
Abstract
Purpose:
To compare the in vitro degree of vaporization in bipolar and monopolar resection.
Materials and Methods:
Using either a bipolar system or a monopolar system, samples of chicken muscle and lamb kidney were resected in an isolated basin and then desiccated in an incubator. The percentual degree of vaporization for each sample was obtained as a difference between the total fresh weight of the sample and the calculated fresh weights of the resected tissue and remains.
Results:
Reference samples showed that the water content was 73% in muscle and 77% in kidney. More muscle (mean 52%) than kidney (32%; P<0.0001) tissue was vaporized. The fraction of vaporized tissue was significantly higher in the bipolar technique. In muscle, the differences between monopolar and bipolar were 17% (P<0.05) and 26% (P<0.001), respectively, depending on the type of irrigation used. For kidney, the differences were 27% (P<0.01) and 34% (P<0.01), respectively. Further exploration of the degree of vaporization when using the bipolar resection showed that the choice of loop (P<0.0001), fluid (P<0.03), and tissue (P<0.0001) were all independently associated with the degree of vaporization.
Conclusions:
This study indicated that vaporization removes 50% more tissue than the weight of the resected tissue during conventional tissue resection. Bipolar standard loop resection resulted in a significantly higher degree of vaporization in both muscle and kidney than did monopolar technique. Bipolar resection worked satisfactorily in Ringer's acetate.
Introduction
The bipolar loop creates a heated vapor “plasma” pocket that destroys rather than cuts the tissue during movement. The technique also allows the surgeon to perform pure vaporization with the bipolar technique only by changing from loop to button-electrode. 3 –5 This raises the question of whether tissue becomes vaporized also during a regular bipolar TURP. There are anecdotal indices of lower resection weights in bipolar TURP, and there are also studies that show lower resection speed. 6 This might be explained by a larger fraction of vaporized tissue during bipolar TURP. Because the amount of destroyed tissue is a crucial efficacy parameter, the possibility of an unknown degree of vaporization is an essential issue in any comparison between open surgery and the mono- and bipolar resection techniques.
The purpose of the present laboratory study was to investigate the degree to which vaporization occurs when resecting tissue by using the mono- and bipolar techniques. Associated parameters were the size of the electrode and the type of irrigating fluid used.
Materials and Methods
Materials
Samples of either chicken muscle or lamb kidney were resected in an isolated plexiglass basin (Fig. 1). The samples were purchased in an ordinary grocery store. Ten samples in each category were resected (Table 1).
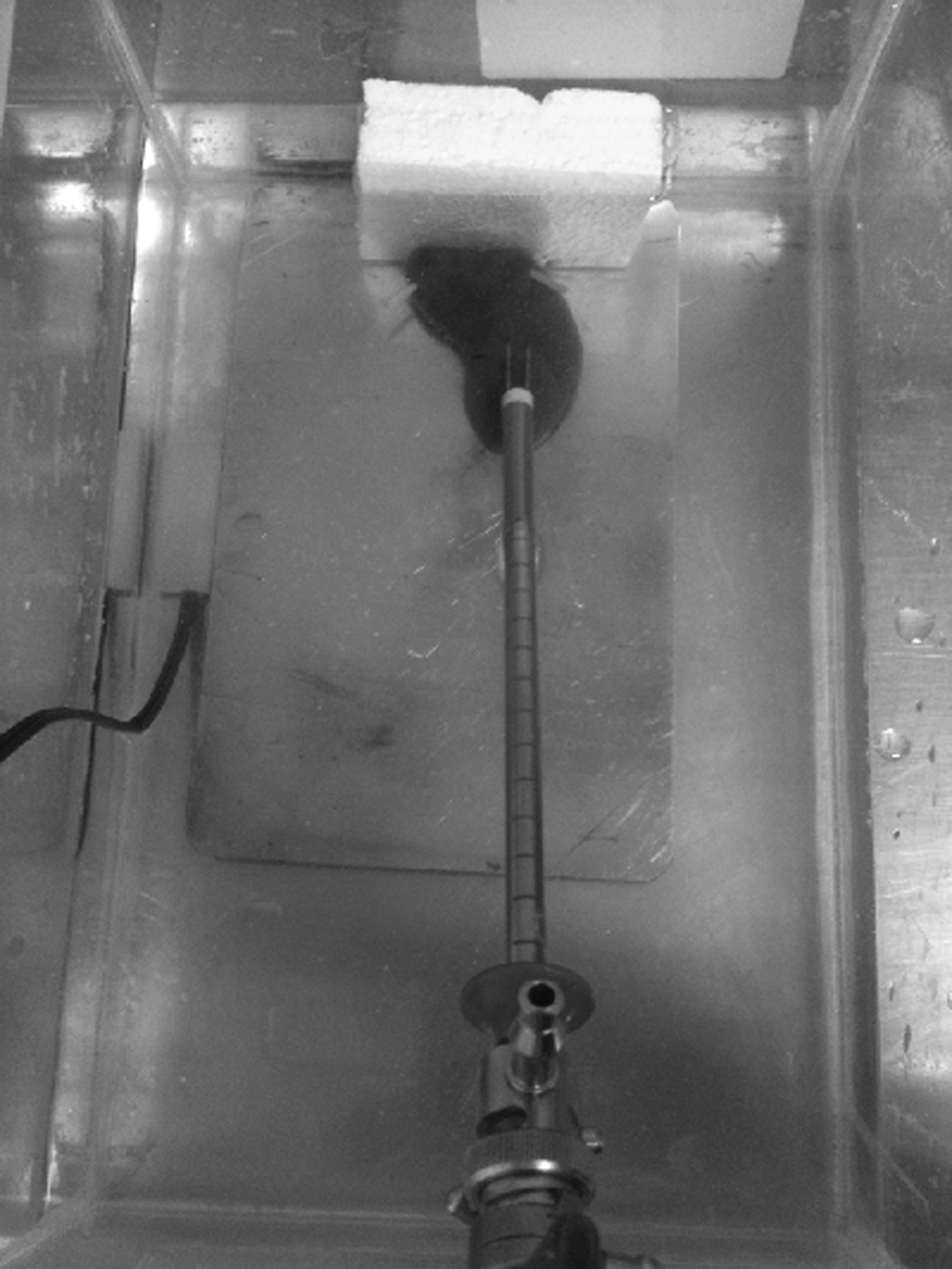
Arrangement of the in vitro resection.
