
Abstract
Purpose:
To identify patients who would benefit from robot-assisted radical cystectomy (RARC), we report perioperative outcomes and complications.
Patients and Methods:
We compared patients who underwent RARC to patients who underwent open cystectomy (OC) in our institution. Data included demographics, operative variables, and recovery. Complications were grouped into early (<30 days), intermediate (31–90 days), and late (>90 days).
Results:
There were 58 patients in the RARC group and 84 patients in the OC group. The mean age was 66±1.2 years in the RARC v 67±1.2 in OC (p=0.53) group. Women constituted 21% in the RARC and 30% in OC (p=0.23) group. The mean American Society of Anesthesiologists scores were 2.9 for the RARC and 2.94 for OC (p=0.5). The mean operative time for RARC was 7.8±1.5 hours v 6.6±1.25 hours for OC (p<0.0001). Estimated blood loss was 276±48 mL in RARC v 1522±369 mL in OC (p<0.0001). Positive margin rate was 7% in RARC v 8% in OC (p=0.8). Early complications of any severity (Clavien scores) occurred in 43% in RARC and 64% in OC (p=0.02). There was one mortality in RARC and two mortalities in OC. Patients were grouped by age (≥70- and <70-years old). The older group consisted of 19 and 44 patients in RARC and OC, respectively. Both age groups in RARC had less early complications than OC patients (p<0.014). The older group in RARC had less early complication rate (17%) than the younger group in OC (59%).
Conclusions:
RARC has improved perioperative outcomes with equivalent oncological parameters when compared to open cystectomy. Patients ≥70-years old benefit from the robotic approach, particularly when compared to younger patients undergoing open cystectomy.
Introduction
We report our experience with 58 consecutive RARCs and compare them to 84 consecutive open cystectomies. Our goal was to identify which patients benefit from the robotic technique. In addition, we describe our ≤30-, 31–90-, >90-day complication rates in the open and robotic cohorts.
Patients and Methods
After obtaining the University of Alabama-Birmingham Institutional Review Board's approval, we retrospectively reviewed the medical record of 58 consecutive RARCs from March 2008 to May 2010 and 84 open cystectomies from January 2006 to May 2010 at our institution. Our robotic bladder program began in March 2008 and includes three surgeons' initial experiences. Six surgeons performed open radical cystectomy during the time studied. The choice of RARC v open was at the discretion of the individual surgeon; however, RARC was the preferred method beginning in March 2008.
All patients underwent preoperative workup, including chest X-ray, computed tomography scan of the abdomen/pelvis, standard preoperative laboratory work, and endoscopic resection. If the endoscopic resection was performed at an outside facility, a dedicated genitourinary pathologist at our institution reviewed the slides to confirm the muscle-invasive disease. A urologic oncologist and a medical oncologist determined the need for neoadjuvant chemotherapy. Criteria generally included presence of lymphovascular invasion, micropapillary disease, hydronephrosis, or pathologically enlarged LNs on preoperative imaging.
RARC and open cystectomy were performed in the standard fashion. 4,7 In the RARC cases, urinary diversion was done either extracorporeally through a 5–7-cm infraumbilical incision, or for orthotopic neobladders, the robot was redocked for the urethral neovesical anastomosis. Pelvic lymphadenectomy was performed in extended format with borders extending from aortic bifurcation proximally, Cooper's ligament distally, genitofemoral nerve laterally, and the sacral promontory medially.
Outcome measures evaluated included operative variables (surgery time, estimated blood loss [EBL], fluid intake, intraoperative transfusion, and type of diversion), hospital recovery (time to flatus, time to regular diet, and LOS), pathological outcomes (pathologic stage, margins, and LN yield), and ≤30-day, 31–90-day, and >90-day complication rates. All complications were graded using the modified Clavien system. 8 All grades were considered complications (Grades I–V). Patient characteristic data included age, gender, body–mass index (BMI), history of abdominal surgery, American Society of Anesthesiologists (ASA) scores, neoadjuvant chemotherapy, adjuvant chemotherapy, and history of radiation therapy. Finally, patients were stratified by age <70 v ≥70 to determine patients who benefitted most from RARC.
SPSS v 8.0. was used for statistical analysis. For univariate analysis, Chi-square test or Student's t-test was used when appropriate. For multivariate analysis, logistic regression was used to evaluate predictors of ≤30-day complication rates. A p-value <0.05 was considered statistically significant.
