
Abstract
We describe flexible ureteroscopy-directed retrograde nephrostomy access using a puncture wire to achieve renal access. This is a natural extension of modern retrograde intrarenal surgical techniques and a modernization of the original Lawson technique for retrograde nephrostomy tract creation. In appropriately selected patients, this approach is safe and permits reduced radiation exposure. We believe this technique is easy to learn and may overcome the difficult learning curve of antegrade nephrostomy techniques faced by urologists who have not undergone subspecialty training in endourology.
Introduction
Retrograde nephrostomy access was first described by Hunter and associates 15 in 1983 and subsequently commercialized into the Lawson Kit (Cook® Medical). Published series of this technique reported a rapid learning curve and minimal complication rate. 16 –20 In 1989, Dr. Larry C. Munch reported passing the Lawson puncture wire through the operating channel of a flexible ureteroscope. 21 More recently, two groups reported on their experience with this technique. 22,23
We herein report our experience at the Detroit Medical Center with ureteroscopy-assisted retrograde nephrostomy for percutaneous nephrolithotomy (PCNL). Further, we describe our technical procedures and coaxial wire exchange system, which we believe further refines this technique.
There are several benefits to this approach compared with antegrade access. First, this procedure applies flexible ureteroscopy skills held by most urologists. Second, calix selection is aided by direct ureteroscopic visualization of caliceal and infundibular relationship to renal pelvis, ureter, and stone. 24 Third, “through and through” access is achieved immediately. This obviates the often difficult step of separately steering a wire down the ureteropelvic junction. In addition, this secures the nephrostomy wire outside of the urethra, potentially obviating the need for a separate safety wire 19 as its chance of being dislodged is minimal. Finally, this technique permits advancement of the nephrostomy balloon dilator under direct vision with the flexible ureteroscope, thereby reducing radiation exposure. This is performed in the modified lithotomy position, which is more intuitive and less cumbersome than performing ureteroscopy in the prone position. 7
Eligibility/case planning
Flank anatomy
The CT scan is reviewed carefully to ensure presence of an “empty flank”—a subjective assessment of a clear, open path between kidney and flank skin without intervening organs: eg, liver, spleen, pleura, and bowel. This evaluation was formalized by Prassopoulos and colleagues 25 in 1990 by drawing straight lines from (I) the posterior renal margin, and (II) the anterior-lateral aspect of the vertebral body through the renal hilum. 26 To qualify for a retrograde approach, the flank must be free of intervening structures posterior to both of these lines. We use Prassopoulos line II for our review (Fig. 1). Figure 2 illustrates a patient eligible for retrograde puncture nephrostomy based on these criteria. CT scan evaluation of the flank must consider whether lower pole, midpolar, or upper pole access is contemplated.
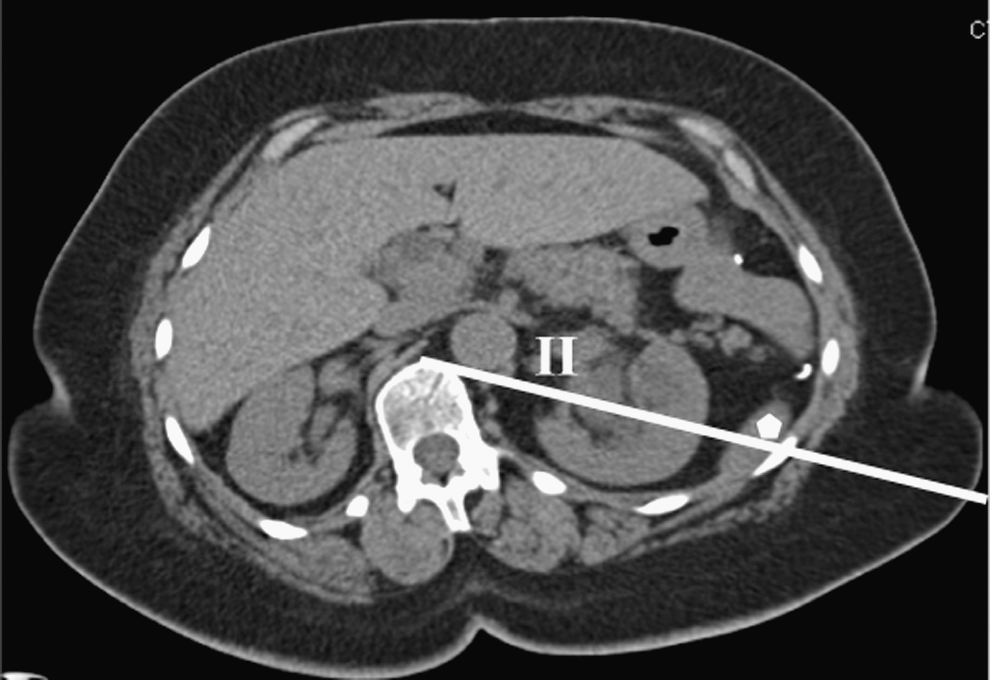
Prassopoulos line II transects spleen tip (dot), rendering patient ineligible for retrograde puncture nephrostomy.

