
Abstract
Purpose:
To determine whether photoselective vaporization has advantages over transurethral resection of the prostate (TURP) in terms of effectiveness and safety for treatment of patients with benign prostatic hyperplasia.
Materials and Methods:
MEDLINE, EMBASE, and the Cochrane Controlled Trial Register were searched for randomized controlled trials. The risk ratio, mean difference, and their corresponding 95% confidence intervals were calculated for dichotomous and continuous outcomes, respectively. Risk of bias of enrolled trials was assessed according to Cochrane Handbook.
Results:
A total of five trials were enrolled. There was no significant difference in the International Prostate Symptom Score and maximum flow rate between photoselective vaporization and TURP at 6-, 12-, and 24-month follow-up. Photoselective vaporization was associated with significantly lower risk of capsule perforation, transurethral resection syndrome, and clot retention, significantly lower transfusion requirements, a shorter catheterization time, and a shorter length of hospital stay. TURP was associated with a shorter operative time and a lower risk of reoperation. In addition, there was no difference in risk of acute urinary retention and urethral/bladder neck sclerosis between photoselective vaporization and TURP.
Conclusions:
Photoselective vaporization and TURP provide comparable improvements in functional results, including International Prostate Symptom Score and maximum flow rate at 6-, 12-, and 24-month follow-up. Photoselective vaporization offers advantages over TURP in terms of intraoperative safety; however, TURP is found to have a shorter operative time and lower reoperative risk.
Introduction
Laser management of BPHhas challenged TURP because of advances in laser technology, and a variety oflasers have been introduced, including neodymium: yttrium aluminium garnet (YAG), holmium:YAG, potassium titanyl phosphate:YAG, thulium, and diode laser. 7
Photoselective vaporization of the prostate (PVP), commonly known as GreenLight laser, is one of the most recent surgical technologies. Green laser energy is strongly absorbed by hemoglobin and vessels, preventing the occurrence of TURS and capsule perforation. 8,9 Over the past decades, the laser power developed from 60 W 10 to 80 W. 8,11 –13 The most recent high-performance system 120 W laser offers a higher tissue ablation capacity and shorter operative time, 14 which leads to the possibility of treating larger prostates. As a result, PVP may have advantages over TURP in terms of safety and efficiency, especially for high-risk patients such as those receiving anticoagulation therapy. 15,16
The aim of our study is to determine whether PVP has advantages over TURP in terms of effectiveness and safety by making a meta-analysis of randomized controlled trials (RCTs) and to provide stronger evidence that will help clinicians make a more suitable choice.
Materials and Methods
Searching strategy
We searched MEDLINE (from 1966), EMBASE (from 1980), and CENTRAL (from 1977), using MeSH phrases such as “laser therapy” [MeSH], “transurethral resection of prostate” [MeSH], “randomized controlled trial” [Publication Type]. There were no limitations of languages. We also reviewed conference abstracts from meetings of the main professional organizations.
Study selection
Two reviewers (XZ, JG) independently selected eligible trials. Any disagreement between the two reviewers was settled by discussing with the third reviewer (JZ). The main inclusion/exclusion criteria: All RCTs comparing PVP with TURP for treating patients with BPH were included in this meta-analysis; studies that were nonrandomized, had no comparator, or were conference abstracts not published as full articles were excluded.
Assessment of study quality
The quality of eligible trials was assessed using the tool of “risk of bias,” according to the Cochrane Handbook V5.0.2. Sequence generation, allocation concealment, blinding, incomplete data, and selective reporting were assessed, and based on the method of the trials, each of them was graded as “yes (+),” “no (-),” or “unclear(?),” which reflected high risk of bias, low risk of bias, and uncertain of bias, respectively. Because the nature of the intervention made blinding of surgeons impossible, if there was blinding of the patients and the outcome assessors, we thought the study was blinded.
Data extraction
Two reviewers (BP, JC) independently extracted data with a standard data collection form. Any disagreement between the two reviewers was settled by discussing with the third reviewer (CL). The following data were collected: Name of first author, publishing time, number of patients in the PVP group and the TURP group, and baseline data, including green laser power, age, prostate volume (cc), prostate-specific antigen (PSA) value (ng/mL), International Prostate Symptom Score (IPSS), and maximum flow rate (Qmax) (mL/s) before the procedure; perioperative results, including operative time (min), catheterization time (hours), in-hospital stay (days); functional results, including IPSS and Qmax at 6, 12, and 24 months after the procedure; complications, such as intraoperative adverse events including capsule perforation, TURS, blood transfusion requirement, postoperative adverse events including acute urinary retention (AUR), clot retention, urethral/bladder neck sclerosis, and reoperation requirement.
