
Abstract
Background and Purpose:
Extended warm ischemia time during partial nephrectomy leads to considerable renal injury. Using a rat model of renal ischemia, we examined the ability of a unique renoprotective cocktail to ameliorate warm ischemia-reperfusion injury and extend warm ischemia time.
Materials and Methods:
A warm renal ischemia model was developed using Sprague–Dawley rats, clamping the left renal artery for 40, 50, 60, and 70 minutes, followed by 48 hours of reperfusion. An improved renoprotective cocktail referred to as I-GPM (a mixture of specific renoprotective growth factors, porphyrins, and mitochondria-protecting amino acids) was administered −24 hours, 0 hours, and +24 hours after surgery. At 48 hours, both kidneys were harvested and examined with hematoxylin and eosin and periodic acid-Schiff stains for the analysis of renal tubular necrosis. Creatinine, protein, and gene expression levels were also analyzed to evaluate several ischemia-specific and antioxidant response markers.
Results:
I-GPM treated kidneys showed significant reversal of morphologic changes and a significant reduction in specific ischemic markers lipocalin-2, galectin-3, GRP-78, and HMGB1 compared with ischemic controls. These experiments also showed an upregulation of the stress response protein, heat shock protein (HSP)-70, as well as the phosphorylated active form of the transcription factor, heat shock factor (HSF)-1. In addition, quantitative RT-PCR analyses revealed a robust upregulation of several antioxidant pathway response genes in I-GPM treated animals.
Conclusions:
By histopathologic and several molecular measures, our unique renoprotective cocktail mitigated ischemia-reperfusion injury. Our cocktail minimized oxidative stress in an ischemic kidney rat model while at the same time protecting the global parenchymal function during extended periods of ischemia.
Introduction
Our laboratory has developed a unique renoprotective cocktail called GPM that consists of several renoprotective growth factors (G), porphyrins (P), and mitochondria protective amino acids (M), and we have previously shown that this cocktail mitigated I/R injury in a rat model of renal ischemia at 40 minutes. 12
In the current study, we test whether an improved renal protective cocktail (referred to as I-GPM), can extend WIT up to 70 minutes in a rat model of renal ischemia, while still preserving renal parenchymal function.
Materials and Methods
Our improved renoprotective cocktail contained growth factor (G) components, mitochondrial-targeting porphyrins (P), and supplemental mitochondrial-protective amino acids (M), including erythropoietin (EPO) and
Obtained from Invitrogen, Inc.
Obtained from ProSci, Inc.
Obtained from Gibco.
Gift from Dr. Ines Batinic-Haberle at Duke University.
Purchased from Sigma-Aldrich, Inc.
G components given at 50 ng/kg of rat weight/d; P components given at 100 μg/kg/d; M components as well as glutamine, N-acetyl cysteine, N-acetyl carnitine, α-lipoic acid were given at 150 μmol/kg/d. Collectively, this mixture is called I-GPM. All injections were in a final volume of 0.4 mL of sterile saline and given intramuscularly (0.20 mL) and intraperitoneally (0.20 mL).
A renal ischemia model was developed and applied in 72 Sprague-Dawley rats randomized into nine groups (n=8 per group) (group 1=sham, no ischemia with saline only; groups 2–5=ischemia with saline at 40, 50, 60, and 70 minutes; groups 6–9=ischemia with I-GPM at 40, 50, 60, and 70 minutes). Renal ischemia was followed by 48 hours of reperfusion (Fig. 1). Our surgical technique has been described previously. 12 Microserrifine clamps (Fine Science Tools, Inc) for small animals were used to clamp the renal hilum en-bloc.