“Empty” flank, suitable for retrograde nephrostomy puncture.
Caliceal anatomy
Retrograde pyelography facilitates selection of the calix for puncture. We performed preoperative retrograde pyelography and stent placement, although this imaging can be obtained at the time of PCNL. On the retrograde study, the position of the calices is considered in relation to the 12th rib, and this information is integrated with the CT scan images in axial and ideally coronal reconstruction views. In general, we prefer a midpolar posterior calix, which provides good access to most stones. We do not perform CT urography because of concern regarding excessive radiation exposure.
Feasibility of lower pole punctures depends primarily on the ureteral-infundibular angle. When this angle is acute, the puncture wire is often deployed at an angle that is too caudad, creating an unacceptably long puncture wire tract (discussed below in “Puncture wire trajectory” section). In these cases, we consider performing a midpolar puncture and then access the stone using a flexible cystoscope, or else we perform an antegrade puncture.
Our primary consideration with upper pole punctures is the location of adjacent organs which can be reasonably assessed after careful review of retrograde pyelography in relation to the 12th rib and CT scan review.
Stone anatomy
We perform flexible ureteroscopy under pressure irrigation. We have found that this adequately distends the renal pelvis around large stones, usually permitting easy advancement of our ureteroscope. Distensibility of infundibulae and calices is relatively limited, however, and stones filling these spaces may need laser lithotripsy to permit access to the calix. Although this will add time to the procedure, we have not found this prohibitive. In one case, however, we did select a calix other than a stone-bearing calix to simplify and speed our access procedure. We believe this procedure can be successfully performed for staghorn calculi. Care must be taken not to advance the flexible ureteroscope with force past a spiculated, rough stone, as this can damage the ureteroscope.
Obesity
We have found this procedure more difficult in obese patients. Positioning of obese patients in the modified lithotomy position is slightly more difficult as is identifying the puncture wire delivery at the flank. The kidney-to-flank distance is greater in these patients, and we thus require a nearly horizontal puncture wire trajectory to minimize tract length. This can limit caliceal selection, which must be considered during case planning.
Technique
Set-up/patient position
After induction of general anesthesia, the posterior axillary line is marked (Fig. 3). The patient is placed in the modified lithotomy position with yellow-fin stirrups and gentle elevation of ipsilateral hips and shoulders with folded sheets, causing the flank to be elevated and exposed. The patient is carefully positioned at the lateral edge of the bed to ensure adequate range of motion of the nephroscope during PCNL. We pad the peroneal nerve on the lateral aspect of the contralateral leg and secure the patient in position with tape. All patients receive preoperative antibiotics and sequential compression stockings for deep vein thrombosis prophylaxis.