Statistical method
The end points of our analysis were functional outcomes, including IPSS and Qmax; perioperative results including operative time (min), catheterization time (hours), in-hospital stay (days); incidence rate of adverse events, including capsule perforation, TURS, blood transfusion requirement, AUR, clot retention, urethral/bladder neck sclerosis, and reoperation requirement. Risk ratio (RR) or mean difference (MD) and their corresponding 95% confidence intervals (CIs) were calculated for the dichotomous and continuous outcome data, respectively; Q-test was used to analyze heterogeneity of trials. With I2>50%, it was considered as heterogeneous and the Mantel-Haenszel random model was performed; otherwise, the Mantel-Haenszel fixed model was used.
Publishing bias was tested by funnel plot. In addition, sensitivity analysis was applied by removing individual studies from the dataset and analyzing the effect on the overall results. All data analysis was performed using professional meta-analysis software Review Manager (V5.0.2).
Results
Description of studies
A total of five trials 17 –21 including 435 patients were enrolled in our analysis after the review of 224 abstracts and 11 full-text articles. Of the six trials excluded after reading the full text, four trials were nonrandomized, 22 –25 one trial had no comparator, 11 and one trial investigated the factors affecting the improvement of the initial peak urinary flow rate after TURP or PVP for treating BPH 26 (Fig. 1). The follow-up of patients was ≥24 months in three studies.
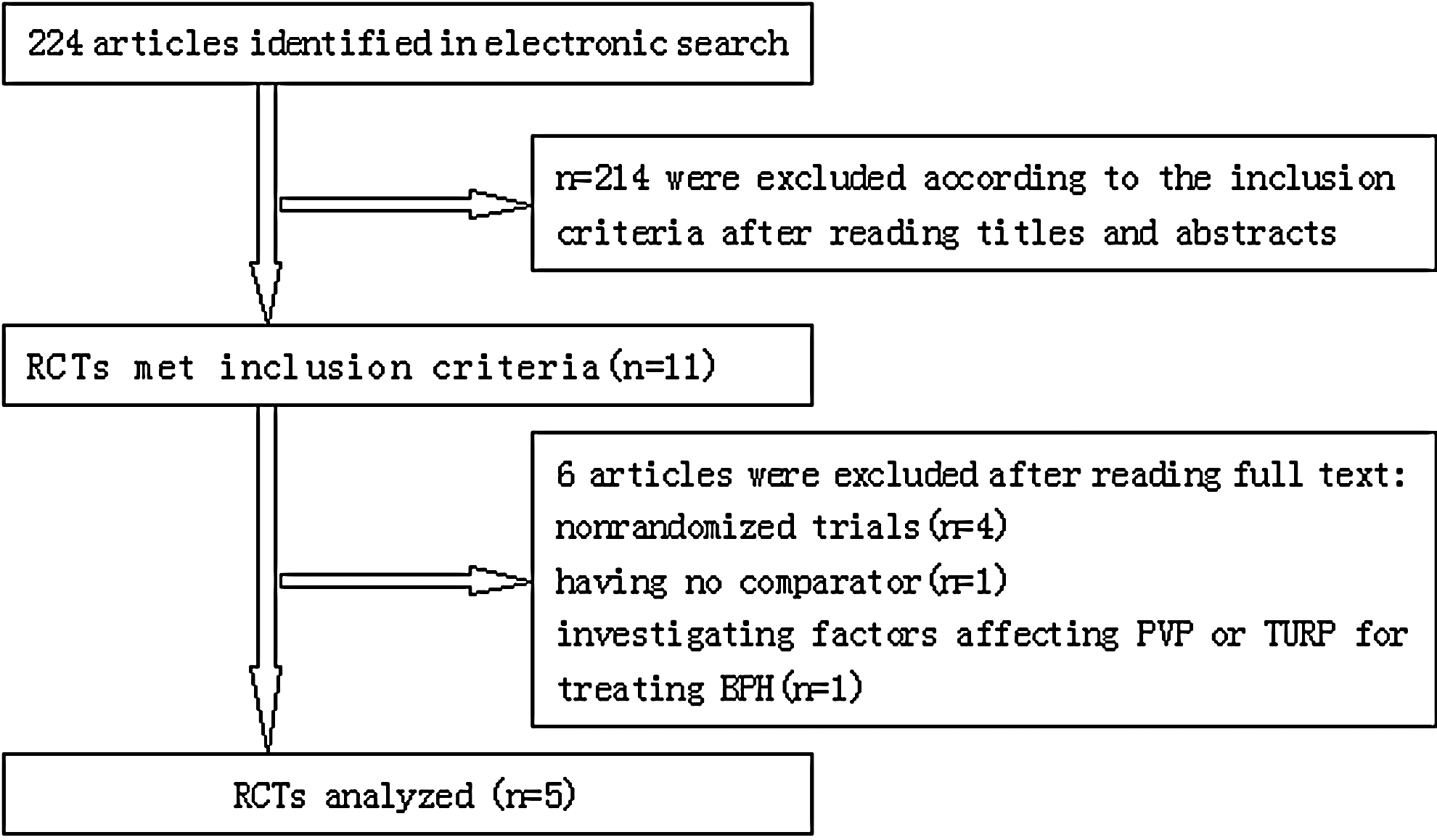
Flow diagram of screened, excluded, and analysed publications. RCTs=randomized controlled trials; PVP=photoselective vaporization of the prostate; TURP=transurethral resection of the prostate; BPH=benign prostatic hyperplasia.