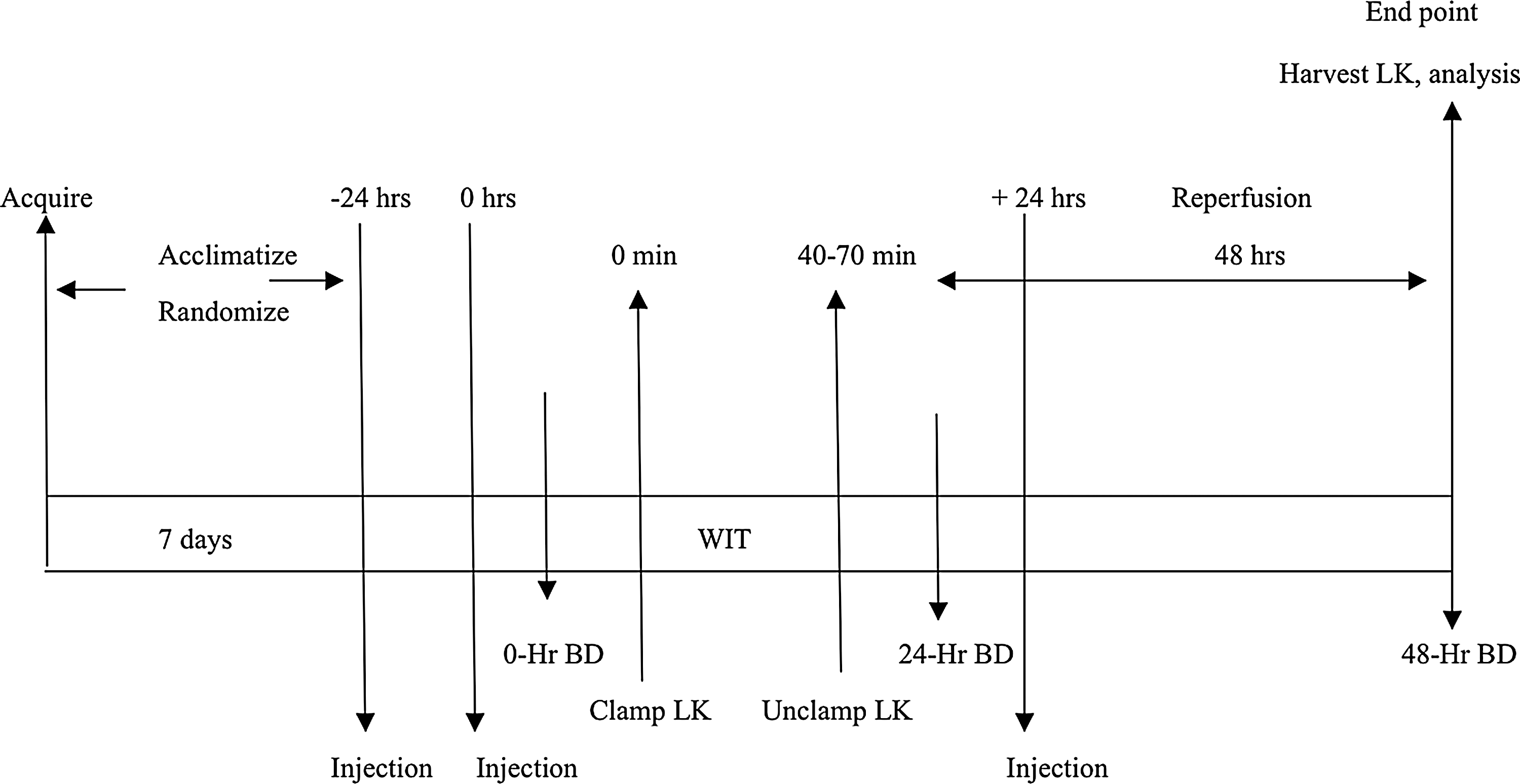
Experimental design of rat renal ischemia model. LK=left kidney; BD=blood draw; WIT=warm ischemia time.
The I-GPM renoprotective cocktail was given intramuscularly and intraperitoneally at −24, 0, and +24 hours after surgery. We chose to include a +24 hour dose to minimize the effects of oxidative stress mediated by I/R that occurs postoperatively. In this setting, the −24 and 0 hour doses can be seen as preconditioning the animals to protect them from the oxidative stress that occurs at the time of surgery, and the +24 hour dose as a booster to help the animals cope with continuing stress after surgery.
