
Abstract
Purpose:
To assess the utility of attenuation coefficients as predictors of surgical outcome after a single flexible ureteroscopy (URS) with holmium laser lithotripsy. Many reports indicate that the efficacy of extracorporeal shockwave lithotripsy (SWL) can be predicted by the target's radiofrequency attenuation, measured as Hounsfield units (HUs) on noncontrast CT (NCCT). Studies of flexible URS, however, have not assessed the predictive value of attenuation coefficients on NCCT.
Patients and Methods:
Patients with renal stones who were treated by flexible URS with holmium laser lithotripsy between December 2009 and October 2011 at a single institute were retrospectively evaluated. Stone-free (SF) status was determined by kidneys-ureters-bladder (KUB) radiography at postoperative month 3. Correlations of possible predictors with SF status were analyzed using a logistic regression model. The comparison between groups with low and high HUs was examined using the Mann-Whitney U test.
Results:
There were 219 eligible procedures. According to the logistic regression model, the maximum attenuation coefficient (P=0.105) and average attenuation coefficient (P=0.175) did not significantly, independently predict SF status. Fragmentation efficiency was significantly different between cases with low and high attenuation coefficients (P=0.001). In groups with less than 20.0-mm diameter stones, overall operative time (P<0.001 and P=0.001) and the time from starting fragmentation (P<0.001 and P=0.002) were significantly high in both attenuation groups. In groups with stones greater than 20.0 mm diameter, the two definitions of operative time revealed no differences between the low and high attenuation groups. The retrospective study design was the major limitation of this study.
Conclusions:
We found that both the maximum and average attenuation coefficients on NCCT are significantly related to the fragmentation efficiency. In addition, this study showed that, in patient groups with stone a burden <20.0 mm in diameter, both the maximum and average attenuation coefficients were significantly predictive of operative time.
Introduction
Many previous reports, however, indicate that the efficacy of extracorporeal shockwave lithotripsy (SWL) is dependent on target attenuation coefficients on NCCT. 6 –8 In vitro studies suggest that the attenuation coefficients of calculi measured in HUs on NCCT may predict the ability to fragment urinary stones. 9 This hints that attenuation on NCCT could also predict stone-free (SF) rates after ureteroscopy (URS). Studies of flexible URS, 10 –14 however, have not assessed the predictive value of attenuation coefficients.
In this study, we retrospectively investigated the utility of attenuation coefficients as measured by HUs as a possible predictor of surgical outcome after single flexible URS with holmium laser lithotripsy for the treatment of patients with intrarenal stones. To our knowledge, this is the first study to investigate the predictive value of attenuation coefficient on the outcome of URS.
Patients and Methods
We retrospectively analyzed 310 procedures using a flexible ureteroscope for removal of intrarenal stones, performed between December 2009 and October 2011. The inclusion criteria and exclusion criteria are shown in Table 1. To minimize the error of volume averaging, cases in which the primary stone was ≤5 mm in diameter were excluded. 5,7,15 Of these 310 procedures, 91 were excluded from the study, and there were 219 eligible procedures.
KUB=kidneys, ureters, and bladder; NCCT=noncontrast computed tomography; URS=ureteroscopy.
The indications for urolithiasis treatment in our hospital are as follows: We generally recommend as a first-line treatment percutaneous nephrolithotripsy for renal stones >20 mm diameter and SWL or medical expulsive therapy for urinary stones <10 mm diameter. For all patients, URS was offered as a first- or second-line treatment for remaining urinary stones. The final decision about the treatment was made by the patients.
This study was approved by the Ethics Review Board of Ohguchi East General Hospital. All patients provided written informed consent for their data to be used for research purposes.
