
Abstract
Background and Purpose:
Ureteral stents are being used exceedingly in the field of urology, and with advancements in endourology, this trend is increasing. Bacterial colonization and proliferation on the stent surface may result in urinary tract infections (UTIs) necessitating the administration of antibiotics that, in turn, may lead to the development of antibiotic-resistant bacterial strains. Several studies have shown that sustained release varnish (SRV) combined with antibiotics or antiseptics can prevent the proliferation of bacteria on urethral catheters. This is the first study that evaluates this technique implemented on ureteral stents.
Materials and Methods:
We evaluated growth inhibition on ureteral stent segments coated with chlorhexidine (CHX) 1% SRV. The tests were conducted using common urinary pathogens: Enterococci, Pseudomonas, and Escherichia coli. Coated stent segments were inserted into bacterial suspensions. Controls included uncoated stent segments and stents coated with placebo SRV (without CHX).
Results:
Bacterial growth measured as turbidity and as colony-forming units showed a significant inhibition effect of initial bacteria adhesion to the CHX-SRV coated stent segments compared with the controls (P<0.001). This inhibitory effect was apparent in each of the bacteria tested and was confirmed by inspection of the stent segments under an electron microscope. In a kinetic experiment using CHX 2% SRV, we were able to prolong the growth inhibition effect from 1 week to nearly 2 weeks.
Conclusions:
We believe this technique may play a significant role in reducing ureteral stent-associated UTIs. Further studies are needed before this approach can be implemented in clinical practice.
Introduction
After insertion of a ureteral stent, it is rapidly coated by proteins, minerals, polysaccharides, and other urine components enabling attachment and proliferation of bacteria on its surface. 1 Attachment and proliferation of bacteria on the stent surface plays an important role in stent encrustation and stent-related urinary tract infection (UTI). 2
The most common bacteria causing UTI are gram-negative organisms—mainly Escherichia coli (E coli) and Pseudomonas species and other gram-positive enterococci. 2
Prophylactic antimicrobial treatment reduces the incidence of UTI, yet frequent antibiotic use results in antibiotic-resistant bacteria.
Various impregnations of urethral catheters have been used in an attempt to prevent catheter-associated infections. These include several types of antibiotics and antiseptic agents such as rifampicin and minocycline, 3 silver salt, 4 triclosan, 5 nitrofurazone, 6 gendine, 7 combination of chlorhexidine (CHX) and protamine sulphate, 8 CHX and triclosan. 9
Several studies have shown that bacterial accumulation on catheters can be prevented by coating the catheter with sustained release varnish (SRV) combined with antibiotics or antiseptics, resulting in a sustained release of the drug enabling a prolonged effect. This technology has been tested on several medical applications. 8 –10
Our previous study has shown this technique to be effective on urethral catheters 8,9,11 ; therefore, we hypothesized a similar beneficial effect on ureteral stents. In our current study, we used CHX, an effective agent used routinely as a medical antiseptic agent. We tested the in vitro effect of CHX-SRV on initial attachment and proliferation of Pseudomonas, E coli, and enterococci on ureteral stents. The inner and outer surfaces of these stents were examined after coating using electron microscopy.
Materials and Methods
Biofilm model
One centimeter segments of ureteral stents (C-flex,® Cook Medical Inc, Bloomington, IN) were immersed in a 70% alcohol solution for 1 hour, dried, and then coated with the CHX-SRV and allowed to dry at room air.
The amount of CHX-SRV was calculated by weighing the stent segment before and after coating with the CHX-SRV. In this study, we compared placebo varnish (coating without CHX) with CHX-SRV. Positive controls were uncoated stent segments incubated in growth media solutions (tryptic soy broth/brain-heart infusion broth [TSB/BHI]) containing each of the three bacteria. Negative controls were stents incubated in TSB and BHI solutions without bacteria.
