
Abstract
Purpose:
To review the results of metallic urethral stents used in patients with neuropathic bladder dysfunction after spinal cord injury (SCI).
Patients and Methods:
In a rehabilitation unit for SCI and stroke in Cape Town, South Africa, we performed a case note review of dual flange Memokath stents placed from March 2008 until October 2011. Stents were placed rather than performing an external sphincterotomy in selected patients. With the patient under deep general anesthesia, a thermosensitive expandable metallic stent was positioned over the internal and external urethral sphincters.
Results:
In total, 33 stents were placed in 28 male patients. SCI was cervical in 23 patients and thoracic in 5. Average follow-up was 18 months (range 1–40 months, median 18 months). The most common indications were repeated catheter blockage in eight patients and urinary tract infection in six. The average time from SCI to stent insertion was 79 months (range 1–468 months, median 21 months). Severe autonomic dysreflexia was present in 17 cases before stent placement and in 7 after stents were placed (P=0.003). Stents failed in 15 patients (45%) and were removed. The most common reason for failure was stone formation. Comparing the group of patients with stents lasting >20 months (n=11) to the group with stent removal before 20 months (n=10), the mean time between SCI and stent placement was 31 vs 119 months (P=0.057). Medium term results (up to 27 months) were significantly influenced by earlier stent placement (P=0.0484). One major complication was stent migration that caused an urethrocutaneous fistula.
Introduction
The dyssynergic external urinary sphincter causes outflow resistance affecting intravesical pressures. An increase of more than 40 mm Hg in detrusor pressure (Pdet) is associated with renal function deterioration, as shown by McGuire and associates, 2 although their study was in myelodysplastic patients.
In our referral area, many patients live far away from the nearest hospital, and home care is not well established. A blocked catheter may trigger autonomic dysreflexia causing severe morbidity or mortality. Patients are often reluctant to undergo external sphincterotomy, because this is irreversible and will impact on continence and ejaculation if a cure for SCI should be found in the future. 3
Patients with high SCI may not have a reliable and constant clean intermittent self-catheterization (CISC) service. The temporary nature of metallic thermolabile expandable urethral stents is attractive, because it does not compromise the possibility of other forms of treatment for neuropathic bladder dysfunction at a later stage, yet it overcomes the increased outflow resistance at the external sphincter, allowing for a safer, low pressure bladder.
Patients and Methods
We performed a retrospective case note review of patients with SCI who had new generation dual flange Memokath™ stents (Pnn Medical A/S, Kvistgaard, Denmark) inserted in the period March 2008 to October 2011. Indications for stent placement were: (1) Severe autonomic dysreflexia related to catheter blockage or residual urine volume (RV); (2) repeated catheter blockage related to bladder spasms; (3) bladder stones related to poor bladder emptying in patients on CISC; (4) recurrent urinary tract infections (UTI); (5) prevention of upper urinary tract damage, if signs of severe bladder hostility were seen on urodynamic study (UDS) and cystography (poor compliance and high Pdet with poor emptying), coupled with symptoms of autonomic dysreflexia (headaches, hypertensive episodes, and sweating).
External sphincter electromyography was not available in this study, and detrusor- sphincter dyssynergia was assumed if a hostile bladder was diagnosed in patients with a high SCI. Bladder hostility scores, such as the Galloway score, were not routinely used. UDS were not performed after stent placement because the stents could be dislodged by inserting the catheter used for infusion and pressure measurement. American Spinal Injury Association scores were not correlated. Most of the patients had severe trauma, however, and partial SCI lesions did not influence the decision for stent placement on that basis alone.
Exclusion criteria were current bladder stones and active UTI, which were first treated. Stents were only inserted in such patients after a cool-down period allowing bladder and urethral mucosa to maximally normalize with catheter drainage.