Patients were given intravenous preoperative antibiotics. Before starting URS, the patient was placed in the dorsal lithotomy position and prepared and draped in sterile fashion while under anesthesia. A 22.5F cystoscope was inserted into the bladder through the urethra, allowing visualization of the ureteral orifice. This was cannulated with an open-ended 5F catheter and a 0.038-inch hydrophilic guidewire. To directly visualize the intraureteral space, a 6/7.5F or 8/9.8F semirigid ureterorenoscope (Wolf,™ Knittlingen, Germany) was passed over a guidewire using fluoroscopic guidance until it reached the proximal ureter or renal pelvis. This semirigid ureteroscopic procedure made dilation of the ureteral orifice and retrograde ureteropyelography unnecessary.
Next, a ureteral access sheath (12/14F or 14/16F, Cook Medical, Bloomington, IN or 11/13F or 13/15F, Boston Scientific, Natick, MA) was placed, and a flexible URS (Flex-X2,™ Storz, Germany, or Olympus P-5,™ Olympus, Tokyo, Japan) with 200 μm holmium laser lithotripsy was performed. We used a holmium laser machine set at an energy level of 0.5–2.0 J and a rate of 5 Hz. When basketing was deemed necessary, we used a 1.9F zero-tip nitinol stone basket (Boston Scientific) and/or a 1.5F N-Circle nitinol tipless basket (Cook Medical).
A Double-J stent was placed in all patients after endoscopy to reduce the risk of complications, and the bypass was removed 2 to 4 weeks postoperatively when we were certain that the bypass was no longer necessary. If the operative time exceeded 120 minutes, we stopped and placed a Double-J stent to reduce the occurrence of perioperative complications, even if large stone fragments remained.
The stones were viewed with helical NCCT (Aquilion 64; Toshiba, Tokyo, Japan) (120 kVp; 300 mA; 0.5–1.0 s; collimation 5 mm; pitch 1:1), and a standard renal stone viewing protocol that uses soft-tissue settings (width 350/length 50) was used. A region of interest was drawn using the center slice of the primary stone on axial reconstructions. The maximum and average attenuation coefficients were measured by placing a freehand region of interest along the inner contours of the renal stone margins. 7,16
The maximum diameter was evaluated on plain kidneys, ureters, and bladder (KUB) radiography. The stone volume was obtained from measurements on three-dimensional reconstructions of the stone, using 5-mm axial and 3.5-mm reconstructed coronal NCCT. We used the following formula to calculate stone volume: Length×width×height×π×1/6. The stone maximum diameter on KUB and stone length, width, and height on NCCT were determined using digital calipers (SYNAPSE-PACS Software Program System, Fujifilm, Tokyo, Japan). The presence of hydronephrosis and lower pole calculi and the number of stones were also determined from the preoperative NCCT. All NCCT scans were interpreted by a single urologist (HI).
Plain KUB radiography was performed at postoperative month (POM) 3 in all cases to assess the presence of stones. Stone status, the primary outcome measure, was judged in all cases by the same person (HI). SF status was defined as no detectable stones on KUB radiography.
Data were analyzed using the SPSS software package (SPSS, Chicago, IL). To evaluate the relationship between SF status and the two attenuation measurements, a logistic regression model was used. The primary end point was set at SF at POM3.
The cutoff point for the cumulative stone diameter was set at 20.0 mm. 10 –12 Maximum and average attenuation coefficients were treated as continuous variables. The operators were six urologists, divided equally into experienced operators (having performed ≥50 URSs) and inexperienced operators (having performed <50 URSs).
A logistic regression model was used to perform univariate and multivariate analysis. A P value of 0.15 was used as the criterion for determining variable entry and removal from the multivariate analysis. All statistical tests were two-sided and were considered to be statistically significant at P<0.05.
Next, to assess the predictive value of target attenuation on URS results in detail, patients in the SF group were divided into two groups using the median value of maximum and average attenuation coefficients: The low and high attenuation groups. Several factors were examined using the Mann-Whitney U test: Operative time, time from starting fragmentation, and fragmentation efficiency. The time from starting fragmentation was defined as operative time from starting fragmentation to the end of the procedure. The parameter mainly consisted of the periods of fragmentation and stone removal. Fragmentation efficiency at URS was defined by the volume of laser use (J)/stone volume (mm3) in this study.