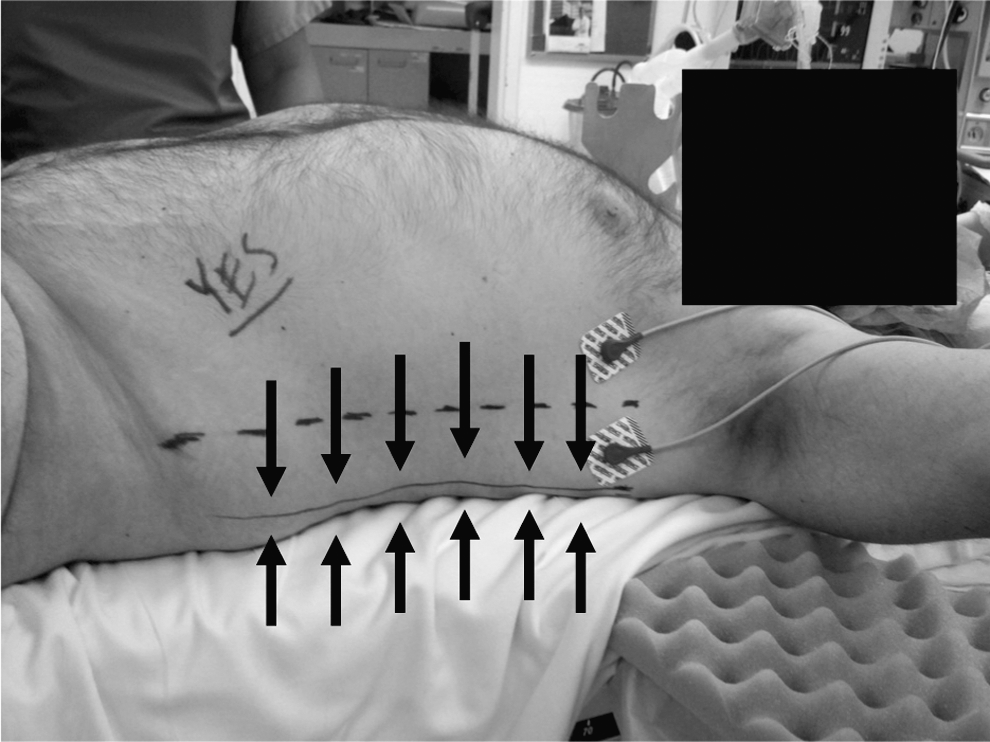
Posterior axillary line marked before positioning patient.
Ureteroscopy setup
A ureteral access sheath is placed with a second wire alongside the access sheath.
Puncture wire ensemble
The puncture wire is a 145 cm, 0.017″ diameter stainless steel wire with a sharpened tip (Fig. 4). During advancement through the ureteroscope working channel, the sharp tip is positioned inside the protective sheath, thus preventing damage to the ureteroscope operating channel. After the puncture wire and sheath emerge from the working channel, they are unlocked in relation to each other by opening the pin-vise lock that relates the two, permitting advancement of the exposed puncture wire.

Sharp puncture wire emerging from protective sheath.
The outer diameter of the protective sheath is 3.0F. This diameter limits irrigation flow through the working channel. To optimize irrigation and visualization while positioning our ureteroscope in our selected calix, we first access our selected calix and only then introduce the puncture wire ensemble through our ureteroscope working channel. Advancement of our ensemble has the same “feel” as advancing a stone basket, passing easily through all but the most acute scope-tip angles; the wire tip is protected by its sheath and thus does not damage the working channel under most circumstances. For calices at sharp angles, we advance our ureteroscope to the calix, back off slightly, advance our puncture wire ensemble, and then readvance the ureteroscope into the calix. We have not experienced significant loss of deflection of the flexible ureteroscope tip because of the wire assembly.
Puncture wire trajectory
After positioning our ureteroscope tip in our selected calix, anterior-posterior fluoroscopy is performed to establish the cephalad-caudad direction of projected puncture wire tract (Fig. 5). It is essential to aim for a straight lateral or less-than 30 degrees caudad trajectory for the puncture wire to minimize the puncture wire tract length (Fig. 6). Oblique fluoroscopy is then performed to evaluate the anterior-posterior directionality of the projected nephrostomy tract. We aim for a posterior direction (Fig. 7) to achieve skin puncture at or behind the posterior axillary line. Once deployed, the puncture wire retains its trajectory set by the direction of the ureteroscope tip.