With the patient under deep general anesthesia to prevent autonomic dysreflexia triggered by bladder distention at cystoscopy, a Memokath thermolabile expandable metallic stent was positioned over the internal and external urethral sphincters (Fig. 1). In addition to the manufacturer's recommendation of measuring the prostatic and sphincteric length, the bladder was also filled with dilute contrast to make sure the stent did not protrude far into the bladder, risking excessive early encrustation. The stent was expanded by irrigating it with warm saline (65°C) when seen in position over the bladder neck and external sphincter on radiographic fluoroscopy. A condom type catheter was applied over the penis to replace any former methods of bladder drainage. Patents were postoperatively observed for fever, signs of autonomic dysreflexia, and high RVs indicating poor emptying of the bladder. If urine did not drain adequately, an F14 catheter was placed through the stent for 3 to 7 days, and radiography was performed to confirm the stent position. Patients were kept overnight in the hospital to treat any immediate complications early and were routinely followed up at 1 month and again between 3 and 6 months.

Memokath stent in position.
Statistical analysis was performed with the Student t test for parametric variables, The McNemar test for contingency table analysis and log-rank analysis with Kaplan- Meier survival curves for stent survival, using GraphPad InStat,® GraphPad Prism® (
Results
From March 2008 until October 2011, 33 stents were placed in 28 patients. The average patient age was 37.4 years (range 23–64 years). The mode of SCI was motor vehicle accident in 14 (50%) cases; fall from height, 5 (18%); water sport accidents, 3 (11%); bicycle accident, 2 (7%); agricultural accident, 1 (3.5%); rugby injury, 1 (3.5%). Most patients had high SCI in the cervical region: C3=1 (3.6%), C4=2 (7.2%), C5=9 (32.1%), C6=7 (21.4%), C7=4 (14.2%), T4=2 (7.2%), T8=3 (10.7%), T10=1 (3.6%). Average serum creatinine level before stent placement was 59.5 μmol/dL (range 37–127, median 79 μmol/L) (normal 60–120 μmol/L).
Of the 33 stents inserted, 2 were replaced in the immediate postoperative period because of failed procedures, and these stents were excluded from analysis. Three patients requested stents again after stent failure at 12, 23, and 35 months follow-up and were re-entered in the analysis as if they were new patients. Indications for placing stents (n=31) were: Repeated catheter blockages, 8 (26%); recurrent UTI related to RV, 6 (19%); severe autonomic dysreflexia related to poor bladder emptying, 6 (19 %); high Pdet seen on UDS, 5 (16%); failed CISC, 3 (10%); failed external sphincterotomy, 2 (6%); and recurrent bladder stones, 1 (3%). Time from SCI to placement of the stent was on average 79.6 months (range 0.75–468, median 36 months). RV before stent placement was 150 mL (range 32–400 mL, median 115 mL) and after stent placement, 33.8 mL (range 0–400 mL).
Mean follow-up was 18 months (range 1–40, median 18 months). UTI was documented in 22 patients before stent placement and in 7 patients during follow-up (P<0.001). Two patients had hydronephrosis before stent insertion, but recovered. Hydronephrosis developed in one patient after stent placement because of a large bladder stone causing bladder outlet obstruction. Average Pdet before stent insertion was 73 cm H2O (range 10–150, median 60 cm H2O). Autonomic dysreflexia decreased from 17 cases before stent placement to 7 cases after stent placement (P=0.003). Bedsores were noted in seven patients before and in two patients after stent placement. No patients reported pain or discomfort as a consequence of stent placement.
Fifteen of 33 (45%) stents were removed during the follow-up period, and 18 (55%) were in situ at a mean follow-up of 18 months (Fig. 2). The average time failed stents were in situ before removal was 15.7 months (range 0.25–38, median 12 months). The average time to placing stents after SCI was 86 months for the group with failed stents vs 87.5 months for the group with the stent in situ at last follow-up (not statistically significant). Stents were removed for stone formation in seven (47%) patients, stent migration in three (20%), large RV in three (20%), new severe autonomic dysreflexia in one (6.5%), and severe hematuria of uncertain cause in one patient (6.5%).