Results
There were 219 eligible procedures. Of these, 212 were performed under general anesthesia and 7 under spinal anesthesia. A ureteral sheath was used in all procedures.
Table 2 shows a comparison of the patients' demographic data and perioperative surgical outcomes according to SF status vs non-SF status at POM3. SF rate at POM3 after the first URS procedure was 59.4% (130/219 cases).
Mann-Whitney U test; bchi-square test.
SF=stone free; POM=postoperative month; HU=Hounsfield units; SWL=shockwave lithotripsy.
There were significant differences between the SF status and non-SF status groups in the following parameters: Number of stones (P<0.001), presence of lower pole calculi (P<0.001), cumulative stone diameter (P<0.001), volume (P<0.001), overall operative time (P<0.001), time from starting fragmentation (P<0.001), and amount of laser use (P<0.001). Both the maximum attenuation coefficient (P=0.233) and average attenuation coefficient (P=0.253) failed to predict the SF differences (Table 2).
One major intraoperative complication occurred—a ureteral perforation resulting in retroperitoneal extravasation of urine in one patient. Minor complications after treatment included high-grade fever in 15 patients. All were treated conservatively.
Long-term complications such as ureteral stricture formation occurred in two patients. One patient was treated with ureteral balloon dilation and has had a successful outcome. Ureteral balloon dilation failure in the other patient was treated with placement of a permanent Double-J stent.
Univariate analysis identified several variables significantly associated with non-SF at POM3 (P<0.15), including number of stones (P=0.001), cumulative stone diameter (P<0.001), presence of lower pole calculi (P<0.001), and maximum attenuation coefficient (P=0.105) (Table 3). Average attenuation coefficient (P=0.175) was not predictive of SF status (Table 3). Including the significant variables in the univariate analysis in the multivariate analysis revealed cumulative stone diameter (P<0.001) and presence of lower pole calculi (P=0.033) to be independent predictors of SF status. Table 3 shows the association of each of the categorical variables with SF status.
HR=hazard ratio; CI=confidence interval; HU=Hounsfield unit; SWL=shockwave lithotripsy.