N=10 in each category.
Methods
After weighing on an electronic scale (PB3002-S Delta Range,® Mettler Toledo, Switzerland), the specimen was placed in a plexiglass container filled with 1500 mL of irrigating fluid at room temperature and fixed to a piece of Styrofoam (Fig. 1). Ten cuts were made in each sample of the 10 study subgroups (Table 1).
Bipolar resection was performed with the Olympus transurethral resection in saline system using the Olympus UES 40 generator (Olympus Surgmaster TURis, Tokyo, Japan) either set at 280 W (0.2 mm, 12-degree medium loop) or 290 W (0.2 mm, 12-degree large loop) for cutting. Saline (0.9% NaCl, Baxter, Kista, Sweden) and acetated Ringer's solution was used as the irrigant.
Monopolar resection was performed with a Storz 24F resectoscope, using an ERBE ICC 350 generator (Tübingen, Germany) set at 130 W for cutting. The resections were performed with standard loops and factory-made irrigating fluid that contained mannitol 3% (Baxter, Kista, Sweden). The neutral electrode was attached to a copper plate of the same size, and the sample was then placed on the plate to obtain a continuous electrical circuit (Fig. 1).
After all resections, the removed tissue and remaining piece of tissue were then weighed (wet weight) and heated in an incubator (B8054 Bacterial Chamber, Termaks, Bergen, Norway) at 65°C for 72 hours. After complete desiccation, the dry weights were recorded.
Because tissue chips may absorb irrigating fluid, we used reference samples to determine the normal water content of the used tissues. Pieces of unresected chicken and kidney were then desiccated in an incubator for 72 hours in an approximate temperature of 65°C. During the period in the incubator, the samples were weighed repeatedly until no further weight loss was registered. This yielded the water content if no vaporization occurred. The procedure also provided the time necessary to gain complete desiccation of the samples.
The amount of vaporized tissue was obtained as the difference between the fresh weight of the uncut sample and the sum of the fresh weights (calculated based on its expected “normal” water content) of the resected tissue and the remains.
All the experimental resections were carried out by a consultant urologist with a substantial experience of both methods.
Statistical methods
All parameters showed a normal distribution. P<0.05 was considered significant. Means were compared with independent samples t test. One-way and three-way analysis of variance (ANOVA) analyses of factors important for vaporization were made. Calculations were made in PASW Statistics 18.0.0 (SPSS Inc, Chicago, IL).
Results
Reference samples
The water content was 73% in muscle and 77% in kidney. This means that 1 g of fresh sample corresponded to 0.27 g of dried muscle and 0.23 g of kidney. These factors were then used throughout the material to convert the total fresh weights into dry weights of the unresected samples (Table 2).
Resected samples
More muscle (mean 52%) than kidney (32%; P<0.0001) tissue was vaporized. For both tissues, the fraction of vaporized tissue was significantly higher with the bipolar than with the monopolar instrument. When analyzing the muscle samples, the differences between monopolar and bipolar were 17% and 26%, respectively, depending on the type of irrigation used (Table 3). For kidney, the differences were 27% and 34%, respectively (Table 4). The degree of vaporization did not differ significantly between the two irrigating fluids used in the bipolar technique, although there was a tendency of a higher degree of vaporization when using Ringer's acetate.
Mean (standard deviation). Pairwise significance comparisons vs monopolar technique, a P<0.05, b P<0.001.
Mean (standard deviation). Pairwise significance comparisons vs monopolar technique, a P<0.01.
In contrast, bipolar and monopolar resection yielded the same degree of vaporization when using the bipolar large loop instead of the standard loop.
The relationship between wet and dried samples showed that there was a quite consistent uptake of the irrigating fluid by the chips of muscle and kidney amounting to 17 and 12%, respectively, regardless of which type of irrigant was used.