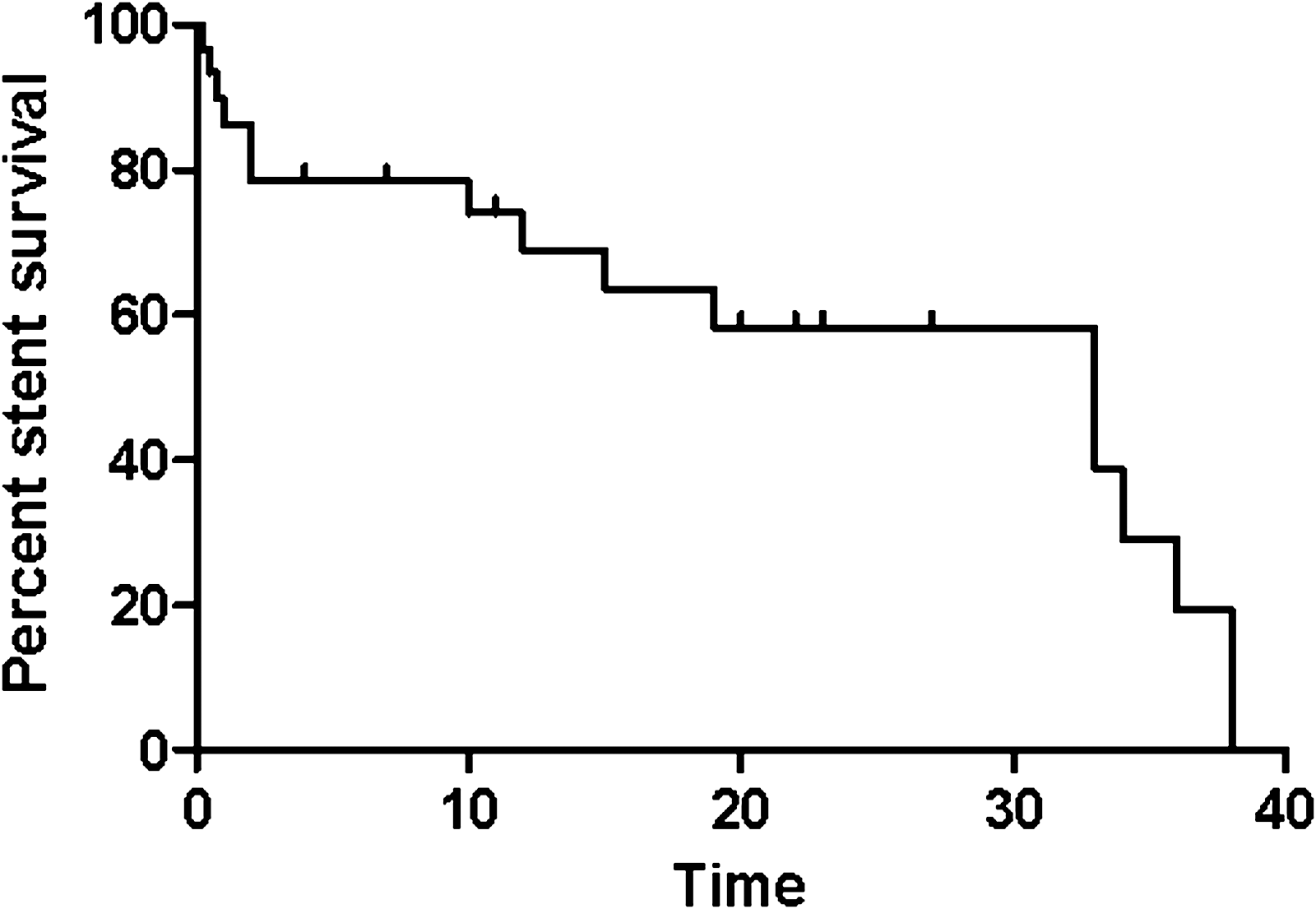
Kaplan-Meier survival curve showing proportion of stents remaining in situ at mean follow-up of 18 months (31 stents, mean follow-up 18 months).