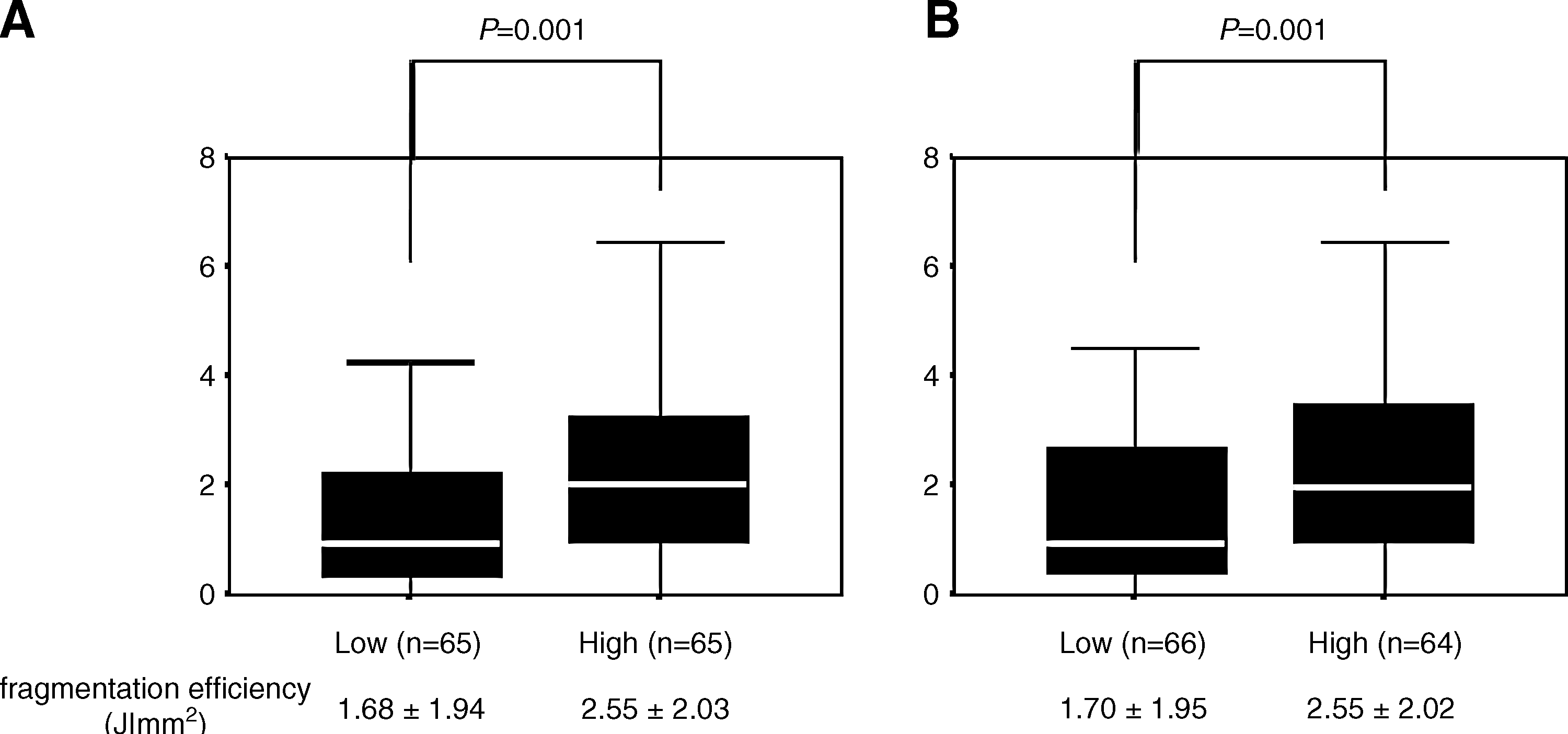
The medians of maximum and average attenuation coefficients in all patients were 1389 HU (range 301–1957 HU) and 1061 HU (range 203–1683 HU), respectively. We compared fragmentation efficiency between patient groups with low and high attenuation coefficients (Fig. 1) and found significant differences between the groups in both maximum and average attenuation coefficients (P=0.001). Furthermore, in groups with stones <20.0 mm in diameter, overall operative time (P<0.001 and P=0.001) and time from starting fragmentation (P<0.001 and P=0.002) were significantly high in the high maximum and high average attenuation groups compared with the low maximum and low average attenuation group (Table 4). In patients with >20.0-mm stones, the two definitions of operative time revealed no differences between the low and high attenuation groups (Table 4).
Mann-Whitney U test.
Discussion
Recent studies reported that attenuation coefficients, measured as HUs, on NCCT have limited value as a predictor of stone composition 17 or response to SWL treatment. 6 –8 No studies of flexible URS have investigated the predictive utility of attenuation coefficients obtained from NCCT, but it is a clinically meaningful issue to determine whether the attenuation coefficients on pretreatment NCCT have clinical utility for predicting successful outcomes of URS. Our goal was to address this issue by determining the priority of maximum and average attenuation coefficients in terms of their clinical utility. Our results revealed the importance of pretreatment measurement of attenuation coefficients on NCCT in predicting the success of URS.
In our logistic models, we found that predicting factors for SF at URS are cumulative stone diameter and presence of lower pole calculi (Table 3). This finding is consistent with those of previously published reports. 18,19 On the other hand, neither the maximum nor average attenuation coefficient was an independent parameter. In univariate analysis, however, the maximum attenuation coefficient showed possible correlation with efficacy of URS (Table 3). The average attenuation coefficient also revealed a similar possible utility as a predictive parameter of URS despite lack of statistical power (Table 3).