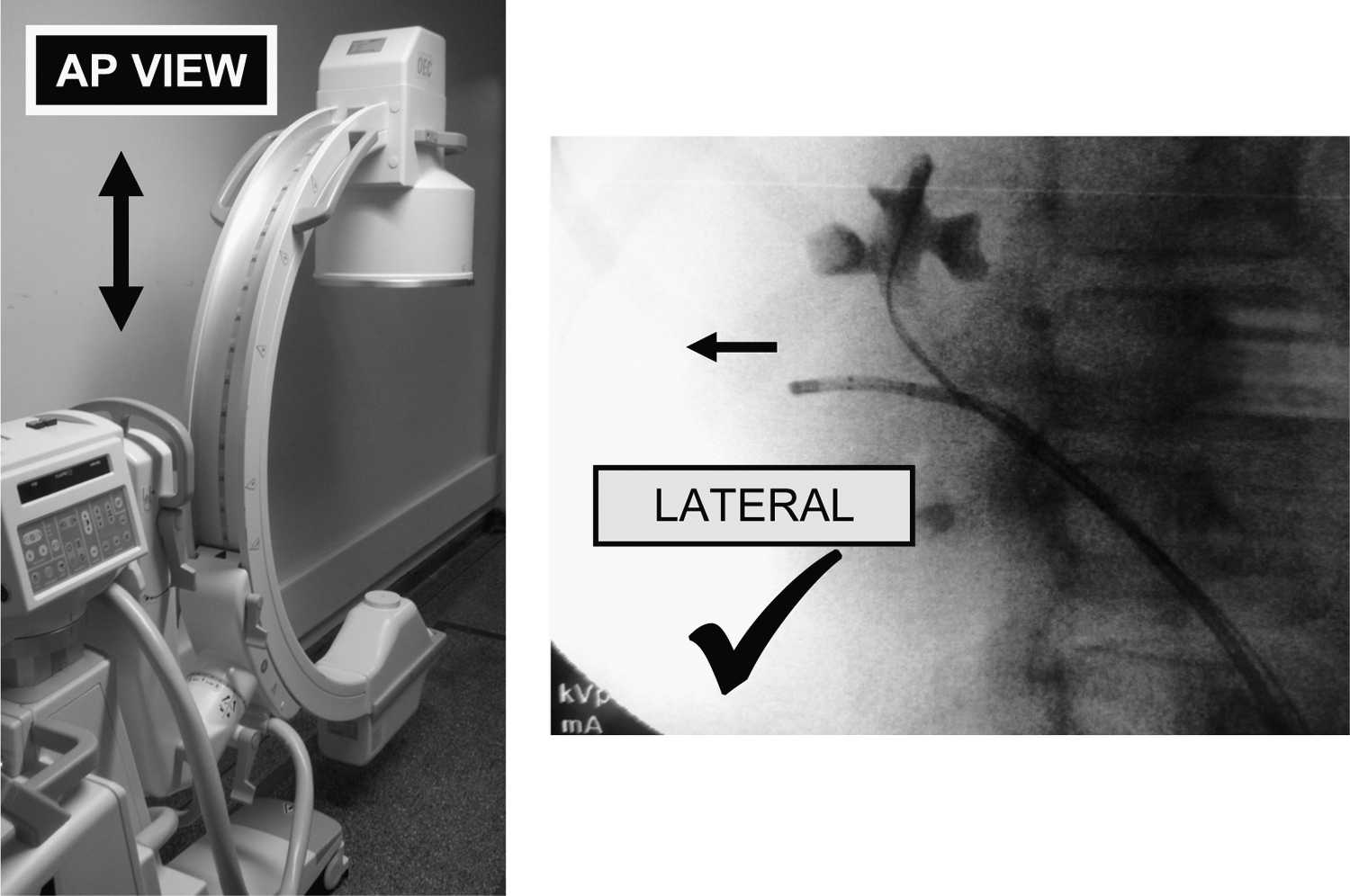
C-arm in anterior-posterior position; confirms lateral trajectory for puncture wire.
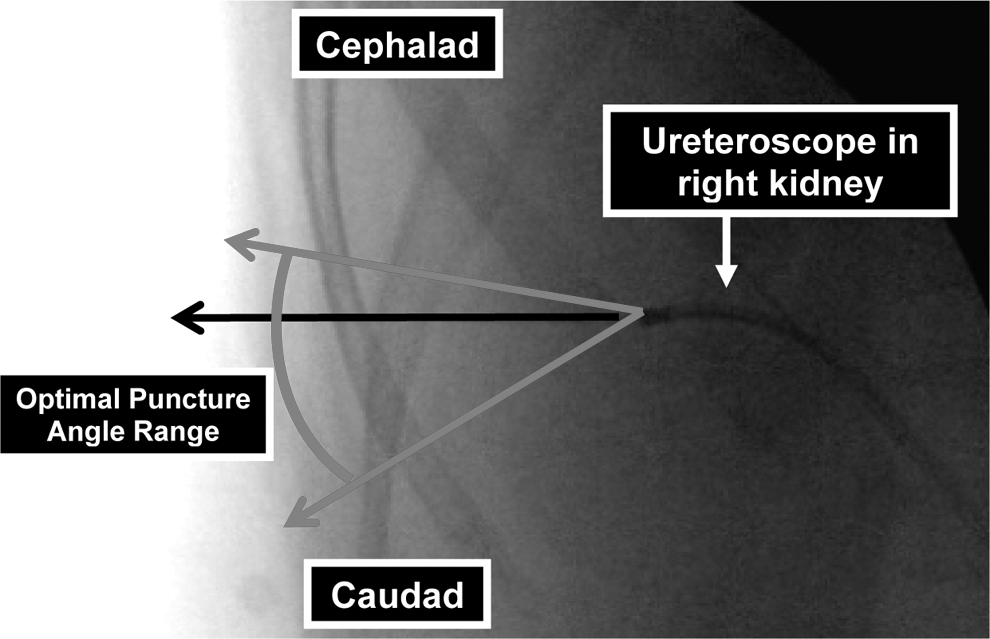
Optimal puncture angle range.
