
Abstract
Background and Purpose:
With the advent of robotics, it may be more feasible to offer minimally invasive nerve-sparing surgery (NSS), in the form of partial nephrectomy (PN), for patients with metachronous recurrence in the ipsilateral kidney after previous NSS. We studied the outcomes of patients undergoing robot-assisted laparoscopic partial nephrectomy (RAPN) after previous ipsilateral open or laparoscopic NSS for renal-cell carcinoma.
Methods:
In this Institutional Review Board approved study, a prospectively maintained PN database was reviewed. Of 230 RAPNs performed between 2003 and 2011, five patients underwent RAPN after previous ipsilateral NSS.
Results:
The mean age was 64.2 years, and time between the first and second surgery was 27 months (range 9–60 mos). All patients were men and previously had open (n=4) or laparoscopic (n=1) NSS for clear-cell (n=2), papillary (n=2), and other (n=1) pathology. Average follow-up was 15.6 months (range 8–21 mos). There were no conversions to open surgery or radical nephrectomy. Total and selective arterial clamping were performed in two and two cases, respectively. One RAPN was performed off-clamp. Mean warm ischemia time was 14 minutes (range 0–32 min), and mean blood loss was 220 mL (range 50–400 mL). Average length of stay was 1.4 days (range 1–2 days) with no perioperative complications. The glomerular filtration rate decreased by a mean of 10%. There were no recurrences detected on cross-sectional imaging at the most recent follow-up.
Conclusion:
RAPN after previous open or laparoscopic PN is safe and efficacious. It offers satisfactory intermediate functional and oncologic outcomes with minimal morbidity.
Introduction
As the number of SRMs treated with NSS increases, so will the number of patients who present with recurrent disease in the ipsilateral kidney and need re-treatment with either ablative or extirpative surgeries. In this article, we present the feasibility of robot-assisted partial nephrectomy (RAPN) in patients who presented with metachronous recurrence of RCC after previous extirpative surgery and review their functional and oncologic outcomes.
Patients and Methods
In this Institutional Review Board approved study, a prospectively maintained RCC database was reviewed. Of 230 NSSs performed between 2003 and 2011, we identified five patients who underwent RAPN after previous ipsilateral PN. Patients who underwent other forms of NSS (cryotherapy, radiofrequency ablation [RFA]) were excluded from analysis. Primary outcomes measured were necessity for open conversion or conversion to RN. Secondary outcomes were renal function and radiographic evidence of recurrence. Patient demographic data and previous pathology, stage, time between surgeries, warm ischemia time (WIT), and most recent follow-up were included in the analyses.
Results
Table 1 outlines the patient demographic data. Mean patient age was 64.2 years, and time between the first and second surgery was 27 months (range 9–60 mos). Average follow-up was 15.6 months (range 8–21 mos). All patients were men and previously had open (n=4) or laparoscopic (n=1) PN for clear-cell (n=2), and papillary (n=2) pathology. One patient in the cohort previously underwent laparoscopic PN at a referring institution, and the final pathology report on the specimen was normal renal parenchyma. The initial stage was pT1a (n=3), pT1b (n=1), and normal kidney tissue (n=1) for the five patients based on the 2010 American Joint Committee on Cancer Tumor-Node-Metastasis staging system.
BMI=body mass index; CCI=Charlson Comorbidity Index.
Operative and perioperative data are presented in Table 2. All procedures were performed via a robot-assisted laparoscopic approach, and there were no conversions to an open procedure or to RN. Total arterial clamping was performed in two cases, selective arterial clamping was performed in two cases, and one RAPN was performed off-clamp with no ischemia. Mean WIT was 14 minutes (range 0–32 min), and mean blood loss was 220 mL (range 50–400 mL), with no patient needing blood transfusion.
RAPN=robot-assisted partial nephrectomy; OPN=open partial nephrectomy; RN=radical nephrectomy; EBL=estimated blood loss; OR=operative; WIT=warm ischemia time; GFR=glomerular filtration rate.
Average length of stay was 1.4 days (range 1–2 days) with no perioperative complications. The glomerular filtration rate (GFR), as calculated by the Modification of Diet in Renal Disease equation, decreased by a mean of 10% after the two operations. Final stage for the second procedure was pT1a in all five patients, and the final pathology determinations were clear-cell carcinoma (n=3) and papillary carcinoma (n=2). There were no recurrences detected on cross-sectional imaging at a mean follow-up of 15.6 months (range 8–21 mos).