In this study, we found that both the maximum and average attenuation coefficients on NCCT are significantly related to the fragmentation efficiency. Fragmentation efficiency would represent stone fragility at URS with holmium laser lithotripsy and be strongly associated with pure operative time needed to break the stones into the desired fragment size. Therefore, this result indicates that we can predict these factors preoperatively from estimating both the maximum and average attenuation coefficients. In addition, we assessed the attenuation coefficients as direct predictors of operative time. Preoperative prediction of operative time enables us to recommend the most sufficient treatment method to patients, predict the need for additional sessions of URS, and avoid surgical complications.
This study showed that, in patient groups with a stone burden <20.0 mm in diameter, both the maximum and average attenuation coefficients were significantly predictive of operative time. Neither the maximum nor average attenuation coefficient, however, was correlated in patients with a stone burden >20.0 mm diameter. This result suggests that operative time can be predicted directly from pretreatment measurement of the attenuation coefficient on NCCT in patients with lower stone burden, especially when <20.0 mm in diameter.
Attenuation coefficients could also predict the other stone fragmentation factors. In procedures for patients with higher stone burden, removing the stone had more influence on operative time. This is in part because, in patients with higher stone burden, attenuation coefficients of the target could not provide accurate information regarding operative time.
Although comparisons of the clinical utility of maximum and average attenuation coefficients were not reported previously, they almost equally predicted with surgical outcome in this study. Prediction of SF status after URS could provide one advantage of the maximum attenuation coefficient over the average attenuation coefficient (Table 3). This result is noteworthy because almost all previous reports have evaluated only average attenuation coefficient as an outcome predictor. 6 –8 There are few reports estimating the impact of the maximum attenuation coefficient as an outcome predictor. The region of maximum attenuation is likely easier to include in a region of interest and demonstrates much less variability because the surrounding region of interest is thrown out, whereas the entire region of interest is included in the average attenuation coefficient. 5,7 The present study proved that the clinical utility of the maximum attenuation coefficient was absolutely as high as or more useful than the average attenuation coefficient.
Previous studies reported that the average attenuation coefficient cutoff point as a predictor of SWL failure was set from 750 to 1000 HU and varied a little from study to study. 6 –8 In this study, we set the overall median value of each attenuation coefficient (maximum 1389 HU and average1061 HU) as the cutoff point for each group, and these cutoff points proved appropriate because they were effective as predictors of surgical outcome (Fig. 1; Table 4). These findings suggest that the cutoff points for URS are similar to those for SWL.
Several recent reports have shown that novel CT methods such as bone windows and micro-CT are useful tools for evaluating urinary stones. 1 –3 This study, however, suggested that, at least in the preoperative assessment of URS, measured attenuation coefficients on NCCT using standard soft-tissue windows could provide enough information to help us in clinical practice.
The strong correlation between stone composition and attenuation coefficient were often reported. 6 –8,15,16 In addition, there are a few reports that have looked at lithotripsy efficiency as it varies by stone composition. 20,21 In terms of rationale of URS, we also presumed that stone composition was a stronger indicator of laser lithotripsy time than attenuation coefficient. The correlation between stone composition and laser lithotripsy time should be evaluated in the immediate future.
There are inherent limitations to this study. Because of its retrospective design and nonblinded interpretation of CT scans, confounding factors and measurement bias cannot be reduced as much as they could be in prospective, randomized studies. Another limitation of the study was that the attenuation coefficients obtained from NCCT with wide slices were likely less accurate, especially in the assessment of small stones. 5,7,15 The error of volume averaging was not considered in the present study. 5,7,15 Nonetheless, we excluded primary stones <5 mm in diameter that may have influenced the outcome to try to offset this. The involvement of only a single medical center was also a limitation, and additional studies involving multiple centers are warranted.
Conclusions
We demonstrate the efficacy of measuring attenuation coefficients before URS. In this study, we found that both the maximum and average attenuation coefficients on NCCT are significantly related to the fragmentation efficiency. In addition, this study showed that, in patient groups with a stone burden <20.0 mm in diameter, both the maximum and average attenuation coefficients were significantly predictive of operative time.
Footnotes
Acknowledgments
All authors participated in the design and conduct of the study. All authors reviewed and approved the final version of the manuscript.
Disclosure Statement
No competing financial interests exist.