Results
Table 1 lists the patient characteristics of both cohorts. There was a statistically significant difference between the two groups in terms of history of abdominal surgery. There were no statistically significant differences in terms of age, BMI, ASA score, clinical stage, diversion type, neoadjuvant chemotherapy, adjuvant chemotherapy, and history of radiation. Mean follow-up in the RARC cohort was 7.5 months v 8 months in the open cohort.
ASA=American Society of Anesthesiologists; BMI=body–mass index; RARC=robot-assisted radical cystectomy; SE=standard error.
Perioperative and pathological outcomes are listed in Table 2. Mean operative time was 7.8 hours in the RARC cohort and 6.6 in the open (p<0.001) cohort. The RARC cohort demonstrated decreased EBL (276 v 1522 mL, p<0.0001), decreased intraoperative fluid administration (3966 v 7466 mL, p<0.0001), and need for transfusion (5% v. 80%, p<0.0001). Mean time to flatus (4.3 v 5.9 days, p=0.028), regular diet (5.4 v 8.1 days, p=0.009), and LOS was also shorter in the RARC cohort (6.3 v 10.8 days, p=0.004). There were more patients with extravesical disease in the open cohort compared to the RARC cohort (57% v 34%, p=0.008). The RARC group yielded more mean LN's with a trend toward statistical significance (21.3 v 17.7, p=0.061).
EBL=estimated blood loss; LOS=length of stay.
Complications were evaluated based on the modified Clavien score and at ≤30, 31–90, and >90 days. The RARC cohort had a reduced complication rate compared with the open (24% v 58%, p<0.0001) at ≤30 days. However, this difference was not seen at 31–90 days (21% v 20%, p=0.525) and at >90 days (17% v 10%, p=0.20).
To identify patients who would potentially benefit from RARC, patients were stratified <70 v ≥70 years of age. There were 19 and 44 patients older than 70-years in the RARC and open cystectomy group, respectively. When comparing ≥70 years of age who underwent RARC v open, there was a difference in ≤30-day complications (17% v 58%, p=0.004). Similar results were found for the patients <70 years at ≤30 days (28% v 59%, p=0.005), seen in Figure 1. The aim of the study was to determine which patients might benefit from RARC. Superior results were found for ≤30-day complication rates when comparing patients ≥70 years who underwent RARC v patients <70 years who underwent an open approach (17% v 59%, p=0.014). This demonstrates that RARC is significantly less morbid in patients ≥70 years and specifically benefits the elderly even compared to younger patients undergoing the open approach. There were no differences in 31–90- and >90-day complication rates between the two cohorts.
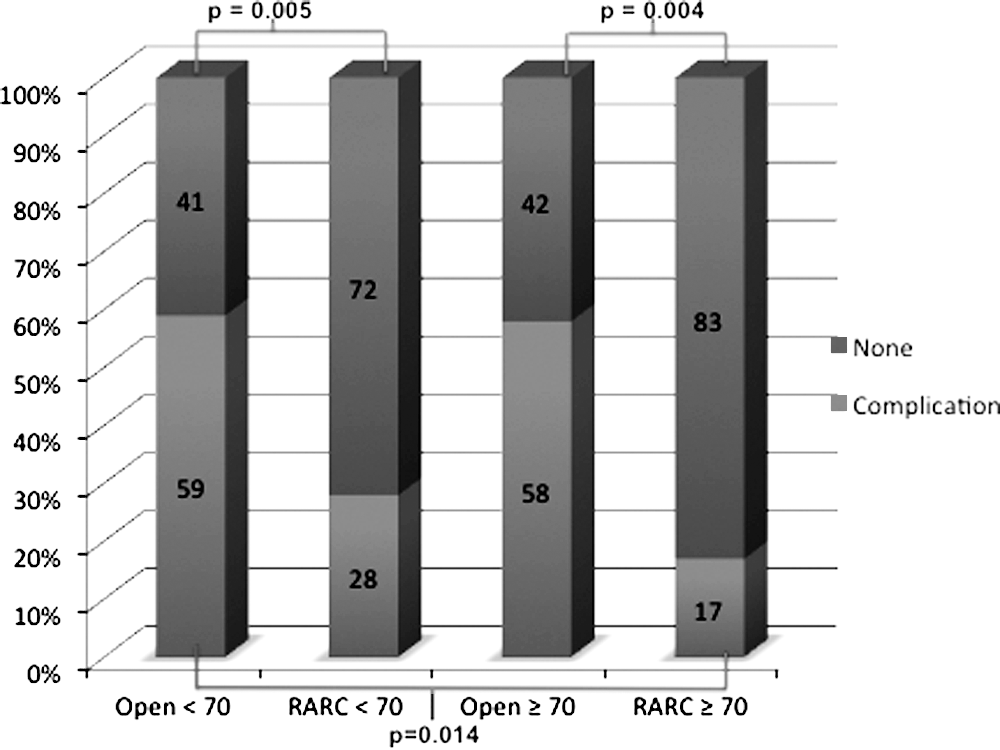
Complications by age. RARC, robot-assisted radical cystectomy.
