
Abstract
Purpose:
The purpose of this study was to introduce a new method for locating the renal artery during retroperitoneal laparoscopic renal surgery.
Patients and Methods:
The medial arcuate ligament (MAL) is a tendinous arch in the fascia under the diaphragm that arches across the psoas major muscle and is attached medially to the side of the first or the second lumbar vertebra. The renal artery arises at the level of the intervertebral disc between the L1 and L2 vertebrae. We evaluate the role of the MAL that serves as an anatomic landmark for locating the renal artery during retroperitoneal laparoscopic renal surgery.
Results:
There is a reproducible consistent anatomic relationship between MAL and the renal artery in 210 cases of retroperitoneal laparoscopic renal surgery. Two main types of the MAL, the “narrow arch” and the “fascial band” types, can be observed.
Conclusion:
MAL can serve as an accurate and reproducible anatomic landmark for the identification of the renal artery during retroperitoneal laparoscopic renal surgery.
Introduction
The medial arcuate ligament (MAL) is a tendinous arch in the fascia under the diaphragm that arches across the psoas major muscle and is attached medially to the side of the first or the second lumbar vertebra. The renal artery arises at the level of the intervertebral disc between the L1 and L2 vertebrae. We introduce the MAL, as a new landmark to facilitate the identification of the renal artery during retroperitoneal laparoscopic renal surgery.
Patients and Methods
Video records of 58 cases of retroperitoneal laparoscopic radical nephrectomy (group A) were reviewed to investigate the anatomic relationship between the MAL and the renal artery. Among these, 32 cases involved left-sided procedures, whereas 26 were right-sided. The operative time involving the time taken for exposure of the renal artery (access to the renal hilum was initiated by developing the plane between the anterior aspect of the psoas major muscle and the posterior aspect of the kidney to the stage where part of the renal artery can be visualized) was recorded.
In the period from March to June 2010, 152 cases of retroperitoneal laparoscopic renal surgeries (group B), including radical nephrectomy in 90, partial nephrectomy in 38, nephroureterectomy in 15 patients, live donor nephrectomy in 5, and simple nephrectomy for nonfunctioning tuberous kidney in 4 patients, were performed. Among these, 72 cases involved left-sided procedures, whereas 80 were right-sided. The MAL was used as an anatomic landmark to guide the process of locating the renal artery, and the operative time for exposure of the renal artery was recorded according to the operation video. The operative time was expressed as a group mean with the standard deviation and compared using the Student t test. The video record was collected from six surgeons, and all six surgeons had performed at least 100 cases of retroperitoneal laparoscopic renal surgery before this study, including radical nephrectomy and partial nephrectomy.
Laparoscopic technique
Under general anesthesia, after placement of a nasogastric tube and a Foley catheter, the patient was positioned in a full lateral decubitus position with the lesion side up. The affected side was overextended by elevating the lumbar bridge of the operative table, and the space between the costal margin and the iliac crest was maximally exposed. A three-port finger dissection and the balloon-dilation retroperitoneal laparoscopic approach were used, as described previously. 1 Briefly, a 2-cm-long skin incision was made below the 12th rib in the posterior axillary line, the peritoneum was pushed forward using the index finger, and balloon dilation was performed to create the retroperitoneal space. Under the guidance of the index finger, a 5- or 12-mm trocar was inserted under the subcostal margin in the anterior axillary line, and a 10-mm trocar was placed above the iliac crest in the midaxillary line for the laparoscope. A third trocar was placed across the 2-cm incision.
The retroperitoneal fat tissue outside the Gerota fascia was dissected near the diaphragm using a harmonic scalpel until it prolapsed downward to the iliac fossa. Some anatomic landmarks, including the Gerota fascia, peritoneal reflection, and psoas muscle, could be recognized.