At 48 hours, both the left and right kidneys were harvested and examined in a blinded fashion. All the animal work was performed in accordance with and after the approval of the animal care and use committee established by the Institute of Comparative Medicine at New York Medical College. Our specimen handling was as described previously. Ten high-power fields (magnification 10× and 40×) were examined per each rat kidney in a blinded fashion by a certified pathologist after hematoxylin and eosin (H&E) staining. Medullary tubular damage/necrosis was graded as follows: 0=none, 1=≤10%, 2=11%–25%, 3=26%–45%, 4=46%–75%, and 5=≥76% based on morphologic changes of tubular necrosis as described in an authoritative article by Hammerschmidt and associates. 13 Western blot analysis was used to identify specific markers of renal ischemia. These included galectin-3, lipacalin-2, and high mobility group B1 protein (HMGB1). 14 –16 Real-time quantitative polymerase chain reaction (PCR) techniques were used to detect oxidative stress genes, including glutathione peroxidase, peroxyredoxins, and superoxide dismutase. Results are expressed as means±standard error of the mean, analyzed using the Student t test. A value of P<0.05 was considered statistically significant.
Results
Table 2 shows serum creatinine levels at end point. We observed a gradual increase in this widely accepted serum marker of overall kidney function when the animals were treated with increasing ischemia times, ranging from 40 to 70 minutes. I-GPM treated animals showed an impressive reduction in creatinine levels compared with controls (P<0.05).
=P<0.05.
SEM=standard error of the mean; I-GPM=improved growth factor, porphyrins, and mitochondrial protective amino acids.
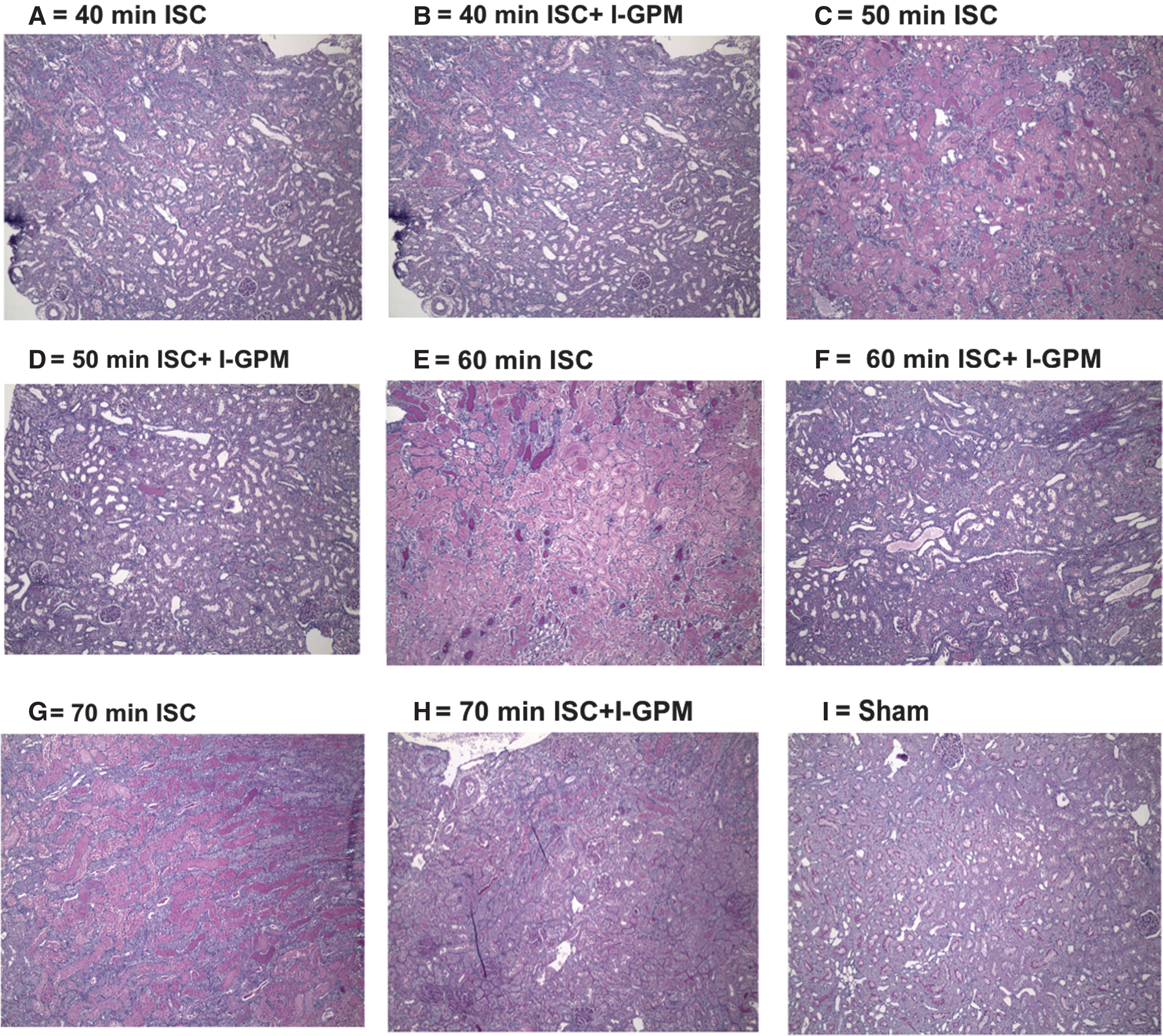
H&E staining of kidney tissue sections from the ischemia-only group revealed levels of renal tubular damage proportional to the ischemic duration, consistently showing an ischemia score of 5 at 70 minutes. In contrast, animals preconditioned with the I-GPM cocktail showed varying degrees of renoprotection, demonstrating the lowest tubular damage score at 70 minutes (Fig. 2).
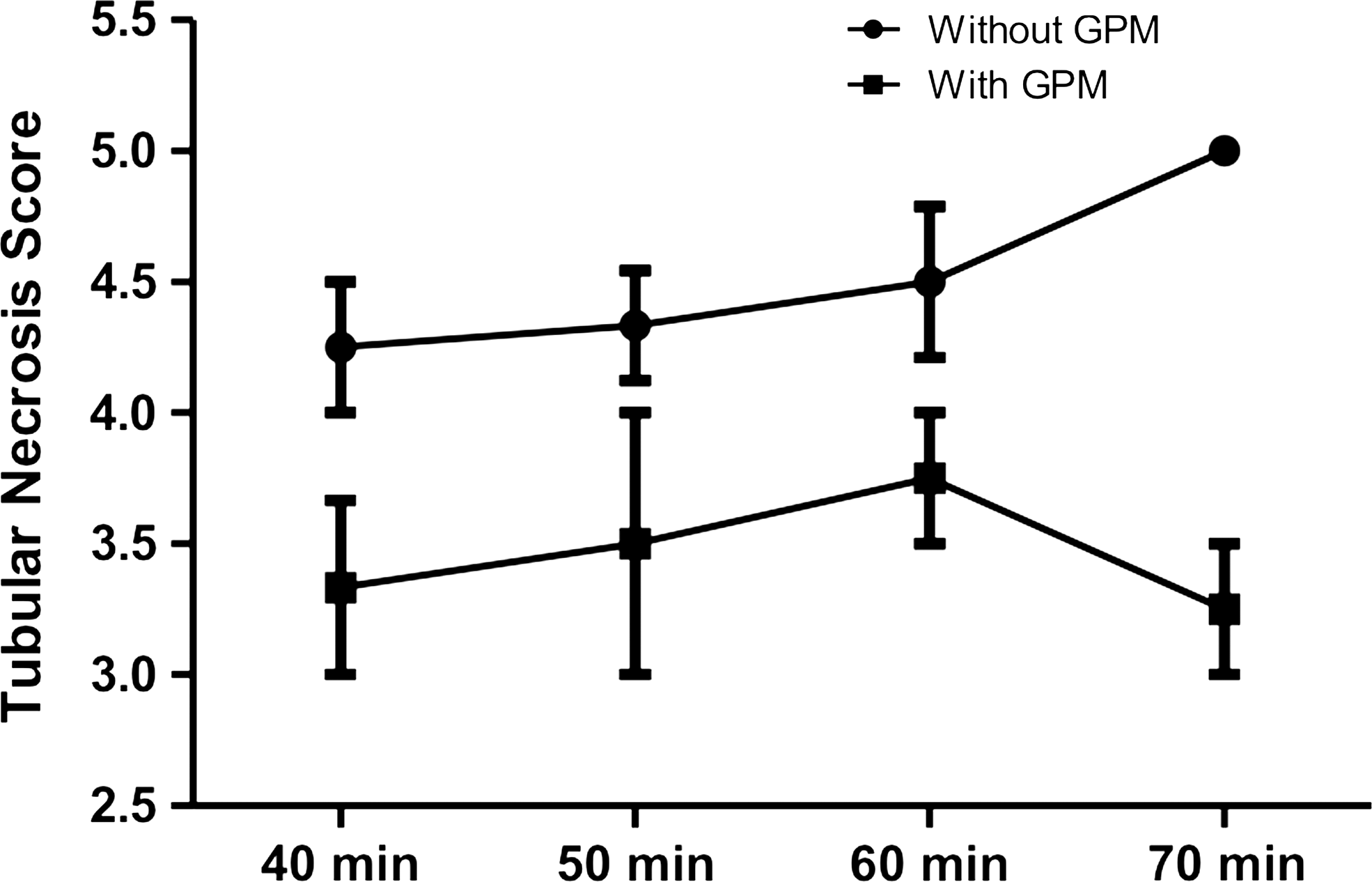
Statistically significant decrease in acute tubular necrosis seen in the ischemic left kidney treated with I-GPM compared with ischemic controls. Statistical analysis performed using a two-tailed Student t test; P<0.05. GPM=growth factors, porphyrins, and mitochondrial-protective amino acids.
Figure 3 demonstrates periodic acid-Schiff stains of selected kidneys. Whereas the ischemia-only animals showed increasing levels of epithelial cell degeneration, significant necrosis, luminal clogging, loss of brush borders, and cast formation, these pathologic changes are attenuated significantly in the I-GPM treated animals for the same ischemia periods (P<0.005).
The immunoblots in Figure 4 depict significant reduction in the levels of three independent tissue ischemia markers (galectin-3, lipacalin-2, and HMGB1), as well as upregulation of two oxidative stress genes (heat shock protein-70 [HSP-70] and phosphorylated heat shock factor-1 [pHSF-1]) in rat kidneys treated with I-GPM. Expressed levels of the housekeeping protein β-actin were used for protein normalization purposes.