Overall, the inclusion and exclusion criteria were similar for the five studies; however, in one trial, 17 only patients with a prostate volume of 70 to 100 cc were accepted, and the mean age of participants was >60 years old. Of the five RCTs included, two used the 80 W laser 17,18 whereas the other three studies used the most recent 120 W laser 19 –21 (baseline data and other details are shown in Table 1). In addition, reporting of outcome measures varied. While the functional outcomes, including IPSS, QoL, and Qmax, were reported in all five studies, only two 17,18 presented them as the mean (SD). We contacted the author and got the unpublished SD. Before operation, the IPSS and Qmax of PVP and TURP patients appeared comparable.
PSA=prostate-specific antigen; IPSS=International Prostate Symptom Score; QoL=quality of life; Qmax=maximum flow rate; PVP=photoselective vaporization of the prostate; N/A=not available; TURP=transurethral resection of the prostate.
Risk of bias
One trial did not describe the methods of sequence generation, and four trials did not describe the methods of allocation concealment; three trials were not double-blind; and all trials addressed incomplete data (Fig. 2).
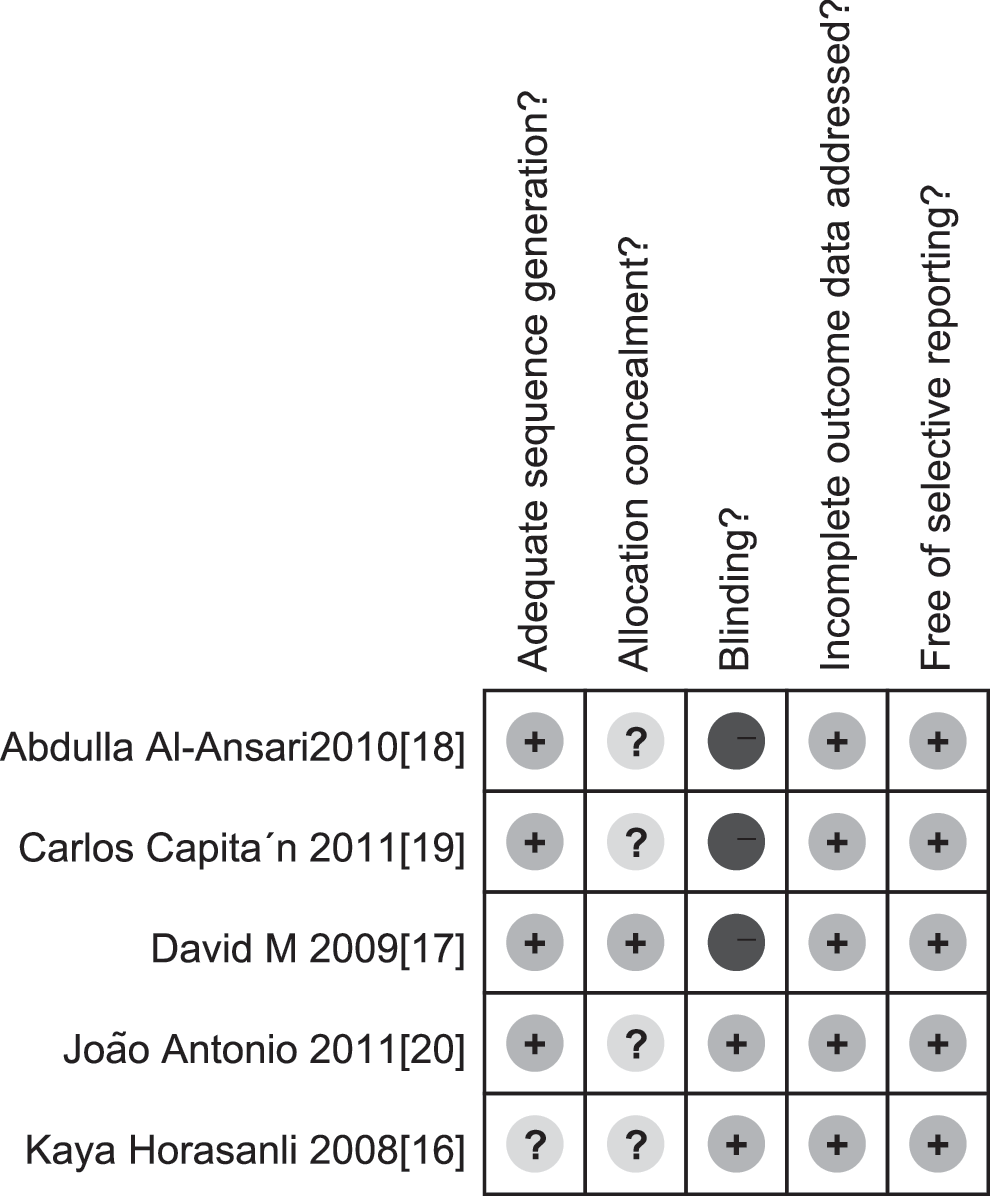
Risk of bias.+is yes, - is no, and ? is unclear, which reflected high risk of bias, low risk of bias, and uncertain of bias, respectively.
Effects of interventions
Functional results
The meta-analysis showed that there was no significant difference in IPSS at the 6-month (MD=0.97, 95% CI=− 2.67–4.62), 12-month (MD=−0.43, 95% CI=−1.77–0.91), and 24-month (MD=0.12, 95% CI=−2.05–2.29) follow-up (Fig. 3). Also, there was no significant difference in Qmax at the 6-month (MD=−0.19, 95% CI=−4.68–4.29), 12-month (MD=0.47, 95% CI=−1.70–2.64), and 24-month (MD=0.72, 95% CI=−0.62–2.06) follow-up (Fig. 4).
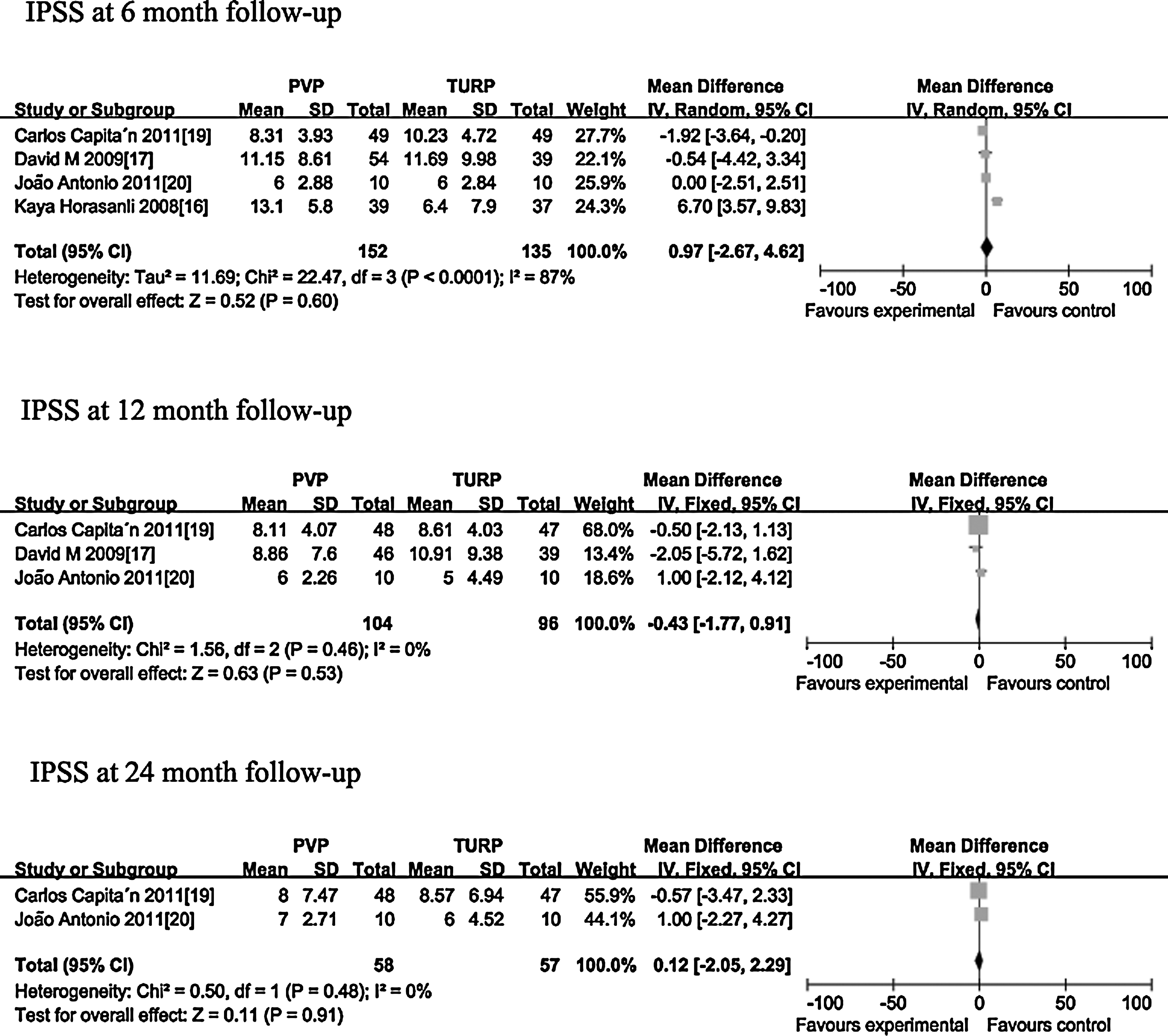
Forest plot of meta-analysis: International Prostate Symptom Score (IPSS) at 6-, 12-, and 24-month follow-up. PVP=photoselective vaporization of the prostate; TURP=transurethral resection of the prostate; CI=confidence interval.
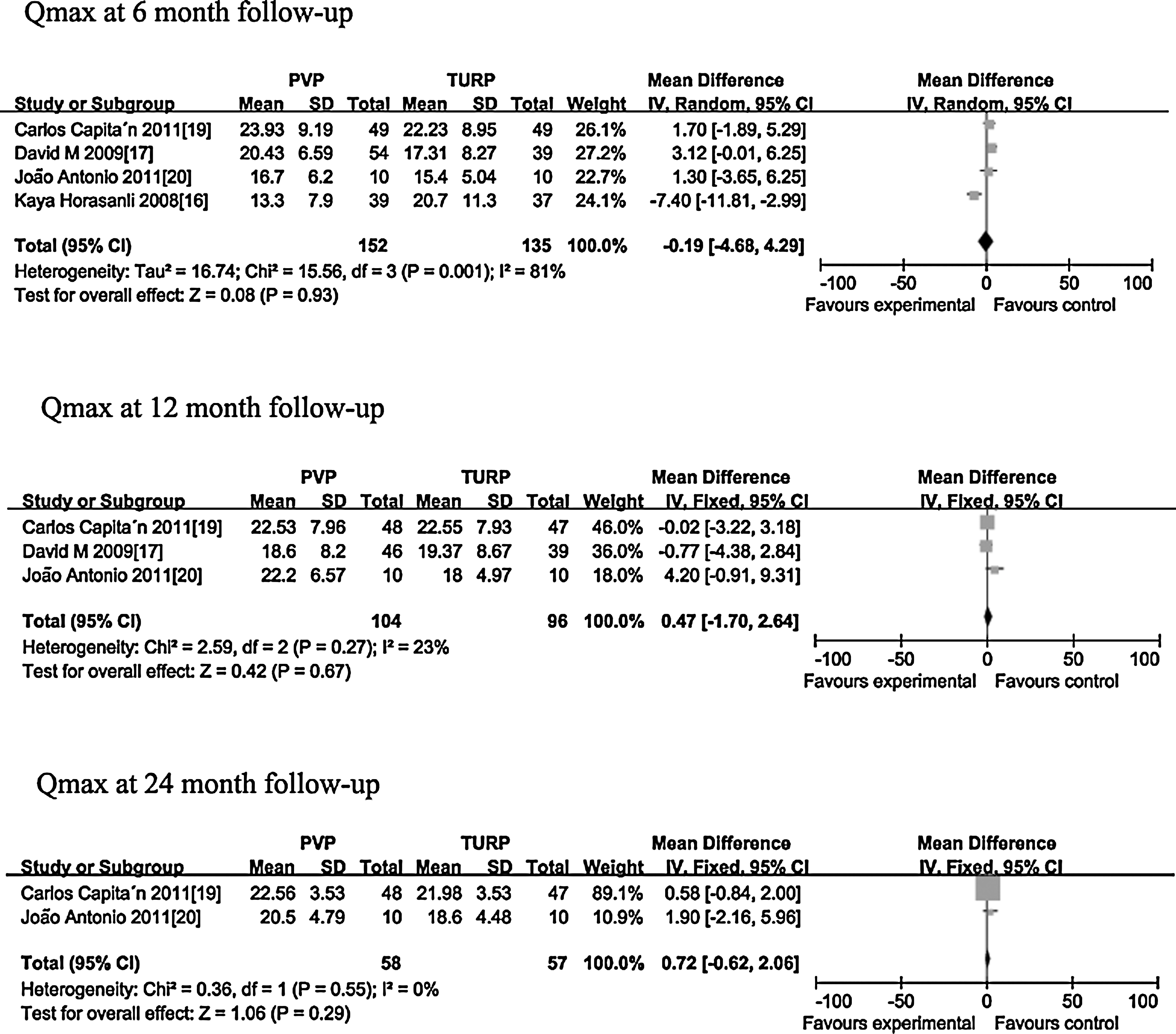
Forest plot of meta-analysis: Maximum flow rate (Qmax) at 6-, 12-, and 24-month follow-up. PVP=photoselective vaporization of the prostate; TURP=transurethral resection of the prostate; CI=confidence interval.