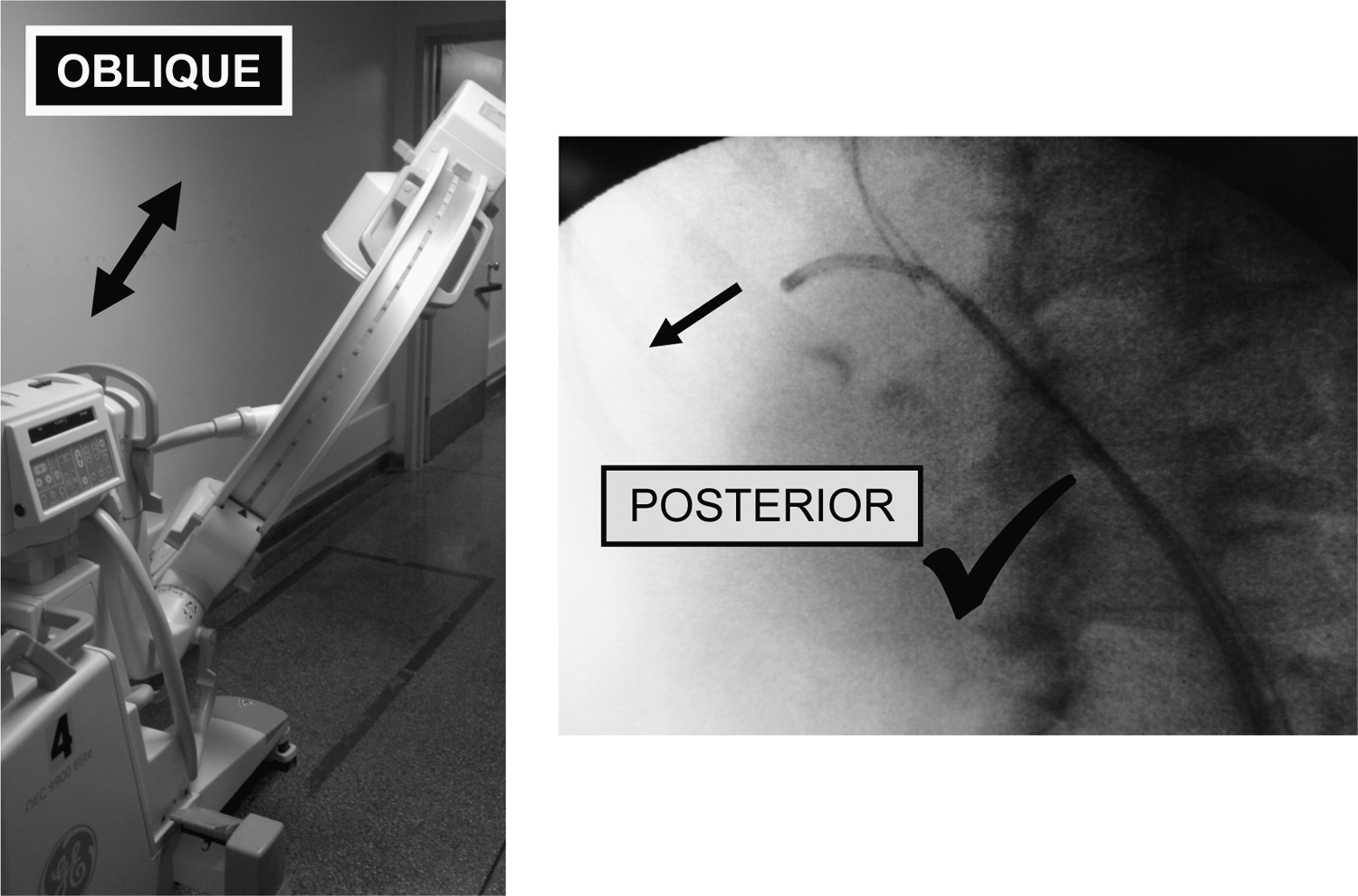
C-arm in oblique position; confirms posterior trajectory for puncture wire.