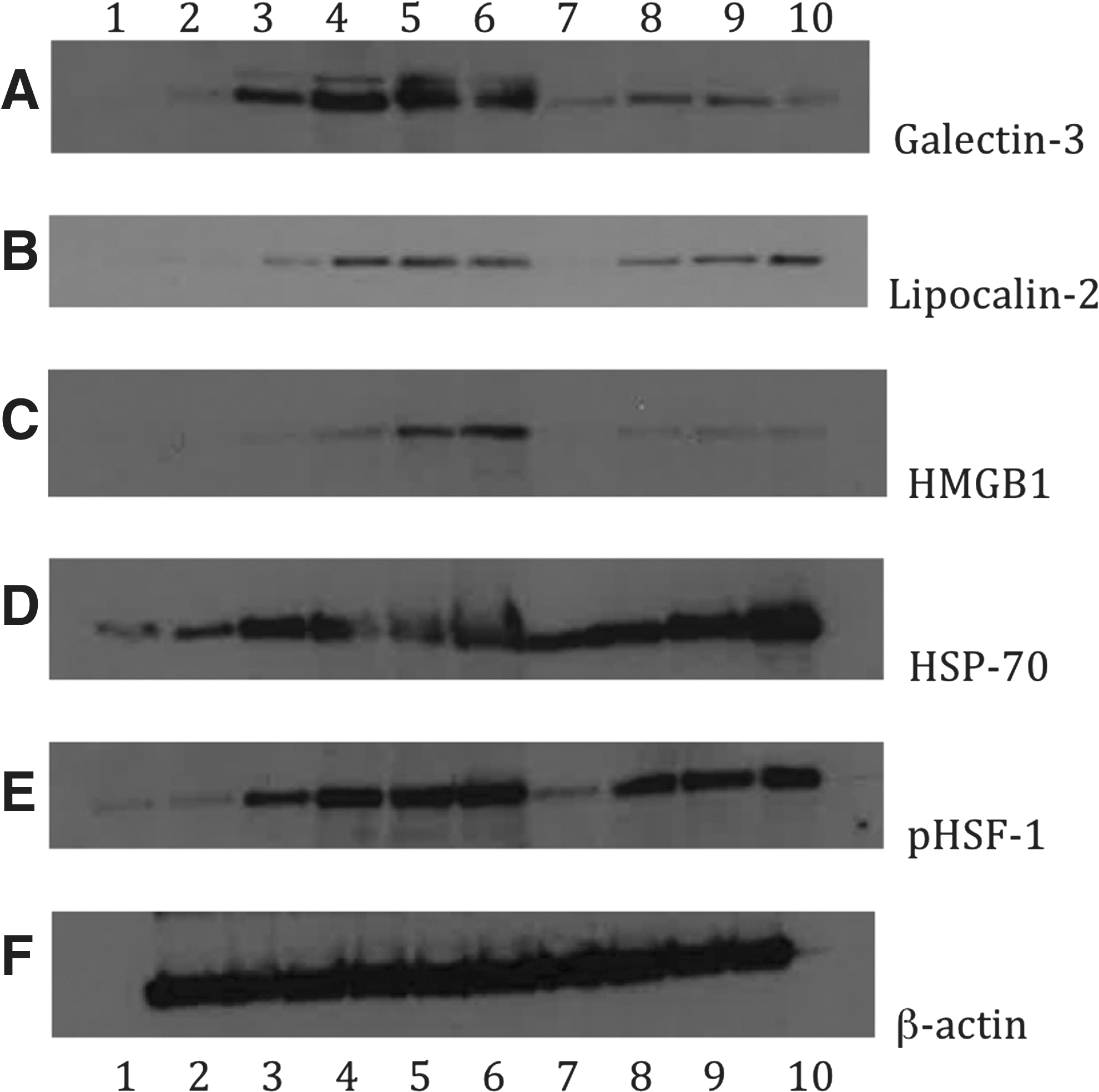
Immunoblotting analysis of ischemia-specific markers galectin-3 (A); lipocalin-2 (B); HMGB1 (C); and HSP-70 (D), phosphorylated HSF-1 (E), and β-actin (F) as the housekeeping protein loading control. Lanes 1, 2: Sham operated left kidneys; lanes 3–6: ischemic left kidney (ischemia only for 40, 50, 60, and 70 minutes, respectively) at end point; lanes 7–10: ischemic left kidneys treated with I-GPM for 40, 50, 60, and 70 minutes ischemia.
Quantitative reverse transcription PCR analysis demonstrated upregulation of several characteristic oxidative stress genes (including glutathione peroxidase, lactoperoxidase, inducible nitric oxide synthetase, etc.) and antioxidant response genes (including superoxide dismutase, thioredoxin reductase 1, and a set of peroxyredoxins) in response to treatment with I-GPM. Qualitatively, the set of oxidant and antioxidant genes that were upregulated strongly correlate with the results obtain in our earlier study, where ischemia was terminated at 40 minutes. Quantitatively, the degree of upregulation of the antioxidant response genes was more robust that in our previously published results, suggesting a very strong antioxidant response in ischemic tissue treated with I-GPM (data not shown).