Complications
The incidence rate of intraoperative complications was lower for PVP, including significantly lower risk of capsule perforation (RR=0.08, 95% CI=0.01–0.63), significantly lower TURS rate (RR=0.17, 95% CI=0.03–0.94) and significantly lower transfusion requirement (RR=0.09, 95% CI=0.02–0.39).
In terms of incidence rate of early postoperative complications, the clot retention rate was lower for PVP (RR=0.13, 95% CI=0.04–0.38), but there was no significant difference in AUR between PVP and TURP (RR=1.31, 95% CI=0.54–3.17). In addition, there was no significant difference in urethral/bladder neck sclerosis rate, which was standing for late postoperative complications between PVP and TURP (RR=0.72, 95% CI=0.36–1.45). Furthermore, to our regret, the reoperation rate is significantly higher for PVP (RR=3.64, 95% CI=1.07–12.35) (Fig. 5).

Forest plot of meta-analysis: Complications. PVP=photoselective vaporization of the prostate; TURP=transurethral resection of the prostate; CI=confidence interval; TURS=transurethral resection syndrome; AUR=acute urinary retention.
Duration of operation, catheterization, and hospital stay
The operative duration is longer for PVP (MD=14.53, 95% CI=0.38–28.69); however, the duration of catheterization is longer for TURP (MD=−40.12, 95% CI=−51.62–−28.62); also, the hospital stay is longer for TURP (MD=−2.24, 95% CI=−2.78–−1.71) (Fig. 6).
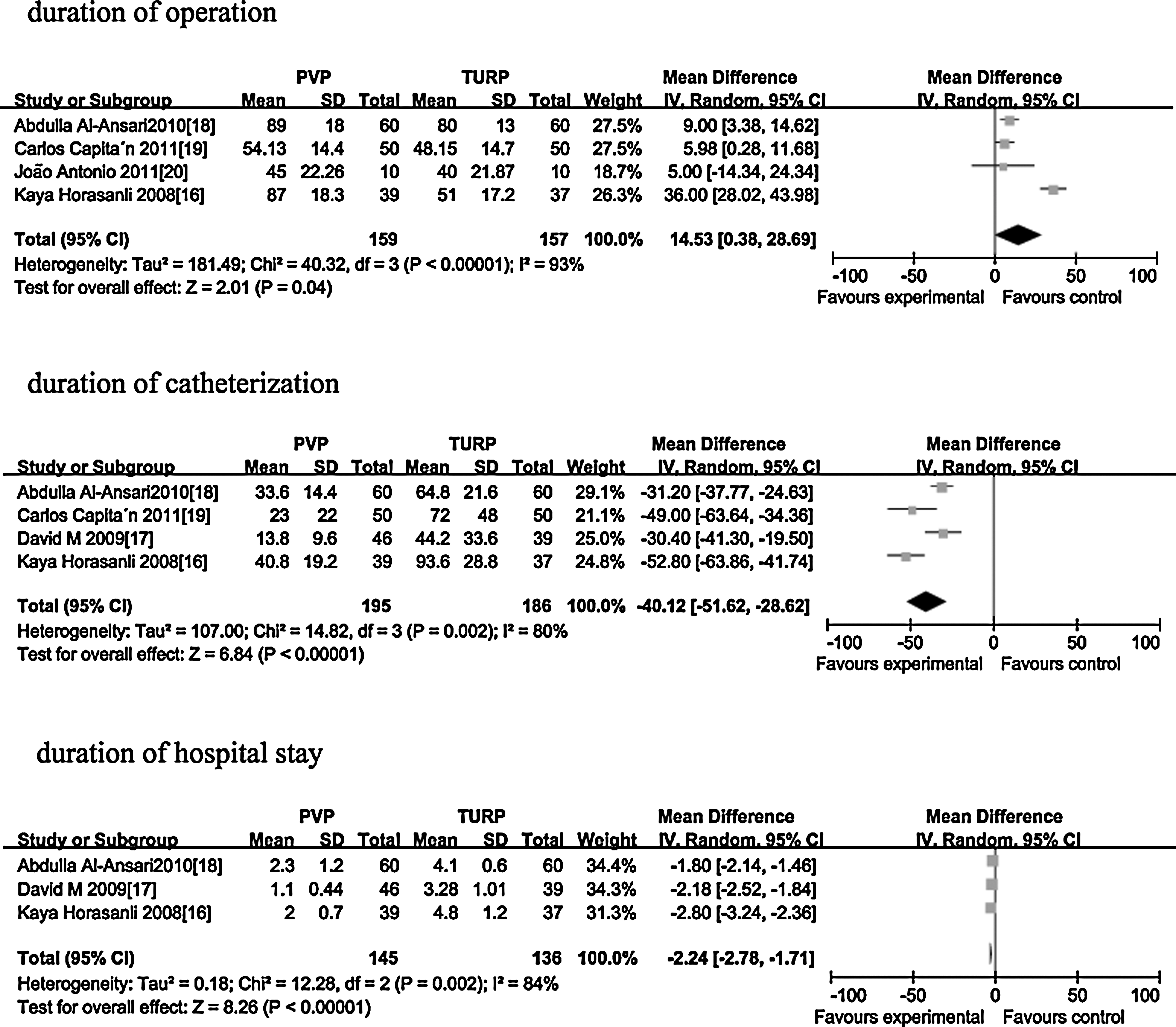
Forest plot of meta-analysis: Duration of operation, catheterization, and hospital stay. PVP=photoselective vaporization of the prostate; TURP=transurethral resection of the prostate; CI=confidence interval.
Discussion
Results explanation
In our analysis, functional outcomes in terms of IPSS and Qmax at 6-, 12-, and 24-month follow-up were comparable in PVP and TURP. There was significant heterogeneity of outcomes between involved trials, however. In the study by Horasanli and associates, 17 the authors investigated the efficacy of PVP and TURP in relatively larger prostates with average volume more than 80 mL, and there was a significant statistical difference in functional outcomes, including IPSS and Qmax, between TURP and PVP within the follow-up of both 3 and 6 months in favor of TURP. A sensitivity analysis that excluded that study from the dataset did not substantially change the result; however, the heterogeneity disappeared (I2=0), which revealed that the prostate volume was the main source of heterogeneity.
In our opinion, for small to midsize prostates, comparable functional results for PVP and TURP were achieved; however, for larger prostates, functional results of PVP in early management (follow-up of 6 months) of the obstructive voiding symptoms may not be comparable to TURP. Furthermore, because the 120 W laser offers a significantly higher tissue ablation capacity compared with the 80W laser, 14 comparable functional results for the 120 W laser PVP and TURP may be achieved. To our regret, however, there is no RCT comparing the 120 W laser PVP and TURP for treating patients with larger prostates.
This meta-analysis showed that PVP has advantages over TURP in terms of a significantly lower intraoperative adverse events rate. As we know, the green laser can be strongly absorbed by oxyhemoglobin, but hardly at all by water, which allows the laser energy to be selectively absorbed by tissue with high oxyhemoglobin content. As a result, occurrence of capsule perforation was hardly seen in PVP treatment. 8,9 The TURS rate was significantly lower for PVP for its use with saline irrigation.