Access to the renal hilum was initiated by developing the plane between the anterior aspect of the psoas major muscle and the posterior aspect of the kidney by sharp dissection using a harmonic scalpel (Fig. 1A). The psoas muscle was exposed up to the diaphragm. A white tendinous arch in the fascia that covered the upper part of the psoas major muscle was recognized, which was the MAL of the diaphragm (Fig. 1B). Medially and deeply, by probing along its contours, the MAL led to the root of the renal artery (Fig. 1C). The kidney was retracted ventrally and anteriorly with laparoscopic forceps. After sharp dissection of the fatty or connective tissues around the root of the renal artery, the renal artery could be identified (Fig. 1D), and further mobilization was achieved by sharply dissecting it using a harmonic scalpel and placing a right-angled forceps circumferentially around it. The renal vein was exposed by ventral and deep dissection under the renal artery.
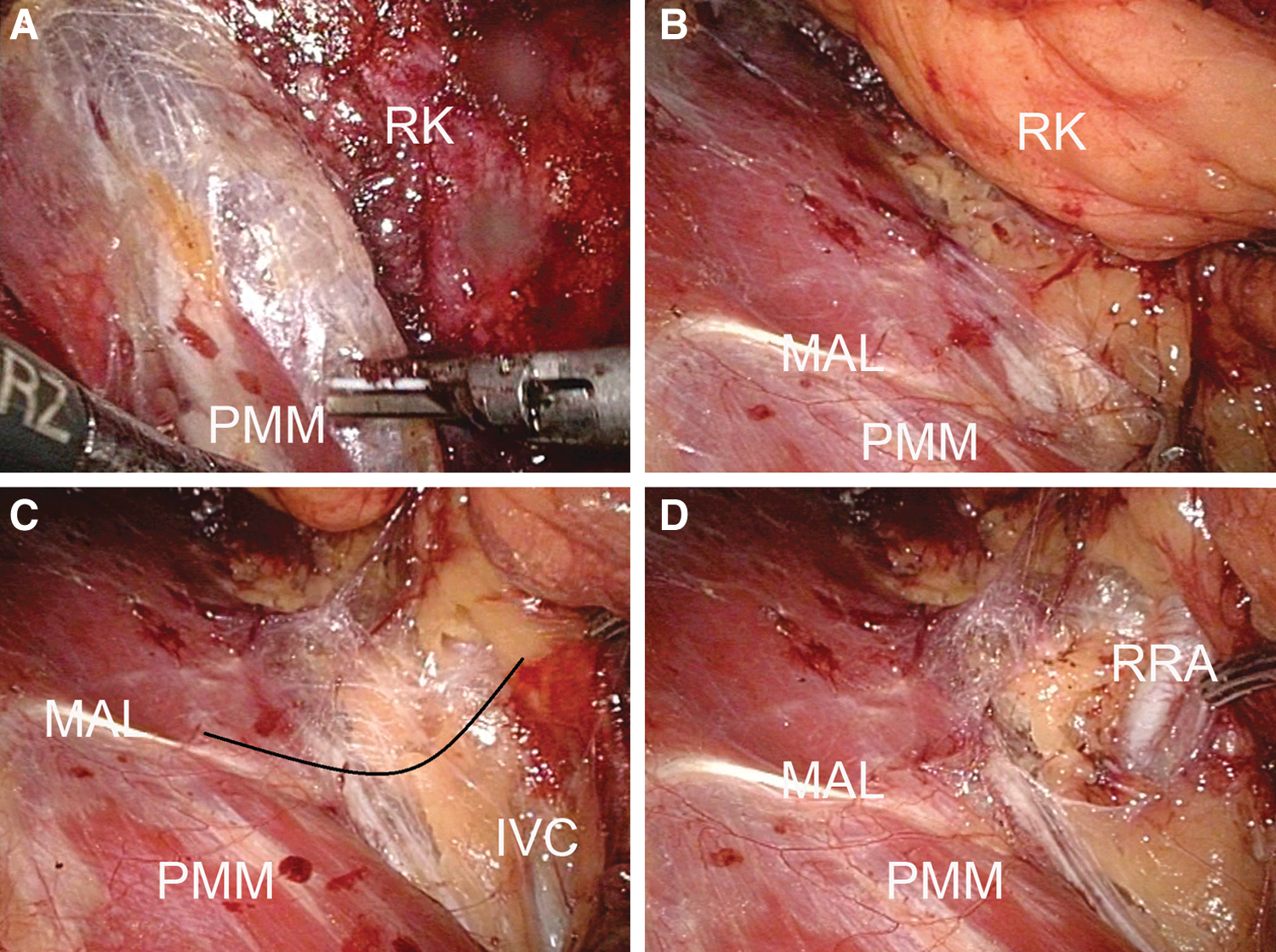
The operative steps of right retroperitoneal laparoscopic renal surgery highlight the use of the medial arcuate ligament as an operative anatomy to locate the renal artery. PMM=psoas major muscle; RK=right kidney; MAL=medial arcuate ligament; IVC=inferior vena cava; RRA=right renal artery.