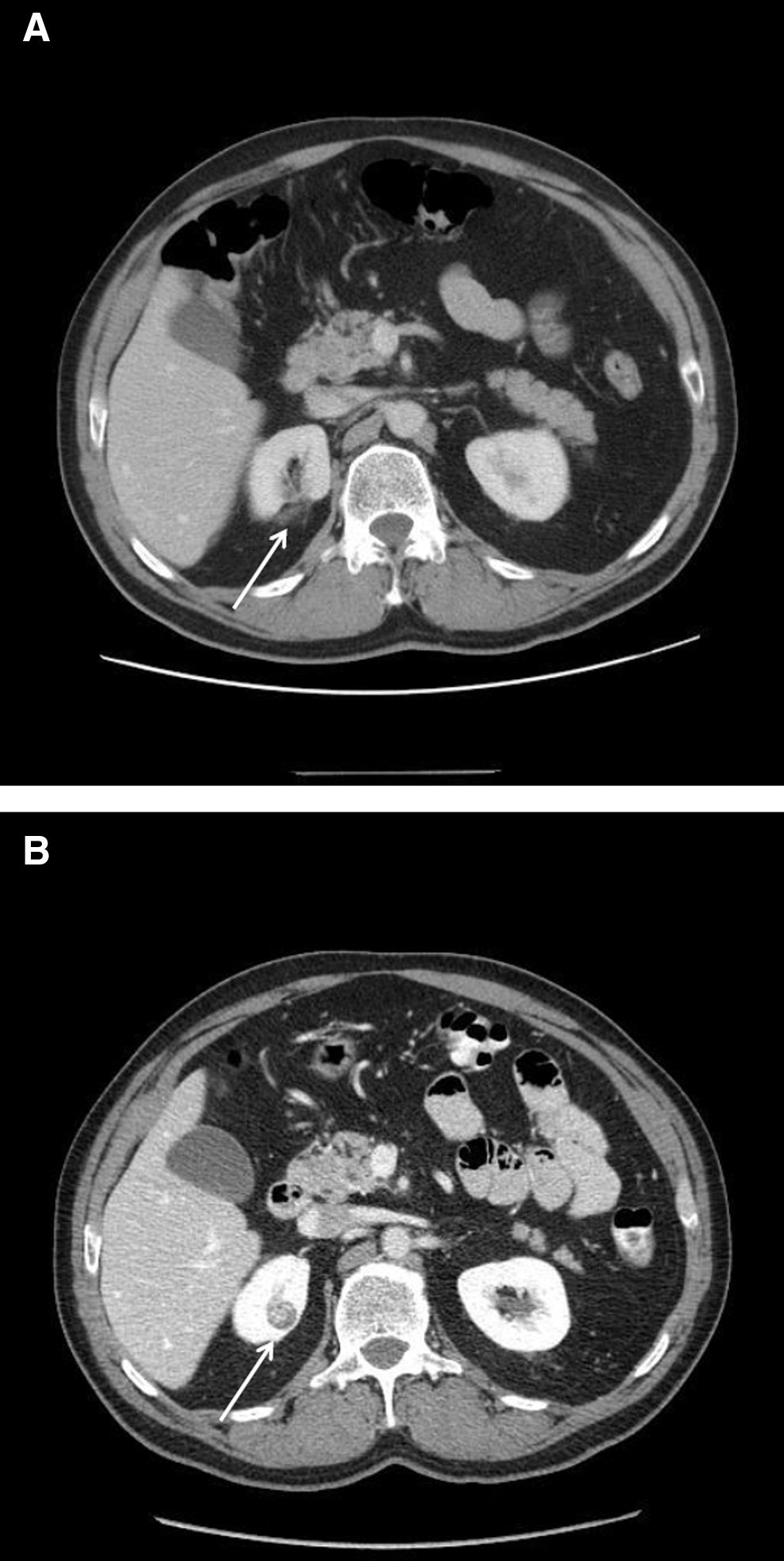
Figure 1 shows a preoperative CT scan for one of the renal units in our series that is representative for the cohort. Figure 1A shows the area of previous excision, and Figure 1B shows the recurrent mass.
Discussion
RCC remains a common and fatal malignancy in the United States. 1 As more cross-sectional imaging is performed, a larger number of SRMs are being discovered. 2 Traditionally, SRMs were managed with RN, but a large amount of literature has shown superiority of PN over RN with respect to renal function, while maintaining equivalent oncologic outcomes. 7 –9 Based on these findings, guidelines released by both the American Urological Association and the European Association of Urology have recommended NSS as the first-line therapy for SRMs in appropriately selected patients/masses. 3,4
Although NSS offers excellent cure rates for patients with SRMs, disease recurrence remains significant and has been estimated to be between 4% and 13%. 10 –15 As a result, as more patients with SRMs undergo NSS, there will be more recurrences in the ipsilateral kidney that will necessitate re-treatment. This will represent a significant challenge for both patients and urologists, since re-treatment of a kidney previously treated with NSS can be fraught with complications.
Liu and associates 16 reported 25 patients who underwent repeated open partial nephrectomy (OPN) for recurrent RCC in the ipsilateral kidney. Twenty-two of the patients successfully underwent the planned PN, but there were three renal unit losses, all secondary to vascular injury. In fact, the most common complication in this report was vascular injury of the major renal vessels in 25% of the cases. Median estimated blood loss (EBL) was 2400 mL, and 19 of the 25 patients needed intraoperative transfusions. The authors commented that previous renal surgery and hilar dissection with subsequent fibrosis and scarring was likely the cause for the high vascular injury rate.