Complications were evaluated based on the Clavien score (Table 3). The main difference in complications was in Clavien grade 2 with a complication rate of 38% in open cystectomy and 12 in RARC (p=0.001). There were two deaths in the open group and one death in the RARC. During evaluating the complications, we found a higher number of ureterointestinal strictures among the early RARC cohort. We found seven unilateral ureterointestinal strictures and two bilateral in the RARC cohort and three unilateral strictures in the open (p=0.031). All of the ureterointestinal strictures in the RARC cohort occurred within the first 37 cases. No other differences were found in the types of complications between the two groups.
Multivariate analysis was used to evaluate for predictors of ≤30-day complications. Variables evaluated included age, gender, BMI, ASA, history of abdominal surgery, clinical stage, pathologic stage, intraoperative fluid, transfusion requirement, and type of diversion. Increasing pathological stage (p=0.0023) and total units of packed red blood cells (PRBC) transfused (p=0.0361) were predictive of complications at 30 days. In addition, RARC was predictive of fewer complications at 30 days (p=0.0009)
Discussion
Open radical cystectomy is associated with significant morbidity as well as a small risk of mortality. Traditionally, morbidity rates have been quoted at 28% with mortality rates of 1%. 9 Improved reporting of complications has resulted in an increased rate compared to older reports. Lowrance et al reported a 41% complication rate for open cystectomy at 30 days with a perioperative mortality of 1.7%. 10 In addition, Shabsigh et al reported a 64% 90-day complication rate for open cystectomy with the use of a standardized grading system. 11
Application of robotic technology has increasingly gained acceptance in the treatment of bladder cancer with improved perioperative outcomes. 2,4,12,13 Maturing experiences in this technique show improved outcomes in EBL, time to flatus, time to bowel movement, and LOS. 14 In addition, equivalent oncologic parameters have been shown in terms of pathologic and LN yield between RARC and open cohorts. 15 In the current study, there was no difference between the RARC and open cohorts in terms of age, BMI, ASA, clinical stage, diversion, neoadjuvant chemotherapy, adjuvant chemotherapy, and preoperative radiation. There was a statistically significant difference in history of abdominal surgery. This may reflect a selection bias with the initial experience. As our RARC experience matures, this difference may disappear.
An aim of this study was to determine which patients might benefit from RARC. To determine this, patients were stratified in groups by age. In this analysis, patients <70- and ≥70-years old had improved ≤30-day complication rates compared to the open cohorts of the same age. There were no differences at 31–90 days and >90 days. Interestingly, patients ≥70 years in the robotic cohort, which included 4 octogenarians, had statistically significant improvement in 30-day complication rates than patients <70 years in the open cohort (17% v 59%, p=0.014). It appears that RARC is superior in patients ≥70 years even when compared to a younger cohort undergoing open cystectomy. This is a significant finding given the increasing elderly population, and the fact that urothelial carcinoma occurs more frequently in this population. In this study, RARC improved complication rates and resulted in equivalent oncological parameters. It is important to note that Donat et al reported that elderly patients undergoing open cystectomy had a significantly higher rate of neurological and cardiac complications. 16 In this study, the RARC cohort had zero patients ≥70 years with neurologic complications or cardiac complications.
Guillotreau et al reported on the outcomes of laparoscopic and robotic radical cystectomy in the elderly patients. In their series, 74 patients were classified as elderly (≥70 years), and 72 patients were considered younger (<70 years). They concluded that laparoscopic/robotic radical cystectomy in the elderly does not have worse perioperative complications or pathologic outcomes compared with younger patients. 17 The present study agrees with these findings, but the present study also found that the outcome is better in robotic than open surgery, and that older patients do benefit from the advantages of robotic surgery.