A subset of stents lasting more than 20 months (n=11) was compared with the subset of stents removed before 20 months (n=10) (this excluded stents remaining in situ for less than 20 months at last follow-up) (Table 1).
SCI=spinal cord injury; RV=residual volume; Pdet=detrussor pressure.
Another subset of stents was evaluated (Figs. 3 and 4): Stents placed less than 18 months after SCI and stents more than 18 months after SCI were compared. For the whole group at 40 months follow-up the difference was not significant (P=0.5542) and the curves crossed at about 34 months. Follow-up for this subset was then further limited to a maximum of 27 months to see if there was a significant difference in the medium term. This excluded stents with longer follow-up than 27 months. Statistical significance could be reached with P value 0.0484.

Kaplan-Meier survival curve comparing early (<18 months after SCI) vs late stents (>18 months after SCI) remaining in situ at maximum follow-up of 40 months (31 stents, mean follow-up 18 months).

Kaplan-Meier survival curve showing proportion of stents remaining in situ at maximum follow-up of 27 months (11 early and 14 late stents; mean follow-up, 13.6 months for early- and 5.1 months for the late groups).
A large stone formed on stent was removed with open surgery (Fig. 5). Complications of the placement of 33 stents were 4 (12%). No patient had more than one complication. Patients who received a second stent did not have any complications. Complications were urethrocutaneous fistula, 1 (3%); severe autonomic dysreflexia, 1 (3%); hematuria, 1 (3%); renal failure from bladder stone and patient lost to follow-up, 1 (3%).
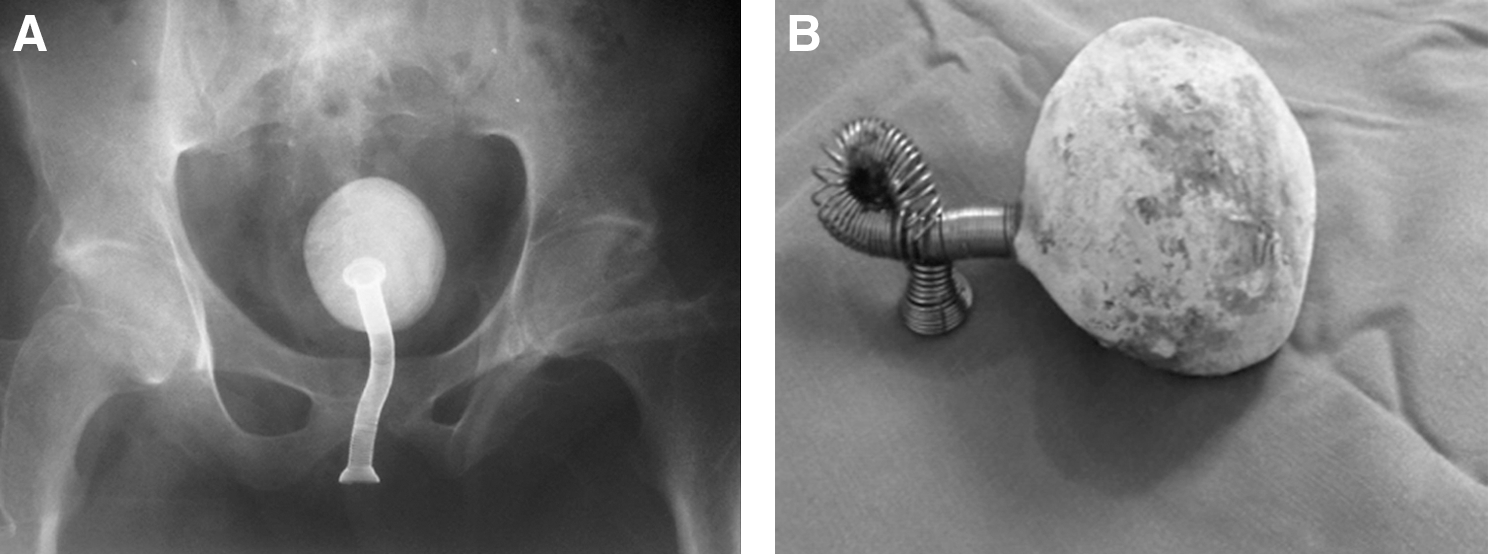
Large stone on Memokath stent before
Discussion
Despite high reported failure rates, urethral stent placement remains popular with SCI patients who are unsure of their choice of bladder management, especially those awaiting a miracle cure and those planning to participate in fertility programs. 3 The patients in this study represent a selected group in a relatively large rehabilitation facility. The average age (37.4 years) represents the age when men are likely to sustain a SCI. No children or adolescents were included in this study because the rehabilitation facility only caters for adults.