Discussion
In the present study, we explored the pathologic and biochemical features of ischemic changes titrated with respect to time, testing the ability of the I-GPM cocktail to protect against ischemic lesions and extend WIT beyond 40 minutes.
Our I-GPM cocktail contains growth factors and morphogens designed to support the mitochondria under conditions of severe oxidative stress. The work of Villanueva and associates 17 indicated that during I/R, the kidney expresses a set of genes and proteins closely resembling embryonic kidney development markers, including basic fibroblast growth factor (bFGF), bone morphogenic protein-7 (BMP-7), and vascular endothelial growth factor (VEGF). 17 Among these proteins, bFGF participates in early kidney development as a morphogen and is expressed in the recovery phase of I/R injury. 18 After I/R injury, the kidney is also known to upregulate stromal cell derived factor-1 (SDF-1), which mobilizes bone marrow derived cells into the circulation to repopulate and repair damaged renal tissue. 19,20 For these reasons, we included bFGF, BMP-7, SDF-1, VEGF in our new renoprotective cocktail.
We supplemented our cocktail with hypoxia-specific gene products—namely, EPO, which has demonstrated a protective effect in a murine acute renal failure model. 21 EPO has been shown to confer significant protective effects on the kidney, possibly because of the positive feedback loop by which EPO itself upregulated the expression of hypoxia inducible factor-1α under hypoxic conditions. 14 –16
Early works of MacMillan-Crow and her coworkers 24,25 have suggested that loss of mitochondrial antioxidant protection (including inactivation of mitochondrial enzyme manganese superoxide dismutase, MnSOD) might play an important role in renal injury after I/R. Subsequently, Saba and colleagues 26 have shown that there was a therapeutic benefit of using the catalytic antioxidant Mn-porphyrin (MnTnHex-2-PyP5+) in animal models of oxidative stress injury. Their work showed that porphyrin derivatives administered to rats 24 hours before surgery protected the animals against adenosine triphosphate (ATP) depletion, nitration of tyrosine residues in proteins, MnSOD inactivation, and renal dysfunction. This porphyrin derivative, “P” in our cocktail, specifically accumulates in the mitochondria because of its higher lipophilicity, where it prevents the inactivation of SOD, which occurs under oxidative stress. 27
Fourth, our cocktail included a set of amino acids (“M”) known to protect the mitochondria from the excess reactive oxygen species generated along the electron-transport chain because of sudden oxygen loss. Weinberg and coworkers
28,29
showed that mitochondrial dysfunction could be prevented by the use of specific citric acid cycle intermediates, such as a mixture of α-ketoglutarate,
Finally, we incorporated
Very recent studies have shown that glutamine induces HSP-70 expression via N-acetylglucosamine modification and subsequent increased expression and transcriptional activity of HSF-1, particularly by increasing the levels of pHSF-1. 37 –39 The increased levels of HSP-70 and pHSF-1 we observed (Fig. 4, D, E) strongly support the protective mechanisms of glutamine. Increased WIT in the presence of the renoprotective cocktail elicits a higher level of expression of HSP-70 and the transcriptional activity of pHSF-1, helping explain why we observed a higher level of renoprotection at 70 minutes as opposed to 50 or 60 minutes. This is likely because of the higher level of ischemic damage eliciting a higher heat shock response. Our study highlights the novel aspects of mitochondria protecting amino acids and the role of a cytoprotective heat shock response built in the design of our strategy.
Conclusion
Our results support our earlier hypothesis that empowering and protecting the mitochondria during I/R injury and eliciting a robust cytoprotective response may be key to reversing ischemic damage during WIT. We are aware that these animal models only approximate human physiology and their response to renal injury and mechanisms of recovery may be different from human pathophysiology. 40 Nevertheless, our renoprotective cocktail may help in extending the WIT while at the same time preserving the global parenchymal function of the kidney during artery occluding procedures, warranting further work.
Footnotes
Acknowledgments
Support from the Susan Schott Memorial Fund and the St. Vincents Urology Research Fund is gratefully acknowledged.
Disclosure Statement
No competing financial interests exist.