All samples were incubated in test tubes containing bacteria in growth media for 48 hours at 37°C. After incubation, the samples were removed and washed three times with a phosphate-buffered saline (PBS) solution for removal of bacteria loosely attached to the stent segments. Next, the samples were transferred into 2 mL of PBS where they underwent sonication in a water bath for 15 minutes. The optical density (OD) of the sonication fluid was measured using a spectrophotometer at a wavelength of 600 nm. The sonication fluid was then sequentially diluted and cultured on BHI agar plates for 24 hours at 37°C after which the number of colony-forming units (CFU) was counted. Each experiment was repeated five times.
Varnish preparation
The SRV was formulated according to Shapur and associates. 11 The SRV is composed of ethyl cellulose (5 g), polyethylene glycol 400, Klucel® EF (4 g), and CHX diacetate dissolved in 100 mL of ethanol in concentrations of CHX: 1% or 2%.
Bacteria
In this study, we used three common bacteria causing UTI. These include Pseudomonas aeruginosa (PA), E coli, and Enterococcus faecalis. The bacteria were incubated in TSB or BHI for 24 hours at 37°C before being used.
Kinetics experiments
Stent segments coated with CHX varnish 1% or 2% were inserted into test tubes containing culture media (BHI/TSB) and bacteria. Positive and negative controls we used as described previously.
After incubation of 48 hours at 37°C, the tubes were assessed for turbidity. The solution containing culture media and bacteria was replaced every 48 hours. This process was repeated until the development of turbidity indicating bacterial growth.
Scanning electron microscopy (SEM)
The stent segments were dried in room air and placed in a palladium-gold 10 nm spraying chamber. Samples were examined using SEM (Sirion high resolution scanning electron microscope) at magnifications of 1500 performed 10,000.
Statistical analysis
Statistical analysis was done using a Student t test. A P value<0.05 was considered statistically significant.
Results
Bacterial analysis
Results of OD and CFU tests indicated an association between the presence of CHX in the varnish and bacterial (biofilm) growth inhibition (Fig. 1). Bacterial growth inhibition was demonstrated in test tubes containing stent segments coated with CHX-SRV compared with test tubes containing placebo SRV coated stent segments. Growth of bacteria as planktonic in the stent-coated samples was found to be (OD 595): E coli – 0.345, PA – 0.296, E faecalis – 0.347.

A comparison of colony forming unit counts in chlorhexidine (CHX)-sustained release varnish, placebo, and positive control of the three types of microorganisms. E faecalis=Enterococcus faecalis; E coli=Escherichia coli; P aeruginosa=Pseudomonas aeruginosa.
When comparing bacterial levels on the coated stents with CHX-SRV with placebo and positive control stents, we found a significant reduction in bacterial count in all three types of bacteria (P<0.001). We did not find a significant difference in reduction of bacterial count in all three types of microorganisms comparing positive control stents with the placebo arm. (PA: P=0.46; E coli: P=0.76, Enterococcus: P=0.38).
SEM
SEM of a bare stent revealed a smooth curved surface area (Fig. 2a). Examination of a varnish-coated stent showed the varnish evenly coating the outer surface of the stents, as well as a small area of its internal aspect, near the edges and through the minor pores (Fig. 2b). In the positive control samples with no SRV-CHX, one could see bacteria colonizing in small groups adhering to the stent (Figs. 2c, 2d). In the placebo-coated samples, small groups of bacteria were visible within the pores (Fig. 3: a. E coli; b. PA; c. Enterococcus) compared with samples coated with CHX-SRV where very little colonized groups of bacteria were observed (Figs. 3d, 3e).