While the primary surgeon holds the position of the flexible ureteroscope within the selected calix, the surgical assistant advances the puncture wire ensemble into the ureteroscope working channel. Once this ensemble emerges from the distal end of the ureteroscope, the pin-vise lock on the puncture wire set is opened, and the assistant advances the puncture wire in 1 to 2 cm increments under direct vision (Fig. 8) and fluoroscopic guidance through calix, kidney, and subcutaneous tissues until the wire is seen tenting the skin or is palpable beneath the skin. If the puncture wire encounters a rib during advancement, the wire is withdrawn slightly and readvanced during deep inspiration or expiration or alternately the ureteroscope angle is changed (Fig. 9).
Puncture wire emerging from protective sheath within calyx.

Fluoroscopic view of straight puncture wire trajectory.
Puncture wire delivery at flank
Once deployed, we have found that the puncture wire “holds its course” and will continue along the trajectory set by the angle of the flexible ureteroscope.
We only dilate punctures posterior to the posterior axillary line to avoid injury to adjacent organs. This criterion is supported by clinical series with the Lawson retrograde nephrostomy. 16 –20 We are consistently able to achieve posterior punctures using the oblique fluoroscopy view (Fig. 7). A misdirected wire can safely be removed and redeployed without concern for injury to adjacent organs. 16 –20 Grasping and delivering the puncture wire at the flank often kinks its tip—this kinked segment is removed with a wire cutter or heavy scissors to permit antegrade loading of the coaxial exchange catheter. We have not found any difficulty advancing the thin puncture wire through flank tissues because of its thin caliber, smooth surface, and good axial strength.
Exchange of puncture wire for working wire using coaxial dilating catheter
Previous descriptions of this technique describe the use of a rigid needle to exchange the puncture wire for a working wire at the flank. 21 –23 We have found that this technique has several drawbacks. First, a rigid needle often cannot be directed into the proximal ureter, especially with lower pole punctures. The new working wire will thus not pass into the ureter, foregoing the ‘through-and-through’ nephrostomy wire position, which is one of the most important benefits of the retrograde access technique. Second, the puncture wire may become kinked during loading of the exchange needle, thereby precluding wire exchange. Finally, this technique necessitates more fluoroscopy than our method, which we describe below.
To address these concerns, we perform wire exchange with a 5F 30 cm tapered coaxial catheter (Greb Set, Vascular Solutions, MN; Fig. 10). First, a 30-cm length of puncture wire is gently drawn out of the flank while the ureteroscope remains in the calix. The ureteroscope is then drawn back into the ureteral access sheath. A 10-mm skin incision is made at the puncture site, and the coaxial catheter is advanced over the puncture wire and into the ureteral access sheath. The inner coaxial catheter, puncture wire, and ureteroscope are removed. A 0.035″ wire is advanced antegrade through the outer coaxial catheter (Fig. 11) until it emerges from the access sheath at the urethral meatus. Notably, the tapered design of this catheter (Fig. 10) permits advancement through flank fascia and renal capsule without separate incision of these structures.