The main problem of neuropathic bladder dysfunction after SCI is elevated Pdet. Temporary reduction in bladder outflow resistance is possible with the use of botulinum A toxin injected into the external urethral sphincter. 4,5 This leads to a significant reduction in postvoid RV, but the effect is short-lived. Moreover, it is an expensive form of treatment and because of funding and medical council restrictions, it was not available to the study group. External sphincterotomy using electrodiathermy has been reported to fail in up to a third of cases and may cause erectile dysfunction because of heat injury to the neurovascular bundles. 6
Most injuries in this study group were in the C5–C6 cervical cord region, known to be most commonly affected in cervical spine fractures. Cervical injuries are highly associated with autonomic dysreflexia because of the nature of sympathetic nervous system outflow. The injuries are often incomplete, so even though the highest affected level is recorded, various degrees of function may remain from spinal cord segments lower down, as in the case of someone with a C3 lesion who can still breathe because of some retained C4 function. The low average creatinine level in the study group is likely related to the reduced muscle mass of patients with SCI.
In this study, the two stents that were replaced within a week postoperatively probably represent part of the learning curve. It is more difficult to place stents correctly than is generally appreciated. The three patients who requested stents again after removal at 12, 23, and 36 months indicate at least some degree of patient satisfaction.
Repeated catheter blockage was the most common reason for stent placement. A degree of overlap between the indications existed; for example, severe autonomic dysreflexia from poor bladder emptying could also be classified under high RV as an indication. In such cases, the most prominent indication was noted.
Two patients had a failed external sphincterotomy before stent placement. One of these had a migrated stent, and it was found at cystoscopy that even though the sphincterotomy had failed, enough tissue had been resected to retain the stent only loosely in position. This is interesting, because the dual flange design did not prevent this migration. This finding is in contrast to a study by Pannek and coworkers 7 who found Memokath stents a good second-line treatment option for failed external sphincterotomy in neuropathic bladder dysfunction.
The time from SCI to placing the stent may be important, because the bladder may undergo morphologic changes such as diverticulum formation that may harbor infection. This will affect the duration a foreign body, such as a stent, will be able to remain in situ. In this study, RV after stent placement decreased significantly, as expected. Pdet could not be measured after stent placement, because catheterization may dislodge the stent. The decrease in episodes of autonomic dysreflexia was statistically significant. The seven patients with persisting autonomic dysreflexia may have had other triggers, such as distended bowel, bedsores, or poorly functioning stents.
The fact that 45% of stents were removed at a mean follow-up of 18 months indicates that stent placement is not a permanent solution to neuropathic bladder dysfunction, and it is possible that with time, all stents will have to be removed. Most stents in our study were removed for stone formation or poor bladder drainage. In a report by Low and McRae, 8 19 of 26 (73%) stents had to be removed. Although stents do not generally last longer than 2 years after placement in SCI patients, a case of ongoing successful stent function after 14 years has been reported. 9 Similar results have been reported for external sphincterotomy and urethral stenting. 3,6 Vaidyanathan and colleagues 10 and Soni and associates 11 reported a 100% success rate at 3 to 7 months after stent placement, but long-term follow-up at 108 months showed a 90% failure rate.