Scanning electron microscopy (×2500):
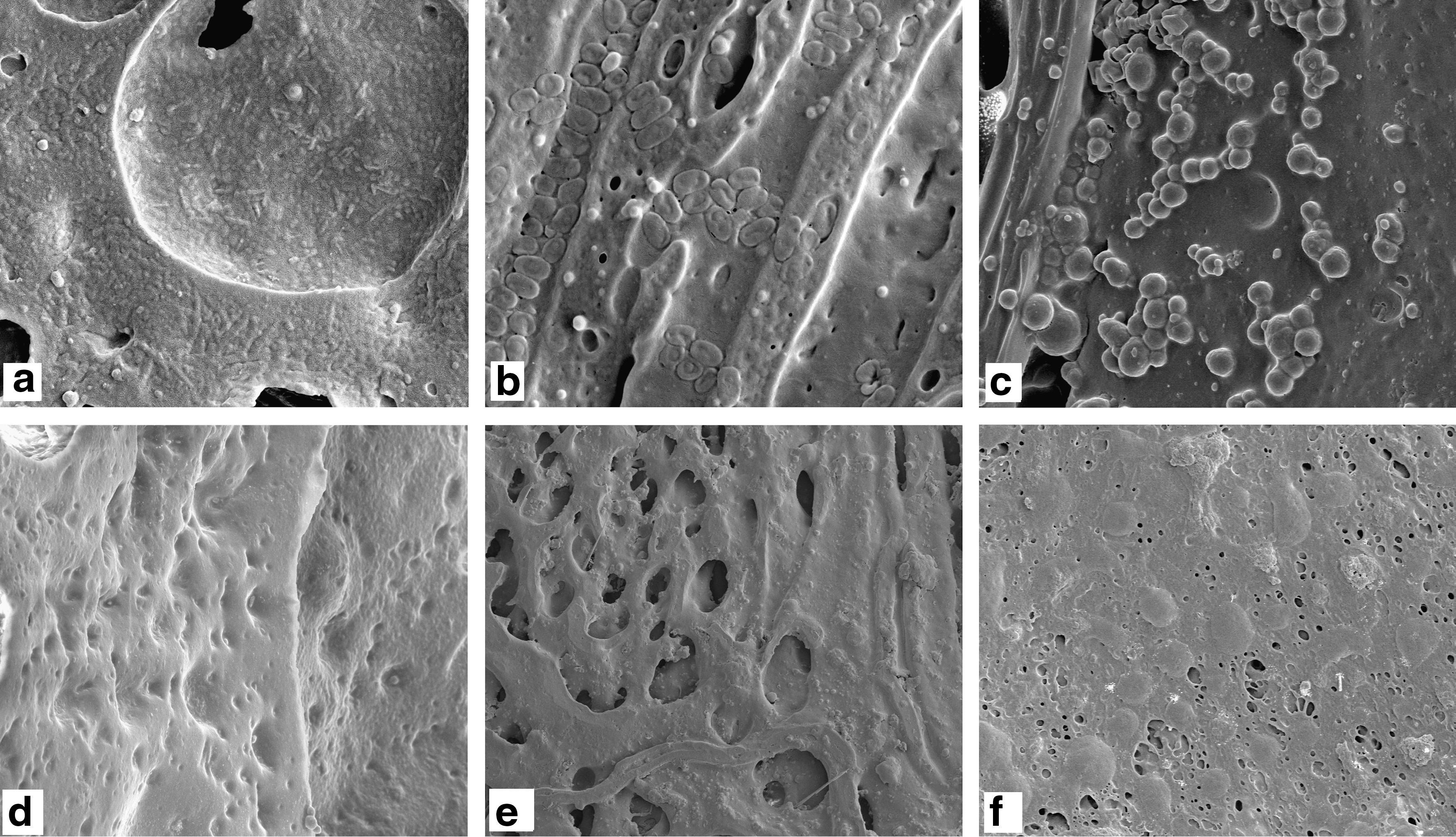
Scanning electron microscopy pictures demonstrating bacteria adhering to the stent surface in the placebo arm.