The RARC group had improved perioperative outcomes compared to the open cohort. This analysis demonstrated significant differences in EBL, intraoperative fluids, time to flatus, time to regular diet, LOS, and transfusion rate. Nix et al found similar results in perioperative outcomes. 3 In addition, Ng et al found similar results when comparing larger open and RARC cohorts. 6 A report from Kaufman et al found that intraoperative fluids >5 L was associated with postoperative complications of any grade, and operative blood loss >500 mL predicted high-grade complications. 18 The mean intraoperative fluids in our RARC cohort was 3966 mL and mean EBL was 276 mL. The RARC cohort benefited from less insensible losses and resultant bowel edema secondary to decreasing intraoperative fluid. Our transfusion rate of 80% for the open cohort is higher compared to recent open series. 11 On multivariate analysis, the total number of units of PRBC transfused was predictive of increased <30-day complications. Several studies have previously shown that EBL and transfusion requirements are correlated with complications. 19,20
There was a significant difference between the open and RARC cohort in terms of pathologic stage. However, there were no differences in the positive margin rate between the two cohorts. Hellenthal et al recently reported a multi-institutional study of 513 patients who underwent RARC with a 6.8% overall positive margin rate and an increasing positive margin based on stage. 21 In the current series, all positive margins occurred in T3 and T4 disease in both cohorts. The positive margin rate of 7% in the RARC cohort compares favorably with Hellenthal's results. In addition, an increased LN yield with the RARC compared to the open with a trend toward statistical significance. Previous articles have shown at least equivalent LN yield with the RARC technique. 3,6,15
In the current analysis, the RARC cohort had a statistically significant difference in ≤30-day complications when compared to the open cohort. This difference was not present at 31–90 days and >90 days. The ≤30-day complication rate of 24% in the RARC group is slightly decreased compared to Ng et al's of 29.8%. 6 When evaluating by the Clavien score, there again was a difference between the two groups with the RARC group having fewer grade-2 Clavien scores (38% v 12%, p=0.019). The RARC cohort had more patients without complications compared to the open cohort (57% v 36%, p=0.019). Grades 1, 3, and 4 had similar rates (Table 3). This is different from Nix et al.'s report, where there was no difference between an open and RARC cohort with regard to Clavien scores. 3 It is important to note that their study compared only 21 RARC cases v 20 open cases. Complications were classified as seen in Table 4, and there was no difference between the RARC and open cohorts other than ureterointestinal strictures. This can potentially be explained by increased tension placed on the ureters during the extracorporeal diversion. All of the ureterointestinal strictures in the RARC cohort occurred within the first 37 cases. In addition, more patients in the RARC cohort experienced acute renal failure. This can be explained by the higher incidence of ureterointestinal strictures causing obstructive hydronephrosis, which was relieved with percutaneous nephrostomy tubes and antegrade ureteral stenting. We started modifying our technique by doing urinary diversion intracorporally with the robot. We hope that these complications will be reduced in the future.
CVA=crebrovascular accident; UTI=urinary tract infection; ARF=acute renal failure; CRF=chronic renal failure; GI=gastrointestinal; SBO=small bowel obstruction; MI=myocardiac infarction; DVT=deep venous thrombosis; PE=pulmonary embolism.
In addition, on multivariate analysis, the RARC approach had significantly improved ≤30-day complication rates. Ng et al found RARC to be an independent predictor of fewer overall and major complications at 30 and 90 days. 6
Limitations of this study include its retrospective nature as well as the small number of patients in the RARC cohort. In addition, six surgeons compromised our open cohort, which could result in outcome differences in the open group. Finally, the results described compromise three surgeons initial RARC experience. Although all the surgeons had experience with other robotic procedures, their initial RARC experience is reported in the present study. As in any initial experience, the selection bias is present; however, complication rates may be increased initially. Further investigation is indicated to corroborate the findings of the present study.
Conclusions
RARC has improved perioperative outcomes and equivalent oncological parameters when compared to open cystectomy. Patients ≥70 years of age specifically benefit from the robotic approach even when compared to younger patients undergoing open cystectomy. These older patients particularly gain from undergoing RARC with a significant difference in morbidity compared to open cystectomy even in younger patients. These data suggest that RARC results in improved ≤30-day outcomes compared to the open approach, specifically among older patients, and should be considered when discussing the treatment options with this patient population.
Footnotes
Acknowledgements
None.
Disclosure Statement
None.