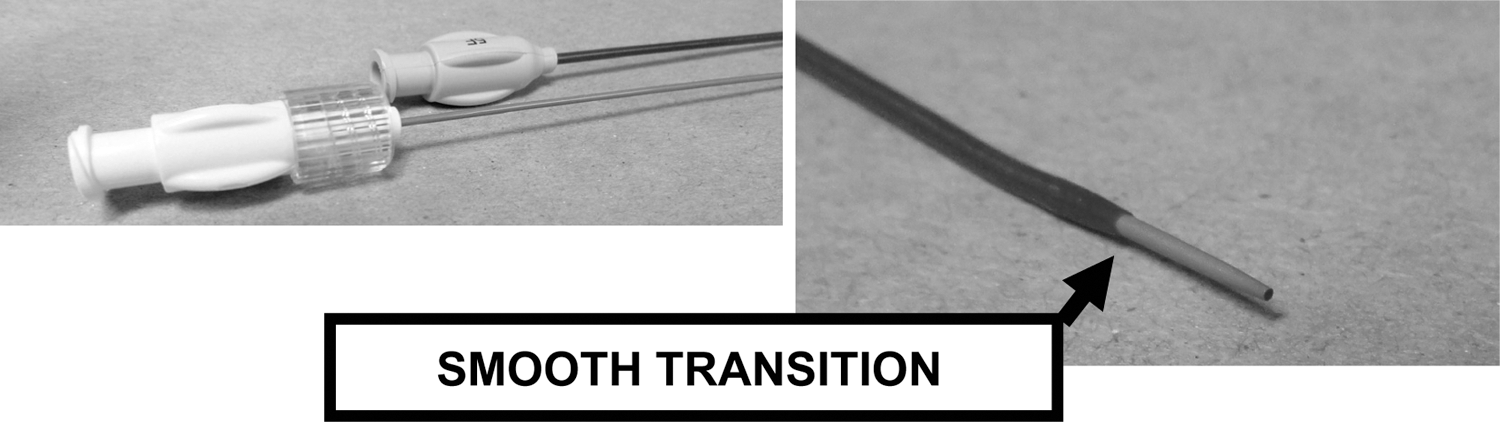
Coaxial transitional dilating catheter.

A 0.035″ working wire advancing through the outer coaxial catheter, antegrade direction from flank until it emerges from the access sheath at the urethra.
Tract dilation
A second wire can be placed using an 8/10 coaxial catheter over the nephrostomy wire at the flank. We did not perform this routinely as we had through and through nephrostomy wire control. The ureteral access sheath is then removed and reloaded over the safety wire. The nephrostomy wire emerging from the urethra is clipped to the drape. The flexible ureteroscope is reintroduced, and direct-vision advancement of nephrostomy balloon over the nephrostomy wire is performed, 7 without the need for fluoroscopy.
Equipment
• Lawson Retrograde Nephrostomy Creation Kit (Cook® Ref. 087000)—only the puncture wire ensemble is used
• 5F GrebSet Coaxial Transitional Dilator (Vascular Solutions, Inc. MN, Ref. 7950)
• Wire cutter or heavy scissors
• Fluoroscopy-compatible cystoscopy table (lithotomy position)
• Flexible ureteroscope (7.5F tip and shaft)
• 8F/10F coaxial dilator-introducer set (2)
• Ureteral access sheath 9.5F/11F or 10F/12F: 35 cm (female patients) or 55 cm (male patients)
• 0.038″ 150-cm floppy-tip guidewire×2 (eg, Bentson or Sensor)
• 30F nephrostomy dilating balloon with 30F sheath
• Rigid and flexible nephroscope
Role in Urologic Practice
Urologists' greatest hesitation with the original Lawson technique was concern regarding adjacent organ injury from errant puncture wire passage. In fact, however, only one nephrostomy-related complication—a colon injury 19 —was reported among 145 punctures across five published series including 14 upper pole accesses, seven of which were above the 12th rib. 16 –20 This colon injury occurred before the CT scan era, was a midaxillary line puncture, and followed two failed antegrade access attempts. This injury was successfully managed conservatively. No pleural, splenic, or hepatic complications have been reported. 16 –20
We have performed this procedure in 12 patients. Two procedures were abandoned without sequelae after puncture wire deployment based on concern regarding potential adjacent organ location. These cases were before and helped institute our systematic preoperative CT scan after which all 10 cases were successful and free of nephrostomy-related complications. Nephrostomy locations were upper pole, two patients; midzone, six patients; and lower pole, two patients. Further data are needed to clarify the performance characteristics of this technique.
We believe the learning curve of this technique compares favorably with that of antegrade techniques. 11 –14 Graduating residents and urologists without endourology fellowship training may find this technique easier to adopt into their practice than antegrade access techniques.
Conclusion
With proper case selection and planning, flexible ureteroscopy-directed retrograde nephrostomy is an intuitive approach to nephrostomy creation for PCNL that is precise, safe, easy to teach, and easy to learn.
Footnotes
Acknowledgment
This study is under Wayne State University IRB (HIC # 020111M1F). The authors wish to thank Dr. Richard A. Santucci for his support of this project.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.