Johnson and colleagues 17 reported on feasibility and outcomes of repeated PN in von Hippel-Lindau RCC patients. Of the 51 patients identified in their study, only three had their repeated PN performed in a minimally invasive fashion via a laparoscopic approach. In their cohort, irrespective of surgical approach, three renal units had to be removed, one because of renal vascular injury, similar to Liu and coworkers, 16 and the other two because the mass was not amenable to NSS. Their median EBL was 1800 mL, and 64.7% of the patients needed an intraoperative blood transfusion. In their series, there was close to a 20% major complication rate.
Nguyen and colleagues 18 published their series of 42 ipsilateral recurrences in kidneys that were previously treated with ablative NSS. Of the 42, there were 16 postcyroablation (CA) and 26 post-RFA tumor recurrences. In the cohort, four had attempted open PNs, of which only two of these procedures were successful. One of the procedures was converted to an open RN, and one was aborted because the patient preferred to be left with the mass instead of having the entire renal unit removed. Patients in the post-CA group had either a minor (5 of 6) or major (1 of 6) intraoperative complication. As a result of the high complication rate, the authors advocated alternative strategies to extirpative therapy in patients with recurrence after CA.
Kowalczyk and associates 19 reported the National Cancer Institute's experience of PN for ipsilateral recurrence after previous RFA. They examined 13 patients who underwent planned PN (12 open, 1 laparoscopic) after RFA failure/recurrence. In this series, all patients successfully underwent PN without any conversion to RN. Their median cold ischemia time was 27 minutes, and EBL was 1500 mL with 50% of the patients needing a blood transfusion. Although there were no renal unit losses, eight of the 13 patients experienced a postoperative complication, with two needing reoperation.
After conducting a thorough online literature review, we believe we are the first to report a series of patients to undergo RAPN after previous extirpative NSS. Four of the patients in our series had OPNs and one had a laparoscopic PN. All patients had previous renal hilar dissection and underwent total arterial clamping at the time of initial PN. In contrast to Liu and associates 16 and Johnson and coworkers, 17 we did not encounter any significant complications during hilar dissection and were able to achieve an adequate dissection to allow for selective arterial clamping in two of the five treated patients. We were able to complete all of our procedures as planned and did not have to perform a completion RN for any of our patients or convert to an open procedure. Mean EBL was 220 mL, and none of our patients needed intraoperative or postoperative blood transfusions. Mean length of stay (LOS) was 1.4 days, which is approximately 3 days shorter than the mean LOS for patients undergoing open NSS at our institution. At a mean of 10 months follow-up, no patients have had a recurrence, and no patient has had a decrease in his GFR of more than 20% (mean 10%).
Our cohort of patients had similar renal functional and oncologic outcomes compared with the previously listed studies; however, in contrast to those studies, we did not experience any major or minor complications. This could be attributed to the limited number of patients in the cohort, but we believe this to be a function of surgical approach, because we performed our procedures with RAPN while the other series performed OPN in almost all of their cases. We preferred RAPN because it allowed for magnified visualization of the renal hilum and precise dissection along the major renal vessels. Although still technically challenging because of fibrosis and scar tissue from the previous procedures and lack of tactile feedback, this magnification along with precision of surgical instruments were critical in avoiding renal vascular injury and facilitated our ability to successfully complete the procedures.
Another possible explanation for our low complication rate could be renal mass selection, with our patients having less complex lesions than those in the studies listed above. Although we did not have any patients with multiple renal lesions as was reported by Johnson and coworkers, 17 four of the five patients in our series had mainly endophytic and/or posterior lesions (represented in Fig. 1), which are typically considered more complicated with respect to a laparoscopic approach.
Each of the cases in our present series offered significant insight into the technical aspects of RAPN in renal units that had previously undergone NSS. These types of cases can be very challenging and are best approached by a surgeon with significant experience in both laparoscopic and RAPN. We also recommend using a variety of technologic tools to facilitate the successful completion of these surgeries. The use of intraoperative ultrasonography can be critical not only for accurate location and subsequent exposure of tumors, but also for identification of hilar vessels during dissection, especially when encountering significant fibrosis and scarring from previous procedures.
Our study is not without limitations. The retrospective nature of our review and small sample size will limit the generalizability of the study. The main purpose of our report, however, was to report the feasibility of this procedure. Based on our current series, we believe that a previous, ipsilateral renal surgery, open or laparoscopic, should not be a contraindication for a minimally invasive PN because we have demonstrated that RAPN is feasible, safe, and can provide excellent intermediate oncologic outcomes.
Conclusion
RAPN after previous open or laparoscopic PN is a challenging and potentially complication prone procedure. With the use of intraoperative ultrasonography and precise surgical equipment and technique, this procedure is also safe and efficacious, and offers satisfactory intermediate functional and oncologic outcomes with minimal morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.