One-way ANOVA showed that the type of loop, the resection method, and the used tissue were factors of importance to the degree of vaporization (Table 5). The choice of irrigant, however, did not affect the vaporization in bipolar resection.
SD=standard deviation.
Further exploration of the degree of vaporization when using the bipolar resection instrument was made by three-way ANOVA. This statistical test separates the effects of the three factors on the degree of vaporization from each other, and thereby eliminates confounding intercorrelations between them. Post hoc testing is not needed, because all three factors have only two alternatives.
One single analysis showed that the choice of loop (P<0.0001), fluid (P<0.03), and tissue (P<0.0001) were all independently associated with the degree of vaporization. In contrast, the choice of loop and the tissue used for cutting did matter much to the amount of tissue that is vaporized.
Discussion
The results show that vaporization of resected tissue is substantial when using a standard resection system for monopolar and bipolar TURP. Approximately 50% more tissue disappears than indicated when weighing the amount of resected tissue. This finding is a new knowledge, which also puts the bipolar technique in a new perspective when considering the choice between pure vaporization and conventional resection. One of the conclusions led by this is that a conventional resection not only results in a significantly greater tissue removal than known until now, but also provides a specimen to be analyzed histologically. These facts, in addition to earlier described advantages, put bipolar resection ahead of monopolar technique as well as pure bipolar vaporization and thus the most valuable choice in surgically treating patients with BPH.
The degree of vaporization varies somewhat depending on the type of resected body tissue, the resection technique, and the type of loop used. When resecting 1 g of muscle, we can expect 1.6 to 1.7 g of total tissue loss and for kidney, 1.4 to 1.6 g. When performing the same procedure with the bipolar large loop, which resembles the monopolar loop, the degree of vaporization was approximately 45% for both techniques. The degree of vaporization, however, rose to 60% to70% higher when the bipolar standard loop was used. In contrast, the type of irrigating fluid used is of some importance but it is not very great.
These calculations are of importance for comparisons between resection methods and for any judgment of the efficacy of open vs transurethral prostatic surgery. In previous work, we have found that blood loss is significantly lower using the bipolar technique. 1 Concerning the higher degree of vaporization, this difference is even greater than reported, as further 50% more tissue is removed when using the bipolar resection instrument as compared with the monopolar. An estimate indicates that the blood loss would then be as low as 6 mL/g resected tissue, which is far below any former reported value of TURP-associated bleeding in previous series of both bipolar and monopolar resection. 7,8
The degree of vaporization in mono- and bipolar TURP has not previously been examined. There is, however, indirect evidence of monopolar vaporization in an earlier study by Sandfeldt and associates. 7 Here, the signs of vaporization are shown by the difference between preoperative and postoperative transrectal ultrasonography (TRUS) volume, in correlation to the resection weight. In this study, the measurements indicate a vaporization of 35% to 67%, a figure compromised by the uncertainty of nonplanimetric TRUS assessment, 9,10 but nevertheless point in the direction of a significant tissue loss that could be explained by vaporization.
The relatively new concept of bipolar TURP has proven advantages. 1,2,11,12 The bipolar technique is superior in terms of blood loss and reduces—or eliminates—the risk of the classical TUR-syndrome. When assessing the quality of histologic specimens from resected tissue, it has also been shown that the coagulation artefacts of the chips are less than in the ones provided by monopolar resection, thus facilitating a more accurate pathologic diagnosis. 13 It is also clear that the cautery effect is less pronounced in bipolar technique, which is a benefit in visibility and surgical accuracy for the performing surgeon. 14,15 The latter is in spite of the fact that the coagulation depth in the residual tissue seems to be deeper than in monopolar resection, 16 a circumstance that might be the reason for the reduced blood loss in the bipolar technique, although this is not yet fully understood.
The concept of desiccating tissue to decide the true weight of the specimen and the water content has been used in several other studies. 17 –19 Here it was necessary to be sure that absorbed irrigating fluid would not interfere with the calculations of the vaporized tissue. The amount of absorbed fluid, however, was not as unpredictable as first apprehended. The tissue absorbed only about 15% of its own weight in a quite regular pattern.
When concerning the water content of the two examined kinds of tissues and comparing this with the water content of the human prostate as stated in the study by Leissner and Tisell, 18 one could assume that the prostate would show approximately the same degree of vaporization as the here examined kidney tissue.
Limitations of the study include that the number of samples was not great, but on the other hand, the results were normally distributed. Another limitation is, of course, that it is not a clear connection between the degree of vaporization of the samples in this study and the one in human prostate tissue, something that needs to be investigated further.
Conclusion
This laboratory study indicated that vaporization removes 50% more tissue than the weight of the resected tissue during conventional tissue resection. When using the standard loops, the bipolar resection technique resulted in a significantly higher degree of vaporization in both muscle and kidney than did the monopolar technique. The difference in vaporization was not seen with the bipolar large loop. Bipolar resection worked satisfactorily in Ringer's acetate, although this fluid tended to increase the vaporization.
Footnotes
Disclosure Statement
No competing financial interests exist.