Kinetic experiment
The kinetics experiments showed that stents coated with CHX varnish 1% delayed bacterial growth for about 1 week in all three tested types of microorganisms (Table 1). The use of CHX varnish 2% resulted in a 2-week inhibition of bacterial growth.
P aeruginosa=Pseudomonas aeruginosa; E coli=Escherichia coli; E faecalis=Enterococcus faecalis; CHX=chlorhexidine.
Discussion
Insertion of ureteral stents is common practice in urology and is frequently associated with patient inconvenience and increased incidence of UTIs. 2,12 Bacterial proliferation and stent-related UTI result in patient morbidity and stent encrustation. 13,14
This process begins with bacteria contaminating the urine, attaching and proliferating on the stent surface. 15 First, the bacteria form an initial monolayer on the stentssurface; next they propagate and form colonies covered by an extracellular polysaccharide layer. Biofilm formation is a multistage process starting with initial bacteria adhesion to the stent surface followed by proliferation. 16,17 In this study, we evaluated the prevention of the first step by coating the stent with a CHX-SRV. Clearly, early colonization of bacteria in the initial stages of biofilm formation is an important step in the process of biofilm maturation.
Bacteria present in the biofilm coating the stent are unique because of their reduced sensitivity to antibacterial therapy compared with planktonic bacteria within the urine. 18 This finding is because of an additional defense mechanism consisting of a polysaccharide layer preventing the diffusion of antibiotics into the deep layers of the biofilm coating the stent. 19
Coating the stents with a SRV results in a high concentration of the antibacterial drug on its surface. Sustained, controlled release ensures a prolonged effect of the drug in the vicinity of the biofilm, thus enabling an improved antimicrobial effect on bacteria adhered to the stent. 10,20
Numerous techniques have been proposed to reduce biofilm formation on urethral catheters and on ureteral stents. 21 –26 SRV technology offers several advantages stemming from a sustained, controlled release of the drug, prolonged therapeutic effect on the biofilm, and reduced local and systemic side effect.
In our study, we evaluated the effect of a CHX-SRV coat on the initial stages of biofilm formation on ureteral stents. SRV technology combined with CHX, or other active agents, has been tested and proven to be effective in the field of dentistry 10 and lately also in an in vitro study on catethers. 11 Our study is the first to evaluate the effectiveness of this technique in the field of urology for the prevention of biofilm formation on ureteral stents. By modifying the SRV formulation, one can control the rate of release of the drug as well as its concentration around the stent.
The active agent we chose, CHX, is a well-known broad-spectrum antiseptic agent. This agent does not interact with the varnish components, which enables a sustained and controlled release of the agent in its active form.
Our results show that the CHX-SRV reduces significantly the amount of bacterial accumulation on the stent surface. The mode of action of the CHX-SRV was as an antibiofilm and not just as antibacteria, because bacteria were to be found in the supernatant fluid of the immersed coated stents. The microbiologic assays were supported by the SEM image analysis that demonstrated almost no bacterial colonization on the surface area of stents coated with CHX-SRV.
In the kinetics experiments, the antibiofilm effect was diminished after about a week, indicating that the CHX was effective only during that time. The effect is based on a dose-response mechanism because the antibiofilm effect was prolonged to about 2 weeks when the concentration of CHX was increased from 1% to 2%.
Modification of the SRV formulation combined with an increased concentration of CHX can prolong the duration of effect on biofilm formation. Reducing the viscosity of the SRV might enable a better penetration of the varnish into the stent lumen and coating the internal surface.
Further studies are needed to evaluate the effect of the SRV coat on the stent draining ability and kinetic characteristics as well as the effect of the active agent on human tissue. It is important to emphasize that in this study we evaluated a technology of SRV in prevention of biofilm on stents. The SRV is a pharmaceutical platform of delivering drugs in a sustained, controlled fashion. Other antibacterial, antiseptic, or cytotoxic agents can be combined into the varnish and be used in the field of urology.
Footnotes
Disclosure Statement
No competing financial interests exist.