Results
There was a reproducible consistent anatomic relationship between the MAL and the renal artery. When the kidney was retracted ventrally and anteriorly with laparoscopic forceps during the operation, the contours of the MAL and the renal artery largely showed mirror symmetry (Fig. 2). Two main types of the MAL, the “narrow arch” (Fig. 2A) and the “fascial band” types, could be differentiated (Fig. 2B). The narrow arch type of MAL accounted for 71.4% (150/210), whereas the fascial or tendinous band accounted for 28.6% (60/210) of the cases.
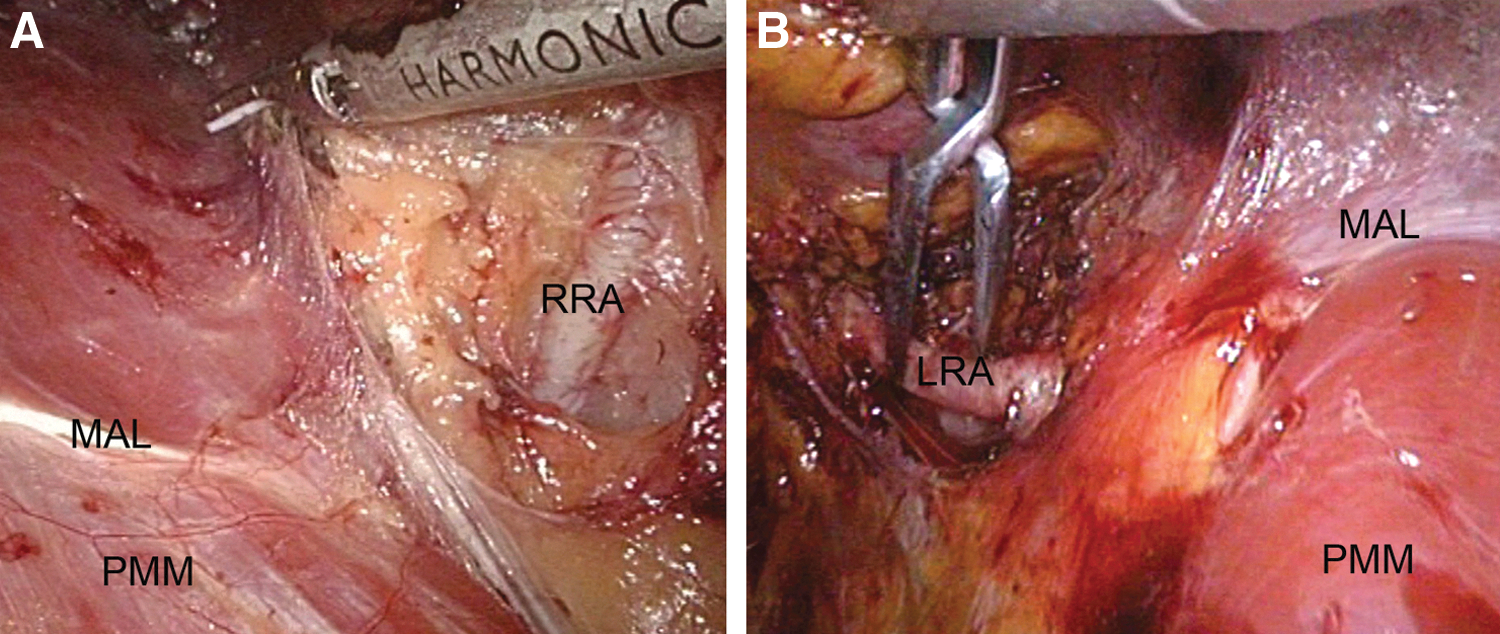
Two types of the medial arcuate ligament (MAL):
The two groups were comparable with regard to age, sex, affected side, and body mass index (22.4 vs 23.3). Three patients had lymphadenopathy around the renal hilum in group A and 10 patients in group B. The mean operative time needed for exposure of the renal artery in group A was 9.2±2.2 minutes (range 5–16 min) and 5.3±1.6 minutes (range 3–9 min) in group B, respectively. The mean operative time needed for exposure of the renal artery in group B was significantly shorter than group A (P<0.001).