The new onset persistent hematuria in one patient in this study is difficult to explain. Except for inflammatory changes at the bladder neck, no obvious source of bleeding was seen at stent removal. Unfortunately, a biopsy was not performed. The new onset autonomic dysreflexia in one patient could possibly be explained by the stent irritating the trigone.
Because approximately 50% of stents had been removed at 20 months (Fig. 2), the group of patients with stents that were in situ for more than 20 months was compared with the group whose stents were removed before 20 months (Table 1). The only statistically significant difference was a smaller RV poststent placement. There was a trend toward significance, however, for time to placing the stent after SCI (31 vs 119 months, P=0.057). This would make sense, because early after SCI, the bladder may still be anatomically normal and reduced RV and bladder pressure may prevent UTI and diverticula formation.
Comparison of the groups with early vs delayed stent placement showed that at a mean follow-up of 18 months (maximum 40 months), the stent survival curves converged (Fig. 3). This indicates that early stent placement (less than 18 months after SCI) compared with delayed stent placement results in substantially better stent survival in the medium term (up to 27 months analyzed, see below), but in the long term (40 months in our study), there is no statistical difference in the stent failure rates.
Comparison of the stents placed less than 18 months vs more than 18 months after SCI showed that at a mean follow-up of 8.9 months (maximum 27 months) and 25 stents, all stents had failed in the group with delayed stent placement, whereas 50% of stents were still in situ in the group with early stent insertion (Fig. 4). This was statistically significant.
The comparative data in Table 2 support the possibility that Memokath urethral stent survival will not be affected in the long term by early vs late stent placement after SCI because nearly all stents with long-term follow-up failed.
The complication of urethrocutanuous fistula in one patient in this study was likely related to poor stent selection, because the stent was protruding into the distal bulbar urethra and perineal pressure could lead to erosion. This patient lived far from the rehabilitation center and did not return for follow-up, which indicates the importance of appropriate patient selection and regular follow-up.
Another application for Memokath stents in SCI has been reported by Gökalp and colleagues, 12 who used stents to bridge acute urethral injuries in five patients on CISC who refused indwelling catheter placement. Only one of five stents migrated, but free drainage was not used. Patients continued performing CISC through the stent. No urethral strictures followed removal of the stents at 3–6 months postinjury.
Agrawal and coworkers 13 reported an 11-year follow-up (with mean follow-up of 16 months) of ureteral stents and had excellent results with only 2 of 74 stents removed for encrustation. This is unlikely to be duplicated in a sphincteric stent where some residual bladder urine may enhance encrustation.
Other forms of temporary urethral stents have also achieved limited success. Gamé and associates 14 used Nissenkorn™ and Diabolo™ stents in 147 patients, with 70% needing alternative treatment over a 10-year period.
In benign prostatic hyperplasia (BPH), Memokath stents have a failure rate of up to 48%. 15 The operative procedure to place the stent in BPH is similar to that in SCI, except that the stent does not traverse the external sphincter.
Conclusion
Memokath stent placement is not a permanent, but good medium term solution to troublesome neuropathic bladder dysfunction after SCI. Early placement after SCI significantly improves the medium term outcome. Stent placement can be seen as a medium/long-term substitute to external sphincterotomy in patients who believe a cure for SCI will be found. At that time, they want to have normal bladder function again without incontinence or ED from an external sphincterotomy. Patient selection is important, and in our series,stent placement was a substitute for external sphincterotomy in what we believed were appropriately selected cases. Early stent placement after SCI may improve long-term stent life, but larger patient numbers are needed to prove this. Low RV after stent placement predicts a positive outcome. Close contact in follow-up is advised to prevent complications. Patient expectations should be realistic about the time a stent can remain in situ, because with time, most stents are likely to fail, but may be replaced should the patient prefer this.
Footnotes
Disclosure Statement
No competing financial interests exist.