Bleeding was one of the most common complications of TURP, and 6% to 31% of the patients may need blood transfusion early. 27 The meta-analysis result revealed that the incidence was significantly lower in the PVP group. Because of the low risk of bleeding, PVP can be used in high-risk patients who are receiving anticoagulant therapy, 16 which further confirms the point of view of Reich and colleagues. 15 In their study, patients were being treated with ongoing oral anticoagulant therapy, or had a severe bleeding disorder, or were at high cardiopulmonary risk; they concluded that PVP was a safe but effective treatment option in seriously ill patients or those receiving oral anticoagulants.
The operative duration was longer for PVP (MD=14.53, 95% CI=0.38–28.69). We did subgroup analysis of the 120 W laser, and the result showed that the difference of operative duration was deflated (MD=7.41, 95% CI=3.49–11.33), which revealed that the 120 W laser can tackle larger prostates more efficiently and may overcome the significantly longer operating duration of the 80 W laser with improvement of surgical experience in the future. Both duration of catheterization and hospital stay were shorter for PVP.
In terms of incidence rate of early postoperative complications, the clot retention rate was significantly lower for PVP, but there was no significant difference in AUR between PVP and TURP. In terms of incidence rate of late postoperative complications, there was no significant difference in urethral/bladder neck sclerosis rate between PVP and TURP. The reoperation rate was significantly higher in the PVP group. This results mainly from the retention of coagulated, necrotic tissue after laser vaporization and reformed adenoma. In the study by Al-Ansari and coworkers, 19 the prostate size of all reoperation patients was >80 g. Therefore, larger prostate volume may lead to higher risk of reoperation. In addition, we should note that in one trial, 18 to assess the ease of uptake of PVP technology, PVP were performed by urologists who had performed fewer than five laser prostatectomies, which may elevated the reoperation rate. We did sensitivity analysis by removing this study from the dataset; however, the reoperation rate did not decrease, which may resulted from the short follow-up duration that may lead to the low reoperation rate. The most extended non-RCT follow-up data (with some patients completing up to 5 years after 80 W laser PVP) demonstrated a TURP-like reintervention rate of 6.9%, 8,28 however. We should evaluate the reoperation rate at a long-term follow-up in the future.
Limitations of the meta-analysis and included RCTs
There are several limitations to our study. First, of the five RCTs included in our meta-analysis, one trial did not describe the methods of sequence generation, four trials did not describe the methods of allocation concealment, and three trials were not double-blind. As a result, there is a high degree of possibility of selection bias, performance bias, and measurement bias.
The second limitation of this meta-analysis is the small number of patients studied. There were only five RCTs including 435 patients, so the efficiency of the statistical test may be inadequate. Therefore, the conclusion must be treated with caution. When new RCTs of a large sample appear, meta-analysis results may change.
The third limitation is heterogeneity of laser power (80 W–120 W) and we did not perform subgroup analysis of the specific power of PVP, which results from inadequacy of RCTs, for there were only two RCTs that investigated 80 W PVP vs TURP and three RCTs that investigated 120 W PVP vs TURP.
The fourth limitation is that there is only one trial that investigated irritative LUTS. In the study by Pereira-Correia and colleagues, 21 all patients had a spontaneous resolution of irritative LUTS within 1 year of surgery, which was not mentioned in the other four RCTs. In addition, only Pereira-Correia and coworkers21 investigated detrusor pressure at Qmax (PdetQmax) and bladder outlet obstruction index (BOOI). BOOI=PdetQmax −2 Qmax and was classified as <20 (unobstructed) vs≥20 (equivocal or obstructed). 29 They found a significant improvement in PdetQmax and BOOI after PVP and TURP, and there was no significant difference between the two methods (P<0.01).
Implications for future research
Further well-designed and long-term follow-up RCTs are needed, especially large sample multicenter RCTs to more accurate assess the effectiveness and safety of 120 W PVP over TURP for treatment of patients with prostates larger than 80 cc. In addition, researchers should investigate irritative LUTS, PdetQmax, BOOI, and adverse sexual events after PVP and TURP. If there are enough RCTs in the future, we should perform subgroup analysis of a specific power of GreenLight, especially 120 W PVP.
Conclusions
Our meta-analysis demonstrates that PVP and TURP provide comparable improvements in functional results, including IPSS and Qmax, for small to midsized prostates at midterm (24-month) follow-up. PVP offers advantages over TURP in terms of intraoperative safety, including lower incidence rate of capsule perforation, TURS, and lower transfusion requirement. The reoperation rate, however, was significantly higher in PVP. Because of the small number of studies and the fact that their methodologic quality is less than ideal, the conclusion should be treated with caution. Well-designed, multicenter RCTs with long-term (more than 24 months) follow-up are needed to evaluate the role of PVP for treatment of patients with BPH in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.