Discussion
Since its original description by Gaur 2 in 1992, retroperitoneal laparoscopy has gradually gained acceptance in the field of urologic surgery. The techniques used for retroperitoneal laparoscopic renal surgery have evolved into a standardized approach that has become the preferred method in many medical centers.
Without the use of tactile feedback, one major concern during laparoscopic renal surgery, such as simple nephrectomy, radical nephrectomy, nephroureterectomy, partial nephrectomy, live-donor nephrectomy, and renal pedicle lymphatic disconnection for chyluria, is control of the renal hilum. Compared with transperitoneal laparoscopy, identifying the renal artery through a retroperitoneal approach is usually straightforward because the artery is superficial. Usually, dissection of the renal artery is aided by observation of the pulsations of the renal artery. The pulsations of a fat-covered renal artery, however, are not easy to identify, 3 especially in obese patients or in patients with dense adhesions or enlarged lymph nodes near the renal hilum. Locating the renal artery may be a confusing and challenging step in these patients, not only for novices, but also for experienced hands.
Gao and associates 4 introduced a five-step method to identify the renal vessels during retroperitoneal laparoscopic renal surgery. Current methods of vessel identification in laparoscopy, however, are highly subjective (limited to visual cues) and depend largely on the surgeon's experience. Some authors have advocated the use of a Doppler probe to facilitate the identification of renal artery during the laparoscopic renal surgery. 5 Apart from the unpopular use of a laparoscopic Doppler probe, the role of Doppler ultrasound technology in laparoscopic renal surgery through the retroperitoneal approach still remains unclear. An accurate and reproducible landmark technique (more objective) is essential and remains to be described.
The MALs (also termed the medial lumbocostal arch) are thickenings of the anterior layer of the thoracolumbar fascia spread over the superior parts of the psoas major muscles. Each ligament forms a fibrous arch that runs anteriorly from the crus of the diaphragm to the psoas major muscle. It is attached to the side of the body of the first or second lumbar vertebra; laterally, it is fixed to the front of the transverse process of the first and, sometimes additionally, to that of the second lumbar vertebra. The renal arteries branch off from the lateral aspect of the abdominal aorta at the level of the L1 vertebra 6 or at the intervertebral disc between the L1 and L2 vertebrae. 7 Each renal artery is directed across the crus of the diaphragm to form an approximate right angle with the abdominal aorta. The MAL and the renal artery have a close anatomic relationship. In fact, renal-artery entrapment by the MAL, resulting in resistant hypertension that can be diagnosed by multidetector CT angiography, has been reported. 8
In our study, the MAL was exposed clearly in all the patients. Although the narrow arch type of MAL was more obvious than the fascial band type, the anatomic relationship between the two types of MAL and the renal artery was confirmed. Under the guidance of the MAL, the renal artery can be located quickly and mobilized safely even in obese patients or in patients with dense adhesions or enlarged lymph nodes located near the renal artery. The mean operative time involved in the exposure of the renal artery in group B was reduced by about 50% compared with that of group A. More importantly, with this new anatomic landmark, surgeons will have more confidence in handling complicated cases.
A surgeon's “best friend,” the psoas major muscle, is a constant anatomic landmark in retroperitoneal laparoscopic surgery. Can the MAL, an arch covering the psoas major muscle, be his or her next friend? To our knowledge, this is the first report of MAL being used as an anatomic landmark in retroperitoneal laparoscopic surgery. Additional studies will be essential to justify its true benefits.
Conclusion
The MAL can be used as a direct, easy-to-identify, and constant anatomic landmark for the identification of the renal artery during retroperitoneal laparoscopic renal surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.