Further in vitro studies using the SRV technology involving biologic tissues are needed. The proposed new strategy of prophylactic antibiotics combined with varnish-coated needles supplemented with antibacterial agents should result in decreased infection rates after prostate biopsies.
Footnotes
Disclosure Statement
No competing financial interests exist.